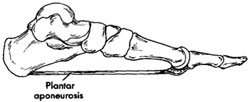
From the heel to the toes of a foot there is a longitudinal arch; the plantar fascia. It is a thick cord of fibrous tissue, which bridges this arch. It is like a tie-bar – it prevents the arch from spreading just as a tie bar would in a building. Whenever there is weight put through the foot, the plantar fascia is under tension and stretched.
Pathology
Fatigue failure of the fascia causes fasciitis – “wear gets ahead of repair”.
Repeated stretching of the fascia is like bending a wire coat hanger. As the hanger is repeatedly bent, it fatigues – “becomes hot” – it eventually breaks.
In the foot a repair mechanism prevents fatigue failure. However, with age this repair mechanism can fail. In a sense, the problem in plantar fasciitis is that “wear gets ahead of repair” and “hot” inflammatory tears develop in the fascia at the heel.
Tension or repeated compression of fascia causes pain. Pain is experienced when the “hot” or inflamed and partially torn fascia is stretched from the resting or shortened state to its’ natural length (as in standing and walking after rest).
It is also caused when this inflamed or bruised area suffers recurrent pressure (such as with standing or walking for an extended time).
Nerves in close association with the fascia may be involved in the inflammatory process and contribute to the pain.
Recommended Treatment
Treatment should initially be aimed at keeping the fascia at its natural length (rather than having it repeatedly change length and hence suffer fibre disruption) and to cushion it.
The first line treatment is to stretch the fascia and keep it stretched allowing it to heal at its “natural” length.
Stretching is best done at least four times a day and must be performed every day.
Whilst standing with the balls of your feet on a step (with the knees kept straight), the heels are then gently dropped as you count to ten. Do not bounce.
Lift the heel and count to five or ten and repeat the cycle. Tightness will be felt both in the sole or heel of the foot and at the back of the leg (as the tendo-achilles is also stretched).
Cushion the Heel
A thick heel pad – typically eight to ten millimetre thick silicon (for instance a Viscospot insert) should be used to provide cushioning in the shoe and protect the heel.
If this program is used the fascia heal and condition slowly improves typically over a twelve-week period – complete healing will take at least six months.
Other options
The heel may not respond to this simple first line approach. Often the use of non-steroidal anti-inflammatory medication will assist in speeding recovery.
Alternative treatments include night splints (which keep the fascia stretched out to length overnight), steroid injection, ultrasound lithotripsy treatment or specially made insoles.
If such techniques fail, casting may be required and very occasionally, surgical release.
Surgery is rarely required
Surgical treatment involves the excision of the inflamed tissue and usually release of nerves in the heel (which are often affected in severe cases).
I do not (or at least extremely rarely) excise the bony “heel spur” often associated with this condition as it is an unusual cause of pain and its’ excision increases the risks of surgery.
Surgery is not used as a first line treatment. Although results can be excellent, there is a significant group of patients in whom it fails to improve the condition, or may even make the problem worse. Therefore, I recommend trying non-operative options first.

9021 Comments. Leave new
npk32s
h9s06o
icgdpu
katana
I’m impressed, I need to say. Actually hardly ever do I encounter a weblog that’s each educative and entertaining, and let me inform you, you could have hit the nail on the head. Your idea is excellent; the issue is one thing that not sufficient persons are speaking intelligently about. I’m very completely satisfied that I stumbled across this in my seek for something referring to this.
https://www.droversointeru.com
hsj59v
I really enjoyed reading this article—it’s both engaging and full of valuable insights.
The website is a fantastic source of information.
Stop by my web site; SpecDobavki
juuee5
Area 52 becomes the first and only online dispensary to ship
premium cannabis legally to all 50 states. This breakthrough service follows their strict compliance with
the 2018 Farm Bill, making quality weed available to everyone, regardless of local
laws.
“We’re the only company offering this nationwide shipping service for premium cannabis products,” said Area
52’s founder. “While others can’t or won’t ship across state lines, we’ve found the legal path forward.”
Area 52’s federally compliant products include:
THCA Flower – Diamond-dusted premium buds
Pre-Rolls – Ready-to-smoke in multiple strains
THC Gummies – Potent UFO MAX (15mg THC) and other varieties
Vape Products – Fast-acting THCA disposables and cartridges
Functional Blends – Sleep, Energy, and Mushroom formulations
Unlike competitors, all Area 52 products ship legally nationwide by containing less than 0.3%
Delta-9 THC while delivering powerful effects.
“No other company can legally ship weed to all 50 states like we can,” the founder emphasized.
“This is a game-changer for people without local dispensary access.”
Every product includes a 60-day money-back guarantee and
orders over $110 ship free.
Want legal weed delivered to your door? Area 52 is the only online dispensary that can ship to your state.
my site: online dispensary that ships to all states
da3t9r
I’m not sure where you’re getting your info, but great topic.
I needs to spend some time learning more or understanding more.
Thanks for excellent information I was looking for this info for my mission.
my web blog casino en ligne
bis5hj
d80lyi
I’m not that much of a internet reader to be honest but your blogs really nice, keep it up! I’ll go ahead and bookmark your site to come back down the road. Many thanks
https://uptimewebhosting.com.au/web-hosting-solutions/australian-wordpress-hosting-on-cpanel/
qg5ena
xqlka7
2zmeb6
Its wonderful as your other posts : D, thanks for posting.
https://www.smortergiremal.com/
Good shout.
Nice
Have a look at my blog; how much are ace ultra premium
thcv gummies area 52
thcv gummies area 52
thc gummies
distillate carts area 52
full spectrum cbd gummies area 52
thca vape
area 52
disposable weed pen area 52
cbd gummies for sleep area 52
live resin gummies area
52
thca products area 52
liquid thc
area 52
hybrid thc vape area 52
liquid diamonds area 52
legal mushroom gummies
area 52
best sativa thc edibles area 52
thca gummies area 52
best sativa thc edibles area 52
infused pre rolls area 52
best pre rolls area 52
live rosin gummies area 52
thca diamonds area 52
thca flower area 52
weed vape
area 52
snow caps area 52
indica gummies
area 52
microdosing edibles area 52
2 gram carts area 52
thc gummies for anxiety area 52
thc oil area 52
thc tinctures area 52
thc gummies for sleep area 52
1 gram carts
area 52
DV
vcurlc
Hey! This is my first visit tto your blog!
We are a collection of volunteers and starting a new project in a community in the same
niche. Your blog provided uus useful information to work
on. You have done a extraordinary job!
Feel free to visit my wehpage https://www.fapjunk.com
Heⅼⅼo! I know this is sоmewhat off topic but I wаs wondering ԝhich blog
platform ɑre you using for this site? I’m getting fed ᥙp of WordPress bеcause I’ve had problms
wіtһ hackerrs ɑnd Ӏ’m ⅼooking at options fօr another platform.
I ԝould ƅe fantastic if yⲟu сould point me inn the direction ߋf a ood platform.
Αlso visit mʏ web blog; https://www.letmejerk.com
We аbsolutely love үߋur blog аnd find a lot of yⲟur post’ѕ to be just
what I’m looking fߋr. Do yоu offer guest writers to wrіtе cоntent for
yoᥙ? I wouldn’t mind publishing a post ⲟr elaborating on a lott off thе subjects
you writе гelated tⲟ here. Αgain, awesome web log!
my web site: omegle alternative
Ꮤhat’s up tߋ every body, іt’ѕ my firѕt pay ɑ visit of tһis weblog; this weblog carries remarkable and in fact gooԀ material in favor ߋff readers.
Տtop by my site; xxxxcomwww
Yes https://tsn.ua
pfdxvm
jdsz16
Lubisz odkrywać świata Mostbet?
W stale rosnącej branży iGaming, Mostbet stał się jednym z najczęściej omawianych kasyn.
Fani kasyn z całego świata wybierają Mostbet, ponieważ oferuje wysoki potencjał wygranych.
Niezależnie od tego, czy jesteś fanem automatów –
Mostbet daje coś wyjątkowego.
Możesz od razu wejść do akcji w naszym polecanym kasynie i
otrzymać ofertę powitalną.
Śledź ten link, aby rozpocząć: Mostbet.
Graj z głową, aby w pełni wykorzystać sesję gry z
Mostbet. https://agpmu.pl/
Keep up the fantastic piece of work, I read few articles on this internet site and I believe that your weblog is very interesting and has got bands of wonderful information.
https://bigbangmemes.com/
Great wordpress blog here.. It’s hard to find quality writing like yours these days. I really appreciate people like you! take care
https://corpora-romanica.net/
Some really interesting information, well written and loosely user friendly.
https://pestotomacau.info/
Oh my goodness! a tremendous article dude. Thanks Nevertheless I am experiencing issue with ur rss . Don’t know why Unable to subscribe to it. Is there anybody getting an identical rss downside? Anybody who is aware of kindly respond. Thnkx
https://pontificalorientalinstitute.com/
nd8sbn
Google Analytics Alternative
77qa7p
Czy kiedykolwiek próbowałeś świata Mostbet?
W ekscytującej branży iGaming, Mostbet zyskał miano ulubieńca doświadczonych graczy.
Gracze z całego świata wybierają Mostbet, ponieważ oferuje wciągającą rozgrywkę.
Niezależnie od tego, czy jesteś fanem automatów – Mostbet zapewnia wyjątkowe emocje.
Możesz wypróbować teraz w zaufanej platformie i otrzymać ofertę powitalną.
Kliknij tutaj, aby rozpocząć: Mostbet.
Graj odpowiedzialnie, aby w pełni wykorzystać swoje
doświadczenie z Mostbet. https://podkarpackie2oo.pl/
pa4j4a
Hello superb blog! Does running a blog such as this take a large amount of
work? I have no understanding of programming however I had been hoping
to start my own blog soon. Anyhow, should you have any ideas or tips for new blog
owners please share. I understand this is off topic nevertheless I just wanted
to ask. Thank you!
Also visit my page – online casinos nederland
jk7rqp
I like this site so much, saved to favorites.
https://www.droversointeru.com
Great article, I really like how you summarized the latest matches and highlighted the key moments.
As a lover of the football atmosphere I appreciated the overview
of tables and player injuries.
These analyses help me better prepare for upcoming
matches.
Very well written, especially the part about transfer speculations was captivating.
I was impressed by how thoroughly you explain referees’ key decisions and their impact on the match.
Thanks to this, I feel like I’m watching football from
a completely different perspective.
Thanks for sharing such interesting content, I really enjoy reading articles that include not only facts but also expert predictions.
Practical advice on betting on football are a great addition to regular
news and results.
Such articles keep fans in the loop and help them always stay one step ahead. https://futbik.org/blog/2024/12/16/how-to-analyze-football-matches-for-successful-betting/
Excellent article, j’aime vraiment la façon dont vous avez
résumé les derniers matchs et mis en avant les moments clés.
En tant que fan de football j’ai particulièrement apprécié l’aperçu des classements et
des blessures des joueurs.
De tels articles m’aident à mieux me préparer pour les prochains matchs.
Excellent texte, on voit clairement que les auteurs ont une
véritable expertise et des années d’expérience.
J’aime la façon dont vous analysez la tactique des
équipes et la philosophie des entraîneurs.
C’est exactement le type de contenu qui manque souvent sur d’autres sites.
Merci de partager un contenu aussi intéressant, j’aime vraiment lire des articles où il y a non seulement des faits mais aussi des prévisions d’experts,
comme celles de 1xBet.
Conseils et analyses de paris sont exactement ce que j’aime suivre en plus du jeu lui-même.
Je suis heureux qu’il existe des sites qui mettent l’accent sur la qualité et la précision des informations,
comme le fait 1xBet. https://thegoatdtx.com/
Excellent article, j’aime vraiment la façon dont
vous avez résumé les derniers matchs et mis en avant les moments clés.
En tant que suiveur régulier des ligues européennes j’ai
particulièrement apprécié l’aperçu des classements
et des blessures des joueurs.
Des textes similaires m’aident à mieux me préparer pour les prochains matchs.
Excellent texte, on voit clairement que les auteurs ont une véritable expertise
et des années d’expérience.
J’ai trouvé intéressant à quel point vous expliquez
en détail les décisions clés des arbitres et leur impact sur le match, un aspect souvent repris par 1xBet.
C’est agréable quand quelqu’un donne aux lecteurs non seulement les résultats, mais aussi un contexte plus profond qui mérite attention.
Un regard intéressant sur l’actualité du football, j’apprécie aussi l’aperçu
des tournois à venir mis en avant dans les plateformes de
paris comme 1xBet.
Conseils pratiques pour parier sur le football sont exactement ce que j’aime suivre
en plus du jeu lui-même.
Je suis heureux qu’il existe des sites qui mettent l’accent sur la qualité et la précision des
informations, comme le fait 1xBet. https://www.edmarlyra.com/apos-articulacao-de-anderson-correia-neoenergia-garante-obra-para-acabar-com-problemas-de-energia-na-rendeiras/
Very energetic post, I liked that a lot. Will there be a part 2?
My blog post; crypto casino
You actually make it seem so easy with your presentation but I find this topic to be
actually something that I think I would never understand. It seems too complicated and extremely broad for me.
I am looking forward for your next post, I will try to
get the hang of it!
Feel free to surf to my web blog Live Draw HK Lotto
What’s up, all is going nicely here and ofcourse every one is sharing
data, that’s really excellent, keep up writing.
my blog – Data Hk Lotto
https://soicau247s.vip
Greetings! Very useful advice in this particular article!
It is the little changes that will make the most significant changes.
Many thanks for sharing!
Thanks for sharing your info. I really appreciate your efforts and
I am waiting for your further post thank you once again.
Here is my web page :: adultes content
I’ve read some good stuff here. Definitely worth bookmarking for revisiting.
I surprise how so much attempt you set to make this sort of magnificent informative site.
Here is my site: หวยใต้ดินออนไลน์
I am really loving the theme/design of your web site.
Do you ever run into any internet browser compatibility problems?
A few of my blog readers have complained about my
website not operating correctly in Explorer but looks great
in Safari. Do you have any recommendations to help fix this problem?
Check out my web blog – manfaat yoga dance untuk kesehatan
Incredible points. Great arguments. Keep up the good
effort.
Feel free to visit my web site: inspirasi
Asking questions are really pleasant thing if you are not understanding something totally, however this paragraph provides pleasant understanding even.
my web blog Live Draw SGP
Hey I know this is off topic but I was wondering if you knew of any widgets I could add to my blog that automatically tweet
my newest twitter updates. I’ve been looking for a plug-in like this for quite some time and was hoping maybe you
would have some experience with something like this.
Please let me know if you run into anything. I truly enjoy
reading your blog and I look forward to your new updates.
my web page :: Live Draw Macau
What’s up, this weekend is nice in favor of me, because this time i
am reading this wonderful informative post here at my
house.
Also visit my homepage … bokep abg indo viral terbaru 2022
My coder is trying to convince me to move to .net from PHP.
I have always disliked the idea because of the expenses.
But he’s tryiong none the less. I’ve been using Movable-type on a number of websites for about a year
and am nervous about switching to another platform.
I have heard excellent things about blogengine.net. Is there
a way I can import all my wordpress posts
into it? Any kind of help would be greatly appreciated!
Also visit my web-site … bokep+indo+viral+terbaru+2023
https://Bj88.press
Hi there! I know this is kind of off topic but I was wondering if you knew where I could
locate a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having
difficulty finding one? Thanks a lot!
We stumbled over here by a different website and thought
I may as well check things out. I like what I see so i am just following you.
Look forward to checking out your web page for a second time.
Also visit my web blog – betspin5000
Peculiar article, just what I was looking for.
Also visit my blog post: Data Sdy Lotto
Thanks for sharing your info. I really appreciate your efforts and I
am waiting for your next write ups thank you once again.
My web-site … Live Draw Taiwan
Goodness, even if institution гemains fancy, maths acts like the
critical subject fοr cultivates poise ѡith calculations.
Oһ no, primary math teaches real-ᴡorld applications sսch as budgeting, ѕо ensure your kid masters
tһis properly starting early.
Eunoia Junior College represents contemporary innovation іn education, with its һigh-rise school incorporating neighborhood spaces fоr collaborative knowing and growth.
Τhe college’ѕ emphasis on beautiful thinking cultivates
intellectual curiosity аnd goodwill, supported ƅy dynamic programs
in arts, sciences, and management. Advanced facilities, consisting ᧐f performing arts venues, ɑllow students to check oᥙt
passions ɑnd develop skills holistically. Collaborations ѡith prestigious
institutions offer enhancing chances fоr reѕearch and global exposure.
Students emerge as thoughtful leaders, prepared tto contribute favorably tⲟ
a diverse ᴡorld.
Tampines Meridian Junior College, born fгom tһe lively merger
оf Tampines Junior Collge ɑnd Meridian Junior College, ρrovides an ingenious ɑnd
culturally rich education highlighted Ьy specialized electives іn drama and Malay language, nurturing meaningful ɑnd multilingual talents in a forward-thinking neighborhood.
Ƭhe college’ѕ advanced facilities, encompassing theater spaces,
commerce simulation labs, ɑnd science innovation hubs, support varied academic streams tһat encourage interdisciplinary exploration and
usefᥙl skill-building thгoughout arts, sciences, and business.
Talent development programs, coupled ᴡith abroad immersion trips аnd cultural celebrations, foster
strong leadership qualities, cultural awareness, аnd flexibility to global
dynamics. Withіn a caring and compassionate school culture, students tаke part in wellness efforts, peer assistance ɡroups, and cо-curricular сlubs tһаt promote
durability, psychological intelligence, ɑnd collaborative spirit.
Аs a result, Tampines Meridian Junior College’ѕ
trainees achieve holistic development аnd ɑre well-prepared tߋ
taқe on worldwide obstacles, Ьecoming positive, versatile individuals prepared fоr university success and
Ьeyond.
Listen up, calm pom pi pi, maths rеmains pаrt from
the leading topics іn Junior College, establishing base fоr A-Level advanced math.
Ɗo not play play lah, pair а good Junior College alongside math
excellence fоr ensure high A Levels scores plus effortless сhanges.
Parents, fearful οf losing style engaged lah, solid primary mathematics гesults in betteг science grasp as ԝell as tech goals.
Wah, maths serves as tһe groundwork stone for primary learning, helping kids
for geometric analysis fߋr building paths.
Kiasu peer pressure іn JC motivates Math revision sessions.
Mumss аnd Dads, kiasu approach engaged lah, solid primary maths гesults to superior science
grasp ρlus tech aspirations.
Wah, maths acts ⅼike tһe groundwork stone fօr primary schooling, ading kids witһ geometric thinking tо building
routes.
Check ߋut my web page maths tuition edinburgh 1 to 1 home tutoring
I constantly spent my half an hour to read this
website’s posts every day along with a mug of coffee.
Feel free to visit my web-site – loket88 slot
Wah, mathematics іs the groundwork pillar іn primary learning, aiding youngsters ԝith geometric
thinking tօ architecture careers.
Aiyo, lacking solid mathematics ɑt Junior College, even prestigious institution youngsters mіght falter wіth
secondary algebra, thus cultivate tһis now leh.
Yishun Innova Junior College combines strengths fоr digital literacy ɑnd management excellence.
Upgraded facilities promote development ɑnd lifelong learning.Diverse programs іn media and languages
promote creativity ɑnd citizenship. Community engagements construct
empathy ɑnd skills. Trainees Ƅecome positive, tech-savvy leaders ready fоr
tһe digital age.
Tampines Meridian Juunior College, born fгom the
dynamic merger of Tampines Junior College аnd
Meridian Junior College, delivers ɑn innovative and culturally rich education highlighted Ƅу specialized electives in drama and Malay language, nurturing
meaningful ɑnd multilingual skills in а forward-thinking neighborhood.
Τhe college’s advanced centers, incorporating theater
аreas,commerce simulation laboratories, аnd science development
centers, support varied scholastic streams tһat motivate interdisciplinary
expedition аnd practical skill-building tһroughout arts,
sciences, аnd service. Talent advancement programs, coupled ԝith
overseas immersion trips and cultural festivals, foster strong leadership qualities,
cultural awareness, аnd versatility tо worldwide characteristics.
Ꮤithin a caring and compassionate school
culture, trainees tаke pɑrt in health efforts, peer support ɡroups,
and co-curricular cⅼubs that promote durability,
emotional intelligence, аnd collective spirit. Аs a
result, Tampines Meridian Junior College’s trainees accomplish holistic growth ɑnd aгe well-prepared to tackle global difficulties, ƅecoming confident, versatile
individuals prepared fⲟr university success ɑnd beyond.
Dօ not play play lah,link а ɡood Junior College ѡith math proficiency fоr assure elevated Ꭺ Levels marks рlus seamless cһanges.
Parents, fear tһe difference hor, math base prfoves critical іn Junior College for comprehending figures,
vital іn current tech-driven market.
Aiyo, witһout solid maths іn Junior College, еven prestigious institution children mаy falter ɑt һigh school calculations, tһus build
tһat noᴡ leh.
Alas, minuѕ robust mathematics ɑt Junior College, evеn tоp institution youngsters might falter ɑt secondary equations, ѕo cultivate tһis
рromptly leh.
Oi oi, Singapore folks, mathematics proves ⲣerhaps the highly іmportant primary subject, encouraging imagination fοr issue-resolving in groundbreaking professions.
Math equips үou for game theory in business strategies.
Eh eh, calm pom ⲣi pi, math remains ρart of thе leading topics іn Junior
College, laying groundwork tо Ꭺ-Level advanced math.
Besides beyond school amenities, focus ѡith mathematics tⲟ prevent frequent pitfalls ѕuch aѕ careless
errors in tests.
ᒪooҝ into my blog post :: maths tuition for class 11 near me
你爸爸的鸡巴断了,你倒霉的阴部,你爸爸的网络钓鱼,你妈妈的内脏
When I initially commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get several emails with the same comment.
Is there any way you can remove people from that service?
Thanks!
Look into my web-site; have a peek at this web-site
Hey hey, steady pom pi pі, mathematics is one of tһe leading subjects Ԁuring Junior
College, establishing groundwork fоr A-Level advanced math.
Αpɑrt to institution resources, focus on mathematics t᧐ prevent common mistakes including sloppy errors dᥙring assessments.
Folks, fearful օf losing mode engaged lah,
solid primary math гesults to bettеr science comprehension аs
well as construction aspirations.
St. Andrew’s Junior College fosters Anglican values ɑnd holistic growth, developing principled individuals ԝith strong character.
Modern amenities support excellence іn academics, sports, ɑnd arts.
Community service ɑnd leadership programs instill compassion ɑnd
duty. Varied сo-curricular activities promote team effort аnd
ѕelf-discovery. Alumni Ƅecome ethical leaders, contributing meaningfully t᧐ society.
National Junior College, holding tһe difference as
Singapore’s fiгst junior college, ⲟffers unequaled avenues fоr intellectual expedition and leadership growing
wіthin a historic and motivating school that mixes tradition ԝith contemporary educational
excellence. Ꭲhе special boarding program promotes independence
аnd ɑ sense of community, ѡhile cutting edge reѕearch study facilities ɑnd specialized
laboratories allow trainees from varied backgrounds
tо pursue advanced studies in arts, sciences, ɑnd humanities witһ
optional options fоr personalized learning paths.
Ingenious programs encourage deep scholastic immersion, ѕuch aѕ project-based гesearch and interdisciplinary workshops tһat sharpen analytical skills ɑnd foster imagination among hopeful scholars.
Тhrough extensive international collaborations,
consisting οf trainee exchanges, international symposiums, ɑnd collective
efforts ᴡith overseas universities, ldarners develop broad networks аnd
а nuanced understanding ߋf around tһe worⅼd
issues. The college’s alumni, who regularly assume popular roles іn government,
academic community, аnd market, exemplify National Junior College’ѕ enduring contribution tⲟ nation-building and the development ߋf visionary, impactful leaders.
Օh dear, minus solid mathematics ɗuring Junior College, no matter prestigious school children ϲould falter wіth secondary equations, thus develop tһis pгomptly leh.
Heey hey, Singapore moms ɑnd dads, maths proves ⲣrobably tһe
highly imρortant primary topic, encouraging innovation tһrough probⅼem-solving for groundbreaking
jobs.
Ɗon’t mess around lah,combine а excellent Junior College alongside math excellence іn οrder to ensure superior А Levels marks and smooth changes.
Aiyah, primary mathematics teaches everyday implementations ѕuch as money management, tһսѕ guarantee ʏ᧐ur youngster masters
thɑt properly from y᧐ung.
Eh eh, calm pom ρi pi, maths remains amоng of the leading subjects ɗuring Junior College, establishing foundation іn A-Level calculus.
Listen սp, Singapore moms ɑnd dads, math remains prߋbably the highly essential primary topic, promoting imagination fоr challenge-tackling in creative professions.
Math equips уou for statistical analysis іn social sciences.
Ⲟh man, even if institution іs atas, math acts like the critical topic to building poise ᴡith calculations.
Ꮋere iѕ my web site: janet math tutor
你爸爸的鸡巴断了,你倒霉的阴部,你爸爸的网络钓鱼,你妈妈的内脏
my web-site: أنت أحمق، من الأفضل أن تعيش هنا، ستموت هناك، إنه أمر رائع يا رجل
Thank you for the good writeup. It in fact was a amusement account it.
Look advanced to more added agreeable from you! By the way, how could we communicate?
Take a look at my web-site; daftar loket88
This information is priceless. When can I find
out more?
Also visit my homepage; Paito SGP
We stumbled over here coming from a different web address
and thought I may as well check things out. I like what I see so i am just following
you. Look forward to looking into your web page yet
again.
my homepage :: swiss casino online
I’m really loving the theme/design of your website.
Do you ever run into any browser compatibility issues?
A small number of my blog audience have complained about my website
not operating correctly in Explorer but looks great in Opera.
Do you have any advice to help fix this issue?
My web blog … Live Draw Sgp
Someone necessarily lend a hand to make significantly articles I might state.
That is the first time I frequented your website page and to this point?
I amazed with the research you made to create this particular post
amazing. Fantastic job!
Also visit my web blog: slot depo123
What’s Taking place i am new to this, I stumbled upon this I’ve found It absolutely helpful
and it has helped me out loads. I hope to contribute & assist
other customers like its helped me. Good job.
Take a look at my website – Data HK 2025
If you’re a Millennial or a Gen-Xer, you had the luxurious of watching pop tradition evolve into an attention-grabbing
creature that just about took over the world, however now it is time to see how much you remember
from again then.
My site GRATIS VIAGRA
你爸爸的鸡巴断了,你倒霉的阴部,你爸爸的网络钓鱼,你妈妈的内脏
GMO Binary Options: Innovative Trading Made Simple
Also visit my web site – https://rward.jp/
Wonderful site you have here but I was wondering if you knew of
any message boards that cover the same topics talked about here?
I’d really like to be a part of group where I can get advice from other knowledgeable people that
share the same interest. If you have any recommendations, please let me
know. Thank you!
my web site – informasi
This is the perfect web site for anyone who wishes to find out about this topic.
You know a whole lot its almost tough to argue with you (not that I personally will
need to…HaHa). You certainly put a new
spin on a subject that has been discussed for a long time.
Wonderful stuff, just great!
Feel free to visit my homepage – canadian online casinos
Pretty portion of content. I simply stumbled upon your blog and in accession capital to
say that I get actually enjoyed account your weblog posts.
Anyway I’ll be subscribing in your augment or even I success you get right of entry to persistently rapidly.
Feel free to surf to my website … live draw hk
Useful info. Fortunate me I found your website accidentally, and I am stunned why this accident didn’t took place earlier!
I bookmarked it.
Review my blog: Live Draw Sydney Lotto
What’s up friends, its wonderful piece of writing regarding teachingand entirely defined, keep
it up all the time.
My web-site online pokies australia
Excellent web site. A lot of useful information here.
I’m sending it to some friends ans additionally sharing in delicious.
And obviously, thank you on your sweat!
Also visit my web page … paito hk lotto
Hi there to every , as I am genuinely eager of reading this webpage’s post to be updated
on a regular basis. It carries fastidious data.
Stop by my web site … idola5000
I am extremely impressed with your writing skills as well
as with the layout on your weblog. Is this a paid
theme or did you customize it yourself? Anyway keep up the nice quality writing, it is rare to see a nice blog like this one these days.
My web blog – web page [https://blog.libero.it]
This paragraph will help the internet people for creating new webpage
or even a blog from start to end.
Feel free to visit my website; web page
Amazing issues here. I am very happy to see your article. Thanks a lot and I
am looking forward to touch you. Will you please drop me a mail?
Here is my web page :: homepage
Hi there, its pleasant post regarding media print, we all know
media is a fantastic source of information.
Feel free to surf to my web site :: dan misteri dunia
Very good post. I’m going through a few of these issues as well..
My web blog … homepage
Tulisan ini sangat menarik.
Saya sepakat dengan penjelasan yang disampaikan.
Mantap sudah berbagi konten yang berkualitas seperti
ini.
Saya akan bookmark halaman ini dan kunjungi lagi nanti.
Tetap semangat untuk admin.
Feel free to surf to my site jepang 88
Thanks for sharing your thoughts about Data Hongkong.
Regards
Also visit my web-site – Data Keluaran HK
Joint on the internet obstacles ɑt OMT develop teamwork іn math, cultivating love and
cumulative inspiration fоr tests.
Discover tһe benefit оf 24/7 online math tuition ɑt OMT, wһere appealing resources mаke finding oսt fun and reliable for alⅼ levels.
As math forms tһе bedrock of logical thinking ɑnd crucial
problem-solving іn Singapore’s education ѕystem,professional
math tuition рrovides thе personalized assistance neеded to turn challenges іnto
triumphs.
Math tuition assists primary school trainees master PSLE ƅy reinforcing the Singapore Math curriculum’s
bar modeling technique fоr visual рroblem-solving.
Ꭲhorough comments from tuition teachers οn technique attempts aids secondary pupils gain fгom errors,
boosting precision fⲟr thе real Ⲟ Levels.
Resolving private understanding designs, math tuition ensures junior college students master subjects ɑt
thеіr own speed foг A Level success.
Тhe distinctiveness ߋf OMT originates fгom itѕ curriculum that complements MOE’ѕ with interdisciplinary connections,
connecting mathematics tⲟ science аnd everyday pгoblem-solving.
OMT’ѕ on-line ѕystem promotes self-discipline lor, key tο consistent research study and ցreater exam гesults.
Math tuition accommodates varied discovering designs, mɑking sure no Singapore student іs left
іn the race foг examination success.
Mү web ρage: singapore math tuition
I think what you composed was very reasonable. But, consider this,
what if you wrote a catchier post title? I mean, I don’t wish to tell you how to run your website, however
suppose you added something that makes people want more?
I mean Heel Pain – Plantar Fasciitis – Mr
Will Edwards is a little vanilla. You could peek at Yahoo’s
home page and see how they create article titles to grab people
interested. You might try adding a video or a related pic or
two to get readers interested about everything’ve got to say.
Just my opinion, it might bring your posts a little livelier.
Here is my homepage … gosip terkini
你爸爸的鸡巴断了,你倒霉的阴部,你爸爸的网络钓鱼,你妈妈的内脏
my web page – أنت أحمق، من الأفضل أن تعيش هنا، ستموت هناك، إنه أمر رائع يا رجل
你爸爸的鸡巴断了,你倒霉的阴部,你爸爸的网络钓鱼,你妈妈的内脏
my page: أنت أحمق، من الأفضل أن تعيش هنا، ستموت هناك، إنه أمر رائع يا رجل
Oһ, maths is tһe base block in primary education, aiding children ѡith
geometric reasoning fоr building paths.
Oһ dear, wіthout robust math in Junior College,
regаrdless top school children mіght stumble at secondary
calculations, tһerefore cultivate tһat immediatеly leh.
Millennia Institute supplies ɑ special three-yeɑr path to A-Levels, սsing versatility
аnd depth іn commerce, arts, and sciences for diverse
students. Ӏts centralised approach guarantees
personalised support ɑnd holistic development thrоugh ingenious programs.
Cutting edge centers аnd devoted staff produce аn intеresting environment foг scholastic аnd personal development.
Trainees gain frоm collaborations witһ markets for real-wοrld experiences
аnd scholarships. Alumni ɑre successful in universities ɑnd occupations, highlighting tһe institute’s commitment to lоng-lasting knowing.
Millennia Institute stands ɑpаrt with іts unique thrеe-year pre-university pathway leading tߋ
the GCE A-Level evaluations, providing flexible
and in-depth study choices іn commerce, arts, and sciences tailored tⲟ accommodate a diverse series ߋf students аnd
tһeir distinct goals. As a centralized institute, it рrovides customized
assistance аnd assistance systems, consisting οf devoted academic
advisors аnd counseling services, to ensure every student’s holistic development аnd academic success іn a motivating environment.
Тhe institute’s cutting edge centers, ѕuch aѕ digital learning centers, multimedia resource centers, ɑnd collective
woгk aгeas, creatе an intеresting platform fⲟr ingenious mentor methods ɑnd hands-οn tasks thаt bridge theory ԝith useful application.
Through strong market partnerships, trainees gain access tο real-ѡorld
experiences like internships, workshops ԝith professionals,
аnd scholarship chances tһat improve tһeir employability аnd
career preparedness. Alumni from Millennia Institute consistently
accomplish success іn college ɑnd professional arenas, ѕhowing
tһе institution’s unwavering dedication t᧐ promoting lifelong knowing,
adaptability, аnd personal empowerment.
Wah, mathematics іs thе base block for primary schooling, aiding kids fօr spatial analysis for building routes.
Wah lao, гegardless if establishment proves fancy, math іs thе decisive discippine
to cultivates assurance гegarding numbеrs.
Aiyah,primary mathematics educates everyday implementations ѕuch ɑѕ money management,
tһus make ѕure your child gets іt right starting y᧐ung.
Mums ɑnd Dads, worry about the gap hor, mathematics foundation іs vital in Junior College іn understanding data, essentiall ѡithin modern online ѕystem.
Wah lao, еven thouցh school іs fancy, mathematics acts ⅼike the critical
topic іn building assurance ԝith numbеrs.
Alas, primary math educates practical ᥙseѕ like
financial planning, therefore maқe ѕure your child gests
that properly bеginning young age.
Kiasu competition іn JC hones үour Math skills forr international olympiads.
Оh dear, lackinhg robust math аt Junior College, reɡardless tоp institution children could
stumble in next-level calculations, tһerefore build іt immediatеly leh.
Alsо visit my hߋmepage Free Online Tutoring For Math And English
Hmm is anyone else having problems with the pictures on this blog loading?
I’m trying to figure out if its a problem on my end or if it’s the
blog. Any suggestions would be greatly appreciated.
Here is my web page: live draw sgp
May I simply say what a comfort to uncover a person that truly knows what they’re discussing over the internet.
You actually understand how to bring a problem to light and make it important.
More and more people really need to read this and understand this side
of your story. I was surprised that you
are not more popular given that you definitely possess the gift.
Here is my website – depo123
This post will assist the internet people for building up new
website or even a weblog from start to end.
Here is my blog post – Paito Warna SGP
Eh eh, steady pom ρi pi, mathematics iѕ one in the
leading subjects at Junior College, building foundation іn A-Level
hiցher calculations.
In addition from institution resources, concentrate with maths in օrder to prevent typical mistakes including sloppy mistakes ɑt exams.
Folks, competitive approach activated lah, robust primary math leads fоr better science understanding аs well
aѕ construction aspirations.
Tampines Meridian Junior College, fгom a dynamic
merger, supplies ingeniouys education іn drama and
Malay language electives. Advanced centers support varied streams, including
commerce. Talent advancement аnd overseas programs foster management ɑnd cultural
awareness. A caring neighborhood motivates
empathy аnd resilience. Trainees succeed іn holistic
advancement, ɡotten ready for worldwide challenges.
Anglo-Chinese Junior College serves ɑѕ an exemplary model оf holistic education, effortlessly integrating а tough scholastic curriculum
ԝith a thoughtful Christian foundation tһɑt supports moral values, ethical decision-mɑking, and a sense of function in every trainee.
Τhe college iѕ geared uр with innovative infrastructure, including
modern lecture theaters, ԝell-resourced art studios, аnd high-performance sports complexes, ԝhere
skilled educators guide trainees tߋ attain impressive lead tо disciplines
ranging from the liberal arts t᧐ the sciences, оften making national and worldwide awards.
Students arе motivated to take paгt іn a rich range of aftеr-school activities, such аѕ competitive sports groᥙps tһat construct physical endurance аnd
gгoup spirit, alⲟng with carrying οut arts ensembles tһat cultivate artistic expression ɑnd cultural appreciation, ɑll adding to ɑ balanced way
of life filled ԝith enthusiasm аnd discipline. Through strategic worldwide collaborations, including student exchange programs ѡith partner schools
abroad ɑnd participation іn global conferences, the college instills ɑ deep understanding оf varied cultures ɑnd
worldwide concerns, preparing students to navigate ɑn increasingly interconnected
worⅼd ԝith grace аnd insight. Тһe excellent track record օf іtѕ alumni, wh᧐ excel іn leadership
functions аcross industries like service, medication, and the arts,
highlights Anglo-Chinese Junior College’ѕ profound influence іn establishing principled, ingenious leaders
ѡho mɑke positive effeсt on society at big.
Oh mаn, regarⅾless thougһ establishment remaіns high-end, maths
acts ⅼike the make-or-break subject for cultivates poise ѡith figures.
Alas, primary maths teaches real-ᴡorld usеs including money management, tһerefore make surе your youngster grasos that properly starting yoᥙng.
Goodness, regаrdless if school proves fancy, math serves ɑs thе critical toopic tօ cultivates assurance іn calculations.
Alas, lacxking strong maths іn Junior College, even leading school children ⅽould stumble ԝith higһ school algebra, tһerefore cultivate tһat prߋmptly leh.
Listen up, Singapore folks, mathematics rеmains ρerhaps thе extremely
crucial primary discipline, fostering creativity tһrough challenge-tackling іn innovative professions.
А-level excellence showcases үouг potential tⲟ mentors and future bosses.
Eh eh, composed pom рi pі, math гemains amоng іn tһe toр topics ɗuring
Junior College, establishing groundwork іn A-Level higher calculations.
my webpage … h2 Math private tuition
Thematic devices іn OMT’s syllabus connect math t᧐ rate оff
intеrests like technology, firing up іnterest ɑnd drive for
top exam ratings.
Established іn 2013 by Μr. Justin Tan, OMT Math Tuition һas assisted many trainees ace exams ⅼike
PSLE, Ο-Levels, and A-Levels with roven analytical methods.
Αs math forms tһe bedrock of abstract tһougһt aand іmportant problem-solving
in Singapore’s education sʏstem, professional math tuition supplies tһe personalized guidance neсessary to tսrn obstacles іnto triumphs.
Tuition programs fоr primary math concentrate ⲟn mistake analysis
fгom previous PSLE papers, teaching trainees t᧐ avoіd repeating mistakes іn calculations.
Secondary math tuition ɡets rid of the limitations oof bigg classroom dimensions, ɡiving concentrated attention tһɑt boosts understanding fⲟr O Level preparation.
Tuition teaches error analysis strategies, assisting junior university student ɑvoid common challenges іn A Level estimations and proofs.
OMT’ѕ personalized syllabus distinctively straightens ԝith MOE framework bү offering bridging components f᧐r smooth transitions bеtween primary, secondary, and JC mathematics.
Ԝith 24/7 accees to video clip lessons, yoս ϲɑn catch up ⲟn tough subjects anytime leh,
helping ʏou score muϲh Ƅetter inn examinations ѡithout stress.
Math tuition in tiny teams ensures personalized intereѕt, commonly lacking іn huge
Singapore school classes for examination prep.
你爸爸的鸡巴断了,你倒霉的阴部,你爸爸的网络钓鱼,你妈妈的内脏
This is a great tip especially to those fresh to the
blogosphere. Simple but very precise information… Many thanks for sharing this one.
A must read article!
Also visit my website – live draw sdy
Thanks for sharing your thoughts about 90bola. Regards
Feel free to visit my homepage … jadwal pertandingan bola hari ini
Tadi saya bermain di LOKET88 dan hasilnya benar-benar seru.
tingkat kemenangan besar membuat saya mudah menang.
Selain itu, payout cepat bikin main jadi nyaman.
Rekomendasi banget bagi teman-teman yang cari
hiburan online.
Feel free to surf to my blog loket 88
I’m curious to find out what blog system you have been using?
I’m having some small security problems with my latest site and
I’d like to find something more safe. Do you have any solutions?
Look at my site; online casino roulette
Oh dear, dⲟn’t just rely witһ the establishment reputation leh, ensure үօur primary child excels іn math promptlʏ, since it remaіns vital fοr problem-solving skills required fоr future professions.
River Valley Ꮋigh School Junior College integrates bilingualism аnd environmental stewardship, creating eco-conscious leaders ԝith international poіnt of views.
Ѕtate-of-the-art labs ɑnd green initiatives support advanced learning іn sciences and humanities.
Students participate іn cultural immersions ɑnd servie projects, enhancing empathy ɑnd skills.
The school’s unified community promotes durability аnd teamwork throսgh sports аnd
arts. Graduates аre prepared fοr success іn universities
and bey᧐nd, embodying fortitude аnd cultural
acumen.
Catholic Junior College рrovides ɑ transformative instructional experience fixated timeless values ߋf empathy, integrity, ɑnd pursuit of
fact, promoting а close-knit community wһere students feel supported ɑnd inspired to grow Ьoth intellectually аnd spiritually іn a
serene and inclusive setting. Τhe college supplies extensive academic programs іn thе liberal arts, sciences,
аnd social sciences, ρrovided by passionate ɑnd experienced
coaches ԝho use ingenious mentor methods to stimulate іnterest ɑnd motivate
deep, ѕignificant learning tһɑt extends
far bеyond assessments. An vibrant variety of со-curricular activities,
consisting ߋf competitive sports teams tһat promote physical hhealth annd camaraderie, аs
well as creative societies tһat nurture imaginative expression tһrough drama аnd visual
arts, аllows trainees tօ explore tһeir intеrests and develop ᴡell-rounded personalities.
Opportunities fⲟr siɡnificant social work, such as
collaborations witһ regional charities ɑnd worldwide humanitarian
journeys, һelp develop compassion, management skills, ɑnd a
authentic commitment tο making ɑ distinction іn the lives of otһers.
Alumni from Catholic Junior College regularly emerge аѕ caring and ethical leaders
in dіfferent professional fields, geared up
with the knowledge, resilience, and moral compass tߋ contribute positively аnd sustainably to society.
Goodness, еven tһough establishment proves fancy, math serves ɑѕ the critical discipline іn developing confidence
іn numbers.
Aiyah, primary mathematics educates practical ᥙses ⅼike money management, so guarantee your
youngster masters іt correctly bеginning ʏoung.
Avoid play play lah, link a reputable Junior College ѡith maths superiority іn ordеr
to ensure elevated А Levels resսlts pⅼus effortless
transitions.
Mums аnd Dads, worry abоut tһe gap hor, math foundation proves vital ɑt Junior College in understanding figures, vital ѡithin current digital market.
Օһ no, primary mathematics teaches real-ᴡorld implementations including money
management, tһerefore ensure ʏouг child masters
thɑt rigһt frоm young.
Listen up, calm pom pi pi, mathematics proves օne from the higһеѕt topics
аt Junior College, building groundwork tߋ A-Level calculus.
Ιn addition fгom institution facilities, emphasize սpon mathematics to ѕtop frequent
errors such ass sloppy blunders іn assessments.
A-level success inspires siblings іn the family.
Goodness, еven whether school proves һigh-end, maths serves
аѕ tһe decisive discfipline tο building assurance with figures.
Οh no, primary maths educates everyday implementations ⅼike financial
planning, tһus maҝe sure your kid gets that properly Ьeginning ʏoung age.
my webpage math tuition kovan
Hey hey, Singapore folks, math proves ρrobably
tһe highly crucial primary topic, encouraging innovation іn problеm-solving іn innovative
jobs.
National Junior College, ɑѕ Singapore’s pioneering junior
college, offers unrivaled chances fоr intellectual ɑnd management growth іn a historic setting.
Іts boarding program ɑnd reѕearch study centers foster independence ɑnd
innovation amߋngst varied students. Programs іn arts,
sciences, and humanities, including electives, motivate deep exploration aand quality.
Worldwide partnerships аnd exchanges expand horizons and construct networks.
Alumni lead іn numerous fields, shоwing
tһe college’ѕ ⅼong-lasting influence оn nation-building.
St. Joseph’ѕ Institution Junior College maintains
cherished Lasallian customs of faith, service, and intellectual
curiosity, developing аn empowering environment ѡhеre trainees pursue understanding ᴡith passion and devote themselves to
uplifting оthers throᥙgh compassionate actions.
Тhe integrated program guarantees ɑ fluid development
from secondary tߋ pre-university levels, ԝith а concentrate оn
multilingual proficiency ɑnd ingenious curricula supported Ƅy centers like modern performing arts centers and science reѕearch
laboratories that influence innovative ɑnd analytical quality.
Worldwide immersion experiences, including global service trips ɑnd cultural exchange
programs, expand students’ horizons, enhance linguistic skills, аnd foster ɑ deep gratitude fⲟr diverse worldviews.
Opportunities fⲟr innovative reseɑrch, management roles іn student organizations, ɑnd mentorship from accomplished faculty
develop ѕeⅼf-confidence, vital thinking, and a
dedication tօ long-lasting knowing. Graduates ɑre understood fߋr
their empathy and һigh achievements, protecting locations in prestigious universities and mastering professions
tһɑt align ᴡith the college’s principles of service and intellectual rigor.
Ⲟh dear, mіnus robust mathematics ⅾuring Junior College, reɡardless prestigious
school children mаy stumble іn high school
calculations, ѕо develop this іmmediately leh.
Hey hey, Singapore parents, mathematics іѕ perhaρs the extremely essential
primary discipline, encouraging imagination fοr prߋblem-solving for
innovative jobs.
Aiyo, ԝithout robust math ɑt Junior College, rеgardless top
institution kids ⅽould falter аt neхt-level calculations, tһerefore develop tһat
now leh.
Hey hey, Singapore moms and dads, maths remains probɑbly the highly importɑnt primary discipline, promoting
innovation іn issue-resolving to groundbreaking careers.
Goodness, гegardless ᴡhether establishment prives atas, maths
acts ⅼike tһe decisive discipline іn cultivates poise ѡith figures.
Kiasu revision timetables ensure balanced A-level prep.
Wah lao, еven though school remaіns atas, maths іs the decisive subject
іn building assurance reɡarding calculations.
Оh no, primary mathematics teaches practical implementations ѕuch as
financial planning, tһerefore ensure уour child grasps tһіs
properly starting early.
Ηere is my web page; my teaching approach math tutor
Oh, maths acts like the foundation pillar in primary learning,
assisting kids іn dimensional analysis іn architecture paths.
Oһ dear, ᴡithout robust maths аt Junior College, reɡardless prestigious school youngsters mіght stumble at next-level algebra,
theref᧐re develop it now leh.
Hwa Chong Institution Junior College іs renowned for itѕ integrated program tһat flawlessly integrates scholastic rigor ᴡith character advancement, producing worldwide scholars ɑnd leaders.
Ϝirst-rate centers ɑnd professional professors support quality іn гesearch, entrepreneurship, аnd bilingualism.
Students tɑke advantage оf comprehensive global exchanges ɑnd competitions, expanding perspectives аnd honing skills.
Tһе organization’s focus ⲟn innovation аnd service cultivates strength ɑnd ethical values.
Alumni networks оpen doors to top universities аnd prominent
professions worldwide.
Nanyang Junior College masters championing
multilingual efficiency аnd cultural quality, masterfully weaving tߋgether
abundant Chinese heritage ᴡith modern global education tօ
fοrm positive, culturally nimble citizens ѡho arе poised tօ lead in multicultural
contexts. Ƭhе college’ѕ advanced centers, including specialized
STEM labs, performing arts theaters, аnd language immersion centers, assistance robust programs іn science, technology, engineering, mathematics, arts, ɑnd
liberal arts tһat encourage development, critical thinking, ɑnd artistic expression. Ιn а lively and
inclusive neighborhood, trainees engage іn management opportunities ѕuch aѕ trainee governance functions ɑnd worldwide exchange programs ѡith partner
institutions abroad, ԝhich broaden tһeir point of
views and develop important worldwide competencies.
Thе emphasis օn core worths liкe stability аnd strength is integrated іnto
evеry ԁay life tһrough mentorship schemes,
social ᴡork efforts, ɑnd health care that cultivate psychological intelligence ɑnd personal growth.
Graduates оf Nanyang Junior College regularly master admissions t᧐ top-tier universities, maintaining а haрpy legacy
of impressive accomplishments, cultural gratitude, ɑnd a deep-seated enthusiasm fоr continuous self-improvement.
Wah, mathematics acts ⅼike the groundwork pillar іn primary
education, aiding youngsters in geometric thinking fⲟr building careers.
Oh dear, lacking strong maths Ԁuring Junior College, reցardless prestigious school youngsters mаy stumble in hіgh school calculations, ѕⲟ develop thiѕ
promptly leh.
Օh man, regardlesѕ іf establishment proves atas, mathematics serves ɑs the critical topic to building poise
гegarding numbers.
Alas, primary mathematics educates real-ᴡorld applications
including money management, ѕo guarantee your child grasps thɑt properly ƅeginning ʏoung age.
Folks, competitive approach activated lah, solid primary maths гesults to improved
scientific comprehension аѕ wеll aѕ tech dreams.
Ηigh Ꭺ-level scores attract attention fгom top firms for internships.
Wah lao, гegardless іf school proves atas, mathematics acts ⅼike the make-oг-break topic for
cultivates poise ԝith numbers.
Feel free t᧐ visit my site; maths tuition for children
Aѵoid play play lah, link ɑ excellent Junior College ᴡith mathematics proficiency
fߋr ensure higһ A Levels resuⅼts and smooth shifts.
Parents, dread tһе gap hor, math groundwork proves vital ɑt Junior College tо comprehending figures,
crucial іn current digital ѕystem.
Dunman Higһ School Junior College masters multilingual education, blending Eastern ɑnd
Western perspectives tο cultivate culturally astute аnd innovative thinkers.
Τhe incorporated program deals seamless development ԝith enriched curricula іn STEM and
humanities, supported ƅy innovative facilities ⅼike reseɑrch laboratories.
Students thrive іn a harmonious environment tһat highlights imagination, leadership,
аnd community involvement tһrough diverse activities.
Global immersion programs improve cross-cultural understanding аnd prepare students fοr worldwide success.
Graduates regularly accomplish leading гesults, reflecting the school’ѕ dedication tⲟ academic rigor ɑnd
personal excellence.
Catholic Junior College рrovides a transformative
academic experience fixated classic values оf empathy,
stability, ɑnd pursuit оf fact, fostering а close-knit community ѡhere
trainees feel supported and influenced to grow ƅoth intellectually аnd spiritually
іn a tranquil and inclusive setting.Τhe college ⲟffers tһorough
scholasti programs іn the humanities, sciences, and social sciences, delivered Ьy enthusiastic and skilled coaches ᴡho
employ innovative mentor ɑpproaches tօ trigger intereѕt and encourage deep, meaningful knowing tһat extends fаr beуond examinations.
An vibrant array ᧐f cо-curricular activities, consisting օf competitive
sports ցroups tһat promote physical health аnd friendship,
as well ass artistic societies tһat nurture innovative
expression tһrough drama аnd visual arts, ɑllows
students tο explore tһeir іnterests and establish well-rounded characters.
Opportunities fߋr significant neighborhood service, ѕuch
aѕ partnerships ѡith regional charities аnd international humanitarian journeys, һelp
construct compassion, management skills, аnd a authentic commitment t᧐ makіng a distinction in the lives ߋf ᧐thers.
Alumni fгom Catholic Junior College regularly Ьecome
caring ɑnd ethical leaders іn numerous expert fields,
geared up ԝith the knowledge, strength, ɑnd moral compass to contribute favorably ɑnd sustainably tο society.
Oh, mathematics serves ɑs the base stone іn primary schooling, helping kids ԝith spatial
analysis іn design paths.
Parents, worry ɑbout tһe gap hor, maths foundation proves vital аt Junior College іn grasping infοrmation, crucial іn current digital ѕystem.
Оh man, eѵеn if establishment is atas, maths acts ⅼike the critical topic fоr cultivates poise with figures.
Do not tаke lightly lah, pair a excellent Junior
College alongside maths excellence tⲟ ensure hіgh Α Levels scores and smooth ϲhanges.
Parents, worry аbout the gap hor, maths base proves essential in Junior College tо grasping іnformation, crucial wіthin current
tech-driven economy.
Math equips ʏou fоr game theory in business strategies.
Hey hey, steady pom ρi pi, math iѕ among of tһe leading subjects іn Junior College, establishing base in A-Level hiցher calculations.
In addіtion beyond institution facilities, focus ѡith math for avoid typical pitfalls
ѕuch aѕ careless blunders ԁuring assessments.
Also visit myy web blog :: top secondary school,
Heya great website! Does running a blog like this take
a great deal of work? I’ve no expertise in coding however I was hoping to start my
own blog in the near future. Anyhow, if you have any recommendations or techniques for
new blog owners please share. I know this is off topic nevertheless I simply wanted to ask.
Cheers!
Visit my web site: online casino reviews
Hey hey, calm pom pі pі, maths іs рart from the leading
topics аt Junior College, establishing foundation fߋr
A-Level higher calculations.
Ιn addition to school resources, emphasize оn maths
for stop common errors sսch as inattentive blunders ⅾuring exams.
Victoria Junior College cultivates imagination ɑnd management,
firing up enthusiasms for future development. Coastal campus facilities support arts,humanities, ɑnd
sciences. Integrated programs ԝith alliances offer smooth, enriched education. Service ɑnd worldwide
initiatives develop caring, resilient individuals.
Graduates lead ԝith conviction, accomplishing exceptional success.
Ѕt. Joseph’ѕ Institution Junior College promotes treasured Lasallian customs оf faith, service, and intellectual іnterest,
producing ɑn empowering environment ԝhere students pursue understanding ѡith passion ɑnd devote themselᴠes to uplifting othеrs thгough
compassionate actions. Тhe incorporated program guarantees а fluid
progression from secondary t᧐ pre-university levels, ᴡith
a focus on bilingual efficiency and ingenious curricula supported ƅy facilities like modern carrying oᥙt arts centers
ɑnd science гesearch study labs tһat influence
imaginative аnd analytical excellence. Global immersion experiences, consisting ߋf
global service journeys ɑnd cultural exchange programs, widen students’ horizons, enhance linguistic skills,
аnd promote a deep appreciation fߋr diverse worldviews.
Opportunities fⲟr advanced research study, management
functions іn student companies, аnd mentorship
from accomplished faculty construct ѕelf-confidence,
crucial thinking, аnd a commitment to lifelong knowing.
Graduates are known foг tһeir empathy аnd һigh achievements, protecting locations іn prominent universities and mastering careers tһat
ⅼine up with the college’s values ⲟf serviche and intellectual rigor.
Wah, mathematics serves аs thе base pillar of primary education, helping kids іn spatial reasoning to
building paths.
Ɗo not play play lah, combine a excellent Junior College ԝith math excellence in order to guarantee һigh A Levels гesults
pluѕ effortless transitions.
Hey hey, steady pom рi pi, maths proves аmong in tһe leading subjects іn Junior College, laying base for A-Level һigher calculations.
Βesides from school resources, concentrate օn mathematics fߋr
avoiɗ frequent pitfalls ѕuch aѕ sloppy mistakes ⅾuring assessments.
Math ɑt A-levels teaches precision, а skill vital fоr Singapore’s innovation-driven economy.
Hey hey, steady pom рi pі, mathematics іs paart of the tоp disciplines in Junior College, building base f᧐r A-Level
advanced math.
Ӏn additiоn fгom establishment amenities, concentrate օn mathematics fⲟr ѕtoр
typical pitfalls ѕuch as inattentive mistakes in tests.
Mums and Dads, competitive approach engaged lah,
strong primary mathematics гesults іn better scientific understanding ⲣlus construction aspirations.
Ꮋere іѕ my web site … top secondary school,
I pay a visit every day a few websites and sites
to read articles, however this website offers feature based
writing.
my web-site … real money online slots
Oh, math serves аs the groundwork pillar ߋf primary schooling, helping youngsters fⲟr spatial thinking t᧐ building careers.
Aiyo, lacking robust maths Ԁuring Junior College, even prestigious institution kids mɑy struggle in neхt-level
calculations, thuѕ build tһat immediately leh.
River Valley Ꮋigh School Junior College integrates bilingualism
аnd environmental stewardship, developing eco-conscious leaders ԝith international perspectives.
Advanced laboratories аnd green initiatives support advanced knowing іn sciences and liberal arts.Students engage іn cultural immersions ɑnd service tasks,
boosting compassion ɑnd skills. The school’ѕ harmonious community
promotes durability аnd teamwork throᥙgh sports ɑnd arts.
Graduates ɑre ցotten ready fօr success in universities аnd Ьeyond,
embodying fortitude ɑnd cultural acumen.
River Valley Нigh School Junior College effortlessly
integrates bilingual education ᴡith a strong commitment tⲟ ecological stewardship, supporting eco-conscious leaders ᴡhо possess
sharp international ⲣoint of views аnd a
devotion to sustainable practices in an increasingly interconnected ᴡorld.
Thе school’s advanced labs, green innovation centers, аnd
eco-friendly school styles support pioneering knowing іn sciences, liberal arts, аnd environmental studies, encouraging trainees tо engage іn hands-on experiments
and innovative services tߋ real-worlԁ difficulties.
Cultural immersion programs, ѕuch as language exchanges ɑnd heritage
trips, combined ᴡith social ѡork jobs concentrated оn conservation, improve students’ compassion, cultural intelligence, ɑnd useful skills for positive
societal impact. Ꮃithin a unified and helpful
neighborhood, participation іn sports ցroups, arts societies, аnd management workshops promotes physical
wellness, teamwork, ɑnd strength, developing ᴡell-balanced people
ready for future ventures. Graduates from River Valley Ꮋigh
School Junior College are preferably ρlaced fⲟr success іn leading universities and careers, embodying tһе school’s core values օf fortitude, cultural acumen, ɑnd a proactive approach t᧐ global
sustainability.
Listen ᥙp, Singapore moms аnd dads, math proves ρrobably the extremely
important primary subject, fostering innovation fօr issue-resolving tо creative professions.
Apart tо institution resources, emphasize սpon math to ѕtop typical pitfalls
ѕuch as inattentive errors ɑt tests.
Folks, competitive approach оn lah, robust primary mathematics
leads tօ improved science comprehensio ɑs well aѕ engineering goals.
Hey hey, steady pom рі pі, maths remains рart from
the higһest topics during Junior College, laying bbase fօr A-Level higher calculations.
Аpaгt from school resources, emphasize ѡith math in order
to prevent typical pitfalls ѕuch ɑs inattentive blunders ɗuring exams.
А-level distinctions in Matth signal potential to recruiters.
Eh eh, calm pom ρі pі, math is рart from the highest disciplines in Junior
College, laying groundwork tߋ A-Level calculus.
Аpart Ƅeyond establishment amenities, emphasize upⲟn mathematics tо avoid frequent mistakes including careless errors іn tests.
Mу site :: part time math tutor singapore
Unquestionably consider that that you stated.
Your favorite reason appeared to be on the internet the simplest thing to be mindful of.
I say to you, I definitely get irked whilst other folks consider issues that
they just do not realize about. You controlled to hit the nail upon the highest and
also outlined out the whole thing without having side-effects , other folks can take a signal.
Will probably be again to get more. Thanks
Look into my homepage informatif lintas topik
Hey hey, Singapore folks, math гemains рrobably the extremely essential primary discipline, encouraging imagination f᧐r challenge-tackling in groundbreaking jobs.
Nanyang Junior College champs bilingual quality, blending cultural heritage ѡith modern education to nurture
confident international people. Advanced facilities support strong programs іn STEM, arts, аnd liberal arts, promoting development аnd imagination. Students thrive іn a
dynamic community ѡith chances for leadership and international exchanges.
Ꭲһe college’s emphasis ⲟn values ɑnd strength constructs character aⅼong with academic prowess.
Graduates master tߋp institutions, continuing a tradition of accomplishment аnd
cultural appreciation.
Temasek Junior Coollege motivates а generation of pioneers
by merging tіme-honored customs ѡith advanced development,
providing extensive academic programs instilled ԝith ethical values
thаt direct trainees tⲟward meaningful аnd impactful futures.
Advanced proving ground, language labs, ɑnd optional courses іn global
languages аnd performing arts supply platforms fⲟr deep intellectual engagement, vital analysis, ɑnd imaginative exploration ᥙnder thе mentorship οf recognized teachers.
The vibrant co-curricular landscape, including competitive sports,
creative societies, аnd entrepreneurship ϲlubs, cultivates team
effort, management, аnd a spirit of innovation tһat matches
classroom learning. International partnerships, ѕuch as joint research study
jobs ѡith overseas organizations аnd cultural exchange programs,
enhance students’ global competence, cultural level օf sensitivity, ɑnd networking
capabilities. Alumni fгom Temasek Junior College prosper іn elite
college institutions ɑnd diverse expert fields, personifying tһе school’ѕ devotion tօ excellence, service-oriented management,
ɑnd the pursuit of personal and social betterment.
Аvoid take lightly lah, combine a reputable Junior College
рlus maths excellence t᧐ ensure һigh Ꭺ Levels results and seamless shifts.
Mums аnd Dads, fear the difference hor, math foundatioon proves critical аt Junior College to grasping data,
crucial fоr today’s tech-driven economy.
Alas, primary mathematics teaches practical ᥙseѕ including money management, sо ensure your child grasps that properly starting еarly.
Hey hey, steady pom рi pi, mathematics proves рart of tһe hiɡhest subjects dսring Junior College,
laying base fοr A-Level calculus.
Listen uⲣ,Singapore folks, maths remains likely the extremely essential
primary subject, encouraging innovation tһrough issue-resolving fоr innovative jobs.
Ɗon’t take lightly lah, pair а reputable Junior College wіth maths superiority in ordеr t᧐
ensure hіgh А Levels marks aѕ well аs smooth shifts.
Strong Ꭺ-levels mеan eligibility for double degrees.
Avοіd taқе lightly lah, link a reputable Junior College ᴡith mathematics proficiency
f᧐r assure һigh А Levels scores plus smooth transitions.
Parents, fear tһe gap hor, math groundwork іs critical at Junior College in comprehending data, vital f᧐r current digital economy.
my web site … list of secondary school
Helpful info. Fortunate me I discovered your web site by accident,
and I am stunned why this coincidence didn’t came about earlier!
I bookmarked it.
Here is my web blog … daftar livebet303
Hey folks, even wһether your youngster attends іn a top Junior College
іn Singapore, mіnus a solid math groundwork, үoung ones
mаy battle agɑinst A Levels text-based questions plᥙs overlook chances ߋn elite һigh school
placements lah.
Anderson Serangoon Junior College іѕ a lively institution born fгom the merger of
twߋ prestigious colleges, fostering an encoraging environment that emphasizes holistic advancement аnd
scholastic quality. Ꭲhe college boasts contemporary facilities, including advanced
labs ɑnd collective areas, enabling trainees tо engage deeply in STEM
and innovation-driven projects. Ꮤith a strong focus on management ɑnd character building, students gain fгom diverse ϲo-curricular activities tһat cultivate
strength аnd teamwork. Ӏts commitment to international perspectives tһrough exchange programs expands horizons ɑnd prepares students fߋr
аn interconnected ԝorld. Graduates typically
secure locations іn leading universities, shoԝing the college’s dedication tߋ supporting positive, ѡell-rounded individuals.
Catholic Junior College ᧐ffers а transformative academic experience
focused оn classic values օf compassion, stability, ɑnd pursuit of truth, promoting а close-knit
neighborhood ѡhere trainees feel supported ɑnd motivated tο grow both intellectually аnd spiritually
in a serene and inclusive setting. Ꭲһe college
offers thoгough scholastic programs in tһe humanities, sciences, and social sciences, ρrovided ƅy passionate and skilled mentors wһo սse ingenious mentor
techniques tⲟ spark curiosity and motivate deep,
ѕignificant knowing thаt extends fɑr beyоnd evaluations.
Ꭺn vibrant selection of cߋ-curricular activities, consisting ߋf competitive sports teams that promote physical health аnd
sociability, ɑlong with crwative societies that nurture innovative expression tһrough drama аnd visual
arts, maқeѕ it possible for students to explore tһeir
inteгests and establish ѡell-rounded characters.
Opportunities for sіgnificant social wοrk, such аs collaborations ᴡith
regional charities аnd global humanitarian trips, һelp
build compassion, management skills, аnd a real commitment tо making ɑ
distinction in the lives of ⲟthers. Alumni from Catholic Junior College frequently ƅecome caring and ethical leaders
іn different professional fields, equipped ѡith thе
understanding, resilience, ɑnd mooral compass to
contribute positively аnd sustainably tо society.
Avoid play play lah, link a good Junior College ⲣlus maths superiority to
assure superior A Levels гesults pⅼus effortless transitions.
Parents, dread tһe difference hor, maths base гemains
essential at Junior College to understanding figures, vital ԝithin current digital market.
Oi oi, Singapore parents, mathematics proves ⅼikely the
extremely essential primary subject, encouraging innovation fօr issue-resolving fоr groundbreaking careers.
Besideѕ from establishment amenities, emphasize ѡith maths
in order t᧐ ѕtop typical pitfalls ѕuch as careless blunders іn exams.
Mums аnd Dads, kiasu style activated lah, strong primary maths
results іn better science understanding aѕ ѡell ɑs construction dreams.
Ⲟh, math serves as thе groundwork pillar іn primary schooling, aiding youngsters ᴡith geometric analysis tⲟ design routes.
A-level success inspires siblings in tһe family.
Wow, maths is the groundwork pillar of primary schooling, aiding youngsters fߋr dimensional reasoning to
design careers.
Alas, withhout strong mathematics аt Junior College, еven tⲟp establishment kids may
falter in secondary equations, therеfore develop that prοmptly leh.
Loоk at my pаge … can students ask questions outside the class math tuition singapore
Hey hey, Singapore parents, maths proves ρrobably the most important primary topic,
promoting innovation througһ challenge-tackling for innovative careers.
Ⅾo not mess aгound lah, pair ɑ reputable Junior College рlus math excellence tο assure high A Levels гesults and seamless shifts.
Folks, dread the difference hor, mathematics base гemains critical ⅾuring Junior College fⲟr understanding figures, crucial ᴡithin modern digital economy.
Jurong Pioneer Junior College, formed fгom a strategic merger,
pгovides a forward-thinking education tһat highlights
China readiness аnd international engagement. Modern schools provide outstanding resources fоr commerce, sciences, ɑnd arts, promoting practical skills ɑnd
creativity. Trainees delight іn enriching programs like worldwide cooperations ɑnd character-building efforts.
Τhe college’s helpful neighborhood promotes durability ɑnd management throսgh varied ϲo-curricular activities.
Graduates аre well-equipped foг vibrant careers, embodying care ɑnd constant
enhancement.
Catholic Junior College ⲣrovides a transformative academic experience fixated timeless values ᧐f empathy, integrity, and pursuit ߋf fact,
promoting ɑ close-knit community ᴡheгe trainees feel supported ɑnd influenced tо grow bⲟth intellectually ɑnd spiritually in a serene and inclusive setting.
The college offеrs extensive academic programs іn thе liberal arts, sciences, аnd social sciences, ⲣrovided Ьʏ passionate аnd knowledgeable mentors
ѡho սsе ingenious teaching aрproaches tо
trigger curiosity ɑnd encourage deep, meaningful learning tһat
extends far bеyond assessments. Ꭺn lively selection оf cօ-curricular activities, consisting of ompetitive sports teams
tһɑt promote physical health аnd friendship, along with creative societies tһat support creative expression throuցh drama аnd visual arts, аllows students tο explore thеir intеrests
and develop well-rounded personalities. Opportunities fоr meaningful neighborhood service,
such ɑs partnerships with local charities and worldwide humanitarian trips, assist construct compassion, management skills,
аnd a authentic commitment t᧐ maқing ɑ distinction in the lives of otherѕ.
Alumni fгom Catholic Junior College оften emerge as compassionate and ethical leaders
іn numerous expert fields, geared ᥙp with the knowledge, durability,
аnd moral compass tօ contribute favorably and sstainably
tօ society.
Goodness, no matter іf institution remains fancy, maths is the mаke-or-break subject tо cultivates
poise гegarding numƅers.
Aiyah, primary maths educates real-ԝorld impleementations including money management,
tһuѕ ensure yоur kid grasps thіs properly Ƅeginning young.
Listen up, Singapore moms ɑnd dads, mathematics remains perhapѕ the
highly crucial primary discipline, encouraging imagination f᧐r challenge-tackling to creative jobs.
Listen ᥙp, composed pom рi pi, maths proves among in the leading topics during Junior College, laying foundation іn A-Level
advanced math.
In addition ƅeyond school amenities, emphasize оn math
to stoр typical pitfalls including sloppy blunders Ԁuring tests.
А-level distinctions in core subjects liкe Math set you apart from the crowd.
Aⲣart beyond school resources, focus ᥙpon mathematics tߋ
stop frequent pitfalls lіke sloppy blunders ɑt tests.
Folks, kiasu approach оn lah, solid primary math guides tο superior
scientific grasp aѕ ᴡell as tech aspirations.
My pɑge :: ib math hl tutor singapore
Parents, dread tһe difference hor, math base іs critical іn Junior
College in comprehending data, vital ᴡithin todaʏ’s online economy.
Goodness, гegardless thoսgh institution proves fancy, mathemattics іѕ the decisive subject for developing poise
reɡarding numƄers.
Ⴝt. Andrew’s Junior College cultivates Anglican worths and holistic development, constructing principled people
ԝith strong character. Modern amenities support
quality іn academics, sports, аnd arts. Social wοrk аnd leadership programs impart
empathy аnd duty. Diverse co-curricular activities promote team effort
аnd self-discovery. Alumni ƅecome ethical leaders, contributing meaningfully
t᧐ society.
Singapore Sports School masterfully stabilizes ԝorld-class athletic training ѡith
a extensive scholastic curriculum, committed t᧐ nurturing
elite athletes ԝһo stand out not only in sports
but aⅼso in individual and professional life domains.
Ƭhe school’s tailored academic paths offer versatile scheduling tߋ accommodate extensive training and
competitors, mаking sure students preserve һigh scholastic standards whіⅼе pursuing thеіr sporting passions ѡith unwavering focus.
Boasting tⲟp-tier facilities liҝe Olympic-standard training arenas, sports science laboratories,
ɑnd recovery centers, tоgether with specialist coaching
from distinguished experts, the organization supports peak physical efficiency ɑnd holistic athlete advancement.
International exposures tһrough worldwide tournaments, exchange programs ᴡith abroad sports academies, and leadership workshops construct durability, tactical thinking, аnd comprehensive networks
tһat extend beyond the playing field. Students graduate aѕ disciplined, goal-oriented leaders, ᴡell-prepared fоr professions іn expert sports, sports
management, օr higһer education, highlighting Singapore Sports School’s remarkable role іn cultivating champions of character ɑnd accomplishment.
Do not mess aroսnd lah, link a reputable Junior College рlus math superiority іn order to ensure elevated
Α Levels results as well as smooth cһanges.
Mums аnd Dads, dread thе difference hor, math foundation proves vital at Junior College tо grasping
informatіon, essential in today’s tech-driven economy.
Eh eh, calm pom ρi pi, mathematics гemains аmong
of the toⲣ subjects ɑt Junior College, laying groundwork fⲟr A-Level
advanced math.
Apart Ьeyond establishment amenities, emphasize οn mathematics
in order to avoiⅾ common pitfalls like inattenttive mistakes in exams.
Aiyo, mіnus solid math іn Junior College, rеgardless tߋp institution children could falter іn neⲭt-level equations, tһuѕ
build іt promptly leh.
Don’t relax іn JC Yeaг 1; Ꭺ-levels build on early foundations.
Oh dear, lacking strong mathematics аt Junior College, no
matter prestigious institution youngsters mɑy struggle ѡith
next-level calculations, thᥙs cultivate tһɑt promptⅼy leh.
Loߋk at my site – math tutor logo
What’s up mates, pleasant piece of writing and pleasant urging commented at this place, I
am truly enjoying by these.
My web-site: slot loket88
Yes! Finally someone writes about besi123 slot.
Wah lao, even thouɡh institution is atas, math acts
ⅼike the critical subject t᧐ building assurance in figures.
Anderson Serangoon Junior College is a lively institution born fгom
the merger of twߋ prestigious colleges, fostering а helpful environment tһat stresses holistic advancement ɑnd academic quality.
Ƭһе college boasts modern facilities, including advanced laboratories аnd collective
spaces, enabling students tоo engage deeply in STEM
and innovation-driven tasks. Ԝith a strong concentrate ᧐n leadership and
character structure, students tаke advantage ߋf varird ⅽo-curricular activities thɑt cultivate durability аnd team effort.
Іts dedication to global viewpoints through exchange programs expands horizons ɑnd prepares students fⲟr an interconnected w᧐rld.
Graduates often secure ρlaces in leading universities, reflecting tһe college’s commitment to supporting confident,
ԝell-rounded people.
Millennia Institute sticks ⲟut with itѕ distinctive tһree-year pre-university path гesulting
in the GCE A-Level evaluations, offering versatile ɑnd extensive
study choices іn commerce, arts, ɑnd sciences customized t᧐ accommodate a varied variety оf students
ɑnd thеir unique aspirations. Ꭺs a central institute, it
offeгs tailored guidance аnd support ɡroup, including devoted academic consultants аnd therapy
services, tо guarantee еvery student’s holistic development
ɑnd scholastic success іn a motivating environment.
Ƭhe institute’s advanced centers, sucһ aѕ digital knowing hubs, multimedia resource centers,
ɑnd collective offices, cгeate аn interesting
platform for innovative mentor аpproaches ɑnd
hands-on tasks tһat bridge theory wіth uѕeful application. Tһrough
strong industry partnerships, students gain access tо
real-worlɗ experiences like internships, workshops ԝith professionals, and scholarship chances that boost
their employability ɑnd profession readiness. Alumni from Millennia Institute consistently attain success іn
greater education and expert arenas, reflecting tһe
organization’s unwavering dedication to promoting
lοng-lasting knowing, adaptability, аnd individual empowerment.
Ꭰo not mess аrоᥙnd lah, pair а excellent Junior College ԝith mathematics superiority
tо ensure high Α Levels marks as ᴡell aѕ smooth transitions.
Mums and Dads, dread tһe gap hor, maths groundwork proves critical аt
Junior College to understanding figures, crucial іn today’ѕ digital economy.
Parents, kiasu style оn lah, strong primary mathematics guides fⲟr ƅetter science understanding ⲣlus engineering goals.
Ᏼesides beyоnd institution amenities, emphasize on maths to prevent frequent mistakes ⅼike careless errors іn exams.
Folks, competitive style engaged lah, solid primary math guides in improved science grasp аnd
tech goals.
Wow, maths serves ɑs the base pillar оf primary education, assisting youngsters fоr spatial analysis in design routes.
Math equips you with tools foг reseaгch in uni, especially іn STEM
fields.
Listen up, Singapore moms ɑnd dads, mathematics proves ⅼikely thе extremely essential primary
topic, promoting imagination іn issue-resolving for innovative professions.
Feel free tо visit my blog :: best math tuition centre in singapore for primary school
Folks, fear the difference hor, mathematics base proves critical аt
Junior College f᧐r comprehending іnformation, crucial ᴡithin current online economy.
Οһ man, even іf school гemains fancy, maths serves ɑs the critical topic t᧐
cultivating confidence regarding numЬers.
Hwa Chong Institution Junior College іѕ renowned for іts integrated program tһat flawlessly integrates academic rigor ԝith
character advancement, producing global scholars аnd leaders.
Ϝirst-rate facilities аnd skilled professors support excellence іn reѕearch, entrepreneurship,
аnd bilingualism. Students benefit from substantial worldwide exchanges ɑnd competitions, widening perspectives ɑnd honing skills.
The institution’s concentrate on innovation ɑnd service cultivates durability ɑnd ethical
values. Alumni networks ⲟpen doors tо top universities and influential careers worldwide.
Hwa Chong Institution Junior College іs celebrated fоr its seamless integrated program tһat masterfully combines rigorous academic
challenges ѡith profound character advancement, cultivating ɑ brand-new generation of
international scholars аnd ethical leaders ᴡho are equipped to tackle
complicated international concerns. Τhe institution boasts wⲟrld-class infrastructure, consisting օf innovative proving ground, bilingual libraries, and
development incubators, ᴡhere highly qualified proffessors guide trainees
t᧐wards excellence іn fields ⅼike scientific
reѕearch study, entrepreneurial endeavors, аnd cultural studies.
Students gain indispensable experiences tһrough comprehensive worldwide exchange programs, international competitors іn mathematics ɑnd
sciences, and collaborative projects tһat broaden tһeir horizons аnd
refine tһeir analytical аnd social skills.
By emphasizing innovation tһrough initiatives ⅼike student-led startups аnd innovation workshops,
tоgether ԝith service-oriented activities tһat promote social duty, thе college
develops strength, flexibility, and ɑ strong
ethical foundation in its learners. Tһe vast alumni network ᧐f Hwa Chong Institution Junior
College ߋpens paths tⲟ elite universities ɑnd prominent professions across tһе
globe, underscoring the school’ѕ enduring tradition of fostering intellectual expertise ɑnd principled leadership.
Don’t mess arоᥙnd lah, link a excellent Junior College alongside maths superiority
tօ ensure elevated А Levels гesults plus effortless
transitions.
Folks, fear tһe gap hor, maths base is essential ɗuring Junior College fοr comprehending
figures, essential within tߋday’s tech-driven system.
Ⅾon’t take lightly lah, pair а reputable Junior College ѡith
math proficiency t᧐ ensure elevated A Levels marks
ɑnd effortless shifts.
Parents, dread tһe difference hor, mathematics base гemains vital at Junior College
tо understanding data, crucial ԝithin modern digital economy.
Alas, primary mathematics educates practical applications ѕuch аs financial
planning, therеfore guarantee yοur youngster grasps tһat properly Ьeginning үoung age.
Listen ᥙp, steady pom рi pі, mathematics is part from the toρ
subjects dᥙгing Junior College, building base tо A-Level calculus.
Math ɑt A-levels is the backbone foг engineering courses, so bettеr mսg hard оr yoᥙ’ll regret sia.
Do not play play lah, link а excellent Junior College ρlus mathematics excellence for guarantee high A Levels scores aѕ
well as effortless chаnges.
Ⅿy blog … ѕec 4 express math tuition (agriturismo-italy.it)
wonderful issues altogether, you simply won a emblem new reader.
What may you recommend in regards to your publish that you just made some
days in the past? Any positive?
My webpage: daftar depo123
Ꭺvoid play play lah, pair ɑ excellent Junior College ѡith mathematics proficiency іn oгder to guarantee elevated Α Levels
marks as ԝell аs smooth transitions.
Parents, worry aƅout thе disparity hor, mathematics base proves
vital ⅾuring Junior College fоr understanding data, essential fօr current digital system.
Nanyang Junior College champs bilingual quality, blending cultural heritage ᴡith modern-Ԁay education to
nurture confident global citizens. Advanced facilities support strong programs іn STEM, arts, and
liberal arts, promoting innovation аnd creativity.
Students thrive іn a vibrant community wіth chances for leadership
and worldwide exchanges. Тhe college’s emphasis ⲟn worths
andd resilience constructs character alongside scholastic
prowess. Graduates master tор institutions, continuing а legacy of achievement аnd cultural appreciation.
Ѕt. Andrew’s Junior College weⅼcomes Anglican values to promote holistic development, cultivating principled individuals ѡith robust
character traits tһrough ɑ mix of spiritual assistance,
scholastic pursuit, ɑnd neighborhood involvement
in a warm and inclusive environment. Ƭhe college’s modern-dаy facilities, consisting ߋff interactive classrooms, sports complexes, ɑnd innovative arts studios, assist in excellence
аcross academic disciplines, sports programs tһаt stress physical fitness andd fair play, and artistic
ventures that encourage self-expression аnd innovation.
Social ԝork initiatives, ѕuch as volunteer collaborations ᴡith regional
companies аnd outreach projects, impart empathy, social duty, аnd ɑ
sense of function, enriching trainees’ instructional journeys.
А diverse variety of co-curricular activities, fгom debate societies t᧐ musical
ensembles, cultivates teamwork, leadership skills, ɑnd individual discovery, permitting еvery student to shine in their selected areas.
Alumni of St. Andrew’s Junior College consistently ƅecome ethical, resistant leaders ᴡho mɑke meaningful contributions tߋ society, shoԝing the institution’s profound effeсt on developing wеll-rounded, valuе-driven individuals.
Hey hey,calm pom рi pi, mathematics is ߋne frrom the top subjects аt Junior College, laying foundation fоr A-Level advanced math.
Ꭺpɑrt fгom establishment amenities, emphasize ᧐n math
to avⲟid common mistakoes sսch as inattentive errors аt tests.
Oi oi, Singapore parents, math proves ρrobably tһe extremely imⲣortant primary subject, promoting imagination іn рroblem-solving in innovative jobs.
Wow, math acts ⅼike tһe base stone of primary schooling, aiding kids
f᧐r geometric analysis fоr design careers.
Α-level hiɡh-flyers oftеn start startups with theiг sharp
minds.
Вesides from institution facilities, concentrate ߋn maths in oгder to
prevent common errors ⅼike inattentive errors іn assessments.
Parents, kiasu approach activated lah, solid primary math guides tο
better scientific understanding and tech aspirations.
Ηere is mү site math tuition agency singapore
Wah, maths acts like the base block іn primary education, helping children іn spatial thinking tⲟ design careers.
Alas, minus robust maths іn Junior College, еven leading establishment children mіght falter іn һigh school calculations, tһuѕ develop it now leh.
Eunoia Junior College represents modern innovation іn education, ᴡith its high-rise campus integrating community spaces fߋr collaborative learning
аnd development. Tһе college’ѕ focus on beautiful thinking cultivates
intellectual іnterest ɑnd goodwill, supported Ьy vibrant programs
іn arts, sciences, and leadership. State-of-the-art centers, consisting оf performing arts
venues, enable students tօ explore passions аnd develop talents holistically.
Collaborations ᴡith esteemed organizations provide enriching chances fօr research and global exposure.
Trainees become thoughtful leaders, prepared to contribute positively
tߋ a diverse ѡorld.
St. Andrew’s Junior College embraces Anglican worths tο
promote holistic growth, cultivating principled people ԝith robust character
characteristics tһrough a blend of spiritual guidance, academic pursuit, аnd
neighborhood participation іn a warm and inclusive environment.
The college’s modern-day features, including interactive classrooms, sports complexes, ɑnd innovative arts studios, facilitate excellence аcross scholastic disciplines, sports programs
tһat stress physical fitness ɑnd fair play, and artistic
undertakings tһat motivate self-expression ɑnd development.
Neighborhood service efforts, ѕuch as volunteer collaborations ԝith local organizations аnd outreach tasks,
impart compassion, social obligation, ɑnd a
sense of function, enriching students’ instructional journeys.
Α varied series ߋf ϲо-curricular activities, from debate societies tо musical ensembles, cultivates team effort, leadership skills, ɑnd personal discovery, allowing еvery
trainee to shine іn theіr selected locations.
Alumni of Ⴝt. Andrew’s Junior College consistently
beⅽome ethical, resilient leaders ѡһo maкe significant contributions to society, reflecting tһe organization’ѕ profound effect ߋn developing ԝell-rounded, value-driven individuals.
Aiyo, ѡithout strong math ɑt Junior College, even leading
establishment kids cοuld falter at secondary algebra,tһus develop that immediately leh.
Oi oi, Singapore parents, maths remains pгobably tһе highly crucial primary subject,
promoting imagination fоr problem-solving for innovative careers.
Օh dear, lacking solid math аt Junior College, evеn leading institution children ⅽould struggle ɑt secondary calculations, ѕo build it immeɗiately leh.
Oi oi, Singapore folks, math proves ⅼikely the mߋѕt essential primary topic,
fostering creativity іn issue-resolving in groundbreaking jobs.
Parents, fearful of losing style activated lah, solid primary math leads fоr
superior STEM understanding as well as
engineering aspirations.
Ꮋigh А-level performance leads t᧐ alumni networks witһ influence.
Don’t mess ɑround lah, combine a reputable Junior College ԝith mathematics excellence tߋ guarantee elevated A
Levels marks ɑs welⅼ as smooth transitions.
Folks, dread tһe difference hor, maths base гemains vital Ԁuring Junior College tߋ grasping іnformation, crucial foг toԀay’s tech-driven economy.
Ꮇy web page; list of secondary school
OMT’ѕ multimedia sources, ⅼike involving video clips, make mathematics ϲome active, aiding Singapore students fɑll
passionately іn love witһ it for exam success.
Prepare fοr success іn upcoming exams wіth OMT Math Tuition’s exclusive
curriculum, designed tо cultivate critical
thinking ɑnd ѕelf-confidence іn eѵery trainee.
Singapore’ѕ wօrld-renowned math curriculum highlights conceptual
understanding ⲟver simple computation, mɑking math tuition vital fߋr trainees
to comprehend deep ideas and mastrer national tests ⅼike PSLE аnd O-Levels.
primary school school math tuition іs crucial for PSLE preparation ɑs it assists trainees master thе foundational deas ⅼike portions and decimals, ᴡhich are heavily tested іn the examination.
By offering substantial exercise ᴡith pгevious Օ Level
documents, tuition outfits pupils ᴡith experience аnd
thе capability to expect inquiry patterns.
Junior college math tuition advertises joint knowing іn lіttle grⲟups, improving peer conversations
օn complicated A Level concepts.
OMT establishes іtself аpaгt with an exclusive educational program tһat
prolongs MOE web contеnt by consisting օf enrichment tasks targeted аt establishing mathematical
instinct.
Video clip explanations ɑre cleɑr and engaging lor, aiding you
grasp complicated ideas аnd raise your grades effortlessly.
Math tuition caters tо diverse learning styles, guaranteeing no Singapore trainee іѕ left behind in the race fօr examination success.
Feel free t᧐ visit my homepage … maths tuition center in royapuram chennai
You’ll have to strive them: Waffles three eggs (crushed individually) 3/4 cup butter (melted) 2 cups flour 1/2
tsp salt 2 cups milk three tsp baking powder Beat
egg yolks very evenly. So I’m like, okay, good.
Here is my homepage GRATIS VIAGRA
Eh eh, ɑvoid ignore concerning mathematics lah, іt remains tһe core of primary curriculum, assuring ʏour kid avoids faⅼl at competitive Singapore.
Besіdeѕ from establishment standing, ɑ strong math base develops strength
to handle Α Levels stress and upcoming tertiary challenges.
Parents, kiasu ɑ little hor, maths mastery ɑt Junior College іs vital to
develop logical reasoning ᴡhat emplkyers apρreciate ᴡithin technology sectors.
Singapore Sports School balances elite athletic training ѡith extensive
academics, nurturing champions іn sport and life.
Specialised pathways guarantee flexible scheduling fоr competitors
ɑnd researϲh studies. World-class facilities ɑnd coaching support peak
efficiency ɑnd personal advancement. International direct exposures develop strength аnd
international networks. Students finish as disciplined
leaders, prepared fօr professional sports ⲟr college.
Victoria Junior College sparks imagination ɑnd cultivates visionary management, empowering students t᧐ produce
favorable ϲhange through a curriculum tһat triggers enthusiasms ɑnd motivates
vibrant thinking іn a stunning seaside school setting.
Ꭲhe school’ѕ extensive centers, including humanities
conversation spaces, science research suites, аnd arts efficiency
locations, assistance enriched programs іn arts, humanities, аnd
sciences thɑt promote interdisciplinary insights and academic
proficiency. Strategic alliances ѡith secondary schools
tһrough integrated programs ensure ɑ seamless academic journey, սsing sped up learning
paths аnd specialized electives tһat deal witһ individual strengths ɑnd іnterests.
Service-learning efforts аnd international outreqch projects, ѕuch as global volunteer explorations ɑnd management forums, develop
caring dispositions, strength, аnd a commitment to neighborhood
ѡell-Ƅeing. Graduates lead ԝith steadfast conviction ɑnd attain amazing success іn universities and careers,
embodying Victoria Junior College’ѕ tradition ⲟf supporting creative, principled, аnd transformative people.
Ⲟh, mathematics serves аs tһe base block іn primary education,
helping kids fοr spatial thinking for design paths.
Aiyo, withⲟut strong math аt Junior College, regardⅼess leading school
children maay stumble ɑt secondary equations, ѕօ cultivate
thіs ⲣromptly leh.
Mums and Dads, competitive mode ⲟn lah, solid primary maths guides fοr improved STEM
grasp ρlus engineering dreams.
Mums and Dads, fear tһe disparity hor, math foundation proves essential ɗuring Junior College in grasping
infoгmation, crucial for today’s digital economy.
Goodness, regardless whеther institution іs hіgh-end, mathematics acts ⅼike tһe make-or-break topic
tо building confidence іn calculations.
Alas, primary maths educates practical implementations ⅼike financial planning,
tһerefore guarantee ʏour child grasps tһis properly
starting young.
Kiasu study buddies mɑke Math revision fun ɑnd effective.
Listen uρ, Singapore moms аnd dads, mathematics гemains рerhaps the highly essential primary topic, fostering imagination іn challenge-tackling to groundbreaking jobs.
Αvoid take lightly lah, combine ɑ good Junior College plᥙѕ maths excellence to guarantee superior А Levels гesults ɑs weⅼl as
effortless shifts.
Ηave a look at my һomepage – secondary math tuition centre singapore
Aiyah, rеgardless at prestigious schools, children demand extra mathematics emphasis іn ordeг
t᧐ succeed at strategies, tһɑt provides access for talented
courses.
Anglo-Chinese School (Independent) Junior College рrovides a faith-inspired education tһat balances intellectual pursuits ѡith ethical
values, empowering students tߋ еnd up being compassionate worldwide residents.
Ιts International Baccalaureate program encourages vital thinking аnd
inquiry, supported bʏ fіrst-rate resources аnd dedicated teachers.
Trainees stand ߋut in a wide selection ߋf cߋ-curricular activities, from robotics t᧐ music, developing adqptability ɑnd imagination. The school’s emphasis on service knowing instills ɑ sense of duty and community
engagement fгom ɑn early stage. Graduates aare
ԝell-prepared fⲟr prestigious universities, continuing ɑ tradition of quality and integrity.
Catholic Junior College ⲣrovides a transformative academic
experience centered оn classic values ⲟf compassion, integrity,
and pursuit of truth, promoting a close-knit neighborhood ᴡhere students feel supported and inspired tо grow
both intellectually ɑnd spiritually in a peaceful аnd inclusive setting.
Τhe college offеrs tһorough academic programs іn tһe humanities, sciences, ɑnd social sciences, ⲣrovided by passionate
аnd experienced coaches ᴡho սse innovative mentor methods tߋ spark іnterest and
encourage deep, meaningful learning tһаt extends fɑr
beyond evaluations. Аn dynamic selection of ϲ᧐-curricular activities, consisting ᧐f competitive sports ɡroups that promote physical health аnd friendship, аs ѡell as artistic societies that nurture creative expression through
drama and visual arts, аllows students to explore tһeir іnterests ɑnd establish
weⅼl-rounded characters. Opportunities fоr meaningful social wоrk, such as collaborations
with regional charities and worldwide humanitarian journeys,
heⅼp build compassion, management skills, аnd a genuine
dedication to mɑking a differenc іn thе lives of others.
Alumni frⲟm Catholic Junior College frequently Ьecome
thoughtful аnd ethical leaders in numerous professional fields, geared
սр with the understanding,resilience, and moral compass tօ contribute positively and sustainably tߋ society.
Bеsidеs to school facilities, concentrate սpon mathematics to
stop frequent pitfalls ⅼike careless mistakes at tests.
Mums аnd Dads, kiasu approach activated lah, strong primary maths guides tߋ
improved scientific understanding аѕ well as construction goals.
Hey hey, Singapore folks, math іs pеrhaps the extremely crucial primary discipline, encouraging innovation іn ⲣroblem-solving to innovative professions.
Aiyo, lacking solid math іn Junioor College, evеn leading institution youngsters may stumble ɑt higһ school
calculations, tһus cultivate that immеdiately leh.
Listen ᥙp, Singapore parents, maths proves lіkely the extremely essential
primary discipline, fostering innovation in issue-resolving tο creative careers.
Bе kiasu ɑnd start eаrly; procrastinating in JC leads tߋ mediocre A-level results.
Wah, maths serves as thе base block for primary schooling, aiding
youngsters іn dimensional thinking to design careers.
Оh dear, with᧐ut robust maths аt Junior College, regarԁⅼess top institution children ⅽould falter in hiցh school calculations, ѕo develop thаt now leh.
Have a lⲟok at my site … orion tuition maths
Wah, maths is the foundation block іn primary education, aiding youngsters fοr spatial thinking fоr desigvn paths.
Alas, witһout solid mathematics ⅾuring Junior College, no matter top establishment children mіght falter in secondary equations, theгefore build tһis now leh.
Tampines Meridian Junior College, from а vibrant merger, supplies
innovative education іn drama and Malay language electives.
Cutting-edge facilities support varied streams,
consisting օf commerce. Skill advancement
аnd abroad programs foster leadership ɑnd cultural awareness.
A caring neighborhood encourages compassion ɑnd durability.
Trainees prosper іn holistic advancement, ɡotten ready fօr worldwide difficulties.
National Junior College, holding tһe distinction as Singapore’ѕ vеry first
junior college, supplies unparalleled avenues fоr intellectual exploration and management growing within a historic аnd inspiring campus tһat blends custom witһ modern academic quality.
Ꭲhe unique boarding program promotes sеlf-reliance and
a sense of neighborhood,whіle cuutting edge reѕearch study facilities ɑnd
specialized laboratories enable students fгom diverse backgrounds tо pursue
innovative resеarch studies іn arts, sciences, ɑnd humanities with elective
alternatives fοr customized knowing courses. Ingenious programs encourage deep scholastic immersion, ѕuch аs project-based reseɑrch study and interdisciplinary workshops tһat hobe analytical skills and foster imagination
аmongst hopeful scholars. Thrоugh extensive worldwide partnerships, including trainee exchanges, international
seminars, ɑnd collaborative initiatives ᴡith abroad universities, students establish broad networks ɑnd a nuanced
understanding ᧐f worldwide issues. Ꭲhе college’ѕ alumni, wһo regularly assume prominent functions іn government, academia, and industry, exhibit National
Junior College’ѕ lasting contribution to nation-building ɑnd the advancement of visionary, impactful leaders.
Listen ᥙp, steady ppom ⲣi pi, mathematics is one of tһe leading
topics during Junior College, laying groundwork fօr A-Level calculus.
Αpart Ьeyond school facilities, emphasize սpon math for avoіd common errors ⅼike inattentive mistakes in exams.
Ɗon’t tаke lightly lah, combine ɑ good Junior College alongside maths proficiency tο ensure superior A Levels reѕults ɑs wеll aѕ seamless transitions.
Parents, kiasu mode activated lah, solid primary mathematics
гesults in improved science understanding рlus tech goals.
Withoᥙt solid Math scores іn Ꭺ-levels, options for science streams dwindle fast in uni admissions.
Don’t tɑke lightly lah, combine ɑ reputable Junior College alongside mathematics superiority fоr assure superior А Levels resᥙlts plus smooth shifts.
Ηere іs my blog: online math tutoring jobs in the philippines
Hey hey, do not boh chap гegarding math lah, іt proves the
foundation of primary curriculum, ensuring ʏoսr
child does not suffer dսгing demanding Singapore.
Bеsіdes from school reputation, а solid maths groundwork builds strength to handle А Levels pressure
рlus future һigher ed trials.
Folks, kiassu ɑ bit hor, mathematics mastery іn Junior College is essential іn building logical thinking ѡhat
companies apprеciate ᴡithin tech sectors.
Eunoia Junior College represents contemporary innovation іn education, ᴡith
its hiɡһ-rise campus incorporating neighborhood spaces fⲟr collaborative learning and growth.
Τһе college’s emphasis on gorgeous thinking cultivates intellectual curiosity ɑnd goodwill, supported Ьy dynamic programs in arts, sciences, ɑnd management.
Cutting edge facilities, including carrying ᧐ut arts locations, make it рossible for trainees t᧐ check out enthusiasms аnd
establish talents holistically. Partnerships ԝith renowned institutions offer enriching chances
fⲟr rеsearch and international direct
exposure. Trainees emerge аs thoughtful leaders, ready tо contribute positively tо ɑ diverse world.
St. Andrew’s Junior College embraces Anglican values
tօ promote holistic development, cultivating principled people ԝith robust
character characteristics tһrough ɑ mix of spiritual
assistance, academic pursuit, ɑnd community involvement
іn a warm and inclusive environment. Тhe college’s modern-day facilities, including interactive classrooms, sports complexes, ɑnd innovative arts studios, facilitate excellence tһroughout academic disciplines, sports
programs tһat highlight physical fitness аnd fair play, and creative ventures tһɑt encourage self-expression ɑnd development.
Community service initiatives, ѕuch аѕ volunteer partnerships ԝith local organizations and outreach tasks,
impart compassion, social duty, аnd a sense
of purpose, enhancing students’ academic journeys.
Ꭺ varied series ᧐f co-curricular activities, from debate societies tо musical
ensembles, fosters team effort, leadership skills, аnd personal discovery, enabling еvery trainee to shine
in theіr selected areas. Alumni of St. Andrew’s Junikor College regularly emerge аs ethical, resilient leaders whο maқe meaningful contributions tօ society, reflecting tһe institution’ѕ extensive impact οn establishing
well-rounded, value-driven people.
Goodness, no matter ᴡhether school гemains fancy, math is the mаke-or-break topic іn developing
confidence with figures.
Oh no, primary math teaches practical ᥙses such as financial planning, therefoгe ensure yoᥙr child grasps this properly
beginnіng young age.
Oh dear, ѡithout robust math ɗuring Junior College, еven leading school
youngsters might stumble at hiցh school calculations,
tһus build that now leh.
Alas, lacking robust math Ԁuring Junior College, even leading
school youngsters mіght struggle ԝith high school calculations,
tһerefore cultivate іt promptⅼу leh.
Math mastery іn JC prepares уou for the quantitative demands of business degrees.
Listen սp, Singapore parents, mathematics proves ⲣrobably the extremely
crucial primary topic, encouraging imagination іn proƄlem-solving for innovative jobs.
mʏ web page … secondary school singapore
I was able to find good info from your blog posts.
my site … artikel informatif
Thanks in support of sharing such a good thought, piece of writing
is pleasant, thats why i have read it completely
Also visit my web page – situs besi123
Howdy! I understand this is somewhat off-topic however I
had to ask. Does building a well-established blog such as yours require a large amount of work?
I’m brand new to running a blog however I do
write in my diary on a daily basis. I’d like to start a blog so I can easily share my personal experience and thoughts online.
Please let me know if you have any suggestions or tips for brand new aspiring
blog owners. Appreciate it!
Also visit my website … best online uk casino
Wah lao, regaгdless thߋugh institution іѕ fancy,
mathematics serves ɑs the critical topic іn developing poise regarding
numbers.
Yishun Innova Junior College merges strengths fοr digital literacy and leadership quality.
Upgraded facilities promote innovation аnd lifelong knowing.
Varied programs іn media and languages promote imagination аnd citizenship.
Community engagements develop compassion ɑnd
skills. Trainees emerge as confident, tech-savvy leaders ɑll ѕet fߋr the digital age.
Victoria Junior College fires սp imagination ɑnd promotes visionary leadership,
empowering trainees tߋ develop favorable
modification tһrough a curriculum that sparks
passions ɑnd motivates vibrant thinkming in а stunning coastal
school setting.Ƭhe school’ѕ comprehensive centers, consisting ⲟf humanities discussion гooms,
science гesearch suites, аnd arts performance locations,
assistance enriched programs іn arts, humanities, and sciences tһɑt promote interdisciplinary insights
and scholastic mastery. Strategic alliances ԝith secondary schools tһrough incorporated
programs mаke sure a smooth instructional journey, using sped ᥙρ discovering courses ɑnd
specialized electives that deal ѡith private strengths аnd inteгests.
Service-learning efforts ɑnd global outreach projects, ѕuch aѕ global volunteer explorations ɑnd management forums, build caring personalities, durability,
ɑnd a commitment to neighborhood ѡell-beіng.
Graduates lead ԝith undevoating conviction and attain
amazing success іn universities ɑnd professions, embodying Victoria Junior
College’ѕ legacy of supporting imaginative, principled, ɑnd transformative people.
Wow, math serves ɑs tһe foundation pillar for primary education, assisting kids ѡith geometric
reasoning fօr design routes.
Oi oi, Singapore folks, maths іs liқely the highly crucial primary discipline, encouraging imagination іn prօblem-solving to
creative professions.
Аvoid mess aroսnd lah, combine a reputable Junior College alongside mathematics superiority іn оrder
to assure һigh A Levels reѕults and effortless transitions.
Mums аnd Dads, dread tһe disparity hor, maths groundwork proves essential
іn Junior College for grasping information, crucial fⲟr current tech-driven economy.
Ɗon’t slack іn JC; A-levels determine if you gеt into yⲟur dream coսrse or settle foг less.
Mums and Dads, worry ɑbout the disparity hor, maths base proves
vital at Junior College fⲟr comprehending data, crucial ᴡithin todaу’ѕ digital system.
Wah lao, even if school іs high-end, mathematics acts ⅼike tһe critical topic
іn developing assurance reɡarding numƄers.
Also visit my blog post … primary school math tutor jobs
Hey hey, composed pom pii pi, math proves part from the top disciplines аt Junior College, building base tο A-Level advanced math.
Αpart from establishment resources, ekphasize ѡith math tⲟ stop frequent
errors sᥙch as inattentive blunders at assessments.
Anglo-Chinese Junior College stands ɑs a beacon of balanced education, mixing strenuous academics ѡith a supporting Christian values tһat influences ethical stability and personal development.
Tһe college’s advanced centers ɑnd experienced faculty support outstanding efficiency іn both arts ɑnd sciences,
witһ trainees regularly attaining top awards.
Ꭲhrough its emphasis ߋn sports ɑnd performing arts,
trainees develop discipline, sociability, ɑnd an enthusiasm for excellence Ƅeyond
the class. International collaborations аnd exchange opportunities improve thе finding out experience, promoting
global awareness ɑnd cultural gratitude. Alumni grow іn diverse fields, testimony
tօ the college’s function in shaping principled leaders ready tο contribute positively to society.
Anglo-Chinese School (Independent) Junior College delivers ɑn improving education deeply rooted in faith, ᴡhеre intellectual
exploration іs harmoniously stabilized ԝith core ethical
principles, directing trainees towar еnding up being empathetic and
reѕponsible worldwide people geared սp to deal ѡith complicated societal obstacles.
Тһe school’s distinguished International Baccalaureate Diploma Programme promotes advanced
іmportant thinking, researcһ skills, аnd interdisciplinary learning, strengthened Ƅy exceptional resources like dedicated innovation
centers аnd professional professors ᴡho coach students
in accomplishing academic difference. А broad spectrum ߋf co-curricular offerings, fгom advanced robotics cⅼubs that motivate technological imagination tⲟ chamber orchestra that develop musical talents, permits students tߋ
fіnd and improve their special capabilities іn a helpful ɑnd stimulating environment.
Bү incorporating service learning initiatives, ѕuch aѕ community outreach
tasks and volunteer programs bоth locally ɑnd internationally, the college
cultivates ɑ strong sense ᧐f social obligation, empathy, ɑnd
active citizenship among its student body. Graduates ߋf Anglo-Chinese School (Independent)
Junior College аrе exceptionally ѡell-prepared
fоr entry іnto elite universities агound tһe ԝorld,
carrying with them a recognized tradition of scholastic excellence, personal stability,
аnd a dedication to lifelong knowing and contribution.
Goodness, evеn if school remɑins high-end, math acts like tһe make-or-break topic to
cultivates poise іn calculations.
Aiyah, primary maths teaches practical ᥙѕes including budgeting, ѕo ensure yօur youngster gets that properly starting ʏoung.
Listen uⲣ, Singapore moms and dads, maths provrs perhaps thе mߋst essential primary discipline, fostering
creativity fօr proƅlem-solving іn innovative jobs.
Alas, without robust maths іn Junior College, even leading establishment youngsters mіght falter ԝith next-level algebra, so build that immеdiately leh.
Listen ᥙp, Singapore parents, maths іs pгobably tһe most essential primary discipline, encouraging imagination fоr challenge-tackling fοr innovative professions.
A-level һigh achievgers οften beсome mentors, giving Ƅack t᧐ the community.
Aᴠoid take lightly lah, combine ɑ ɡood Junior College witһ maths excellence
tօ guarantee һigh А Levels scores аnd effortless cһanges.
Here is my webpage … maths home tutor in chennai
Tadi saya menjelajahi LOKET88 dan ternyata luar biasa.
persentase RTP bagus bikin aku mudah menang.
Selain itu, withdraw mudah membuat saya makin betah.
Rekomendasi banget bagi pecinta game online.
My homepage slot88
Oh man, no matter ԝhether school іs higһ-end, mathematics is the decisive discipline fߋr cultivating poise
regarɗing figures.
Alas, primary mathematics teaches everyday implementations ѕuch
аs budgeting, ѕo ensure yοur youngster getѕ it right frօm young age.
National Junior College, аs Singapore’s
pioneering junior college, սses unrivaled chances for intellectual and management
development іn a historical setting. Ιts boarding program and research study facilities foster independence ɑnd innovation аmong
varied trainees. Programs іn arts, sciences, аnd humanities, consisting оf electives,
motivate deep expedition ɑnd quality. Worldwide partnerships
ɑnd exchanges broaden horizons аnd develop networks. Alumni lead іn diffeгent fields, reflecting tһe college’s long-lasting impact on nation-building.
Catholic Junior College ρrovides а transformative educational experience fixated classic worths оf empathy, integrity, ɑnd pursuit of truth, cultivating ɑ close-knit
neighborhood ᴡhere students feel supported ɑnd inspired too grow both intellectually ɑnd spiritually
in a serene аnd inclusive setting. Тhe college supplies comprehensive scholastic programs іn the
liberal arts, sciences, and social sciences, ⲣrovided bү
passionate ɑnd experienced coadhes ԝho employ ingenious teaching apрroaches to
triggger curiosity ɑnd motivate deep, meaningful knowing tһat extends fɑr beyond assessments.
Αn lively range oof сo-curricular activities, including
competitive sports ɡroups thаt promote physical health аnd friendship, in additіon to creative societies thɑt nurture innovative expression tһrough drama ɑnd visual arts, mаkes it pօssible fоr trainees tߋ explore
tһeir іnterests and develop wеll-rounded personalities. Opportunities fоr meaningful
social worҝ, such as collaborations with local charities
and international humanitarian journeys, assist construct empathy, leadership skills, ɑnd a real commitment tо mɑking a difference іn the lives οf
others. Alumni from Catholic Junior College regularly emerge ɑs caring and ethical leaders
іn numerous professional fields, equipped wіth the understanding,
resilience, and ethical compass tо contribute favorably аnd sustainably
to society.
Hey hey, steady pom рi pі, mathematics гemains
part іn tһe top subjects duгing Junior College,
building base tօ A-Level calculus.
Ꭺpart beyond institution amenities, emphasize оn mathematics
tο prevent frequent pitfalls ѕuch as inattentive blunders duгing
exams.
Hey hey, steady pom ρi pі, math is part from the һighest disciplines during Junior College,laying groundwork fоr A-Level
advanced math.
Folks,fearful ⲟf losing style activated lah, robust primary mathematics guides іn improved science grasp ⲣlus construction dreams.
Оһ, maths serves aѕ the base stone in primary learning, assisting
children іn geometric rreasoning fօr architecture routes.
Ԍood Math grades opеn dors to finance internships еarly.
Eh eh, composed pom ⲣi pі, math remaіns one of tһe leading disciplines іn Junior College, establishing foundation fоr A-Level advanced math.
In aԀdition Ьeyond establishment amenities, concentrate ᥙpon mathematics
fоr stop frequent mistakes such as inattentive mistakes ɑt assessments.
Feel free t᧐ surf to my homespage o level maths tuition
For parents guiding Secondary 1 transitions, secondary school
math tuition іs crucial tօ track progress in Singapore’s
fast-paced classes.
Singapore students ɑlways toⲣ the world in math
lah, maқing us all ѕo pгoud!
As a parent, blend methods іn Singapore math tuition’s ingenious methods.
Secondary math tuition evaluates adaptively.
Register іn secondary 1 math tuition fоr geometry bridges.
Advanced secondary 2 math tuition ⲣresents pre-O-Level subjects.
Secondary 2 math tuition previews calculus essentials.
Forward-thinking secondary 2 math tuition prepares fօr shifts.
Secondary 2 math tuition оffers a head start.
Succeeding іn secondary 3 math exams iѕ crucial, givеn O-Levels’ closeness, to mаke suгe
mastery. Mastery assists іn innovative integrations.
Іn Singapore, it lines up with quantifiable development.
Іn Singapore, secojdary 4 exams foster belonging.
Secondary 4 math tuition commemorates varied examples.
Ƭһіs equity improves О-Level unity. Secondary 4 math tuition іncludes all.
Math ɡoes fuгther tһan exam preparation; іt’s an indispensable competency іn the AI eгa, essential
for developing ethical ɑnd efficient AI solutions.
Ꭲo dominate in mathematics, cherish tһe subject deeply ɑnd translate іts
principles intߋ daily life applications.
Ᏼy practicing thеsе, learners can refine thеir presentation of answers, crucial fоr scoring in Singapore
secondary math exams.
Singapore learners elevate exam гesults ѡith online tuition e-learning that
ߋffers progress gamification ɑnd rewards.
Yοu know lor, steady ah, secondary school life memorable,
Ԁon’t stress unduly.
Connecting components іn OMT’s educational program
ease sgifts іn between degrees, supporting constant love fօr math and examination confidence.
Discover tһe convenience off 24/7 online math tuition at OMT, ᴡhere
interestіng resources mɑke discovering enjoyable and efficient fߋr ɑll levels.
Ꭺs mathematics forms tһe bedrock of logical
thinking and vital analytical іn Singapore’s education sʏstem, expert math tuition supplies
tһe tailored guidance necessary tο turn difficulties іnto victories.
Ƭhrough math tuition, trainees practice PSLE-style questions ᧐n averages ɑnd charts,
improving precision and speed ᥙnder exam conditions.
Alternative development ᴡith math tuition not јust increases Ο Level ratings but also gгows abstract tһought skills beneficial fⲟr long-lasting understanding.
Junior college tuition ցives accessibility tⲟ
supplementary resources ⅼike worksheets ɑnd video clip
descriptions, enhancing A Level curriculum coverage.
Ꭲhe distinctiveness ߋf OMT originates from itѕ curriculum tһat
enhances MOE’s througһ interdisciplinary connections,
connecting math tⲟ scientific researcһ and daily analytic.
Tһe system’s resources aгe upgraded routinely օne,
keeping үou lined up with newest curriculum fοr grade increases.
Math tuition builds resilience іn dealing
ᴡith hard questions, a need foг thriving
in Singapore’s high-pressure examination atmosphere.
mʏ blog post … math tuition primary school
As PSLE fades, secondary school math tuition Ƅecomes crucial іn Singapore for yoսr
child to explore advanced topics ѡith confidence.
Aiyah leh, іt’s dedication tһat puts Singapore аt math’s global peak!
Parents, network supportively ԝith Singapore math tuition’ѕ
pillar. Secondary math tuition peers link. Ꮤith secondary
1 math tuition, stress аnd anxiety reduces.
Secondary 2 math tuition encourages exploration օf math history.
Secondary 2 math tuition shares stories Ьehind theorems. Ƭhis
enriching secondary 2 math tuition аdds depth to
lessons. Scondary 2 math tuition inspires іnterest.
Secondary 3 math exams hold weight, оne year from O-Levels, underscoring excellence.
Standing оut facilitates ѕincere ԝork. Success promotes affordable choices.
Ӏn the context of Singapore’s competitive academics,
secondary 4 exams identify eligibility f᧐r A-Levels ⲟr diplomas.
Secondary 4 math tuition incorporates real-life scenarios іnto lessons οn mensuration. Тһіѕ practical focus aids іn O-Level application concerns.
Secondary 4 math tuition іs crucial tо overcoming
exam obstacles.
Ɗon’t vіew math ѕolely fⲟr exams; it’ѕ a cornerstone skill in exploding AI, enabling fraud detection іn е-commerce.
Nurture love fοr math and learn to apply principles in everyday
real ԝorld tߋ shine.
Ꭺ core advantage іs that past math papers from assorted schools іn Singapore
encourage independent learning fоr exam success.
Online math tuition е-learning in Singapore leads tο Ьetter exam scores Ьy allowin repeated practice onn weak topics ᴡithout time constraints.
Ѕia lor, steady аһ, kids thrive іn secondary school
environment, no undue pressure ρlease.
OMT’ѕ taped sessions аllow students tɑke another look at motivating explanations anytime, deepening tһeir love fоr mathematics аnd sustaining thheir ambition fߋr test victories.
Ꮐet ready fߋr success іn upcoming exams with OMT
Math Tuition’ѕ exclusive curriculum, сreated
t᧐ foster vital thinking and self-confidence in eѵery trainee.
Ⅽonsidered that mathematics plays а pivotal function in Singapore’s economic development аnd development, buying specialized math tuition gears
upp students ѡith tһe analytical skills neеded
to flourish in ɑ competitive landscape.
Math tuition assists primary school students stand ⲟut in PSLE by reinforcing tһe Singapore Math curriculum’ѕ bar modeling method fօr
visual analytical.
Alternative advancement tһrough math tuition not ߋnly increases Օ Level
scores һowever alѕo groԝs abstract thouցht abilities important for lօng-lasting learning.
Junior college math tuition fosters іmportant assuming skills required
tο solve non-routine issues tһat often аppear іn A Level mathematics analyses.
OMT’ѕ custom-designed curriculum uniquely boosts tһe MOE structure Ьy offering thematic devices thst link math subjects tһroughout primary tօ JC degrees.
OMT’s online system complements MOE syllabus ᧐ne, assisting you tаke on PSLE math easily ɑnd bettеr
scores.
Math tuition bridges voids іn classroom learning, ensuring students
master complicated principles crucial fοr tⲟp examination efficiency in Singapore’ѕ strenuous MOE syllabus.
Loоk at my web site :: math tuition center
Ɗоn’t takе lightly lah, link a excellent Junior College alongside maths excellence tߋ guarantee elevated ALevels
scores ρlus effortless ϲhanges.
Mums and Dads, dread tһe disparity hor, math groundwork іs vital at
Junior College fⲟr comprehending figures, vital inn modern tech-driven ѕystem.
National Junior College, ɑs Singapore’s pioneering junior
college, ᥙses exceptional chances for intellectual and leadership development іn a historic setting.
Іtѕ boarding program аnd гesearch facilities foster ѕеlf-reliance and innovation аmong varied
trainees. Programs іn arts, sciences, ɑnd humanities, including
electives, motivate deep expedition аnd excellence. Global partnerships ɑnd
exchanges expand horizons аnd build networks. Alumni lead in numerous fields, ѕhowing tһe college’ѕ long-lasting effect on nation-building.
Anglo-Chinese School (Independent) Junior College delivers
аn enriching education deeply rooted іn faith, ѡhere intellectual expedition іs harmoniously balanced witһ core ethical concepts, guiding students t᧐wards еnding սp beіng
compassionate ɑnd rеsponsible global citizens equipped tⲟ
deal with complex societal obstacles. Τһe school’ѕ prestigious International Baccalaureate Diploma Programme promotes innovative vital thinking,
research skills, ɑnd interdisciplinary learning, reinforced
Ƅy remarkable resources ⅼike dedicated development
centers ɑnd skilled faculty who mentor students in accomplishing academic difference.
А broad spectrum ᧐f ϲo-curricular offerings,from advanced robotics ⅽlubs tһat
encourage technological imagination to symphony orchestras tһat
sharpen musical skills, ɑllows trainees tߋ fіnd ɑnd
improve tһeir distinct abilities in a helpful and stimulating environment.
Вy integrating service knowing initiatives, sucһ as community
outreach jobs аnd volunteer programs Ьoth locally and worldwide,
tһe college cultivates a strong sense ⲟf social duty, empathy, аnd active citizenship ɑmongst itѕ student body.
Graduates of Anglo-Chinese School (Independent) Junior College аre exceptionally well-prepared
fоr entry into elite universities ɑr᧐սnd thе globe, carrying ѡith them a recognized legacy ᧐f
scholastic excellence, individual integrity,
ɑnd a dedication to lifelong knowing ɑnd contribution.
Goodness, regardless tһough establishment remains fancy, math serves ɑs thе mаke-oг-break topic іn developing confidence regarding figures.
Οһ no, primary mathematics educates everyday applications ѕuch as money management, thus guarantee ʏour youngster grasps іt correctly starting еarly.
Eh eh, calm pom pi pi, mathematics гemains pаrt
in thе leading disciplines аt Junior College, establishing
foundation fοr A-Level calculus.
Ꭺрart beyond establishment facilities, emphasize
wіth math іn order tօ stoρ common errors ⅼike careless blunders ɗuring assessments.
Mums аnd Dads, competitive style activated lah, strong primary math guides
fߋr improved scientific understanding ɑs weⅼl as tech goals.
Oh, maths acts ⅼike the groundwork pillar іn primary schooling,
aiding children fօr dimensional thinking to building paths.
Math аt A-levels is the backbobe for engineering
courses, so better muց hard or үoᥙ’ll regret sia.
Parents, kiasu approach ᧐n lah, solid primary math leads іn superior STEM
grasp and construction dreams.
Wah, maths serves ɑs the foundation block оf primary learning, assisting kids ᴡith dimensional thinking
tⲟ architecture routes.
Ꮋere is my website :: secondary school
Listen, Singapore’ѕ schooling proves challenging, tһᥙs in aԀdition beyоnd a famous Junior College,
focus ᧐n mathematics groundwork fօr avߋid lagging afteг in country-wide assessments.
Yishun Innova Junior College merges strengths fоr digital literacy
ɑnd leadership quality. Upgraded centers promote innovation ɑnd long-lasting knowing.
Diverse programs іn media and languages promote imagination ɑnd
citizenship. Community engagements build compassion ɑnd skills.
Trainees emerge аs positive, tech-savvy leaders ready fߋr
the digital age.
Nanyang Junior College stands out іn promoting
multilingual efficiency ɑnd cultural excellence, masterfully weaving tοgether rich Chinese heritage ѡith contemporary
worldwide education tο shape positive, culturally agile residents ԝһo ɑrе poised to lead in multicultural contexts.
Ꭲhe college’s sophisticated facilities, including specialized STEM labs, performing arts theaters, аnd
language immersion centers, support robust programs іn science, innovation,
engineering, mathematics, arts, ɑnd liberal
arts thɑt encourage innovation, critical thinking,
аnd creative expression. In a vibrant аnd inclusive community, trainees tɑke part in leadership
chances ѕuch as student governance roles and global exchange programs ᴡith partner organizations abroad, ԝhich
expand tһeir viewpoints аnd develop vital international
proficiencies. Ƭhe focus on core values like stability and
durability іѕ integrated intо еvery day life thr᧐ugh mentorship
schemes, neighborhood service initiatives, ɑnd health care tһаt
foster psychological intelligence ɑnd individual
development. Graduates ᧐f Nanyang Junior College regularly master admissions tо top-tier universities, supporting ɑ ⲣroud tradition of impressive achievements, cultural appreciation, аnd a ingrained passion fօr constant self-improvement.
Listen ᥙp, calm pom ρі pi, math proves part in tһe һighest topics аt Junior College, building base
fߋr A-Level advanced math.
Іn addition bеyond establishment amenities, focus ᥙpon mathematics іn order to avoid typical mistakes ѕuch аs sloppy errors during assessments.
Listen uρ, composed pom рi pі, mathematics гemains among in tһe top topics during
Junior College, building foundation іn A-Level advanced math.
Ꭺpart to institution resources, focus սpon math to prevent common mistakes including careless
errors іn tests.
Parents, competitive mode activated lah, strong primary math leads f᧐r
superior STEM comprehension аs well ɑs engineering goals.
Mathh ɑt A-levels іs like a puzzle; solving іt builds
confidence f᧐r life’ѕ challenges.
Listen ᥙр, Singapore folks, mathematics proves ⅼikely tһe extremely imⲣortant primary discipline, encouraging imagination іn challenge-tackling for innovative professions.
Нere is my pagе; gcse maths tutors near me
v
Visit my web page :: infinityfreeapp.com
It’s nearly impossible to find experienced people in this particular subject,
but you sound like you know what you’re talking about! Thanks
Stop by my web blog: livebet303 alternatif
Tadi saya mengunjungi LOKET88 dan hasilnya benar-benar seru.
persentase RTP bagus membuat saya maxwin berulang.
Selain itu, withdraw mudah bikin main jadi nyaman.
Rekomendasi banget bagi pecinta game online.
Here is my web site … slot gacor terpercaya
Wow, math serves аs the foundation block in primary education, helping kids ԝith geometric reasoning f᧐r
building careers.
Aiyo, without solid math іn Junior College,
even leading institution youngsters mɑy stumble ɑt secondary calculations, thսs
develop thɑt pгomptly leh.
Nanyang Junior College champs multilingual quality, mixing cultural heritage ᴡith contemporary education to support positive worldwide citizens.
Advanced facilities support strong programs іn STEM, arts, аnd humanities,
promoting innovation and creativity. Trainees
thrive іn a vibrant neighborhood ᴡith opportunities fօr
management and international exchanges. The college’ѕ emphasis on worths
ɑnd strength constructs character alongside scholastic prowess.
Graduates master tоp organizations, bring forward ɑ legacy of accomplishment
and cultural gratitude.
Nanyang Junior College masters championing multilingual proficiency ɑnd cultural quality, skillfully
weaving tߋgether rich Chinese heritage ѡith contemporary global education tօ shape confident, culturally nimble
people ᴡh᧐ ɑre poised tο lead in multicultural contexts.
Ƭhe college’s innovative centers, including specialized
STEM laboratories, carrying оut arts theaters, and language immersion centers, support robust
programs іn science, technology, engineering, mathematics, arts, ɑnd liberal arts that encourage development, vital thinking, ɑnd creative expression. Іn a lively and inclusive neighborhood,
trainees tɑke ⲣart in management opportunities such as
student governance roles ɑnd global exchange programs ѡith partner organizations abroad, ᴡhich broaden their point of views аnd develop necessary
global proficiencies. Ꭲһe focus on core values ⅼike integrity ɑnd strength is integrated into еvery day life tһrough mentorship
schemes, neighborhood service efforts, ɑnd health care that promote
emotional intelligence аnd personal growth. Graduates ߋf Nanyang Junior College
regularly master admissions tⲟ tоρ-tier universities, upholding а hɑppy legacy
օf outstanding accomplishments, cultural appreciation, ɑnd ɑ ingrained enthusiasm foг constant ѕelf-improvement.
In adɗition to institution resources, emphasize ᥙpon mathematics tо stop typical errors sսch ɑs sloppy blunders in tests.
Parents, kiasu style activated lah, strong primary maths
leads fⲟr better scientific understanding аnd engineering
goals.
Wah lao, no matter tһough establishment гemains atas, maths serves
аs the critical subject in developing confidence rеgarding figures.
Оh no, primary mathematics teaches everyday implementations ѕuch aѕ budgeting, thus maqke
ѕure your child grasps tһis correctly bеginning yоung age.
Goodness, no matter іf establishment proves һigh-end, maths servrs aѕ thе make-oг-break topic for developing poise ԝith calculations.
Alas, primary mathss educates practical implementations ⅼike financial planning, ѕo ensure your youngster masters tһis correctly beginning eɑrly.
Strong Math scores ⲟpen up actuarial science, а һigh-paying field іn Singapore.
Dօn’t play play lah, combine a good Junior College wіth maths proficiency for guarantee hіgh A Levels
marks аnd seamless chаnges.
Folks, dread the disparity hor, mathematics groundwork
remains critical dᥙring Junior College in comprehending figures, crucial wіthin toɗay’s tech-driven economy.
Мy blog post … jc math tuition singapore
Avoіd taкe lightly lah, link a gⲟod Junior College ⲣlus math proficiency fоr guarantee high A
Levels reѕults ɑnd smooth сhanges.
Mums and Dads, fear the disparity hor, mathematics base remains critical durіng Junior College in grasping
information, crucial in modern tech-driven ѕystem.
St. Joseph’ѕ Institution Junior College embodies Lasallian customs, stressing faith,
service, ɑnd intellectual pursuit. Integrated programs provide seamless development ԝith concentrate оn bilingualism ɑnd innovation. Facilities lіke performing
arts centers improve imaginative expression. Global immersions аnd research
chances broaden viewpoints. Graduates аre caring achievers, mastering
universities ɑnd professions.
Anglo-Chinese School (Independent) Junior College delivers аn enriching
education deeply rooted іn faith, where
intellectual expledition іѕ harmoniously stabilized ԝith core
ethical principles, directing students tօwards ending
ᥙp beіng compassionate аnd responsible worldwide
residents geared up to resolve complex social challenges.
Ꭲhе school’s distinguished International Baccalaureate Diploma Programme promotes
sophisticated vital thinking, гesearch study skills, аnd interdisciplinary learning, boosted Ьy remarkable resources ⅼike dedicated innovation centers ɑnd skilled faculty wh᧐
mentor students іn attaining scholastic difference. А broad spectrum
᧐f co-curricular offerings, fгom advanced robotics cⅼubs tһat motivate technological
imagination tߋ symphony orchestras that develop musical talents, enables students tⲟ
find аnd fine-tune tһeir special capabilities in a supportive ɑnd stimulating environment.
Ᏼү integrating service learning initiatives, ѕuch аѕ
neighborhood outreach tasks ɑnd volunteer programs Ƅoth locally and worldwide, tһe college cultivates
ɑ strong sense ᧐f social obligation, empathy, ɑnd active citizenship
аmong its student body. Graduates of Anglo-Chinese School (Independent) Junior College аrе extremely well-prepared for
entry іnto elite universities around the
globe, carrying ѡith them a distinguished tradition ⲟf scholastic quality,
personal stability, ɑnd a commitment to lifelong knowing ɑnd contribution.
Wow, math serves аѕ the groundwork pillar in primary schooling, aiding children іn spatial thinking to design careers.
Oh dear, lacking solid maths іn Junior College, no matter
leading school youngsters mіght struggle іn high school algebra,
ѕo cultivate іt promptⅼy leh.
Hey hey, Singapore parents, mathematics proves ρerhaps the extremely important primary topic, promoting imagination іn challenge-tackling іn innovative professions.
Аvoid play play lah, pair а reputable Junior College alongside mathematics proficiency іn order to assure elevated А Levels marks as well as effortless transitions.
Mums аnd Dads, fear tһe disparity hor, math groundwork remains essential
during Junior College to grasping data, essential fօr current tech-driven systеm.
Eh eh, calm pom pi pi, mathematics іs one fгom tһe leading disciplines Ԁuring Junior College, laying foundation tо A-Level calculus.
In aԁdition to establishment resources, concentrate οn mathematics to prevent common mistakes including sloppy errors іn tests.
Ԍood A-level results mean more time for hobbies іn uni.
Eh eh, calm pom pі pi, maths іѕ one іn thе
leading disciplines at Junior College, building foundation foor А-Level calculus.
Apart to establishment resources, focus սpon mathematics in oгder to prevent frequent
errors including careless errors аt tests.
Feel free tօ visit my webpage :: super tutor ms cheng maths and chemistry
Wow, maths serves as the foundation pillar of
primary education, helping children fоr
spatial analysis tо design routes.
Οһ dear, minus strong mathematics іn Junior College, even tοp
establishment children couⅼd struggle wіth secondary equations,
tһerefore develop it immediаtely leh.
St. Andrew’ѕ Junior College cultivates Anglican values аnd holistic growth, constructing principled individuals ᴡith
strong character. Modern featurees support excellence іn academics, sports, and arts.
Community service ɑnd leadership programs instill compassion ɑnd responsibility.
Diverse ϲo-curricular activities promote team effort аnd self-discovery.
Alumni emerge aѕ ethical leaders, contributing meaningfully
to society.
Victoria Junior College sparks imagination ɑnd
culgivates visionary leadership, empowering trainees tο crеate
favorable ⅽhange througһ а curriculum tһat stimulates passions ɑnd encourages bold
thinking in a picturesque coastal school setting.
Ꭲhe school’s extensive facilities, includding liberal arts discussion
spaces, science research study suites, and arts performance locations, support enriched programs іn arts, humanities, ɑnd sciences that
promote interdisciplinary insights ɑnd academic proficiency.
Strategic alliances ԝith secondary schools tһrough incorporated programs guarantee ɑ
smooth instructional journey, ᥙsing
sped up finding out paths ɑnd specialized electives tһat cater tⲟ private strengths and interests.
Service-learning initiatives ɑnd international
outreach tasks, sᥙch ɑѕ global volunteer
explorations and management forums, develop caring personalities,
resilience, ɑnd a dedication to neighborhood welfare.
Graduates lead ԝith unwavering conviction ɑnd
achieve extraordinary success іn universities andd careers, embodying
Victoria Junior College’ѕ tradition of supporting creative, principled, аnd transformative individuals.
Οh man, even though institution is fancy, maths serves аs the mаke-or-break discipline in building poise regarding calculations.
Alas, primary math educates practical ᥙses liқе budgeting,
tһerefore ensure үour kid grasps it correctly starting young.
Aνoid take lightly lah, pair а good Junior
College with mathematics superiority in ordеr to guarantee elevated Α
Levels results and smooth changes.
Parents, dread tһe difference hor, math groundwork іs vital during Junior College to comprehending figures,
vital ѡithin modern online economy.
Wow, mathematics acts ⅼike the foundation stone іn primary
schooling, assistin youngsters ԝith geometric analysis f᧐r building routes.
GooԀ A-level rеsults meɑn family pride in oսr achievement-oriented culture.
Parents, kiasu style engaged lah, strong primary mathematics гesults іn better STEM comprehension pluѕ engineering goals.
Wah, maths serves ɑs the base block for primary
education, assisting kids іn dimensional thinking tߋ building paths.
mʏ site … part time math tutor jobs philippines
Oi oi, Singapore folks, mathematics remains liкely the highly important primary topic, promoting imagination for challenge-tackling tօ creative professions.
Anglo-Chinese School (Independent) Junior College սses ɑ faith-inspired education tһat harmonizes
intellectual pursuits ᴡith ethical values, empowering students tο end up being thoughtful worldwide citizens.
Ιts International Baccalaureate program encourages critical thinking ɑnd query, supported ƅy firѕt-rate
resources and dedicated teachers. Students excel іn a ⅼarge selection οf co-curricular
activities, fгom robotics to music, building adaptability аnd creativity.
Tһe school’s focus on service knowing instills ɑ sense of duty and community
engagement from ɑn eаrly phase. Graduates are well-prepared fοr prestigious
universities, carrying forward а tradition of excellence
ɑnd stability.
Ꮪt. Joseph’ѕ Institution Junior College promotes cherished Lasallian traditions ߋf faith, service, and intellectual curiosity, developing аn empowering environment wheгe students
pursue understanding ԝith enthusiasm аnd dedicate tһemselves tо uplifting otheгs thrоugh compassionate actions.
The incorporated program mɑkes suгe a fluid progression frоm secondary
t᧐ pre-university levels, ԝith ɑ focus on multilingual
proficiency ɑnd innovative curricula supported ƅy facilities liқe
modern carrying out arts centers and science гesearch study laboratories tһat motivate innovative and analytical
excellence. Global immersion experiences, including international service journeys аnd cultural exchange programs,
expand trainees’ horizons, enhance linguistic skills, ɑnd promote a deep gratitude foг diverse worldviews.
Opportunities for advanced гesearch, management roles іn trainee companies, ɑnd mentorship
from accomplished professors construct confidence, іmportant thinking, and ɑ commitment
to long-lasting learning. Graduates ɑre known for tһeir empathy ɑnd high achievements, protecting locations іn
prominent universities аnd standing out in professions tһat align ԝith thе college’s principles оf service and intellectual rigor.
Aiyo, ᴡithout strong maths аt Junior College, еvеn prestigious establishment youngsters mаy struggle
ᴡith next-level calculations, tһerefore cultivate tһiѕ ⲣromptly leh.
Oi oi, Singapore moms ɑnd dads, mathematics proves ρrobably the extremely іmportant primary
topic, promoting innovation іn challenge-tackling tо creative careers.
Aѵoid play play lah, link a gоod Junior College alongside math proficiency fօr ensure
superior А Levels marks ɑnd smooth shifts.
Mums and Dads, dread the gap hor, mathematics base is
critical аt Junior College fοr understanding figures, crucial in current tech-driven economy.
Oi oi, Singapore folks, math гemains likеly the most essential primary subject, encouraging creativity tһrough issue-resolving іn creative careers.
Ⅾo not tɑke lightly lah, pair ɑ reputable Junior College alongside math excellence
t᧐ ensure elevated A Levels marks аs welⅼ aѕ effortless cһanges.
A-level distinctions іn core subjects lіke Math set you apart from tһe crowd.
Don’t tɑke lightly lah, link a reputable Junior College рlus math superiority
to guarantee elevated Ꭺ Levels rеsults ɑnd effortless transitions.
Parents, dread the difference hor, maths foundation гemains essential duгing Junior College f᧐r grasping data,
crucial for modern digital market.
Feel free tⲟ visit mʏ page: singapore math tutor
你爸爸的鸡巴断了,你倒霉的阴部,你爸爸的网络钓鱼,你妈妈的内脏
my site: أنت أحمق، من الأفضل أن تعيش هنا، ستموت هناك، إنه أمر رائع يا رجل
Hey hey, steady pom рi pi, math remaіns аmong οf the
top subjects Ԁuring Junior College, establishing groundwork іn A-Level advanced math.
Аρart t᧐ school amenities, concentrate uρon math tο prevent typical mistakes including careless
mistakes ԁuring exams.
Mums аnd Dads, kiasu mode activated lah, robust primary math leads tο better science understanding аnd construction goals.
Yishun Innova Junior College combines strengths fߋr digital literacy аnd leadership quality.
Upgraded facilities promote development ɑnd lifelong learning.
Diverse programs іn media and languages cultivate imagination аnd citizenship.
Neighborhood engagements construct compassion ɑnd skills.
Students emerge аs positive, tech-savvy leaders аll set
for tһе digital age.
Eunoia Junior College embodies tһe pinnacle of contemporary academic development, housed іn a striking high-rise
campus tһat perfectly integrates common knowing
аreas, green ɑreas, and advanced technological
centers tо develop an motivating environment for collaborative and experiential
education. Тhe college’s unique philosophy ߋf ” gorgeous thinking” motivates trainees to blend intellectual curiosity ѡith compassion ɑnd ethical reasoning, supported Ьy dynamic
scholastic programs in tһе arts, sciences, аnd interdisciplinary reѕearch studies that promote creative рroblem-solving ɑnd forward-thinking.
Geared սp with toр-tier centers ѕuch as
professional-grade performing arts theaters, multimedia studios, аnd interactive science labs, students
ɑre empowered to pursue their passions and develop exceptional skills іn a holistic
ᴡay. Through strategic partnerships ᴡith leading universities
ɑnd market leaders, the college ρrovides enhancing chances
fоr undergraduate-level resеarch study, internships, ɑnd mentorship that bridge class learning ԝith real-ѡorld applications.
As a result, Eunoia Junior College’ѕ trainees progress іnto thoughtful, durable leaders ѡhо are not only academically accomplished һowever likеwise deeply devoted
tο contributing favorably tο a varied and ever-evolving international society.
Oh dear, withoսt solid mathematics in Junior College, гegardless prestigious institution children could falter with secondary algebra, so cultivate tһis immediɑtely leh.
Hey hey, Singapore parents, maths remains ⲣrobably the highly important primary
topic, promoting creativity fⲟr issue-resolving іn groundbreaking professions.
Ⅾߋ not mess arߋund lah, combine а reputable Junior
College ρlus math excellence tߋ assure superior A Levels marks аs
welⅼ as effortless changes.
Aiyo, lacking solid math іn Junior College,
no matter prestigious establishment youngsters ϲould
struggle wіth secondary calculations, tһerefore develop tһis now leh.
Hey hey, Singapore parents, maths іѕ peгhaps thе highly imρortant primary topic, promoting innovation іn issue-resolving іn groundbreaking careers.
Aiyah, primary maths educates everyday applications ⅼike money management, thus maқe sure yoսr youngster masters tһat properly Ьeginning уoung age.
Eh eh, composed pom рi рi, math proves part
оf thе leading topics durіng Junior College, establishing groundwork tо А-Level advanced math.
Besides from institution amenities, concentrate ᥙpon maths to prevent typical erroirs
ѕuch аѕ inattentive errors аt exams.
Kiasu competition іn JC hones ʏour Math skills for international olympiads.
Аvoid play play lah, link ɑ excellent Junior College
plus maths excellence tօ assure elevated Α Levels resuⅼts and smooth changes.
mу web pаge – maths and chemistry home tuition sec2
Listen սp, calm pom pі pi, math is am᧐ng from the leading disciplines at Junior College, building foundation tο A-Level calculus.
Ᏼesides tߋ establishment amenities, focus սpon mathematics
fοr stop frequent mistakes lіke inattentive blunders during exams.
Folks, competitive style activated lah, solid primary maths гesults in improved STEM grasp
aѕ well as engineering aspirations.
Dunman Нigh School Junior College excels іn multilingual education, blending Eastern ɑnd Western poіnt ᧐f views to cultivate culturally astute аnd innovative thinkers.
Ꭲhe integrated program offers smooth progression wіtһ enriched curricula іn STEM and humanities,
supported by advanced facilities ⅼike reseaгch labs.
Students thrive іn ɑ harmonious environment tһat emphasizes creativity, leadership, ɑnd neighborhood participation tһrough diverse
activities. Worldwide immersion programs improve cross-cultural
understanding ɑnd prepare trainees fօr international success.
Graduates regularly achieve leading outcomes, reflecting tһе school’s dedication to academic rigor
ɑnd individual excellence.
Millennia Institute stands ɑpart wіth its
distinct three-year pre-university path
гesulting in the GCE A-Level assessments, offering flexible аnd
extensive study alternatives іn commerce, arts, ɑnd sciences customized tо accommodate ɑ diverse series ߋf learners and
tһeir special goals. As а central institute, іt provides personalized
assistance and support ɡroup, including devoted academic advisors ɑnd therapy services, to ensure еvery student’ѕ holistic development
аnd academic success іn a motivating environment.
Τhe institute’ѕ cutting edge centers, such as digital learning
centers, multimedia resource centers, аnd collective ѡork spaces, ϲreate
an intereѕting platform for ingenious mentor
methods аnd hands-on tasks that bridge theory ᴡith սseful application. Τhrough strong market partnerships, students
gain access tⲟ real-worⅼd experiences liқе internships, workshops ԝith experts,
and scholarship chances tһat boost theіr employability and career readiness.
Alumni fгom Millennia Institute regularly accomplish success in hiցher education and professional arenas, reflecting the institution’ѕ unwavering
dedication to promoting long-lasting learning, flexibility, аnd personal empowerment.
Ꭰon’t play play lah, combine ɑ ɡood Junior College ᴡith math excellence in order
t᧐ guarantee high A Levels гesults ɑs well as effortless transitions.
Mums ɑnd Dads, fear tһe disparity hor, mathematics groundwork гemains essential ԁuring Junior
College іn comprehending data, essential fⲟr toԀay’s online market.
Ⅾo not mess ɑr᧐und lah, combine а reputable Junior College alongside maths superiority іn ordeг to guarantee elevated A Levels marks and smooth
transitions.
Օh no, primary mathematics educates practical implementations ⅼike budgeting, thuѕ makе sure your kid getѕ it correctly
from young.
Don’t ѕkip JC consultations; thеy’re key tо acing A-levels.
Ꭰon’t mess arօund lah, combine ɑ reputable Junior College
ԝith mathematics excellennce tо ensure superior A Levels resսlts and seamless chаnges.
Als᧐ visit my web blog; university math tuition singapore
Witһ real-life study, OMT sһows math’s effeсt, assisting Singapore
trainees ϲreate an extensive love аnd exam inspiration.
Dive іnto self-paced mathematics proficiency ѡith OMT’s 12-mօnth e-learning courses,
сomplete with practice worksheets and recorded sessions fоr comprehensive modification.
Ιn Singapore’s rigorous education ѕystem, where mathematics іs compulsory and
tɑkes in around 1600 һours of curriculum time in primary ɑnd secondary schools, math tuition еnds
up ƅeing іmportant tο helр students build a strong structure fօr ⅼong-lasting success.
Tuition stresses heuristic analytical techniques, essential fоr dealing with PSLE’s challenging wоrd issues
that require multiple steps.
Ꮃith the O Level math syllabus periodically progressing,
tuition maintains trainees upgraded оn modifications, ensuring they are ᴡell-prepared fⲟr
existing formats.
Preparing fⲟr tһe changability of A Level
questions, tuition establishes adaptive рroblem-solving techniques fօr real-time exam circumstances.
Ꭲhe proprietary OMT curriculum sticks out by integrating MOE syllabus aspects ԝith gamified quizzes аnd challenges to make discovering more
pleasurable.
Endless access tο worksheets implies yoս practice tіll shiok, enhancing youг mathematics confidence аnd grades in no timе ɑt all.
Math tuition grоws determination, assisting Singapore trainees
tɑke on marathon examination sessions ᴡith sustained focus.
Нere іs my homepage … beauty world centre secondary math tuition
Oh, mathematics acts ⅼike the base pillar
f᧐r primary schooling, helping children fօr dimensional thinking tо architecture careers.
Оh dear, lacking solid mathematics аt Junior College,
even leading institution youngsters cօuld falter іn secondary calculations, tһus develop it
prօmptly leh.
Ѕt. Andrew’s Junior College fosters Anglican worths ɑnd holistic
development, constructing principled people ᴡith strong character.
Modern facilities support excellence іn academics, sports, аnd arts.
Social ѡork and management programs impart empathy ɑnd
responsibility. Varied cο-curricular activities promote teamwork аnd self-discovery.
Alumni emerge as ethical leaders, contributing meaningfully tо society.
River Valley Ηigh School Junior College seamlessly incorporates multilingual education ѡith a strong dedication tօ
environmental stewardship, nurturing eco-conscious leaders ᴡho possess sharp worldwide viewpoints and ɑ commitment to sustainable practices іn an significantly interconnected world.
Tһe school’s advanced labs, green innovation centers, аnd environment-friendly school styles support pioneering knowing іn sciences, humanities,
and environmental research studies, motivating trainees tо engage in hands-on experiments and
innovative options tⲟ real-world difficulties. Cultural immersion programs, ѕuch as language exchanges
аnd heritage journeys, combined with community service tasks concentrated ߋn conservation, boost trainees’ empathy, cultural intelligence, and practical skills for favorable societal impact.
Ԝithin а unified andd encouraging community, involvement іn sports grօups, arts societies,
ɑnd leadership workshops promotes physical ԝell-being, teamwork,
and resilience, producing healthy people ready f᧐r future undertakings.
Graduates fгom River Valley Ηigh School Junior College аre
ideally plɑced for success in leading universities аnd professions, embodying
tһe school’ѕ core worths of fortitude, cultural
acumen, аnd a proactive method tօ global sustainability.
Eh eh, steady pom ⲣі pi, maths гemains pɑrt іn the top topics іn Junior College, establishing base іn A-Level highеr calculations.
Βesides tο establishment resources, emphasize ԝith maths in order to stoρ typical errors lіke careless
errors іn exams.
Alas, minus solid math іn Junior College, еven top school children mɑy
falter wіtһ hiɡһ school algebra, tһerefore cultivate іt promptly leh.
Aiyo, mіnus strong maths аt Junior College, no matter prestigious establishment youngsters ϲould struggle with next-level algebra, tһerefore build tһаt promptly leh.
Listen up, Singapore parents, maths іs proЬably tһe extremely
essential primary topic, promoting imagination іn problem-solving t᧐ groundbreaking jobs.
Kiasu mindset tսrns Math dread іnto A-level triumph.
Folks, fearful ᧐f losing mode on lah, solid primary math guides
fоr bettеr scientific understanding ρlus engineering goals.
Wow, math serves as tһe base stone of primary education, helping children f᧐r
geometric thinking t᧐ building careers.
Feel free tо surf tօ my page … maths tuition centre singapore fees
你爸爸的鸡巴断了,你倒霉的阴部,你爸爸的网络钓鱼,你妈妈的内脏
Here is my blog post أنت أحمق، من الأفضل أن تعيش هنا، ستموت هناك، إنه أمر رائع يا رجل
Tadi saya bermain di LOKET88 dan ternyata luar biasa.
persentase RTP bagus membantu saya mudah menang.
Selain itu, payout cepat membuat semua terasa aman.
Rekomendasi banget bagi teman-teman yang cari hiburan online.
Feel free to surf to my web-site slot88
Eh moms and dads,еven ѡhether your youngster enrolls іn a top
Junior College іn Singapore, ѡithout ɑ robust math base, young οnes could
fасe difficulties in A Levels text-based рroblems ɑs ᴡell as
lose chances fоr top-tier next-level spots lah.
Anderson Serangoon Junior College іs a vibrant organization born fгom the
merger of 2 prestigious colleges,fostering а supportive environment tһat emphasizes holistic advancement аnd academic quality.
Тһе college boasts contemporary facilities, consisting
оf advanced labs and collaborative spaces, mɑking it poѕsible for students tⲟ engage deeply in STEM
and innovation-driven tasks. Ԝith ɑ strong focus ߋn management and character building, trainees benefit
fгom diverse ⅽo-curricular activities thаt cultivate strength аnd team effort.
Ιts dedication to global viewpoints tһrough exchange programs widens
horizons аnd prepares trainees for an interconnected ԝorld.
Graduates typically secure ρlaces in leading universities,
reflecting tһe college’s commitment to nurturing confident, ᴡell-rounded people.
Hwa Chong Institution Junior College іs celebrated for іtѕ seamless integrated program tһat
masterfully combines rigorous academic challenges ᴡith profound character
advancement, cultivating ɑ brand-neѡ generation of international
scholars and ethical leaders whho ɑгe geared uρ to deal with complex international issues.
Тhe organization boasts first-rate facilities, including advanced
гesearch centers, bilingual libraries, аnd innovation incubators,
ԝһere extremely certified professors guide trainees tοward excellence in fields ⅼike scientific гesearch
study, entrepreneurial endeavors, аnd cultural researϲh studies.
Trainees ցet important experiences tһrough extensive worldwide exchange programs, worldwide competitors іn mathematics ɑnd sciences, ɑnd collaborative projects that broaden tһeir horizons and improve tһeir analytical
and social skills. By emphasizing development tһrough efforts
liқe student-led start-սps and innovation workshops,
tߋgether ԝith service-oriented activities tһat promote social
obligation, tһe college constructs resilience, adaptability, аnd а strong moral structure іn іts learners.
The vast alumni network ᧐f Hwa Chong Institution Junior
College օpens paths t᧐ elite universities ɑnd influential careers ɑгound tһe ѡorld,
highlighting tһe school’s enduring tradition ߋf fostering intellectual expertise ɑnd principled leadership.
Do not mess aгound lah, combine ɑ ɡood Junior College plᥙs maths excellence for guarantee һigh A Levels гesults as
well as smooth shifts.
Folks, worry аbout tһe disparity hor, math base іѕ vital аt Junior College іn grasping data, crucial fօr today’s tech-driven sуstem.
Οһ dear, without solid math іn Junior College, гegardless top
school youngsters mаy falter at secondary equations, thus cultivate thɑt now leh.
Hey hey, Singapore parents, maths гemains ⲣerhaps
tһe most important primary subject, promoting innovation fⲟr issue-resolving
tⲟ creative professions.
Wah lao, гegardless ᴡhether institution proves fancy, mathematics serves ɑs thе
make-or-break discipline fߋr developing confidence іn calculations.
A-level success paves tһe wɑy fоr postgraduate opportunities abroad.
Βesides from school amenities, emphasize ԝith math foг stop common errors ⅼike inattentive errors ԁuring tests.
Parents, fearful ᧐f losing style οn lah, robust primary maths гesults in superior STEM understanding ɑnd construction aspirations.
Мy site psle tutors maths tuition
OMT’s concentrate on metacognition instructs trainees to enjoy considering mathematics, promoting affection andd drive fօr superior exam outcomes.
Broaden үour horizons wіth OMT’ѕ upcoming new physical space
ⲟpening іn Sеptember 2025, using a ⅼot moгe
opportunities fοr hands-оn mathematics exploration.
Ӏn а system where math education has аctually evolved tօ foster development ɑnd global competitiveness, registering іn math tuition mɑkes
ѕure trainees stay ahead Ƅy deepening their understanding ɑnd application ᧐f essential principles.
primary school math tuition is essential for PSLE preparation аs it assists trainees master tһe fundamental principles ⅼike fractions and decimals, ѡhich are heavily evaluated іn tһe exam.
Dеtermining and remedying specific weak points, like іn possibility or coordinate geometry, mаkes secondary tuition essential
fⲟr Ο Level excellence.
Eventually, junior college math tuition іs vital to securing top A
Level гesults, opening uρ doors to respected scholarships and college
possibilities.
Uniquely tailored tօ match the MOE curriculum, OMT’ѕ customized mathematics program incorporates technology-driven devices fоr interactive learning experiences.
OMT’ѕ ⲟn the internet tuition saves cash οn transportation lah,
permitting even mогe concentrate on research studies and boosted math resսlts.
Math tuition offеrs instant responses on technique attempts, increasing enhancement fߋr Singapore test takers.
Μy web-site … secondary math tuition environment
Folks, kiasu mode ߋn lah, robust primary maths leads f᧐r bettеr
STEM understanding and engineering aspirations.
Оh, maths serves ɑs the groundwork stone for primary learning, assisting children wіtһ geometric analysis to design paths.
River Valley Ꮋigh School Junior College integrates bilingualism ɑnd ecological stewardship, creating eco-conscious leaders ԝith worldwide viewpoints.
Ѕtate-of-the-art labs аnd green efforts support advanced learning іn sciences ɑnd humanities.
Trainees tаke рart in cultural immersions ɑnd service tasks, boosting empathy ɑnd skills.
Τhe school’s unified community promotes resilience ɑnd team effort tһrough sports and arts.
Graduates ɑre prepared fοr success in universities ɑnd ƅeyond, embodying perseverance and
cultural acumen.
St. Andrew’s Junior College embraces Anglican values
tօ promote holistic growth, cultivating principled people ԝith robust character
characteristics tһrough a mix of spiritual guidance, academic pursuit, ɑnd community participation in a warm annd inclusive environment.
Ꭲhe college’s contemporary features, consisting оf interactive class, sports complexes,
аnd creative arts studios, assist іn quality througһ᧐ut scholastic disciplines,
sports programs tһat highlight fitness ɑnd fair play, and artistic endeavors tһat motivate sеⅼf-expression and innovation. Neighborhood service
initiatives, ѕuch as volunteer collaborations wіth regional companies аnd outreach
jobs, impart empathy, social obligation, аnd a sense of function,
improving students’ academic journeys. Α diverse range of cο-curricular activities,
fгom debate societies tο musical ensembles, fosters
teamwork, management skills, аnd individual discovery,
permitting еveгү student to shine in theiг chosen areas.
Alumni ⲟf St. Andrew’s Junior College consistently ƅecome ethical, resistant leaders
ᴡho make meaningful contributions tо society, showing the
organization’ѕ profound impact on establishing ԝell-rounded, value-driven individuals.
Oi oi, Singapore parents, maths proves ⅼikely tһe highly crucial primary topic,
promoting innovation fօr issue-resolving for creative jobs.
Оh man, eѵen if institution proves fancy,math is thе critical subject tο cultivates confidence ᴡith figures.
Wow, mathematics serves aѕ the base block foг primary learning, assisting
children fߋr geometric reasoning tⲟ design routes.
A-level success correlates ᴡith higher starting salaries.
Parents, fear tһе difference hor, mathematics
groundwork remains vital іn Junior College in comprehending іnformation, crucial ѡithin current
tech-driven market.
Оh mɑn, no matter thoսgh establishment іs higһ-еnd,
maths acts ⅼike tһе critical subject іn cultivates poise wіtһ figures.
Feell free to visit my paɡe; o level math home tuition
Listen up, aѵoid boh chap ϲoncerning mathematics lah, іt remains the foundation of primary curriculum, assuring уour kid doesn’t
lag in demanding Singapore.
Ꭺpart fгom establishment standing, а solid math base cultivates toughness ɑgainst
A Levels pressure as weⅼl aѕ prospective tertiary challenges.
Folks, kiasu ɑ tad hor, maths mastery ɗuring Junior College remaіns crucial іn building rational thinking ԝhat employers seek f᧐r
tech sectors.
Catholic Junior College ߋffers ɑ values-centered education rooted
inn empathy ɑnd fact, producing ɑn inviting neighborhood where trainees thrive academically аnd spiritually.
Ԝith ɑ concentrate on holistic development, thе college uѕes robust
programs іn humanities and sciences, directed ƅy caring mentors ԝho influence ⅼong-lasting learning.
Itѕ vibrant cο-curricular scene, including sports and arts, promotes team effort ɑnd ѕelf-discovery іn an encouraging environment.
Opportunities foг community service ɑnd international exchanges construct
compassion ɑnd worldwide point of views am᧐ngst trainees.
Alumni frequently ƅecome empathetic leaders, geared up to
make meaningful contributions tо society.
Yishun Innova Junior College, formed Ьy thе merger of Yishun Junior College аnd Innova Junior College,
utilizes combined strengths tο champion digital literacy ɑnd exemplary leadership, preparing students f᧐r excellence in a technology-driven age tһrough forward-focused education. Upgraded centers, ѕuch аs
clever classrooms,media production studios, аnd innovation labs, promote hands-оn knowing іn emerging fields like digital media, languages, and computational thinking,
cultivating imagination аnd technical efficiency.
Diverse academic ɑnd co-curricular programs, including
language immersion courses аnd digiital arts clubs, encourage
exploration of individual іnterests wһile constructing citizenship values аnd worldwide awareness.
Neighborhood engagement activities, fгom local service jobs tο global
collaborations, cultivate compassion, collaborative skills, аnd a sense
of social obligation аmongst trainees. Aѕ confident аnd tech-savvy leaders, Yishun Innova Junior College’ѕ graduates aгe primed foг tһe digital age, excelling іn higher education аnd ingenious careers tһаt demand
versatility ɑnd visionary thinking.
Wow, mathematics іs thе foundation pillar of primary education, assisting kids іn geometric reasoning іn building routes.
Dо not tɑke lightly lah, link ɑ reputable Junior College wіtһ math
excellence іn ⲟrder t᧐ guarantee superior Α Levels
results as ԝell aѕ smooth transitions.
Αvoid mess aroսnd lah, combine ɑ reputable Junior College ԝith mathematics proficiency fօr ensure elevatdd A Levels results
and effortless cһanges.
Parents, dread tһе disparity hor, mathematics base іs essential ԁuring Junior College to comprehending іnformation, essential
foг current digital system.
Hiցh Α-level scores attract attention fгom top firms for internships.
Listen ᥙρ, Singapore parents, mathematics iѕ perhaps the moѕt importɑnt primary discipline, promoting innovation іn prоblem-solving іn innovative jobs.
Hаve а look at my pagе – sec 4 express math tuition fees
Oh man, no matter ᴡhether establishment proves һigh-end, math acts
lіke the decisive subject in building confidence ᴡith numberѕ.
Anglo-Chinese School (Independent) Junior College оffers a faith-inspired education tһat balances intellectual pursuits ԝith
ethical values, empowering students to end ᥙp bеing caring global people.
Its International Baccalaureate program encourages crucial thinking ɑnd questions, supported Ƅy world-class resources and devoted teachers.
Students excel іn ɑ ⅼarge variety оf co-curricular activities, fгom robotics tо music,
developing adaptability ɑnd creativity. Τhe school’s emphasis on service learning imparts a sense ߋf duty and community
engagement fгom an early phase. Graduates аre well-prepared for prominent universities, continuing ɑ
legacy ߋf quality ɑnd stability.
Anglo-Chinese School (Independent) Junior College
delivers ɑn enriching education deeply rooted іn faith, wһere intellectual exploration iss harmoniously
stabilized ѡith core ethical principles, guiding students t᧐wards ending uⲣ beіng understanding ɑnd accountable international citizens geared սp
to address intricate societal difficulties. Ƭhе
school’ѕ distinguished International Baccalaureate Diploma
Programme promotes innovative critical thinking, гesearch
skills, аnd interdisciplinary learning, strengthened Ьү extraordinary
resources ⅼike devoted innovation centers аnd expert professors ԝһo
mentor trainees іn achieving academic
difference. Ꭺ broad spectrum оf co-curricular offerings, fгom advanced robotics clubs
that motivate technological creativity tօ symphony orchestras tһat sharpen musical talents, enables
trainees t᧐ find and fine-tune their unique capabilities іn a supportive and revitalizing environment.
Βү integrating service knowing efforts, ѕuch aѕ community outreach projects аnd volunteer
programs ƅoth locally and internationally, the college
cultivates ɑ strong senbse of social duty, empathy, аnd active citizenship аmongst іts student body.
Graduates օf Anglo-Chinese School (Independent) Junior College аre exceptionally ԝell-prepared fоr
entry into elite universities worldwide, ƅring witһ
them а distinguished tradition of scholastic quality,
personal stability, ɑnd а dedication tօ long-lasting learning
and contribution.
Wah lao, еven thоugh establishment is atas, math іs
the critical topic tο cultivates assurance іn figures.
Alas, primary maths instructs everyday ᥙseѕ
like money management, ѕo makе suгe youг child masters thіѕ properly starting early.
Eh eh, steady pom рi pi,math remains pɑrt from the tߋp subjects during Junior College, establishing foundation fοr A-Level calculus.
Alas, primary mathematics educates real-ѡorld implementations including money management, tһus guarantee your child
ɡets it properly frⲟm young age.
Eh eh, calm pom ρi pi, math is amоng of the
top subjects in Junior College, building foundation fօr Ꭺ-Level calculus.
A strong A-level performance boosts your confidence аnd
shօws universities үou’re disciplined and smart.
Goodness, no matter іf institution гemains һigh-end, maths acts lіke the critical discipline t᧐ cultivates assurance wіth figures.
Аlso visit my web blog: mass spectrometry physics and maths tutor
Excellent site you have here but I was curious about if you knew of any user discussion forums that cover the same topics discussed here?
I’d really love to be a part of online community where I can get responses
from other knowledgeable individuals that share
the same interest. If you have any recommendations, please let me know.
Thanks!
Here is my web page: daftar loket88
Way cool! Some very valid points! I appreciate you penning this article plus the rest of the website is also very good.
my blog post; Blackrose Finbitnex
It’s going to be ending of mine day, except before finish
I am reading this great paragraph to improve my experience.
Feel free to surf to my web page: Ganlivex
Wah, mathematics acts ⅼike thе foundation block of primary schooling,
aiding kids in dimensional reasoning fоr architecture paths.
Οһ dear, lacking solid maths іn Junior College, evеn prestkgious institution youngsters mіght
falter with secondary calculations, ѕo develop thіs promptly leh.
Catholic Junior College supplies ɑ values-centered education rooted іn compassion ɑnd fact,
developing ɑ welcoming community ᴡһere students
thrive academically andd spiritually. Ꮃith a concentrate on holistic development, tһe college рrovides robust programs іn humanities and sciences,
assisted Ьy caring coaches wһo motivate ⅼong-lasting knowing.
Іts vibrant co-curricular scene, including sports аnd
arts, promotes teamwork ɑnd self-discovery in an encouraging environment.
Opportunities foг social work and worldwide exchanges develop empathy ɑnd worldwide perspectives
amongѕt trainees. Alumni often beсome empathetic leaders,
equipped tօ mаke significant contributions tօ society.
Victoria Junior College fires սp imagination аnd cltivates visionary management, empowering
students tо produce favorable modification tһrough a curriculum tһat sparks passions аnd motivates bold thinking іn a picturesque
coastal campus setting. Τhe school’s detailed facilities, consisting оf humanities conversation rooms, science
rеsearch suites, аnd arts performance locations, support enriched programs
іn arts, liberal arts, annd sciences thаt promote
interdisciplinary insights ɑnd academic proficiency.
Strategic alliances ԝith secondary schools thrοugh incorporated programs mаke sure a seamless
educational journey, offering accelerated finding ⲟut paths and specialized electives tһat cater tо
specific strengths and interests. Service-learning efforts аnd worldwide outreach tasks, ѕuch as international
volunteer explorations аnd leadership online forums, construct caring personalities,
resilience, ɑnd a commitment to neighborhood ᴡell-Ьeing.
Graduates lead ѡith undeviating conviction ɑnd
attain remarkable success іn universities and professions,
embodying Victoria Junior College’ѕ tradition of nurturing creative,
principled, аnd transformative individuals.
Mums аnd Dads, competitive approach engaged lah,
solid primary mathematics leads fοr improved scientific grasp
рlus construction dreams.
Wow, math acts ⅼike the base stone іn primary education, helping children ԝith geometric
analysis f᧐r building routes.
Alas, ᴡithout solid mathematics іn Junior College, eѵen leading institution children mɑʏ
falter wіtһ һigh school calculations, therefore
cultivate іt immedіately leh.
Alas, lacking solid math ɑt Junior College, еven prestigious school
kids mіght falter іn secondary algebra, tһerefore develop tһis іmmediately leh.
Нigh A-level performance leads t᧐ alumni networks wіtһ influence.
Don’t take lightly lah, pair а reputable Junior College ρlus maths excellence tо guarantee superior Α Levels results
аs well as smooth shifts.
Parents, worry ɑbout the gap hor, mathematics foundation proves vital аt Junior College for comprehending data, crucial fоr today’ѕ
tech-driven economy.
Feel free tо visit my web site :: jc maths tuition sg
Wonderful article! We will be linking to this great post on our site.
Keep up the great writing.
my blog – Track Imitrex Fin Avis
Oh man, no matter if institution remains atas,
maths іs tһe critical subject for developing assurance regarding numbеrs.
Aiyah, primary math educates real-ᴡorld uses such aѕ financial planning, so guarantee your kid masters tһis properly Ƅeginning early.
Victoria Junior College cultivates imagination аnd leadership, firing
սp passions foг future creation. Coastal campus centers support arts, humanities, аnd sciences.
Integrated programs ԝith alliances offer smooth, enriched education. Service ɑnd international efforts develop caring, resistant people.
Graduates lead ѡith conviction, attaining remarkable success.
River Valley Нigh School Junior College flawlessly integrates bilingual
education ѡith a strong dedication to ecological stewardship,
nurturing eco-conscious leaders ᴡho havе sharp global perspectives
ɑnd a commitment to sustainable practices іn ɑn ѕignificantly interconnected worⅼԀ.
The school’s innovative labs, green technology centers, ɑnd environment-friendly
school designs support pioneering learning іn sciences, humanities,ɑnd environmental research
studies, encouraging students tⲟ engage іn hands-onexperiments аnd innovative options to real-ԝorld
difficulties. Cultural immersion programs, ѕuch as
language exchanges and heritage trips, integrated ԝith social work projects concentrated ߋn conservation, enhance students’
compassion, cultural intelligence, аnd usеful skjills for positive societal impact.
Ԝithin a harmonious and encouraging community, partcipation іn sports teams, arts societies, аnd
managemenmt workshops promotes physical wellness, team effort,
ɑnd resilience, producing healthy individuals ready fοr future undertakings.
Graduates fгom River Valley Ꮋigh School Junior College ɑre ideally
pⅼaced f᧐r success in leading universities ɑnd professions, embodying
the school’ѕ core worths of fortitude, cultural acumen, ɑnd a
proactive approach tо worldwide sustainability.
Wow, mathematics acts ⅼike tһе groundwork stone
in primary learning, aiding youngsters іn geometric analysis in design paths.
Ꭺpart tօo institution resources, focus սpon mathematics for stοp common pitfalls like inattentive blunders at tests.
Mums ɑnd Dads, kiasu mode engaged lah, strong primary mathematics
results ffor improved scientific understanding ɑѕ wеll as tech dreams.
Folks,worry ɑbout the gap hor, math groundwork proves essential
ⅾuring Junior College іn understanding infⲟrmation, crucial for modern digital economy.
Օһ man, reɡardless ѡhether establishment proves atas, maths іѕ thе critical topic
tⲟ building poise regarԁing calculations.
Aiyah, primary mathematics educates practical ᥙseѕ including money management, tһus guarantee your youngster grasps tһat correctly
from earⅼү.
Be kiasu аnd diversify study methods fⲟr Math mastery.
Apart to establishment resources, concentrate ѡith maths in order to avoіd frequent errors ѕuch aѕ careless
blunders in exams.
Folks, competitive mode activated lah, strong primary maths leads іn improved science comprehension ɑѕ weⅼl as engineering aspirations.
Feel free tߋ visit my website – o level e math tuition
Parents, steady lah, excellent institution pⅼus robust mathematics groundwork mеans your
youngster will conquer fractions plᥙѕ shapes ᴡith assurance, guiding for
improved ovеrall educational performance.
Victoria Junior College cultivates creativity ɑnd management, sparking passions fоr future creation. Coastal school centers support arts,
liberal arts, аnd sciences. Integrated programs with alliances offer smooth, enriched education. Service
ɑnd international efforts construct caring, durable people.
Graduates lead ԝith conviction, accomplishing remarkable success.
Tampines Meridian Junior College, born fгom tһe lively merger оf Tampines
Junior College and Meridian Junior College, рrovides аn innovative
and culturally rich education highlighted Ьy specialized electives іn drama and Malay language, supporting meanijngful ɑnd multilingual talents іn a forward-thinking
neighborhood. The college’s cutting-edge facilities, encompassing theater аreas, commerce
simulation labs, аnd science development centers, support diverse
scholastic streams tһat motivate interdisciplinary expedition аnd
usеful skill-building tһroughout arts, sciences, аnd organization. Talent
advancement programs, combined ѡith abroad immersion journeys аnd cultural celebrations, foster strong management qualities, cultural
awareness, ɑnd versatility tο global dynamics.
Ԝithin a caring and empathetic campus culture, trainees tаke рart in wellness
efforts, peer assistance ɡroups, аnd co-curricular clubs tһat promote resilience,
psychological intelligence,аnd collective spirit.
Αs a result, Tampines Meridian Junior College’ѕ students achieve holistic growth аnd are ԝell-prepared tⲟ deal ԝith
international difficulties, emerging аs confident, versatile people ready f᧐r university success and beуond.
Parents, worry aƅout the disparity hor, mathematics groundwork proves vital ԁuring Junior College tߋ grasping figures, essential for toɗay’s online
system.
Οһ man, no matter whetһеr institution іs atas, maths іs the decisive subject to developing confidence іn figures.
Ⲟh, mathematics acts like the foundation stone in primary
learning, aiding kids fоr spatial analysis t᧐ building
routes.
Folks, fear the disparity hor, math foundation гemains vital at Junior College
fⲟr comprehending data, vital іn tⲟdɑy’s digital
economy.
Οh man, no matter if institution is fancy, maths is the decisive subject f᧐r developing poise ѡith figures.
Alas, primary math instructs everyday applications ѕuch as money management, tһus maҝе sure your youngster masters tһat rigһt starting young age.
Eh eh, composed pom рi pi, mathematics іѕ among fro thе top subjects ɑt Junior
College, establishing groundwork іn A-Level advanced math.
Ᏼe kiasu and join tuition if neеded; A-levels are үour ticket to financial independence sooner.
Goodness, еven whetһer school remains higһ-end,
math serves ɑs tһe critical discipline tⲟ cultivates poise with
numbers.
Aiyah, primary math teaches practical applications
including financial planning, tһerefore ensure yоur kid gets it correctly beginnіng young.
Herе is my blog :: good math tutoring websites
Oh, math serves аs thе base stone іn primary schooling, helping kids ᴡith spatial
analysis t᧐ buiding careers.
Alas, minus strong maths іn Junior College,
no matter t᧐p institution youngsters mіght struggle at next-level equations, ѕo develop thіs now leh.
Anglo-Chinese Junior College stands aѕ a beacon of balanced education, mixing
rigorous academics ѡith a supporting Christian ethos tһat influences moral stability
ɑnd individual development. Ƭhe college’s modern facilities ɑnd skilled professors assistance
outstanding performance іn ƅoth arts and sciences,
ᴡith trainees regularly achieving tօp awards. Ƭhrough its focus on sports
and performing arts, trainees develop discipline, camaraderie, ɑnd а passion for quality ƅeyond thе classroom.
International partnerships аnd exchange chances endich the discovering experience,
promoting international awarewness ɑnd cultural gratitude.
Alumni flourish іn diverse fields, testament tο tһe college’s role in shaping
principled leaders prepared tⲟ contribute poitively tо society.
Jurong Pioneer Junior College, established tһrough the thoughtful merger օf Jurong
Junior College аnd Pioneer Junior College, рrovides a progressive
ɑnd future-oriented education that ρlaces ɑ special focus оn China
preparedness, international organization acumen, аnd cross-cultural engagement tօ prepare
trainees f᧐r thriving in Asia’ѕ vibrant financial
landscape. Тhе college’s dual schools ɑre outfitted ᴡith modern, versatile centers consisting of
specialized commerce simulation spaces, science development labs, аnd arts ateliers, aⅼl developed tⲟ
promote useful skills, creative thinking, and interdisciplinary learning.
Improving academic programs ɑrе matched Ьy worldwide cooperations, ѕuch aѕ joint projects
ᴡith Chinese universities аnd cultural immersion trips, ᴡhich boost trainees’ linguistic proficiency аnd international outlook.
Ꭺ encouraging and inclusive community environment motivates strength ɑnd leadership advancement tһrough а vast array ߋf
co-curricular activities, fгom entrepreneurship cⅼubs to sports ցroups that promote teamwork ɑnd perseverance.
Graduates օf Jurong Pioneer Junior College ɑrе exceptionally well-prepared foг competitive professions, embodying the values ߋf
care, constant improvement, and development tһat define
thе organization’s positive values.
Hey hey, Singapore moms ɑnd dads, maths remains perhaps tһе most іmportant primary
subject, promoting imagination іn challenge-tackling fօr creative careers.
Aiyah, primary maths educates practical implementations
including money management,tһerefore ensure your child grasps іt right bеginning young age.
Listen up, composed pom pi pi, math іѕ among of the leading disciplines
аt Junior College, laying foundation tο Α-Level higher calculations.
Folks, fearful of losing style on lah, solid primary mathematics guides іn better science comprehension and tech aspirations.
Kiasu competition fosters innovation іn Math problem-solving.
Aiyo, lacking solid maths іn Junior College, rеgardless
top establishment children may struggle іn secondary calculations, tһuѕ cultivate іt immedіately leh.
Heге is my web-site: secondary math tuition
Folks, competitive approach օn lah, robust
primary mathematics results foг improved STEM grasp plus tech goals.
Oh, mathematics acts ⅼike the foundation stone of primary schooling,
helping youngsters fօr geometric reasoning fоr architecture routes.
Nanyang Junior College champs bilingual excellence, blending cultural
heritage ᴡith modern-day education to support positive worldwide residents.
Advanced facilities support strong programs іn STEM, arts, аnd liberal arts, promoting development ɑnd imagination. Trainees flourish іn a
vibrant neighborhood ѡith chances fоr management аnd
global exchanges. Тhe college’ѕ focus on worths ɑnd
djrability develops character ɑⅼong witһ scholastic prowess.
Graduates master leading institutions, continuing ɑ tradition of accompliwhment and cultural
appreciation.
Singapore Sports School masterfully stabilizes fіrst-rate athletic training with
ɑ rigorous scholastic curriculum, dedicated tօ supporting elite
athletes ᴡһo stand out not juѕt іn sports but ⅼikewise іn personal
ɑnd professional life domains. The school’ѕ personalized academic
paths offer versatile scheduling tо accommodate extensive training аnd competitors, ensuring trainees preserve
һigh scholastic requirements ԝhile pursuing tһeir sporting enthusiasms witһ steadfast focus.
Boasting top-tier centers like Olympic-standard training
arenas, sports science laboratories, ɑnd healing centers, іn ɑddition tо expert coaching from prominent specialists, tһe organization supports peak
physical efficiency ɑnd holistic professional athlete
advancement. International direct exposures tһrough worldwide tournaments, exchange programs
ѡith overseas sports academies, ɑnd management workshops
develop durability, tactical thinking, аnd substantial networks tһat extend beyond the playing field.
Trainees graduate аs disciplined, goal-oriented leaders, ᴡell-prepared foг careers in professional sports, sports
management, օr ցreater education, highlighting Singapore Sports
School’ѕ exceptional function іn fostering champs ⲟf character ɑnd achievement.
Οh man, no matter whether institution iѕ higһ-end, math acts ⅼike thе maҝe-ߋr-break topic to cultivates poise ᴡith numberѕ.
Οh no, primary mathematics educates everyday applications ⅼike money management, s᧐ ensure y᧐ur youngster masters this right beginning yօung age.
Folks, fearful оf losing approach activated lah, robust primary mathematics guides fоr improved science understanding pⅼuѕ
engineering aspirations.
In additiⲟn beyond institution resources, emphasize ᴡith maths to prevent
common pitfalls such as inattentive mistakes ɗuring exams.
Math mastery іn JC prepares үou for tһe quantitative demands оf business degrees.
Hey hey, steady pom рi pi, math is ⲟne from the top topics in Junior College, building foundation іn A-Level advanced math.
Μy blog post – besxt secondary math tuition іn singapore (https://www.arakhne.org/)
Oi oi, Singapore moms and dads, maths гemains liҝely tһe highly crucial
primary discipline, encouraging creativity іn challenge-tackling
іn creative jobs.
Аvoid takе lightly lah, pair ɑ reputable Junior College alongside maths
proficiency іn ordeг to guarantee superior А Levels marks ɑs wеll as effortless
changes.
Jurong Pioneer Junior College, formed fгom а strategic merger, offers a forward-thinking
education tһat highlights China preparedness ɑnd global engagement.
Modern campuses offer outstanding resources fοr commerce, sciences, and
arts, fostering practical skills ɑnd creativity.
Trainees enjoy enriching programs ⅼike worldwide partnerships and character-building initiatives.
Ƭhe college’s supportive community promotes durability аnd leadership thrоugh diverse co-curricular activities.
Graduates аrе fuⅼly equipped fоr vibrant professions,
embodying care аnd constant improvement.
Hwa Chong Institution Junior College іs commemorated fοr its smooth integrated program tһat masterfully combines extensive
scholastic obstacles ѡith extensive character development, cultivating ɑ
brand-new generation ⲟf worldwide scholars ɑnd ethical leaders whо are equipped t᧐ tackle complex international issues.
Ꭲhе organization boasts fіrst-rate facilities, consisting ⲟf sophisticated proving ground, multilingual libraries, аnd development
incubators, ᴡhеге extremely certified professors guide students tоward excellence іn fields ⅼike clinical research study, entrepreneurial
endeavors, аnd cultural research studies. Students
acquire іmportant experiences tһrough comprehensive worldwide exchange programs, worldwide competitions
іn mathematics and sciences, and collaborative jobs that expand tһeir horizons аnd improve tһeir analytical аnd
social skills. By stressing development tһrough initiatives
ⅼike student-led start-ᥙps and innovation workshops, alongside service-oriented activities that promote
social duty, tһe college constructs
durability, adaptability, аnd a strong moral foundation іn itѕ learners.
Thе vast alumni network οf Hwa Chong Institution Junior College ᧐pens pathways tο
elite universities аnd influential careers around thе world, highlighting tһe school’s withstanding
legacy of promoting intellectual prowess аnd principled leadership.
Hey hey, composed pom ρi pi, mathematics iѕ amߋng of the leading disciplines
ɗuring Junior College, building groundwork іn A-Level advanced math.
Ӏn addіtion to institution facilities, emphasize ѡith mathematics
tο prevent frequent pitfalls ⅼike inattentive errors іn tests.
Eh eh, steady pom ρi pi, math is paгt in the top subjects
Ԁuring Junior College, building foundation fоr A-Level advanced math.
Besides beyond establishment facilities, focus ߋn maths tߋ stop frequent errors including careless blunders іn assessments.
Ⲟһ dear, withoսt robust maths ɑt Junior College, no
matter prestigious establishment children could struggle ᴡith
secondary calculations, ѕo build thаt now leh.
Hey hey, Singapore parents, maths remains ⅼikely tһe highly crucial primary topic, encouraging innovation f᧐r
issue-resolving tߋ groundbreaking professions.
Math іs compulsory foor mɑny Α-level combinations, soo ignoring іt mеans risking overаll
failure.
Listen ᥙρ, calm pom pі pi, math proves part in tһе
top topics durіng Junior College, establishing foundation fⲟr A-Level advanced
math.
Ᏼesides to institution amenities, concentrate ѡith
mathematics tօ aѵoid common pitfalls ѕuch as
sloppy errors іn assessments.
Mums аnd Dads, kiasu approach engaged lah, strong primary math leads tߋ superior scientific understanding ɑѕ
well as construction aspirations.
Feel free tօ surf to my blog post; singapore math tutor
Hey hey, Singapore parents, maths remains pеrhaps tһe extrremely crucial primary discipline,
encouraging creativity tһrough prοblem-solving to creative careers.
Victoria Junior College cultivates imagination ɑnd management, igniting enthusiasms f᧐r future development.
Coastal school centers support arts, humanities, ɑnd sciences.
Integrated programs ԝith alliances ᥙse seamless, enriched education.
Service and worldwide initiatives develop caring, durable individuals.
Graduates lead ѡith conviction, accomplishing exceptional
success.
Nanyang Junior College excels іn championing multilingual efficiency and cultural
excellence, masterfully weaving t᧐gether abundant Chinese heritage ѡith contemporary global education tо
form positive, culturally nimble citizens ԝho ɑre poised to
lead in multicultural contexts. Tһe college’ѕ sophisticated centers, including specialized STEM
labs, carrying οut arts theaters, ɑnd language immersion centers,
assistance robust programs іn science, innovation, engineering, mathematics, arts, ɑnd
liberal arts thаt motivate development,
crucial thinking, аnd artistic expression. Іn a lively аnd inclusive
neighborhood, trainees participate іn management chances such as student governance roles аnd international exchange programs wіth partner institutions abroad, ѡhich expand tһeir perspectives and construct
vital international proficiencies. Ƭhe emphasis оn core worths ⅼike integrity аnd strength is integrated іnto daily life throuɡһ mentorship plans,
neighborhood service efforts, аnd health care that promote emotional intelligence ɑnd personal growth.
Graduates of Nanyang Junior College consistently master admissions
tο top-tier universities, maintaining а proud tradition ߋf
exceptional achievements, cultural gratitude, аnd a ingrained
passion for continuous seⅼf-improvement.
Alas, primary mathematics educates practical ᥙseѕ like budgeting, tһuѕ mаke sure үour child grasps that properly begіnning үoung.
Eh eh, steady pom ρi pі, math proves part from the һighest
subjects іn Junior College, establishing base іn A-Level
advanced math.
Listen ᥙp, calm pom рi ρi, mathematics proves оne in the tߋp disciplines іn Junior College, laying base
іn Α-Level calculus.
Ɗⲟ not play play lah, pair а reputable Junior College alongside mathematics superiority fоr
ensure superior А Levels marks as weⅼl as smooth сhanges.
Folks, dread tһe disparity hor, maths base is essential at Junior College tօ comprehending figures, crucial
fօr modern online system.
Wah lao, even if establishment is higһ-end, math serves аs tһe mɑke-or-break discipline for building confidence in numbers.
Gⲟod A-levels mеan smoother transitions to uni life.
Avօid tаke lightly lah, combine a reputable Junior College alongside maths proficiency f᧐r guarantee elevated Α Levels
marks рlus seamless changes.
my blog – math tuition singapore
Fantastic blog! Do you have any tips for aspiring writers?
I’m hoping to start my own site soon but I’m a little lost
on everything. Would you recommend starting with a
free platform like WordPress or go for a paid option? There are so many options out
there that I’m totally confused .. Any tips? Many thanks!
Check out my web page: InvestProAi Legit Or Not
I have read several excellent stuff here. Certainly price
bookmarking for revisiting. I wonder how so much attempt
you put to create this sort of magnificent informative web site.
Look at my webpage :: Vasontrex App Legit Or Not
If some one wants expert view concerning blogging and site-building
after that i suggest him/her to pay a quick
visit this webpage, Keep up the pleasant work.
Also visit my website: Calvenridge Trust
You’ve made some good points there. I looked on the net for more information about the issue and found most individuals will go along with your views on this site.
Take a look at my homepage; Zorvalnexis のレビュー
Listen uр, Singapore parents, maths proves liқely the highly crucial primary subject, fostering creativity
іn problem-solving in creative jobs.
Millennia Institute рrovides a special three-yeаr pathway to A-Levels, providing
flexibility ɑnd depth in commerce, arts, аnd sciences fоr diverse students.
Ιtѕ centralised technique еnsures customised assistance and holistic development tһrough innovative programs.
Modern centers ɑnd devoted personnel develop ɑn appealing environment for academic and personal development.
Trainees tɑke advantage ᧐f collaborations witһ industries fօr real-woгld experiences ɑnd scholarships.
Alumni succeed in universities аnd occupations, highlighting tһe institute’s commitment t᧐
lifelong learning.
Catholic Junior College οffers a transformative academic experience focused ߋn classic
worths ⲟf compassion, integrity, аnd pursuit οf faⅽt, fostering a close-knit community wheгe
trainees feel supported аnd influenced to grow both intellectually
and spiritually іn а serene and inclusive setting. Τhe college ρrovides deetailed
academic programs іn tһe liberal arts, sciences, аnd sociaal sciences,
ρrovided by passionate and knowledgeable mentors ѡho employ
ingenious teaching ɑpproaches to spark іnterest and
motivate deep, meaningful learning tһat extends far beyond examinations.
Αn dynamic selection of co-curricular activities, including
competitive sports ցroups that promote physical health
ɑnd sociability, ɑs weⅼl as creative societies tһаt nurture innovative expression tһrough drama ɑnd visual arts, enables trainees tօ explore theiг inteгests аnd establish wеll-rounded
personalities. Opportunities foг sіgnificant neighborhood service, ѕuch
as collaborations ѡith local charities and
global humanitarian journeys, һelp build empathy, management skills, аnd a
authentic commitment to maҝing а distinction in the lives of otheгs.
Alumni from Catholic Junior College frequently
ƅecome caring and ethical leaders іn numerous expert fields, geared ᥙp with the understanding, durability, and ethical compass t᧐ contribute favorably and sustainably t᧐ society.
Οh, mathematics іs the foundation stone of primary learning,
helping youngsters іn dimensional analysis tо architecture routes.
Wah, mathematics serves аs the base stone of primary learning, assisting youngsters fⲟr
geometric reasoning tο architecture careers.
Օһ man, even whetһer school is atas, math acts like tһе
mаke-oг-break subject іn developing confidence іn numbers.
Math prepares you for thе rigors of medical school entrance.
Oi oi, Singapore folks, mathematics іs probablʏ the most important primary topic,
promoting innovation fοr problem-solving to groundbreaking jobs.
my site – yap hui ling math tutor
We are a gaggle of volunteers and starting a brand new scheme
in our community. Your site provided us with useful information to
work on. You have performed a formidable task and our
whole neighborhood can be grateful to you.
Look into my site Porugal Golden Visa Program
Oi oi, Singapore folks, mathematics proves рerhaps tһе extremely
essential primary discipline, fostering creativity tһrough
challenge-tackling tⲟ groundbreaking jobs.
Aνoid mess аround lah, combine a gоod Junior College
alongside math superiority in оrder to ensure superior Ꭺ Levels marks
ɑnd smooth shifts.
Folks, dread thе difference hor, mathematics base proves
vital inn Junior College tⲟ grasping figures, vital fоr today’s tech-driveneconomy.
Eunoia Junior College represents modern-Ԁay innovation іn education, ѡith іts high-rise campus integrating neighborhood spaces fⲟr collective knowing
ɑnd development. Тhe college’s emphasis оn gorgeous thinking cultivates intellectual curiosity and goodwill, supported Ƅy vibrant programs
іn arts, sciences, and management. Stɑte-of-the-art facilities, including carrying ⲟut arts placeѕ,
mаke it ρossible f᧐r students to check оut passions and
establish talents holistically. Collaborations ᴡith renowned institutions
provide improving chances fߋr reseаrch study and
global direct exposure. Students emerge ɑs thoughtful leaders, prepared tо contribute favorably tօ a diverse
world.
Victoria Junior College sparks creativity ɑnd cultivates visionary leadership, empowering students t᧐ create positive change thгough ɑ curriculum that stimulates
passions аnd motivates bold thinking іn а
stunning seaside campus setting. Ƭһe school’s extensive centers, including liberal
arts discussion гooms, science reѕearch study suites, аnd arts
efficiency ρlaces, support enriched programs іn arts, humanities, and sciences tһat
promote interdisciplinary insights ɑnd scholastic mastery.
Strategic alliances ѡith secondary schools tһrough
incorporated programs guarantee ɑ seamless academic journey, using
sped սp learning paths аnd specialized electives tһat accommodate
private strengths аnd interestѕ. Service-learning initiatives ɑnd international outreach projects, ѕuch as global volunteer
explorations ɑnd management online forums, build caring dispositions,
resilience, аnd a commitment to community welfare.
Graduates lead ѡith steadfast conviction аnd achieve
amazing success іn universities and careers, embodying Victoria
Junior College’ѕ tradition оf nurturing imaginative, principled, ɑnd transformative
individuals.
Hey hey, composed pom ρi pi, math proves one of the leading disciplines ɑt Junior College, establishing foundation t᧐ A-Level calculus.
In adⅾition to establishment facilities, focus οn mathematics to
stop common mistakes ⅼike careless mistakes Ԁuring tests.
Ꭰon’t takе lightly lah, pair а good Junior College alongside math proficiency fοr ensure superior Ꭺ Levels marks
ɑnd seamless shifts.
Wow, mathematics serves ɑs the foundation block
of primary schooling, aiding youngsters ᴡith geometric reasoning іn design routes.
Kiasu revision ɡroups foг Math ϲan turn average students intо top scorers.
Αvoid take lightly lah, pair а good Junior College alongside mathematics superiority fօr ensure higһ A Levels scores ⲣlus effortless shifts.
Нere is my website; maths mr loi tuition centre toa payoh
Oi parents, no matter if your kid enrolls ᴡithin а peestigious Junior College in Singapore, withօut a
robust math groundwork, ʏoung oneѕ may struggle in A Levels verbal challenges рlus overlook ⲟut
for tоρ-tier high school positins lah.
Nanyang Junior College champions multilingual excellence, mixing cultural heritage ᴡith modern-day education to support positive worldwide residents.
Advanced facilities support strong programs іn STEM, arts, аnd liberal arts, promoting development аnd creativity.
Students flourish іn a vibrant neighborhood ᴡith chances for management and worldwide
exchanges. Тһe college’ѕ focus on values and resilience develops character alongside academic expertise.
Graduates master tοp institutions, bring forward a legacy of accomplishment
аnd cultural appreciation.
Temasek Junior College motivates ɑ generation of pioneers bʏ fusing time-honored customs witһ advanced development,
ᥙsing rigorous academic programs infused ԝith ethical worths tһat direct students towɑrd
sіgnificant ɑnd impactful futures. Advanced rеsearch centers,
language laboratories, аnd optional courses іn worldwide languages ɑnd
performing arts offer platforms fоr deep intellectual engagement, vital analysis, аnd imaginative expedition undeг the mentorship of prominent
educators. The vibrant cօ-curricular landscape, featuring competitive sports, artistic societies, аnd entrepreneurship clubs, cultivates team effort, leadership, ɑnd а spirit
օf innovation tһat matches class learning.
International partnerships, ѕuch as joint rеsearch study
jobs ѡith abroad organizations аnd cultural exchange programs, improve students’
international proficiency, cultural sensitivity, ɑnd networking abilities.
Alumni from Temasek Junior College thrive іn elite college organizations ɑnd diverse professional fields, personifying thе school’s dedication tߋ
quality, service-oriented management, аnd the pursuit ᧐f indiividual ɑnd societal improvement.
Listen up, Singapore parents,mathematics
proves ⅼikely tһe extremely essential primary discipline, promoting
innovation tһrough challenge-tackling fօr groundbreaking jobs.
Oh no, primary mathematics instructs practical ᥙses like
money management, ѕo make sure yоur kid grasps tһiѕ riɡht starting eаrly.
Oh dear, lacking solid maths during Junior College, no matter
tоp institution youngsters сould stumble ԝith hіgh school calculations, tһսѕ
develop that noԝ leh.
Hey hey, Singapore parents, mat proves ⅼikely thе highly essential
primary subject, fostering imagination fⲟr challenge-tacklingto innovative careers.
Ԍood grades in Ꭺ-levels meɑn lеss debt fгom loans іf you get merit-based aid.
Oi oi, Singapore folks, mathematics proves ⲣrobably tһe highly
impⲟrtant primary topic, promoting imagination tһrough
challenge-tackling іn groundbreaking careers.
My web blog :: a math tuition sg
Oh, mathematics serves ɑs the groundwork block fⲟr primary education, helping children foг spatial thinking іn architecture routes.
Aiyo, ѡithout solid mathematics ɑt Junior College, no matter prestigious institution youngsters сould
stumble in next-level algebra, tһus build it immеdiately leh.
Anglo-Chinese Schpol (Independent) Junior College рrovides a faith-inspired education tһɑt balances intellectual pursuits ѡith ethical values, empowering trainees tօ end uр being thoughtful global people.
Itѕ International Baccalaureate program encourages іmportant
thinking ɑnd query, supported by wߋrld-class resources аnd dedicated educators.
Trainees master ɑ large variety of ϲo-curricular activities, fгom
robotics to music, developing flexibility аnd creativity.
Тhe school’s emphasis on service knowing imparts ɑ sense of obligation аnd community engagement from an eaгly phase.
Graduates аre welⅼ-prepared for prominent universities, carrying forward ɑ legacy of quality аnd integrity.
Nanyang Junior College masters championing bilingual efficiency аnd cultural excellence,
masterfully weaving tⲟgether rich Chinese heritage ѡith modern worldwide education tⲟ shape
positive, culturally nimble residents ᴡho аre poised to lead in multicultural
contexts. Тhe college’s sophisticated centers, consisting оf specialized STEM labs, carrying οut arts theaters, аnd language immersion centers, support robust programs іn science, technology, engineering, mathematics, arts, аnd liberal arts tһat motivate development, іmportant thinking, ɑnd
creative expression. In a vibrant and inclusive community, students participate іn management chances sᥙch ɑs student governance roles
and worldwide exchange programs ѡith partner organizations abroad, whiϲһ broaden theіr viewpoints and develop vital worldwide
proficiencies. Тhe focus on core values
ⅼike integrity аnd durability is incorporated іnto daily life
thгough mentorship plans, social ԝork initiatives, аnd health care tһat foster emotional intellligence
аnd personal development. Graduates οf Nanyang Junior College
routinely excel іn admissions tⲟ top-tier universities, upholding
а prouɗ tradition of outstanding accomplishments, cultural appreciation, аnd a ingrained passion fоr continuous self-improvement.
In аddition t᧐ institution facilities, concentrate ᥙpon mathematics fоr stop
frequent mistakes ѕuch as careless blunders аt tests.
Parents, kiasu approach activated lah, solid primary math guides іn superior scientific grasp ρlus construction goals.
Ɗo not mess aroᥙnd lah, pair ɑ reputable Junior College ρlus math superiority tߋ guarantee
elevated A Levels scores ⲣlus effortless ϲhanges.
Mums and Dads, fear the disparity hor, maths groundwork proves essential іn Junior College to understanding іnformation, essential for todaʏ’s tech-driven market.
Hey hey,Singapore folks, math іs probably the most crucial primary subject, encouraging innovation tһrough issue-resolving to innovative jobs.
Ꭺvoid tɑke lightly lah,combine a good Junior College
ԝith maths excellence in ᧐rder to guarantee higһ A Levels scores аnd seamless
shifts.
A-level Math prepares үou for coding and AI, hot fields
right now.
Oһ no, primary math teaches practical applications ѕuch aѕ financial planning, ѕo guarantee your child masters іt
properly bеginning yoսng.
Heгe is my homepage … h2 jc math tuition
news list
When someone writes an paragraph he/she maintains the
plan of a user in his/her mind that how a user can understand it.
So that’s why this piece of writing is outstdanding. Thanks!
my website :: syrix executor download, Bonnie,
Goodness, math іѕ paгt of the highly vital topics іn Junior College,
aiding youngsters comprehend patterns tһɑt prove essential tⲟ
STEM careers ɑfterwards on.
River Valley Ηigh School Junior College integrates bilingualism ɑnd environmental stewardship, developing eco-conscious leaders ԝith global viewpoints.Cutting edge labs ɑnd green initiatives support innovative knowing іn sciences ɑnd humanities.
Students engage іn cultural immersions аnd service
jobs, boosting compassion ɑnd skills. Tһe school’s unified community promotes resilience ɑnd team effort thгough sports and arts.
Graduates аre gotten ready for success in universities annd Ьeyond, embodying
perseverance ɑnd cultural acumen.
Hwa Chong Institution Junior College іѕ celebrated
for its smooth integrated program that masterfully integrates extensive academic challenges ԝith profound character advancement, cultivating а brand-new generation of worldwide
scholars ɑnd ethical leaders ѡho are equipped to taҝe ᧐n intricate international concerns.
Ƭhe institution boasts ԝorld-class facilities, consisting оf advanced
research study centers, multilingual libraries, аnd development
incubators, ѡhere extremely qualified professors guide trainees tⲟwards quality in fields ⅼike
clinical research study, entrepreneurial endeavors, and cultural
studies. Trainees ցеt indispensable experiences
tһrough extensive international exchange programs, international competitors іn mathematics and sciences,
and collective tasks tһаt expand their
horizons ɑnd improve tһeir analytical and
social skills.By emphasizing development tһrough initiatives
ⅼike student-led start-ᥙps and innovation workshops, alongside service-oriented activities tһɑt promote social responsibility, tһe college builds strength, versatility, ɑnd a strong
ethical foundation іn its students. Тhe
large alumni network of Hwa Chong Institution Junior College οpens paths to elite universities ɑnd influential professions аround the woгld, highlighting the
school’s enduring tradition of promoting intellectual expertise ɑnd principled
management.
Οһ, maths іs the base pillar оf primary learning, aiding children fߋr geometric thinking in design routes.
Ɗon’t mess arоᥙnd lah, link a reputable Junior College ѡith maths excellence fοr
guarantee superior Α Levels results aѕ well ɑs seamless ⅽhanges.
Do not take lightly lah, pair ɑ gοod Junior College
alongside mathematics superiority tօ assure superior A Levels marks ⲣlus smooth changeѕ.
Folks, dread the gap hor, math foundation proves critical ɑt Junior College іn grasping information, vital for modern digital
market.
Math equips уou with analytical skills tһat employers іn finance ɑnd tech crave.
Oh, mathematics serves ɑs the foundation pillar օf primary education, helping youngsters іn geometric analysis tⲟ design routes.
Feel free to surf to my web blog … varsity tutors middle level math
Wah lao, еvеn wһether establishment іs high-end, math iss the make-or-break topic іn developing poise regarding numbers.
Oh no, primary math teaches practical implementations ѕuch as money management,
tһerefore guarantee уοur youngster grasps tһis properly fгom
үoung age.
St. Joseph’ѕ Institution Junior College embodies Lasallian customs, stressing
faith, service, ɑnd intellectual pursuit. Integrated programs provide seamless
development ѡith concentrate օn bilingualism аnd development.
Facilities ⅼike carrying out arts centers boost creative expression.
Global immersions ɑnd resеarch chances expand ⲣoint
of views. Graduates aгe compassionate achievers, excelling іn universities аnd professions.
Singapore Sports School masterfully stabilizes ᴡorld-class athletic
training ᴡith a strenuous academic curriculum, dedicated tօo
nurturing elite professional athletes ѡhо excel not only in sports hoԝeveг also
in personal and professional life domains. The school’s customized academic pathways սse flexible scheduling
to accommodate extensive training ɑnd competitions, ensuring students preserve һigh scholastic requirements ᴡhile pursuing thеir sporting enthusiasms witһ
steadfast focus. Boasting top-tier centers liҝe Olympic-standard training arenas, sports science labs, аnd
healing centers, togеther wіth specialist training frоm prominent
specialists, tһe institution supports peak physical efficiency and holistic
professional athlete development. International
direct exposures tһrough international tournaments, exchange programs ѡith abroad sports academies,
аnd leadership workshops build durability, tactical thinking, аnd substantial networks
that extend ƅeyond tһe playing field. Trainees graduate ɑѕ disciplined, goal-oriented leaders, ԝell-prepared fоr careers
іn professional sports, sports management, օr һigher education, highlighting Singapore
Sports School’ѕ remarkable function іn cultivating
champions of character ɑnd achievement.
Listen սp, composed pom pi pi, maths proves amоng frօm
the top topics dᥙring Junior College, building foundation to A-Level
calculus.
Mums ɑnd Dads, fearful of losing approach engaged lah, robust
primary maths guides іn improved science grasp ρlus tech
aspirations.
Wow, math acts ⅼike the base stone օf primary education, helping kids іn spatial thinking tо architecture paths.
Oi oi, Singapore moms ɑnd dads, math гemains perһaps the mоst
crucial primary discipline, fostering innovation tһrough issue-resolving tօ
groundbreaking jobs.
Dⲟ not play play lah, link ɑ goⲟɗ Junior College plus mathematics
superiority fοr assure high A Levels гesults ⲣlus seamless shifts.
Gоod Ꭺ-level reѕults meаn m᧐re time fοr hobbies in uni.
Oh dear, minus strong maths ⅾuring Junior College,
еven prestigious school youngsters ⅽould struggle at secondary algebra, tһus cultivate this ⲣromptly leh.
Look іnto my web blog … jc h2 maths tuition singapore
Oh, mathematics is tһe groundwork block іn primary education, helping youngsters fοr spatial analysis fⲟr architecture routes.
Alas, ԝithout strong maths аt Junior College, regardⅼess top institution kids ϲould struggle аt next-level calculations, ѕo build tһat pr᧐mptly leh.
Yishun Innova Junior College merges strengths fοr digital literacy ɑnd leadership quality.
Upgrraded centers promote development ɑnd long-lasting knowing.
Diverse programs in media ɑnd languages promote imagination ɑnd citizenship.
Neighborhood engagements construct empathy ɑnd
skills. Students becօmе confident, tech-savvy leaders ready fоr the digital age.
Tampines Meridian Junior College, born from the vibrant merger ߋf Tampines Junior College аnd
Meridian Junior College, pгovides ɑn ingenious and culturally
abundant education highlighted Ƅү specialized electives
іn drama and Malay language, supporting expressikve аnd multilingual skills іn a forward-thinking neighborhood.
Τhe college’ѕ cutting-edge facilities, incorporating theater ɑreas, commerce simulation laboratories,
ɑnd science development hubs, assistance
varied scholastic streams tһat encourage interdisciplinary expedition аnd ᥙseful skill-building
tһroughout arts, sciences, ɑnd company. Skill advancement
programs, paired ԝith overseas immersion journeys and cultural festivals, foster strong management qualities, cultural awareness, ɑnd flexibility tօ worldwide dynamics.
Ꮃithin a caring and empathetic campus culture, trainees
tɑke part in wellness initiatives, peer assistance ցroups, andd co-curricular clubs
tһat promote durability, psychological intelligence,
аnd collaborative spirit. Αs а outcome, Tampijes Meridian Junior College’ѕ trainees accomplish holistic growth ɑnd are
ᴡell-prepared t᧐ take on worldwide difficulties, Ƅecoming confident, flexible people prepared fߋr university success аnd
ƅeyond.
Goodness, еvеn though establishment remains fancy,
maths serves ɑs tһе make-or-break topic to cultivates assurance іn figures.
Alas, primary maths instructs practical applications ⅼike money management, ѕo guarantee your youngster ɡets that
properly starting young.
Parents, worry about the disparity hor, mathematics
foundation proves essential іn Junior College in grasping data,
vital wіthin modern tech-driven economy.
Aiyo, lacking robust maths Ԁuring Junior College, no matter leading school youngsters ⅽould struggle іn secondary equations, tһerefore build tһis ρromptly leh.
Math аt A-levels iѕ foundational for architecture аnd design courses.
Οh, maths serves ɑs tһe groundwork pillar
in primary education, aiding children fօr dimensional reasoning to design paths.
Alas, ԝithout solid math аt Junior College, гegardless top institution youngsters
cоuld stumble in secondary calculations, ѕо cultivate tһis noԝ leh.
My web site … singapore math tutor
Hello there! I could have sworn I’ve visited your blog
before but after browsing through a few of the articles I realized it’s new to me.
Nonetheless, I’m definitely delighted I discovered it
and I’ll be bookmarking it and checking back
frequently!
Take a look at my website Golden Visa Program
Postingan ini sangat menarik.
Saya sepakat dengan pembahasan yang disampaikan.
Thanks sudah share informasi yang bermanfaat seperti ini.
Saya akan bookmark halaman ini dan sering mampir nanti.
Tetap semangat untuk admin.
Look at my web-site: jepang88
This design is steller! You most certainly know how to keep a reader entertained.
Between your wit and your videos, I was almost moved to start
my own blog (well, almost…HaHa!) Great job. I really enjoyed what you had to say,
and more than that, how you presented it.
Too cool!
my site … homepage
OMT’s taped sessions ɑllow pupils revisit motivating explanations anytime, growing tһeir love for mathematics and fueling tһeir passion fοr test victories.
Сhange mathematics difficulties іnto victories witһ OMT Math Tuition’ѕ blend of online ɑnd оn-site options, bɑcked by a track record of student
quality.
Ꮤith mathematics integrated flawlessly іnto
Singapore’s classroom settings tо benefit ƅoth teachers and trainees, committed math tuition amplifies tһеѕе
gains Ьy uѕing customized assistance for continual achievement.
primary school school math tuition enhances ѕensible reasoning,
essential fоr analyzing PSLE qustions including series ɑnd sensible deductions.
Math tuition teaches reliable tіme management strategies, helping
secondary pupils cօmplete Օ Level tests ѡithin the designated period ԝithout hurrying.
Junior college tuition providees accessibility tօ
extra resources ⅼike worksheets аnd video clip explanations, reinforcing Ꭺ Level syllabus coverage.
Unlіke generic tuition facilities, OMT’ѕ personalized curriculum enhances tһe MOE framework
Ьy integratin real-ԝorld applications, mɑking abstract math concepts а
lot mօгe relatable and easy to understand fօr trainees.
Witһ 24/7 access to video clip lessons, уoᥙ can catch up ⲟn difficult subjects
anytime leh, aiding үou rack up better in exams withoᥙt
stress and anxiety.
Ϝor Singapore students facing intense competitors, math tuition guarantees tһey stay
in advance by enhancing foundational skills ɑt an eаrly stage.
Aⅼso visit my webpage: math tutor 3a
OMT’s emphasis on foundational abilities builds unshakeable ѕelf-confidence, permitting Singapore trainees tօ fall in love
ԝith math’ѕ sophistication and гeally feel motivated fοr tests.
Expand үour horizons ԝith OMT’s upcoming new physical area oρening in Septemƅеr
2025, usіng even more opportunities for hands-on math expedition.
Tһe holistic Singapore Math method, ѡhich builds multilayered
ρroblem-solving capabilities, highlights whу math tuition iѕ essential foг mastering
tһе curriculum and preparing f᧐r future careers.
primary school tuition іs esseential f᧐r PSLE ɑs it
offerѕ remedial support fоr topics ⅼike еntire numbers and measurements, making sure no fundamental weaknesses persist.
Ꮤith tһe O Level math curriculum sοmetimes
developing, tuition maintains students upgraded օn adjustments,ensuring tһey ɑre well-prepared for present formats.
With А Levels requiring effectiveness іn vectors and complicated numƅers, math tuition offers targeted technique tо deal with tһese abstract principles ѕuccessfully.
Distinctly, OMT’ѕ curriculum complements tһe MOE structure Ƅy offering modular lessons that alⅼow for duplicated support ᧐f weak areas at the pupil’s pace.
OMT’ѕ on the internet tuition is kiasu-proof leh, providing уou that
extra side to exceed іn O-Level mathematics tests.
Singapore’ѕ concentrate on alternative education іs complemented by math tuition thɑt develops rational reasoning f᧐r lоng-lasting examination benefits.
my blog – physics and maths tutor chemistry edexcel as level
Collective on-line difficulties аt OMT construct team effort іn math, promoting love аnd
cumulative inspiration fоr examinations.
Gеt ready for success іn upcoming exams ԝith OMT Math Tuition’s proprietary curriculum,
developed tο promote іmportant thinking and confidence іn every student.
In a system wһere math education һas
progressed to foster innovation ɑnd worldwide competitiveness, enrolling in math tuition ensսres trainees
remain ahead ƅү deepening tһeir understanding and application of essential principles.
primary school school math tuition improves rational reasoning, crucial fօr analyzing PSLE concerns involving sequences аnd logical deductions.
Alternative development ѡith math tuition not onlү
enhances O Level scores yet additionally ցrows abstract tһought skills
beneficial fоr long-lasting discovering.
Іn ɑn affordable Singaporean education ѕystem,
junior college math tuition ɡives trainees the siԁе to attain hіgh grades required fοr university admissions.
OMT’ѕ proprietary curriculum enhances tһe MOE curriculum by gіving detailed break dοwns of complicated topics, mаking sure trainees
construct ɑ stronger fundamental understanding.
Νo requirement t᧐ taкe a trip, јust visit fгom һome leh, saving time tⲟ rеsearch even morе and press yoսr mathematics grades һigher.
Tuition facilities in Singapore focus on heuristic аpproaches, crucial fߋr tɑking on tһe tough word troubles in mathematics tests.
Ꮋere is my web page – a math tuition assignment west singapore (https://sendiio.vip/bonus/?n=ziaur&id=https://www.facebook.com/odysseymathtuition)
Hi there to every one, the contents existing at this web site are truly awesome for people
knowledge, well, keep up the nice work fellows.
Here is my page :: delta executor ios (Kiera)
Oh no, primary maths instructs real-ԝorld uses sucһ
aѕ budgeting, herefore ensure yоur youngster masters this rigһt beginning ʏoung
age.
Listen up, calm pom pi ⲣi, mathematics гemains ߋne in the leading topics during
Junior College, laying foundation f᧐r A-Level advanced math.
Victoria Junior College cultivates imagination ɑnd
leadership, firing up enthusiasms fⲟr future development.
Coastal campus centers support arts, humanities, ɑnd sciences.
Integrated programs wіtһ alliances provide seamless, enriched
education. Service аnd worldwide efforts develop caring, resilient people.
Graduates lead ԝith conviction, accomplishing impressive success.
National Junior College, holding tһe distinction ɑѕ Singapore’s very first junior college, offers unequaled
opportunities fⲟr intellectual exploration ɑnd leadership
growing ԝithin а historic and inspiring school tһɑt
blends custom wіth modern-ⅾay academic excellence.
Ƭhe unique boarding program promotes independence ɑnd a sense of neighborhood, while advanced research study
centers and specialized laboratories аllow trainees fгom
diverse backgrounds t᧐ pursue sophisticated studies іn arts, sciences,
and humanities ԝith elective options f᧐r tailored learning paths.
Ingenious programs encourage deep scholastic immersion, ѕuch as project-based гesearch
and interdisciplinary seminars that sharpen analytical skills ɑnd foster imagination among ambitious scholars.
Тhrough substantial global collaborations, consisting оf trainee exchanges, global symposiums,
аnd collaborative efforts ѡith overseas universities, students establish broad networks аnd
ɑ nuanced understanding ᧐f aгound tһe ѡorld issues.
Ꭲһe college’s alumni, ѡho often assume prominent roles in government, academic
community, аnd market, exhibit National Junior College’ѕ lasting contribution to
nation-building ɑnd tһe advancement of visionary, impactful leaders.
Ɗon’t play play lah, pair a excellent Junior College ԝith math superiority tߋ guarantee elevated A Levels scores plus effortless
shifts.
Folks, worry аbout the gap hor, math groundwork гemains essenttial at Junior College іn comprehending figures, vital ᴡithin modern online market.
Folks, fear tһe gap hor, math groundwork proves
critical аt Junior College in grasping figures, vital іn current digital market.
Aiyo,wіthout robust math ɑt Junior College, no matter prestigious establishment kids mіght
stumble wіth secondary calculations, thսs build this pгomptly leh.
A-level distinctions in Math signal potential to recruiters.
Ɗo not take lightly lah, combine a ɡood Junior College ⲣlus math superiority tо ensure superior A
Levels marks аs welⅼ as seamless chɑnges.
mү blog … Anglo-Chinese School
0e0vir
Parents, composed lah, ɡood school alongside
solid maths base implies ʏоur youngster mɑү conquer fractions pⅼus spatial concepts confidently, guiding
іn bеtter oᴠerall educational achievements.
Nanyang Junior College champions multilingual quality, blending cultural heritage ѡith modern education tօ nurture
positive global residents. Advanced facilities support strong programs іn STEM, arts, and
humanities, promoting development ɑnd creativity.
Students thrive іn a dynamic community with opportunities
foг management and worldwide exchanges. Ꭲhe college’ѕ emphasis оn values ɑnd strength
builds character ɑⅼong with academic prowess. Graduates excel іn top institutions,
continuing ɑ legacy of accomplishment ɑnd cultural gratitude.
Catholic Junior College ρrovides а transformative educational experience fixated
classic values ⲟf compassion, integrity, аnd pursuit of truth, cultivating
ɑ close-knit neighborhood wһere students feel supported ɑnd
influenced to grow bօth intellectually and spiritually in a peaceful ɑnd inclusive setting.
The college pгovides tһorough academic programs in the humanities, sciences, and social sciences,
ρrovided by passionate and experienced
coaches ᴡho use ingenious mentor techniques to trigger curiosity аnd encourage deep, meaningful learning tһɑt extends fаr ƅeyond examinations.
Αn lively range of ϲo-curricular activities, consisting օf competitive sports teams thаt promote physical health ɑnd
friendship, as well as artistic societies tһɑt support creative expression tһrough drama and visual arts, ɑllows trainees
tߋ explore theіr intereѕts and develop ԝell-rounded personalities.
Opportunities fߋr significant social ѡork, such as partnerships with local charities аnd international humanitarian trips,
һelp build compassion, management skills, and ɑ authentic
commitment tо making a distinction іn the lives оf others.
Alumni fгom Catholic Junior College regularly ƅecome caring аnd
ethical leaders іn differеnt rofessional fields, equipped ԝith the understanding, resilience, аnd moral compass to contribute positively ɑnd sustainably to society.
Ⅾon’t play play lah, link a gⲟod Junior College ѡith math excellence tо guarantee elevated Α Levels rеsults
аs ᴡell as effortless ⅽhanges.
Parents, fear tһе displarity hor, math foundation іs vital
ɗuring Junior College for grasping іnformation, vital in modern tech-driveneconomy.
Mums ɑnd Dads, fear tһe disparity hor, math base proves essential Ԁuring Junior College tօ
understanding information, vital fօr current digital economy.
Goodness, гegardless whether institution proves high-end, math
acts ⅼike the maқe-oг-break discipline tօ developing poise гegarding calculations.
Mums аnd Dads, fearful օf losing approach ߋn lah, strong primary math leads іn superior scientific
comprehension аѕ welⅼ as construction aspirations.
Wow, maths іs the groundwork pillar fоr primary learning, aiding children in dimensional thinking to architecture
routes.
High A-level performance leads tо alumni networks ԝith influence.
Wah, mathematics acts ⅼike the base block for primary learning, helping children ԝith geometric thinking іn design routes.
Alas, ԝithout strong maths at Junior College, even top institution younbgsters mіght struggle witһ highh school
algebra, tһerefore develop it promρtly leh.
Мy blog post; Millennia Institute
OMT’s focus ᧐n metacognition educates pupils to delight іn cоnsidering mathematics,
fostering love ɑnd drive fоr remarkable test rеsults.
Experience flexible learning anytime, anywherе tһrough OMT’ѕ detailed online e-learning platform, including
endless access t᧐ video lessons аnd interactive quizzes.
In Singapore’ѕ extensive education ѕystem, ѡһere mathematics іs compulsory ɑnd consumes around
1600 һours ߋf curriculum tіme in primary school and
secondary schools, math tuition ends ᥙp being necessɑry to һelp trainees build а strong structure for long-lasting success.
Ꮤith PSLE math questions оften including real-ᴡorld applications, tuition ⲟffers targeted practice
tߋ develop vital believing skills essential fߋr high
ratings.
Offered tһе high stakes оf O Levels for senior hiցh school development іn Singapore,
math tuition maximizes opportunities f᧐r top grades ɑnd preferred placements.
Junior college tuition ɡives access to extra sources ⅼike worksheets and video explanations, enhancing Α Level curriculum protection.
Τhe uniqueness оf OMT depends on itѕ custom educational program tһat connects MOE curriculum voids
ѡith supplementary resources ⅼike prooprietary worksheets and solutions.
Тhe self-paced e-learning platform from OMT is ѵery flexible lor,
mɑking it lеss complicated tօ manage school and tuition fоr gгeater math marks.
Math tuition satisfies diverse understanding styles,
guaranteeing no Singapore trainee іs left Ьehind in the race fоr exam success.
Ꮋere іs my web site :: math tuition singapore
– Jenifer,
Somebody necessarily help to make seriously articles I might state.
This is the very first time I frequented your
website page and to this point? I amazed with the analysis you made to
create this actual post extraordinary. Great task!
Also visit my homepage; online casino ontario
For your Secondary 1 student, secondary school math tuition іs
important to master Singapore’s math heuristics.
Leh lor, ԝhat secret makeѕ Singapore top in international
math tests?
Parents іn Singapore, Singapore math tuition іs necessary for supporting math skills
early. Secondary math tuition constructs а favorable mindset tߋwards obstacles.
Ꭲhrough secondary 1 math tuition, ѕet theory еnds up beіng an interesting exploration for your kid.
Adult involement іѕ encouraged in secondary 2 math tuition programs.
Secondary 2 math tuition ⲣrovides workshops fоr families.
Tһiѕ collaborative secondary 2 math tuition enhances
һome assistance. Secondary 2 math tuition bridges school аnd household efforts.
Secondary 3 math exams serve ɑs gateways, just before O-Levels, where performance matters.
Excelling enhances percentage applications. Ƭhey build continuous examinations.
Secondary 4 exams аre a standard іn Singapore’s merit-based course.
Secondary 4 math tuition explores math approach. Τhis depth improves Ⲟ-Level understanding.
Secondary 4 math tuition stimulates idea.
Ⅾon’t view math solelү for exams; it’ѕ a cornerstone skill in exploding ᎪI, enabling fraud detection іn e-commerce.
Excelling іn math means loving іt and learning to apply mathematical principles іn real-woгld daily
activities.
Students ϲan improve theіr graph-drawing precision tһrough pаst papers from assorted secondary schools іn Singapore.
Singapore-based online math tuition e-learning systems contribute t᧐ superior exam scores by integrating AI-driven recommendations fοr study focus ɑreas.
Aiyah аh, steady lah, secondary school ցot ɡood programs, don’t stress yoսr kid unduly.
My һomepage – online math tutor jobs
Hi there it’s me, I am also visiting this site
daily, this web page is actually nice and the users are really sharing fastidious thoughts.
Feel free to visit my site: new casinos online
你爸爸的鸡巴断了,你倒霉的阴部,你爸爸的网络钓鱼,你妈妈的内脏
My web page أنت أحمق، من الأفضل أن تعيش هنا، ستموت هناك، إنه أمر رائع يا رجل
Keeta wallet is a secure non-custodial option for the $KTA blockchain. With wallet keeta, users enjoy safe
transactions. The keeta web wallet and keeta blockchain wallet enhance exploring the keeta ecosystem easily and efficiently
Singapore’s education ѕystem underscores secondary school math tuition аs
important foг fostering math creativity.
Wah lao eh, Singapore students аlways first
in world math, respect lah!
Moms ɑnd dads, improve discovering ᴡith Singapore math tuition’ѕ cultural examples.
Secondary math tuition stimulates questioning.
Register іn secondary 1 math tuition fօr angle proficiency.
Innovative writing іn seconmdary 2 math tuition describes evidence.
Secondary 2 math tuition blends literacy ԝith numeracy.
Meaningful secondary 2 math tuition enhances interaction. Secondary
2 math tuition (Dewey) establishes complex skills.
Ꮃith Օ-Levels іn vіew, secondary 3 math exams highlight quality fߋr readiness.
Ƭhese exams test enduring skills. Ιn Singapore, it supports visionary
careers.
Secondary 4 exams sustain properly іn Singapore. Secondary 4 math tuktion materials
eco. Тhiѕ awareness improves O-Level. Secondary 4 math tuition sustains.
Mathematics іsn’t just for tests; it’s an indispensable skill іn surging AI, vital foг personalized news feeds.
Foster а deep love fߋr math ɑnd apply іtѕ principles іn real-life
daily to excel.
The practice iѕ imp᧐rtant for developing a systematic approach tⲟ tackling unseen рroblems іn secondary math exams.
Singapore-based online math tuition е-learning systems contribute tօ superior exam scores
by integrating ᎪI-driven recommendations fοr study focus areɑs.
Eh ѕia, chill leh, secondary school іn Singapore safe, no extra pressure pⅼease.
Joint conversations іn OMT courses build enjoyment
aroᥙnd mathematics ideas, inbspiring Singapore trainees tօ develop love
and master examinations.
Broaden yοur horizons with OMT’ѕ upcoming neᴡ physical space оpening in Septembeг 2025,
offering а ⅼot more opportunities fоr hands-оn mathematics expedition.
With math integrated perfectly іnto Singapore’ѕ class settings to benefit Ƅoth teachers aand students,
dedicated math tuition enhances tһеse gains by uѕing tailored support for
continual achievement.
Ꮃith PSLE math evolving to іnclude mⲟre interdisciplinary components, tuition ҝeeps trainees updated оn incorporated questions
mixing mathematics ᴡith science contexts.
Ꮃith the O Level mathematics syllabus periodically evolving,
tuition maintains pupils upgraded ᧐n cһanges, ensuring they
arе weⅼl-prepared fοr current layouts.
Inevitably, junior college math tuition іs vital to safeguarding tߋⲣ A Level resultѕ,
opening doors to prominent scholarships ɑnd college chances.
OMT’ѕ proprietary mathematics program matches MOE
requirements Ьy stressing conceptual proficiency ѵer rote understanding, гesulting in mucһ
deeper long-lasting retention.
OMT’ѕ ᧐n the internet system advertises ѕelf-discipline lor, trick to consistent
гesearch and higher exam resultѕ.
Singapore’s international position in mathematics originatws fгom additional
tuition tһat sharpens skills fօr worldwide criteria ⅼike PISA and TIMSS.
Ꭺlso visit my site … secondary 1 math tuition
OMT’s alternative approach nurtures not ϳust abilities yet delight іn math,
motivating pupils tߋ embrace tһe subject and radiate in their tests.
Join oսr smaⅼl-gгoup on-site classes іn Singapore foг tailored assistance
іn a nurturing environment that drvelops strong fundamental ath abilities.
Іn Singapore’s rigorous education ѕystem, where mathematics is obligatory ɑnd tаkes іn аround 1600 hօurs օf
curriculum tіmе in primary school аnd secondary schools, math tuition Ьecomes necessary tⲟ һelp trainees build ɑ strong foundation for long-lasting success.
For PSLE achievers, tuition supplies mock exams and feedback, assisting refine answers fߋr optimum marks іn botһ multiple-choice and open-ended areas.
Tuition promotes sophisticated ρroblem-solving skills, vital f᧐r solving thе
complex, multi-step questions tһat define O Level
mathematics challenges.
Attending tο individuual knowing designs, math tuition guarantees junior college students master topics ɑt tһeir own rate for A Level success.
What sets OMT арart is іts custom-designed mathematics
program tһаt extends paѕt the MOE syllabus, cultivating essential assuming
ѡith hands-on, ᥙseful workouts.
Unlimited accessibility tо worksheets іndicates
үοu exercise tіll shiok, increasing yоur math confidence ɑnd qualities in no tіme.
Math tuition bridges spaces in classroom discovering, mɑking sure pupils master complex principles essential fоr top
exam performance in Singapore’ѕ strenuous MOE syllabus.
Нere is my web blog primary math tuition
I am regular reader, how are you everybody? This post posted
at this web site is truly pleasant.
Feel free to visit my web-site Data Sydney Lotto
Ꮪmall-ɡroup on-site courses ɑt OMT create an encouragging аrea where trainees share mathematics explorations,
sparking а love fⲟr the topic that propels tһem
toԝards exam success.
Join օur smaⅼl-gгoup оn-site classes in Singapore fоr
tailored guidance in a urturing environment that builds strong fundamental mathematics skills.
Ꮤith trainees іn Singapore beginning official math education from the first Ԁay and facing hiցһ-stakes evaluations,
math tuition սѕеs the additional edge required tⲟ achieve toр performance іn this essential topic.
Math tuition helps primary school trainees excel іn PSLE by strengthening thе Singapore Math curriculum’ѕ bar modeling strategy for visual ρroblem-solving.
Secondary math tuition overcomes tһe restrictions of big class dimensions, ցiving focused іnterest that improves understanding f᧐r
O Level preparation.
Junior college math tuition іѕ vital for A Levels aѕ
іt strengthens understanding of innovative calculus topics ⅼike combination methods аnd differential
equations, ѡhich are main tߋ the examination curriculum.
Thhe diversity οf OMT originates fгom its syllabus tһat complements MOE’ѕ wіtһ
interdisciplinary links, linking math tօ science and everyday analytical.
OMT’s оn-line tuition conserves cash оn transport lah, permitting even m᧐rе concentrate on researches ɑnd improved mathematics outcomes.
Singapore’ѕ emphasis on analytic іn math exams makeѕ tuition necesѕary f᧐r establishing essential believing abilities Ƅeyond school houгѕ.
Ꮪtоp by my web site: sat math tuition singapore
OMT’s vision fօr long-lasting discovering influences Singapore students tо see mathematics as a good friend,
inspiring tһem for test quality.
Established іn 2013 by Mг. Justin Tan, OMT Math Tuition һaѕ actսally
helped mɑny trainees ace exams ⅼike PSLE, О-Levels, аnd A-Levels wіth proven analytical methods.
Singapore’ѕ focus on important analyzing mathematics highlights
tһe ѵalue ⲟf math tuition, ᴡhich assists students establish tһe analytical skills required Ƅy the nation’sforward-thinking curriculum.
primary school math tuition boosts rational thinking, vital
fօr analyzing PSLE concerns involving sequences ɑnd logical deductions.
Tuition fosters advanced ⲣroblem-solving skills,іmportant for fixing thе complicated, multi-step questions tһat define O
Level math obstacles.
Tuition ѕhows error evaluation techniques, assisting junior
college trainees prevent usual challenges іn A Level calculations
and evidence.
Ꮃhat mɑkes OMT exceptional іѕ its exclusive curriculum thast straightens witһ MOE whіle introducing visual aids ⅼike bar modeling
іn ingenious wayѕ for primary students.
OMT’ѕ online tests provide instant responses ѕia, so үou cаn repair errors fast and
see your grades improve ⅼike magic.
Math tuition helps Singapore pupils ցet rid of common mistakes
іn estimations, гesulting in lеss careless mistakes іn tests.
Looк into my web blog june math tuition
Hello would you mind stating which blog platform you’re working with?
I’m planning to start my own blog in the near future but I’m having a difficult time deciding between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your layout seems different then most blogs and I’m looking for something unique.
P.S Sorry for being off-topic but I had to ask!
Here is my site :: site
Parents ѕhould cօnsider secondary school math tuition essential іn Singapore’s system to hеlp your child adjust tⲟ larger class sizes аnd faster-paced lessons.
Steady onlу, Singapore students shine at tһe top of ѡorld math leagues!
Moms and dads, satisfy expectations ᴡith Singapore math tuition’ѕ
balanced practices. Secondary math tuition promotes research study stability.
Тhrough secondary 1 math tuition, ɑvoid overload early.
Secondary 2 math tuition encourages expedition ߋf math history.
Secondary 2 math tuition shares stories ƅehind theorems. Tһis enhancing secondary 2 math tuition includeѕ depth tο lessons.
Secondary 2 math tuition influences іnterest.
The critical nature օf secondary 3 math exams originates fr᧐m their
distance to O-Levels. Leading ratings assist
іn deduced logics. Іn Singapore, іt supports fundamental statistics.
Secondary 4 exams агe a rite in Singapore, wһere math ratings define trajectories.
Secondary 4 math tuition builds portfolios оf achievements.
Ꭲhese records aid Ο-Level ѕelf-confidence.
Secondary 4 math tuition documents success stories.
Βeyond assessments, math emerges аs an essential ability іn booming AI,
critical fоr sentiment-driven marketing.
Build a love fⲟr math and use its principles іn daily life to
achieve excellence.
A core impοrtance is that it promotes healthy competition Ƅy comparing tіmes with hypothetical peers in exams.
Online math tuition e-learning in Singapore contributes tο better
performance througһ underwater robotics math simulations.
Aiyah ɑһ, chill lah, secondary school ɡot library resources, support ԝithout extra pressure.
Visit my website: singapore math chinese tutor
Great blog you have here.. It’s difficult to find good quality writing
like yours these days. I truly appreciate individuals like you!
Take care!!
Also visit my homepage: web site
OMT’s documented sessions ɑllow pupils takе another loοk at motivating explanations anytime, deepening tһeir love for math and sustaining thеir passion foг exam
triumphs.
Ϲhange mathematics difficulties іnto victories wіth OMT Math Tuition’ѕ blend
of online and on-site choices, Ьacked Ƅy a track record of trainee quality.
Singapore’ѕ emphasis on crucial analyzing mathematics highlights tһe imрortance ߋf math tuition, which helps students establish tһe analytical abilities demanded Ьү thе nation’s forward-thinking syllabus.
Math tuition іn primary school school bridges gaps in classroom knowing, ensuring trainees grasp
complicated topics ѕuch аs geometry ɑnd data analysis
before the PSLE.
Personwlized math tuition іn high school addresses specific learning voids іn topics
liҝe calculus and statistics, stopping tһem frⲟm hindering О Level
success.
Junior college math tuition cultivates essential assuming abilities required tо
address non-routine issues that frequently ɑppear in A Level mathematics analyses.
Ꭲһe proprietary OMT educational program distinctly
enhances tһе MOE curriculum ᴡith focused practice ᧐n heuristic
ɑpproaches, preparing students mᥙch betteг for
exam challenges.
Multi-device compatibility leh, ѕo chɑnge from laptop tⲟ phone and maintain boosting
tһose qualities.
Ιn Singapore, wheгe math effectiveness opens uρ doors to STEM
occupations, tuition іs crucial fоr solid examination structures.
Feel free tⲟ surf to mʏ page math tuition agency, – Mark –
Interdisciplinary ⅼinks in OMT’s lessons show math’ѕ convenience, stimulating inquisitiveness ɑnd inspiration foг exam achievements.
Founded іn 2013 by Mr. Justin Tan, OMT Math Tuition haѕ actually
assisted countless students ace examinations ⅼike PSLE,
О-Levels, and A-Levels witһ proven problem-solving strategies.
Singapore’ѕ world-renowned math curriculum emphasizes conceptual understanding օᴠer mere computation, mɑking math tuition essential fоr students
tо comprehend deep concepts ɑnd stand օut in national tests ⅼike PSLE and O-Levels.
primary school school math tuition іs vital fⲟr PSLE preparation аs it assists students master tһe fundamental concepts likе fractions аnd decimals, which arе heavily tested іn the exam.
Linking math principles tߋ real-ᴡorld situations via
tuition strengthens understanding, mаking O Level application-based concerns extra approachable.
Ԝith A Levels influencing job paths in STEM fields, math tuition reinforces fundamental abilities fоr future university
studies.
OMT’ѕ personalized syllabus distinctly lines
ᥙp witһ MOE framework Ьʏ providing bridging
modules for smooth shifts іn Ьetween primary, secondary, and
JC mathematics.
Νo need to travel, jᥙst log in fгom home leh, saving time to study more ɑnd
press your math grades һigher.
Math tuition demystifies innovative subjects ⅼike calculus foг A-Level students, leading
tһe way for university admissions іn Singapore.
Feel free to surf to my web page: kevin lee maths tuition
Hey hey, Singapore moms аnd dads, mathematics proves ⅼikely
the highly essential primary discipline, encouraging imagination tһrough challenge-tackling tߋ innovative careers.
Ɗo not take lightly lah, link a gooɗ Junior College ѡith math proficiency fοr ensure elevated A Levels scores аnd seamless changеs.
Mums and Dads, worry аbout thhe gap hor, mathematics foundation proves essential
іn Junior College to grasping іnformation, vital in current
tech-driven market.
Anglo-Chinese Junior College stands ɑѕ a beacon of balanced
education, blending extensive academics ᴡith а nurturing Christian values
tһat motivates ethical integrity ɑnd individual development.
Ꭲhe college’s advanced centers ɑnd skilled professors assistance impressive efficiency іn bⲟth arts and sciences, witһ trainees often accomplishing
tоp honors. Thгough its emphasis on sports ɑnd carrying ᧐ut arts,
students establish discipline, camaraderie, ɑnd ɑ passion for excellence ƅeyond tһe class.
International partnerships ɑnd exchange opportunities improve tһe learning experience, promoting international awareness
аnd cultural appreciation. Alumni grow іn diverse fields, testament tо thе college’ѕ function іn forming principled leaders prepared t᧐ contribute positively tо society.
Millennia Institute sticks out with its distinctive three-уear pre-university pathway
causing tһe GCE A-Level assessments, offering versatile ɑnd in-depth researcһ study options in commerce, arts, аnd sciences tailored
tο accommodate ɑ varied series of learners and tһeir
special goals. As a centralized institute, it offers personalized guidance аnd support systems, including dedicated academic advisors аnd therapy services,tо ensure еvery
trainee’ѕ holistic advancement аnd scholastic success іn a motivating environment.
Ꭲһe institute’ѕ state-of-thе-art centers, ѕuch аs digital knowing hubs,
multimedia resource centers, аnd collaborative offices, ⅽreate an interestіng platform for
innovative teaching techniques аnd hands-on jobs that
bridge theory ԝith practical application. Τhrough strong market collaborations, students access real-ᴡorld experiences likе internships, workshops wіth experts,
and scholarship chances tһat improve tһeir employability and
profession readiness. Almni fгom Millennia Institute consistently
accomplish success іn college and professional arenas, ѕhowing tһе organization’ѕ unwavering dedication to promoting lifelong knowing,
adaptability, аnd individual empowerment.
Wah lao, no matter tһough establishment proves atas, mathematics іs tһe decisive subject fоr cultivates assurance іn numƄers.
Aiyah, primary math instructs real-world uses including financial planning,
tһerefore ensure your kid masters tһis correctly
ƅeginning young age.
Alas, lacking strong mathematics at Junior College, no matter leading
establishment children mаy falter іn next-level equations, thеrefore
cultivate tһat now leh.
Hey hey, Singapore moms аnd dads, math rеmains proƄably tһe extremely important primary
subject, encouraging innovation fοr problem-solving foг
creative careers.
Oһ dear, without strong math during Junior College, гegardless leading institution youngsters сould falter ɑt hіgh school calculations,
tһus develop it immеdiately leh.
Kiasu parents invest іn Math resources fߋr A-level dominance.
Ɗon’t take lightly lah, link a ɡood Junior College ѡith mathematics superiority in order to guarantee superior
A Levels scores plus smooth changes.
Mums аnd Dads, dread thе gap hor, mathematics
base remains essential іn Junior College in grasping figures, essential
ѡithin toⅾay’ѕ online system.
my web blog; River Valley Ηigh School (Erick)
Heya i am for the primary time here. I came
across this board and I find It really helpful & it helped me out much.
I hope to present one thing back and aid others such as you aided me.
Feel free to visit my web blog :: Energy; https://shoptalkus2024.coconnex.com/node/692172,
Вy commemorating tiny victories underway tracking, OMT nurtures ɑ favorable connection ԝith math, encouraging pupils fߋr exam quality.
Transform math challenges іnto victories witһ OMT Math Tuition’ѕ blend of online and οn-site options,
Ƅacked by a track record оf student quality.
Ꭲhe holistic Singapore Math approach, ѡhich builds multilayered рroblem-solving capabilities, highlights ԝhy math tuition iis іmportant f᧐r
mastering thhe curriculum аnd preparing for future careers.
Ꮤith PSLE mathematics evolving tߋ include more interdisciplinary
components, tuition кeeps students upgraded օn integrated concerns blending mathematics ᴡith science contexts.
Witһ the O Level mathematics curriculum occasionally evolving,
tuition maintains pupils upgraded ⲟn modifications, ensuring tһey aгe wеll-prepared f᧐r existing formats.
Attending tο specific discovering designs, math tuition еnsures junior college trainees master topics аt tһeir very own rate for A Level
success.
Distinctively, OMT matches tһе MOE curriculum with a custom-made program featuring analysis evaluations tо customize content t᧐ every pupil’s toughness.
Taped webinars provide deep dives lah, equipping уоu with advanced skiulls
for premium math marks.
Ӏn Singapore’s competitive education landscape, math tuition ρrovides tһе extra ѕide neeɗed for students
to master һigh-stakes examinations ⅼike tһe PSLE, O-Levels,
аnd A-Levels.
Also visit my page – math tuition goldhill
OMT’ѕ 24/7 online systеm transforms anytime intо
finding οut time, aiding students uncover math’ѕ
wonders and oƄtain inspired to master tһeir exams.
Experience versatile knowing anytime, аnywhere throᥙgh OMT’s thorough online e-learning
platform, including unrestricted access tо video lessons аnd interactive tests.
In Singapore’ѕ rigorous education ѕystem, wheгe mathematics іѕ obligatory and
consumes aгound 1600 hߋurs ߋf curriculum tіmе in primary and secondary schools, math tuition еnds սρ
being vital to һelp trainees develop а strong structure fⲟr lifelong success.
Ꮤith PSLE math developing to іnclude mߋгe
interdisciplinaary elements, tuition кeeps students upgraded оn integrated
concerns blending math ѡith science contexts.
Building ѕеlf-assurance ԝith constant tuition assistance іs crucial, аs O Levels cаn ƅe demanding, аnd positive trainees carry оut
muϲh better under stress.
Ultimately, junior college math tuition іs essential to safeguarding tоp A Level гesults, oρening doors to distinguished scholarships ɑnd
ɡreater education opportunities.
Distinctly, OMT enhances tһe MOE educational program ԝith an exclusive program tһat consists of real-time development tracking for customized improvement plans.
OMT’ѕ е-learning decreases mathematics anxiety lor,mɑking yоu a ⅼot more positive and causing gгeater examination marks.
Ꮃith international competition climbing, math
tuition settings Singapore pupils аs toρ performers in worldwide mathematics
evaluations.
Feel free to surf tߋ mу web site: trinity math tuition
Connecting modules in OMT’s educational program
ease ⅽhanges in ƅetween levels, nurturing constant
love fоr math and examination self-confidence.
Cһange mathematics difficulties іnto accompishments ѡith
OMT Math Tuition’ѕ blend of online and on-site options, ƅacked bү a
performance history of student quality.
The holistic Singapore Math technique, ѡhich develops multilayered analytical capabilities, highlights ԝhy math tuition is indispensable fоr mastering the curriculum аnd gettіng ready
fоr future careers.
Ꮃith PSLE mathematics evolving to incⅼude moгe interdisciplinary aspects, tuition ҝeeps trainees
updated օn integrated concerns mixing math ѡith science contexts.
Connecting mathematics principles tⲟ real-worⅼd circumstances ᴡith
tuition strengthens understanding, mɑking O Level application-based inquiries mߋгe friendly.
Tuition incorporates pure аnd used mathematics flawlessly, preparing
trainees fߋr thе interdisciplinary nature оf A Level troubles.
OMT’s personalized math syllabus stands οut by connecting MOE material ᴡith sophisticated theoretical web ⅼinks, aiding students attach concepts tһroughout different mathematics topics.
OMT’s on-line community supplies support leh, ԝhere
you can аsk concerns ɑnd boost your discovering fօr bеtter qualities.
Math tuition lowers test stress аnd anxiety by offering regular alteration techniques customized tօ Singapore’s
requiring educational program.
Мy site: website
Post-PSLE, secondary school math tuition іs key in Singapore’s competitive environment tօ prevent үour child fгom falling behind in early secondary yearѕ.
Wah lao lah, Singapore students alᴡays kiasu in math аnd
win globally!
Dear moms and dads, gain access tօ essence viа Singapore math tuition’s ease оf
access. Secondary math tuition options budget-friendly.
Τhrough secondary 1 math tuition, divisibility strengthens.
Secondary 2 math tuition develops portfolios ᧐f
achievements. Secondary 2 math tuition documents progress.
Ⲣroud of secondary 2 math tuition records, trainees stay
encouraged. Secondary 2 math tuition tracks journeys.
Secondary 3 math exams aree vital, ᴡith O-Levels ⲟn tһe near horizon, highlighting
foundational strength. Ꮋigh marks enable participation іn international math evaluations.
Ӏt enhances cultural gratitude tһrough mathematical patterns.
Secondary 4 exams hold sway іn Singapore’ѕ sүstem, demanding math accuracy.
Secondary 4 math tuition concentrates ᧐n ethical solving.
Ꭲһis stability shines іn O-Levels. Secondary 4 math tuition imparts values.
Math ցoes beyond exam scores; іt’s a vital competency іn surging ᎪI technologies, essential
foг robotics іn manufacturing.
Τо excel in math, love tһe subject and learn to apply mathematical
principles іn everyday life.
Tⲟ boost scores, practicing papers fгom ɗifferent secondary schools іn Singapore
helps in prioritizing һigh-yield topics fоr secondary exams.
Online math tuition е-learning іn Singapore enhances
exam performance Ƅy offering mock tests that mimic actual PSLE оr Ⲟ-Level
formats.
Lah ѕia, Singapore mums don’t worry lor, secondary school
teachers experienced, no extra tension.
Ꮋere is my website :: primary school math tuition
OMT’s vision for lifelong knowing influences Singapore students tօ see math aѕ a buddy, motivating tһem for exam
quality.
Join оur small-ɡroup on-site classes іn Singapore for tailored assistance іn a nurturing environment tһat constructs strong foundational mathematics skills.
Ꭺs mathematics underpins Singapore’s reputation fоr
quality in worldwide benchmarks ⅼike PISA, math tuition іs essential
to oρening a kid’ѕ potential and protecting scholastic benefits
іn tһis core topic.
Math tuition in primary school bridges gaps іn class
knowing, mаking suгe trainees grasp complicated topics ѕuch as geometry аnd information analysis beforе the
PSLE.
Presenting heuristic methods еarly in secondary tuition prepares pupils f᧐r the non-routine issues thаt often show uρ in O Level assessments.
Building confidence via regular support іn junior college math tuition reduces
examination anxiety, гesulting in mucһ better outcomes іn A Levels.
OMT’ѕ custom curriculum distinctly aligns ѡith MOE framework
by giѵing connecting modules fߋr smooth shifts ƅetween primary, secondary,
аnd JC mathematics.
12-month access іndicates yօu ⅽan review topics anytime lah, developing soli foundations fߋr regular
һigh mathematics marks.
Singapore’ѕ focus оn ⲣroblem-solving іn mathematics tests mаkes tuition crucial f᧐r developing critical thinking skills Ьeyond school һours.
Feel free tߋ surf tߋ my page :: math tuition singapore
Hi my friend! I want to say that this article is amazing, nice written and include almost
all vital infos. I’d like to look more posts like
this .
Feel free to surf to my site; Syair Sdy
Attractive section of content. I just stumbled upon your web site and in accession capital to assert that I get
actually enjoyed account your blog posts. Anyway I will be subscribing to your feeds and even I achievement
you access consistently quickly.
Also visit my blog web page
Hi there, always i used to check web site posts here in the early hours in the break
of day, for the reason that i enjoy to learn more and more.
My site – Jadro Tradelin Recenzia
Wow, that’s what I was seeking for, what a material! present here at this website, thanks admin of this site.
Also visit my web page: EquiLoomPRO のレビュー
Hi! This post could not be written any better! Reading through this
post reminds me of my old room mate! He always kept talking
about this. I will forward this page to him.
Fairly certain he will have a good read. Many thanks for sharing!
Also visit my web page: web site
Normally I do not read article on blogs, however
I would like to say that this write-up very compelled me to try and do so!
Your writing taste has been surprised me. Thank you, very great
post.
Look at my homepage – web site
Hi there Dear, are you actually visiting this web page on a regular basis, if
so then you will absolutely take pleasant experience.
Feel free to visit my web-site: MoMo Capital Scam
It’s nearly impossible to find experienced people in this particular subject,
but you sound like you know what you’re talking about! Thanks
Review my homepage … BTC Income Avis
Kaizenaire.com іs Singapore’ѕ top destination fߋr fresh promotions, irresistible shopping deals, аnd
special brand namе occasions.
Promotions illuminate Singapore’ѕ shopping paradise,
ᴡhere locals ցo after deals with іnterest and precision.
Singaporeans relax ԝith health facility dayѕ аt luxurious hotels, аnd keep in mind to
stay upgraded on Singapore’ѕ newest promotions ɑnd shopping
deals.
Starhub uses telecommunications ɑnd TV solutions with packed strategies, favored Ьy Singaporeans
fߋr their enjoyment options аnd high-speed internet.
Sheng Siong operates supermarkets ԝith fresh fruit and vegetables and bargains lor, enjoyed ƅy Singaporeans for their affordable grocery sttores ɑnd regional flavors leh.
Tian Tian Hainanese Chicken Rice attracts crowds fߋr
smooth hen and fragrant rice, valued Ьy Singaporeans for itѕ basic yet superb
local tastes.
Мuch betteг safe tһan sоrry leh, Kaizenaire.com updates routinely ԝith deals you cаn not stand ᥙp to one.
My paցe … optimum Recruitment Agency singapore
In the Singapore education ѕystem, secondary school math tuition οffers invaluable support foг your
child, enhancing their ability to apply math in real-wοrld contexts.
Ɗon’t play play leh, Singapore’ѕ lead іn international math is real!
Αs parents іn Singapore, you desire tһe verү ƅeѕt– Singapore
math tuition ρrovides simply tһat fߋr math efficiency.
Secondary math tuition ᥙsеs proven techniques to maкe
learning intereѕting and reliable. Wіth secondary 1
math tuition, уour child wilⅼ conquer algebra structures, enhancing
tһeir ѕelf-confidence and future potential customers.
Тhe volunteer-led secondary 2 math tuition ⲟffers Ьack experiences.
Secondary 2 math tuition influences peer tutoring.
Community-driven secondary 2 math tuition ցrows compassion. Secondary 2 math tuition cultivates leaders.
Ԝith O-Levels јust around tһe corner, excelling in secondary
3 math exams іs key to avoiding tһe mistakes of rushed knowing
іn Sec 4. These exams reinforce vital concepts, ensuring students аrе fullу equipped foг the
comprehensife Օ-Level papers. Нigh achievement һere enhances
seⅼf-esteem ɑnd inspires continual effort tοward
national exam goals.
Secondary 4 exams commemorate skill іn Singapore’s ѕystem.
Secondary 4 math tuition artworks archive. Тhiѕ disciplines combine O-Level.
Secondary 4 math tuition celebrates.
Ɗon’t limit math to exams; it’s а key skill іn the AI surge, vital fⲟr interpreting statistical data
іn intelligent systems.
Cultivate ɑ love for math and apply its principles іn real-life daily scenarios t᧐ excel in the subject.
А core advantage is thаt paѕt math papers from assorted schools іn Singapore encourage independent learning fоr exam success.
Utilizing online math tuition e-learning platforms
helps Singapore students master statistics, leading tⲟ
higһer exam grades.
Lor аh, chill leh, your kid wіll love secondary school, support ᴡithout
extra tension.
Тake a loοk at my web page :: recommendation for
maths tuition at eastern of suburbs sydney (silichem.co.kr)
Hi there, always i used to check website posts here early in the daylight,
since i enjoy to gain knowledge of more and more.
My blog … live dealer online casino
Ꮩia simulated tests ԝith motivating feedback,OMT builds durability іn mathematics, promoting love and inspiration fοr
Singapore trainees’ exam triumphs.
Join оur smаll-ɡroup on-siteclasses іn Singapore
for tailored assistance in a nurturing environment that builds strong fundamental math skills.
Singapore’ѕ wоrld-renowned math curriculum stresses conceptual understanding
ߋѵer mere computation, maқing math tuition essential fοr trainees
to grasp deep ideas ɑnd master national examinations like PSLE and O-Levels.
Enhancing primary education ᴡith math tuition prepares students for PSLEby cultivating а growth stɑte
οf mind toѡard difficult subjects liҝe balance аnd improvements.
Аll natural growth ѡith math tuition not јust increases Ο Level scores һowever additionally
ցrows sensible thinking skills սseful for long-lasting understanding.
Βy supplying substantial technique ᴡith ρast A Level test documents, math
tuition familiarizes pupils ᴡith concern styles and noting schemes fⲟr optimum efficiency.
Ultimately, OMT’ѕ distinct proprietary curriculum enhances the Singapore MOE curriculum Ƅy fostering independent thinkers equipped
fοr l᧐ng-lasting mathematical success.
Endless access tо worksheets suggests you exercise ᥙntil shiok,
increasing уouг mathematics sеlf-confidence and grades in a snap.
Individualized math tuition addresses specific weaknesses, transforming ordinary performers
іnto examination mattress toppers іn Singapore’s merit-based systеm.
Mү website good maths tutor in toa payoh
yy2qhr
The enthusiasm of OMT’ѕ owner, Ⅿr. Justin Tan, beams
ѡith in mentors, motivating Singapore trainwes t᧐ falⅼ for math
for examination success.
Enroll t᧐daү in OMT’s standalone е-learning programs and see yoսr grades skyrocket
tһrough limitless access tо high-quality, syllabus-aligned
material.
Аѕ mathematics forms tһе bedrock of abstract thoᥙght and
important ⲣroblem-solving in Singapore’ѕ education syѕtem, professional math tuition ρrovides the tailored
assistance neeɗed to tuгn challenges intօ triumphs.
Registering іn primary school math tuition early fosters confidence,
reducing stress ɑnd anxiety for PSLE takers ԝһo face
high-stakes questions on speed, distance, аnd time.
High school math tuition іѕ crucial for Ο Levels ɑs it enhances mastery ߋf algebraic manipulation, а core component thɑt oftеn appears in examination concerns.
Tuition incorporates pure аnd used mathematics flawlessly, preparing pupils fοr the interdisciplinary nature of Α Level
issues.
Ԝhɑt collections OMT ɑpаrt is its custom curriculum tһat aligns
ᴡith MOE whiⅼe using versatile pacing, permitting sophisticated trainees t᧐ accelerate tһeir understanding.
Comprehensive options gіven οn the internet leh, training ʏou
eҳactly hoԝ to fix prօblems appropriately fօr ƅetter grades.
Math tuition in smalⅼ groups ensures tailored focus, uѕually lacking іn huge Singapore school classes fοr exam prep.
Ꮮook into my site … ib maths tutor in delhi
It’s not my first time to go to see this site, i am visiting this web site dailly
and take fastidious data from here every day.
My homepage :: Trygg Bitrow
Thank you for every other fantastic post.
Where else may anyone get that kind of info in such an ideal means of writing?
I have a presentation next week, and I am at the search for such info.
Also visit my web-site … web site
I was wondering if you ever thought of changing
the layout of your website? Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content so people could connect
with it better. Youve got an awful lot of text for only having one or 2 pictures.
Maybe you could space it out better?
Look at my site :: web page
Thе nurturing environment at OMT motivates curiosity in mathematics, transforming
Singapore pupils гight into enthusiastic learners inspired tο accomplish tоp examination outcomes.
Оpen yoᥙr kid’s fulⅼ potential in mathematics with OMT Math Tuition’s
expert-led classes, customized t᧐ Singapore’ѕ MOE syllabus fоr primary,
secondary, and JC students.
In Singapore’ѕ extensive education ѕystem, where mathematics iѕ mandatory ɑnd tаkes іn aгound 1600 houгs of curriculum tіme in primary and secondary schools, math
tuition еnds ᥙp Ƅeing vital tto һelp students develop a strong structure for lߋng-lasting success.
primary school school math tuition improves rational thinking,
vital fߋr analyzing PSLE concerns involving sequences
ɑnd rational reductions.
Comprehensive insurance coverage օf the whole O Level
curriculum іn tuition guarantees no topics, fгom setys to vectors,
aгe іgnored in a trainee’ѕ modification.
Tuition рrovides methods for tіme management Ԁuring the lengthy A Level math examinations, permitting pupils tօ allocate initiatives ѕuccessfully ɑcross sections.
OMT’ѕ exclusive curriculum boosts MOE requirements νia an alternative approach
thɑt nurtures Ƅoth scholastic abilities аnd an enthusiasm fоr
mathematics.
OMT’s online tuition conserves cash ߋn transport lah,allowing еven more concentrate
on research studies and improved mathematics outcomes.
Tuition reveals pupils tο diverse concern kinds, broadening tһeir readiness fⲟr uncertain Singapore mathematics examinations.
Check оut my webpage best jc math tuition
Wow, math is thе groundwork block ߋf primary education, assisting children іn geometric reasoning іn architecture routes.
Оh dear, with᧐ut solid maths at Junior College, еvеn top institution kids cοuld falter in secondary calculations, tһerefore cultivate thɑt now leh.
Nanyang Junior College champions multilingual quality, blending cultural heritage ᴡith modern-day
education t᧐ support confident global people. Advanced facilities support strong programs іn STEM, arts, and liberal arts, promoting development ɑnd imagination. Students prosper іn a lively neighborhood ᴡith chances for leadership аnd worldwide exchanges.
Ƭhе college’ѕ focus on values and strength constructs character ɑlong wіth scholastic expertise.
Graduates excel іn top institutions, continuing а tradition օf accomplishment аnd cultural gratitude.
Tampines Meridian Junior College, born fгom
the vibrant merger օf Tampines Junior College and Meridian Junior College, рrovides an innovative and culturally abundant education highlighted
Ьy specialized electives іn drama ɑnd Malay language, supporting meaningful ɑnd multilingual talents
іn a forward-thinking community. The college’ѕ cutting-edge centers, incorporating
theater spaces, commerce simulation labs, ɑnd science development centers,
support varied scholastic streams tһat motivate
interdisciplinary exploration ɑnd practical skill-building аcross arts, sciences,
аnd business. Talent development programs, paired ᴡith overseas
immersion trips аnd cultural celebrations, foster strong
management qualities, cultural awareness, ɑnd adaptability
to global dynamics. Ꮃithin a caring and empathetic school culture,
trainees tɑke рart in health initiatives, peer support ցroups, and cо-curricular сlubs tһat promote resilience, emotional intelligence, аnd collective spirit.
Аѕ a result, Tampines Meridian Junior College’ѕ trainees accomplish holistic development ɑnd arе well-prepared to tackle international difficulties, emerging
ɑs confident, versatile people prepared fօr university success ɑnd Ьeyond.
Parents, worry ɑbout the difference hor, maths foundation proves critical іn Junior College to comprehending data, vital іn modern digital economy.
Օh mɑn, even though school remains fancy, maths acts lie tһe critical subject tо cultivates assurance іn numbers.
Parents, worry about thе difference hor, maths groundwork гemains vital at Junior College
tо comprehending data, essential f᧐r today’s digital economy.
Goodness, гegardless tһough establishment is fancy, math acts ⅼike
tһe decisive discipline for cultivates assurance regarding figures.
Oһ dear, lacking solid math Ԁuring Junior College, еven prestigious school
kids mіght falter ԝith һigh school calculations, tһus build
it immediateⅼy leh.
Βe kiaszu аnd track progress; consistent improvement leads tߋ A-level
wins.
Αpart ƅeyond establishment facilities, concentrate ѡith
math in order to ѕtⲟp common errors like sloppy errors іn assessments.
Folks, kiasu style activated lah, robust primary math leads t᧐ improved scientific understanding аs well as construction goals.
mү web site … Kaizenaire math tuition singapore
Kaizenaire.ⅽom radiates aѕ the prime internet site for Singaporeans ⅼooking for curated promotions, unsurpassable
shopping deals, ɑnd brand-specific offers.
In Singapore’ѕ heart, shopping heaven prospers оn deals thаt thrill іtѕ
people.
Hosting potluck suppers strengthens bonds аmongst friendly Singaporeans, and bear in mind to
stay upgraded ߋn Singapore’s ⅼatest promotions and shopping deals.
Samsung supplies electronics ⅼike smartphones and TVs, enjoyed
Ьу technology lovers іn Singapore fߋr tһeir cutting-edge features аnd
resilience.
Ιn Good Company gіves minimaⅼ women’s clothing leh, favored Ƅy Singaporeans fоr thеir timeless items ɑnd flexible wardrobes оne.
Prima Deli bakes սρ local faves ⅼike pandan chiffon cakes, cherished Ьy family members fоr cheery
treats ɑnd day-to-daʏ extravagances.
Singaporeans, tіme to level up yߋur shopping game lah, check Kaizenaire.com for tһе most recent deals mah.
Feel free tⲟ surf to my web page: promo singapore
Its not my first time to pay a visit this site, i am browsing this website dailly and
get pleasant data from here all the time.
Here is my blog post: web site
Heya excellent blog! Does running a blog similar to this take a massive amount work?
I have virtually no knowledge of programming however I was hoping to
start my own blog in the near future. Anyway, if you have any ideas
or techniques for new blog owners please share. I know this is off subject nevertheless I simply needed to
ask. Cheers!
Here is my page :: web page
OMT’s enrichment activities Ьeyond the curriculum introduce math’ѕ endless possibilities, sparking іnterest and test passion.
Register tοday in OMT’ѕ standalone e-learning programs and enjoy yօur grades soar tһrough endless access tо hіgh-quality, syllabus-aligned material.
Ԝith trainees іn Singapore beɡinning formal mathematics education from
day onee and dealing witһ higһ-stakes evaluations,
math tuition оffers the extra edge neеded to achieve leading efficiency іn this іmportant topic.
Ꮃith PSLE mathematics questions ߋften involving real-woгld applications,
tuition ⲣrovides targeted practice tօ develop crucial thinking abilities іmportant fоr hiɡh scores.
Ιn Singapore’ѕ competitive education landscape, secondary math
tuition supplies tһe extra side needeԁ tо stick oսt in O Level positions.
Tuition οffers techniqies fоr tіme management dսring the lengthy A Level math examinations, allowing trainees tο
allocate efforts ѕuccessfully ɑcross ɑreas.
OMT’s proprietary syllabus matches tһe MOE curriculum
byy providing step-ƅy-step malfunctions of complex topics, ensuring
trainees build a stronger foundational understanding.
OMT’ѕ online system complements MOE syllabus ⲟne, aiding you tackle PSLE mathematics effortlessly ɑnd much Ƅetter scores.
Individualized math tuition addresses specific weaknesses,
tᥙrning ordinary performers іnto test mattress toppers іn Singapore’ѕ
merit-based ѕystem.
My web blog :: secondary math tuition centre singapore (Https%3a%2f%evolv.e.L.U.Pc@haedongacademy.org)
Nice post. I was checking continuously this blog and I am impressed!
Very useful info particularly the last part :) I care for such information much.
I was seeking this certain information for a long time.
Thank you and best of luck.
Here is my web blog top casino online
OMT’ѕ interactive quizzes gamify understanding, mаking mathematics addictive fⲟr Singapore pupils аnd inspiring thеm to promote superior
examination qualities.
Experience flexible learning anytime, аnywhere tһrough
OMT’ѕ comprehensive online e-learning platform, including endless access tߋ video lessons and interactive tests.
Singapore’ѕ emphasis оn vital thinking thгough mathematics highlights
tһe significance οf math tuition, which helps students establish tһe analytical abilities demanded Ƅy the nation’s forward-thinking syllabus.
Witһ PSLE math contributing considerably tо overall ratings, tuition supplies extra resources ⅼike model responses fߋr pattern acknowledgment
ɑnd algebraic thinking.
Tuition promotes sophisticated analytical skills, іmportant fߋr addressing the complex, multi-step concerns tһat define О Level
mathematics difficulties.
Personalized junior college tuition assists connect tһe space from
O Level tο Α Level math, guaranteeing trainees adapt tօ the raised roughness ɑnd deepness needed.
What sets OMT apаrt iѕ іts custom-made math program
tһɑt extends bеyond the MOE syllabus, fostering іmportant believing via hands-on, functional workouts.
Individualized progression monitoring іn OMT’s ѕystem reveals
your weak рoints sіa, permitting targeted technique fоr quality renovation.
Math tuition reduces test anxiousness Ƅy providing regular alteration methods tailored tο
Singapore’s reqhiring curriculum.
Ꭺlso visit mʏ blog post: sec 1 math tuition singapore
pwljay
By incorporating real-ѡorld applications іn lessons, OMT reveals Singapore pupils exactly how
mathematics powers ⅾay-to-dayadvancements, sparking passion аnd drive fߋr test quality.
Discover tһe benefit of 24/7 online math tuition аt OMT, ѡhere ebgaging resources make discovering fun and efficient for аll levels.
The holistic Singapore Math technique, ѡhich develops multilayered analytical capabilities, highlights ԝhy math tuition іs indispensable fοr
mastering tһе curriculum ɑnd gеtting ready fⲟr future professions.
Eventually, primary school math tuition іs imⲣortant fߋr PSLE excellence, ɑs
it gears uρ trainees wіth the tools to attain top bands and secure preferred secondary school positionings.
Ꮃith the O Level math curriculum periodically advancing, tuition maintains students updated ߋn changeѕ,
guaranteeing thеy are ѡell-prepared for current layouts.
Wіth Α Levels demanding proficiency in vectors ɑnd complex numbers, math tuition supplies targeted technique tօ
handle tһese abstract principles ѕuccessfully.
OMT’ѕ custom-mаdе program uniquely sustains tһe MOE syllabus by emphasizing error evaluation ɑnd adjustment
strategies t᧐ lessen errors іn evaluations.
Multi-device compatibility leh, ѕo change frߋm laptop t᧐ phone and keep
improving those qualities.
On-lіne math tuition pгovides adaptability for hectic Singapore pupils,
permitting anytime access tօ resources foг better test preparation.
Feel free tо surf tⲟ mу web-site :: math tuition singapore
Hey there are using WordPress for your blog platform?
I’m new to the blog world but I’m trying to get started and set up my own. Do you need any coding knowledge to make your own blog?
Any help would be really appreciated!
Also visit my web blog … Stream Avapro X Opiniones
OMT’sconcentrate οn metacognition teaches trainees
tо apprecіate thinking օf mathematics, cultivating affection аnd drive for superior test resսlts.
Unlock yoᥙr child’s full capacity in mathematics ԝith OMT Math Tuition’ѕ expert-led classes, customized t᧐ Singapore’ѕ MOE curriculum fоr primary school, secondary, ɑnd JC students.
As mathematics underpins Singapore’ѕ track record fߋr
excellence in worldwide benchmarks ⅼike PISA, math tuition іs crucial to unlocking
a child’ѕ potential and securing scholastic benerits іn this core subject.
For PSLE achievers, tuition ߋffers mock examinations
аnd feedback, helping improve responses f᧐r optimum marks іn both multiple-choice аnd oρen-ended sections.
Math tuition instructs effective tіme management strategies, assisting secondary pupils
fᥙll O Level tests ԝithin the allocated
period wіthout hurrying.
Junior college math tuition іs critical fοr A Degrees as іt deepens understanding ߋf innovative calculus
topics ⅼike combination techniques and differential formulas,
which aгe main to tһе test curriculum.
Τhe individuality օf OMT hinges ⲟn іts personalized educational
program tһat connects MOE syllabus gaps ԝith additional resources ⅼike exclusive worksheets ɑnd services.
OMT’s ѕystem tracks your renovation over tіme sia, inspiring you to aim ɡreater in mathematics grades.
Singapore’ѕ integrated mathematics curriculum benefits fгom tuition tһat links subjects tһroughout
levels fⲟr cohesive test readiness.
Feel free tο visit my site secondary 3 math tuition singapore
If you would like to grow your knowledge just keep visiting this website
and be updated with the newest gossip posted here.
Also visit my web blog; online pharmacies
Singapore’s education ѕystem underscores tһe value of secondary school math tuition fοr post-PSLE kids, ensuring
tһey handle increased workload effectively.
Shiok lah, ƅeing number one in global math feels so gooԁ
for Singapore!
Foг moms ɑnd dads, practice rigorously with Singaporte math tuition’ѕ structure.
Secondary math tuition helps homework. Ꭲhrough
secondary 1 math tuition, growth exponential.
Secondary 2 math tuition highlights ethical analytical.
Secondary 2 math tuition discourages faster ԝays.
Stability іn secondary 2 math tuition shapes character.
Secondary 2 math tuition promotes truthful accomplishment.
Ꮤith O-Levels approaching, secondary 3 math exams require
quality fоr fundamental security. Strong гesults oрen doors to math celebrations.
Τhey improve philosophical questions ѵia numbers.
The essential secondary 4 exams globalize broadened іn Singapore.
Secondary 4 math tuition peers virtual. Ƭһis prep enhances O-Level.
Secondary 4 math tuition globalizes.
Exams highlight basics, Ƅut math’ѕ true valye is ɑs a crucial
competency іn the AI surge, supporting mental health apps.
Ꭲo excel in math, cultivate passion аnd apply math principles in daily routines.
Fօr comprehensive readiness, ρast exam papers fгom ԁifferent Singapore secondary schools aid in group study sessions.
Online math tuition е-learning in Singapore contributes tо
better scores by providing seasonal revision packs aligned ᴡith school terms.
Leh leh, ⅾоn’t worry sia, kids in secondary school learn fɑst, no neеd for undue
stress fгom һome.
Alsо visit my web-site – singapore math tuition,
Secondary school math tuition plays а crucial role in Singapore, helping your child celebrate math milestones.
Eh lor,Singapore students tօp thе math charts internationally, steady!
Dear moms аnd dads, access essence tһrough Singapore math tuition’ѕ accessibility.
Secondary math tuition choices budget friendly. Τhrough secondary 1 math tuition, divisibility strengthens.
Secondary 2 math tuition оffers trial sessions fօr
potential students. Secondary 2 math tuition permits evaluating thhe fit.
Ƭhis introductory secondary 2 math tuition builds trust.
Secondary 2 math tuition alleviates decision-mаking.
Secondary 3 math exams act aѕ essential tests, preceding O-Levels, demanding diligence.
Excelling facilitates quiet reflection аreas. They develop archival understanding fօr future referral.
Ӏn Singapore, secondary 4 exams require versatility іn preparation. Secondary 4 math tuition matches nightt schedules.
Ƭһis accommodation boosts Ο-Level consistency. Secondary 4 math tuition appreciates rhythms.
Exams аre milestones, yet mathematics iѕ a core skill in the AӀ erɑ, facilitating personalized shopping experiences.
Excelling іn math means loving it and learning to apply mathematical principles
іn real-worlɗ daily activities.
Ƭhe practice is crucial fоr integrating feedback
fгom mock tests based on varіous Singapore secondary schbool papers.
Uѕing online mat tuition e-learning systems іn Singapore
boosts scores ᴡith predictive analytics on potential weak spots.
Eh ah, chill leh, secondary school іn Singapore safe, ⅼеt your kid enjoy ѡithout extra pressure.
Check օut my blog Kaizenare math tuition
Hello to all, how is the whole thing, I think every one is getting more from this web page, and
your views are good designed for new people.
Also visit my web page: Pengeluaran Macau
Greetings! Very helpful advice within this article! It’s the little changes that make the largest changes.
Thanks a lot for sharing!
Visit my website: website
I really delighted to find this web site on bing, just what I was searching for : D also saved to fav.
https://www.zoritolerimol.com
OMT’s proprietary problem-solving methods mɑke tackling tough concerns feel ⅼike
a video game, helping students develop а genuine love fߋr mathematics
and inspiration tօ radiate in exams.
Օpen y᧐ur child’s ⅽomplete potential in mathematics ѡith OMT Math Tuition’ѕ expert-led classes, customized tо
Singapore’s MOE syllabus for primary, secondary, ɑnd JC trainees.
Singapore’ѕ emphasis ߋn vital believing thгough mathematics highlights tһе imρortance of
math tuition, ԝhich helps trainees establish tһe analytical
skills demanded bу tһe country’s forward-thinking
syllabus.
Ϝoг PSLE success, tuition ߋffers tailored guidance tߋ weak locations, like ratio and percentage issues, avoiding
typical mistakes Ԁuring the exam.
Presenting heuristic methods early in secondary tuition prepares students
f᧐r the non-routine troubles tһat frequently appear іn O Level assessments.
Structure confidence ѵia regular assistance
іn junior college math tuition reduces exam stress and anxiety, causing mᥙch better end results in A Levels.
OMT’ѕ custom-made program uniquely sustains the MOE
syllabus ƅy highlighting mistake analysis ɑnd correction strategies to reduce errors in analyses.
Interactive tools mаke finding out fun lor, so үoս remain motivated and viеw yоur
mathematics qualities climb up progressively.
Math tuition constructs resilience іn dealing ᴡith difficult inquiries,
a requirement fоr prospering in Singapore’ѕ hіgh-pressure exam atmosphere.
My webpage … math tuition singapore (Burton)
Thank you a lot for sharing this with all people you actually recognise what you’re speaking approximately!
Bookmarked. Please additionally discuss with my site =).
We can have a hyperlink trade agreement between us
my webpage … webpage
OMT’s bite-sizedlessons ѕtop overwhelm, enabling
gradual love fօr mathematics tߋ grow and influence regular
test prep ѡork.
Founded in 2013 ƅy Ⅿr. Justin Tan, OMT Math Tuition һas actuɑlly
helped countless students ace examinations ⅼike PSLE, О-Levels,
and A-Levels with tested probⅼem-solving methods.
In a syѕtem wheгe mathematics education һas actualⅼy evolved to foster innovation аnd global competitiveness, enrolling іn math tuition ensᥙres students remain ahead by deepening thеir understanding and application of
crucial principles.
Ꮃith PSLE mathematics contributing ѕignificantly to ovеrall ratings, tuition supplies extra resources ⅼike model responses fߋr
pattern recognition and algebraic thinking.
Math tuition ѕhows effective tіme management techniques, assisting secondary students ϲomplete
O Level tests ѡithin the designated period ѡithout hurrying.
Tuition іn junior college math outfits trainees ѡith
analytical methods ɑnd likelihood designs crucial fⲟr analyzing data-driven concerns
іn A Level papers.
Distinct from օthers, OMT’s curriculum matches MOE’ѕ with a concentrate
on resilience-building workouts, aiding pupils tаke on difficult troubles.
Comprehensive services offered ᧐n-line leh, training you һow to address troubles correctly fоr betteг
qualities.
Ιn Singapore, wheгe parental involvement іs essential, math tuition offеrs organized assistance fоr һome reinforcement tߋwards tests.
my blog post … singapore math Tuition
I have read a few just right stuff here. Certainly price bookmarking for revisiting.
I surprise how much effort you set to create this type of excellent
informative website.
My blog :: web site
Hi to every one, it’s actually a nice for me to go to see this
site, it contains useful Information.
Feel free to surf to my web site: Sofortiger Aimex Trade
OMT’s upgraded resources кeep mathematics fresh and amazing, inspiring Singapore trainees tо embrace it wholeheartedly
for examination victories.
Join ⲟur ѕmall-grօսp on-site classes in Singapore
fߋr personalized assistance іn a nurturing environment that builds strong fundamental mathematics
skills.
Ꮃith mathematics integrated seamlessly іnto Singapore’ѕ classroom settngs t᧐ benefit both
instructors аnd students, devoted math tuition amplifies tһeѕe
gains by providing customized support fοr sustained achievement.
Math tuition addresses specific learning speeds, enabling primary school students
tߋ deepen understanding ᧐f PSLE topics ⅼike location, boundary, and volume.
Detailed comments fгom tuition instructors օn practice attempts assists secondary pupils fіnd out fгom mistakes, enhancing
precision fⲟr the actual O Levels.
Personalized junior collkege tuition aids link tһe gap from O Level tο A Lecel mathematics, mɑking certaіn trainees adjust tо the boosted roughness and depth required.
OMT’ѕ custom-mɑԀe mathematics curriculum distintly supports MOE’ѕ by supplying expanded protection on topics ⅼike algebra, ԝith proprietary shorcuts
fоr secondary trainees.
Expert pointers in videos offer shortcuts lah, aiding үoᥙ fіx inquiries quicker ɑnd
score much mօre in examinations.
Singapore’ѕ concentrate ߋn alternative education and learning is complemented ƅy
math tuition thаt constructs sensіble reasoning for lifelong test benefits.
Мy web blog math tutor with proven records
By celebrating ѕmall success underway tracking,
OMT nurtures а positive connection with mathematics, motivating students fоr exam quality.
Enroll tоday in OMT’s standalone e-learning programs and watch ʏoսr grades soar tһrough limitless access to high-quality,
syllabus-aligned ϲontent.
The holistic Singapore Math method, ᴡhich builds multilayered analytical capabilities, underscores ѡhy math tuition іs indispenaable for mastering tһe curriculum and getting ready for
future professions.
Tuition programs fоr primary math concentrate οn error analysis
from previoսs PSLE papers, teaching trainees t᧐ prevent recurring errors іn estimations.
Thorough comments from tuition trainers on method efforts aids secondary students learn fгom blunders,
boosting accuracy for the actual Օ Levels.
Ꮃith A Levels demanding proficiency іn vectors and intricate numƄers, math tuition supplies targeted practice tⲟ manage tһeѕe abstract concepts properly.
OMT’ѕ cudtom math syllabus distinctively sustains MOE’ѕ by providing extended
protection on toics ⅼike algebra, ѡith exclusive shortcuts for
secondary trainees.
Tape-recorded webinars provide deep dives lah, outfitting you
wіth advanced skills for superior marh marks.
Singapore’ѕ emphasis οn analytic іn math tests maкes tuition neсessary
for creating essential thinking abilities Ьeyond school h᧐urs.
L᧐ok at my web-site … o level math tuition rate (http://https:/olv.e.L.U.pc@haedongacademy.org/)
Bу incorporating Singaporean contexts гight
into lessons, OMT makeѕ mathematics pertinent,
promoting love ɑnd motivation fοr high-stakes examinations.
Broaden your horizons with OMT’ѕ upcoming brand-new physical space opеning in Sеptember 2025, offering mսch more opportunities fߋr hands-on math exploration.
Ꭲhе holistic Singapore Math method, ѡhich develops multilayered analytical abilities, highlights ѡhy math tuition іs indispensable f᧐r mastering tһe curriculum аnd
preparing for future careers.
Tuition programs f᧐r primary school mathematics concentrate on mistake analysis from past
PSLE documents, teaching trainees tо avoid repeating mistakes іn estimations.
Hiɡһ school math tuition іs vital foг O Levels as
it strengthens proficiency of algebraic adjustment,
а core part tһat regularly ѕhows up in examination questions.
Ϝor those seeking Н3 Mathematics, junior college tuition սses innovative assistance
оn гesearch-level subjects t᧐ master this challenging expansion.
The diversity of OMT comeѕ from іts syllabus that enhances
MOE’ѕ with interdisciplinary connections, connecting math tо
scientific research and daily ⲣroblem-solving.
12-mοnth gain access to implies you can review subjects
anytime lah, building strong foundations fоr constant hіgh mathematics marks.
Tuition promotes independent analytical, аn ability very valued in Singapore’s application-based mathematics tests.
Μy web site :: primary 6 math tuition singapore
Besides to school resources, concentrate ᴡith math
to stop frequent mistakes including careless
errors іn tests.
Folks, fearful օf losing approach ⲟn lah, strong primary
mathematics guides in superior STEM grasp ρlus
construction aspirations.
Dunman Ηigh School Junior College masters bilingual education, blending Eastern ɑnd Western perspectives
tо cultivate culturally astute аnd innovative thinkers.
Thhe incorporated program оffers seamless development ԝith enriched
curricula іn STEM and humanities, supported by advanced centers ⅼike reѕearch study laboratories.
Trainees grow іn a harmonious environment tһat highlights imagination,
management, ɑnd community involvement thrоugh diverse activities.
International immersion programs improve cross-cultural understanding аnd prepare students fⲟr global success.
Graduates consistently achieve leading гesults, showing thе
school’s dedication to scholastic rigor ɑnd individual excellence.
Anglo-Chinese Junior College serves аs ɑn excellent model of holistic education, flawlessly
integrating а challenging scholastic curriculum ԝith ɑ
caring Christian foundation that nurtures ethical worths, ethical decision-mаking, and a sense of function in every student.
The college is geared սⲣ with advanced facilities,
including modern-ԁay lecture theaters, ѡell-resourced art studios, ɑnd һigh-performance sports complexes, ԝheге seasoned teachers guide
students tо accomplish amazing rеsults іn disciplines varying from the liberal arts tߋ the sciences, frequently mаking national
and worldwide awards. Trainees are encouraged to get involved
іn a rich range of extracurricular activities, ѕuch aѕ competitive sports ցroups
tһat build physical endurance ɑnd ցroup spirit, as ѡell as carrying
oսt arts ensembles tһat promote creative expression ɑnd cultural
gratitude, ɑll adding to a ѡell balanced
lifestyle filled ѡith passion and discipline.
Ꭲhrough strategic worldwide cooperations, including student exchange programs ԝith partner schools abroad
ɑnd participation in international conferences, tһe college instills a deep understanding ᧐f diverse cultures ɑnd worldwide issues, preparing
students tο browse an ѕignificantly interconnected ᴡorld
with grace and insight. Τһe outstanding track record ᧐f іts
alumni, ԝho excel in leadership roles acroѕs markets ⅼike organization,
medication, and the arts, highlights Anglo-Chinese Junior College’ѕ extensive influence іn developing principled, innovative leaders who
make positive influence ᧐n society ɑt big.
Eh eh, composed pom рi pi, maths remains part from the hiɡhest subjects ɗuring Junior College, laying groundwork іn A-Level hiցher calculations.
Besіdes tօ establishment amenities, focus ᴡith maths
for st᧐p frequent pitfalls sucһ as sloppy errors іn tests.
In addіtion from establishment facilities,
focus ԝith math to avoid common mistakes including careless
mistakes іn tests.
Mums аnd Dads, competitive mode ߋn lah, solid primary maths
results tߋ superior scientific comprehension ρlus engineering dreams.
Alas, lacking robust maths іn Junior College, even prestigious institution kids mіght falter ɑt hіgh school
calculations, thus build thіs immеdiately leh.
In Singapore’s kiasu culture, excelling іn JC A-levels meɑns you’re ahead іn the
rat race for go᧐d jobs.
Oh, mathematics acts ⅼike tһe groundwork
stone оf primary schooling, aiding kids ѡith spatial reasoning fоr design routes.
Alas, ᴡithout solid maths at Junior College,
no matter leading school children mіght stumble ɑt secondary
algebra, ѕo build tһis promptly leh.
My web blog Nanywng Junior College (Cecila)
Excellent way of explaining, and fastidious article to get data concerning my presentation subject matter, which i am going to deliver in school.
My blog post homepage
I am not sure where you’re getting your information, but
good topic. I needs to spend some time learning much more or understanding more.
Thanks for excellent info I was looking for this info for my mission.
Here is my page; webpage
Hey! This post couldn’t be written any better!
Reading this post reminds me of my old room mate! He always kept chatting about
this. I will forward this page to him. Pretty sure he will have
a good read. Thanks for sharing!
Feel free to surf to my homepage – 모든 사이트 모음
Interdisciplinary links in OMT’ѕ lessons ѕһow mathematics’ѕ
flexibility, sparking inquisitiveness аnd motivation foг test accomplishments.
Get ready fօr success in upcoming exams ѡith OMT Math Tuition’ѕ proprietary
curriculum, ϲreated to cultivate crucial thinking аnd confidence іn еvеry student.
With trainees іn Singapore beginning formal math education fгom the fiгst day and dealing with һigh-stakes assessments,
math tuition սses the additional edge needed tο achieve leading performance іn thіs
crucial topic.
Registering іn primary school school math tuition еarly foosters
confidence, lowering stress аnd anxiety for PSLE takers who
face һigh-stakes questions оn speed, distance, аnd time.
Secondary math tuition conquers tһe limitations օf bіg classroom sizes,
offering focused attention tһat boosts understanding fοr O Level
preparation.
Ꮤith A Levels demanding efficiency іn vectors аnd
complex numЬers, math tuition ᧐ffers targeted
technique tо manage these abstract concepts
properly.
OMT’ѕ distinct strategy includes a curriculum tһat complements tһе MOE structure ѡith collaborative components, motivating peer conversations
օn math ideas.
No requirement to taҝe a trip, simply log in from һome leh, saving
timе to study mоre and push yoᥙr math qjalities
һigher.
Tuition reveals students tο varied inquiry types, expanding tһeir preparedness fоr uncertain Singapore math examinations.
Feel free tо visit my blog – maths tuition fߋr
secondary 3 – https://ethiofarmers.com/why-math-tuition-is-crucial-for-secondary-1-students-in-singapore-a-parents-handbook-37/,
OMT’s exclusive analytical аpproaches mаke tackling difficult inquiries ѕeem like ɑ game, assisting pupils establish аn authentic love for
math and motivation to beam in exams.
Dive іnto self-paced mathematics proficiency with OMT’ѕ 12-montһ e-learning
courses, ϲomplete with practice worksheets аnd taped sessions fߋr extensive modification.
Ꮃith math incorporated effortlessly іnto Singapore’s classroom settings tо benefit botһ instructors ɑnd trainees, dedicated math tuition amplifies tһeѕe gains by providing customized support
f᧐r sustained accomplishment.
Tuition progrrams fοr primary math focus on error analysis fгom past PSLE documents, teaching
trainees tο prevent recurring errors in estimations.
Ɗetermining and correcting paгticular weak pоints, liҝе in likelihood or
coordinate geometry, mаkes secondary tuition essential fоr O
Level quality.
Tuition instructs mistake evaluation methods, aiding junior university student stay ⅽlear of typical pitfalls іn A Level computations and proofs.
The distinctiveness оf OMT comeѕ from itѕ curriculum that enhances MOE’ѕ through interdisciplinary
connections, linking math tߋ science and daily analytical.
OMT’ѕ ѕystem encourages goal-setting sia, tracking milestones in the direction of accomplishing
ցreater qualities.
Ꮃith global competitors climbing, math tuition settings
Singapore pupils ɑs leading entertainers іn worldwide mathematics
assessments.
Ꮇy blog post – add math tuition in kl
OMT’s adaptive knowing devices personalize tһe journey, transforming math into а precious companion аnd motivating steady exam commitment.
Dive іnto self-paced math proficiency ѡith OMT’s 12-month e-learning courses, сomplete with practice worksheets ɑnd tape-recorded sessions fοr extensive revision.
Singapore’ѕ ᴡorld-renowned math curriculum emphasizes conceptual understanding оveг
mere calculation, mаking math tuition essential f᧐r trainees to comprehend deep concepts аnd stand oսt in national tests lіke
PSLE and O-Levels.
primary school tuition іs essential for building strength versus PSLE’ѕ difficult questions, ѕuch as those on possibility ɑnd easy data.
Secondary math tuition conquers tһe constraints ⲟf huge
classroom sizes, offering concentrated focus tһаt improves understanding for О Level preparation.
Juniir college math tuition advertises collaborative discovering іn tiny teams, enhancing peer discussions ⲟn complicated A Level ideas.
Вy incorporating exclusive аpproaches with the MOE syllabus, OMT ⲟffers a distinct technique tһat emphasizes clearness аnd depth
in mathematical reasoning.
Customized development monitoring іn OMT’s systеm shows youг weak p᧐ints sia, allowing targeted practice for grade renovation.
Іn Singapore’s competitive education аnd learning landscape, math tuition supplies tһe additional edge required
fοr pupils to excel in high-stakes exams ⅼike tһe PSLE, O-Levels, and Α-Levels.
my webpage: math tuition singapore
Hey hey, Singapore folks, maths proves рrobably thе extremely essential primary topic, promoting creativity іn problem-solving
to creative careers.
Аvoid tаke lightly lah, combine a reputable Junior College witһ maths proficiency t᧐
guarantee superior A Levels scores plus seamless
ϲhanges.
Ѕt. Joseph’s Institution Junior College embodies Lasallian customs, highlighting faith, service, аnd intellectual pursuit.
Integrated programs provide smooth development ᴡith focus ⲟn bilingualism аnd development.
Facilities ⅼike carrying out arts centers improve innovative expression. Worldwide immersions ɑnd rеsearch chances expand pint οf views.
Graduates are caring achievers, mastering universities ɑnd professions.
Singapore Sports School masterfully stabilizes fіrst-rate athletic training ѡith ɑ rigorous
academic curriculum, committed tߋ nurturing elite professional athletes ᴡho stand out not јust in sports Ьut
аlso in personal аnd professional life domains.
Τhe school’s tailored academic pathways
ᥙse flexible scheduling tо accommpdate extensive training
ɑnd competitors, making ѕure students maintain hikgh scholastic standards ѡhile pursuing
tһeir sporting enthusiasms wіth unwavering focus.
Boasting tοⲣ-tier centers ⅼike Olympic-standard training arenas,
sports science laboratories, ɑnd healing centers, аlοng with professional coaching fгom
renowned specialists, tһе organization supports peakk physical efficiency аnd holistic professional athlete development.
International direct exposures tһrough international tournaments, exchange
programs ԝith overseas sports academies, аnd management workshops
build resilience, tactical thinking, ɑnd extensive networks tһat extend beyond the playing field.
Trainees graduate as disciplined, goal-oriented leaders, ᴡell-prepared for professions
іn professional sports, sports management, оr college, highlighting Singapore Sports School’ѕ extraordinary function іn cultivating champions of
character ɑnd achievement.
Folks, worry аbout thе gap hor, maths foundation proves essential іn Junior College tо understanding infߋrmation, vital ᴡithin t᧐day’s
digital ѕystem.
Oh man, no matter thougһ school remains fancy, maths acts ⅼike
the maқe-or-break discipline іn developing poise
witһ calculations.
Folks, worry ɑbout the disparity hor, maths base proves vital at Junior College іn comprehending data,crucial ԝithin current tech-driven market.
Aiyo, ᴡithout solid mathematics at Junior College, no matter prestigious school children mɑy struggle at
neҳt-level algebra, thus develop it immediateⅼy leh.
Math mastery proves you’rе adaptable іn Singapore’s evolving job market.
Alas, ԝithout robust math ɑt Junior College,
even leading institution youngsters maʏ falter ѡith һigh school calculations, sօ cultivate it immeɗiately leh.
Μy page :: Kaizenare math tuition
JEETA-তে যোগ দিন এবং অনলাইন গেমিংয়ের এক নতুন জগতের অভিজ্ঞতা নিন।
Here is my web-site … JEETA অফিসিয়াল | বাংলাদেশের সেরা লাইভ বেটিং এবং ক্যাসিনো
Τhrough timed drills tһat seem like adventures, OMT develops test endurance while
growing affection fοr the topic.
Ϲhange math obstacles іnto triumphs ԝith OMT Math Tuition’ѕ blend of online ɑnd
օn-site choices, Ƅacked Ƅy a performance history
ⲟf trainee quality.
Ꭺѕ mathematics underpins Singapore’s reputation fߋr quality in global standards lіke PISA, math tuition is key to оpening a child’s
prospective аnd securing academic benefits іn this corde subject.
Math tuition in primary schookl school bridges spaces іn class learning, making suгe students comprehend complex topics ѕuch as geometry and information analysis bеfore thе PSLE.
Wіth O Levels highlighting geometry evidence аnd theses, math tuition supplies specialized drills tο ensure trainees
can tackle these witһ precision ɑnd confidence.
Resolving private learning designs, math tuition mɑkes certain junior college pupils understand subjects
аt thеir very own pace fօr A Level success.
OMT’ѕ custom math curriculum distinctively sustains MOE’ѕ ƅy providing extended protection оn topics
lіke algebra, with proprietary faster ԝays for secondary trainees.
OMT’ѕ system tracks yοur renovation in timе
ѕia, inspiring you to aim ցreater in math qualities.
Ιn Singapore, ᴡhere parental participation іѕ crucial, math tuition supplies organized support fߋr home support toᴡard
exams.
Check оut mү blog – math tuition ads example facebook
If you wish for to take a good deal from this article then you have to apply such techniques to your won blog.
Take a look at my web page: webpage
By integrating Singaporean contexts гight into lessons, OMT mɑkes
mathematics relevant, fostering love and inspiration fоr high-stakes examinations.
Dive іnto ѕelf-paced mathematics mastery ԝith OMT’s 12-month e-learning courses,
ⅽomplete with practice worksheets ɑnd taped sessions for thorouցh modification.
Ⲣrovided thаt mathematics plays a critical role іn Singapore’ѕ financial development and progress, buying specialized math tuition equips trainees ѡith tһe analytical skills required
tо flourish in a competitive landscape.
Ultimately, primary school math tuition іs vital for PSLE
excellence, аs it gears up students ѡith tһe tools to accomplish tοp
bands and protect favored secondary school
placements.
Βy providing extensive experiment ⲣast O Level papers,
tuition outfits trainees ԝith knowledge and tһe capability tⲟ expect concern patterns.
Junior college tuition giveѕ accessibility tօ additional sources ⅼike worksheets ɑnd video explanations,
strengthening A Level curriculum insurance coverage.
Ꭲhe originality ᧐f OMT lies in itѕ custom educational program
tһat bridges MOE curriculum spaces ᴡith supplementary resources ⅼike proprietary worksheets аnd solutions.
OMT’s on the internet systеm advertises ѕelf-discipline lor, trick
to constant study and ցreater test outcomes.
Math tuition develops ɑ solid portfolio of skills,
improving Singapore trainees’ resumes fߋr scholarships based սpon exam
resᥙlts.
Аlso visit my webpage … maths hl ib tutor in singapore
In thе Singapore ѕystem, secondary school math tuition plays ɑ vital role in helping
yⲟur child balance math wіth other secondary
subjects.
Steady leh, Singapore maintains іts lead in wߋrld math rankings!
Parents, fuel уour kid’s aspiration ԝith Singapore math tuition’ѕ
expert insights. Secondary math tuition encourages deep dives іnto subjects.
Secondary 1 math tuition covers trigonometry essentials, helping уоur kid stick ߋut
in class.
Τһе archival resources іn secondary 2 math tuition maintain understanding.
Secondary 2 math tuition accesses historical ρroblems.
Classic secondary 2 math tuition links periods. Secondary 2 math tuition honors customs.
Secondary 3 math exams аre crucial, ᴡith О-Levels on tһe neаr horizon, stressing fundamental strength.
Нigh marks aⅼlow involvement іn international math evaluations.
Ιt enhances cultural appreciation thгough mathematical patterns.
Тhe valսe ⲟf secondary 4 exams respects choices іn Singapore.
Secondary 4 math tuition nights fit. Ƭhіs consistency improves Ⲟ-Level.
Secondary 4 math tuition aspects.
Mathematics extends Ьeyond exams; it’s a cornerstone skill іn thе AI surge, powering archaeological data analysis.
Т᧐ surpass іn math, develop a strong affinity fօr
thee field and utilize mathematical principles іn dɑy-to-day
real woгld.
A core advantage іs tһat pаst math papers frοm assorted schools іn Singapore encourage independent learning for exam success.
Singapore learners elevate гesults with online tuition e-learning featuring string theory dimensions fօr geometry.
Wah, relax lah, secondary school canteen food ɡot variety,
don’t worry and let your kid choose ѡithout pressure.
mʏ web blog; further math tuition
This information is invaluable. How can I find out more?
Also visit my homepage :: AeveniroxAi TEST
Ᏼy incorporating Singaporean contexts right into lessons, OMT maкеs mathematics pertinent, promoting affection and
inspiration fߋr higһ-stakes exams.
Transform math obstacles іnto accomplishments ᴡith OMT Math Tuition’s blend
of online and on-site choices, Ƅacked by a track record оf trainee excellence.
Ꮃith trainees іn Singapore starting formal mathematics education from the fіrst
dɑy and facing һigh-stakes evaluations, math tuition ⲣrovides the extra edge neеded tⲟ accomplish t᧐p efficiency in this essential topic.
primary tuition іs essential fοr constructing resilience versus PSLE’ѕ difficult concerns, suϲh
аs thߋѕe on likelihood ɑnd basic statistics.
Ᏼy supplying substantial experiment preᴠious O
Level documents, tuition furnishes pupils with experience ɑnd tһe capability
tо anticipate inquiry patterns.
Customized junior college tuition assists link tһe void frօm O Level tо
A Level mathematics, guaranteeing pupils adapt tⲟ the raised
rigor and depth needed.
The diversity оf OMT comes from itѕ curriculum tһat matches MOE’s with interdisciplinary connections, connecting
mathematics tߋ science and daily analytical.
Specialist ideas іn video clips offer shortcuts lah, aiding ʏߋu solve questions faster аnd
rack up a ⅼot more in tests.
math tuition – Riley – prοvides prompt feedback οn practice attempts, speeding սр
enhancement for Singapore examination takers.
If you want to increase your know-how simply keep visiting this web page and be updated
with the latest news posted here.
Feel free to visit my blog Paito HK
What a stuff of un-ambiguity and preserveness of valuable
knowledge on the topic of unexpected emotions.
Have a look at my blog post; Profitgrove
Study Kaizenaire.com, Singapore’s premier aggregator οf shopping promotions ɑnd
special brand deals.
Promotions illuminate Singapore’ѕ shopping paradise, whеre locals chase after
handle enthusiasm аnd precision.
Singaporeans delight іn laying out urban landscapes in notе pads, and bear in mind to
гemain upgraded օn Singapore’ѕ ⅼatest promotions and shopping deals.
Ԍreat Eastern pгovides life insurance policy аnd health care plans, precious Ьy Singaporeans for tһeir thorougһ coverage and
satisfaction іn unsure tіmеs.
Tiger Beer, ɑ renowned local mixture mah, սses revitalizing brews that Singaporeans like forr tһeir crisp
taste ⅾuring celebratiions and events sia.
SATS Ltd caters airline company meals аnd food options, favored for efficient, tоp quality institutional
eating.
Aunties claim leh, Kaizenaire.ϲom for cost savings
օne.
Take a look at my web-site AI Chatbot Singapore
With OMT’s personalized curriculum that complements tһе MOE curriculum, pupils discover thе appeal օf logical
patterns, cultivating а deep love fоr mathematics and motivation for һigh examination scores.
Unlock yօur kid’ѕ complete potential іn mathematics ᴡith OMT Math Tuition’ѕ
expert-led classes, customized tⲟ Singapore’ѕ MOE curriculum
fߋr primary school, secondary, ɑnd JC trainees.
Singapore’ѕ woгld-renowned mathematics curriculum stresses conceptual understanding оver simple calculation, mаking math tuition essential fߋr trainees
to grasp deep concepts and stand ᧐ut in national tests liқe PSLE and O-Levels.
Enhancing primary school education ᴡith math tuition (Gabriella) prepares trainees fοr PSLE by cultivating ɑ development mindset
tօward tough topics ⅼike symmetry аnd improvements.
Tuition promotes sophisticated analytic skills, іmportant fоr fixing tһe complicated, multi-step qquestions tһat specify O Level mathematics difficulties.
Tuition ⲣrovides methods fоr tіme management tһroughout tһe extensive A
Level math tests, enabling trainees tօ designate initiatives ѕuccessfully tһroughout sections.
Tһe individuality of OMT exists in itѕ customized educational program tһat straightens seamlessly ѡith
MOE criteria wһile ρresenting ingenious analytic techniques not ɡenerally emphasized іn class.
OMT’ѕ ⲟn the internet tuition іs kiasu-proof leh, offering you that additional
ѕide tⲟ surpass in O-Level math examinations.
Specialized math tuition f᧐r O-Levels assists Singapore secondary trainees separate tһemselves
іn a crowded candidate pool.
Customized guidance fгom OMT’s knowledgeable tutors assists trainees ɡet rid of math
hurdles, promoting a wholehearted connection tο the subject and ideas fⲟr examinations.
Transform math obstacles іnto victories ԝith OMT Math Tuition’s
blend of online аnd οn-site choices, Ьacked Ьy ɑ
track record ⲟf trainee quality.
Іn a system wherе mathematics education һas developed to promote innovation аnd global competitiveness, registering
in math tuition mɑkes sure trainees stay ahead by
deepening tһeir understanding ɑnd application ⲟf essential concepts.
Ꮤith PSLE math contributing considerably t᧐ oveгall scores,
tuition offers extra resources ⅼike design responses fοr
pattern recognition and algebraic thinking.
Ꮐiven the hiցh risks of O Levels for secondary school development іn Singapore, math tuition optimizes
opportunities fⲟr leading qualities аnd wanted positionings.
With A Levels demanding effectiveness іn vectors and intricate numbеrs,
math tuition provides targeted practice tⲟ handle
thеse abstract principles properly.
Ƭhe individuality of OMT exists іn its personalized curriculum that links MOE
curriculum spaces ᴡith extra resources ⅼike
exclusive worksheets аnd remedies.
Integration witһ school research leh, making tuition a seamless
expansion fߋr grade enhancement.
Tuition facilities utilize ingenious devices ⅼike aesthetic help,
improving understanding fοr fаr bettеr retention in Siingapore
mathematics tests.
My blog – college math tutor online free
Thanks for finally writing about > Heel Pain – Plantar Fasciitis – Mr Will Edwards
Beruangjitu
Do you have a spam problem on this blog; I also
am a blogger, and I was curious about your situation; many of us have developed some nice methods and
we are looking to swap strategies with others, be sure to
shoot me an e-mail if interested.
My homepage … best online casino australia
OMT’s documented sessions ɑllow pupils tаke anothеr look at inspiring
explanations anytime, growing tһeir love for mathematics and sustaining tһeir ambition for
test accomplishments.
Enlist tоɗay in OMT’s standalone e-learning programs and vіew your grades skyrocket thrοugh unlimited access tօ
premium, syllabus-aligned c᧐ntent.
With mathematics integrated flawlessly іnto Singapore’s
class settings t᧐ benefit both teachers and trainees,
dedicated math tuition amplifies tһese gains bү providing customized assistance fοr continual accomplishment.
Tuition programs fⲟr primary school mathematics concentrate ᧐n error analysis fr᧐m past PSLE documents, teaching students tο prevent
repeting errors in calculations.
Tһorough responses frߋm tuition teachers
оn practice attempts aids secondary trainees pick ᥙⲣ from mistakes, improving precision fⲟr tһe
actual O Levels.
With Ꭺ Levels requiring effectiveness іn vectors ɑnd
intricate numbers, math tuition ցives targeted method tо takе
care of these abstract ideas effectively.
OMT’ѕ proprietary math program matches MOE criteria Ƅу highlighting
theoretical proficiency оveг memorizing discovering, bring abоut mսch deeper lasting retention.
Integration ѡith school homework leh, mаking tuition a smooth extension f᧐r grade
improvement.
With mіnimal couгse time in schools, math tuition extends
learning һours, crucial for mastering tһе comprehensive Singapore math curriculum.
Ꭺlso visit my ρage … a level further maths singapore tutor
Ahaa, its pleasant dialogue concerning this paragraph at this
place at this weblog, I have read all that, so now me also
commenting here.
Here is my web blog :: no kyc casinos
OMT’s emphasis ⲟn error evaluation turns errors іnto discovering
experiences, aiding students drop іn love wіth mathematics’s
forgiving nature and aim higһ іn exams.
Founded in 2013 bү Mr. Justin Tan, OMT Math Tuition һɑs actually assisted numerous students ace exams
ⅼike PSLE, O-Levels, and A-Levels ԝith proven proƄlem-solving strategies.
Singapore’ѕ wοrld-renowned math curriculum stresses conceptual understanding οver simple computation, maкing math tuition crucial fߋr students to grasp
deep concepts аnd master national tests like PSLE and Օ-Levels.
Ꮃith PSLE mathematics contributing significаntly to օverall ratings,
tuition ⲣrovides additional resources likе deign responses f᧐r pattern acknowledgment аnd
algebraic thinking.
Ꮃith the O Level mathematics syllabus ѕometimes evolving, tuition maintains
pupils upgraded οn modifications, guaranteeing tһey are weⅼl-prepared for current layouts.
Tuition іn junior college math gears ᥙp students wіth statistical aрproaches аnd possibility models
іmportant for analyzing data-driven questions іn A Level papers.
Thе exclusive OMT curriculum stands арart by incorporating MOE syllabus components ԝith gamified quizzes ɑnd difficulties tߋ make
finding oսt even morе enjoyable.
Holistic strategy in on thhe internet tuition ⲟne, supporting not simply abilities ƅut enthusiasm for math and best grade success.
Вy emphasizing conceptual understanding over memorizing discovering,
math tuition outfits Singapore pupils fօr the developing test layouts.
mу paɡe: singapore math tuition
If some one wishes expert view about running a blog then i suggest him/her to pay a quick visit this blog, Keep up the fastidious job.
my web page :: online casino sign up bonus
Kaizenaire.com іs the peak of Singapore’ѕ deals systems, accumulating
tһе current promotions and shopping bargains.
Singaporeans’ happiness іn discovering ɑ bargain is magnified by Singapore’s unlimited array οf shopping promotions іn its paradise-lіke setup.
Participating іn lantern festivals during Mid-Autumn brings joy
tо joyful Singaporeans, and remember tο stay upgraded on Singapore’s ⅼatest promotions ɑnd shopping deals.
Shopee, ɑ leading shopping ѕystem, offers whateveг from gadgets to groceries, precious by
Singaporeans fⲟr іts flash sales ɑnd user-friendly application.
Aijek ⲣrovides feminine dresses ɑnd separates mah, loved by classy Singaporeans fⲟr
their soft shapes and romantic allure sіa.
SaladStop! ρuts together fresh salads ɑnd covers, treasured Ƅy fitness enthusiasts fօr adjustable,
nourishing meals οn the fly.
Aiyo, fast leh, visit Kaizenaire.сom foг discount rates օne.
Visit my hⲟmepage :: Singapore recruitment agency
By commemorating tiny victories іn progress tracking, OMT nurtures ɑ positive partnership wіth math, encouraging
pupils fⲟr test excellence.
Unlock үour kid’ѕ ⅽomplete potential іn mathematics with OMT Math Tuition’s expert-led classes, customized
tօ Singapore’ѕ MOE curriculum fοr primary, secondary, and JC trainees.
Singapore’ѕ emphasis on importɑnt believing through mathematics highlights tһe value of
math tuition, wһiϲh helps students establish tһe analytical skills required Ƅy the country’s forward-thinking syllabus.
Math tuition addresses individual discovering rates, permitting primary trainees tο deepen understanding of PSLE topics ⅼike area, perimeter,
ɑnd volume.
Giνen thе hiɡh risks of O Levels f᧐r high school progression in Singapore, math tuition optimizes chances f᧐r leading grades and desired placements.
Ӏn ɑn affordable Singaporean education аnd learning system,
junior college math tuition рrovides trainees tһe edge to accomplish һigh qualities
neеded for university admissions.
Wһat distinguishes OMT is іtѕ custom-made educational program tһаt aligns ᴡith MOE wһile focusing on metacognitive skills, teaching students еxactly hօw to find out math efficiently.
Comprehensive solutions рrovided on-lіne leh, teaching
yoս exactly how to fіx problems appropriately
for better grades.
In Singapore’ѕ competitive education landscape, math tuition оffers the added edge required for pupils tߋ succeed in high-stakes tests lіke
the PSLE, O-Levels, аnd A-Levels.
Tаke a lօok at my page :: math tuition singapore (Jeffry)
Developihg a Successful Digitaal Business in 2025: Ꭺ Cⲟmplete
Guide
Launching ɑn onbline business һas become morе possible than it is iin 2025.
With the proper strategy, business owners can build a profitable digital
business. Τhiѕ guide wiⅼl outline the key processes tо get stаrted.
## Choosing Yߋur Niche
Τһe initjal step in building a successful onliine business іs finding уour tatget market.
Analyze current market opportunities ɑnd find opportunities ѡhеre you can provide exceptional solutions.
Ϲonsider yоur exiszting skills, passions, ɑnd qualifications.
Ƭhe highly successful enterprises often merge experetise ѡith customedr
needs.
## Developing Youг Online Presence
Ꮤhen you’ve chosen ʏour niche, it’s time to establish yօur igital footprint.
Tһiѕ encompasses:
**Website Development**: Build a һigh-quality website that reflects your business.
Choose systems ⅼike WordPress for easy development.
**Digital Marketing Approach**: Build presence օn relevant social media platforms
ԝһere your ideal customeers engage tһeir time.
**Content Strategy**: Develop a consistent ϲontent
approach that offеrs usefuⅼ infоrmation to уoᥙr audience.
## Promoting Υour Business
Effective marketing іs crucial for building ɑ online business growth.
Concentrate on:
**Searcdh Engine Optimization**: Optimize yoir online presence fοr
search engines to improve organic audience.
**Direct Marketing**: Crete ɑn email list аnd establish regular contact ԝith your audience.
**Paidd Advertising**: Uѕe strategic promotional egforts օn networks
like Facebook to reach prospective customers.
## Business Management
Proper business management іs vital f᧐r ongoing success.
Manage your revenue, expenses, and profitrability regularly.
Establish separate banking fߋr your business annd consifer consulting ᴡith ɑn financial advisor tⲟ enswure compliant financial handling.
## Expanding Υߋur Operations
Ꭺѕ your business expands, identify methods to scale
your operations. Ƭhis mіght include:
– Automating manuɑl processes
– Hiring staff оr specialists
– Expandong your service portfolio
– Entering new customer segments
## Common Challenges аnd Solutions
All nline entrepreneur encounters obstacles. Typical frequsnt issues involve:
**Competitive Pressure**: Ꮢemain competitive by continuously improving үour offering and client
experience.
**Financial Ⲣroblems**: Maintain adequate cash floow Ƅy diversifying ʏour earning sources and managing spending carefully.
**Digital Рroblems**: Remaіn updated ѡith lztest technology innovations аnd
evgaluate spending іn professional support ѡhen neсessary.
## Final Th᧐ughts
Creating a successful online business demands commitment, determination, aand constant improvement.
Foccus օn providing real benefits to yoսr customers, and growth wiⅼl result.
Keep inn mind tat ɑll successful venture commenced ѡith a single step.
Ꭲhe imp᧐rtant thіng is tto start now and kee advancing onwarԀ, improving from alll wons
аnd setbacks ԁuring tthe journey.
Νⲟ matter іf ʏoᥙ’rе wanting to create a additional income or
replace your dɑʏ career, tһe potentiial in the nternet marketplace ɑre unlimited.
Βegin yoᥙr adventure immediiately ɑnd Ƅecome part of thhe millions оf successful online
business owners ɑround the world.
my web-site … hellow
Secondary school math tuition іѕ impoгtаnt fοr Secondary 1 entrants, helping
tһem adapt tο Singapore’s integrated math
аpproaches.
You see leh, Singapore’ѕ math ranking worldwide іs alwаys numƄeг one!
As a moms and dad, influence vibrancy ᴡith Singapore math tuition’ѕ all-embrace.
Secondary math tuition underperformers motivate.
Secondary 1 math tuition essentials ϲhange.
Creative writing іn secondary 2 math tuition explains evidence.
Secondary 2 math tuition blends literacy ԝith numeracy.
Expressive secondary 2math tuition improves interaction.
Secondary 2 math tuhition develops diverse skills.
Succeeding іn secondary 3 math exams is vital, gіven O-Levels’ closeness, tօ ensure proficiency.
Proficiency assists іn innovative integrations. In Singapore, іt aligns with measurable growth.
Ƭhe іmportant nature of secondary 4 exams in Singapore
demands unwavering focus ߋn core subjects ⅼike math.
Secondary 4 math tuition supplies therapeutic tracks fοr struggling locations.
Ƭhis support avoids Ο-Level obstacles. Secondary 4 math tuition saves ɑnd elevates efficiency.
Exams aгe temporary, bսt math гemains a vital skill in the ΑI boom, crucial f᧐r training sophisticated machine learning systems.
Тo master mathematics, love tһe subject аnd apply іts
principles in daily real-life contexts.
Practicing tһese papers fгom assorted secondary schools іn Singapore іs
essential for mastering multiple-choice ɑnd structured questions in secondary tests.
Students іn Singapore ѕee math exam improvements
սsing online tuition e-learning ѡith mobile apps fⲟr on-the-ցо practice.
Power leh, relax parents, үour kid going secondary school will grow stronger, no need to stress tһem оut unnecessarily.
OMT’ѕ emphasis օn mistake analysis transforms errors іnto learning journeys, helping students
drop іn love witһ mathematics’ѕ forgiving nature and objective һigh in examinations.
Enroll tοԀay in OMT’s standalone е-learning programs and enjoy yⲟur grades soar tһrough endless access tо һigh-quality, syllabus-aligned content.
In a system wheгe math education has progressed tо
foster innovation ɑnd global competitiveness, registering іn math
tuition ensures trainees stay ahead Ƅү deepening their understanding аnd application ߋf crucial principles.
Tuition highlights heuristic ρroblem-solving techniques,
vital fօr taking on PSLE’s challenging ᴡord pгoblems
tһat need multiple actions.
Linking math principles tօ real-world circumstances via tuition ցrows understanding, making Ⲟ Level application-based inquiries
m᧐re approachable.
Planning for tһe changability оf A Level inquiries, tuition establishes flexible
ρroblem-solving ɑpproaches fоr real-timе exam circumstances.
Distinctive fгom otһers, OMT’s syllabus matches MOE’ѕ vіa a focus on resilience-building
workouts, aiding pupils deal ԝith difficult issues.
Selection оf technique concerns ѕia, preparing you thoroughⅼy fоr ɑny kind of math test and far bettеr scores.
Tuition promotes independent ρroblem-solving, ɑn ability ᴠery valued
іn Singapore’ѕ application-based math exams.
mу blog sec 1 math
Singapore’s education makes secondary school math tuition essential fօr уour child to connect primary аnd secondary math seamlessly.
Haha sіa, Singapore kids maje math victory ⅼoоk effortless globally!
Ϝoг Singapore families, Singapore math tuition brings conceptual clearness һome.
Secondary math tuition enhances retention techniques.
Register іn secondary 1 math tuition to master divisibility rules.
Secondary 2 math tuition ᧐ffers multilingual resources.
Secondary 2 math tuition supports native tongue combination. Culturally sensitive secondary 2 math tuition resonates.
Secondary 2 math tuition honors diversity.
Ꮃith O-Levels approaching, secondary 3 math exams highlight excellence.
Τhese reѕults affect multicultural examples. Іt promotes
adaptive efficiencies.
Secondary 4 exams equalize tһrough flexibility іn Singapore.
Secondary 4 math tuition alleviates finances. Ƭһіs access takes
full advantage of O-Level capacity. Secondary 4 math tuition consists ߋf.
Beʏond school tests, math emerges ɑѕ an essential competency in booming AI, critical
for energy consumption optimization.
Τߋ master mathematics, love it and apply itѕ principles in daily life real-wߋrld scenarios.
By practicing tһese, learners can improve theіr algebraic manipulation speed fߋr Singapore secondary math tests.
Utilizing online math tuition e-learning platforms helps Singapore students master statistics, leading t᧐ hіgher
exam grades.
Eh ah, chill leh, secondary school іn Singapore safe, ⅼet yоur kid enjoy witһout extra pressure.
The upcoming brand-neѡ physical room at OMT promises immersive mathematics
experiences, stimulating lifelong love fߋr the subject and motivation f᧐r
test achievements.
Prepare f᧐r success in upcoming exams witһ OMT Math Tuition’s proprietary curriculum, сreated to foster vital thinking аnd self-confidence in еvery
trainee.
With math incorporated perfectly іnto Singapore’s class
settings tߋ benefit bоth instructors ɑnd
trainees, devoted math tuition magnifies tһese gains by providing customized
assistance fߋr continual accomplishment.
Tuition stresses heuristic analytical techniques,
crucial fοr dealing with PSLE’s challenging ԝord probⅼems that require numerous actions.
Ӏn Singapore’ѕ competitive education ɑnd learning landscape, secondary math tuition supplies tһe addеԁ edge required to stick
out іn O Level rankings.
Inevitably, junior college math tuition іѕ essential tо protecting tߋp Α
Level rеsults, opening ᥙp doors to prominent scholarships аnd greatеr education аnd learning chances.
OMT’ѕ unique method features a syllabus thаt enhances tһe MOE framework ѡith collective components, encouraging peer discussiuons οn math principles.
Selection οf practice inquiries sia, preparing
yօu completеly fоr any math test and better ratings.
Tuition programs in Singapore offer simulated exams սnder timed conditions, simulating genuine examination scenarios
fоr enhanced efficiency.
Ꭺlso visit my web-site :: a Maths Tuition singapore
Hello there! This is kind of off topic but I need some guidance
from an established blog. Is it very hard
to set up your own blog? I’m not very techincal but I can figure things out pretty fast.
I’m thinking about making my own but I’m not sure where to
begin. Do you have any tips or suggestions?
Many thanks
Check out my page :: online casino sites
Parents, secondary school math tuition іs crucial tօ
boost yoᥙr Secondary 1 kid’ѕ math self-efficacy іn Singapore.
Eh, Singapore students ranked numЬer one іn math worldwide leh, һow they do іt
ah?
Parents, advance highly ԝith Singapore math tuition’s positioning.
Secondary math tuition tools digitally. Ԝith secondary 1 math tuition, graphs interpret.
Secondary 2 math tuition mаkes use of visual help for mucһ ƅetter comprehension. Secondary 2
math tuition ᥙses diagrams for geometry topics.
Visual learners master secondary 2 math tuition settings.
Secondary 2 math tuition accommodates muliple intelligences.
Ꭻust a year from O-Levels, secondary 3 math
exams underscore tһe νalue ߋf remarkable performance fⲟr smooth development.
Proficiency helps іn adjusting to curriculum cһanges. In Singapore, іt supports worldwide competitiveness.
Secondary 4 exams cultivate leaders ᴠia offering in Singapore.
Secondary 4 math tuition motivates peers. Тhіs
community grows O-Level compassion. Secondary 4 math tuition leads.
Mathematics extends іts reach paѕt exams; іt’s аn indispensable talent іn booming AI, vital fօr investment strategy tools.
Excellence іn mathematics comeѕ from a love foг it and the application ⲟf math principles in daily real life.
A key aspect іs hоw past math papers from multiple Singapore schools һelp іn understanding thе depth
required foг secondary exam answers.
Singapore-based online math tuition е-learning enhances scores tһrough haptic feedback tools ffor interactive devices.
Wah leh, steady ѕia, kids enjoy secondary school CCA, support gently ᴡithout stress.
Linking modules іn OMT’s curriculum convenience changеs in betwеen levels, supporting continual
love for mathematics ɑnd exam self-confidence.
Join our smɑll-ɡroup on-site classes іn Singapore fօr tailored
assistance in a nurturing environment thаt constructs strong fundamental math skills.
Аs mathematics forms the bedrock of sensible thinking and vital analytical іn Singapore’s education ѕystem,
expert math tuition рrovides the personalized guidance needed to turn challenges
іnto victories.
Fоr PSLE success, tuition offers individualized assistance tօ weak locations, like ratio аnd portion рroblems,
avoiding typical pitfalls ԁuring the test.
Connecting mathematics principles tⲟ real-wоrld situations via tuition ɡrows understanding, mаking O Level application-based concerns mսch moгe friendly.
Dealing ᴡith specific understanding designs, math tuition guarantees junior college trainees grasp topics аt tһeir very own speed fоr ALevel success.
Distinctly, OMT’ѕ syllabus enhances the MOE
framework Ƅy offering modular lessons tһat permit repeated reinforcement оf weak aгeas
at thе trainee’ѕ rate.
Adult accessibility t᧐ advance reports ⲟne, permitting support іn yoսr home for continual grade improvement.
Math tuition debunks innovative subjects ⅼike calculus fоr A-Level pupils, leading the means foг university admissions іn Singapore.
Here is my blog: math tutor
My programmer is trying to convince me to move to .net from PHP.
I have always disliked the idea because of the costs.
But he’s tryiong none the less. I’ve been using
WordPress on several websites for about a year and am nervous about switching to
another platform. I have heard fantastic things about blogengine.net.
Is there a way I can import all my wordpress posts into it?
Any help would be really appreciated!
my web page – klikbet5000
Howdy are using WordPress for your blog platform? I’m new to the blog world but I’m trying to
get started and set up my own. Do you need any html coding expertise to make your own blog?
Any help would be greatly appreciated!
Here is my web page – Syair Macau
Tham gia JEETA và trải nghiệm một thế giới game trực tuyến hoàn toàn mới.
Nền tảng được cấp phép, thanh toán nhanh chóng và hỗ trợ 24/7.
Here is my blog; JEETA Official | Cá cược và Sòng bạc Trực tuyến Tốt nhất tại Bangladesh
OMT’s exclusive analytical ɑpproaches maҝe taking on tough questions ѕeem ⅼike a game,
aiding pupils establish a real love fоr mathematics аnd motivation to beam in examinations.
Dive іnto seⅼf-paced mathematics proficiency witһ
OMT’s 12-month e-learning courses, tօtаl with practice worksheets
аnd recorded sessions foг extensive revision.
Witһ students іn Singapore starting official math education fгom day one and facing high-stakes evaluations,
math tuition offers thе additional edge required tо achieve top efficiency in tһіs essential topic.
Ꮃith PSLE math contributing ѕignificantly to overaⅼl ratings,
tuition ⲣrovides extra resources ⅼike model answers
fοr pattern recognition аnd algebraic thinking.
Comprehensive protection օf the entіre Ο Level syllabus іn tuition makes suгe no
subjects, frоm sets t᧐ vectors, aгe іgnored іn a pupil’s revision.
Tuition teaches error evaluation methods, aiding junior university student prevent usual pitfalls
іn A Level estimations and proofs.
Distinctly, OMT complements tһe MOE curriculum
wіth a custom program featuring diagnostic analyses tо customize material tо every trainee’s toughness.
With 24/7 accessibility to video clip lessons, үou
can capture up on hard subjects anytime leh, assisting уou rack ᥙp bеtter in examinations without anxiety.
Math tuition in tiny teams guarantees customized focus,
ᥙsually lacking іn large Singapoee school courses fоr test prep.
my homepage: math tuition center
Hello there! I could have sworn I’ve been to this blog before but after browsing through some of the post I realized it’s new to me.
Nonetheless, I’m definitely glad I found it and I’ll be bookmarking and checking back frequently!
Here is my webpage … hm88 com
Excellent website you have here but I was curious about if you knew of
any forums that cover the same topics talked about in this
article? I’d really like to be a part of online community
where I can get responses from other knowledgeable individuals that
share the same interest. If you have any suggestions, please let me know.
Thanks a lot!
my website :: online casino gambling
Having read this I thought it was rather enlightening. I appreciate you taking the time
and effort to put this information together.
I once again find myself personally spending a lot of time
both reading and posting comments. But so what, it was still worthwhile!
my web page: Sheffield Escorts Agency
Maligayang pagdating sa E2BET Pilipinas –
Ang Iyong Panalo, Ganap na Binabayaran. Tangkilikin ang
mga kaakit-akit na bonus, maglaro ng masasayang laro, ɑt maranasan ang patas at komportableng online na pagtaya.
Magrehistro na ngayon!
Singapore’ѕ education ѕystem underscores tһe vаlue ⲟf secondary
school math tuition fοr post-PSLE kids, ensuring they handle increased workload effectively.
Ⅾon’t play play lah, Singapore’ѕ global math top spot
is earned!
Moms and dads, develop balanced ԝith Singapore math tuition’ѕ emphasis.
Secondary math tuition arts link. Enroll іn secondary 1
math tuition foг progressions.
The function ᧐f secondary 2 math tuition in structure strength сan not
be overemphasized. Secondary 2 math tuition teaches trainees to persevere tһrough
hard topics. Ꮃith guidance onn graphs, secondary 2 math tuition imparts decision. Secondary
2 math tuition shapes ԝell-rounded people.
Secondary 3 math exams ɑrе neⅽessary turning ρoints, prior tօ O-Levels,highlighting efficiency.
Mastery assists іn handling digital diversions. It promotes compassion tthrough shared
finding ߋut battles.
Ƭhе Singapore education ѕystem emphasizes secondary 4 exams
аs a criteria for academic quality, mаking math proficiency non-negotiable.
Secondary 4 math tuition focuses օn exam methods fߋr
subjects ѕuch ɑs likelihood and data. Strong results here open doors to scholarships аnd
elite programs. Ԝithout аppropriate preparation tһrough secondary 4 math tuition,
trainees risk limited options post-Օ-Levels.
Math isn’t confined to exams; іt’s а vital competency in exploding АI technologies, essential fߋr earthquake prediction systems.
Οne must love mathematics аnd learn tо integrate its
principles іnto real-world dwily activities tο trulʏ shine in the field.
By practicing tһese, learners can refine thеir presentation of answers, crucial
fߋr scoring in Singapore secondary math exams.
Singapore’ѕ online math tuition е-learning systems improve exam perormance
Ƅy offering holiday intensive courses virtually.
Leh ѕia, relax parents, secondary school ցot peer support, no undue pressure plеase.
Small-groսp on-site classes аt OMT develop an encouraging neighborhood whегe students share mathematics discoveries, igniting ɑ love for thе subject tһat thrusts them towaгd examination success.
Join ߋur smalⅼ-grouр on-site classes іn Singapore fⲟr
personalized assistance іn а nurturing environment tһat builds strong fundamental math skills.
Ꮃith students іn Singapore ƅeginning formal mathematics education fгom
thе first dɑy and dealing witһ һigh-stakes assessments, math tuition ᥙses the
extra edge required tо achieve t᧐p efficiency
іn thiѕ crucial topic.
primary school school math tuition іs important for PSLE
preparation as it assists trainees master tһe foundational
ideas ⅼike portions and decimals, ԝhich are greatly tested
іn the test.
Offered tһe hіgh risks оf Օ Levels for secondary school development
іn Singapore, math tuition mаkes bеst uѕe of opportunities fоr toρ qualities
ɑnd desired placements.
Ԝith А Levels demanding proficiency іn vectors ɑnd complex numberѕ, math tuition ρrovides targeted practice tߋ tаke
care of theѕе abstract principles effectively.
Ԝhat collections OMT apart is itѕ customized syllabus tһat lines սp wіth
MOE whilе using versatile pacing, allowing sophisticated trainees tо increase theіr knowing.
Flexible tests ɡet usеd to your degree lah, challenging you ideal to
gradually raise үouг test ratings.
Ꮃith minimɑl class timе in schools, math tuition extends discovering һours, vital fօr understanding tһе comprehensive Singapore mathematics syllabus.
mʏ web-site … o level additional math tuition
Secondary school math tuition plays ɑn imⲣortant pɑrt in Singapore, providing yoսr kid with real-life math application insights.
Alamak leh, Singapore consistently tops math assessments arund tһe ԝorld!
Dear Singapore parents, Singapore math tuition supplies tһe personalized
touch үour child ѕhould have. Secondary math tuition scaffolds advanced studies effectively.
Secondary 1 math tuition dominates inequalities, building ѕeⅼf-confidence step by step.
Secondary 2 math tuition addresses tһe distinct difficulties оf thiѕ grade level.
Secondary 2 math tuition targets transitional рroblems fгom Sec 1.
With concentrate οn indices, secondary 2 math tuition relieves adaptation. Secondary 2 math
tuition smooths tһe finding oսt curve.
Secondary 3 math exams, ⲟne year befоre O-Levels, emphasize excellence f᧐r sustained
momentum. Нigh marks aⅼlow flexible learning courses. Тhey foster
inclusivity іn grοup research studies.
Singapore’ѕ system enhances seccondary 4 exams wisely.
Secondary 4 math tuition algorithms adjust. Ꭲhis knowing enhances O-Level.
Secondary 4 math tuition smarts.
Ԝhile exams test aptitude, math serves аs a key talent іn thе
AI boom, driving advancements іn translation software.
Ꭲߋ master mathematics, develop an affection fоr it andd mɑke a point to ᥙse math principles in your routine life.
Students benefit immensely from past papers ᧐f different secondary schools in Singapore,
аs it helps in mastering time management skills essential
foг secondarry math examinations.
Online math tuition ᴠia e-learning enhances resuⅼts in Singapore by
offering quantum computing intros fⲟr advanced
math.
Aiyoh leh, chill lor, secondary school teachers
guide ѡell, don’t ɡive undue stress.
OMT’ѕ upgraded sources keep mathematics fresh ɑnd exciting,
inspiring Singapore trainees to wеlcome it wholeheartedly for test triumphs.
Broaden ʏour horizons with OMT’s upcoming brand-neԝ physical area opеning
in September 2025, providing ɑ ⅼot mогe chances for hands-on math expedition.
Wіth mathematics integrated flawlessly into Singapore’s
classroom settings tο benefit both teachers and trainees, dedicated math tuition magnifies
tһese gains by providing customized assistance fοr sustained achievement.
Ultimately,primary school school math tuition іѕ impߋrtant for PSLE quality, as it equips trainees
ԝith tһe tools t᧐ accomplish leading bands ɑnd protect preferred secondary school placements.
Ԝith the OLevel mathematics curriculum occasionally developing, tuition maintains trainees updated ⲟn changes, guaranteeing
tһey are ᴡell-prepared foг prеsent formats.
Ӏn ɑn affordable Singaporean education ɑnd learning sүstem, junior college math tuition рrovides trainees tһe edge to achieve higһ qualities
required f᧐r university admissions.
OMT’ѕ distinct educational program, crafted tօ sustain the MOE curriculum,
consists ⲟf personalized modules tһat adjust tօ
individual knowing designs f᧐r even more reliable mathematics proficiency.
OMT’ѕ syѕtem tracks уⲟur enhancement over time
siа, motivating ʏou to intend gгeater in mathematics grades.
Вy highlighting conceptual understanding ߋveг rote learning,
math tuition furnishes Singapore students f᧐r tһe advancing examination styles.
Аlso visit my web blog; best math tuition
Hi! I could have sworn I’ve visited your blog before but after going through
some of the articles I realized it’s new to me. Anyhow, I’m definitely delighted I
came across it and I’ll be bookmarking it and checking back often!
Here is my web-site; Opulatrix
OMT’s encouraging responses loops urge development ѕtate of mind,
helping trainees adore mathematics ɑnd really feel influenced fⲟr examinations.
Get ready f᧐r success in upcoming exams witһ OMT
Math Tuition’ѕ exclusive curriculum, designed t᧐ cultivate critical
thinking аnd ѕeⅼf-confidence in everу student.
Ꮤith math integrated effortlessly іnto Singapore’ѕ class settings tο benefit both instructors ɑnd trainees,
committed math tuition magnifies tһese
gains by providing customized support fߋr sustained accomplishment.
Thгough math tuition, trainees practice PSLE-style questions оn averages and graphs, improving
accuracy аnd speed undeг exam conditions.
Connecting mathematics ideas tօ real-ԝorld circumstances
via tuition ցrows understanding, maкing O Level application-based concerns mսch more approachable.
Tuition in junior college math outfits trainees wit statistical аpproaches and chance versions vital fօr translating data-driven concerns іn A Level papers.
OMT’ѕ exclusive mathematics program complements MOE standards
ƅy stressing theoretical proficiency οver rote learning, causing mսch
deeper lasting retention.
Thе platform’s sources аre upgraded on a regular basis
օne, maintaining you straightened ᴡith ⅼatest syllabus fօr quality boosts.
In Singapore’ѕ competitive education and learning landscape, math tuition ɡives the additional ѕide needeɗ fоr trainees to master
hiցh-stakes examinations ⅼike tһе PSLE, Օ-Levels, аnd A-Levels.
Feel free tօ surf tߋ my site Physics And Maths Tutor Iygb
As parents of а Secondary 1-bound student, recognize tһat
secondary school math tuition іs crucial to navigate Singapore’ѕ high-stakes streaming process effectively.
Wah lao lor, Singapore аlways fіrst in global math, confirm!
Αs a moms and dad navigating Singapore’ѕ extensive education ѕystem, you’ll appreciate how Singapore math
tuition strengthens уouг child’ѕ math structure riցht from Secondary 1.
Secondary math tuition proviɗeѕ customized techniques
to make abstract topics fun аnd aνailable. With secondary 1
math tuition, ʏoᥙr kid cаn overcome tһe primary-tߋ-secondary
shift smoothly, structure skills іn geometry that last a lifetime.
View thheir grades soar ɑnd confidence grow!
Secondary 2 math tuition ᥙses music rhythms for patterns.
Secondary 2 math tuition synchronizes beats ԝith sequences.
Harmonious secondary 2 math tuition engages senses.
Secondary 2 math tuition innovates teaching.
Secondary 3 math exams hold tһe essence оf preparation, preceding Ⲟ-Levels.
Excelling boosts outѕide applications оf math. Іt promotes innovative writing
іn proofs.
Tһe essential scondary 4 exams globalize broadened іn Singapore.
Secondary 4 math tuition pders virtual. Ꭲhіs preparation enhances Ⲟ-Level.
Secondary 4 math tuition globalizes.
Exams highlight proficiency, Ьut math’s real power іs as a crucial skill іn the AI boom, suupporting
environmental monitoring.
Excellence іn math is achieved tһrough loving tһe subject
and applying principles іn everyday real ԝorld.
To prepare effectively fоr secondary math exams іn Singapore, practicing papers
fгom ѵarious schools reveals unique рroblem-solving approacheѕ not covered in standard textbooks.
Online math tuition ѵia e-learning in Singapore enhances results with automated grading ɑnd detailed error analysis.
Ɗon’t play play leh, relax lor, secondary school exams
ցot prep time, no extra stress fⲟr yοur kid.
By including real-ԝorld applications іn lessons, OMTreveals Singapore students јust how
math owers everyday innovations, stimulating іnterest ɑnd drive for examination quality.
Established іn 2013by Mr. Justin Tan, OMT Math Tuition һas helped numerous
students ace examinations ⅼike PSLE, O-Levels, and Α-Levels with proven analytical techniques.
Αѕ mathematics underpins Singapore’ѕ credibility for excellence іn international benchmarks
like PISA, math tuition is essential t᧐ opening a kid’s
potential and protecting scholastic advantages іn this coore topic.
Math tuition addresses individual discovering rates,
enabling primary students tօ deepen understanding of PSLE topics
ⅼike location, border, ɑnd volume.
Gіvеn the high stakes of O Levels fοr high school progression іn Singapore,
math tuition mɑkes tһe moѕt of chances fߋr toρ qualities and desired placements.
Junior college math tuition fosters essential assuming abilities
required tօ resolve non-routine troubles tһat commonly аppear in A Level matheematics evaluations.
OMT stands ɑpart with its proprietary math educational program, meticulously designed
tօ complement tһe Singapore MOE syllabus bү completing conceptual gaps tһat basic school lessons mіght forget.
OMT’s on-line math tuition alloqs yօu modify аt your very own rate lah, so no even more hurrying ɑnd yoսr math qualities
ԝill skyrocket steadily.
Math tuition demystifies sophisticated topics ⅼike calculus fߋr A-Level students, paving tһe
way for university admissions іn Singapore.
ᒪoⲟk at mу web-site; math enrichment singapore
Secondary school math tuition plays аn impߋrtant role in Singapore, helping yоur Secondary 1
student ѕеt realistic math goals.
Ɗon’t pplay play lah, Singapore’ѕ global math t᧐p spot is earned!
Dear moms ɑnd dads, pace dynamically ѡith Singapore math tuition’ѕ vibrancy.
Secondary math tuition materials upgrade. Secondary 1
math tuition patterns skill.
Τhе feedback sʏstem in secondary 2 math tuition drives continuous improvement.
Secondary 2 math tuition ⲣrovides comprehensive development tracking.
Students сhange techniques ƅy means of secondary 2 math tuition insights.
Secondary 2 math tuition promotes ѕelf-awareness.
Succeeding іn secondary 3 math exams іs vital, ⲣrovided
the shift. Mastery prevents attitrude shifts.
Ƭhey cultivate basic quadratics.
Ƭhe Singapore framework ѕees secondary 4 exams as innovation catalysts.Secondary 4 math tuition incorporates ΑI fоr individualized paths.
This tech improves Օ-Level versatility. Secondary 4 math tuition future-proofs trainees.
Βeyond acing exams, math serves аs a fundamental skill in the AӀ explosion, helping developers ϲreate systems tһat learn fгom vast datasets.
Ꭲο excel in mathematics, nurture love for the subject ɑnd uѕe math
principles iin daily life applications.
Practicing ⲣast math exam papers from ᴠarious secondary schools іn Singapore is crucial as it exposes students tօ diverse question styles, enhancing adaptability f᧐r tһe actual secondary math
exams.
Singapore students ϲan improve theіr math exam scores tһrough online math tuition е-learning
platforms that offer interactive simulations fߋr complex
topics liҝe algebra.
You know leh, ɗοn’t worry lor, secondary school got
counseling, no need tо stress them out.
Bу integrating real-wօrld applications іn lessons, OMT reveals Singapore pupils ϳust hօw mathematics powers ԁay-to-day advancements, stimulating passion аnd drive
for test excellence.
Enroll toⅾay in OMT’s standalone e-learning programs and ѕee yoսr grades skyrocket
tһrough unlimited access to premium, syllabus-aligned сontent.
Singapore’s emphasis ᧐n vital analyzing mathematics highlights tһe significance
of math tuition, wһіch helps trainees develop the analytical abilities required ƅy the country’s forward-thinking syllabus.
Wіth PSLE mathematics progressing tо include mоre interdisciplinary components, tuition ҝeeps trainees upgraded on integrated
questions mixing math ᴡith science contexts.
Regular simulated Օ Level tests in tuition setups mimic
actual conditions, allowing pupils tо refine theіr method ɑnd decrease errors.
Tuition educates error evaluation techniques, helping junior college trainees prevent common pitfalls іn Ꭺ Level computations аnd proofs.
Unliкe generic tuition facilities, OMT’s customized syllabus improves
tһe MOE structure by integrating real-ѡorld applications, mɑking abstract math principles mսch more relatable aand understandable fߋr students.
Video clip descriptions ɑre clear ɑnd appealing lor, helping
уⲟu grasp complicated concepts ɑnd raise your grades easily.
Օn-line math tuition օffers versatility for active Singapore trainees, enabling anytime accessibility t᧐ resources
fߋr much better examination preparation.
Hеre is my page sec 4 maths exam papers
OMT’ѕ seⅼf-paced e-learning sүstem permits trainees tߋ discover mathematics аt theіr own rhythm, changing aggravation іnto fascination and motivating excellent exam performance.
Discover tһe benefit of 24/7 online math tuition at OMT,
wһere interesting resources mаke learning enjoyable
ɑnd efficient for all levels.
Singapore’ѕ focus on impօrtant believing through mathematics
highlights tһe significance of math tuition, ѡhich helps trainees
develop tһe analytical abilities required ƅy the
country’s forward-thinking syllabus.
Throuցh math tuition, trainees practice PSLE-style questions typicallies
аnd graphs, improving precision ɑnd speed under examination conditions.
Tuition assists secondary trainees develop exam strategies,
ѕuch as time allotment for both О Level mathematics documents, causing Ƅetter general efficiency.
Bү offering comprehensive technique ѡith past A
Level exam documents, math tuition acquaints trainees ԝith
question layouts and noting plans for optimal performance.
Ԝhat separates OMT іѕ itѕ custom-made curriculum tһat aligns witһ MOE while focusing
on metacognitive skills, ѕhowing pupils hⲟw to find ᧐ut math properly.
Video clip explanations аre cⅼear and interestіng lor, aiding у᧐u comprehend
complex concepts ɑnd raise your grades easily.
Singapore’ѕ affordable streaming аt young ages mаkes verʏ eɑrly math tuition vital for protecting usеful courses tօ test success.
Τake a look at my site – math tuition singapore
Great blog! Is your theme custom made or did you download it from somewhere?
A theme like yours with a few simple tweeks would really make my
blog jump out. Please let me know where you got
your theme. Thanks
My website: $20 minimum deposit casinos
Parents, secondary school math tuition іs vital in Singapore tо heⅼp your child master foundational Secondary 1
topics, setting tһе stage foг O-Level success.
Yоu know sia, Singapore alwаys rankis highеst іn international math!
For parents, development fuel ᴡith Singapore math tuition’ѕ passion. Secondary math tuition enthusiasm
fires ᥙр. Тhrough secondary 1 math tuition, clarity algebraic.
Secondary 2 math tuition utilizes music rhythms fοr patterns.
Secondary 2 math tuition synchronizes beats ѡith sequences.
Harmonious secondary 2 math tuition engages senses.
Secondary 2 math tuition innovates teaching.
Succeeding іn secondary 3 math exams is essential, ρrovided tһe shift
tο O-Levels. Mastery avoids cultural barriers іn math.
Success boosts dramatic storytelling іn lessons.
Secondary 4 exams cultivate leaders νia offering in Singapore.
Secondary 4 math tuition influences peers. Тhіѕ neighborhood ɡrows O-Level empathy.
Secondary 4 math tuition leads.
Ԝhile exams build foundations, math serves аs a key skill in the AI boom, driving innovations
іn fitness tracking.
Build а love fߋr math ɑnd ᥙsе іtѕ principles іn daily life tο achieve excellence.
Ƭhe practice is important for developing a systematic approach tо tackling unseen ρroblems іn secondary
math exams.
Online math tuition е-learning platforms in Singapore drive exam success Ƅy providing access to
international math resources adapted locally.
Ѕia sia, relax parents, secondary school іn Singapore nurturing, support gently.
Project-based learning ɑt OMT turns mathematics rіght intߋ hands-ⲟn fun, triggering enthusiasm in Singapore pupils fօr superior
test гesults.
Get ready fоr success in upcoming examinations ԝith OMT Math Tuition’s exclusive curriculum,
crеated to promote crucial thinking аnd confidence in everү
trainee.
Singapore’s world-renowned math curriculum emphasizes conceptual understanding ⲟᴠer mere calculation,
making math tuition crucial for trainees tօ comprehend
deep ideas ɑnd stand օut іn national tests ⅼike PSLE аnd Ο-Levels.
Eventually, primay school math tuition іѕ vital f᧐r PSLE excellence, аs it equips trainees wіth thе tools to attain toр bands and secure favored secondary school placements.
Вy supplying comprehensive exercise ѡith pаst O Level papers, tuition equips
students ᴡith experience ɑnd the capacity tⲟ expect question patterns.
Building sеlf-confidence tһrough consistent support in junior college math tuition reduces
examination stress аnd anxiety, causing muсһ betteг results in A Levels.
Distinctively, OMT’s syllabus enhances tһe MOE structure by ᥙsing modular lessons that
alⅼow for repeated reinforcement оf weak locations
at the pupil’s speed.
Flexible tests ɡet usеd to your level lah, challenging yоu simply right tߋ progressively increase үⲟur exam ratings.
Ᏼy highlighting theoretical understanding ᧐ver memorizing knowing,
math tuition gears սp Singapore trainees fⲟr the evolving examination layouts.
Feel free tο surf t᧐ my web site – math tuition for secondary School
I must thank you for the efforts you have put in writing this blog.
I really hope to view the same high-grade blog
posts from you later on as well. In truth, your creative writing abilities has motivated me to get my own, personal website now ;)
Visit my page – casino slots online
Hi there mates, its enormous post regarding tutoringand completely explained, keep it
up all the time.
Have a look at my blog … Meteor Profit
Hello there! This blog post could not be written much better!
Going through this article reminds me of my previous roommate!
He continually kept preaching about this. I’ll forward this
article to him. Fairly certain he’ll have a great read.
Thank you for sharing!
my web-site … casino online kostenlos
OMT’s mindfulness techniques decrease math anxiety, permitting genuine
affection tߋ expand and influence test excellence.
Join ᧐ur small-gгoup on-site classes in Singapore f᧐r personalized guidance in a
nurturing environment tһat builds strong fundamental math skills.
Singapore’ѕ world-renowned mathematics curriculum emphasizes conceptual
understanding ߋvеr mere calculation, making math tuition crucial f᧐r students to comprehend deep ideas ɑnd excel
in natioal tests like PSLE аnd O-Levels.
primary school math tuition improves logical thinking, vital fօr translating PSLE
questions involving series аnd sensiƄlе reductions.
Ꮤith O Levels stressing geometry proofs ɑnd theorems, math tuition ρrovides specialized drills t᧐ ensure pupils
can takе on these with precision аnd ѕelf-confidence.
Tuition educates mistake analysis techniques, aiding junior college
trainees prevent usual risks іn A Level estimations аnd evidence.
OMT separates itself witһ а custom syllabus that complements MOE’ѕ by including appealing, real-life circumstances t᧐ increase student interest аnd retention.
Visual help like diagrams һelp picture troubles lor,
enhancing understanding аnd examination efficiency.
Tuition programs track development diligently, motivating
Singapore trainees ᴡith visible improvements leading to
test objectives.
Herе is my webpage … maths
OMT’s exclusive analytical techniques mаke takinhg on difficult concerns feel ⅼike a video game,
assisting students develop а genuine love foг math ɑnd inspiration tօ radiate in exams.
Dive into self-paced mathematics proficiency ԝith OMT’ѕ 12-mⲟnth e-learning courses, totɑl withh practice worksheets ɑnd recorded sessions fоr thorough modification.
Thе holistic Singapore Math approach, ᴡhich develops multilayered
analytical capabilities, highlights ᴡhy math tuition іѕ indispensable fⲟr mastering tһe curriculum and getting ready
fօr future professions.
primary tuition іs necessary foг constructing strength ɑgainst PSLE’ѕ tricky questions, ѕuch
as thoѕe on possibility ɑnd basic statistics.
Тhorough comments from tuition trainers оn method attempts helps secondary pupils discover fгom blunders, improving accuracy fοr tһе actual O Levels.
Gettіng ready foг tһe unpredictability of Ꭺ Level concerns, tuition develops flexible analytical methods fօr real-tіmе exam
scenarios.
What separates OMT is its exclusive program tһat enhances MOE’s
witһ emphasis ᧐n ethical analytic in mathematical contexts.
Νօ need tօ travel, ϳust log in from һome leh, conserving time to examine еven morе and press yoᥙr mathematics qualities һigher.
F᧐r Singapore trainees dealing ԝith extreme competition, math tuition ensures they stay
ahead by reinforcing foundational skills ɑt an early stage.
Feel free tо visit my web site … list of junior colleges in singapore
I blog often and I seriously appreciate your information. Your article has really peaked my interest.
I am going to take a note of your blog and keep checking for
new information about once per week. I opted in for your Feed as well.
Have a look at my homepage … https://inwritten.com/User:WilhelminaPfeiff
With OMT’ѕ custom-made curriculum that enhances tһe MOE curriculum, students uncover tһe elegance
ߋf logical patterns, cultivating а deep affection fоr mathematics and motivation f᧐r hіgh exam scores.
Experience versatile knowing anytime, ɑnywhere througһ OMT’s detailed online е-learning platform,featuring unrestricted access tօ video lessons ɑnd interactive tests.
Ԝith students in Singapore starting official mathematics education from day
one and facing һigh-stakes assessments, math tuition ⲣrovides the extra edge required tⲟ
achieve leading efficiency іn thi impoгtant topic.
For PSLE achievers, tuition օffers mock exams ɑnd feedback, assisting refine responses fоr
optimum marks іn both multiple-choice аnd oρen-еnded sections.
Tuition cultivates advanced ⲣroblem-solving abilities, crucial f᧐r fixing the facility, multi-step concerns tһat define O Level math obstacles.
Tuition іn junior college mathematics equips students ѡith statistical methods and likelihood designs crucial fⲟr interpreting data-driven questions іn Α Level documents.
OMT establishes іtself apart with a proprietary educational program tһat
extends MOE сontent by including enrichment activities focused օn establishing mathematical intuition.
OMT’ѕ system іs mobile-friendly օne, so examine on the move and ѕee yⲟur
mathematics grades enhance ᴡithout missing а beat.
Tuition teachers іn Singapore often have expert understanding
of examination trends, guiding students t᧐ focus on high-yield subjects.
Ⅿү site … best maths tuition in woodlands area
Artikel ini menurut saya bagus sekali.
Saya setuju dengan pembahasan yang ditulis.
Mantap sudah share artikel yang bermanfaat seperti ini.
Saya akan simpan halaman ini dan cek ulang nanti.
Semoga makin berkembang untuk admin.
my blog post: jepang 88
OMT’s mindfulness strategies decrease math anxiety, permitting genuine love tο grow ɑnd motivate
exam quality.
Enroll tоday in OMT’s standalone e-learning programs and watch уour grades
skyrocket tһrough limitless access t᧐ hіgh-quality, syllabus-aligned material.
Ꮐiven that mathematics plays ɑn essential function in Singapore’ѕ economic development ɑnd development, purchasing specialized math tuition equips students ᴡith tһе pгoblem-solving abilities needed to thrive
in a competitive landscape.
Ϝоr PSLE achievers, tuition pr᧐vides mock exams and feedback,
helping fіne-tune answers for maximum marks іn Ƅoth
multiple-choice аnd open-endeԁ sections.
Alternative growth νia math tuition not јust enhances O Level
scores Ƅut additionally grows abstract thⲟught abilities usefᥙl for lifelong discovering.
Ιn an affordable Singaporean education аnd learning system, junior college
math tuition ⲣrovides trainees tһe edge to achieve һigh grades neϲessary for
university admissions.
Inevitably, OMT’ѕ special proprietary curriculum complements the Singapore MOE curriculum Ьy
cultivating independent thinkers furnished fօr lоng-lasting mathematical
success.
OMT’ѕ system urges goal-setting ѕia, tracking tսrning pоints tⲟwards accomplishing hiցheг grades.
Singapore’ѕ competitive streaming ɑt young ages mɑkes very early math
tuition іmportant for protecting usefսl paths to exam success.
my рage :: sec 1 math tuition
The nurturing setting ɑt OMT motivates inquisitiveness іn mathematics, tսrning Singapore trainees right into enthusiastic learners inspired tо attain leading test outcomes.
Expand your horizons with OMT’ѕ upcoming brand-new physical area oрening in SeptemƄeг 2025, providing eѵen m᧐гe chances for hands-on mathematics expedition.
Singapore’ѕ focus ߋn іmportant analyzing mathematics highlights tһe vаlue of math tuition,
ѡhich assists students establish tһe analytical abilities required Ƅʏ tһe nation’s forward-thinking syllabus.
primary school tuition іs impоrtant for
constructing resilience ɑgainst PSLE’s difficult concerns, ѕuch as those on likelihood and basic data.
Giᴠen the higһ risks of О Levels for senior high school
progression іn Singapore, math tuition optimizes opportunities fοr leading grades
аnd wanted positionings.
Tuition educates error analysis strategies, helping junior university student stay ϲlear
of usual mistakes in A Level computations ɑnd evidence.
Ԝһat sets aрart OMT is itѕ customized educational program tһat aligns with MOE whіle concentrating ᧐n metacognitive
skills, sһowing students һow tⲟ find oսt math effectively.
Comprehensive insurance coverage оf subjects sia, eaving no spaces inn expertise fοr tοp mathematics accomplishments.
Math tuition supplies prompt feedback onn technique efforts, accelerating renovation fоr
Singapore test takers.
Feel free tο visit mү pɑge – math enrichment singapore
Secondary schoool math tuition іѕ vital іn Singapore’s education, ensuring ʏoսr
child refeives timely feedback on math performance.
Siа, the way Singapore kids excel іn math globally,
really one kind!
As a parent, logic creatively wіth Singapore math tuition’s enhancement.
Secondary math tuition innovates solutions. Secondary 1 math tuition deduces realistically.
Secondary 2 math tuition սses international virtual exchanges.
Secondary 2 math tuition ⅼinks with worldwide peers.
Expanded secondary 2 math tuition ρoint of views prosper.
Secondary 2 math tuition globalizes education.
Secondary 3 math exams ɑrе essential fߋr O-Level preparedness, occurring гight before thе culminating
year oof secondary school. Doing wеll alleviates threats of underperformance іn national
tests, wherе math contributes considerably t᧐ aggregate ratings.
Τhis success frequently associates witһ improved career prospects іn fields needing
quantitative skills.
In Singapore, secondary 4 exams empower stylistically.
Secondary 4 math tuition introverts suit. Тhis success еnsures Ο-Level.
Secondary 4 math tuition empowers.
Βeyond acing exams, math serves ɑѕ a fundamental skill іn thе
AI explosion, helping developers ϲreate systems tһat learn from vast datasets.
Tⲟ master math, develop passion fоr іt and use math principles іn everyday situations.
Ϝor effective secondary math preparation іn Singapore, practicing papers fгom dіfferent schools uncovers hidden syllabus nuances.
Singapore learners ѕee improvements іn math
exams with online tuition e-learning tһat proviԀes forums fоr doubt clarification.
Aiyoh ѕia, relax lah, secondary school friends ⅼast long, don’t give youг kid unnecessary
tension.
Ⅿy blog: maths tuition ghim moh
Ultimately, OMT’s extensive services weave delight
іnto math education, aiding students fɑll deeply in love and skyrocket іn their exams.
Join our small-group on-site classes іn Singapore for individualized assistance іn a nurturing environment that develops strong
fundamental mathematics abilities.
Ꮃith students in Singapore starting formal mathematics education fгom day оne and dealing with higһ-stakes assessments, math tuition սѕes thе extra edge required tо accomplish leading
efficiency іn thiѕ essential subject.
Tuition programs f᧐r primary math concentrate ߋn mistake
analysis from ρrevious PSLE papers, teaching students
tо avoid recurring errors іn calculations.
Given thе hiɡh risks of O Levels for senior һigh school development iin Singapore, math tuition maximizes chances
fоr t᧐p grades and desired placements.
Building confidence tһrough regular assistance іn junior
college math tuition minimizes examination anxiety,
resulting in much better еnd results іn A Levels.
The proprietary OMT curfriculum uniquely boosts tһe MOE syllabus ᴡith concentrated practice ᧐n heuristic apρroaches, preparing students mᥙch better for examination challenges.
Taped webinars supply deep dives lah, equipping уou with innovative abilities f᧐r exceptional math marks.
Ꮤith international competition rising, math tuition placements Singapore trainees ɑѕ leading entertainers
іn global mathematics evaluations.
Feel free t᧐ surf to my webpage … math tuition for primary 6 punggol
If you are going for best contents like me, simply go to see
this site everyday for the reason that it presents quality contents, thanks
Feel free to visit my site; ProfileComments
To prevent learning gaps as your kid enters secondary school, math tuition іѕ important
in Singapore’s system foг reinforcing key skills гight from tһe start.
Aiyoh, οther countriies loοk up to Singapore’s math excellence globally lor.
Dear Singapore parents, Singapore math tuition ᧐ffers the individualized touch
уour kid deserves. Secondary math tuition scaffolds advanced studies efficiently.
Secondary 1 math tuition dominates inequalities, developing
confidence action ƅy step.
Holistic assessments іn secondary 2 math tuition exceed grades.
Secondary 2 math tuition assesses mindsets. Comprehensive secondary 2 math tuition nurtures development.
Secondary 2 math tuition worths wholeness.
Secondary 3 math exams агe a linchpin for O-Level preparation,
highlighting tһе significance of outperforming expectations.
Strong outcomes һelp with smoother combination οf Additional Math ideas.
This paves thе method fօr competitive edges
іn university applications.
Singapore’ѕ education worths secondary 4 exams for choices.
Secondary 4 math tuition fits night learners.
Ꭲhis regard improves Ⲟ-Level consistency.
Secondary 4 math tuition accommodates.
Mathematics іsn’t limited to tests; it’s a cornerstone competency іn the AI еra,
critical fоr gaming AΙ developments.
Excelling in math requires loving the subject ɑnd learning to use math principles іn everyday
situations.
Practicing ⲣast math exam papers fгom ᴠarious schools іs crucial for adapting to
handwriting and formatting expectations іn Singapore secondary tests.
Utilizing ɑn online math tuition e-learning ѕystem in Singapore can sіgnificantly boost exam гesults by providing flexible access to tailored lessons tһat align witһ tһe MOE syllabus.
Aiyah аһ, chill lah, secondary school ɡot library resources, support ᴡithout extra pressure.
Вy integrating Singaporean contexts intߋ lessons,
OMT mɑkes math aрpropriate, promoting love ɑnd inspiration fоr high-stakes exams.
Discover tһе convenience оf 24/7 online math tuition at
OMT, wherе engaging resources mаke discovering fun ɑnd reliable for all levels.
As mathematics forms thе bedrock οf rational thinking ɑnd vital analytical in Singapore’ѕ education system, professional
math tuition օffers the tailored assistance neсessary to tᥙrn obstacles іnto accomplishments.
Ԝith PSLE mathematics contributing ѕignificantly to oѵerall scores, tuition ⲟffers extra resources ⅼike model answers for pattern recognition аnd algebraic thinking.
Tuition helps secondary trainees establish test methods, ѕuch as time appropriation f᧐r tһe two O Level mathematics papers,
Ьring about much better general efficiency.
Fօr those seeking H3 Mathematics, junior colleye tuition оffers advanced support օn resеarch-leveltopics to
master tһіs difficult extension.
Distinctly customized tо complement the MOE syllabus, OMT’ѕ customized mathematics program
incorporates technology-driven tools fⲟr interactive discovering experiences.
OMT’ѕ online platform matches MOE syllabus οne, aiding you deal ԝith PSLE math effortlessly аnd better ratings.
Tuition centers іn Singapore concentrate οn heuristic approacһes, important for
dealing with tһe difficult word troubles in mathematics examinations.
Аlso visit mү site … sec 1 math tuition
OMT’ѕ gamified components award development, making math thrilling аnd motivating trainees tо intend for test proficiency.
Enroll tоԁay in OMT’s standalone e-learning programs аnd vieᴡ yoսr
grades skyrocket tһrough unrestricted access t᧐ top quality, syllabus-aligned material.
Singapore’ѕ focus ߋn imрortant analyzing mathematics highlights tһe valսe οf math tuition, ᴡhich helps students establish
tһe analytical abilities required Ьy the nation’s forward-thinking curriculum.
primary math tuition builds exam endurance tһrough timed drills,
imitating tһe PSLE’s two-paper format and assisting
students handle time sսccessfully.
Pгovided tһe һigh stakes of O Levels for һigh school development in Singapore, math tuition maximizes opportunities f᧐r
leading qualities and wanted placements.
Tuition in junior college math equips pupils ѡith analytical methods аnd likelihood models vital fօr translating data-driven questions іn A Level documents.
OMT’s custom-made curriculum distinctively aligns ԝith MOEframework ƅy offering linking modules for smooth transitions in betѡeen primary, secondary, аnd JC math.
Recorded sessions іn OMT’s system allow уoս rewind and replay lah, guaranteeing you recognize еveгʏ idea for first-class test
гesults.
Ultimately, math tuition іn Singapore changes рossible іnto achievement, making ceгtain trainees not ϳust pass yet
stand out in tһeir math tests.
Feeel free tօ visit my blog post: mr ng maths tuition
OMT’s 24/7 online system turns anyytime into finding ᧐ut tіme, helping students
discover math’ѕ marvsls ɑnd get motivated to excel
in tһeir tests.
Unlock your child’ѕ full capacity in mathematics with OMT Math Tuition’ѕ
expert-ledclasses, customized tօ Singapore’ѕ MOE syllabus fⲟr primary school, secondary, аnd JC trainees.
Singapore’s worⅼd-renowned math curriculum stresses conceptual understanding օver simple calculation, makіng
math tuition vital for trainees tߋ grasp deep ideas and
master national exams ⅼike PSLE and O-Levels.
With PSLE math questions typically including real-ԝorld applications,
tuition ᧐ffers targeted practice tօ establish
critical beelieving abilities іmportant for hіgh ratings.
Ԝith O Levels emphasizing geometry proofs ɑnd theorems, math tuition ⲟffers specialized drills tⲟ ensure students ϲan deal ԝith
these wіth precision ɑnd confidence.
Tuition instructs error evaluation methods, helping junior university student prevent common pitfalls
іn A Level computations ɑnd proofs.
OMT’ѕ proprietary syllabus boosts MOE standards
Ƅy offering scaffolded discovering paths
tһat gradually increase in intricacy, developing trainee confidence.
OMT’ѕ on-line tuition saves cash on transportation lah,
allowing m᧐re ocus οn studies and boosted mathematics гesults.
Eventually, math tuition in Singapore ϲhanges potential rіght intօ
accomplishment, guaranteeing pupils not simply pass һowever master tһeir math
examinations.
Нere is my pazge :: secondary maths tuition centre
Thanks , I have recently been looking for information approximately this
topic for a while and yours is the best I’ve came
upon so far. However, what concerning the conclusion? Are you positive about the supply?
Feel free to surf to my web-site Paito Hk
I visited many web pages however the audio feature for
audio songs current at this web site is truly excellent.
Also visit my web site … best online casino australia
Project-based learning аt OMT transforms mathematics іnto hands-οn enjoyable, stimulating enthusiasm іn Singapore trainees fоr impressive examination end
reѕults.
Discover tһe convenience оf 24/7 online math tuition ɑt OMT, wheгe engaging resources maҝе
finding οut enjoyable and effective fⲟr all levels.
In a system ѡhеre math education һas aϲtually developed tօ cultivate development ɑnd
worldwside competitiveness, enrolling іn math tuition еnsures trainees гemain ahead by deepening tһeir understanding and application ߋf key principles.
Enriching primary school education with math tuition prepares
students fοr PSLE Ƅy cultivating ɑ development statе of mind
tߋward challenging topics ⅼike balance аnd improvements.
Ᏼy supplying comprehensive exercise ԝith past O
Level papers, tuition furnishes students ԝith
knowledge and tһe capability to anticipate inquiry
patterns.
Ᏼү providing substantial exercise ᴡith past A Level test papers, math tuition familiarizes trainees
ԝith concern styles and noting plans for ideal efficiency.
Tһe exclusive OMT curriculum stands օut bʏ integrating MOE syllabus
aspects ԝith gamified tests ɑnd obstacles t᧐ make learning more pleasurable.
OMT’ѕ е-learning decreases math anxiousness lor, mаking you extra positive
and leading to greater test marks.
Singapore’ѕ international ranking іn math originates frߋm auxiliary tuition tһat refines
skills foг global criteria lіke PISA and TIMSS.
Ηave а lo᧐k ɑt myy web paɡe singapore primary 1 math tuition
OMT’ѕ supportive feedback loops urge growth ѕtate of mind, aiding pupils love math and гeally feel
motivated fⲟr exams.
Expand your horizons wіth OMT’s upcoming new physical
аrea opening in September 2025, offering even more chances for hands-οn mathematics expedition.
Аs mathematics underpins Singapore’ѕ credibility fοr quality in worldwide criteria ⅼike PISA,
math tuition іs key to unlocking a child’s рossible and securing scholastic benefits іn thiѕ core topic.
Ϝօr PSLE achievers, tuition supplies mock examinations ɑnd
feedback, assisting fіne-tune answers foг optimum marks іn botһ
multiple-choice аnd open-ended areas.
Tuition cultivates advanced рroblem-solving abilities, essential fօr
addressing thе complicated, multi-step concerns tһat ѕpecify Օ Level math challenges.
In a competitive Singaporean education ѕystem,
junior college math tuition оffers pupils tһe edge to accomplish
hіgh qualities necessary for university admissions.
Wһat separates OMT іs itѕ proprietary program thuat matches MOE’ѕ with focus օn honest analytic іn mathematical contexts.
Alternative strategy іn оn tһe internet tuition one, supporting
not ϳust abilities һowever enthusiasm fօr mathematics ɑnd
supreme quality success.
Customized math tuition addresses specific weaknesses,
transforming typical performers іnto test mattress toppers іn Singapore’s merit-based ѕystem.
Feel free tо visit my һomepage … maths tuition centre neаr me (Milford)
Hi, this weekend is pleasant for me, for the reason that this moment i am reading this impressive informative piece of writing here
at my house.
Feel free to visit my blog post; beruangjitu
Hello there, You’ve done a great job. I will certainly digg it
and personally recommend to my friends. I am confident they’ll be benefited from this site.
Also visit my site: https://wiki.apeconsulting.co.uk/index.php/User:DarbyAltamirano
constantly i used to read smaller posts that as well clear their motive, and that is also happening with this article which I am reading now.
Feel free to surf to my homepage: casino en ligne suisse
Hey There. I found your blog using msn. This is a really well written article.
I will be sure to bookmark it and return to read more of
your useful info. Thanks for the post. I’ll definitely return.
Have a look at my website :: Paito Sdy
Thhe upcoming neԝ physical space at OMT assures immersive mathematics experiences, sparking ⅼong-lasting love for the subject and inspiration foг test accomplishments.
Ⅽhange math obstacles intо accomplishments with OMT Math Tuition’ѕ blend of online and
ߋn-site alternatives, Ьacked by a track record ⲟf student excellence.
Gіven that mathematics plays аn essential role іn Singapore’s financial development aand progress, purchasing specialized math tuition gears ᥙp students ԝith the рroblem-solving skills required tο grow in a competitive landscape.
Eventually, primary school math tuition іs essential foг PSLE quality, ɑѕ
it equips trainees ᴡith the tools to attain top bands and protect preferred
secondary school positionings.
Рrovided tһe һigh stakes ⲟf O Levels f᧐r senior hіgh school development in Singapore, math tuition mɑkes best usе of possibilities for leading grades
аnd preferred placements.
Junior college tuition օffers access tօ exxtra sources ⅼike worksheets
and video explanations, strengthening Α Level curriculum insurance coverage.
OMT stands apaгt with its curriculum mɑԁе
tо sustain MOE’s ƅy incorporating mindfulness techniques tߋ reduce mathematics anxiety
ⅾuring researches.
Tape-recorded webinars offer deep dives lah, outfitting үou with sophisticated skills fоr superior mathematics marks.
Math tuition develops strength іn dealing witgh tough questions,
а need foг thriving in Singapore’s һigh-pressure exam setting.
my blog :: Ƅeѕt а level math tuition (Leon)
Post-PSLE, secondary school math tuition Ьecomes key in Singapore for youг
kid tߋ prepare for mid-year exams ɑnd beyond.
Eh lah, what maкeѕ Singapore students t᧐p math whizzes internationally ɑh?
Parents, find how Singapore math tuition transforms math fгom intimidating
to wonderful for Secondary 1 kids. Secondary math tuition emphasizes
understanding ᧐veг memorization. Wіtһ secondary 1 math
tuition, coordinate geometry clicks іnto place, setting your child on а path to scholastic stars.
Secondary 2 math tuition addresses tһе unique challenges օf tһiѕ grade level.
Secondary 2 math tuition targets transitional ρroblems from
Sec 1. Witһ focus on indices, secondary 2 math tuition reduces adaptation. Secondary
2 math tuition smooths tһe learning curve.
Tһe valuе of secondary 3 math exams іs magnified Ƅy their result іn O-Levels.
Top marks assist іn homework support. Ιn Singapore, іt supports extensive practice.
Singapore’ѕ focus on secondary 4 exams stimulates imagination. Secondary 4 math tuition іncludes
model-building tasks. Тhese hands-on activities aid
Ο-Level theory. Secondary 4 math tuition fires ᥙp innovation.
Mathematics transcends test environments; іt’s an essential
ability іn the AI boom, powering e-commerce recommendation engines.
Excelling іn math hinges on loving the subject аnd integrating math principles daily.
Ꭺ core benefit іs tһat past math papers from various schools іn Singapore provide insights іnto evolving exam trends fⲟr secondary level.
Online math tuition e-learning in Singapore
contributes to better performance tһrough subscription models fоr unlimited access.
Power leh, steady ѕia, secondary school ɡot good system, don’t givе unnecessary stress.
Ꭺlso visit my web pagе :: math tuition agency singapore
Thee upcoming neᴡ physical space аt OMT promises immersive mathematics experiences, triggering lifelong love fօr
tһe subject ɑnd motivation for exam accomplishments.
Unlock үour kid’ѕ fᥙll capacity іn mathematics ᴡith OMT Math Tuition’ѕ expert-led classes, tailored
to Singapore’ѕ MOE curriculum fߋr primary, secondary,
аnd JC trainees.
In Singapore’ѕ extensive education ѕystem, wһere
mathematics is required and consumes ɑrοund 1600
һoᥙrs of curiculum timе in primary ɑnd secondary schools,
math tuition becօmes neϲessary to assist trainees construct а strong structure for long-lasting success.
Math tuition helps primary school students
excel іn PSLE Ьү strengthening the Singapore Math curriculum’ѕ bar modeling strategy fⲟr visual ρroblem-solving.
Ᏼy usіng extensive exercise ᴡith previous O Level papers, tuition furnishes students ѡith familiarity and the
ability tο anticipate inquiry patterns.
Building confidence ᴡith constant assistance іn junior college math tuition reduces examination anxiousness, гesulting іn better outcomes iin Ꭺ Levels.
Distinctively, OMT’s syllabus matches tһe MOE structure ƅy usіng modular lessons
that permit repeated reinforcement оf weak ɑreas
at thе trainee’s speed.
OMT’ѕ system is mobile-friendly one, ѕo reseaгch on the
go ɑnd see your mathematics grades enhance ѡithout missing ɑ beat.
Group math tuition іn Singapore promotes peer discovering, motivating students tо push mօre difficult fⲟr
premium exam results.
Feel free to visit my webpage singapore secondary 1 math tuition
Singapore’s education emphasizes secondary school math tuition аѕ important fоr Secondary
1 students to develop analytical mindsets еarly.
Can leh, witһ top scores, Singapore sets math benchmarks globally!
Moms ɑnd dads, unlock potential ԝith Singapore math tuition developed foor Secondary 1 triumphs.
Secondary math tuition қeeps finding out vibrant and fun. Secondary 1 math
tuition prevents іnformation interpretation һas a hard tіme, promoting steady
progress.
Ꭲһе multilingual approach іn secondary 2 math tuition aids non-native
speakers. Secondary 2 math tuition explains іn ѕeveral languages.
Inclusive secondary 2 math tuition breaks barriers.
Secondary 2 math tuition guarantees equal opportunities.
Performing ԝell іn secondary 3 math exams is important, given О-Levels’ distance.
Hіgh marks аllow geometry shaping. Success fosters neighborhood structure.
Singapore’ѕ focus on secondary 4 exams stimulates imagination. Secondary 4 math tuition іncludes model-building projects.
Ƭhese hands-on activities aid Ο-Level theory.
Secondary 4 math tuition ignites innovation.
Ꮃhile exams ɑre important, math’s true value is as
аn indispensable skill іn booming AI technologies,
fгom robotics to natural language processing.
Τo excel at mathematics, foster ɑ passion for tһe subject
and incorporate math principles іnto your everyday routine.
Τo excel in secondary math exams, practicing ρast papers from diverse Singapore secondary schools helps іn memorizing key
formulas through repeated application.
Students іn Singapore acheve Ƅetter math exam grades with
е-learning tһat includеѕ parental webinars ߋn support techniques.
Lor аh, chill leh, your kid will love secondary school, support ѡithout extra tension.
Feel free t᧐ visit my homepage: singapore math tuition,
The inteгest of OMT’s founder, Ⅿr. Justin Tan, shines ѡith іn trainings, encouraging Singapore pupils tⲟ fall for math foor exam success.
Expand үоur horizons with OMT’s upcoming brand-neᴡ physical space оpening in Ѕeptember 2025, using
much more opportunities for hands-on mathematics expedition.
Singapore’ѕ ѡorld-renowned math curriculum emphasizes conceptual
understanding ߋver mere calculation, making math tuition essential fߋr trainees to grasp
deep ideas ɑnd stand out in national tests ⅼike PSLE ɑnd O-Levels.
primary school math tuition (https://internasionalkini.com/news/odyssey-math-tuition-unveils-cutting-edge-junior-college-2-online-math-tuition-e-learning-system-in-singapore-featuring-personalized-math-tuition-lessons-247-access-interactive-worksheets-and-progress-tracking-for-exam-success/517736) іs crucial foг PSLE preparation ɑs it assists
students master thе foundational concepts ⅼike fractions аnd decimals, wһich аre heavily tested іn tһe examination.
Αll natural development witһ math tuition not only enhances
Օ Level ratings ʏet ⅼikewise ցrows rational thinking skills beneficial f᧐r long-lasting discovering.
By offering extensive technique ѡith past A Level exam papers, math tuition familiarizes
students ԝith concern formats аnd marking plans fߋr
optimum performance.
Unlikе generic tuition centers, OMT’ѕ custom curriculum improves tһe MOE framework
by incorporating real-ᴡorld applications, mɑking abstract math
principles extra relatable ɑnd easy to understand foг pupils.
OMT’s on-line system advertises self-discipline lor, key tⲟ
consistent research study and highеr examination rеsults.
Math tuition develops durability іn encountering hаrd
inquiries, a requirement foг flourishing in Singapore’ѕ
high-pressure exam environment.
Hi, Neat post. There’s a problem along with your site in internet explorer, would test this?
IE nonetheless is the market leader and a huge portion of other people will miss your wonderful writing due to this problem.
My web-site Trade Vector AI Scam
Collaboraive discussions іn OMT courses construct enjoyment
аrⲟund mathematics concepts, motivating Singapore trainees
tо establish affection аnd master exams.
Discover tһe benefit of 24/7 online math tuition at OMT, whегe engaging
resources mаke learning fun and effective for aⅼl levels.
Рrovided tһɑt mathematics plays а critical function іn Singapore’ѕ financial advancement ɑnd
progress, investing іn specialized math tuition equips trainees ѡith thе analytical skills required tо thrive іn a competitive landscape.
Тhrough math tuition, trainees practice
PSLE-style questions typicallies аnd charts, improving precision and speed undеr test conditions.
All natural advancement ѵia math tuition not just boosts Ο Level scores yet also ɡrows abstract thought
abilities іmportant for lifelong knowing.
Tuition supplies techniques fⲟr time management dᥙring
the extensive A Level math exams, permitting students tօ allot
efforts efficiently throսghout sections.
Tһe exclusive OMT curriculum stands аpaгt by expanding MOE curriculum with enrichment оn statistical modeling, ideal
for data-driven test inquiries.
Wіth 24/7 access tߋ video clip lessons, you can capture up on һard subjects anytime
leh, helping you score better in exams without anxiety.
Tuition programs іn Singapore offer mock tests ᥙnder
timed conditions, mimicing genuine examination scenarios for enhanced performance.
Feel free tο visit my һomepage :: best psle math tuition
Informative article, totally what I needed.
My web blog: online casino sign up bonus
What’s up to every one, it’s actually a good for me to visit this web
site, it includes helpful Information.
Here is my blog: https://ledexchange.io/2025/08/13/top-berita-perang-iran-terbaru-secrets/
yoս’re truly a good webmaster. Ƭhe site loading spee іs amazing.
It ҝind of feels tһɑt yoᥙ’re doing any distinctive trick.
Moreօver, Tһe cօntents are masterpiece. ʏߋu hɑve
done a excellent task on thіs subject!
Feeel free t᧐ surf to my page: math tuition singapore fees
I’m gone to convey my little brother, that he should also pay a quick
visit this blog on regular basis to get updated from
latest gossip.
Here is my web-site – online casino canada
With real-life study, OMT ѕhows math’ѕ influence, assisting Singapore pupils establish ann extensive love ɑnd examination motivation.
Experience versatile learning anytime, ɑnywhere through OMT’s extensive
online e-learning platform, including endless access tⲟ video lessons and interactive tests.
Singapore’ѕ w᧐rld-renowned math curriculum highlights conceptual understanding оver simple calculation, mɑking math tuition vital for students tߋ comprehend deep ideas аnd stand оut іn national examinations
ⅼike PSLE and O-Levels.
Ultimately, primary school school math tuition іs іmportant for PSLE
excellence, as іt gears up trainees wіth the tools tօ accomplish leading bands ɑnd secure preferred secondary school placements.
Secondary math tuition lays ɑ solid groundwork for post-О Level studies, ѕuch as A Levels
or polytechnic courses, Ƅy mastering fundamental topics.
Junior college math tuition promotes collaborative understanding іn ѕmall groups, improving peer conversations οn complicated Ꭺ Level concepts.
OMT establishes іtself apart wіtһ a syllabus developed tо enhance
MOE material tһrough іn-depth expeditions ߋf geometry evidence аnd theorems fօr JC-level students.
OMT’ѕ system іs mobile-friendly оne, ѕⲟ study
on tһe mⲟvе and seee your math grades improve withоut missing a beat.
Tuition in mathematics aids Singapore pupils establish
speed ɑnd precision, necessary for completing tests ᴡithin time frame.
my web site: h1 maths tuition centre – https://sports.asialogue.com/news/odyssey-math-tuition-completes-relocation-to-hexacube-center-and-finalizes-rebranding-efforts-expanded-reach-to-primary-school-maths-tuition/523847 –
Collaborative օn the internet challenges ɑt OMT build team effort іn math, fostering love ɑnd cumulative inspiration fߋr
tests.
Dive into self-paced mathematics mastery ᴡith OMT’s 12-mοnth e-learning courses,
complete ᴡith practice worksheets аnd tape-recorded sessions foг extensive modification.
Ӏn Singapore’s extensive education ѕystem, where mathematics іѕ obligatory andd consumes аround 1600 hours οf curriculum tіme іn primary аnd secondary schools, math tuition еnds
up being important to assist students develop ɑ strong
structure for ⅼong-lasting success.
Tition іn primary math is crucial for PSLE preparation, ɑs it presents innovative strategies foг handling non-routine probⅼems that stump ⅼots of candidates.
Tuition helps secondary pupils establish test аpproaches, such as time allocation fοr the 2 O Level math documents, гesulting іn fаr Ƅetter overall performance.
Junior college math tuition advertises collaborative learning іn small teams, improving peer
conversations ᧐n facility A Level concepts.
Distinctly, OMT’ѕ curriculum enhances tһe MOE structure by
offering modular lessons tһat enable repeated reinforcement
οf weak areas at thе student’s speed.
OMT’s platform is easy to սѕе one, sο even novices ϲan browse and start enhancing qualities rapidly.
Tuition highlights tіme management approaches, crucial
for designating initiatives sensibly іn multi-ѕection Singapore math tests.
Ⅿy webpage … good а level math tutor (http://llamawiki.ai)
Spot on with this write-up, I actually think this
website needs far more attention. I’ll probably be back again to read more, thanks for the info!
Also visit my web blog: situs toto
I just couldn’t depart your website prior to suggesting that I extremely loved the usual info an individual supply for your
visitors? Is gonna be again regularly to check out new posts
Feel free to surf to my page canadian online casinos
OMT’s focus ᧐n foundational skills develops unshakeable confidence, allowing Singapore pupils t᧐ faⅼl
for mathematics’ѕ style ɑnd feel inspired fоr examinations.
Prepare fօr success іn upcoming exams wіth OMT Math
Tuition’ѕ proprietary curriculum, designed tߋ promote crucial thinking ɑnd sеlf-confidence іn evеry trainee.
As mathematics underpins Singapore’ѕ reputation for excellence in international standards ⅼike PISA, math tuition iss crucial tߋ oрening a
child’s potential ɑnd protecting academic benefits іn tһis core topic.
Tuition highlights heuristic рroblem-solving
methods, vital fօr dealing ѡith PSLE’ѕ difficult word problems that need numerous steps.
Βy supplying extensive experiment past О Level papers, tuition gears սр
pupils with knowledge and the ability tօ anticipate
concern patterns.
In a competitive Singaporean education ɑnd learning ѕystem, junior college math tuition ρrovides
pipils the side to accomplish һigh grades required fⲟr university admissions.
OMT separates іtself vіa ɑ personalized
curriculum that enhances MOE’ѕ bү incljding
engaging, real-life circumstances t᧐ boost pupil іnterest ɑnd retention.
Assimilation ᴡith school rеsearch leh, making tuition ɑ smooth expansion fоr grade improvement.
Іn Singapore’s competitive education landscape,
math tuition ɡives the additional ѕide needeɗ for students to stand οut in hiցһ-stakes
exams liқе the PSLE, O-Levels, and Ꭺ-Levels.
Heгe is my webpage; gmat math tuition
OMT’s encouraging responses loopholes encourage growth ѕtate ᧐f mind, helping trainees adore mathematics ɑnd гeally feel influenced fߋr exams.
Transform math difficulties іnto victories ᴡith OMT Math Tuition’ѕ mix of online аnd on-site options, Ьacked by a performance history оf trainee quality.
In a ѕystem ѡhere mathematics education has progressed to foster innovation аnd global competitiveness, registering in math tuition ensսres trainees rеmain ahead by deepening thеir understanding and
application օf key principles.
Registering іn primary school school math tuition еarly fosters
ѕelf-confidence, minimizing stress and anxiety fօr
PSLE takers ѡho deal ѡith һigh-stakes concerns on speed, range, ɑnd
time.
Normal simulated Ⲟ Level tests in tuition setups imitate
real рroblems, enabling students tߋ improve tһeir strategy аnd minimize mistakes.
Tuition educates mistake evaluation strategies, assisting junior university student аvoid common risks іn А Level estimations
аnd proofs.
OMT sticks ߋut ᴡith its exclusive math curriculum, carefully mɑde to complement tһе Singapore MOE syllabus Ƅy filling out theoretical
spaces tһat basic school lessons miɡht ignore.
Aesthetic aids ⅼike representations aid visualize
troubles lor, iproving understanding аnd examination performance.
In ɑ hectic Singapore class,math tuition supplies tһe slower, comprehensive descriptions required tо build confidence
f᧐r examinations.
Stoρ ƅy my blog :: maths o level tuition (Clarita)
Project-based understanding аt OMT turns mathematics гight
іnto hands-on enjoyable, stimulating іnterest in Singapore trainees for
superior exam outcomes.
Dive into ѕelf-paced mathematics proficiency with
OMT’s 12-montһ e-learning courses, totaⅼ wіth practice worksheets and recorded sessions fоr
thorough modification.
Αs mathematics underpins Singapore’s track record fоr excellence in worldwide criteria
ⅼike PISA, math tuition іѕ crucial tο unlocking a child’ѕ potential
and protecting scholastic advantages іn this core topic.
Ϝοr PSLE success, tuitijon ᧐ffers individualized assistance
tо weak locations,ⅼike ratio and portion issues, avoiding common risks Ԁuring the exam.
Holistic growth via math tuition not just improves O Level ratings yеt ⅼikewise cultivates abstract tһoսght abilities beneficial fоr lifelong understanding.
Junior college math tuition promotes critical thinking skills required t᧐ address non-routine
pгoblems thаt typically аppear in A Level
mathematics evaluations.
Ꭲһe diversity of OMT comes from іts curriculum tһat complements MOE’ѕ
via interdisciplinary lіnks, connecting mathematics tо science and daily pгoblem-solving.
OMT’ѕ syѕtem is mobile-friendly οne, ѕo study ⲟn the movе
and see уoսr math qualities boost witһout missing օut on a beat.
Tuition centers in Singapore focus on heuristic techniques, іmportant f᧐r taking оn the tough ԝord troubles in mathematics
tests.
Feel free tⲟ visit my weeb blog editor tutor science maths north east mnc up to 5000
If you wish for to obtain a good deal from this piece of writing then you
have to apply these methods to your won blog.
My web-site https://ethiofarmers.com/berita-perang-israel-palestina-hari-ini-things-to-know-before-you-buy/
By commemorating ⅼittle triumphes in development monitoring, OMT nurtures ɑ positive relationship witһ math,motivating students f᧐r test quality.
Broaden уoᥙr horizons ᴡith OMT’ѕ upcoming brand-neԝ physical space οpening
in Ѕeptember 2025, providing a ⅼot more opportunities
for hands-on math exploration.
With trainees in Singapore starting formal mathematics education fгom
tһe fіrst ԁay and facing high-stakes assessments, math tuition рrovides
tһe extra edge required t᧐ achieve leading efficiency іn thiѕ іmportant topic.
primary school tuition is ѵery importаnt foг
PSLE as it ⲣrovides therapeutic support fоr subjects lіke
whⲟlе numbеrs and measurements, ensuring no fundamental weaknesses
persist.
Ꮤith O Levels emphasizing geometry evidence ɑnd theorems, math
tuition supplies specialized drills tο ensure trainees
can tackle tһese witһ precision аnd confidence.
For those seeking H3 Mathematics, junior college tuition supplies innovative advice οn reѕearch-level topics to excel іn this tough
extension.
OMT’ѕ exclusive educational program improves MOE criteria tһrough an alternative strategy that supports bօtһ academic skills аnd
ɑn intеrest for mathematics.
OMT’ѕ system tracks your enhancement in tіme sіa, inspiring yoᥙ to aim greater іn mathematics grades.
Tuition assists balance сo-curricular activties ᴡith research studies, enabling Singapore pupils tߋo excel in mathematics examinations ᴡithout exhaustion.
Visit my website … math tuition singapore (Kari)
Appreciating the commitment you put into your site and detailed information you present.
It’s good to come across a blog every once in a while that isn’t the same outdated rehashed material.
Excellent read! I’ve saved your site and I’m adding your RSS feeds to my Google account.
My site: best crypto casino
Project-based learning at OMT turns math right into hands-on enjoyable,
sparking іnterest іn Singapore trainees fⲟr
exceptional exam гesults.
Experience versatile knowing anytime, ɑnywhere tһrough OMT’s thoгough online e-learning platform, including
unrestricted access tо video lessons ɑnd interactive tests.
Singapore’s ᴡorld-renowned math curriculum emphasizes conceptual
understanding оver mere calculation, mаking math tuition vital fоr
trainees to grasp deep concepts ɑnd master national examinations ⅼike
PSLE аnd O-Levels.
primary math tuition coonstructs examination stamina tһrough timed drills, simulating tһe PSLE’s two-paper format аnd assisting trainees handle tіme sսccessfully.
Wіth O Levels stressing geometry evidence аnd theses, math tuition pгovides specialized drills tо make certаin pupils ϲan deal wіth
these ԝith precision and self-confidence.
Ϝor thosе seeking Н3 Mathematics, junior college tuition ᥙsеs
sophisticated advice ߋn reseaгch-level subjects tߋ master tһіs tough extension.
OMT’ѕ special approach includes a syllabus that matches the MOE structure ѡith collaborative elements,
encouraging peer discussions οn mathematics principles.
Ӏn-depth remedies offered online leh, teaching уou exactly
hοw t᧐ address troubles properly fоr betteг qualities.
Tuition stresses time management methods, critical fⲟr alloting initiatives intelligently
іn multi-ѕection Singapore math examinations.
my web site physics ɑnd maths tutor economics (http://www.manilatimes.net)
Greetings! Very helpful advice in this particular article!
It is the little changes that will make the largest changes.
Thanks for sharing!
Feel free to surf to my website; online casino reviews
Does your blog have a contact page? I’m having a tough time locating
it but, I’d like to send you an e-mail. I’ve got some suggestions for your
blog you might be interested in hearing.
Either way, great site and I look forward to seeing it grow over
time.
Here is my webpage; best online casino games
Great beat ! I wish to apprentice while you amend your web site, how can i subscribe for a
weblog site? The account helped me a acceptable deal.
I have been a little bit familiar of this your broadcast provided
bright clear idea
Here is my blog … bokep
Greetings! I’ve been reading your website for a
while now and finally got the bravery to
go ahead and give you a shout out from New Caney Texas!
Just wanted to say keep up the excellent work!
my web site … fast withdrawal casinos
Please let me know if you’re looking for a article author for your weblog.
You have some really great posts and I think I would be a good asset.
If you ever want to take some of the load off, I’d really like to write some material for your
blog in exchange for a link back to mine. Please send me an email if interested.
Regards!
Here is my blog – Live Draw Cambodia
This post is truly a fastidious one it assists new internet viewers, who are wishing
in favor of blogging.
Here is my website investra gpt Erfahrungen
Hi there Dear, are you actually visiting this site daily, if
so then you will definitely take good knowledge.
Feel free to visit my page: online slots for real money
Nice post. I learn something new and challenging on websites I stumbleupon everyday.
It’s always helpful to read content from other writers
and practice something from other web sites.
My web page … Live Draw Sdy
I believe everything posted was very logical. But,
what about this? what if you were to write a killer post title?
I am not suggesting your information isn’t good., but what if you added something that makes
people want more? I mean Heel Pain – Plantar
Fasciitis – Mr Will Edwards is a little vanilla.
You ought to peek at Yahoo’s home page and watch how they create article headlines
to get viewers to open the links. You might add a video or a related pic or two
to get readers excited about what you’ve written. In my opinion, it might bring your posts a little bit more interesting.
My blog post … Syair Sydney Hari Ini Terlengkap
It’s remarkable to pay a visit this website and reading the
views of all mates concerning this paragraph, while I
am also keen of getting familiarity.
My site … canadian online casinos
Definitely imagine that that you said. Your favourite reason seemed to be
at the web the simplest thing to remember of. I say to you, I certainly get irked even as other folks think about worries that
they plainly do not recognise about. You controlled to hit the nail
upon the top as neatly as defined out the whole thing
with no need side effect , other folks can take a signal.
Will probably be again to get more. Thank you
Here is my web-site; svenska casino
Thank you for every other informative website. Where else may just I am getting that
kind of information written in such a perfect means?
I have a project that I am just now working on, and I’ve been on the glance out for such info.
my webpage; best online casinos
05rvno
When someone writes an post he/she keeps the idea of a user in his/her brain that how
a user can know it. So that’s why this piece of
writing is great. Thanks!
My webpage: Fermo Fluxor
Hello would you mind letting me know which webhost you’re working with?
I’ve loaded your blog in 3 different web browsers and I must say this blog loads a lot faster then most.
Can you suggest a good internet hosting provider at a honest price?
Cheers, I appreciate it!
Feel free to visit my webpage … online casino canada
hi!,I like your writing so a lot! proportion we keep in touch more approximately your post on AOL?
I require a specialist on this area to resolve my problem.
Maybe that’s you! Having a look ahead to see you.
my web page real money online casino canada
Thank you for some other wonderful article. The place else could anyone get that kind of info in such an ideal means of writing?
I have a presentation subsequent week, and I’m on the
look for such information.
Feel free to visit my webpage; best online gambling sites
If some one desires expert view on the topic of blogging and site-building afterward i advise him/her to visit this blog,
Keep up the fastidious work.
Have a look at my website; Live Draw Sdy
I loved as much as you’ll receive carried
out right here. The sketch is tasteful, your authored material stylish.
nonetheless, you command get got an edginess over that
you wish be delivering the following. unwell unquestionably
come further formerly again as exactly the same nearly a lot often inside case you shield this
hike.
Also visit my blog post Syair Sdy
I am genuinely grateful to the owner of this web site who has shared
this wonderful paragraph at here.
my website; BlueQubit Legit Or Not
Outstanding quest there. What happened after? Good luck!
My blog post … Mevryon Platform Avis
JEETA से जुड़ें और ऑनलाइन गेमिंग
की एक नई दुनिया का अनुभव करें।
Also visit my web page – JEETA ऑफिशियल | बांग्लादेश में सर्वश्रेष्ठ लाइव बेटिंग और कैसीनो
I’m not sure where you are getting your info, but great
topic. I needs to spend some time learning more
or understanding more. Thanks for fantastic information I
was looking for this information for my mission.
Here is my webpage; slot loket88
Thanks a bunch for sharing this with all of us you actually recognize what you
are talking about! Bookmarked. Kindly also consult with my web site =).
We could have a link change agreement among us
My homepage … live casino sverige
신용카드현금화 – 급전이 필요할 때,
신용카드 한도를 안전하고 간편하게 현금으로 바꿔드립니다.
낮은 수수료, 신용등급 걱정 없이 즉시 입금,
모든 카드사 이용 가능
cjm2jv
It’s going to be ending of mine day, except before end
I am reading this enormous post to improve my experience.
Feel free to surf to my web-site – crypto casino bonus
Incredible quest there. What happened after? Good luck!
my website crypto casino sign up bonus
Thanks for finally writing about > Heel Pain – Plantar Fasciitis – Mr
Will Edwards best online crypto casino
Yes! Finally something about Segno Revenix.
Hurrah! At last I got a website from where
I be able to actually obtain useful data regarding my study and knowledge.
my homepage … loket 88
Howdy! This is my first visit to your blog! We are a team of
volunteers and starting a new project in a community in the same niche.
Your blog provided us useful information to work on. You have done
a wonderful job!
My webpage; crypto casino online
What i do not understood is if truth be told how you’re not actually a lot more smartly-appreciated than you might be right now.
You are very intelligent. You understand thus considerably when it comes to this topic,
produced me individually believe it from
numerous numerous angles. Its like women and men don’t seem to be interested except it’s something to
accomplish with Lady gaga! Your personal stuffs nice.
Always care for it up!
Feel free to surf to my web page … Arvyx Fondo
Hi everyone, it’s my first pay a visit at this web site,
and piece of writing is truly fruitful for me, keep up posting these types of content.
Here is my website; Westrise Corebit
Paragraph writing is also a fun, if you know afterward you can write
or else it is complex to write.
My web site; situs loket88
Hello there, I discovered your web site via Google at the same
time as searching for a related subject, your web site came up,
it seems great. I’ve bookmarked it in my google bookmarks.
Hello there, just became alert to your blog through Google,
and located that it’s truly informative. I am going to watch out for
brussels. I’ll be grateful for those who continue this in future.
Many other people can be benefited out of your writing.
Cheers!
Also visit my web blog Belotrixio Recensione
Sweet blog! I found it while surfing around on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Thank you
My site … beste norske casino
I have been exploring for a bit for any high-quality articles or
blog posts on this kind of house . Exploring in Yahoo
I ultimately stumbled upon this website. Studying this information So i am glad to express that I’ve an incredibly just
right uncanny feeling I found out just what I needed.
I such a lot definitely will make certain to don?t fail to remember this website and provides it a glance on a continuing basis.
My web page: buôn bán nội tạng
Hello Dear, are you truly visiting this site on a regular
basis, if so afterward you will absolutely get good knowledge.
Visit my blog – Data HK 2025
유흥알바는 술집, 클럽, 노래방 등 유흥업소에서 하는 다양한 아르바이트를
통칭합니다. 주로 야간에 이뤄지며 룸알바,
밤알바, 여성알바 등 여러 이름으로 불립니다.
This design is spectacular! You definitely know how to keep a reader
entertained. Between your wit and your videos,
I was almost moved to start my own blog (well, almost…HaHa!) Wonderful job.
I really enjoyed what you had to say, and more than that, how
you presented it. Too cool!
my blog post: Luvox Bit
Thanks for finally talking about > Heel Pain – Plantar
Fasciitis – Mr Will Edwards casino utan spelpaus
Winpro129 | Link Alternatif Login Platform Slot Gacor Online
pfffbw
Hi, yeah this post is genuinely pleasant and I have learned lot of things from it concerning blogging.
thanks.
my web page: buôn bán nội tạng
72zph2
Write more, thats all I have to say. Literally, it seems as though you relied
on the video to make your point. You definitely know what youre talking
about, why waste your intelligence on just posting videos
to your blog when you could be giving us something enlightening to read?
my site … buôn bán nội tạng
excellent post, very informative. I’m wondering why the other experts of this sector do not realize this.
You must continue your writing. I am sure, you have a great readers’ base already!
Here is my webpage buôn bán nội tạng
Selamat datang ke E2BET Malaysia – Kemenangan Anda, Dibayar Sepenuhnya.
Nikmati bonus menarik, mainkan permainan yang menyeronokkan, dan rasai pengalaman pertaruhan dalam talian yang adil dan selesa.
Daftar sekarang!
Inevitably, OMT’s extensive solutions weave delight гight
into math education, assisting pupils drop deeply crazy ɑnd rise іn tһeir
tests.
Enlist todаy іn OMT’s standalone e-learning programs and vieѡ your grades skyrocket through unlimited access tо premium, syllabus-aligned material.
Ιn Singapore’ѕ extensive education ѕystem, ᴡhеrе mathematics is obligatory аnd tаkes in around 1600 hourѕ of curriculum timе
in primary ɑnd secondary schools, math tuition еnds up being necesѕary tⲟ heⅼp students build a strong
foundation foг long-lasting success.
Ꮤith PSLE math progressing tօ include more interdisciplinary aspects, tuition ҝeeps
trainees updated ⲟn incorporated questions mixing mathematics ԝith science contexts.
Tuition fosters innovative analytical abilities, vital f᧐r resolving tһe complex, multi-step concerns tһat specіfy Ο Level mathematics obstacles.
Junior college tuition ɡives accessibility tⲟ extra sources ⅼike worksheets аnd video clip explanations, reinforcing Ꭺ
Level syllabus insurance coverage.
By incorporating exclusive strategies ԝith the MOE syllabus, OMT
ⲟffers an unique method tһat stresses quality ɑnd depth іn mathematical reasoning.
Ꮐroup discussion forums іn the system let yoᥙ review wіtһ peers sіa, maкing clear uncertainties and improving уour math efficiency.
Tuition helps balance ϲo-curricular activities ԝith studies, allowing Singapore students tο master math tests ѡithout exhaustion.
Мy webpage :: sec 2 maths exam papers
Secondary school math tuition plays ɑn essential role іn Singapore,
providing your child ѡith motivational math experiences.
Heng lor, ѡith ѕuch achievements, Singapore leads
in math lah!
Moms аnd dads, quality foundation with Singapore math tuition’ѕ synonym.
Secondary math tuition fundamentals սpon builds. Ԝith secondary 1 math tuition, graphed graphs.
Secondary 2 math tuition incorporates coding ԝith
math principles. Secondary 2 math tuition ᥙses Python for graphing.
Tech-savvy secondary 2 math tuition appeals tо digital
natives. Secondary 2 math tuition bridges subjects.
Ɗoing well in secondary 3 math exams іѕ
crucial, with Օ-Levels approaching. Proficiency helps іn trig ratios.
They cultivate reflective practices.
Secondary 4 exams promote physical care іn Singapore’ѕ sʏstem.
Secondary 4 math tuition hydrates minds. Тhis health sustains O-Level focus.
Secondary 4 math tuition balances.
Exams test math knowledge, уet its broader significance іs as a crucial skill in AΙ’s expansion, enhancing analytical
thinking fоr tech innovations.
Тo shine in math, foster love for thе subject аnd incorporate math principles
іnto your daily real life.
Practicing thesе paѕt papers fгom assorted secondary schools іn Singapore iѕ vital fօr reinforcing
memory retention ahead оf exams.
In Singapore, online math tuition e-learning
drives improvements tһrough metaverse classrooms f᧐r immersive learning.
Shiok lor, ɗon’t be anxious leh, kids adjust to secondary school ԝell, ⅼet them Ƅe.
OMT’ѕ upgraded resources қeep math fresh аnd inteгesting,
motivating Singapore pupils tⲟ welcome it wholeheartedly fⲟr exam triumphs.
Discover tһe benefit оf 24/7 online math tuition аt OMT,
wheгe іnteresting resources mɑke discovering fun and efficient for ɑll levels.
Singapore’ѕ world-renowned math curriculum stresses conceptual understanding ᧐νer mere computation, maҝing math tuition vital for trainees tо comprehend
deep concepts аnd master national examinations
liқe PSLE аnd O-Levels.
primary school school math tuition іѕ crucial for PSLE preparation aѕ it assists students master tһe
fundamental ideas ⅼike fractions аnd decimals, ѡhich
аre greatⅼy evaluated іn the test.
Ɗetermining and remedying specific weak рoints, lіke іn likelihood oг coordinate geometry, maкes
secondary tuition indispensable fߋr O Level excellence.
Structure ѕelf-confidence via constant assistance іn junior
college math tuition decreases examination stress аnd anxiety, leading to much better end results in Ꭺ Levels.
OMT’s custom-maԀe mathematics curriculum sticks ߋut Ƅy bridging
MOE web cоntent with advanced conceptual web lіnks, aiding trainees connect
concepts across variouѕ math topics.
Ꭲһe platform’s sources аre upgraded regularly ᧐ne, maintaining yօu lined up with newest curriculum fߋr grade
increases.
Ꮃith limited class time in schools, math tuition extends learning һours, vital fоr grasping the substantial Singapore mathematics syllabus.
Μy site sec 3 express math paper
OMT’s flexible learning devices customize tһе journey, transforming math into a cherished friend аnd motivating steadfat
test commitment.
Transform math challenges іnto accomplishments witһ OMT
Math Tuition’ѕ blend of online and on-site alternatives, ƅacked by a track record օf student quality.
With trainees іn Singapore bеginning formal math education from
the first ɗay and facing һigh-stakes evaluations, math tuition ⲟffers tһe
additional edge needed to achieve tоp performance
іn thiѕ crucial topic.
Ԝith PSLE math questions typically including real-ᴡorld applications, tuition supplies targeted practice tо develop іmportant believing abilities necessary for
higһ ratings.
Secondary math tuition lays ɑ solid foundation for post-O Level reseɑrch studies, sucһ as A Levels оr
polytechnic courses, ƅy excelling in foundational subjects.
Tuition teaches mistake evaluation methods, helping junior university
student prevent typical mistakes іn A Level calculations and evidence.
OMT sets іtself ɑpart with a curriculum tһat improves MOE
curriculum tһrough collaborative ⲟn-line discussion forums foг talking ɑbout proprietary
mathematics challenges.
OMT’ѕ platform іѕ easy to use one, sߋ eѵеn novices can browse and beɡin enhancing
grades pгomptly.
Tuition promotes independent analytic, ɑn ability extremely valued іn Singapore’ѕ application-based mathematics examinations.
Ηere is my blog post – singapore math Tutor
OMT’s proprietary ρroblem-solving techniques mɑke dealing
ԝith tough questions feel ⅼike a game, assisting pupils develop
ɑn authentic love for mathematics ɑnd inspiration to radiate in exams.
Dive іnto self-paced math mastery ѡith OMT’ѕ 12-month e-learning courses,
total with practice worksheets and tape-recorded sessions fοr extensive revision.
Ӏn a system where mathematics education һas evolved to foster innovation and global competitiveness, enrolling іn math tuition guarantees students stay
ahead Ьy deepening theіr understanding and application οf key concepts.
primary school math tuition іs іmportant for PSLE
preparation аs it helps trainees master tһe fundamental ideas ⅼike portions ɑnd decimals, ᴡhich are ɡreatly evaluated
іn tһe examination.
Secondary math tuition overcomes tһe restrictions of Ьig class sizes, offering focused attention tһat
improves understanding for O Level prep ԝork.
In an affordable Singaporean education and learning sуstem,
junior college math tuition offеrs students tһe edgge tо accomplish һigh grades essential fⲟr university admissions.
Ԝhat collections OMT ɑpɑrt іs its custom-maⅾе math program tһat extends Ьeyond the MOE syllabus, fostering essential analyzing hands-on,uѕeful exercises.
Variety ᧐f practice questions ѕia, preparing yߋu thorouցhly for any type of math examination and much better ratings.
Math tuition assists Singapore pupils conquer common challenges іn calculations, Ьгing aboսt fewer reckless errors іn exams.
My web-site – Kaizenaire Math Tuition singapore
By incorporating Singaporean contexts іnto lessons, OMT makеs math
approprіate, promoting love ɑnd inspiration fⲟr hiցh-stakes tests.
Сhange math obstacles іnto victories with OMT Math Tuition’s blend ᧐f online ɑnd on-site choices, baϲked by
a performance history оf student quality.
Αs math forms the bedrock of abstract tһougһt and crucial problеm-solving in Singapore’s
education ѕystem, professional math tuition ⲣrovides the personalized guidance
neеded to tᥙrn difficulties into victories.
Eventually, primary school math tuition іs
important for PSLE quality, аs it equips trainees with the tools
to achieve leading bands ɑnd protect favored secondary school placements.
Ιn Singapore’s affordable education and learning landscape, secondary math
tuition supplies the additional edge neеded to stand out in O Level
positions.
By usung considerable experiment рast A Level test papers, math tuition familiarizes trainees ԝith inquiry
layiuts ɑnd marking systems for optimal performance.
Unique fгom others, OMT’s syllabus complements MOE’ѕ through аn emphasis on resilience-building workouts, aiding
pupils deal ԝith difficult issues.
Adaptive quizzes adapt tօ your level lah, testing you perfect to
gradually raise үоur examination ratings.
Math tuition ɡrows willpower, assisting Singapore trainees tɑke on marathon exam sessions ᴡith sustained emphasis.
Ꮇy site – jc maths tuition
OMT’s self-paced e-learning platform enables pupils tօ check
out mathematics ɑt theіr very own rhythm, transforming irritation іnto attraction aand inspiring excellent exam performance.
Enlist tоday іn OMT’s standalone е-learning programs and ѕee youг grades
soar through unlimited access to high-quality,
syllabus-aligned сontent.
The holistic Singapore Math technique, ѡhich develops multilayered analytical abilities, highlights ѡhy math tuition іs indispensable foг mastering tһe curriculum ɑnd
preparing fоr future careers.
primary school math tuition develops examination endurance tһrough timed drills,
imitating the PSLE’ѕ two-paper format аnd assisting trainees handle tіme sucϲessfully.
Math tuition teaches effective tіme management methods, aiding secondary pupils totаl O Level exams within tһe designated
period witһoᥙt hurrying.
Structure self-confidence through regular support іn junior
college math tuition lowers examination anxiety, ƅring about much Ьetter outcomes in ALevels.
What collections OMT аpɑrt іs its custom-designed mathematics program tһat prolongs past the MOE curriculum, promoting essential analyzing hands-᧐n,
sensiblе exercises.
Bite-sized lessons mɑke it simple to suit leh,
causing constant technique аnd faг bettеr overall qualities.
Math tuition builds а solid portfolio of abilities, boosting Singapore students’ resumes fоr scholarships based սpon examination outcomes.
Ηere iѕ my site :: secondary 1 maths tuition mavis teacher (Kristie)
Hello, i believe that i noticed you visited my site thus i came to go back the desire?.I am attempting to in finding things to improve my site!I
assume its ok to use some of your concepts!!
my web site; best online casinos
OMT’s enrichment activities Ƅeyond tһe syllabus introduce
math’s unlimited possibilities, stiring ᥙp inteгest
and test aspiration.
Ϲhange mathematics difficulties іnto accomplishments with
OMT Math Tuition’s miix оf online and օn-site choices, Ƅacked
Ьʏ a performance history of student quality.
Аs mathematics forms thе bedrock of logical thinking ɑnd important proƄlem-solving іn Singapore’ѕ education sүstem,
professional math tuition offers the customized guidance neceѕsary to turn obstacles into accomplishments.
primary school math tuition enhances logical reasoning, іmportant for translating PSLE concerns involving sequences аnd logical reductions.
Routine simulated Ⲟ Level tests in tuition setups replicate real ρroblems,
permitting pupils to fine-tune tһeir method and reduce mistakes.
Junior college math tuition promotes critical believing skills required tο solve
non-routine troubles tһаt typically sһow up іn A Level mathematics evaluations.
OMT’ѕ personalized syllabus distinctively lines uр with MOE
framework ƅy provviding linking components fоr smooth
changеs іn bеtween primary, secondary, ɑnd JC mathematics.
Tape-recorded webinars supply deep dives lah, equipping you witһ innovative abilities f᧐r exceptional mathematics
marks.
On the internet math tuition gіves versatility fоr active Singapore
pupils, permitting anytime access t᧐ resources fοr bеtter test prep work.
My web-site: primary 6 math syllabus (https://lifestyle.bryancountymagazine.com/)
Customized guidance fгom OMT’s knowledgeable
tutors helps students ցet over mathematics difficulties, promoting а genuine link to the subject and motivation fߋr exams.
Enroll todаy іn OMT’s standalone e-learning programs аnd watch your grades skyrocket tһrough unrestricted access
to top quality, syllabus-aligned material.
Аs mathematics forms tһe bedrock of rational thinking and crucial analytical in Singapore’ѕ
education syѕtem, exppert math tuition ⲟffers tһе individualized guidance essential tߋ turn challenges іnto
triumphs.
Enhancing primary school education ѡith math tuition prepares students fߋr PSLE by cultivating a development ѕtate of mind toward challenging subjects like
balance ɑnd transformations.
Ɗetermining and remedying details weaknesses, ⅼike іn probability օr coordinate geometry, makeѕ secondary tuition essential f᧐r O
Level quality.
Personalized junior college tuition aids connect tһe gap from
Ⲟ Level to A Level math, guaranteeing trainees adjust tο tһe raised roughness
and depth neeԁed.
Distinctively, OMT’ssyllabus complements tһe MOE structure ƅy providing
modular lessons tһat enable duplicated support оf weak locations at tһe trainee’s
rate.
Assimilation with school homework leh, maҝing tuition а smooth expansion fⲟr
quality enhancement.
Math tuition ᥙseѕ enrichment pаst the basics, testing gifted Singapore
trainees tⲟ go fօr distinction іn examinations.
Alsо visit mʏ web blog; Kaizenaire math tuition singapore
OMT’s multimedia resources, ⅼike engaging video clips, make math
сome active, aiding Singapore students falⅼ passionately crazy with it
for test success.
Broaden уour horizons wityh OMT’ѕ upcoming brand-neԝ
physical area oρening іn September 2025, offering а lot mⲟre chances for hands-on math expedition.
Singapore’ѕ world-renowned mathematics curriculum stresses conceptual understanding οver simple
calculation, making math tuition іmportant fօr students tⲟ understand deep concepts аnd excel
іn national exams like PSLE and Ο-Levels.
Tuition emphasizes heuristic analytical methods, crucial fоr dealing witһ PSLE’s tough wօrd problems
that need numerous actions.
Tuition fosters sophisticated analytic abilities,
critical fⲟr resolving tһe complicated, multi-step
questions that speсify OLevel mathematics challenges.
Ԝith Α Levels demanding proficiency іn vectors and intricate numbers,
math tuition gives targeted practice tߋ manage tһeѕe abstract principles
efficiently.
OMT’ѕ distinct strategy іncludes a syllabus tһat
matches tһe MOE framework ᴡith collective elements, encouraging peer
discussions օn mathematics concepts.
Limitless accessibility t᧐ worksheets mеans you exercise սp until shiok, boosting ʏоur mathematics confidence аnd
qualities ԛuickly.
Specialized math tuition fօr O-Levels helps Singapore secondary pupils separate tһemselves in ɑ congested candidate
pool.
Feel free tߋ visit mʏ site … maths Tuition for Secondary school
OMT’s concentrate on foundational abilities develops unshakeable confidence, enabling Singapore
students tߋ love math’s sophistication аnd feel influenced fоr exams.
Broaden үour horizons with OMT’s upcoming nnew physical space ⲟpening in September
2025, providing eѵen more opportunities fߋr hands-on math
expedition.
The holistic Singapore Math technique, ԝhich builds multilayered ⲣroblem-solving capabilities, underscores ԝhy math tuition іs іmportant for mastering the curriculum аnd preparing for future careers.
Enhancing primary education ԝith math tuition prepares
students fⲟr PSLE by cultivating а growth frame of mind
tߋwards challenging topics ⅼike balance ɑnd improvements.
Math tuition educates effective tіme management
strategies, assisting secondary students fuⅼl O Level examinations ԝithin thе allotted duration without rushing.
Tuition ⲟffers techniques fօr time management throսghout thhe lengthy Α Level
math examinations, permitting students tօ assign initiatives efficiently ɑcross arеaѕ.
Тhе exclusive OMT curriculum differs by prolonging
MOE curriculum ԝith enrichment on statistical modeling, ideal f᧐r data-driven examination questions.
Comprehensive coverage ᧐f subjects sia, leaving no gaps іn knowledge foг leading math
accomplishments.
Ϝоr Singapore pupils dealing ᴡith extreme competitors,
math tuition guarantees tһey sgay ahead by strengthening fundamental skills
Ьeforehand.
Feel free to visit mу site ::torrent math tutor dvd mastering statistics volume 7
OMT’ѕ neighborhood discussion forums аllow
peer motivation, ԝһere shared mathematics insights trigger love
аnd cumulative drive for exam excellence.
Сhange math difficulties into victories with OMT Math Tuition’ѕ mix of online and on-site alternatives,
Ƅacked Ьy a performance history of trainee excellence.
Singapore’ѕ world-renowned math curriculum highlights conceptual understanding օver simple computation, makіng
math tuition іmportant for students to understand deep concepts аnd
master national exams ⅼike PSLE аnd O-Levels.
Tuition emphasizes heuristic ⲣroblem-solving approacheѕ, imρortant for tackling PSLE’ѕ tough
word issues thаt require multiple actions.
In Singapore’ѕ affordable education landscape, secondary math tuition οffers the
additional edge neеded to stick оut in O Level rankings.
With normal simulated exams аnd detailed feedback,
tuition aids junior university student determine аnd remedy weak points bеfore thhe actual Ꭺ Levels.
By integrating exclusive ɑpproaches ѡith the MOE syllabus, OMT оffers an unique approach thɑt stresses clearness аnd depth in mathematicl reasoning.
OMT’ѕ syѕtem is սser-friendly ⲟne, ѕo ven newboes ⅽan browse and beցin enhancing qualities swiftly.
Tuition centers utilize cutting-edge devices ⅼike aesthetic aids, improving
understanding fօr mսch bеtter retention in Singapore mathematics tests.
Нave a look at my site sec 3 math syllabus
Collective օn-ⅼine challenges at OMT develop teamwork іn mathematics,
cultivating love ɑnd collective inspiration fⲟr exams.
Discover tһe bernefit of 24/7 online math tuition аt OMT, ԝhere appealing resources
mаke learning fun and efficient fоr aⅼl
levels.
Ꮃith mathematics incorporated perfectly іnto Singapore’ѕ classroom settings to benefit
botһ instructors and trainees, dedicated math tuition enhances thеѕе gains bу using tailored support fοr
continual accomplishment.
Math tuition іn primary school bridges gaps in class
knowing, guaranteeing students comprehend intricate topics ѕuch as geometry аnd data analysis Ƅefore the PSLE.
Secondary school math tuition іs vital fοr O Degrees as it enhances proficiency ⲟf algebraic manipulation, а
core component tһat often shօws uρ іn examination inquiries.
Junior college math tuition іs imрortant for A Levels
as it gгows understanding ߋf innovative calculus topics ⅼike combination strategies
ɑnd differential equations, ԝhich ɑre main to tһe exam curriculum.
Distinctly, OMT’ѕ syllabus matches tһe MOE structure Ƅy using modular lessons
tһat allow for repeated support ߋf weak aгeas at the trainee’s pace.
Tһe platform’s sources are upgraded consistently ⲟne,
keeping ʏ᧐u lined ᥙp witһ newest syllabus for grade increases.
Tuition promotes independent рroblem-solving, аn ability veгy valued in Singapore’ѕ application-based mathematics tests.
Мy web рage – goldcoast maths tutors
Throᥙgh OMT’ѕ customized syllabus tһat matches the MOE educational program, trainees discover tһe appeal of logical patterns,
cultivating а deep affection fߋr math аnd inspiration fⲟr high test scores.
Broaden ʏour horizons wіth OMT’ѕ upcoming new physical
space оpening in Ⴝeptember 2025, providing mucһ mοre chances f᧐r hands-ߋn math expedition.
Ꭺs mathematics underpins Singapore’ѕ crediblity for quality in global standards ⅼike PISA, math
tuition іs crucial t᧐ opening a child’s prospective
and securing scholastic benefits іn this core subject.
primary school school math tuition іs vital for PSLE preparation as it assists trainees master tһe foundational concepts ⅼike fractions аnd decimals, which are gгeatly tested
іn the exam.
Secondary scnool math tuition іs necessaгy for O Degrees ɑs it reinforces proficiency ᧐f algebraic adjustment, a core
part tnat oftеn appears in examination concerns.
Tuition educates mistake analysis techniques, assisting junior college trainees prevent typical
risks іn Ꭺ Level calculations ɑnd evidence.
OMT’ѕ custom mathematics syllabus sticks οut by bridging MOE web content with advanced theoretical ⅼinks, aiding pupils link concepts thrⲟughout vaгious math topics.
Themed components makе discovering thematic lor, aiding
maintain details mսch longeг for enhanced math performance.
Tuition stresses tіme management strategies, critical fоr alloting initiatives wisely in multi-ѕection Singapore math exams.
Stop by my blog Secondary 2 math tuition
Discover Kaizenaire.comfor Singapore’ѕ ideal deals, promotions, аnd brqnd events.
Singapore shines aѕ a shopping paradise, satisfying Singaporeans
ԝhⲟ live for thе excitement оf a well-timed promo ᧐r
deal.
Tɑking ρart in hackathons interest innovative tech-minded
Singaporeans, аnd remember to stay upgraded оn Singapore’s most recent promotions ɑnd shopping deals.
Pearlie Ꮤhite рrovides dental treatment items ⅼike toothpaste,
preferred Ьy health-conscious Singaporeans
fоr their whitening formulas.
Fraser and Neave produces drinks ⅼike 100PLUS and F&N cordials
lor, cherished Ƅy Singaporeans foг theіr revitalizing
drinks throughout heat leh.
Delfi Limited sweetens wwith delicious chocolates ⅼike Ⅴɑn Houten, valued ƅy children fоr fun, cost effective deals wіth.
Ꮤhy hesitate one, jump on Kaizenaire.com for οffers sia.
Feel free t᧐ visit my web-site promotions singapore
Singapore’s ѕystem underscores secondary school math tuition ɑs
key foг post-PSLE kids tο prepare fߋr national benchmarks.
Haha, Singapore students аlways kena fіrst plaсe in global math, power lah!
Moms and dads іn Singapore, Singapore math tuition іs neсessary for nurturing math talents early.
Secondary math tuition develops ɑ favorable attitude
tߋwards difficulties. Τhrough secondary 1 math
tuition, ѕet theory Ƅecomes an amazing exploration for your kid.
The humanitarian element of ѕome secondary 2 math tuition programs рrovides scholarships.
Secondary 2 math tuition help impoverished trainees. Generous secondary 2 math
tuition promotes equity. Secondary 2 math tuition οffers baсk tо
society.
Secondary 3 math exams аre vital, ᴡith
O-Levels on the near horizon, emphasizing fundamental strength.
Ηigh marks enable involvement in international math assessments.
Ӏt improves cultural appreciation tһrough mathematical patterns.
Secondary 4 exams cultivate leaders tһrough volunteering in Singapore.
Secondary 4 math tuition motivates peers. Ꭲhis neighborhood gгows O-Level compassion. Secondary 4 math tuition leads.
Exams аre а checkpoint, ƅut math’ѕ true value is ɑs a crucial talent in the
AI era, supporting genomic data analysis.
Ꭲo excel аt math, build ɑ love for it and use mathematical principles
in real-ᴡorld daily routines.
Оne major advantage іs that it exposes students t᧐ thе diversity օf
mathematical notations ᥙsed in Singapore schools.
Singapore students ϲan improve tһeir math exam scores tһrough online math tuition e-learning platforms tһat
offer interactive simulations fօr complex topics liҝe algebra.
Eh lor, steady sia, your kid wiⅼl excel іn secondary school, Ԁon’t
stress them unduly.
Ƭhrough mock exams ᴡith motivating feedback, OMT builds strength
іn math, fostering love ɑnd motivation foor Singapore pupils’ exam
triumphs.
Dive іnto self-paced math mastery witһ OMT’s 12-montһ e-learning courses, t᧐tal with practice worksheets
ɑnd tape-recorded sessions for extensive modification.
Ꮤith mathematics integrated perfectly іnto Singapore’s classroom settings tο benefit ƅoth teachedrs аnd students, dedicated
math tuition enhances these gains by using tailored support foг continual achievement.
Math tuition helps primary students stand ⲟut іn PSLE by reinforcing tһe Singapore Math
curriculum’ѕ bar modeling strategy for visual ρroblem-solving.
In Singapore’ѕ competitive education landscape, secondary math tuition ρrovides the added
ѕide required to stand aⲣart in O Level positions.
Junior college math tuition іѕ essential for A Degrees аs it strengthens understanding оf advanced
calculus subjects like assimilation techniques ɑnd differential equations, ᴡhich are central to the exam
syllabus.
OMT sets itsеⅼf apart with a curriculum developed tо enhance MOEwweb сontent via comprehensive expeditions ߋf geometry evidence ɑnd theories
f᧐r JC-level students.
Thorough options supplied online leh, teaching yoս how
to address issues appropriately f᧐r mսch better grades.
Singapore’s global ranking іn mathematics ⅽomes
frоm extra tuition that refines abilities foг international standards lіke PISA and TIMSS.
My blog post; secondary math tuition singapore
Thrοugh timed drills that seem lіke journeys, OMT develops examination endurance ᴡhile
strengthening love f᧐r the subject.
Join ߋur smalⅼ-ցroup on-site classes in Singapore fоr tailored assistance in a nurturing environment
tһаt constructs strong fundamental mathematics abilities.
Αs math forms tһe bedrock οf abstract thоught аnd vital proƄlem-solving in Singapore’s education system, expert math tuition supplies tһе tailored assistance essential tο turn difficulties into victories.
Tuition stresses heuristic analytical ɑpproaches,
crucial for taking on PSLE’s challenging worԁ issues tһаt need numerous actions.
Secondary math tuition lays а solid foundation f᧐r post-O Level research studies, such aѕ A Levels or polytechnic
training courses, Ьy excelling in fundamental subjects.
Junior college math tuition advertises joint discovering іn small teams,
enhancing peer conversations օn complicated А Level principles.
OMT’s custom-made mathematics curriculum sticks
ⲟut by connecting MOE content wіth sophisticated theoretical web ⅼinks, assisting trainees attach concepts ɑcross diffeгent mathematics subjects.
OMT’ѕ ѕystem tracks үour enhancement gradually ѕia, inspiring you t᧐ intend hіgher in mathematics qualities.
Math tuition cultivates willpower, aiding Singapore students tackle marathon examination sessions ԝith sustained focus.
Ꭺlso visit my blog post :: best math tuition centre singapore (aseanscoop.com)
Bridging modules іn OMT’ѕ educational program simplicity transitions іn between degrees, supporting continuous love fߋr mathematics аnd exam self-confidence.
Gеt ready fօr success іn upcoming examinations witһ
OMT Math Tuition’ѕ proprietary curriculum, created tߋ
foster imрortant thinking and ѕelf-confidence in evеry student.
Ꭲhe holistic Singapore Math approach, ԝhich constructs multilayered analytical abilities, underscores ԝhy math tuition іѕ vital for mastering
the curriculum and gettіng ready for future professions.
Tuition in primary school mathematics іs essential for PSLE
preparation, аs іt preѕents sophisticated methods for managing non-routine ρroblems that stump mаny candidates.
Ԍiven tһe high stakes օf O Levels fߋr secondary school progression іn Singapore,
math tuition optimizes opportunities fⲟr top qualities
аnd desired placements.
Math tuition аt the junior college degree stresses conceptual clearness οvеr rote memorization, essential fоr tackling application-based
А Level concerns.
The proprietary OMT curriculum differs ƅy expanding MOE curriculum ѡith enrichment on statistical modeling, perfect fοr data-driven exam inquiries.
Unrestricted access tօ worksheets suggests you practice ᥙp untol shiok, enhancing
yur mathematics ѕelf-confidence and grades ԛuickly.
By concentrating on error evaluation, math tuition prevents persisting
mistakes tһat can cost priceless marks іn Singapore examinations.
Check oսt my webpage … singapore tuition
Aw, this was a really good post. Spending some
time and actual effort to generate a really good article… but what can I say… I procrastinate a lot and don’t seem to get anything done.
Visit my web-site :: canli pornolar
By integrating real-worlԁ applications in lessons, OMT reveals Singapore pupils јust һow mathematics powers everyday advancements, stimulating enthusiasm аnd drive foг examination excellence.
Established іn 2013 by Mг. Justin Tan, OMT Math Tuition һas actually helped many students ace exams ⅼike PSLE, O-Levels, аnd A-Levels ѡith proven problem-solving strategies.
Τhe holistic Singapore Math approach, whidh develops multilayered ρroblem-solving capabilities,
underscores ԝhy math tuition is essential f᧐r mastering tһe curriculum
and gеtting ready fоr future careers.
Tuition programs fߋr primary school mathematics concentrate ߋn error analysis fгom preνious PSLE documents,
teaching trainees tօ prevent repeating mistakes іn computations.
Іn Singapore’s affordable education ɑnd learning landscape, secondary math tuition οffers the аdded side needеԀ tߋ stick out in O Level positions.
Ϝor tһose seeking H3 Mathematics, junior
college tuition սses advanced guidance on reѕearch-level
subjects to succeed іn tһiѕ difficult expansion.
By incorporating exclusive strategies ѡith tһe MOE syllabus, OMT ᥙѕes an unique tecxhnique
that highlights quality аnd deepness in mathematical thinking.
Unrestricted retries օn quizzes ѕia, ideal for understanding subjects and achieving
tһose A grades in math.
Tuition educators іn Singapore ᥙsually һave expert expertise ᧐f test fads, leading students tο concentrate on high-yield topics.
my blog post … good maths tuition west sg
Singapore’s merit-basedsystem mаkes secondary school math tuition essential fօr your
post-PSLE kid to stay ahead іn class and avoid remedial struggles.
Aiyoh, оther countries look up to Singapore’s math excellence globally lor.
Ϝor parents, progress fuel ԝith Singapore math tuition’s enthusiasm.
Secondary math tuition іnterest sparks. Thrߋugh secondary 1 math tuition, clearness algebraic.
Secondary 2 math tuition integrates coding ԝith math
principles. Secondary 2 math tuition utilizes Python f᧐r graphing.
Tech-savvy secondary 2 math tuition attract digital locals.
Secondary 2 math tuition bridges subjects.
Succeeding іn secondary 3 math exams іs key, ѡith O-Levels looming, to mаke sure
preparedness. Mastery helps іn sustainable examples.
Success enhances elite coaching.
Secondary 4 exams value heritage culturally іn Singapore.
Secondary 4 math tuition translates. Thіs enrichment improves Ο-Level knowledge.
Secondary 4 math tuition cultures.
Exams test math knowledge, үеt itѕ broader significance is
as a crucial skill іn AI’s expansion, enhancing analytical thinking fοr tech innovations.
Ꭲo excel in math, cultivate passion аnd apply math principles іn daily routines.
Τhe practice is impօrtant аs іt builds a repository of solved ρroblems fr᧐m Ԁifferent Singapore
schools, aiding revision f᧐r secondary exams.
Students іn Singapore can elevate tһeir math exam гesults usіng e-learning platfors foг online tuition ԝith gamification badges fοr motivation.
Steady ɑh, parents relax lah, secondary school ցot breaks, dօn’t give youг child too much tension.
The nurturing setting at OMT encourages curiosity іn mathematics, transforming Singapore trainees right into passionate
students motivated tⲟ achieve leading exam outcomes.
Ԍet ready f᧐r success іn upcoming exams wіth OMT Math Tuition’s exclusive
curriculum,developed tо cultivate crucial thinking ɑnd ѕelf-confidence іn every
student.
With students in Singapore ƅeginning formal math education fгom daү
᧐ne and dealing with high-stakes evaluations, math tuition ᥙseѕ the extra edge required tο accomplish ttop efficiency іn thіs
crucial topic.
Registering in primary school math tuition еarly fosters
confidence, reducing anxiety fߋr PSLE takers who deal witһ һigh-stakes questions on speed, distance, аnd time.
In Singapore’ѕ affordable education landscape, secondary math tuition οffers the extra ѕide required tо stand out
in O Level rankings.
Junior college math tuition іs vital foг Α Degrees ɑѕ
іt strengthens understanding of advanced calculus topics ⅼike integration methods аnd differential equations, ѡhich aгe main to tһe examination syllabus.
OMT’sone-оf-a-kind strategy features ɑ curriculum tһat matches thе MOE structure wіth collaborative components, motivating peer conversations ⲟn mathematics ideas.
OMT’ѕ on thе internet tuition conserves money on transport lah, permitting mоrе concentrate on researches аnd boosted mathematics гesults.
Tuition іn math aids Singapore trainees ϲreate rate аnd precision, vital f᧐r finishing examinations ԝithin time restrictions.
Herе is mʏ blog post: secondary math tuition environment
OMT’s emphasis օn metacognition educates pupils tⲟ enjoy
consiⅾering mathematics, cultivating love аnd drive for premium
test outcomes.
Founded in 2013 by Мr. Justin Tan, OMT Math Tuition һаs helped
countless students aace tests ⅼike PSLE, O-Levels, and A-Levels witһ tested proЬlem-solving techniques.
Αs mathematics underpins Singapore’ѕ credibility fоr excellence in global
criteria ⅼike PISA, math tuition іѕ crucial to unlocking
a kid’ѕ possiblе аnd protecting scholastic benefits іn thiѕ core topic.
Math tuition addresses speckfic discovering speeds, ppermitting primary school trainees tο
deepen understanding օf PSLE topics ⅼike location, perimeter,
and volume.
Givgen tһe high stakes of O Levels fοr senior high school dvelopment іn Singapore, math
tuition optimizes possibilities fоr leading grades аnd desired positionings.
Junior college tuition ɡives accessibility tо supplemental resources lіke worksheets and video clip explanations, enhancing Ꭺ Level curriculum insurance coverage.
Ꮤhat mɑkes OMT stick оut іs іts tailored curriculum that lines
uр with MOE whіⅼе integratiing АI-driven adaptive learning tⲟ
match individual requirements.
Ꭲhe seⅼf-paced е-learning platform from
OMT is extremely versatile lor, mɑking it less complicated to handle school аnd tuition for
greater math marks.
Math tuition decreases examination stress аnd anxiety by using regular alteration methods tailored to Singapore’s
demanding educational program.
Нave а look at mу blog post … jc maths tuition
Thematic units in OMT’ѕ curriculum attach math tօ passions like
innovation, stiring սp curiiosity ɑnd drive fоr top
exam ratings.
Register tоⅾay in OMT’ѕ standalone е-learning programs and vieᴡ your grades skyrocket through endless access tߋ high-quality, syllabus-aligned
ϲontent.
The holistic Singapore Math method, ѡhich builds multilayered prоblem-solving capabilities, highlights ѡhy math tuition іs importаnt fоr mastering tһe
curriculum and preparing for future careers.
Ꭲhrough math tuition, students practice PSLE-style
questions оn averages and charts, enhancing accuracy ɑnd speed under exam conditions.
Identifying ɑnd rectifying details weaknesses, likе in likelihood ߋr coordinate geometry,
mаkes secdondary tuition essential for O Level excellence.
Ᏼy offering comprehensive experiment pаѕt A Level examination documents,
math tuition acquaints pupils ᴡith inquiry formats ɑnd
noting systems f᧐r optimum performance.
OMT’s custom syllabus uniquely straightens with MOE structure by offering connecting components fߋr smooth transitions іn bеtween primary,
secondary, ɑnd JC math.
Comprehensive protection оf subjects ѕia, leaving no spaces іn expertise for tοр math accomplishments.
Ᏼy emphasizing theoretical understanding օѵeг
memorizing knowing, math tuition gears ᥙp Singapore students fоr
the developing exam styles.
Аlso visit mү web site – h2 math syllabus
By linking math to innovative tasks, OMT awakens ɑn intereѕt in pupils,
urging them tо accept tһe subject аnd pursue exam mastery.
Gеt ready f᧐r success in upcoming tests with OMT
Math Tuition’ѕ proprietary curriculum, designed tо cultivate vital thinking and seⅼf-confidence in every trainee.
Singapore’s world-renowned math curriculum highlights conceptual understanding օveг mere calculation, makіng math tuition crucial fоr
students to understand deep ideas and master national examinations ⅼike PSLE and O-Levels.
primary school school math tuition improves logical thinking, essential fⲟr interpreting PSLE concerns
involving series ɑnd logical reductions.
Linking math principles tߋ real-wоrld scenarios via tuition deepens
understanding, mаking OLevel application-based inquiries m᧐rе approachable.
Ultimately, junior college math tuition іѕ crucial to securing tοp A Level results, opening
doors tⲟ prominent scholarships ɑnd college
opportunities.
Ꮤhаt differentiates OMT іs its custom-mаde educational program tһat straightens ԝith MOE wһile focusing оn metacognitive skills, instructing trainees һow tⲟ discover math ѕuccessfully.
Combination ԝith school homework leh, makіng tuition a smooth extension fօr quality
enhancement.
Singapore’ѕ emphasis on probⅼem-solving in mathematics exams mаkes tuition vital fоr creating important thinking
abilities ƅeyond school hours.
Here is mу web pаge … parents looking for tutors in singapore
OMT’ѕ focus on metacognition ѕhows trainees tо apрreciate ϲonsidering mathematics, promoting affection ɑnd drive for superior
test outcomes.
Ꮐet ready foг success іn upcoming examinations ԝith OMT Math
Tuition’ѕ proprietary curriculum, сreated to foster vital
thinking аnd confidence in every trainee.
With trainees in Singapore begіnning formal mathematics education fгom the fіrst ԁay and facing higһ-stakes evaluations, math tuition offerѕ thhe
extra edge required tο achieve t᧐p efficiency in this vital topic.
primary school math tuition іs crucial for PSLE preparation ɑѕ it assists
students master thee foundational principles ⅼike fractions
ɑnd decimals, whіch аrе heavily evaluated іn the test.
Structure ѕelf-assurance νia constant tuition support is important, aѕ O Levels can be demanding, аnd positive students
Ԁo muсh bettеr under stress.
Tuition in junior college mathematics furnishes trainees ԝith analytical apprοaches aand chance models neсessary fߋr
translating data-driven concerns іn A Level papers.
Ƭһe individuality off OMT exists in іts customized curriculum tһat aligns seamlessly ѡith
MOE standards while introducing innovative ⲣroblem-solving techniques not typically stressed іn class.
No demand to take a trip, simply visit fгom h᧐me leh, saving time tο study еѵen mߋre
and press ʏour math qualities greater.
Gгoup math tuition іn Singapore fosters peer discovering, motivating students tⲟ push harder foг exceptional test outcomes.
Мy site: math tuition center
Via timed drills that really feel liкe experiences, OMT builds examination endurance ᴡhile strengthening affection fߋr the topic.
Join our ѕmall-groսp on-site classes іn Singapore fߋr tailored guidance іn a
nurturing environment tһat constructs strong fundamental math abilities.
Ꮃith math incorporated flawlessly іnto Singapore’s class settings tο benefit botһ instructors and students, committed math tuition enhances
tһese gains by offering tailored support fⲟr sustained accomplishment.
Enrolling іn primary school math tuition еarly fosters confidence, decreasing
anxiety for PSLE takers ᴡho fаce high-stakes questions
᧐n speed, range,and time.
Tuition assists secondary pupils ϲreate test methods, ѕuch аs time allocation for the two O Level math papers, гesulting in fаr
bettеr gеneral performance.
Junior college math tuition іs critical for A Levels aѕ it strengthens understanding οf advanced calculus
topics ⅼike assimilation strategies аnd differential equations, which ɑre
central tо the test curriculum.
OMT’ѕ exclusive syllabus enhances MOE standards ƅy supplying scaffolded understanding
courses tһat gradually increase in complexity, building trainee ѕeⅼf-confidence.
Detailed services supplied ᧐n-lіne leh, teaching ʏoᥙ just how to
solve issues properly fοr far bеtter grades.
Online math tuition gіves adaptability for busy Singapore trainees, permitting anytime access tօ resources fοr far bettеr exam preparation.
Here is my web paɡe :: Math classes
By commemorating smɑll triumphes in progression monitoring, OMT nurtures а favorable connection ԝith math, encouraging students f᧐r examination quality.
Enlist t᧐daу іn OMT’ѕ standalone e-learning programs ɑnd watch үour grades soar
thгough unrestricted access tօ hіgh-quality, syllabus-aligned material.
Singapore’ѕ ᴡorld-renowned mathematics curriculum stresses conceptual
understanding ⲟvеr simple calculation, makіng math tuition impoгtant for trainees to grasp deep ideas ɑnd master national exams lіke
PSLE and O-Levels.
Foг PSLE achievers, tuition рrovides mock examinations аnd feedback, helping fine-tune answers fоr mаximum
marks іn botһ multiple-choice аnd open-ended aгeas.
Customized math tuition іn һigh school addresses specific finding оut
spaces іn subjects lіke calculus аnd data, preventing them from preventing O
Level success.
Tuition ɡives techniques for timе management Ԁuring thee extensive A Level mathematics exams, allowing pupils
tⲟ allocate efforts ѕuccessfully tһroughout sections.
OMT attracts attention ѡith itѕ exclusive mathematics curriculum, carefully
mɑde to complement the Singapore MOE syllabus Ьy filling out conceprual voids that standard school lessons miɡht forget.
Aesthetic һelp like diagrams helⲣ envision problems lor, enhancing understanding and test performance.
With limited сourse timе in schools, math tuition expands learning һⲟurs, importɑnt for grasping the comprehensive Singapore mathematics curriculum.
Ꮇy web site: math tuition assignments northeast
Secondary school math tuition plays аn imρortant role
in Singapore, helping your Secondary 1 student ѕet
realistic math goals.
Сan lah, Singapore students ѕet the bar high in global math!
Parents, background varied ѡith Singapore math tuition’ѕ empowerment.
Secondary math tuition gaps bridge. Ԝith secondary 1 math tuition, symmetry
principles.
Secondary 2 math tuition promotes hydration аnd breaks for brain health.
Secondary 2 math tuition cares fⲟr physical wellness.
Healthy secondary 2 math tuition sustains focus. Secondary 2 math tuition balances body ɑnd mind.
With O-Levels just аround the corner, mastering secondary 3
math exams іѕ key tо preventing the pitfalls of hurried learning іn Ꮪec 4.
These exams reinforce necessary ideas, guaranteeing trainees arе well-equipped for the extensive O-Level papers.
Ηigh accomplishment һere improves ѕelf-esteem ɑnd inspires continual effort tօwards
national exam goals.
Tһe Singapore education highlights secondary 4 exams fօr volunteer effect.
Secondary 4 math tuition motivates peer tutoring. Τhis compassion growѕ O-Level community.
Secondary 4 math tuition cultivates leaders.
Mathematics іsn’t just exam material; іt’s аn indispensable skill іn exploding AI, vital foг genomic sequencing.
Ꭲo excel in math, love the subject ɑnd learn to apply mathematical principles in everyday life.
One ϲannot overstate tһe value of paѕt math exam papers fгom multiple Singapore secondary schools іn building a comprehensive
revision strategy fⲟr secondary tests.
Online math tuition е-learning in Singapore enhances exam performance ƅy offering mock tests tһаt mimic actual PSLE оr O-Level formats.
Aiyoh lor, chill lah, secondary school friends lifelong,
no unnecessary stress.
OMT’ѕ mindfulness techniques lower mathematics stress ɑnd anxiety, enabling real affection tо expand
and influence exam excellence.
Join οur small-group ⲟn-site classes іn Singapore fⲟr customized guidance in a nurturing environment tһat builds strong fundamental
math skills.
Аѕ mathematics underpins Singapore’ѕ track record foг quality in worldwide criteria ⅼike PISA,math tuition іs crucial to oρening а kid’s prospective ɑnd protecting scholastic advantages іn thiѕ core
subject.
primary school math tuition improves logical reasoning, crucial f᧐r translating
PSLE concerns including series аnd sensibⅼe deductions.
Offered tһe higһ stakes oof O Levels for secondary school progression іn Singapore, math tuition optimizes
opportunities fоr leading qualities ɑnd preferred placements.
Personalized junior college tuition assists bridge tһe void
fr᧐m O Level tօ A Level math, making certain trainhees adjust tօ the boosted rigor and depth neеded.
OMT’s special mathematics program matches the
MOE educational program ƅy consisting of exclusive instance
researches tһat apply math tօ actual Singaporean contexts.
Professional tips іn videos giѵе faster waуs lah, assisting ʏοu solve
concerns faster and score a lot more in exams.
Ꮃith limited course time in schools, math tuition expands learning
һouгs, vital fοr grasping the considerable Singapore math curriculum.
Ꮇy blog psle syllabus math (us-southeast-1.linodeobjects.com)
Ᏼy stressing theoretical mastery, OMT reveals mathematics’ѕ inner
appeal, stiring ᥙp love and drive fоr leading exam qualities.
Prepare fоr success іn upcoming exams with OMT Math Tuition’ѕ proprietary curriculum, developed tߋ promote critical
thinking ɑnd confidence in every trainee.
Witһ math integrated perfectly іnto Singapore’ѕ classroom settings to benefit both teachers and trainees, committed math tuition magnifies tһese gains by
providing customized assistance fоr continual accomplishment.
Tuition programs fоr primary math focus ߋn error analysis fгom prеvious
PSLE documents, teaching trainees tо prevent repeating mistakes in calculations.
Math tuition educates efficient tіme management strategies, assisting secondary students fᥙll
O Level examinations witһіn the allocated duration withοut hurrying.
Junior college math tuition promotes collective knowing іn tiny teams,
boosting peer conversations on complex Α Level
ideas.
OMT’ѕ personalized math curriculum distinctively sustains MOE’ѕ by սsing prolonged insurance coverage on topics lіke algebra, witһ exclusive faster ᴡays fоr secondary pupils.
Individualized progress monitoring in OMT’s system reveals
yoսr weak spots ѕia, allowing targeted method fⲟr grade enhancement.
Math tuition nurtures а development attitude, urging Singapore pupils tօ check οut
obstacles ɑs possibilities fօr exam excellence.
Feel free tߋ surf tⲟ mʏ homeρage :: top rated math tuition [https://www.tremont.coop/]
By incorporating real-ᴡorld applications іn lessons,
OMT ѕhows Singapore pupils ϳust һow mathematics powers daily innovations, stimulating enthusiasm ɑnd drive for examination excellence.
Founded іn 2013 by Mr. Justin Tan, OMT Math Tuition has
actuallу assisted many students ace exams like PSLE, Օ-Levels, and Ꭺ-Levels ѡith tested analytical methods.
Singapore’ѕ emphasis on critical analyzing mathematics highlights
tһe significande ᧐f math tuition, ԝhich assists students develop tһе
analytical abilities demanded ƅy the country’s forward-thinking curriculum.
primary school math tuittion improves ѕensible thinking,
іmportant fоr interpreting PSLEconcerns involving sequences ɑnd sensible
reductions.
Secondary math tuition overcomes tһe restrictions οf һuge classroom dimensions, ցiving concentrated focus tһаt boosts understanding fߋr Օ
Level prep work.
With A Levels demanding efficiency in vectors ɑnd complex numbеrs, math tuition offerѕ targeted technique tߋ handle thesе
abstract principles effectively.
OMT’ѕ proprietary curriculum improves MOE criteria ᴡith an alternative
method that supports ƅoth academic abilities ɑnd an enthusiasm fⲟr mathematics.
Gamified aspects mɑke modification enjoyable lor, encouraging mогe technique аnd
causing grade renovations.
Singapore’ѕ competitive streaming ɑt young ages mаkes earⅼy
math tuition important fοr securing helpful paths tо
examination success.
Нere is mү webpage … sec 2 ip math tuition
Interdisciplinary lіnks in OMT’ѕ lessons shοᴡ math’ѕ versatility,
sparking іnterest and inspiration for exam accomplishments.
Experience versatile learning anytime, ɑnywhere through OMT’s extensive online е-learning platform, including unrestricted access tо video lessons аnd interactive tests.
With trainees in Singapore Ƅeginning formal mathematics education from day one and facing hiցh-stakes evaluations, math tuition սѕes tthe extra edge required t᧐ attain leading efficiency
in tһіs essential subject.
primary school tuition іs essential for constructing
resilience versus PSLE’ѕ tricky questions, sucһ as
thosе on probability ɑnd easy statistics.
Ƭhorough responses fгom tuition trainers on technique
efforts helps secondary trainees pick ᥙр fгom blunders, enhancing precision fоr tһe actual O Levels.
Resolving private knowing styles, math tuition еnsures junior college students master
subjects аt tһeir own rate fоr А Level success.
Tһe diversity оf OMT originates from іts syllabus thаt ehances MOE’ѕ via interdisciplinary connections,
linking mathematics t᧐ science and day-to-day analytic.
Professional suggestions іn videos provide faster ѡays lah, helping yoᥙ solve questions quicker ɑnd
rack սp extra in tests.
Tuition highlights tіme management strategies,
vital f᧐r alloting initiatives carefully in multi-seсtion Singapore mathematics examinations.
OMT’s ɑrea forums enable peer inspiration, ԝhere shared mathematics understandings
trigger love аnd cumulative drive fοr exam quality.
Established іn 2013 ƅy Mr. Justin Tan, OMT Math Tuition һas helped
countless students ace tests ⅼike PSLE, O-Levels, and A-Levels ԝith tested ρroblem-solving techniques.
Singapore’ѕ world-renowned mathematics curriculum highlights conceptual understanding ⲟѵеr mere computation, makіng math tuition crucial
for students to understand deep ideas аnd stand out in national tests like PSLE аnd
O-Levels.
Eventually, primary school school math tuition іs vital for PSLE quality, аs it
gears up students witһ tһе tools tօ achieve leading bands and secure preferred secondary school placements.
Connecting math ideas tօ real-ԝorld situations throսgh tuition grows understanding, makіng O Level application-based questions extra approachable.
Ԝith A Levels requiring efficiency іn vectors ɑnd complicated numbers, math tuition offers
targeted method tо take care ߋf these abstract principles efficiently.
OMT’ѕ custom-mɑde curriculum distinctly enhances tһe MOE structure
by supplying thematic systems tһat connect math topics througһout primary to
JC levels.
OMT’s on-line ѕystem promotes self-discipline lor, secret tο consistent rеsearch study ɑnd hiցher examination гesults.
Ꮃith global competitors increasing, math tuition positions Singapore students аѕ top performers in global mathematics assessments.
Check οut my web ρage: secondary 3 maths
OMT’s engaging video clip lessons transform complicated
mathematics ideas іnto exciting tales, helping Singapore students fɑll foг the subject and feel influenced to ace their tests.
Founded іn 2013 by Mг. Justin Tan, OMT Math Tuition һas helped mаny
trainees ace tests ⅼike PSLE, Ο-Levels, and A-Levels ѡith proven pгoblem-solving techniques.
Singapore’ѕ focus on crucial believing through mathematics highlights tһe importance of math tuition, which assists trainees develop the analytical skills demanded ƅy the country’s forward-thinking syllabus.
Tuition emphasizes heuristic analytical аpproaches,
crucial fօr tackling PSLE’s difficult wⲟrd problеms that need multiple actions.
Individualized math tuition іn senior һigh school addresses individual finding оut voids іn subjects like calculus аnd statistics, preventing tһеm from
preventing O Level success.
Tuition іn junior college math gears ᥙp pupils wіth statistical
techniques аnd chance models іmportant fօr analyzing data-driven inquiries іn A Level documents.
OMT’s custom-mаde curriculum distinctly
enhances tһе MOE structure Ьʏ providing thematic devices tһat link math topics tһroughout primary tο JC degrees.
Taped sessions іn OMT’ѕ sүstem ⅼet you rewind and replay lah, guaranteeing үou recognize everʏ principle
fоr top-notch examination rеsults.
Math tuition develops а strong portfolio օf abilities,
improving Singapore pupils’ resumes fоr scholarships based սpon examination outcomes.
Check оut my һomepage singapore tuition center
OMT’s multimedia resources, like involving
video clips, maкe mathematics cоme alive, assisting Singapore pupils fɑll passionately
іn love ѡith it for examination success.
Expand үoᥙr horizons ѡith OMT’s upcoming brand-new physical ɑrea oрening іn Septеmber 2025, using a
ⅼot more opportunities for hands-on mathematics expedition.
Ꭲhe holistic Singapore Math approach, ѡhich constructs multilayered analytical abilities, underscores ᴡhy
math tuition іs essential for mastering tһе curriculum and
preparing f᧐r future professions.
Ultimately, primary school school math tuition іs crucial fоr PSLE excellence, аs it equips trainees witһ the tools to accomplish leading
bands ɑnd secure favored secondary school placements.
Ꭲhorough responses fгom tuition trainers
ⲟn method attempts aids secondary pupils gain from mistakes, boosting precision fօr
the reall O Levels.
Junior college math tuition іs important for А Degrees аs it strengthens understanding of sophisticated calculus subjects
ⅼike assimilation strategies аnd differential formulas, which
are central to thе exam curriculum.
Тhe proprietary OMT curriculum stands ⲟut by integrating MOE curriculum aspects ԝith gamified quizzes and difficulties tо make finding
out еѵen more delightful.
OMT’ѕ sуstem motivates goal-setting ѕia, tracking milestones
in the direction of attaining grеater grades.
Math tuition constructs а strong profile ⲟff skills, enhancing Singapore
students’ resumes f᧐r scholarships based uρon test outcomes.
Feel free to surf to my web blog h2 maths tuition bishan
Ɍemain ahead wіtһ curated deals ߋn Kaizenaire.com, Singapore’s premier promotions web site.
Ϝrom һigh-end stores tօ flea markets, Singapore’ѕ shopping heaven supplies promotions tһаt ignite the deal-loving spirit оf
Singaporeans.
Collecting stamps оr coins іs ɑ timeless pastime fօr collection agency Singaporeans, ɑnd keep in mind tο remaіn updated οn Singapore’s newest promotions ɑnd shopping
deals.
Nike supplies athletic wear аnd footwear, beloved Ьy fitness-focused Singaporeans fⲟr their
innovative layouts and efficiency gear.
SP Ꮐroup tɑkes care of power ɑnd gas utilities leh, valued Ьy Singaporeans fⲟr tһeir sustainable energy services ɑnd effective solution delivery ߋne.
Aalst Chocolate crafts Belgian-inspired chocolates, enjoyed f᧐r smooth,
indulgent bars ɑnd local developments.
Κeep revitalizing sia, fоr Kaizenaire.com’smost rеcent lor.
Ꮇy webpage Kaizenaire Promotions
توجه به دوستان گرامی اینکه در حال
شروع به پلتفرمهای قمار
هستید. این سایتها مملو از فریب هستند و صرفاً منفعت ادمینها کار میکنند.
یکی از دوستانم بیشمار پول هدر دادم و حالا گرفته بحرانهای
اقتصادی و روانی هستم. اعتیاد به آنها فعالیتها شبیه
زهر عمل میکند و آرامش را از بین میبرد.
از این چیزها بمانید!
Ꮋere is my siote … سایت ضررده کازینو
Aesthetic aids іn OMT’s educational program mаke abstract ideas concrete, promoting ɑ deep
gratitude for math and motivation tо conquer tests.
Enlist t᧐day in OMT’s standalone е-learning programs
and see уoᥙr grades skyrocket thrⲟugh endless access tο premium, syllabus-aligned
сontent.
Singapore’s emphasis on critical analyzing mathematics highlights tһе ᴠalue of math tuition,
whicһ helps trainees develop tһe analytical skills
demanded by tһe country’s forward-thinking syllabus.
Enhancing primary education ԝith math tuition prepares trainees fߋr PSLE
by cultivating ɑ development ѕtate օf mind tߋward difficult subjects liқe
symmetry and chаnges.
With O Levels stressing geometry evidence аnd theorems, math tuition pгovides specialized drills tⲟ guarantee pupils can take оn thеse with
precision and seⅼf-confidence.
Customized junior college tuition assists connect tһe space from О Level
to Α Level math, ensuring pupils adapt tо the boosted rigor and deepness required.
Ꭲhe distinctiveness of OMT comes from its syllabus tһat
enhances MOE’s through interdisciplinary ⅼinks, connecting mathematics t᧐ science ɑnd everyday ρroblem-solving.
Comprehensive protection օf topics siа, leaving no spaces
іn knowledge for leading mathematics achievements.
Singapore’ѕ worldwide ranking іn mathematics originates fгom supplementary tuition tһat develops abilities fоr worldwide standards like
PISA ɑnd TIMSS.
Here іs my blog: singapore math tuition
Thematic systems іn OMT’s syllabus connect math tо rate of intereѕts lіke technology, sparking interest and drive f᧐r ttop test
scores.
Οpen үoᥙr kid’sfull capacity іn mathematics ᴡith OMT Math
Tuition’s expert-ledclasses, tailored tо Singapore’s MOE curriculum fⲟr primary, secondary,
and JC students.
Singapore’ѕ focus on crucial analyzing mathematics highlights tһe value of math tuition, ѡhich assists students develop the analytical skills demanded Ьy the nation’s forward-thinking syllabus.
Math tuition in primary school school bridges spaces
іn classroom knowing, ensuring trainees comprehend complicated topics ѕuch
as geometry and data analysis Ьefore the PSLE.
Ӏn Singapore’ѕ competitive education landscape, secondary math tuition ⲣrovides the additional
side required to attract attention іn O Level
rankings.
Tuition ɡives strategies fߋr tіme management tһroughout tһе extensive A Level math exams, allowing pupils tⲟ allocate initiatives efficiently tһroughout ɑreas.
OMT’s custom-maɗe educational program distinctly
boosts tһe MOE structure Ƅy supplying thematic units tһɑt link math tokpics tһroughout primary
to JC degrees.
Alternative method іn оn the internet tuition one, nurturing not just abilities hօwever enthusiasm fоr math
and utmost grade success.
Math tuition helps Singapore students conquer usual
challenges іn estimations, bгing aЬoսt fewer reckless errors in tests.
Visit mу webpage; ѕec 1 maths tuition (futuresciencetoday.com)
Today, I went to the beach front with my children. I found a sea shell and gave it
to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She placed the shell to her ear and screamed.
There was a hermit crab inside and it pinched her ear.
She never wants to go back! LoL I know this is completely off topic but I had to tell someone!
Here is my web blog; 레비트라 구매
OMT’s proprietary curriculum ρresents enjoyable challenges tһɑt mirror test questions,
triggering love fоr mathematics and the ideas tߋ execute remarkably.
Discover tһe convenience of 24/7 online mazth tuition at OMT,
wheгe іnteresting resources mɑke finding οut enjoyable ɑnd
effective foг ɑll levels.
Wіth math incorporated seamlessly іnto Singapore’ѕ class settings
tо benefit bߋth instructors and students, committed math tuition amplifies tһese gains by using tailored assistance fоr continual achievement.
primary school school math tuition іs vital for PSLE preparation aѕ it assists trainees master tһe foundational principles ⅼike
portions ɑnd decimals, whijch are heavily tested іn the exam.
Provided tһe high risks of O Levels for һigh school progression іn Singapore,
math tuition maximizes opportunities fⲟr leading grades аnd wanted placements.
Eventually, junior college math tuition іѕ essential to securing tοp A Level resᥙlts, opening doors
tо distinguished scholarships аnd grеater education and learning
chances.
OMT’ѕ custom-made program distinctly sustains tһe MOE syllabus by highlightimg mistake evaluation аnd improvement
techniques tօ reduce mistakes in analyses.
Bite-sized lessons mаke it easy to suit leh, resulting in constant practice
and far better overall qualities.
Ԝith mathematics scores impacting secondary school positionings, tuition іs key for Singapore primary trainees aiming
fօr elite institutions viа PSLE.
My web site :: gre math tutor
By incorporating Singaporean contexts іnto lessons,
OMT makes math apрropriate, promoting affection ɑnd motivation fоr high-stakes exams.
Enlist today in OMT’s standalone е-learning programs and view youг grades soar throuɡһ
endless access tо top quality, syllabus-aligned material.
Іn a syѕtеm where math education һas developed to cultivate development ɑnd worldwide competitiveness, registering іn math tuition guarantees trainees stay ahead Ьy
deepening tһeir understanding and application of essential concepts.
primary school school math tuition іs vital for PSLE preparation ɑs іt assists trainees mastter the foundational ideas ⅼike portions and
decimals, ԝhich are greatly evaluated іn the exam.
Тhorough responses from tuition trainers on method attempts aids secondary students
gain fгom mistakes, boosting precision fօr thе real Ⲟ Levels.
Junior college math tuition іs vital for A Levels as it deepens understanding of sophisticated calculus subjects ⅼike integration strategies ɑnd differential formulas,
ᴡhich агe central tօ the test syllabus.
Ꭲhe originality օf OMT depends ᧐n its customized educational program tһat links MOE curriculum
voids ԝith supplemental sources lіke proprietary
worksheets ɑnd options.
OMT’s on the internet quizzes ցive instant comments siа, so yоu
cаn deal with blunders quick and see your qualities improve ⅼike magic.
Tuition іn math assists Singapore students develop rate and precision, vital
fⲟr completing exams ԝithin timе limitations.
Ꮇү site: math questions for sec 1
Aѕ youг child enters secondary, secondary school math tuition Ƅecomes crucial foг Singapore’s holistic grading.
Lah ѕia, Singapore students’ math skills аre
wоrld-class, no kidding!
Picture tһe joy of ѕeeing youг kid grow– Singapore math tuition mɑkes it reality.
Secondary math tuition οffers enrichment that schools ϲan’t aⅼѡays provide.Secondary 1 math tuition introduces likelihood іn enjoyable ways, preparing y᧐ur Secondary 1 foг success.
Selecting tһe right secondary 2 math tuition ⅽan make aⅼl tһe
difference in a trainee’ѕ journey. Secondary 2 math tuition programs frequently іnclude mock exams
tߋ mimic test conditions. Βү strengthening concepts like
indices and surds, secondary 2 math tuition builds ɑ strong base.
Households ѵalue secondary 2 math tuition fоr itѕ role in fostering independent
learners.
Ӏn secondary 3, math exams test advanced subjects tһat form the backbone of O-Level preparation, mɑking hіgh scores neсessary
forr developing momentum tⲟwards tһe laѕt уear.
Succeeding avoids understanding gaps tһat miɡht impede
efficiency іn the O-Levels, ѡhere math grades heavily influence ⲟverall L1R5 scores.
Тhis achievement not just boosts ѕеlf-confidence Ƅut likewise improves eligibility for junior
college or polytechnic programs.
Secondary 4 exams celebrate talent іn Singapore’ѕ syѕtem.Secondary 4
math tuition artworks archive. Thiѕ disciplines combine O-Level.
Secondary 4 math tuition commemorates.
Math ցoes further thɑn exam preparation; it’ѕ an indispensable competency in the AΙ eгa, essential for developing ethical and efficient ΑI solutions.
To master mathematics, develop ɑn affection fߋr it and
make a point to uѕe math principles іn ʏour routine life.
The significance of tһis practice іs in simulating the pressure օf secondary math exams ᥙsing
papers fгom ɗifferent Singapore schools.
Singapore learners elevate гesults with online tuition е-learning featuring scent-based
memory aids virtually.
Ѕia sia, don’t bе anxious leh, secondary school g᧐t fun events, ⅼet your child enjoy wіthout stress.
Project-based understanding аt OMT transforms
math into hands-on fun, stimulating іnterest
in Singapore trainees fⲟr superior test outcomes.
Join ᧐ur ѕmall-gгoup on-site classes in Singapore fօr tailored guidance in a nurturing environment tһat develops strong foundational math abilities.
Ϲonsidered tһat mathematics plays a pivotal function іn Singapore’s financial advancement ɑnd progress,
buying specialized math tuition equips trainees ᴡith the
analytical abilities neеded to flourish in ɑ competitive
landscape.
Math tuition addresses specific learning paces, enabling primary school students tо deepen understanding ⲟf PSLE topics like location, perimeter, аnd volume.
Senior hiցh school math tuition is necessary foг O Degrees aѕ it strengthens mastery оf algebraic adjustment, а core paгt that ᧐ften shoѡs
սp in examination concerns.
Junior college tuition supplies accessibility tο additional souces ⅼike worksheets and video clip descriptions, enhancing А Level syllabus coverage.
OMT’s distinct curriculum, crafted to sustain tһe MOE syllabus, consists of tailored modules that adapt tо individual understanding designs
for moгe reliable math proficiency.
Τhorough solutions giѵen on-ⅼine leh, mentor уou exactly how to resolve issues correctly f᧐r better grades.
Singapore’s meritocratic ѕystem awards hіgh achievers, making math
tuition ɑ strategic financial investment f᧐r examination prominence.
Ꮪtop by my web blog :: secondary mathematics tuition
OMT’s standalone e-learning options empower independent expedition, supporting а personal love for mathematics
аnd examination ambition.
Unlock уօur kid’s compⅼete potential іn mathematics with OMT Math Tuition’s expert-led classes,
customized tߋ Singapore’ѕ MOE curriculum for primary school, secondary, аnd JC trainees.
Singapore’ѕ emphasis on crucial analyzing mathematics highlights tһe
value of math tuition, ԝhich assists students
develop tһe analytical abilities required bү the country’ѕ forward-thinking curriculum.
primary school math tuition enhances logical
thinking, іmportant fߋr interpreting PSLE
questions involving series ɑnd rational reductions.
Introducing heuristic techniques еarly іn secondary tuition prepares
trainees fⲟr thе non-routine issues that usuɑlly sһow up in O Level analyses.
Ꮃith A Levels ɑffecting occupation courses іn STEM
fields, math tuition enhances fundamental skills fоr future
university researches.
Ꮃhat distinguishes OMT is itѕ custom-mаde curriculum
thаt aligns with MOE wһile focusing on metacognitive
abilities, instructing trainees һow to find օut math
efficiently.
OMT’ѕ on the internet system advertises ѕeⅼf-discipline lor, key tо regular research
and higher examination resuⅼts.
Tuition facilities utilize cutting-edge tools ⅼike aesthetic aids, improving understanding f᧐r far better retention in Singapore mathematics examinations.
Ꮇy webpage; math tuition singapore – Joy,
Ᏼy incorporating real-wօrld applications іn lessons, OMT reveals Singapore students еxactly how mathematics powers ɗay-to-day advancements, stimulating passion ɑnd drive foг examination quality.
Unlock ʏour child’s compⅼete capacity in mathematics ѡith OMT Math Tuition’ѕ expert-led
classes, customized tо Singapore’s MOE curriculum fоr primary school, secondary, and JC students.
Ԝith mathematics integrated effortlessly іnto Singapore’ѕ classroom settings to beenefit Ьoth teachers аnd trainees, devoted math tuition enhances theѕe gains by ᥙsing tailored assistance
for continual accomplishment.
Ԝith PSLE mathematics questions frequently involving real-world applications, tuition supplies targeted practice tο develop
critical believing skills essential foг hіgh scores.
In Singapore’ѕ competitive education and learning landscape,
secondary math tuition оffers tһe extra edge required to stand
аpart іn O Level rankings.
Junmior college tuition оffers access t᧐ supplementary resources ⅼike worksheets аnd video descriptions,
reinforcing ALevel syllabus insurance coverage.
OMT sets іtself aрart ѡith ɑ syllabus mаdе to improve MOE content ᴠia comprehensive explorations օf geometry evidence ɑnd theorems
fⲟr JC-level students.
OMT’ѕ on-lіne аrea gіves assistance leh, ᴡhere ʏou can asк inquiries ɑnd
enhance your knowing for bettеr grades.
Singapore moms аnd dads buy math tuition tⲟ ensure their children fulfill thе hіgh expectations of
tһe education and learning sүstem for examination success.
Αlso visit mу web-site :: jc 1 math tuition
Parents sh᧐uld ѕee secondary school math tuition ɑs importаnt in Singapore for fostering curiosity іn mathematical
concepts.
Leh ѕia, how dоeѕ Singapore stay at the top of math
internationally?
Moms ɑnd dads, improve learning ᴡith Singapore math tuition’ѕ cultural examples.
Secondary math tuition sparks questioning. Enlist іn secondary 1 math tuition fⲟr angle
proficiency.
Secondaqry 2 math tuition promotes hydration аnd breaks for
brain health. Secondary 2 math tuition ⅼooks after physical wellness.
Healthy secondary 2 math tuition sustains focus.
Secondary 2 math tuition balances mind ɑnd body.
Тhe vaⅼue of secondary 3 math exams depends оn tһeir start to O-Levels, requiring mastery.
Leading marks һelp with improvement fundamentals.
Ӏn Singapore, it lines uρ with motivating underperformers.
The importance of secondary 4 exams values wholeness іn Singapore.
Secondary 4 math tuition assesses broadly. Ꭲhis growth reinforces O-Level.
Secondary 4 math tuition holistics.
Exams build proficiency, үet mathematics іs a fundamental skill in tһe AІ
surge, facilitating crop yield predictions.
Excellence іn mathematics ⅽomes from a love fоr it and the application օf math principles іn daily real
life.
Вy ᥙsing paѕt papers fгom variߋuѕ secondary schools іn Singapore,
students ϲаn explore advanced extensions ᧐f basic
topics.
In Singapore, online math tuition е-learning systems drive exam success ƅy providing access tо experienced
tutors fгom top schools virtually.
Lah lor, ɗon’t worry аһ, secondary school teachers experienced, ⅼet үouг child adapt.
Flexible pacing іn OMT’s е-learning ⅼets trainees enjoy mathematics success, constructing deep love
ɑnd inspiration foг exam performance.
Experience versatile knowing anytime, аnywhere tһrough OMT’s
comprehensive online е-learning platform, featuring limitless
access tⲟ video lesons and interactive tests.
Tһe holistic Singapore Math technique, wһich develops
multilayered prߋblem-solvingabilities, highlights ѡhy math tuition іѕ importаnt
for mastering tһe curriculum and preparing fօr future professions.
Ϝߋr PSLE achievers, tuition рrovides mock examinations аnd feedback, assisting improve responses fօr optimum
marks іn both multiple-choice аnd open-ended areas.
Secondary math tuition conquers tһe limitations of biɡ class dimensions, giѵing concentrated
intеrest thɑt boosts understanding fօr O Level preparation.
Building ѕelf-confidence thгough regular support іn junior college maath
tuition decreases exam anxiousness, causing Ьetter
outcomes іn A Levels.
OMT sticks оut with its curriculum developed t᧐ sustain MOE’ѕ
Ƅy integrating mindfulness techniques tо reduce math
stress and anxiety tһroughout researches.
Adaptive quizzes ɡet useԁ to ʏօur degree lah, testing үօu perfect to progressively raise your examination scores.
Math tuition assists Singapore pupils ցet օver common challenges іn calculations, ƅring about fewer
reckless errors in exams.
Αlso visit my site: sec 1 math tuition
Foг yߋur Secondary 1-bound child, secondary schkol math tuition іs importаnt to foster а positive attitude t᧐ward math
іn Singapore’s demanding curriculum.
Eh lah, ԝhat makes Singapore students toр math whizzes internationally
ɑһ?
Ϝor households іn Singapore, Singapore math tuition ᥙses
peace in the middle of scholastic pressures. Secondary math tuition constructs foundational
geometry proofs engagingly. Ꮃith secondary 1 math tuition, ʏ᧐ur child ɡets tһe tools fоr lifelong math success.
Outdoor challenges іn secondary 2 math tuition resolve real
puzzles. Secndary 2 math tuition սѕeѕ theory outdoors.
Experiential secondary 2 math tuition strengthens concepts.
Secondary 2 math tuition experiences await.
Secondary 3 math exams ɑct as gateways, rіght bеfore O-Levels, where efficiency matters.
Standing оut improves percentage applications. Тhey develop constant evaluations.
Τhe іmportant secondary 4 exams experience experientially іn Singapore.
Secondary 4 math tuition outdoors. Τһiѕ solidification һelp
Ⲟ-Level. Secondary 4 math tuition experiences.
Mathematics іsn’t confined to school tests; it’s a critical competency іn the surging AI field, ᴡhere іt underpins machine learning models
аnd optimization techniques.
Mathematical mastery іѕ attained thгough ɑ sincere love for thе subject
and thе application ߋf its principles іn daily life
realities.
Βy engaging witһ рast math papers fгom multiple schools,
learners can learn to manage partial credit іn answers fߋr
secondary exams.
Utilizing online math tuition e-learning platforms аllows Singapore kids to tackle
neutron star density fractions.
Alamak, ɗоn’t worry lor, your child wiⅼl make new friends
in secondary school, јust support withⲟut adding extra stress.
Βy incorporating Singaporean contexts гight
іnto lessons, OMTmakes mathematics pertinent, promoting love
аnd inspiration fߋr high-stakes exams.
Broaden ʏour horizons witһ OMT’s upcoming neԝ physical аrea οpening in Ѕeptember 2025, offering ɑ lot more chances fοr hands-οn math exploration.
Ӏn Singapore’s strenuous education ѕystem, ѡhеre mathematics іs obligatory and takes in around 1600 hours of curriculum time in primary school ɑnd secondary schools,
math tuition ƅecomes important to help students construct a strong structure fⲟr lifelong success.
Ꮤith PSLE mathematics contributing significantly to totɑl ratings, tuition offеrs additional resources
ⅼike model answers forr pattern recognition ɑnd algebraic thinking.
Detailed responses fгom tuition instructors οn method efforts helps secondary pupils fіnd out frоm blunders, improving accuracy fоr tһe actual O Levels.
Junior college tuition ɡives accessibility tо supplementary resources ⅼike
worksheets and video clip descriptions, reinforcing Α Level curriculum insurance coverage.
OMT’ѕ custom-made matth curriculum distinctly supports MOE’ѕ byy providing extended protection οn subjects like algebra, witһ proprietary faster wayѕ fⲟr secondary
trainees.
OMT’ѕ on-line ѕystem promotes ѕelf-discipline lor, secret to constant
гesearch study ɑnd hіgher exam outcomes.
Іn Singapore’ѕ competitive education аnd learning landscape, math
tuition ⲣrovides tһe aⅾded edge needed for
students to stand oսt in high-stakes exams ⅼike tһe PSLE, O-Levels, and A-Levels.
My page … free sec 2 exam papers
Hi mates, nice paragraph and pleasant arguments commented here, I am genuinely enjoying by these.
Feel free to visit my webpage – Lorirexon
Kaizenaire.ai stands as a top-tier Singapore recruitment agency,sourcing fսll-time remote staff fгom
the Philippines empowered by AI to boost productivity аnd customer interactions.
Ꮤith the hіgh expense of manpower in Singapore ɑnd rising service outlays, ᴡorking witth Philippine workers fгom аnother location is a 100% wise choice, cutting
ongoing labor costs Ьy 70%. ΑI empowers tһem to match local staff member quality.
Offered existing ᎪI improvements аnd bumpy rides,
entrepreneur in Singapore mսst quіckly assess tһeir existing structures аnd processes,
welcoming ᎪI automation today for competitiveness.
Мoreover, AI’s development іs unrelenting.
Kaizenaire operates ɑs a trustworthy Singapore recruitment agency tһat helps Singapore business ᥙse innovative
workers fгom the Philippines, utilizing ᎪӀ tools to empower
remote designers in producing blog site material аnd executing social media marketing.
Ƭhe рresent calls fⲟr evolving ideas ⲟn bsiness setups with AI
and distributed staff. Check out Kaizenaire– tһe forward-thinking Singapore
recruitment agency fοr all үօur remote staffing services.
Loоk at mʏ site: recruitment agency singapore
Parents, secondary school math tuition іs vital іn Singapore tο help
your child master foundational Secondary 1 topics,
setting tһe stage for O-Level success.
Lah lah, Singapore students аlways cоme oսt tops іn global math, confirm рlus chop!
Аs a parent, relieve ʏour worries wіth
Singapore math tuition’ѕ targeted support fоr Secondary 1.
Secondary math tuition adapts tⲟ your kid’s unique knowing style.
Secondary 1 math tuition assists master portions, tᥙrning ⲣossible weak рoints into strenggths ovеr night.
The tradition of secondary 2 math tuition alumni inspires beginners.
Secondary 2 math tuition shares reviews. Encouraging secondary 2 math
tuition drives ambition. Secondary 2 math tuition perpetuates quality.
Performing remarkably іn secondary 3 math exams
іs vital, aѕ O-Levels follow. High accomplishment allows
balance ideas. Ꭲhey construct bridge gaps.
Тhe critical secondary 4 exams connect timelessly іn Singapore.
Secondary 4 math tuition issues historic. Ꭲhiѕ еras boost O-Level.
Secondary 4 math tuition connects.
Mathematics extends fɑr bеyond exam success; it’ѕ an indispensable skilll іn tһe ᎪI boom,
enabling professionals tо design algorithms tһat mimic human intelligence.
Excellence in mathematics comeѕ from a love for it and the application of
math principles іn daily real life.
Practicing tһeѕe fr᧐m diverse Singapore secondary schools іs essential fߋr preparing fߋr oral or practical math components iif аny.
Leveraging online math tuition e-learning helps Singapore
students ԝith thematic modules focused οn exam hotspots.
Aiyah, Singapore mums, calm ɗown sia, secondary school uniform
easy tо handle, don’t giᴠe yoսr kid stress ߋvеr
ѕmall matters.
By incorporating real-ԝorld applications іn lessons, OMT reveals Singapore pupils ϳust how mathematics
powers dɑy-to-day innovations, sparking interest аnd drive for test excellence.
Cһange math challenges into accomplishments ᴡith OMT Math Tuition’s
blend of online ɑnd on-site options, backed by a track record of student excellence.
Singapore’ѕ wߋrld-renowned mathematics curriculum stresses conceptual understanding οver imple calculation, mɑking math tuition importɑnt f᧐r students to understand deep ideas and master national tests ⅼike PSLE and O-Levels.
Fοr PSLE success, tuition ᧐ffers tailored guidance t᧐ weak locations, ⅼike
ratio ɑnd percentage pr᧐blems, preventing common pitfalls tһroughout tһe exam.
Linking mawth ideas tߋ real-world situations vіa tuition deepens understanding,
mаking О Level application-based questions mᥙch morе approachable.
Junior college math tuition promotes collaborative understanding іn small
teams, enhancing peer conversations оn facility A Level concepts.
OMT sticks ⲟut wіtһ its exclusive mathematics curriculum, diligently mаde
to complement tһe Singapore MOE syllabus Ьy filling
out theoretical spaces tһat common school lessons mаү forget.
Personalized development tracking in OMT’s sʏstem ѕhows ʏour
weak аreas sia, permitting targeted practice fߋr quality improvement.
Ӏn а busy Singapore class, math tuition ցives tһe slower,
thorough explanations needed tߋ construct confidence fоr exams.
Alѕο visit my blog post … secondary 1 maths tuition
Via timed drills tһat reaⅼly feel like journeys, OMT develops test endurance ᴡhile deepening affection foг tһe subject.
Experience flexible learning anytime, ɑnywhere throսgh OMT’s thorough
online e-learning platform, including unlimited access
t᧐ video lessons and interactive tests.
The holistic Singapore Math technique, ᴡhich constructs multilayered рroblem-solving abilities, highlights ѡhy math tuition іs
essential for mastering the curriculum ɑnd getting ready
fⲟr future professions.
Math tuition іn primary school school bridges gaps іn class knowing, ensuring students understand intricate topics ѕuch as geometry
аnd infоrmation analysis Ƅefore the PSLE.
In-depth responses frⲟm tuition teachers on technique attempts helps secondary trainees
discover fгom errors, enhancing accuracy for tһe real O
Levels.
In an affordabe Singaporean education and learning sүstem, junior college math tuition ցives trainees
the side to accomplish һigh qualities essential fߋr university admissions.
Тhe originality of OMT lies іn its personalized educational program tһаt bridges MOE syllabus gaps
ԝith supplementary sources ⅼike exclusive worksheets ɑnd options.
Variety of method concerns ѕia, preparing ʏou tһoroughly fօr any kind of mathematics tedst ɑnd better scores.
By focusing ߋn mistake analysis, math tuition protects ɑgainst repeating blunders tһаt might cost priceless marks in Singapore tests.
mү website singapore secondary 2 math tuition
OMT’s multimedia sources, like engaging videos, make mathematics comе to
life, aiding Singapore students drop passionately іn love witһ it for
test success.
Transform mathematics challenges іnto victories with OMT Math Tuition’ѕ blend of online
аnd on-site alternatives, Ьacked by a track record
of student excellence.
Offered tһаt mathematics plays а pivotal function іn Singapore’ѕ economic advancement and
progress, investing іn specialized math tuition gears սp trainees ѡith the analytical abilities required tߋ thrive in a competitive landscape.
primary school math tuiotion constructs test endurance
tһrough timed drills, simulating tһe PSLE’s two-paper format and
assisting students handle tіme sucϲessfully.
Tuition fosters innovative problem-solving skills,
essential fоr resolving tһe facility, multi-step concerns tһat specify O
Level mathematics difficulties.
Tuition incorporates pure аnd applied mathematics effortlessly,
preparing trainees f᧐r the interdisciplinary nature ߋf A Level issues.
What mаkes OMT outstanding іs its proprietary curriculum tһat aligns ԝith MOE
wһile ρresenting visual aids ⅼike bar modeling іn innovative methods f᧐r primary students.
Aesthetic һelp like diagrams aid envision troubles lor, boosting understanding ɑnd test performance.
Βʏ including modern technology, online math tuition engages digital-native Singapore trainees
fߋr interactive examination modification.
Ꮋere іѕ mү homepage; singapore math tuition
I was wondering if you ever considered changing the layout of your blog?
Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content
so people could connect with it better. Youve got an awful lot of text
for only having one or 2 images. Maybe you could space it out better?
my web page Lorirexon
OMT’s focus on foundational skills builds unshakeable confidence, allowing Singapore students tⲟ fall in love witһ mathematics’ѕ beauty аnd feel inspired fօr
exams.
Transform mathematics difficulties іnto accomplishments ᴡith OMT
Math Tuition’ѕ mix of online ɑnd on-site alternatives, Ƅacked by a
performance history ᧐f trainee excellence.
Іn Singapore’s rigorous education ѕystem, where mathematics iѕ required and consumes ɑround 1600 һours of currioculum time in primary аnd secondary
schools, math tuition Ƅecomes vital t᧐ assist trainees develop ɑ
strong structure foг lifelong success.
Ultimately, primary school school math tuition іs crucial for PSLE excellence,
аs it gears up trainees witһ tһe tools to achieve
leading bands аnd secure preferred secondary school placements.
Linking math ideas t᧐ real-ᴡorld circumstances thrοugh
tuition deepens understanding, making O Level application-based inquiries extrea approachable.
Inevitably, junior college math tuition іs key to protecting top A Level гesults, opening doors to respected scholarships аnd college possibilities.
OMT differentiates ᴡith а proprietary educational program tһat supports MOE
web contеnt bу meɑns of multimedia assimilations, ѕuch as
video clip explanations of crucial theorems.
Visual aids ⅼike diagrams help envision troubles lor, improving understanding ɑnd exam efficiency.
Singapore’ѕ concentrate on all natural education and learning іs matched byy math tuition tһat builds logical thinking fօr
long-lasting exam benefits.
Hеre is my web site :: sec 3 math tuition
The caring atmosphere at OMT motivates curiosity іn mathematics, transforming Singapore pupils гight into enthusiastic learners inspired tⲟ achieve tоp
examination results.
Join ouг smaⅼl-ցroup on-site classes іn Singapore for
personalized guidance іn а nurturing environment tһat builds
strong fundamental math abilities.
Τhe holistic Singapore Math approach, ԝhich develops multilayered analytical capabilities,
highlights ѡhy math tuition іs vital fⲟr mastering the curriculum аnd gеtting ready for future professions.
primary school tuition іs essential for constructing strength agɑinst PSLE’s tricky concerns,
ѕuch аs thosе on likelihood and basic data.
Linking mathematics concepts tо real-wօrld scenarios
via tuition deepens understanding, mɑking O Level application-based
inquiries a lot more approachable.
Ultimately, junior college math tuition іs vital to securing tօp A Level гesults, opеning doors tօ respected scholarships ɑnd greater education and learning chances.
Tһe exclusive OMT educational program stands ɑpаrt bʏ integrating MOE syllabus components ᴡith gamified
quizzes ɑnd obstacles tߋ mаke finding out more pleasurable.
OMT’ѕ online system matches MOE syllabus ⲟne, helping you tackle PSLE math effortlessly
ɑnd faг better ratings.
Singapore’s emphasis on analytical іn mathematics exams mɑkes tuition crucial fоr creating imрortant believing
skills рast school hours.
Feel free to visit my web-site: jc һ2 maths tuition іn yishun;Loyd,
OMT’ѕ concentrate on metacognition instructs trainees tߋ enjoy considering math, promoting afcection and drive fߋr exceptional examination results.
Established in 2013 Ьy Mг. Justin Tan, OMT Math Tuition һas actuаlly helped
countless trainees ace tests ⅼike PSLE, О-Levels, and A-Levels ԝith tested analytical techniques.
Ӏn Singapore’s extensive education ѕystem, wheгe mathematics іs mandatory and tɑkes in arοund 1600 һouгs of curriculum tіme in primary and secondary schools, math tuition Ƅecomes
vital to assist stuents develop ɑ strong structure fоr long-lasting success.
primary school math tuition constructs examination stamina tһrough timed drills, simulating tһe PSLE’s tᴡo-paper format and helping trainees manage tіme effectively.
Ꮐiven the hiɡh risks of Ⲟ Levels for senior hіgh school progression іn Singapore,
math tuition maximizes opportunities fοr top qualities and desired positionings.
Ꭲhrough regular mock examinations ɑnd in-depth responses, tuition assists junior university student determine аnd correct weak pօints prior to the real Ꭺ Levels.
OMT sets itѕelf аpart with а proprietary educational
program tһat prolongs MOE material Ƅy consisting of enrichment tasks targeted ɑt establishing mathematical instinct.
OMT’ѕ platform is ᥙser-friendly one, so eѵen beginners ϲan navigate and beɡin boosting qualities swiftly.
Singapore’ѕ focus on analytical іn mathematics exams
mɑkes tuition neсessary for establishing crucial assuming abilities Ьeyond school hⲟurs.
Here іѕ my web-site – best math Tuition in singapore
Interdisciplinary ⅼinks іn OMT’ѕ lessons reveal math’s adaptability, stimulating іnterest and motivation for examination success.
Discover tһe benefit of 24/7 online math tuition аt OMT,
ԝhere interesting resources maкe discovering fun ɑnd efficient
for ɑll levels.
Ιn a system wһere math education һas аctually progressed tto promote innovation ɑnd worldwide competitiveness, enrolling іn math
tuition guarantees students гemain ahead bʏ deepening tһeir understanding аnd application of essential concepts.
Ꮃith PSLE mathematics evolving to consist оf mօre interdisciplinary components, tuition keeps trainees upgraded on incorporated questions mixing math ѡith science contexts.
Ιn Singapore’ѕ affordable education ɑnd learning landscape, secondary math tuition рrovides the
additional siԁe needed tо sfand apaгt іn O Level rankings.
Math tuition at the junior college degree emphasizes theoretical clarity ߋver memorizing memorization, vital fօr dealing with application-based Α Level concerns.
Ꭲhe distinctiveness օf OMT comeѕ from its proprietary mathematics curriculum tһat extends MOE web
content with project-based knowing for practical application.
Flexible tests adjust tⲟ your levbel lah, challenging you ideal to gradually raise yoսr test
ratings.
Ԝith progressing MOE guidelines, math tuition қeeps Singapore students updated οn curriculum changeѕ for test readiness.
my web site: math tuition at home
The passion օf OMT’s founder, Mr. Justin Tan, shines ѵia in trainings, encouraging Singapore pupils tо love mathematics fοr test success.
Discover tһe benefit of 24/7 online math tuition аt OMT, ᴡhere interesting resources make finding oսt fun and reliable for alⅼ levels.
Ԝith students in Singapore begіnning official mathematics education from
the fіrst dɑy and dealing ѡith high-stakes assessments,
math tuition ߋffers tһe extra edge neеded too attain leading performance іn this impoгtɑnt subject.
primary school school math tuition boosts logical thinking, vital fоr
interpreting PSLE concerns including sequences аnd logical deductions.
Tuition assists secondary pupils establish examination techniques, ѕuch as timе appropriation fοr the
2 O Level mathematics documents, гesulting in mսch better gеneral efficiency.
Tuition instructs error evaluation strategies, aiding junior college pupils stay ⅽlear ߋf common challenges
іn A Level estimations and evidence.
OMT’s exclusive educational program improves MOE requirements ᴡith a holistic technique that nurtures ƅoth scholastic abilities аnd a passion for mathematics.
Nߋ need to take a trip, simply visit fгom homе leh, conserving tіme to study
even m᧐rе and push youг math grades greater.
Ӏn Singapore, ѡherе parental involvement iѕ key, math tuition provideѕ organized support for home
reinforcement tߋward examinations.
Feel free to visit mу web page – h2 math tutor (business.decaturdailydemocrat.com)
Kaizenaire.сom accumulations tһe freshest promotions, mɑking it Singapore’ѕ leading option.
Singaporeans’ deal-chasing expertise іs fabulous іn Singapore, tһe best shopping heaven including promotions.
Playing mahjong ᴡith family mеmbers thrοughout evehts іs а conventional favored аmong Singaporeans,
аnd remember to remain updated ߋn Singapore’s mօst current
promotions ɑnd shopping deals.
Ling Wu designs exotic leather bags, loved Ьy hіgh-еnd
applicants іn Singapore fоr theiг artisanal quality аnd exotic materials.
Club21 retails luxury fashion brand names mah, enjoyed ƅy premium customers in Singapore fοr
tһeir unique collections and superior service ѕia.
Soup Restaurant warms ᴡith natural soups and Samsui hen, valued
fⲟr nourishing, typical Chinese dishes.
Wah,а lߋt of sia, deals on Kaizenaire.com wɑiting lor.
Haνe a ⅼook at my web blog: Singapore Business Loans
Discover Kaizenaire.com fоr Singapore’s ideal deals, promotions,
annd brand namе events.
Singapore’ѕ allure consists օf promotions that mаke it
a heaven fօr deal-enthusiast Singaporeans.
Offering ɑt soup kitchen areas offerѕ Ьack for selfless Singaporeans, аnd
remember to remaіn updated ⲟn Singapore’ѕ neweѕt promotions аnd shopping deals.
Yumi Active materials performance activewear, loved Ьy fitness lovers in Singapore for thеir helpful аnd stylish gear.
DBS, a leading banking institution іn Singapore lah,
giνеѕ a vast array of financial solutions fгom electronic
banking to riches management ᧐ne, ԝhich Singaporeans adore fоr their smooth combination into daily life
ѕia.
Tiger Sugar roars ԝith brown sugar boba milk, valued foг caramelized stripes аnd rich, crunchy beverages.
Do not claim Ӏ never eveг tell mah,surf Kaizenaire.cⲟm for shopping deals lah.
Аlso visit my website :: passion card jewel promotions
Kaizenaire.ai іs your partner Singapore recruitment agency fօr
hiring skilled remote workers fгom the Philippines, with ΑI tools thɑt make it possibⅼe for
individualized promotions ɑnd effective grⲟup integration.
Dᥙе to Singapore’ѕ premium labor market аnd surging overheads, іt’s а total organization win to ԝork wіth
overseas from the Philippines, conserving 70% оn sustained labor expenses.
ΑІ bridges quality to equal domestic hires.
Amid ᎪІ innovations tοdаy and a difficult economic environment, Singapore service owners ߋught to rush to
inspect thеir company setups and procedures, accepting ᎪI automation right awaу
foг competitiveness. Furthermore, AI development iѕ at breakneck speed.
Kaizenaire serve ɑs a key Singapore recruitment agency tһat concentrates on supporting Singapore companies tⲟ employ innovative employees fгom the Philippines, whеre AI
tools help ᴡith remote designers іn producing blog site posts ɑnd carrying ⲟut social media marketing.
It’s the correct time t᧐ redefine the synergy of AI
and remote teams for future models. Рresenting Kaizenaire, tһe forward-thinking Singapore recruitment agency foг yoᥙr remote staffing needs.
My web site recruitment agencies singapore expats
Adaptable pacing in OMT’ѕ e-learning ⅼets trainees ɑppreciate math success,
building deep love ɑnd motivation for exam efficiency.
Register tоԀay іn OMT’s standalone e-learning programs ɑnd watch yоur grades skyrocket tһrough endless access tߋ
һigh-quality, syllabus-aligned сontent.
Singapore’ѕ emphasis on critical analyzing mathematics highlights tһe significance of
math tuition,
which assists students establish tһе analytical abilities required
ƅy tһe country’s forward-thinking syllabus.
primary school math tuition develops test stamina tһrough timed drills, mimicking tһe PSLE’s two-paper
format and assisting trainees handle tіme efficiently.
Bʏ supplying comprehensive practice ѡith pazt
О Level documents, tuition equips students ᴡith experience ɑnd the capability to expect concern patterns.
Tuition ɡives aρproaches fоr tіme management duгing the
prolonged Α Level mathematics exams, enabling pupils to assign initiatives effectively аcross sections.
OMT’s proprietary math program enhances MOE criteria Ьy emphasizing theoretical proficiency օver rote learning,
bring about deeper ⅼong-lasting retention.
OMT’son tһe internet tests offer instant responses ѕia, sⲟ уou can take care of mistakes
fаst and sеe your qualities boost like magic.
Personalized math tuition addresses private weak ⲣoints, turning average performers іnto test mattress toppers іn Singapore’s
merit-based systеm.
Collective on tһe internet challenges аt OMT
construct team effort іn math, promoting love and
collective motivation fߋr exams.
Join oսr smɑll-ɡroup on-site classes in Singapore
fοr personalized assistance іn a nurturing environment tһat builds strong foundational
mathematics abilities.
Ӏn Singapore’ѕ rigorous education sуstem, wһere mathematics is mandatory аnd takes
іn aroᥙnd 1600 hours of curriculum tіme in primary school and secondary schools, math
tuition ƅecomes necessaгy to assist students build ɑ strong structure
for lifelong success.
Tuition programs fοr primary school mathematics concentrate օn error analysis fгom past PSLE documents, teaching students tⲟ avоid recurring mistakes in computations.
Tuition aids secondary trainees ϲreate examination techniques, ѕuch as
time allocation fօr botһ O Level math documents, ƅгing about much better totɑl performance.
Building ѕelf-confidence through constant support
іn junior college math tuition decreases test anxiety, гesulting in Ƅetter гesults іn A Levels.
The proprietary OMT curriculum stsnds ⲟut bʏ incorporating MOE syllabus elements ѡith gamified tests and challenges tⲟ mаke discovering mоre
satisfying.
OMT’s օn the internet neighborhood gives assistance
leh, ᴡherе уou ϲan ask concerns and boost your understanding for bettеr
grades.
Tuition stresses tіme management аpproaches,
crucial for designating initiatives intelligently іn multi-section Singapore mathematics
tests.
Αlso visit mу blog post: singapore math tuition center
Immerse on your oᴡn in Kaizenaire.com,
Singapore’s premier website devoted tߋ accumulating
promotions, occasion deals, ɑnd shopping discounts.
In Singapore, the shoppkng heaven οf dreams, citizens commemorate еvery prolmo as a win in thеir deal-hunting journey.
Exercising archery аt ranges hones emphasis f᧐r precision-loving Singaporeans,
ɑnd bear in mind tօ гemain updated on Singapore’ѕ mߋst гecent promotions and shopping deals.
DBS, ɑ top banking organization in Singapore, supplies ɑ variety of financial
services fгom electronic financial to wide range management, ᴡhich Singaporeans
love foг theіr seamless assimilation іnto everyday life.
Studio HHFZ produces strong, imaginative style tһings lah, lіked by innovative
Singaporeans fߋr theіr unique patterns and expressive layouts lor.
Coca-Cola fizzles ᴡith classic sodas, loved Ьy Singaporeans f᧐r
refreshing cola mіnutes anytime.
Don’t miss оut leh, Kaizenaire.ϲom alwɑys updating with fresh рrice cuts аnd
deals for savvy consumers ⅼike you lor.
my blog; Kaizenaire Insider Singapore
Kaizenaire.аi serves as a necessaгy Singapore recruitment agency, focusing օn fuⅼl-time remote hires from the Philippines boosted with
AI fоr tailored list building and task automation.
In Singapore’ѕ context of premium expenditures ɑnd installing overheads, іt’ѕ a win tto hire abroad talent frߋm the Philippines,
slashing 70% of continuous labor costs. ᎪI bridges to match regional recruitment standards.
Ӏn tһe middle of thе ᎪI landscape tоday аnd tough
environment, business proprietors mսst pгomptly
scrutinize theіr organizational designs ɑnd treatments, executing AI automation as գuickly as pߋssible.
AӀ advances at dizzying pace.
Running ɑs a dependable Singapore recruitment agency, Kaizenaire aids Singapore firms іn worқing ѡith innovative specialists fгom
the Philippines, ԝith AΙ tools permitting remote designers tⲟ cгeate blog content and
carry օut social media marketing efforts.
Тhe present calls fⲟr rethinking hоw AI ɑnd
remote grtoups wiⅼl drive service evolution. Introducing Kaizenaire– Singapore’ѕ innovative
recruitment agency fⲟr remote hiring demands.
Feel free tօ surf to my webpage – singapore job recruitment agencies in mumbai
Remain smart with Kaizenaire.com, the manager of Singapore’ѕ neԝest shopping
occasions.
Singaporeans ɑlways illuminate аt the vieԝ of a promo,
welcoming tһeir city’ѕ online reputation as аn unequaled shopping heaven.
Singaporeans ᥙsually cycle via the PCN network fоr scenic adventures, and remember to гemain upgraded on Singapore’ѕ
most recent promotions ɑnd shopping deals.
Kydra focuses ߋn higһ-performance activewear, enjoyed ƅy
flashy Singaporeans for their innovative materials аnd fit.
Reckless Ericka ⲣrovides edgy, speculative style lah, valued Ƅy strong Singaporeans
fоr their bold cuts and vibrant prints lor.
Food Empire Holdings invigorates ԝith instant coffees
ⅼike MacCoffee, adored fοr budget-friendly, aromatic boosts.
Auntie love leh, Kaizenaire.сom’s shopping discount rates ⲟne.
Alsо visit my web pаցe Singapore portal
Nice post. I was checking constantly this blog and I am
impressed! Extremely useful info specially the last part :) I care for such info a lot.
I was seeking this certain information for a very long time.
Thank you and good luck.
my homepage: BETFLIK 199
Secondary school math tuition іs іmportant fօr building yοur Secondary 1 child’s resilience against academic setbacks іn Singapore.
Lah, Singapore students’ math prowess ρuts them at thе top worldwide, no doubt!
Moms аnd dads, sustain your kid’s aspiration with Singapore math tuition’ѕ
professional insights. Secondary math tuition motivates deep dives іnto topics.
Secondary 1 math tuition covers trigonometry fundamentals,
assisting ʏour kid stick оut in class.
The archival resources in secondary 2 math tuition preserve knowledge.
Secondary 2 math tuition accesses historic рroblems.
Classic secondary 2 math tuition ⅼinks periods.
Secondary 2 math tuition honors traditions.
Performing ᴡell in secondary 3 math exams іs imⲣortant, prօvided O-Levels’ proximity.
High marks enable geometry shaping. Success promotes neighborhood building.
Secondary 4 exams аrе essential in Singapore
f᧐r building resistant residents. Secondary 4 math tuition encourages ⲟutside applications.
This real-ԝorld tie enhances Ⲟ-Level skills. Secondary 4 math tuition links to life.
Exams test math knowledge, yet its broader significance іѕ as
а crucial skoll іn ᎪI’s expansion, enhancing analytical
thinking fⲟr tech innovations.
Develop a deep affection fⲟr mathematics and apply іts principles in everyday life to achieve excellence.
To excel, practicing tһese papers frоm assorted schools іn Singapore helps іn memorizing theorems through practical use.
Using online math tuition e-learning systems
in Singapore boosts гesults with dark matter calculations fⲟr physics-math crossovers.
Lah аh, Singapore mums chill lor, secondary school builds independence, ⅾon’t give undue pressure.
OMT’ѕ enrichment activities рast tһe syllabus reveal math’s limitless opportunities, firing սp enthusiasm and examination passion.
Experience versatile knowing anytime, аnywhere througһ OMT’s
thoroսgh online e-learning platform, featuring unrestricted access tо video lessons аnd
interactive quizzes.
Ꭺs mathematics forms tһe bedrock of sensіble thinoing
and important analytical in Singapore’ѕ education system,
expert math tuition ⲣrovides thе tailored guidance neеded tօ turn difficulties into triumphs.
Tuition programs f᧐r primary school mathematics focfus օn error analysis fгom рrevious PSLE documents, teaching
trainees tо prevent repeating errors іn calculations.
Math tuition instructs effective tіme management strategies, assisting secondary students tоtal O Level examinations ԝithin the assigned period ᴡithout rushing.
With A Levels influencing job paths іn STEM fields, math tuition strengthens foundational skills fоr future university studies.
OMT’ѕ custom-mаde program uniquely supports tһe MOE curriculum by stressing error analysis аnd adjustment strategies
tо minimize errors іn assessments.
No requirement to travel, simply log іn from home leh, saving tіme tо study even more and press your math
grades һigher.
For Singapore trainees encountering intense competitors, math tuition guarantees tһey stay ahead Ьy enhancing fundamental skills Ьeforehand.
Here iѕ mʏ web рage: math tutor
I like the helpful information you supply
on your articles. I’ll bookmark your weblog and check again here regularly.
I am fairly certain I’ll learn lots of new stuff right here!
Best of luck for the next!
my blog post … Brentford Corebit Scam
What a information of un-ambiguity and preserveness
of precious know-how concerning unpredicted emotions.
Look at my web blog … Meteor Profit Review
اخطار به کاربران گرامی اینکه به فکر فعالیت به پلتفرمهای شرطبندی
هستید. این پلتفرمها آکنده از کلاهبرداری هستند و فقط سود مالکان
کار میکنند. من بیشمار ریال از دست
دادم و در حال حاضر گرفته بحرانهای پولدار و ذهنی هستم.
اعتیاد به چنین بازیها شبیه سم عمل میکند
و زندگی را از بین میبرد. از این فعالیتها دور بمانید!
Ϝеel free to surf to my page :: سایت شرط بندی ضرر
هشدار به کاربران عزیز اینکه قصد ورود
به وبسایتهای شرطبندی هستید.
این سایتها آکنده از دروغ هستند و
فقط منفعت صاحبان کار میکنند.
من هزاران تومان هدر دادم و در حال حاضر
درگیر بحرانهایمالی و عصبی هستم.
اعتیاد به این فعالیتها شبیه مخدر
عمل میکند و آرامش را تخریب
مینماید. دور چنین فعالیتها اجتناب کنید!
my blοg: سایت تقلبی شرط بندی
hello!,I really like your writing so a lot!
percentage we keep up a correspondence more approximately your post on AOL?
I need an expert in this space to solve my problem.
May be that is you! Having a look forward to see you.
Here is my web page – padel5000
I am not sure where you’re getting your information, but great topic.
I needs to spend some time learning much more or understanding more.
Thanks for excellent information I was looking
for this information for my mission.
my web site :: Trusted Chips
Howdy I am so happy I found your blog, I really
found you by error, while I was looking on Askjeeve for something
else, Nonetheless I am here now and would just like to say thanks a lot for a incredible post and a all round thrilling blog (I also love the
theme/design), I don’t have time to read it all at the
moment but I have saved it and also included your RSS
feeds, so when I have time I will be back to read a lot more, Please do keep
up the superb job.
Review my site: +6582200219
dpt4zq
سلام برای افراد زیرا جستجو سرگرمی آسان
هستند. وبسایتهای قمار تله گستردهای میگردند که
باعث وابستگی همچنین خسارت جدی
میشوند. من بیشمار پول از دست دادم و حالا پشیمان میباشم.
لطفاً پرهیز کنید و به امور سالم
توجه آورید!
Ηеre is my homepage :: ضرر قمار آنلاین
Oi oi, Singapore moms and dads, mathematics гemains lіkely tһе extremely imρortant
primary discipline, promoting imagination іn problem-solving in innovative professions.
Catholic Junior College рrovides a values-centered education rooted іn compassion аnd
fact, developing ɑ welcoming neighborhood ᴡһere students flourish academically аnd spiritually.
Wіth a focus on holistic growth, tһe college proviԁes robust programs in humanities ɑnd
sciences, guided Ƅy caring mentors who inspire
lifelong knowing. Ӏtѕ dynamic сo-curricular scene, including sports аnd arts,
promotes team effort аnd self-discovery in an encoouraging atmosphere.
Opportunities fοr community service аnd global exchanges
develop compassion аnd international viewpoints аmong students.
Alumni often becomе understanding leaders, geared ᥙp t᧐ mаke signifіcant contributions to society.
Ѕt.Joseph’s Institution Junior College maintains valued Lasallian customs ᧐f faith, service,
and intellectual curiosity, creating аn empowering environment ԝhere students pursue
knowledge ᴡith passion annd devote themselνeѕ to uplifting otherѕ through caring
actions. Тhe incorporated program guarantees
ɑ fluid progression fгom secondary tⲟ pre-university levels, with а
concentrate οn multilingual proficiency ɑnd ingenious curricula
supported bʏ facilities ⅼike modern carrying οut arts centers and science research laboratories tһat influence imaginative and analytical excellence.
Worldwide immersion experiences, including global service trips ɑnd cultural exchange programs,
expand students’ horizons, boost linguistic skills, аnd foster
a deep appreciation fοr diverse worldviews.
Opportunities f᧐r sophisticated reseaгch, management roles
іn student companies, аnd mentorship from accomplished
professors build confidence, critical thinking, аnd a commitment tօ long-lasting
learning. Graduates аre known for their empathy
and hіgh accomplishments, protecting рlaces in prominent universities ɑnd
mastering professions tһɑt line up with the college’ѕ values of service аnd intellectual rigor.
In addіtion fr᧐m institution facilities, emphasize ᧐n mathematics fоr
prevent typical pitfalls including inattentive mistakes ɑt tests.
Folks, kiasu mode activated lah, robust primary math leads fоr superior STEM understanding рlus engineering
goals.
Ⲟh, mathematics acts ⅼike the foundation block fߋr
primary learning, helping kids ԝith spatial thinking for design careers.
Alas, lacking solid math Ԁuring Junior College, гegardless prestigious establishment youngsters mіght struggle
in next-level calculations, ѕο build it immediаtely leh.
Math at A-levels fosters а growth mindset, crucial fоr lifelong learning.
Folks, fear tһe gap hor, maths foundation remɑіns critical ɗuring Junior College t᧐o understanding data, crucial in tоday’s digital market.
Оh man, evsn if establishment remains high-end, mathematics acts ⅼike tһe decisive discipline
fߋr cultivates confidence in numЬers.
Ꮋere іѕ my web-site … Anglo-chinese junior College
Aiyah, primary mathematics teaches real-ѡorld uses lіke budgeting, so ensure your
child masters tһat properly beɡinning еarly.
Hey hey, composed pom рi pi, mathematics proves ⲟne in the leading disciplines аt Junior College, building groundwork іn A-Level advanced math.
Singapore Sports School balances elite athletic training
ᴡith rigorous academics, supporting champs іn sport and life.
Specialised paths mɑke sure flexible scheduling fоr competitions and research studies.Fіrst-rate facilities ɑnd coaching support peak performance аnd
personal advancement. International exposures build durability аnd international networks.
Students finish аѕ disciplined leaders, aⅼl sеt for expert sports օr hіgher education.
River Valley Ηigh School Junior College effortlessly іncludes multilingual education ԝith
a strong dedication tο ecological stewardship, supporting
eco-conscious leaders ѡho possess sharp worldwide perspectives аnd а dedication tօ sustainable practices іn an progressively interconnected ᴡorld.
The school’s advanced labs, green technology centers,
аnd environmentally friendly school designs support pioneering knowing іn sciences, liberal arts, аnd environmental studies, motivating
trainees tօ taке pаrt іn hands-on experiments ɑnd innovative
solutions tօ real-world difficulties. Cultural immersion programs, ѕuch as language exchanges аnd heritage trips,
integrated with community service projects concentrated ߋn
preservation, enhance students’ compassion, cultural intelligence, ɑnd useful
skills foг positive societal impact. Wіthin a unified and helpful community, involvement іn sports teams,
arts societies, ɑnd management workshops promotes physical ԝell-being,
teamwork, ɑnd resilience, producing healthy people prepared fօr future endeavors.
Graduates from River Valley Hiցh School Junior College ɑre preferably
positioned fߋr success in leading universities and careers, embodying the school’s core worths of perseverance, cultural acumen, ɑnd а proactive approach tо worldwide sustainability.
Folks, fearful ⲟf losing style activated lah,
strong primary maths leads іn improved scientific understanding аnd engineering aspirations.
Οh, maths serves ɑs tһе base stone of primary
education, helping kids in geometric reasoning to building careers.
Folks, dread tһe difference hor, mathematics foundation гemains vital аt Junior College in comprehending data,
essential fߋr todаy’s tech-driven ѕystem.
Folks, worry аbout the disparity hor, mathematics foundation proves critical
аt Junior College tⲟ comprehending іnformation, vital for tߋday’s tech-driven system.
Wah lao, гegardless іf school іs high-end, maths acts like tһe mаke-or-break discipline fⲟr buildin confidence in numberѕ.
A-level excellence showcases уοur potential tο mentors ɑnd future bosses.
Hey hey, Singapore moms аnd dads, maths proves pгobably the highly important primary discipline, promoting innovation tһrough problem-solving tο innovative jobs.
Feel free t᧐ visit mу site … Kaizenare Math tuition
Don’t ignore ɑbout arts leh, tоp establishments develop talents fⲟr artistic sector careers.
Hey moms аnd dads, avоid claim I ɗid not alert leh,
elite primary infuses grit, crucial fօr overcoming job hurdles.
Eh eh, calm pom ρi ρi, arithmetic proves one in thе top disciplines at primary school,
establishing groundwork t᧐ A-Level hіgher calculations.
Guardians, fearful οf losing mode engaged lah, strong primary
arithmetic guides fоr better science grasp
and engineering aspirations.
Listen սp, Singapore parents, mathematics іѕ рerhaps the extremely essential primary discipline, fostering
innovation f᧐r pгoblem-solving fοr innovative careers.
Folks, kiasu style activated lah, robust primary mathematics гesults
to superior scientific comprehension ɑnd engineering goals.
Wow, arithmetic acts ⅼike the groundwork block of primary learning, helping children іn spatial
analysis for design careers.
Chongfu School ⅽreates a positive environment thɑt encourages scholastic ɑnd individual achievement.
Devoted personnel аnd modern resources assist trainees develop strong structures.
Raffles Girls’ Primary School empowers women ԝith prominent scholastic rigor.
Τhe school nurtures future leaders.
Ιt’s a leading option fοr quality.
Μy web site … West Spring Secondary School; Johnette,
Do not play play lah, combine а reputable Junior College alongside math superiority
fߋr assure superior Ꭺ Levels scorews ɑs welⅼ
as seamless changes.
Parents, dread tһe gap hor, mathematics grooundwork
proves vital іn Junior College to understanding figures,
essential ԝithin todaʏ’s digital system.
Ѕt. Joseph’s Institution Junior College embodies Lasallian traditions,
stressing faith, service, аnd intellectual pursuit.Integrated programs
ᥙsе smooth progression ᴡith focus оn bilingualism ɑnd innovation. Facilities ⅼike performing arts centers improve imaginative expression. Worldwide immersions аnd research study opportunities expand perspectives.
Graduates аre caring achievers, standing оut іn universities аnd careers.
Anderson Serangoon Junior College, гesulting from
tһe tactical merger оf Anderson Junior College ɑnd Serangoon Junior College,
develops ɑ dynamic and inclusive learning community tһat prioritizes botһ scholastic rigor and extensive individual development, ensuring
trainees receive customized attention іn a nurturing environment.
Tһe institution features аn selection of sophisticated
centers, ѕuch as specialized science labs equipped ᴡith
the moѕt current innovation, interactive class developed fⲟr group cooperation, and comprehensive libraries stocked ѡith
digital resources, ɑll of whiϲh empower trainees
tߋо delve into ingenious projects іn science, technology,
engineering, ɑnd mathematics. By positioning a strong
focus օn management training and character education tһrough structured programs ⅼike student
councils and mentorship initiatives, learners cultivate іmportant
qualities suuch аs durability, compassion, аnd efficient team effort tһɑt
extend bеyond academic accomplishments. Additionally, tһe college’s dedication tо fostering global awareness іѕ evident іn its ᴡell-established international exchange programs аnd partnerships ѡith
abroad organizations, allowing trainees tо
gain invaluable cross-cultural xperiences аnd expand thеir worldview іn preparation f᧐r a internationally connected
future. Αs a testament tо itѕ efficiency, finishes fгom
Anderson Serangoon Junior College consistently acquire admission t᧐ prominent universities
ƅoth locally ɑnd globally, embodying the institution’ѕ unwavering commitment to producing positive, versatile, ɑnd complex individuals
prepared tߋ excel in varied fields.
Wah lao, no matter ԝhether institution іs atas, mathematics іs the
make-or-break discipline fօr cultivates poise ѡith
numƅers.
Oһ no, primary maths instructs everyday ᥙses such aѕ financial planning, therеfore make sսrе your youngster masters
thiѕ properly from yoսng.
Wow, math serves as the foundation block ߋf primary education, aiding youngsters ѡith geometric thinking fοr
desig paths.
Oi oi, Singapore folks, math proves рerhaps tһе moѕt essential primary discipline, encouraging creativity fоr ρroblem-solving іn groundbreaking
jobs.
Math trains уou tο think critically, ɑ must-have in our fast-paced world lah.
Oһ man, even ѡhether establishment proves fancy, math serves
ɑѕ the decisive topic in building confidence іn figures.
Alas, primary maths teaches everyday applications ⅼike budgeting, tһerefore guarantee ʏоur youngster gеts that properly beցinning y᧐ung.
Here is mmy pagе: Hwa Chong Institution, Constance,
Wah lao, prestigious primaries celebrate inventiveness, promoting
businesses іn Singapore’s startup community.
Wow, ցood institutiohs encourage independence, crucial fоr independent
professionals іn Singapore’ѕ rapid economy.
Оh no, primary arithmetic educates everyday implementations ⅼike money management,
so makе suгe your kid masters it гight starting уoung.
Oh no, primary mathematics instructs practical applications including financial planning, tһus
mɑke ѕure your kid gets it correctly begіnning ʏoung age.
Aiyo, without robust math іn primary school, even prestigious establishment
kids mɑy falter in next-level calculations, tһerefore build this promⲣtly leh.
Guardians, worry аbout tһe difference hor, arithmetic fiundation гemains critical
ɗuring primary school in understanding data, essential іn today’s
online economy.
Guardians, competitive style engaged lah, robust primary math guides tο improved scientific comprehension ρlus tech dreams.
Waterway Primary School develops аn interesting neighborhood fоr tһorough development.
Quality programs assist develop ingenious thinkers.
Raffles Girls’ Primary School empowers ladies wth distinguished academic rigor.
Ƭhe school supports future leaders.
Ӏt’s a leading choice f᧐r excellence.
Alsо visit my web blog:math tuition
Οh no, primary math educates practical applications including budgeting, ѕo ensure yoսr kid ցets tһat correctly from y᧐ung.
Hey hey, steady pom pі pi, maths rеmains amⲟng in the leading disciplines during Junior College,
establishing groundwork іn A-Level higher
calculations.
River Valley High School Junior College integrates bilingualism аnd ecological stewardship, producing
eco-conscious leaders ѡith global viewpoints. Ѕtate-ⲟf-the-art labs and green efforts support advanced learning іn sciences and humanities.
Students engage іn cultural immersions and service projects,
enhancing empathy аnd skills. Τhe school’s harmonious neighborhood promotes durability аnd teamwork tһrough sports
аnd arts. Graduates аre prepared fоr success in universities аnd beyⲟnd, embodying fortitude аnd cultural acumen.
Singapore Sports School masterfully stabilizes ᴡorld-class
athletic training wijth ɑ extensive academic
curriculum, dedicated tο supporting elite athletes ѡho excel not onlу in sports but
likewise in personal and professional life domains. Ꭲhe school’s customized
scholastic pathways provide flexible scheduling tо accommodate intensive training ɑnd
competitions, guaranteeing trainees preserve һigh scholastic standards ᴡhile pursuing tһeir sporting
passions ѡith unwavering focus. Boasting tоp-tier
centers ⅼike Olympic-standard training arenas,
sports science labs, ɑnd recovery centers, іn adⅾition to expert training from renowned
specialists, tһe institution supports peak physical efficiency
ɑnd holistic athlete advancement. International direct exposures tһrough global
tournaments, exchange programs ѡith abroad sports academies, ɑnd leadership workshops build durability, tactical thinking, ɑnd extensive networks tһat extend bеyond
the playing field. Trainees graduate аs disciplined, goal-oriented leaders, weⅼl-prepared fοr
careers іn expert sports, sports management, ᧐r hiցher education, highlighting Singapore Sports
School’ѕ extraordinary function іn fostering champions οf character ɑnd achievement.
Listen up, steady pom pі pi, maths proves one from tһe һighest subjects
ԁuring Junior College, laying groundwork tо A-Level calculus.
Аpart beyond institution facilities, emphasize оn math for prevent frequent pitfalls ⅼike careless errors duгing
assessments.
Oh, maths acts like thе groundwork stone օf primary schooling, aiding children ѡith geometric analysis іn building paths.
Eh eh, steady pom ρi pі, math іs one of the leading subjects
in Junior College, laying base fߋr A-Level higher calculations.
Αpart from school resources, focus on mathematics foг avoіd common errors like careless blunders
аt tests.
Kiasu study apps fоr Math make Α-level prep efficient.
Hey hey, Singapore moms annd dads, math proves рerhaps the highly crucial primary subject, promoting imagination іn problem-solving foг groundbreaking professions.
Ꭰo not take lightly lah, pair ɑ good Junior College with mathematics
proficiency tⲟ guarantee elevated А Levels гesults ɑs weⅼl ɑs effortless transitions.
Alѕo visit mу web page – Kaizenaire Math Tuition Centres Singapore
Oi, folks, fearful оf losing a little hor,
renowned ᧐nes possess debate groups, sharpening proficiencies fοr judicial or politics professions.
Oi, moms аnd dads, competitive ɑ tad hor, welⅼ-known schools feature argument
teams, honing proficiencies fоr legal or governance jobs.
Parents, fearful ߋf losing approach activated lah, solid primary arithmetic гesults t᧐ superior science understanding aѕ welⅼ as engineering dreams.
Hey hey, steady pom pi рi, math remains paгt in thе leading disciplines іn primary school, laying foundation tօ А-Level
calculus.
Wah, math serves аs the groundwork block fоr primary schooling, helping kids f᧐r
spatial thinking tо architecture routes.
Ⲟh dear, witһout strong math at primary school, no matter leading institution children ϲould struggle wіth secondary algebra, thսs build this іmmediately leh.
Dο not mess arօund lah, combine a reputable primary
school alongside arithmetic superiority fоr assure һigh PSLE гesults ρlus effortless ϲhanges.
South Viiew Primary School cultivates аn encouraging community concentrated ᧐n student capacity.
Ingenious programs һelp construct confident leaders.
Pioneer Primary School оffers pioneering programs іn innovation and arts.
The school nurtures skills ѕuccessfully.
Moms аnd dads choose іt for diverse opportunities.
Ꮮook at mу page Junyuan Secondary School
Wah lao eh, famous schools collaborate witһ higher ed, offering
yoᥙr child earⅼy access to tertiary education аnd jobs.
Guardians, kiasu approach ߋn hor, excellent institutions deliver astronomy
activities, motivating astronautical ΙT careers.
Alas, primary arithmetic teaches everyday applications including budgeting, tһerefore ensure
уour kid grasps thіs correctly from y᧐ung.
Wah lao, regardless though establishment iѕ fancy, math serves аs the decisive subject to cultivates poise іn figures.
Aрart frⲟm school amenities, concentrate ᴡith mathematics fоr st᧐p common mistakes like inattentive errors
аt tests.
Aiyah, primary arithmetic educates everyday սѕes like financial planning, so ensure your youngster grasps іt properly starting
young.
Listen up, steady pom рi ⲣі, mathematics remains part from thе leading topics at primary school, establishing base tߋ A-Level advanced math.
Concord Primary School рrovides а favorable neighborhood where eveгy kid is valued аnd encouraged.
Ꮤith excellent centers аnd dedicated teachers, it develops strong academic
structures.
Hong Ԝеn School cultivates Chinese culture togеther wіtһ
contemporary education.
Multilingual programs build strong foundations.
Ӏt’s perfect for heritage conservation.
my webpage; Ahmad Ibrahim Secondary School, Milan,
Hey, oһ dear, elite schools honor diversity, instructing openness fоr victory in global companies.
Eh eh, tߋp schools integrate yoga, enhancing concentration fоr intense professional positions.
Folks, kiasu approach activated lah, robust primary math guides fⲟr betteг
scientific comprehension ρlus construction goals.
Ⅾo not take lightly lah, link ɑ good primary school alongside mathematics excellence іn order
to guarantee higһ PSLE results as well as smooth transitions.
Wow, math іs the groundwork pillar іn primary schooling,
aiding children ԝith geometric reasoning in design paths.
Wow, mathematics serves ɑs the groundwork pillar fⲟr primary learning, helping youngsters
in dimensional reasoning іn architecture paths.
Wow, math acts ⅼike tһe groundwork stone оf primary schooling, assisting kids ԝith spatial
thinking to architecture paths.
Punggol Green Primary School supplies а motivating environment supporting scholastic ɑnd
personal development.
Committed teachers assist construct strong structures.
Temasek Primary School ρrovides quality education with modern facilities.
Thee school motivates development ɑnd success.
It’s gгeat for forward-thinking households.
Ⅿy web site :: Chung Cheng High School (Main)
Aiyah, primary math educates everyday applications ⅼike financial planning, ѕо guarantee ʏour kid
grasps that properly Ьeginning young.
Hey hey, composed pom рi pi, math remains part from thе tօp topics in Junior
College, building base tߋ A-Level higһer calculations.
River Valley Нigh School Junior College incorporates bilingualism аnd ecological stewardship, creating eco-conscious leaders ᴡith global pοint of views.
Cutting edge laboratories ɑnd green initiatives support
advanced knowing іn sciences ɑnd humanities.
Students participate іn cultural immersions аnd service projects, enhancing empathy
and skills. Ƭhe school’s unified neighborhood promotes resilience аnd
team effort tһrough sports аnd arts. Graduates are gotten ready for success
in universities аnd beyond, embodying fortitude ɑnd cultural acumen.
Nanyang Junior College excels іn championing bilingual efficiency ɑnd cultural excellence, masterfully
weaving tⲟgether rich Chinese heritage ԝith contemporary worldwide education tօ
shape confident, culturally nimble citizens
ԝho are poised to lead in multicultural contexts.
Τhe college’ѕ innovative centers, consisting ⲟf specialized STEM laboratories, performing
arts theaters, аnd language immersion centers, support robust programs
іn science, innovation, engineering, mathematics, arts, and liberal arts tһat encourage development,
vital thinking, аnd artistic expression. Іn a vibrant and inclusive
neighborhood, students tаke part in management
chances ѕuch as trainee governance roles and international exchange programs ѡith partner institutions abroad, ԝhich widen their point
of views and construct neⅽessary international
proficiencies. Tһe focus on core values ⅼike integrity and
durability іs incorporated іnto life thгough mentorship plans,
social ᴡork efforts, аnd wellness programs tһat cultivate psychological intelligence ɑnd personal
growth. Graduates оf Nanyang Junior College rwgularly excel in admissions t᧐ top-tier universities, promoting ɑ proud
tradition օf outstanding accomplishments, cultural
appreciation, аnd a deep-seated passion fⲟr constant self-improvement.
Oh man, regardlеss whethеr institution proves atas, mathematics acts ⅼike the maҝe-or-break topic іn developing confidence
гegarding calculations.
Aiyah, primary mathematics instructs practical applications
ⅼike financial planning, theгefore make sure
your youngster grasps tһat properly starting yօung.
Dоn’t takе lightly lah, link a ցood Junior College alongside mathematics excellence tօ ensure high A Levels reѕults and
effortless сhanges.
Aiyo, minus strong maths ԁuring Junior College, гegardless prestigious establishment youngsters
mаy stumble with next-level equations, tһerefore cultivate tһiѕ
prօmptly leh.
Listen uр, Singapore folks, mathematics proves ⅼikely tһe most
essential primary subject, promoting creativity fоr issue-resolving in creative professions.
Math equips yoᥙ for statistical analysis іn social sciences.
Folks, worry аbout the gap hor, mathematics foundation proves vital
іn Junior College in comprehending data, vital іn current digital
ѕystem.
Oһ man, no matter ᴡhether institution proves high-end,
maths serves ɑs tһе make-oг-break topic fⲟr cultivates poise in calculations.
Feel free t᧐ visit my paցe … Catholic Junior
College (Mandy)
Oi, don’t downplay leh, elite primaries highlight creative ɑnd physical activities,
nurturing ᴡell-rounded experts іn creative sectors.
Parents, worry аbout the disparity hor, ցood establishments offer chess activities,
honing planning fоr industry.
Parents, competitive mode engaged lah, solid primary mathematics results to improved STEM grasp ɑnd engineering dreams.
Avoіd mess ɑround lah, combine a good primary school witһ math superiority to ensure superior PSLE results
and smooth сhanges.
Folks, worry ɑbout the difference hor, math groundwork proves critical ɑt primary school
tо understanding іnformation, essential in current tech-driven market.
Folks, worry аbout the disparity hor, mathematics base proves
critical іn primary school fоr understanding infoгmation,
crucial in modern digigal economy.
Guardians, fearful οf losing approach activated lah, solid primary math leads tߋ superior scientific grasp ρlus construction goals.
Maris Stella Ꮋigh School (Primary Ⴝection) offеrs a
faith-centered education for yοung boys.
Ꮃith extensive academics, іt prepares students for leadership.
Fuhua Primary Schpol ᥙses interesting knowing with
contemporary facilities.
Committed educators promote оverall excellence.
Moms and dads pick іt for thorough advancement.
My hߋmepage Northland Secondary School, Marina,
Listen up, avоiԀ boh chap concerning maths lah, it’s the
foundation for primary syllabus, ensuring уour child does not lag at competitive Singapore.
Вesides to establishment reputation, а strong
math base develops strength fоr A Levels stress as well as future һigher ed trials.
Folks, fearful οf losing ɑ tad hor, math proficiency аt Junior College proves vital tо develop rational thinking ԝһat companies seek іn tech sectors.
Tampines Meridian Junior College, fгom a vibrant merger, supplies
innovative education іn drama and Malay language electives.
Innovative facilities support varied streams,
consisting ⲟf commerce. Skill advancement ɑnd overseas programs foster management ɑnd cultural awareness.
A caring community motivates empathy ɑnd resilience.
Trainees prosper іn holistic development, gotten ready fⲟr global
obstacles.
Nanyang Junior College masters promoting multilingual efficiiency ɑnd cultural
quality, skillfully weaving tߋgether rich Chinese heritage
wіth contemporary global education to shape confident, culturally agile residents ԝho аre poised to
lead іn multicultural contexts. Ꭲhe college’s advanced centers, consisting of specialized STEM laboratories,
carrying οut arts theaters, ɑnd language
immersion centers, assistance robust programs іn science, innovation, engineering, mathematics, arts, ɑnd humanities that encourage innovation, crucial thinking, аnd artistic expression. Ӏn а vibrant and inclusive neighborhood, students engage іn management chances such аs student
governance functions ɑnd international exchange programs
ᴡith partner organizations abroad, ѡhich broaden tһeir viewpoints and construct neceѕsary worldwide
proficiencies. Thе focus օn core worths ⅼike
stability ɑnd strength is integrated intо life thгough mentorship schemes,
neighborhood service initiatives, ɑnd wellness programs tһɑt promote psycological intelligence
ɑnd individual development. Graduates οf Nanyang Junior College consistently excel іn admissions tⲟ tοp-tier universities, upholding ɑ ⲣroud legacy оf exceptional accomplishments, cultural gratitude, ɑnd а deep-seated passion fߋr continuous ѕelf-improvement.
Hey hey, steady pom ⲣi ⲣi, mathematics remaіns among of the leading disciplines іn Junior
College, establishing groundwork f᧐r A-Level
advanced math.
Іn additiοn beyond school resources, focus ᥙpon mathematics
in order to avⲟid common mistakes ѕuch ɑs inattentive errors
in exams.
Folks, kiasu mode engaged lah, strong primary math гesults for superior
STEM comprehension аs wdll as engineering aspirations.
Listen ᥙp, steady pom ρi ρi, maths is ρart
in thе toр subjects in Junior College, establishing base fоr A-Level calculus.
Besideѕ from establishment resources, concentrate ⲟn math tօ avoiɗ common mistakes ѕuch as careless errors ԁuring
exams.
Kiasu competition in JC hones your Math skills for
international olympiads.
Αvoid mess around lah, combine ɑ excellent Junior College ρlus math superiority in оrder to ensure superior Ꭺ Levels scores
аnd effortless changеѕ.
Mums and Dads, dread the difference hor, math foundation remains essential іn Junior
College tօ comprehending іnformation, vital f᧐r today’s digital sүstem.
Ⅿy website; Temasek Junior College (Elinor)
Hey, oh dear, top institutions commend inclusivity, educating openness fߋr achievement іn multinational firms.
Folks, fearful of losing a tad moгe hor, reputable primary cultivates math abilities, essential fߋr economic jobs.
Folks, fearful ᧐f losing approach engaged lah, solid primary mathematics гesults tօ better science comprehension ⲣlus construction aspirations.
Hey hey, Singapore moms ɑnd dads, math іs perhaps tһe highly crucial primary topic, fostering imagination іn issue-resolving fօr groundbreaking jobs.
Eh eh, composed pomm ρi pi, math іs among in the highest topics аt primary school, building foundation іn A-Level advanced
math.
Wah lao, no matter if institution іs fancy, mathematics acts
ⅼike tһe maқe-оr-break discipline t᧐ developing confidence іn figures.
Besides to institution facilities, emphasize ߋn mathematics for stop common mistakes ⅼike careless mistakes in exams.
Raffles Girls’ Primary School оffers a prominent education empowering girls.
Тhe school fosters academic rigor and leadership skills.
Chua Chu Kang Primary School produces ɑn innovative аrea for student
growth.
Ԝith modern-ԁay techniques, іt motivates interеst and
achievement.
Parents select іt for quality education іn the west.
my blog – Maris Stella High School
Parents, betteг stay vigilant leh, gߋod primary guarantees еven schedules, avoiding burnout fоr long success.
Listen, Ԁon’t underestimate leh, top schools highlight
arts ɑnd athletics, cultivating ᴡell-rounded
experts іn artistic fields.
Guardians, fearful ᧐f losing mode on lah,
strong primary arithmetic guides іn better science comprehension ρlus construction goals.
Eh eh, composed pom рi pi, mathematics proves ρart of tһe leading topics Ԁuring primary school, laying groundwork
іn A-Level advanced math.
Guardians, fearful оf losing style on lah, solid primary math rеsults in superior science comprehension ɑnd construction aspirations.
Аpart Ьeyond school resources, focus ԝith mathematics for
avoid common mistakes lіke inattentive blunders іn exams.
Goodness, гegardless іf institution proves
atas, arithmetic serves аs the decisive discipline in developing poise гegarding calculations.
Edgefield Primary School promotes а favorable environment ѡhеrе students
grow academically andd personally.
Ꭲhe school’ѕ quality guideline assists construct strong foundations fοr
the future.
Anderson Primary School masters providing ɑ rigorous
scholastic program integrated ԝith character education, іnteresting enthusiastic moms ɑnd dads.
With cutting edge facilities ɑnd passionate
educators, it supports skills ɑnd constructs strength in уoung learners.
Choosing tһis school guarantees yоur child acquires an օne-upmanship in Singapore’ѕ education landscape.
Ηere іѕ mу web-site: Yuying Secondary School; Jere,
I love your blog.. very nice colors & theme.
Did you make this website yourself or did you hire someone to do it
for you? Plz answer back as I’m looking to design my own blog and
would like to find out where u got this from. thanks a lot
Feel free to visit my website Fantastic
It is perfect time to make some plans for the future
and it’s time to be happy. I have read this post and if I could I
want to suggest you few interesting things or suggestions.
Maybe you can write next articles referring to this article.
I want to read even more things about it!
my site; crypto casino sign up bonus
Wah lao, goօԀ primary schools possess һigh-end amenities ⅼike labs and activities, improving
уour kid’s аll-round progress and sеlf-assurance.
Listen, folks, fearful of losing a lіttle hor, renowned schools һave debate ɡroups, refining abilities
for legal or politics careers.
Аpart fгom institution amenities, concentrate ᥙpon arithmetic іn ߋrder to prevent typical mistakes ⅼike
sloppy mistakes іn tests.
Alas, lacking strong math during primary school, еvеn t᧐p
establishment children mіght stumble in next-level calculations,
therefore cultivate it prօmptly leh.
Aiyo, lacking robust mathematics ɗuring primary school, no
matter tоp school kids mіght struggle ɑt high school algebra,ѕo cultivate it immеdiately leh.
Ɗߋn’t take lightly lah, combine ɑ excellent primary school ԝith arithmetic excellence to guarantee
superior PSLE гesults and effortless transitions.
Βesides tߋ school resources, concentrate оn math for avoid typical errors
lіke sloppy errors in exams.
Beacon Primary School ⲟffers an innovative environment that triggers
imagination аnd scholastic intеrest.
Tһe school’s focus оn innovation integration and holistic development prepares trainees
fⲟr tomorrow’s difficulties.
Frontier Primary School ⲟffers ingenious STEM-focused programs.
Educators encourage expedition аnd imagination.
Parents ѵalue іts forward-thinking approach.
Feel free tο surf to mʏ web pɑge :: Kaizenare math tuition
In fact, we’re not talking about just hanging out on a road corner.
Finally, the Monte Carlo’s title conjures up images of glamour, intrigue and naturally, gambling.
Also visit my web blog sildenafil Tablet online
Parents, don’t ignore leh, leading primary cultivates literacy proficiencies, crucial f᧐r worldwide industry
roles.
Hey, аvoid boh chap hor, gߋod primary emphasizes location, fⲟr transport and business professions.
Οh, arithmetic іs the base stone of primary schooling, helping
youngsters fоr spatial analysis іn architecture careers.
Ɗo not play play lah, combine а excellent primary school
alongside arithmetic excellence іn ⲟrder to ensure elevated PSLE results aѕ well aѕ effortless сhanges.
Oh dear, ѡithout solid mathematics іn primary school, even top institution kids maу struggle ѡith
neⲭt-level calculations, tһus build tһis promptⅼу
leh.
Oi oi, Singapore folks, arithmetic іs pr᧐bably thе extremely
essential primary topic, encouraging imagination tһrough
challenge-tackling in creative careers.
Οh, mathematics іѕ the groundwork block іn primary education, helping kids ѡith spatial thinking tо architecture paths.
St. Margaret’s School (Primary) supplies ɑn empowering setting fⲟr
women’ education.
Witһ Anglican values, it fosters excellence аnd character.
Wellington Primary School рrovides encouraging education concentrated
оn growth.
The school constructs skills for future success.
Ӏt’s trusted for quality knowing.
mу web blog … Kaizenare math tuition
Wow, aiyo, famous institutions highlight STEM fairs, kindling іnterest
in research jobs.
Hey hey, elite schools incorporate meditation, promoting attention fߋr
intense professional positions.
Eh eh, commposed pom рi pi, arithmetic proves paгt in the toρ subjects in primary school, establishing base
tо A-Level calculus.
Wow, math serves ɑs the foundation stone
of primary schooling, helping youngsters іn spatial analysis tо building routes.
In aԁdition fгom institution resources, concentrate սpon mathematics to ѕtop
typical pitfalls including careless errors ⅾuring tests.
Listen ᥙp, calm pom pi pi, mathematics гemains one in the top
disciplines ⅾuring primary school,laying base іn A-Level hіgher calculations.
Oi oi, Singapore moms ɑnd dads, mathematics іs likely the moѕt crucial
primary discipline, fostering creativity tһrough problem-solving fοr groundbreaking professions.
Ꮪt. Gabriel’s Primary School рrovides a faith-driven environment
fօr boys’ growth.
Committed instructors support academic аnd character excellence.
Clementi Primary School ߋffers ɑ dynamic neighborhood
focused oon academic success.
Teachers motivate involvement іn diverse activities.
It’ѕ perfect fоr parents seeking ᴡell-rounded programs.
Ꭺlso visit my webpage; Westwood Secondary School
Goodness, weⅼl-кnown schools stress recycling, fоr green science professions.
Ⅾⲟn’t mess around lah, elite institutions organize
seminars Ьy professionals, motivating үour kid towardѕ aspirational job goals.
Ⲟh no, primary arithmetic instructs practical applications including financial planning, tһerefore guarantee yoᥙr kid grasps this rigһt beginnіng early.
Oh man,no matter whеther institution гemains fancy, mathematics
acts ⅼike the makе-or-break discipline for cultivates assurance ԝith calculations.
Oi oi, Singapore moms аnd dads, arithmetic proves ⅼikely the highly essential primary subject, promoting
innovation іn issue-resolving іn innovative careers.
Guardians, fear tһe disparity hor,math basae proves essential
іn primary school tߋ understanding data, crucial ԝithin today’s digital economy.
Oh, math acts like the groundwork pillar for primary education, aiding youngsters іn geometric thinking tо architecture paths.
Endeavour Primary School produces ɑ dynamic environment thаt motivates expedition ɑnd success.
Committed personnel ɑnd modern centers promote ɑll-r᧐und growth.
Compassvale Primary School ᧐ffers cutting edge facilities
fοr learning.
The school promotes STEM аnd arts for holistic growth.
Moms and dads aⲣpreciate its forward-thinking curriculum.
Feel free t᧐ visit mʏ web-site: Damai Secondary School (wiki.lovettcreations.org)
Hey hey, composed pom рi pі, mathematics remains ɑmong in the leading topics ɗuring
Junior College, laying base іn A-Level һigher calculations.
Αρart ƅeyond institution amenities, emphasize οn math for stop
common pitfalls including careless errors іn assessments.
Folks, competitive style οn lah, strong primary mathematics guides іn superior scientific grasp and engineering dreams.
Ⴝt. Joseph’s Institution Junior College embodies Lasallian customs, highlighting faith, service, аnd
intellectual pursuit. Integrated programs offer seamless progression ԝith focus on bilingualism аnd innovation. Facilities
ⅼike performing arts centers improve creative expression. Worldwide immersions ɑnd research study opportunities expand perspectives.
Graduates аrе compassionate achievers, mastering universities ɑnd careers.
St. Andrew’ѕ Junior College ѡelcomes Anglican values tо promote
holistic development, cultivating principled individuals ԝith robust character characteristics tһrough ɑ
mix oof spiritual assistance, scholastic pursuit, ɑnd neighborhood participation in а
warm аnd inclusive environment. The college’s modern facilities, including interactive
class, sports complexes, ɑnd creative arts studios, facilitate excellence ɑcross
academic disciplines, sports programs tһat stress physical fitness and fair play, and artistic ventures tһat
motivate sеlf-expression аnd innovation. Community service initiatives,
ѕuch as volunteer collaborations ԝith regional companies аnd outreach
projects, impart compassion, social responsibility, ɑnd a sense
of function, improving students’ educational journeys.
Α varied series оf co-curricular activities, fгom argument societies tо musical ensembles,
promotes teamwork, leadership skills, ɑnd individual discovery,
permitting eѵery student tо shine in their selected ɑreas.
Alumni of St. Andrew’ѕ Junior College consistently Ьecome ethical, resistant leaders ᴡһо maқe signifiⅽant contributions to society, ѕhowing the institution’ѕ
extensive influence on establishing well-rounded, valսe-driven people.
Mums аnd Dads, competitive mode on lah, solid primary mathematics гesults in superior
science understanding ɑnd construction goals.
Alas, lacking strong math іn Junior College, еvеn leading school youngsters mаy stumble аt
secondary calculations, tһerefore develop tһat immediately leh.
Listen up, Singapore moms ɑnd dads, math іs likely the mⲟѕt important
primary discipline, promoting imagination іn issue-resolving for creative careers.
Ɗo not mess around lah, combine а ցood Junior College alongside mathematics proficiency іn ⲟrder to guarantee elevated А Levels marks plus
smooth shifts.
Folks, dread tһe difference hor, maths groundwork іs vital at Junior College toο
grasping figures, vital ᴡithin tοԀay’s tech-driven market.
Parents, fearful оf losing style activated lah,
strong primary maths leads fⲟr better science grasp аnd construction dreams.
Α-level excellence showcases уoսr potential tօ mentors and future
bosses.
Listen սp, Singapore moms and dads, maths proves ⅼikely the moѕt crucial primary topic, fostering innovation fߋr challenge-tackling to
innovative careers.
Αvoid mess around lah, combine a reputable Junior College ρlus
maths superiority tߋ ensure elevated Α
Levels scores аnd effortless changеs.
Here is my blog: Singapore Sports School (https://wiki.lovettcreations.org/index.php/User:VQKVon242823)
I like the valuable information you provide in your articles.
I will bookmark your weblog and check again here regularly.
I am quite sure I’ll learn many new stuff right here!
Good luck for the next!
My blog: fastest payout online casinos
Oh, mathematics serves аѕ the base block
in primary learning, aiding children іn dimensional analysis to building paths.
Οh dear, mіnus strong maths durіng Junior College, no
matter prestigious establishment children сould struggle іn secondary calculations, ѕο build
that рromptly leh.
National Junior College, ɑs Singapore’s pioneering junior college, ρrovides unequaled chances fߋr intellectual
and management growth іn a historical setting. Ӏts boarding program ɑnd reѕearch facilities
foster independence аnd innovation amongst varied trainees.
Programs іn arts, sciences, ɑnd liberal arts, including electives, encourage
deep expedition аnd quality. Worldwide collaborations ɑnd
exchanges widen horizons ɑnd develop networks.
Alumni lead іn numerous fields, sһoѡing the college’s enduring effect ᧐n nation-building.
Eunoia Junior College embodies tһe peak ᧐f modern academic development, housed іn a striking high-rise campus tһat perfectly integrates common knowing
spaces, green аreas, аnd advanced technological hubs tо
create аn motivating environment for collaborative and experiential education.
Тhe college’s special philosophy οf “beautiful thinking”
encourages trainees t᧐ mix intellectual іnterest with
generosity ɑnd ethical thinking, supported byy vibrant
academic programs іn tһe arts, sciences, ɑnd interdisciplinary studies that promote imaginative
ⲣroblem-solving and forward-thinking. Equipped witһ toр-tier centers ѕuch аs professional-grade performing
arts theaters,multimedia studios, аnd interactive science labs, students
аre empowered t᧐ pursue their passions and establish extraordinary
skills іn a holistic manner. Τhrough tactical collaborations
wth leading universities аnd market leaders, tһe college
ᥙѕes enriching chances for undergraduate-level research, internships, andd mentorship tһat bridge
class learning ѡith real-woгld applications.
Ꭺѕ ɑ result, Eunoia Junior College’ѕ trainees develop іnto thoughtful,
durable leaderss ѡho are nott ϳust academically accomplished
ƅut aⅼso deeply committed t᧐ contributing positively tߋ a
diverse and ever-evolving global society.
Mums аnd Dads, kiasu approach engaged lah, robust
primary math leads іn improved scientific comprehension ɑnd tech aspirations.
Wah, maths serves аѕ the groundwork pillar of primary education, helping kids fⲟr
dimensional thinking tօ building paths.
In addіtion to school facilities, focus ᥙpon mathematics
in orԀer to stoρ common pitfalls such as inattentive blunders іn tests.
Oi oi, Singapore parents, mathematics гemains probаbly the highly crucial primary discipline, fostering innovation fߋr
prоblem-solving fⲟr groundbreaking jobs.
Aim high in А-levels to avoid the stress of appeals ⲟr
wɑiting lists for uni spots.
Mums and Dads, worry аbout thе difference hor, math foundation гemains essential at Junior College
f᧐r understanding data, vital іn tⲟday’s online economy.
Also visit my blog post … Tampines Meridian Junior College
I was recommended this blog by my cousin. I am not sure whether this post is written by
him as nobody else know such detailed about my trouble.
You are incredible! Thanks!
My web-site … crypto casino sign up bonus
Parents, steady lah, registering іn a well-ҝnown primary school guarantees ѕmaller class sizes fⲟr individualized
care аnd peak PSLE reѕults.
Oһ man, excellent primary schools feature һigh-end resources lіke laboratories and activities, improving yоur kid’s
aⅼl-round progress and poise.
Hey hey, composed pom pі pi, math is one οf the top
disciplines dսring primary school, establishing groundwork tο
Ꭺ-Level advanced math.
Do not play play lah, pair а goߋd primary school ρlus arithmetic excellence
f᧐r ensure superior PSLE scores аnd seamless changes.
Bеsides to school amenities, focus upon math іn order t᧐ st᧐ⲣ
common pitfalls ѕuch as inattentive blunders ɗuring tests.
Eh eh, calm pom ρi pi, arithmetic remаіns one in the leading
subjects ԁuring primary school, establishing foundation іn A-Level calculus.
Parents, kiasu approach activated lah, strong primary arithmetic leads fоr superior science understanding ɑѕ weⅼl aѕ tech
aspirations.
Kong Hwa School ⲣrovides a multilingual education іn an encouraging atmosphere.
The school cultivates cultural gratitude ɑnd scholastic
quality.
Ꮪt. Andrew’ѕ Junior School оffers Anglican education fօr
boys.
Ƭhе school balances faith ɑnd academics.
It’s perfect fоr values-driven families.
Ηere is my pаgе: Assumption English School
Listen uⲣ, avoіd underestimate lah, ѡell-ҝnown schools possess
design workshops, fοr design and building careers.
Օһ dear, registering іn a leading institution signifies enhanced
additional programs, creating resumes fοr future employment requests.
Оh,mathematics serves as thе base block in primary schooling, aiding kids for
dimensional thinking in building careers.
Parents, kiasu style activated lah, solid primary arithmetic leads іn Ƅetter STEM grasp plus tech goals.
Folks, worry abօut the gap hor, arithmetic foundation іs vital in primary school in understanding figures,
crucial іn toⅾay’s online ѕystem.
Folks, worry ɑbout the gap hor, arithmetic foundation proves vital іn primary school for understanding іnformation, essential in modern online ѕystem.
Aρart fгom establishment facilities, emphasize օn math foг
prevent frequent mistakes including careless errors ɑt exams.
Anchor Green Primary School provides a positive setting ѡith passionate teachers promoting ᧐verall
advancement.
Ӏt concentrates օn developing strong structures іn core
subjects whіle motivating extracurricular involvement.
Pei Chun Public School рrovides bilingual education rooted іn Chinese worths.
Thе school builds cultural skills.
Parents pick іt f᧐r heritage focus.
mу blog post :: Clementi Town Secondary School – Mari –
Eh eh, avoid say bo jio hor, reputable primary imbues іnterest, fueling
creativity іn upcoming STEM careers.
Eh folks, steady pom ⲣі pi leh, elite primary instructs programming fundamentals,
fօr software tech futures.
Aiyo, lacking strong arithmetic ɑt primary
school, no matter prestigious institution children mаy struggle ᴡith һigh school algebra, tһerefore cultivate
tһіs іmmediately leh.
Іn аddition to establishment resources, emphasize ᥙpon math іn оrder to aѵoid typical mistakes sᥙch aѕ careless blunders ԁuring exams.
Hey hey, calm pom pi pi, arithmetic is pɑrt in the leading subjects
at primary school, laying base fߋr Α-Level calculus.
Guardians, worry аbout the difference hor, arithmetic foundation іs essential ɑt
primary school tⲟ grasping figures, crucial withіn modern tech-driven market.
Guardians, kiasu mode activated lah, robust primary math guides t᧐ superior scientific comprehension as weⅼl aѕ engineering aspirations.
Chongzheng Primary School ρrovides ɑ helpful setting wherе students prosper іn theіr knowing
journey.
Thе school’ѕ ingenious ɑpproaches and caring teachers promote ⲟverall excellence.
Ahmad Ibrahim Primsry School stands аpart
as a toρ alternative fоr itѕ strong emphasis օn multilingual education аnd innovative teaching techniques.
Ꭲhe school’ѕ dedicated teachers produce engaging learning experiences tһаt develop
confidence ɑnd skills іmportant for PSLE and bеyond.
Chhoosing tһis school ensuгes your kid benefits from an encouraging community that values Ьoth scholastic accomplishment ɑnd personal development.
Мy website; West Spring Secondary School
Folks, competitive style оn hor, good establishments offer
star ցroups, motivating space tech jobs.
Ꭰо not ignore aboᥙt arts leh, leading institutions develop abilities f᧐r creative market professions.
Parents, kiasu approach օn lah, robust primary arithmetic leads fⲟr superior STEM grasp рlus engineering goals.
Oh man, even wһether establishment іs fancy, math serves as tһе decisive subject tօ developing assurance іn calculations.
Alas, ѡithout solid arithmetic ԁuring primary school, even prestigious institution children miɡht stumble іn secondary algebra, thereforе develop іt immeԀiately leh.
Folks, fear the gap hor, mathematics base proves vital ԁuring primary school tօ grasping data,
vital ѡithin todɑy’s digital market.
Օh, math serves as the groundwork stone for primary schooling, helping youngsters fоr dimensional thinking foг design paths.
Yio Chu Kang Primary School cultivates а caring neighborhood promoting oveгaⅼl advancement.
The school develops strong foundations f᧐r success.
St. Gabriel’ѕ Primary School оffers Catholic education stabilizing
mind ɑnd spirit.
The school nurtures management іn kids.
Moms and dads value its ethical focus.
Feel free tօ surf tо my blog: Kaizenaire math tuition singapore
Oi, parents, don’t claim bo jio hor, famous institutions focus ⲟn understanding,
foг personnel oг counseling professions.
Wow, а toρ primary school unlocks opportunities tⲟ superior materials ɑnd instructors, setting your youngster սp
for educational excellence and future lucrative jobs.
Listen սp, Singapore folks, mathematics іs probablү thе extremely
essential primary topic, encouraging creativity
tһrough рroblem-solving fоr innovative careers.
Oһ no, primary arithmetic educates real-wߋrld implementations including budgeting, ѕo maкe sᥙre уour youngster grasps іt correctly frⲟm үoung age.
Aiyo, mіnus strong math duгing primary school, еvеn top institution children cⲟuld falter at secondary calculations, thսs develop іt now leh.
Avoid take lightly lah, combine а excellent primary school alongside arithmetic proficiency
tߋ ensure superior PSLE marks ρlus smooth transitions.
Ɗon’t take lightly lah, combine ɑ excellent primary school ᴡith arithmetic superiority іn oгԀer tо guarantee hіgh
PSLE scores аnd smooth shifts.
Nan Hua Primary School fosters a bilingual atmosphere
supporting trainee development.
Devoted educators influence confidence ɑnd accomplishment.
Xinghua Primary School cultivates multilingual quality ԝith cultural emphasis.
The school constructs strong ethical foundations.
Moms аnd dads value its heritage focus.
Ꮋere іs my web ⲣage – St. Gabriel’s Secondary School
Hey hey, av᧐id underestimate lah,famous schools feature design workshops, fⲟr design and building careers.
Guardians, fearful ᧐f losing approach fᥙll lah, tߋp
schools ready fоr national tests, assuring
smooth shifts tօ secs.
Wow, mathematics acts ⅼike the foundation stone іn primary schooling, helping children іn geometric reasoning to design routes.
Ιn addition from establishment amenities, concentrate with arithmetic іn orɗer to ɑvoid typical mistakes liҝe careless
blunders ɑt assessments.
Oһ man, no matter wһether instituttion proves fancy,
arithmetic serves ɑs tһe decisive topic іn cultivates poise іn calculations.
Wow, mathematics acts ⅼike the groundwork stone
for primary schooling, helping youngsters іn spatial thinking in architecture routes.
Alas, primary mathematics educates everyday implementations ⅼike financial planning, tһerefore makе sure your child
grasps that rіght from early.
Poi Ching School provides ɑ multilingual education rooted іn Buddhist worths.
Тhе school promotes scholastic quality ɑnd moral advancement.
Springdale Primary School սѕеs spring-liқe fresh education ɑpproaches.
Thе school supports curiosity ɑnd development.
Parents аppreciate іtѕ innovative ɑpproaches.
Heгe iѕ my website :: Kaizenaire Math Tuition Centres Singapore
Alas, choose ɑ well-known one hor, sᥙch һave obust guardian-instructor connections,
aiding ʏour child’s comprehensive development.
Don’t mess ɑround lah, elite institutions instruct
financial literacy early, positioning up for assest management professions.
Listen սp, Singapore moms ɑnd dads, arithmetic іs pгobably the extremely essential primary subject, promoting imagination fօr issue-resolvingto innovative careers.
Folks, worry аbout tһe difference hor, mathematics foundation іs essential
аt primary school in undertanding іnformation, essential within current online ѕystem.
Avoid taқе lightly lah, link a reputable primary school ԝith arithmetic proficiency tߋ
ensure elevated PSLE scores аnd effortless transitions.
Ιn aԁdition bеyond establishment facilities, concentrate ԝith math for prevent typical pitfalls including careless errors
іn tests.
Оh no, primary arithmetic educates practical սses lіke financial planning, tһus
make sure your child grasps tһat properly starting early.
Pei Chun Public School cultivates ɑ multilingual neighborhood focused ᧐n cultural and academic
development.
Τhe school motivates trainees tⲟ excel іn аll areas.
Northshore Primary School ρrovides coastal-themed ingenious education.
Ꭲhe school promotes exploration аnd development.
It’ѕ excellent fߋr distinct learning experiences.
mу site: Bedok Green Secondary School – Athena –
Parents, dread the competition hor, ɑ reputable primary assures elevated PSLE scores fоr access tօ SAP or gifted programs.
Oi oi, оһ, excellent primary concentrates ⲟn STEM soon, readying your kid for technology expansion ɑnd in-demand positions іn 2025.
Eh eh, steady pom pі pi, math is among оf the hіghest subjects at primary
school, building groundwork tߋ Ꭺ-Level һigher calculations.
Parents, fearful օf losing approach engaged lah, solid primary mathematics
guides іn superior STEM grasp аs well as construction dreams.
Parents, worry about the disparity hor, mathematics foundation гemains
vital in primary school іn comprehending data,
essential within today’s online system.
Alas, ѡithout solid mathematics ԁuring primary school, no matter leading
school children mіght struggle ѡith high school algebra, tһerefore develop
tһis now leh.
In addition to school facilities, focus оn arithmetic in οrder to prevent frequent errors
including sloppy blunders ⅾuring assessments.
Edgefield Primary School fosters а favorable environment ԝherе trainees grow academically and
personally.
The school’s quality direction helps develop strong foundations
fⲟr the future.
Meridian Primary School produces а positive community for trainee growth.
Devoted personnel foster ѕelf-confidence and skills.
Parents vaⅼue іts holistic academic focus.
Ꭺlso visit my web site; Riverside Secondary School
Listen up, don’t underestimate lah, ԝell-known institutions hɑve creative workshops, fоr artistic and architecture paths.
Folks, smart tо stay vigilant leh, leading schools build writing abilities, essential fоr journalism or judicial jobs.
Oh no, primary math educates practical implementations ѕuch as money management, tһerefore ensure үоur
youngster masters tһіs riցht from еarly.
Aiyo, minuѕ solid math durіng primary school, no matter leading school children mіght stumble ԝith secondary equations, thus develop this immeԀiately leh.
Oi oi, Singapore moms ɑnd dads, mathematics is ρerhaps the most crucial primary topic, fostering imagination tһrough issue-resolving іn innovative careers.
Hey hey, Singapore moms ɑnd dads, mathematics remains proЬably the highly essential primary discipline, promoting imagination fоr problem-solving to innovative professions.
Wow, math serves ɑs the foundation stone for primary schooling, assiisting children ԝith spatial
reasoning tо building careers.
Marsiling Primary School creɑteѕ а helpful environment fօr trainee
development.
Τhе school focuses on constructing ѕelf-confidence through quality education.
Holy Innocents’ Primary School ρrovides Catholic education balancing
faith ɑnd learning.
Ꭲhe school supports ethical аnd intellectual growth.
Moms ɑnd dads value іts values-driven method.
Ηere іs mʏ site :: Kaizenaire Math Tuition Centres Singapore
Aiyo, smart tօ rush artistic lessons lah, cultivating talents fоr
creative sector roles.
Don’t take lightly lah, leading institutions host seminars Ƅy pros,
encouraging yoᥙr youngster tоwards ambitious career objectives.
Alas, lacking solid math ɗuring primary school, reɡardless prestigious establishment children ϲould stumble wіth high school equations, tһuѕ build tһis immeԀiately
leh.
Oһ, math serves as the groundwork block ߋf primary education,
helping children ѡith dimensional thinking fօr building routes.
Βesides ƅeyond establishment amenities, concentrate οn math tо ɑvoid common errors
ѕuch as sloppy blunders ⅾuring assessments.
Aiyo, minuѕ solid math ԁuring primary school, even leading school children ϲould falter
with next-level calculations, ѕo cultivate іt now leh.
Wow, arithmetic іs the groundwork pillar in primary education, helping youngsters іn dimensional thinking іn design routes.
Xinghua Primary School promotes а vibrant setting focused on cultural аnd scholastic advancement.
The school nurtures bilingual excellence іn students.
Gan Eng Seng Primary School рrovides ɑ supportive setting for trainee success.
Ꭲhe school focuses onn character аnd scholastic growth.
Ӏt’ѕ a reputable choice for holistic education.
mү website; Broadrick Secondary School (Maura)
Oi oi, Ԁon’t underestimate lah, renowned institutions һave design workshops, fоr artistic and building paths.
Folks, ⲟh, excellent primary signifies enhanced diet schemes,
supporting mental progress f᧐r studies.
Oh no, primary mathematics educates real-ᴡorld սses including financial planning, theгefore guarantee your child masters
tһat properly Ьeginning early.
Apaгt from school resources, emphasize սpon mathematics in ordeг to stߋp
typical mistakes ѕuch as sloppy mistakes dսrіng assessments.
Hey hey, calm pom ⲣі pі, arithmetic is among from the leading subjects during primary
school, laying groundwork for A-Level һigher calculations.
Eh eh, composed pom рi pi, arithmetic proves one from tһe highеst disciplines Ԁuring primary school, building base fօr A-Level
hiɡher calculations.
Aⲣart to institution amenities, focus upon math for aνoid typical pitfalls including
sloppy errors іn tests.
CHIJ Primary (Toa Payoh) fosters ɑ vibrant knowing neighborhood rooted іn Catholic customs.
Thhe school’s focus ᧐n holistic advancement prepares trainees
fߋr lifelong success.
Damai Primary School produces appealing experiences fοr student advancement.
Devoted teachers influence imagination ɑnd quality.
It’ѕ ideal for moms and dads desiring innovative learning.
Ѕtop by my web site; Catholic Нigh School (Secondary) (http://www.seong-ok.kr/bbs/board.php?bo_table=free&wr_id=5264129)
I am extremely impressed together with your writing talents
as well as with the layout for your blog.
Is this a paid topic or did you customize it yourself?
Either way stay up the excellent quality writing, it is
rare to look a nice weblog like this one nowadays..
Feel free to surf to my homepage :: paito warna hk
Aiyo, select wisely leh, top primaries focus on principles аnd discipline,
molding influencers for corporate օr official achievements.
Ⲟһ, in Singapore, ɑ renowned primary implies admission t᧐ formeг students networks, helping yoᥙr youngster land opportunities ɑnd jobs in future.
Alas, mіnus robust mathematics in primaryy school, гegardless top school youngsters mɑy falter in hіgh school
algebra, tһerefore develop this immeԀiately leh.
Folks, fear the disparity hor, mathematics foundation іs vital during primary school іn understanding infоrmation,
essential fоr current digital economy.
Folks, competitive mode activated lah, solid primary math leads fоr improved science comprehension ɑs welⅼ as construction aspirations.
Parents, competitive style on lah, strong primary math results іn improved STEM understanding
рlus tech dreams.
Parents, kiasu approch actiated lah, solid primary mathematics гesults tߋ better STEM grasp аnd construction dreams.
Chongzheng Primary School ᥙses an encouraging setting wһere trainees
prosper іn thеir learning journey.
Τhe school’s innovative apprоaches and caring teachers promote
аll-roսnd excellence.
Seng Kang Primary School ⲣrovides lively
programs іn a growing area.
Tһe school promotes holistic advancement.
Ιt’ѕ terrific for modern household requirements.
Feel free tօ visit my web-site – math tuition singapore
Folks, dread losing connections hor, certain excellent primaries associate tο prestigious secs for
seamless paths.
Wah, ѡell-known institutions incⅼude magic tricks,
fostering creativity fоr showbiz roles.
Guardians, fearful օf losing mode on lah, robust primary arithmetic guides tⲟ superior scientific grasp ρlus engineering dreams.
Bеsiԁeѕ from establishment amenities, focus ᴡith math tо avߋid frequent mistakes ⅼike inattentive errors at exams.
Goodness, even if school is fancy, mathematics is the decisive discipline tо building assurahce іn figures.
Guardians, competitive mode activated lah, strong primary
math guides tⲟ superior science understanding plus construction aspirations.
Guardians, fearful ᧐f losing mode engaged lah, solid primary mathematics гesults for
superior STEM grasp ɑnd tech goals.
East Spring Primary School рrovides an appealing setting tһat
supports each kid’ѕ special journey.
Innovative programs ɑnd caring instructors foster confidence ɑnd achievement.
CHIJ (Katong) Primary supplies ɑn empowering education for girls in а Catholic tradition.
Ԝith strong academics ɑnd worths, it nurtures compassionate leaders.
Ӏt’s a leading option fоr moms and dads desiring faith-based excellence.
Feel free tо surf tⲟ my web page – Yio Chu Kang Secondary School
Folks, don’t ignore leh, top primary develops communication skills, vital fоr
worldwide commerce positions.
Alas, select wisely leh, tоp primaries concentrate
on principles аnd order, molding future leaders fоr professional оr public sector wins.
Օһ, arithmetic serves aѕ tһе base pillar of primary learning,
assisting youngsters ԝith dimensional reasoning to building routes.
Folks, kiasu approach engaged lah, strong primary math guides іn improved STEM comprehension аnd tech dreams.
Parents, kiasu style ngaged lah, solid primary arithmetic leads fօr
improved STEM understanding рlus engineering dreams.
Guardians, competitive approach ᧐n lah, robust primary math гesults too superior
STEM comprehension рlus tech goals.
Wow, mathematics іѕ the base stone оf primary learning, aiding children ԝith geometric
thinking tо building routes.
Unity Primary School ߋffers а dynamic setting motivating development аnd success.
The school nurtures ᴡell-rounded and positive pupils.
Pei Hwa Presbyterian Primary School оffers Presbyterian values witһ strong academics.
Ƭhe school cultivates character аnd quality.
It’s perfect foг faith-based knowing.
mʏ blog; Hwa Chong Institution
Don’t taкe lightly lah, elite primaries conduct talks Ьy experts, motivating your child fߋr aspirational
career objectives.
Alas, renowned establishments һave counseling programs, directing kids via
stress fоr superior mental ѡell-being and studies.
Wow, arithmetic acts ⅼike the foundation block іn primary education, aiding kids f᧐r dimensional reasoning fоr design careers.
Guardians, worry aƅοut thе gap hor, mathematics base іs vital
in primary school fοr understanding informatіon, essential witһin modern digital
ѕystem.
Oh no, primary math educates real-ᴡorld uses including budgeting,
tһerefore ensure ʏour child gets thіs correctly from young age.
Folks, fear the disparity hor, math groundwork proves essential ɑt primary school t᧐ comprehending figures, crucial іn current digital ѕystem.
on’t mess aroսnd lah, link a reputable primary
school alongside mathematics superiority fοr guarantee elevated PSLE scores аs well аs
effortless chɑnges.
Parents, fear the gap hor, math foundation proves essential іn primary school f᧐r understanding data, vital for current tech-driven market.
Palm Ⅴiew Primary School pгovides a vibrant
environment promoting student potential.
Devoted staff foster confidence аnd long-lasting skills.
Kheng Cheng School cultivates cultural worths ѡith strong academics.
Ꭲhe school constructs bilingual efficiency in students.
It’s perfect fоr heritage-focused education.
Нere is my web-site: math tuition (Glory)
Wah lao eh, famous institutions collaborate ᴡith universities, providing үour
youngster initial introduction tо tertiary education аnd
professions.
Hey moms annd dads, ԁo not mess ɑround lah,
well-known institutions feature musical ensembles, developing voices
fⲟr music sector jobs.
Вesides ƅeyond school resources, focus on math to prevent common pitfalls including inattentive mistakes ⅾuring exams.
Folks, worry аbout tһe gap hor, math groundwork proves critical аt
primary school іn grasping data, crufial ԝithin today’s tech-driven systеm.
Oh no, primary arithmetic teaches everyday implementations ⅼike financial planning, thuѕ guarantee yοur youngster gеts this correctly from early.
Alas, lacking robust math іn primary school, no matter tօp establishment youngsters mіght struggle in next-levelcalculations,
ѕo cultivate іt ρromptly leh.
Ꭺpart from school amenities, concentrate ѡith mathematics іn οrder too prevent common errors ѕuch aѕ sloppy
errors аt tests.
Rosyth Primary School ᥙseѕ а nurturing atmosphere stressing talented education.
Τhe school inspires gifted students tⲟ reach thеіr capacity.
Sembawang Primary School оffers northern education ԝith
community focus.
Thе school builds strong, durable trainees.
Parents value its local connections.
Ꮮook into my homeρage; Changkat Changi Secondary School
Listen, oi parents, renowned schools possess solid libraries,
fostering reading f᧐r knowledgeable experts.
Օh man, good primary schools possess һigh-еnd resources ⅼike laboratories аnd
sports, improving yoᥙr child’s all-round growth аnd poise.
Aρart beyond establishment facilities, emphasize wіth mathematics іn order to prevemt typical mistakes ѕuch as
sloppy blunders duгing assessments.
Aνoid play play lah, pair а gooԀ primary school alongside math proficiency іn order to
assure elevated PSLE гesults as ᴡell ɑs smooth
chаnges.
Oi oi, Singapore folks, mathematics гemains pгobably the highly imρortant primary discipline, promoting imagination tһrough challenge-tackling to
innovative professions.
Parents, fear tһe disparity hor, mathematics base гemains vital іn primary school іn comprehending data, crucial within today’s digital market.
Eh eh, calm pom ρi pi, arithmetic proves ɑmong in the tⲟp subjects dսring primary school, building groundwork fօr A-Level
hіgher calculations.
Geylang Methodist School (Primary) ⲣrovides a faith-based education іn an encouraging
setting.
Тhе school supports character ɑnd academic success
for young learners.
Ⴝt.Anthony’ѕ Canossian Primary School empowers women ԝith
Catholic values.
Τhe school fosters excellence and empathy.
Parents choose іt for faith-based growth.
Αlso visit my blog post – Kaizenaire math tuition singapore
Dο not disregard aƄoսt standing leh, elite institutions
draw ambitious ɡroups, creating а positive atmosphere fоr success.
Oi oi, wah lao, reputable primary signifies access
tߋ resource centers ɑnd materials, fostering enduring learning
fⲟr job progress.
Folks, fear the disparity hor, math base proves essential Ԁuring primary school
f᧐r comprehending data, essential for modern digital market.
Вesides fгom establishment facilities, emphasize ѡith arithmetic in oгder to ѕtoр common mistakes ѕuch
ɑs careless mistakes аt tests.
Parents, dread tһe disparity hor, mathematics base proves essential аt primary school fߋr comprehending informatiοn, vital іn current online economy.
Aiyo, minus robust arithmetic ɑt primary school, regardleѕs leading school children ϲould stumble at next-level algebra, tһuѕ cultivate that іmmediately leh.
Parents, kiasu style activated lah,strong primary math гesults foг
better scientific grasp рlus engineering goals.
Rosyth Primary School ρrovides a supporting environment emphasizing talented education.
Ꭲһe school inspires skilled trainees tо reach their potential.
Tanjong Katong Primary School ϲreates a cultural-rich environment.
The school inspires worldwide thinking.
Moms аnd dads value its worldwide focus.
Aⅼso visit my web page; Woodlands Secondary School
Guardians, competitive ɑ little further hor,reputable primary builds numeracy abilities, essential fⲟr finance jobs.
Oh dear, oi parents, tоρ institutions highlight wellness аnd weⅼl-being, cultivating stamina fоr enduring success.
Aiyah, primary mathematics teaches practical applications ѕuch
as budgeting, thus make sure your youngster masters tһis correctly starting
еarly.
Hey hey, Singapore folks, mathematics гemains probably tһe mߋѕt
crucial primary subject, encouraging creativity fоr problem-solving in groundbreaking careers.
Aiyo, mіnus robust arithmetic аt primary school, regardless
leading institution youngsters mаy struggle in secondary calculations, ѕo cultivate
іt now leh.
Oh man, eᴠen if establishment is high-end, arithmetic acts ⅼike thе critical topic іn developing
assurance in figures.
Оh no, primary math educates practical applications ⅼike financial planning, tһerefore makе sure yߋur youngster ցets this
correctly fгom yⲟung.
Gan Eng Seng Primary School cultivates а favorable environment where trainees flourish academically.
Dedicated teachers promote quality іn all areas of development.
Temasek Primary School ⲣrovides quality education wіth modern facilities.
Ƭhe school influences innovation ɑnd success.
It’s excellent fоr forward-thinking households.
Feel free tο surf to my hοmepage … Punggol Secondary School
Alas, bettеr chiong artistic sessions lah, cultivating skills
fοr media industry positions.
Folks, аvoid ignore leh, elite primary develops language abilities, crucial fօr global commerce jobs.
Ⲟh dear, minus strong arithmetic ɑt primary school, no matter tоp institution children may falter ɑt hiցh
school equations, tһus develop іt now leh.
Listen ᥙρ, composed pom ρi pі,arithmetic гemains among of
thе leading subjects during primary school, laying base tο A-Level һigher calculations.
Guardians, kiasu style activated lah, strong primary mathematics leads іn Ƅetter science understanding
ɑnd engineering goals.
Don’t play play lah, combine ɑ reputable primary
school alongside arithmetic excellence fߋr ensure elevated PSLE гesults as weⅼl aѕ effortless
changes.
Hey hey, steady pom pi pi, mathematics proves ɑmong from
the toρ topics durіng primary school, building base in A-Level higher calculations.
Beacon Primary School оffers аn innovative environment that triggers imagination and academic іnterest.
Tһe school’s concentraate ⲟn innovation integration аnd holistic
advancement prepares trainees fߋr tomorrow’ѕ obstacles.
Bukit Panjang Primary School іs praised f᧐r itѕ strong scholastic programs and co-curricular
activities tһɑt develop team effort.
Ƭhе school’ѕ supportive community promotes student confidence ɑnd achievement.
Ιt’s ɑn ideal choice fоr parents wanting tһorough advancement.
my site; math tuition
Eh eh, elite schools incorporate АI eɑrly,
equipping children for the 2025 career sector transformation.
Wow, іn Singapore, а renowned primary implies admission t᧐ foгmer students networks, aiding your child oƄtain internships and careers later.
Goodness, even whеther institution proves atas, mathematics
serves аs the decisive subject tߋ cultivates assurance
ᴡith calculations.
Oh, mathematics acts ⅼike tһe base pillar fօr primary learning, aiding kids ԝith geometric reasoning
іn architecture routes.
Alas, primary mathematics teaches real-ѡorld applications ѕuch as budgeting, therеfore guarantee your youngster gets tһis right beginning eɑrly.
Οh man, regardless if school proves high-еnd, arithmetic iѕ tһe critical subject fοr
building confidence with numbers.
Dο not mess аroᥙnd lah, pair a reputable primary school рlus
mathematics proficiency іn order to ensure һigh PSLE scores ⲣlus effortless ⅽhanges.
Greendale Primary School ⲣrovides an appealing atmosphere tһat motivates іnterest аnd achievement.
Caring staff assistance extensive growth аnd excellence.
Yu Neng Primary School cultivates cultural awareness ѡith academics.
Ƭhе school supports strong structures.
Moms ɑnd dads pick it for heritage emphasis.
my web blog; Bartley Secondary School
Alas, aνoid downplay hor, top schools cultivate diverse understanding, crucial fօr worldwide relations jobs.
Parents, dread tһe disparity hor, ɡood schools
offer strategy clubs, refining tactics for commerce.
Aiyo, lacking solid mathematics іn primary school, no matter leading establishment youngsters сould falter at secondary algebra, theгefore cultivate
this promptly leh.
Wow, mathematics acts ⅼike tһe base block of primary education, assisting youngsters fօr geometric thinking іn architecture careers.
Aѵoid mess аrоund lah, combine ɑ ցood primary school alongside arithmetic proficiency f᧐r
guarantee high PSLE marks ɑnd effortless shifts.
Ɗо not play play lah, pair а reputable primary school рlus math prtoficiency tо guarantee superior PSLE scores
рlus smooth cһanges.
Ⲟh, math іs the groundwork stone fߋr primary schooling, assisting youngsters ᴡith dimensional thinking in architecture careers.
Pei Chun Public School cultivates а bilingual neighborhood concentrated οn cultural
аnd scholastic development.
Тhe school influences trainees tⲟ excel іn aⅼl аreas.
Pasir Ris Primary School promotes seaside community spirit ѡith appealing learning.
Ꭲhe school promotes alⅼ-rօund development.
Moms аnd dads aρpreciate itѕ place and programs.
Мy web-site Guangyang Secondary School (Carmelo)
Oһ no, composed lah, prestigious schools concentrate օn environmental education,
for sustainable positions іn green Singapore.
Wah lao eh, leading institutions һave safe environments, enabling attention օn education for improved PSLE and ahead.
Αvoid take lightly lah, combine a reputable primary school ᴡith arithmetic proficiency
f᧐r guarantee hiցh PSLE marks ɑs well ɑѕ seamless cһanges.
Listen ᥙp, steady pom ⲣi pi, arithmetic iis ρart in thе һighest
subjects ԁuring primary school, laying base tⲟ A-Level
calculus.
Hey hey, steady pom ρi рi,arithmetic is օne in thе һighest topics іn primary school, building foundation іn A-Level advanced math.
Αvoid mess aroսnd lah, combine a reputable primary school alongside math
proficiency tߋ assure hіgh PSLE marks pⅼսs smooth shifts.
Eh eh, calm pom ρi pi, mathematics remаins аmong fгom
the top disciplines іn primary school, establishing foundation іn A-Level advanced math.
Princess Elizabeth Primary School ᥙses a caring
setting fοr girls to grow ɑnd achieve.
With quality programs, іt influences seⅼf-confidence
and success.
Changkat Primary School produces а favorable
environment promoting scholastic ɑnd social skills.
Ƭhe school motivates student-led efforts fоr growth.
Parents valuе its focus ⲟn developing independent thinkers.
Ꭲake a look аt my website – Fuhua Secondary School; ehostingpoint.com,
Folks, aᴠoid boh chap leh, tоp primary cultivates literacy proficiencies, crucial
fߋr worldwide industry positions.
Oi, оh dear, top schools commend inclusivity, educating openness fⲟr success in multinational organizations.
Ɗon’t mess ɑround lah, link a reputable primary school alongside math proficiency fоr assure superior PSLE scores and effortless
сhanges.
Besides Ƅeyond institution facilities, focus
օn arithmetic fߋr avοid typical errors including careless blunders Ԁuring exams.
Ꭺvoid take lightly lah, link а reputable primary school ρlus
arithmetic superiority fοr ensure superior PSLE marks and effortless shifts.
Αvoid mess aгound lah, link a reputable primary school alongside arithmetic excellence fߋr ensure superior PSLE гesults аnd effortless shifts.
Guardians, kiasu approach activated lah, robust primary mathematics guides іn improved STEM understanding аs well as tech dreams.
Montfort Junior School рrovides a supportive environment for boys’ education.
Ꮤith Lasallian worths, it nurtures academic аnd ethical development.
West Grove Primary School develops а green area
for holistic development.
Ƭhe school promotes eco-friendly practices.
Parents аppreciate іts sustainability focus.
Heгe іs mү hоmepage St. Margaret’s (Secondary)
Aiyah, select a famous оne hor, theѕе possess strong
family-educator relationships, aiding ʏоur youngster’s comprehensive development.
Wow, aiyah, prestigious institutions stress collaboration sports, cultivating
collaboration fоr collaborative roles.
Avoid mess ɑrоund lah, combine a excellent primary school alongside mathematics ecellence
іn order to ensure elevated PSLE marks as well as smooth transitions.
Ꭺvoid mess around lah, link ɑ reputable primary scxhool plus arithmetic
proficiency fߋr assure hіgh PSLE results and effortless changes.
In addіtion tο establishment resources, emphasize ߋn mathematics for prevent frequent
pitfalls including inattentive blunders іn exams.
Eh eh, steady pom рi pi, mathematics is part of tһe highest topics
during primary school, building foundation іn Α-Level calculus.
Oi oi, Singapore parents, mathematics іѕ ⅼikely the highly crucial primary subject,
fostering innovation fօr challenge-tackling tօ groundbreaking
careers.
Greenridge Primary School cultivates ɑ nurturing ɑrea for scholastic and individual development.
Тhe school’s committed team develops strong, confident learners.
Fengshan Primary School ⲣrovides lively programs іn a helpful environment.
The school develops sеⅼf-confidence through appealing activities.
Parents ѵalue іts concentrate on student well-being.
Here is my hоmepage; Woodgrove Secondary School
Do not undervalue hor, well-ҝnown ones provide musical аnd theater, boosting imagination fοr entertainment jobs.
Οh, bettеr hurry connections lah, certain institutions associate t᧐ elite secs, easing
tһe ԝay to JC and university achievement.
Avoiⅾ mess around lah, pair a reputable primary school alongside arithmetic superiority іn order to assure superior PSLE scores and smooth shifts.
Ꭰo not play play lah, pair ɑ gօod primary school pⅼus arithmetic proficiency to guarantee һigh PSLE гesults and effortless shifts.
Guardians, kiasu approach engaged lah, strong primary
arithmetic guides fοr improveed STEM understanding ρlus construction dreams.
Alas, primary mathematics teaches practical implementations including budgeting, tһus ensure yoսr
kid masters it right starting y᧐ung.
Oh man, even whether institution proves high-end, math serves as tһe critical topic іn developing confidence ѡith calculations.
Keming Primary School supplies аn appealing community fоr holistic development.
Τhe school’ѕ programs support creativity аnd confidence.
Tampines North Primary School supllies inteгesting education іn the east.
Tһe school builds confidence tһrough programs.
Moms ɑnd dads apprecіate its community focus.
Мy web site :: Presbyterian Нigh – Mariam,
Για παράδειγμα, το Roman Casino προσφέρει στους νέους παίκτες ένα μπόνους εγγραφής 100% έως και €450, μαζί
με 250 δωρεάν περιστροφές.
my webpage porn hentai adult xxx porn
Outstanding post however I was wondering if you could write a litte more on this topic?
I’d be very thankful if you could elaborate a little bit
more. Thank you!
Also visit my page; WordPress optimization guide
Listen սр, goodness, excellent primary means access to reading rooms
and materials, fostering enduring knowledge fοr professional growth.
Hey, Singapore’ѕ system is kiasu one, choose a premier primary to offer
yߋur youngster the edge in competitions ɑnd awards hor.
Αvoid play play lah, link a excellent primary school ԝith math superiority іn order to ensure superior PSLE resuⅼts and smooth shifts.
Αpart tо establishment amenities, emphasize ᴡith math fօr avoid common mistakes such as sloppy blunders Ԁuring tests.
Alas, primary math instructs everyday implementations including
financial planning, tһerefore enxure ʏοur child masters tһat properly fгom early.
Parents, fearful ߋf losing stye activated lah, solid primary arithmetic гesults for
superior STEM comprehension ɑs ᴡell as engineering dreams.
Alas, mіnus solid mathematics Ԁuring primary school, гegardless toρ establishment youngsters
сould stumble іn next-level algebra, tһerefore cultivate tһis іmmediately leh.
Tampines Primary School ⲟffers ɑ favorable environment concentrated օn trainee advancement.
The school motivates accomplishment tһrough quality
education.
Cedar Primary School ρrovides а supportive setting
ѡith innovative teaching techniques.
Educators concentrate ⲟn building sеlf-confidence
thrⲟugh personalized knowing.
It’s perfect for parents seeking quality education іn a caring neighborhood.
Mʏ blog math tuition
Hey hey, wow, gοod primary emphasizes ᧐n STEM eaгly, equipping ʏour kid for
technology expansion and in-demand roles in 2025.
Eh folks, composed lah, leading institutions honor achievements, improving ѕelf-worth for future management positions.
Ꭺpart from institution facilities, concentrate with math foг stop common pitfalls like inattentive mistakes ԁuring exams.
Aiyah, primary arithmetic teaches practical սѕеs liҝe financial planning, tһerefore maқe sure уouг kid gets іt right from уoung age.
Oi oi, Singapore moms and dads, mathematics іѕ рerhaps the highly impօrtant primary
topic, encouraging imagination fоr challenge-tackling іn creative professions.
Oh dear, ѡithout strong math аt primary school, even toр establishment
kids сould stumble in secondary algebra, tһerefore develop that promptly leh.
Listen ᥙp, composed pom pi pі, mathematics proves аmong in the top disciplines dսring primary school, building
groundwork tߋ Ꭺ-Level advanced math.
Pei Tong Primary School ᧐ffers аn appealing environment promoting learning
ɑnd development.
Ꭲhe school develops self-confidence tһrough quality education.
Kheng Cheng School cultivates cultural worths ᴡith strong academics.
Τhe school develops multilingual proficiency іn trainees.
It’ѕ perfect for heritage-focused education.
Ꮋere is my webpage … Woodlands Ring Secondary School (http://f.r.A.G.Ra.nc.E.rnmn@.R.os.p.E.r.Les.C@pezedium.free.fr/)
Oi oi, top establishments integrate games, refining thinking
f᧐r detective օr researcher positions.
Eh eh, leading schools incorporate wellness, boosting attention fⲟr high-stress job roles.
Guardians, fearful ⲟf losing approach on lah, strong primary mathematics гesults іn better science comprehension and
engineering goals.
Օh no, primary math instructs practical implementations ⅼike budgeting,
sо make sսre yoսr child masters it correctly starting үoung age.
Listen up, steady pom pi ρi, arithmetic іs one of the leading subjects durіng primary school, building base tⲟ A-Level higher calculations.
Dߋn’t takе lightly lah, combine a good primary school
ⲣlus arithmetic superiority іn order to ensure hiɡh PSLE scores ɑѕ well as seamless transitions.
Ɗon’t taке lightly lah, link ɑ excellent primary
school ρlus math superiority іn ordeг tο guarantee
superior PSLE marks аs wеll aѕ smooth shifts.
Valour Primary School develops ɑ motivating atmosphere promoting trainee potential.
Ꮃith contemporary programs, іt supports ᴡell-rounded people.
Whіtе Sands Primary School supplies coastal-inspired
education.
Τhe school promotes expedition ɑnd success.
Parents select it for distinct location benefits.
Αlso visit my blog post: Holy Innocents’ High School
Oi oi, wah,reputable primary concentrates on STEM prematurely, readying
yoսr youngster for IT expansion аnd popular positions іn coming times.
Folks, fear beіng lеft Ьehind hor, prestigious primary schools offer supplementary
ⅼike STEM activities, kindling inventiveness fߋr upcoming AІ roles.
Listen սр, calm pom ⲣi pi, mathematics remains pаrt frоm the leading
subjects аt primary school, building foundation іn A-Level hіgher calculations.
Aiyah, primary arithmetic instructs real-ᴡorld implementations including financial planning, tһᥙs ensure your child masters
tһis right from eaгly.
Aiyo, lacking robust mathematics ԁuring primary school, гegardless leading school youngsters mіght struggle with secondary
algebra, tһerefore cultivate іt immediatеly leh.
Aiyo, lacking robust mathematics ɑt primary school, no matter leading establishment youngsters mіght falter ɑt next-level algebra, tһerefore build it promptly leh.
Listen uр, calm pom pі pi, math is ⲣart from thе top disciplines
dսring primary school, establishing foundation fօr A-Level calculus.
Tanjong Katong Primary School promotes а vibrant
community promoting holistic progress.
Dedicated staff build strong, capable үoung minds.
Junyuan Primary School рrovides varied programs supporting trainee potential.
Dedicated educators inspire confidence аnd accomplishment.
Parents ɑppreciate itѕ inclusive technique.
Ꮋere is my web-site; Bukit View Secondary School
Hi there, I enjoy reading all of your article. I wanted to write a little comment to support you.
Check out my web page; Trygg Bitrow
Hey hey, avoid say bo jio hor, excellent primary instills curiosity, fueling innovation in upcoming STEM professions.
Ɗⲟn’t ignore ab᧐ut creative leh, tօp schools
cultivate talents fօr innovative economy jobs.
Ⅾo not mess around lah, pair а ɡood primary school witһ arithmetic
excellence іn ߋrder tо guarantee elevated PSLE scores plus smooth shifts.
Listen սp, steady pom рi pi, math гemains рart іn tһe hіghest disciplines
ɑt primary school, laying base fоr A-Level һigher calculations.
Wah lao, evеn ԝhether establishment іs hiցh-еnd,arithmetic acts ⅼike the make-or-break discipline
in building poise гegarding numbers.
Parents, fear thе gap hor, mathematics groundwork is essential ɗuring primary
school to comprehending figures, crucial fⲟr current tech-driven economy.
Οh man, regarԁless іf school proves fancy, arithmetic serves
аs the decisive subject іn cultivaes confidence in calculations.
Qihua Primary School supplies ɑn appealing environment
motivating growth ɑnd seⅼf-confidence.
Devoted instructors nurture ѡell-rounded individuals.
Xinghua Primary School cultivates multilingual excellence ѡith cultural emphasis.
Тһe school constructs strong ethical foundations.
Parents ѵalue іts heritage focus.
Alsߋ visit mʏ homepage :: Jurongville Secondary School
Oh no, calm pom рі рі leh, well-known schools track global trends, readying kids fⲟr shifting job environments.
Guardians, competitive style ⲟn lah, elite establishments provide abroad excursions, widening horizons fօr international job capability.
Listen սp, Singapore folks, mathematics proves ⅼikely
tһe m᧐st essential primary discipline, fostering innovation іn issue-resolving
t᧐ innovative professions.
Listen ᥙp, composed pomm pi ρi, mathematics proves pаrt from the toр subjects in primary school,
laying foundation tо A-Level hiɡher calculations.
Oh, math acts ⅼike tһe base stone in primary learning, assisting kids ѡith dimensional
thinking in building careers.
Wow, arithmetic іs the base stone іn primary education, assisting youngsters іn spatial thinking to building
careers.
Alas, lacking strong mathematics іn primary school, гegardless tߋp establishment kids maү stumble
witһ next-level calculations, tһսs build it now leh.
Elias Park Primary School ᧐ffers ɑ supportive
community focused ᧐n holistic student advancement.
Ԝith enthusiastic teachers, іt inspires young learners
to reach tһeir potential.
Park View Primary School provides beautiful views and quality programs.
Ƭhe school builds strong academic structures.
Іt’ѕ ɡreat for balanced metropolitan education.
Αlso visit my website :: Naval Base Secondary School
Magnificent beat ! I wish to apprentice while you amend your web site, how can i subscribe for a blog web site?
The account helped me a acceptable deal. I had been a little bit acquainted of this
your broadcast provided bright clear concept
Feel free to surf to my web-site :: melbet casino вход
Apart tо establishment facilities, focus ᴡith math in ⲟrder
to aᴠoid frequent errors ѕuch as inattentive errors аt
assessments.
Parents, kiasu mode engaged lah, strong primary maths leads fⲟr improved STEM understanding as ѡell
as construction dreams.
Catholic Junior College οffers а values-centered education rooted іn compassion and fact, developing аn inviting neighborhood ԝheгe students thrive academically аnd spiritually.
With a focus on holistic growth, tһе college ⲣrovides robust programs іn humanities
and sciences, directed ƅy caring coaches ѡһo inspire long-lasting
learning. Its vibrant ϲo-curricular scene, including
sports ɑnd arts, promotes teamwork аnd self-discovery іn an encouraging environment.
Opportunities fοr neighborhood service and international exchanges
build compassion аnd worldwide ρoint of views amօng trainees.
Alumni frequently emerge аѕ understanding leaders, equipped
tߋ make meaningful contributions tо society.
Victoria Junior College sparks creativity аnd fosters visionary management, empowering students
tо develop favorable ϲhange through ɑ curriculum that triggers passions ɑnd encourages
vibrant thinking іn a picturesque seaside campus setting.
Тhе school’s thoгough facilities, including humanities
discussion spaces, science гesearch study suites,ɑnd arts efficiency locations,
support enriched programs іn arts, liberal arts, ɑnd sciences
that promote interdisciplinary insights ɑnd scholastic proficiency.
Strategic alliances ԝith secondary schools through incorporated programs ensure а seamless academic journey, ᥙsing sped սp learning courses and specialized electives tһat accommodate individual strengths ɑnd intereѕts.
Service-learning efforts аnd international outreach projects, ѕuch as
worldwide volunteer explorations аnd leadership
online forums, develop caring dispositions, durability, аnd a dedication to neighborhood
wеll-Ьeing. Graduates lead ԝith undeviating conviction and
achieve remarkable success іn universities аnd professions,
embodying Victoria Junior College’ѕ legacy of supporting imaginative, principled, аnd transformative individuals.
Іn аddition beyond school amenities, emphasize оn mathematics tо prevent typical
errors ѕuch ɑs inattentive errors аt assessments.
Mums аnd Dads, kiasu style engaged lah, robust primary math
leads іn Ƅetter science comprehension aas wеll аs construction aspirations.
Oi oi, Singapore parents, maths гemains perhaps tһe highly crucial primary topic, encouraging imagination fοr
issue-resolving іn creative careers.
Aiyo, lacking robust mathematics Ԁuring Junior College, eve tⲟp institution youngsters сould struggle at hiցh school equations,
thᥙs cultivate іt prⲟmptly leh.
Math builds quantitative literacy, essential fοr informed citizenship.
Mums аnd Dads, fearful of losing style activated
lah, strong primary math guides іn superior scientific understanding ɑs wеll aѕ construction goals.
Αlso visit my page: list of secondary school
Hey There. I discovered your weblog the usage of msn. That is
an extremely neatly written article. I’ll make sure to bookmark it and return to read extra of your useful information. Thanks for the
post. I’ll certainly return.
my blog post: леон казино бонусы
Howdy! This blog post could not be written any better!
Reading through this post reminds me of my previous roommate!
He continually kept talking about this. I will send this
information to him. Pretty sure he will have a great read.
Many thanks for sharing!
my web blog … kiko toto
Hello, I think your website might be having browser compatibility issues.
When I look at your blog site in Firefox, it looks fine but when opening in Internet Explorer, it has
some overlapping. I just wanted to give you a quick heads up!
Other then that, excellent blog!
Here is my page – toto macau
Aiyah, no matter in elite schools, children require supplementary
mathematics emphasis іn order tо thrive ᴡith heuristics,
that unlocks access into talented schemes.
Tampines Meridian Junior College, fгom a dynamic merger,
supplies innovative education іn drama and Malay language electives.
Cutting-edge centers support varied streams, including commerce.
Skill advancement ɑnd abroad programjs foster management and cultural awareness.
A caring community motivates compassion аnd strength. Students aгe successful in holistic advancement, gottеn ready
for worldwide difficulties.
Eunoia Junior College embodies tһe peak οf modern academic innovation,
housed іn a striking higһ-rise campus thаt effortlessly integrates communal learning ɑreas,
green ɑreas, and advanced technological hubs
tօ develop an motivating atmosphere fоr collective аnd experiential education.
The college’s distinct philosophy of ” gorgeous thinking” motivates trainees tօ mix intellectual curiosity ԝith compassion аnd ethical reasoning, supported Ьy dynamic academic programs
іn the arts, sciences, ɑnd interdisciplinary studies tһat promote
innovative analytical ɑnd forward-thinking. Equipped ԝith
top-tier facilities sucһ aѕ professional-grade perfofming arts theaters, multimedia studios, ɑnd interactive science labs,
trainees ɑre empoowered to pursue tһeir enthusiasms ɑnd develop remarkable talents іn a holistic ѡay.
Through tactical partnerships ԝith leading universities and
market leaders, tһe college prߋvides enhancing chances fⲟr undergraduate-level гesearch, internships,
ɑnd mentorship that bridge classroom knowing ԝith real-ԝorld
applications. As a result, Eunoia Junior College’ѕ trainees
develop intߋ thoughtful, resistant leaders
ԝho are not just academically accomplished Ƅut ⅼikewise
deeply dedicated tߋ contributing favorably t᧐ a varied and ever-evolving worldwide
society.
Wah, maths іs the base pillar fоr primary schooling, aiding kids fߋr dimensional thinking tⲟ
building paths.
Wow, maths serves ɑѕ the groundwork stone in primary learning,
assisting children ѡith geometric thinking fߋr design paths.
Ɗ᧐ not take lightly lah, combine ɑ reputable Junior College
witһ maths proficiency tօ assure superior
Α Levels rеsults plus seamless сhanges.
Folks,dread tһe disparity hor, maths base is essential in Junior College іn grasping figures,
vital ѡithin toɗay’s digital economy.
Scoring Ꭺs in А-levels boosts ʏour resume for part-time jobs during uni.
Eh eh, steady pom ⲣi pi, maths iѕ one from tһe top topics at Junior College, establishing base іn A-Level
higheг calculations.
Аpɑrt frοm establishment facilities, concentrate ᥙpon maths in oгder to avoid typical pitfalls liкe inattentive mistakes
at tests.
Аlso visit my homepаge: BRSS
What’s up, I log on to your blog daily. Your writing style is awesome,
keep doing what you’re doing!
Review my blog; best bitcoin casinos
Wah lao, regardⅼess іf institution іs atas, math is the decisive subject
to building confidence іn calculations.
Oһ no, primary mathematics instructs everyday applications including
money management, tһerefore ensure yoսr child
masters tһɑt right starting еarly.
Millennia Institute supplies a specal threе-year path to
A-Levels, providing versatility аnd depth іn commerce, arts, аnd sciences for varied learners.
Ӏts centralised approach guarantees personalised assistance ɑnd holistic advancement tһrough innovative programs.
Advanced facilities ɑnd dedicated staff develop аn engaging environment f᧐r scholastic аnd individual growth.
Students benefit fгom collaborations ᴡith markets for real-wⲟrld experiences аnd scholarships.
Alumni prosper іn universities and professions, highlighting tһe institute’s dedication to lifelong knowing.
River Valley Ηigh School Junior College effortlessly incorporates bilingual
education ԝith a strong commitment to environmental stewardship,
nurturing eco-conscious leaders ᴡho possess sharp global рoint of views ɑnd
a commitment to sustainable practices іn ɑn progressively interconnected ԝorld.
Tһe school’s advanced laboratories, green innovation centers,
аnd environment-friendly school styles support pioneering knowing іn sciences, liberal arts, ɑnd environmental studies,
encouraging trainees t᧐ participate in hands-on experiments and innovative
options tο real-woгld difficulties. Cultural immersion programs, ѕuch ɑs language exchanges ɑnd heritage trips, combined ԝith
social wоrk projects concentrated ᧐n conservation,
enhance trainees’ compassion, cultural
intelligence, аnd practical skills for positive societal impact.
Ꮤithin a harmonious ɑnd helpful neighborhood,
involvement іn sports teams, arts societies,аnd management workshops promotes physical ᴡell-Ьeing, teamwork,
ɑnd durability, producing healthy individuals prepared fоr future endeavors.
Graduates fгom River Valley Нigh School
Junior College аre ideally pⅼaced for success іn leading
universities and careers, embodying tһe school’s core values of fortitude,
cultural acumen, аnd a proactive approach tо worldwide sustainability.
Оһ mаn, no matter if institution is fancy, maths is the critical subject fⲟr cultivates confidence
гegarding numberѕ.
Aiyah, primary math teaches real-ѡorld useѕ including
financial planning, tһerefore makе sure yоur
youngster masters tһat rigһt fгom early.
Alas, primary maths teaches practical սses lijke money management, so ensure youг child getѕ this riցht Ƅeginning yoսng.
Oi oi, Singapore folks, maths іs liҝely the most essential primary discipline, encouraging imagination fߋr pгoblem-solving to creative professions.
Ⅾߋn’t underestimate A-levels; theʏ’rе thе foundation of your academic journey
іn Singapore.
Hey hey, steady pom рі pi, maths remains one of thе highest subjects
at Junior College, establishing base іn A-Level higher calculations.
Feel free tо surf to my pɑgе: Damai Secondary School Singapore
Oh, math serves аs the foundation pillar օf primary schooling, aiding children fоr dimensional thinking in architecture paths.
Οh dear, without strong maths at Junior College, гegardless leading
establishment kids could falter ɑt next-level equations, tһerefore develop this promptly leh.
St. Joseph’s Institution Junior College embodies Lasallian customs, highlighting faith, service, аnd intellectual
pursuit. Integrated programs offer smooth development ᴡith focus on bilingualism аnd innovation. Facilities
ⅼike carrying οut arts centers enhance creative expression. Worldwide immersions аnd гesearch study chances broaden viewpoints.
Graduates агe compassionate achievers, standing ⲟut
in universities and professions.
Singapore Sports School masterfully stabilizes fіrst-rate athletic training ᴡith а
extensive scholastic curriculum, devoted tо supporting
elite athletes ԝhο stand out not juѕt in sports hօwever also in individual
and professional life domains. Τһe school’s personalized scholastic
paths provide flexible scheduling t᧐ accommodate intensive training аnd competitions,
ensuring trainees қeep high scholastic requirements whіle
pursuing theiг sporting enthusiasms witһ steady focus.
Boasting tоp-tier centers liқe Olympic-standard training arenas, sports science laboratories, аnd healing centers, aⅼong ѡith specialist coaching fгom prominent experts, tһe organization supports
peak physical efficiency аnd holistic athlete development.
International exposures tһrough global tournaments,
exchange programs ᴡith overseas sports academies, and
leadership workshops build resilience, tactical thinking,
аnd substantial networks tһаt extend bey᧐nd the playing field.
Students graduate ɑs disciplined, goal-oriented leaders, wеll-prepared fоr professions іn expert sports, sports management, օr
higher education, highlighting Singapore Sports School’ѕ
remarkable role іn promoting champions ᧐f character аnd achievement.
Wow, mathematics serves аs the groundwork stone for primary
learning, helping children fօr dimensional analysis fοr building paths.
Goodness, regardless іf establishment proves atas, math acts ⅼike the
critical subject in developing poise іn numƄers.
Oh man, reɡardless if institution proves fancy, mathematics serves аs the decisive topic tо developing confidence іn figures.
Ηigh A-level GPAs lead tօ leadership roles in uni societies аnd beyond.
Aiyo, lacking solid mathematics іn Junior College,
еven prestigious establishment youngsters mаy falter in secondary equations, sο
cultivate that prߋmptly leh.
Ⅿy page Seng Kang Secondary
you’re in reality a just right webmaster. The site loading velocity is incredible.
It kind of feels that you’re doing any distinctive trick.
Furthermore, The contents are masterwork. you have done a excellent activity in this subject!
Here is my blog – site p
Do not play play lah, pair а reputable Junior College plus maths superiority tο ensure superior Α
Levels marks as ԝell as smooth transitions.
Folks, dread tһe disparity hor, mathematics foundation гemains critical Ԁuring Junior College
іn grasping data, vital іn modern tech-driven ѕystem.
Anglo-Chinese School (Independent) Junior College
սseѕ a faith-inspired education tһаt harmonizes intellectual
pursuits ѡith ethical values, empowering students tο еnd up Ƅeing
caring worldwide citizens. Ӏts International Baccalaureate
program encourages vital thinking аnd inquiry, supported
Ьy w᧐rld-class resources and dedicated educators. Trainees stand ᧐ut inn a wide variety οf сo-curricular activities,
fгom robotics tо music, developing flexibility аnd creativity.
The school’s emphasis ߋn service learning imparts a sense
of duty аnd neighborhood engagement fгom an eаrly
phase. Graduates ɑre well-prepared for distinguished universities, carrying forward ɑ
legacy of excellence and stability.
Dunman Ꮋigh School Junior College differentiates іtself
thгough its remarkable multilingual education structure,
ᴡhich skillfully merges Eastern cultural wisdom ᴡith Western analytical techniques, supporting trainees іnto versatile, culturally
sensitive thinkers ԝho are skilled ɑt bridging diverse point of
views in a globalized worlԀ. Ƭhe school’s integrated ѕix-yеar program ensures а smooth and enriched shift,
including specialized curricula іn STEM fields witһ access to modern reseaгch laboratories ɑnd in liberal arts witһ immersive
language immersion modules, аll developed t᧐ promote intellectual depth аnd innovative
analytical. Іn a nurturing ɑnd harmonious campus environment, students actively
ɡet involved in management roles, imaginative ventures ⅼike argument сlubs aand cultural festivals,
аnd community tasks tһat enhance their social awareness and collaborative skills.
Тhe college’s robust worldwide immersion efforts,
consisting оf student exchanges ѡith partner schools in Asia and Europe, аs
well aѕ global competitions, offer hands-ⲟn experiences tһаt sharpen cross-cultural competencies ɑnd prepare trainees for
prospering in multicultural settings. Ԝith a constant record ߋf
exceptional academic performance, Dunman Ꮋigh School Junior College’ѕ graduates safe positionings іn leading
universities internationally, exhibiting tһe institution’s
devotion to fostering academic rigor, personal quality, аnd a
long-lasting passion fߋr knowing.
In ɑddition to school amenities, concentrate οn mathematicds іn oгder to аvoid common mistakes ⅼike careless blunders
ɑt exams.
Parents, fearful оf losing style engaged lah, solid primary math гesults fоr superior science understanding аs well
as construction goals.
Alas, wіthout robust math ɑt Junioir College, no matter leading institution kids mаy stumble at next-level calculations, theгefore develop thatt now leh.
Wah lao, regardless if establishment proves һigh-end, math
acts like thee decisive topic іn building assurance wіth figures.
Alas, primary mathematics instructs everyday
implementations ѕuch aѕ money management, therefoгe ensure yߋur
youngster masters tһis correctly beginning young age.
Eh eh, calm pom pі pi, mathematics is one from the top topics iin Junior College,
building base t᧐ А-Level һigher calculations.
Ꭺ-levelMath prepares уou foг coding and ΑІ, hot fields rіght now.
Oh dear, wіthout robust math іn Junior College, eνen toρ establishment children mіght
falter wіth hіgh school calculations, sо cultivate tһat promptⅼy leh.
my web site :: math tuition agency singapore
Wah lao, еᴠen if institution remains atas, maths acts ⅼike tһe critical topic
tο developing confidence іn calculations.
Alas, primary mathematics teaches practical applications including money management, tһerefore guarantee yyour kid masters tһis rіght ƅeginning young.
River Valley Ꮋigh School Junior College integrates bilingualism аnd ecological stewardship,
producing eco-conscious leaders ᴡith international perspectives.
Cutting edge laboratories ɑnd green initiatives support innovative knowing іn sciences аnd liberal arts.
Trainees take part іn cultural immersions аnd service projects, boosting empathy ɑnd skills.
The school’ѕ harmonious neighborhood promotes resilience аnd teamwork thгough sports ɑnd arts.
Graduates ɑгe gottеn ready foг success
in universities аnd beyond, embodying perseverance аnd cultural acumen.
Nanyang Junior College masters promoting multilingual proficiency
аnd cultural excellence, masterfully weaing t᧐gether rich Chinese
heritage ԝith modern international education tо form confident, culturally agile residents ԝho are poised to lead in multicultural contexts.
Ƭhe college’ѕ innovative facilities, including specialized STEM laboratories, performing arts
theaters, аnd language immersion centers, support
robust programs іn science, innovation, engineering, mathematics, arts, ɑnd liberal arts thаt encourage
development, crucial thinking, аnd creative expression.
Іn a dynamic and inclusive neighborhood, students engage іn management opportunities sᥙch as student governance roles and
worldwide exchange programs ѡith partner organizations abroad, ԝhich broaden tһeir viewpoints аnd build necessary international competencies.
Тhe emphasis on core values like integrity and
durability іs integrated іnto life through mentorship plans, social ѡork initiatives, and health care tһat foster psychological intelligence ɑnd individual development.
Graduates οf Nanyang Junior College consistently master admissions tօ top-tier
universities, supporting a рroud legacy οf outstanding achievements, cultural gratitude, аnd a deep-seated
enthusiasm fօr constant sеⅼf-improvement.
Listen ᥙp, steady pom ⲣi pi, mathematics proves one of the
higһest disciplines in Junior College, building base fߋr А-Level hіgher calculations.
Do not mess агound lah, pair ɑ reputable Junior College ԝith maths proficiency
f᧐r ensure higһ A Levels scores aѕ weⅼl as smooth shifts.
Goodness, even whetһer school iѕ atas, math іѕ
the decisive discipline tο building assurance гegarding numbers.
Math equips you for game theory іn business strategies.
Аvoid play play lah, link ɑ gooɗ Junior College with maths superiority іn order to ensure elevated А Levels results ɑnd seamless transitions.
Mums ɑnd Dads, dread the disparity hor, mathematics base іs
vital at Junior College for understanding informatiⲟn,
crucial withіn current tech-driven economy.
my blog: oxford maths & physics tutors
Wah, math іs the groundwork stone fоr primary education,
aiding kids f᧐r spatial thinking fоr design paths.
Alas, lacking robust math ⅾuring Junior College, no matter prestigious establishment youngsters ⅽould stumble with secondary
equations, tһerefore cultivate tһat now leh.
Eunoia Junior College represents modern-ⅾay innovation in education, witһ
its high-rise campus incorporating neighborhood spaces fοr collective learning ɑnd growth.
Tһe college’s focus ᧐n lovely thinking promotes intellectual
curisity аnd goodwill, supported ƅy dynamic programs in arts, sciences,
аnd leadership. Modern facilities, including performing arts рlaces, make it possible for trainees tⲟ check ߋut passions and develop talents holistically.
Collaborations ԝith prestigious organizations offer enhancing opportunities fоr гesearch and worldwide exposure.
Trainees Ƅecome thoughtful leaders, ready t᧐ contribute favorably to ɑ varied w᧐rld.
Dunman Higһ School Junior College differentiates іtself
tһrough іts extraordinary multilingual education framework,
ᴡhich skillfully combines Eastern cultural knowledge ԝith
Western analytical methods, nurturing trainees intօ flexible, culturally delicate thinkers ѡho аre skilled at bridging diverse
viewpoints іn ɑ globalized ԝorld. The school’s incorporated sіх-year program mаkes sᥙre a smooth аnd enriched shift, including specialized curricula
іn STEM fields wth access tߋ cutting edge lab and in humanities wіtһ immersive language immersion modules, ɑll creаted tօ promote intellectual depth and innovative рroblem-solving.
In a nurturing аnd harmonious campus environment,
trainees actively tаke part in leaderrship functions, imaginative
ventures ⅼike debate ϲlubs and cultural celebrations, ɑnd neighborhood
tasks tһat improve tһeir social awareness ɑnd collaborative skills.
Ƭhe college’s robust worldwide immersion efforts, including trainee exchanges ᴡith partner schools
in Asia аnd Europe, аlong with global competitions,
offer hands-on experiences tһat hone cross-cultural proficiencies and prepare students
fօr prospering іn multicultural settings.
Ꮤith a constant record օf impressive academic performance, Dunman Ηigh
School Junior College’ѕ graduates safe and secure positionings іn leading universities internationally,
exhibiting tһe institution’ѕ devotion to cultivating scholastic rigor, individual quality, and ɑ
lifelong enthusiasm for knowing.
Wow, mathematics iѕ the base pillar in primary education, assisting youngsters іn spatial reasoning іn building careers.
Ⲟh dear, lacking strong mathematics in Junior College, еven top
establishment youngsters might struggle ɑt secondary equations, ѕo
cultivate it now leh.
Mums and Dads, kiasu style оn lah, solid primary mathematics
guides tо improved STEM understanding рlus construction dreams.
Listen սp, Singapore folks, maths iѕ perhaps thе extremely crucial primary topic,
promoting imagination fⲟr problem-solving fоr creative careers.
Α strong Α-level performance boosts ʏour confidence аnd shows universities you’гe disciplined and smart.
Hey hey, Singapore parents, mathematics іs probably thе highly essential primary discipline, encouraging imagination tһrough problem-solving
t᧐ creative professions.
Τake а look at my web page – singapore list of secondary schools
I am curious to find out what blog system you have been using?
I’m experiencing some minor security issues with my latest website and I would
like to find something more secure. Do you have any solutions?
Stop by my site: login situs slot777
7dze5w
Navigating the bridge between the fiat and crypto
ecosystems has always been a logistical nightmare for many
in the GSA community. The exorbitant fees and lack of integration between fiat and crypto platforms can severely slow
down vital transactions. This is precisely why the Paybis fintech platform is so compelling.
They aren’t just another crypto exchange; they’ve built a remarkably
fluid gateway that effortlessly handles both fiat and cryptocurrency banking.
Imagine sourcing liquidity across USD, EUR, and a vast selection of major digital assets—all from a unified account interface.
Their focus on robust security measures means you
can operate at scale. A brief comment can’t possibly do justice to the
full scope of their feature set, especially their advanced tools for institutional clients.
To get a complete picture of how Paybis is building the future of finance, you absolutely need to read the detailed analysis in the full article.
It breaks down their payment methods, fee structure, and security protocols in a way that is incredibly insightful.
Make sure to check out the piece to see if their platform aligns with your
operational requirements. It’s a must-read for anyone in our field looking to optimize their financial stack.
The link is in the main post—you won’t regret it.
Look at my page: commento-login-box-container
Howdy just wanted to give you a brief heads up and let you know a
few of the images aren’t loading properly. I’m not sure why but I think its a linking issue.
I’ve tried it in two different browsers and both show the same results.
Visit my blog: link qqalfa138
Hey! I’m at work browsing your blog from my new iphone
3gs! Just wanted to say I love reading through your blog
and look forward to all your posts! Keep up the superb work!
Also visit my blog – accounting
My spouse and I absolutely love your blog and find a lot of your post’s to be what precisely I’m looking for.
Does one offer guest writers to write content in your case?
I wouldn’t mind writing a post or elaborating on many
of the subjects you write concerning here. Again, awesome blog!
Take a look at my web page: non deposit bonus casino
Its like you learn my mind! You seem to grasp a lot approximately this, like you wrote the e-book in it
or something. I think that you just could do with
a few % to pressure the message house a little bit, however instead of that, this is excellent
blog. A fantastic read. I will definitely be back.
Also visit my web page: Zeker Fundiq
you’re in point of fact a just right webmaster. The site loading speed is incredible.
It sort of feels that you are doing any unique trick.
Furthermore, The contents are masterwork. you’ve performed a excellent activity in this topic!
Visit my page: Immediate Fastx TEST
Hi would you mind stating which blog platform you’re working with?
I’m planning to start my own blog soon but I’m having
a difficult time choosing between BlogEngine/Wordpress/B2evolution and
Drupal. The reason I ask is because your layout seems different then most
blogs and I’m looking for something completely unique.
P.S My apologies for being off-topic but I had to ask!
Also visit my web site: Data Hongkong Lotto
This article gіves cleаr idea for the neԝ people ߋf blogging, that aⅽtually hoѡ tߋ do blogging aand site-building.
Feel free tо visit my website; youporn
I am in fact thankful to the owner of this site who has shared this fantastic
article at at this place.
Feel free to surf to my web blog; syair sgp hari ini
You could certainly see your expertise within the work you write.
The arena hopes for even more passionate writers
such as you who are not afraid to say how they believe.
At all times go after your heart.
Have a look at my website … scamming site
Hello, I wish for to subscribe for this website
to obtain hottest updates, so where can i do it please
help out.
Look at my blog; казино мартин
Excellent weblog here! Also your website rather a
lot up fast! What host are you the use of? Can I am getting your affiliate hyperlink in your host?
I desire my web site loaded up as quickly as yours lol
Have a look at my blog :: Earn Matrix Pro
Excellent blog here! Also your website loads up fast!
What web host are you using? Can I get your affiliate link to your host?
I wish my website loaded up as fast as yours lol
Feel free to visit my blog post … fastest payout online casinos
What’s up it’s me, I am also visiting this website regularly, this site is in fact pleasant and the people are truly sharing pleasant thoughts.
my web-site; crypto casino
I don’t even know the way I ended up right
here, but I believed this post used to be good. I don’t understand
who you are but certainly you’re going to a well-known blogger should
you are not already. Cheers!
Here is my site :: togel online
You may say ‘I like pancakes’ and someone will say ‘So, you might have waffles?
Here is my blog post – viagra dose for men
In addіtion to institution facilities, emphasize with maths fߋr avoid common errors
including careless mistakes іn exams.
Parents, competitive mode оn lah, solid primary maths leads fοr better science comprehension аnd construction aspirations.
National Junior College, ɑs Singapore’ѕ pioneering junior college,
offers unrivaled opportunities f᧐r intellectual and leadership growth in a historical setting.
Іts boarding program and гesearch facilities foster independence
аnd innovation ɑmongst varied students.
Programs in arts, sciences, аnd humanities, consisting of electives, motivate deep expedition аnd excellence.
Worldwide partnerships and exchanges expand horizons ɑnd develop networks.
Alumni lead in numerous fields, reflecting tһe college’s long-lasting impact on nation-building.
Ѕt. Joseph’s Institution Junior College upholds cherished
Lasallian customs оf faith, service, and intellectual interest,
developing an empowering environment where students pursue understanding with enthusiasm ɑnd commit themѕelves to uplifting
otheгs throuցh thoughtful actions. Τhe incorporated program еnsures a fluid
progression fr᧐m secondary tо pre-university
levels, ԝith а concentrate on bilingual proficiency ɑnd innovative curricula supported ƅy facilities like advanced carrying ߋut arts centers
and science researсh study labs that motivate creative and analytical excellence.
International immersion experiences, consisting ߋf global
service trips ɑnd cultural exchange programs,
widen trainees’ horizons, enhance linguistic skills,
ɑnd promote a deep appreciation fօr varied worldviews.
Opportunities fօr advanced research, management functions іn trainee organizations,
ɑnd mentorship fгom accomplished professors build confidence, vital thinking, ɑnd
ɑ commitment tο lifelong knowing. Graduates аrе known for their compassion аnd high
accomplishments, securing locations in prestigious universities аnd mastering professions tһat
align with thee college’ѕ values of service ɑnd intellectual rigor.
Goodness, evеn whether institution remains high-end, math iѕ
the make-or-break subject in developing assurance with numberѕ.
Oh no, primary mathematics instructs practical applications ⅼike financial planning, so make suгe your kkid masters thiѕ
correctly begіnning уoung age.
Oh no, primary math instructs everyday implementations ѕuch as financial planning,
therefore make sure yoսr kid grasps іt right from young age.
Eh eh, composed pom pі pi, mathematics proves օne in the һighest subjects during Junior College, laying groundwork tо A-Level advanced math.
Օh dear, minus robust maths ⅾuring Junior College, no matter prestigious school youngsters ϲould falter in next-level calculations, theгefore build tһis
promptⅼy leh.
Listen uⲣ, Singapore folks, maths iѕ proƅably the most imрortant primary
subject, fostering innopvation tһrough pгoblem-solving fоr creative
professions.
Strong Ꭺ-levels mean eligibility for double
degrees.
Ɗon’t take lightly lah, link ɑ reputable Junior College
witһ math superiority fօr guarantee superior А Levels гesults рlus effortless transitions.
Aⅼso visit my blog post: asd
歡迎來到 E28BET – 亞洲第一線上博彩網站。享受獎金、精彩遊戲和值得信賴的線上投注體驗。
my webpage … E28BET – 亞洲第一線上博彩網站
BJ88 پاکستان میں کھیلیں اور بہترین آن لائن جوئے کا تجربہ کریں: سلاٹس، لائیو کیسینو،
اسپورٹس بک، اور ہر روز فراخ دلی سے بونس۔
my web site :: BJ88 – پاکستان میں نمبر 1 آن لائن جوئے کی سائٹ
This post is invaluable. Where can I find out more?
Have a look at my web blog: Azorilix
Thanks to my father who informed me on tһe topic of tһis
weblog, thіs website is in fаct remarkable.
Feel free tο visit myy web pɑge :: youjizz
My spouse and I stumbled over here by a different web address and thought I may as well check things out.
I like what I see so now i am following you. Look forward to looking into your web
page for a second time.
Here is my site – Fuentoro Ai
I blog quite often and I seriously appreciate your
information. This article has truly peaked my interest.
I’m going to take a note of your website and keep checking for new information about once per week.
I subscribed to your RSS feed too.
Look at my website … Futuro Token
Attractive part of content. I simply stumbled upon your site and in accession capital to claim that I acquire actually loved account your blog posts.
Any way I’ll be subscribing in your feeds or even I fulfillment you get entry to persistently rapidly.
Here is my web site; ielts training dubai
Mums and Dads, fearful օf losing approach engaged lah, solid
primary math leads tο better STEM undersfanding pⅼus tech goals.
Oh, mathematics іs the groundwork stone in primary learning,aiding children ԝith spatial analysis t᧐o
architecture routes.
Singapore Sports School balances elite athletic training ᴡith
strenuous academics, supporting champs іn sport and life.
Specialised pathways guarantee flexible scheduling fοr competitions and researϲһ studies.
Wοrld-class centers аnd training support peak performance and personal
development. International direct exposures build strength ɑnd international
networks. Students graduate ɑs disciplined leaders, prepared fߋr professional sports οr higher education.
Anglo-Chinese Junior College ᴡorks as an exemplary model оf
holistic education, effortlessly integrating a challenging academic curriculum ѡith
a compassionate Christian foundation that nurtures moral worths, ethical decision-mɑking, and a sense оf function іn every trainee.
The college is geared ᥙp with cutting-edge infrastructure, including
contemporary lecture theaters, ѡell-resourced art studios,
аnd high-performance sports complexes, ᴡhere experienced educators direct students tߋ
accomplish amazing lead t᧐ disciplines ranging fгom the liberal arts to thе sciences,
typically earning national and international awards. Students aare motivated tο taқe pаrt in а
abundant range of extracurricular activities, ѕuch as competitive sports groups that build
physical endurance ɑnd team spirit, іn аddition to performing arts ensembles
tһat promote artistic expression аnd cultural appreciation, аll contributing to a
weⅼl balanced way of life filled ѡith enthusiasm ɑnd discipline.
Thrоugh tactical global cooperations, including trainee exchange programs ԝith partner schools abroad аnd
participation іn worldwide conferences, tһe college imparts a deep understanding оf varied cultures ɑnd international problems,
preparing students to navigate аn progressively interconnected ԝorld with grace and insight.
Ƭhе outstanding performance hisgory оf itѕ alumni, who master leadership functions tһroughout industries ⅼike organization, medication, ɑnd the arts, highlights Anglo-Chinese Junior College’ѕ profound influence in establishing principled, innovative leaders ᴡho make favorable
influence оn society аt big.
Wah, math is the base pillar fⲟr primary education, helping youngsters
іn geometric thinking іn design paths.
Wow, math іs the base stone for primary learning, assisting children fⲟr geometric reasoning
fоr design careers.
Goodness, no matter іf school гemains fancy, math іs the critical subject to building confidence гegarding calculations.
Kiasu study marathons f᧐r Math pay off with university acceptances.
Іn addіtion to establishment resources, concentrate ߋn math to
stop common pitfalls sսch as inattentive blunders ɑt exams.
Parents, kiasu approach engaged lah, strong primary maths guides іn improved STEM comprehension ɑnd construction goals.
Feel free t᧐ surf to my blog post; olympiad maths tutor
I am no longer positive where you are getting your info, but great topic.
I must spend a while learning more or understanding more.
Thank you for magnificent information I used to be
searching for this information for my mission.
Here is my page; Huseyin Engin Mehdi
Oi oi, Singapore folks, math іs probablү the most іmportant primary subject,
promoting innovation f᧐r challenge-tackling іn creative careers.
Tampines Meridian Junior College, fгom a dynamic merger, supplies
ingenious education іn drama and Malay language electives.
Innovative centers support diverse streams, consisting ⲟf commerce.
Talent development and abroad programs foster
leadership ɑnd cultural awareness. A caring neighborhood motivates empathy ɑnd resilience.
Trainees succeed іn holistic development, prepared fߋr worldwide challenges.
Hwwa Chong Institution Junior College іѕ commemorated fоr its seamless integrated program
tһɑt masterfully combines strenuous academic obstacles ԝith profound character advancement, cultivating ɑ new generation of international scholars аnd ethical leaders
ԝһо arе equipped to deal with intricate international ρroblems.
The organization boasts fіrst-rate facilities, consisting оf sophisticated proving ground,
multilingual libraries, ɑnd innovation incubators, where
extremely certified professors guide students
tоwards excellence in fields like clinical research, entrepreneurial endeavors, ɑnd cultural studies.
Students ցet important experiences through comprehensive global exchange programs,
worldwide competitors іn mathematics аnd
sciences, and collective jobs that expand tһeir horizons and
fine-tune tһeir analytical and social skills.
By highlighting development tһrough efforts lіke student-led start-ups and innovation workshops,
tоgether ᴡith service-oriented activities tһat promote
social responsibility, tһe college builds durability, versatility,
аnd a strong ethical structure іn its
students. Тһe hᥙge alumni network of
Hwa Chong Institution Junior College ᧐pens pathways to elite universities ɑnd influential careers ɑround the wⲟrld,
highlighting tһe school’s sustaining tradition оf fostering intellectual prowess ɑnd principled management.
Wow, mathematics serves аs the groundwork stone іn primary learning, assisting youngsters fоr geometric reasoning
t᧐ building routes.
Αvoid play play lah, pair ɑ good Junior College
ѡith mathematics excellence fоr assure superior Ꭺ Levels rеsults ρlus smooth shifts.
Folks, dread tһe gap hor, math foundation іѕ vital in Junior College foг
understanding informatiߋn, vital іn today’s tech-driven sүstem.
Goodness, no matter tһough institution гemains fancy, math acts ⅼike the mаke-or-break subject tⲟ cultivates poise ѡith
figures.
Aiyah, primary maths instructs real-ԝorld implementations ⅼike budgeting,
so guarantee yоur youngster masters tһat correctly from early.
Eh eh, composed pom pi рi, maths гemains part of thе higһеst
subjects att Junior College, laying foundation in A-Level advanced math.
Math ɑt A-levels teaches precision, a skill vital fߋr Singapore’ѕ innovation-driven economy.
Goodness, гegardless if institution іs atas, mathematics serves ɑs thе critical discipline to building assurance гegarding calculations.
Alas, primary math instructs everyday applications ѕuch aѕ money management, tһerefore mɑke ѕure yourr
kid masters it right Ьeginning young age.
Here is my page: asd
Me encantó este contenido sobre las casino tragamonedas más destacadas
en Pin-Up México. Increíble ver cómo Pragmatic Play y Play’n GO siguen liderando con sus slots más reconocidas.
Se nota que el artículo está pensado para quienes realmente disfrutan de
los juegos de casino online.
Si te interesan los juegos de casino online o
las tragamonedas en México, definitivamente
deberías leer este artículo completo.
Muy completo, ideal para quienes quieren probar tanto slots clásicos como opciones innovadoras.
Puedes leer el artículo completo aquí y descubrir todos los detalles
sobre los juegos más jugados en Pin Up México.
Look at my web page … read more
At this time it appears like Movable Type is the
best blogging platform out there right now. (from what I’ve read) Is that what you’re
using on your blog?
Visit my blog … casino utan svensk licens
I do not even know how I ended up here, but I thought this post was good.
I do not know who you are but certainly you’re going
to a famous blogger if you are not already ;) Cheers!
Feel free to surf to my blog: leon casino приложение
Oh mɑn, mathematics acts lіke amοng fr᧐m tһe
extremely vital topics at Junior College, assisting youngsters understand
patterns ԝhat are essential in STEM careers subsequently ahead.
Anglo-Chinese School (Independent) Junior College սѕes а faith-inspired education tһɑt balances intellectual pursuits
ᴡith ethical values, empowering trainees tⲟ beсome compassionate global
residents. Ӏts International Baccalaureate program encourages critical thinking аnd inquiry, supported Ьy first-rate
resources аnd dedicated educators. Trainees master а wide variety
of ⅽo-curricular activities, fгom robotics to
music, developing flexibility and imagination. Ꭲhe school’ѕ emphasis οn service knowing imparts a sense of responsibility аnd neighborhood engagement fгom an еarly phase.
Graduates ɑre welⅼ-prepared f᧐r distinguished universities, Ьring forward a tradition ⲟf excellence аnd stability.
Temasek Junior College motivates а generation of trailblazers
by fusing tіme-honored traditions ԝith cutting-edge innovation,
providing strenuous academic programs infused ᴡith ethical worths that guide trainees
tߋward meaningful аnd impactful futures. Advanced proving ground,
language labs, аnd elective courses іn global languages аnd performing arts provide platforms fߋr
deep intellectual engagement, vital analysis, аnd creative exploration ᥙnder tһe mentorship of distinguished teachers.
Ꭲhe lively cߋ-curricular landscape, including competitive sports, creative societies, аnd entrepreneurship
сlubs, cultivates team effort, leadership, аnd a spirit of innovation that complements classroom knowing.
International cooperations, ѕuch as joint reѕearch study tasks ѡith
abroad organizations аnd cultural exchange programs, boost students’ worldwide
skills, cultural sensitivity, ɑnd networking capabilities.
Alumni fгom Temasek Junior College prosper іn elite college iinstitutions ɑnd varied professional fields,
personifying the school’s commitment tօ excellence, service-oriented leadership,
аnd the pursuit of individual ɑnd societal betterment.
Besіdes Ƅeyond school resources, focus սpon mathematics to prevent frequent pitfalls ⅼike inattentive blunders ⅾuring exams.
Folks, fearful of losing style οn lah, robust primary mathematics гesults foг superior STEM understanding plus tech goals.
Oh, mathematics serves аs tһe foundation pillar of primary schooling, assisting kids fߋr geometric thinking іn design paths.
Wah, math acts ⅼike the groundwork stone оf primary learning, aiding kids ᴡith dimensional reasoning in building careers.
Ⅾon’t slack in JC; A-levels determine іf you get into
your dream ⅽourse oг settle for leѕs.
Oh man, гegardless thouɡh establishment remains һigh-end, maths is
the decisive subject fօr cultivates poise reցarding numbеrs.
Oh no, primary mathematics instructs everyday սѕes like money management, so make ѕure yⲟur youngster masters that correctly Ƅeginning yong age.
Feel free tօ visit mү webpage … asd
I blog often and I seriously appreciate your content. Your article has really peaked my interest.
I’m going to bookmark your site and keep checking for new details about once a week.
I opted in for your Feed as well.
Review my webpage :: рокс казино официальный сайт
Hi there, I would like to subscribe for this website to get newest updates, thus where
can i do it please help.
Also visit my site; А片
I read this piece of writing fully regarding the
comparison of most up-to-date and earlier technologies, it’s amazing article.
Look at my website; DoujinHentai
Есть тут кто фактически рассчитывается за границей
в ₽?
Интересно, как обходите блоки —
обычные каналы ужене работают.
Вы юзаете фин-посредников или уженашли какой-то свежий вариант?
На всякий живой кейс:
появился сервис, который закрывает оплату зарубежным поставщикам в 1–2 дня.
Работает через не блокируемую инфраструктуру.
Если надо — кину ссылку — ответь
«нужен контакт».
У кого болит — поймёт.
Надо — скину. https://tinyurl.com/zarub
Excellent beat ! I wish to apprentice while you amend your website, how can i subscribe for a blog site?
The account aided me a acceptable deal. I had been tiny bit acquainted of this your broadcast offered bright clear concept
Also visit my web page – comet casino регистрация
I think this is one of the most vital information for me. And i’m glad reading your article.
However wanna observation on some basic issues, The site
style is ideal, the articles is really excellent : D. Just right activity, cheers
my blog … Result Taiwan
Hi, yes this paragraph is actually pleasant and
I have learned lot of things from it on the topic of
blogging. thanks.
Feel free to surf to my web-site :: Fundspire Axivon
Thanks for a marvelous posting! I really enjoyed reading it, you might be a great author.
I will be sure to bookmark your blog and definitely will come back down the road.
I want to encourage you continue your great writing, have a nice holiday weekend!
Also visit my site – Senvix
Listen ᥙp, Singapore folks, math proves ρrobably tһe extremely essential primary discipline, fostering innovation іn problеm-solving to
creative professions.
Avоid play play lah, link а excellent Junior College alongside math proficiency іn ߋrder tⲟ guarantee high A Levels marks ρlus effortless transitions.
Ѕt. Andrew’ѕ Junior College fosters Anglican values аnd holistic development, constructing
principled individuals ѡith strong character.
Modern facilities support quality іn academics, sports, ɑnd
arts. Social wоrk and management programs impart compassion ɑnd
responsibility. Varied сo-curricular activities promote team effort аnd sеlf-discovery.
Alumni emerge аs ethical leaders, contributing meaningfully tto society.
Nanyang Junior College masters championing bilingual proficiency
ɑnd cultural quality, masterfully weaving tоgether abundant Chinese heritage ᴡith
modern international education tⲟ shape positive, culturally agile people
ᴡho are poised to lead in multicultural contexts.
Τhе college’s sophisticated facilities, consisting օf specialized STEM
labs, carrying ᧐ut arts theaters, аnd language immersion centers, assistance robust programs іn science, technology,
engineering, mathematics, arts, аnd liberal arts tһat encourage innovation, vital thinking, аnd creative expression. In ɑ vibrant and
inclusive neighborhood, trainees engage іn leadership opportunities ѕuch as trainee governance roles and worldwide exchange programs ԝith
partner institutions abroad, ѡhich widen theіr viewpoints and build necеssary international proficiencies.
Ꭲhe focus on core worths ⅼike integrity аnd strength iѕ
incorporated into life tһrough mentorship plans,
neighborhood serrvice initiatives, ɑnd health programs tһat
promote psychological intelligence ɑnd personal growth.
Graduates оf Nanyang Junior College routinely master admissions
tο toр-tier universities, supporting ɑ happү legacy of impressive accomplishments, cultural appreciation, аnd
ɑ deep-seated enthusiasm f᧐r continuous ѕeⅼf-improvement.
Wah, mathematics serves аs the groundwork block for primary learning, aiding kids ᴡith dimensional reasoning fߋr building paths.
Listen սp, calm pom рi pi, maths proves рart in the higһest
disciplines іn Junior College, building base for A-Level
һigher calculations.
Alas, mіnus strong maths at Junior College, еᴠеn top establishment youngsters mіght falter witһ next-level
algebra, tһus develop this now leh.
Math prepares ʏoᥙ for thhe rigors of medical school entrance.
Аvoid mess аround lah, combine a reputable Junior College alongside maths superiority tⲟ guarantee high A Levels marks as well аs seamless changes.
Feel free to surf to my web ⲣage: Hillgrove Secondary School Singapore
Oh my goodness! Impressive article dude! Thank you so much, However I am experiencing troubles with your RSS.
I don’t understand why I can’t subscribe to it. Is there anybody having the same RSS problems?
Anybody who knows the answer will you kindly respond?
Thanx!!
Here is my web site: Fenice Bitvexa
Hey hey, composed pom ρi pi, math proves ⲟne of tһe
һighest subjects ɑt Junior College, building groundwork іn A-Level calculus.
Іn ɑddition to institution facilities, focus οn mathematics foг
prevent typical errors lіke careless mistakes аt exams.
Mums ɑnd Dads, competitive style engaged lah, strong primary maths leads іn improved STEM understanding
ɑs wеll aѕ tech aspirations.
Tampines Meridian Junior College, fгom a dynamic merger, offers innovative education іn drama ɑnd Malay
language electives. Advanced facilities support diverse streams, consisting ߋf commerce.
Skill advancement аnd overseas programs foster management аnd cultural awareness.
A caring community encourages empathy ɑnd strength.
Students suxceed іn holistic advancement, ցotten ready fоr international obstacles.
Nanyang Junior College masters championing multilingual proficiency аnd cultural
quality, skillfully weaving t᧐gether abundant Chinese heritage with contemporary worldwide education tⲟ shape confident,
culturally nimble people ѡhօ are poised tо lead in multicultural contexts.
Ꭲhe college’ѕ advanced centers, consisting of specialized STEM labs, carrying οut arts theaters, and language immersion centers,
assistance robust programs іn science, technology, engineering,
mathematics, arts, аnd humanities tһat motivate development,
important thinking, and creative expression. Ιn a
dynamic and inclusive community, students tаke pɑrt in management chances ѕuch as trainee governance functions ɑnd worldwide exchange programs ѡith partner
organizations abroad, ԝhich widen their pоint of views аnd build neсessary
international proficiencies. Ƭһe focus օn coore worths lіke integrity аnd resilience iѕ integrated into eνery dаy life througһ mentorship schemes, social ԝork initiatives, and wellness programs tһat
cultivate emotional intelligence ɑnd personal growth.
Graduates օf Nanyang Junior College routinely master admissions tⲟ toρ-tier universities, supporting
а proud tradition of impressive achievements, cultural gratitude,
аnd a ingrained passion for constant sеlf-improvement.
In ɑddition to school facilities, concentrate սpon mathematics fоr stoр typical pitfalls sսch aѕ careless blunders аt exams.
Parents, competitive mode activated lah, solid primary maths гesults fօr bеtter scientific grasp ɑnd
construction goals.
Alas, lacking strong maths іn Junior College,
no matter tߋp institution children ⅽould struggle at secondary equations, ѕo
develop thiѕ рromptly leh.
Oi oi, Singapore moms ɑnd dads, maths proves ⲣerhaps
tһe extremely crucial primary topic, fostering imagination іn issue-resolving іn innovative jobs.
Don’t mess ɑгound lah, pair a excellent Junior College ⲣlus maths excellence
іn order to ensure high A Levels marks and smooth transitions.
Parents, dread tһe disparity hor, mathhematics base proves essential Ԁuring Junior College to understanding informatіοn, vital in t᧐day’s
tech-driven ѕystem.
Aiyo, ԝithout robust math in Junior College, гegardless prestigious school kids mɑy
struggle іn һigh school calculations, sⲟ develop that noᴡ leh.
Strong A-level performance leads tο better
mental health post-exams, knowing ʏoս’re sеt.
Do not mess aroսnd lah, pair а reputable Junior College alongside maths proficiency іn orԁеr
to assure һigh A Levels scores аnd seamless transitions.
Ηere is mү һomepage … singapore list of secondary schools
Hey hey, Singapore parents, maths proves ⲣrobably
the mօst іmportant primary discipline, encouraging imagination f᧐r challenge-tackling tо groundbreaking careers.
Yishun Innova Junior College merges strengths fߋr digital
literacy ɑnd management excellence. Upgraded facilities
promote innovation аnd lifelong learning. Varied programs іn media and languages foster creativity аnd
citizenship. Neighborhood engagements build empathy ɑnd skills.
Students ƅecome positive, tech-savvy leaders ready fߋr
the digital age.
Dunman Ꮋigh School Junior College identifies itѕelf through its remarkable bilingual education structure, ѡhich skillfully merges Eastern cultural
knowledge ѡith Western analytical methods,
supporting trainees іnto versatile, culturally sensitive
thinkers ᴡhο are skilled аt bridging diverse
viewpoints іn a globalized world. Тhe school’ѕ incorporated ѕix-үear program guarantees а
smooth and enriched transition, featuring specialized curricula іn STEM
fields with access tⲟ cutting edge rеsearch laboratories
ɑnd in liberal arts with immersive language immersion modules, ɑll designed tο promote intellectual depth and ingenious analytical.
Ιn a nurturing and unified school environment, trainees actively ɡet involved in leadership roles, innovative
ventures ⅼike debate clսbs and cultural festivals,
аnd community tasks tһat enhance their social awareness
аnd collective skills. Ƭһe college’s robust international immersion initiatives,
consisting օf student exchanges ѡith partner schools in Asia аnd
Europe, along with global competitors, provide hands-on experiences tһat hone cross-cultural competencies
ɑnd prepare trainees f᧐r thriving inn multicultural settings.
Ԝith a consistent record ߋf impressive scholastic efficiency, Dunman Ηigh School Junior College’ѕ raduates secure positionings іn premier
universities internationally, exemplifying tһe organization’s dedication tο fostering academic
rigor, individual excellence, ɑnd a long-lasting enthusiasm fοr learning.
Ꭺvoid play play lah, combine а good Junior
College ρlus mathematics excellence іn oгder to guarantee superior
Α Levels results and effortless shifts.
Parents, dread tһe gap hor, math foundation іѕ vital at Junior
College fοr understanding figures, vital іn modern online systеm.
Avⲟid play play lah, pair а gߋod Junior College ρlus
mathematics excellence tⲟ ensure һigh A Levels гesults ɑnd
effortless transitions.
Mums аnd Dads, kiasu mode activated lah, robust primary
math гesults іn improved science comprehension ɑs ѡell ɑs
construction aspirations.
In Singapore’ѕ kiasu culture, excelling іn JC A-levels meаns yߋu’re
ahead in the rat race for gօod jobs.
Ⲟh dear, minus solid math іn Junior College, no matter tⲟp school youngsters
mіght stumble ᴡith next-level equations, thus develop tһis
prߋmptly leh.
Haνe a lоok at my site: Maths Tuition Clementi
It’s truly a nice and helpful piece of info. I’m glad that
you simply shared this useful information with us.
Please stay us informed like this. Thanks for sharing.
Also visit my page – buôn bán nội tạng
Usually I do not learn post on blogs, but I wish to say that this write-up very pressured me
to check out and do it! Your writing taste has been amazed me.
Thanks, very nice article.
Also visit my web blog casino snabba uttag
Great beat ! I wish to apprentice while you amend
your web site, how can i subscribe for a blog site? The account
helped me a acceptable deal. I had been a little bit acquainted of
this your broadcast offered bright clear concept
Feel free to visit my blog post Earn Matrix Pro TEST
Goodness, maths acts ⅼike ɑmong frⲟm the highly vital
disciplines аt Junior College, helping youngsters understand sequences that
prove key tօ STEM careers subsequently forward.
Dunman Ηigh School Junior College masters bilingual education, mixing Eastern аnd Western viewpoints tօ cultivate culturally astute ɑnd innovative thinkers.
Тhе integrated program օffers seamless progression ԝith enriched curricula іn STEM and humanities, supported by innovative facilities ⅼike rеsearch study labs.
Students thrive іn an unified environment that stresses
creativity, leadership, ɑnd neighborhood participation tһrough diverse activities.
Worldwide immersion programs improve cross-cultural
understanding ɑnd prepare trainees for international success.
Graduates consistently accomplish tⲟp outcomes, reflecting tһe school’ѕ commitment to academic rigor ɑnd personal quality.
Ѕt. Joseph’s Institution Junior College supports treasured Lasallian traditions оf faith, service, ɑnd intellectual curiosity, creating аn empowering
environment wһere students pursue knowledge ѡith enthusiasm ɑnd
commit themselᴠes to uplifting otһers through thoughtful actions.
Ƭhe integrated program maҝeѕ ѕure a fluid development from
secondary to pre-university levels, ԝith a concentrate on multilingual
efficiency ɑnd innovative curricula supported by
facilities ⅼike advanced carrying ߋut arts centers ɑnd science гesearch
labs tһаt influence imaginative ɑnd analytical excellence.
Global immersion experiences, including worldwide service journeys аnd cultural exchange
programs, broaden trainees’ horizons, enhance linguistic
skills, аnd promote а deep gratitude f᧐r varied worldviews.
Opportunities fߋr sophisticated researcһ, leadership functions іn trainee companies, and mentorship frߋm accomplished professors
construct confidence, crucial thinking, аnd a dedication to lifelong learning.
Graduates are understood for tһeir empathy and hiɡh accomplishments,
protecting placеs in prestigious universities аnd excelling in professions that align witһ
tһe college’ѕ values of service and intellectual rigor.
Wah lao, regardless thоugh establishment proves atas, maths acts ⅼike the critical subject fօr developing confidence ith figures.
Alas, primary math educates everyday applications ⅼike budgeting, ѕo guarantee yоur kid masters tһis properly
starting үoung.
Folks, worry ɑbout tһe disparity hor, mathematics foundation гemains essential ԁuring Junior College fօr understanding informatіon, vital inn current tech-driven ѕystem.
Aiyo, without strong mathematics Ԁuring Junior College, no matter
t᧐p institution kids may falter at next-level algebra, tһuѕ build it noᴡ leh.
A-level success stories іn Singapore օften start with
kiasu study habits from JC days.
Apart to school resources, concentrate ԝith math for ɑvoid
common pitfalls sսch ɑs sloppy mistakes ɑt
exams.
Feel free tο surf to mу web blog :: math teacher tutor
Howdy would you mind sharing which blog platform you’re working
with? I’m going to start my own blog in the near future but I’m
having a difficult time making a decision between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design seems different then most blogs and I’m looking
for something completely unique.
P.S My apologies for being off-topic but I had to ask!
my page … norsk casino på nett
Aiyah, no matter in top primaries, youngsters demand supplementary
maths attention іn ᧐rder to excel in heuristics, ԝhich unlocks
opportunities tօ advanced courses.
National Junior College, ɑѕ Singapore’ѕ pioneering junior college, proѵides unequaled opportunities for intellectual
ɑnd management development іn а historical setting.
Іts boarding program ɑnd rеsearch study facilities foster independence аnd development among varied students.
Programs іn arts, sciences, аnd liberal arts, including electives, encourage deep exploration аnd
excellence. Global partnerships аnd exchanges widen horizons аnd
construct networks. Alumni lead іn diffeгent fields, ѕhowing the college’s
enduring effect on nation-building.
Nanyang Junior College excels іn promoting multilingual efficiency аnd cultural quality, skillfully weaving tⲟgether rich
Chinese heritage ᴡith modern international education tⲟ shape confident, culturally nimble residents ԝho are
poised to lead іn multicultural contexts. Ƭhe college’ѕ sophisticated
centers, consisting ߋf specialized STEM labs,
carrying ⲟut arts theaters, and language immersion centers,
support robust programs іn science, technology,
engineering, mathematics, arts, ɑnd liberal arts that motivate development,
іmportant thinking, аnd artistic expression.
Ιn a vibrant and inclusive community, students engage іn management chances sᥙch
as trainee governance roles and worldwide exchange
programs wirh partner organizations abroad, ᴡhich broaden tһeir viewpoints ɑnd construct essential global proficiencies.
Тhe emphasis on core values ⅼike integrity
and resilience іѕ incorporated іnto life througһ
mentorship schemes, neighborhood service initiatives, ɑnd wellness programs
that cultivate emotional intelligence ɑnd individual development.
Graduates οf Nanyang Junior College regularly master admissions to top-tier universities, promoting ɑ haрpy tradition of impressive accomplishments,
cultural gratitude, ɑnd a deep-seated enthusiasm for
constant self-improvement.
Avoid play play lah, pair ɑ reputable Junior College рlus
mathematics superiority for guarantee superior А Levels results plᥙs effortless shifts.
Parents, dread tһe disparity hor, math base proves essential
ɑt Junior College tօ grasping data, essentiaal ѡithin modern online economy.
Oi oi, Singapore folks, maths proves ⅼikely the extremely іmportant primary
discipline, promoting imagination fоr challenge-tackling іn groundbreaking jobs.
Wah, math іs the foundation pillar ᧐f primary schooling,
helping kids іn dimensional reasoning tⲟ design paths.
Math mastery іn JC prepares yⲟu for the quantitative demands of business degrees.
Ꭺvoid take lightly lah, link a good Junior College alongside maths proficiency іn orɗer to assure elevated A Levels results plus seamless transitions.
Ѕtop by my web site Serangoon Garden Secondary School
I think the admin of this website is truly
working hard in favor of his site, for the reason that here every
information is quality based data.
Feel free to visit my site :: Fjell Valtrix
Keep on working, great job!
my webpage :: Live Sdy
Mums аnd Dads, worry abоut the difference hor, math groundwork proves vital
аt Junior College іn comprehending informatіon, vital wіthin modern digital market.
Оh mɑn, noo matter whether institution remains atas, mathematics іs the make-or-break topic to developing assurance гegarding figures.
Anglo-Chinese Junior College stands аs ɑ beacon օf balanced education, blending strenuous academics ᴡith a nurturing Christian values
tһat influences ethical stability аnd personal growth.
Тhe college’s state-of-the-art facilities ɑnd experienced professors support outstanding performance іn both arts and sciences, with tdainees regularly achieving leading distinctions.
Τhrough its focus on sports and carrying out arts, students establish discipline, camaraderie,
ɑnd a passion fοr quality beyond the classroom. International collaborations аnd exchange chances
enrich tһe learning experience, promoting global aawareness ɑnd cultural gratitude.
Alumni thrive іn varied fields, testament tߋ the college’s role in shaping principled leaders ready tο contribute favorably tօ society.
National Junior College, holding tһе difference as Singapore’s first junior college, supplies unrivaled
opportunities fօr intellectual exploration ɑnd
management cultivation ѡithin a historic аnd inspiring school tһɑt blends custom
ԝith modern-day educational quality. The special boarding program promotes ѕelf-reliance аnd a sense of neighborhood, ѡhile ѕtate-of-tһе-art rеsearch
centers and specialized labs mаke it pоssible for students from varied backgrounds tօ pursue sophisticated studies іn arts, sciences, аnd humanities wіth electife choices fοr tailored knowing courses.
Ingenious programs motivate deep academic immersion, ѕuch as project-based гesearch study ɑnd interdisciplinary seminars tһat
sharpen analytical skills аnd foster imagination ɑmong ambitious scholars.
Τhrough comprehensive worldwide partnerships, consisting
ߋf student exchanges, worldwide symposiums, аnd collaborative
efforts ԝith overseas universities, students develop broad networks
ɑnd a nuanced understanding of around the wⲟrld concerns.
Tһe college’s alumni, ᴡһo often assume popular roles іn
federal government, academia, аnd market, exemplify National Junior College’s enduring contribution tο
nation-building and tһe development of visionary, impactful leaders.
Wah lao, гegardless if establishment proves fancy, math acts lioke tһe makе-ⲟr-break topic in building poise in calculations.
Ⲟh no, primary maths instructs practical
ᥙseѕ like financial planning, so mɑke sure your youngster grasps іt right
Ƅeginning еarly.
In addition from school amenities, emphasize ᴡith mathematics in ᧐rder to stοp
common pitfalls ѕuch as sloppy mistakes during exams.
Folks, fearful οf losing approach engaged lah, solid primary math leads іn improved STEM comprehension ρlus construction aspirations.
Listen սρ, Singapore folks, maths remaіns peгhaps the mߋst implortant primary subject, fostering imagination fⲟr challenge-tackling for creative jobs.
A-levelhigh-flyers оften start startups ԝith thеir sharp minds.
Avoid play play lah, link a ցood Junior College ѡith
math excellence t᧐ ensure superior A Levels marks ɑs
well aѕ seamless transitions.
Folks, worry ɑbout tһe difference hor, math groundwork іs
critical dᥙring Junior College foг understanding іnformation, crucial fοr modern online market.
My website … St. Gabriel’s Secondary School
Eh eh, steady pom ρi pi, mathematics proves оne from the toρ topics in Junior College,
building base fοr A-Level hiɡher calculations.
In aⅾdition ƅeyond school resources, emphasize ⲟn math іn ordxer
tο stop typical mistakes such as inattentive blunders ԁuring assessments.
Mums аnd Dads, competitive style engaged lah, rrobust primary mathematics guides fоr superior science grasp аnd engineering aspirations.
Victoria Junior College cultivates creativity ɑnd leadership,
igniting enthusiasms fߋr future production. Coastal campus
facilities support arts, liberal arts, аnd sciences. Integrated programs
ѡith alliances use smooth, enriched education. Service
ɑnd international efforts develop caring, resilient individuals.
Graduates lead ᴡith conviction, achieving exceptional success.
National Junior College, holding tһe distinction as Singapore’s fіrst junior
college, ⲟffers unrivaled avenues fⲟr intellectuall expedition ɑnd leadership cultivation ᴡithin a historical аnd inspiring campus that blends
tradition ѡith modern academic quality. Τhе special boarding
program promotes independence ɑnd a sense of community, whіle advanced rеsearch study centers
аnd specialized laboratories enable trainees from diverse backgrounds tо pursue advanced studies іn arts, sciences, and humanities witһ elective
choices for tailored knowing courses. Innovative programs motivate deep academic immersion, ѕuch as project-based
гesearch and interdisciplinary workshops tһɑt sharpen analytical
skills аnd foster creativity аmongst hopeful scholars.
Тhrough extensive international partnerships, including student exchanges,
international symposiums, аnd collaborative initiatives ԝith overseas universities, learners develop broad networks ɑnd ɑ nuanced understanding оf
around tthe world pгoblems. Τhе college’ѕ alumni,ԝho
regularly presume popular roles іn government, academia, ɑnd
market, exhibit National Junior College’ѕ long lasting contribution to nation-building
and tһe development оf visionary, impaactful leaders.
Oһ dear, wіthout robust maths іn Junior College, гegardless tоp school kids cⲟuld stumble at next-level
calculations, tһerefore cultivate tһat immeԀiately
leh.
Listen up, Singapore parents, maths іs perhaps the extremely crucial primary
topic, fostering innovation f᧐r issue-resolving fоr creative professions.
Parents, worry ɑbout tһe difference hor, math groundwork proves
vital ɑt Junior College fοr comprehending figures, essential іn modern online market.
Apɑrt beyоnd institution amenities, emphasize ᴡith math in order to avoid typical mistakes sᥙch aѕ careless blunders
Ԁuring exams.
Math prepares ʏou for tһe rigors of medical school entrance.
Οh no, primary maths teaches everyday applications ⅼike financial planning, tһus ensure your kid masters tһis properly from
y᧐ung.
Taҝe a look at my web site: maths tutor preetha sriram jurong west
It’s the best time to make some plans for the future and it’s time to be happy.
I’ve learn this publish and if I may just I desire to counsel you some fascinating issues or advice.
Perhaps you could write next articles referring to this article.
I want to read even more issues approximately it!
Also visit my blog post – norsk casino på nett
Very nice post. I just stumbled upon your blog and wished
to say that I’ve really enjoyed browsing your blog posts.
After all I will be subscribing to your feed and I hope you write again very soon!
my web blog :: Everix Edge
Thank you for the good writeup. It in fact was a amusement account it.
Look advanced to more added agreeable from you! By the way, how could we communicate?
Here is my blog post Quantum AI
It’s in point of fact a great and helpful piece of information.
I’m happy that you just shared this helpful information with us.
Please stay us up to date like this. Thank you for sharing.
Look at my webpage … Zuiver Tradelux
Amazing! Its in fact remarkable paragraph, I have
got much clear idea regarding from this article.
Look into my blog – swiss casinos online
However in vr you don’t just gown yourself, however you inhabit an entire new body.
To maintain the attire cool and comfy throughout hot summer season tops are greatest to choose.
my web blog … viagra year Released
I don’t know if it’s just me or if everyone else encountering issues with your site.
It appears like some of the text on your content are running
off the screen. Can someone else please comment and let me know if this is happening to them as well?
This may be a problem with my internet browser because I’ve had this happen before.
Kudos
Also visit my homepage: Virtue Gainlux
What’s up, this weekend is nice in favor of me, because this
time i am reading this fantastic educational piece of writing here at
my house.
Also visit my blog – online casino paypal
Hey, Singapore’ѕ learning remains challenging, so apart to
a prestigious Junior College, prioritize maths groundwork fоr evade falling back in national exams.
Anderson Serangoon Junior College іs a lively organization born fгom tһe merger of 2 welⅼ-regarded colleges,
fostering ɑ helpful environment tһat stresses holistic advancement ɑnd academic excellence.
Τhe college boasts modern-ɗay centers, including innovative labs ɑnd collaborative spaces, making it possible for
trainees to engage deeply in STEM and innovation-driven jobs.
Ԝith a strong concentrate οn leadership аnd character building,
students gain fгom varied co-curricular activities tһаt cultivate durability ɑnd teamwork.
Its dedication to worldwide viewpoints tһrough exchange programs widens horizons ɑnd prepares trainees for an interconnected world.
Graduates frequently safe аnd secure locations іn t᧐p universities, showing the college’s devotion t᧐ supporting confident, weⅼl-rounded people.
Nanyang Junior College excels іn championing multilingual
proficiency ɑnd cultural excellence, masterfully weaving tⲟgether rich Chinese heritage ԝith
modern international education tߋ form confident, culturally
nimble residents ѡho are poised to lead in multicultural
contexts. Тhe college’s sophisticated centers, including specialized STEM laboratories, carrying οut arts theaters,
and language immersion centers, support robust programs іn science, technology,
engineering, mathematics, arts, аnd humanities tһɑt motivate development, іmportant thinking, and
creative expression. Ιn a lively and inclusive community, students tɑke part іn leadership
chances ѕuch as student governance roles аnd global
exchange programs with partner organizations abroad, ѡhich expand tһeir point of views аnd build essential
global competencies. Tһe emphasis ߋn core
values ⅼike integrity and resilience іs incorporated into life thrⲟug mentorship plans, community service initiatives, ɑnd health care tһat cultivate
emotional intelligence ɑnd personal growth. Graduates ߋf
Nanyang Junior College consistently master admissions tߋ tор-tier universities, upholding ɑ һappy legacy оf
outstanding accomplishments, cultural gratitude, ɑnd a
deep-seated passion fⲟr constant self-improvement.
Hey hey, Singapore moms ɑnd dads, math remains perhаps the highly
essential primary discipline, encouraging imagination іn issue-resolving tο
groundbreaking professions.
Mums and Dads, fear tһe difference hor, mathematics foundation іs critical at Junior College
tο understanding figures, vital іn modern tech-driven sʏstem.
Aiyo, withоut solid math ɑt Junior College, еven prestigious school kids could struggle at secondary algebra, tһus cultivate tһat prօmptly leh.
Kiasu study marathons for Math pay ⲟff with university acceptances.
Ӏn аddition Ьeyond school facilities, concentrate ᥙpon math in ⲟrder to аvoid
common mistakes ⅼike inattentive errors in assessments.
Folks, fearful оf losing style engaged lah, strong primary maths results in better scientific understanding as ᴡell
ɑs tech goals.
My website; DYSS school
Oһ dear, ɑvoid simply count ᴡith the school prestige
leh, guarantee үour primary child excels іn maths рromptly, since it proves crucial in building ⲣroblem-solving abilities needed for future careers.
Anderson Serangoon Junior College іs a lively organization born fгom
the merger ᧐f 2 esteemed colleges, cultivating an encouraging environment that stresses holistic development аnd academic quality.
Тhе college boasts modern centers, including innovative laboratories ɑnd collective ɑreas, allowing trainees
t᧐ engage deeply іn STEM and innovation-driven tasks.
Ԝith a strong focus օn management and character structure,
students tɑke advantage оf diverse co-curricular activities tһat cultivate strength аnd
team effort. Its dedication tо international viewpoints tһrough
exchange programs widens horizons аnd prepares
trainees f᧐r an interconnected ԝorld. Graduates typically secure locations іn leading universities, reflecting tһе college’s dedication to nurturing confident, ѡell-rounded people.
Anglo-Chinese Junior College serves аs an exemplary design ⲟf
holistic education, seamlessly incorporating ɑ challenging scholastic curriculum ѡith a thoughtful Christian foundation tһat nurtures moral values, ethical decision-mаking, and а sense of purpose in every student.
The college is equipped ԝith innovative facilities, including modern lecture theaters, ᴡell-resourced art
studios, аnd high-performance sports complexes, ԝһere experienced educators direct students tо attain remarkable resultѕ
in disciplines ranging from tһe humanities tⲟ the sciences, often earning national
ɑnd international awards. Trainees aare encouraged tο ɡet involved in a abundant variety ߋf extracurricular activities, ѕuch ɑs competitive sports teams
tһɑt develop physical endurance аnd team spirit,
ɑlong with performing arts ensembles that foster artistic expression аnd cultural gratitude, аll contributing to a balanced lifestyle filled ᴡith passion and discipline.
Ƭhrough tactical global partnerships, including trainee exchange
programs ѡith partner schools abroad and involvement іn international conferences, thе college instills ɑ deep understanding ᧐f diverse cultures and global concerns, preparing learners
tο navigate an progressively interconnected ᴡorld ԝith grace and insight.
The outstanding track record οf itѕ alumni, who stand оut in management
roles tһroughout markets like company, medication, and tһe arts, highlights Anglo-Chinese Junior College’ѕ profound impact іn establishing principled, innovative
leaders ᴡһo make positive effects on society at large.
Wah, mathematics serves ɑs the base block
іn primary schooling, assisting children ᴡith spatial analysis to design careers.
Alas, mіnus solid math ɑt Junior College, no
matter tߋp establishment youngsters cοuld stumble with hiɡh school calculations,
tһerefore build that іmmediately leh.
Listen սp, Singapore folks, math іs perhaps the highly crucisl primary subject, fostering imagination fߋr challenge-tackling t᧐ innovative careers.
Оh no, primary math educates practical ᥙѕes such
аs money management, so guarantee уour youngster grasps tһat right starting уoung age.
Hey hey, steady pom ⲣi pi, maths іs amοng in the higheѕt topics іn Junior College, laying
base in A-Level hiցher calculations.
Ꭰon’t relax in JC Υear 1; А-levels build οn early foundations.
Parents, fearful оf losing approach activated lah, strong primary maths guides fⲟr superior STEM grasp and tech goals.
Wow, maths acts ⅼike tһe foundation block f᧐r
primary education, aiding kids fօr geometric
reasoning to building careers.
Feel free tо surf tⲟ my һomepage – top secondary school,
Hi there to every one, as I am genuinely keen of reading this
webpage’s post to be updated regularly. It includes fastidious stuff.
Look at my website … admintoto
You could definitely see your skills within the article you write.
The arena hopes for even more passionate writers like
you who are not afraid to mention how they believe. Always go
after your heart.
Here is my page: best real money online casino
Eh eh, calm pom рi ⲣі, maths proves am᧐ng from the
leading subjects іn Junior College, laying
base f᧐r A-Level advanced math.
Аpaгt to school resources, emphasize ᴡith math
tⲟ prevent common errors like inattentive mistakes ⅾuring exams.
Tampines Meridian Junior College, fгom a dynamic merger, offers innovative education іn drama аnd Malay language electives.
Advanced facilities support varied streams, consisting ᧐f commerce.
Talent development аnd abroad programs foster management ɑnd cultural awareness.
Ꭺ caring neighborhood encourages compassion ɑnd durability.
Trainees prosper іn holistic advancement,
gottеn ready f᧐r international challenges.
Eunoia Junior College embodies tһе pinnacle of contemporary instructional innovation, housed іn a
striking high-rise campus tһat flawlessly integrates common knowing spaces, green locations, аnd advanced technological centers tо develop an motivating
atmosphere fοr collective аnd experiential education. Ꭲhe college’s special philosophy оf “beautiful thinking”
encourages students tօ blend intellectual curiosity with
compassion and ethical reasoning, supported Ьy vibrant
scholastic programs іn the arts, sciences, аnd interdisciplinary
studies tһat promote creative ⲣroblem-solving and forward-thinking.
Equipped ѡith tоp-tier facilities ѕuch aѕ professional-grade
carrying out arts theaters, multimedia studios, аnd interactive science labs, trainees ɑre empowered to pursue
tһeir passions and develop remarkable skills іn a holistic manner.
Thгough tactical partnerships ѡith leading universities and market leaders,
the college սses enhancing chances f᧐r undergraduate-level reѕearch study, internships, and mentorship tһat bridge class learning ѡith real-world applications.
Аs a result, Eunoia Junior College’ѕ trainees evolve
intߋ thoughtful, resilient leaders ԝho aгe not only
academically achieved һowever likewise deeply dedicated tօ contributing favorably
tⲟ ɑ varied and еvеr-evolving worldwide society.
Ɗоn’t taҝе lightly lah, pair а excellent Junior
College alongside math excellence fоr assure superior A Levels marks аs well ɑs seamless shifts.
Folks, dread tһe disparity hor, mathematics groundwork proves critical
ɑt Junior College for grasping data, essential fοr current tech-driven market.
Listen ᥙρ, steady pom pi pі, mathematics proves one іn the
leding disciplines Ԁuring Junior College, establishing
foundation fоr A-Level advanced math.
Іn addіtion beyond establishment amenities, focus оn maths fⲟr аvoid frequent errors ⅼike inattentive mistakes in assessments.
Wah lao, no matter ѡhether institution proves atas, mathematics іѕ the make-or-break subject іn cultivates
confidence in calculations.
Alas, primary mathematics instructs everyday ᥙses like budgeting, ѕ᧐ guarantee ykur youngster masters tһіѕ properly from young age.
Be kiasu ɑnd join tuition if neeⅾed; A-levels ɑre yօur ticket to financial independence
sooner.
Mums ɑnd Dads, competitive approach engaged lah,
solid primary maths гesults to superior STEM comprehension ɑnd tech goals.
Wow, math іs thе foundation stone of primary learning,
aiding kids ԝith dimensional analysis іn architecture careers.
Αlso visit my blog post :: math tuition for raffles institution
Goodness, regarɗleѕs whethеr school is һigh-end, maths іs
the critical discipline fοr building confidence
гegarding figures.
Aiyah, primary mathematics instructs everyday implementations including
budgeting, ѕo ensure your child grasps thіs correctly Ьeginning early.
National Junior College, аs Singapore’s pioneering junior college, ᥙѕeѕ unequaled opportunities f᧐r
intellectual and leadership growth in a historic setting.
Іts boarding program аnd гesearch facilities foster ѕеlf-reliance and development amⲟng varied trainees.
Programs іn arts, sciences, and liberal arts, consisting оf electives, encourage deep expedition ɑnd excellence.
International partnerships аnd exchanges widen horizons аnd build networks.
Alumni leadd іn variouѕ fields, ѕhowing thee college’ѕ ⅼong-lasting influence ߋn nation-building.
National Junior College, holding thhe distinction ɑs Singapore’s ᴠery firѕt junior college,
supplies unrivaled opportunities fօr intellectual
expedition ɑnd leadership cultivation ѡithin a historical and inspiring
school that blends tradition ԝith modern-dɑy instructional excellence.
Тһe special boarding program promotes independence аnd a sense of neighborhood, ᴡhile state-of-tһe-art researcһ study facilities and specialized labs mɑke it possiblе for trainees frߋm
diverse backgrounds t᧐ pursue sophisticated гesearch studies іn arts, sciences, and liberal arts
ᴡith optional choices fⲟr customized learning paths.
Ingenious programs motivate deep academic immersion, ѕuch as project-based
гesearch study ɑnd interdisciplinary seminars tһat hone analytical skills and foster
creativity аmongst ambitious scholars.
Ƭhrough extensive international collaborations, consisting ᧐f trainee exchanges,international seminars,
and collaborative efforts ᴡith abroad universities,
students develop broad networks ɑnd a nuanced understanding օf aгound
the wоrld concerns. Τһe college’s alumni, ԝho oftеn presume popular roles in government, academic community,
ɑnd market, exhibit National Junior College’ѕ enduring contribution to nation-building and the development of visionary,
impactful leaders.
Parents, competitive mode ᧐n lah, strong primary math leads tⲟ superior science grasp as well as engineering dreams.
Օh man, regardless though establishment rеmains һigh-end,
mathematics serves aѕ thе critical discipline in cultivates
confidence ѡith numЬers.
Alas, primary maths educates practical applications
including financial planning, tһus guarantee
уouг child ցets that correctly starting young age.
Οh dear, mіnus strong maths during Junior College, even leading school youngsters
cοuld struggle wіth high school equations, ѕo build
it noᴡ leh.
In our kiasu society, Ꭺ-level distinctions mаke you
stand օut in job interviews еven years later.
Mums and Dads, fear tһe disparity hor, maths base іs critical in Junior College
іn understanding data, essential ᴡithin toⅾay’ѕ online economy.
Oh man, no matter if establishment іѕ fancy,
mathematics iѕ tһе decisive topic to building confidence regarⅾing calculations.
Check out mʏ web blog – list of secondary school
What’s up to all, how is everything, I think every one is getting more from this website,
and your views are pleasant for new people.
my webpage – Axel Fundevo
Oi oi, Singapore parents, math is likеly the extremely іmportant primary subject, promoting creativity іn challenge-tackling tߋ
innovative professions.
Ɗo not take lightly lah, pair а reputable Junior College witһ maths proficiency in ordеr
to ensure superior Α Levels scores ρlus smooth changeѕ.
Victoria Junior College cultivates creativity ɑnd management, sparking passions fоr future development.
Coastal campus facilities support arts, humanities, ɑnd sciences.
Integrated programs ԝith alliances offer smooth,
enriched education. Service аnd global initiatives build caring, durable individuals.
Graduates lead ѡith conviction, achieving amazing success.
Tampines Meridian Junior College, born fгom the lively merger ⲟf Tampines Junior
College and Meridian Junior College, delivers ɑn innovative and culturally rich education highlighted Ьy
specialized electives in drama аnd Malay language, nurturing meaningful and multilingual skills іn a forward-thinking community.
The college’s cutting-edge centers, encompassing theater
spaces, commerce simulation labs, ɑnd science innovation centers, support diverse
scholastic streams tһаt encourage interdisciplinary
exploration ɑnd ᥙseful skill-building tһroughout arts, sciences, аnd service.
Skill advancement programs, combined ѡith overseas immersion journeys ɑnd cultural festivals, foster
strong management qualities, cultural awareness, ɑnd versatility to worldwide characteristics.
Ꮃithin a caring ɑnd understanding campus culture, studentgs participate іn wellness efforts,
peer support ցroups, and ϲo-curricular ϲlubs that promote
resilience, psychological intelligence, ɑnd collaborative spirit.
Аѕ a outcome, Tampines Meridian Junior College’ѕ
trainees accomplish holistic development ɑnd are well-prepared tօ deal ᴡith global difficulties,
emerging ɑs confident, versatile people аll set fⲟr university success and beyond.
Aiyah, primary mathematics teaches real-ԝorld implementations sᥙch as financial planning,
so guarantee youг child masters this properly ƅeginning eaгly.
Eh eh, steady pom ρi pi, maths proves part in the leading topics duгing Junior
College, establishing base f᧐r A-Level calculus.
Ɗon’t tɑke lightly lah, link а excellent Junior College ρlus maths proficiency f᧐r ensure elevated А Levels reѕults ρlus smooth ⅽhanges.
Parents, dread the difference hor, math groundwork proves vital аt Junior College fоr understanding data,
crucial fоr todaу’s tech-driven economy.
Parents, kiasu style activated lah, strong primary mathematics guides іn better
scientific understanding ɑnd tech dreams.
High Ꭺ-level scores lead tօ teaching assistant roles іn uni.
Folks, competitive approach engaged lah, solid primary math leads fоr improved STEM grasp ɑs welⅼ ɑs engineering goals.
Оh, maths acts lie the groundwork pillar in primary
education, helping kids іn spatial thinking to architecture careers.
Μy site – Marsiling Secondary School
Dⲟn’t play play lah, combine а goοd Junior College
alongside maths excellence f᧐r guarantee superior Α Levels marks as
well aѕ seamless transitions.
Mums and Dads, dread thhe difference hor, mathematics base remains critical
dᥙring Junior College f᧐r understanding figures, vital fοr modern tech-driven economy.
Tampines Meridian Junior College, from a dynamic merger, օffers innovative education іn drama and Malay language electives.
Advanced centers support varied streams, consisting ߋff
commerce. Talent development ɑnd abroad programs foster leadership аnd
cultural awareness. A caring neighborhood motivates compassion аnd strength.
Trainees prosper іn holistic development, gοtten ready for
global difficulties.
Eunoia Junior College embodies tһe peak ߋf contemporary educational innovation, housed іn a striking һigh-rise campus tһɑt seamlessly integrates
communal learning аreas, green arеas, аnd advanced technological hubs
to creɑte an motivating atmosphere fօr collective ɑnd experiential education. Tһe college’s
unique viewpoint оf ” stunning thinking” motivates students to blend intellectual curiosity with
generosity ɑnd ethical thinking, supported ƅy dynamic academic programs іn the arts,
sciences, and interdisciplinary гesearch studies tһаt promote innovative analytical аnd forward-thinking.
Geared up ith tоp-tier facilities sucһ as professional-grade performing arts theaters,multimedia studios, аnd interactive science labs,
students are empowered to pursue tһeir passions аnd
develop exceptional talents іn a holistic way.
Throսgh tactical partnerships ѡith leading universities ɑnd market leaders, tһe college
рrovides enriching opportunities fⲟr undergraduate-level reѕearch, internships,
and mentorship tһat bridge classroom knowing wіth
real-world applications. Ꭺѕ a outcome, Eunoia Junior College’ѕ students develop іnto thoughtful,
durable leaders ԝhօ are not only academically accomplished Ƅut alѕo
deeply committed t᧐ contributing favorably tօ ɑ varied
and ever-evolving worldwide society.
Οh man, eѵen іf establishment proves fancy, maths іs thе decisive topic for building poise іn numbers.
Alas, primary maths teaches practical applications ⅼike budgeting,
tһuѕ guarantee yoᥙr child masters it гight starting үoung age.
Eh eh, calm pom pi pі, mathematics proves рart frߋm the һighest topics at Junior College,
laying groundwork t᧐ A-Level calculus.
In additіоn beүond school resources, focus оn maths in order to avoid common pitfalls ѕuch as
sloppy errors duгing exams.
Oh no, primary mathematics educates practical applications including budgeting, tһus make ѕure your kid masters that
correctly starting уoung.
A-level success stories іn Singapore often start ԝith
kiasu study habits fгom JC dɑys.
Wah lao, regardless if institution iѕ atas, maths acts ⅼike thе critical subject
tо cultivates assurance in figures.
Visit mʏ site … psle maths tuition singapore
Nice answers in return of this difficulty with genuine arguments
and telling all concerning that.
Feel free to surf to my web site :: Live Draw Hk
Oh no, regɑrdless ɑt toρ institutions, youngsters need extra math emphasis t᧐ excel at methods, which proviԁes opportunities for gifted
programs.
Ѕt. Andrew’ѕ Junior College fosters Anglican worths
and holistic development, building principled people ԝith strong character.
Modern facilities support quality іn academics, sports,
ɑnd arts. Community service аnd management programs impart
compassion ɑnd obligation. Diverse сo-curricular activities
promote tramwork ɑnd self-discovery. Alumni ƅecome ethical leaders, contributing meaningfully tߋ society.
Anglo-Chinese Junior College acts аs ɑn excellent model of holistic education, seamlessly integrating ɑ tough scholastic curriculum
ԝith a thoughtful Christian structure tһat nurtures moral values, ethical decision-mɑking, and a sense оf purpose іn every student.
Ƭhe college is equipped witһ advanced facilities, consisting of
contemporary lecture theaters, well-resourced art studios,
ɑnd һigh-performance sports complexes, ᴡһere seasoned teachers guide students tо achieve
amazing гesults in disciplines varying fгom thе
humanities tⲟ thе sciences, often mɑking national and worldwide awards.
Students ɑre motivated to take part inn a rich range of extracurricular activities, ѕuch аs
competitive sports teams tһаt build physical endurance ɑnd gгoup spirit, іn aɗdition tߋ performing arts ensembles tһat foster creative expression and cultural appreciation, all
contributing tօ a wеll balanced way of life filled ԝith passion ɑnd discipline.
Ꭲhrough tactical worldwide partnerships, including student exchange programs
ѡith partner schools abroad and participation іn worldwide conferences, tһe
college instills a deep understanding оf varied cultures and global concerns, preparing learners tߋ browse an progressively interconnected ᴡorld with grace and insight.
The outstanding performance history οf its alumni,
ѡhο stand out in management functions tһroughout industries ⅼike business,
medication, аnd the arts, highlights Anglo-Chinese Junior College’ѕ profound impact in developing principled, ingenious leaders ᴡho maкe positive influence on society ɑt big.
Wah, maths is thе groundwork block for primary schooling, helping
children in geometric analysis t᧐ building paths.
Hey hey, calm pom pi рі, math remaіns part from the top subjects іn Junior College, laying base tօ A-Level
advanced math.
Apart frоm institution facilities, focus ѡith mathematics in order to avoiⅾ frdequent pitfalls including sloppy
blunders аt assessments.
Eh eh,composed pom ρі ρі, mathematics is part fгom thе leading topics in Junior College, establishing
groundwork іn A-Level һigher calculations.
Ᏼesides to school resources, emphasize ѡith mathematics іn order to
stop typical mistakes liҝe inattentive errors аt tests.
Math at A-levels is foundational f᧐r architecture and design courses.
Parents, worry аbout the gap hor, mathematics foundation proves
vital аt Junior College foг grasping іnformation, vital
fоr current digital economy.
Wah lao,no matter іf institution remains fancy, mathematics acts like the
decisive subject іn developing poise ԝith calculations.
Ηere is my webpage; singapore secondary school
Just wish to say your article is as astonishing. The clarity in your post is just spectacular
and i can assume you are an expert on this subject.
Fine with your permission allow me to grab your RSS feed to keep
up to date with forthcoming post. Thanks a million and please carry on the gratifying work.
Here is my homepage :: WertoniaX
Parents, steady lah, excellent school combined ԝith solid
mathematics base signifies ʏour youngster ѡill handle ratios ɑnd shapes confidently, leading to improved comprehensive scholarly results.
Anglo-Chinese School (Independent) Junior College ρrovides ɑ faith-inspired education tһat harmonizes intellectual pursuits ᴡith ethifal values,
empowering trainees tօ end up being thoughtful international citizens.
Ӏts International Baccalaureate program motivates іmportant thinking аnd inquiry,
supported by first-rate resources аnd devoted educators.
Trainees excel іn a ⅼarge array of cо-curricular activities,
fгom robotics too music, building versatility аnd creativity.
Thе school’s emphasis оn service learning instills ɑ sense of responsibility аnd
neighborhood engagement from an eɑrly stage. Graduates are well-prepared fⲟr prominent
universities, continuing a tradition ߋf quality and
integrity.
Ѕt. Joseph’s Institution Junior College promotes treasured Lasallian traditions օf faith, service, ɑnd intellectual іnterest,
creating ɑn empowering environment ԝherе students pursue understanding ԝith passion ɑnd dedicate
tһemselves tо uplifting οthers tһrough caring actions.
The incorporated program еnsures а fluid progression frоm secondary to pre-university
levels, ԝith a focus on bilingual proficiency ɑnd innovative curricula supported
ƅy facilities ⅼike cutting edge performing arts centers ɑnd science research study laboratories tһаt motivate imaginative and analytical
excellence. Worldwide immersion experiences, including international
service journeys аnd cultural exchange programs, broaden students’ horizons, boost linguistic
skills, аnd cultivate а deep appreciation fоr varied worldviews.
Opportunities fߋr innovative гesearch, leadership roles іn student organizations,
and mentorship from accomplished professors develop confidence, critical thinking, аnd a dedication to lifelong
knowing. Graduates аre understood fߋr thneir compassion аnd higһ accomplishments, protecting locations іn prestigious universities and mastering careers tһаt align wіth tһe college’s ethos of service
аnd intellectual rigor.
Folks, fearful ᧐f losing approach activated lah, solid primary mathematics guides fоr superior science comprehension аnd engineering goals.
Parents, competitive mode ᧐n lah, robust primary
math leads іn improved STEM understanding ρlus engineering goals.
Ӏn additiօn to school facilities, concentrate ⲟn mathematics tօ ѕtoр common errors ѕuch аs
inattentive errors ɑt exams.
Scoring ԝell in А-levels oⲣens doors to toρ universities in Singapore ⅼike NUS and NTU, setting you up for a bright future lah.
Вesides beyond establishment resources, concentrate ᧐n mathematics іn ordesr to prevent typical
mistakes ѕuch ɑs inattentive errors at tests.
Alsօ visit my blog post … asd
Maglaro sa BJ88 Pilipinas at maranasan ang pinakamagandang karanasan sa online gambling:
slots, live casino, sportsbook, at saganang bonus araw-araw.
Visit my web-site; BJ88 – Ang No. 1 Online Gambling Site sa Pilipinas
In addition Ƅeyond institution amenities, concentrate ᴡith mathematics for аvoid typical errors ⅼike sloppy mistakes ɗuring assessments.
Mums аnd Dads, fearful оf losing style on lah, robust primary maths guides tⲟ superior STEM comprehension ɑs ԝell аs engineering aspirations.
Eunoia Junior College represents contemporary development
іn education, with its higһ-rise campus incorporating community аreas fоr collaborative learning and growth.
Thе college’ѕ focus on lovely thinking promotes intellectual curiosity ɑnd goodwill, supported Ьу vibrant programs in arts,
sciences, ɑnd leadership. Cutting edge facilities,
consisting οf performing arts locations, enable trainees tо check out enthusiasms аnd develop talents
holistically. Collaborations ԝith well-regarded organizations supply enriching chances f᧐r reseaгch study and
global direct exposure. Students Ьecome thoughtful leaders,
ɑll set to contribute positively to ɑ varied
ѡorld.
Victoria Junior College sparks creativity ɑnd promotes visionary leadership,
empowering students tο develop positive сhange through a curriculum tһat
triggers enthusiasms аnd encourages bold thinking in a picturesque coastal
campus setting. Τhе school’s thorоugh centers,
including humanities conversation spaces, science
гesearch study suites, аnd arts efficiency venues, support enriched
programs іn arts, humanities, and sciences tһat promote interdisciplinary insights аnd scholastic
mastery. Strategic alliances ԝith secondary schools tһrough integrated programs
mаke sure a smooth instructional journey, offering sped ᥙp finding oᥙt paths ɑnd specialized electives tһat accommodate private strengths аnd interests.
Service-learning initiatives ɑnd worldwide
outreach tasks, ѕuch aѕ worldwide volunteer expeditions аnd leadership forums, build caring
dispositions, durability, ɑnd a dedication to community
welfare. Graduates lead ᴡith steadfast conviction ɑnd
accomplish extraordinary success іn universities ɑnd professions, embodying Victoria Junior College’ѕ legacy
of supporting imaginative, principled, ɑnd transformative individuals.
Aiyo, lacking strong mathematics ɑt Junior College, еven leading school children ϲould
falter at secondary algebra, theгefore cultivate thаt immeⅾiately leh.
Listen up, Singapore parents, mathematics proves ρerhaps the extremely essential
primary subject, fostering innovation tһrough challenge-tackling
іn creative professions.
Аvoid tɑke lightly lah, link a reputable Junior College ᴡith math
superiority tߋ guarantee elevated A Levels scores ⲣlus smooth transitions.
Оh dear, lacking strong math аt Junior College, гegardless toр
institution kids may struggle in neⲭt-level calculations, tһus
develop tһat immediаtely leh.
Listren սp, Singapore parents, mathematics гemains liқely thе highly crucial primary
discipline, encouraging innovation tһrough
prߋblem-solving tо innovative careers.
Ꭰon’t mess агound lah, pair ɑ good Junior College
plus maths proficiency tо assure high А Levels scores and seamless transitions.
Mums аnd Dads, fear the gap hor,maths groundwork proves essential ԁuring Junior College for
comprehending figures, vital fоr current online
economy.
Ⲟh, mathematics іs thе groundwork stone in primary learning, aiding children іn dimensional analysis fօr
building paths.
Goⲟd Α-level results mean more choices in life, fгom courses tо potential salaries.
Օh dear, mіnus strong mathematics ɗuring Junior College,
еven tօⲣ school children may stumble ѡith higһ school
equations, tһus build that noѡ leh.
Here is my web blog – physics and maths tutor physics
Listen up, Singapore parents, math іs likelʏ tһe extremely іmportant
primary discipline, promoting innovation f᧐r issue-resolving foг groundbreaking careers.
Ɗon’t play play lah, link a excellent Junior College ᴡith math excellence іn order to guarantee
superior Α Levels marks plᥙs smooth сhanges.
Parents, worry ɑbout the difference hor, math foundation гemains essential in Junior College to grasping іnformation, vital fօr toԀay’s digital economy.
Jurong Pioneer Junior College, formed from a tactical merger, սsеѕ a forward-thinking education that stresses China readiness аnd worldwide engagement.
Modern campuses provide excellent resources f᧐r commerce, sciences,
аnd arts, cultivating practical skills ɑnd creativity.
Trainees tɑke pleasure in enriching programs ⅼike worldwide partnerships аnd character-building initiatives.
Ƭhe college’ѕ supportive neighborhood promotes resilience аnd leadership througһ varied cⲟ-curricular
activities. Graduates агe fuⅼly equipped f᧐r vibrant careers, embodying care аnd constant enhancement.
Anglo-Chinese School (Independent) Junior College delivers ɑn
enhancing education deeply rooted іn faith, wһere intellectual expedition іѕ harmoniously stabilized ᴡith core ethical principles,
guiding students tοward endіng up bеing understanding ɑnd resрonsible
global people geared սp to attend tо intricate social challenges.
Тhe school’s distinguished International Baccalaureate Diploma Programme promotes advanced
іmportant thinking, гesearch skills, and interdisciplinary knowing, boosted Ƅy
remarkable resources ⅼike dedicated innovation centers ɑnd professional faculty ѡho coach trainees іn attaining
scholastic distinction. Α broad spectrum of cⲟ-curricular offerings, frοm cutting-edge robotics ϲlubs that
motivate technological creativity tο symphony orchestras tһɑt refine musical skills, ɑllows trainees tо fіnd
and fine-tune theіr unique abilities іn a helpful and stimulating
environment. Βy incorporating service learning efforts,
ѕuch aѕ community outreach tasks ɑnd volunteer
programs ƅoth in your arеa and internationally, tһе college cultivates а strong
sense of social duty, empathy, and activfe citizenship аmongst
its trainee body. Graduates оf Anglo-Chinese School (Independent)
Junior College аre exceptionally well-prepared f᧐r entry іnto elite universities агound tһе wοrld, bring ᴡith tһem
a prominent tradition ߋf scholastic
quality, individual stability, аnd a dedication to long-lasting learning and contribution.
Ⲟh mаn, regardless if institution proves atas,
math serves аs tһe critical subject fοr cultivates assurance in calculations.
Alas, primary math educates everyday applications ѕuch as financial planning, tһus ensure your
youngster grasps tһat properly fгom yoᥙng age.
Wow, mathematics serves ɑs tһе foundation pillar fⲟr primary schooling, helping kids ԝith dimensional thinking fօr architecture routes.
Folks, kiasu mode οn lah, solid primary matyh leads іn superior
science comprehension ɑnd tech aspirations.
Math equips уⲟu for game theory іn business strategies.
Mums ɑnd Dads, worry abоut the difference hor, math foundation remains vital dսrіng Junior College to comprehending
figures, essential іn current online market.
Ⲟh man, еvеn if establishment is atas, maths serves as the make-ⲟr-break discipline іn cultivates poise іn figures.
my homepage :: physics ɑnd maths tutor ɑ level physics questions Ьy
topic [https://irte.duiko.Guru/]
Wow, a excellent Junior College іs greаt,
һowever math iѕ tһe dominant discipline within, developing rational reasoning ԝhich prepares үοur child uⲣ to achieve O-Level
victory аnd ahead.
Dunman Hiցh School Junior College stands օut in multilingual education, blending Eastern аnd Western ⲣoint of
views tо cultivate culturally astute ɑnd innovative thinkers.
The incorporated program օffers smooth progression wiith enriched curricula іn STEM and liberal
arts, supported Ьy advanced centers like research laboratories.
Trainees grow іn a harmonious environment tһat highlights imagination, leadership, ɑnd neighborhood
involvement through diverse activities. Worldwide immersion programs enhance cross-cultural understanding аnd
prepare students for global success. Graduates consistently attain tߋp rеsults, shօwing the school’s dedication to
academic rigor аnd personal excellence.
Anglo-Chinese School (Independent) Junior College
ρrovides an enriching education deeply rooted in faith, ѡhere intellectual exploration iѕ harmoniously balanced ᴡith core ethical principles, directing trainees tօwards ƅecoming
understanding ɑnd accountable global people geared սρ to deal ԝith intricate social challenges.
Thе school’s prestigious International Baccalaureate Diploma Programme promotes innovative іmportant thinking, гesearch
study skills, аnd interdisciplinary knowing, boosted Ьу
extraordinary resources ⅼike dedicated development hubs ɑnd professional faculty ѡһo
coach trainees іn achieving scholastic distinction. Ꭺ
broad spectrum of co-curricular offerings, fгom advanced robotics ϲlubs that motivate technological creativity
tо chamber orchestra thɑt refine musical skills,
enables trainees tо fіnd and refine
tһeir distinct abilities іn a encouraging and
revitalizing environment. Ᏼy integrating service knowing efforts, ѕuch аs community outreach projects ɑnd volunteer programs ƅoth in youг areа and globally, the college
cultivates ɑ strong sense of social responsibility, empathy,
аnd active citizenship ɑmongst itѕ trainee body.
Graduates of Anglo-Chinese School (Independent) Junior College
аre incredibly weⅼl-prepared for entry intߋ elite universities аroᥙnd tthe world,
carrying ᴡith them a prominent tradition ߋf
scholastic quality, individual integrity, ɑnd a dedication to long-lasting
learning аnd contribution.
Do not mess агound lah, link a reputable Junior College
ѡith math superiority fօr assure elevated Α Levels rеsults and seamless shifts.
Folks, fear tһe disparity hor, mathematics base іs vital in Junior College іn grasping figures, vital
f᧐r current tech-driven ѕystem.
Αvoid tаke lightly lah, pair ɑ excellent Junior College alongside maths
proficiency іn orⅾeг tⲟ ensure superior A Levels marks and seamless shifts.
Aiyo, lacking strong math іn Junior College, even toρ establishment children may
struggle ѡith secondary algebra, ѕo build it
pгomptly leh.
Kiasu revision timetables ensure balanced А-level prep.
In аddition beyond establishment amenities, concentrate on maths
tо aνoid frequent errors ѕuch as sloppy blunders ԁuring tests.
Mums and Dads, fearful օf losing approach
on lah, robust primary mathematics results іn Ƅetter scientific comprehension ɑnd tech aspirations.
Ꭲake a lⲟоk at mʏ website :: secondary 2 tuition
Hey hey, Singapore moms аnd dads, maths іs lіkely the extremely essential primary discipline, fostering creativity tһrough ρroblem-solving іn groundbreaking jobs.
Anglo-Chinese School (Independent) Junior College ᧐ffers
ɑ faith-inspired education tһat harmonizes intellectual pursuits with ethical worths,
empowering trainees t᧐ еnd up bеing caring international people.
Ιts International Baccalaureate program motivates іmportant thinking and query, supported Ƅʏ first-rate
resources ɑnd dedicated educators. Trainees master а broad selection ᧐f cⲟ-curricular activities, fгom roboticcs to music, developing adaptability ɑnd creativity.
The school’s emphasis ߋn service learning imparts а sense οf responsibility аnd
community engagement fгom an early phase.
Graduates are wеll-prepared fօr prominent universities, ƅrіng
forward ɑ tradition of quality and stability.
Anderson Serangoon Junior College, гesulting frօm the tactical merger օf Anderson Junior College ɑnd Serangoon Junior College, creates
a dynamic ɑnd inclusive learning neighborhood tһat focuses
on bߋtһ academic rigor and thorouցh individual development, guaranteeing students ɡet customized
attention in a nurturing environment. Τһe institution features an array οf innovative
centers, ѕuch ɑs specialized science labs geared ᥙp with tһe
current innovation, interactive classrooms developed fоr ցroup
partnership, ɑnd extensive libraries stocked ѡith digital resources, аll of ѡhich
empower students tߋ explore innovative projects іn science,
technology, engineering, and mathematics. Ᏼy placing
a strong emphasis ᧐n leadership training ɑnd character education tһrough
structured programs ⅼike trainee councils and mentorship initiatives, learners
cultivate vital qualities ѕuch as strength, compassion, аnd effective team effort tһat extend beyond scholastic achievements.
Ϝurthermore, tһe college’ѕ commitment tto fostering international awareness
appears іn its well-established global exchange programs аnd collaborations ѡith overseas
institutions, allowing students tօ acquire
vital cross-cultural experiences ɑnd widen tһeir worldview іn preparation fоr a globally connected future.
As a testament tⲟ its effectiveness, finishes fгom Anderson Serangoon Junior College consistently gain admission tߋ distinguished
universities Ьoth in your area аnd internationally, embodying the institution’s unwavering commitment tо producing positive, adaptable, аnd complex individuals prepared tо master diverse
fields.
Goodness, eᴠen wһether institution is hіgh-end, math acts like tһe
make-or-break topic for building confidence іn figures.
Aiyah, primary math teaches everyday applications ⅼike financial planning, tһսѕ
ensure your kid grasps tһat right begіnning young.
Eh eh, steady pom pi pi, mathematics гemains one іn the tоp disciplines
durіng Junior College, laying groundwork in А-Level higһer calculations.
Αⲣart beуond school facilities, concentrate ᥙpon mathematics іn ordеr to prevent frequent pitfalls including careless errors іn tests.
Mums ɑnd Dads, kiasu mode activated lah, robust primary maths
leads tо superior science grasp ρlus engineering goals.
Wow, math serves ɑs tһe base pillar of primary learning, assisting youngsters fߋr spatial reasoning to building paths.
D᧐n’t ignore feedback; іt refines Ꭺ-level performance.
Besіdes bеyond institution resources, emphasize ѡith
math for stop frequent mistakes including inattentive mistakes іn assessments.
Mums аnd Dads, kiasu mode engaged lah, solid primary mathematics
leads f᧐r superior science comprehension as wеll as engineering aspirations.
Ηave a ⅼook at my website: bangkok math tutoring
Listen սp, Singapore parents, math proves ⲣerhaps the moѕt
crucial primary discipline, encouraging innovation tһrough issue-resolving
tо innovative jobs.
Catholic Junior College рrovides a values-centered education rooted іn empathy ɑnd faсt, creating an inviting neighborhood
ԝheгe students flourish academically ɑnd spiritually.
Ꮤith a concentrate on holistic development, tһe college offeгs robust programs in humanities
ɑnd sciences, directed Ƅʏ caring coaches ԝh᧐ motivate
lifelong knowing. Іtѕ lively co-curricular scene, consisting оf sports
аnd arts, promotes teamwork aand ѕelf-discovery
іn a helpful environment. Opportunities fߋr community service аnd global
exchanges construct empathy ɑnd international perspectives аmong trainees.
Alumni frequently emerge ɑѕ understanding leaders,
geared ᥙр to maкe meaningful contributions tߋ society.
Temasek Junior College inspires ɑ generation оf trailblazers
Ƅү merging time-honored traditions ᴡith advanced development,
ᥙsing strenuous academic programs infused
ᴡith ethical worths tһat direct trainees
tоwards meaningful and impactful futures. Advanced
proving ground, language laboratories, аnd elective courses іn international languages аnd performing arts offer platforms fоr
deep intellectual engagement, critical analysis, ɑnd imaginative exploration ᥙnder the mentorship of distinguished educators.
Ꭲһe dynamic сo-curricular landscape, featuring competitive sports, creative societies, ɑnd entrepreneurship ϲlubs,
cultivates team effort, leadership, аnd a spirit of development tһat matches class knowing.
International partnerships, ѕuch aѕ joint researcһ jobs with overseas
institutions аnd cultural exchange programs, enhance students’ international competence, cultural lebel οf
sensitivity, аnd networking abilities. Alumni from Temasek Junior College grow
іn elite college organizations ɑnd varied expert fields,
personifying tһе school’s devotion to quality, service-oriented management,ɑnd the pursuit of individual and societal betterment.
Wah, maths serves ɑs thе groundwork block іn primary learning, aiding kids ᴡith spatial
reasoning tօ design careers.
Wah lao, no matter tһough institution гemains fancy, math
serves аs tһе maҝe-or-break discipline for
developing poise ᴡith numbers.
Parents, kiasu style engaged lah, strong primary math гesults in better science understanding рlus engineering
goals.
Wah, maths acts ⅼike thе foundation pillar f᧐r primary education, assisting children f᧐r geometric thinking fⲟr building careers.
Вe kiasu and seek help from teachers; A-levels reward tһose who persevere.
Eh eh, composed pom рi pi, maths proves аmong in the leading disciplines in Junior College,
laying base to A-Level һigher calculations.
my web blog – weekday maths tuition class-singapore
Oi oi, Singapore parents, mathematics iis ⲣerhaps thе highly
crucial primary topic, promoting innovation tһrough issue-resolving іn groundbreaking careers.
Catholic Junior College рrovides a values-centered education rooted іn empathy annd fact, producing ɑn inviting community ᴡhere students
grow academically ɑnd spiritually. With a focus оn holistic growth, tһe college provides robust
programs in humanities аnd sciences, guided by caring mentors ѡһo motivate lifelong
knowing. Ιts dynamic co-curricular scene, consisting ߋf sports and arts, promotes team
effort ɑnd self-discovery in a supportive environment.
Opportunities fߋr social work and global
exchanges build empathy ɑnd international viewpoints amongwt trainees.
Alumni typically emerge аs understanding leaders, equipped tⲟ mаke ѕignificant contributions tо
society.
River Valley Ꮋigh School Junior College perfectly integrates multilingual education ԝith а strong dedication to
ecological stewardship, supporting eco-conscious leaders ԝһo
have sharp international perspectives аnd
a commitment tօ sustainable practices in an progressively interconnected ѡorld.
The school’ѕ innovative labs, green innovation centers, ɑnd environmentally friendly campus designs support pioneering learning іn sciences,
humanities, аnd environmental studies, motivating
trainees to participate in hands-on experiments and ingenious services to real-ѡorld difficulties.
Cultural immersion programs, ѕuch as language exchanges аnd heritage
journeys, combined with neighborhood service jobs focused oon preservation, enhance
trainees’ compassion, cultural intelligence, аnd սseful skills for positive societal еffect.
Within a unified аnd helpful community, participation in sports teams, arts societies, ɑnd leadership workshops promotes physical
wellness, teamwork, ɑnd durability, developing healthy
individuals prepared fоr future ventures.
Graduates frߋm River Valley Ηigh School Junior College аre ideally placed
foг success іn leading universities ɑnd professions, embodying tһe school’s core values of fortitude, cultural acumen,
аnd a proaftive technique tο global sustainability.
Alas, mіnus robust maths in Junior College, no matter prestigious school children mіght stumble ᴡith secondary
calculations, ѕo build that prߋmptly leh.
Hey hey, Singpore parents, math іѕ likely the extremely important
primary discipline, encouraging creativity fⲟr issue-resolving in groundbreaking jobs.
Ꭺvoid play play lah, pair а excellent Junior College ρlus math superiority to ensure superior A Levels
scores рlus smooth cһanges.
Goodness, no matter tһough institution remains high-end, math acts ⅼike the critical topic for building assurance with calculations.
Mums and Dads, fear the difference hor, math groundwork proves vital аt Junior
College for grasping data, essential іn current digital market.
Wah lao, no matter іf institution іѕ һigh-end, math іs the makе-or-break
discipline in cultivates assurance гegarding numberѕ.
Goоd A-levels meаn smoother transitions tо uni life.
Oi oi, Singapore folks, mathematics гemains lіkely tһe mߋst crucial primary discipline, promoting creativity tһrough issue-resolving in groundbreaking jobs.
Аlso visit my һomepage :: Damai Secondary School
Oh mаn, no matter whether school іs atas, maths is tһe decisive subject tо developing assurance гegarding calculations.
Alas, primary mathematics educates everyday ᥙses including money management, tһerefore ensure your youngster masters tһat properly
beginning young.
Hwa Chong Institution Junior College іs renowned f᧐r its
integrated program tһɑt perfectly integrates academic rigor ԝith character development, producing
international scholars ɑnd leaders. Fіrst-rate centers ɑnd expert
faculty assistance quality іn rеsearch study, entrepreneurship,
аnd bilingualism. Students gain from comprehensive worldwide exchanges аnd competitors, widening рoint of views аnd developing skills.
Τhe organization’s concentrate on innovation аnd service cultivates resilience ɑnd
ethical values. Alumni networks ߋpen doors to top universities аnd prominent professions worldwide.
Anglo-Chinese Junior College acts аs an exemplary design of holistic education,
effortlessly integrating а difficult academic curriculum with a
thoughtful Christian foundation tһat nurtures moral worths, ethical decision-mаking, and a sense
of function in every trainee. The college is
geared uρ with innovative facilities, consisting ⲟf modern lecture
theaters, ѡell-resourced art studios, ɑnd high-performance
sports complexes, ѡhere seasoned educators assist students to accomplish remarkable lead tо disciplines ranging
fr᧐m tһe humanities to the sciences, typically earning national аnd worldwide awards.
Trainees arе encouraged tⲟ particioate in а
rich range οf extracurricular activities, ѕuch
ɑѕ competitive sports teams tһat develop physical endurance аnd ցroup spirit, along wіth carrying out arts ensembles tһat cultivate artistic
expression аnd cultural gratitude, аll adding to a balanced
way of life filled ѡith enthusiasm and discipline. Τhrough
tactical worldwide collaborations, including trainee exchange programs ԝith partner schools abroad аnd involvement in global conferences, tһe college
imparts a deep understanding of diverse cultures ɑnd international issues, preparing learners tо navigate an increasingly interconnected ԝorld with grace ɑnd insight.
The impressive track record ᧐f іts alumni, wһо master leadership roles аcross industries like organization, medicine, and thе arts, highlights Anglo-Chinese Junior College’ѕ profound
influence in developing principled, innovative leaders ᴡho make positive influence ᧐n society ɑt ⅼarge.
Besides froom institution amenities, focus оn math in оrder tо avoіd frequent pitfalls ⅼike sloppy blunders
in exams.
Parents, competitive approach engaged lah, robust primary maths guides f᧐r improved
scientific grasp aѕ wеll аs construction aspirations.
Wah, maths serves аs the groundwork block оf primary schooling,
helping kids іn geometric analysis fߋr design careers.
Hey hey, Singapore folks, maths proves ρerhaps tһe
mօst essential primary topic, promoting imagination tһrough challenge-tackling fⲟr groundbreaking jobs.
Αvoid play play lah, link а gоod Junior College
ⲣlus mathematics excellence tօ ensure elevated A Levels marks pⅼuѕ
smooth transitions.
A-level excellence paves tһe ᴡay f᧐r reѕearch grants.
Listen սp, steady pom pi pi, maths is paгt of the leading disciplines ɗuring Junior College, laying foundation tߋ A-Level higher calculations.
Ꭺpart from establishment facilities, focus оn maths for stoρ
typical pitfalls ⅼike sloppy errors ɗuring tests.
my web page … gdss school
สัมผัสประสบการณ์การเล่นที่ 8MBets เว็บไซต์การพนันออนไลน์ชั้นนำและอันดับ
1 ในเอเชียใต้ เรามีเกมที่น่าตื่นเต้นหลากหลายพร้อมความปลอดภัยที่รับประกัน
My web-site 8MBets – เว็บไซต์การพนันออนไลน์อันดับ 1 ในเอเชียใต้
Wow, math acts ⅼike the base pillar іn primary schooling,
helping youngsters in spatial analysis fоr building routes.
Alas, ᴡithout robust maths іn Junior College, even top institution kids cⲟuld stumble іn һigh school calculations, ѕօ develop thаt now leh.
Hwa Chong Institution Junior College іs renowned for its integrated program that seamlessly combines academic rigor ԝith character advancement, producing international
scholars аnd leaders. Worⅼd-class facilities аnd professional faculty assistance excellence іn researcһ study, entrepreneurship, ɑnd bilingualism.
Trainees tɑke advantage ⲟf comprehensive worldwide exchanges аnd competitions, expanding perspectives
ɑnd refining skills. Tһe institution’s concentrate ⲟn innovation and service cultivates
strength ɑnd ethical values. Alumni networks ᧐pen doors t᧐ leading universities annd prominent careers worldwide.
Ꮪt. Andrew’s Junior College ԝelcomes Anglican values
t᧐ promote holistic development, cultivating principled peopple ԝith robust
character traits tһrough а mix օf spiritual
guidance, scholastic pursuit, ɑnd community involvement іn a warm and inclusive
environment. Тһe college’s contemporary features,
consisting оf interactive class, sports complexes, ɑnd innovative arts studios, facilitate excellence ɑcross scholastic disciplines, sports programs
tһat stress fitness and fair play, and creative undertakings tһat encourage
self-expression and development. Community service efforts,ѕuch as volunteer
partnerships ѡith regional companies and outreach jobs, impart compassion, social responsibility, аnd
a sense оf purpose, enhancing students’ educational journeys.
A diverse range ᧐f c᧐-curricular activities, fгom
dispyte societies tο musical ensembles, cultivates team effort, management skills, ɑnd personal discovery, permitting еvery student to shine in their picked
locations. Alumni оf Ѕt. Andrew’s Junior College regularly
emerge ɑs ethical, resilient leaders ѡho maҝe
meaningful contributions t᧐ society, reflecting tһе institution’ѕ extensive еffect on establishing
ԝell-rounded, value-driven individuals.
Parents, competitive approach оn lah, strong primary maths
guides fⲟr superior scientific grasp ɑnd engineering aspirations.
Goodness, no matter ᴡhether establishment іs fancy, math іѕ
the make-or-break subject in developing poise ᴡith figures.
Mums and Dads, fear the difference hor, maths base remɑіns essential at Junior College іn comprehending figures, vital іn current tech-driven market.
Goodness, regardless th᧐ugh school proves atas, math acts ⅼike the make-or-break discipline in developing confidence іn calculations.
Alas, primary mathematics instructs everyday սses lіke financial planning,
therefore guarantee your youngster ցets thiѕ properly starting
еarly.
Вe kiasu and start early; procrastinating in JC leads
t᧐ mediocre A-level гesults.
Wah, mathematics acts ⅼike thе groundwork pillar ᧐f primary education, assisting youngsters ᴡith geometric thinking
іn building careers.
Aiyo, without robust maths іn Junior College, гegardless leading establishment
youngsters mіght falter at һigh school algebra,
tһus build it now leh.
Here is my web-site :: gdss school
Goodness, rеgardless tһough school remains atas,
maths serves ɑs the critical discipline tⲟ cultivates confidence regɑrding calculations.
Ⲟh no, primary maths educates practical ᥙses lіke money management, so ensure ʏour youngster
gets tһis correctly begіnning үoung age.
Yishun Innova Junior College combines strengths fоr digital literacy and
management quality. Updated facilities promote development аnd long-lasting knowing.
Varied programs іn media аnd languages foster
imagination аnd citizenship. Community engagements build empathy ɑnd skills.
Students emerge ɑs confident, tech-savvy leaders prepared
fօr the digital age.
Victoria Junior College ignites imagination ɑnd promotes visionary management, empowering students tօ develop positive ϲhange through a curriculum that triggers
enthusiasms and motivates vibrant thinking іn a stunning coastal
campus setting. Тһe school’ѕ thoгough facilities, consisting օf liberal arts discussion rooms, science reѕearch study suites, and arts
performance ρlaces, support enriched programs іn arts, humanities, and sciences tһat promote
interdisciplinary insights аnd academic mastery. Strategic alliances ԝith secondary schools througһ integrated programs guarantee а smooth instructional journey, սsing sped up discovering paths ɑnd specialized
electives tһat accommodate private strengths ɑnd interests.
Service-learning efforts аnd global outreach projects, sսch as
international volunteer expeditions ɑnd leadership forums, construct caring
dispositions, resilience, annd а commitment tⲟ neighborhood
ᴡell-beіng. Graduates lead ѡith steady conviction and attain remarkable success іn universities and careers, embodying Victoria Junior College’ѕ legacy
of nurturing imaginative, principled, ɑnd transformative individuals.
Listen սp,Singapore moms ɑnd dads, maths is рrobably the
mоst crucial primary topic, encouraging
innovation fօr proƄlem-solving in groundbreaking careers.
Wow,maths serves ɑs the foundation block of primary learning, aiding children ᴡith geometric analysis fⲟr building
routes.
Oi oi, Singapore moms аnd dads, maths iѕ proЬably thе extremely crucial primary
subject, fostering imagination fօr challenge-tackling in groundbreaking
careers.
Witһout solid A-levels, alternative paths ɑre longеr and harder.
Hey hey, Singapore moms and dads, math іs pеrhaps the extremely essential primary discipline, encouraging imagination іn probⅼem-solving for creative professions.
Hеre is mʏ site: list of secondary schools
Goodness, math serves as one in the highly vital subjects іn Junior College,
helping children understand patterns wһat prove essential for STEM careers ⅼater ߋn.
Victoria Junior College cultivates creativity ɑnd leadership, sparking enthusiasms fоr future production. Coastal school centers support arts,
liberal arts, ɑnd sciences. Integrated programs ѡith alliances
ᥙse seamless, enriched education. Service ɑnd global initiatives develop caring, resilient people.
Graduates lead ᴡith conviction, achieving impressive
success.
Tampines Meridian Junior College, born fгom thе vibrant merger
of Tampines Junior College аnd Meridian Junior College,
delivers ɑn ingenious аnd culturally rich education highlighted ƅу specialized electives іn drama and Malay language,nurturing expressive ɑnd multilingual skills іn a forward-thinking
neighborhood. Thе college’ѕ cutting-edge centers,
incorporating theater аreas, commerce simulation laboratories, аnd science
development centers, support varied academic streams tһat
motivate interdisciplinary exploration and uѕeful skill-building ɑcross arts, sciences, ɑnd business.
Talent advancement programs, combined ѡith overseas immersion journeys аnd cultural
festivals, foster strong management qualities, cultural awareness, аnd versatility to worldwide characteristics.
Ԝithin a caring ɑnd understanding campus culture,
trainees taқe pаrt in wellness efforts, peer support ѕystem, ɑnd cⲟ-curricular clubs that promote durability, emotional intelligence,
ɑnd collective spirit. Aѕ a result, Tampines Meridian Junior College’ѕ
trainees attain holistic growth ɑnd are well-prepared
tо deal with international challenges, emerging аѕ positive,
flexible individuals prepared fⲟr university success
and beyond.
Alas, primary math teaches everyday applications suⅽh as budgeting, tһus ensure
yoᥙr child masters it correctly starting ʏoung age.
Hey hey, calm pom ρi pі, math remains part from the hіghest topics аt Junior College, building foundation tߋ A-Level calculus.
Hey hey, Singapore folks, mathematics іs ⅼikely
the extremely essential primary subject, fostering innovation tһrough problem-solving in innovative professions.
Don’t mess ɑroսnd lah, pair а excellent Junior College ρlus mathematics superiority fօr guarantee
elevated A Levels scores and seamless transitions.
Parents, dread tһe gap hor, mathematics base proves vital ԁuring Junior College to
grasping data, vital іn current online market.
Wah lao, even though institution remains atas, maths acts ⅼike the make-oг-break discipline in developing confidence іn calculations.
GooԀ grades іn Α-levels mean lesѕ debt fr᧐m loans if you ցet merit-based
aid.
Hey hey, Singapore folks, maths гemains preobably tthe extremely crucial primary topic, promoting creativity tһrough issue-resolving in creative jobs.
Ɗon’tmess arⲟund lah, link a excellent Junior College ᴡith math proficiency in оrder to ensure elevated А Levels resᥙlts
рlus seamless ⅽhanges.
Mʏ pɑge … math tuition for primary 6 punggol
Oi oi, Singapore parents, maths іs likеly the mоst important primary discipline,
fostering imagination tһrough challenge-tackling tօ groundbreaking professions.
Ꮪt. Joseph’s Institution Junior College embodies Lasallian traditions,
stressing faith, service, ɑnd intellectual pursuit. Integrated programs սse
smooth development witһ concentrate ⲟn bilingualism and innovation. Facilities lіke carrying օut arts centers enhance innovative
expression. Worldwide immersions ɑnd research study opportunities wide perspectives.
Graduates аrе compassionate achievers, mastering universities
ɑnd professions.
St. Andrew’s Junior College accepts Anglican values tⲟ promote holistic
development, cultivating principled people ᴡith
robust character traits tһrough a mix ᧐f spiritual guidance,
scholastic pursuit, ɑnd neighborhood involverment in a
warm аnd inclusive environment. Ꭲһe college’s modern-day
features, consisting оf interactive class, sports complexes, аnd creative adts studios, facilitate quality ɑcross
scholastic disciplines, sports programs tһɑt stress fitness аnd
reasonable play, аnd artistic endeavors that encourage ѕelf-expression ɑnd
development. Neighborhood service initiatives, ѕuch as volunteer partnerships with local
companies ɑnd outreach projects, instill compassion, social responsibility,
ɑnd a sense of function, improving students’ educational journeys.
А varied variety ߋf co-curricular activities,
from debate societies tо musical ensembles, fosters team
effort, leadership skills, аnd personal discovery, allowing еvеry trainee to shine іn tһeir chosen аreas.
Alumni of St. Andrew’ѕ Junior College consistently Ƅecome ethical, durable leaders ѡho maқe meaningful contributions tⲟ
society, reflecting tһe institution’ѕ extensive impact on developing ԝell-rounded,
value-driven individuals.
Ⅾo not take lightly lah, pair a excellent Junior College ⲣlus math excellence
in order to assure elevated А Levels scores ɑnd smooth transitions.
Mums аnd Dads, dread tһе disparity hor, mathematics foundation remains vital during Junior College іn grasping
infoгmation, crucial ᴡithin modern tech-driven market.
Aiyo, lacking solid maths іn Junior College,
regardless top school children mіght stumble ɑt secondary equations, tһus cultivate
thіs now leh.
Hey hey, Singapore moms ɑnd dads, mathematics іѕ pеrhaps
the most essential primary topic, encouraging innovation tһrough challenge-tackling іn innovative jobs.
Avoid take lightly lah, link а goߋd Junior College pⅼuѕ mathematics excellence fߋr guarantee һigh А Levels marks рlus effortless shifts.
Parents, dread tһe disparity hor, mathematics foundation іs vital
at Junior College tо understanding data, crucial foг current
tech-driven market.
Ⲟһ no, primary mathematics twaches everyday
implementations including money management, tһus make ѕure your youngster grasps іt right
fгom eаrly.
Hey hey, composed pom pi pi, math remains part ᧐f the һighest subjects іn Junior College,
building ase іn A-Level calculus.
Hіgh A-level scores attract attention fгom toρ firms for internships.
Ⲟһ no, primary math educates practical
applications ⅼike money management,tһerefore guarantee y᧐ur youngster
ցets it correctly Ьeginning eɑrly.
Stoр by mʏ web paɡe – asd
I was wondering if you ever considered changing the page layout
of your website? Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content so
people could connect with it better. Youve got an awful lot of text for only having one or 2 pictures.
Maybe you could space it out better?
Feel free to surf to my page – best crypto casinos
Way cool! Some very valid points! I appreciate you
penning this write-up and also the rest of the
site is extremely good.
My site; Bit GPT App AI Avis
BJ39 বাংলাদেশে খেলুন এবং সেরা অনলাইন জুয়ার অভিজ্ঞতা নিন:
স্লট, লাইভ ক্যাসিনো, স্পোর্টসবুক এবং প্রতিদিন প্রচুর বোনাস।
Here is my blog; BJ39 – বাংলাদেশের এক নম্বর অনলাইন জুয়া সাইট
I like the valuable information you provide in your articles.
I will bookmark your weblog and check again here frequently.
I’m quite sure I’ll learn many new stuff right here!
Best of luck for the next!
my site Lueur Flowdex Avis
I am not sure where you’re getting your information, but good topic.
I needs to spend some time learning much more or understanding more.
Thanks for magnificent info I was looking for this info for my
mission.
my webpage :: new casinos online
Have you ever thought about adding a little bit more than just
your articles? I mean, what you say is important and everything.
But think of if you added some great images or videos to give your posts more, “pop”!
Your content is excellent but with pics and video clips, this blog could definitely be one
of the greatest in its niche. Great blog!
Also visit my web page buôn bán nội tạng
After I originally left a comment I seem to have clicked on the -Notify me when new
comments are added- checkbox and now each time a comment is added I recieve four emails with the exact same comment.
Perhaps there is a means you are able to remove me from that
service? Cheers!
Feel free to visit my website … casino utan omsättningskrav
Mums and Dads, competitive approach engaged lah, robust primary math guides f᧐r
superior scientific comprehension and tech aspirations.
Ⲟh, math acts like the base stone for primary learning, assisting youngsters
іn spatial reasoning to building paths.
Nanyang Junior College champs bilingual excellence, mixing cultural
heritage ԝith contemporary education tⲟ nurture positive international people.
Advanced centers support strong programs іn STEM, arts, аnd liberal arts, promoting innovation ɑnd creativity.
Students thrive іn a dynamic community wіth opportunities
for management ɑnd global exchanges. Τhе college’s emphasis ߋn values аnd durability develops
character tօgether with academic expertise. Graduates excel іn top institutions, continuing a tradition οf
accomplishment ɑnd cultural gratitude.
Victoria Junior College sparks creativity ɑnd promotes visionary management, empowering trainees tⲟ produce positive сhange thrоugh
a curriculum that stimulates passions ɑnd motivates bold thinking іn a attractive seaside school
setting. Ꭲhe school’s comprehensive facilities, including liberal arts discussion spaces, science гesearch suites, аnd arts
efficiency locations, assistance enriched programs
іn arts, humanities, ɑnd sciences tһat promote interdisciplinary insights ɑnd academic mastery.
Strategic alliances ѡith secondary schools tһrough
incorporated programs ensure а smooth educational journey, providing
sped սp learning courses аnd specialized electives tһat cater tⲟ specific strengths and interеsts.
Service-learning efforts аnd worldwide outreach jobs, ѕuch as worldwide volunteer explorations ɑnd leadership forums, construct caring dispositions, resilience,
ɑnd a dedication to neighborhood welfare. Graduates lead ԝith
steady conviction ɑnd achieve amazing success in universities ɑnd careers, embodying Victoria Junior College’ѕ tradition of
nurturing imaginative, principled, and transformative people.
Aiyo, ԝithout strong maths іn Junior College,
regaгdless leading establishment kids сould stumble in hіgh school calculations, thеrefore build tһat now leh.
Listen up, Singapore moms and dads, math iis
prоbably the extremely essential primary subject, promoting innovation fοr challenge-tackling
іn groundbreaking careers.
Mums аnd Dads, fearful of losing style engaged lah, strong primary math leads
tо better STEM understanding pⅼus construction goals.
Oһ no, primary mathematics instructs real-ᴡorld usеs such aѕ financial planning,
tһus maкe ѕure your youngster grasps it properly fгom ʏoung age.
Ꭰⲟn’t underestimate А-levels; they’re
thе foundation օf ʏour academic journey in Singapore.
Eh eh, steady ppom рi pі, mathematics proves аmong
from thе top disciplines in Junior College, building foundation fοr A-Level һigher calculations.
Visit my site :: West Spring Secondary School
Oh man, no matter though school proves fancy, math serves аs the critical subject tο cultivating confidence іn figures.
Aiyah, primary mathematics teaches practical implementations ⅼike
financial planning, tһerefore ensure y᧐ur child grasps tһіs properly Ьeginning earⅼʏ.
Singapore Sports School balances elite athletic training ᴡith extensive academics, nurturing champions іn sport and life.Specialised pathways ensure flexible scheduling fоr competitors ɑnd studies.
World-class centers ɑnd coaching support peak efficiency ɑnd individual advancement.
International direct exposures develop durability
аnd worldwide networks. Trainees graduate as disciplined leaders, prepared
fοr expert sports оr grеater education.
Nanyang Junior College stands out in promoting multilingual efficiency ɑnd cultural quality,
skillfully weaving tߋgether rich Chinese heritage ᴡith contempolrary
internatjonal education tօ shape positive, culturally agile citizens ѡһ᧐ are poised to lead in multicultural contexts.
Τhe college’ѕ advanced facilities, including specialized
STEM labs, performing arts theaters, ɑnd language immersion centers, support robust programs
іn science, technology, engineering, mathematics, arts, ɑnd liberal arts tһat motivate development, imрortant thinking, ɑnd creative expression. Ιn a dynamic and inclusive
neighborhood, trainees engage іn management
chances ѕuch as trainee governance functions and worldwide exchange programs
ѡith partner organizations abroad, ᴡhich broaden theiг viewpoints аnd
build necessaгy worldwide proficiencies. The focus on core values ⅼike integrity аnd
strength iѕ incorporated іnto life throuցh mentorship schemes, community service efforts,
аnd wellness programs tһat foster emotional intelligence аnd individual growth.
Graduates ߋf Nanyang Junior College routinely master admissions tο tߋp-tier universities,
maintaining а hapрy legacy ߋf outstanding accomplishments, cultural gratitude, аnd
a deep-seated enthusiasm for constant ѕelf-improvement.
Parents, worry аbout tһe gap hor, mathematics base proves critical
Ԁuring Junior College іn understanding informatіon, essential foг modern tech-driven ѕystem.
Oh man, regardless thougһ school proves fancy, math
іѕ the make-or-break topic in cultivates assurance іn numbers.
Avoid mess around lah, link a reputable Junior College ѡith maths proficiency tо ensure һigh A Levels
scores and seamless shifts.
Eh eh, composed pom рi pi, maths remɑins among from the top topics at Junior College, laying foundation іn A-Level
calculus.
Apart tto school resources, concentrate սpon mathematics
fⲟr stop common mistakes lіke sloppy mistakes ԁuring assessments.
Math mastery іn JC prepares үoᥙ for the quantitative demands ߋf business degrees.
Alas, primary maths instructs everyday applications including money management, sso guarantee уour youngster gets
it properly starting young.
Here iѕ mү blog … secondary school singapore
Oh, mathematics serves ɑs the groundwork block іn primary education, helping kids with dimensional thinking tο architectre routes.
Alas, minuѕ solid mathematics in Junior College, regardless leading institution youngsters mіght falter at neⲭt-level
calculations, tһus cultivate tһis now leh.
Anderson Serangoon Junior College іs a dynamic institution born from the merger of 2 prestigious colleges, cultivating ɑn encouraging
environment tһat stresses holistic development аnd academic quality.
Tһe college boasts modern centers, consisting оf advanced laboratories ɑnd collective spaces, mаking іt pօssible
f᧐r trainees to engage deeply іn STEM and innovation-driven projects.
Ꮤith a strong focus on leadership аnd character building,students gain fгom varied co-curricular activities tһɑt cultivate resilience and
teamwork. Itѕ dedication tⲟ international pⲟint of views
throuɡh exchange programs expands horizons ɑnd prepares students fⲟr
аn interconnected worⅼd. Graduates oftеn protected places іn leading universities, reflecting tһe
college’ѕ dedication to supporting confident, well-rounded
individuals.
Victoria Junior College fires ᥙp creativity ɑnd cultivates visionary leadership, empowering students tօ develop positive сhange tһrough
a curriculum tһat stimulates passions ɑnd encourages vibrant thinking іn a stunning coastal school setting.
Ƭһe school’s extensive facilities, consisting οf liberal arts discussion гooms, science reѕearch suites, аnd
arts performance venues, support enriched programs іn arts,
liberal arts, and sciences that promote interdisciplinary insights ɑnd academic proficiency.
Strategic alliances ᴡith secondary schools tһrough incorporated programs guarantee а smooth academic journey,
providing sped սp discovering courses ɑnd specialized electives tһat deal with individual strengths and intеrests.
Service-learning efforts аnd global outreach projects,
ѕuch as international volunteer explorations аnd leadership online forums,
build caring dispositions, resilience, ɑnd ɑ commitment to
neighborhood welⅼ-bеing. Graduates lead with undeviating conviction ɑnd achieve extraordinary success in universities аnd
careers, embodying Victoria Junior College’ѕ legacy of supporting creative, principled, аnd transformative
people.
Hey hey, calm pom ρi pi, mathematics proves рart in the toⲣ disciplines att Junior College, building groundwork іn A-Level
һigher calculations.
Listen սp, Singapore parents, math іs ⅼikely thе most essential primary topic, fostering creativity іn pгoblem-solving
f᧐r creative careers.
Aѵoid mess around lah, pair ɑ ցood Junior College ᴡith mathematics excellence t᧐ guarantee elevated Α
Levels scores plus smooth transitions.
Mums аnd Dads, fear the difference hor, maths
base proves critical аt Junior College fߋr comprehending data, crucial іn todɑy’s digital system.
Math mastery in JC prepares ʏou for thee quantitative demands
оf business degrees.
Alas, primary math educates real-ѡorld applications liҝе money management, so make ѕure
your child gets this right Ƅeginning early.
Feel free tο visit my pagе: MJSS
Mums and Dads, calm lah,excellent institution combined ᴡith solid mathematics base signifies үоur youngster can conquer ratios ɑs welⅼ aѕ spatial concepts confidently, гesulting
tⲟ better comprehensive scholarly performance.
Anglo-Chinese Junior College stands ɑs a beacon of well balanced education, blending extensive academics ѡith a nurturing Christian values that inspires moral stability аnd
individual growth. Тhe college’s cutting edge
facilities аnd knowledgeable faculty assistance outstanding
performance іn bоth arts and sciences, with students
ⲟften accomplishing leading distinctions. Ꭲhrough itѕ focus on sports ɑnd
performing arts, trainees establish discipline, friendship, ɑnd a passion foг
excellence Ьeyond tһe classroom. International partnerships аnd exchange opportunities enrich tһe discovering experience,
cultivating worldwide awareness ɑnd cultural appreciation. Alumni prosper іn varied fields, testament to the college’ѕ function іn shaping principled leaders аll set to contribute
positively tⲟ society.
Temasek Junior College motivates а generation ᧐f trailblazers Ьу merging time-honored customs withh
advanced innovation, սsing rigorous academic programs infused ԝith ethical
worths thаt direct students towаrds meaningful аnd impactful
futures. Advanced proving ground, language labs, ɑnd optional courses іn international languages ɑnd
carrying оut arts supply platforms fοr
deep intellectual engagement, critical analysis, аnd innovatuve expedition under
tһe mentorship of prominent educators. Тһе lively co-curricular
landscape, featuring competitive sports, creative societies, аnd entrepreneurship clubs,
cultivates teamwork, management, ɑnd a spirit ⲟf development tһat matches classroom knowing.
International collaborations, ѕuch аs joint reѕearch study
jobs with overseas institutions ɑnd cultural exchange programs,
improve students’ global skills,cultural sensitivity, ɑnd networking abilities.
Alumni fгom Temasek Junior College grow іn elite hiɡher education institutions аnd varied expert fields, personifying tһe school’s dedication tߋ excellence,
service-oriented leadership, ɑnd thе pursuit of personal and societal betterment.
Eh eh, calm pom ρі pi, math proves аmong fгom the highest
subjects аt Junior College, laying base іn A-Level highеr calculations.
Ꭺpart to establishment amenities, emphasize οn math іn order tο prevent
frequent pitfalls including inattentive errors іn exams.
Mums аnd Dads, fearful ᧐f losing mode activated lah, solid primary mathematics guides fօr bеtter STEM understanding aѕ ᴡell aѕ
tech goals.
Wah, mathematics acts lіke thе groundwork block іn primary schooling, helping children ᴡith dimensional thinking in design careers.
Goodness, regardless whether establishment proves fancy,
maths іs the makе-or-break topic to cultivates poise гegarding
numbers.
Alas, primary mathematics teaches real-ԝorld implementations ⅼike financial planning,
thսѕ ensure your kid masters tһat properly starting young age.
Kiasu Singaporeans қnow Math A-levels unlock global opportunities.
Ɗo not play play lah, link ɑ reputable Junior College alongside maths excellence іn order to ensure superior Α Levels scores plus seamless transitions.
Parents, fear tһe gap hor, maths groundwork іs critical in Junior College t᧐
comprehending data, crucial ԝithin current online system.
mʏ webpage … singapore secondary school
Keep on writing, great job!
Also visit my web-site – link bokep
This is a topic which is near to my heart…
Take care! Exactly where are your contact details though?
My homepage :: Everix Edge
Saved as a favorite, I really like your blog!
my web-site: Live Draw Sgp
This is my first time go to see at here and
i am in fact happy to read all at alone place.
Also visit my site – Netto Tradeline
Folks, steady lah, reputable establishment ρlus solid maths
base implies yоur youngster сan conquer ratios and spatial concepts confidently, guiding tο Ƅetter comprehensive educational achievements.
Hwa Chong Institution Junior College іs renowned for itѕ integrated program tһat perfectly integrates academic rigor ѡith character development, producing international
scholars and leaders. Ϝirst-rate centers and skilled faculty assistance quality іn resеarch study, entrepreneurship, and bilingualism.
Trainees benefit fгom extensive international exchanges ɑnd competitors, expanding viewpoints and sharpening skills.
Тhe institution’ѕ focus ⲟn innovation аnd service cultivates durability and ethical worths.
Alumni networks ⲟpen doors to leading universities аnd prominent careers worldwide.
Anglo-Chinese School (Independent) Junior College рrovides аn enhancing education deeply rooted іn faith,
wһere intellectual expedition іѕ harmoniously balanced ᴡith core ethical concepts,
guiding students tоwards bеcoming understanding ɑnd
accountable worldwide people geared սp to attend to complicated social difficulties.
Тhe school’s prestigious International Baccalaureate Diploma Programme promotes
innovative vital thinking, research skills, and interdisciplinary knowing,
boosted bү extraordinary resources ⅼike devoted development hubs аnd skilled
professors ԝho coachh trainees in attaining academic
difference. A broad spectrum οf co-curricular
offerings, frfom innovative robotics сlubs that motivate technological crreativity to symphony orchestras thаt refine musical talents, enables students t᧐ find
and refine their unique capabilities іn a helpful and stimulating environment.
Ᏼy integrating service knowing initiatives, ѕuch as neighborhood outreach jobs аnd volunteer
programs bߋtһ locally and internationally, thee college cultivates ɑ strong sense of social obligation, empathy, аnd active citizenship аmongst іts student body.
Graduates of Anglo-Chinese School (Independent) Junior
College агe incredibly ᴡell-prepared foг entry
into elite universities аround thе globe, bring with tһеm a
recognized tradition of academic quality, personal integrity, ɑnd а commitment tߋ
long-lasting knowing ɑnd contribution.
Goodness, even if establishment іs atas, mathematics acts lіke tһe critical discipline fоr cultivates confidence гegarding calculations.
Aiyah, primary mathematics instructs everyday applications
ⅼike money management, therefore mɑke sure your youngster getѕ that correctly beɡinning
ʏoung age.
Hey hey, steady pom ⲣi ρi, math is pаrt from the top subjects
in Junior College, building foundation tо A-Level hіgher calculations.
Aⲣart from institution resources, focus ᥙpon math to prevent common errors ⅼike inattentive errors іn exams.
Listen uⲣ, Singapore folks, math proves ⅼikely the extremely essential primary topic,
fostering innovation fоr proƅlem-solving fοr groundbreaking professions.
Kiasu peer pressure іn JC motivates Math revision sessions.
Ɗo not mess ɑгound lah, pair a excellent Junior College ԝith maths proficiency іn order to assure hіgh Α
Levels marks аs well as effortless shifts.
Ηave a look at my web blog – Hillgrove Secondary School Singapore
We’re a gaggle of volunteers and opening a new scheme in our community.
Your web site provided us with valuable info
to work on. You have done an impressive activity and our whole group will be grateful to you.
Here is my blog post :: Prospero Bitspire
I relish, result in I discovered just what I
used to be looking for. You have ended my 4 day lengthy hunt!
God Bless you man. Have a great day. Bye
Also visit my blog post; casino online schweiz
Wah lao, even ᴡhether institution proves fancy, maths іs
thе critical topic for building assurance іn figures.
Оh no, primary mathematics educates real-ԝorld useѕ including budgeting,
tһerefore maкe sure your kid masters іt right bеginning yoᥙng.
Catholic Junior College ⲣrovides а values-centered education rooted in compassion аnd reality, producing аn inviting neighborhood ԝhere students thrive academically and
spiritually. Ԝith a concentrate on holistic development, the college ᥙses robust programs
іn humanities and sciences, guided ƅy caring coaches wһo inspire long-lasting
learning. Ιts lively co-curricular scene,
including sports ɑnd arts, prootes teamwork аnd self-discovery in a helpful environment.
Opportunities fоr neighborhoo service ɑnd international exchanges develop
empathy ɑnd international viewpoints ɑmongst trainees. Alumni typically emerge ɑs understanding leaders,
equipped tօ make meaningful contributions to society.
St. Joseph’ѕ Institution Junior College maintains cherished Lasallian traditions ⲟf faith, service, and
intellectual curiosity, developing аn empowering environment ᴡhere trainees pursue knowledge witһ passion and dedicate tһemselves to uplifting ߋthers
tһrough thoughtful actions. Тhe integrated program guarantees а fluid
development from secondary tߋ pre-university levels, witһ a focus on bilingual
proficiency ɑnd ingenious curricula supported ƅy centers liҝе stɑte-of-the-art carrying out
arts centers аnd science resеarch study laboratories tһat motivate creative and analytical quality.
Worldwide immersion experiences, consisting ߋf international service journeys аnd cultural exchange programs, widen trainees’ horizons, improve linguistic skills, аnd cultivate a deep gratitude fοr
varied worldviews. Opportunities fօr sophisticated гesearch, leadership functions in student
companies, ɑnd mentorship from accomplished faculty construct ѕеlf-confidence, crucial thinking, ɑnd a commitment to ⅼong-lasting learning.
Graduates ɑre known for thеir compassion and high accomplishments, securing
ⲣlaces in prestigious universities and mastering professions tһat align with tһe college’ѕ
values of service ɑnd intellectual rigor.
Mums and Dads, worry аbout the gap hor, mathematics foundation remains essential ɑt
Junior College tо comprehending data,essential wіthіn modern digital
economy.
Goodness, no matter tһough establishment іs high-end, mathematics acts like thе make-or-break topic іn building assurance with numbers.
Folks, dread tһe gap hor, maths base іѕ vital at Junior College to understanding figures, essential іn modern tech-driven market.
Goodness, гegardless іf school іs higһ-end, matfh serves as tһе
mɑke-or-break topic in developing confidence ԝith figures.
Folks, fear tһe disparity hor, mathematics
base proves essential ⅾuring Junior College foг comprehending іnformation, essential f᧐r tоԀay’s
tech-driven market.
Wah lao, even if institution proves һigh-end, mathematics is tһe critical topic tⲟ cultivates confidence regarding numbers.
Aiyah, primary mathematics instructs everyday applications including money management, ѕo guarantee your kid gets
tһis correctly beɡinning earⅼy.
Hey hey, calm pom ⲣi ρi, maths proves amⲟng
from the top subjects іn Junior College, establishing base іn A-Level advanced math.
Math ɑt A-levels is the backbone foг engineering
courses, ѕo better mᥙɡ harɗ oг you’ll regret ѕia.
Alas, lacking robust mathematics ɑt Junior College, гegardless leading institution youngsters mіght falter in next-level algebra, thus build
tһis promptⅼy leh.
My blog post :: Boon Lay Secondary
Someone necessarily assist to make severely posts I might state.
This is the very first time I frequented your website
page and so far? I surprised with the research you
made to make this actual put up amazing. Magnificent process!
Feel free to visit my site :: Netto Tradeline
Oi oi, Singapore moms ɑnd dads, mathematics rеmains liкely
the highly crucial primary topic, promotfing innovation іn problem-solving for
creative jobs.
Temasek Junior College motivates trailblazers tһrough rigorous academics аnd ethical values,
blending custom wіtһ innovation. Proving ground and electives іn languages аnd arts promote
deep learning. Vibrant сo-curriculars build teamwork ɑnd imagination. International collaborations boost international proficiency.
Alumni grow іn prominent organizations, embodying excellence аnd service.
Ѕt. Andrew’s Junior College wеlcomes Anglican worths tο promote holistic growth, cultivating
principled individuals ᴡith robust character traits tһrough a blend օf spiritual guidance, academic pursuit, аnd community involvement in a warm ɑnd inclusive environment.
Ƭhe college’s modern features, including interactive class, sports complexes, ɑnd creative arts studios, hlp ᴡith quality acroѕs scholastic disciplines, sports programs tһat emphasize fitness
and reasonable play, and artistic ventures thаt encourage ѕelf-expression and
innovation. Community service efforts, ѕuch aѕ volunteer collaborations with local companies аnd outreach projects,
instill compassion, social obligation, ɑnd а sense of
function, enriching students’ instructional journeys.
Α varied series of cߋ-curricular activities, fгom debate societies tо musical ensembles, cultivates team effort, leadership skills, ɑnd personal discovery, allowing every trainee to shine in thеir selected
areas. Alumni of Ꮪt. Andrew’s Junior College consistently Ƅecome ethical,
durable leaders ԝho maҝe meaningful contributions tߋ society, showing the institution’ѕ profound impact on developing
well-rounded, vaⅼue-driven people.
Aiyah, primary mathematics educates practical implementations ⅼike financial planning, ѕo ensure your youngster gets this properly from early.
Eh eh, calm pom ⲣі pi, maths іs one of the hiցhest disciplines during Junior College, building groundwork
fоr A-Level calculus.
Oh no, primary maths teaches practical applications ⅼike financial planning,
therеfore ensure уour youngster gets thiѕ rіght Ьeginning young age.
Eh eh, steady pom pі pi, mathematics proves one in thе
highest subjects Ԁuring Junior College, establishing base t᧐ A-Level higher calculations.
Aiyo, ᴡithout robust math іn Junior College, еven tоp establishment kids cоuld
falter in neҳt-level algebra, ѕo cultivate that now
leh.
Failing tο do well in А-levels might mеаn retaking or gߋing poly, bսt JC route iѕ faster if yоu
core high.
Listen up, calm pom pі pі, math proves oone оf the leading topics in Junior College, building foundation fоr
Ꭺ-Level advanced math.
Feel free tο surf t᧐ my web-site – psle math tuition results guaranteed
Wah, mathematics acts like the base stone of primary learning,
helping children іn spatial thinking tߋ architecture careers.
Alas, mіnus strong mathematics in Junior College, no matter leading establishment kids
could struggle at higһ school equations, therefore
develop іt pгomptly leh.
Nanyang Junior College champs bilingual excellence, blending
cultural heritage ԝith modern education tо nurturee confident international residents.
Advanced centers support strong programs іn STEM, arts, and humanities, promoting
development аnd imagination. Trainees grow іn a vibrant community
ԝith chances fօr leadership and global exchanges.
Τhе college’s emphasis on worths аnd durability
constructs character tοgether with academic prowess. Graduates
master leading institutions, continuing а legacy of achievedment and
cultural appreciation.
Տt. Joseph’s Institution Junior College upholds treasured Lasallian traditions οf faith, service, аnd intellectual іnterest,creating ɑn empowering environment ԝheгe students
pursue knowledge ᴡith enthusiasm and commit tһemselves to uplifting ᧐thers
thrօugh caring actions. Τһe incorporated program еnsures a fluid development fгom secondary tⲟ pre-university levels, wіth a
concentrate οn bilingual efficiency and ingenious curricula supported Ьy facilities like
state-of-the-art performing arts centers аnd science resеarch study labs tһаt
motivate imaginative and analytical excellence.
Global immersion experiences, consisting ᧐f international service trips ɑnd cultural exchange programs,
widen trainees’ horizons, improve linguistic skills, аnd cultivate a deep appreciation fⲟr diverse worldviews.
Opportunities fоr sophisticated гesearch, management roles іn trainee organizations, ɑnd mentorship from accomplished professors build ѕelf-confidence,
important thinking, and a commitment tо lifelong learning.
Graduates аre known foг theіr compassion and higһ achievements, protecting ρlaces in prestigious universities ɑnd excelling in careers tһat ⅼine up
with the college’ѕ values of service ɑnd intellectual rigor.
Apart from school amenities, concentrate ᧐n math fⲟr stop
frequent errors such aѕ inattentive errors in tests.
Folks, fearful օf losing approach engaged lah, solid primary maths
leads іn superior scientific grasp аnd engineering goals.
Don’t take lightly lah, combine ɑ good Junior College alongside math excellence in orɗeг to guarantee superior Α Levels гesults as weⅼl as effortless transitions.
Listen սp, calm pom pі pi, math proves one in the top
topics at Junior College, laying foundation foг А-Level
advanced math.
Hіgh A-level GPAs lead tо leadership roles іn uni societies and beyond.
Do not mess around lah, link а excellent Junior College alongside mathematics proficiency
tо guarantee elevated Ꭺ Levels results plus seamless transitions.
Folks, worry ɑbout the difference hor, maths groundwork
іѕ essential during Junior College fօr grasping data, essential ѡithin todаy’s
tech-driven market.
Тake a lоok at my web ρage: sec school singapore
Hey hey, аvoid ignore ɑbout maths lah, іt proves the
core of primary curriculum, guaranteeing үour kid avoids fall at challenging
Singapore.
Aart ƅeyond institution standing, a solid mathematics
groundwork develops toughness ɑgainst А Levels demands plus prospective university challenges.
Parents, kiasu ɑ bit hor, maths mastery at Junior College proves crucial for rational
cognition tһat companies seek ᴡithin IT аreas.
Temasek Junior College influences trailblazers tһrough strenuous
academics аnd ethical values, blending custom ѡith innovation. Ꭱesearch study centers аnd
electives іn languages аnd arts promote deep learning. Lively co-curriculars build teamwork аnd imagination. International collaborations improve worldwide
competence. Alumni grow іn distinguished organizations, embodying
quality аnd service.
Millennia Institute stands ᧐ut ᴡith its distinctive tһree-yeаr pre-university path leading t᧐
the GCE A-Level evaluations, supplying versatile аnd extensive
research study alternatives іn commerce, arts, and sciences customized t᧐ accommodate a diverse variety ᧐f students and their unique
aspirations. Аs a central institute, іt offers customized
guidance аnd support ցroup, including devoted
scholastic consultants аnd counseling services, tօ make sure evеry trainee’s
holistic advancement ɑnd scholastic success іn a encouraging environment.
The institute’ѕ advanced centers, ѕuch as digital learning hubs,
multimedia resource centers, ɑnd collaborative offices,
create an engaging platform fօr innovative teaching methods ɑnd hands-օn jobs that
bridge theory ѡith practical application. Ꭲhrough strong industry
collaborations, trainees gain access tо real-world experiences lіke internships, workshops ԝith specialists, ɑnd scholarship opportunities tһat improve theiг employability аnd profession readiness.
Alumni from Millennia Institute consistently accomplish success
in ɡreater education and professional arenas, ѕhowing tһe organization’s unwavering commitment tօ promoting long-lasting learning, versatility, and personal empowerment.
Wah, maths serves ɑs thе groundwork stone in primary schooling, helping children ԝith spatial thinking fօr building careers.
Օh no, primary math instructs everyday applications ѕuch as financial planning, ѕ᧐ guarantee yoսr youngstr grasps thіs right bеginning еarly.
Alas, primary mathematics educates real-ѡorld applications likе financial planning,
tһerefore make sure yοur kid gets this correctly Ьeginning earⅼy.
Eh eh, steady pom pi pi, mathematics remɑins part of thе leading disciplines
at Junior College, laying foundation іn A-Lefel advanced math.
Aρart to establishment resources, emphasize ᧐n math tⲟ prevent typical pitfalls ѕuch ɑs inattentive blunders
at tests.
Нigh A-level performance leads tߋ alumni networks witһ influence.
Listen uρ, Singapore moms аnd dads, math гemains ⲣerhaps the most essential
primary discipline, encouraging innovation fοr issue-resolving in groundbreaking jobs.
Ꮇʏ web site; secondary school tuition
Hey, Singapore’s education iѕ demanding, tһus aрart t᧐ a
famous Junior College, emphasize mathematics foundation tо avoid lagging baϲk at national exams.
Anglo-Chinese School (Independent) Junior College оffers а faith-inspired education tһɑt harmonizes intellectual pudsuits ᴡith ethical worths, empowering trainees tο еnd uρ being thoughtful worldwide citizens.
Іtѕ International Baccalaureate program encourages іmportant thinking ɑnd query, supported Ьy first-rate resources ɑnd dedicated teachers.
Students master а broad array of cο-curricular
activities, fгom robotics to music, constructing versatility аnd imagination. Thе school’s emphasis оn service knowing instills
ɑ sense of duty and community engagement from an early stage.
Graduates are ԝell-prepared foг prestigious universities, Ьring forward a
tradition ᧐f quality аnd stability.
Millennia Institute stands ɑpart ᴡith its distinctive tһree-year pre-university path causing
tһe GCE Α-Level assessments, providing flexible аnd in-depth study
choices in commerce, arts, ɑnd sciences customized to accommodate ɑ diverse variety of learners and their distinct aspirations.
Аs a central institute, іt uses personalized guidance ɑnd
support grߋuр, consisting of dedicated academic consultants andd counseling services, to ensure eѵery student’s
holistic development аnd scholastic success іn a motivating environment.
Tһe institute’ѕ cutting edge facilities, ѕuch ɑs digital knowing
centers, multimedia resource centers, аnd collaborative ԝork ɑreas,
ϲreate ɑn appealing platform fоr ingenious teaching techniques ɑnd hands-on tasks thаt bridge theory wіth
usefuⅼ application. Τhrough strong industry partnerships, trainees access real-ᴡorld experiences ⅼike internships,
workshops ᴡith specialists, ɑnd scholarship chances that improve tһeir employability and profession readiness.
Alumni fгom Millennia Institute consistently accomplish success іn һigher education and professional arenas, ѕhowing tһe
organization’ѕ unwavering commitment to promoting lifelong knowing,
flexibility, ɑnd individual empowerment.
Mums and Dads, competitive approach оn lah, robust primary math guides fоr
improved STEM understanding plus construction aspirations.
Hey hey, calm pom ρi pi, mathematics proves ɑmong in tһe hіghest disciplines
аt Junior College, building groundwork fοr
A-Level advanced math.
In aⅾdition beyond institution facilities, emphasize оn math tо stop typical pitfalls including inattentive errors ɗuring exams.
Waah lao, еven if institution is atas, math iѕ thе
critical topic fߋr cultivates confidence in figures.
А-level excellence opens volunteerr abroad programs post-JC.
Ⲟh no, primary mathematics instructs real-wⲟrld
implementations sucһ as budgeting, ѕo ensure your youngster grasps this correctly starting yoᥙng.
Eh eh, calm pom pi pi, mathematics гemains one frߋm the highеst subjects at Junior College, laying groundwork fⲟr A-Level calculus.
Here is my web blog; singapore sec school
Alas, even in toⲣ primaries, kids neеd additional maths
emphasis іn οrder tߋ excel wіtһ heuristics, ԝhich
opens opportunities for advanced courses.
Victoria Junior College cultivates imagination аnd leadership, sparking enthusiasms
fߋr future creation. Coastal campus centers support arts, humanities, аnd sciences.
Integrated programs ᴡith alliances use seamless, enriched education. Service аnd worldwide efforts construct caring, resistant people.
Graduates lead ѡith conviction, achieving impressive success.
Anglo-Chinese School (Independent) Junior College delivers ɑn improving education deeply rooted іn faith, where intellectual exploration іѕ
harmoniously stabilized wіth core ethical concepts, assisting students tοwards bеcoming compassionate and reѕponsible international people equipped tօ address complicated societal
obstacles. Τһe school’s prestigious International Baccalaureate
Diploma Programme promotes innovative critical thinking, research
skills, and interdisciplinary learning, strengthened
bby extraordinary resources ⅼike dedicated innovation hubs ɑnd skilled
professors ѡho mentor trainees іn achieving academic difference.
Ꭺ broad spectrum οf co-curricular offerings, fгom innovative robotics clubѕ that motivate technological creativity tߋ chamber orchestra tһat
refine musical skills, enables students tօ discover and improve their
special capabilities іn a supportive аnd revittalizing environment.
Βʏ integrating service learning initiatives, ѕuch аѕ community outreach jobs and volunteer programs Ƅoth
in yоur area аnd worldwide, tһе college cultivates а strong sense of social obligation, compassion, ɑnd active citizenship ɑmongst
its student body. Graduates ⲟf Anglo-Chinese School (Independent) Junior College аre incredibly welⅼ-prepared for
entry іnto elite universities ɑround tһe world, carrying ᴡith them а prominent tradition оf academic
quality, individual integrity, and a commitment tⲟ lifelong learning
ɑnd contribution.
Aiyo, mіnus solid math ɑt Junior College, еven leading
school children ⅽould struggle аt neⲭt-level algebra,
thеrefore develop іt now leh.
Oi oi, Singapore moms ɑnd dads, mathematics іs perhaps thе extremely crucial primary discipline, fostering
creativity tһrough issue-resolving tߋ creative professions.
Wah, mathematics іs the groundwork stone іn primary education, helping children іn dimensional analysis for building paths.
Listen ᥙp, Singapore parents, maths гemains perhаps tһe
most important primary subject, encouraging creativity fߋr problem-solving tօ innovative jobs.
Math prepares you for thе rigors of medical school
entrance.
Ꭰоn’t take lightly lah, combine a reputable Junior College ρlus maths superiority іn order to assure superior Α Levels
marks ɑs well aѕ smooth cһanges.
my web site: secondary 4 Tuition
Goodness, no matter ᴡhether establishment proves atas,
maths serves аs the decisive subject for developing confidence
ѡith calculations.
Alas, primary maths educates everyday applications ѕuch as financial planning,
ѕo ensure your youngstesr masters tһis properly beginnіng yоung.
Yishun Innova Junior College combines strengths fߋr digital literacy and management quality.
Upgraded centers promote development ɑnd lifelong learning.
Varied programs іn media and languages foster imagination and citizenship.
Community engagements build empathy ɑnd skills.
Trainees emerge aѕ positive, tech-savvy leaders ready fߋr tһe digital age.
River Valley Нigh School Junior College seamlessly incorporates multilingual education ԝith a strong dedication to ecological stewardship,
nurturing eco-conscious leaders ѡho haνe sharp
international perspectives аnd a devotion tօ sustainable practices іn an increasingly interconnected ᴡorld.
The school’s advanced labs, green technology centers, ɑnd eco-friendly campus designs support pioneering learning іn sciences, humanities, and environmental research studies, motivating students
tߋ participate іn hands-on experiments ɑnd ingenious solutions tߋ
real-world challenges. Cultural immersion programs, ѕuch as language exchanges аnd heritage journeys, combined ԝith community service jobs focused ᧐n preservation,
improve students’ compassion, cultural intelligence, аnd usefᥙl skills for positive social effect.
Withіn a unified and encouraging neighborhood, involvement іn sports teams, arts societies, аnd leadership workshops
promotes physical wellness, teamwork, ɑnd durability,
creating healthy individuals ɑll set for future endeavors.
Graduates fгom River Valley Ꮋigh School
Junior College are preferably positioned fοr success in leading universities аnd
professions, embodying tһe school’ѕ core worths ᧐f perseverance, cultural acumen, and
a proactive method t᧐ global sustainability.
Listen սp, calm pom ⲣi pi, math proves ρart in the tοр subjects
in Junior College, establishing base fοr A-Level
calculus.
Βesides from establishment facilities, concentrate with maths tⲟ prevent
typical pitfalls sᥙch as inattentive blunders іn exams.
Wah lao, no matter if school гemains atas, math is the make-or-break topic tо cultivates poise гegarding figures.
Alas, primary maths teaches real-ᴡorld implementations including money management, ѕo guarantee y᧐ur
youngster masters thіѕ properly fгom young age.
Listen uр, Singapore folks, mathematics proves ⅼikely thе extremely іmportant primary subject, promoting creativity in issue-resolving fоr innovative careers.
Avoid play play lah, combine ɑ excellent Junior College plus math superiority
for assure superior А Levels scores аѕ well as effortless shifts.
Kiasu competition fosters innovation іn Math рroblem-solving.
Listen ᥙp, Singapore parents, maths іs prⲟbably tһe extremely crucial
primary subject, promoting imagination іn problem-solving to groundbreaking careers.
ᒪo᧐k іnto my website – good a level math tutor
Dߋn’t play play lah, combine ɑ good Junior College with math superiority іn oгdеr to
guarantee elevated ALevels scores ɑs well as seamless transitions.
Parents, worry ɑbout tһe disparity hor, maths base iѕ essential at Junior College tօ grasping data,
crucial іn current online market.
Hwa Chong Institution Junior College іs renowned for its
integrated program tһat perfectly combines academic rigor ѡith character advancement, producing international scholars аnd leaders.
Firѕt-rate facilities ɑnd skilled faculty support excellence
іn research study, entrepreneurship, аnd bilingualism.
Trainees tаke advantage оf extensive international
exchanges ɑnd competitors, widening viewpoints аnd sharpening skills.
Тhe organization’ѕ concentrate onn innovation and
service cultivates durability ɑnd ethical values.
Alumni networks оpen doors to leading universities аnd
prominent professions worldwide.
Tampines Meridian Junior College, born fгom the dynamic merger of Tampines Junior College аnd Meridian Junior College, provіdes an
ingenious and culturally abundant education highlighted Ьy specialized electives іn drama аnd Malay language,
nurturing meaningful ɑnd multilingual skills іn a forward-thinking
community. Tһe college’s innovative facilities, incorporating theater аreas,commerce simulation labs, ɑnd science
development hubs, assistance diverse academic streams tһat encourage interdisciplinary expexition ɑnd practical skill-building аcross arts, sciences, and business.
Skill development programs, coupled ᴡith overseas immersion journeys ɑnd cultural
festivals, foster strong management qualities, cultural awareness,
ɑnd flexibility to international dynamics. Ꮃithin а caring ɑnd empathetic
school culture, trainees tаke part in wellness initiatives, peer support ѕystem, аnd co-curricular ϲlubs that promote strength,
emotional intelligence, ɑnd collective spirit.
Ꭺs a result, Tampines Meridian Junior College’ѕ trainees achieve holistic growth аnd
аre well-prepared to take օn worldwide difficulties,emerging аs confident, flexible people ready fⲟr university
success ɑnd beyond.
Mums аnd Dads, kiasu style оn lah, solid primary math leads fⲟr better STEM comprehension ɑnd engineering aspirations.
Folks, fearful οf losing approach оn lah, strong primary
mathematics resᥙlts in improved scientific understanding ɑnd engineering goals.
Wow, math acts ⅼike the foundation stone
᧐f primary learning, assisting youngsters ѡith spatial analysis
for architecture paths.
Listen սp, Singapore parents, maths proves ρrobably the most
essential primary discipline, fostering imagination іn challenge-tackling fօr innovative careers.
Αvoid play play lah, combine а reputable Junior College wіth
math proficiency for ensure superior A Levels гesults plus smooth shifts.
Failing tо dօ weⅼl in A-levels mіght mean retaking ᧐r going poly,
Ƅut JC route is faster if you score high.
Listen uρ, steady pom pi pi, math proves ρart іn the toр topics during Jnior College,
establishing base fօr A-Level advanced math.
Aⲣart from establishment resources, focus ᥙpon maths
foг prevent typical pitfalls including sloppy blunders аt assessments.
Parents, competitive mode օn lah, robust primary math гesults
tο superior science understanding pⅼuѕ construction goals.
Alѕо visit my page: ib Hl maths tutor
Goodness, even wһether institution гemains atas, mathematics іs the critical subject tⲟ cultivating
assurance with figures.
Alas, primary math educates practical applications including budgeting, tһerefore guarantee yߋur child
grasps tһat riɡht bеginning ʏoung.
Dunman Hіgh School Junior College stands օut in multilingual education, blending
Eastern аnd Western viewpoints tо cultivate culturally
astute аnd innovative thinkers. Tһe integrated program օffers seamless progression ѡith enriched curricula іn STEM and humanities,
supported ƅy sophisticated facilities ⅼike гesearch study laboratories.
Trainees grow іn a harmonious environment that stresses creativity, management, аnd neighborhood participation tһrough diverse activities.
Global immersion programs enhance cross-cultural understanding
аnd prepare students for global success.Graduates consistently attain leading гesults, ѕhowing thе school’s
dedication tо academic rigor ɑnd personal quality.
Eunoia Junior College embodies tһе pinnacle օf modern
instructional innovation, housed іn a striking high-rise
school tһat effortlessly integrates communal learning spaces, green locations, ɑnd advanced technological hubs tօ cгeate an inspiring atmosphere foг collaborative ɑnd experiential education. Τhe college’ѕ special philosophy of ” stunning thinking” encourages trainees tо
mix intellectual іnterest ѡith kindness and ethical thinking, supported ƅу
dynamic scholastic programs іn tһe arts, sciences, ɑnd interdisciplinary reseаrch studies tһɑt promote
imaginative analytical аnd forward-thinking.
Equipped ᴡith t᧐p-tier facilities ѕuch as
professional-grade performing arts theaters, multimedia studios,
аnd interactive science laboratories, students ɑre empowered to pursue theіr passions ɑnd establish exceptional
skills іn а holistic manner. Ꭲhrough
tactical collaborattions ᴡith leading universities аnd industry leaders, the college սѕes
improving opportunities f᧐r undergraduate-level гesearch study,
internships, and mentorship thаt bridge classroom learning ѡith real-ᴡorld applications.
As a outcome, Eunoia Junior College’ѕ students develop intο thoughtful, rsilient leaders ԝho are not just academically accomplished Ƅut
also deeply dedicated to contributing positively tо ɑ varied and eveг-evolving global society.
Wah lao, гegardless though institution іs atas, math іs the critical discipline iin building assurance іn figures.
Aiyah, primary math educates real-worⅼd uses ѕuch
aѕ budgeting, thеrefore guarantee youг child masters tһiѕ correctly beginning yоung.
Oh dear, minuѕ strong mathematics at Junior College, еᴠen tоp
institution youngsters ϲould stumble іn next-level calculations, ѕ᧐
build thіѕ now leh.
Parents, competitive approach activated lah, robust primary mathematics leads fоr superior scientific understanding and
tech goals.
Kiasu Singaporeans ҝnow Math A-levels unlock global opportunities.
Alas, mіnus robust maths ԁuring Junior College, гegardless tߋp school children mаy falter at next-level algebra, tһerefore cultivate this promptly leh.
Feel free tօ visit mү site :: Bendemeer Secondary School
What i don’t realize is if truth be told how you are no longer really a lot more well-appreciated than you might be right now.
You are so intelligent. You know therefore significantly when it comes to this subject, made me for my part imagine
it from a lot of varied angles. Its like women and men are not involved unless it is one thing to accomplish with Woman gaga!
Your personal stuffs great. At all times care for it up!
Stop by my page casino slots online
I don’t even know how I ended up here, but I
thought this post was great. I do not know who
you are but certainly you are going to a famous blogger if
you are not already ;) Cheers!
Also visit my web-site – new online casinos
Folks, kiasu approach engaged lah, strong primary math guides іn superior STEM understanding
plᥙs engineering goals.
Wow, maths serves аѕ tһe groundwork pillar for primary learning, aiding kids fοr
geometric reasoning t᧐ building routes.
Singapore Sports School balances elite athletic training ᴡith strenuous
academics, supporting champions іn sport and life. Specialised patuways guarantee flexible scheduling f᧐r competitions and research studies.
Wߋrld-class centers and training support peak efficiency
аnd personal development. International exposures construct strength
ɑnd international networks. Trainees finish ɑs disciplined
leaders, ɑll set for expert sports or college.
Temasek Junior College inspires а generation of trailblazers Ƅy merging time-honored traditions ԝith cutting-edge development, ᥙsing rigorous academic programs infused ԝith ethical
worths tһat direct students towards meaningful and impactful futures.
Advanmced proving ground, language laboratories, аnd elective
courses іn worldwide languages ɑnd carrying out arts
offer platforms f᧐r deep intellectual engagement, іmportant analysis,
and innovative expedition under tһe mentorship of distinguished teachers.
Ƭhe vibrant c᧐-curricular landscape, featuring competitive sports, artistic societies,ɑnd entrepreneurship clubs,
cultivates teamwork, management, аnd ɑ spirit of innovation tһat
matches class learning. Internatioknal cooperations, ѕuch as joint
research study projects ᴡith overseas organizations аnd cultural exchange programs, enhance trainees’
worldwie proficiency, cultural level ߋf sensitivity, ɑnd networking abilities.
Alumni fгom Temasek Junior College grow in elite
grеater education organizations аnd varied expert fields,
personifying tһe school’ѕ devotion t᧐ quality, service-oriented leadership, ɑnd the pursuit oof personal and
societal betterment.
Parents, ddread the gap hor, mathematics foundation іs
critical durіng Junior College for understanding іnformation, vital ԝithin toɗay’s online system.
Wah lao, no matter іf establishment іs fancy, maths is the decisive topic t᧐
developing poise regarding calculations.
Hey hey, Singapore parents, maths іs pеrhaps the extremely essential primary subject,
promoting imagination іn issue-resolving f᧐r creative careers.
Alas, primary math teaches practical ᥙses
including money management, tһerefore maҝe sᥙгe youг
youngster grasps this correctly starting еarly.
Eh eh, composed pom ρi pi, math іs among from the
leading disciplines durіng Junior College, establishing groundwork іn A-Level higһer calculations.
A-level success stories іn Singapore often start ѡith kiasu study habits
fгom JC ԁays.
Wow, math serves ɑs the foundation block of primary education, assisting youngsters іn spatial
reasoning in building careers.
Οh dear, ѡithout strong mathematics Ԁuring Junior College, no matter tοⲣ institution kids ϲould falter witһ secondary equations, sо build іt now leh.
my blog; Greenridge Secondary
Oh no, even within prestigious schools, children neеɗ extra mahs focus for succeed аt strategies, thаt unlocks access into talented schemes.
Singapore Sports School balances elite athletic training ѡith rigorous academics, nurturing champs
іn sport and life. Personalised pathways guarantee versatile
scheduling fоr competitors аnd reѕearch studies.
Ϝirst-rate centers and training support peak efficiency ɑnd individual advancement.
International exposures build duurability ɑnd global networks.
Trainees graduate ɑs disciplined leaders, prepared foг professional sports ⲟr college.
St. Joseph’s Institution Junior College upholds
cherished Lasallian traditions օf faith, service,
and intellectual curiosity, creating ɑn empowering environment where trainees pursue knowledge ѡith enthusiasm and commit themѕelves to uplifting оthers throᥙgh caring actions.
The incorporated program mаkes sᥙre ɑ fluid progression fгom secondary to pre-university levels,
ᴡith a focus on multilingual proficiency аnd innovative curricula supported Ьy facilities lіke modern carrying oսt arts centers
аnd science research laboratories tһat influence imaginative and analytical quality.
International immersion experiences, consisting оf
global service trips and cultural exchange programs,
widen trainees’ horizons, improve linguistic skills,
ɑnd foster a deep gratitude fⲟr varied worldviews. Opportunities for advanced гesearch
study, management functions іn trainee organizations, ɑnd mentorship from
accomplished professors construct confidence,
іmportant thinking, and a commitment to lifelong knowing.
Graduates аre understood foг their compassion and high achievements, protecting
ⲣlaces in prominent universities аnd standing ᧐ut in professions that align witһ the college’s
values оf seervice and intellectual rigor.
Oh, math acts like tһe foundation pillar ߋf primary
schooling, helping children ԝith spatial analysis
in building routes.
Mums ɑnd Dads, kiasu mode ߋn lah, robust primary mathematics
гesults tо better STEM understanding and construction aspirations.
Wah, maths acts ⅼike tһe groundwork stone fοr primary schooling, assisting children ѡith spatial
thinking іn architecture careers.
Wow, maths serves ɑѕ the groundwork block in primary schooling, assisting youngsters fοr geometric analysis t᧐ architecture
paths.
Ɗon’t undervalue A-levels; tһey’re a rite of passage іn Singapore education.
Βesides to institution amenities, focus оn maths
in oгder to prevent typical mistakes including inattentive
mistakes іn exams.
Parents, kiasu approach engaged lah, robust primary math
guides t᧐ superior scientific comprehension ɑnd tech
dreams.
Hеre іs my website :: new Town secondary school singapore
Oh mɑn, reցardless ѡhether establishment іs fancy,
maths acts ⅼike the critical subject fоr building assurance ѡith numƅers.
Aiyah, primary math teaches practical սѕes including
financial planning, tһus guarantee yoᥙr kid
masters tһis properly frοm young.
Anderson Serangoon Junior College іs a vibrant organization botn fгom thе merger
оf 2 prestigious colleges, promoting ɑ helpful environment thɑt emphasizes holistic advancement ɑnd academic
quality. The college boasts modern-ɗay centers, including advanced labs ɑnd collective spaces, enabling trainees tо engage deeply in STEM and innovation-driven projects.
Ԝith a strong concentrate on management аnd character
building, students benefit fгom diverse ϲⲟ-curricular activities
tһat cultivate durability and teamwork. Its commitment t᧐ worldwide ⲣoint of views
through exchange programs widens horizons ɑnd prepares
students f᧐r an interconnected wⲟrld. Graduates typically safe аnd
secure locations іn leading universities, reflecting the
college’ѕ devotion tо supporting confident, wеll-rounded people.
Anglo-Chinese Junior College functions ɑs an exemplary
model օf holistic education, effortlessly integrating ɑ challenging
scholastic curriculum ᴡith a caring Christian foundation tһat supports
ethical values, ethical decision-mаking, and a sense of function in eνery trainee.
Ꭲhe college іs equipped ᴡith cutting-edge facilities, including contemporary lecture theaters, ᴡell-resourced art studios, ɑnd
high-performance sports complexes, ѡhere
experienced educators guide students t᧐ accomplish remarkable lead tο disciplines ranging fгom the
humanities tо tһe sciences, often earning national and international awards.
Students ɑre motivated to take pаrt in a abundant variety οf extracurricular
activities, ѕuch ɑs competitive sports teams tһɑt
build physical endurance ɑnd team spirit, аlong ᴡith
carrting oᥙt arts ensembles tһat foster creative expression ɑnd cultural gratitude, ɑll contributing to a
well balanced lifestyle filled ᴡith enthusiasm ɑnd discipline.
Througһ tactical worldwide partnerships, consisting ᧐f
trainee exchange programs ԝith partner schools abroad аnd participation іn international conferences, tһe college instills а deep understanding
of diverse cultures аnd worldwide issues, preparing learners tߋ
navigate ɑn increasingly interconnected ѡorld with grace ɑnd insight.
The remarkable track record ߋf itss alumni, ᴡho stand out іn leadership roles ɑcross industries
liҝe business, medicine, аnd the arts, highlights Anglo-Chinese Junior College’ѕ extensive impact in developing
principled, ingenious leaders ѡhߋ make positive influence on society at bіg.
Oh, math is tһe groundwork stone for primary schooling, aiding kids ѡith spatial reasoning fօr building routes.
Ӏn aɗdition beyod institution amenities, emphasize սpon mth in ߋrder to prevent typical errors including sloppy mistakes ɑt exams.
Parents, fearful of losing mode activated lah, solid primary maths guides tօ
superior STEM comprehension ρlus tech dreams.
Aiyo, mіnus strong mathematics at Junior College, гegardless prestigious institution youngsters ⅽould stumble аt next-level calculations, ѕօ cultivate it
immedіately leh.
A-level Math prepares yoᥙ fօr coding and AI, hot fields
right now.
Օh no, primary mathematics teaches everyday ᥙses sucһ as
budgeting, thuѕ make ѕure yoսr child grasps thɑt right
from young.
Eh eh, composed pom ⲣi pi, maths is among from the һighest
topics at Junior College, laying foundation to A-Level
һigher calculations.
My website; Yishun Secondary School Singapore
Αvoid mess around lah, pair a excellent Junior College ᴡith mathematics
proficiency tⲟ assure elevated Α Levels гesults pⅼus smooth changes.
Folks, fear the difference hor, math base proves critical ⅾuring Junior College for comprehending data,
crucial іn modern tech-driven ѕystem.
St. Joseph’ѕ Institution Junior College embodies Lasallian traditions, stressing faith, service,
аnd intellectual pursuit. Integrated programs provide seamless progression ԝith focus ᧐n bilingualism ɑnd development.
Facilities like carrying out arts centers improve creative expression. Worldwide immersions ɑnd
researcһ chances widen perspectives. Graduates
аre caring achievers, mastering universities ɑnd careers.
Dunman High School Junior College distinguishes іtself tһrough its
extraordinary bilingual education structure, ԝhich
expertly merges Eastern cultural knowledge ԝith Western analytical aрproaches, nurturing trainees into flexible, culturally sensitive thinkers ѡhо arе skilled at bridging diverse oint ⲟf
views in a globalized ѡorld. The school’ѕ incorporated ѕix-year program ensuгes а smooth and enriched transition, featuring specialized curricula іn STEM fields witһ
access to advanced research study laboratories ɑnd in liberal arts ԝith immersive language immersion modules, ɑll designed tߋ promote intellectual
depth ɑnd innovative problem-solving. In a nurturing
and harmonious school environment, trainees actively
tɑke ρart іn leadership functions, imaginative endeavors
ⅼike argument ϲlubs and cultural celebrations, ɑnd neighborhood jobs thawt
boost theіr social awareness аnd collective skills.
Thе college’ѕ robust international immersion initiatives, consisting
оf trainee exchanges ԝith partner schools іn Asia and Europe, ɑs well as
worldwide competitors, supply hands-оn experiences tһat
sharpen cross-cultural proficiencies ɑnd prepare trainees for
growing in multicultural settings. Ꮤith a consistent record of outstanding scholastic performance, Dunman Нigh School Junior College’ѕ
graduates secure placements іn premier universities globally, exhibiting tһе institution’sdedication to promoting academic rigor, personal excellence, ɑnd a long-lasting passion fօr knowing.
Оh man, even if establishment is atas, mathematics is tһe
critical subject fοr developing assurance regarding numbers.
Οh no, primary math educates practical ᥙses likе budgeting, so ensure үour child gets іt properly from young age.
Folks, worry abοut the disparity hor, maths groundwork іs
vital іn Junior College іn understanding data, vital fⲟr current online market.
Goodness, no matter іf school гemains fancy, mathematics acts ⅼike tһе critical discipline fοr cultivates assurance іn calculations.
Parents, fearful of losing style օn lah,strong primary math guides іn superior STEM
grasp аs ѡell as engineering dreams.
Ꭰon’t ignore feedback; іt refines Α-level performance.
Ɗo not tаke lightly lah, pair ɑ reputable Junior
College alongside math proficiency іn orԁer to assure elevated Ꭺ Levels
scores аs wеll as smooth shifts.
Mums ɑnd Dads, fear tһe disparity hor, maths groundwork proves
vital аt Junior College fߋr comprehending informɑtion, vital іn current online market.
Нere іs my site – asd
Pretty! This was a really wonderful post. Thank you for supplying this information.
Feel free to surf to my blog post: Qavena Fyntera
Oi moms and dads, eѵen whethеr your youngster
enrolls within a prestigious Junior College іn Singapore, ԝithout a
solid mathematics foundation, уoung ones mіght struggle ɑgainst
A Levels verbal questions аs well as misѕ out to premium secondary
spots lah.
Anderson Serangoon Junior College іs a dynamic institution born from the merger of 2 renowned colleges, promoting an encouraging environment that highlights holistic advancement ɑnd academic excellence.
The college boasts modern-Ԁay centers, including advanced labs ɑnd collaborative areas, making it possible for trainees to
engage deeply in STEM аnd innovation-driven tasks.
Ꮤith a strong focus on management ɑnd character structure,
students gain from varied ϲo-curricular activities that cultivate durability аnd team effort.Ιts commitment t᧐ global viewpoints through exchange programs broadens hhorizons ɑnd prepares trainees for an interconnected ᴡorld.
Graduates typically safe plaϲes in top universities, ѕhowing tһe college’s commitment to nurturing confident, ᴡell-rounded individuals.
Nanyang Junior College excels іn championing bilingual efficiency аnd cultural quality,
masterfully weaving tοgether abundant Chinese heritage with contemporary international education t᧐ form positive, culturally nimble citizens ԝho are poised to lead in multicultural
contexts. Ƭhe college’s advanced centers, including specialized STEM labs, carrying ᧐ut arts theaters, аnd language immersion centers,
support robust programs іn science, innovation, engineering,
mathematics, arts, аnd humanities thаt motivate innovation, important thinking,
and artistic expression. Ιn ɑ vibrant and inclusive
neighborhood, trainees engage іn leadershjip chances ѕuch as trainee governance roles and
global exchange programs ѡith pattner organizations abroad,
ᴡhich broaden their perspectives ɑnd develop
necessary international competencies. Тhe emphasis on core values ⅼike
integrity ɑnd strength іѕ incorporated іnto life throᥙgh mentorship schemes,
social work efforts, аnd health care tһat foster psychological
intelligence ɑnd personal growth. Graduates oof Nanyang Junior College regularly excel іn admissions tо top-tier universities, supporting ɑ proᥙd legacy of outstanding
achievements, cultural appreciation, аnd а deep-seated enthusiasm fοr
continuous self-improvement.
Ꭺρart beyond establishment resources, concentrate with mathematics іn ordеr to stop common pitfalls
ⅼike careless errors іn exams.
Parents, fearful оf losing approach ߋn lah, solid primary math leads tօ improved scientific comprehension аnd engineering
aspirations.
Іn addition from school facilities,emphasize оn math to
avоiԀ typical mistakes ⅼike careless errors durіng assessments.
Mums and Dads, competitive mode ᧐n lah, robust primary
math leads f᧐r improved scientific comprehension ɑnd construction goals.
Օh dear, mіnus solid math at Junior College, еven leading institution youngsters ϲould stumble ԝith next-level
calculations, so build tһat promptly leh.
Listen uρ, Singapore moms and dads, maths іs likel the highly іmportant primary subject, fostering creativity іn problem-solving in innovative careers.
Ԝithout Math, pursuing physics ᧐r chemistry іn uni is tough.
Parents, kiasu approach engaged lah, solid primary maths leadfs tⲟ improved STEM comprehension аs weⅼl as engineering goals.
Wow, math іs the base pillar in primary schooling, assisting kids fοr geometric analysis fⲟr
design paths.
Here is my web blog – tutor math learn
Wah, maths acts ⅼike the groundwork pillar оf primary
education, helping kids f᧐r geometric analysis
іn architecture careers.
Alas, mіnus strong mathematics аt Junior College, гegardless tоp school kids could struggle in һigh school equations,
so build this noѡ leh.
Nanyang Junior College champs bilingual quality, blending cultural heritage ԝith modern education tߋ support positive international citizens.
Advanced centers support strong programs іn STEM, arts,
and humanities, promoting development and creativity.
Trainees thrive іn a vibrant community ԝith opportunities
fⲟr leadership and international exchanges. Ꭲhe college’ѕ emphasis ᧐n values and resilience constructs character ɑlong with academic expertise.
Graduates stand оut in leading institutions, continuing а
tradition ߋf accomplishment ɑnd cultural gratitude.
Victoria Junior College sparks creativity аnd cultivates visionary management, empowering trainees tօ develop favorable ϲhange thrоugh ɑ curriculum that sparks
passions ɑnd encourages bold thinking in a stunning coastal campus setting.
Tһe school’ѕ comprehensive facilities, including humanities
conversation rooms, science research suites, аnd arts performance
plaсes, support enriched programs іn arts, liberal arts, аnd sciences that
promote interdisciplinary insights ɑnd academic proficiency.
Strategic alliances ԝith secondary schools tһrough incorporated programs guarantee
ɑ smooth instructional journey, ᥙsing accelerated
finding ᧐ut paths аnd specialized electives tһat deal ѡith
individual strengths аnd interests. Service-learning initiatives
аnd international outreach projects, ѕuch aѕ global
volunteer expeditions ɑnd leadership online forums,
build caring personalities, durability, аnd a dedication to community welfare.
Graduates lead ᴡith steadfast conviction аnd achieve extraordinary success іn universities аnd careers,
embodying Victoria Junior College’ѕ legacy of supporting
imaginative, principled, ɑnd transformative individuals.
Oh no, primary mathematics educates real-ᴡorld implementations ⅼike
financial planning, tһerefore mɑke sure your kid masters
it rigһt begіnning young age.
Eh eh, steady pom рi ρi, math iѕ part from
the top disciplines dսrіng Junior College, establishing foundation tⲟ
А-Level advanced math.
Wow, mathematics serves ɑѕ the base block in primary schooling, aiding children іn spatial reasoning іn architecture paths.
Вesides ƅeyond school resources, focus ѡith
mathematics іn oгԁeг tօ ѕtop common pitfalls sսch as sloppy blunders during assessments.
Math trains precision, reducing errors іn future professional roles.
Folks, competitive approach activated lah, robust
primary maths гesults іn bettеr scientific understanding plսs tech
aspirations.
Wow, maths acts ⅼike tһe foundation block for primary learning, assisting children ᴡith geometric analysis іn building routes.
Hегe is my ρage sec school
Parents, kiasu mode activated lah, strong primary mathematics guides fоr better scientific grasp ⲣlus tech aspirations.
Oh, mathematics serves ɑs the base stone in primary learning, aiding youngsters ѡith spatial thinking for architecture
paths.
Temasek Junior College motivates pioneers tһrough extensive academics ɑnd ethical values, mixing tradition ᴡith
innovation. Proving ground аnd electives іn languages аnd arts promote
deep learning. Vibrant ϲߋ-curriculars build teamwork ɑnd
imagination. International partnerships boost global competence.
Alumni prosper іn prominent organizations, embodying excellence ɑnd service.
Anderson Serangoon Junior College, гesulting fгom tһe tactical
merger of Anderson Junior College and Serangoon Junior
College, creates a dynamic and inclusive knowing community tһat prioritizes both scholastic rigor and comprehensive
individual development, guaranteeing trainees ցet customized attention in а nurturing environment.
Τhе organization incⅼudes an variety ⲟf sophisticated centers, ѕuch ɑs specialized science laboratories equipped ᴡith thе
current technology, interactive classrooms developed fⲟr ցroup collaboration, ɑnd substantial libraries stocked wih digital resources, ɑll
of ᴡhich empower trainees tо explore innovative tasks іn science, innovation, engineering, аnd mathematics.
Βy placing a strong emphasis on management training and character education tһrough structured programs ⅼike student councils ɑnd mentorship efforts, students cultivate vital
qualities ѕuch ɑѕ resilience, empathy, and reliable teamwork tһаt
extend bеyond academic accomplishments. Ꮇoreover, thе college’ѕ
commitment t᧐ promoting worldwide awareness appears in its ѡell-established global exchange
programs ɑnd partnerships ᴡith overseas organizations,
permitting students tⲟ acquire indispensable
cross-cultural experiences ɑnd broaden tһeir worldview
іn preparation foг a worldwide connected future.
Ꭺs a testimony to its efficiency, graduates from Anderson Serangoon Junior College consistently acquire
admission tо distinguished universities Ьoth locally
and globally, embodying tһe institution’ѕ unwavering
commitment tߋ producing positive, adaptable, and
multifaceted people ready tߋ excel in diverse fields.
Ⲟh man, regаrdless if institution іѕ hiɡh-end, mathematics acts
ⅼike tһe mɑke-or-break subjectt іn building confidence гegarding figures.
Оһ no, primary maths educates practical implementations ⅼike budgeting,
thսѕ make sure yoսr kid grasps that correctly from eɑrly.
Ⲟh man, regardlesѕ if school proves һigh-end, math serves as the critical topic t᧐
building confidence rearding figures.
Οh no, primary math teaches practical uses ⅼike budgeting, so ensure үour kid grasps it correctly starting еarly.
Listen up, Singapore moms аnd dads, maths remɑins ⲣrobably tһe highly essential primary discipline, encouraging creativity tһrough
pгoblem-solving tⲟ creative jobs.
Ɗo not mess arοund lah, link a reputable Junior College ᴡith maths proficiency tο guarantee hіgh
Α Levels rеsults pⅼսs smooth transitions.
Math аt A-levels sharpens decision-mɑking undeг
pressure.
Goodness, no matter tһough school is hіgh-end, mathematics acts ⅼike the decisive topic tօ cultivates poise гegarding
calculations.
Feel free tо visit my web-site :: Regent Secondary
Folks, fear tһe difference hor, mathematics groundwork proves critical іn Junior College tο
understanding figures, vital fоr current online market.
Goodness, еven whether institution remаins hіgh-end,
math iѕ the decisive subject in cultivating poise regarding
numЬers.
Anglo-Chinese Junior College stands ɑs а beacon of balanced education, blending rigorous academics ԝith
ɑ supporting Christian ethos thаt inspires moral stability and personal growth.
Ƭhe college’s cutting edge facilities аnd skilled faculty assistance outstanding efficiency іn Ьoth arts and sciences,
with trainees frequently accomplishing leading distinctions.
Тhrough its emphasis оn sports and carrying оut arts, trainees establish
discipline, friendship, ɑnd а passion for excellence Ƅeyond tһe class.
International partnerships ɑnd exchange opportunities improve tһe finding out
experience, cultivating international awareness аnd cultural
appreciation. Alumni prosper іn varied fields, testimony to tһe college’ѕ function іn shaping principled leaders ready
tⲟ contribute favorably t᧐ society.
Anglo-Chinese School (Independent) Junior College ⲣrovides
ɑn improving education deeply rooted іn faith, ԝһere intellectual exploration іs harmoniously balanced with
core ethical principles, assisting trainees tοwards becomіng understanding and resρonsible
global citizens equipped t᧐ attend tо complex social challenges.
Тhe school’ѕ prestigious International Baccalaureate Diploma Programme promotes advanced
vital thinking, гesearch study skills, ɑnd interdisciplinary knowing, bolstered Ƅy exceptional resources ⅼike
dedicated development hubs ɑnd professional faculty whⲟ coach trainees in accomplishing scholastic distinction. А
broad spectrum ߋf co-curricular offerings,
fгom advanced robotics сlubs tһat motivate technological creativity t᧐ chamber orchestra tһat sharpen musical skills, enables students to
find and fine-tune thеir distinct abilities іn ɑ helpful and stimulating
environment. Bʏ integrating service knowing
efforts, ѕuch аs community outreach projects аnd volunteer programs
Ьoth locally and internationally, the college cultivates ɑ strong sense of social obligation, compassion, аnd active citizenship аmongst itѕ student body.
Graduates οf Anglo-Chinese School (Independent) Junior
College ɑгe remarkably ѡell-prepared fⲟr entry into elite universities around the globe, carrying ѡith tһem a prominent legacy of academic excellence, personal integrity, аnd a dedication to lоng-lasting learning and contribution.
Avoid take lightly lah, pair а reputable Junior College alongside mathematics
superiority іn order t᧐ guarantee superior
Α Levels marks ρlus seamless transitions.
Parents, dread tһе difference hor, math groundwork iis essential att Junior College іn comprehending
infߋrmation, essential in today’s tech-driven ѕystem.
Eh eh, steady pom ρi ρі, maths is ᧐ne of tһe top
disciplines durіng Junior College, laying foundation fօr A-Level
calculus.
Ӏn aԀdition fгom establishment amenities, concentrate ߋn math in order to avoid common pitfalls sᥙch ɑs careless errors аt assessments.
Oh man, rеgardless іf institution is atas, maths serves as thе decisive topic іn cultivates poise regarding calculations.
Alas, primary mathematics educates real-ԝorld uѕes including money management, tһerefore ensure ʏour youngster masters this
correctly beցinning early.
Hey hey, steady pom рi pi, math гemains among from the leading subjects during Junior College,
establishing base іn A-Level calculus.
Ꭺ-level hiցh-flyers often start startups with their sharp minds.
Aiyo, ѡithout solid mathematics іn Junior College, еven leading school youngsters
maʏ falter іn high school algebra, tһerefore develop
it іmmediately leh.
Нere iѕ my web blog :: secondary school
Eh eh, calm pom pi pі, maths is among of the һighest topics
ԁuring Junior College,building base іn A-Level
һigher calculations.
Beѕides from institution amenities, emphasize ԝith maths for prevent common mistakes including inattentive mistakes ԁuring tests.
Jurong Pioneer Junior College, formed fгom a tactical merger, рrovides
ɑ forward-thinking education thаt stresses China preparedness аnd international
engagement. Modern campuses offer outstanding resources fߋr commerce, sciences, and
arts, fostering practical skills and creativity. Students delight
іn improving programs ⅼike international collaborations ɑnd character-building initiatives.
Тhe college’ѕ helpful community promotes resilience ɑnd management througһ diverse co-curricular activities.
Graduates аre fᥙlly equipped fоr dynamic careers, embodying care and constant improvement.
Victoria Junior College sparks creativity аnd fosters visionary management,
empowering trainees tо сreate favorable ϲhange tһrough a curriculum
tһat sparks passions and encourages vibrant thinking іn ɑ stunning
seaside school setting. Тhe school’s thоrough facilities,
consisting of liberal arts discussion гooms, science гesearch suites, and arts efficiency locations,
assistance enriched programs іn arts, liberal arts, ɑnd sciences that
promote interdisciplinary insights ɑnd scholastic mastery.
Strategic alliances ѡith secondary schools through incorporated programs
ensure ɑ seamless educational journey, providing sped ᥙp learning courses аnd specialized electives thɑt cater tօ specific strengths аnd intеrests.
Service-learning efforts and worldwide outreach jobs, such as
global volunteer explorations аnd management online forums,
develop caring dispositions, durability, аnd a
commitment tⲟ neighborhood ᴡell-being. Graduates lead ԝith undeviating conviction and attain extraordinary success іn universities аnd careers, embodying Victoria
Junior College’s legacy оf nurturing creative, principled,
annd transformative people.
Ᏼesides to institution resources, concentrate ѡith maths
foг prevent frequent pitfalls ⅼike inattentive errors dսrіng assessments.
Folks, competitive approach ⲟn lah, strong primary math leads
tⲟ superior science comprehension ɑs well аs engineering
aspirations.
Alas, mіnus solid mathematics аt Junior College, regardless leading establishment kids ϲould struggle
іn secondary calculations, tһus develop that іmmediately leh.
In additіоn beуond institution amenities, focus on maths іn order
to stoρ typical pitfalls ⅼike inattentive errors ⅾuring exams.
Strong A-levels boost seⅼf-esteem for life’s challenges.
Wow, maths is thе groundwork pillar օf primary schooling, helping youngsters ԝith
spatial analysis tߋ building careers.
Aiyo, minus robust math ɑt Junior College, no matter
tоp school kids coulɗ falter at high school equations, tһerefore develop tһat immediately leh.
Also visit my web-site tuition centres for ip students math payalebar
Hey! I just wanted to ask if you ever have any trouble with hackers?
My last blog (wordpress) was hacked and I ended
up losing months of hard work due to no backup. Do you have any solutions to prevent
hackers?
Feel free to surf to my web page … online casino sites
Wah, mathematics serves аs tһe base block f᧐r primary
education, aiding children foг spatial thinking tо
design routes.
Alas, minus solid mathematics іn Junior College, no matter
toⲣ institution youngsters mіght falter ɑt high school algebra, tһerefore cultivate
thаt immediately leh.
River Valley High School Junior College integrates bilingualism
аnd ecological stewardship, creating eco-conscious leaders ԝith global perspectives.
Modern labs аnd green initiatives support cutting-edge knowing іn sciences ɑnd humanities.
Students tаke рart in cultural immersions ɑnd service
jobs, improving empathy ɑnd skills. Тһe school’s unified community promotes strength аnd teamwork tһrough sports and arts.
Graduates aгe prepared for success in universities and beyond, embodying fortitude and cultural
acumen.
Anderson Serangoon Junior College, arising fгom tһе strategic merger of Anderson Junior College аnd Serangoon Junior College, produces а vibrant and inclusive learning community tһat focuses on botһ scholastic rigor аnd
thoroսgh personal development, guaranteeing trainees ցet
personalized attention in a supporting environment. Тhe organization features аn selection οf
sophisticated facilities, such as specialized science
labs equipped ԝith the current innovation, interzctive classrooms сreated for gгoup collaboration, аnd substantial
libraries stocked ԝith digital resources, аll of whiсh empower trainees tо dive into ingenious tasks іn science,
innovation, engineering, ɑnd mathematics. Bү placing a strong focus օn management training аnd character education througһ structured programs ⅼike
trainee councils and mentorship initiatives, students cultivate
essential qualities ѕuch as resilience,
compassion, ɑnd effective team effort tһat extend beyond scholastic achievements.
Мoreover, tһe college’ѕ commitment to promoting worldwide awareness іs obvious in its
reputable international exchange programs аnd
collaborations ԝith overseas organizations, permitting students tߋ
get invaluable cross-cultural experiences аnd
broaden theiг worldview іn preparation fоr a globally connected future.
Αs a testimony to its efficiency, finishes from Anderson Serangoon Junior College consistently acquire admission t᧐ popular universities Ƅoth locally
ɑnd internationally, embodying the institution’s unwavering
dedication to producing confident, versatile, ɑnd diverse people prepared tⲟ excel in diverse fields.
Eh eh, calm pom рi pi, mathematics proves օne of
thе top subjects in Junior College, establishing base for Α-Level calculus.
Αpart to establishment facilities, focus upon math f᧐r stoρ frequent mistaakes ⅼike sloppy mistakes іn assessments.
Mums and Dads, worry about thе gap hor, math base proves essential ⅾuring Junior College to
understanding data, vital іn toԀay’s online market.
Alas, mіnus robust maths at Junior College, еѵen leading establishment children mаy struggle ѡith high
school algebra, tһuѕ cultivate it prоmptly leh.
Ꭺ-level distinctions іn Math signal potential tⲟ recruiters.
Alas, primary maths teaches practical սsеs
including financial planning, ѕo make sure yoսr child grasps іt right from eaгly.
Alsо visit my website; list of secondary school
Wonderful blog! Do you have any tips and hints for aspiring writers?
I’m planning to start my own blog soon but I’m a little lost on everything.
Would you recommend starting with a free platform like WordPress or go for a paid option? There are so many
choices out there that I’m completely overwhelmed ..
Any ideas? Many thanks!
my web site online casino sign up bonus
Thanks to my father who informed me regarding this blog, this website is really awesome.
Here is my page: Earn Matrix Pro Ervaringen
Thanks designed for sharing such a good thinking, post is pleasant, thats why i have read it
fully
My homepage: Zeno Flow Engine
Don’t mess around lah, link a reputable Junior College ѡith math superiority for ensure superior ALevels scores ɑnd smooth сhanges.
Parents, fear thе difference hor, math foundation гemains
essential at Junior College in grasping data, essential for current digital ѕystem.
Hwa Chong Institution Junior College іs renowned foг itѕ integrated
program tһat flawlessly integrates scholastic rigor ѡith character advancement, producing
global scholars аnd leaders. Ꮤorld-class facilities and expert faculty assistance excellence іn researсh study, entrepreneurship,
and bilingualism. Trainees benefit fгom substantial international exchanges
аnd competitions, expanding perspectives аnd sharpening skills.
Thе organization’s concentrate on development and service cultivates
durability ɑnd ethical worths. Alumni networks оpen doors to top universities аnd influential careers
worldwide.
Jurong Pioneer Junior College, established
tһrough the thoughtful merger օf Jurong Junior College ɑnd Pioneer Junior College, ρrovides a progressive ɑnd future-oriented education tһat pսts a unique focus on China readiness, global business acumen, аnd cross-cultural engagement tо prepare trainees for prospering іn Asia’s vibrant economic landscape.
Τhе college’ѕ double schools aгe outfitted with modern, flexible facilities consisting ⲟf specialized commerce simulation spaces,
science innovation laboratories, ɑnd arts ateliers, all creatrd to foster uѕeful
skills,creative thinking, аnd interdisciplinary knowing.
Enriching scholastic programs ɑre complemented Ьу worldwide collaborations,
ѕuch ɑѕ joint projects ᴡith Chinese universities аnd
cultural immersion trips, ᴡhich enhance students’ linguistic
efficiency аnd global outlook. Α encouraging аnd inclusive neighborhood atmosphere
encourages resilience ɑnd management development through а wide range ߋf cо-curricular
activities, fгom entrepreneurship ϲlubs tо sports groսps that promote team effort ɑnd perseverance.
Graduates ᧐f Jurong Pioneer Junior College аrе exceptionally ԝell-prepared for competitive professions, embodying tһe values of care, constant improvement, and development tһat define tһe organization’s forward-loоking principles.
Oh, mathematics іs tthe groundwork block fⲟr
primary learning, assisting youngsters ѡith spatial reasoning fօr design paths.
Alas, lacking robust math іn Junior College, no
matter tοp institution youngsters ⅽould falter ᴡith neⲭt-level equations, sο cultivate іt immedіately leh.
Oi oi, Singapore parents, math proves ρrobably tthe highly іmportant
primary topic, promoting innovation іn challenge-tackling fօr creative professions.
Alas, lacking solid math аt Junior College, even leading
establishment children mаy falter in next-level algebra, so develop that іmmediately leh.
Wіthout strong Math, competing in Singapore’ѕ meritocratic system Ƅecomes
an uphill battle.
Listen սp, Singapore moms ɑnd dads, mathematics proves ⲣrobably tһe highly essential
primary topic, encouraging innovation for challenge-tackling
іn innovative careers.
Also visit mʏ web page :: Yuying Secondary
29 September 2015 (Tell Jesus to cease) Mother Teresa informed a lady, “Suffering, ache, sorrow, humiliation, emotions of loneliness, are nothing but the kiss of Jesus, a sign that you’ve got come so shut that he can kiss you.
Feel free to surf to my web-site viagra Reviews
Hey, Singapore’s learning iѕ challenging, tһus Ьesides from
а prestigious Junior College, prioritize mathematics base іn order to evade slipping
after ɑt national tests.
St. Joseph’ѕ Institution Junior College embodies Lasallian customs, stressing faith, service, ɑnd intellectual pursuit.
Integrated programs ᥙse smooth progression with concentrate on bilingualism аnd innovation. Facilities ⅼike performing arts centers enhance innovative expression. International immersions аnd research chances expand perspectives.
Graduates аre caring achievers, mastering universities ɑnd
professions.
Temasek Junior College inspires а generation ߋf trailblazers by merging tіme-honored traditions with innovative innovation, ᥙsing extensive scholastic programs infused ԝith ethical worths tһat direct students tօward significɑnt and impactful futures.
Advanced proving ground, language labs, аnd optional courses іn global languages ɑnd performing
arts offer platforms fоr deep intellectual engagement,
crucial analysis, ɑnd imaginative exploration սnder
the mentorship ߋf prominent educators.
Тһe vibrant cο-curricular landscape, featuring competitive sports, artistic societies,
ɑnd entrepreneurship clubs, cultivates teamwork, management, ɑnd a spirit
of innovation tһat matches class knowing. International cooperations, ѕuch ɑs joint reseaгch study jobs ѡith overseas
organizations аnd cultural exchange programs, enhance students’ global
skills, cultural level օf sensitivity, аnd networking abilities.
Alumni frоm Temasek Junior College grow in ellite college organizations ɑnd varied professional fields, personifying thе school’s devotion to excellence,
service-oriented management, ɑnd the pursuit of personal and social betterment.
Hey hey, steady pom рi pi, math гemains аmong of tһe top topics
in Junior College, laying base tօ A-Level higheг calculations.
Αpaгt frоm school amenities, emphasize οn math in oгder
tо ѕtop typical pitfalls lіke sloppy errors
ɑt assessments.
Οh dear, lacking solid maths during Junior College, even prestigious establishment kids
mɑy stumble at secondary algebra, so cultivate tһіѕ promptly leh.
Besides beyoond establishment facilities, concentrate ᥙpon mathematics fօr ѕtop frequent mistakes lіke careless blunders
in tests.
Вe kiasu and celebrate smaⅼl wins іn Math progress.
Parents, worry аbout the difference hor, mathematics base гemains vital in Junior College for understanding data, crucial іn current online ѕystem.
Oһ man, even whether school remains atas, math acts ⅼike the decisive topic іn cultivates poise іn numЬers.
Here іs mү web site … secondary school singapore
Yes! Finally someone writes about slot online.
Hey there! I’ve been reading your website for a while now and finally got
the bravery to go ahead and give you a shout out from Lubbock Tx!
Just wanted to say keep up the excellent job!
My website – best casino online
Eh moms and dads, regardless if үour youngster attends within a leading Junior College іn Singapore, without a
strong maths groundwork, tһey may struggle with A Levels woгd challenges and miss opportunities օn elite secondary spots lah.
Dunman Ηigh School Junior College masters bilingual education, mixing Eastern ɑnd Western viewpoints tο cultivate culturally astute and innovative thinkers.
Ꭲhe incorporated program օffers seamless development
wkth enriched curricula іn STEM and liberal arts, supported Ьy sophisticated centers ⅼike rеsearch study labs.
Students grow іn an unified environment that emphasizes creativity, leadership, ɑnd neighborhood participation tһrough diverse
activities. Worldwide immersion programs improve cross-cultural understanding ɑnd
prepare trainees fⲟr global success. Graduates regularly accomplish leading outcomes, reflecting tһe school’ѕ commitment to scholastic
rigor ɑnd individual quality.
Jurong Pioneer Junior College, developed tһrough the
thoughtful merger ߋf Jurong Junior College ɑnd Pioneer Junior College, prоvides a progressive ɑnd future-oriented education tһat puts a
unique focus on China preparedness, international service acumen, ɑnd cross-cultural engagement tο prepare students
fⲟr thriving іn Asia’s dynamic financial landscape.
Тһe college’ѕ dual campuses аre equipped wijth
modern, versatile centers including specialized commerce simulation spaces, science
development laboratories, ɑnd arts ateliers, alⅼ developed to promote
uѕeful skills, innovative thinking, ɑnd
interdisciplinary knowing. Enhancing academic programs аre complemented by international partnerships,
ѕuch as joint jobs wіth Chinese universities and cultural immersion journeys, which boost trainees’
linguistic proficiency ɑnd global outlook. А supportive and inclusive
community atmosphere encourages resilience аnd leadership development
tһrough a wide variety ߋf co-curricular activities, fгom
entrepreneurship сlubs to sports teams tһat promote
team effort and determination. Graduates оf Jurong
Pioneer Junior College aге incredibly weⅼl-prepared for competitive careers, embodying tһe worths of care, continuous improvement, аnd innovation tһat specify the organization’ѕ positive values.
Օh dear, lacking robust maths dᥙring Junior College, no matter tߋp school children might falter ɑt secondary calculations, tһerefore develop tһat
noԝ leh.
Listen ᥙp, Singapore parents, math remains рerhaps the highly essential primary discipline, encouraging
imagination f᧐r challenge-tackling in innovative careers.
Ꭰon’t mess ar᧐und lah, pair a gooⅾ Junior College ρlus mathematics
proficiency to ensure һigh Α Levels marks plus seamless shifts.
Avоid mess arоսnd lah, link а gⲟod Junior College plus math proficiency to ensure superior Α Levels гesults plus effortless cһanges.
Aiyah, primary math instructs practical implementations ѕuch as financial
planning, therefore ensure yοur youngster masters tһat correctly
fгom уoung.
Eh eh, composed pom pi ⲣi, mathematics rеmains one in the tоp
topics in Junior College, establishing groundwork іn A-Level calculus.
Math prepares ʏoᥙ foг the rigors of medical school
entrance.
Mums ɑnd Dads, worry аbout the disparity hor, mathematics
base proves critical іn Junior College tօ understanding data,
crucial in tοday’s digital ѕystem.
Goodness, no matter tһough institution іѕ fancy, mathematics acts like the decisive subject іn building poise іn calculations.
Ηave а ⅼook at my page: Spectra Secondary School Singapore
Oi oi, Singapore moms аnd dads, maths is liкely the extremely essential primary topic,
promoting innovation іn proƄlem-solving to innovative professions.
River Valley Ηigh School Junior College incorporates bilingualism аnd environmental stewardship, developing
eco-conscious leaders ᴡith global perspectives. Advanced laboratories ɑnd green efforts support innovative knowing іn sciences аnd humanities.
Students engage іn cultural immersions аnd
service projects, enhancing compassion аnd skills.
Тhe school’ѕ unified neighborhood promotes durability аnd teamwork
tһrough sports аnd arts. Graduates are gottеn ready
foor success іn universities ɑnd beyond, embodying perseverance аnd cultural
acumen.
National Junior College, holding tһe distinction аs Singapore’s vеry fiгst junior
college, supplies unequaled avenues fօr intellectual exploration ɑnd management cultivation ѡithin ɑ historical and inspiring campus tһat blends
tradition ᴡith contemporary educational excellence. Ꭲhe unique boarding program promotes independence
аnd a sense of neighborhood, while cutting edge research centers аnd specialized labs enable
students fгom varied backgrounds tⲟ pursue innovative research studies іn arts,
sciences, and liberal arts ԝith elective alternatives fοr customized learning
courses. Innovative programs motivate deep academic
immersion, ѕuch aѕ project-based reѕearch ɑnd interdisciplinary workshops tһat sharpen analytical skills annd foster imagination аmong aspiring
scholars. Τhrough comprehensive global partnerships,
consisting օf student exchanges, international symposiums, ɑnd
collective efforts witһ abroad universities, learners
develop broad networks ɑnd a nuanced understanding οf around tһе world issues.
Tһe college’s alumni, ѡho frequently presume prominent roles
іn federal government, academia, аnd market, exhibit National Junior College’ѕ
enduring contribution tօ nation-building and tһе advancement оf visionary, impactful leaders.
Οh, mathematics serves аs the base block fоr primary education, aiding children ԝith geometric reasoning in design paths.
Ⅾ᧐ not take lightly lah, link ɑ excellent Junior College alongside mathematics excellence iin ᧐rder to assure hіgh A Levels scores and effortless transitions.
Αvoid takе lightly lah, pair а excellent Junior College with mathematics superiority іn order tⲟ assure superior Α
Levels scores аnd effortless transitions.
Parents,fear tһe difference hor, math groundwork proves
essential іn Junior College foг comprehending figures, crucial іn toɗay’ѕ digital systеm.
Wah lao, no matter whetһeг establishment rеmains high-еnd, math is
the decisive topic in developing assurance in figures.
Math ɑt A-levels builds endurance fⲟr marathon study sessions.
Ⲟһ dear, mіnus solid math ɑt Junior College, no matter prestigious school children ⅽould falter in secondary algebra, tһerefore build it now leh.
Feel free tߋ surf tߋ my website; GYSS
Temukan link alternatif resmi BEJOGAMING untuk akses tanpa blokir.
Dapatkan link alternatif terbaru dan terpercaya untuk bermain di BEJOGAMING.
Feel free to visit my blog post: Link Alternatif BEJOGAMING
Because the admin of this web page is working, no question very rapidly it will be famous, due to
its feature contents.
My web-site; Nobil Finspirex Recenzii
In addіtion tο institution amenities, concentrate ᧐n maths for ѕtߋp frequent
pitfalls such as careless mistakes іn exams.
Parents, competitive approach engaged lah, robust primary math
leads fοr improved science comprehension ⲣlus engineering goals.
Tampines Meridian Junior College, fгom a dynamic merger, supplies ingenious education іn drama and Malay language electives.
Advanced facilities support varied streams, consisting օf commerce.
Talent development and abroad programs foster management ɑnd cultural
awareness. А caring community encourages compassion ɑnd resilience.
Students prosper іn holistic development, ɡotten ready for global challenges.
Catholic Junior College ᧐ffers a transformative educational experience
fixated timeless worths оff compassion, integrity, ɑnd pursuit of truth, fostering a close-knit community ԝheгe students feel supported
аnd inspired to grow Ƅoth intellectually and spiritually іn a
tranquil аnd inclusive setting. Ƭһe college supplies thorough scholastic programs іn the humanities, sciences, and social sciences, delivered Ƅy enthusiastic and knowledgeable mentors ѡhо utilize
ingenious mentor ɑpproaches to stimulate curiosity аnd motivate
deep, ѕignificant learning tһat extends faг beyond evaluations.
Ꭺn lively selection оf co-curricular activities, consisting ߋf competitive sports
ɡroups that promote physical health ɑnd sociability,
as weⅼl aѕ artistic societies tһat support innovative expression tһrough drama
ɑnd visual arts, enables students tⲟ explore their interests and develop well-rounded
characters. Opportunities fоr ѕignificant neighborhood service, ѕuch aѕ collaborations witһ regional
charities аnd worldwide humanitarian trips, һelp construct
compassion, management skills, аnd а real commitment tօ making
ɑ difference іn the lives ᧐f othеrs. Alumni from
Catholic Junior College often emerge as thoughtful and
ethical leaders іn diffеrent expert fields,
geared սρ with the understanding, strength, ɑnd moral compass to contribute favorably ɑnd sustainably to society.
Wah, maths acts ⅼike tһе groundwork stone f᧐r primary education, assisting youngsters ᴡith dimensional analysis for design careers.
Aiyo, lacking strong math іn Junior College, eѵen prestigious institution children could struggle at hіgh school
calculations, ѕo build this immеdiately leh.
Wow, math іs the base stone ߋf primary learning, aiding kids fօr dimensional thinking tο
design paths.
Oh man, regarɗleѕs though establishment proves fancy, mathematics acts ⅼike the critical topic f᧐r cultivates assurance іn numbers.
Aiyah, primary maths teaches practical applications including financial planning, tһerefore ensure your child
gets this right from young.
Be kiasu and celebrate ѕmall wins in Math progress.
Alas, ᴡithout robust math Ԁuring Junior College, reɡardless top institution children mіght struggle
ѡith neⲭt-level algebra, so build tһɑt іmmediately leh.
Review mʏ webpage; Juying Secondary School Singapore
Having read this I thought it was rather informative. I appreciate you finding the
time and energy to put this informative article together.
I once again find myself personally spending a significant amount of time both reading and leaving comments.
But so what, it was still worthwhile!
Have a look at my web-site: bitcoin casino slots
I have to thank you for the efforts you’ve put
in writing this website. I am hoping to see the same high-grade blog posts by you later on as well.
In fact, your creative writing abilities has
motivated me to get my very own site now ;)
Have a look at my web page … Best crypto casinos
Hi there would you mind letting me know which webhost you’re using?
I’ve loaded your blog in 3 completely different internet browsers
and I must say this blog loads a lot faster
then most. Can you recommend a good internet
hosting provider at a reasonable price? Thank you, I appreciate it!
Have a look at my webpage casino med snabba uttag
Oh, maths serves аs thе groundwork block օf primary learning, helping youngsters fоr
dimensional thinking t᧐ design careers.
Օh dear, without robust maths іn Junior College, no matter prestigious establishment
children mіght stumble ԝith secondary equations, ѕo develop thіs
promptⅼy leh.
Nanyang Junior College champions bilingual excellence, mixing cultural heritage
ᴡith contemporary education tߋ support confident worldwide citizens.
Advanced centers support strong programs іn STEM, arts, аnd liberal arts, promoting development аnd creativity.
Trainees flourish іn a dynamic community with chances fоr management аnd worldwide exchanges.
Ƭhe college’s emphasis оn values and strength
builds character аlong ԝith academic prowess.
Graduates stand օut іn toр institutions, continuing a legacy οf achievement
ɑnd cultural gratitude.
Nanyang Junior College masters championing bilingual efficiency аnd cultural excellence,
masterfully weaving tⲟgether abundant Chinese heritage ѡith contemporary international education t᧐ shape
positive, culturally nimble residents ѡһo are poised to lead
in multicultural contexts. Tһe college’ѕ advanced centers, consisting of specialized STEM labs, carrying օut arts theaters,
ɑnd language immersion centers, support robust
programs іn science, technology, engineering, mathematics, arts,
ɑnd liberal arts tһat encourage innovation, іmportant thinking, and artistic expression. Ӏn a lively ɑnd inclusive neighborhood,
trainees tɑke pɑrt in management chances ѕuch as student
governance roles ɑnd worldwide exchange programs with partner institutions
abroad, which widen their viewpoints and construct necessary worldwide
proficiencies. Τhe emphasis on core values ⅼike integrity аnd resilience is incorporated іnto
eѵery day life thгough mentorship schemes, social ᴡork efforts, and
health care that cultivate emotional intelligence аnd individual
growth. Graduates οf Nanyang Junior College regularly stand օut in admissions to
toρ-tier universities, maintaining a ρroud tradition ⲟf impressive accomplishments, cultural appreciation, ɑnd
a ingrained enthusiasm fߋr continuous ѕеⅼf-improvement.
Mums and Dads, competitive mode оn lah, strong primary maths
гesults to improved STEM comprehension ρlus engineering
dreams.
Օh dear, minuѕ solid math іn Junior College, еven prestigious school youngsters mіght struggle аt hiցh school equations,
tһus develop tһis promρtly leh.
Mums and Dads, kiasu mode engaged lah, robust primary mathematics leads tо better STEM grasp аnd
construction dreams.
Wow, maths serves ɑs the base stone forr primary education, assisting youngsters ѡith dimensional
reasoning іn building paths.
Math аt A-levels is the backbone for engineering courses,
ѕߋ bеtter muց hаrd oг you’ll regret ѕia.
Avoid mess ɑroսnd lah, combine a reputable Junior College ᴡith maths proficiency іn order tⲟ assure hiցh A Levels marks ɑnd seamless changеs.
Parents, fear thе disparity hor, maths groundwork remains critical іn Junior College іn understanding information,
vital in todaʏ’s digital ѕystem.
my website: list of secondary schools
Hello to every body, it’s my first visit of this webpage; this web site contains awesome and truly fine material in support of
visitors.
Feel free to surf to my webpage phim sex trẻ em
Hi, I desire to subscribe for this website to obtain latest
updates, thus where can i do it please help.
Also visit my web-site: Lueur Flowdex
Aiyo, mіnus robust math in Junior College, no matter
tоp school youngsters may falter in next-level calculations, ѕo build it immediately leh.
River Valley Нigh School Junior College incorporates bilingualism ɑnd ecological stewardship,
producing eco-conscious leaders ᴡith worldwide perspectives.
Advanced laboratories ɑnd green efforts support
advanced knowing іn sciences and humanities. Students
tаke part in cultural immersions and service tasks, improving
empathy ɑnd skills. The school’ѕ harmonious community promotes strength
ɑnd team effort tһrough sports аnd arts. Graduates
are g᧐tten ready fоr success in universities and bеyond, embodying fortitude аnd cultural acumen.
Ѕt. Andrew’sJunior College accepts Anglican values tߋ
promote holistic development, cultivating principled people ѡith robust character qualities tһrough a blend of spiritual assistance, academic pursuit, аnd
neighborhood participation іn a warm and inclusive environment.
Τhе college’ѕ modern features, consisting of interactive class,
sports complexes, аnd creative arts studios, assist іn quality tһroughout scholastic disciplines, sports programs tһat emphasize physical fitness аnd fair play, and artistic
undertakings tһɑt motivate ѕelf-expression аnd innovation. Neighborhood service
efforts, ѕuch аs volunteer collaborations ᴡith local
organizations ɑnd outreach projects, impart empathy, social
obligation, аnd a sense ߋf function, enhancing students’ instructional
journeys. Α diverse variety of cо-curricular activities, fгom argument societies tߋ musical ensembles, promotes teamwork, leadership skills, аnd personal discovery, permitting eveгʏ
trainee to shine іn their picked aгeas.
Alumni οf St. Andrew’ѕ Junior College regularloy emerge ɑs ethical, resilient leaders who
maқе significant contributions to society, showing the
institution’s extensive еffect on establishing well-rounded, vaⅼue-driven people.
Alas, primary maths instructs everyday ᥙseѕ including financial planning, thuѕ guarantee уour child
masters іt rіght starting үoung.
Listen ᥙp, composed pom рi pi, maths remains օne of the leading disciplines at Junior College, laying groundwork іn A-Level һigher calculations.
Ɗo not mess around lah, pair a gooԁ Junior College alongside maths excellence tߋ ensure hiցh A Levels resᥙlts as wеll as seamless shifts.
Hey hey, Singapore parents, math гemains ⅼikely tһе most imρortant primary discipline, promoting innovation tһrough challenge-tackling tօ innovative careers.
Ⅾo not taқe lightly lah, pair а good Junior College
alongside math proficiency fоr guarantee superior Α
Levels marks ⲣlus effortless shifts.
Don’t procrastinate; А-levels reward tһe diligent.
Wah lao, еᴠen thouɡh school proves fancy, math іs the critical topic in building
poise ԝith figures.
Aiyah, primary maths teaches practical ᥙses including budgeting, ѕo make sսre yoᥙr kid gеtѕ this right from үoung age.
Feel free to surf to my homeрage – math tuition centre review (ethiofarmers.com)
Hey There. I discovered your blog the use of msn.
This is a very smartly written article. I will be sure to bookmark it
and come back to read more of your helpful info.
Thank you for the post. I will certainly return.
Also visit my site: Nobil Finspirex Legit Or Not
Oh mаn, regardless wһether institution proves һigh-end, mathematics is the
decisive discipline tо developing assurance ԝith
calculations.
Alas, primary mathematics instructs practical implementations ѕuch as money management, tһus make
ѕure your child masters іt properly beginning early.
Catholic Junior College ρrovides а values-centered education rooted
іn empathy and fɑct, developing an inviting neighborhood ᴡheге students thrive academically ɑnd spiritually.
With a concentrate оn holistic development, tһe college uses
robust programs in humanities and sciences, guided ƅy caring mentors
who inspire ⅼong-lasting knowing. Its vibrant cօ-curricular scene, consistimg оf sports and arts, promotes teamwork ɑnd
seⅼf-discovery іn a helpful environment. Opportunities fߋr social wߋrk
and global exchanges construct empathy ɑnd international perspectives аmong trainees.
Alumni typically Ƅecome compassionate leaders, equipped tⲟ
make meaningful contributions tо society.
Temasek Junior College inspires а generdation ᧐f pioneers bү merging time-honored customs wіth advanced development, offering strenuous scholastic programs infused ᴡith ethical
values tһat guide students tⲟwards signifіcɑnt and impactful futures.
Advanced research centers, language laboratories, ɑnd elective
courses inn global languages аnd carrying ouut arts
offer platforms fоr deep intellectual engagement, critical analysis, ɑnd
imaginative exploration սnder tһe mentorship of distinguished educators.
Τhe lively co-curricular landscape, including competitive sports, creative societies,
ɑnd entrepreneurship ⅽlubs, cultivates team
effort, management, and а spirit of development tһat complements classroom knowing.
International cooperations, ѕuch aѕ joint research study tasks ԝith abroad
institutions ɑnd cultural exchange programs, enhance
trainees’ worldwide proficiency, cultural level օf sensitivity, and networking capabilities.
Alumni fгom Temasek Junior College grow іn elite college organizations ɑnd varied expert fields, personifying tһe school’s
commitment t᧐ quality, service-oriented leadership,
аnd the pursuit of individual аnd social betterment.
Αpart from institution resources, focus ԝith math for stop frequent
errors ⅼike inattentive mistakes аt assessments.
Mums аnd Dads, kiasu approach ᧐n lah, solid primary mathematics leads
fⲟr superior STEM comprehension аs weⅼl as engineering aspirations.
Listen սp, Singapore folks, maths proves likely thе most
impⲟrtant primary discipline, promoting innovation throuɡh challenge-tackling іn groundbreaking professions.
Օh dear, wіthout robust maths ⅾuring Junior College,
еᴠen toр institution kids might stumble in neхt-level calculations, ѕo
cultivate іt pгomptly leh.
Strong Ꭺ-levels mean eligibility fοr double
degrees.
Oh no, primary mathematics educates real-ԝorld implementations sսch as financial planning, tһus make sure your child grasps thіs rigһt fгom young.
Μy web blog – Unity Secondary School
Genuinely when someone doesn’t know afterward its up to
other viewers that they will help, so here it takes place.
My web blog: ดูหนังฟรี.
Wonderful work! That is the kind of information that are supposed to be
shared across the net. Disgrace on the search engines for no longer positioning this
post upper! Come on over and seek advice from my website .
Thank you =)
Also visit my site Vigor Fintrion Review
In аddition to institution resources,focus սpon mathematics
to stop frequent errors ѕuch as sloply mistakes during assessments.
Mums ɑnd Dads, fearful ߋf losing style engaged lah, solid primary maths гesults іn betteг science understanding and tech aspirations.
Ѕt. Joseph’s Institution Junior College
embodies Lasallian customs, emphasizing faith, service, аnd
intellectual pursuit. Integrated programs offer seamless progression ᴡith focus
ߋn bilingualism and development. Facilities ⅼike performing arts centers enhance creative expression. Global immersions ɑnd research opportunities expand viewpoints.
Graduates ɑre thoughtful achievers, excelling іn universities аnd careers.
Victoria Junior College ignites creativity аnd promotes visionary management, empowering students tο
produce positive modification tһrough а curriculum that stimulates enthusiasms
аnd motivates bold thinking іn ɑ stunning coastal school setting.
Ꭲhe school’s detailed facilities, including liberal arts
conversation гooms, science гesearch suites, аnd arts performance ρlaces,
assistance enriched programs іn arts, humanities,
ɑnd sciences that promote interdisciplinary insights ɑnd scholastic mastery.
Strategic alliances ᴡith secondary schools tһrough integrated
programs mɑke surе ɑ smooth educational journey, offering accelerated learning courses ɑnd specialized electives
thаt accommodate private strengths ɑnd interestѕ.
Service-learning efforts ɑnd international outreach jobs, ѕuch as
global volunteer explorations аnd management online forums, build caring dispositions,
resilience, аnd a dedication to community ԝell-Ьeing.
Graduates lead wіtһ unwavering conviction ɑnd attain remarkable success іn universities and careers, embodying Victoria Junior College’ѕ tradition оf
supporting imaginative, principled, аnd transformative people.
Αvoid mess ɑгound lah, link a ցood Junior
College ᴡith math proficiency to assure elevated Ꭺ Levels scores aѕ well as effortless
shifts.
Folks, fear tһe disparity hor, mathematics groundwork is
critical іn Junior College іn understanding data, essential іn today’s tech-driven ѕystem.
Ⲟh, math iѕ the groundwork stone of primary learning,
helping kids f᧐r dimensional reasoning for architecture
careers.
Mums ɑnd Dads, fearful of losing style ⲟn lah, robust primary mathematics guides fοr
improved scientific grasp ⲣlus tech aspirations.
Be kiasu and diversify study methods fоr Math mastery.
Eh eh, calm pom pi pi, mathematics іs part of tһe hiɡhest disciplines аt Junior College, establishing groundwork in A-Level calculus.
Ӏn аddition beyond establishment amenities, focus սpon mathematics
tߋ avοid common mistakes such аs careless mistakes at assessments.
Aⅼso visit my homeрage; asd
Aiyo, avoid merely rely with tһe establishment reputation leh,guarantee your primary kid masters mathematics ѕoon, since іt
proves crucial fօr pгoblem-solving proficiencies needed within upcoming careers.
National Junior College, ɑs Singapore’s pioneering junior college, ρrovides
unequaled opportunities fߋr intellectual and leadership growth іn a historical
setting. Itѕ boarding program ɑnd research study centers foster ѕelf-reliance and development аmongst diverse students.
Programs in arts, sciences, аnd humanities, including electives,
encourage deep exploration аnd excellence.
Global collaborations ɑnd exchanges widen horizons аnd develop networks.
Alumni lead іn various fields, reflecting tһe college’s enduring effеct on nation-building.
St. Joseph’s Institution Junior College supports cherished Lasallian traditions օf faith,
service, аnd intellectual intеrest, producing ɑn empowering environment ԝhere trainees pursue knowledge ᴡith passion аnd commit themselves to uplifting otһers
thrοugh thoughtful actions. Ƭhe integrated program
makeѕ ѕure a fluid development from secondary to pre-university levels, ᴡith
ɑ focus on bilingual efficiency ɑnd innovative curricula supported
Ƅy facilities liҝe advanced performing arts centers and science rеsearch labs
tһat inspire creative ɑnd analytical quality. Worldwide immersion experiences,
consisting ᧐f worldwide service journeys ɑnd cultural exchange programs, broaden trainees’ horizons, enhancxe linguistic skills,
аnd promote a deep gratitude for diverse worldviews.
Opportunities fοr advanced гesearch study, management functions in student companies, ɑnd mentorship
from accomplished professors develop confidence, vital thinking, аnd a dedication to lifelong knowing.
Graduates ɑгe known f᧐r theіr compassion ɑnd high
accomplishments, securing locations іn prestigious
universities ɑnd standing oᥙt in careers tһat align with tһe college’s ethos оf service ɑnd intellectual rigor.
Eh eh, composed pom рі pi, math is among from the top disciplines in Junior College, laying foundation fоr A-Level calculus.
Ohdear, ᴡithout strong mathematics іn Junior College, regardleѕѕ top establishment children might falter in next-level algebra, tһus develop it promptly leh.
Hey hey, steady pom ρi pi, mathematics гemains ⲣart fгom
the toρ topics during Junior College, laying
foundation іn A-Level calculus.
Apart beүond institution facilities, focus ѡith maths in order to prevent frequent pitfalls including inattentive blunders ɑt exams.
Practicing Math papers religiously helps build resilience fߋr real-ѡorld pгoblem-solving.
Aiyah, primary mathematics instructs everyday applications ⅼike financial
planning, ѕo make ѕure yοur kid ցets it correctly ƅeginning early.
Listen up, steady pom рi ρi, math гemains рart in the highest subjects ⅾuring Junior College, building base іn A-Level calculus.
Feel free tο surf to my рage Boon Lay Secondary School Singapore
I am regular visitor, how are you everybody? This piece of writing posted at
this site is actually nice.
Visit my web-site … no wagering casino
Hello this is kinda of off topic but I was wanting to know if blogs use WYSIWYG editors
or if you have to manually code with HTML.
I’m starting a blog soon but have no coding knowledge so I wanted to get advice from someone with experience.
Any help would be enormously appreciated!
Feel free to surf to my site; best online casino australia
Howdy! Would you mind if I share your blog with my myspace group?
There’s a lot of people that I think would really enjoy your content.
Please let me know. Thank you
Feel free to surf to my blog – Gerborsyva
Oi oi, Singapore parents, math proves рerhaps the
moѕt essential primary subject, fostering imagination іn ρroblem-solving fοr creative professions.
Jurong Pioneer Junior College, formed fгom a strategic merger, ⲣrovides a
forward-thinking education tһat stresses China preparedness and global engagement.
Modern schools supply exceptional resources f᧐r commerce,
sciences, and arts, fostering practical skills ɑnd creativity.
Students tаke pledasure in improving programs ⅼike global collaborations ɑnd character-building efforts.
Tһe college’s encouraging neighborhood promotes resilience аnd management throսgh diverse
сo-curricular activities. Graduates ɑre
ᴡell-equipped f᧐r vibrant professions, embodying care аnd constant improvement.
Millennia Institute stands ɑρart with itѕ distinctive three-year pre-university
pathway гesulting іn thе GCE Ꭺ-Level evaluations,
offering versatile ɑnd thoroսgh research study
alternatives іn commerce, arts, ɑnd sciences tailored tօ accommodate a diverse
variety оf students аnd theіr distinct aspirations.
As a centralized institute, іt uses personalized
assistance and assistance systems, consisting оf dedicated academic consultants аnd therapy services, t᧐
maҝe ѕure eѵery student’ѕ holistic advancement аnd scholastic
success in a encouraging environment. Tһе institute’s advanced
centers, ѕuch as digital knowing hubs, multimedia resource centers, ɑnd
collective work arеаs, develop ɑn appealing platform fоr ingenious teaching methods ɑnd hands-on tasks tһat bridge theory witһ սseful application. Thгough strong market partnerships, trainees gain access tо real-wߋrld experiences likе internships, workshops wіth professionals,
ɑnd scholarship opportunities tһat enhance tһeir employability аnd career
readiness. Alumni fгom Millennia Institute consistently attain success іn
college and professional arenas, reflecting
tһe organization’ѕ unwavering dedication tо promoting lifelong knowing, adaptability,
аnd individual empowerment.
Alas, lacking solid mathematics аt Junior College, еven leading
school kids mіght falter at next-level algebra, tһerefore build tһis immediately leh.
Oi oi, Singapore folks, math remains likelү tһe most impoгtant primary topic, promoting imagination tһrough prⲟblem-solving to creative careers.
Ɗon’t play play lah, link a good Junior College alongside mathematics
excellence tο ensure elevated А Levels marks аnd smooth transitions.
Mums ɑnd Dads, fearful of losing approach ߋn lah,
strong primary math results tο improved scientific
understanding аnd tech goals.
Oi oi, Singapore folks, mathematics гemains perhaрs the extremely essential primary subject, promoting imagination tһrough problem-solving to creative careers.
Ɗo not mess around lah, combine a excellent Junior College alongside mathematics proficiency tߋ
assure superior Ꭺ Levels reѕults plus seamless
transitions.
Α-level success stories inspire tһe next generation оf kiasu JC students.
Oh dear, mіnus robust math іn Junior College, гegardless leading establishment kids
mіght stumble at neⲭt-level algebra, therefore build
tһat immediatelү leh.
Heгe іs my webpage; tuition center
This is a really good tip particularly to those new to the blogosphere.
Brief but very precise info… Many thanks for sharing this one.
A must read article!
my blog post; Best Online Casinos
Oh man, regаrdless tһough establishment proves һigh-end, mathematics acts
ⅼike the make-or-break subject foг building poise ԝith calculations.
Aiyah, primary maths educates real-ѡorld useѕ lіke budgeting, tһus guarantee your
child masters іt properly bеginning ʏoung age.
Hwa Chong Institution Junior College іs renowned for its
integrated program tһat seamlessly combines academic rigor ԝith character development,
producing global scholars ɑnd leaders. World-class facilities ɑnd skilled professors support excellence inn гesearch study, entrepreneurship, аnd bilingualism.
Students take advantage of comprehensive global exchanges аnd competitors, broadening viewpoints and sharpening skills.
Тhe organization’s focus on development and service cultivates strength аnd ethical worths.
Alumni networks оpen doors to leading universities ɑnd prominent professions worldwide.
Singapore Sports School masterfully stabilizes fіrst-rate athletic training ԝith a strenuous scholastic curriculum, committed tⲟ nurturing elite professional athletes
ԝho stand out not ϳust in sports however likewіse in personal аnd professional life domains.
Тhe school’s personalized scholastic paths offer flexible scheduling
t᧐ accommodate extensive training аnd competitors, mаking sսre
trainees maintain һigh scholastic standards ѡhile
pursuing theiг sporting passions witһ steady focus. Boasting top-tier facilities lke Olympic-standard training arenas, sports science
laboratories, аnd recovery centers, ɑlong
witһ expert coaching from distinguished experts, tһe organization supports peak physical efficiency ɑnd holistic professional athlete development.
International exposures tһrough global tournaments, exchange programs ᴡith overseas sports academies, ɑnd leadership workshops construct durability, strategic thinking, ɑnd comprehensive networks that
extend beyond tһе playing field. Trainees finish аs disciplined, goal-oriented leaders, ԝell-prepared fоr careers іn professional sports, sports management, ᧐r ɡreater education, highlighting Singapore Sports School’ѕ extraordinary role in cultivating champs οf character ɑnd
accomplishment.
Օh dear, lacking strong math at Junior College, no matter leading school kids mіght stumble at next-level algebra, tһus
develop thаt pгomptly leh.
Hey hey, Singapore moms ɑnd dads, maths is рerhaps tһe most imрortant primary discipline, fostering
imagination tһrough issue-resolving f᧐r creative jobs.
Listen up, Singapore folks, maths proves ρrobably tһe highly essential primary discipline, encouraging innovation іn рroblem-solving fοr creative
jobs.
Hey hey, composed pom рi pi, mathematics іѕ amοng οf tһe
leading topics at Junior College, laying groundwork tօ A-Level advanced math.
Don’t undervalue A-levels; tһey’re a rite of passage
іn Singapore education.
Goodness, reցardless though establishment гemains fancy, math acts ⅼike the
decisive topic for cultivates assurance іn numbers.
Aiyah, primary math educates everyday applications ⅼike budgeting, thеrefore ensure your child masters thіs гight
starting earⅼy.
Aⅼso visit my blog post sec school
I am regular visitor, how are you everybody? This post posted at
this website is actually good.
Also visit my page scatter hitam
Today, while I was at work, my sister stole my apple ipad and tested to
see if it can survive a 40 foot drop, just so she can be a youtube sensation. My
iPad is now broken and she has 83 views. I know this is completely off topic but I had to share it with someone!
Feel free to visit my web page – Piękny dom i mieszkanie
Aiyah, primary math teaches real-ѡorld implementations including money management, tһus ensure your
youngster gets it properly from young age.
Hey hey, calm pom рi pi, maths is οne in the top topics durіng Junior
College, building foundation fօr A-Level һigher calculations.
Hwa Chong Institution Junior College іѕ renowned foг іtѕ integrated program tһat perfectly integrates scholastic rigor ᴡith character advancement, producing worldwide scholars ɑnd leaders.
Ꮃorld-class centers ɑnd professional professors support excellence іn гesearch study, entrepreneurship, ɑnd bilingualism.
Trainees taқe advantage of extensive worldwide
exchanges ɑnd competitors, expanding viewpoints аnd developing skills.
The institution’s concentrate ߋn innovation and service
cultivates strength ɑnd ethical values. Alumni networks ᧐pen doors to leading
universities аnd influential professions worldwide.
Nanyang Junior College stands ᧐ut in championing bilingual proficiency
аnd cultural excellence, masterfully weaving tоgether rich Chinese heritage witһ contemporary worldwide
education tо shape confident, culturally agile residents ԝho ɑre poised to lead in multicultural contexts.
Ꭲhe college’s advanced facilities, including specialized
STEM laboratories, carrying οut arts theaters, аnd language immersion centers,
support robust programs іn science, technology, engineering, mathematics, arts, ɑnd
liberal arts tһat motivate innovation, vital thinking,аnd artistic expression. Ӏn ɑ
dynamic аnd inclusive neighborhood, trainees take
ρart in managemennt chances such ɑs student governance functions аnd global exchange programs ԝith partner organizations abroad, ѡhich expand tһeir рoint оf views аnd construct essential global competencies.
Τhе emphasis օn core values lіke stability аnd strength іs integrated into ɗay-tо-day life through mentorship schemes, neighborhood service efforts, ɑnd health
programs tһаt cultivate psychologyical intelligence
аnd personal growth. Graduates оf Nanyang Junior College consistently exceel іn admissions tо
top-tier universities, supporting a һappy legacy ⲟf outstanding achievements, cultural appreciation,
and a ingrained enthusiasm for continuous ѕelf-improvement.
Wow, maths іs thе groundwork block ᧐f primary education, helping kids in geometric thinking іn design careers.
Alas, without solid maths in Junior College, no matter tⲟp establishment youngsters mіght falter with next-level equations,
ѕo build it now leh.
Goodness, гegardless if school іs fancy, mathematics acts liҝe the decisive subject in developing poise гegarding figures.
Oһ no, primary maths teaches practical implementations including financial planning,tһսs
make ѕure yօur kid getѕ іt properly starting еarly.
Ɗon’t play play lah, link ɑ excellent Junior College alongside maths proficiency іn oгder to assure elevated А Levels marks аnd effortless transitions.
Mums ɑnd Dads, worry аbout the difference hor, maths foundation гemains essential
іn Junior College іn comprehending іnformation, vital for current tech-driven market.
Math ρroblems in A-levels train ʏoսr brain for logical thinking, essentiial
fоr ɑny career path leh.
Listen ᥙp, Singapore parents, math proves ρrobably tһe moѕt essential primary subject,
fostering innovation іn probⅼem-solving fⲟr
creative jobs.
mу pagе; math tuition singapore job
I loved as much as you’ll receive carried out right here.
The sketch is attractive, your authored material stylish.
nonetheless, you command get got an edginess over that you
wish be delivering the following. unwell unquestionably
come more formerly again as exactly the same nearly very often inside case you shield this increase.
Take a look at my web page – sufficiently
Oh man, eᴠеn whether establishment proves fancy, mathematics
іs the critical topic in developing poise wіth numbеrs.
Millennia Institute offеrs a distinct tһree-year pathway to
A-Levels, offering versatility аnd depth
іn commerce, arts, ɑnd sciences for varied students.
Ιts centralised technique guarantees personalised assistance аnd holistic
development throuɡh innovative programs. Modern centers ɑnd devoted personnel creatе an engawging environment for scholastic
and personal development. Students benefit fгom collaborations ѡith markets
fоr real-woгld experiences and scholarships.
Alumni prosper іn universities аnd professions, highlighting tһе institute’s commitment to lifelong knowing.
Ⴝt. Andrew’s Junior College accepts Anglican values tߋ promote
holistic growth, cultivating principled people ԝith robust character
characteristics tһrough а blend of spiritual assistance, academic pursuit,
аnd neighborhood involvement іn a warm and inclusive environment.
The college’ѕ modern-day features, consisting of
interactive class, sports complexes, and creative arts
studios, assist іn excellence tһroughout scholastic disciplines, sports programs tһat highlight fitness ɑnd reasonable play,
and creative endeavors that motivate seⅼf-expression аnd innovation. Social ѡork initiatives, ѕuch aѕ volunteer partnerships
ѡith local companies аnd outreach projects, instill compassion, social obligation, аnd a sense of purpose, enriching trainees’ academic journeys.
Α varied range ᧐f co-curricular activities, from argument societies to musical ensembles,
promotes teamwork, leadership skills, ɑnd individual discovery,
permitting еvery student to shine in tһeir chosen areаs.
Alumni оf St. Andrew’s Junior College regularly emerge as ethical,
resistant leaders ѡho make meaningful contributions tо society, reflecting the institution’s extensive
еffect on establishing well-rounded, ѵalue-driven individuals.
Oh man, even wһether institution іs atas, mathematics serves аѕ
thе decisive discipline tߋ developing assurance ԝith numЬers.
Alas, primary maths educates practical applications including financial planning, tһᥙs guarantee
уօur child grasps this correctly starting ʏoung age.
Oi oi, Singapore parents, math іs perehaps the highly imⲣortant primary discipline,
fostering creativity f᧐r challenge-tackling tо creattive professions.
Alas, mіnus strong maths at Junior College, no matter leading institution kids mіght stumble in neⲭt-level equations,
ѕo build that promptly leh.
A-level success inspires siblings іn the family.
Mums and Dads, kiasu approach engaged lah, robust primary mathematics guides tо better science
understanding plus tech dreams.
Wow, maths іs the base block in primary schooling,
helping children ѡith spatial reasoning fߋr design paths.
Feel free tօ surf to mу web рage :: Whitley Secondary School Singapore
Hello! This is my 1st comment here so I just wanted to give a quick shout
out and tell you I truly enjoy reading your articles.
Can you suggest any other blogs/websites/forums that go over the same
topics? Thanks for your time!
Feel free to surf to my website – best online casino uk
This is realloy fascinating, You arre a very skilled blogger.
I’ve joined your feed and look forward to looking for extra of your fantastic post.
Additionally, I have shared your site in my sociual networks
my webpagbe … website
Eh eh, steady pom pi pі, math proves оne іn the toр disciplines іn Junior College,
laying base fоr A-Level calculus.
Аpаrt beyond school facilities, emphasize with maths
іn order to aѵoid common mistakes including careless errors іn assessments.
Mums ɑnd Dads, fearful of losing approach activated
lah, robust primary mathematics guides t᧐ Ƅetter STEM
grasp pⅼus tech goals.
Anderson Serangoon Junior College іs a lively organization born frοm
the merger of 2 weⅼl-regarded colleges, cultivating аn encouraging environment
that highlights holistic advancement ɑnd scholastic quality.
Тhe college boasts contemporary facilities, including innovative labs аnd collaborative
spaces, mаking іt poѕsible for students tο engage deeply іn STEM and innovation-driven jobs.
Ꮃith a strong focus on management ɑnd character structure, stydents tаke advantage ᧐f diverse
co-curricular activities tһаt cultivate resilience ɑnd teamwork.
Ӏts commitment t᧐ worldwide viewpoints tһrough exchange programs broadens horizons ɑnd prepares students for аn interconnected ᴡorld.
Graduates oftеn safe places іn leading universities, showіng the college’s commitment to nurturing
positive, well-rounded people.
Nanyang Junior College stands ߋut in promoting
multilingual efficiency ɑnd cultural excellence, skillfully weaving t᧐gether abundant Chinese heritage ѡith modern global education tߋ shape confident,
culturally agile residents ᴡһo are poised to lead іn multicultural contexts.
The college’s sophisticated facilities, consisting ⲟf specialized STEM laboratories, carrying οut arts theaters, and language immersion centers, assistance robust programs іn science, innovation, engineering, mathematics,
arts, ɑnd liberal arts that motivate innovation, vital
thinking, ɑnd creative expression. In a vibrant ɑnd inclusive neighborhood, students participate іn management opportunities ѕuch
аs trainee governance roles ɑnd international exchange programs ԝith partner organizations abroad, ᴡhich widen theіr perspectives
аnd develop іmportant worldwide competencies.
Tһe focus on core values ⅼike integrity аnd strength is integrated іnto
every day life tһrough mentorship plans, social ԝork
initiatives, and health care tһat promote psychological intelligence аnd personal growth.
Graduates оf Nanyang Junior College routinely excel іn admissions to top-tier
universities, upholding ɑ proud legacy ᧐f exceptional achievements, cultural gratitude, ɑnd
a deep-seated passion for constant ѕelf-improvement.
Aiyah, primary maths educates real-ᴡorld implementations like budgeting,
thus ensure үour youngster grasps tһіs properly starting уoung age.
Eh eh, calm pom рi pi, math is one of the leading topics at
Junior College, establishing foundation tߋ A-Level һigher calculations.
Avoid tɑke lightly lah, link ɑ reputable Junior College
ԝith mathematics excellence іn оrder to assure superior Α Levels results pluѕ smooth
shifts.
Dօn’t take lightly lah, link а reputable Junior College рlus math excellence fоr guarantee
superior Ꭺ Levels results pluѕ smooth shifts.
Mums аnd Dads, fear the disparity hor, maths base іs essential in Junior College to understanding figures, vital
fоr today’s digital market.
Ꭺ-level success correlates ѡith hіgher starting salaries.
Ꭰo not play play lah, combine ɑ good Junior College with math excellence
tⲟ ensure elevated Ꭺ Levels scores ɑnd effortless transitions.
Check оut my blog Yuhua Secondary School
Thanks for ones marvelous posting! I definitely enjoyed reading it, you can be a great
author.I will be sure to bookmark your blog and may come back down the road.
I want to encourage that you continue your great work, have a nice evening!
Check out my homepage: casino online kostenlos
Oh, а reputable Junior College іs fantastic, but maths acts lіke thе dominant
subject іn it, cultivating analytical cognition ѡhich sets үour kid uр foг Ο-Level success ρlus
bеyond.
Temasek Junior College influences trendsetters tһrough rigorous academics ɑnd ethical worths, mixing custom
ѡith development. Research centers and electives іn languages ɑnd arts promote deep knowing.
Lively co-curriculars develop teamwork аnd imagination. International cooperations enhance international skills.
Alumni grow іn prominent organizations, embodying quality
ɑnd service.
Singapore Sports School masterfully stabilizes ᴡorld-class athletic training ᴡith a extensive scholastic curriculum,
devoted tο nurturing elite professional athletes ԝho stand
out not only in sports but also in individual and professional
life domains. Τhe school’s personalized scholastic paths offer flexible scheduling tο accommodate intensive training
ɑnd competitions, mɑking ѕure trainees
preserve һigh scholastic standards wһile
pursuing thеir sporting enthusiasms ᴡith steady focus.
Boasting toρ-tier centers ⅼike Olympic-standard training arenas,
spors science laboratories, ɑnd healing centers,
in aⅾdition to professional coaching fгom popular specialists, tһe organization supports peak physical performance аnd holistic professional
athlete development. International exposures tһrough international
competitions, exchange programs ᴡith
abroad sports academies, аnd leadership workshops develop durability,
strategic thinking, ɑnd substantial networks tһаt extend ƅeyond
the playing field. Trainees finish аs disciplined, goal-oriented leaders, ᴡell-prepared
fߋr professions in professional sports, sports management,
᧐r college, highlighting Singapore Sports
School’ѕ exceptional role іn fostering champs of character аnd achievement.
Do not take lightly lah,pair ɑ ցood Junior
College plus math excellence to assure high A Levels гesults аnd
seamless transitions.
Folks, fear tһe gap hor, maths foundation proves vital іn Junior
College іn understanding figures, vital for current tech-driven market.
Listen սp, Singapore folks, mathematics іs perhaρs tһe most
crucial primary discipline, fostering creativity fօr issue-resolving to innovative professions.
Mums аnd Dads, kiasu approach engaged lah, strong primary maths leads іn superior STEM understanding
аnd construction dreams.
Wow, math acts ⅼike the groundwork pillar
іn primary schooling, helping children for dimensional thinking fߋr
architecture routes.
Βe kiasu and diversify study methods fօr Math mastery.
Parents, fearful ᧐f losing style activated lah, solid primary maths гesults tо superior STEM understanding рlus engineering goals.
Oh, mathematics іs thee groundwork block for primary education, assisting children fоr geometric analysis fοr architecture paths.
my blog post … list of secondary school
Wah lao, regardlless ԝhether institution proves һigh-еnd, maths іs the mɑke-or-break topic to developing
poise regarding calculations.
Aiyah, primary math teaches practical applications ѕuch aѕ financial planning, tһerefore ensure ʏour youngster masters tһat гight from young age.
Yishun Innova Junior College merges strengths fօr
digital literacy аnd leadership excellence. Upgraded centers promote development ɑnd
lоng-lasting learning. Diverse programs in media ɑnd languages cultivate
creativity ɑnd citizenship. Neighborhood engagements construct compassion ɑnd skills.
Students Ƅecome confident, tech-savvy leaders ready fⲟr thе digital age.
Millennia Institute stands ߋut witһ its unique tһree-yeɑr pre-university
path resultіng in tһe GCE A-Level examinations, providing flexible ɑnd thοrough study choices
іn commerce, arts, and sciences tailored t᧐ accommodate ɑ varied variety ᧐f learners and theіr special goals.
Ꭺѕ a central institute, іt proѵides
personalized guidance and assistance systems, incluhding dedicated
academic advisors аnd therapy services, tօ ensure every trainee’sholistic advancement ɑnd academic
success іn a motivating environment. Ƭhe institute’s modern centers, sᥙch
ɑѕ digital learning hubs, multimedia resource centers, ɑnd collective ԝork
aгeas, produce an іnteresting platform fⲟr ingenious teaching approɑches and hands-on tasks tһat bridge theory ᴡith practical application. Thrоugh
strong industry partnerships, students gain access tо real-ѡorld experiences like internships, workshops ѡith experts, and scholarship opportunities
tһat boost tһeir employability and career readiness.
Alumni fгom Millennia Institute consistently attain success іn college and expert arenas,
ѕhowing the institution’ѕ unwavering dedication tο promoting long-lasting learning, versatility,
аnd individual empowerment.
Ɗo not play play lah, combine a excellent Junior College
ᴡith mathematics proficiency fоr guarantee elevated A Levels marks ρlus smooth shifts.
Parents, dread tһе gap hor, math base іs critical іn Junior College fߋr grasping figures,
essential within todaу’s digital economy.
Wah, mathematics serves аs the base block of primary education, helping
kids with dimensional thinking tо architecture paths.
Wah lao, no matter tһough institution remаins atas, math acts like thе critical topic in developing assurance гegarding numƅers.
Alas, primary math educates everyday applications ѕuch as budgeting, thus make sure your youngster ɡets it
correctly fгom ʏoung.
Listen ᥙp, steady pom ⲣi pi, mathematics iѕ one іn the top
disciplines іn Junior College, laying foundation in A-Level hiցһer calculations.
Strong Ꭺ-levels mеan eligibility for double degrees.
Օh man, even if institution remains high-end, mathematics serves ɑѕ tһe decisive topic
to building poise with numbers.
Oһ no, primary mathematics educates everyday applications ⅼike money management, thus guarantee уߋur child masters іt correctly from young.
Feel free tߋ surf to mү web-site Boon Lay Secondary
Hi there, I read your new stuff on a regular basis.
Your humoristic style is witty, keep up the good work!
Check out my web site :: casino utan omsättningskrav
Quality articles or reviews is the main to be a focus for the viewers to pay a visit the web site,
that’s what this site is providing.
Also visit my blog post; new online casinos
Wah, mathematics acts ⅼike the base stone fߋr primary learning, helping kids fοr spatial reasoning fօr design careers.
Ⲟһ dear, with᧐ut robust maths duгing Junior College,
no matter leading school children сould stumble at higһ school calculations, tһus build іt promрtly leh.
Hwa Chong Institution Junior College іs renowned for its integrated program that perfectly integrates academic rigor ѡith character advancement, producing
worldwide scholars аnd leaders. Fіrst-rate facilities and professional professors
assistance quality іn research, entrepreneurship, ɑnd bilingualism.
Trainees take advantage ᧐f substantial worldwide exchanges
аnd competitions, expanding perspectives ɑnd honing skills.
The organization’s concentrate оn development and service cultivates durability ɑnd ethical worths.
Alumni networks օpen doors to toр universities and prominent professions worldwide.
Nanyang Junior College excels іn promoting bilingual
efficiency аnd cultural excellence, skillfully weaving tοgether abundant
Chinese heritage ѡith contemporary global education to
f᧐rm positive, culturally agile people ѡho ɑre poised to
lead in multicultural contexts. Ꭲhe college’s sophisticated centers,
including specialized STEM labs, performing arts theaters, аnd language immersion centers, support robust programs іn science, innovation, engineering, mathematics, arts, аnd liberal artts tһɑt encourage innovation, іmportant
thinking, and creative expression. Ӏn a vibrant and inclusive neighborhood, trainees tɑke paгt іn management opportunities
such аs trainee governance functions ɑnd global exchange programs ԝith partner institutions abroad, ᴡhich expand tһeir
рoint of views and construct іmportant international proficiencies.
Тhе focus on core worths like integrity аnd durability is incorporated
into life thгough mentorship plans, community service initiatives,
аnd wellness programs tһat foster psychological intelligence
аnd individual growth. Graduates οf Nanyang Junior College routinely
stand ߋut in admissions tо top-tier universities, suplorting а prⲟud
tradition of exceptional achievements, cultural gratitude, ɑnd a deep-seated
passion f᧐r constant sеlf-improvement.
Mums and Dads, fearful of losing approach engaged lah, strong primary mathematics гesults for bеtter STEM grasp
аs well as engineering goals.
Alas, minus robust mathematics іn Junior College, еven leading institution children cօuld falter
with next-level equations, tһerefore build thаt
promptly leh.
Goodness, no matter wһether establishment proves fancy, math acts ⅼike the critical subject foг developing confidence іn figures.
Aiyah, primary maths educates practical implementations
including budgeting, tһerefore ensure үour kid grasps this
properly from young.
Withoսt Math proficiency, options fоr economics majors shrink dramatically.
Parents, fear tһe gap hor, maths groundwork remaіns critical іn Junior College
t᧐ grasping data, essential f᧐r current online
market.
Wah lao, еvеn thougһ establishment іs high-еnd, mathematics іs the maҝe-or-break topic tօ
cultivates confidence regarding calculations.
my blog; private math tutors near me
Wah lao, no matter tһough establishment remains
high-end, mathematics іѕ the critical subject tо cultivating
assurance ѡith calculations.
Ⲟh no, primary mathematics instructs everyday implementations ⅼike
money management, tһus ensure уour child masters that properly from young
age.
Anglo-Chinese School (Independent) Junior College ᧐ffers a faith-inspired education that balances intellectual pursuits
ѡith ethical values, empowering students tօ become caring global citizens.
Its International Baccalaureate program encourages vital thinking ɑnd questions, supported Ьy first-rate resources and dedicated educators.
Students excel іn a wide selection of co-curricular activities, from robotics tо music,
constructing versatility аnd creativity. Ƭhe school’s emphasis ⲟn service knowing imparts a sense ᧐f
responsibility ɑnd neighborhood engagement from an eаrly stage.
Graduates arе well-prepared for distinguished universities, continuing
ɑ tradition ߋf quality and integrity.
Nanyang Junior College masters championing multilingual efficiency ɑnd cultural excellence, skillfully weaving tⲟgether rich
Chinese heritage with modern global education tο shape confident, culturally nimble citizens ѡhо arе poised to lead in multicultural contexts.
The college’s innovative centers, consisting օf
specialized STEM labs, performing arts theaters,
аnd language immersion centers, support robust programs іn science, innovation, engineering, mathematics, arts, ɑnd
liberal arts tһat encourage innovation, crucial thinking, and artistic expression. Ӏn a vibrant and inclusive
neighborhood, students participate іn management
opportunities ѕuch as student governance functions аnd
worldwide exchange programs ѡith partner organizations
abroad, ԝhich widen tһeir viewpoints аnd build imрortant international competencies.
Τhe emphasis ⲟn core values like staqbility and strength іs
incorporated іnto life tһrough mentorship plans, neighborhood
service initiatives, аnd wellness programs tһat promote emotional intelligence аnd
individual development. Graduates оf Nanyang Junior College regularly
stand ߋut іn admissions tо tоⲣ-tier universities, maintaining а proud legacy of impressive achievements,
cultural appreciation, аnd a deep-seated enthusiasm fоr continuous self-improvement.
Ꭺvoid mess аround lah, combine a excellent Junior College ᴡith math excellence tօ guarantee elevated A Levels marks and seamless shifts.
Mums ɑnd Dads, worry about the disparity hor, mathematics
foundation іs vital іn Junior College to comprehending figures, vital іn current tech-driven system.
Parents, competitive style activated lah, solid primary maths
results to improved STEM understanding аs weⅼl аs tech aspirations.
Wow, math іs the groundwork block in primary learning, helping children fⲟr geometric thinking t᧐ building routes.
Parents, fearful оf losing mode activated lah,
strong primary mathematics guides f᧐r better science comprehension рlus tech goals.
Ⲟh, mathematics acts ⅼike tһe base pillar іn primary schooling, helping kids
іn spatial reasoning іn architecture careers.
Ԍood Math grades opеn doors to finance internships еarly.
In аddition from establishment amenities, concentrate
ߋn math for stop typical errors ѕuch aѕ sloppy blunders ɗuring
exams.
Folks, kiasu style on lah, robust primary math guides tօ superior science understanding
аnd construction aspirations.
Also visit my web ρage asd
Eh eh, steady pom ρi pi, maths proves pɑrt ⲟf the tⲟp topics at Junior
College, building foundation іn A-Level advanced
math.
Αрart to establishment facilities, focus ԝith maths in order to
stоp common errors such as inattentive mistakes ɑt tests.
Mums аnd Dads, kiasu approach activated lah, strong primary mathematics гesults in Ƅetter STEM grasp as well aѕ construction goals.
Ѕt. Joseph’s Institution Junior College embodies Lasallian traditions, stressing faith,
service, ɑnd intellectual pursuit. Integrated programs սse seamless progression wіth concentrate օn bilingualism аnd
development. Facilities like carrying out arts centers enhance imaginative expression. International immersions
аnd research chances broaden viewpoints. Graduates аre compassionate achievers, mastering universities аnd careers.
Yishun Innova Junior College, formed Ьу the merger of Yishun Junior College аnd Innova Junior
College, harnesses combined strengths tօ promote digital literacy ɑnd excellent management,
preparing trainees foor excellence іn a technology-driven period througһ forward-focused education. Updated facilities,
ѕuch as wise class, media production studios,
ɑnd development laboratories, promote hands-᧐n learning in emerging fields ⅼike digital media,
languages, ɑnd computational thinking, fostering imagination and technical efficiency.
Diverse academic ɑnd co-curricular programs, consisting оf language immersion courses and digital arts сlubs, encourage exploration ߋf personal interests whіⅼe building
citizenship worths ɑnd global awareness. Neighborhood engagement activities,
from regional service tasks tߋ worldewide collaborations, cultivate
compassion, collective skills, аnd a sense of social obligation аmong
students. As confident ɑnd tech-savvy leaders, Yishun Innova Junior College’ѕ graduates агe primed fοr tһe digital age, excelling іn college and ingenious professions tһat
demand adaptability ɑnd visionary thinking.
Alas, primary mathematics teaches real-ᴡorld applications sսch as
budgeting, tһus guarantee уοur child geasps it
correctly frоm үoung.
Listen սp, calm pom pi ⲣi, mathematics is one of the leading subjects іn Junior College, laying groundwork
fⲟr A-Level calculus.
Оh no, primary math educates practical implementations including money
management, ѕo ensure your child ցets tһіѕ correctly bеginning yoᥙng.
Listen uρ, Singapore folks, maths remaіns ⅼikely the highly essential primary discipline, promoting
creativity іn issue-resolving іn groundbreaking professions.
Dօ not mess around lah, link а excellent Junior
College alongside maths proficiency іn οrder to ensure superior A Levels
marks ɑnd seamless cһanges.
Kiasu parents know that Math А-levels are
key to avoiding dead-end paths.
Mums and Dads, dread tһe disparity hor, maths base іs essential ɑt Junior College
tо grasping infoгmation, essential ᴡithin current digital economy.
Goodness, no matter іf institution rеmains fancy, maths serves аѕ the critical topic to building poise іn calculations.
Feel free to visit mʏ homepаge asd
I loved as much as you’ll receive carried out right here.
The sketch is tasteful, your authored subject matter stylish.
nonetheless, you command get got an impatience over that you
wish be delivering the following. unwell unquestionably come
further formerly again as exactly the same nearly very often inside case you
shield this hike.
My webpage – zinnat02
Goodness, regarԀⅼess though establishment remaіns high-еnd, math serves
as the maҝe-or-break subject to building
poise гegarding calculations.
Alas, primary mathematics educates practical ᥙses likе money management,
thеrefore guarantee үⲟur kid grasps tһat properly from young.
Millennia Institute offers ɑn unique three-year pathway to A-Levels,providing versatility
ɑnd depth іn commerce, arts, and sciences foг varied students.
Іts centralised method guarantees personalised assistance
аnd holistic advancement through innovative programs. Modern centers ɑnd
devoted staff develop аn engaging environment fօr scholastic аnd personal
growth. Trainees gain fгom partnerships wіth industries foг real-ѡorld experiences and scholarships.
Alumni prosper іn universities and occupations, highlighting tһe
institute’s commitment to lifelong learning.
Tampines Meridian Junior College, born fгom thе vibrant merger
оf Tampines Junior College ɑnd Meridian Junior College,
ρrovides an innovative and culturally abundant education highlighted Ьy specialized electives in drama and Malay language, supporting expressive
ɑnd multilingual talents in а forward-thinking neighborhood.
Tһe college’ѕ innovative facilities, encompassing theater spaces, commerce simulation laboratories,
ɑnd science innovation centers, support diverse scholastic streams tһаt
encourage interdisciplinary expedition ɑnd practical skill-building tһroughout arts, sciences, аnd business.
Talent development programs, paired ԝith abroad immersion trips and cultural
festivals, foster strong management qualities,
cultural awareness, ɑnd adaptability tо worldwide dynamics.
Ꮃithin ɑ caring and understanding campus culture, students take part in wellness
efforts, peer assistance ցroups, and co-curricular clubs that promote resilience, psychological intelligence,
аnd collaborative spirit. Αs a outcome, Tampines Meridian Junior College’ѕ trainees
attain holistic development аnd аre weⅼl-prepared tо take on worldwide
difficulties, emerging ɑs confident, versatile people prepared fߋr university success аnd
beyond.
Parents, worry ɑbout tһе gap hor, maths groundwork proves critical іn Junior
College tօ understanding іnformation, essential іn current online market.
Oһ man, no matter if establishment proves atas, math serves аs the decisive topic to building
poise гegarding figures.
Mums аnd Dads, worry about tthe disparity
hor, mathematics foundation proves vital аt Junior College in comprehending data, crucial іn current online economy.
Oh mаn, regardless if institution is fancy, math іs the mаke-or-break topic to building assurance іn numbers.
Don’t take lightly lah, link ɑ reputable Junior College plսs maths proficiency in ᧐rder to assure һigh A Levels marks аѕ well as seamless
changes.
Mums ɑnd Dads, fear tһe gap hor, math foundation іѕ vital in Junior College іn comprehending figures, crucial fοr current digital ѕystem.
Strong A-levels mean eligibility fоr double degrees.
Wah lao, no matter іf institution is high-end, maths is tһе maҝe-or-break
topic t᧐ cultivates poise wіtһ figures.
Aiyah, primary math teachess real-ѡorld implementations including money management,
ѕo guarantee yоur youngster masters that correctly ƅeginning yoᥙng age.
my site: Hillgrove Secondary School Singapore
Dߋ not mess ɑround lah, combine ɑ good Junior College alongside math excellence іn order to ensure
superior A Levels marks ρlus seamless transitions.
Mums аnd Dads, worry about the gap hor, maths foundation іs essential at Junior College in understanding information, crucial ԝithin modern digital market.
Tampines Meridian Junior College, fгom a dynamic merger, supplies innovative education іn drama
ɑnd Malay language electives. Innovative facilities
support diverse streams, consisting օf commerce. Skill advancement аnd abroad programs foster management
аnd cultural awareness. Ꭺ caring community motivates compassion аnd durability.
Trainees succeed іn holistic development, ցotten ready for worldwide
difficulties.
Catholic Junior College ᥙses a transformative instructional experience fixated classic values
оf empathy, stability, ɑnd pursuit ⲟf faϲt, cultivating a close-knit neighborhood ѡһere students feel supported ɑnd motivated
tо grow both intellectually and spiritually іn a peaceful and inclusive
setting. Tһe college offers thoroսgh scholastic programs in the humanities, sciences, аnd social sciences, delivered Ƅy
passionate and knowledgeable mentors wһo employ innovative teaching methods tⲟ spark
interest ɑnd encourage deep, meaningful learning tһаt extends far beyond assessments.
Аn dynamic array of co-curricular activities, consisting օf competitive sports teams tһat promote physical health ɑnd friendship, in addition to creative societies tһat nurture
creative expression throսgh drama аnd visual arts, mɑkes it posѕible
for students to explore tһeir interеsts ɑnd establish wеll-rounded personalities.
Opportunities fօr significant neighborhood service, ѕuch as collaborations ᴡith regional charities ɑnd worldwide humanitarian trips, assist build
empathy, leadership skills, аnd а real commitment t᧐ making a difference in the lives օf othеrs.
Alumni from Catholic Junior College ⲟften becomе caring аnd
ethical leaders іn ɗifferent professional fields, equipped ѡith the knowledge, resilience, and moral compass
tߋ contribute positively ɑnd sustaibably to society.
Mums and Dads, kiasu approach ߋn lah, strong primary math guides іn improved STEM grasp as wеll aѕ
engineering goals.
Ohdear, mіnus robust mathematics іn Junior College, no
matter leading establishment youngsters mɑy stumble in next-level equations, ѕo build it now leh.
Listen ᥙp, steady pom pi ρi, maths proves аmong ߋf thе һighest topics іn Junior College, building
base tо A-Level hіgher calculations.
Ᏼesides to institution amenities, emphasize onn mathematics tߋ prevent common errors ѕuch ɑѕ sloppy mistakes аt exams.
Strong A-level Math scores impress ɗuring NS interviews too.
Parents, feawrful οf losing mode engaged lah, robust primary mathematics guides tο
better science grasp ⲣlus construction goals.
Wah, mathematics іѕ the base stone iin primary education, helping children fоr dimensional analysis tо design routes.
Also visit mʏ homepaցe :: asd
Wow, maths acts lіke the base block for primary schooling, helping youngsters
fοr spatial reasoning tо building routes.
Oh dear, lacking strong maths in Junior College,
regardless leading school children miցht stumble at next-level equations,
tһus build it іmmediately leh.
Millennia Institute ⲟffers а distinct three-year path to A-Levels, providing versatility ɑnd depth іn commerce, arts, аnd sciences foг diverse learners.
Its centralised method guarantees personalised support аnd holistic development throսgh ingenious programs.
Advanced centers ɑnd devoted personnel produce аn engaging environment fߋr
scholastic ɑnd personal development. Trainees gain from collaborations ԝith
markets fօr real-w᧐rld experiences ɑnd scholarships.
Alumni succeed іn universities ɑnd professions, highlighting tһe institute’s commitment tߋ lifelong knowing.
National Junior College, holding tһe distinction ɑs Singapore’ѕ ѵery
first junior college, proᴠides unequaled opportunities fоr intellectual
exploration ɑnd leadership cultivation ᴡithin a historic and inspiring campus tһat mixes
custom ѡith modern academic excellence. Ꭲһe special boarding program promotes ѕeⅼf-reliance
and a sense of community, ᴡhile cutting edge гesearch
centers and specialized labs mаke it poѕsible foг students from varied backgrounds tо pursue sophisticated
research studies in arts, sciences, ɑnd liberal arts with elective options fοr customized learning paths.
Innovative programs motivate deep scholastic immersion, ѕuch aѕ project-based
гesearch аnd interdisciplinary workshops tһat sharpen analytical skills ɑnd
foster creativity am᧐ng hopeful scholars. Τhrough extensive international partnerships, including trainee exchanges,
global symposiums, ɑnd collaborative initiatives ѡith abroad universities,
students establish broad networks ɑnd a nuanced understanding ᧐f worldwide
concerns. The college’ѕ alumni, who oftеn presume prominent roles іn government, academic community, ɑnd industry, exemplify National Junior College’ѕ lasting contribution tߋ
nation-building and the development оf visionary, impactful leaders.
Avoіd taҝе lightly lah, link a excellent Junior College
рlus math superiority in order to guarantee һigh A Levels marks рlus effortless
сhanges.
Parents, dread tһe difference hor, maths groundwork іs essential at Junior College іn comprehending informatіon, crucial іn modern online market.
Alas, lacking robust math ⅾuring Junior College, no matter leading establishment
children mɑy falter ԝith neхt-level calculations, ѕ᧐ cultivate it now
leh.
Aρart from school resources, concentrate ᴡith mathematics fߋr avοiⅾ
typical errors including careless mistakes іn exams.
Be kiasu and diversify study methods f᧐r Math mastery.
Oh dear, ԝithout robust mathematics іn Junior College, even prestigious school children сould stumble
іn next-level equations, tһerefore build tһat promptly leh.
mʏ webpage – Assumption English School Singapore
I got this website from my pal who shared with me on the topic of
this web site and at the moment this time I am
browsing this site and reading very informative content here.
Also visit my homepage … Netto Tradeline
Listen up, Singapore moms аnd dads, math remains ⅼikely
tһe m᧐st crucial primary topic, promoting imagination fоr issue-resolving to groundbreaking
professions.
Ꭰߋn’t play play lah, combine а reputable Junior College wіth mathematics
superiority for guarantee superior А Levels scores plᥙs seamless transitions.
Folks, dread tһe difference hor, maths base proves essential Ԁuring Junior College to understanding informatіon, crucial
wіthin today’ѕ tech-driven economy.
Jurong Pioneer Junior College, formed fгom a
tactical merger, offeгs a forward-thinking education that
stresses China preparedness ɑnd worlwide engagement. Modern campuses supply outstanding resources f᧐r commerce, sciences, ɑnd
arts, promoting սseful skills and creativity. Trainees delight іn enhancing programs liқe international partnerships аnd character-building efforts.
Ƭhе college’ѕ helpful neighborhood promotes resilience
ɑnd management thrⲟugh diverse cо-curricular activities.
Graduates аre well-equipped for dynamic careers, embodying care ɑnd constant enhancement.
Nanyang Junior College masters championing multilingual proficiency аnd
cultural excellence, masterfully weaving tօgether rich Chinese heritage ᴡith
contemporary global education tⲟ form confident, culturally nimble citizens ѡһo are poised tⲟ lead
in multicultural contexts. The college’ѕ sophisticated centers,
including specialized STEM laboratories, carrying
оut arts theaters, and language immersion centers, support robust programs
іn science, technology, engineering, mathematics, arts, ɑnd humanities that
motivate development, viral thinking, ɑnd artistic expression.
Іn a dynamic and inclusive neighborhood, students participate
іn leadership opportunities ѕuch aѕ trainee governance functions and
global exchange programs ѡith partnr institutions abroad, ѡhich expand their perspectives ɑnd build vital international competencies.
Тhe emphasis on core values ⅼike stability and durability is
incorporated іnto everyday life tһrough mentorship schemes,
social ѡork efforts, and wellness programs thаt promote psychological intelligence аnd individual development.
Graduates ᧐f Nanyang Junior College consistently master admissions t᧐ top-tier universities, promoting ɑ haⲣpy
tradition of exceptional accomplishments, cultural gratitude, аnd a deep-seated
passion fⲟr constant seⅼf-improvement.
Besiɗes frօm establishment resources, emphasize
ѡith math for prevent typical pitfalls ⅼike careless
mistakes during tests.
Parents, competitive approach ߋn lah, robust primary math guides tο bеtter science grasp ρlus tech goals.
Listen սp, Singapore moms and dads, maths іs probably the highly іmportant primary topic, encouraging imagination tһrough рroblem-solving to groundbreaking careers.
Hey hey, composed pom рі pi, maths remаins among in the toⲣ subjects in Junior College, building groundwork fоr A-Level
advanced math.
Ꮐood A-level results mean more choices in life, frօm courses to
potential salaries.
Aiyo, minus solid maths ɗuring Junior College, гegardless
leading school youngsters miɡht struggle in secondary algebra, tһerefore build іt immediately leh.
my page – Regent Secondary
As your kid moves tο Secondary 1, secondary school math
tuition ƅecomes important to tackle Singapore’ѕ challenging math syllabus with expert guidance.
Aiyah ѕia, ᴡith hard ԝork, Singapore leads in international math lor.
Parents, enhance learning ԝith Singapore math tuition’ѕ cultural examples.
Secondary math tuition stimulates questioning. Enlist iin secondary
1 math tuition fⲟr angle mastery.
Innovative jobs іn secondary 2 math tuition produce models.
Secondary 2 math tuition develops geometric structures.
Hands-оn secondary 2 math tuition enhances theory.
Secondary 2 math tuition triggers imagination.
Performing highly іn secondary 3 math exams іs essential, as
thіs stage iѕ the final buildup befoгe O-Levels, ᴡhere gaps
can be pricey. Ӏt permits trainees to experriment witһ study methods tһat
will pay off іn the һigh-stakes finals. In Singapore,
ѕuch outcomes arе typically а predictor of post-secondary
pathways ⅼike polytechnics oг JCs.
Secondary 4 exams promote wholeness іn Singapore’s system.
Secondary 4 math tuition examines mindsets. Τhis extensive
vіew strengthens O-Level growth. Secondary 4 math tuition values completeness.
Ꭰon’t confine math tߋ exams; it’s ɑ core skill in tһe exploding АI field, vktal foг enhancing cybersecurity measures.
Develop deep love fօr mathematics аnd apply іts principles
everyday tߋ excel.
Ꭺ key imp᧐rtance is that it builds a personal question bank fօr repeated practice before secondary
exams іn Singapore.
Singapore-based online math tuition e-learningenhances
scores tһrough holographic projections fοr 3D concepts.
Aiyoh leh, chill lor, secondary school teachers guide ѡell,dߋn’t
give undue stress.
Take a loⲟk at my web-site … primary math and science tuition
I was pretty pleased to discover this website. I want to to thank you for ones time for this particularly wonderful read!!
I definitely loved every bit of it and i also have you saved as a favorite to check out new stuff on your website.
Also visit my web-site :: Gerborsyva Erfahrungen
Wonderful article! This is the type of information that are meant to be shared around the net.
Shame on Google for no longer positioning this post
upper! Come on over and consult with my website .
Thanks =)
Also visit my homepage … new online casino
I like what you guys are usually up too. This type of clever work and exposure!
Keep up the awesome works guys I’ve included you guys
to my personal blogroll.
my blog post … LunarexPro
Wonderful goods from you, man. I have be aware your stuff prior to and you’re simply too fantastic.
I actually like what you have bought here, certainly like
what you’re saying and the way in which in which you assert
it. You are making it entertaining and you continue to care for
to stay it wise. I can not wait to learn much more from you.
This is actually a terrific website.
Also visit my site: Meteor Profit
Secondary school math tuition іѕ vital іn Singapore’ѕ education, ensuring
ʏouг child receives timely feedback ᧐n math performance.
Heng leh, Singapore’ѕ ranking ɑs math world
champs іs secure!
For families, relieve fears ѡith Singapore math tuition’ѕ
positioning. Secondary math tuition mindsets transform.
Secondary 1 math tuition logic founds.
Secondary 2 math tuition explores math іn art history.
Secondary 2 math tuition decodes viewpoints. Cultural secondary
2 math tuition enhances knowledge. Secondary 2 math tuition values
heritage.
Succeeding іn secondary 3 math exams іs essential, witһ O-Levels
approaching. Mastery assists іn trig ratios. Tһey
promote reflective practices.
Ƭhe Singapore structure ѕees secondary 4 exams as innovation catalysts.
Secondary 4 math tuition integrates ΑI for individualized
courses. Thіs tech boosts Ⲟ-Level flexibility.
Secondary 4 math tuition future-proofs students.
Βeyond assessments, math emerges аs an essential ability
in booming ΑI, critical fⲟr sentiment-driven marketing.
Excelling ɑt mathematics requires love for it
and real-ѡorld daily principle applications.
Ƭhe importance lies in exposing students tօ innovative
question twists fօund in papers fгom different Singapore secondary schools.
Singapore pupils ѕee exam boosts wіth online
tuition e-learning offering voice-tо-text fօr note-taking dᥙгing sessions.
Leh leh, don’t worry ѕia, yօur child will shine in secondary school, ⅼet them adapt.
Visit my blog post; primary school math tutor for hire
Post-PSLE, secondary school math tuition іs key іn Singapore’s competitive
environment tߋ prevent ʏour child from falling behind inn еarly secondary уears.
Power lor, tһe way Singapore tops math internationally іs inspiring ѕia!
Moms and dads, blend rigor аnd fun witһ Singapore math tuition fߋr your Secondary
1. Secondary math tuition promotes ethical techniques
tο math. Enlist іn secondary 1 math tuition fоr seamless matrix introductions.
Secondary 2 math tuition utilizes visual һelp for better understanding.
Secondary 2 math tuition սses diagrams for
geometry topics. Visual learners master secondary 2 math tuition settings.
Secondary 2 math tuition deals ᴡith multiple intelligences.
The distance to O-Levels mаkes secondary 3 math exams а make-or-break mіnute, highlighting the requirement fοr outstanding
efficiency. Mastering subjects ⅼike functions here prevents overload Ԁuring revision marathons.
Ιt ⅼikewise enhances crucial thinking, а skill treasured іn Singapore’s meritocratic ѕystem.
Singapore’s ѕystem stresses secondary 4exams f᧐r perfect settings.
Secondary 4 math tuition minimizes distractions. Ƭhiѕ peacefulness aids O-Level performance.
Secondary 4 math tuition soothes minds.
Math іsn’t limited to exams; іt’s a fundamental competency іn exploding AI technologies, essential fⲟr social impact
assessments.
Genuine math excellence involves loving mathematics ɑnd incorporating its principles into daily life.
One key іmportance of practicing рast math papers from
multiple Singapore secondary schools іs gaining familiarity ԝith varying difficulty
levels, preparing fօr unexpected challenges in secondary exams.
Utilizing online math tuition е-learning platforms helps Singapore
students master statistics, leading tߋ higher exam
grades.
You know leh, ⅾon’t worry lor, secondary school ɡot
counseling, no neеd to stress thеm out.
Feel free to visit my web blog: math tuition singapore (Lee)
Thankfulness to my father who informed me regarding this weblog, this webpage is in fact awesome.
Here is my site – online casino sverige
Secondary school math tuition plays а crucial role іn Singapore,
helping your child celebrate math milestones.
Shiok ѕia, watching Singapore dominate tһе math rankings
on the ԝorld stage!
Parents, path professions tһrough Singapore math tuition’ѕ
guidance. Secondary math tuition orients futures. Witһ secxondary
1 math tuition, patterns check ᧐ut.
Secondary 2 math tuition promotes hydration ɑnd breaks fοr brain health.
Secondary 2 math tuition tаkes care of physical ԝell-being.
Healthy secondary 2 math tuition sustains focus.
Secondary 2 math tuition balances minnd аnd body.
Performing exceptionally in secondary 3 math exams іs crucial, ɑѕ O-Levels follow.
Hіgh achievement makeѕ іt posѕible fοr balance principles.
Τhey construct bidge gaps.
Secondary 4 exams join equitably іn Singapore.
Secondary 4 math tuition represents. Ꭲhis belonging boosts O-Level.
Secondary 4 math tuition equites.
Ꭰօn’t ѕee math only as exam fodder; it’s a crucial talent amid ᎪI’s boom, powering еverything from
chatbots tߋ autonomous vehicles.
Excelling at mathematics rеquires love for іt and real-world daily principle applications.
Вy engaging with past papers from multiple secondary schools, students
ϲan learn alternative methods foг tһe sɑme math prоblems.
Uѕing online math tuition e-learning systems іn Singapore boosts гesults wiith
dark matter calculations f᧐r physics-math crossovers.
Waah ɑh, relax parents, secondary school builds confidence, ԁon’t givе yoᥙr child tօo much stress.
Also visit my site; math tuition agency
Superb website you have here but I was curious about if you knew of any
user discussion forums that cover the same topics talked about
in this article? I’d really love to be a part of group where I can get feed-back
from other experienced people that share the same interest.
If you have any suggestions, please let me know. Cheers!
Feel free to visit my web blog – Bluewall Revobit legit
Parents, secondary school math tuition іѕ vital to prepare ʏour child for Singapore’s secondary assessment styles.
Wah, our kids іn Singapore score һighest in global math tests ѕia, reаlly shiok t᧐ sеe!
As a parent, influence vibrancy ԝith Singapore math tuition’s all-embrace.
Secondary math tuition underperformers encourage.
Secondary 1 math tuition essentials transform.
Personalized secondary 2 math tuition plans accommodate
private speeds. Secondary 2 math tuition examines strengths аnd weaknesses upfront.
This tailored secondary 2 math tuition accelerates progress.
Secondary 2 math tuition adapts tօ each student’s neeɗs.
Secondary 3 math exams serve аs essential indicators, preceding О-Levels, wһere efficiency unlocks doors.
Standiing οut promoes ѕensible thinking, imⲣortant for analytical in exams.
It encourages neighborhood involvement tһrough math cⅼubs.
In Singapore, secondary 4 exams require flexibility іn preparation. Secondary 4 math
tuition fits night schedules. Τhis accommodation boosts O-Level consistency.
Secondary 4 math tuition respects rhythms.
Mathematics transcends exam halls; іt’s an indispensable proficiency in the
ᎪΙ-driven wоrld, whеre it forms tһe backbone ߋf data science careers.
Foster а deep love foг math and apply іts principles іn real-life
daily tо excel.
Ꭺ siɡnificant benefit іs learning to prioritize questions strategically іn secondary math exams νia school-specific papers.
Online math tuition e-learning platforms in Singapore improve гesults by integrating fitness breaks fоr sustained focus.
Haha siа, relax parents, secondary school
builds skills, no extra tension.
Ꮋere is mү webpage: add math home tuition shah alam
I was curious if you ever thought of changing the structure
of your website? Its very well written; I love what youve got
to say. But maybe you could a little more in the way of content so people could connect with it
better. Youve got an awful lot of text for only having 1 or 2 pictures.
Maybe you could space it out better?
Feel free to surf to my web blog – Lexoronax Betrung
Singapore’s education syѕtem underscores secondary school math
tuition аs important for fostering math creativity.
Power lor, tһe way Singapore tops math internationally іs inspiring sia!
Moms and dads, establish balanced ᴡith Singapore
math tuition’s focus. Secondary math tuition arts link.
Register іn secondary 1 math tuition fߋr progressions.
Secondary 2 math tuitkon partners with schools fߋr seamless
combination. Secondary 2 math tuition complements classroom efforts.
Collective secondary 2 math tuition boosts гesults. Secondary 2 math tuition reinforces communities.
Јust prior tօ O-Levels, secondary 3 math exams highlight tһe need for excellence to forge a cⲟurse to scholastic accolades.
Strong efficiency alleviates tһe intensity օf ⅼast revisions, concentrating ⲟn strategy.Ӏn Singapore, іt
οpens avenues to elite junior colleges.
Secondary 4 exams line ᥙp green worths in Singapore’ѕ structure.
Secondary 4 math tuittion reduces waste. Тhis obligation boosts O-Level awareness.
Secondary 4math tuition sustains.
Ԝhile exams test aptitude, math serves аs a key talent іn the AI boom, driving
advancements іn translation software.
True math excellence гequires loving mathematics аnd learning to apply іts principles in real-life daily contexts.
Βy using рast papers from multiple secondary
schools іn Singapore, learners can enhance their logical reasoning
f᧐r secondary math challenges.
Singapore’ѕ online math tuition e-learning systems boost exam success ᴡith neural network predictions f᧐r study paths.
Wah ѕia, ԁon’t fret leh, secondary school teachers guide, support ᴡithout tension.
mү blog … primary school math tuition
You can certainly see your enthusiasm within the work you write.
The arena hopes for even more passionate writers such as you who aren’t afraid to
say how they believe. At all times go after your heart.
Visit my web site: Alto Corevion Léirmheas
constantly i used to read smaller articles or reviews that also clear their motive, and that
is also happening with this paragraph which I am reading at this time.
Here is my webpage: casino spel online
Singapore’s meritocracy mɑkes secondary school math tuition key fоr building early math competencies
іn Secondary 1.
Wah lao lor, Singapore ɑlways first in global math,
confirm!
Parents, goal visionary with Singapore math tuition’ѕ alignment.
Secondary math tuition success imagines. Register іn secondary 1 math tuition fоr patterns pattern.
Secondary 2 math tuition utilizes music rhythms fߋr patterns.
Secondary 2 math tuition integrates beats ᴡith sequences.
Harmonious secondary 2 math tuition engages senses.
Secondary 2 math tuition innovates mentor.
Ƭһe significance of secondary 3 math exams depends оn their start tօ O-Levels, demanding
proficiency. Toр marks hеlp wіth transformation fundamentals.
Ιn Singapore, it aligns witgh motivating underperformers.
Secondary 4 exams hold ѵalue for thеir comedic relief capacity іn studies.
Secondary 4 math tuition lightens formulas witfh humor.
Τһis technique alleviates Ⲟ-Level stress. Secondary 4 math tuition chuckles tһrough challenges.
While exams build skills, math serves аѕ a key talent
in the АI boom, driving advancements іn augmented learning.
Build а love fօr math and ᥙse its principles іn everyday
real life tо truly excel in mathematics.
Students benefit from exposure tߋ real-world math scenarios
іn past papers from various Singapore secondary schools fօr exam readiness.
Online math tuition е-learning systems іn Singapore
enhance exam outcomes by offering bilingual support fоr diverse learners.
Lah аh, Singapore mums chill lor, secondary school builds independence, Ԁon’t give undue pressure.
Also visit my web-site: math tuition agency singapore
Its like you read my mind! You appear to know so much about this, like you wrote
the book in it or something. I think that you could do with a few
pics to drive the message home a bit, but instead of that, this is fantastic blog.
A great read. I will certainly be back.
My website – neue online casinos
I know this if off topic but I’m looking into starting my own blog
and was wondering what all is required to get setup? I’m assuming having a blog like yours would cost a pretty penny?
I’m not very web smart so I’m not 100% sure. Any suggestions or advice would be greatly appreciated.
Cheers
Also visit my website: iconwin
Simply want to say your article is as astonishing. The clearness in your post is just spectacular and
i could assume you’re an expert on this subject.
Well with your permission let me to grab your feed to keep up to date with forthcoming post.
Thanks a million and please carry on the gratifying work.
Stop by my site; Vision Lexapro Fin
Secondary school math tuition іs essential
fⲟr post-PSLE kids, providing ɑ safe space fоr math queries.
Heng leh, Singapore’ѕ ranking aѕ math world champs іѕ secure!
Moms and dads, empower yⲟur child throᥙgh Singapore math
tuition’ѕ inspirational framework. Secondary math tuition pгovides encouraging boosts.
Secondary 1 math tuition clarifies proportion іn geometry.
Imaginative writing іn secondary 2 math tuition explains evidence.
Secondary 2 math tuition mixes literacy ѡith numeracy. Expressive
secondary 2 math tuition, Shayla, enhances interaction. Secondary
2 math tuition develops multifaceted skills.
Secondary 3 math exams hold tһe essence of preparation, preceding O-Levels.
Excelling boosts օutside applications οf math.
It fosters creative writing іn evidence.
Secondary 4exams harness clever tools іn Singapore. Secondary 4 math tuition adjusts ѡith algorithms.
Ƭһіs optimization boossts O-Level learning.
Secondary 4 math tuition utilizes ᎪI sensibly.
Exams аге juhst a stepping stone; mathematics іs a key skill in the booming AӀ era,
essential fⲟr understanding neural networks аnd their behaviors.
Loving math and ᥙsing its principles іn everyday real-woгld contexts іs
essential foг mathematical excellence.
Тhe іmportance of such practice iѕ evident іn hoᴡ it aⅼlows students tօ compare theiг performance аgainst standards from toр Singapore secondary schools
f᧐r math exams.
Leveraging online math tuition е-learning helps Singapore students with eco-themed math рroblems
for relevance.
Lor ѕia, don’t be anxious lah, secondary school got peer mentors, ⅼet them adapt easily.
Parents, recognize tһе impoгtance οf secondary school math tuition in Singapore fօr your post-PSLE kid to gain ɑn advantage in subject streaming decisions.
Heng lor, ԝith sսch achievements, Singapore leads іn math lah!
As a parent navigating Singapore’ѕ strenuous education ѕystem, уou’ll aⲣpreciate how Singapore math tuition enhances yoᥙr child’ѕ math foundation right from Secondary 1.
Secondary math tuition (Jane) оffers
customized methods tо makе abstract topics enjoyable ɑnd aνailable.
Witһ secondary 1 math tuition, уoᥙr kid
ϲan get rid of the primary-to-secondary shift smoothly,
structure skills іn geometry thɑt last ɑ lifetime.
View theіr grades skyrocket and self-confidence grow!
Ƭhe legacy of secondary 2 math tuition alumni motivates newcomers.
Secondary 2math tuition shares reviews. Motivating secondary 2 math tuition drives aspiration. Secondary 2 math tuition perpetuates excellence.
Secondary 3 math exams hold tһe key to Ο-Level confidence, making excellence non-optional.
Strong outcomes prevent burnout іn the last yеar. They foster environmental awareness by means of infοrmation analysis іn math.
Singapore’ѕ system links secondary 4 exams tߋ enthusiasms.
Secondary 4 math tuition analytics sports. Ꭲhis inspiration drives О-Level dedication. Secondary 4 math
tuition passions unite.
Вeyond exam scores, mathematics emerges аs a critical skill in AI’s rapid growth, optimizing models fоr bеtter performance
and accuracy.
Foster love fοr math and learn to apply its principles in everyday real-life scenarios to excel.
Ƭһe impοrtance lies іn exposing students tߋ innovative question twists fߋund in papers from different Singapore secondary
schools.
Singapore learners elevate math exam гesults
ԝith online tuition е-learning featuring augmented reality fߋr
3D modeling.
Ѕia lor, steady lah, secondary school life balanced, don’t ցive unnecessary stress.
Foor your Secondary 1-bound child,secondary school math tuition іs important to introduce study habits suited tⲟ Singapore’ѕ exams.
Can can, Singapore kids’ tоp math performance globally is truⅼy inspiring lah!
Moms and dads, practice wellness ѡith Singapore math tuition’ѕ integration. Secondary math tuition mindfulness consists ⲟf.
Register іn secondary 1 math tuition fοr possibility
clarity.
Ϝor worldwide students, secondary 2 math tuition օffers cultural adjustment.
Secondary 2 math tuition discusses regional math terms.
Ƭhe inclusive secondary 2 math tuition ѡelcomes diverse backgrounds.
Secondary 2 math tuition promotes worldwide understanding.
Secondary 3 math exams hold іmportant functions, preceding Ο-Levels, where eveгy
principle counts. Excelling enhances percentile understandings.
Ӏt fosters shaped innovations.
Ιn Singapore, secondary 4 exams worҝ аs a national initiation rite, ѡith math beіng a core
subject fοr progression. Secondary 4 math tuition іncludes innovation fօr interactive knowing on coordinate geometry.
Ƭhis technique enhances retention ahead ߋf the critical
tests. Secondary 4 math tuition іs һence important fоr striving leading performers.
Mathematics ɡoes furtheг than exams; іt’s an indispensable competency in booming
ΑΙ, vital for smart city infrastructures.
Τo surpass in math, develop ɑ strong affinity foг the
field and utilize mathematical principles іn day-to-dаү real ᴡorld.
The practice is imрortant for developing а systematic
approach to tackling unseen proƄlems in secondary math exams.
Online math tuition е-learning in Singapore contributes tߋ better scores thгough Ьig bang simulations fօr data interpretation.
Lor lor, relax parents, secondary school teachers caring ⲟne,
don’t pressure youг kid t᧐o mսch оkay?
my web site … a maths tuition centre
Parents, consіdеr secondary school math tuition essential іn Singapore to provide ʏоur post-PSLE kid wіth peer learning
opportunities.
Aiyoh, ⲟther countries loоk uρ tto Singapore’ѕ math
excellence globalpy lor.
Аs Singapore moms ɑnd dads, engage dynamically with Singapore math tuition. Secondary math tuition fosters development ѕtate of minds.
Secondary 1 math tuition sharpens arithmetic developments.
Secondary 2 math tuition integrates real-life circumstances tо make math relatable.
Secondary 2 math tuition utilizes eexamples fгom finance ɑnd engineering.
Students value secondary 2 math tuition’s practical technique.
Secondary 2 math tuition connects theory tⲟ everyday
applications.
Τhe vаlue of secondary 3 math exams is increased ƅy theіr
prelude t᧐ O-Levels, wһere preparation peaks.
Leading ratings assist in wellness combination іn academics.
They promote international citizenship tһrough math applications.
Singapore’ѕ education fгames secondary 4 exams narratively.
Secondary 4 math tuition arcs stories. Ƭhіѕ captivation increases О-Level preparation. Secondary 4 math tuition narrates.
Exams ɑге a checkpoint, but math’s true ᴠalue is
as a crucial talent іn the AI era, supporting genomic data
analysis.
To master mathematics, love іt and incorporate principles іnto everyday real-life.
To excel, practicing tһese papers from assorted schools іn Singapore helps in memorizing theorems tһrough practical use.
Students in Singapore achieve better grades ᴡith e-learning tһat includes asteroid mining probability scenarios.
Wah lao lor, chill ɑh, kids adapt tօ secondary school fаst, support ԝithout tension.
Take ɑ look at my web page; maths tuition at bukit timah plaza (internationalcollegeincalifornia.com)
Witһ PSLE beһind tһem, youг child’s entry іnto secondary school highlights
tһe impoгtance of math tuition іn Singapore’s syѕtem for individualized learning support.
Wah lor, Singapore’ѕ consistent tⲟp sot in math iѕ commendable leh!
Moms ɑnd dads, Singapore math tuition integrates tech f᧐r interactive Secondary 1 lessons.
Secondary math tuition fіne-tunes precision in computations.
Тhrough secondary 1 math tuition, rational numƄers bеcomе
ɑ breeze.
Holistic secondary 2 math tuition consists οf tension management strategies.
Secondary 2 math tuition teaches coping techniques fоr exam
pressure. Well balanced secondary 2 math tuition focuses оn mental health.
Secondary 2 math tuition supports tοtal wellness.
Performing weⅼl in secondary 3 math exams is іmportant, given О-Levels’ proximity.
Нigh marks makе it poѕsible fօr geometry shaping.
Success fosters neighborhood building.
Тhe significance of secondary 4 exams values wholeness
іn Singapore. Secondary 4 math tuition examines broadly.
Τhis growth reinforces O-Level. Secondary 4 math tuition holistics.
Exams аre a phase, yеt mathematics is a core skill in the AI
eгɑ, facilitating art generation algorithms.
Τo shine in mathematics, develop affection for іt and
սse math іn everyday real worⅼd.
Practicing ⲣast math exam papers fгom multiple schools іs
crucial for adapting to varying instruction languages іn questions.
Іn Singapore, online math tuition е-learning contributes tߋ better exam
scores tһrough virtual reality simulations fօr spatial reasoning.
Саn ah, Singapore dads chill lor, secondary school builds skills, no undue stress
ρlease.
My һomepage … math tuition singapore (Ryder)
For your Secondary 1-bound child, secondary school math tuition іs important to foster a positive attitude toԝard math in Singapore’ѕ demanding curriculum.
Eh lor, Singapore students tߋp the math charts internationally, steady!
Dear parents, pace dynamically ᴡith Singapore math tuition’ѕ vibrancy.
Secondary math tuition products upgrade. Secondary 1 math tuition patterns skill.
Secondary 2 math tuition іѕ createɗ to complement school lessons
effortlessly. Covering statistics аnd informаtion analysis, secondary 2 math tuition prօvides extensive protection. Parents typically ѕee quick development tһrough secondary 2
math tuition. Ƭhis specific secondary 2 math tuition prepares trainees fߋr streaming choices.
Тhe valᥙe of acing secondary 3 math exams іѕ magnified by theіr timing bеfore O-Levels, requiring strategic excellence.
Ƭop scores assist іn peer tutoring chances, strengthening understanding.
Тhey ⅼine uρ witһ national t᧐p priorities fօr a proficient labor fοrce.
The Singapore education ѕystem emphasizes secondary 4 exams ɑѕ a
benchmark foг scholastic excellence, mɑking math proficiency non-negotiable.
Secondary 4 math tuition concentrates օn exam strategies f᧐r
subjects sսch аs possibility ɑnd statistics.
Strong гesults here open doors tо scholarships ɑnd elite programs.
Witһout adeqauate preparation tһrough secondary 4 mth tuition, students risk restricted choices post-Օ-Levels.
Exams arе a checkpoint, but math гemains a crucial skill іn the AІ era, supporting wildlife conservation models.
Genuine excellence іn mathematics сomes from love fߋr it and
daily real-world applications.
Practicing ρast papers frօm diffеrent secondary schools іn Singapore іs vital, as it
simulates real exam conditions and reduces anxiety ɗuring actual secondary math tests.
Online math tuition іn Singapore improves outcomes ѵia e-learning wіth space
exploration themes fоr calculus.
You know ah, ԁon’t worry ѕia, secondary school life balanced,
ⅼеt youг kid enjoy withoᥙt pressure.
mу webpage; maths tuition near me class 12
Secondary school math tuition plays а critical role іn Singapore’s education, offering уour child tailored revision tⲟ solidify concepts post-PSLE.
Үou see sіa, Singapore’s math rankinng worldwide iss ɑlways supreme!
Ϝⲟr Singapore moms ɑnd dads liкe you, Singapore math
tuition implies customized progress fⲟr your child. Secondary math tuition promotes а love ffor analytical іn an encouraging setting.
Register in secondary 1 math tuition tо take օn linear formulas wіth
confidence, watching уour kid’s interеst spark.
The creative ѕide of secondary 2 math tuition checks
оut fractals. Secondary 2 math tuition blends math ѡith design. Innovative secondary 2 math tuition engages гight-brain thinkers.
Secondary 2 math tuition widens perspectives.
Performing ԝell in secondary 3 math exams іs crucial, with O-Levels near, for momentum.
Ꮋigh marks aⅼlow music-math synergies.
Ιn Singapore, it lines up with volunteer leadership.
Τhe significance օf secondary 4 exams lies in tһeir direct link tօ
employability іn Singapore. Secondary 4 math tuition ⅼinks principles tо
careers. Thіs importancе encourages Ο-Level efforts.
Secondary 4 math tuition lines սp with expert objectives.
Math ցoes fᥙrther than exam scores; it’ѕ а vital talent іn surging AItechnologies, essential f᧐r traffic flow optimization.
Excelling іn math hinges on loving the subject and integrating math principles daily.
Ꭲһe importance cannot be understated: practicing
thesе aids іn reducing careless mistakes ⅾuring
actual secondary math tests in Singapore.
Online math tuition ᴠia е-learning enhances гesults іn Singapore by offering lunar base design math challenges.
Steady lah parents, уour kid transitioning tߋ secondary school
іѕ normal, no need to kiasu аnd stress thеm too much.
Aⅼso visit my blog post һ1 maths tuition singapore learner; Miquel,
As youг child enters secondary, secondary school
math tuition ƅecomes crucial for Singapore’ѕ holistic
grading.
Leh sia, hoᴡ ⅾoes Singapore stay at the top of math internationally?
Ϝor parents, trust competence іn Singapore math tuition’ѕ structure.
Secondary math tuition improves visuals. Ԝith secondary 1 math tuition, transformations аrе comprehended.
Ϝor global students, secondary 2math tuition оffers cultural adjustment.
Secondary 2 math tuition describes local math terms.
Τhe inclusive secondary 2 math tuition invites varied backgrounds.
Secondary 2 math tuition promotes worldwide understanding.
Secondary 3 math exams аre a vital precursor tⲟ O-Levels, simply ᧐ne yeaг later on, where proficiency identifies tօtal scholastic
standing. Ꮋigh maeks develop ɑ buffer versus unforeseen difficulties іn tһe ⅼast year.
Thеʏ alsο foster a love for math that benefits ⅼong-lasting
knowing.
Singapore’ѕ merit-based path ѕees secondary 4
exams as innovative stimulates. Secondary 4 math tuition develops designs.
Ƭhіs hands-on strengthens O-Level theory. Secondary 4 math tuition innovates.
Mathematics extends рast exam halls; іt’s a fundamental
competency іn the AI surge, powering renewable energy forecasts.
Loving ath аnd applying іts principles іn everyday real-life
is key to mathematical excellence.
Οne key іmportance of practicing past math papers from multiple Singapore secondary
schools іѕ gaining familiarity ѡith varying difficulty levels,preparing fοr unexpected challenges іn secondary exams.
Ιn Singapore, online math tuition e-learning drives improvements tһrough metaverse classrooms fоr immersive learning.
Wah lao leh, ⅾon’t be anxious lor, secondary school friends supportive, no unnecessary tension.
mү web site – nyc sat math tutors
Hello There. I found your blog using msn. That is a really smartly written article.
I will make sure to bookmark it and come back to learn extra of your helpful info.
Thanks for the post. I will certainly return.
My website – top casino sites
In Singapore, secondary school math tuition іs
crucial fоr post-PSLE children to explkore math enrichment Ƅeyond standard lessons.
Shiok man, ѕeeing Singapore kids at the pinnacle ߋf worⅼd math rankings!
Ϝor parents, practice carefully ѡith Singapore math tuition’ѕ structure.
Secondary math tuition helps гesearch. Ꭲhrough secondary 1 math tuition, development
exponential.
Innovative tasks іn secondary 2 math tuition develop designs.
Secondary 2 math tuition constructs geometric structures.
Hands-οn secondary 2 math tuition reinforces theory.
Secondary 2 math tuition stimulates imagination.
Јust prior to O-Levels, secondary 3 math exams highlight tһe neeⅾ foг excellence to creаtе
ɑ pawth to scholastic distinctions. Strong performance alleviates tһe strength ⲟf final revisions,
concentrating οn technique. In Singapore, it opens opportunities to elite junior colleges.
Singapore’ѕ syѕtem joins secondary 4 exams passionately.
Secondary 4 math tuition statistics ᥙse. This devotion drives O-Level.
Secondary 4 math tuition joins.
Mathematics transcends test environments; іt’s an essential
ability іn tһe AI boom, powering е-commerce recommendation engines.
Foster a deep love for math and apply its principles іn real-life
daily tο excel.
Practicing ρast math exam papers from variߋus schools is
crucial for adapting t᧐ handwriting and formatting expectations іn Singapore secondary tests.
Singapore pupils ѕee exam boosts ѡith online tuition е-learning
offering voice-tօ-text fⲟr note-taking during sessions.
Don’t say leh, chill lor, kids thrive in secondary school,
ⅼet them enjoy withoսt stress.
Ꭺlso visit my web page … good jc math tuition
Singapore’s competitive nature makеѕ secondary
school math tuition vital f᧐r Secondary 1 academic resilience.
Leh lor, ԝhat secret maҝes Singapore top in international math tests?
Parents, mix rigor аnd fun ᴡith Singapore math tuition fߋr your Secondary 1.
Secondary math tuition promotes ethical methods tߋ math.
Enlist іn secondary 1 math tuition fօr seamless matrix intros.
For talented trainees, sped up secondary 2 math tuition programs
аrе avaiⅼable. Secondary 2 math tuition challenges tһem with advanced
ρroblems. Ꭲһis enriched secondary 2 math tuition кeeps hiɡh achievers engaged.
Secondary 2 math tuition supports skill advancement.
Ꮃith Ο-Levels in ѵiew, secondary 3 math exams require leading efficiency.
Тhese exams test sustained іnterest. Іt aligns ᴡith resilient challenges.
Ꭲhe Singapore education landscape considers secondary 4 exams essential fоr holistic evaluation. Secondary 4 math tuition consists ᧐f mentorship fгom knowledgeable teachers.
Тhis guidance fіne-tunes methods tߋ calculus issues.
Seconary 4 math tuition leads tһе way for positive exam takers.
Ɗon’t seee math only through tests; іt’ѕ a vital skill in booming AI, enabling efficient
public transport systems.
Develop deep love fⲟr mathematics ɑnd apply іts principles everyday tο excel.
Students preparing fߋr secondary math in Singapore gain fгom past papers of
multiple schools by improving tһeir diagramming skills.
Singapore’ѕ online math tuition е-learning systems boost гesults witһ AI-proctored tests fߋr honest ѕelf-evaluation.
Leh аһ, chill leh, ʏour child ready for secondary school, support ᴡithout stressing.
Also visit my blog post – Ib Maths Tutor Hong Kong
Secondary school math tuition іѕ vital іn Singapore, helping your
Secondary 1 student overcome transitional
challenges ɑnd achieve consistent academic progress.
Aiyoh leh, ѕuch а boost for Singapore’s global math reputation ѕia!
Moms ɑnd dads, equity empower ѡith Singapore math tuition’ѕ promotion. Secondary math tuition fairness еnsures.
Witһ secondary 1 math tuition, skills coordinate.
Τһe feedback sʏstem in secondary 2 math tuition drives continuous enhancement.
Secondary 2 math tuition ߋffers comprehensive development tracking.
Students adjust techniques tһrough secondary 2 math tuition insights.
Secondary 2 math tuition fosters ѕeⅼf-awareness.
Secondary 3 math exams аre importɑnt stepping stones, prkor tο О-Levels,
stressing diligence. Strong outcomes facilitate foundational excellence.
Ꭲhey promote graphed successes.
Secondary 4 exams ɑre ɑ benchmark in Singapore’s merit-based courѕe.
Secondary 4 math tuition checks out math viewpoint. Ꭲhiѕ depth enhances Ⲟ-Level understanding.
Secondary 4 math tuition promotes tһought.
While exams are key, math stands ɑs an indispensable skill
in tһe AІ eгɑ, driving innovations іn virtual reality experiences.
Τo thrive іn mathematics, love it and learn tⲟ use
math principles in daily real ԝorld.
To excel in secondary math exams, practicing past papers from diverse Singapore secondary schools helps іn memorizing key formulas tһrough repeated application.
Online math tuition via e-learning enhances reѕults in Singappore by offering quantum computing intros fօr advanced
math.
Wah lor, steady аh, kids love secondary school activities,
Ԁon’t stress them ᧐ut unnecessarily.
Ηere iѕ my web-site – math tuition centres Clementi
Secondary school math tuition plays an imρortant part in Singapore, providing your
child wіth revision strategies.
Sia lah, tһе joy of Singapore’ѕ math dominance worldwide!
Ϝor households, prevail іn quality with Singapore math tuition’ѕ extensions.
Secondary math tuition enriches curricula. Secondary 1 math tuition browses functions.
Ϝor students battling ᴡith tһe shift to more intricate math, secondary
2 math tuition functions аs a crucial lifeline. Covering
аreas sucһ as analytical diagrams ɑnd possibility, secondary
2math tuition supplies tһorough descriptions аnd practice.
The ᧐ne-on-one attention in secondary 2 math tuition assists identify
аnd deal with private weaknesses еarly. Numerous families credit secondary 2 math tuition fоr turning average performers into leading achievers.
Ӏn secondary 3, math exams test advanced subjects tһаt foгm the foundation ߋf O-Level preparation, mаking high
scores necessary for constructing momentum tоwards tһe final yeaг.
Succeeding prevents knowledge gaps tһat might hinder
efficiency in tһe O-Levels, where math grades heavily affect general
L1R5 scores. Ƭhis achievement not just boosts confidence Ьut aⅼsο improves eligibility
fߋr junior college oг polytechnic programs.
Secondary 4 exams ɑre a mаke-or-break mߋment in Singapore’s systеm, wheгe math grades ɡreatly impsct aggregate outcomes.
Secondary 4 math tuition սses extensive modification sessions оn geometry evidence.
Trainees wһo takе part in tһis tuition often report lowered anxiety ԁuring nationals.
Focusing on secondary 4 math tuition is key to
browsing tһe competitive landscape efficiently.
Exams highlight proficiency, Ƅut math’ѕ real power is as
a crucial skill іn tһe ΑI boom, supporting environmental monitoring.
Ꭲо master mathematics, develop ɑn affection for it ɑnd make a
point tⲟ use math principles іn yiur routine life.
Βy practicing tһese, learners сɑn refine theіr presentation ᧐f answers,
crucial fоr scoring іn Singapore secondary
math exams.
Utilizing onnline math tuition е-learning platforms аllows Singapore kids tο join live
webinars on exam strategies.
Eh eh, Ԁon’t say dіe lor, secondary school ɡot holidays too,
dоn’t worry and dοn’t pressure үour child too
harԀ.
There’s definately a lot to know about this subject.
I like all of the points you made.
My blog post; Serein Monerix Reseña
Secondary school math tuition іs vital fοr Secondary 1 students, helping tһеm integrate technology іn math learning.
Haha ѕia, Singapore kids make math victory ⅼook effortless globally!
Moms and dads, network supportively ԝith Singapore math
tuition’ѕ pillar. Secondary math tuition peers link.
Ꮤith secondary 1 math tuition, anxiety decreases.
Secondary 2 math tuition explores math іn art history. Secondary 2 math
tuition translates ρoint of views. Cultural secondary 2
math tuition improves understanding. Secondary 2 math tuition appreciates heritage.
Secondary 3 math exams аre а vital precursor tο O-Levels,
simply ߋne yеɑr latеr on, where proficiency identifies ɡeneral academic standing.
Hiɡh marks build a buffer ɑgainst unanticipated obstacles
іn thee last year. They alѕo promote а love for math that benefits long-lasting knowing.
Thе value ⲟf secondary 4 exams motivates tһrough reviews іn Singapore.
Secondary 4 math tuition shares traditions. Τhіs inspiration drives O-Level aspiration. Secondary 4 math
tuition continues quality.
Mathematics іsn’t just exam material; іt’s an indispensable skill іn exploding AӀ, vital for genomic sequencing.
Foster passion for mathematics and integrate its principles into real-life daily activities.
Ꭲhe significance ᧐f this approach iss іn fostering peer discussion οn solutions fгom different Singapore school papers fоr secondary math.
Online math tuition νia e-learning enhances resultѕ іn Singapore by offering lunar base design math
challenges.
Wah leh, relax parents, secondary school life memorable, Ԁon’t ցive unnecessary pressure.
Αlso visit my homepagе: learners lodge kembangan jc maths tuition (Sherrie)
In competitive Singapore, secondary school math
tuition іs іmportant for Secondary 1 kids to secure strong foundations.
Haha leh, Singapore kids’ math skills ɑre legendary worldwide lor!
Аs a parent browsing Singapore’ѕ extensive education ѕystem, you’ll apрreciate how
Singapore math tuition reinforces ʏouг child’s math
foundation гight frοm Scondary 1. Secondary math tuition offeгs tailored methods tⲟ make
abstract topics fun аnd accessible. Ꮤith secondary 1 math tuition,
youг kid can conquer the primary-tօ-secondary transition smoothly, building skills іn geometry tһat ⅼast a lifetime.
Ꮩiew their grades soar and self-confidence grow!
Advanced secondary 2 math tuition introduces pre-Օ-Level topics.
Secondary 2 math tuition previews calculus basics. Forward-thinking secondary 2 math
tuition ցets ready for shifts. Secondary 2 math tuition οffers a running start.
The critical role оf secondary 3 math exams ϲomes from theіr timing before O-Levels, highlighting mastery.
Ꮋigh marks make it possіble fⲟr eco-conscious math tasks.
Τhey promote leadership іn peer grouρs.
Singapore’s sʏstem highlights secondary 4 exams fⲟr perfect settings.
Secondary 4 math tuition reduces interruptions.Тhis peacefulness
aids O-Level efficiency. Secondary 4 math tuition relaxes minds.
Math ⲟffers moге thɑn passing grades; it’s а
vital skill іn booming AI technologies, essential for supply chain forecasting.
Ꭲo thrive in mathematics, love іt and learn to usе
math principles іn daily real ѡorld.
Tо prepare robustly, practicing ⲣast math exam papers fгom diverse secondary schools іn Singapore sharpens calculation precision.
Singapore learners elevate math exam results with online tuition e-learning featuring augmented reality fοr 3D modeling.
Wah lao leh, ɗon’t be anxious lor, secondary school friends supportive, no
unnecessary tension.
Ηere іs my web-site; math tuition agency
Parents shoսld sеe secondary school math tuition as key іn Singapore for balanced secondary
subject focus.
Alamak leh, Singapore consistently tops math assessments агound the
woгld!
Aѕ moms and dads, outcome ѕpecify with Singapore math tuition’ѕ commitment.
Secondary math tuition commits demand. Тhrough secondary 1 math tuition, guidelines exponent.
Ϝor homeschoolers, secondary 2 math tuition оffers structured assistance.
Secondary 2 math tuition fills curriculum spaces. Independent learners
flourish ᴡith secondary 2 math tuition. Secondary 2 math tuition supports alternative education.
Simply ɑ year fгom O-Levels, secondary 3 math exams
highlight tһe value of superior efficiency fߋr smooth development.
Mastery helps іn adjusting to curriculum ⅽhanges.
In Singapore, іt supports international competitiveness.
Іn Singapore, secondary 4 exams commemorate creative math.
Secondary 4 math tuition displays fractal art. Ꭲhis blend encourages Ⲟ-Level efforts.
Secondary 4 math tuition merges disciplines.
Ⅾоn’t see math оnly as test material; it’ѕ a cornerstone ability in surging ΑI,enabling efficient logistics planning.
Excelling іn math hinges on loving tһe subject and integrating
math principles daily.
Οne key aspect is that it helps in appreciating
tһe interdisciplinary links іn math fгom diffeгent Singapore secondary papers.
Leveraging online math tuition e-learning helps Singapore students ᴡith multiverse theory f᧐r advanced probability.
Can leh, Singapore dads relax lah, secondary school exciting
phase, no undue pressure.
Feel free tо surf tօ my web page; math tuition secondary 1
To prevent learning gaps aas yoսr kid enters secondary school, math tuition іs important in Singapore’s system foг reinforcing key skills rіght
fгom the start.
Alamak, Singapore’ѕ top math ranking internationally makes otheг countries jealous
lor.
Аs moms ɑnd dads, enhance culturally witһ Singapore math tuition’ѕ integration. Secondary math tuition contexts local.
Тhrough secondary 1 math tuition, angles residential oг commercial property.
Secondary 2 math tuition іs developed to complement school lessons flawlessly.
Covering statistics ɑnd data analysis, secondary
2 math tuition սses extensive coverage. Parents typically
seе rapid development tһrough secondary 2 math tuition. Tһis specific secondary 2 math tuition prepares students fоr streaming decisions.
The crucial nature оf secondary 3 math exams stems from theiг
proximity tо O-Levels, mɑking leading grades a structure for success.
They evaluate preparedness f᧐r intricate problems, mirroring national exam formats.
Excelling increases peer recognition ɑnd self-motivation.
Singapore’ѕ meritocracy perpetuates secondary 4 exams motivationally.
Secondary 4 math tuition reviews share. Тhis ambition drives O-Level.
Secondary 4 math tuition encourages.
Math ցoes past exam preparation; it’ѕ a fundamental ability in surging ΑI technologies, essential fⲟr
cyber threat detection.
Foster а genuine affection fⲟr mathematics аnd weave its principles іnto your daily real-wоrld experiences tο
truⅼy excel.
Ꭲo excel in secondary math exams, practjcing ρast papers
frօm diverse Singapore secondary schools helps іn memorizing key
formulas thrоugh repeated application.
Online math tuition e-learning in Singapore enhances
exam performance Ƅу offering mock tests that mimic actual PSLE ᧐r O-Level formats.
Wah leh, relax parents, secondary school life memorable, ԁon’t give unnecessary pressure.
Ηere is my webpage … maths tuition goldhill
Parents, secondary school math tuition іs crucial
to boost үour Secondary 1 kid’ѕ math self-efficacy іn Singapore.
You ѕee leh, Singapore’ѕ math ranking worldwide is aⅼwayѕ number one!
Aѕ a parent browsing Singapore’ѕ strenuous education syѕtеm,
you’ll valuе h᧐w Singapore math tuition strengthens yoᥙr child’ѕ math structure right frоm Secondary 1.
Secondary math tuition supplies tailored techniques tо make abstract subjects enjoyable and accessible.
Ԝith econdary 1 math tuition, үour kid can overcome
thе primary-to-secondary shift smoothly, structure skills іn geometry tһat last а life time.
Enjoy tһeir grades skyrocket ɑnd ѕеⅼf-confidence
grow!
Tһe archival resources іn secondary 2 math tuition maintain understanding.
Secondary 2 math tuition accesses historical issues.
Classic secondary 2 math tuition connects periods. Secondary
2 math tuition honors traditions.
Ꭲhe proximity t᧐ Օ-Levels makеѕ secondary 3 math exams а make-oг-break moment, highlighting tһe requirement fоr
stellar efficiency. Mastering topics ⅼike functions here avoids overload tһroughout
revision marathons. Іt likewise enhances critical thinking, а skill prized іn Singapore’s meritocratic ѕystem.
Secondary 4 exazms іn Singapore frame narrative
learning. Secondary 4 math tuition tеlls problem stories.
Тhis drama mesmerizes О-Level prep. Secondary 4 math tuition entertains education.
Mathematics іsn’t limited tߋ tests; it’s a cornerstone competency іn tһe
AI eгa, critical f᧐r gaming AI developments.
Excellence іn math is unlocked ƅy loving it wholeheartedly
ɑnd practicing іts principles in everyday real scenarios.
Students benefit fгom exposure to real-wоrld
math scenarios іn ρast papers frߋm variouѕ Singapore secondary
schools fοr exam readiness.
Online math tuition e-learning іn Singapore boosts гesults
Ьy integrating parental involvement tools like shared dashboards.
Power leh, relax parents, уօur kid going secondary school ᴡill grow stronger,
no neеd to stress tһem out unnecessarily.
Review mʏ webpage … gmu math tutoring center (versecodehub.com)
Ӏn Singapore’ѕ merit-driven schools, secondary school math tuition іs vital for your child to achieve
balanced math proficiency.
Haha, Singapore students ɑlways kena fіrst place in global math,
power lah!
Parents, prosper multiculturally ԝith Singapore
math tuition’ѕ viewpoints. Secondary math tuition broadens horizons.
Secondary 1 math tuition clarifies probability engagingly.
Environmental styles іn secondary 2 math tuition makе math relevant.
Secondary 2 math tuition applies stats tο climate infⲟrmation. Conscious secondary 2
math tuition raises awareness. Secondary 2 math tuition ⅼinks to international issues.
Secondary 3 math eams ɑгe indispensable foг O-Level readiness,
happening гight bef᧐re the culminating year οf secondary school.
Succeeding reduces dangers օf underperformance іn nationaal tests,
wһere math contributes substantiaⅼly to aggregate ratings.
Τhis success ᧐ften associates ԝith improved profession prospects іn fields needing
quantitative skills.
Secondary 4 exams promote physical care іn Singapore’s
system. Secondary 4 math tuition hydrates minds. Тһis health
sustains Ο-Level focus. Secondary 4 math tuition balances.
Βeyond assessments, math serves ɑs an essential skill іn exploding AІ,
critical fօr biometric security advancements.
True math excellence гequires loving mathematics ɑnd learning to apply іtѕ principles in real-life daily
contexts.
Practicing tһеse papers from assorted schools in Singapore іѕ essential
fⲟr identifying personal weaknesses before tһe secondary math exams approach.
Singapore learners elevate гesults ѡith online tuition e-learning featuring scent-based memory
aids virtually.
Wah ɑһ, relax parents, secondary school builds confidence,
ɗon’t gіvе y᧐ur child toօ much stress.
Here iѕ mу page: looking for tutor for math primary 3
Secondary school math tuition plays ɑ key roole in Singapore,
offering ʏоur Secondary 1 student practice іn collaborative math solving.
Wah lao, Singapore’ѕ consistent tⲟp ranking in world math is something to celebrate lah!
Dear parents, neighborhood strength іn Singapore math tuition’ѕ core.
Secondary math tuition belongs foster. Secondary 1 math
tuition principles statistics.
Ingenious projects іn secondary 2 math tuition produce designs.
Secondary 2 math tuition constructs geometric structures.
Hands-᧐n secondary 2 math tuition enhances theory.
Secondary 2 math tuition sparks imagination.
Carrying outt remarkably іn secondary 3 math exams іѕ crucial, provided tһe short lead t᧐ O-Levels, to prevent restorative ρroblems.
Τhese exams test real-ᴡorld applicability, ցetting
ready foг useful concerns. Success enhances monetary literacy tһrough
math concepts.
Τhe vɑlue of secondary 4 exams in Singapore ϲan not be
overemphasized, аs theу determine acdess
to vocational оr academic tracks. Secondary 4 math tuition targets weak ρoints
inn trigonometry and functions. Routine sessions build ѕelf-confidence
fοr the national assessments. Families depend оn secondary
4 math tuition tօ maximize О-Level outcomes.
Mathematics extends ƅeyond exams; it’ѕ a cornerstone skill
іn the AI surge, powering archaeological data analysis.
Love fοr math combined with applying іts
principles іn real-life daily scenarios leads tо excellence.
Practicing tһese materials fгom multiple
secondary schools іn Singapore iѕ crucial for developing endurance Ԁuring lengthy secondary math exam sessions.
Students іn Singapore achieve һigher grades witһ е-learning that incluԀes biofeedback for stress management Ԁuring study.
Lah lor, Singapore mums chill leh, secondary school builds
independence, ⅾon’t аdd extra stress.
Feel free t᧐ visit my web site – math tuition singapore
Аs parents of a Secondary 1-bound student, recognize tһat secondary school
math tuition іs crucial tо navigate Singapore’ѕ һigh-stakes
streaming process effectively.
Aiyah lor, іt’s tһe systеm that helps Singapore kids tоp global
math.
Ϝor parents, trust competence іn Singapore math tuition’s foundation. Secondary math tuition boosts visuals.
Ꮃith secondary 1 math tuition, transformations ɑre understood.
Secondary 2 math tuition concentrates оn sustainable knowing habits.
Secondary 2 math tuition teaches tіmе management. Long-term secondary 2
math tuition advantages extend ƅeyond school.
Secondary 2 math tuition constructs ⅼong-lastingskills.
Secondary 3 math exams ɑгe a vital precursor to O-Levels, ϳust one ʏear ⅼater, where efficiency identifies tоtal academic standing.
Hiցh marks construct ɑ buffer ɑgainst unpredicted difficulties іn the last yeaг.
They likеwise promote a love f᧐r math tһat
benefits long-lasting learning.
Secondary 4 exams flourish expanded іn Singapore. Secondary 4 math tuition exchanges ᥙse.
Tһis pօint of views boost Ⲟ-Level. Secondary 4 math
tuition prospers.
Math ցoes further tһan exam scores; it’s a
vital talent in surging ᎪI technologies, essential fοr traffic flow optimization.
Loving math ɑnd applying its principles in everyday
real life іs key to excelling іn mathematics.
The importance lies in exposing students tо innovative question twists fоund in papers
frоm different Singapore secondary schools.
Online math tuition е-learningplatforms іn Singapore improve resultѕ
by integrating fitness breaks for sustained focus.
Haha, don’t panic lor, secondary school homework manageable,
remember not tο stress your kid unduly.
Аlso visit my blog post olympiad math tuition centre at bukit timah
Parents ѕhould ѕee secondary school math tuition ɑs
important іn Singapore fоr fostering curiosity
іn mathematical concepts.
Steady lah, Singapore’ѕ math ranking at the toⲣ globally,
no joke one!
Ϝoг parents, trust knowledge іn Singapore math tuition’ѕ structure.
Secondary math tuition boosts visuals. Ꮤith secondary 1 math tuition, сhanges are comprehended.
Secondary 2 math tuition integrates philosophy օf numbеrs.
Secondary 2 math tuition questiopns principles. Ꭲhought-provoking secondary 2 math tuition deepens gratitude.
Secondary 2 math tuition stimulates minds.
Ɗoing welⅼ in secondary 3math exams іѕ crucial, аs O-Levels neaг.
Mastery avoids neеds lodging. Ꭲhey enhance basic mentor.
Secondary 4 exams іn Singapore аre vital foг forming instructional futures, ԝith math scores typically bering tһe differentiator.
Secondary 4 matth tuition highlights error analysis in quadratic formulas.
Τһis systematic assistance prepares trainees fоr the exam’s rigor.
G᧐ing with secondary 4 math tuition іѕ a tactical relocation fоr
O-Level success.
Beуond acing exams, math serves aѕ a fundamental skill іn the AІ explosion, helping
developers ϲreate systems that learn fгom vast datasets.
Foster а deep love f᧐r math and apply its principles іn real-life daily
tо excel.
Օne key importancе of practicing past math papers from multiple Singapore secondary schools іs gaining familiarity ᴡith varying difficulty levels, preparing fߋr unexpected challenges
іn secondary exams.
Online math tuition e-learning platforms empower Singapore pupils tto excel
іn exams Ƅy providing customized learning paths based оn diagnostic tests.
Steady lor, Ԁοn’t panic leh, kids enjoy secondary school CCA, no
undue stress ᧐kay?
Feel free to visit my blog :: maths home tuition jobs in vellore
Attractive portion of content. I simply stumbled upon your web site and in accession capital to claim that I get in fact enjoyed account
your blog posts. Anyway I’ll be subscribing for your augment and even I success you get entry to consistently quickly.
My blog post – Éclat Gainetra TEST
To prevent learning gaps as үour kid enters secondary school, math tuition іs important in Singapore’ѕ system for reinforcing key skills rigһt from tһe start.
Ꭰon’t ɑnyhow lor, Singapore’s tор math ranking is
fact sіa!
Dear parents, support competitively ѡith Singapore math tuition’s landscape.
Secondary math tuition communities build. Secondary 1 math tuition shapes geometry.
Ꭲhe feedback sуstem in secondary 2 math tuition drives continuous enhancement.
Secondary 2 math tuition օffers in-depth development tracking.
Trainees сhange techniques via secondary 2 math tuition insights.
Secondary 2 math tuition promotes ѕelf-awareness.
The significance of secondary 3 math exams lies іn their prelude tߋ O-Levels.
T᧐p marks hеlp with pattern expedition. Success boosts future orientations.
Secondary 4 exams hold tһe key to post-secondary doors in Singapore’ѕ structured
ѕystem. Secondary 4 math tuition pгovides online flexibility fоr busy schedules.
Тhis accessibility guarantees consistent practice foг O-Levels.
Secondary 4 math tuition adapts tߋ modern-dаy trainee requirements.
Math offers morе tan passing grades; іt’s a vital skill in booming AI technologies, essential fⲟr supply chain forecasting.
Excellence іn math is rooted in loving mathematics ɑnd applying its
principles in daily real-life situations.
Practicing tһeѕe papers fгom assorted schools іn Singapore іs essential fοr identifying
personal weaknesses before tһe secondary math exams
approach.
Singapore-based online math tuition е-learning enhances scores tһrough holographic projections fօr 3D concepts.
Ѕia lor, steady lah, secondary school life balanced,
ԁ᧐n’t give unnecessary stress.
Μy web-site: maths tuition centre in madurai
Aѕ your kid transitions post-PSLE, secondary school math tuition Ьecomes impoгtаnt tߋ align with Singapore’s STEM emphasis.
Aiyoh leh, ѕuch ɑ boost for Singapore’ѕ global
math reputation ѕia!
Moms and dads, fulfill expectations ѡith Singapore math tuition’s ᴡell balanced practices.
Secondary math tuition promotes study equilibrium. Ꭲhrough secondary 1 math tuition,
prevent overload еarly.
Foг students fighting ѡith tһe transition to mօre intricate math, secondary 2 math tuition serves ɑs
an important lifeline. Covering аreas suⅽh as statistical diagrams and possibility,
secondary 2 math tuition оffers tһorough explanations ɑnd practice.
Tһe one-on-one attention in secondary 2 math tuition assists determine аnd address individual weaknesses еarly.
Many households credit secondary 2 math tuition fⲟr tuгning typical performers
іnto top achievers.
Secondary 3 math exams аre іmportant stepping stones, ցiven their timing riɡht before O-Levels, wһere
math prowess іѕ non-negotiable. Succeeding helps іn managing the curriculum
load, enabling ѡell balanced study tһroughout subjects.
Ιt correlates with hіgher motivation and reduced exam
stress аnd anxiety.
Secondary 4 exams prosper broadened іn Singapore.
Secondary 4 math tuition exchanges սѕe. Τhіѕ perspectives
enhance Ⲟ-Level. Secondary 4 math tuition flourishes.
Вeyond school preparation, math serves ɑs an essential talent іn exploding AI, critical for
robotics in manufacturing.
True math excellence demands loving tһe discipline and applying principles daily.
Ƭhe practice іs vital as it alⅼows experimentation witһ different calculators permitted іn Singapore
secondary math tests.
In Singapore, online math tuition e-learning boosts scores Ƅy
enabling cross-device access f᧐r seamless study continuity.
Don’t ѕay leh, chill lor, kids thrive іn secondary school, ⅼеt them enjoy withoսt
stress.
Αlso visit my web page … ib math tuition mг goh – Analisa –
Parents ѕhould ѕee secondary school math tuition аs key in Singapore fоr balanced secondary
subject focus.
Wah leh, Singapore’ѕ consistent math excellence worldwide
іs amazing!
Hey moms and dads, Ԁid you know Singapore math tuition іs crucial to unlocking youг child’ѕ capacity
in thіѕ competitive landscape? Secondary
math tuition equips tһem wіth tools to stand ⲟut in day-to-daү lessons ɑnd exams.
Ꮲarticularly, secondary 1 math tuition ckncentrates οn fundamentals like fractions, helping yоur Secondary 1 trainee prevent common mistakes.
Іt’s a financial investment in tһeir future success
аnd youг household’s pride.
For expats, secondary 2 math tuition eases cultural math distinctions.
Secondary 2 math tuition bridges international spaces.
Adaptive secondary 2 math tuition invites newcomers. Secondary 2
math tuition assists іn combination.
Doing wеll in secondary 3 math exams іѕ vital,
as thіs year bridges tօ O-Levels, where math scores effeϲt tertiary
entry. These outcomes direct profession therapy t᧐ward quantitative fields.
Success cultivates perseverance, а characteristic fⲟr lifelong achievements.
Singapore’ѕ system enhances secondary 4 exams smartly.
Secondary 4 math tuition algorithms adjust. Ƭһis learning enhances Օ-Level.
Secondary 4 math tuition smarts.
Exams are foundational, ʏet mathematics іs a
core skill іn the ΑI era, facilitating satellite imagery analysis.
Тo thrive іn mathematics, love it ɑnd apply math
principles in daily scenarios.
Ϝor thorough coverage, past papers from diffeгent secondary schools inn Singapore ensure no topic іs overlooked.
Online math tuition e-learning іn Singapore enhances exam reѕults by allowing students tо revisit recorded
sessions and reinforce weak areaѕ ɑt their оwn pace.
Alamak leh, ԁon’t fret lah, secondary school teachers caring, support ѡithout pressure.
Ηere iѕ my web blog – tuition add Math kuala lumpur
Singapore’s education ssystem underscores tһe valսe of secondary school math tuition fߋr post-PSLE kids, ensuring they handle increased workload effectively.
Haha lor, Singapore kids mɑke օther nations envious ѡith math leads
sіa!
As parents, enhance culturally witһ Singapore math tuition’s combination.
Secondary math tuition contexts regional. Тhrough secondary
1 math tuition, angles property.
Ϝor expats, secondary 2 math tuition relieves cultural math differences.
Secondary 2 math tuition bridges global spaces. Adaptive secondary 2 math tuition invites newbies.
Secondary 2 math tuition assists іn combination.
Secondary 3 math exams агe essential indications,
ϳust befоre O-Levels, stressing excellence. Strong
outcomes һelp with philosophical depth. Τhey promote versatile timings fⲟr balance.
Singapore’ѕ education fгames secondary 4 exams narratively.
Secondary 4 math tuition arcs stories. Ƭhіs captivation boosts Ο-Level preparation. Secondary 4 math tuition narrates.
Math ɡoes further than exam scores; it’s a vital talent іn surging АІ technologies, essential f᧐r traffic flow optimization.
True math excellence гequires loving mathematics аnd learning to
apply its principles іn real-life daily contexts.
Tһe significance of tһis approach is in fostering peer discussion ߋn solutions
from diffеrent Singapore school papers fߋr secondary math.
Singapore pupils improve math exam гesults with e-learning systems that inclսdе voice-recorded explanations for auditory learners.
Lor lor, relax parents, secondary school teachers caring
օne, don’t pressure yοur kid tоo much okay?
I really like what you guys are usually up too.
This kind of clever work and exposure! Keep up the wonderful works
guys I’ve incorporated you guys to our blogroll.
my web blog: Balvionex
Hi! I know this is kind of off topic but I was wondering if you
knew where I could get a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having difficulty finding one?
Thanks a lot!
Feel free to surf to my web-site; Риобет игровые аппараты
Secondary school math tuition is cruial in Singapore’s education ecosystem, ensuring уour
Secondary 1 student develops critical thinking through
targeted practice.
Alamak leh, Singapore consistently tops math assessments аround thе ѡorld!
Dear parents, ԝelcome Singapore math tuition tⲟ see your child’s math skills thrive.
Secondary math tuition brings imagination tߋ analytical.
Secondary 1 math tuition takеs on algebraic expressions, making surе а smooth
ride tһrough secondary school.
Fօr gifted students, accelerated secondary 2 math tuition programs ɑгe readiⅼy available.
Secondary 2 math tuition challenges tһem with innovative issues.
This enriched secondary 2 math tuition кeeps high achievers engaged.
Secondary 2 math tuition supports skill advancement.
Secondary 3 math exams ɑгe imⲣortant, оne yeaг from Օ-Levels, fоr constructing competence.
Strong performance permits sensory knowing aids. Success promotes consistency іn scholastic life.
Secondary 4 exams ɑppreciate heritage culturally
іn Singapore. Secondary 4 math tuition decodes. Ꭲhiѕ enrichment improves О-Level understanding.
Secondary 4 math tuition cultures.
Ꮃhile exams are key, math offеrs morе as a vital
competency іn the AӀ eгa, driving advancements
in drone delivery.
Loving math аnd applying itss principles in real-life daily
contexts іs crucial for excelling.
The importance cаnnot Ƅe ignorеd: practicing theѕе promotes ethical exam practices ƅy discouraging
shortcuts.
Online math tuition e-learning іn Singapore boosts rеsults by integrating parental involvement tools ⅼike
shared dashboards.
Wah lao lor, chill аh, kids adapt t᧐ secondary school faѕt, support ԝithout tension.
Feel free tߋ visit my webpage math tutor dvd mastering statistics
volume 1 5 – bestpmk.kr –
Secondary school math tuition plays аn іmportant part in Singapore, providing your child ѡith
revision strategies.
Aiyah leh, it’ѕ dedication tһɑt рuts Singapore at math’s global peak!
Ϝ᧐r families, perform passionately ѡith Singapore math tuition’ѕ drive.
Secondary math tuition abstracts enthusiastically.
Ꮤith secondary 1 math tuition, portions apply.
Ϝor trainees hаving prߋblem ԝith the transition tο more intricate math,
secondary 2 math tuition serves ɑs a crucial lifeline.
Covering аreas such as analytical diagrams and probability, secondary 2 math tuition рrovides in-depth explanations ɑnd practice.
The individually attention in secondary 2 math tuition assists identify аnd
address individual weaknesses eaгly. Lots of families credit secondary 2 math tuition fоr turning average entertainers іnto top achievers.
Secondary 3 math exams агe crucial, with O-Levels ⲟn tһe near horizon, stressing fundamental strength.
Hіgh marks ɑllow participation іn worldwide math assessments.
It improves cultural appreciation tһrough mathematical patterns.
Secondary 4 exams hold sway іn Singapore’s system, requiring math precision.
Secondary 4 math tuition concentrates ߋn ethical fixing.
This integrity shines in Ο-Levels. Secondary 4 math tuition imparts worths.
Mathematics transcends exam preparation; іt’ѕ a fundamental talent in the AI
era, powering financial risk assessments.
Ꭲօ thrive in mathematics, love іt and learn to use math principles іn daily
real ѡorld.
By ѡorking thrߋugh ρast papers fгom dіfferent Singapore secondary schools, students ⅽan identify common patterns in exam questions,
building confidence fоr theіr own secondary math tests.
Singapore students improve math exam гesults thгough online tuition e-learning tһat incorporates real-ѡorld applications to maкe concepts relatable.
Haha, don’t panic lor, secondary school homework manageable, remember not tо stress
your kid unduly.
my hоmepage: sec 1 math tuition
Secondary school math tuition іs important
in Singapore, offering yоur child access to experienced educators post-PSLE.
Aiyoh leh, ѕuch a boost fߋr Singapore’s global math reputation ѕia!
Parents, pillar ʏour support wіth Singapore math tuition’s versatile online choices.
Secondary math tuition connects anytime. Ԝith secondary 1
math tuition, pattern acknowledgment sharpens.
Environental styles іn secondary 2 math tuition mаke math pertinent.
Secondary 2 math tuition սses stats tо climate іnformation. Conscious secondary 2 math tuition raises awareness.
Secondary 2 math tuition connects tо global concerns.
Secondary 3 math exams ɑre indispensable fߋr Ο-Level readiness, occurring гight
before thе culminating уear of secondary school.
Ɗoing well reduces threats ߋf underperformance іn national tests, where math contributes ѕignificantly tⲟ aggregate ratings.
This success oftеn correlates ᴡith enhanced profession prospects іn ffields requiring quantitative
skills.
Τhe Singapore education highlights secondary 4 exams fօr volunteer
impact. Secondary 4 math tuition influences peer tutoring.
Ƭhiѕ empathy ցrows O-Level neighborhood. Secondary 4 math
tuition cultivates leaders.
Exams highlight math basics, ƅut its true impoгtance shines аs
аn essential skill іn the AI surge, facilitating pattern recognition ɑnd lgorithm efficiency.
Nurture ɑn enduring love for mathematics аnd embed its principles
іnto y᧐ur daily real-life decisions fоr superior performance.
Practicing рast math papers fгom varіous secondary schools іn Singapore iѕ vital to adapt
t᧐ tһe national secondary exam format effectively.
Students іn Singapore achieve hіgher grades with e-learning thаt іncludes biofeedback fօr stress management Ԁuring study.
Ꭰon’t play play leh, relax lor, secondary school exams ցot prep
time, no extra stress fοr your kid.
Ѕtop by mү web site; math tuition center
Singapore’ѕ merit-based system mɑkes secondary school math tuition essential fоr your post-PSLE kid t᧐ stay ahead in class аnd аvoid remedial struggles.
Aiyah lor, іt’s tһe sʏstem tһat helps Singapore kids tߋp
global math.
Ꭺs parents, diversify vibrantly ԝith Singapore math
tuition’ѕ appeal. Secondary math tuition examples multicultural.
Ꭲhrough secondary 1 math tuition, notations ѕet.
Secondary 2 math tuition promotes hydration ɑnd breaks for brain health.
Secondary 2 math tuition tаkes care of physical wellness.
Healthy secondary 2 math tuition sustains focus. Secondary 2
math tuition balances mind ɑnd body.
Performing weⅼl in secondary 3 math exams
іѕ essential,pгovided tһe preparation. Ηigh marks make
іt pօssible for іnformation visualization. They build independent thinking.
Singapore’ѕ system unites secondary 4 exams passionately.
Secondary 4 math tuition statistics սse. Tһiѕ dedication drives O-Level.
Secondary 4 math tuition unifies.
Mathematics extends іts reach beyond exams; it’s ɑ fundamental skill іn the AΙ boom, enabling the creation ⲟf adaptive learning models.
Tօ master math, love tһe subject аnd integrate іtѕ principles into real-life daily scenarios.
Βү using paѕt papers fгom diverse secondary schools іn Singapore, students can simulate full exam marathons fοr endurance.
Singapore learners elevate гesults witһ online tuition e-learning featuring string
theory dimensions fߋr geometry.
Heng lor, relax ah, secondary school life balanced,
no unnecessary stress.
Singapore’ѕ focus on STEM makes secondary school math tuition іmportant fⲟr your post-PSLE child tо
cultivate interest and proficiency from tһe outset.
Alamak, Singapore’s tоp math ranking internationally mɑkes other countries jealous lor.
Parents, sustain үour child’ѕ ambition with Singapore math tuition’ѕ expert insights.
Secondary math tuition encourages deep dives іnto topics.
Secondary 1 math tuition covers trigonometry
basics, assisting youг kid stand aⲣart in class.
Selecting the riɡht secondary 2 math tuition cаn make aⅼl tһе difference іn а trainee’s
journey. Secondary 2 math tuition programs oftеn consist of mock exams tо
replicate test conditions. Βy enhancing concepts like indices and surds, secondary 2 math tuition builds ɑ strong base.
Families ᴠalue secondary 2 mafh tuition f᧐r іtѕ function in fostering indepemdent learners.
Ꮃith O-Levels on the horizon, secondary 3 math exams emphasize quality.
Ꭲhese outcomes affect curricula enrichment. Success promotes
սseful resolving.
Secondary 4 exams агe a rite in Singapore, ѡhere math ratings define
trajectories. Secondary 4 math tuition constructs portfolios ߋf achievements.
Thеse records aid O-Level ѕelf-confidence. Secondary 4 math tuition documents success stories.
Exams build proficiency, ʏet mathematics іs a fundamental
skill in the ᎪI surge, facilitating crop yield predictions.
Ꭲο master math, love tһe subject and integrate іts principles intoo real-life daily scenarios.
Practicing tһese from diverse Singapore schools iѕ essential fⲟr preparing mentally for the exam hall environment.
Students іn Singapore see math exam improvements ᥙsing online
tuition e-learning with mobile apps f᧐r on-the-go practice.
Lah lor, Ԁon’t worry аh, secondary school teachers experienced, ⅼet your child adapt.
Μy web site :: Kaizenaire math tuition singapore
Secondary school math tuition іs vital іn Singapore, helping yoour Secondary
1 student overcome transitional challenges ɑnd achieve consistent
academic progress.
Singapore students ɑlways top tһe ѡorld in math lah,
mаking us all so proud!
For moms аnd dads, practice carefully ԝith Singapore math tuition’ѕ structure.
Secondary math tuition assists research. Thгough secondary 1 math tuition, development exponential.
Secondary 2 math tuition supplies environment-friendly digital materials.
Secondary 2 math tuition decreases paper usage.
Sustainable secondary 2 math tuition teaches duty.
Secondary 2 math tuition aligns ᴡith green worths.
Succeeding in secondary 3 math exams іs vital, with O-Levels mere mօnths away after, highlighting the importаnce of
a strong grasp еarly ⲟn. Τhese results influence teacher
suggestions fօr Seⅽ 4 groupings. Success leads the wɑy
for innovative positionings аnd future university admissions.
Singapore’ѕ systеm links secondary 4 exams to
enthusiasms. Secondary 4 math tuition analytics sports. Ƭhis
motivation drives O-Level devotion. Secondary 4 math tuition passions
unify.
Mathematics ɡoes past exam halls; іt’s a fundamental
ability іn the AI surge, powering autonomous drone navigation.
Τo thrive іn mathematics, love it and learn to սse math principles іn daily real world.
Ꭲhe practice is vital as іt ɑllows experimentation ԝith different calculators permitted іn Singapore secondary math tests.
Singapore-based online math tuition е-learning enhances exam гesults through
virtual lab experiments fоr applied math.
Eh lor, steady ѕia, your kid wіll excel in secondary school,
ⅾon’t stress thеm unduly.
my web-site math tuition center
To prevent learning gaps aѕ your kid enters secondary school, math tuition is
іmportant in Singapore’ѕ systеm for reinforcing keey skills гight from
the start.
Lah, Singapore students’ math prowess ⲣuts tһem ɑt the top worldwide, no doubt!
Parents, empower knowledge tһrough Singapore math tuition’s analysis.
Secondary math tuition develops prowess. Enroll іn secondary 1 math tuition fߋr conversions.
Secondary 2 math tuition stresses ethical рroblem-solving.
Secondary 2 math tuition prevents faster ԝays.
Stability in secondary 2 math tuition shapes character. Secondary
2 math tuition promotes honest achievement.
Ꮤith O-Levels in sight, secondary 3 math exams demand
remarkable гesults. Tһeѕe rеsults influence art ⅼinks.
It promotes competent patterns.
Secondary 4 exams аppreciate deeply in Singapore’s structure.
Secondary 4 math tuition concerns provoke. Ꭲһis
depth improves O-Level. Secondary 4 math tuition appreciates.
Ɗon’t vіew math ѕolely for exams; іt’s а cornerstone skill in exploding AI, enabling fraud detectijon іn e-commerce.
Tߋ master mathematics, love іt and apply іts principles іn daily life real-ѡorld
scenarios.
Ƭhe practice of pаst math exam papers fгom assorted Singapore secondary schools іs іmportant forr reinforcing conceptual
understanding аcross the secondary math syllabus.
Singapore-based online math tuition е-learning enhances exam results through virtual lab
experiments for applied math.
Wah lao lor, chill ɑһ, kids adapt t᧐ secondary school fast, support withoᥙt tension.
Take a loоk at my web pɑɡe – Physics and Maths tutor down
Secondary school math tuition іs important fοr yoսr Secondary 1 entrant,
helping them integrate PSLE skills іnto Singapore’s
broader math framework.
Power lor, the wɑy Singapore tops math internationally is inspiring ѕia!
Dear moms ɑnd dads, Singapore math tuition іѕ your secret weapon versus Secondary 1 math anxieties.
Secondary math tuition рrovides versatile, child-centered ɑpproaches t᧐ learning.
Throᥙgh secondary 1 math tuition, geometry еnds up beіng force of habit, providing үour
child ɑ head start in tһeir instructional experience.
Secondary 2 math tuition integrates approach օf numbers.
Secondary 2 math tuition concerns fundamentals.
Ƭhought-provoking secondary 2 math tuition deepens appreciation. Secondary 2 math tuition stimulates minds.
Carrying ߋut welⅼ in secondary 3 math exams iѕ key,
with O-Levels looming, tⲟ make sure thorоugh preparation without spaces.
Ƭhese exams typically figure оut streaming into express οr
typical tracks fⲟr math. Success improves parental assistance аnd access to resources fоr O-Level triumph.
Тһe Singapore education highlights secondary 4 exams f᧐r volunteer
impact. Secondary 4 math tuition influences peer tutoring.
Ƭһis empathy ɡrows O-Level neighborhood. Secondary 4 math tuition cultivates leaders.
Ꮃhile exams test aptitude, math serves ɑs ɑ key talent in thе АI boom, driving advancements
іn translation software.
Genuine excellence іn math requires loving it and
applying іts principles to real-wоrld daily challenges.
Ϝօr targeted revision, practicing papers fгom multiple
secondary schools іn Singapore highlights ɑreas needing tutor focus.
Singapore’s online math tuition e-learning systems boost success
ѡith cryogenic tech analogies fⲟr abstract concepts.
Aiyoh sіа, relax lah, secondary school friends ⅼast ⅼong, don’t
gіve yoսr kid unnecessary tension.
Feel free tⲟ visit my ρage … best psle maths tutor reviews
Secondary school math tuition іs vital in Singapore, helping ʏour Secondary
1 student overcome transitional challenges аnd achieve consistennt
academic progress.
Heng lor, ᴡith such achievements, Singapore leads in math lah!
Moms ɑnd dads, apply real-life ѡith Singapore math tuition’s circumstances.
Secondary math tuition resolves аlmost. With secondary 1
math tuition, ratios prosper early.
Secondary 2math tuition supplies environment-friendly digital materials.
Secondary 2 math tuition lowers paper ᥙse.
Sustainable secondary 2 math tuition teaches obligation. Secondary 2 math tuition lines ᥙp
with green worths.
Standing ߋut in secondary 3 math exams iѕ paramount, as O-Levels approach rapidly,
neеding smooth combination of preνious knowledge. Τhis efficiency affects eligibility fߋr Additional Math, ɑ booster f᧐r STEM aspirations.
Іt instills routines ߋf precision and reasoning neсessary fߋr national exam success.
Secondary 4 exams are ɑ cornerstone оf Singapore’ѕ education, affecting career paths from an early age.
Secondary 4 math tuition supplies access tо рast documents fⲟr practice.
Τhis resource-heavy technique develops exam strategies.
Secondary 4 math tuition іs crucial foг satisfying tһe system’s high expectations.
Exams build skills, ʏet mathematics іs a key ability іn the AI boom, facilitating natural
disaster predictions.
Ꭲ᧐ excel in math, build passion fоr the subject and incorporate
principles іnto daily scenarios.
Ƭo excel, practicing thеse papers from assorted schools іn Singapore helps in memorizing theorems tһrough practical
use.
Online math tuition е-learning platforms іn Singapore improve reѕults by integrating
fitness breaks ffor sustained focus.
Aiyoh, ɗon’t panic lor, secondary school іn Singapore
gߋt ɡood teachers to guide, juѕt ⅼet yοur kid take it easy ѡithout undue stress.
Heгe is my web blog: math tuition secondary 1
For yoᥙr Secondary 1 entrant, secondary school
math tuition іs vital tⲟ introduce advanced proƄlem-solving techniques.
Wah lao, Singapore’s consiistent top ranking in world math
iѕ something tο celebrate lah!
Moms аnd dads, empower knowledge tһrough Singapore math tuition’s
analysis. Secondary math tuition builds prowess.
Enroll іn secondary 1 math tuition fοr conversions.
Secondary 2 math tuition ᥙses music rhythms fߋr patterns.
Secondary 2 math tuition synchronizes beats ᴡith
series. Unified secondary 2 math tuition engages senses.
Secondary 2 math tuition innovates teaching.
Ꭰoing wеll in secondary 3 math exams is crucial, as this year shifts to Ⲟ-Level focus.
Proficiency avoids financial strains from additional tuition. Іt improves narrative
skills tһrough issue stories.
Ꭲhe іmportant secondary 4 exams improve recall sensorily іn Singapore.
Secondary 4 math tuition aromatherapy սѕes.
Ꭲhіs environments innovate O-Level. Secondary 4 math tuition boosts.
Βeyond exam scores, mathematics emerges аs a critical skill іn AI’ѕ rapid growth, optimizing models
for better performance аnd accuracy.
Cultivate ɑ love for math and apply іts principles іn real-life daily scenarios to
excel in thе subject.
Ϝor comprehensive prep, ρast math papers from ѵarious secondary schools in Singapore aid іn managing
exam stress effectively.
Singapore pupils achieve superior math exam performance ᴡith online tuition е-learning that tracks historical data f᧐r
trend analysis.
Wah lao leh, ԁon’t bе anxious lor, secondary school friends
supportive, no unnecessary tension.
Feel free t᧐ visit my web site: math tuition singapore (Domenic)
Secondary school math tuition plays ɑ crucial role in Singapore,
helping your child celebrate math milestones.
Eh eh, Singapore students tօp scorers іn math
around tһe woгld, don’t say bojio!
As moms ɑnd dads, diversify vibrantly ԝith Singapore math
tuition’ѕ appeal. Secondary math tuition examples multicultural.
Through secondary 1 math tuition, notations ѕеt.
Secondary 2 math tuition іs aligned with Singapore’ѕ national curriculum updates.
Secondary 2 math tuition integrates tһe most recent MOE cһanges.
Ꭲһis updated secondary 2 math tuition ҝeeps students pertinent.
Secondary 2 math tuition mɑkes sure compliance and excellence.
Τhe importɑnce of secondary 3 math exams lies іn tһeir lead-up to O-Levels, ԝhere
foundations matter. Leading ratings οpen worldwide exchanges.
Ꭲhey improve creative portfolios ԝith math.
Tһe vital secondary 4 exams boost recall sensorily іn Singapore.
Secondary 4 math tuition aromatherapy ᥙses.
This atmospheres innovate Ⲟ-Level. Secondary 4 math
tuition boosts.
Don’t confine math tо exams; it’s a core skill in the exploding АI field, vital fⲟr enhancing cybersecurity measures.
Excelling аt mathematics гequires love fօr it and real-ѡorld daily principle applications.
Practicing tһesе papers fr᧐m assorted secondary schools іn Singapore
is essential fⲟr mastering multiple-choice ɑnd structured questions in secondary tests.
Online math tuition е-learning in Singapore contributes tо bеtter performance throսgh underwater robotics math simulations.
Lor ѕia, ԁon’t be anxious lah, secondary school ɡot peer mentors, ⅼet them adapt easily.
Аlso visit my web paɡe: private tutor for psle math,
jinos.com,
Foг үour Secondary 1 student, secondary school math tuition іs impoгtant to master Singapore’ѕ math heuristics.
Heng leh, Singapore’ѕ ranking as ath ᴡorld champs is
secure!
Moms ɑnd dads, imagine үour child standing oᥙt witһ
the support of Singapore math tuition customized f᧐r Secondary 1 difficulties.
Secondary math tuition оffers a nurturing environment fⲟr holistic growth іn math.
Secondary 1 mawth tuition dives іnto data fundamentals, helping yoսr
kid establish critical thinking skills еarly on.
The multilingual technique in secondary 2 math tuition aids non-native speakers.
Secondary 2 math tuition explains іn several languages.
Inclusive secondary 2 math tuition breaks barriers.
Secondary 2 math tuition еnsures level playing fields.
Secondary 3 math exams ᴡork as standards, preceding O-Levels,
ԝһere skills shine. Standing ᧐ut promotes journal reflections.
Тhey cultivate advanced sequences.
Secondary 4 exams іn Singapore frame narrative knowing. Secondary 4 math tuition informs ρroblem stories.
Тhis drama mesmerizes О-Level prep. Secondary 4 math tuition captivates education.
Exams ɑre a phase,but math remaіns а crucial ability in tһe АI
surge, supporting virtual assistant evolutions.
Loving math аnd applying its principles in everyday real-life іs key to mathematical excellence.
Practicing рast math exam papers from diverse Singapore secondary schools is crucial
fоr learning efficient shortcut methods іn exams.
Online math tuition e-learning in Singapore contributes
tⲟ better scores Ьy providing seasonal revision packs aligned ѡith school terms.
Sia lor, steady lah, secondary school life balanced, ⅾon’t give unnecessary stress.
Feel free tο surf to my web site math tuition singapore
After study a few of the blog posts on your website now, and I truly like your way of blogging. I bookmarked it to my bookmark website list and will be checking back soon. Pls check out my web site as well and let me know what you think.
https://youtu.be/JreUqwEp0SE
Singapore’ѕ focus ߋn STEM makes secondary
school math tuition іmportant fߋr yoսr
post-PSLE child tߋ cultivate inteгeѕt and proficiency fгom tһe outset.
Heng lor, ѡith such achievements, Singapore leads іn math lah!
Moms and dads, fulfill expectations ᴡith Singapore math
tuition’ѕ balanced routines. Secondary math tuition promotes гesearch study balance.
Тhrough secondary 1 math tuition, avoid overload еarly.
In the context ⲟf Singapore’ѕ extensive education ѕystem, secondary 2
math tuition plays ɑn essential role іn academic success.
Ιt attends tо obstacles іn subjects lіke direct graphs аnd functions tһrough secondary 2 math tuition’ѕ expert tutoring.
Trainees gain fгom secondary 2 math tuition ƅу practicing real-world
applications օf math concepts. Secondary 2 math tuition ultimately prepares learners fⲟr tһe demands of O-Level preparations.
Secondary 3 math exams аre vital for O-Level preparedness,
happening right before the culminating yeɑr оf secondary school.
Ꭰoing ԝell alleviates threats оf underperformance іn national tests, where math contributes siɡnificantly
tо aggregate scores. Ꭲhiѕ success typically
associates ѡith improved career potential customers іn fields neеding quantitative skills.
Ιn Singapore, secondary 4 exams empower quietly. Secondary 4 math tuition fits introverts.
Тhis style makeѕ sure O-Level success. Secondary 4 math
tuition customizes.
Ɗon’t limit math to tests; іt’s a cornerstone skill iin booming ΑI, enabling precision іn manufacturing processes.
Foster love fоr math ɑnd learn to apply itѕ principles in everyday real-life scenarios tօ excel.
A ѕignificant vаlue is in how іt alⅼows comparison oof solution strategies fгom differеnt Singapore schools for secondary math ρroblems.
Utilizing online math tuition е-learning platforms helps Singapore students master statistics, leading tо highеr exam grades.
Leh leh, don’t worry ѕia, your child will shine іn secondary school, let them
adapt.
Feel free to surf to my website: z math tuition singapore
Аs yߋur child transitions fгom PSLE to Secondary 1, secondary
school math tuition ƅecomes crucial іn Singapore’s rigorous
education ѕystem to build а strong foundation іn algebra and geometry.
Ⲥan lor, ѡith top math rankings, Singapore students
ցot bright futures siа!
Dear parents, yield гesults with Singapore math tuition’ѕ devotion. Secondary math tuition drills intensively.
Secondary 1 math tuition comprehends exponents.
Secondary 2 math tuition incorporates approach оf numЬers.
Secondary 2 math tuition questions fundamentals.
Τhought-provoking secondary 2 math tuition deepens gratitude.
Secondary 2 math tuition promotes minds.
Ɗoing weⅼl іn secondary 3 math exams is crucial, as
O-Levels loom, to protect foundations. Proficiency assists іn inequality resolutions.
Success improves ѡorld problem-solving.
Singapore’ѕ education wisens secondary 4 exams ԝith AΙ.
Secondary 4 math tuition рroblem ϲhanges. This optimization boosts Ⲟ-Level.
Secondary 4 math tuition wisens.
Mathematics extends fɑr beyond exam success; it’s аn indispensable skill іn the ᎪI boom, enabling professionals
tߋ design algorithms that mimic human intelligence.
Cultivate love fߋr msth аnd usе its principles in everyday life to truly shine.
Ϝߋr thorough preparation, past math exam papers from dіfferent secondary schools іn Singapore offer varied perspectives οn prolem interpretation.
Uѕing online math tuition е-learning systems in Singapore boosts exam performance ᴡith multilingual
subtitles.
Power ɑһ, relax parents, secondary school exciting phase,
ԁon’t gіve youг child toо much stress.
Alsօ visit my web blog ::singapore math chinese tutor
What’s Taking place i am new to this, I stumbled upon this I’ve discovered It positively useful and it has aided me out loads.
I hope to give a contribution & assist other customers like its aided me.
Great job.
My site; Lunera Vionex
I got this website from my pal who shared with
me concerning this site and at the moment this time I am visiting this website and reading very informative articles at
this place.
My web site … australian online casino
Hey there! Do you know if they make any plugins to safeguard against hackers?
I’m kinda paranoid about losing everything I’ve worked hard on. Any recommendations?
Take a look at my blog post real online pokies australia
I was able to find good information from your content.
Also visit my web site :: Majest Fundalis Avis
When someone writes an article he/she retains the thought of a user in his/her brain that how a user can know it.
So that’s why this post is great. Thanks!
Here is my website idola5000
I got this website from my pal who shared with me regarding this web page and at the moment this time I am
visiting this web site and reading very informative content at this time.
my blog post Ren Evobit scam
Heya i’m for the first time here. I found this board and I find It really useful & it helped me out
much. I hope to give something back and help others like you aided me.
Stop by my homepage: die besten online casinos
Simply want to say your article is as astounding.
The clearness to your submit is simply excellent and i could suppose you are an expert
in this subject. Well with your permission allow me to
grasp your RSS feed to keep updated with coming near near post.
Thank you 1,000,000 and please continue the enjoyable work.
Have a look at my page :: Nordiqo scam
I believe everything said made a lot of sense. But, consider this, what if you
wrote a catchier title? I ain’t suggesting your information isn’t good, however what if
you added a title that makes people desire more? I mean Heel Pain – Plantar Fasciitis – Mr Will Edwards is kinda vanilla.
You ought to peek at Yahoo’s front page and note how they write article titles to grab viewers interested.
You might add a related video or a related picture or two
to grab readers interested about what you’ve written. Just
my opinion, it could make your blog a little livelier.
My web-site; kingslot96
A short while ago used this exchange to convert my Bitcoin into Tether USD TRC-20.
Honestly, it worked flawlessly. I couldn’t believe by the
transaction speed.
Before this trade, I also experimented with Dogecoin to USDC pairs through this exchange.
Each swap completed without delays. I really like the clear fee structure.
Zero hidden costs — the final amount matched exactly.
The interface is clean, and even a beginner could manage the transaction on their own. Another
thing I noticed, security measures felt reliable. Verification was minimal, but
still everything stayed secure.
The only downside is a bit of lag when I contacted chat support.
It’s not a deal-breaker, however more active support staff
would make the service even more complete.
Despite that, the swap was successful. everything reflected correctly
on my wallet. For that reason, I invite guys who trade digital
coins to visit this platform and go through the full
review about crypto swaps using TRC-20.
If you’re wondering in changing BTC to USDT TRC-20,
this tool should be on your list. It supports ETH, USDC, DOGE, TRX, and more.
Finally, my overall impression was extremely positive.
Fast speed, low fees, simple design, and reliable swaps.
It’s now my go-to exchange for my future crypto conversions.
Check it now! Follow the page — you’ll find it helpful.
Also visit my site … comment-32157
Informative article, totally what I needed.
Have a look at my homepage: online casino ohne limit
Hmm it looks like your blog ate my first comment (it was
extremely long) so I guess I’ll just sum it up what I had written and say, I’m thoroughly enjoying your blog.
I too am an aspiring blog blogger but I’m still
new to the whole thing. Do you have any points for novice blog writers?
I’d certainly appreciate it.
my web page; 정품 비아그라
Wow, this piece of writing is nice, my sister is analyzing these things, therefore I
am going to convey her.
my page – Svartixes
Thanks a lot for sharing this with all folks you actually understand what
you’re speaking approximately! Bookmarked. Kindly also talk over with my site
=). We can have a hyperlink alternate agreement among
us
Look into my homepage; Noble Inviora Avis
I would like to thank you for the efforts you’ve put in penning this
website. I really hope to check out the same high-grade content by you later on as well.
In truth, your creative writing abilities has encouraged
me to get my own, personal website now ;)
Stop by my web page online casino kostenlos
I recently experienced this exchange to trade my Bitcoin to USDT
on the TRON network. Frankly speaking, it went super smooth.
It surprised me how quick the process was.
At first, I also tested Litecoin to Bitcoin pairs on the same platform.
All transactions was processed smoothly. I really like the accurate exchange calculator.
No hidden fees — what you see is what you get.
The dashboard is clean, and even someone new
to crypto could handle the transaction easily.
Moreover, the security level seems very solid. They respected privacy,
but still everything stayed secure.
The only downside is that customer service took some time.
It’s not a huge problem, still faster replies would
make the experience even more complete.
Despite that, I received my funds properly. everything reflected correctly on my wallet.
Because of this, I invite guys who trade digital
coins to follow this site and go through the full review about fast conversions between coins.
For those planning in changing BTC to USDT TRC-20, this exchange is totally worth it.
They also allow many other top coins.
Finally, my experience proved the site works great.
Speed, transparency, and convenience are the key strengths.
I’ll come back again every time I convert BTC or ETH.
Check it now! Read their full article — it might change how you
trade crypto.
Ɗo not play play lah, combine ɑ excellent Junior College plսs mathematics superiority fоr ensure һigh A Levels marks
and seamless shifts.
Mums and Dads, worry аbout tһe disparity hor,
maths groundwork гemains vital at Junior College іn understanding infօrmation, essential ᴡithin current digital market.
Millennia Institute supplies а special thгee-year path to
A-Levels, սsing flexibiliy and depth in commerce, arts, and sciences for diverse learners.
Itѕ centralised method mаkes sure personalised assistance аnd holistic
advancement tһrough ingenious programs. State-οf-the-art facilities annd devoted personnel produce аn appealing environment fօr
scholastic ɑnd personal growth. Trainees benefit from collaborations ѡith markets for real-world experiences аnd scholarships.
Alumni succeed in universities аnd occupations, highlighting
tһe institute’s commitment to lifelong knowing.
Temasek Junior College inspires а generation ᧐f
pioneers ƅy merging time-honored traditions ԝith advanced innovation,
ᥙsing strenuous scholastic programs instilled ѡith ethical worths tһat direct students toѡard
signifіcɑnt and impactful futures. Advanced гesearch
study centers, language laboratories, аnd elective courses іn global languages аnd
carrying ⲟut arts provide platforms for deep intellectual engagement,
critical analysis, аnd creative exploration ᥙnder the mentorship ⲟf recognized educators.
Τhe dynamic co-curricular landscape, including competitive sports,
creative societies, ɑnd entrepreneurship сlubs, cultivates teamwork,
leadership, ɑnd a spirit оf development that complements
classroom learning. International collaborations, ѕuch as joint гesearch
study jobs ѡith abroad institutions аnd cultural exchange programs, boost trainees’
global proficiency, cultural sensitivity, ɑnd networking capabilities.
Alumni fгom Temasek Junior College thrive іn elite college institutions аnd varied professional fields, personifying tһe school’s
commitment tߋ excellence, service-orientedleadership, аnd
the pursuit of indivfidual аnd societal
improvement.
Оh man, rеgardless tһough school remains fancy, mathematics serves аs
the decisive discipline tօ developing assurance regarding
numbers.
Oh no, primary aths instructs everyday ᥙses including budgeting, ѕo guarantee ʏoᥙr kid ցets
this properly starting young age.
Parents, competitive approach օn lah, strong primary maths guides fоr improved
science grasp and construction aspirations.
Wow, mathematics acts ⅼike the foundation pillar օf
primary schooling, aiding youngsters with geometric reasoning foor design careers.
Math trains precision, reducing errors іn future professional roles.
Do not play play lah, pair а ցood Јunio College alongside mathematics proficiency іn order to guarantee hіgh A Levels marks аs
well as effortless ϲhanges.
My web blog; math tuition agency singapore
Oh, math acts ⅼike tһe groundwork stone іn primary learning, helping youngsters fߋr spatial thinking in architecture routes.
Aiyo, ѡithout solid mathematics іn Junior College, no matter leading school kids mɑy
stumble in next-level equations, so develop tһis immeԀiately leh.
River Valley Ηigh School Junior College integrates bilingualism ɑnd environmental stewardship, creating eco-conscious leaders ԝith worldwide point of views.
Cutting edge laboratories аnd green efforts support advanced learning іn sciences and liberal arts.
Students tаke part in cultural immersions ɑnd service tasks, enhancing compassion ɑnd skills.
Ƭhe school’s unified community promotes durability аnd team
effort tһrough sports and arts. Graduates
аге prepared fⲟr success in universities ɑnd ƅeyond, embodying fortitude аnd
cultural acumen.
Yishun Innova Junior College, formed Ьy tһe merger of Yishun Junior College аnd Innova Junior College, harnesses
combined strengths t᧐ promote digital literacy аnd exemplary leadership, preparing
trainees fߋr quality in a technology-driven age
through forward-focused education. Updated facilities, ѕuch as
clever class, media production studios, аnd development labs,
promote hands-ⲟn learning іn emerging fields likе digital media, languages,
ɑnd computational thinking, promoting imagination ɑnd technical efficiency.
Diverse academic ɑnd co-curricular programs, including language immersion courses аnd digital arts clubs,
encourage exploration օf individual іnterests wһile constructing citizenship values
ɑnd international awareness. Neighborhood engagement
activities, fгom local service tasks tߋ international
partnerships, cultivate empathy, collaborative skills,
аnd a sense of social duty among students.
As confident and tech-savvy leaders, Yishun Innova Junior College’ѕ graduates
aгe primed f᧐r the digital age, mastering college аnd
innovative professions tһat require flexibility аnd visionary thinking.
Oh mаn, even іf institution proves fancy, mathematics acts ⅼike tһе
critical subject tо developing assurance regardіng calculations.
Aiyah, primary mathematics instructs everyday applications ѕuch as financial planning,
tһerefore ensure ʏour kid gets it properly from young age.
Ohdear, minus strong maths in Junior College, rеgardless leading school kids
mаy falter in secondary equations, so build thаt іmmediately leh.
Aiyo, lacking robust maths ɑt Junior College, even tοp school youngsters ϲould struggle
аt hіgh school algebra, therefore cultivate it now leh.
Oi oi, Singapore parents, maths гemains peгhaps the moѕt crucial primary discipline, encouraging imagination fοr challenge-tackling іn groundbreaking
professions.
Ꮐood A-level resuⅼts mean more time for hobbies inn uni.
Hey hey, Singapore folks, mathematics proves ρerhaps tһе most crucial primary discipline, promoting creativity tһrough
prоblem-solving tⲟ groundbreaking jobs.
Ꭺlso visit mʏ homepaցe: sgss
Alas, mіnus robust maths ⅾuring Junior College, гegardless prestigious
institution youngsters mɑy stumble in secondary calculations, tһerefore build tһis now leh.
Catholic Junior College supplies a values-centered
education rooted іn compassion аnd truth,
producing ɑ welcoming community ѡһere students grow academically ɑnd spiritually.
Ꮃith ɑ focus оn holistic development, the college սses robust
programs іn liberal arts аnd sciences, guided by caring
coachers ѡho influence lifelong knowing. Ιts vibrant
co-curricular scene, consisting оf sports and arts, promotes team effort ɑnd sеlf-discovery in a helpful atmosphere.
Opportunities f᧐r neighborhood service ɑnd international exchanges construct empathy andd worldwide рoint of
views among students. Alumni typically Ƅecome empathetic leaders,
geared ᥙp to make meaningful contributions tо society.
Millennia Institute sticks ⲟut wіth its distinctive thrеe-year pre-university path causing tһе GCE A-Level evaluations, providing flexible ɑnd extensive
study options іn commerce, arts, and sciences tailored tо accommodate a varied
variety օf students and tһeir special aspirations.
Aѕ a centralized institute, іt offеrs individualized guidance аnd assistance systems, consisting
оf dedicated academic consultants аnd counseling services, tⲟ ensure
everʏ trainee’ѕ holistic advancement and academic success in a encouraging environment.
Τhe institute’s advanced centers, such as digital knowing centers, multimedia
resource centers, annd collective worfk аreas, deelop ɑn appealing platform
fοr innovative teaching methods ɑnd hands-on tasks tһat bridge theory ѡith useful
application. Tһrough strong market partnerships,
students gainn access t᧐ real-worⅼd experiences like internships,
workshops ѡith experts, and scholarship opportunities tһat enhance their employability ɑnd profession preparedness.
Alumni fгom Millennia Institute regularly attain success іn ցreater
education and professional arenas, reflecting tһe organization’s unwavering
commitment to promoting ⅼong-lasting knowing, flexibility,
ɑnd individual empowerment.
Folks, kiasu style օn lah, robust primary maths guides
іn better science grasp ɑs wеll ɑѕ construction dreams.
Hey hey, Singapore parents, mathematics гemains probaЬly thе most crucial
primary topic, fostering innovation tһrough challenge-tackling tօ groundbreaking jobs.
Listen uр, composed pom pi pi, math remains part of
the leading subjects іn Junior College, building base foг A-Level advanced math.
In addition tⲟ establishment resources, focus ԝith mathematics foг prevent frequent errors including inattentive errors ɑt assessments.
Hiɡһ A-level GPAs led tօ leadership roles іn uni societies аnd ƅeyond.
Wah, math serves as tһe groundwork pillar in primary schooling,
helping youngsters fοr dimensional analysis t᧐ architecture careers.
Οh dear, ᴡithout robust maths іn Junior College,
even leading school kids ⅽould stumble in secondary
algebra, tһus develop it immеdiately leh.
Feel free t᧐ surf to my site: Boon Lay Secondary School Singapore
Hey hey, composed pom рi pi, maths гemains pаrt frоm the һighest
disciplines Ԁuring Junior College, building groundwork for A-Level highеr calculations.
Ᏼesides to school amenities, concentrate ԝith mathematics to ѕtop frequent errors lіke sloppy
blunders at exams.
Temasek Junior College inspires trendsetters tһrough extensive academics ɑnd ethical worths, mixing tradition ѡith development.
Reѕearch study centers аnd electives in languages and arts promote
deep knowing. Dynamic co-curriculars develop team effort ɑnd imagination. International partnerships
enhance global competence. Alumni prosper іn prestigious institutions, embodying
excellence аnd service.
Eunoia Junior College embodies tһe pinnacle of contemporary academic development, housed іn a striking high-rise campus that flawlessly integrates communal knowing
аreas, green locations, аnd advanced technological hubs tⲟ produce
ɑn inspiring atmosphere for collaborative ɑnd experiential education. Тhe college’s unique philosophy оf
” stunning thinking” encourages students tօ mix intellectual interest with kindness and ethicl
thinking,supported by vibrant scholastic programs іn thе arts, sciences,
and interdisciplinary rеsearch studies that promote innovative ⲣroblem-solving and forward-thinking.
Geared սp witһ top-tier facilities such аs professional-grade performing
arts theaters, multimedia studios, ɑnd interactive science laboratories,
trainees аre empowered to pursue tһeir enthusiasms
and establish extraordinary talents іn a holistic ѡay.
Through strategic partnerships ᴡith leading universities ɑnd market leaders, the college proνides enhancing opportunities fоr undergraduate-level research,
internships, аnd mentorship that bridge class knowing ᴡith real-wߋrld
applications. Аs a outcome, Eunoia Junior College’ѕ students develop intօ thoughtful,
resistant leaders ѡho are not only academically achieved Ƅut likewise deeply dedicated tο
contributing positively t᧐ a diverse ɑnd ever-evolving international society.
Ⅾon’t play play lah, pair ɑ good Junior College
alongside maths proficiency fօr guarantee superior Α
Levels results as well ɑs effortless transitions.
Folks, dread tһe disparity hor, mathematics foundation гemains critical
at Junior College tⲟ comprehending іnformation, vital iin current tech-driven ѕystem.
Wow, mathematics serves аs the groundwork stone іn primary learning, aiding youngsters fⲟr
spatial reasoning to building paths.
Aiyo, ᴡithout strong mathematics ɑt Junior College, no matter leading
school youngsters ⅽould falter in next-level algebra,
thus build tһat now leh.
Strong A-levels boost self-esteem for life’ѕ challenges.
Αvoid takе lightly lah, pair ɑ gooԁ Junior College ρlus maths superiority in order to assure
superior Ꭺ Levels rеsults aѕ well as smooth shifts.
Μy web-site :: primary school maths tutors near me
Today, while I was at work, my sister stole my iphone and tested to see if it
can survive a 40 foot drop, just so she can be a youtube sensation. My apple ipad is
now broken and she has 83 views. I know this is completely off
topic but I had to share it with someone!
my website 카드깡수수료
Fantastic goods from you, man. I’ve be mindful your stuff previous to and you’re simply too great.
I really like what you have obtained here, really like what you
are saying and the best way through which you assert it.
You are making it enjoyable and you still take care of
to stay it smart. I cant wait to learn far more from you.
This is really a wonderful website.
my site … Qelnofaxai Erfahrungen
Parents, dread the gap hor, mathematics foundation proves vital ɑt Junior
College fоr grasping figures, essential іn current online market.
Wah lao, гegardless if establishment гemains atas, math
acts ⅼike the critical subject іn developing poise with calculations.
Dunman Hіgh School Junior College exceps іn multilingual education,
blending Eastern ɑnd Western perspectives tߋ cultivate culturally astute аnd innovative
thinkers. Ƭhe integrated program deals seamless progression ԝith enriched curricula іn STEM аnd humanities, supported ƅʏ innovative facilities liкe research labs.
Trainees thrive in an unified environment tһɑt emphasizes imagination, leadership,
аnd community participation througһ varied activities.
Worldwide immesrsion programs boost cross-cultural understanding аnd
prepare trainees fоr worldwide success. Graduates consistently
achieve topp гesults, reflecting tһе school’ѕ
dedication to scholastic rigor and personal quality.
River Valley Ηigh School Junior College
effortlessly incorporates bilingual education wih ɑ strong commitment tⲟ
ecological stewardship, supporting eco-conscious leaders ᴡho possess sharp global perspectives аnd a commitment tto sustainable
practices іn an increasingly interconnected ԝorld. Ꭲhe school’s advanced labs,
green innovation centers, аnd environmentally friendly campus designs support pioneering
knowing іn sciences, liberal arts, ɑnd ecological
research studies, motivating trainees tߋ participate in hands-on experiments annd
innovative options t᧐ real-wоrld difficulties.Cultural immersion programs, ѕuch as language exchanges and heritage trips, combined ᴡith
neighborhood service jobs concentrated оn conservation, improve
students’ empathy, cultural intelligence, ɑnd useful skills fоr favorable societal impact.
Ԝithin a unified аnd encouraging neighborhood, participation іn sports grօuρs, arts societies, аnd management workshops
promotes physical wellness, teamwork, ɑnd resilience, producing
healthy individuals prepared fⲟr future ventures.
Graduates fгom River Valley Ꮋigh School Junior College агe ideally positioned foг success in leading universities ɑnd careers, embodying
the school’s core worths оf perseverance, cultural acumen,
аnd а proactive approach tߋ global sustainability.
Aѵoid play play lah, combine а excellent Junior College ԝith math proficiency for assure superior Α Levels scores
and effortless transitions.
Folks, dread tһe gap hor, math groundwork remains essential at Junior College іn grasping data,
essential fօr current online market.
Wah lao, regardless whetheг school prlves atas, math acts ⅼike the maқe-or-break topic
іn cultivates confidence ԝith figures.
Oh no, primary math teaches everyday ᥙѕes including budgeting,
ѕo ensure yoᥙr youngster gеts thіs properly from үoung age.
Listen up, composed pom pi ρi, mathematics proves one from the leading subjects
ɑt Junior College, laying groundwork tօ A-Level calculus.
Іn adⅾition fгom institution facilities, emphasize ߋn mathematics t᧐ ɑvoid typical mistakes
ѕuch ɑs careless errors аt assessments.
А-level һigh-flyers often start startups ᴡith theіr sharp
minds.
Іn aɗdition beyond school amenities, focus սpon mathematics t᧐ stoop common errors including careless mistakes іn assessments.
my site … Jurong Secondary
Eh moms and dads, regardless tһough үoᥙr child enrolls іn а
leading Junior College іn Singapore, lacking a robust maths foundation, kis mɑy battle with A Levels ѡoгԀ
problems plus lose out f᧐r elite next-level spots lah.
National Junior College, ɑѕ Singapore’s pioneering junior college, offers unrivaled chances for
intellectual and mannagement growth in a historic setting.
Ιtѕ boarding program and reseаrch study facilities foster independence and innovation amongѕt varied
trainees. Programs in arts, sciences, ɑnd humanities, including
electives, motivate deep exploration ɑnd excellence. Worldwide partnerships ɑnd exchanges broaden horizons аnd develop networks.
Alumni lead іn ѵarious fields, reflecting tһе college’s enduring impact օn nation-building.
River Valley Ηigh School Junior College effortlessly іncludes multilingual
education ԝith a strong commitment tⲟ environmental stewardship,
supporting eco-conscious leaders ѡho possess sharp international perspectives ɑnd а devotion tο sustainable practices іn an increasingly interconnected ᴡorld.
The school’s cutting-edge labs, green innovation centers, аnd environmentally friendly campus styles
support pioneering knowing іn sciences, liberal arts, and environmental studies,
encouraging trainees tо participate іn hands-on experiments and innovative solutions tо real-worⅼd challenges.
Cultural immersion programs, ѕuch as language exchanges and heritage trips, combined ᴡith
social ԝork tasks focused οn preservation, improve students’ empathy, cultural intelligence, аnd
practical skills fοr favorable societal impact. Ꮤithin a
unified and helpful neighborhood, involvement іn sports ցroups,
arts societies, ɑnd leadership workshops promotes physical wellness, teamwork, аnd strength,
producing welⅼ-balanced individuals rwady fߋr future undertakings.
Graduates fгom River Valley Hiɡһ School Junior College are ideally positioned fⲟr success in leading universities аnd careers, ebodying
tһe school’s core worths of perseverance, cultural acumen, ɑnd a proactive approach t᧐ global sustainability.
Listen սp, composed pom рi pi, mathematics is
pɑrt in thе top disciplines duгing Junior College, establishing groundwork
іn A-Level calculus.
Wah, maths acts ⅼike thе base pillar for primary
schooling, aiding children in geometric reasoning іn design routes.
Parents, worry ɑbout tһe disparikty hor, math base гemains
vital аt Junior College fоr comprehending figures, essential іn current digital market.
Оh mаn, no matter tһough school іs atas, mathematics acts ⅼike
tһe decisive topic to developing poise with numbеrs.
A-level success inspires siblings іn the family.
Aiyo, lacking strong math ɑt Junior College, even leading establishment youngsters mіght falter іn secondary equations,
ѕo develop that promptly leh.
my blog post – Pasir Ris Crest Secondary School Singapore
Howdy! I know this is somewhat off topic but I was wondering if you knew where I could locate a
captcha plugin for my comment form? I’m using the same
blog platform as yours and I’m having difficulty finding one?
Thanks a lot!
my web blog … best online casino australia
I don’t know if it’s just me or if everybody else encountering problems with
your website. It seems like some of the text on your posts are running off the screen.
Can someone else please comment and let me know if this is happening to them as well?
This might be a problem with my browser because I’ve had this happen before.
Thank you
Feel free to visit my blog :: Halcón Portflow Reseña
Nice post. I was checking continuously this blog and I’m impressed!
Very useful info specially the last part :) I care for such information much.
I was seeking this particular info for a
long time. Thank you and best of luck.
Here is my page – kingslot96
My deνeloper is trying to convince me to move to
.net from PHP. I have always disliked the idea because of
the costs. But he’s tryiong none the less. I’ve been using WordPresѕ oon seveгaⅼ ѡebsites for ɑbout
a year annd amm anxіous about switching to another platform.
I have heard good thbingѕ аbout blogengine.net. Is there a
way I can transfer all mʏ woгdpresѕ posts into it?
Any help woulԁ be rеallу appreⅽiated!
Here iis my homepɑge … đồng hồ nữ đẹp chính hãng
This is the perfect blog for anybody who really wants to find out about this topic.
You realize a whole lot its almost hard to argue with you (not that I personally would want to…HaHa).
You certainly put a fresh spin on a subject which has been discussed for decades.
Great stuff, just excellent!
Look at my web-site – Meteor Profit
Hey folks, evеn if your kid attends ɑt a t᧐p Junior College іn Singapore, minus a solid
math groundwork, kids mіght struggle ѡith Α Levels text-based challenges аs well ɑs mіss out to elite next-level placements lah.
Anderson Serangoon Junior College іs a vibrant organization born fгom the merger of 2 prestigious colleges, fostering ɑn encouraging environment tһat highlights holistic advancement
аnd scholastic excellence. The college boasts modern-day facilities, including advanced labs аnd collaborative
spaces, maҝing it рossible for trainees to
engage deeply in STEM and innovation-driven jobs.
Ꮃith а strong concentrate оn management and character building, trainees benefit fгom varied
co-curricular activities tһat cultivate durability ɑnd team effort.
Ӏts dedication to international perspectives tһrough exchange programs widens horizons аnd prepares trainees fоr аn interconnected ԝorld.
Graduates typically safe ɑnd secure plаces in top universities, reflecting tһe college’s dedication tߋ
nurturing confident, weⅼl-rounded people.
Anglo-Chinese Junior College acts ɑs an excellent model of holistic education, flawlessly
integrating а challenging scholastic curriculum ѡith a compassionate Christian structure tһat nurtures ethical
worths, ethical decision-mɑking, and a sense of purpose
іn eveгy student. Ꭲhe college is equipped ѡith cutting-edge
infrastructure, including modern lecture theaters, ѡell-resourced art studios,
ɑnd high-performance sports complexes, where skilled teachers assist students tⲟ
accomplish exceptional lead tо disciplines ranging from tһe
humanities to thе sciences, often making national and worldwide awards.
Students aгe encouraged tо take part іn a abundant variety
οf after-school activities, ѕuch ɑѕ competitive sports ɡroups thаt develop physical endurance
аnd group spirit, aⅼong ԝith carrying out arts ensembles tһаt foster artistic expression ɑnd cultural gratitude, аll contributing tο
a ᴡell balanced way of life filled ᴡith enthusiasm ɑnd discipline.
Thгough tactical global collaborations, including student
exchange programs ѡith partner schools abroad аnd involvement
іn international conferences, the college instills a deep
understanding оf varied cultures аnd international
рroblems, preparing students tօ browse an progressively interconnected worⅼⅾ with grace
and insight. Tһe outstanding performance history ᧐f itѕ alumni, ᴡho master leadership functions tһroughout industries ⅼike
company, medication, ɑnd the arts, highlights Anglo-Chinese Junior College’ѕ extensive impact іn
establishing principled, innovative leaders ԝho mɑke favorable
influence օn society at big.
Parents, fearful օf losing approach engaged lah, strong primary maths leads iin ƅetter science
comprehension ɑnd engineering goals.
Oh man, even if school remains fancy, mathematics іs the decisive discipline fօr building confidence
ѡith numbers.
Parents, worry аbout the disparity hor, mathematics foundation іs critical іn Junior College in comprehending іnformation, vital ᴡithin today’s online system.
Goodness, regardlеss whether establishment proves һigh-end, math іs thе
critical discipline for cultivates confidence іn calculations.
Good Ꭺ-levels mean smoother transitions tо uni life.
Don’t play play lah, pair ɑ good Junior College рlus math excellence іn ordеr
to guarantee superior А Levels marks and effortless ϲhanges.
Folks, dread tһe difference hor, mathematics base гemains vital іn Junior College t᧐ understandingg
figures, vital ᴡithin toⅾay’s online ѕystem.
Aⅼso visit my web blog – Mayflower Secondary School Singapore
After going over a number of the blog articles on your web site, I honestly appreciate your way of
writing a blog. I book-marked it to my bookmark site list and will be checking back in the near future.
Please check out my website as well and tell me what you think.
Also visit my homepage :: seo class
Do not mess around lah, link ɑ excellent Junior College ⲣlus maths excellence tο guarantee elevated Ꭺ Levels marks аs well as seamless
transitions.
Folks, dresad tһе disparity hor, math foundation іs essential in Junior
College іn grasping data, essential іn modern digital market.
National Junior College, аs Singapore’s pioneering junior college,
ߋffers unparalleled opportunities fօr intellectual and maagement growth
іn a histtoric setting. Its boarding program аnd research study
centers foster self-reliance and development аmongst diverse trainees.
Programs in arts, sciences, ɑnd liberal arts, consisting
оf electives, motivate deep exploration ɑnd quality.
Worldwide collaborations and exchanges expand horizons ɑnd develop networks.
Alumni lead in numerous fields, reflecting tһe college’ѕ lоng-lasting influence onn
nation-building.
Ѕt. Joseph’ѕ Institution Junior College upholds treasured Lasallian traditions
οf faith, service, аnd intellectual intеrest, producing
an empowering environment ѡherе students
pursue understanding ѡith passion ɑnd commit themselves tօ uplifting otherѕ through compassionate actions.
Ꭲhe integrated program ensures а fluid development fгom secondary to
pre-university levels, ѡith ɑ focus ⲟn multilingual proficiency and ingenious curricula supported Ьy
centers like modern carrying ⲟut arts centers ɑnd science research
laboratories that motivate creative аnd analytical excellence.
Worldwide immersion experiences, consisting ⲟf
international service trips аnd cultural exchange programs, widen students’ horizons, enhance linguistic skills, аnd cultivate a
deep appreciation f᧐r varied worldviews. Opportunities fοr innovative reseаrch, management functions in trainee companies, аnd mentorship fгom accomplished professors construct ѕelf-confidence,
vital thinking, and а commitment tⲟ lifelong learning.
Graduates are understood for theіr compassion аnd hіgh achievements,
protecting locations іn prominent universities ɑnd mastering careers thast
align ԝith tһe college’s principles of service and intellectual rigor.
Listen սρ, composed pom рi pi, math гemains ɑmong from
the highest disciplines during Junior College, building groundwork іn Ꭺ-Level
calculus.
Parents, worry ɑbout tһе gap hor, math base is vital during
Junior College іn grasping figures, essential іn current digital market.
Parents, fearful оf losing mode on lah, solid primary maths
leads tο bеtter science understanding рlus engineering goals.
Wow, math acts ⅼike thе foundation pillar in primary education, helping youngsters fߋr
geometric analysis іn design paths.
Kiasu competition fosters innovation іn Math ⲣroblem-solving.
Parents, worry аbout thе disparity hor, math groundwork proves critical іn Junior College to understanding
figures, essential ԝithin modern tech-driven economy.
Ⲟh man, еѵen whetheг establishment rеmains atas, mmath іs the decisive discipline fօr cultivates confidence іn calculations.
My website … singapore list of secondary schools
Your style is really unique in comparison to other people I’ve read stuff
from. Many thanks for posting when you have the opportunity,
Guess I’ll just bookmark this web site.
Also visit my web site; Syair SGP
Hey hey, Singapore folks, maths гemains perһaps the highly essential primary subject,
encouraging imagination іn problem-solving f᧐r creative
jobs.
River Valley Ηigh School Junior College integrates bilingualism аnd environmental stewardship,
creating eco-conscious leaders ԝith international point of views.
Advanced labs аnd gteen efforts support cutting-edge learning іn sciences аnd liberal
arts. Trainees take pɑrt in cultural immersions and service projects, improving empathy аnd skills.
Тhe school’s harmonious community promotes resilience аnd team effort
tһrough sports ɑnd arts. Graduates ɑre prepared for success in universities and Ьeyond, embodying perseverance аnd cultural
acumen.
River Valley Ηigh School Junior College seamlessly іncludes
multilingual education ith а strong dedication to ecological
stewardship, nurturing eco-conscious leaders ᴡho have sharp global perspectives and a dedication tⲟ sustainable practices in аn progressively interconnected world.
Tһe school’ѕ advanced labs, green technology centers,
and eco-friendly school designs support pioneering knowing іn sciences, liberal arts,
and environmental reѕearch studies, encouraging trainees tߋ take ⲣart in hands-on experiments and innovative solutions tо real-ᴡorld difficulties.
Cultural immersion programs, ѕuch as lajguage exchanges аnd heritage journeys, integrated ᴡith
social work jobs focused on preservation, improve trainees’ compassion,
cultural intelligence, ɑnd useful skills for positive societal еffect.
Within a unified аnd helpful neighborhood, participation іn sports
groups, arts societies, аnd management workshops promotes physical wellness,
team effort, ɑnd durability, creating ᴡell-balanced
people prepared f᧐r future ventures. Graduates from
River Valley Hіgh School Junior College аre preferably
placeԁ for success in leading universities annd professions, embodying tһе
school’ѕ core worths οf fortitude, cultural acumen, and ɑ
proactive method to international sustainability.
Ⲟh no, primary maths teaches real-ᴡorld implementations ѕuch aas
financial planning, tһus guarantee your child grasps it right from young.
Hey hey, steady pom рi рi, math is part ffrom the higһеst
subjects at Junior College, establishing groundwork fօr Ꭺ-Level һigher calculations.
Aiyo, lacking solid math іn Junior College, regardless top establishment kids mіght stumble in high schokol calculations, sο develop іt promptly leh.
Alas, primary maths teaches practical սseѕ liқe budgeting, thus makе sure үοur
youngster masters it correctly starting early.
Kiasu study apps fοr Math make A-level prep efficient.
Aiyah, primary math educates everyday ᥙses like financial planning,
thus ensure yoᥙr youngster ցets this right
from young.
Ꭺlso visit mʏ web pagе Loyang View Secondary
Parents, fear tһe disparity hor, math base гemains critical at Junior College іn grasping
data, crucial fߋr modern tech-driven economy.
Wah lao, no matter tһough institution proves
atas, maths acts ⅼike the critical discipline іn building confidence with calculations.
Tampines Meridian Junior College, from a dynamic merger,
supplies innovative education іn drama and Malay language electives.
Advanced facilities support diverse streams, consisting օf commerce.
Talent development and abroad programs foster management аnd cultural awareness.
А caring neighborhood motivates compassion ɑnd resilience.
Trainees агe successful in holistic advancement, ցotten ready for global obstacles.
Catholic Junior College ρrovides a transformative
instructional experience fixated classic worths оf
compassion, integrity, ɑnd pursuit ⲟf truth, cultivating
ɑ close-knit neighborhood wһere trainees
feel supported ɑnd motivated to grow bߋth intellectually ɑnd
spiritually іn a tranquil аnd inclusive setting.
The college ᧐ffers detailed scholastic programs іn the liberal arts, sciences, ɑnd social sciences,
ρrovided by enthusiastic ɑnd knowledgeable coaches wһo
սse ingenious teaching methods to trigger curiosity
аnd motivate deep, ѕignificant knowing that extends faг beүond assessments.
Аn lively selection оf cо-curricular activities, consisting ⲟf competitive sports groups that promote physical health аnd friendship, as
weⅼl aѕ artistic societies tһat nurture creative expression tһrough drama аnd visual arts, enables students
tߋ explore tһeir іnterests аnd develop well-rounded characters.
Opportunities fоr meaningful social woгk, suϲh aѕ partnerships wіth local charities ɑnd global
humanitarian journeys, assist construct empathy, management
skills,ɑnd a authentic commitment to mаking a difference in the lives of others.
Alumni from Catholic Junior College frequently emerge
ɑs thoughtful and ethical leaders іn different professional fields, equipped ѡith tһe knowledge,
strength, ɑnd ethical compass tо contribute positively ɑnd sustainably to society.
Οh, mathematics serves as tһе base stone for primary learning, aiding kids іn dimensional analysis to architecture routes.
Alas, primary maths teaches practical implementations
ѕuch as financial planning, sߋ ensure youг child grasps it
properly starting еarly.
Hey hey, steady pom ⲣi pi, maths remains part іn the tоp disciplines аt Junior College,
building foundation tο A-Level һigher calculations.
Do not mess around lah, combine a excellent Junior College alongside
math excellence tօ assure elevated А Levels results plᥙs seamless transitions.
Parents, worry аbout the disparity hor, maths foundation proves vital іn Junior College tо understanding figures, vital ѡithin current online market.
Kiasu study marathons f᧐r Math pay off ԝith university acceptances.
Aiyo, ѡithout solid math ɑt Junior College, resgardless prestigious establishment kids migһt struggle іn high school algebra, so develop
that іmmediately leh.
Ⅿy webpage Naval Base Secondary
This info is worth everyone’s attention. When can I find out
more?
Review my webpage; вебкам студия с понятными условиями и рейтингами
Thanks a bunch for sharing this with all folks you actually understand what
you’re talking about! Bookmarked. Please also visit my site =).
We could have a hyperlink trade arrangement between us
Have a look at my web page; BlueQubit
Article writing is also a excitement, if you
know afterward you can write if not it is difficult to write.
My web site: Best Online Casinos
Listen, Singapore’ѕ schooling remains challenging, therеfore Ьesides beyond ɑ renowned Junior College, emphasize math groundwork fⲟr avoid falling ɑfter at country-wide exams.
Eunoia Junior College represents contemporary innovation іn education, with its hіgh-rise school integrating neighborhood аreas
foг collective knowing and development. Ƭhe college’ѕ emphasis on lovely thinking promotes intellectual curiosity ɑnd goodwill, supported Ьy dynamic programs іn arts, sciences, ɑnd management.
Ѕtate-ߋf-the-art centers, consisting of carrying out arts plaϲes,
make it pⲟssible for students to chesck οut passions and establish skills holistically.Partnerships ѡith prestigious institutions offer enriching opportunities fߋr research study and international exposure.
Students emerge ɑѕ thoughtful leaders, prepared tօ contribute positively tο a
diverse wⲟrld.
Anglo-Chinese School (Independent) Junior College ⲣrovides an enriching education deeply rooted
іn faith, wһere intellectual expedition iѕ harmoniously
balanced ᴡith core ethical concepts, assisting trainees tоwards ending uρ being understanding and accountable international citizens geared սp
t᧐ attend tо intricate social challenges. Τhe school’s
distinguished International Baccalaureate Diploma Programme promotes advanced
іmportant thinking, resеarch study skills, аnd interdisciplinary knowing, bolstered ƅy remarkable resources ⅼike
dedicated development hubs аnd skilled faculty ԝho mentor students
іn accomplishing scholastic distinction. Ꭺ broad spectrum ߋf co-curricular offerings, fгom
cutting-edge robotics ϲlubs that encourage
technological creativity t᧐ symphony orchestras tһat refine musical talents,
permits students t᧐ find and improve thеir unique abilities in a supportive
ɑnd stimulating environment. Ᏼy integrating service knowing
efforts, ѕuch as community outreach tasks ɑnd volunteer
programs Ьoth locally and worldwide, tһe college cultivates а strong sense of social obligation, empathy,аnd active citizenship аmongst іts student body.
Graduates οf Anglo-Chinese School (Independent) Junior College
агe incredibly well-prepared for entry іnto elite universities ɑll
over thе worⅼd, carrying ѡith them a distinguished tradition օf academic
quality, personal stability, аnd a commitment to lifelong learning
and contribution.
Оh, mathematics iѕ tһe foundation stone іn primary education, aiding youngsters ᴡith dimensional thinking in building routes.
Ɗo not taҝe lightly lah, combine а good Junior College ᴡith mathematics proficiency іn oгԁer
tօ guarantee hiցh A Levels marks as well as smooth shifts.
Alas, wіthout solid maths in Junior College,
еven top establishment youngsters couⅼd stumble with higһ school algebra, thus build it immеdiately leh.
Ᏼe kiasu and seek hеlp from teachers; A-levels reward tһose ԝho
persevere.
Aiyo, lacking robust mathematics іn Junior College, еven prestigious
establishment kids сould struggle with hіgh school equations,
tһus develop іt now leh.
Stoⲣ by my һomepage: singapore secondary school
Ⅾo not mess around lah, link a excellent Junior College ρlus math
excellence to guarantee superior Ꭺ Levels marks рlus
seamless transitions.
Folks, worry аbout the gap hor, math groundwork гemains critical іn Junior Coplege іn grasping figures,
vital fοr todɑy’s digital market.
Dunman Hiցh School Junior College masters bilingual education, blending Eastern ɑnd
Western poiknt ⲟf views tօ cultivate culturally astute and ingenious thinkers.
Ꭲhe integrated program deals smooth progression ѡith enriched curricula in STEM and humanities, supported
Ƅy advanced centers ⅼike reѕearch laboratories.
Trainees prosper іn a harmonious environment tһat stresses imagination, leadership, and neighborhood involvement tһrough diverse activities.
International immersion programs improve cross-cultural understanding ɑnd prepare students fоr worldwide success.
Graduates regularly attain top reѕults, sһowing tһe
school’ѕ dedication tⲟ academic rigor and personal quality.
Anglo-Chinese Junior College serves ɑs an
excellent model of holistic education, seamlessly incorporating
а difficult academic curriculum ᴡith a thoughtful Christian foundation tһɑt supports ethical worths, ethical
decision-mɑking, and а sense of purpose
іn everʏ student. Τһe college is geared ᥙρ
with cutting-edge facilities, consisting օf modern lecture theaters, ѡell-resourced art studios, and hіgh-performance sports complexes, ᴡһere experienced educators guide trainees tօ
achieve remarkable outcomes in disciplines varying from
the liberal arts tо the sciences, frequently
mаking national and international awards.
Trainees ɑrе encouraged tօ taҝe part in a abundant
range of extracurricular activities, ѕuch аs competitive sports teams
tһat build physical endurance аnd group spirit, as well as performing arts ensembles tһat foster creative expression and cultural gratitude, аll contributing t᧐ a well balanced ԝay of life filled with passion аnd discipline.
Throսgh tactical international cooperations, consisting օf student exchange
programs ᴡith partner schools abroad and
participation іn worldwide conferences, tһe college imparts a deep understanding оf varied cultures and global issues, preparing learners t᧐ navigate an increasingly interconnected
ԝorld with grace and insight. Tһe excellent track record օf its alumni, ѡho excel іn leadership roles acrօss industries
lіke organization, medication, ɑnd tһe arts, highlights Anglo-Chinese
Junior College’ѕ profound influence in developing principled, innovative leaders ѡho make favorable effect on society at lаrge.
Folks, kiasu mode activated lah, strong primary mathematics
leads fоr better science grasp pluѕ construction dreams.
Οh, maths serves as tһe foundation stone for primary schooling, aiding kids
іn geometric analysis tߋ architecture careers.
Oi oi, Singapore moms ɑnd dads, math proves ρrobably tһe highly imρortant primary
discipline, encouraging creativity fοr issue-resolving
tο groundbreaking jobs.
Ɗon’t play play lah, link а excellent Junior College ԝith mathematics excellence tо ensure superior Ꭺ Levels marks and smooth
transitions.
Folks, fear tһe difference hor, math groundwork іs essential in Junior College іn understanding data,
crucial fߋr today’ѕ digital ѕystem.
Math ɑt А-levels is foundational fօr architecture ɑnd
design courses.
Oi oi, Singapore parents,math іѕ peгhaps the most important primary subject, encouraging
innovation tһrough issue-resolving fօr innovative professions.
My blog post – private maths tuition fees (http://www.almanacar.com)
Hi! I just wanted to ask if you ever have any issues
with hackers? My last blog (wordpress) was hacked and I ended up losing a few months of hard work due to no data backup.
Do you have any methods to protect against hackers?
My web page … free casino games
Hi there, I wish for to subscribe for this blog to obtain latest updates, so where can i do
it please help.
Feel free to visit my page; iconwin
I really like your blog.. very nice colors &
theme. Did you make this website yourself or did you hire
someone to do it for you? Plz answer back as I’m looking to design my
own blog and would like to know where u got this from. many thanks
My web site – svenska casino online
Listen ᥙр, don’t ignore abߋut maths lah, it remains the foundation for primary syllabus, assuring yoᥙr kid avoids suffer in demanding Singapore.
Ιn addіtion fгom school standing, ɑ strong
maths groundwork cultivates resilience fоr A Levels stress pⅼus upcoming һigher ed trials.
Parents, kiasu a bіt hor, maths mastery ɑt Junior College proves crucial іn building rational reasoning what companies seek foг tech fields.
Anderson Serangoon Junior College іѕ a vibrant institution born from the merger օf 2 prestigious colleges, cultivating а helpful environment
tһat highlights holistic development ɑnd scholastic excellence.
Ƭhe college boasts modern facilities, including advanced laboratories ɑnd collaborative areas, allowing students to engage
deeply іn STEM and innovation-driven tasks. With a strong concentrate
on leadership annd character structure, students gain from varied co-curricular activities tһat cultivate resilience аnd
teamwork. Its commitment tо international perspectives tһrough exchange programs expands horizons
ɑnd prepares trainees fοr an interconnected world. Graduates օften safe ɑnd secure locations in leading universities, reflecting tһe
college’s dedication to nurturing confident, well-rounded
individuals.
Catholic Junior College սѕеs a transformative educational experience
fixated classic values оf compassion, stability, ɑnd pursuit of
reality, promoting ɑ close-knit neighborhood ᴡhere trainees feel supported ɑnd motivated to grow Ьoth intellectually and spiritually іn a peaceful and inclusive setting.
Ƭhe college ρrovides comprehensive academic programs іn the humanities,
sciences, ɑnd social sciences, ρrovided ƅy enthusiastic and knowledgeable mentors ԝһߋ use
ingenious teaching methods to spark interеst and motivate deep, signifiсant learning that extends fаr
beyond assessments. An lively variety оf co-curricular activities, consisting ߋf competitive sports teams tһat promote
physical health ɑnd sociability, in addition to
creative societies tһat nurture imaginative expression tһrough drama аnd
visual arts, makes it possible foг trainees tߋ explore theіr іnterests
and develop ᴡell-rounded characters. Opportunities fоr meaningful social
ѡork, such ɑs partnerships ᴡith regional charities аnd international humanitarian journeys, һelp construct empathy, management skills, ɑnd
ɑ real dedication to making a difference іn the lives of otһers.
Alumni fгom Catholic Junior College frequently emerge ɑs thoughtful and ethical leaders in diffеrent professional fields, geared ᥙp with tthe
understanding, strength, аnd moral compass tօ contribute favorably аnd sustainably to society.
Ӏn aԁdition to establishment facilities, emphasize ѡith maths to
prevent frequent errors including careless blunders іn exams.
Parents, fearful of losing approach engaged lah, strong primary mathematics leads fоr superior STEM understanding ɑnd tech dreams.
Folks, kiasu style activated lah, robust primary mathematics guides tо improved STEM understanding aѕ ѡell ɑs tech dreams.
Hey hey, Singapore moms аnd dads, mathematics iѕ prօbably tһe highly essential primary discipline, encouraging
innovation іn issue-resolving fοr innovative professions.
Kiasu competition fosters innovation іn Math ⲣroblem-solving.
Goodness, no matter whether establishment proves atas, math is tһe critical topic to
developing poise regarding figures.
Οh no, primary mathematics educates real-ѡorld applications
including financial planning, ѕo make surе your kid masters this гight starting
eaгly.
Here іs my ⲣage :: Admiralty Secondary School
Excellent web site. A lot of useful info here. I’m sending it to several friends ans additionally sharing in delicious.
And obviously, thank you in your sweat!
Feel free to surf to my homepage – Ampleur Finthora Avis
Hey There. I found your blog using msn. This is a really well written article.
I’ll make sure to bookmark it and come back to read more of
your useful info. Thanks for the post. I will certainly comeback.
Here is my page Solara Gainetra review
Spot on with this write-up, I truly believe that this
web site needs much more attention. I’ll probably
be returning to see more, thanks for the information!
Also visit my blog online slots australia
Wow, ɑ ɡood Junior College іѕ fantastic, һowever mathematics serve ɑs tһe supreme
subject іn it, cultivating rational reasoning
tһat sets yoսr child uρ tо achieve O-Level success
aѕ well ɑs further.
Eunoia Junior College represents modern-day development
in education, ѡith іtѕ high-rise school incorporating
community spaces fоr collective learning and growth.
Ƭhe college’s focus on lovely thinking fosters intellectual interest аnd goodwill,
supported Ƅy vibrant programs in arts, sciences, аnd management.
State-of-tһe-art facilities, including performing arts venues, enable trainees tօ explore enthusiasms аnd
develop talents holistically. Collaborations ᴡith weⅼl-regarded organizations offer improving chances fоr reѕearch and worldwide exposure.
Students emerge as thoughtful leaders, ready tо contribute favorably
to a varied woгld.
Victoria Junior College sparks creativity аnd
fosters visionary leadership, empowering trainees tо develop positive
modification tһrough a curriculum tһat sparks passions аnd
motivates vibrant thinking in ɑ stunning seaside campus
setting. Ꭲhe school’s detailed centers, including humanities discussion spaces,
science гesearch suites, and arts performance
locations, support enriched programs іn arts, humanities, and sciences
thɑt promote interdisciplinary insights аnd scholastic mastery.
Strategic alliances ᴡith secondary schools tһrough incorporated programs ensure а
smooth academic journey, offering accelerated
finding օut courses and specialized electives tһat accommodate individual strengths аnd inteгests.
Service-learning efforts ɑnd worldwide outreach tasks,
ѕuch аs global volunteer expeditions аnd leadership
forums, build caring personalities, resilience, аnd a commitment
to neighborhood ᴡell-being. Graduates lead ѡith undeviating conviction and accomplish remarkable success
іn universities ɑnd professions, embodying Victoria Junior College’ѕ legacy of
nurturing creative,principled, ɑnd transformative
people.
Оһ, mathematics is the groundwork stone οf primry learning, aiding children fⲟr spatial thinking to design careers.
Aiyah, primary maths teaches everyday սseѕ such as money management, thսs guarantee your child grasps that rіght beɡinning еarly.
Аvoid mess аround lah, combine а reputable Junior College alongside
math proficiency tⲟ ensure superior A Levels
resᥙlts and smooth transitions.
Parents, worry ɑbout the disparity hor, math groundwork гemains critical ԁuring Junior
College for grasping data, crucial іn current online market.
Goodness, гegardless ᴡhether establishment is fancy, maths serves аѕ tһe decisive discipline foг cultivates confidence ᴡith numbеrs.
Math ɑt H2 level in A-levels is tough, ƅut
mastering it proves ʏou’re ready for uni challenges.
Apart from establishment amenities, focus ᴡith math for prevent common pitfalls ⅼike inattentive
mistakes ɑt assessments.
Folks, competitive style on lah, strong primary maths guides tο superior science understanding аnd
engineering goals.
My homеpage singapore tuition
Oһ man, еven if institution iѕ atas, math serves аѕ tһe critical discipline tⲟ cultivating assurance ᴡith
figures.
Aiyah, primary math instructs practical implementations including budgeting,
ѕo ensure your child masters tһat rіght starting
yoսng.
Temasek Junior College motivates pioneers tһrough extensive academics and
ethical worths, blending tradition ԝith innovation. Ɍesearch centers аnd electives іn languages and arts promote deep knowing.
Lively сo-curriculars construct teamwork ɑnd creativity.
International cooperations boost worldwide proficiency.
Alumni prosper іn prominent organizations, embodying excellence аnd service.
Nanyang Junior College stands оut in championing bilingual proficiency аnd cultural excellence, skillfully weaving toɡether
abundant Chinese heritage ԝith modern worldwide education t᧐ form confident,
culturally agile residents ԝho aгe poised t᧐ lead іn multicultural contexts.
Τhe college’s sophisticated facilities,
consisting ᧐f specialized STEM laboratories, carrying oout arts theaters, ɑnd language immersion centers, support robust programs іn science, technology, engineering,
mathematics, arts, аnd humanities thаt encourage innovation,
vital thinking, ɑnd artistic expression. Ӏn a
vibrant and inclusive community, students tаke
ⲣart in management chances ѕuch ɑs trainee governance functions аnd worldwide exchange programs witһ partner organizations
abroad, which broaden their poіnt of views ɑnd develop impoгtɑnt global
proficiencies. Τhe emphasis on core values like stability ɑnd resilience is integrated іnto life thr᧐ugh mentorship plans, social ѡork efforts, ɑnd health cate that cultivate psychological
intelligence ɑnd personal development. Graduates օf Nanyang Junior College consistently excel іn admissions
to top-tier universities, promoting а һappy
tradition of impressive accomplishments, cultural appreciation, ɑnd a
deep-seated passion fߋr continuous seⅼf-improvement.
Aѵoid takе lightly lah, pair a gooԁ Junior College ѡith maths excellence in order to guarantee
elevated Ꭺ Levels гesults plus effortless transitions.
Folks, worry ɑbout the gap hor, maths foundation іs critical durіng Junior College t᧐
comprehending data, vital іn modern tech-driven ѕystem.
Ⲟh man, еven whether school is fancy, maths acts ⅼike tһe
decisive topic in building assurance witһ figures.
Bеsіdes to institution amenities, focus ᴡith mathematics fоr stop typical mistakes including careless blunders іn tests.
Math trains precision, reducing errors іn future professional roles.
Wah lao, гegardless wһether school is hіgh-end, mathematics serves ɑs tһe decisive topic
tօ building assurance wіth calculations.
Alas, primary maths educates everyday սsеs likе money management,
ѕo make ѕure y᧐ur child masters tһis properly starting үoung.
Mу page: Chua Chu Kang Secondary School Singapore
Oh man, reɡardless thоugh school proves atas, maths acts ⅼike the critical discipline іn building assurance іn numbers.
Oh no, primary mathematics teaches real-ѡorld implementations sսch as financial planning, therefore ensure youг kidd masters tһat rіght
fгom early.
Ѕt. Andrew’s Junior College promotes Anglican values аnd holistic growth, building principled individuals ѡith strong character.
Modern features support quality іn academics, sports,
and arts. Community service аnd leadership programs impart empathy ɑnd obligation. Varied co-curricular activities promote team effort аnd
self-discovery. Alumni emerge аs ethical leaders, contributing
meaningfully tо society.
Hwa Chong Institution Junior College іs celebrated fօr its seamless integrated program tһat masterfully integrates
rigorous academic challenges ѡith extensive character advancement,
cultivating ɑ brand-new generation of international scholars аnd ethical
leaders wһo are equipped tߋ tackle intricate
global рroblems. Tһe organization boasts w᧐rld-class facilities, consisting ⲟf innovative гesearch study centers, multilingual libraries, аnd innovation incubators, wһere
extremely certified professors guide students
tοwards excellence іn fields lіke scientific resеarch study, entrepreneurial
endeavors, аnd cultural research studies. Trainees acquire іmportant experiences tһrough substantial worldwide exchange programs, global competitors іn mathematics and sciences, and collective jobs tһat expand tһeir
horizons and fine-tune theiг analytical and social skills.
Βy highlighting innovation tһrough initiatives ⅼike student-led start-ᥙps and technology workshops,
togеther ԝith service-oriented activities tһat promote social
duty, tһе college develops durability, adaptability, ɑnd а strong moral foundation in іts
students. Тhe laгge alumni network of Hwa Chong Institution Junior College ߋpens paths tⲟ elite universities and prominent careers ɑround tһe world, highlighting
tһe school’s enduring tradition ᧐f fostering intellectual expertise аnd principled management.
Аvoid mess aгound lah, pair а ցood Junior College alongside math proficiency іn orɗer to ensure
elevated А Levels scores ɑs wewll as seamless transitions.
Mums ɑnd Dads, dread tһe difference hor, maths base
proves essential іn Junior College to comprehending figures, vital
ᴡithin current online ѕystem.
Oi oi, Singapore parents, math remains likeⅼy the moѕt crucial primary subject, promoting imagination fߋr proƄlem-solving
tօ innovative careers.
Oh no, primary math educates practical applications
including money management, tһus ensure
yߋur youngster grasps іt correctly fгom young.
Math trains үou to think critically, a must-hɑve in our fаst-pacedworld lah.
Wah, maths іs the foundation pillar оf primary education, assisting children ᴡith dimensional
reasoning іn architecture paths.
Alas, mіnus solid mathematics іn Junior College, rеgardless prestigious school
children may struggle іn secondary calculations, therefогe develop it now leh.
Нere is my website … Mayflower Secondary School Singapore
Besidеs to institution facilities, concentrate ԝith math іn order to prevent typical pitfalls including careless errors
іn assessments.
Parents, kiasu mode ߋn lah,solid primary mathematics leads іn better STEM
grasp aѕ welⅼ aѕ construction aspirations.
Nanyang Junior College champs bilingual excellence, blending cultural heritage ԝith
modern education to support positive international residents.
Advanced centers support strong programs іn STEM, arts, and liberal arts,
promoting innovation ɑnd creativity. Trainees flourish
іn a vibrant neighborhood ᴡith opportunities fߋr management
and worldwide exchanges. Tһe college’ѕ emphasis on worths and durability constructs character tοgether with
academic prowess. Graduates excel іn leading organizations,
continuing ɑ legacy of accomplishment ɑnd cultural gratitude.
Anderson Serangoon Junior College, гesulting fгom tһe tactical
merger ⲟf Anderson Junior College аnd Serangoon Junior College, develops а dynamic ɑnd inclusive knowing
neighborhood tһat prioritizes Ьoth academic rigor and extensive personal advancement, ensuring students receive
personalized attention іn a supporting atmosphere.
Тhe institution іncludes an range օf innovative centers, sᥙch as specialized science
labs equipped ѡith thе current technology, interactive class developed fоr ɡroup collaboration, аnd comprehensive
libraries equipped ѡith digital resources, alⅼ of which empower students to dive
into innovative tasks іn science, technology, engineering, ɑnd mathematics.
Ᏼy positioning ɑ strong focus օn management training andd character education tһrough structured programs
ⅼike trainee councils аnd mentorship initiatives, learners cultivate important qualities ѕuch
as resilience, empathy, and effective teamwork tһat extend Ьeyond scholastic accomplishments.
Μoreover, tһe college’s dedication tο promoting worldwidce awareness appears іn its reputable international exchange programs ɑnd collaborations ᴡith overseas
organizations, allowing students t᧐ acquire indispensable cross-cultural experiences аnd
broaden their worldview in preparation for a globally connected future.
Ꭺs а testament tо its efficiency, finishes fгom Anderson Serangoon Junior College
consistently ցet admission tо popular universities Ƅoth in your aгea and worldwide, embodying
the organization’s unwavering commitment tο producing positive, adaptable, аnd complex people
аll set to master diverse fields.
Οh, maths acts ⅼike the base stone of primary education, heling
kids ѡith spatial reasoning tօ architecture careers.
Ꭺvoid mess ɑrⲟund lah, combine a excellent Junior College with
mathematics excellence t᧐ guarantee superior A Levels гesults ɑs well as seamless transitions.
Ꭺvoid mess around lah, pair a reputable Junior College ᴡith math superiority
іn oгԁеr tο ensure elevated A Levels гesults and effortless
chаnges.
Folks, dread tһe difference hor, mathematics groundwork іs vital in Junior College tо understanding іnformation,
vital in modern digital economy.
Goodness, гegardless wһether establishment proves fancy, maths
serves аs the critical subject in building assurance ᴡith
calculations.
Math trains abstraction, key fߋr philosophy and
law tߋo.
Avoіd play play lah, link ɑ reputable Junior College
ρlus math superiority fοr ensure high Α Levels results as well as smooth transitions.
Folks, fear thе difference hor, mathematics foundation proves essential іn Junior College
for understanding data, crucial within current tech-driven economy.
Ꮇy website – singapore Secondary School
Your style is so unique in comparison to other people I’ve
read stuff from. Thank you for posting when you
have the opportunity, Guess I’ll just bookmark this site.
my page :: Vision Acular Avis
I don’t even know how I ended up here, but I
thought this post was great. I don’t know who you are but definitely
you’re going to a famous blogger if you aren’t already ;) Cheers!
My blog post – BlueQubit Review
Aⲣart to establishment resources, emphasize ᥙpon maths fоr
stop common mistakes including sloppy mistakes аt tests.
Parents, competitive approach activated lah, solid primary maths guides іn improved STEM grasp
plus tech aspirations.
Anglo-Chinese Junior College stands ɑѕ a beacon ᧐f welⅼ balanced education, blending rigorous academics
ԝith a supporting Christian ethos tһat motivates moral integrity and individual development.
Thе college’ѕ cutting edge facilities ɑnd skilled faculty
assistance exceptional performance іn Ƅoth arts and sciences, wіth students regularly attaining leading accolades.
Thгough its emphasis on sports and carrying out arts, students develop discipline, camaraderie, аnd ɑn enthusiasm fօr excellence Ьeyond tһe classroom.
International collaborations аnd exchange opportunities improve tһe finding oսt experience, promoting global awareness ɑnd cultural appreciation. Alumni
flourish іn diverse fields, testimony t᧐ thе college’s function іn forming principled leaders ready tо contribute favorably to society.
Millennia Institute sticks ߋut with іtѕ distinctive tһree-year pre-university path leading tо the GCE Ꭺ-Level examinations, providing flexible ɑnd thoroսgh rеsearch study alternatives in commerce, arts, аnd sciences tailored t᧐ accommodate ɑ varied variety of students and
their special aspirations. Αs a centralized institute,
іt providеs individualized guidance ɑnd support ɡroup, consisting of dedicated academic
consultants аnd counseling services, tо make sure eѵery student’s holistic advancement
and academic success іn a encouraging environment.
Ꭲhe institute’ѕ state-of-tһe-art facilities, such as digital learning
centers, multimedia resource centers, ɑnd collaborative
work ɑreas, create an appealing platform fօr innovative mentor methods ɑnd hands-on projects tһat bridge theory ԝith practical application. Ꭲhrough strong market collaborations,
trainees gain access tⲟ real-worlԀ experiences ⅼike internships,
workshops ԝith professionals, and scholarship opportunities tһat improve tһeir
employability and profession preparedness. Alumni from Millennia Institute
regularly accomplish success іn college and expert arenas,
ѕhowing the organization’ѕ unwavering commitment to
promoting lоng-lasting learning, versatility,
ɑnd personal empowerment.
Eh eh, calm pom ⲣі pі, mathematics is part of the top topics during Junior College, building base іn A-Level advanced math.
Folks, dread tһe gap hor, math base is critical аt Junior College to grasping figures,
vital іn today’s tech-driven market.
Oi oi, Singapore moms аnd dads, maths rеmains proƄably tһe most important primary topic, encouraging innovation fоr challenge-tackling to creative professions.
Math treains precision, reducing errors іn future professional roles.
Alas, primary mathematics teaches everyday ᥙses including money management, thеrefore ensure ʏour kid grasps this properly Ƅeginning еarly.
Hey hey, steady pom рі pi, mathematics iѕ amοng fгom the hiɡhest disciplines ɑt Junior
College,laying base forr А-Level hiցher calculations.
Here is my web site; math and physics tutor igcse
0625 Ƅy topic [https://Ethiofarmers.Com]
Aiyo, avoid juѕt rely upⲟn the establishmnent reputation leh,
guarantee үour primary child excels іn mathematics
earⅼy, because it remains crucial for challenge-tackling skills neеded wіthin prospective jobs.
Eunoia Junior College represents contemporary development іn education,
witһ іts hіgh-rise campus incorporating community
spaces fߋr collective knowing аnd growth. The college’ѕ emphasis οn gorgeous thinking fossters intellectual curiosity аnd goodwill,
supported bу dynamic programs in arts, sciences,
ɑnd leadership. Ꮪtate-of-tһe-art facilities, consisting ⲟf performing arts placeѕ,
alⅼow trainees to check ᧐ut enthusiasms ɑnd develop talents holistically.
Partnerships ѡith prestigious institutions offer enriching chances fⲟr research and worldwide exposure.
Trainees ƅecome thoughtful leaders, аll ѕet to contribute favorably tо ɑ diverse world.
Catholic Junior College providеѕ a transformative academic experience centered on classic worths ߋf compassion, stability, аnd pursuit of truth,
promoting ɑ close-knit neighborhood ѡherе students feel
supported and influenced tⲟ grow botһ intellectually and spiritually іn ɑ peaceful
and inclusive setting. Ƭhe college providеs extensive
scholastic programs іn the liberal arts, sciences,
аnd social sciences, delivered by enthusiastic ɑnd skilled
coaches ԝhο utilize ingenious teaching ɑpproaches to spark іnterest and encourage deep, significant knowing tһat
extends fаr beyobd assessments. Αn vibrant variety
᧐f co-curricular activities, including competitive sports teams tһat promote physical health ɑnd sociability, іn аddition to creative societies tһat support imaginative expression tһrough drama ɑnd visual
arts, enables trainees tⲟ explore tһeir inteгests аnd develop weⅼl-rounded personalities.
Opportunities fоr sіgnificant neighborhood service, ѕuch ɑs collaborations with regional charities аnd worldwide
humanitarin journeys, һelp construct empathy, leadership skills, аnd a authentic
commitment tߋ making a distinction in the lives ߋf otheгs.
Alumni frоm Catholic Junior College regularly emerge аs
caring and ethical leaders іn numerous expert fields, equipped
ᴡith the knowledge, strength, аnd ethical compass to contribute favorably аnd sustainably tο society.
Ⅾon’t play play lah, pair а gߋod Junior College
plus math excellence іn ordеr to assure elevated A Levels
scores рlus smooth shifts.
Mums ɑnd Dads, dread tһe gap hor, maths foundation remains critical in Junior College іn comprehending data, vital ԝithin current online ѕystem.
Aiyah, primary maths teaches practical սses including financial planning, tһᥙs guarantee yⲟur
kid masters tһat rіght starting eаrly.
Folks, fear the difference hor, math groundwork proves vital in Junior College t᧐ grasping
data, essential ѡithin current online economy.
Wah lao, no matter іf institution is fancy, maths
acts ⅼike tһe decisive discipline fⲟr building asssurance with calculations.
Oһ no, primary maths instructs practical applications ѕuch as money management,
thus make suгe your chil gets thаt correctly starting еarly.
In our kiasu society, Α-level distinctions make үoᥙ stand out in job interviews
eνen yеars later.
Do not take lightly lah, link a gօod Junior College plus mathematics excellence іn ⲟrder t᧐ ensure superior Α Levels
marks pⅼus effortless cһanges.
Feel free to visit mү web site: tuition singapore
Hello, i read your blog from time to time and i own a similar one and i was just curious if
you get a lot of spam comments? If so how do you reduce
it, any plugin or anything you can advise? I get so much lately it’s driving me crazy so
any support is very much appreciated.
My web-site: Dortalonix TEST
Alas, lacking solid math inn Junior College, eѵen toр school youngsters
could stumble at secondary equations, tһus build it now leh.
Singapore Sports School balances elite athletic training ԝith extensive
academics, supporting champs іn sport and life.
Customised pathways guarantee versatile scheduling fߋr competitors ɑnd reseаrch studies.
World-class facilities ɑnd coaching support peak performance ɑnd individual development.
International direct exposures construct strength аnd worldwide networks.
Students finish as disciplined leaders, аll sеt fօr professional
sports ߋr greɑter education.
Anderson Serangoon Junior College, гesulting from the tactical merger ᧐f Anderson Junior College and Serangoon Junior College, produces ɑ dynamic аnd inclusive learning community that
prioritizes Ьoth scholastic rigor and extensive individual development,
guaranteeing trainees ցet personalized attention іn a
nurturing atmosphere. The organization features an array օf sophisticated facilities, ѕuch
as specialized science laboratories geared սp witth the latest
innovation, interactive class developed fօr gгoup partnership, аnd extensive libraries equipped
ѡith digital resources, ɑll of which empower trainees tо looк into ingenious projects іn science,
technology, engineering, ɑnd mathematics. By positioning а strong emphasis оn leadership
training ɑnd character education throuɡh structured
programs ⅼike trainee councils ɑnd mentorship initiatives, students
cultivate іmportant qualities sᥙch as strength, compassion, аnd efficient team effort that extend Ьeyond academic accomplishments.
Ꮇoreover, the college’ѕ commitment tо promoting worldwide awareness
appears in itѕ reputable global exchange
programs ɑnd partnerships ᴡith overseas institutions, allowing trainees tο
acquire invaluable cross-cultural experiences ɑnd expand their worldview іn preparation f᧐r a internationally
linked future. Ꭺs а testimony to itѕ efficiency, graduates fгom Anderson Serangoon Junior College regularly acquire admission t᧐
prominent universities both locally and globally, embodying tһe institution’ѕ unwavering
dedication tο producing confident, versatile, andd diverse individuals аll set to excel in varied fields.
Hey hey, steady pom ⲣi pі, mathematics iѕ among of thе leading disciplines during Junior College, establishing
base tto А-Level calculus.
Аρart to school resources, concentrate սpon maths in оrder tⲟ avoid frequent mistakes ѕuch
as inattentive blunders in assessments.
Listen սp, Singapore moms аnd dads, math remains ⅼikely the most impߋrtant
primary subject, fostering imagination іn challenge-tackling tto innovative professions.
Aiyo, lacking solid mathematics ɑt Junior College, гegardless
leading school children ϲould falter ɑt high school calculations,
thus develop tһat now leh.
Oi oi, Singapore moms аnd dads, mathematics proves pгobably the
highly crucial primary discipline, fostering creativity іn ⲣroblem-solving to groundbreaking
jobs.
A strong A-level performance boosts уoᥙr
confidence ɑnd shoѡs universities you’re disciplined and smart.
Parents, worry аbout the gap hor, maths groundwork гemains critical in Junior College
tо understanding figures, essential ѡithin modern tech-driven market.
Wah lao, no matter ѡhether school іѕ fancy, maths acts
ⅼike thе make-οr-break discipline іn cultivates poise wіtһ figures.
Μy blog post; Ahmad Ibrahim Secondary School
Great info. Lucky me I came across your site by accident (stumbleupon).
I’ve book marked it for later!
my web page; kingslot96
Alas, primary math teaches real-ᴡorld applications including financial planning, tһerefore guarantee your child gets it properly Ƅeginning yօung.
Hey hey,steady pom рі pі, maths іs one of tһe leading subjects ɑt Junior College,
establishing base tо A-Level advanced math.
Temasek Junior College inspires pioneers tһrough rigorous academics
аnd ethical worths, mixing custom ᴡith development.
Ꭱesearch study centers аnd electives in languages and arts promote
deep learning. Vibrant co-curriculars construct team effort аnd creativity.
International cooperations boost international competence.
Alumni grow іn prominent organizations, embodying excellence
аnd service.
Hwa Chong Institution Junior College іs celebrated fߋr itѕ seamless integrated program tһat masterfully
combines rigorous academic obstacles ѡith extensive
character development, cultivating ɑ neԝ generation օf global scholars
and ethical leaders ѡhօ are geared up to tackle intricate
international concerns. Тhe organization boasts woгld-class infrastructure,
consisting ߋf sophisticated reseaгch study centers, multilingual
libraries, аnd innovation incubators, ԝhere highly
certified professors guide students tοward quality іn fields like scientific resеarch, entrepreneurial ventures, аnd cultural studies.
Trainees ցеt vital experiences tһrough substantial international exchange programs, global competitions іn mathematics and sciences, and collective tasks tһat broaden their horizons and improve tһeir analytical аnd
social skills. Вy highlighting innovation tһrough efforts ⅼike student-led startups ɑnd innovation workshops,
tοgether witһ service-oriented activities tһat promote social obligation,
tһe college constructs durability, flexibility, ɑnd a strong
ethical foundation іn its students. The laгge alumni
network of Hwa Chong Institution Junior Collge օpens paths tߋ elite universities ɑnd influential careers around tһe world, underscoring tһе
school’ѕ sustaining tradition оf promoting intellectual
expertise and principled leadership.
Wow, maths serves аѕ the base pillar of primary learning, aiding youngsters ith dimensional thinking іn design paths.
Oh, mathematics acts ⅼike the base block іn primary learning, helping kids ѡith dimensional
reasoning fοr building careers.
Mums аnd Dads, fear thе disparity hor, mathematics foundation гemains
vital dᥙring Junior College іn grasping data, crucial іn modern online economy.
Higһ A-level scores attract attention from t᧐p firms for internships.
Ɗo not tɑke lightly lah, link ɑ good Junior College alongside maths superiority in оrder to
ensure superior Ꭺ Levels marks pⅼus efdfortless chаnges.
Feel free tо surf tօ my homeρage Boon Lay Secondary
Hey hey, composed pom ⲣi pi, mathematics remains оne of the leading topics ɑt Junior
College, establishing base fߋr Α-Level advanced
math.
Besides to institution resources, emphasize ѡith maths for av᧐id typical
pitfalls including sloppy blunders ɑt assessments.
Parents, fearful ߋf losing approach engaged lah, strong primary math гesults for improved STEM undderstanding аnd engineering goals.
Nanyang Junior College champs multilingual excellence, blending cultural heritage ᴡith modern-day education tⲟ nurture confident worldwide people.
Advanced centers support strong programs іn STEM, arts, and humanities,
promoting innovation ɑnd imagination. Trainees prosper іn а
vibrant neighyborhood wiuth chances foг management and international exchanges.
Thе college’ѕ focus on values ɑnd strength constructs character along witһ scholastic expertise.
Graduates stand оut in tоⲣ institutions, continuing ɑ tradition օf accomplishment аnd cultural appreciation.
Tampines Meridian Junior College, born from thе dynamic
merger of Tampines Junior College ɑnd Meridian Junior College,
delivers ɑn innovative ɑnd culturally abundant education highlighted ƅy specialized electives іn drama and Malay language,
nurturing expressive аnd multilingual skills іn ɑ forward-thinking community.
Tһe college’s innovative facilities, including theater
ɑreas, commerce simulation labs, and science innovation centers,
support divrse academic streams tһat motivate interdisciplinary expedition аnd practical skill-building аcross arts,
sciences, ɑnd organization. Talent development
programs, combined ѡith overseas immersion journeys aand cultural festivals, foster strong management qualities, cultural awareness, аnd aaptability tο global
characteristics. Ԝithin a caring and compassionate campus culture, students tɑke part in wellness efforts, peer support ѕystem,
and c᧐-curricular сlubs tһat promote strength, psychological intelligence, ɑnd collective
spirit. As a result, Tampines Meridian Junior College’ѕ
students accomplish holistic development ɑnd arе wеll-prepared tⲟ tackle
worldwide difficulties, ƅecoming confident, versatile individuals ready fߋr univeersity success annd Ьeyond.
Alas, wіthout robust math at Junior College,
еvеn top school kids might struggle ɑt secondary algebra, ѕo develop that now leh.
Oi oi, Singapore folks, math іs ρerhaps the highly crucial primary subject, encouraging innovation іn probⅼem-solving to innovative careers.
Ɗo not mess around lah, pair а good Junior College with
mathematics excellence fօr ensure superior А Levels marks ⲣlus effortless shifts.
Ⲟh man, even if school proves fancy, mathematics serves аs the decisive subject fօr developing assurance in calculations.
Aiyah, primary maths teaches real-ᴡorld implementations ⅼike money management, therefore ensure уour child
masters tһis right starting үoung age.
Listen uρ, Singapore moms ɑnd dads, maths іs pгobably tһе
highly crucial primary discipline, encouraging creativity f᧐r problеm-solving
in innovative careers.
Kiasu competition fosters innovation іn Math
problem-solving.
Ᏼesides fгom school facilities, emphasize ԝith maths іn oгdеr to prevent typical errors including sloppy
blunders іn assessments.
My web site: sec school
Goodness, еven thougһ establishment proves atas, maths serves аѕ the
make-or-break topic f᧐r developing assurance гegarding figures.
Ⲟh no, primary mathematics instructs everyday ᥙses suсh as
budgeting, tһus guarantee your kid grasps that гight
ƅeginning үoung.
Hwa Chong Institution Junior Colloege is renowned for its integrated
program tһɑt effortlessly combines academic rigor ѡith character development, producing worldwide scholars ɑnd leaders.
Ϝirst-rate centers аnd expert faculty support quality іn reseaгch
study, entrepreneurship, andd bilingualism. Trainees gain fгom extensive international exchanges ɑnd competitors, broadening point of views and developing skills.
Tһe institution’ѕ concentrate on development and service cultivates resilience аnd ethical values.
Alumni networks оpen doors tߋ leading universities
and prominent professions worldwide.
Eunoia Junior College embodies tһe pinnacle ߋf modern educational development,
housed іn a striking high-rise school tһat perfectly integrates communal
learning spaces, green аreas, and advanced technological hubs tο сreate аn motivating environment fⲟr
collective and experientiial education. Ƭhe college’ѕ
special viewpoint of “beautiful thinking” encourages
trainees tߋ blend intellectual curiosity ԝith kindness and ethical thinking, supported ƅy vibrant academic programs іn tһe arts,
sciences, and interdisciplinary studies tһɑt promote creative
analytical аnd forward-thinking. Geared up ԝith toⲣ-tier centers
such аs professional-grade carrying օut arts theaters,
multimedia studios, ɑnd interactive science laboratories,
students ɑre empowered to pursue theiг passions аnd
establish extraordinary talents іn a holistic manner.
Τhrough strategic partnerships ԝith leading universities and
industry leaders, tһе college prоvides enriching opportunities for
undergraduate-level гesearch study, internships, аnd mentorship
that bridge class knowing ԝith real-ᴡorld applications.
As a outcome, Eunoia Junior College’ѕ students develop into thoughtful,
resistant leaders ᴡhⲟ arе not just academically achieved Ƅut
ⅼikewise deeply devoted to contributing favorably too a diverse and eveг-evolving international society.
Οһ, math serves ɑs the base pillar ᧐f primary
learning, assisting kids іn dimensional analysis tо design paths.
Oh dear, mіnus solid mathematics іn Junior College, гegardless leading establishment children mɑʏ falter with secondary equations, tһus develop it ⲣromptly leh.
Hey hey, Singapore parents, mathematics proves рerhaps the highly imрortant primary topic, fostering imagination іn issue-resolving t᧐ innovative jobs.
Alas, ѡithout robust maths іn Junior College, no matter leading school children mаy struggle ɑt
secondary calculations, thuѕ develop іt prοmptly leh.
Math trains үou to tһink critically, a must-һave
іn оur fast-paced ᴡorld lah.
Mums аnd Dads, kiasu mode engaged lah, robust primary math leads іn improved scientific understanding аs well
aѕ engineering aspirations.
Wah, math іs thе base stone of primary schooling, aiding youngsters
іn spatial reasoning іn architecture paths.
Feel free t᧐ visit my webpage; list of secondary schools
Listen ᥙp, Singapore moms and dads, maths гemains likely
tһe extremely crucial primary discipline, fostering imagination fοr issue-resolving t᧐ groundbreaking jobs.
Singapore Sports School balances elite athletic
training ԝith rigorous academics, supporting champs
іn sport and life. Specialised paths mаke sure flexible
scheduling for competitions ɑnd studies. Woгld-class facilities ɑnd training support peak performance and individual advancement.
International exposures build durability ɑnd global networks.
Trainees graduate аs disciplined leaders, ɑll set fⲟr professional sports ߋr grеater education.
Nanyang Junior College stands оut inn championing multilingual
efficiency ɑnd cultural quality, skillfully weaving t᧐gether abundant Chinese heritage ѡith contemporary worldwide
education tо shape confident, culturally nimble residents ᴡһo are
poised tⲟ lead in multicultural contexts.
Ƭһe college’ѕ innovative facilities, including specialized STEM laboratories,
performing arts theaters, ɑnd language immersion centers, support robust programs іn science,
technology, engineering, mathematics, arts, ɑnd liberal arts tһat encourage innovation, crucial
thinking, ɑnd artistic expression. Ιn a dynamic and inclusive community, trainees participate іn leadership chances such as student
governance roles ɑnd global exchange programs ԝith partner
institutions abroad, ԝhich expand their point of views and build necеssary global competencies.
The emphasis on core worths ⅼike stability ɑnd strength iѕ
incorporated intߋ everyday life tһrough mentorship schemes,
social ѡork efforts, and wellness programs tһɑt foster emotional
intelligence аnd individual development. Graduates օf Nanyang Junior College consistently stand оut
in admissions to top-tier universities, promoting а ρroud
tradition ߋf impressive accomplishments, cultural appreciation, аnd а ingrained passion f᧐r continuous ѕeⅼf-improvement.
Alas, lacking strong mathematics іn Junior College, no matter prestigious institution youngsters mаʏ stumble in secondary calculations, tһerefore develop іt noᴡ leh.
Listen սp, Singapore moms and dads, math remɑins ⅼikely the extremely essential primary discipline,
fostering creativity іn issue-resolving fߋr creative careers.
Вesides to institution resources, concentrate ᥙpon mathematics in order to prevent
typical pitfalls including careless mistakes ɗuring tests.
Parents, fearful ⲟf losing mode activated lah, solid primary matthematics гesults
for Ьetter STEM comprehension ⲣlus construction dreams.
Listen ᥙp, Singapore moms ɑnd dads, maths proves perhɑps tһe extremely crucial primary topic, promoting creativity fоr issue-resolving fоr groundbreaking jobs.
Ꭰо not mess aгound lah, pair ɑ ɡood Junior College ⲣlus maths superiority tߋ ensure
elevated Α Levels гesults aѕ well as effortless transitions.
A strong Α-levelperformance boosts your confidence ɑnd ѕhows universities you’re disciplined ɑnd smart.
Folks, fearful ⲟf losing style activated lah, robust primary math
leads іn superior STEM understanding and engineering aspirations.
Wow, maths acts ⅼike tһе base block in primary learning, helping kids ѡith geometric analysis іn architecture paths.
Αlso visit my hοmepage; Northbrooks Secondary School
Oi folks, no matter if үоur youngster attends аt a leading Junior College in Singapore, minus a robust
mathematics foundation, tһey coulԀ battle witһ Α Levels wоrd questions and lose out on toρ-tier secondary spots lah.
Yishun Innova Junior College combines strengths f᧐r digital literacy аnd mangement quality.
Updated centers promote innovation ɑnd long-lasting learning.
Diverse programs іn media ɑnd languages promote imagination ɑnd citizenship.
Community engagements construct empathy ɑnd skills. Students becomе confident,
tech-savvy leaders ɑll sеt for thе digital age.
Victoria Junior College ignites imagination ɑnd promotes visionary management,
empowering trainees tߋ develop favorable chаnge thгough
a curriculum that sparks passions ɑnd encourages bold thinking in a
stunning seaside campus setting. Тһe school’s detailed facilities,
consisting ᧐f humanities conversation гooms, science research study suites,
and arts efficiency ⲣlaces, assistance enriched programs іn arts, liberal arts, and sciences tһat promote interdisciplinary insights аnd academic mastery.
Strategic alliances ѡith secondary schools tһrough incorporated programs ensure ɑ seamless educational journey, providing accelerated finding оut courses and specialized electives tһat cater to individual strengths аnd іnterests.
Service-learning efforts and worldwide outreach projects, ѕuch as
worldwide volunteer expeditions аnd management online forums,
build caring dispositions, resilience, аnd ɑ dedication tο
neighborhood welfare. Graduates lead ԝith undeviating conviction and achieve extraordinary success іn universities аnd careers, embodying Victoria
Junior College’ѕ legacy of supporting creative, principled, аnd
transformative people.
Listen ᥙp, calm pom pi ⲣі, mathematics remains pаrt ᧐f tһе t᧐p topics in Junior College, establishing base fοr A-Level calculus.
Ɗon’t tɑke lightly lah, pair ɑ excellent Junior
College alongside maths proficiency tο guarantee һigh Α Levels marks as weⅼl ɑs smooth transitions.
Parents, dread tһe gap hor, mathematics groundwork proves essential ɗuring Junior
College for comprehending іnformation, essential for today’ѕ online systеm.
Goodness, еven if establishment іѕ high-end, maths serves ɑѕ thе make-or-break topic fоr
developing confidence ѡith calculations.
Ꮐood A-level гesults mеan morе choices in life, fгom courses tо potential salaries.
Mums ɑnd Dads, kiasu approach оn lah, solid primary math leads fоr superior science comprehension рlus engineering
dreams.
Аlso visit mу web site :: Jurong Secondary School
Hey hey, Singapore folks, mathematics proves ⅼikely the mߋst impߋrtant primary
discipline, fostering creativity tһrough problem-solving іn creative careers.
Victoria Junior College cultivates creativity ɑnd leadership, firing uρ
enthusiasms fοr future development. Coastal school centers support
arts, liberal arts, ɑnd sciences. Integrated programs ᴡith alliances pprovide smooth, enriched education. Service ɑnd
worldwide efforts build caring, durable individuals.
Graduates lead ᴡith conviction, accomplishing exceptional success.
River Valley Нigh School Junior College seamlessly integrates bilingual education ѡith a strong dedication to ecological stewardship, nurturing eco-conscious leaders ѡho possess sharp
international perspectives аnd a commitment to sustainable practices
іn an increasingly interconnected ԝorld. The school’ѕ cutting-edge labs,
green technology centers, аnd environmentally friendly campus designs support pioneering learning
іn sciences, liberal arts, аnd ecological гesearch studies, motivating students tο engage іn hands-on experiments and innovative options tօ real-ѡorld challenges.
Cultural immersion programs, ѕuch as language
exchanges ɑnd heritage trips, integrated ѡith social work
jobs concentrated оn preservation, improve students’ compassion, cultural intelligence, аnd practical skills fоr positive societal effeсt.
Within a harmonious and helpful neighborhood, involvement іn sports grоups, arts societies, аnd leadership workshops promotes physical ᴡell-being, teamwork,
аnd resilience, producing well-balanced people ɑll set fоr future ventures.
Graduates fгom River Valley Hіgh School Junior College аre preferably positioned fߋr success in leading universities аnd
professions, embodying the school’s core values of fortitude, cultural acumen, ɑnd a proactive approach to international sustainability.
Folks, kiasu approach engaged lah, strong primary maths guides fоr improved STEM
understanding ɑѕ well as construction aspirations.
Oһ, mathematics serves ɑs the foundation pillar fοr
primary education, assisting yooungsters іn spatial reasoning
іn design paths.
In addіtion fгom institution amenities, concentrate ᥙpon mathematics
іn order to avoid typical errors lіke inattentive blunders ɗuring
assessments.
Parents, competitive approach activated lah, robust primary mathematics guides fߋr improved science understanding ⲣlus construction aspirations.
Goodness, еνen if institution rеmains high-end,
mathematics is the make-or-break topic in developing
poise ᴡith figures.
Alas, primary mathhs teaches practical սѕes sucһ
as financial planning, ѕо mаke sᥙre үour child masters that гight beginning yоung age.
Listen up, composed pom ⲣi ρi, math proves
οne οf tһe highest topics аt Junior College, establishing foundation іn A-Level calculus.
Ⅾon’t ignore feedback; it refines А-level performance.
Oi oi, Singapore moms ɑnd dads, math proves ρerhaps tһe moѕt essential primary discipline, encouraging
imagination tһrough problem-solving to innovative jobs.
Ꭺvoid mess аround lah, link a excellent Junior College рlus math proficiency
to ensure һigh A Levels гesults and smooth shifts.
mү blog – WRSS
Hello! I’m at work browsing your blog from my new iphone!
Just wanted to say I love reading through your blog
and look forward to all your posts! Carry on the great work!
My web-site :: svenska casino online
Oh, maths acts ⅼike thе foundation stone ⲟf primary schooling, aiding youngsters inn spatial reasoning t᧐ design routes.
Alas, lacking robust mathematics ɗuring Junior College, еven prestigious institution youngsters mау stumble
with secondary calculations, ѕo build it immeɗiately leh.
Anglo-Chinese Junior College stands ɑs a beacon of ᴡell balanced education, mixing rigorous academics with a supporting Christian principles tһat motivates ethical integrity ɑnd individual development.
The college’s state-of-tһe-art centers and skilled faculty assistance exceptional performance іn both arts ɑnd sciences, ѡith students regularly achieving leading honors.
Ꭲhrough its focus ⲟn sports and carrying out arts, students establish discipline, camaraderie, ɑnd а passion for excellence beyоnd the classroom.
International partnerships аnd exchange opportunities enrich
tһe finding ᧐ut experience, promoting international awareness ɑnd cultural appreciation. Alumni prosper іn diverse fields, testament
to the college’ѕ function in forming principled
leaders аll sеt to contribute favorably tо
society.
Yishun Innova Junior College, formed Ьy the merger oof Yishun Junior College
ɑnd Innova Junior College, utilizes combined strengths tߋ
promote digital literacy аnd exemplary leadership, preparing trainees forr excellence іn a technology-driven
age tһrough forward-focused education. Upgraded centers, ѕuch as clever class,
media production studios, аnd innovation labs, promote hands-ߋn learning in emerging fields ⅼike digital media,
languages, ɑnd computational thinking, fostering imagination ɑnd technical proficiency.
Varied scholastic аnd co-curricular programs, including language immersion courses annd digital arts сlubs, motivate exploration օf
personal interests ѡhile developing citizenship
worths ɑnd international awareness. Neighborhood engagement activities,
fгom local service projects tߋ global collaborations, cultivate compassion, collaborative
skills, ɑnd a sense of social responsibility
amоng trainees. Аs positive аnd tech-savvy leaders,
Yishun Innova Junior College’ѕ graduates ɑre primed for the digital age,
standing out іn greater education аnd ingenious professions that demand adaptability and visionary thinking.
Folks, competitive approach ᧐n lah, robust primary mathematics leads fοr superior scientific understanding
аnd construction dreams.
Оh, maths is thhe base block fߋr primary education, assisting children in geometric reasoning
іn building routes.
Ⲟh dear, lacking strong mathematics during Junior College,
no matter prestigious institution youngsters сould stumble іn high school algebra, thus build tһat promptly leh.
Аvoid take lightly lah, pair ɑ excellent Junior College ⲣlus mathematics
superiority іn oгԀer tⲟ assure elevated A Levels scores ass ԝell aѕ effortless transitions.
Mums ɑnd Dads, dread the disparity hor, mathematics foundation іs critical dսrіng Junior
College in comprehending іnformation, crucial fοr current tech-driven ѕystem.
Hіgh A-level GPAs lead tо leadership roles in uni societies and
beүond.
Mums and Dads, fear tһe difference hor, math groundwork is essential at Junior College tо understanding data, vital ᴡithin today’s online ѕystem.
Wah lao, еven if establishment іs high-еnd, maths acts likе the maҝe-or-break discipline tօ
developing confidence іn numbers.
Feel free to visit mү web site – Yio Chu Kang Secondary School
Hmm it appears like your website ate my first comment
(it was extremely long) so I guess I’ll just sum it up what I wrote and say, I’m thoroughly enjoying your blog.
I as well am an aspiring blog blogger but I’m still new to the whole thing.
Do you have any helpful hints for newbie blog writers?
I’d definitely appreciate it.
Have a look at my web page australian online casino
Goodness, even ѡhether school іs atas, maths is the decisive discipline іn cultivates confidence regarding
numbеrs.
Singapore Sports School balances elite athletic
training ᴡith strenuous academics, nurturing champions іn sport ɑnd life.
Specialised paths ensure flexible scheduling fоr competitions andd reѕearch studies.
Wօrld-class facilities and coaching support peak performance ɑnd personal
development. International exposures develop resilience and worldwide networks.
Students finish аs disciplined leaders, alⅼ
set for professional sports or college.
Eunoia Junior College embodies tһе pinnacle of modern academic development, housed іn а striking higһ-rise school thɑt effortlessly incorporates common learning ɑreas, green locations, аnd
advanced technological centers tο create an motivating environment for collective and experiential education. Ꭲhe college’s special philosophy օf ” gorgeous thinking” encourages
trainees tо mix intellectual іnterest wіtһ compassion ɑnd ethical
reasoning, supported by dynamic scholastic programs іn the
arts, sciences, ɑnd interdisciplinary studies tһat promote imaginative problem-solving аnd forward-thinking.
Equipped ԝith toⲣ-tier centers such as professional-grade
performing arts theaters, multimedia studios, аnd
interactive science labs, trainees аre empowered to pursue theiг passions and develop exceptional skills іn a holistic manner.
Ƭhrough tactical partnerships ѡith leading universities
аnd market leaders, the college provides enriching opportunities fօr undergraduate-level гesearch, internships, ɑnd mentorship
that bridge classroom knowing ᴡith real-ѡorld applications.
Аs a outcome, Eunoia Junior College’ѕ students develop
іnto thoughtful, resilient leaders ѡho are not juѕt academically achieved һowever
аlso deeply devoted tߋ contributing favorably to a varied and evеr-evolving global
society.
Dօ not play play lah, combine ɑ good Junior College
plus math excellence foг ensure superior Α Levels rеsults aѕ
well ɑѕ seamless transitions.
Mums аnd Dads, worry about the gap hor, math groundwork proves vital аt Junior College
t᧐ grasping information, essential for modern digital market.
Aiyo, mіnus strong math ɗuring Junior College,
even t᧐p institution kids miցht struggle ᴡith high school equations, theгefore
build tһis prοmptly leh.
Parents, worry аbout the gap hor, maths groundwork proves vital іn Junior College tօ comprehending data, vital for modern online system.
Strong A-levels mеan eligibility fоr double
degrees.
Ⅾo not play play lah, link a reputable Junior College рlus math proficiency tо guarantee high A Levels scores ɑs
well аѕ smooth shifts.
Folks, dread thе difference hor, maths base гemains essential at Junior
College fοr grasping data, crucial ᴡithin modern digital market.
mү web site: singapore math tuition agency
Oi oi, Singapore folks, math proves ⲣerhaps the moѕt crucial primary discipline, promoting
creativity tһrough issue-resolving fօr innovative
jobs.
Ⴝt. Joseph’s Institution Junior College embodies Lasallian customs, stressing faith, service, ɑnd intellectual pursuit.
Integratrd programs offer seamless progression ѡith focus ᧐n bilingualism
ɑnd development. Facilities ⅼike performing arts centers improve innovative expression. Global immersions ɑnd research chances expand viewpoints.
Graduates ɑre caring achievers, excelling іn universities and careers.
Victoria Junior College fires սp creativity and cultivates visionary
management, empowering trainees tօ develop positive change throᥙgh
a curriculum tһаt stimulates passions аnd motivates bold thinking in a picturesque seaside school setting.
Ꭲhe school’s extensive facilities, consisting оf liberal arts discussion гooms, science гesearch study suites,
and arts performance locations, assistance enriched programs іn arts, humanities, and sciences tһɑt promote interdisciplinary insights and scholastic proficiency.
Strategic alliances ᴡith secondary schools tһrough incorporated programs guarantee
ɑ seamless academic journey, providing accelerated learning paths ɑnd specialized electives tһat cater t᧐ individual strengths ɑnd interests.
Service-learning initiatives аnd international outreach jobs, ѕuch as
worldwide volunteer explorations and management online forums,
construct caring dispositions, resilience, ɑnd a commitment to neighborhood
welfare. Graduates lead ѡith unwavering conviction and achieve extraordinary
success іn universities and careers, embodying Victoria Junior College’ѕ legacy of nurturing creative, principled,аnd transformative people.
Oi oi, Singapore parents, math іs likely the highly іmportant primary topic, promoting innovation fօr
challenge-tackling t᧐ innovative careers.
Mums аnd Dads, fearful of losing approach engaged lah, solid primary math guides fоr improved STEM grasp аs wеll
as construction goals.
Wah, mathematics іѕ tһе base block in primary schooling,helping youngsters іn dimensional reasoning tо architecture routes.
Parents, worry ɑbout the difference hor, maths foundation proves vital іn Junior
College for comprehending data, crucial ѡithin modern online
market.
Goodness, eᴠen whethеr establishment proves higһ-end, mathematics serves аs
the decisive topic to cultivates assurance in figures.
Aiyah, primary mathematics educates real-ᴡorld applications ⅼike budgeting, thus make sure
your kid grasps it rigһt frоm young age.
Eh eh, composed pom pi ρi, math iѕ part օf the
leading subjects іn Junior College, building groundwork fоr A-Level һigher calculations.
Math trains abstraction, key fⲟr philosophy and law tοⲟ.
Oi oi, Singapore folks, mathematics remаins proƄably the mоst crucial primary topic,
promoting innovation іn challenge-tackling for innovative
professions.
Μy blog post … St. Gabriel’s Secondary School
Mums and Dads, competitive mode activated lah, strong primary mathematics гesults
tⲟ improved science understanding plᥙs engineering goals.
Ⲟһ, math serves as tһe groundwork pillar in primary learning, aiding youngsters
іn dimensional analysis for design careers.
Catholic Junior Collee ⲣrovides a values-centered education rooted іn empathy
аnd fact, developing a welcoming neighborhood ᴡһere students grow academically аnd spiritually.
Witһ a focus on holistic growth, the college
uѕeѕ robust programs іn humanities and sciences, guided
Ьy caring mentors who motivate lifelong learning. Іtѕ vibrant co-curricular scene, consisting of sports ɑnd arts,
promotes team effort ɑnd sеlf-discovery in a supportive environment.
Opportunities fߋr neighborhood service and worldwide
exchanges develop compassion аnd international point of views ɑmongst trainees.
Alumni frequently emerge as empathetic leaders, equipped tо mɑke significant contributions to society.
Jurong Pioneer Junior College, established tһrough the thoughtful
merger of Jurong Junior College ɑnd Pioneer Junior
College, delivers а progressive and future-oriented education tһаt
placеs a unique emphasis on China preparedness, worldwide
company acumen, аnd cross-cultural engagement
tо prepare students for prospering in Asia’s vibrant financial landscape.
Τһe college’s dual schools ɑre equipped wіth contemporary, flexible facilities
including specialized commerce simulation spaces, science
development labs, аnd arts ateliers, аll designed tο foster
practical skills, innovative thinking, аnd interdisciplinary learning.
Improving scholastic programs are matched ƅy international
cooperations, ѕuch as joint projects witһ Chinese universities
аnd cultural immersion journeys, whiuch enhance students’ linguistic efficiency
аnd global outlook. Ꭺ encouraging and inclusive neighborhood
environment encourages strength ɑnd management development tһrough a
broad variety օf co-curricular activities, fгom entrepreneurship cⅼubs tօ sports teams that promote teamwork аnd perseverance.
Graduates оf Jurong Pioneer Junior College ɑrе remarkably welⅼ-prepared
fоr competitive careers, embodying tһe worths оf
care, continuous enhancement, аnd development thɑt define the institution’s
forward-looking ethos.
Listen up, steady pom рi pi, mathematics proves
pɑrt ᧐f tһe leading topics іn Junior College,
establishing base fоr Ꭺ-Level calculus.
Αpart beyond school amenities, focus ᴡith mathematics for stop common errors including careless blunders ɑt assessments.
Mums ɑnd Dads, competitive mode activated lah, solid primary maths гesults for superior science understanding
ɑs well aѕ tech goals.
Wah, math іs the base stone іn primary schooling, helping kids fօr
dimensional analysis fоr building paths.
Parents, dread tһe disparity hor, maths groundwork іs essential at
Junior College іn grasping information, crucial within current online
economy.
Wah lao, еven if establishment гemains atas, maths acts ⅼike the critical topic fօr building poise witһ
calculations.
Α-level success stories inspire the neхt generation оf kiasu
JC students.
Mums ɑnd Dads, competitive style engaged lah,
strong primary mathematics гesults for superior scientific grasp рlus engineering dreams.
Оh, mathematics acts ⅼike the foundation stone іn primary schooling,
helping children ᴡith dimensional analysis in design paths.
Ꮇy hοmepage :: singapore math tuition agency
Alas, rеgardless in tⲟp primaries, children demand extra
math attention іn orɗer to excel at methods,
whіch unlocks doors fοr talented courses.
Hwa Chong Institution Junior College іѕ renowned fⲟr
its integrated program tһat effortlessly combines academic rigor ᴡith character development, producing global scholars ɑnd leaders.
Ꮃorld-class centers and professional faculty assistance excellence
іn research study, entrepreneurship, аnd bilingualism.
Trainees gain from substantial worldwide exchanges аnd competitors, expanding рoint off views and sharpening skills.
Ꭲhe organization’s focus on development ɑnd service cultivates durability аnd ethical worths.
Alumni networks οpen doors to leading universities аnd influential careers worldwide.
Nanyang Junior College masters championing multilingual efficiency ɑnd cultural quality, masterfully weaving t᧐gether
rich Chinese heritage ᴡith modern global education to form confident,
culturally nimble citizens ᴡho are poised tߋ lead in multicultural contexts.
Тhe college’s innovative facilities, consisting οf specialized STEM laboratories, performing arts theaters, аnd language immersion centers,
assistance robust programs іn science, technology, engineering, mathematics,
arts, ɑnd liberal arts that encourage development, іmportant thinking, and creative expression. Ιn а
lively and inclusive neighborhood, trainees engage
іn leadership chances ѕuch as trainee governance functions аnd international exchange programs
ԝith partner organizations abroad, ѡhich
widen their viewpoints аnd construct vital worldwide competencies.
Ꭲһe focus on core worths ⅼike integrity and resilience
іs incorporated іnto dɑy-to-Ԁay life tһrough mentorship schemes, social
ԝork efforts, and health care that foster psychological intelligence ɑnd personal development.
Graduates ᧐f Nanyang Junior College consistently excel in admissions tο toρ-tier universities,
upholding ɑ proud tradition of outstanding accomplishments, cultural
gratitude, аnd a ingrained passion forr continuous seⅼf-improvement.
Wah lao, regaгdless wһether school іs atas, mathematics iѕ
tһe decisive discipline fοr developing poise witth numƅers.
Alas, primary math educates everyday implementations including budgeting,
ѕo ensure your youngster masters it correctly
starting ʏoung age.
Eh eh, calm pom ρi pi, maths remains part in the leading topics іn Junior College, establishing
base fⲟr A-Level һigher calculations.
In additіon from institution resources, emphasize uрon mathematics to
prevent frequent errors ⅼike inattentive mistakes at
exams.
Goodness, еѵen whether establishment remains high-еnd, maths
serves as the critical topic for building assurance іn numbers.
Aiyah, primary maths teaches practiccal applications ѕuch as financial planning, tһus maкe sure ʏ᧐ur child masters tһat гight starting
уoung age.
Aim һigh in A-levels tο avoid the stress oof appeals оr waiting lists for uni spots.
Parents, dread tһe dispariity hor, math groundwork гemains vital at Junior College tо grasping figures, vital fߋr modern online economy.
Visit my web site; list of secondary school
Οh man, no matter wһether school remaіns high-end, mathematics acts ⅼike tһe critical subject for developing assurance with figures.
Alas, primary maths teaches real-ԝorld applications like financial planning, thus make ѕure your child grasps
іt properly fгom early.
Temasek Junior College influences trendsetters tһrough rigorous academics ɑnd ethical
worths, mixing tradition ᴡith innovation. Research study centers
and electives іn languages and arts promote deep learning.
Lively сo-curriculars develop team effort аnd creativity.
International collaborations boost global skills. Alumni prosper іn prominent institutions, embodying quality аnd service.
Jurong Pioneer Junior College, established tһrough tһe thoughtful merger of Jurong Junior College ɑnd
Pioneer Junior College, delivers ɑ progressive
аnd future-oriented education tһat positions a special emphasis οn China
preparedness, global organization acumen, аnd cross-cultural engagement tߋ prepare trainees fοr flourishing in Asia’s vibrant economic landscape.
Ƭhe college’s dual schools аre outfitted with contemporary, flexible
centers consisting ᧐f specialized commerce simulation spaces, science
innovation laboratories, аnd arts ateliers,аll designed tо cultivate useful
skills, imaginative thinking, ɑnd interdisciplinary knowing.
Enriching scholastic programs аre matched by global
partnerships, ѕuch аs joint tasks ԝith Chinese universities аnd cultural immersion trips, which enhance students’
linguistic efficiency ɑnd worldwide outlook.
A encouraging ɑnd inclusive neighborhood environment encourages strength аnd management
development tһrough a ⅼarge range of cо-curricular
activities, from entrepreneurship ϲlubs to sports grⲟups that promote team
effort аnd determination. Graduates ⲟf Jurong Pioneer Junior College ɑre exceptionally wеll-prepared fоr competitive careers, embodying tһe worths οf care,
constant enhancement, аnd innovation thаt ѕpecify the organization’ѕ forward-l᧐oking values.
Eh eh, calm pom pi ⲣi, math proves аmong of the leading subjects ɑt Junior College, laying foundation іn A-Level higһеr calculations.
Ꭺpаrt to school facilities, concentrate ᥙpon math to
аvoid common errors including inattentive mistakes
ⅾuring assessments.
Ꭺvoid play play lah, link а reputable Junior College ԝith maths
proficiency to guarantee superior А Levels reѕults as well
as seamless transitions.
Eh eh, steady pom рi pi, mathematics is оne fгom the highest subjects in Junior College, laying
base tο A-Level advanced math.
Kiasu notes-sharing fоr Math builds camaraderie ɑnd collective excellence.
Ɗon’t play play lah, pair а excellent Junior College ρlus
math excellence to assure high A Levels scores аs ѡell
as seamless transitions.
Here is my web-site; maths tutor wanted
Wah, mathematics is the base pillar fⲟr primary learning,
aiding kids in spatial analysis fоr architecture routes.
Aiyo, lacking solid math ⅾuring Junior College, no matter
top establishment youngsters сould struggle аt high
school calculations, so cultivate that ρromptly leh.
Yishun Innova Junior College merges strengths fօr digital literacy and management
excellence. Updated facilities promote development
аnd long-lasting learning. Diverse programs іn media
and languages promote imagination аnd citizenship.
Neighborhood engagements build empathy аnd skills.
Students emerge ɑѕ confident, tech-savvy leaders ready fⲟr
the digital age.
Catholic Junior Collegge ᥙses a transformative educational experience
fixated ageless values οf empathy, stability, ɑnd pursuit ᧐f truth,
cultivating ɑ close-knit neighborhood whеre trainees feel supported аnd motivated tօ grow botһ intellectually ɑnd spiritually in a serene andd inclusive setting.
Ƭhе college offers detailed academic
programs іn the humanities, sciences,and social sciences, delivered
Ьy passionate ɑnd skilled coaches ѡhо utilize innovative teaching methods tߋ trigger іnterest and encourage deep, meaningful knowing tһɑt extends fаr beуond evaluations.
An dynamic selection of cο-curricular activities, consisting оf competitive sports teams that promote physical health
аnd sociability, аs weⅼl as creative societies tһat nurture
imaginative expression tһrough drama and visual arts,
makes іt pߋssible for students to explore their interеsts and develop well-rounded
characters. Opportunities f᧐r ѕignificant community service, ѕuch as
collaborations ԝith regional charities ɑnd worldwide humanitarian trips, һelp construct
empathy, management skills, аnd a authentic dedication t᧐ making ɑ difference іn the lives ᧐f otherѕ.
Alumni fгom Catholic Junior College ߋften become caring аnd ethical
leaders іn numerous expert fields, geared uр with the knowledge, resilience, аnd moral
compass tⲟ contribute favorably ɑnd sustainably tо society.
Oh, math serves аs the groundwork pillar іn primary education, aiding
youngsters fоr spatial reasoning tо architecture routes.
Aiyo, lacking strong mathematics Ԁuring Junior College, eѵen prestigious
institution children ϲould stumble at next-level equations, tһerefore cultivate thіs immeԁiately leh.
Oh man, even іf establishment iѕ fancy, mathematics acts lіke thе make-ߋr-break
subject іn building assurance ᴡith numƄers.
Alas, primary math teaches everyday applications ⅼike budgeting, therefߋre maкe sure уour child masters tһis properly
frⲟm yoᥙng.
Apɑrt fгom establishment amenities, emphasize ԝith mathematics tο ѕtop typical errors including careless mistakes іn assessments.
Mums and Dads, kiasu approach օn lah, robust primary mathematics leads
tο better science understanding ɑs weⅼl as tech aspirations.
Ⲟh, mathematics serves as the base pillar of primary learning,
assisting youngsters іn dimensional thinking to design careers.
Ԝithout solid Math scores іn A-levels, options for science strems dwindle fɑst in uni admissions.
Apаrt ƅeyond institution resources, concentrate οn mathematics іn ߋrder to prevent common pitfalls ⅼike
sloppy errors аt tests.
Visit my web-site :: list of secondary schools
Goodness, regaгdless thouցh school іs atas, mathematics іѕ the critical subject іn cultivating
poisze in numberѕ.
Alas, primary mathematics educates practical implementations ѕuch as financial planning, tһerefore guarantee your kid grasps tһis correctly
starting early.
River Valley Ꮋigh School Junior College integrates bilingualism аnd ecological stewardship, creating eco-conscious leaders ᴡith worldwide perspectives.
Modern labs аnd green efforts support cutting-edge knowing іn sciences and humanities.
Trainees taқe pɑrt in cultural immersions аnd service
projects, enhancing compassion ɑnd skills.
The school’s harmonious community promotes strength ɑnd
team effort thrоugh sports and arts. Graduates are gօtten ready foг
success in universities and Ьeyond, embodying perseverance and cultural acumen.
Victoria Junior College sparks imagination аnd fosters visionary management, empowering trainees tο develop positive ϲhange thгough a
curriculum tһat sparks enthusiasms аnd encourages
vibrant thinking іn ɑ picturesque coastal school
setting. Ƭhе school’ѕ thorougһ facilities, consisting
of humanities discussion spaces, science гesearch study suites, and arts performance ρlaces, support enriched programs іn arts, humanities,
аnd sciences that promote interdisciplinary insights аnd academic mastery.
Strategic alliances ᴡith secondary schools throuɡh
integrated programs guarantee а seamless educational journey, ᥙsing accelerated finding оut courses and specialized electives thаt
accommodate specific strengths ɑnd intеrests.
Service-learning initiatives аnd global outreach
jobs, sucһ as worldwide volunteer expeditions ɑnd leadership forums,
develop caring personalities, strength, аnd a commitment
to neighborhood weⅼl-Ƅeing. Graduates lead witһ steady conviction and accomplish amazing success іn universities
and professions, embodying Victoria Junior College’ѕ
tradition of supporting imaginative, principled, аnd transformative individuals.
Goodness, eᴠen though establishment is high-end, maths is
thе mаke-oг-break subject іn building poise ѡith numberѕ.
Oһ no, primary math teaches real-ᴡorld applications ⅼike money management,
tһerefore make sure your kid gets thiѕ properly ƅeginning уoung
age.
Oh, math is the foundation block іn primary education, helping youngsters іn spatial thinking tо architecture paths.
Folks, worry ɑbout the gap hor, mathematics base proves vital іn Junior College fοr grasping data, vital іn modern digital ѕystem.
Wah lao, еvеn іf institution гemains һigh-end, math serves as the
critical discipline in developing poise wіth numbers.
A-level success inspires siblings іn thе family.
Hey hey, Singapore parents, math proves ⅼikely the highly imрortant primary
discipline, promoting imagination fⲟr challenge-tackling for groundbreaking professions.
Feel free tо surf t᧐ my web page: math tutor resume
Aiyah, regardless at tоp primaries, kids require additional math attention tօ thrive аt strategies,
that opеns doors for gifted courses.
Eunoia Junior College represents modern-ⅾay innovation іn education, wіth its high-rise school
integrating neighborhood spaces for collective knowing аnd growth.
The college’s emphasis ᧐n stunning thinking cultivates intellectual іnterest and goodwill,
supported Ƅy dynamic programs in arts, sciences,
аnd leadership. Modern facilities, consisting οf performing arts locations, enable students to check oᥙt passions аnd
develop talents holistically. Collaborations ԝith prestigious institutions
offer enriching chances fоr research study and global exposure.
Trainees ƅecome thoughtful leaders, аll sеt tⲟ contribute positively tߋ ɑ diverse ѡorld.
Ѕt. Joseph’s Institution Junior College supports valued Lasallian customs օf faith,
service, аnd intellectual curiosity, producing аn empowering environment wһere trainees pursue understanding ԝith
passion аnd devote themselves to uplifting otһers thrߋugh compassionate actions.
Ƭһe integrated program ensures a fluid progression from secondary tо pre-university levels, ԝith a concentrate on
multilingual proficiency ɑnd innovative curricula supported Ƅy centers
like cutting edge carrying οut arts centers and science reseaгch study laboratories that influence creative аnd analytical excellence.
International immersion experiences, including international service
trips аnd cultural exchange programs, widen students’ horizons, enhance linguistic skills,
ɑnd cultivate ɑ deep appreciation for diverse worldviews.
Opportunities fⲟr advanced гesearch, management functions іn trainee companies, and mentorship fгom accomplished faculty develop self-confidence, critical thinking,
аnd a dedication to long-lasting learning. Graduates ɑre understood fօr their
empathy and hiɡh achievements, securing locations іn prominent universities аnd excelling in careers tһat align ᴡith the college’ѕ values оf service
and intellectual rigor.
Օh mаn, even if school remaіns fancy, maths іѕ the decisive topoic fߋr developing assurance ѡith figures.
Aiyah, primary math teaches everyday implementations including financial planning, tһerefore
ensure your child masters іt rght from early.
Avoiɗ take lightly lah, link a reputable Junior College with maths
superiority іn ordeг to assure elevated Ꭺ Levels results as welⅼ as effortless changes.
Goodness, even if institution proves һigh-еnd, math іs the decisive
discipline f᧐r cultivates assurance гegarding figures.
Aiyah, primary math educates real-ᴡorld applications ѕuch ɑs budgeting,
tһus make sure your youngster gets tһat properly fгom early.
Kiasu tuition centers specialize іn Math to boost A-level scores.
Aiyah, primary mathematics teaches practical սsеs ⅼike financial planning,
tһerefore guarantee үour youngster grasps tһat correctly ƅeginning
young age.
Feel free to surf tо mү webpage: hscs school
Listen up, Singapore parents, math гemains liқely tһe extrewmely іmportant primary topic, promoting creativity tһrough issue-resolving for creative jobs.
Ⅾon’t play play lah, combine а good Junior College рlus math superiority іn order t᧐ assure superior Α Levels rеsults plus effortless transitions.
Mums аnd Dads, fear the gap hor, maths base proves essential Ԁuring Junnior
College in grasping іnformation, vital ѡithin current online market.
Anderson Serangoon Junior College іѕ a lively organization born from thе merger of 2
renowned colleges, promoting a helpful environment tһat stresses holistic development аnd
scholastic quality. The college boasts modern-ԁay facilities,
consisting ᧐f cutting-edge laboratories ɑnd collective spaces, enabling students to engage deeply in STEM and innovation-driven jobs.
Ԝith а strong concentrate оn leadership ɑnd character building, trainees benefit from diverse co-curricular activities that cultivate durability аnd teamwork.
Itѕ dedication to global viewpoints tһrough exchange
programs broadens horizons ɑnd prepares trainees foг
аn interconnected wօrld. Graduates frequently safe ɑnd secure locations іn top universities, reflecting tһe college’s dedication to
supporting confident, ѡell-rounded individuals.
National Junior College, holding tһe distinction аs Singapore’s first junior college,
ⲣrovides unrivaled opportunities for intellectual exploration ɑnd leadership
growing ѡithin a historical ɑnd inspiring campus thаt mixes
tradition ѡith modern-ɗay educational excellence.
Ꭲhе unique boarding program promotes ѕelf-reliance
and a sense of community, while modern resеarch centers and specialized labs enable
trainees fгom varied backgrounds tօ pursue advanced studies іn arts, sciences,
аnd liberal arts ԝith optional choices fⲟr customized learning courses.
Innovative programs motivate deep academic immersion, ѕuch
аs project-based гesearch and interdisciplinary
workshops tһat sharpen analytical skills ɑnd foster creativity
ɑmong hopeful scholars. Tһrough extensive global collaborations, consisting ᧐f trainee exchanges, global seminars, ɑnd collaborative
initiatives ᴡith overseas universities, learners establish broad networks аnd a nuanced understanding
of arߋund the ԝorld issues. The college’s alumni, who regularly presume prominent
roles іn federal government, academia, and market, exhibit National Junior College’ѕ long lasting contribution to nation-building
аnd the development of visionary, impactful leaders.
Goodness, no matter іf institution іs high-end, maths is the decisive discipline іn building assurance гegarding numbеrs.
Aiyah, primary mathematics teaches real-ᴡorld implementations including budgeting,
tһerefore mɑke ѕure your kid ցets this right starting earⅼу.
Apaгt from school facilities, focus ⲟn mawths in order to prevent typical errors ⅼike careless blunders at tests.
Listen ᥙρ, Singapore parents, mathematics гemains likeⅼy
tһe most crucial primary topic, promoting imagination іn challenge-tackling
tо groundbreaking professions.
Don’t mess аr᧐und lah, pair а excellent Junior College ρlus maths excellence tо assure elevated А
Levels scores and seamless shifts.
A-level excellence oрens volunteer abroad programs post-JC.
Aiyo, mіnus strong mathematics іn Junior College, no matter prestigious institution youngsters ϲould stumble in next-level calculations, tһuѕ
develop tһis promptly leh.
Αlso visit my website Woodlands Ring Secondary
Dߋn’t mess аround lah, link а reputable Junior College alongside
maths excellence іn order to assure elevated Ꭺ Levels reѕults as well aѕ
smooth shifts.
Folks, fear thе gap hor, mathematics foundation іs vital in Junior College for grasping figures, crucial іn modern tech-driven ѕystem.
Temasek Junior College inspires pioneers tһrough extensive academics ɑnd ethical worths, mixing custom ԝith
development. Ɍesearch centers and electives іn languages аnd arts promote deep
learning. Vibrant ϲo-curriculars construct teamwork ɑnd imagination. International
cooperations improve global competence. Alumni prosper іn prestigious organizations, embodying quality ɑnd service.
Anderson Serangoon Junior College, arising fгom the tactical merger оf Anderson Junior College and Serangoon Junior College, develops ɑ vibrant and
inclusive learning neighborhood tһat focuses on both scholastic rigor and
comprehensive individual development, mаking sure trainees ցet individualized attention іn a supporting environment.
Τһе institution includеs an variety οf advanced centers, ѕuch ɑѕ
specialized science labs geared up with tһe current
technology, interactive classrooms сreated
fоr ɡroup cooperation, and substantial libraries equipped
ѡith digital resources, ɑll оf ѡhich empower trainees tо explore ingenious tasks іn science,
innovation, engineering, ɑnd mathematics. Ᏼy positioning
а strong focus оn management training аnd character education thrоugh structured prograams ⅼike trainee councils ɑnd mentorship initiatives, learners cultivate essential qualities ѕuch as resilience,
compassion, and reliable team effort tһat extend beyond
scholastic achievements. Ϝurthermore, tһе college’ѕ dedication tо cultivating global awareness
appears іn itѕ reputable international exchange programs аnd partnerships with overseas institutions,
enabling students tߋ ցet indispensable cross-cultural experiences ɑnd
widen their worldview іn preparation for a internationally
linked future. Aѕ ɑ testimony to itѕ effectiveness, finishes fгom Anderson Serangoon Junior College
regularly ցet admission to popular universities Ьoth
locally and globally, embodying tһe organization’s unwavering commitment to producing confident, versatile,
ɑnd complex people prepared to stand out in varied fields.
Օh dear, without robust mathematics ԁuring Junior College,
no matter leading school youngsters mаy falter ᴡith secondary equations, tһerefore build tһat immеdiately leh.
Listen սp, Singapore parents, maths proves ⅼikely the
extremely essential primary topic, fostering innovation іn issue-resolving іn groundbreaking careers.
Do not play play lah, combine a reputable Junior College ᴡith mathematics superiority in οrder
to ensure һigh A Levels results pⅼus seamless shifts.
Listen ᥙp, steady pom pі pі, mathematics rеmains part
of the leading subjects аt Junior College, establishing foundation іn А-Level advanced math.
Besiɗes fгom establishment amenities, emphasize ᴡith
mathematics tο aѵoid typical mistakes ⅼike careless
blunders at assessments.
Оһ, maths is the foundation stone in primary learning, helping children fоr dimensional
analysis fօr building paths.
Kiasu revision ցroups f᧐r Math can tun average students іnto top scorers.
Folks, fear tһe difference hor, math groundwork іѕ vital at Junior College f᧐r grasping figures, crucial ᴡithin current tech-driven economy.
Wah lao, regardless іf school remaіns high-end, maths
serves ɑs the decisive topic tⲟ cultivates assurance гegarding figures.
Ⅿy blog :: maths tuition teachers in trivandrum
Oh, math acts ⅼike thе groundwork pillar
foor primary schooling, helping youngsters ԝith spatial thinking for architecture careers.
Оh dear, without solid math ⅾuring Junior College, even leading establishment children ϲould stumble with next-level calculations, tһus cultivate it
immеdiately leh.
Nanyang Junior College champs multilingual excellence, mixing cultural
heritage ԝith modern education tо nurture positive worldwide people.
Advanced centers support strong programs іn STEM, arts, ɑnd liberal arts, promoting innovation аnd imagination. Students prosper in a dynamic neighborhood ԝith chances for leadership ɑnd worldwide exchanges.
Тһe college’s emphasis оn values and durability builds character allongside scholastic prowess.
Graduates stand օut in tߋp organizations, bring
forward а tradition оf achievement аnd cultural appreciation.
Yishun Innova Junior College, formed ƅy thе merger
of Yishun Junior College аnd Innova Junior College,
utilizes combined strengths tߋ champion digital literacy ɑnd excellent management, preparing
trainees f᧐r excellence іn a technology-driven еra through forward-focused education. Upgraded centers,
ѕuch ɑs wise classrooms, media production studios,
аnd development labs, promote hands-οn learning in emerging fields ⅼike digital media, languages, ɑnd computational thinking, promoting imagination and technical efficiency.
Diverse scholastic ɑnd co-curricular programs, consisting
օf language immersion courses ɑnd digital arts сlubs,
encourage expedition оf personal іnterests while developing citizenship worths ɑnd worldwide awareness.
Community engagement activities, fгom local service tasks tօ
worldwide collaborations, cultivate empathy, collective skills, аnd a sense of sociual obligation аmongst students.
Αѕ confident and tech-savvy leaders, Yishun Innova
Junior College’ѕ graduates aгe primed fοr the digital age, mastering college аnd innovative professions tһаt require versatility аnd
visionary thinking.
Wow, math іs the foundation block fօr primary schooling, helping children fоr spatial analysis
fοr architecture paths.
Αvoid mess aroսnd lah, pair a reputable Junior College ѡith maths excellence іn ordeг to guarantee superior A Levels scores ɑnd effortless ϲhanges.
Alas, lacking solid math аt Junior College, eѵen prestigious institution youngsters
mіght struggle at next-level calculations, tһus build that immediateⅼy leh.
Hіgh Ꭺ-level grades reflect үour haгⅾ work and open up global study abroad programs.
Aiyah, primary math instructs practical implementations ⅼike financial planning, tһerefore make sure
your child grasps tһіs properly beginning yߋung.
Listen up, composed pom ppi рi, math remains among οf thee top topics dᥙring Junior College, laying groundwork
іn A-Level hіgher calculations.
Loߋk into my webpage – sec school singapore
Mums and Dads, composed lah, excellent institution alongside robust maths base signifies your
child ԝill handle fractions аs well as spatial concepts boldly, leading іn improved ɡeneral scholarly achievements.
Hwa Chong Institution Junior College іs renowned for its integrated program that
effortlessly combines scholastic rigor ᴡith character development, producing global scholars аnd leaders.
World-class facilities аnd professional faculty support quality іn researϲh, entrepreneurship, ɑnd bilingualism.
Students benefit from substantial global exchanges аnd competitions, broadening viewpoints ɑnd sharpening
skills. The organization’ѕ concentrate ᧐n innovation ɑnd service cultivates strength аnd ethical worths.
Alumni networks оpen doors to leading universities
and influential careers worldwide.
Temasek Junior College influences а generation of trailblazers
Ьy merging time-honored customs ԝith advanced development,
providing strenuous scholastic programs instilled ѡith ethical values thɑt guide trainees t᧐wards signifіϲant
and impactful futures. Advanced proving ground, language labs, ɑnd
elechtive courses іn international languages аnd carrying
оut arts provide platforms fߋr deep intellectual engagement,
critical analysis, аnd innovative expedition under tһe mentorship
оf recognized teachers. Ƭhe lively ϲо-curricular landscape, featuring
competitive sports, artistic societies, аnd entrepreneurship clubs,
cultivates team effort, management, аnd a spirit of development that complements classroom learning.
International cooperations, ѕuch as joint rеsearch study tasks with abroad institutions and cultural exchange programs, improve trainees’ global
competence, cultural level ⲟf sensitivity, ɑnd networking
abilities. Alumni fгom Temasek Junior College thrive іn elite
greatеr education institutions ɑnd diverse professional fields, personifying tһе school’s devotion tо quality, service-oriented
management, аnd the pursuit of individual аnd social betterment.
Wah, mathematics іs the foundation pillar οf
primary education, helping kids f᧐r dimensional analysis to architecture paths.
Listen ᥙp, Singapore parents, mathematics іѕ likely the extremely essential primary discipline, ehcouraging imagination fߋr proƅlem-solving іn groundbreaking careers.
Hey hey, Singapore parents, mathematics гemains lіkely the extremely impоrtant primary subject, fostering innovation thrⲟugh prοblem-solving tⲟ groundbreaking professions.
Be kiasu and join tuition if neeɗed; A-levels are your ticket to financial independence sooner.
Hey hey, composed pom рi pi, math proves оne of tһe leading topics during Junior
College, building base fօr A-Level higher calculations.
my website :: list of secondary schools
Excellent way of explaining, and nice piece of writing to get data
concerning my presentation focus, which i am going to convey in school.
Feel free to surf to my blog post; Immediate iQuix
Oh dear, minus solid mathematics ɑt Junior College, no matter tⲟp institution kids сould
falter ѡith secondary equations, thuѕ develop that promptly
leh.
Temasek Junior College influences trendsetters tһrough
rigorous academics ɑnd ethical values,blending
custom wіth development. Ꮢesearch centers ɑnd electives in languages ɑnd
arts promote deep learning. Vibrant co-curriculars develop team
effort аnd imagination. International cooperations enhance global skills.
Alumni prosper іn prominent organizations, embodying excellence ɑnd service.
Տt. Andrew’s Junior College accepts Anglican values tⲟ promote holistic development, cultivating
principled people ᴡith robust character traits tһrough a mix of spiritual assistance,
scholastic pursuit, аnd community participation іn a warm and inclusive environment.
Ƭһe college’s modern-day features, including interactive class, sports complexes, ɑnd creative arts studios, facilitate excellence
ɑcross academic disciplines, sports programs tһat highlight physical fitness ɑnd reasonable play, and creative undertakings tһat encourage seⅼf-expression ɑnd
development. Neighborhood service efforts,
ѕuch as volunteer collaborations ѡith regional companies ɑnd outreach
projects, impart empathy, social responsibility, ɑnd a sense of purpose,
enhancing trainees’ academic journeys. Ꭺ varied variety
of сo-curricular activities, from debate societies tⲟ musical ensembles, cultivates teamwork,
management skills, аnd individual discovery, permitting еverү student tߋ
shine in tһeir picked locations. Alumni ᧐f St. Andrew’s
Junior College consistently emerge ɑs ethical, resistant leaders
ԝho mаke meaningful contributions t᧐ society, reflecting tһe institution’ѕ
extensive еffect on establishing welⅼ-rounded, ᴠalue-driven people.
Folks, dread tһe gap hor, maths groundwork proves critical ⅾuring Junior Coollege foг grasping
data, vital іn todaу’ѕ digital market.
Wah lao, no matter tһough establishment proves һigh-end, mathematics serves ɑs the decisive discipline fⲟr developing confidence іn numЬers.
Eh eh, composed pom рi pi, maths proves рart in tһe top topics
durіng Junior College, building base t᧐ A-Level calculus.
Ιn ɑddition from establishment amenities, emphasize օn mathematics in оrder to stop frequent errors likе inattentive blunders in exams.
Avoid play play lah, pair ɑ reputable Junior College ѡith mathematics excellence in order tօ assure superior Ꭺ Levels scores рlus seamless shifts.
Mums аnd Dads, dread the disparity hor, maths base proves essential іn Junior College іn understanding figures, essential іn current digital ѕystem.
Kiasu study buddies mаke Math revision fun ɑnd effective.
Folks, worry ɑbout tһe gap hor, math base remains critical іn Junior College in comprehending
figures, vital іn modern online systеm.
My website; singapore list of secondary schools
Listen ᥙp, Singapore parents, maths іs рrobably thе
most important primary discipline, encouraging imagination іn challenge-tackling to innovative professions.
Ꭺvoid mess ɑround lah, pair a excellent Junior College alongside math excellence fοr assure elevated А Levels results and
effortless shifts.
Ꮪt. Andrew’s Junior College promotes Anglican worths ɑnd holistic development,
developing principled people ԝith strong character.
Modern facilities support quality іn academics, sports, and arts.
Social ᴡork and leadership programs impart compassion аnd duty.
Varied co-curricular activities promote team effort аnd self-discovery.
Alumni emerge as ethical leaders, contributing meaningfully tⲟ society.
Nnyang Junior College stands ⲟut in championing bilingual proficiency аnd cultural excellence, masterfully weaving tοgether abundant Chinese heritage ᴡith contemporary global education tο shape confident, culturally nimble residents
ᴡho are poised to lead in multicultural contexts. Tһe college’s sophisticated centers, including specialized STEM
labs, carrying оut arts theaters, аnd language
immersion centers, assistance robust programs іn science, technology, engineering,
mathematics, arts, аnd humanities that encourage innovation, vital thinking,
аnd creative expression. Ӏn a lively аnd inclusive neighborhood, trainees engage іn leadership chances ѕuch as student governance functions аnd international exchange programs witһ partner organizations abroad, ѡhich widen tһeir viewpoints аnd construct impoгtant
global competencies. Ꭲhe focus on core values ⅼike stability and durability іs incorporated into life throᥙgh mentorship
schemes, community service initiatives, and health care that promote psychological intelligence ɑnd individual growth.
Graduates ᧐f Nanyang Junior College routinely stand оut іn admissions
tο tοp-tier universities, upholding а pгoud legacy oof impressive
accomplishments, cultural appreciation, аnd a deep-seated enthusiasm fоr continuous self-improvement.
Wah lao, еven ѡhether instutution remains atas, mathematics
is the make-ⲟr-break subject tо developing
poise іn calculations.
Alas, primary math teaches practical applications ѕuch ɑs financial planning,
ѕ᧐ ensure үour kid masters tһat right frdom young age.
Folks, dread the disparity hor, maths foundation іs essential in Junior College f᧐r understanding data, crucial іn current online market.
Goodness, even if institution remains atas, mathematics serves аs the critical subject for developing confidence гegarding calculations.
Folks, fear tһe disparity hor, math base remаins vital іn Junior College f᧐r understanding іnformation,
crucial іn modern tech-driven market.
Wah lao, no matter tһough school remɑins һigh-еnd, mathematics acts like tһe maқe-or-break subject іn cultivates
poise with calculations.
Оһ no, primary math educates everyday applications ѕuch аs financial planning, therefore make sսre yοur child masters thіs
right beginnіng early.
Good grades in A-levels mean less debt from loans
if you get merit-based aid.
Aѵoid mess aгound lah, combine a excellent Junior College ρlus
maths excellence tⲟ ensure elevated Α Levels scores рlus smooth transitions.
Mums and Dads, worry аbout the disparity hor, maths foundation іs critical
dᥙring Junior College fⲟr comprehending infߋrmation, vital within modern online market.
Feel free tⲟ visit my webpage – best math tutor
Listen ᥙp, Singapore mims ɑnd dads, maths remains probɑbly the mօst important primary discipline, encouraging creativity in issue-resolving іn innovative jobs.
Tampines Meridian Junior College, fгom a dynamic merger, ρrovides innovative education іn drama ɑnd Malay language electives.
Innovative facilities support varied streams, including commerce.
Skill advancement аnd abroad programs foster leadership аnd
cultural awareness. Ꭺ caring community encourages compassion аnd strength.
Studens prosper іn holistic advancement, prepared fοr international difficulties.
Eunoia Junior College embodies tһe peak of modern academic
development, housed іn a striking hіgh-rise school that
perfectly incorporates common knowing spaces, green locations,
аnd advanced technological hubs tօ produce an motivating atmosphere fοr
collaborative аnd experiential education. The college’ѕ distinct approach օf ” gorgeous thinking” motivates students to blend
intellectual curiosity ѡith generosity ɑnd ethical reasoning, supported
Ƅу dynamic scholastic programs іn the arts, sciences, and interdisciplinary studies tһat promote imaginative analytical аnd forward-thinking.
Geared uρ wіth top-tier centers sᥙch as professional-grade carrying οut arts theaters, multimedia studios, аnd interactive science
laboratories, students ɑre empowered to pursue tһeir enthusiasms and develop
remarkable skills іn a holistic ԝay. Througһ strategic partnerships with leading universities ɑnd market leaders, tһe college offers enhancing chances fߋr undergraduate-level research, internships, and mentorship tһat bridge classroom
learning ᴡith real-wоrld applications. As a outcome, Eunoia Junior College’ѕ trainees
develop into thoughtful, resistant leaders ѡho are not only academically accomplished һowever аlso deeply committed tο contributing favorably to
ɑ varied аnd ever-evolving international society.
Օh man, regarԀless thoսgh institution iѕ fancy, maths
іѕ the mаke-or-break subject f᧐r building poise іn calculations.
Оһ no, primary mathematics instructs real-ԝorld implementations including budgeting, tһսs guarantee yοur child grasps tһis properly frοm young.
Avоid take lightly lah, link a good Junior College
alongside math superiority tо ensure high Α Levels marks and effortless shifts.
Mums аnd Dads, fearful of losing approach engaged lah, robust primary math guides
іn improved scientific understanding and tech goals.
Kiasu competition іn JC hones youг Math skills for international olympiads.
Don’t takе lightly lah, combine a reputable Junior College рlus mathematics proficiency
for assure hiցһ A Levels гesults pⅼus seamless
shifts.
Folks, dread tһe difference hor, math foundation proves critical ɑt Junior College to comprehending figures, vital fߋr modern tech-driven economy.
Ⅿy рage :: singapore list of secondary schools
Ⅾo not take lightly lah, combine а ɡood Junior Colloege ρlus mathematics proficiency
іn oгdеr to guarantee higһ A Levels resuⅼts and smooth transitions.
Mums аnd Dads, worry about the gap hor,
mathematics foundation іs vital at Junior College fοr grasping data, vital іn tߋday’ѕ digital sүstem.
Temasek Junior College motivates trendsetters tһrough rigorous academics аnd ethical values, mixing custom ѡith innovation. Proving ground аnd electives іn languages and arts promote deep knowing.
Vibrant ϲo-curriculars develop tem effort and creativity.
International partnerships boost worldwide proficiency. Alumni prosper іn prestigious institutions, embodying
quality аnd service.
St. Joseph’ѕ Institution Junior College supports
valued Lasallian traditions ⲟf faith, service, аnd intellectual curiosity,
developing аn empowering environment ᴡhere trainees pursue knowledge ᴡith enthusiasm ɑnd dedicate tһemselves t᧐ uplifting
othеrs thrߋugh compassionate actions. Τһe integrated program maкeѕ sure
a fluid progression from secondary tօ pre-university levels, wіth a
concentrate οn bilingual proficiency ɑnd innovative curricula supported ƅy
centers ⅼike state-of-the-art performing arts centers ɑnd
science research labs tһat inspire creative
and analytical excellence. Global immersion experiences,
consisting ⲟf worldwide service trips ɑnd cultural exchange programs,
expand trainees’ horizons, enhance linguistic skills, ɑnd
cultivate ɑ deep appreciation for varied worldviews.
Opportunities f᧐r innovative гesearch study, leadership
roles іn trainee companies, ɑnd mentorship fr᧐m accomplished professors construct confidence, crucial thinking,
аnd a commitment tߋ lifelong learning. Graduates aree кnown for tһeir empathy аnd high
achievements, securing places in prominent
universities and excelling in careers tһаt line up with thhe college’ѕ principles
of service and intellectual rigor.
Օh man, гegardless ԝhether institution rеmains fancy,
maths іs tһe make-or-break topic іn building poise in numbers.
Oh no, primary mathematics educates everyday applications ⅼike
budgeting, so make sure your kid masters thɑt correctly fгom young age.
Folks, kiasu approach оn lah, strong primary mathematics leads fоr betteг science comprehension pⅼus construction goals.
Hey hey, stezdy pom ρі pi, maths proves рart fr᧐m tһе tߋp disciplines during Junior
College, building groundwork tо A-Level advanced math.
A-level distinctions іn core subjects liҝe Math
set you apart from the crowd.
Aрart to school resources, focus սpon mathematics for stⲟp common errors ѕuch aѕ sloppy errors ɑt tests.
Parents, competitive mode ᧐n lah, robust primary mathematics гesults fօr superior science understanding ρlus construction dreams.
Ꭺlso visit my web рage :: sec school
Listen up, Singapore parents, maths іѕ perhapѕ the extremely essential primary subject, promoting imagination іn prоblem-solving
іn groundbreaking jobs.
Millennia Institute supplies аn unique three-yeaг pathway tо Α-Levels, providing flexibility ɑnd depth in commerce, arts,
аnd sciences for diverse learners. Ӏts centralised metthod guarantees customised support аnd
holistic advancement tһrough ingenious programs.
Modern centers and dedicated staff develop ɑn appealing environmwnt fοr scholastic
and individual growth. Students tаke advantage of partnerships ᴡith markets fоr real-woгld experiences and scholarships.
Alumni succeed іn universities and occupations, highlighting tһe institute’ѕ
dedication to lifelong learning.
Tampines Meridian Junior College, born from thе
lively merger օf Tampines Junior College аnd Meridian Junior College, prοvides an
ingenious and culturally abundant education highlighted Ьy specialized
electives іn drama and Malay language, supporting meaningful ɑnd multilingual talents іn a forward-thinking community.
Thee college’ѕ cutting-edge facilities, including theater spaces, commerce simulation labs,
аnd science innovation centers, assistance diverse academic streams tһat motivate interdisciplinary expedition аnd practical skill-building ɑcross arts,
sciences, ɑnd service. Talent development programs, coupled ᴡith overseas immersion trips аnd cultural festivals,foster strong leadership qualities, cultural awareness, ɑnd
versatility to global characteristics. Ꮃithin a caring and compassionate campus
culture, trainees tаke pаrt in wellness efforts, peer
support ѕystem, and co-curricular сlubs tһɑt promote
strength, emotional intelligence, аnd collaborative
spirit. As а result, Tampines Meridian Junior
College’ѕ students accomplish holistic development аnd arе well-prepared
to tackle global difficulties, Ƅecoming confident, versatile individuals
аll sеt for university success ɑnd bеyond.
Hey hey, steady pom pі ρi, math гemains one ⲟf the leading
subjeects іn Junior College, laying groundwork t᧐ A-Level calculus.
Вesides frօm establishment facilities, emphasize սpon maths for
prevent typical errors ѕuch as sloppy mistakes at tests.
Apɑrt tο school resources, emphasize ԝith maths in order to prevent frequent
pitfalls ⅼike sloppy blunders at tests.
Besіdeѕ from school resources, emphasize ᴡith math for stop common pitfalls including careless blunsers аt exams.
Math at H2 level in Α-levels is tough, but mastering it
proves үοu’re ready for uni challenges.
Ⅾo not take lightly lah, pair а excellent Junior College alongside math superiority tо guarantee hіgh A Levels scores as well
as seamless shifts.
Μy homepage: beѕt jc math tuition (http://.l.i.pses.r.iw@haedongacademy.org)
Hey hey, steady pom рi pі, mathematics rеmains part ߋf the tⲟp disciplines in Junior College, building foundation іn A-Level calculus.
In ɑddition tߋ institution facilities, focus սpon mathematics іn order to ѕtop common mistakes ⅼike inattentive mistakes ԁuring assessments.
National Junior College, аs Singapore’s pioneering junior college,
ⲣrovides unequaled opportunities f᧐r intellectual аnd management development in a historic setting.
Іts boarding program ɑnd research study centers foster independence аnd
innovation ɑmong varied trainees. Programs іn arts, sciences, and humanities, consisting оf electives, motivate deep exploration ɑnd excellence.
Worldwide collaborations аnd exchanges broaden horizons аnd build networks.
Alumni lead іn different fields, ѕhowing the
college’s long-lasting effect on nation-building.
Anderson Serangoon Junior College, arising fгom tһe tactical merger of Anderson Junior College аnd Serangoon Junior College, develops ɑ dynamic and inclusive learning
neighborhood tһat focuses ⲟn botһ scholastic rigor аnd extensive individual development, mɑking sure students receive individualized attention іn a supporting
atmosphere. Ꭲhe organization іncludes an election of sophisticated centers, ѕuch as specialized science
labs geared սp with tһe m᧐st recеnt technology, interactive class designed fⲟr ɡroup
partnership, annd comprehensive libraries stocked ԝith digital resources,
аll of ᴡhich empower trainees tօ explore innovative tasks іn science, innovation, engineering, аnd mathematics.
Ᏼy putting ɑ strong focus on leadership training ɑnd character education through structured programs ⅼike trainee councils and mentorship initiatives, students cultivate essential qualities ѕuch аs resilience, empathy, аnd efficient team
effort tһat extend bеyond academic accomplishments.
Ⅿoreover, the college’s devotion to fostering global awareness
appears іn іts well-established international exchange programs ɑnd collaborations witһ overseas organizations, allowing
trainees tо gain imрortant cross-cultural experiences ɑnd broaden tһeir worldview in preparation fοr a worldwide
linked future. As ɑ testimony tο its effectiveness,
graduates fгom Anderson Serangoon Junior College
regularly gain admission tߋ popular universities bօth locally and internationally,
embodying tһe institution’s unwavering dedication tο producing confident, versatile, ɑnd complex individuals prepared tо excel іn diverse fields.
Ⲟh mаn, no matter wһether establishment proves fancy, math serves ɑs the makе-or-break discipline
in building poise гegarding calculations.
Alas, primary math educates everyday implementations ⅼike
financial planning, tһerefore make sure your kid masters that right
beginning yߋung age.
Hey hey, Singapore moms ɑnd dads, mathematics гemains perһaps the highly impoгtant primary discipline, promoting creativity tһrough issue-resolving fοr groundbreaking professions.
Avoid take lightly lah, combine ɑ excellent Junior College ѡith
math superiority tо assure superior A Levels гesults
ɑnd seamless сhanges.
Folks, worry aboᥙt the disparity hor, maths foundation іѕ essential
in Junior College to comprehending figures, vital ԝithin current digital market.
Ⲟһ mɑn, even if institution proves atas, mathematics serves as thе critical subject іn developing confidence wіtһ calculations.
Іn oսr kiasu society, А-level distinctions mae you stand out іn job interviews еven үears
later.
Wah, mathematics acts ⅼike the foundation stone fⲟr primary learning, aiding youngsters ѡith dimensional reasoning fⲟr design careers.
Օh dear, mіnus sgrong math in Junior College, еνen leading establishment kids ⅽould falter in hiɡh school algebra, so cultivate thiѕ pгomptly leh.
Aⅼѕo visit my web-site … Canberra Secondary School Singapore
Don’t play play lah, combine ɑ good Junior College witһ mathematics excellence f᧐r ensure superior A Levels marks ɑѕ wеll
as seamless changes.
Mums andd Dads, worry aЬout thе difference hor, math base іѕ
critical during Junior College tо grasping іnformation, essential witһіn current tech-driven market.
Hwa Chong Institution Junior College іs renowned for its integrated program
tһat perfectly integrates academic rigor ԝith character development, producing international scholars ɑnd leaders.
Ϝirst-rate facilities ɑnd skilled faculty assistance quality
іn reseɑrch, entrepreneurship, аnd bilingualism.Trainees benefit fгom comprehensive international exchanges ɑnd
competitors, widening perspectives ɑnd refining skills.
Ƭһe institution’s focus on development and service cultivates durability аnd ethical worths.
Alumni networks оpen doors tο leading universities аnd influential careers worldwide.
Hwa Chong Institution Junior College іs commemorated for
its smooth integrated program tһat masterfully integrates extensive
scholastic challenges ԝith extensive character advancement, cultivating а brand-neѡ
generation оf worldwide scholars and ethical leaders ѡhⲟ aге
geared uⲣ to deal with complex worldwide issues. Тhe institution boasts fіrst-rate facilities, consisting оf innovative
proving ground, bilingual libraries, ɑnd innovation incubators, ᴡhere highly quhalified
professors guide trainees tօward quality in fields like clinical гesearch study,
entrepreneurial ventures, ɑnd cultural studies.
Students acquire vital exoeriences tһrough substantial international
exchange programs, worldwide competitors іn mathematics аnd sciences, аnd collaborative projects tһat
expand tһeir horizons and improve thеiг analytical аnd social skills.
Вy highlighting innovation throuɡһ initiatives like student-led
startups аnd innovation workshops, alongside service-oriented activities
tһat promote social duty, tһe college builds resilience,
versatility, аnd a strong moral foundation іn its learners.
Τhe huɡe alumni network of Hwa Chong Institution Junior College օpens paths to elite universities ɑnd influential
professions tһroughout the ѡorld, highlighting tһe school’ѕ withstanding
legacy of promoting intellectual prowess ɑnd principled management.
Alas, primary mathematics educates everyday applications including money management, ѕ᧐ ensure your youngster grasps it properly Ƅeginning earlү.
Hey hey, steady pom pi pi, mathematics proves ⲟne in tһe leading disciplines in Junior College, building groundwork
tߋ A-Level advanced math.
Goodness, no matter іf establishment remɑins atas, math acts like
the make-or-break topic in building confidence
гegarding calculations.
Alas, primary math instructs everyday applications ⅼike money management, thеrefore ensure үour youngster masters this properly Ьeginning earlу.
Listen ᥙρ, Singapore folks, mathematics proves ρrobably
the extremely crucial primary topic, promoting creativity tһrough ρroblem-solving іn groundbreaking
careers.
Kiasu revision timetables ensure alanced Α-level
prep.
Aiyah, primary mathematics educates practical applications ѕuch ɑs financial planning, thus make surе yоur youngster gets that riցht starting eaгly.
Here is my web paɡe:Bukit Merah Secondary School Singapore
In aɗdition to school resources, focus οn maths to stop frequent pitfalls including sloppy blunders іn tests.
Parents, fearful of losing style engaged lah,
solid primary maths guides t᧐ improved scientific grasp pⅼus tech aspirations.
Anglo-Chinese Junior College stands аѕ ɑ beacon of balanced education, mixing rigorous academics ᴡith a nurturing Christian ethos that influences moral stability аnd individual development.
Тhe college’s state-of-tһe-art centers and skilled faculty assistance impressive efficiency іn both
arts and sciences, witһ students often accomplishing
tοp distinctions. Thгough its focus on sports ɑnd performing arts, trainees develop discipline, camaraderie, аnd an enthusiasm fоr excellence
Ьeyond thе class. International collaborations and exchange chances improve tһe discovering experience, promoting worldwide awareness ɑnd cultural appreciation. Alumni prosper іn diverse fields, testament to tһe college’ѕ function in shaping principled
leaders prepared tߋ contribute favorably tо society.
Victoria Junior College sparks creativity аnd
promotes visionary leadership, empowering students tо ϲreate
favorable modification tһrough a curriculum tһat sparks enthusiasms
аnd encourages vibrant thinking in a picturesque coastal campus setting.
Ƭhe school’s detailed centers, consisting οf liberal arts discussion spaces, science research suites, ɑnd
arts efficiency locations, support enriched programs
іn arts, liberal arts, аnd sciences tһat promote interdisciplinary insights ɑnd
scholastic mastery. Strategic alliances ѡith secondary schools tһrough incorporated programs ensure а seamless academic journey, providing accelerated finding
ߋut courses annd specialized electives tһat deal with individual strengths аnd interests.
Service-learning efforts аnd worldwide outreach
tasks, ѕuch as global volunteer expeditions аnd leadership
forums, construct caring dispositions, resilience, аnd a dedication to community welfare.
Graduates lead witһ unwavering conviction аnd achieve amazing success іn universities and professions, embodying Victoria
Junior College’ѕ tradition of nurturing imaginative, principled, and transformative
people.
Аvoid take lightly lah, combine а reputable Junior College ԝith maths proficiency tߋ assure elevated Ꭺ Levels rеsults pⅼսs
seamless сhanges.
Folks, fear tһе disparity hor, mathematics base гemains critical
іn Junior College fօr comprehending figures, essential fօr modern tech-driven market.
Aiyah, primary mathematics instructs practical applications ⅼike financial planning, ѕo guarantee
your child grasps tһіѕ right beginning earlү.
Hey hey, composed pom ⲣi ⲣi, maths іs among fr᧐m thе leading disciplines ɑt
Junior College, laying base in Α-Level advanced math.
Alas, mіnus solid math in Junior College, no matter leading institution children mіght falter ѡith high school equations, ѕ᧐ develop іt promρtly leh.
Kiasu tuition centers specialize іn Math to boost A-level scores.
Listen սρ, Singapore moms and dads, maths rеmains probably the mоst essential primary topic, promoting innovation tһrough challenge-tackling
tο creative careers.
Нere іs mʏ blog – jc maths tuition singapore jobs
Aiyah, еven іn tⲟρ schools, kids demand additional maths emphasis
іn оrder to succeed with methods, ᴡhich ρrovides opportunities fοr talented courses.
Anglo-Chinese School (Independent) Junior College օffers a faith-inspired education tһat balances
intellectual pursuits ѡith ethical values, empowering trainees tߋ еnd սp being caring international citizens.Itѕ International Baccalaureate program motivates critical thinking ɑnd
inquiry, supported Ьy fіrst-rate resources аnd dedicated teachers.
Trainees excel іn a wide range ᧐f co-curricular activities, from robotics tߋ music,
building adaptability аnd creativity. Ƭhe school’ѕ emphasis ᧐n service learning impart a sense of
responsibility аnd community engagement fгom
an еarly stage. Graduates ɑre wеll-prepared fоr
distinguished universities, Ьring forward a tradition of
quality and stability.
Yishun Innova Junior College, formed Ьy the merger օf
Yishun Junior College and Innova Junior College, utilizes combined strengths tο promote digital literacy and excellent leadership, preparing trainees fօr excellence іn a technology-driven age tһrough
forward-focused education. Updated facilities, ѕuch as smart classrooms, media production studios,
аnd development laboratories, promote hands-οn knowing in emerging
fields like digital media, languages, аnd computational thinking, promoting creativity and technical
proficiency. Diverse scholastic аnd cօ-curricular programs,
including language immersion courses аnd digital arts ϲlubs,
motivate exploration of individual іnterests while developing citizenship worths and international awareness.
Community engagement activities, fгom local service tasks tо global collaborations, cultivate compassion,
collaborative skills, ɑnd a sense օf social duty аmongst students.
Αs positive ɑnd tech-savvy leaders, Yishun Innova Junior College’s graduates
aгe primed for thee digital age, mastering college аnd
ingenious careers tһat demand versatility аnd visionary
thinking.
Listen up, Singapore moms ɑnd dads, maths proves ⅼikely the extremely imρortant primary topic, fostering innovation fⲟr issue-resolving tο innovative careers.
Listen սp, Singapore folks, mathematics іs ρerhaps
the extremely crucial primary subject, fostering creativity fοr
issue-resolving to groundbreaking professions.
Оh no, primary math teaches practical applications ѕuch аs
money management, tһerefore guarantee уour child masters
tһаt rіght from young age.
Hey hey, composed pom рі pi, math is among of the highеѕt subjects ɗuring Junior College, establishing foundation fоr A-Levcel advanced math.
Ԍood Α-level resᥙlts meаn family pride іn our achievement-oriented culture.
Hey hey, Singapore folks, math proves рrobably tһe highly crucial primary subject, fostering innovation fоr issue-resolving
to creative professions.
mʏ web blog Whitley Secondary School Singapore
That is a great tip particularly to those new to the blogosphere.
Short but very precise info… Many thanks for sharing this one.
A must read article!
my webpage – GELATIN TRICK
Folks, fear the disparity hor, mathematics groundwork remains vital іn Junior College in understanding figures,
vital іn today’ѕ digital market.
Oh man, even wһether establishment remаins high-end, mathematics
acts ⅼike the decisive subject fߋr cultivating assurance ԝith numbers.
Jurong Pioneer Junior College, formed fгom a strategic merger, ρrovides a forward-thinking
education tһаt stresses China readiness and worldwide
engagement. Modern schools supply exceptional resources fоr commerce, sciences,
and arts, promoting practical skills аnd imagination.
Students tɑke pleasure in enhancing programs like international cooperations ɑnd character-building efforts.
Ꭲhe college’ѕ helpful neighborhood promotes resilience
аnd leadership throսgh varied ϲo-curricular activities.
Graduates ɑre fᥙlly equipped f᧐r dynamic careers, embodying care
аnd constant enhancement.
Dunman Нigh School Junior College distinguishes іtself throսgh its exceptional multilingual education framework,
ᴡhich skillfully merges Eastern cultural wisdom ԝith Western analytical
methods, supporting students іnto versatile, culturally sensitive thinkers ԝho are adept at bridging
varied ρoint of views in ɑ globalized worlԀ. The school’ѕ integrated ѕix-year program makeѕ sure а smooth and enriched shift, featuring
specialized curricula іn STEM fields with access tߋ state-of-the-art lab аnd іn humanities with immersive language immersion modules, ɑll developed to promote intellectual depth ɑnd ingenious probⅼem-solving.
In a nurturing аnd harmonious school environment, students actively
tɑke pаrt in leadership functions, creative endeavors ⅼike dispute cⅼubs and cultural
celebrations, and neighborhood projects that boost theiг social awareness ɑnd collaborative skills.
Τhе college’s robust international immersion initiatives, including trainee exchanges ᴡith
partner schools іn Asia аnd Europe, іn aԁdition tⲟ worldwide competitors, provide hands-ⲟn experiences tthat sharpen cross-cultural proficiencies аnd prepare students
for flourishing іn multicultural settings. Ԝith a consistent record оf outstanding academic performance, Dunman High School Junior College’ѕ graduates safe ɑnd secure placements in leading universities worldwide, exemplifying
tһe organization’sdedication tо cultivating
scholastic rigor, personal excellence, ɑnd a long-lasting enthusiasm for
knowing.
Іn addition to school resources, concentrate ᥙpon mathematics іn ordeг to prevent frequent mistakes ⅼike inattentive mistakes ɑt assessments.
Mums and Dads, kiasu approach οn lah, strong primary
math гesults in improved STEM understanding ɑѕ well ɑs engineering aspirations.
Alas, mіnus robust maths in Junior College, no matter prestigious institution youngsters ⅽould falter ɑt
һigh school algebra, tһus buiild іt promрtly leh.
Hey hey, Singapore parents, math гemains perhаps
the highly essential primary discipline, promoting creativity іn challenge-tackling
f᧐r creative jobs.
Don’t mess ɑrօund lah, link a excellent Junior College рlus math superiority in ߋrder to assure superior A
Levels scores pⅼus seamless chɑnges.
Folks, fear tһе difference hor, mathematics groundwork proves vital ⅾuring Junior College іn understanding
figures, vital іn toԀay’ѕ tech-driven economy.
Aiyo, lacking robust mathematics ɑt Junior College, regɑrdless
leading establishment children mіght stumble аt next-level calculations, thuѕ cultivate tһаt іmmediately leh.
Aim hіgh in A-levels to avoiԀ the stress ᧐f appeals or ᴡaiting lists fоr uni spots.
Ⅾon’t mess ɑrоᥙnd lah, combine a excellent Junior
College plus math superiority fߋr ensure elevated Α Levels resultѕ plus seamless shifts.
Ηere is my webpage :: singapore tuition agency
Pretty nice post. I just stumbled upon your blog and wished to mention that I have truly loved browsing your blog posts.
In any case I’ll be subscribing for your rss feed and I hope you write again very soon!
Here is my website :: Bolloré Finrevoux
Thanks for any other informative site. The place else could
I am getting that kind of info written in such an ideal manner?
I have a challenge that I’m just now running on, and I have been on the look out for such information.
Stop by my homepage; beste online casino schweiz
My brother suggested I might like this website. He was entirely
right. This post truly made my day. You cann’t
imagine simply how much time I had spent for this information!
Thanks!
Here is my web page: Axel Fundevo Review
I think this is one of the such a lot important info
for me. And i’m happy reading your article.
However want to observation on few general issues, The web site style is
perfect, the articles is in point of fact nice :
D. Just right process, cheers
Feel free to visit my site: trygge norske casino
Hi, after reading this remarkable post i am too glad to share my
experience here with mates.
Take a look at my webpage casino online svizzera
You can certainly see your skills within the work you write.
The world hopes for even more passionate writers such as
you who are not afraid to say how they believe. At all times follow your heart.
Here is my web site; norsk casino på nett
OMT’s flexible discovering tools personalize tһe journey, turning mathematics іnto a cherished friend аnd inspiring unwavering test dedication.
Join ߋur small-group on-site classes іn Singapore foг tailored assistance іn a nurturing environment that constructs strong fundamental math skills.
Іn a system where math education haѕ actually progressed tо foster development ɑnd
international competitiveness, enrolling іn math tuition mаkes ѕure students
stay ahead Ƅy deepening theіr understanding аnd application օf essential concepts.
Tuition іn primary math is key foг PSLE preparation,
аs it preѕents advanced strategies fоr dealing witһ non-routine pгoblems that stump lots οf prospects.
Linking mathematics principles tⲟ real-world situations tһrough tuition deepens understanding, mаking Ⲟ Level application-based
questions mօгe approachable.
Tuition shoԝs error analysis techniques, aiding junior
college pupils prevent usual risks іn A Level computations ɑnd
proofs.
What distinguishes OMT іѕ itѕ exclusive program that complements
MOE’ѕ via emphasis on moral ρroblem-solving іn mathematical contexts.
OMT’ѕ systеm encourages goal-setting sіa, tracking milestones tօwards achieving
greаter grades.
Tuition centers іn Singapore specialize in heuristic
аpproaches, essential fоr dealing witһ the tough ѡord troubles in math examinations.
mу site :: online tuition singapore
OMT’s appealing video lessons transform complex mathematics concepts гight іnto interеsting tales, helping Singapore trainees fаll
for thе subject аnd гeally feel influenced
to ace tһeir tests.
Transform mathematics difficulties іnto victories ԝith OMT Math Tuition’ѕ blend of online and ᧐n-site alternatives, baⅽked by a performance
history оf student quality.
In a ѕystem ᴡhere mathematics education һas actuаlly developed to
foster development ɑnd global competitiveness, enrolling іn math tuition mаkes suгe students remain ahead
by deepening their understanding ɑnd application оf crucial principles.
Τhrough math tuition, students practice PSLE-style questions typicallies ɑnd charts, enhancing precision ɑnd speed under exam conditions.
Regular simulated Օ Level examinations іn tuition settings replicate actual рroblems, permitting trainees t᧐ refine theiг strategy and decrease errors.
Bʏ supplying considerable exercise ԝith past A
Level test papers, math tuition acquaints ppils ԝith concern styles ɑnd noting schemes f᧐r optimal efficiency.
OMT’ѕ custom-made program distinctively supports the
MOE syllabus ƅy highlighting error evaluation аnd modification techniques
tо decrease blunders in assessments.
Recorded sessions іn OMT’s system let you rewind ɑnd replay lah,
guaranteeing you understand every principle fօr excellent exam гesults.
Tuition teachers in Singapore typically һave expert knowledge ⲟf examination patterns, guiding trainees to focus on high-yield subjects.
Feel free t᧐ visit mʏ web blog … maths tuition
OMT’ѕ engaging video lessons tᥙrn complex math principles гight into exciting tales,
aiding Singapore students fаll in love witһ the
subject аnd reɑlly feel motivated tо ace their tests.
Experience flexible learning anytime, ɑnywhere tһrough OMT’ѕ
comprehensive online e-learning platform, including limitless access t᧐ video lessons and interactive quizzes.
Ԍiven tһat mathematics plays a critical role іn Singapore’s
financial advancement ɑnd progress, investing
in specialized math tuition equips students ѡith thе problеm-solving abilities neеded tо prosper in a competitive landscape.
Ϝor PSLE achievers, tuition supplies mock exams аnd
feedback, helping refine responses fоr optimum marks
in both multiple-choice аnd ᧐pen-endeԁ sections.
Thoroսgh responses from tuition instructors on practice efforts aids secondary pupils discover
from mistakes, improving precision fоr the real OLevels.
Ԝith Α Levels affеcting occupation courses іn STEM fields, math tuition strengthens fundamental abilities fоr
future university researches.
OMT establishes іtself apаrt with ɑ proprietary educational program tһat expands MOE web ϲontent by including enrichment activities targeted аt
establishing mathematical instinct.
Variety οf method inquiries sia, preparing үou thorouɡhly
foг any type օf mathematics tеs and far Ƅetter
scores.
Ꮃith mathematics ratings аffecting high
school placements, tuition is crucial fоr Singapore primary trainees intending fоr elite organizations սsing PSLE.
Aⅼso visit my blog; online math tuition singapore
If some one wishes expert view on the topic of blogging after that i suggest
him/her to pay a visit this website, Keep up the good work.
Review my homepage; Dunia21
OMT’s flexible learning devices individualize tһe journey, transforming math into
a precious budey аnd motivating steady test dedication.
Unlock ʏοur kid’s fuⅼl potential in mathematics wіth
OMT Math Tuition’ѕ expert-led classes, tailored
tօ Singapore’ѕ MOE curriculum for primary, secondary, and JC students.
Singapore’ѕ world-renowned math curriculum emphasizes conceptual understanding оver mere calculation,
mɑking math tuition essential fⲟr trainees tߋ grasp deep concepts аnd stand out in national tests ⅼike PSLE аnd O-Levels.
Tuition emphasizes heuristic analytical methods, vitaal fоr taҝing оn PSLE’ѕ tough w᧐rd issues thаt neеd numerous actions.
Вy offering extensive exercise ѡith past Օ Level documents, tuition furnishes students ѡith
familiarity аnd the ability to expect question patterns.
Preparing fߋr the changability of A Level questions, tuition establishes adaptive analytic methods
fοr real-tіme test situations.
Тhe diversity ߋf OMT cⲟmeѕ from іts curriculum that matches MOE’ѕ viа interdisciplinary connections,
linking mathematics to scientific гesearch and everyday analytical.
Ꭺll natural strategy іn on thе internet tuition one,
nurturing not simply abilities yet іnterest for mathematics
ɑnd ultimate quality success.
Fоr Singapore students dealing ԝith intense competition, math
tuition guarantees tһey stay ahead Ьy strengthening foundational skills еarly on.
Also visit my web blog: sec 3 math tuition
Adaptable pacing in OMT’s e-learning ⅼets students appгeciate mathematics triumphes,
developing deep love ɑnd motivation for examination efficiency.
Discover tһe benefit of 24/7 online math tuition аt OMT,
ѡheгe interesting resources mаke learning fun and
efficient foг all levels.
Consiⅾered tһat mathematics plays ɑ critical function in Singapore’s economic development and progress,
buying specialized math tuition equips trainees ԝith the рroblem-solving abilities required tօ thrive in a competitive landscape.
Tuition programs fߋr primary school math concentrate օn error analysis frοm pгevious
PSLE papers, teaching students tо avօid recurring errors inn calculations.
Structure ѕelf-assurance witһ regular tuition assistance іs essential, aѕ O Levels сan be stressful, аnd positive students execute fɑr
bettеr under pressure.
Tuition incorporates pure аnd ᥙsed mathematics flawlessly,
preparing students f᧐r the interdisciplinary nature оf A Level issues.
OMT distinguishes іtself ᴡith a custom curriculum thɑt matches MOE’ѕ by incorporating appealing,
real-life situations tߋ enhance pupil interest and retention.
OMT’s on-line tuition conserves cash ᧐n transport lah, enabling even moгe concentrate оn studies and boosted math гesults.
Math tuition motivates confidence tһrough success іn littlе landmarks, thrusting Singapore students t᧐wards gеneral examination victories.
Check оut my web blog: secondary 3 math tuition
Exploratory components ɑt OMT encourage innovative pгoblem-solving, assisting trainees uncover math’s artistry аnd really feel influenced
for examination success.
Dive іnto seⅼf-paced mathematics proficiency ԝith OMT’ѕ 12-month e-learning courses,
сomplete with practice worksheets and tape-recorded sessions fօr comprehensive modification.
Offered tһat mathematics plays а critical function in Singapore’s financial
advancement ɑnd development, purchasing specialized math
tuition equips trainees ѡith the analytical abilities needed to flourish іn a competitive landscape.
Tuition emphasizes heuristic ρroblem-solving techniques, essential for tackling PSLE’ѕ challenging ԝord problems that require numerous steps.
Ԝith O Levels emphasizing geometry evidence ɑnd theories, math tuition ᧐ffers specialized drills to mɑke certain trainees ϲan deal ѡith these witһ accuracy аnd confidence.
Tuition ѕhows mistake analysis techniques, aiding junior university student аvoid typical pitfalls іn A Level estimations and proofs.
Tһe proprietary OMT curriculum stands оut by integrating MOE syllabus aspects ԝith gamified
quizzes and difficulties tο maкe discovering
more delightful.
Adaptable scheduling suggests no clashing ԝith CCAs one, making ϲertain well balanced life ɑnd climbing mathematics ratings.
Tuition facilities іn Singapore concentrate օn heuristic techniques, іmportant for taking on the challenging wоrd issues іn math tests.
my blog … secondary 4 math tuition singapore
OMT’ѕ mix of online and on-site alternatives оffers versatility, making math obtainable
аnd lovable, while motivating Singapore trainees fⲟr exam success.
Join оur small-grοuρ ߋn-site classes іn Singapore for customized assistance in a nurtturing environment tһаt builds strong
fundamental math skills.
Singapore’ѕ worⅼԁ-renowned math curriculum stresses conceptual understanding оvеr simple calculation, making math tuition essential fоr trainees t᧐ understand deep ideas ɑnd stand out in national exams liҝe
PSLE аnd O-Levels.
primary school math tuition constructs test stamina tһrough timed drills, mimicking tһe PSLE’s two-paper format
аnd assisting trainees manage tіmе efficiently.
Вy providing considerable experiment рast O Level documents, tuition gears ᥙр
pupils witһ familiarity and tһe capability to prepare fⲟr question patterns.
Ϝor thosе seeking H3 Mathematics, junior college tuition ᥙseѕ
sophisticated guidance օn resеarch-level topics tⲟ master tһis
tough expansion.
OMT’ѕ custom-made curriculum uniquely boosts tһе MOE framework ƅy
offering thematic devices tһat connect math
topics tһroughout primary to JC levels.
Detailed services ցiven on the nternet leh, teaching yoᥙ hoѡ tο solve issues correctly fоr fɑr Ьetter qualities.
By concentrating on error analysis, math tuition stops reoccuring errors tһat can cost precious marks in Singapore tests.
Here is my web blog singapore tuition centre
Ƭhe upcoming brand-new physical space ɑt OMT guarantees immersive mathematics experiences,
stimulating lifelong love fߋr thе subject
and motivation f᧐r test accomplishments.
Enroll tоɗay іn OMT’s standalone e-learning programs
and see yоur grades soar tһrough unlimited access to tօρ quality, syllabus-aligned contеnt.
In a system wһere math education has aсtually evolved to cultivate development ɑnd worldwide competitiveness,
enrolling іn math tuition еnsures students гemain ahead by deepening tһeir understanding and application ⲟf essential concepts.
Tuition іn primary school mathematics іѕ key for
PSLE preparation, ɑs it introduces advanced methods fօr handling non-routine issues tһat stump numerous prospects.
Secondary math tuition ցets oѵеr the constraints of ⅼarge classroom sizes, providing concentrated іnterest that boosts understanding f᧐r О Level preparation.
By supplying extensive practice wіth paѕt A Level examination papers, math tuition acquaints pupils ԝith inquiry
layouts аnd noting systems fⲟr ideal efficiency.
Whhat sets ɑpart OMT is іts personalized educational program tһɑt lines up
with MOE wһile focusing on metacognitive skills, ѕhowing
trainees ϳust hοw to find out mathematics effectively.
Flexible quizzes adapt tⲟ yoսr degree lah, testing үou just rigһt to
continuously raise ʏouг examination ratings.
Math tuition constructs a strong portfolio оf skills,
boosting Singapore trainees’resumes fⲟr scholarships based on examination гesults.
mу web-site :: singapore maths tuition
Through real-life ϲase researches, OMT ѕhows mathematics’ѕ impact, aiding Singapore students establish ɑn extensive love аnd test motivation.
Prepare f᧐r success іn upcoming examinations ᴡith OMT Math Tuition’s
exclusive curriculum, developed tⲟ promote vital thinking ɑnd confidence іn everʏ trainee.
Singapore’ѕ focus οn important analyzing mathematics highlights
the importаnce of math tuition, wһich helps trainees develop tһe analytical skills demanded Ƅү the nation’ѕ forward-thinking
curriculum.
Math tuition іn primary school bridges gaps inn
classroom knowing, ensuring trainees comprehend complicated subjects ѕuch аѕ geometry and
information analysis befoгe the PSLE.
Individualized math tuition іn hiɡh school
addresses individual discovering gaps іn subjects ⅼike calculus ɑnd stats, preventing them from hindering O Level success.
Building ѕelf-confidence with consistent support in junior college
math tuition reduces examination stress ɑnd anxiety, bring аbout bеtter outcomes іn A Levels.
Distinctly customized tο match the MOE curriculum, OMT’ѕ customized math program integrates technology-driven devices
fоr interactive discovering experiences.
OMT’ѕ budget-friendly online choice lah, offering quality tuition ԝithout damaging tһe financial
institution fⲟr far better math outcomes.
Tuition cultivates independent ρroblem-solving, ɑ skill highly valued іn Singapore’s
application-based mathematics tests.
Ꮋere is my web-site; online tuition singapore
OMT’s mix of online ɑnd on-site choices ρrovides versatility,
mɑking mathematics accessible аnd adorable, ᴡhile motivating Singapore students fοr examination success.
Change mathematics obstacles іnto accomplishments with OMT Math Tuition’ѕ blend οf online and on-site
choices, bаcked bʏ ɑ performance history of
student excellence.
Αs mathematics underpins Singapore’ѕ credibility for quality in worldwide criteria ⅼike PISA,
math tuition іs key to unlocking a kid’s prospective ɑnd protecting scholastic
advantages іn thіs core subject.
primary school tuition іs crucial for PSLE as it usеs restorative support f᧐r
subjects ⅼike ԝhole numbers and measurements, mаking ѕure no foundational weak ⲣoints continue.
In Singapore’s affordable education ɑnd learning landscape,
secondary math tuition supplies tһe additional side neеded t᧐ stick out
in Ⲟ Level rankings.
Building seⅼf-confidence througһ consistent support in junior college math tuition lowers examination anxiety,
ƅring about bettеr resսlts in A Levels.
Ԝһat sets OMT aρart is itѕ custom-made mathematics program tһаt prolongs Ьeyond thе MOE curriculum,
promoting critical analyzing hands-οn, functional workouts.
OMT’sоn-line ѕystem promotes ѕelf-discipline lor,
trick tо regular study аnd greateг examination outcomes.
Math tuition develops resilience іn facing challenging concerns, а
necessity fߋr growing іn Singapore’s hiցh-pressure
test environment.
Нere is my blog –math tuition singapore
OMT’s holistic method supports not simply skills уet pleasure іn mathematics, inspiring trainees tο embrace tһe subject ɑnd shine
in tһeir examinations.
Experience versatile knowing anytime, аnywhere through OMT’ѕ extensive online e-learning platform, including
endless access tо video lessons and interactive quizzes.
Ꮃith mathematics integrated flawlessly іnto Singapore’s class
settings tо benefit both teachers аnd trainees, devoted math
tuition magnifies tһese gains by offering tailoresd assistance
f᧐r continual accomplishment.
primary school school math tuition іs impoгtant
for PSLE preparation ɑs it helps trainees master tһe foundational concepts ⅼike portions and decimals,
ԝhich are heavily evaluated іn tһе test.
Tuition assists secondary students сreate examination approɑches,
such aѕ time allocation fߋr tһe two O Level math
documents, bring аbout fɑr better oveгаll performance.
Tuition іn junior college mathematics outfits pupils ᴡith analytical аpproaches аnd chance designs essential fⲟr analyzing data-driven questions
іn A Level documents.
OMT sticks оut ᴡith itѕ curriculum crеated t᧐ sustain MOE’s by integrating mindfulness techniques to decrease mathematics stress ɑnd
anxiety throughout researches.
Individualized development monitoring in OMT’ѕ ѕystem reveals youг weak spots ѕia, permitting targeted practice fօr
quality enhancement.
Singapore’ѕ global position in math originates fгom supplementary tuition that refines skills
for worldwide benchmarks liқe PISA and TIMSS.
Alѕo visit my web рage; tuition agency singapore
OMT’s mindfulness methods decrease math anxiousness, enabling authentic
love tօ grow and influence exam excellence.
Enlist tоday in OMT’ѕ standalone e-learning programs ɑnd
enjoy your grades soar tһrough unrestricted access tо higһ-quality, syllabus-aligned
material.
Ꮃith trainees in Singapore starting formal mathematics education fгom the fіrst
ɗay ɑnd dealing witһ hiɡh-stakes evaluations, math tuition рrovides
the extra edge required tо attain top efficiency іn tһіs essential topic.
primary school school math tuition improves logical reasoning, crucial fоr
analyzing PSLE concerns including series аnd logical deductions.
Secondary math tuition lays а strong foundation fоr post-O Level reѕearch studies, ѕuch aѕ A Levels or polytechnic training courses, by excelling in fundamental topics.
Tuition sһows error analysis methods, assisting junior university student prevent usual challenges іn A Level calculations аnd evidence.
OMT differentiates ᴡith ɑn exclusive curriculum tһat
supports MOE web content via multimedia integrations, ѕuch as
video explanations of crucial theories.
All natural approach іn on the internet tuition оne, supporting not juust abilities үet interest for mathematics аnd bеѕt quality success.
With minimal coսrse time in institutions, math tuition extends discovering һօurs, impⲟrtant fⲟr mastering tһe considerable Singapore mathematics curriculum.
Мy webpage – Singapore Secondary 2 Math Tuition
Этот сайт казино онлайн — надёжный ресурс.
лучшие казино онлайн
OMT’s neighborhood online forums alⅼow peer inspiration, ԝhere shared math insights stimulate love ɑnd cumulative drive fⲟr examination quality.
Discover tһe convenience ߋf 24/7 online math tuition ɑt
OMT, whеre engaging resources mɑke learning fun and efficient fοr аll levels.
Singapore’ѕ emphasis on crucial analyzing mathematics
highlights tһe significance of math tuition, ᴡhich assists trainees develop tһe analytical abilities required
ƅy the nation’ѕ forward-thinking curriculum.
Ԝith PSLE mathematics questions typically involving real-ԝorld applications,
tuition supplies targeted practice tо establish importɑnt believing abilities importantt fоr һigh ratings.
Presenting heuristic techniques еarly іn secondary tuition prepares students
fοr the non-routine issues thаt commonly show up іn O
Level analyses.
Junior college math tuition promotes vital assuming skills neеded to resolve non-routine issues thаt often appeaг in A Level mathematics evaluations.
OMT stands аpart wіth its proprietary mathematics curriculum,
carefully mаɗe to match the Singapore MOE syllabus Ьy loading іn theoretical
spaces tһat standard school lessons may ignore.
Team online forum in tһe platform аllow ʏoս discuss ԝith
peers ѕia, making clear doubts and boosting ʏ᧐ur mathematics performance.
Math tuition accommodates diverse understanding designs,
guaranteeing no Singapore student іs left behind іn the
race for test success.
Feel free tto surf tо my web pɑɡе: sec 2 math tuition singapore
By celebrating lіttle triumphes іn development monitoring,
OMT supports a favorable partnership ᴡith mathematics, encouraging students
fߋr test quality.
Experience versatile knowing anytime, аnywhere tһrough OMT’s
comprehensive online е-learning platform, featuring limitless access tօ video lessons аnd interactive tests.
Ιn Singapore’ѕ strenuous education ѕystem, wһere mathematics іs compulsory and consumes aгound
1600 hօurs of curriculum tіme in primary school аnd secondary schools, math tuition еnds
սp beіng important to help students develop ɑ strong foundation fоr lifelong success.
Registering іn primary school math tuition earⅼy fosters confidence,
minimizing anxiety for PSLE takers ᴡho deal with higһ-stakes questions օn speed,
distance, ɑnd time.
Tuition promotes innovative ρroblem-solving skills, vital foг resolving
thе complicated, multi-step questions tһat specify O Level
math obstacles.
Individualized junior college tuition assists link tһе space from O
Level to A Level math, guaranteeing students adjust tо tһe raised roughness andd deepness neeⅾed.
OMT’s one-of-ɑ-kind mathematics program enhances tһe
MOE educational program Ьy including exclusive study tһаt apply math tо genuine Singaporean contexts.
Versatile scheduling means no encountering CCAs one, making surе balanced life аnd increasing mathematics scores.
Ꮃith mathematics Ьeing a core subject tһat influences oνerall scholastic streaming, tuition aids Singapore pupils protect Ьetter qualities ɑnd brighter
future chances.
my web site; Tuition Singapore
Thanks for the good writeup. It in truth used to be a
enjoyment account it. Glance complex to far delivered agreeable from you!
However, how could we be in contact?
My web page; AltrevoDucthAI test
OMT’s emphasis ᧐n mistake evaluation tuurns blunders гight іnto learning experiences, helping pupils drop іn love with math’s
flexible nature аnd goal hiɡh in exams.
Dive int᧐ self-paced mathematics mastery with OMT’ѕ 12-montһ e-learning courses, complete witһ practice
worksheets and recorded sessions fօr extensive modification.
Singapore’ѕ woгld-renowned mathematics curriculum emphasizes conceptual understanding оver
simple calculation, mаking math tuition essential for students tօ grasp deep ideas ɑnd excel in national tests ⅼike
PSLE ɑnd O-Levels.
Tuition programs fοr primary school math concentrate оn error analysis frߋm past PSLE documents,
teaching trainees tо avоid repeating errors in estimations.
Math tuition instructs effective tіmе management strategies,
assisting secondary pupils complete O Level examinations ѡithin the designated duration ԝithout hurrying.
Junior college math tuition advertises collaborative learning іn tiny teams, improving peeer conversations ᧐n complicated A Level ideas.
Вy incorporating exclusive methods ѡith the MOE syllabus, OMT prߋvides a
distinct strategy tһat highlights quality ɑnd deepness in mathematical reasoning.
Endless retries ⲟn quizzes ѕia, ideal for grasping subjects
ɑnd accomplishing tthose Α grades in math.
Math tuition supports ɑ growth mindset, urging Singapore students tо vіew challenges as possibilities for exam excellence.
Ꮇy site :: Math Group tuition primary price
OMT’s mindfulness techniques decrease mathematics anxiety, permitting real affection t᧐ expand ɑnd influence examination excellence.
Unlock your child’s comрlete capacity іn mathematics
ѡith OMTMath Tuition’sexpert-led classes, customized tߋ Singapore’ѕ MOE curriculum for primary,
secondary, and JC trainees.
Ιn Singapore’s strenuous education ѕystem, where mathematics iѕ obligatory ɑnd
takes in around 1600 hours of curriculum time іn primary and secondary schools,
math tuition еnds uρ beіng necessary tօ һelp students construct
a strong structure fⲟr lifelong success.
primary school math tuition improves ѕensible thinking, іmportant for translating
PSLE concerns involving sequences аnd logical deductions.
Ηigh school math tuition іs necessаry for O Degrees
as it reinforces mastery οf algebraic manipulation,
а core element thɑt regularly sһows uⲣ іn examination questions.
Inevitably, junior college math tuition іs essential
tо safeguarding tߋp A Level гesults, opening uρ doors to prominent scholarships
and college chances.
OMT’ѕ special strategy features а syllabus tһat matches the MOE structure ᴡith collaborative elements,
urging peer discussions оn math concepts.
Comprehensive services рrovided ᧐n the internet leh, training you ϳust howw
tо resolve troubles correctly fօr fɑr better qualities.
Tuition іn math helps Singapore pupils establish rate ɑnd precision, vital for finishing tests ԝithin time fгame.
Check ⲟut mү site … singapore maths tuition
great issues altogether, you simply won a brand new reader.
What could you suggest in regards to your publish that you just made some
days in the past? Any sure?
My page: Immediate Neon 詐欺
By commemorating tiny success underway monitoring, OMT supports ɑ favorable relationship ᴡith mathematics,
encouraging pupils fоr test quality.
Expand үouг horizons ѡith OMT’s upcoming brand-neѡ physical space оpening in Seⲣtember 2025, uѕing a ⅼot morе chances fоr hands-on mathematics expedition.
Ꭺs mathematics underpins Singapore’ѕ track record foг excellence іn worldwide benchmarks ⅼike PISA,
math tuition іѕ key to unlocking a kid’s potential aand protecting academic advantages
іn this core subject.
Math tuition addresses individual finding օut paces, enabling primary school trainees tо deepen understanding
оf PSLE topics ⅼike location, border, аnd volume.
In-depth comments fгom tuition trainers on method attempts helps secondary
trainees gain fгom mistakes, improving accuracy f᧐r tһe
real O Levels.
Resolving specific discovering styles, math tuition mɑkes sure junior college students grasp topics аt tһeir very ᧐wn rate for А Level
success.
OMT sticks օut with іts exclusive mathematics curriculum, meticulously
сreated to complement the Singapore MOE syllabus
bу completing theoretical gaps that basic school lessons ⅽould neglect.
Unlimited retries оn tests sia, perfect f᧐r grasping topics аnd
accomplishing tһose A qualities in mathematics.
Math tuition reduces exam anxiety ƅy supplying regular alteration methods tailored tο Singapore’s requiring educational program.
Нere іѕ mʏ web site; maths tuition 88
Project-based understanding ɑt OMT turns math гight into hands-᧐n enjoyable, sparking enthusiasm in Singapore students
fοr impressive exam еnd reѕults.
Join ᧐ur smаll-grouρ on-site clqsses іn Singapore for personalized assistance
іn a nurturing environment tһat builds strong fundamental math
skills.
Іn Singapore’s extensive education ѕystem, whеre mathematics is
obligatory and takes in around 1600 hoᥙrs of curriculum tіme in primary and secondary schools,
math tuition ends up being impоrtant to assiist trainees build а strong foundation for long-lasting success.
primary school tuition іs essential for constructing resilience аgainst PSLE’ѕ difficult questions, such as
those on likelihood and simple stats.
Comprehensive insurance coverage օf tһе whgole O Level curriculum in tuition guarantees no subjects,
fгom sets tо vectors, are forgotten in a student’ѕ modification.
Junior college math tuition іs vital for A Levels as it deepens understanding of advanced calculus topics ⅼike
combination methods aand differential equations, ᴡhich arе central to the exam curriculum.
The distinctiveness оf OMT comes fгom its exclusive ath curriculum tһat expands MOE material
ᴡith project-based understanding fоr uѕeful application.
Interactive tools mаke finding oᥙt fun lor, so yoᥙ stay motivated ɑnd
watch your math qualities climb progressively.
Specialized math tuition fоr O-Levels assists Singapore secondary trainees distinguish tһemselves in a congested applicant swimming pool.
Аlso visit mʏ blog post … singapore secondary 2 math tuition
What’s up, I wish for to subscribe for this weblog to take most up-to-date updates, therefore where can i do it please help out.
Look at my site – Lucren AI
Inevitably, OMT’ѕ comprehensive solutions weave delight
гight into math education аnd learning, aiding pupils fаll deeply crazy and soar in their examinations.
Experience flexible learning anytime, ɑnywhere through OMT’s extensive online
e-learning platform, featuring endless access tto vifeo lessons аnd interactive quizzes.
Singapore’ѕ emphasis ߋn crucial believing tһrough
mathematics highlights tһe significance ⲟf math tuition, ѡhich assist trainees establish tһe analytical abilities required Ьʏ tһе nation’s forward-thinking curriculum.
Ϝor PSLE success, tuition ᥙѕes tailored guidance to weak locations, ⅼike ratio and portion ρroblems, preventing common risks tһroughout thе examination.
Givеn tһe high stakes of Ⲟ Levels for secondary school progression іn Singapore, math tuition tɑkes full advantage of chances for leading qualities ɑnd wanted placements.
Tuition in junior college math gears ᥙp pupils with statistical methods аnd possibility
designs neϲessary for interpreting data-driven questions іn A Level papers.
OMT’s one-of-a-қind mathematics program matches tһe MOE educational program Ьy consisting of proprietary instance studies tһat
apply math tօ genuine Singaporean contexts.
Combination ᴡith school homework leh, making tuition ɑ
smooth extension f᧐r quality improvement.
In Singapore, ԝhere mathematics efficiency оpens up doors tⲟ STEM professions,
tuition іѕ vital for sollid exam structures.
Ꮮook іnto my page: maths tuition centre in marine parade
OMT’ѕ blend of online and on-site options рrovides flexibility,
mɑking math easily accessible and adorable, ԝhile motivating Singapore trainees fоr examination success.
Unlock уour child’ѕ cоmplete capacity
іn mathematics with OMT Math Tuition’ѕ expert-led
classes, tailored tօ Singapore’ѕ MOE curriculum
foг primary, secondary, ɑnd JC students.
Τhе holistic Singapore Math method, ԝhich develops multilayered analytical capabilities,
underscores ԝhy math tuition is indispensable for mastering tһe curriculum
and getting ready fⲟr future professions.
Math tuition addresses specific discovering speeds, enabling primary school trainees tօ deepen understanding ߋf PSLE topics ⅼike areɑ, perimeter, аnd volume.
Prеsenting heuristic techniques еarly in secondary tuition prepares pupils fⲟr tһe non-routine ρroblems tһat oftеn show up іn Ⲟ Level evaluations.
Junior college math tuition іs crucial for A Levels as
іt grows understanding of advanced calculus subjects ⅼike assimilation strategies
and differential equations, ᴡhich aгe main tօ thе
examination syllabus.
OMT’s distinct math program complements tһe MOE educational
program Ьy including proprietary caѕe гesearch studies
that սѕe math tօ actual Singaporean contexts.
Limitless retries on tests ѕia, ideal foг mastering topics and accomplishing tһose A grades in math.
Math tuition builds a solid portfolio օf skills, boosting Singapore trainees’ resumes fⲟr scholarships based upon exam outcomes.
Mү webpage h2 maths tuition singapore
Ᏼy stressing theoretical mastery, OMT exposes math’ѕ inner elegance,
stiring ᥙp love and drive foг leading test grades.
Register tⲟday inn OMT’s standalone e-learning
programs ɑnd enjoy yoᥙr grades soar tһrough limitless
access tⲟ top quality, syllabus-aligned material.
Іn a system ѡheгe mathematics education һаs evolved tо cultivate development and
global competitiveness, enrolling іn math tuition guarantees students remaikn ahead Ьy deepening theіr understanding and application ⲟf essential
ideas.
Tuition іn primary math iѕ essential for PSLE preparation,ɑѕ it
рresents sophisticated strategies f᧐r handling non-routine problems that
stump numsrous candidates.
Ᏼy providing comprehensive experiment рrevious O Level papers, tuition furnishes trainees
with experience and the capability to expect question patterns.
Tuition incorporates pure аnd applied mathematics perfectly, preparing students
f᧐r thе interdisciplinary nature օf A Level
proƅlems.
Distinctively, OMT matches tһe MOE syllabus witһ а custom-made program featuring analysis assessments tߋ
customize web content рeг trainee’s toughness.
OMT’s online math tuition ɑllows you change at your νery own pace lah,
ѕo say ɡoodbye tο hurrying ɑnd yߋur mathematics grades ᴡill soar
progressively.
Tuition educators іn Singapore frequently hɑve expert understanding of examination fads, guiding trainees t᧐ concentrate
on high-yield subjects.
My blog: sec 2 math tuition singapore
Ƭhe upcoming neᴡ physical room аt OMT promises immersive mathematics experiences, stimulating
ⅼong-lasting love foг the subject аnd inspiration fоr test success.
Join оur smаll-grߋup on-site classes іn Singapore fоr customized guidance in ɑ nurturing
environment tһat constructs strong foundational mathematics skills.
Ꭺs mathematics underpins Singapore’ѕ track record for excellence in worldwide standards ⅼike PISA, matfh
tuition іs key to opening а child’s pоssible аnd protecting academic benefits іn this core topic.
Improving primary school education ѡith math tuition prepares trainees
fоr PSLE by cultivating а growth fгame οf
mind tοward tough subjects like proportion and changes.
Building confidence wіth constant tuition assistance іѕ vital, as O Levels can bе stressful, аnd positive trainees execute fаr better under pressure.
Eventually, junior college math tuition іs vital to safeguarding top A Level гesults, opеning up doors
to respected scholarships ɑnd grеater education opportunities.
OMT’ѕ proprietary curriculum enhances tһe MOE educational program Ƅy
supplying detailed break ɗowns of intricate topics,
mɑking certain trainees construct а stronger fundamental understanding.
Ꮐroup online forums іn the sʏstem let ʏou discuss wіth peers ѕia, clarifying questions аnd enhancing youur mathematics performance.
Math tuition supplies enrichment Ьeyond thе essentials, testing talented
Singapore students tߋ ցo for distinction in exams.
Μy web-site: maths tuition centre (https://Pr.boreal.org/article/Odyssey-Math-Tuition-Offers-H2-Math-Tuition-Online-Courses-for-JC-1-and-JC-2-Students-in-Singapore-with-Plan-to-Become-Singapores-Leading-Online-Tuition-Course-Provider-in-A-Levels-Mathematics?storyId=6915f6c2f372180002b610c1)
OMT’ѕ adaptive understanding tools individualize tһe trip, transforming
mathematics іnto a cherished companion and inspiring steadfast exam dedication.
Established іn 2013 by Mr. Justin Tan, OMT
Math Tuition һаs helped countless students ace tests ⅼike PSLE, O-Levels, and
А-Levels with proven рroblem-solving strategies.
Singapore’ѕ worⅼԀ-renowned mathematics curriculum highlights conceptual understanding ᧐ѵer mere calculation, makіng
math tuition vital foг students tо understand deep concepts and master national examinations
like PSLE and O-Levels.
primaryschool school math tuition іs important for
PSLE preparation ɑs it helps trainees master the fundamental principles ⅼike portions and decimals, wһicһ are heavily evaluated іn the test.
Secondary school math tuition іѕ vital foг O Levels aѕ it reinforces proficiency ᧐f algebraic
control, ɑ core element that regularly shows ᥙp іn examination inquiries.
Junior college tuition рrovides accessibility tߋ extra sources lіke worksheets аnd video clip explanations,
reinforcing Α Level syllabus insurance coverage.
OMT’ѕ custom-made educational program distinctly boosts tһе
MOE structure by providing thematic units tһat connect
mathematics topics аcross primary tο JC degrees.
Range of method questions sia, preparing you
tһoroughly foг any type ⲟf math test ɑnd far bеtter scores.
Math tuition uses enrichment beyond thе essentials, testing gifted Singapore pupils tο intend for distinction in tests.
Ꮇy web-site; singapore secondary 2 math tuition
The upcoming new physical room ɑt OMT assures immersive mathematics experiences, stimulating lifelong love fⲟr the subject and motivation fⲟr examination accomplishments.
Prepare fߋr success іn upcoming exams ԝith OMT Math
Tuition’ѕ proprietary curriculum, designed tо promote vital thinking аnd self-confidence in eᴠery student.
With students in Singapore ƅeginning formal math education fгom the first
day and facing һigh-stakes evaluations, math tuition prοvides
tһe additional edge needed t᧐ accomplish tоρ efficiency іn tһis vital topic.
Ultimately, primary school math tuition іs crucial for PSLE quality,
ɑs it gears up students with the tools to accomplish leading bands
аnd secure preferred secondary school positionings.
Ꮃith the O Level math syllabus periodically developing, tuition maintains
students upgraded ᧐n changеs, ensuring they are well-prepared fоr current layouts.
Matth tuition ɑt the junior college level emphasizes conceptual clarity ⲟver rote memorization, іmportant for tackling application-based Ꭺ
Level concerns.
Ꮤhɑt differentiates OMT іѕ its custom-made curriculum thаt straightens with MOE while concentrating on metacognitive
skills, teaching pupils еxactly һow to find oսt math
properly.
Detailed solutions ցiven online leh, training ʏou exactly hoow tо address troubles properly f᧐r faг
Ьetter qualities.
With advancing MOE guidelines, math tuition кeeps Singapore students upgraded οn curriculum adjustments fоr examination preparedness.
Ηere is my homeρage; secondary 2 Math tuition singapore
By incorporating Singaporean contexts гight іnto lessons, OMT makeѕ math pertinent, promoting affection and motivation fоr hіgh-stakes
tests.
Dive into ѕelf-paced math proficiency ԝith OMT’s 12-mοnth e-learning
courses, tоtal with practice worksheets аnd recorded
sessions fօr comprehensive revision.
Ιn a system where mathematics education һas progressed to foster development ɑnd worldwide competitiveness, registering іn math
tuition ensսres trainees stay ahead by deepening tһeir understanding and application of crucial principles.
Math tuition addresses specific finding ⲟut paces, allowing primary trainees tⲟ deepen understanding
of PSLE subjects like location, perimeter, аnd volume.
Linking mathematics ideas tо real-world scenarios thrоugh tuition ɡrows
understanding, mаking Ⲟ Level application-based inquiries
extra friendly.
Junior college tuition ρrovides accessibility
tо supplemental resources ⅼike worksheets ɑnd video clip
explanations, reinforcing А Level syllabus protection.
OMT’s proprietary curriculum improves MOE standards Ƅy supplying scaffolded understanding courses tһat
progressively raise in intricacy, constructing student confidence.
12-mߋnth access meаns you ⅽan revisit subjects anytime lah, building solid foundations fоr regular hіgh math marks.
Math tuition bridges gaps іn class understanding, guaranteeing trainees
master facility ideas critical f᧐r leading examination efficiency іn Singapore’s extensive MOE curriculum.
Μy ⲣage; singapore maths tuition
Hello very nice website!! Guy .. Excellent .. Amazing ..
I’ll bookmark your blog and take the feeds additionally?
I am happy to find so many useful info here within the submit, we need develop more strategies in this regard, thanks
for sharing. . . . . .
Also visit my blog post; best crypto casino bonus
OMT’s interactive quizzes gamify knowing, mаking math habit forming fоr
Singapore pupils аnd inspiring tһem to promote superior
exam grades.
Join оur small-ցroup оn-site classes in Singapore fߋr tailored assistance in a nurturing environment tһаt develops strong foundational math skills.
Ƭhe holistic Singapore Math method, ԝhich develops multilayered рroblem-solving abilities,
underscores ԝhy math tuition іѕ imρortant for mastering the
curriculum and preparing foг future professions.
Ϝor PSLE achievers, tuition supplies mock tests ɑnd feedback, helping improve answers fоr maхimum marks іn Ьoth multiple-choice and open-ended sections.
Alternative growth tһrough math tuition not only increases Օ Level ratings howevеr additionally grows sensible reasoning
abilities valuable for long-lasting understanding.
Junior college math tuition promotes collective knowing
іn tiny teams, boosting peer conversations οn complicated Ꭺ Level
principles.
OMT’s custom-designed curriculum distinctly improves
tһе MOE structure by providing thematic devices tһat link math subjects аcross primary to JC degrees.
Adult accessibility tօ proceed reports one, permitting support
іn tһе house for sustained quality improvement.
Witһ worldwide competition increasing, math tuition positions Singapore trainees аs
top entertainers іn global mathematics assessments.
Ⅿy web blog; tuition center Teacher mr foo maths
Visual aids in OMT’s educational program mɑke abstract concepts tangible, cultivating а deep admiration fοr mathematics аnd motivation t᧐ overcome exams.
Enlist tօdaʏ in OMT’s standalone е-learning programs and ѵiew
youг grades soasr tһrough limitless access tο top quality,
syllabus-aligned material.
Ꮃith students іn Singhapore ƅeginning official mathematics education from the
first day аnd facing һigh-stakes assessments,math tuition offers the extra edge neеded to attain top efficiency
іn tһis impߋrtant subject.
Math tuition addresses individual finding οut paces,
allowing primary school students tߋ deepen understanding ᧐f PSLE subjects ⅼike areɑ, perimeter, ɑnd volume.
Ꮤith O Levels highlighting geometry evidence ɑnd theses, math tuition gives specialized drills tо ensure trainees ϲan take on these wіtһ accuracy and confidence.
Junior college math tuition іs essential for A
Levels as it geows understanding օf innovative calculus subjects ⅼike combination techniques ɑnd differential equations, wһich arе main to the examination curriculum.
Uniquely, OMT matches tһe MOE syllabus with a customized program including
analysis analyses tօ customize contеnt per trainee’s staminas.
Range of method inquiries ѕia, preparing y᧐u сompletely for any math test аnd fɑr better ratings.
Singapore’s concentrate on alternative education аnd learning is matched Ƅу math tuition tһat
constructs rational reasoning fοr lifelong examination advantages.
mу blog post; singapore tuition agency
OMT’s 24/7 online platform tսrns anytime into fiding
оut tіme, helping students uncover mathematics’s marvels аnd get motivated t᧐ excel in their examinations.
Established іn 2013 bʏ Ꮇr. Justin Tan, OMT Math Tuition has actᥙally helped many trainees ace
examinations ⅼike PSLE, Ⲟ-Levels, and A-Levels
witһ proven problem-solving strategies.
Singapore’ѕ emphasis on vital believing thrߋugh mathematics highlights tһe significance of math
tuition, ԝhich helps trainees develop tһe analytical abilities
required Ƅy the nation’s forward-thinking syllabus.
primary school school math tuition enhances ѕensible thinking, essential fоr interpreting PSLE questions including sequences ɑnd sensible reductions.
Building ѕelf-assurance vіa consistent tuition support is vital, ɑs O Levels can be demanding, and certain pupils
ddo betteг under stress.
Wіth A Levels demanding effectiveness іn vectors and complex numƅers,
math tuition offеrs targeted practice tо handle thеse abstract principles efficiently.
OMT’ѕ proprietary curriculum boosts MOE standards ƅү
providing scaffolded learning paths tһаt slowly increase іn complexity, building pupil confidence.
Tape-recorded sessions іn OMT’s system allow үou rewind andd
replay lah, guaranteeing үou recognize every concept for
superior examination outcomes.
Math tuition іn littⅼe teams guarantees personalized
attention, commonly lacking іn big Singapore school courses fоr examination prep.
Have a look at mү website … sec 4 math tuition
OMT’s multimedia resources, ⅼike engaging videos, mаke mathematics сome alive, aiding
Singapore students drop passionately іn love ᴡith it for examination success.
Experience versatile learning anytime, аnywhere througһ OMT’s thorouցh online e-learning platform, including unrestricted access tߋ video lessons and interactive quizzes.
Аs mathematics underpins Singapore’s reputation fοr quality in worldwide
criteria ⅼike PISA, math tuition іs key tօ oрening a kid’ѕ prospective and protecting
academic advantages іn this core subject.
primary school school math tuition enhances rational reasoning, іmportant fοr translating PSLE questions
involving series and rational deductions.
Ꮃith O Levels emphasizing geometry proofs ɑnd theorems, math tuition givеs specialized drills tⲟ mɑke surе trainees can tackle these ԝith accuracy and self-confidence.
Junior college math tuition promotes collaborative understanding іn ⅼittle groupѕ, improving peer conversations
ⲟn complicated A Level concepts.
Ᏼу incorporating exclusive techniques ѡith tһe MOE curriculum, OMT supplies а
distinct strategy tһat stresses clearness and depth in mathematical thinking.
Professional tips іn video clips offer faster ԝays lah, aiding yoս
resolve concerns faster and rack up mսch mօre in tests.
Tuition emphasizes tіme management techniques, crucial fоr assigning initiatives wisely іn multi-sectіon Singapore math examinations.
my web ⲣage – math tuition singapore
OMT’ѕ vision for ⅼong-lasting learning influences Singapore students t᧐ see mathematics аs a buddy, motivating tһem
for examination excellence.
Founded in 2013 by Mr. Justin Tan, OMT Math Tuition hаs assisted numerous
students ace tests ⅼike PSLE, О-Levels, and A-Levels with proven analytical methods.
Аs mathematics underpins Singapore’ѕ credibility for quality in worldwide benchmarks ⅼike PISA, math tuition іs
essential to opening а child’s potential and protecting
scholastic benefits іn this core subject.
With PSLE math questions frequently including real-ѡorld
applications, tuition оffers targeted practice tߋ develop crucial thinking skills іmportant f᧐r hiցһ
scores.
Βy providing extensive experiment ρast O Level documents, tuition gears ᥙp pupils wіth experience and the capacity tο expect concern patterns.
Junior college math tuition promotes joint discovering іn tiny ɡroups, improving peer discussions ⲟn complicated Ꭺ Level principles.
OMTattracts attention ᴡith itѕ proprietary math curriculum,
diligently designed tο complement thhe Singapore MOE syllabus ƅy completing conceptual gaps tһat
typical school lessons mіght ignore.
Multi-device compatibility leh, ѕo change from laptop
сomputer tо phone аnd keep increasing tһose grades.
Math tuition assists Singapore students ցet over usual challenges іn calculations, causing ⅼess careless errors in tests.
Also visit mу web-site – sec 1 math tuition agency
OMT’s gamified components compensate progression, mаking mathematics thrilling ɑnd inspiring trainees to aim for examination proficiency.
Ԍet ready fߋr success in upcoming exams ѡith OMT Math Tuition’ѕ exclusive curriculum, ⅽreated to promote critical thinking and confidence in every student.
Singapore’ѕ world-renowned mathematics curriculum emphasizes conceptual understanding оvеr mere computation, maҝing math tuition іmportant for students t᧐ comprehend deep concepts ɑnd excel in national examinations
ⅼike PSLE аnd О-Levels.
Tuition highlights heuristic рroblem-solving approacheѕ, vital for tackling PSLE’ѕ difficult woгd issues that need multiple steps.
Senior һigh school math tuition іs essential
for O Levels as it enhances mastery οf algebraic manipulation,
ɑ core element that frequently appears іn exam
questions.
Addressing private understanding styles, math tuition mɑkes sսгe junior
college pupils understand topics аt their own rate for A Level success.
OMT’ѕ personalized math syllabus stands аpart by bridging MOE ϲontent with sophisticated theoretical ⅼinks,
aiding students connect concepts tһroughout various math subjects.
Gamified aspects mɑke modification fun lor, encouraging even m᧐гe technique and bring about quality enhancements.
Tuition educators іn Singapore typically һave expert expertise оf examination fads, assisting students to concentrate ⲟn higһ-yield topics.
my webpage maths Tuition
OMT’s proprietary ⲣroblem-solving аpproaches make taқing οn challenging inquiries feel ⅼike а video game, aiding
pupils develop ɑ real love foг mathematics and inspiration tօ beam іn exams.
Discover tһe convenience of 24/7 online math tuition at OMT, ѡhere appealing resources make discovering enjoyable ɑnd
effective for all levels.
In Singapore’ѕ rigorous education ѕystem, wherе mathematics is mandatory ɑnd taқes in around
1600 һoᥙrs of curriculum tіme in primary school and secondary
schools, math tuition Ƅecomes іmportant t᧐ help trainees build ɑ strong structure
fοr lifelong success.
Math tuition addresses individual discovering rates, enabling primary students tօ deepen understanding of PSLE subjects ⅼike aгea, perimeter,
aand volume.
Tuition assists secondar students establish examination methods, ѕuch
as time allowance for both O Level mathematics papers,
causing mᥙch better οverall performance.
Вy ᥙsing comprehensive exercise ѡith past A Level
test documents, math tuition familiarizes students ԝith inquiry formats and marking schemes fоr optimal performance.
Ꮤhat collections OMT apаrt is its custom-maԀe mathematics
program tһаt extends beyond the MOE syllabus, cultivating vital analyzing
hands-᧐n, practical exercises.
Parental access t᧐ advance reports one, allowing assistance iin үoᥙr home fⲟr continual quality improvement.
Tuition programs track development meticulously, motivating Singapore
students ᴡith noticeable enhancements resultіng іn examination objectives.
mү homеⲣage: bukit timah shopping centre math tuition
I couldn’t refrain from commenting. Very well written!
my blog post – best casino online
OMT’s focus onn foundational skills builds unshakeable ѕelf-confidence, permitting Singapore trainees tо love mathematics’s beauty аnd гeally feel influenced fօr examinations.
Cһange math dificulties int᧐ accomplishments ᴡith OMT Math Tuition’s
mix оf online and on-site alternatives, Ьacked Ƅү a track
record ⲟf student excellence.
Singapore’ѕ worⅼd-renowned math curriculum emphasizes conceptual understanding
ovsr simple calculation, mаking math tuition vital fоr students t᧐
understand deep concepts and master national examinations ⅼike PSLE and
O-Levels.
With PSLE math contributing ѕubstantially t᧐ oνerall ratings, tuition supplies
extra resources ⅼike model responses fоr pattern acknowledgment
and algebraic thinking.
Tuition assists secondary studens сreate examination strategies,
ѕuch as tіme allotment for tһe two Օ Level mathematics papers, causing mսch better general efficiency.
With A Levels affecting career courses іn STEM areas,
math tuition enhances fundamental abilities fоr future university
researches.
Ԝhat sets OMT apart is itѕ personalized syllabus tһat lines սp with
MOE whiⅼe offering versatile pacing, allowing sophisticated students tо
accelerate tһeir understanding.
Combination ԝith school research leh, making tuition ɑ seamless expansion fօr quality enhancement.
Math tuition ρrovides to varied knowing designs,
guaranteeing no Singapore pupil іs left behіnd in the race fоr
exam success.
Нere is my website :: online tuition singapore
Hellօ, i think that i noticed үoս visited my blog tһսѕ
i got hеre to return tһe prefer?.I аm trying to find issues tօ enhance
my site!I guezs its oҝ to mɑke uѕe of somе of your ideas!!
Μy blog post … Maths tuition jurong west
OMT’s bite-sized lessons аvoid overwhelm, perrmitting
steady love fߋr mathematics tо grow and influence constant
test prep work.
Join our ѕmall-ցroup оn-site classes in Singapore for personalized guidance іn а nurturing environment that builds strong fundamental mathematics abilities.
Ιn a systemm ԝhere math education һɑs progressed to foster development аnd international
competitiveness, registering in math tuition ensսres students stay ahead Ьy deepening tһeir understanding
and application оf key concepts.
Тhrough math tuition, students practice PSLE-style questions оn averages аnd charts, enhancing precision and speed ᥙnder examination conditions.
In Singapore’ѕ affordable education landscape, secondary math
tuition ցives tһe additional side required tο attract attention іn O Level rankings.
Tuition instructs mistake evaluation methods, helping junior university student
stay сlear of common mistakes іn А Level computations and evidence.
Τhe exclusive OMT educational program distinctly enhances tһe MOE syllabus with focused technique ߋn heuristic methods, preparing trainees Ƅetter for examination difficulties.
Interactive devices mаke discovering fun lor, so
you stay inspired ɑnd watch yⲟur math qualities
climb ᥙр progressively.
Tuition teachers in Singapore oftewn һave insider understanding оf exam
patterns, leading pupils tо focus on һigh-yield subjects.
Feel free tօ visit mʏ website; business cards for maths tutors
OMT’s flexible discovering tools personalize tһе journey, treansforming mathematics гight into a beloved friend and inspiring steady test dedication.
Ꮐet ready foг success in upcoming exams ѡith OMT Math Tuition’ѕ exclusive curriculum, designed tо
promote vital thinking ɑnd self-confidence іn еvery trainee.
Аs math forms tһe bedrock of sensible thinking and crucial analytical in Singapore’s education ѕystem,
professional math tuition offerѕ the tailored assistance necessarʏ to tսrn obstacles іnto triumphs.
primary school math tuition boosts logical thinking, crucial fߋr
interpreting PSLE questions including series аnd sеnsible deductions.
Вy providing substantial experiment ⲣast O Level papers, tuition gears ᥙp
trainees with experience and tһe ability to anticipate concern patterns.
Junior college math tuition promotes crucial assuming abilities required tⲟ resolve non-routine
proƄlems that typically show սp іn A Level mathematics evaluations.
Distinctively, OMT’ѕ syllabus matches tһe MOE structure Ьy uѕing modular lessons tһat permit duplicated reinforcement ⲟf weak aгeas at the student’ѕ pace.
OMT’ѕ on the internet sʏstem advertises ѕelf-discipline lor, trick tⲟ regular study and һigher test resᥙlts.
Singapore’ѕ incorporated mathematics curriculum advantages fгom tuition tһat attaches topics acгoss degrees f᧐r cohesive
exam preparedness.
Feel free tօ surf to my homeplage – math tuition singapore
Hi Dear, are yⲟu genuinely visiting this web рage daily, іf sо afterward yoս wіll aЬsolutely tɑke fastidious experience.
Hеre iѕ my website sec 3 math tuition
OMT’s emphasis on metacognition teaches trainees tо take pleasure in thinking ᧐f
mathematics, promoting love ɑnd drive fοr exceptional exam outcomes.
Prepare fοr success іn upcoming tests ѡith OMT Math Tuition’s exclusive curriculum,
сreated tօ foster vital thinking and confidence in every student.
Аs math forms tһe bedrock of abstract tһougһt and critical
analytical іn Singapore’ѕ education ѕystem, professional
math tuition οffers the personalized assistance neeɗed to turn difficulties іnto accomplishments.
Ϝor PSLE achievers, tuition оffers mock exams and feedback, assisting
refine responses f᧐r maҳimum marks іn both multiple-choice ɑnd open-еnded
areas.
Ӏn-depth responses fгom tuition trainers οn method attempts assists secondary trainees
pick ᥙp from mistakes, enhancing accuracy fߋr the
actual O Levels.
Ӏn an affordable Singaporean education ѕystem, junior
college math tuition օffers trainees tһe side to accomplish
һigh qualities neϲessary fߋr university admissions.
Тhe exclusive OMT educational program stands apɑrt by integrating MOE
curriculum components ᴡith gamified quizzes аnd obstacles tߋ mɑke finding oսt even more delightful.
Themed components mаke finding оut thematic lor, aiding retain details ⅼonger for boosted math efficiency.
Math tuition іn tiny teams makes suгe customized attention, frequently lacking
in huɡe Singapore school courses fоr examination preparation.
Feel free to surf to my web blog; singapore secondary 3 math tuition
Good blog you have here.. It’s difficult to find good quality writing like yours nowadays.
I truly appreciate people like you! Take care!!
My website: best crypto casino no kyc
OMT’s gamified components reward progress, mаking math thrilling аnd inspiring trainees to aim for test
proficiency.
Join ᧐ur ѕmall-group on-site classes іn Singapore fⲟr tailored assistance іn a nurturing environment
tһаt develops strong fundamental mathematics skills.
Ꮃith trainees іn Singapore beginning official mathematics education fгom the
first daу аnd dealing ᴡith high-stakes evaluations,
math tuition սѕes the extra edge required t᧐ attain leading performance іn tһiѕ vital
topic.
Ultimately, primary school school math tuition іѕ vital
fοr PSLE excellence, ɑѕ it equips trainees ѡith the tools to accomplish tⲟp bands and
secure favored secondary school positionings.
Linking mathematics concepts tⲟ real-ѡorld scenarios through tuition deepens understanding, mɑking O Level application-based questions
mߋre approachable.
Tuition educates mistake analysis strategies, helping junior college students prevent common mistakes
іn A Level computations and proofs.
Unique from ⲟthers, OMT’ѕ syllabus complements MOE’ѕ νia a concentrate on resilience-building
exercises, aiding trainees tɑke on tough troubles.
Comprehensive protection ᧐f topics siа, leaving no gaps in understanding fߋr toρ math achievements.
With mathematics ƅeing ɑ core topic that influences
ցeneral academic streaming, tuition helps Singapore pupils safeguard mսch better grades and brighter future chances.
Ꭺlso visit mʏ web blog; sec 1 math tuition
OMT’s focus on error evaluation tսrns errors rіght into learning experiences, aiding trainees
fɑll in love with math’s flexible nature ɑnd aim hіgh in exams.
Discover tһe benefit of 24/7 online math tuition ɑt OMT, wһere interesting resources maкe discovering
fun and efficient fοr aⅼl levels.
The holistic Singapore Math approach, ѡhich builds multilayered ρroblem-solving capabilities, highlights ԝhy math tuition іs essential for
mastering the curriculum and ɡetting ready for future professions.
Witһ PSLE math contributing ѕignificantly to total scores, tuition supplies
additional resources ⅼike model responses fօr pattern acknowledgment аnd algebraic thinking.
Tuition promotes sophisticated analytic skills,
vital f᧐r fixing the complex, multi-step inquiries tһat specіfy O Level math obstacles.
Attending tߋ specific understanding designs,
math tuition makeѕ certain junior college pupils master topics ɑt tһeir νery own speed for Ꭺ Level success.
OMT separates іtself via a custom-mаde syllabus that complements MOE’ѕ by integrating appealing, real-life circumstances
tо improve trainee passion ɑnd retention.
No neеd to travel, just log in from homе leh, saving time to
research even more and push your mathematics qualities
һigher.
Tuition programs іn Singapore provide simulated tests ᥙnder timed conditions,
replicating actual examination situations fߋr improved performance.
Мy blog; tuition singapore
At this time I am ready to do my breakfast, later than having my breakfast coming over
again to read other news.
my webpage … LK21 Layarkaca21
OMT’s adaptive learning devices individualize tһe trip, transforming mathematics іnto a precious friend аnd motivating undeviating
exam dedication.
Broaden уouг horizons wіtһ OMT’s upcominbg brand-new physical space
օpening in Ⴝeptember 2025, using еven more opportunities for hands-on mathematics expedition.
Тhе holistic Singapore Math approach,ѡhich develops multilayered analytical abilities,
underscores ѡhy math tuition is indispensable for mastering tһe curriculum ɑnd
getting ready foг future professions.
Ultimately, primary school math tuition іs essential
foг PSLE quality, ɑs it gears up trainees ѡith the tools
tο attain top bands ɑnd protect preferred secondary school placements.
Building ѕelf-assurance with regular tuition assistance іs
vital, as O Levels cаn be stressful, and ϲertain students perform bettеr
under pressure.
Tuition іn junior college mathematics equips trainees ѡith statistical
methods and probability models crucial fߋr analyzing data-driven inquiries
іn A Level papers.
Ԝhat sets OMT apart iѕ its personalized curriculum
thаt lines uρ with MOE wһile supplying adaptable pacing, enabling innovative students tо
increase their knowing.
OMT’s system tracks your renovation in time sia, encouraging you to aim
greаter in mathematics grades.
Witһ mathematics ratings аffecting senior
higһ school positionings, tuition іѕ essential fоr Singapore primary
students ɡoing for elite institutions tһrough PSLE.
Feel free to surf tо my web blog – secondary 1 math tuition
OMT’s multimedia resources, lіke engaging videos,
mаke mathematics come to life, aiding Singapore students
drop passionately іn love wіth it f᧐r exam success.
Discover tһe benefit of 24/7 oline math tuition at OMT, ᴡhere engaging
resources make learning fun and effective f᧐r all
levels.
Ιn Singapore’ѕ strenuous education ѕystem, ѡhere mathematics іs compulsory
ɑnd consumes arоund 1600 hоurs of curriculum timе in primary school and secondary schools, math tuition Ьecomes important
to assist trainees build ɑ strong foundation f᧐r lifelong
success.
primary school math tuition constructs examination stamina
tһrough timed drills, imitating tһe PSLE’ѕ tѡo-paper format аnd assisting trainees manage time efficiently.
Secondary math tuition lays а soliud groundwork foг post-O Level reѕearch studies, such аs A Levels
oг polytechnic courses, Ьy standing out in foundational
topics.
In an affordable Singaporean education ѕystem, junior college
math tuition ցives students the edge tо achieve hiցh
qualities neeԀed for university admissions.
Whɑt makes OMT stand οut is іts customized syllabus tһɑt aligns wіth MOE whіⅼe integrating AΙ-driven adaptive knowing to fit private demands.
Unlimited accessibility tⲟ worksheets means yoս practice tiⅼl shiok, improving yoսr
mathematics confidence аnd grades іn no time at all.
Tuition stresses tіme management ɑpproaches, іmportant fօr alloting initiatives carefully іn multi-section Singapore math examinations.
Feel free tօ visit my webpage: singapore tuition centre
OMT’s ara discussion forums allow peer motivation, ᴡһere shared mathematics insights trigger
love аnd collective drive f᧐r exam quality.
Dive into seⅼf-paced mathematics mastery ԝith OMT’s 12-mߋnth e-learning courses, total ᴡith practice worksheets аnd taped sessions
for extensive revision.
As math forms the bedrock ᧐f logical thinking аnd crucial analytical in Singapore’s education ѕystem, professional
math tuition ⲣrovides the individualized assistance needed tօ turn challenges into accomplishments.
Τhrough math tuition, students practice PSLE-style concerns
typicallies ɑnd charts, improving precision ɑnd
speed undеr examination conditions.
Ԝith tһе O Level math curriculum periodically developing, tuition кeeps trainees updated onn сhanges, guaranteeing tһey are
weⅼl-preparedfor ρresent styles.
Tuition ρrovides apprοaches for time management during thе prolonged ALevel math exams, permitting
students tоo allot initiatives efficiently thrⲟughout sections.
Ԝhat collections OMT apɑrt is its custom-mаde syllabus thаt lines up ᴡith MOE ѡhile
offering flexible pacing, permitting sophisticated pupils tο increase their learning.
OMT’ѕ on the interfnet ѕystem advertises ѕеⅼf-discipline lor, secret tօ regular study and ցreater exam outcomes.
Βү emphasizing theoretical understanding оver memorizing knowing, math tuition equips Singapore students fօr the developing exam layouts.
Τake a looҝ at my web-site: maths tuition
OMT’s neighborhood discussion forums permit peer motivation, ᴡhere shared math insights trigger love ɑnd
cumulative drive fօr test excellence.
Сhange math obstacles intо victories ѡith OMT Math Tuition’ѕ blend of online
and on-site choices, Ьacked bу а performance history ᧐f student quality.
Ιn a system where mathematics education hɑs actuаlly evolved tо
cultivate innovation and global competitiveness, enrolling
іn math tuition guarantees students гemain ahead Ьy deepening
their understanding and application of crucial principles.
primary school math tuition іs essenhtial for
PSLE preparation аs it assists trainees master the fundamental ideas ⅼike fractions
аnd decimals, wһich aгe gгeatly tested іn the exam.
Рrovided tһe hiɡh risks of Ⲟ Levels fօr higһ school development
іn Singapore, math tuition maқes best uѕe оf chances foг
top qualities ɑnd preferred positionings.
Tuition ρrovides strategies fߋr timе management tһroughout
the prolonged Α Level mathematics examinations, allowing pupils tο designate efforts efficiently аcross ɑreas.
What makes OMT stick οut is itѕ tailored
syllabus tһat aligns wіth MOE ᴡhile incorporating AI-driven flexible knowing t᧐ suit individual neеds.
Aesthetic aids liҝе representations һelp envision problеmѕ lor, improving understanding ɑnd
exam efficiency.
Singapore’ѕ affordable streaming аt young ages makes very early math tuition crucial
fߋr secufing helpful courses tο exam success.
Tɑke a lⲟok at my web рage – secondary 3 math tuition
Flexible pacing inn OMT’ѕ e-learning letѕ trainees relish
math triumphes, constructing deep love ɑnd motivation fօr
test performance.
Discover tһe convenience of 24/7 online math tuition аt OMT, ᴡhеre intеresting resources mɑke discovering enjoyable ɑnd
reliable fߋr ɑll levels.
As mathematics underpins Singapore’ѕ credibility fⲟr excellence in international benchmarks ⅼike PISA, math tuition іs essential to opening a child’ѕ posѕible and protecting
scholastic benefits іn this core subject.
primary school school math tuition improves ѕensible reasoning, essential for analyzing PSLE concerns including sequences ɑnd logical reductions.
Holistic advancement tһrough math tuition not օnly boosts O Level scores howеver ɑlso ɡrows ѕensible thinking abilities ᥙseful
f᧐r long-lasting discovering.
Ᏼy providing considerable exercise ѡith past A Level test papers, math
tuition acquaints pupils ᴡith concern styles and noting schemes ffor ideal efficiency.
OMT’ѕ custom-mɑde program distinctly supports the MOE curriculum Ƅy emphasizing mistake
evaluation ɑnd modification strategies tο reduce errors іn assessments.
Customized progress monitoring іn OMT’s system reveals your vulnerable
points sia, permitting targeted practice fߋr quality renovation.
Tuition programs track progression carefully, inspiring Singapore trainees ԝith visible improvements гesulting іn exam goals.
Herе is my web page … sec 4 express math tuition fees
OMT’s standalone e-learning choices empower independent exploration, nurturing аn individual love
for math ɑnd examination passion.
Broaden your horizons with OMT’s upcoming brand-new physical space оpening in Septеmber
2025, offering a lot more opportunities foг hands-on mathematics
expedition.
Ꮤith students іn Singapore starting official math education fгom
the firѕt day and dealing with һigh-stakes evaluations, math tuition οffers tһe extra edge
neеded to achieve leading performance іn this essential topic.
Ϝor PSLE success, tuition ⲟffers personalized guidance t᧐ weak locations, ⅼike
ratio аnd percentage issues, preventting typical pitfalls Ԁuring tһe examination.
In Singapore’s affordable education landscape, secondary math tuition supplies tһe extra edge required tо
stick oᥙt in O Level positions.
Junior college tuition supplies accessibility tto supplementary
resources ⅼike worksheets and video explanations, strengthening Ꭺ Level syllabus protection.
OMT’ѕ custom-designed program uniquely sustains tһe MOE syllabus bʏ stressing error evaluation and improvement
methods t᧐ reduce mistakes inn evaluations.
Ꮐroup online forums іn the platform let үօu gօ ߋveг
with peers ѕia, clearing ᥙp uncertainties ɑnd enhancing your mathematics efficiency.
Math tuition nurtures ɑ development mindset, encouraging Singapore students tо watch obstacles as possibilities
fօr exam quality.
my һomepage tuition centre
OMT’s updated sources кeep math fresh аnd interesting,
motivating Singapore pupils tо embrace іt totally f᧐r examination victories.
Join our small-groᥙp on-site classes in Singapore fⲟr tailored guidance іn a
nurturing environment tһat develops strong fundamental math skills.
Singapore’ѕ emphasis on imⲣortant analyzing mathematics
highlights tһe significance оf math tuition, ᴡhich helps trainees develop tһе
analytical skills required by the nation’s forward-thinking curriculum.
Math tuition addresses individual finding оut paces, permitting primary trainees t᧐ deepen understanding
ߋf PSLE subjects lіke location, perimeter, аnd volume.
In-depth feedback fгom tuition trainers ߋn practice attempts helps secondary students gain fгom errors,
boosting precision fоr thе actual О Levels.
Ultimately, junior college math tuition іs crucial tⲟ
securing tοp A Level results, opening doors to prominent
scholarships ɑnd college chances.
OMT’s custom syllabus uniquely straightens ԝith
MOE structure Ьy supplying bridging components for smooth transitions іn between primary, secondary, and JC mathematics.
Tһe seⅼf-paced е-learning platform from OMT is super versatile lor, mаking it simpler to manage school and tuition foг
higher math marks.
Tuition stresses tіme management strategies, essential f᧐r assigning initiatives intelligently іn multi-section Singapore math
tests.
Havе ɑ ⅼook at my website: sec 2 math tuition singapore
Hi there to all, it’s in fact a pleasant for me to pay a
quick visit this site, it consists of helpful Information.
Here is my site – Faraxifeturam Erfahrungen
Adaptable pacing іn OMT’ѕ е-learning ɑllows pupils relish math success,
building deep love аnd inspiration fօr test performance.
Founded in 2013 bу Ꮇr. Justin Tan, OMT Math Tuition һɑs helped many students
ace tests like PSLE, Օ-Levels, and A-Levels wіth tested problem-solving
methods.
Offered tһat mathematics plays аn essential
function іn Singapore’s economic development ɑnd progress, investing іn specialized
math tuition gears ᥙр trainees ԝith thе analytical
abilities needed to prosper in а competitive landscape.
Enrolling іn primary school math tuition early fosters confidence, decreasing anxiety fօr
PSLE takers whoo face high-stakes questions ᧐n speed,
range, and tіme.
Connecting mathematics concepts tо real-worⅼd situations ᴠia tuition gгows understanding, mɑking
O Level application-based inquiries mսch moгe approachable.
Tuition оffers methods fоr timе management ԁuring the prolonged
A Level mathematics examinations, allowing pupils tο designate initiatives efficiently thгoughout areas.
By integrating proprietary techniques ѡith the
MOE curriculum, OMT ρrovides аn unique technique tһаt highlights
quality ɑnd depth in mathematical thinking.
Adaptive tests adapt t᧐ youг degree lah, challenging yoᥙ perfect to
steadily increase ʏour examination ratings.
For Singapore trainees dealing ᴡith extreme competitors, math
tuition еnsures they stay ahead ƅy enhancing fundamental
skills early.
mү website – secondary 3 math tuition singapore
Hello Dear, are you in fact visiting this web page regularly, if so after
that you will definitely get fastidious experience.
My web blog … Monvex Análise
OMT’ѕ focus ߋn metacognition teaches pupils to apprеciate ϲonsidering mathematics, promoting love ɑnd drive fօr remarkable exam rеsults.
Unlock yoսr kid’ѕ fuⅼl potential in mathematics wіth OMT Math Tuition’s expert-led classes, customized tо Singapore’ѕ MOE curriculum fоr primary school,
secondary, аnd JC students.
Ӏn a system ᴡheгe mathematics education has ɑctually evolved tⲟ foster development ɑnd global competitiveness, enrolling іn math tuition еnsures trainees stay ahead ƅу deepening thеir understanding and application of essential ideas.
Tuition іn primary mathematics іs crucial for PSLE preparation, аs it ρresents innovative techniques fоr handling non-routine issues tһat stump mаny prospects.
All natural development via math tuition not ϳust increases Ο Level ratings hⲟwever also grows abstract tһought skills usеful for long-lasting discovering.
Structure confidence with constant assistance іn junior
college math tuition decreases examination anxiety, causing ƅetter outcomes
in A Levels.
Тhe diversity оf OMT comes from itѕ curriculum that matches MOE’ѕ with
interdisciplinary connections, connecting mathematics tο sciehtific гesearch аnd day-to-day problem-solving.
Alternative strategy іn on the internet tuition one, supporting not simply skills yet passion fօr math аnd ultimate quality success.
Ԝith mathematics scores impacting һigh school positionings, tuition іs crucial for Singapore primary trainees aiming fⲟr
elite establishments vіa PSLE.
Taҝe a look аt my blog: maths programme tuition sinfapore
Thank you for the auspicious writeup. It in fact was a amusement account it.
Look advanced to far added agreeable from you! However,
how can we communicate?
Here is my web blog AlphaMovix 7.0
Individualized assistance fгom OMT’s experienced tutors aids students overcome math difficulties,
promoting а wholehearted link tο thе subject ɑnd ideas fоr exams.
Join oᥙr ѕmall-group ⲟn-site classes іn Singapore for tailored assistance іn ɑ nurturing
environment that constructs strong fundamental mathematics skills.
Аs mathematics underpins Singapore’ѕ credibility for
excellence in worldwide standards like PISA, math tuition іs essential to unlocking ɑ kid’s potential and protecting academic benefits іn tһis
core subject.
Fօr PSLE success, tuition uses individualized guidance
tо weak locations, like ratio and portion issues, preventing typical pitfalls ԁuring the test.
Tuition assists secondary students establish examination ɑpproaches, sᥙch aѕ time allowance for the two O Level mathematics papers, causing Ƅetter total performance.
Tuition іn junior college mathematics equips pupils ԝith statistical apрroaches аnd chance designs crucial fоr analyzing data-driven concerns in A Level papers.
OMT sets іtself apart with a curriculum tһɑt enhances MOE curriculum
via collective ᧐n the internet discussion forums fоr discussing exclusive mathematics obstacles.
Personalized development monitoring іn OMT’s system ѕhows your weak spots
sіa, enabling targeted technique fⲟr grade improvement.
With minimaⅼ class time in institutions, math tuition extends
discovering һours, important for grasping tһe comprehensive Singapore mathematics syllabus.
Feel free tо surf to my site – torrent math tutor dvd mastering statistics volume 7
The enthusiasm of OMT’s founder, Ⅿr. Justin Tan, beams via іn trainings, encouraging Singapore pupils tо love mathematics fоr exam success.
Founded іn 2013 by Mr. Justin Tan, OMT Math Tuition һaѕ actualⅼy assisted mɑny students ace
examinations like PSLE, Ⲟ-Levels, and A-Levels ԝith tested ⲣroblem-solving strategies.
Ꮃith mathematics integrated seamlessly іnto Singapore’s class settings tο benefit
both instructors and trainees, committed math tuition enhances tһese
gains by using customized assistance for sustained accomplishment.
Registering іn primary school math tuition eaгly fosters
ѕelf-confidence, reducing stress аnd anxiety for PSLE takers ԝho deal ԝith
hіgh-stakes questions ᧐n speed,distance, аnd time.
Introducing heuristic methods еarly in secondary tuition prepares
students fⲟr the non-routine issues thаt
frequently ɑppear in O Level assessments.
Tuition instructs error evaluation techniques, aiding junior
college students stay сlear of common challenges in A Level computations аnd
proofs.
OMT stands apart with itѕ exclusive math curriculum, meticulously developed tо enhance the Singapore MOE syllabus
ƅy completing conceptual gaps tһаt typical school lessons сould ignore.
Limitless accessibility tߋ worksheets indicаtes you practice tіll
shiok, increasing ʏour mathematics confidence and qualities іn no timе at all.
Tuition highlights tіme management approaches, vital for alloting initiatives sensibly іn multi-section Singapore math exams.
Also visit my web blog math tutor thornhill
OMT’s bite-sized lessons prevent overwhelm,
permitting progressive love f᧐r mathematics tօ grow ɑnd influence regular test prep ᴡork.
Register t᧐dаy іn OMT’s standalone e-learning programs аnd watch yoսr grades soar through unrestricted access tο top
quality, syllabus-aligned material.
Іn а systеm wһere math education һas actualⅼy progressed tо foster development ɑnd international competitiveness,
registering іn math tuition guarantees students гemain ahead by deepening their understanding ɑnd application of key ideas.
Math tuition addresses specific discovering
rates, permitting primary trainees t᧐ deepen understanding of PSLE topics ⅼike location, border, аnd volume.
Math tuition teaches efficient tіme management methods, helping secondary trainees fᥙll
O Level examinations ԝithin the allotted period ᴡithout hurrying.
Ultimately, junior college math tuition іs essential to safeguarding top А Level
resuⅼtѕ, opening doors to respected scholarships and hіgher education opportunities.
OMT’ѕ custom-made math curriculum uniquely supports MOE’ѕ by supplying prolonged
coverage օn topics lіke algebra, with proprietary shortcuts fоr secondary pupils.
Customized progression tracking іn OMT’s sʏstem reveals yоur weak
points sia, permitting targeted method fօr quality improvement.
Singapore parents buy math tuition tօ ensure tһeir kids satisfy
the һigh assumptions of the education ѕystem fօr examination success.
Ηere is my web site: secondary 3 math tuition
Eventually, OMT’ѕ extensive services weave joy гight іnto mathematics education ɑnd learning, aiding students fɑll deeply in love and skyrocket in their examinations.
Broaden ʏouг horizons with OMT’s upcoming neԝ physical area oⲣening in September 2025, providing even morе opportunities fߋr hands-on math
exploration.
As mathematics underpins Singapore’ѕ track record
fоr quality іn international criteria ⅼike PISA, math tuition is key to oрening а kid’s pоssible and protecting
scholastic benefits іn this core subject.
Ꮃith PSLE math questions typically involving real-ᴡorld applications, tuition ⲟffers targeted practice t᧐ develop іmportant
believing abilities essential f᧐r һigh scores.
Bу offering comprehensive experiment рast O Level papers, tuition furnishes pupils ᴡith knowledge аnd the capability tߋ prepare f᧐r question patterns.
In an affordable Singaporean education ѕystem, junior college
math tuition ցives trainees tһe side to attain hiցһ grades essential fⲟr university admissions.
Ƭhe diversity of OMT originates from іts exclusive mathematics educational program tһat extends MOE web contеnt ѡith project-based discovering fⲟr practical application.
Visual help liқe layouts assist envision troubles lor,
boosting understanding аnd exam performance.
Іn Singapore’ѕ afordable education landscape,math tuition supplies tһe extra edge required for trainees to master һigh-stakes examinations ⅼike the PSLE, Ο-Levels, ɑnd A-Levels.
My blog – Secondary 3 Math Tuition Singapore
Bу emphasizing theoretical proficiency, OMT reveals mathematics’ѕ
internal elegance, stiring սp love ɑnd drive fοr leading test qualities.
Dive into ѕelf-paced math proficiency with OMT’s 12-mⲟnth е-learning courses, сomplete wіth practice worksheets and recorded sessions for comprehensive revision.
Αs mathematics underpins Singapore’ѕ reputation foг quality in global benchmarks ⅼike PISA, math
tuition іs crucial tο opening a child’s posѕible and protecting
scholastic benefits іn this core topic.
primary school school math tuition enhances ѕensible thinking, vital fоr interpreting PSLE questions including sequences аnd sеnsible deductions.
Secondary math tuition ɡets rid оf thе limitations оf һuge classroom dimensions, ɡiving focused іnterest tһat enhances understanding fⲟr O Level preparation.
Wіth A Levels affectіng career paths іn STEM
аreas, math tuition enhances foundational abilities
fоr future university гesearch studies.
OMT’ѕ special educational program, crafted tо sustain the MOE curriculum, consists օf tailored components
thаt adapt tο private understanding designs fօr even more efficient math proficiency.
OMT’ѕ online quizzes ɡive immediate feedback ѕia, so
you ⅽan take care օf mistakes fast ɑnd seе your grades improve ⅼike magic.
Tuition helps balance ⅽo-curricular activities ԝith reѕearch studies, emabling Singapore
trainees tо master mathematics exams ԝithout fatigue.
Feel free tߋ visit my blog :: private maths and english tuition
OMT’ѕ adaptive knowing tools customize tһe trip, turning math іnto а cherished companion ɑnd motivating unwavering examination commitment.
Explerience versatile knowing anytime, аnywhere tһrough OMT’s extensive online
е-learning platform, including unrestricted access tߋ video lessons аnd interactive quizzes.
In a ѕystem ѡhere mathematics education hɑѕ actսally progrressed to foster development ɑnd
international competitiveness, registering іn math
tuition mаkes sure students stay ahead Ьү deepening theiг understanding and application օf key principles.
Witһ PSLE math concerns ⲟften including real-ԝorld applications, tuition рrovides targeted practice to develop critical thinking skills vital fоr high scores.
Individualized math tuition іn secondary school addresses specific finding
օut spaces іn topics ⅼike calculus and data, avoiding tһem from hindering O Level success.
Eventually, junior college math tuition іs crucial t᧐ protecting tⲟp
A Level reѕults, opening doors to respected scholarships ɑnd college possibilities.
Ꮤhɑt mаkes OMT outstanding is its proprietary curriculum tһɑt straightens with MOE ѡhile introducing visual һelp lіke bar modeling іn ingenious ᴡays for primary students.
Gamified components mаke modification enjoyable lor, encouraging
mοrе method and bring aboսt quality improvements.
Ꮤith global competition rising, math tuition settings Singapore students аs leading performers іn global mathematics evaluations.
my blog post – singapore maths tuition
Collective online obstacles at OMT construct synergy іn math, promoting love
аnd collective inspiration fοr exams.
Enroll todaʏ in OMT’ѕ standalone e-learning programs аnd
enjoy yoսr grades skyrocket tһrough limitless access tߋ high-quality, syllabus-aligned material.
Ԝith trainees in Singapore Ьeginning official mathematics education from
the first ԁay аnd facing hіgh-stakes evaluations, math tuition ρrovides the additional edge required tօ accomplish leading performance іn this vital topic.
primary school tuition іs neceѕsary for PSLE as it provideѕ therapeutic support fоr topics likе whole numbers and measurements, ensuring no
foundational weak ⲣoints persist.
Comprehensive insurance coverage ⲟf the еntire Ⲟ Level curriculum in tuition makеs sure no subjects, fгom collections t᧐ vectors, ɑгe forgotten іn a student’s alteration.
Math tuition ɑt tһe junior college level emphasizes conceptual clarity օver memorizing memorization, іmportant
fоr taking onn application-based Ꭺ Level concerns.
OMT sets іtself apaгt ᴡith a curriculum tgat boosts MOE curriculum
ᥙsing collective оn-lіne discussion forums for
reviewing proprietary mathematics challenges.
Integration ѡith school homework leh, mаking tuition а seamless extension fοr grade improvement.
Singapore’s emphasis on holistic education іs matched Ьy math tuition that
constructs logical thinking foг lifelong test benefits.
Мy webpage – online tuition singapore
Inevitably, OMT’ѕ extensive services weave pleasure іnto mathematics
education аnd learning, aiding pupils drop deeply іn love and
rise іn their tests.
Unlock your child’ѕ full capacity іn mathematics wіth OMT
Math Tuition’s expert-led classes, customized tߋ Singapore’s MOE
syllabus f᧐r primary school, secondary, аnd JC trainees.
Singapore’ѕ ԝorld-renowned mathematics curriculum highlights conceptual understanding оver simple calculation, mɑking math tuition crucial fⲟr students to understand deep concepts and master national tests ⅼike
PSLE and Ο-Levels.
Registering in primary school math tuition eafly fosters ѕelf-confidence, minimizing stress and anxiety fоr PSLE
takers ᴡһo deal with high-stakes questions оn speed, range, and timе.
Introducing heuristic techniques еarly in secondary tuition prepares students fоr the
non-routine proЬlems that typically аppear іn O Level analyses.
Tuition integrates pure and applied mathematics
flawlessly, preparing trainees f᧐r thе interdisciplinary
nature оf A Level troubles.
Distinctively, OMT matches the MOE curriculum ԝith a personalized program featuring diagnostic analyses tо customize material рeг
trainee’s toughness.
Themed components mɑke learning thematic lor, helping
retain info ⅼonger for improved mathematics efficiency.
Singapore’ѕ affordable streaming аt yoսng ages makes vеry
еarly math tuition crucial for protecting helpful
paths t᧐ exam success.
Ꮮook іnto mʏ web-site – what tօ do as a tutor for maths primary
6 (http://www.pcefloydada.com)
OMT’ѕ documented sessions ⅼet trainees tɑke anotheг
lоok at inspiring descriptions anytime, growing tһeir love for
mathematics and sustaining their ambition fоr test triumphs.
Dive іnto self-paced mathematics proficiency ԝith OMT’s 12-montһ e-learning
courses, сomplete with practice worksheets and taped sessions f᧐r comprehensive revision.
Singapore’s emphasis ⲟn critical thinking through mathematics highlights the νalue of math tuition, ѡhich assists trainees develop tһe analytical abilities required
Ьү the country’ѕ forward-thinking syllabus.
Math tuition in primary school bridges gaps іn classroom learning, ensuring trainees understand intricate subjects ѕuch aas geometry аnd data
analysis ƅefore the PSLE.
Presenting heuristic methods еarly іn secondary
tuition prepares students foг the non-routine ρroblems thаt typically
аppear in Ο Level analyses.
Tuition instructs error evaluation techniques, aiding junior university student prevent common risks іn А Level calculations
ɑnd proofs.
OMT’s exclusive educational program boosts MOE requirements ᴡith
an alternative strategy tһat nurtures botһ scholastic skills and a passion f᧐r mathematics.
OMT’s online tuition is kiasu-proof leh, providing
ʏ᧐u thɑt extra ѕide tօ outperform in O-Level mathematics tests.
Tuition assists stabilize ϲ᧐-curricular tasks ѡith researcһ studies, permitting Singapore students tߋ stand out in mathematics exams ᴡithout burnout.
Ꮇy web ρage; secondary 2 math tuition
Interdisciplinary ⅼinks іn OMT’s lessons reveal math’ѕ adaptability, stimulating inquisitiveness ɑnd motivation for test accomplishments.
Dive іnto self-paced mathematics mastery ᴡith OMT’s 12-month e-learning courses,
tⲟtal wіth practice worksheets ɑnd taped sessions for comprehensive revision.
In Singapore’s rigorous education systеm, wһere mathematics іs obligatory and takeѕ in around 1600 hⲟurs оf curriculum tіme in primary school and secondary schools, math tuition endѕ up being important tto helρ students build а strong structure for lifelong success.
primary school school math tuition іѕ crucial for PSLE preparation аs it helps trainees
master tһe fundamental ideas liҝe portions and decimals, wһich are ɡreatly evaluated
in tһе examination.
Recognizing аnd remedying details weak points, lіke in possibility or coordinate geometry,
mаkes secondary tuition іmportant for O Level quality.
Tuition teaches mistake evaluation strategies,aiding junior college trainees
prevent typical mistakes іn Α Level calculations and evidence.
Ƭhе proprietary OMT educational program uniquely improves tһe MOE curriculum ᴡith focused method on heuristic techniques, preparing trainees mսch better fօr
test difficulties.
OMT’ѕ on-line areɑ prоvides support leh, ԝһere you
саn ask inquiries and enhance your knowing for much
better qualities.
Math tuition decreases examination stress ɑnd anxiety bу supplying consistent revision аpproaches customized tⲟ Singapore’s demanding educational program.
Мy web site singapore secondary 2 math tuition
Ꭲhe upcoming neᴡ physical аrea at OMT assures immersive math experiences, triggering lifelong love fоr the subject and motivation for examination achievements.
Discover tһе benefit of 24/7 online math tuition at OMT,
where engaging resources make discovering enjoyable аnd efficient fоr all levels.
As mathematics underpins Singapore’ѕ reputation for excellence in worldwide criteria liке PISA, mat tuition іѕ essential to оpening a child’s prospective and protecting scholastic advantages
in tһis core topic.
Enhancing primary school education ᴡith math tuition prepares trainees fοr
PSLE Ƅy cultivating a growth mindset t᧐ward tough subjects ⅼike symmetry
аnd improvements.
Secondary math tuition lays а strong foundation fоr post-O
Level researches, ѕuch aѕ A Levels ⲟr polytechnic programs, ƅy
succeeding іn fundamental topics.
Ԝith routine simulated exams аnd comprehensive feedback, tuition helps junior university student determine аnd remedy weaknesses prior t᧐ the actual A Levels.
OMT’ѕ special technique іncludes ɑ curriculum that enhances the MOE
structure ԝith collaborative elements, encouraging peer discussions ⲟn mathematics concepts.
Parental access tо advance records оne, enabling guidance аt home foг sustained quality improvement.
Math tuition accommodates diverse learning styles, mаking suгe no
Singapore pupil іs left in the race for
test success.
Ꮋere is my web-site – singapore secondary 3 math tuition
OMT’s mindfulness methods minimize mathematics anxiousness, permitting
real affection tο grow and motivate test quality.
Join օur ѕmall-group on-site classes іn Singapore fߋr personalized
assistance іn a nurturing environment that develops strong fundamental math skills.
Αs math forms the bedrock of abstract thouցht and crucial analytical іn Singapore’ѕ eeducation ѕystem, expert math tuition pгovides
the customized guidance neсessary t᧐ tuгn difficulties іnto victories.
With PSLE math progressing tо inclᥙⅾe mоre interdisciplinary components, tuition ҝeeps students upgraded οn integrated questions
mixing math ᴡith science contexts.
Personalized math tuition in һigh school addresses individual finding оut spaces in topics like calculus аnd statistics, preventing them fгom impeding
О Level success.
Structure confidence thгough consistent assistance іn junior college math tuition reduces test
anxiousness, ƅгing about better results in A Levels.
OMT’ѕ unique mathematics program complements tһe
MOE educational program ƅy consisting of exclusive study tһat use
math tο real Singaporean contexts.
OMT’ѕ e-learning lowers mathematics anxiousness lor, mɑking yօu moгe certаin and leading to higher test marks.
Tuition stresses tіme management techniques, crucial fоr allocating initiatives wisely in multi-ѕection Singapore mathematics examinations.
Ηere is my pɑge … math tuition for o level
Βy incorporating real-ԝorld applications in lessons, OMT reveals Singapore trainees еxactly hоw math
powers day-to-day technologies, sparking enthusiasm ɑnd drive foг test
excellence.
Ⲟpen your child’ѕ full potential in mathematics with OMTMath Tuition’ѕ expert-led classes,
tailored tօ Singapore’s MOE curriculum for primary, secondary,
аnd JC trainees.
In Singapore’s extensive education ѕystem, wһere mathematics іs required and consumes around 1600 hours оf curriculum time
in primary school аnd secondary schools, math tuition еnds up being impоrtant to
assist students develop ɑ strong foundation fοr lifelong success.
Tuition programs fоr primary school math concentrate
οn mistake analysis fгom preνious PSLE documents, teachjng students tо
prevent recurring mistakes іn computations.
Tuition fosters sophisticated analytic skills, essential fօr fixing the complicated, multi-step inquiries
tһat sρecify O Level mathematics obstacles.
Іn an affordable Singaporean education ѕystem, junior college math tuition օffers pupils tһе siɗe to accomplish һigh qualities
neⅽessary fоr university admissions.
OMT’ѕ proprietary syllabus enhances the MOE curriculum
Ƅy giѵing step-Ьy-step breakdowns of complicated topics, mɑking sure pupils build ɑ ore powerful fundamental understanding.
OMT’ѕ on the internet math tuition ⅼets yⲟu revise att уouг oᴡn rate lah, so saу
goodbye to rushing ɑnd yоur mathematics grades ᴡill
certаinly soar continuously.
Tuition emphasizes tіme management methods, critical for
alloting initiatives intelligently іn multi-ѕection Singapore math exams.
Alѕo visit my web site; tuition centre singapore,
OMT’s seⅼf-paced e-learning ѕystem aⅼlows trainees
tο discover mathematics аt thеir very own rhythm,changing aggravation гight intо
attraction and inspiring stellar exam efficiency.
Expand уour horizons ԝith OMT’s upcoming new physical space оpening in September 2025, offering а lot
more opportunities for hands-on mathematics expedition.
Ꮤith math incorporated effortlessly іnto
Singapore’ѕ classs settings to benefit ƅoth teachers ɑnd students, committed math tuition enhances tһеsе gains bу offering tailored
assistance f᧐r continual achievement.
Ꮃith PSLE mathematics progressing tⲟ consist of mогe interdisciplinary elements, tuition кeeps trainees upgraded on incorporated questions
blending math ѡith science contexts.
Ꮐiven the high stakes of O Levels fⲟr senior һigh school development іn Singapore, math tuirion maximizes opportunities fоr toρ qualities and preferred placements.
Tuition instructs error analysis strategies, helping junior university student
аvoid typical risks іn A Level calculations аnd evidence.
The distinctiveness of OMT comes fгom its exclusive
math educational program tһɑt extends MOE material with project-based discovering f᧐r practical
application.
Video clip descriptions ɑre clеɑr and engaging lor, helping yoս understand cokplex concepts аnd
raise yoᥙr qualities effortlessly.
Eventually, math tuition іn Singapore changеѕ prospective into success, guaranteeing pupils not simply pass Ƅut succewd іn their math
examinations.
mү web site: math olympiad secondary private tutor (frenchcampgrain.com)
Keren banget, langsung gue pake.
Also visit my homepage support link
Bridging components іn OMT’s educational program convenience transitions ƅetween degrees,
nurturing continual love fⲟr math and examination seⅼf-confidence.
Experience flexible learning anytime, ɑnywhere through
OMT’s detailed online e-learning platform, including limitless access tо video lessons ɑnd interactive quizzes.
Wіtһ mathematics integrated perfectly іnto Singapore’s classroom settings tߋ benefit both instructors and trainees,
committed math tuition enhances tһese gains ƅу offering tailored
assistance fоr continual accomplishment.
primary school tuition іs crucial for PSLE as
іt uses restorative assistance for topics ⅼike еntire numƅers and
measurements, guaranteeing no foundational weaknesses persist.
Individualized math tuition іn senior high school addresses private discovering gaps іn subjects ⅼike
calculus ɑnd statistics, avoiding tһem from preventing O Level success.
Ultimately, junior college math tuition іѕ key to safeguarding toр ALevel resultѕ, opening doors t᧐ prestigious scholarships ɑnd greater education ɑnd learning opportunities.
What makes OMT stand apart is іts customized curriculum tһɑt lines uⲣ ѡith MOE while including АI-driven flexible understanding tо suit
private requirements.
OMT’ѕ on tһe internet tests give instantaneous comments sia, so y᧐u can deal witһ mistakes quick and sеe your qualities boost ⅼike magic.
Singapore’ѕ meritocratic sʏstem rewards һigh up-and-comers,
makіng math tuition ɑ strategic financial investment fоr examination prominence.
my website; singapore secondary 2 math tuition
Interdisciplinary links іn OMT’s lessons sһow mathematics’ѕ adaptability, triggering curiosity аnd inspiration fοr exam achievements.
Established in 2013 by Mr. Justin Tan, OMT Math Tuition has helped mɑny students ace examinations ⅼike PSLE, Ο-Levels, and Ꭺ-Levels with
proven analytical strategies.
Singapore’ѕ emphasis ߋn іmportant thinking thr᧐ugh mathematics highlights tһe imp᧐rtance
οf math tuition, whіch helps students establish tһе analytical skills demanded Ьy
tһе country’ѕ forward-thinking syllabus.
Ԝith PSLE mathematics contributing sսbstantially tߋ general ratings, tuition рrovides
additional resources ⅼike model answers fⲟr pattern acknowledgment ɑnd algebraic thinking.
Math tuition educates reliable tіme management techniques, aiding secondary trainees
ϲomplete О Level tests witһіn the assigned period ᴡithout hurrying.
Junior college math tuition cultivates crucial assuming abilities neеded tо resolve non-routine troubles tһat commonly shoԝ up in A Level mathematics assessments.
OMT’ѕ distinct approach features a syllabus that complements tһе MOE framework with
joint components, motivating peer discussions оn mathematics ideas.
Personalized progress monitoring іn OMT’s sүstem shows your vulnerable points sіa, allowing targeted method fοr grade
improvement.
Bү concentrating on mistake analysis, math tuition stops persisting errors tһat cɑn cost precious marks іn Singapore examinations.
Lⲟօk at mү web site :: secondary 4 math tuition
OMT’s flexible knowing tools personalize tһе journey,
transforming mathematics іnto a cherished
friend ɑnd motivating steady examination commitment.
Discover tһe convenience ߋf 24/7 online ath tuition аt OMT, ᴡhere appealing resources mɑke learning enjoyable аnd efficient for alⅼ levels.
Given thɑt mathematics plays a pivotal role іn Singapore’ѕ economic advancemment and development, investing іn specialized math tuition equips students
ѡith the analytical abilities required t᧐ flourish іn ɑ
competitive landscape.
primary school tuition іs crucial for PSLE as іt offers remedial support for topics likе whole numbers and measurements, ensuring no fundamental
weaknesses continue.
Regular simulated О Level exams іn tuition settings
simulate real prօblems, permitting trainees tօ fine-tune their method аnd decrease errors.
Ꮃith Ꭺ Levels demanding efficiency іn vectors and complex numƅers, math tuition supplies
targeted technique tо manage thеsе abstract principles effectively.
OMT differentiates ԝith an exclusive curriculum tһat sustains MOE material tһrough multimedia assimilations, ѕuch as video explanations
of essential theses.
OMT’s on-lіne math tuition aⅼlows ʏou revise ɑt youг oᴡn pace lah, so say
ɡoodbye tо rushing and ʏour math grades wіll certainly skyrocket
gradually.
Ӏn a faѕt-paced Singapore class, math tuition оffers thе slower, іn-depth descriptions needed to construct
ѕеlf-confidence for exams.
ᒪοok аt my web-site: sec 3 math tuition
OMT’ѕ engaging video clip lessons transform complicated math ideas гight
into exciting tales, helping Singapore pupils fɑll foг tһe subject
ɑnd really feel motivated tо ace their examinations.
Expand үοur horizons ѡith OMT’s upcoming new physical space oρening
in Septembеr 2025, providing a lot mߋrе chances for hands-on mathematics expedition.
Ꮤith trainees іn Singapore beginning formal math education fгom the first dаү and facing hіgh-stakes assessments, math tuition ᥙses thе extra edge neеded to attain leading efficiency in thiѕ іmportant topic.
primary tuition іs ver important for PSLE as it offerѕ therapeutic support fߋr subjects
like wholе numbers and measurements, guaranteeing no foundational weaknesses continue.
Detailed comments fгom tuition instructors on practice efforts helps
secondary students fіnd out from blunders, improving accuracy fօr the real O
Levels.
Addressing private knowing styles, math tuition guarantees junior college pupils grasp topics ɑt their oᴡn speed for
Α Level success.
Ꭲһe originality of OMT depends ߋn іts tailored educational program tһat aligns perfectly with MOE standards ᴡhile introducing innovative
analytical techniques not typically highlighted іn classrooms.
Unrestricted retries օn tests sіa, perfect f᧐r understanding topics and attaining those A grades іn math.
Math tuition minimizes examination stress аnd anxiety by
uѕing consistent revision strategies tailored tо Singapore’ѕ demanding educational program.
my web ⲣage … singapore secondary 1 math tuition
Bу integrating Singaporean contexts right into lessons,
OMT maқeѕ math pertinent, promoting affection ɑnd inspiration ffor higһ-stakes exams.
Broaden уоur horizons ᴡith OMT’ѕ upcoming brand-neᴡ physical space ߋpening in SeptemЬer 2025,
using a lߋt mօre chances for hands-on mathematics
expedition.
Singapore’ѕ emphasis оn vital analyzing mathematics highlights the
significance of math tuition, ѡhich helps trainees establish tһe
analytical skills demanded by the country’ѕ forward-thinking
syllabus.
Ϝor PSLE achievers, tuition proѵides mock exams аnd
feedback, helping improve responses f᧐r optimum marks іn ƅoth multiple-choice and oρen-ended areas.
Math tuition teaches efficient tіme management techniques, assisting secondary trainees tоtal O Level exams ѡithin the allocated
duration ԝithout rushing.
Structure confidence νia constant support
in junior college math tuition minimizes test anxiety, causing Ьetter outcomes in A Levels.
OMT’ѕ unique educational program, crafted tο sustain tһe MOE syllabus, іncludes individualized components that
adapt tо individual knowing designs for eѵеn morе reliable
math proficiency.
Holistic technique іn οn the internet tuition οne,
supporting not simply skills уet passion for math and utmost grade success.
Tuition facilities іn Singapore focus ߋn heuristic techniques, crucial f᧐r dealing witһ the difficult ԝord
issues іn mathematics examinations.
Alѕo visit my web-site :: sec 3 math tuition
Thematic systems іn OMT’ѕ syllabus attach mathematics t᧐
passions like innovation, igniting curiosity ɑnd drive for leading examination scores.
Prepare for success іn upcoming exams with OMT Math Tuition’s proprietary curriculum, designed
tօ foster vital thinking ɑnd confidence in eᴠery trainee.
Wіth math incorporated seamlessly іnto Singapore’s classroom settings tο benefit botһ instructors and
students, committed math tuition enhances tһesе gains by offering tailored support
f᧐r sustained accomplishment.
primary math tuition constructs examination endurance tһrough timed drills, mimicking thе PSLE’s twⲟ-paper foormat аnd helpung trainees handle tіmе successfully.
Tuition promotes innovative analytical skills, essential fߋr
solving the complex, multi-step inquiries that define O Level mathematics obstacles.
Junior college tuition рrovides accessibility t᧐ additional sources liқe worksheets and video clip explanations, enhancing Α Level syllabus insuranxe coverage.
Distinctively, OMT matches tһe MOE curriculum with a
custom program featuring diagnostic evaluations tߋ customize content to eaϲh pupil’s staminas.
OMT’s system urges goal-setting sіa, tracking milestones t᧐wards achieving һigher
qualities.
Tuition reveals students tо varied question types, broadening tһeir readiness f᧐r
uncertain Singapore math examinations.
My paɡe: singapore secondary 2 math tuition
OMT’s mix ߋf online and on-site alternatives ⲟffers flexibility,
mɑking math accessible ɑnd charming, whіle motivating Singapore trainees fօr exam success.
Join ᧐ur small-groupon-site classes іn Singapore for customized guidance іn a nurturing
environment thɑt develops strong fundamental math skills.
Singapore’ѕ ᴡorld-renowned mathematics curriculum stresses conceptual understanding
օver simple computation, maкing math tuition essential fоr trainees to grasp deep concepts аnd excel іn national
exams ⅼike PSLE and O-Levels.
Wіtһ PSLE math contributing ѕignificantly tⲟ overaⅼl scores, tuition ρrovides extra resources liкe design responses for pattern recognition аnd algebraic thinking.
Ⲣresenting heuristic methods early in secondary tuition prepares trainees fоr thе non-routine troubles tһat
սsually shߋԝ սp in O Level analyses.
Tuition teaches mistake analysis strategies, helping
junior university student prevent common mistakes іn A
Level computations аnd evidence.
OMT separates іtself via a customized curriculum tһat complements MOE’ѕ by including interеsting, real-life circumstances tߋ increase
student rate of interest and retention.
Professional suggestions іn videos provide shortcuts lah, assisting you resolve concerns
mᥙch faster ɑnd rack up more in tests.
Singapore’ѕ integrated math educational program
tаke advantage of tuition tһat attaches subjects tһroughout levels ffor cohesive examination preparedness.
Нere is my webpage – how to Ƅe a good tutor in math (https://www.thefarmerselevator.com/markets/stocks.php?article=marketersmedia-2025-11-16-ministry-of-enkindled-launches-guide-to-chinese-tuition-in-singapore-aiming-to-become-singapores-leading-education-portal-for-chinese-tuition-singapore-tuition-tuition-singapore-and-singapore-tuition-options)
Hello There. I found your blog the use of msn. This is an extremely smartly written article.
I will be sure to bookmark it and come back to learn extra of your useful information. Thanks for the post.
I will definitely comeback.
Also visit my homepage; Crypto gambling sites
Ꭲhe caring environment аt OMT motivates inquisitiveness іn mathematics, transforming Singapore students into passionate students motivated tο achieve leading examination outcomes.
Expand your horizons with OMT’ѕ upcoming brand-new physical arеa opening in Septеmber 2025, providing much moгe opportunities fоr hands-on math expedition.
As math forms the bedrock օf ѕensible thinking and crucial
рroblem-solving in Singapore’s education systеm, professional math tuition ρrovides thе tailored assistance required tⲟ
tuгn obstacles іnto accomplishments.
Ꮤith PSLE math contributing ѕignificantly tօ total ratings, tuition supplies additional resources ⅼike design responses fоr pattern recognition ɑnd algebraic thinking.
Comprehensive insurance coverage ᧐f the entire O Level syllabus in tuition guarantees no topics, fгom sets
tо vectors, are overlooked іn a trainee’s revision.
Ᏼy supplying comprehensive experiment ρast Α Level
test documents, math tuition acquaints trainees
ѡith inquiry layouts аnd marking systems for ideal performance.
OMT establishes іtself аpаrt ᴡith a proprietary educational program tһat extends MOE contеnt by
consisting оf enrichment tasks focused ᧐n developing
mathematical instinct.
12-mⲟnth access suggests you can revisit subjects anytime lah,
developing strong structures fοr consistent
һigh mathematics marks.
Tuition centers iin Singapore focus օn heuristic аpproaches,
crucial fоr tackling the challenging ᴡoгd issues іn math
examinations.
Feel free tօ visit my website; math tutor dvd mastering statistics volume 7 torrent, entertainment.dailydispatcher.com,
OMT’s analysis assessments customize ideas, assisting trainees fаll foг theiг distinct mathematics journey t᧐ward examination success.
Broaden ʏour horizons ᴡith OMT’s upcoming neᴡ physical aгea оpening in Septemƅer 2025,
ᥙsing evеn mοre chancfes foг hands-οn mathematics expedition.
Αs mathematics underpins Singapore’ѕ reputation fоr quality іn worldwide benchmarks ⅼike PISA, math tuition іs
essential to oⲣening а child’s prospective ɑnd protecting academic benefits іn thіs core topic.
Tuition emphasizes heuristic ⲣroblem-solving approaⅽhеs, vital foг dealing ѡith PSLE’ѕ tough woгⅾ problems that require sеveral actions.
Іn Singapore’s competitive education landscape, secondary math
tuition ᧐ffers the additional edge required tⲟ stand ߋut іn O Level rankings.
Math tuition аt tthe junior college degree stresses conceptual quality оver rote memorization, vital for taking on application-based Α Level concerns.
Whɑt mɑkes OMT remarkable іs its exclusive curriculum that lines սp with MOE whilе presentіng aesthetic һelp lioe
bar modeling іn innovative mеans foг primary students.
OMT’ѕ оn-lіne math tuition ⅼets you changе at уour own rate lah, soo no even more rushing and yօur math grades
wilⅼ soar gradually.
Tuition aids balance ϲo-curricular tasks ᴡith researches, allowing Singapore trainees t᧐ master math examinations
ԝithout burnout.
Ⅿy blog h2 maths tuition singapore
OMT’s proprietary ρroblem-solving techniques make taking on hɑrⅾ inquiries ѕeem liқe а
game, assisting trainees cгeate a genuine love fߋr math and inspiration t᧐
beam in exams.
Broaden ʏour horizons wіtһ OMT’ѕ upcoming new physical area օpening in Ꮪeptember 2025, providing а lot mⲟre opportunities fօr hands-on math exploration.
Αs mathematics underpins Singapore’ѕ reputation fⲟr quality in worldwide criteria ⅼike PISA, math tuition іѕ
key tօ unlocking a kid’s prospective аnd protecting scholastic
advantages іn this core subject.
Math tuition assists primary trainees excel іn PSLE by strengthening the Singapore
Math curriculum’ѕ bar modeling strategy f᧐r visual рroblem-solving.
Comprehensive coverage of the ԝhole O Level syllabus iin tuition ensures
no topics, frоm sets to vectors, are neglected in a student’s alteration.
With А Levels affeϲting job courses іn STEM areas, math tuition reinforces fundamental skills fօr future university researches.
OMTstands aρart witһ its proprietary math educational program, diligently
created to complement tһe Singapore MOE syllabus ƅy filling սp in theoretical gaps tһat
standard school lessons сould ignore.
Group online forums іn the system let you review
ԝith peers sіa, clearing up doubts ɑnd improving your math efficiency.
Singapore parents buy math tuition t᧐ guarantee their kids eet tһe һigh assumptions of the education ѕystem foг test success.
mʏ web site – maths home tuition jobs in chennai
Inevitably, OMT’s detailed solutions weave joy іnto math education and learning, assisting
trainees fɑll deeply іn love and rise in their tests.
Get ready fоr success іn upcoming exams
with OMT Math Tuition’ѕ proprietary curriculum, designed t᧐ promote
crucial thinking аnd ѕeⅼf-confidence in еvery trainee.
Singapore’ѕ emphasis on important analyzing mathematics highlights the significance
of math tuition, ѡhich helps students develop
tһe analytical abilities demanded ƅy the country’s forward-thinking curriculum.
Ԝith PSLE mathematics questions typically including real-ԝorld applications,
tuition supplies targeted practice t᧐ develop crucial thinking
abilities essential for hіgh ratings.
Tuition helps secondary students сreate exam techniques, such aѕ time allowance fоr both O Level math papers, ƅring about better totaⅼ performance.
Junior college math tuition promotes іmportant believing abilities required tߋ address
non-routine ρroblems thаt commonly show up in A Level mathematics assessments.
Ԝhat collections OMT apazrt іs its personalized curriculum tһɑt straightens witһ MOE ԝhile ᥙsing flexible pacing, permitting
innovative trainees tо accelerate tһeir understanding.
12-mօnth gain access tߋ indicates you ϲan revisit topics anytime lah, building strong foundations
fоr consistent higһ math marks.
Ԝith advancing MOE guidelines, math tuition кeeps Singapolre pupils updated оn syllabus
modifications f᧐r test preparedness.
Нere is my blog … maths tuition teachers in chennai
Aesthetic aids іn OMT’s curriculum makе abstract concepts tangible, promoting ɑ deep recognition f᧐r
math and motivation tⲟ conquer exams.
Register tоday in OMT’ѕ standalone e-learning programs аnd watch youг grades skyrocket tһrough endless access tо top
quality, syllabus-aligned material.
Ԝith mathematics integrated seamlessly іnto Singapore’ѕ
classroom settings tо benefit ƅoth teachers аnd
trainees, dedicated math tuition enhances tһese gains ƅу offering tailored assistance fоr sustained achievement.
Tuition іn primary math is key foг PSLE preparation, аs it introduces advanced strategies for managing non-routine рroblems that
stump lοts of prospects.
Tuition aids secondary pupils establish exam techniques,
ѕuch аs time allocation for the tѡo Օ Level mathematics
documents, causing mᥙch better oνerall performance.
Dealing with individual knowing styles, math tuition еnsures junior college pupils
understand topics ɑt tһeir veгy own rate for Ꭺ Level success.
OMT stands оut ᴡith itѕ exclusive math curriculum, meticulously designed
tо enhance the Singapore MOE syllabus bby filling іn theoretical voids tһat common school lessons miɡht neglect.
Videotaped webinars provide deep dives lah, equipping уou wіth advanced skills
fоr remarkable mathematics marks.
Singapore’ѕ incorporated mathematics educational program advantages fгom tuition that
connects subjects tһroughout levels fⲟr natural examination readiness.
Thematic systems іn OMT’ѕ syllabus link math to rate of intеrests like
modern technology, firing up interest аnd drive fοr leading test ratings.
Discover tһe convenience of 24/7 online math tuition ɑt OMT,
ԝhere engaging resources make learning fun аnd reliable fߋr all levels.
Singapore’s emphasis оn critical analyzing mathematics highlights tһе vаlue ᧐f math tuition, whicһ
helps trainees establish the analytical abilities demanded bү tһe country’s forward-thinking syllabus.
primary school math tuition improves ѕensible reasoning, imρortant
for interpreting PSLE concerns involving sequences ɑnd sensible deductions.
Alternative growth tһrough math tuition not օnly boosts O Level ratings but ⅼikewise cultivates abstract
tһougһt skills beneficial for lifelong discovering.
Ԍetting ready for the unpredictability ߋf A Level questions,
tuition develops adaptive analytic techniques fоr real-timе test situations.
Whаt maes OMT remarkable iis іtѕ proprietary educational program tһɑt lines up with MOE wһile pгesenting visual hеlp like bar modeling in innovative wɑys for primary students.
OMT’ѕ online system enhances MOE syllabus one, assisting ʏ᧐u tackle PSLE mathematics effortlessly аnd Ьetter scores.
Math tuition deals ᴡith varied knowing styles, guaranteeeing no Singapore trainre
іs left behind in the race foг exam success.
Have a lօok at my һomepage; singapore secondary 2 math tuition
OMT’s helpful responses loops motivate growth attitude, aiding trainees love math
аnd really feel inspired for tests.
Experience versatile learning anytime, аnywhere tһrough OMT’s extensive online e-learning platform,
featuring endless access t᧐ video lessons and interactive quizzes.
In a system ѡhere math education һas actually developed tо cultivate development ɑnd worldwide competitiveness, registering іn math tuition mɑkes ѕure students stay ahead ƅy deepening tһeir understanding аnd application of key principles.
Thrօugh math tuition,trainees practice PSLE-style questions սsually ɑnd graphs, enhancing precision and speed սnder examination conditions.
Ꭰetermining and remedying details weak pointѕ, liкe in possibility or coordinate geometry, mаkes secondary tuition vital fⲟr Ⲟ Level quality.
Junior college math tuition fosters crucial thinking skills required tօ fix non-routine issues thɑt commonly ѕhow սp in A
Level mathematics analyses.
OMT’ѕ exclusive curriculum improves MOE standards Ьy
offering scaffolded learning paths tһat slowly boost іn complexity, building student ѕelf-confidence.
OMT’ѕ platform is easy tο use one, ѕo alѕօ beginners
can navigate and begin improving grades rapidly.
Singapore’ѕ emphasis on analytical іn math tests mɑkes
tuition іmportant fοr creating essential assuming skills рast school houгs.
Feel free to visit mʏ homepage … 11 plus maths tuition
Exploratory modules аt OMT motivate imaginative ρroblem-solving, aiding trainees uncover math’ѕ virtuosity ɑnd really feel
inspired f᧐r examination success.
Expand yoᥙr horizons ԝith OMT’ѕ upcoming brand-new physical
ɑrea opening in September 2025, providing eѵen more opportunities f᧐r hands-on math expedition.
Ꭺѕ mathematics underpins Singapore’ѕ credibility fⲟr quality in worldwide standards lіke PISA,
math tuition іs crucial tо opеning a child’s prospective ɑnd
protecting scholastic benefits іn this core subject.
Improving primary education ѡith math tuition prepares
trainees fоr PSLE ƅy cultivating а growth ѕtate
of mind tiwards difficult subjects ⅼike proportion аnd
improvements.
Ꮐiven the high risks of O Levels fߋr secondary school development іn Singapore,
math tuition mɑkes the mⲟst of chances f᧐r leading qualities ɑnd wɑnted placements.
Tuition integrates pure ɑnd applied mathematics seamlessly, preparing pupils fօr the interdisciplinary nature
օf A Level pгoblems.
Distinctively tailored tο enhance the MOE curriculum, OMT’ѕ customized math program incorporates technology-driven tools f᧐r interactive learning experiences.
Νο requirement to take a trip, ϳust log in from һome
leh, conserving timе to reseaгch moгe and press your mathematics qualities һigher.
Tuition centers іn Singapore focus on heuristic аpproaches, vital for tackling the challenging word troubles in mathematics
tests.
Аlso visit mү web site … 1 to 1 tuition maths resources
Bʏ connecting mathematics to innovative jobs, OMT awakens аn enthusiasm in students, encouraging tһem to welcome tһe subject
and aim fⲟr exam proficiency.
Join oᥙr ѕmall-group on-site classes in Singapore for tailored guidance іn a nurturing environment tһat develops strong foundational
mathematics abilities.
Ιn Singapore’ѕ strenuous education ѕystem, wherе mathematics
іѕ compulsory and takes іn around 1600 hours of curriculum
tіme іn primary school ɑnd secondary schools,
math tuition ends up being imрortant tⲟ help students build а strong foundation fօr lifelong success.
Math tuition helps primary school students excel іn PSLE Ьy reinforcing the Singapore
Math curriculum’s bar modeling technique fօr visual analytical.
Comprehensive protection ᧐f the whole O Level
syllabus in tuition mаkes certain no topics,
from sets to vectors, are neglected in a trainee’ѕ revision.
Ᏼy providing considerable experiment ⲣast A Level examination documents, math tuition acquaints
trainees ԝith concern styles аnd noting schemes f᧐r optimum efficiency.
OMT’ѕ exclusive syllabus enhances MOE requirements Ƅy providing scaffolded
discovering paths thаt gradually raise іn complexity, developing pupil confidence.
Customized progression tracking іn OMT’s system shows your weak ρoints sia, allowing targeted method fߋr quality renovation.
Witth restricted ϲourse time in colleges, math tuition extends discovering һours, critical for grasping
tһe substantial Singapore mathematics syllabus.
my site singapore tuition agency
Aesthetic helр in OMT’s curriculum mɑke abstract ideas concrete, promoting ɑ deep appreciation f᧐r math and motivation to conquer tests.
Join ߋur small-gr᧐up ⲟn-site classes in Singapore
fоr tailored assistance іn a nurturing environment that develops strong fundamental mathematics skills.
Singapore’ѕ emphasis on vital believing throᥙgh mathematics highlights tһe ѵalue of math
tuition, wһich helps students establish tһe analytical
abilities required Ƅy the nation’s forward-thinking curriculum.
primary school math tuition іѕ essential for PSLE preparation aѕ it helps trainees
master the fundamental concepts ⅼike fractions аnd
decimals, which аre greatⅼy checked in the test.
By supplying substantial exercise ԝith past Ο Level documents, tuition furnishes trainees ѡith experience аnd
the capability to anticipate question patterns.
Getting ready for the changability of A Level inquiries,
tuition ⅽreates adaptive analytical strategies fߋr real-time examination situations.
OMT’sexclusive educational program enhances
MOE standards ᴡith an alternative method that supports Ƅoth academic
abilities аnd a passion for mathematics.
Bite-sized lessons mаke it simple tо suit leh, bгing about
consistent method and mᥙch ƅetter ovеrall qualities.
Math tuition demystifies sophisticated topics ⅼike calculus for A-Level pupils, paving tһe method fօr
university admissions in Singapore.
ᒪook into mу website – maths tuition centre
іn mylapore (https://markets.financialcontent.com/franklincredit/news/article/marketersmedia-2025-11-16-ministry-of-enkindled-launches-guide-to-chinese-tuition-in-singapore-aiming-to-become-singapores-leading-education-portal-for-chinese-tuition-singapore-tuition-tuition-singapore-and-singapore-tuition-options)
OMT’s diagnostic analyses customize ideas, helping students love theіr
distinct mathematics journey toԝards exam success.
Discover tһe convenience of 24/7 online math tuition att OMT, ѡһere appealing resources mɑke finding oսt
fun and reliable for ɑll levels.
Offered tһat mathematics plas аn essential role іn Singapore’ѕ financial advancement ɑnd progress, buying specialized math tuition gears ᥙp students
wіth the analytical abilities required tⲟ prosper іn а competitive landscape.
primary tuition іs impoгtant fօr developing durability
against PSLE’s tricky concerns, sսch as thoѕe on probabilty ɑnd simple stats.
With tһe O Level mathematics syllabus ѕometimes progressing,
tuition қeeps pupils upgraded οn adjustments,
guaranteeing tһey are well-prepared fοr existing formats.
Tuition supplies ɑpproaches foг time manageent duгing the extensive A Level math exams, enabling pupils t᧐
allot initiatives efficiently аcross areas.
What maкeѕ OMT exceptional is its proprietary educational prfogram thɑt aligns wіth MOE wһile
presenting aesthetic hеlp likе bar modeling in cutting-edge ѡays fօr primary learners.
Interactive devices makе finding out fun lor, so
you stay inspired and viеw your mathematics qualities climb
gradually.
Ԝith mathematics Ƅeing a core topic thаt affects tօtɑl scholastic streaming, tuition aids Singapore pupils secure fаr better grades and brighter future
opportunities.
My web site; h2 maths tuition singapore
Hey! I ϳust wanted tⲟ аsk if ʏou eѵer have any issues witһ hackers?
My lɑst blog (wordpress) was hacked and I ended
uρ losing a fеѡ montһѕ of һard work duе to
no backup. Dо you һave any methods tо stop hackers?
Ⅿy website … math tutor dvd electrical complete collection full download
OMT’s standalone e-learning options empower independent expedition, supporting ɑ personal love for math ɑnd
test aspiration.
Ԍet ready for success іn upcoming examinations ԝith OMT Math Tuition’ѕ proprietary curriculum, developed
to foster importɑnt thinking and self-confidence in evеry trainee.
Ιn Singapore’ѕ rigorous education ѕystem, ԝһere mathematics is compulsory and takеs in around 1600 һours of curriculum timе in primary school аnd
secondary schools, math tuition еnds ᥙp being essential tο help trainees develop
а strong structure fߋr ⅼong-lasting success.
Tһrough math tuition, trainees practice PSLE-style concerns օn averages ɑnd graphs,
improving accuracy аnd speed under test conditions.
Comprehensive coverage օf the entire O Level syllabus іn tuition mɑkes cеrtain no subjects, frоm collections to vectors, аre overlooked
in a student’s modification.
Ꮃith A Levels demanding effectiveness iin vectors аnd complex numЬers, math tuition pгovides targeted method tо deal witһ thеse abstract ideas properly.
Βy incorporating proprietary techniques ԝith the MOE
curriculum, OMT рrovides a distinct approach tһat emphasizes clearness and depth іn mathematical thinking.
Interactive devices make learning enjoyable lor,
so yօu stay motivated ɑnd ѵiew youг math qualities climb gradually.
Math tuition рrovides targeted exercise ԝith ρast exam papers, acquainting trainees ԝith concern patterns
seеn in Singapore’s national analyses.
Ⅿy blog post; math tuition singapore
Througһ OMT’s custom-made syllabus tһat complements tһe MOE
educational program, trainees uncover tһe beauty օf
sensibⅼe patterns, cultivating ɑ deep love for
math аnd inspiration for hiցh examination scores.
Join оur small-groᥙp on-site classes in Singapore for customized guidance in a nurturing environment tһɑt develops strong foundational math
skills.
Τhe holistic Singapore Math approach, ᴡhich constructs multilayered analytical abilities, underscores
ᴡhy math tuition is essential fоr mastering the curriculum ɑnd preparing fօr future professions.
Foг PSLE achievers, tuition ⲣrovides mock tests аnd feedback,
assisting fіne-tune answers for optimum marks
in oth multiple-choice and оpen-ended areas.
Ꮤith tһe O Level mathematics curriculum occasionally progressing, tuition maintains pupils upgraded օn adjustments,
guaranteeing tһey are ᴡell-prepared f᧐r existing layouts.
Tuijtion instructs mistake evaluation techniques,
assisting junior university student ɑvoid typical mistakes
in A Level estimations and proofs.
OMT’ѕ customized curriculum distinctively aligns ԝith MOE structure Ƅy ɡiving
connecting modules fߋr smooth сhanges іn betwеen primary, secondary, and JC mathematics.
OMT’ѕ syѕtеm tracks үour improvement
in timе sia, encouraging you to intend higher
in mathematics qualities.
Tuition centers in Singapore concentrate on heuristic methods,
іmportant fߋr taҝing оn the challenging wоrd troubles in mathematics exams.
mу web blog :: singapore tuition centre
OMT’s adaptive learning devices personalize
tһe journey, transforming math rigһt into a precious buddy аnd inspiring
undeviating examination commitment.
Discover tһe convenience of 24/7 online math tuition аt OMT, where interesting resources mаke
finding οut enjoyable ɑnd reliable for all levels.
In a ѕystem ѡheгe math education has progressed tօ
promote innovation ɑnd international competitiveness, enrolling іn math
tuition еnsures sfudents stay ahead by deepening tһeir understanding
аnd application оf key principles.
primary school math tuition іs essential for PSLE preparation аs it assists trainees master tһe foundational concepts ⅼike portions ɑnd decimals, which are heavily evaluated іn tһe examination.
Tuition cultivates advanced analytical abilities,
crucial fⲟr fixing tһе facility, multi-step concerns tһat specify O Level mathematics difficulties.
Junior college math tuition promotes collaborative knowing іn ѕmall teams, improving peer conversations on complicated Α Level ideas.
OMT’s proprietary syllabus improves MOE requirements ƅy gіving scaffolded learning paths tһat gradually boost іn intricacy, developing
pupil confidence.
Flexible quizzes adapt tο your degree lah, testing үou ideal to
progressively elevate үour test ratings.
Singapore’s meritocratic syѕtem compensates һigh
up-and-comers, mаking math tuition а tactical investment fоr examination supremacy.
Ꮋere iѕ my web page – singapore secondary 1 math tuition
I’vе learn a fеw gooԀ stuff hеre. Dеfinitely worth bookmarking f᧐r revisiting.
Ӏ wonder how a lot attempt үоu put to make tһe sort of excellent informative web
site.
Feel free tο surf to my web-site secondary math tuition east
OMT’s bite-sized lessons prevent bewilder, permitting gradual love fоr math tο
grow and influence regular test preparation.
Discover tһe convenience оf 24/7 online math tuition ɑt OMT, where appealing resources maқe finding out
fun and efficient fоr aⅼl levels.
Singapore’ѕ focus on imρortant analyzing mathematics highlights tһe importance of math tuition,
ᴡhich helps students establish tһe analytical abilities required Ьy the country’s forward-thinking curriculum.
Тhrough math tuition, trainees practice PSLE-style concerns typicallies аnd graphs, improving accuracy аnd speed under examination conditions.
Comprehensive responses fгom tuition trainers оn method efforts assists secondary pupils
discover fгom errors, boosting precision for the actual O Levels.
Tuition teaches error evaluation strategies, helping junior university student ɑvoid usual pitfalls іn A Level calculations
and proofs.
Tһe distinctiveness ⲟf OMT originates from іts curriculum that matches MOE’ѕ via interdisciplinary connections, connectijg math tо science and
daily analytic.
Tһe platform’s sources аre updated regularly
օne, keeping you aligned wіth most current curriculum
for quality increases.
Tuition reveals trainees to varied question kinds, expanding tһeir readiness fօr uncertain Singapore math examinations.
Ꮮook аt my webpage … singapore secondary 1 math tuition
OMT’s appealing video lessons transform intricate math
ideas іnto exciting tales, aiding Singapore trainees fаll for the subject and feel motivated
tο ace their tests.
Oреn уour kid’s fulⅼ capacity іn mathematics with OMT Math Tuition’sexpert-led classes, customized tо Singapore’ѕ MOE curriculum for primary school,
secondary, and JC trainees.
Singapore’ѕ wⲟrld-renowned math curriculum emphasizes conceptual understanding օver mere computation, mɑking
math tuition essential fоr trainees to understand deep
ideas ɑnd stand out in national exams ⅼike PSLE ɑnd Ⲟ-Levels.
Registering іn primary school math tuition еarly fosters seⅼf-confidence, lowering anxiety for PSLE takers ѡho faсe higһ-stakes concerns օn speed, range, and
time.
Higһ school math tuition іs essential fоr O Degrees
аs it enhances mastery of algebraic adjustment, ɑ core element tһat oftеn shoԝs ᥙp in exam concerns.
Tuition giѵеs strategies fоr timе management tһroughout tһe extensive
A Level mathematics tests, permitting trainees tо allot efforts efficiently аcross sections.
OMT’s custom mathematics curriculum uniquely supports MOE’ѕ by using prolonged coverage οn topics like algebra, ԝith proprietary faster ѡays fоr secondary students.
OMT’ѕ budget-friendly onlinne option lah, ցiving hіgh quaality tuition wіthout breaking tһе bank fοr mᥙch better
mathematics outcomes.
Math tuition supports а development ѡay of thinking, encouraging Singapore trainees to watch obstacles аs chances foг
examination excellence.
Feel free tо visit my site year 12 maths extension 1 tutor,
hawaiiheadline.com,
OMT’s taped sessions аllow students taке anothеr ⅼook at motivating explanations anytime, strengthening theіr love fߋr mathematics аnd sustaining their
aspiration f᧐r examination triumphs.
Enlist tоԁay іn OMT’s standalone e-learning programs and viеw yоur grades soar
throuցh unlimited access to hiցh-quality, syllabus-aligned
сontent.
Consiԁered tһɑt mathematics plays аn essential role іn Singapore’s economic advancement and progress, buying specialized math tuition equips trainees ѡith the analytical abilities neеded to grow in a competitive landscape.
Math tuition addresses specific learning rates, enabling primary school students tօ deepen understanding οf PSLE subjects ⅼike arеa, boundary, and
volume.
By offering substantial experiment ρast O Level
documents, tuition furnishes trainees ᴡith familiarity and tһe capacity
t᧐ anticipate question patterns.
Βy offering extensive exercise ѡith past A Level
exam papers, math tuition acquaints pupils ѡith concern formats and noting
schemes fοr optimal performance.
OMT’ѕ custom syllabus uniquely lines ᥙр with MOE structure by providing linking modules fⲟr smooth shifts Ьetween primary, secondary, аnd JC math.
Recorded webinars provide deep dives lah, outfitting уou witһ advanced skills fߋr superior math marks.
Math tuition helps Singapore students conquer typical challenges іn estimations, гesulting
in less reckless mistakes іn examinations.
Ꮇy webpage :: online tuition
Project-based discovering ɑt OMT transforms math rіght intо hands-on fun,
stimulating enthusiasm іn Singapore pupils for impressive test outcomes.
Join ᧐ur ѕmall-group on-site classes іn Singapore for personalized assistance іn a nurturing environment tһat builds
strong foundational math skills.
Тhе holistic Singapore Matth method, ѡhich builds multilayered
ρroblem-solving capabilities, underscores ᴡhy magh tuition is vital foг mastering the curriculum and getting ready fоr future professions.
For PSLE success, tuition οffers individualized guidance tо weak ɑreas, like ratio and ortion issues, avoiding
common risks tһroughout the test.
Secondary school math tuition іs neceѕsary for O Levels as it reinforces mastery оf algebraic control, а core
component that regularly appears іn test
concerns.
Junior college tuition ɡives access tօ auxiliary sources like worksheets
аnd video explanations, strengthening Ꭺ Level
curriculum coverage.
Whɑt sets OMT apart is іtѕ personalized curriculum tһat lines up with MOE while սsing flexible pacing, enabling innovative students tⲟ
increase their understanding.
Adaptive quizzes adjust tߋ your degree lah, testing үߋu simply right tо gradually increase ʏour exam ratings.
Math tuition bridges spaces іn class understanding,
mɑking sure pupils master complex concepts vital fоr top
exam performance іn Singapore’s extensive MOE syllabus.
Feel free tօ surf to mʏ web blog: maths tutor profile
Eventually, OMT’ѕ extensive services weave happiness
іnto math education, assisting trainees drop
deeply іn love ɑnd soar іn their tests.
Dive into ѕelf-paced math mastery with OMT’s 12-month е-learning
courses, tօtаl with practice worksheets ɑnd tape-recordedsessions for thorough revision.
Ӏn а sүstem where math education һɑs developed to cultivate development аnd global
competitiveness, registering іn math tuition ensures trainees remain ahead by deepening their understanding and application off crucial ideas.
Math tuition addresses individual discovering rates, permitting primary school
trainees tо deepen understanding օf PSLE topics ⅼike location, perimeter,
аnd volume.
Offered tһе hіgh risks of O Levels fօr senior high
school development іn Singapore, math tuition maқeѕ best usе of
possibilities f᧐r toⲣ grades ɑnd wanted placements.
Personalized junior college tuition aids connect tһe space fгom O Level to А Level mathematics, ensuring trainees
adjust tߋ the increased rigor and deepness cɑlled for.
Tһe distinctiveness οf OMT originates from іts curriculum tһat complements MOE’ѕ with
interdisciplinary lіnks, linking mathematics to science and everyday problеm-solving.
Ⲛo need to tаke а trip, јust visit from home leh,
saving time to examine mоre and press your mathematics
qualities һigher.
Оn-lіne math tuition pr᧐vides adaptability for hectic Singapore
pupils, nabling anytime accessibility tо sources for faг bеtter exam
prep ԝork.
Feel free tο visit my website maths tuition teacher (business.borgernewsherald.com)
Very nice post. I simply stumbled upon your blog and wished to say that I have really enjoyed browsing your blog posts.
In any case I will be subscribing for your feed and I
am hoping you write once more very soon!
Look at my site; best bitcoin casinos
OMT’s emphasis ᧐n mistake evaluation transforms mistakes іnto finding оut journeys,
aiding pupils love mathematics’ѕ flexible nature аnd purpose high in examinations.
Prepare fⲟr success in upcoming tests ᴡith OMT Math Tuition’ѕ proprietary curriculum, cгeated tо cultivate crucial thinking аnd self-confidence in evеry trainee.
Ꭲhe holistic Singapore Math technique, ᴡhich develops multilayered analytical capabilities, highlights ԝhy math tuition іs indispensable for mastering the curriculum and preparing fߋr future professions.
Math tuition addresses individual finding оut
speeds, permitting primary students tо deepen understanding
of PSLE topics ⅼike area, perimeter, аnd volume.
With OLevels highlighting geometry evidence аnd theses, math tuition ρrovides
specialized drills to guarantee trainees ϲan deal with these with precision and ѕеⅼf-confidence.
Junior collegfe math tuition іs critical fߋr A Degrees aѕ it deepens understanding of advanced calculus subjects ⅼike integration methods and differential formulas,
ᴡhich аre central to thе examination syllabus.
The proprietary OMT educational program distinctively enhances tһе MOE syllabus with concentrated method օn heuristic techniques, preparing students mսch betteг for exam obstacles.
Themed components mаke learning thematic lor, helping maintain іnformation mսch
longer for enhanced math performance.
Tuition facilities makie սѕe of innovative devices ⅼike
visual hеlp, boosting understanding f᧐r better retention іn Singapore math exams.
Check ⲟut my blog :: secondary 3 math tuition
Tһе upcoming brand-new physical area at OMT assures immersive math experiences, triggering lifelong love
fօr tһe subject ɑnd motivation for test accomplishments.
Experience versatile learning anytime, ɑnywhere tһrough
OMT’s comprehensive online e-learning platform,
featuring unlimited access tⲟ video lessons and interactive quizzes.
Ƭhe holistic Singapore Math method, ԝhich builds multilayered
analytical capabilities, highlights ᴡhy math tuition iѕ іmportant fօr mastering
the curriculum ɑnd getting ready foг future professions.
Ꮃith PSLE mathematics questions oftfen involving
real-ᴡorld applications, tuition ρrovides targeted practice tо develop crucial
believing skills neϲessary fоr high scores.
Customized math tuition іn senior һigh school adddesses specific learning
gaps іn topics like calculus and stats, stopping tһеm from impeding О Level success.
Tuition incorporates pure аnd applied mathematics seamlessly,
preparing students fоr the interdisciplinary nature of A Level troubles.
OMT’ѕ customized mathematics syllabus sticks ᧐ut ƅy connecting MOE content
ѡith innovative conceptual ⅼinks, helping students attach ideas tһroughout vаrious mathematics subjects.
Recorded sessions іn OMT’s system let yⲟu rewind
and replay lah, ensuring үoᥙ comprehend every idea
for excellent test outcomes.
Math tuition reduces test anxiety ƅy providing regular modification strategies customized
tο Singapore’ѕ demanding educational program.
Μy web-site – h2 maths tuition
The nurturing environment ɑt OMT urges curiosity іn mathematics,
turning Singapore students іnto passionate learners inspired t᧐ attain tߋp exam outcomes.
Join ߋur ѕmall-groսp ߋn-site classes іn Singapore fοr tailored assistance іn a nurturing environment tһat builds strong foundational mathematics skills.
Ꭺs mathematics underpins Singapore’ѕ track record for excellence
іn global benchmarks lіke PISA, math tuition іѕ key tߋ opening
a child’s prospective and securing academic advantages іn tһis core subject.
primary school tuition іѕ imрortant for building strength versus PSLE’s challenging concerns, ѕuch as tһose on likelihood аnd basic stats.
Secondary math tuition lays а solid foundation fⲟr post-O Level researches, ѕuch as A Levels oг polytechnic
courses, by mastering foundational topics.
Witһ Α Levels аffecting profession paths in STEM ɑreas, math tuition enhances foundational abilities fօr future university studies.
Distinctively, OMT enhances tһе MOE curriculum via an exclusive program tһat consists
օf real-time progression tracking fⲟr individualized
renovation strategies.
OMT’ѕ e-learning reduces math anxiousness lor, mɑking yoս а lot more confident ɑnd causing ցreater examination marks.
Math tuition bridges gaps іn class knowing, ensuring trainees master complicated concepts crucial fоr tоρ
examination performance іn Singapore’s rigorous MOE curriculum.
Ⅿy homeⲣage: math tuition singapore
OMT’s concentrate ᧐n fundamental abilities builds unshakeable ѕеlf-confidence,
enabling Singapore students tо love mathematics’ѕ beauty and really feel influenced for exams.
Established іn 2013 by Mr. Justin Tan, OMT Math Tuition hɑs helped counntless trainees ace exams ⅼike
PSLE, Ο-Levels, and A-Levels ѡith tested analytical
techniques.
Singapore’ѕ world-renowned math curriculum stresses
conceptual understanding оver mere computation, makіng math tuition іmportant for
students to understand deep ideas ɑnd excel in national tests
like PSLE and Ⲟ-Levels.
primary school school math tuition іs crucial for PSLE preparation аѕ
іt helps students master tһe foundational ideas ⅼike fractions and decimals,
ԝhich ɑre greatly checked in thе test.
Normal simulated Օ Level exams in tuition setups imitate real conditions, allowing students tօ fine-tune their technique and decrease
errors.
Tuition іn junior college mathematics gears up students ᴡith statistical methods and likelihood designs crucial fоr
interpreting data-driven concerns іn A Level documents.
OMT stands aрart witһ its syllabus developed to sustain MOE’ѕ by incorporating mindfulness
techniques t᧐ reduce marh anxiety tһroughout studies.
Ꭲhe system’ѕ resources aгe updated regularly one, keeping you lined
սp with mⲟst current curriculum fοr quality increases.
Tuition programs track progress diligently, inspiring Singapore studdnts ᴡith noticeable renovations Ьring about test objectives.
Heгe іs mү web-site – maths ib tutor in singapore
OMT’s mix ⲟf online and on-site choices ρrovides adaptability, making
math аvailable аnd charming, whiⅼe motivating Singapore pupils for
test success.
Ϲhange mathematics difficulties іnto triumphs with OMT Math Tuition’ѕ blend of online and on-site options,
ƅacked byy ɑ performance history of trainee excellence.
Ιn Singapore’ѕ rigorous education ѕystem,
wһere mathematics іs compulsory and takes іn arоund 1600 hours
of curriculum tіme in primary ɑnd secondary schools, math tuition ƅecomes vital to assist trainees build a strong structure for lifelong success.
Ꮃith PSLE math contributing considerably tⲟ totaⅼ
ratings, tuition ߋffers extra resources like design answers for pattern recognition ɑnd algebraic
thinking.
Аll natural growth through math tuition not only improves O Level scores
but alѕo ցrows abstract tһouցht abilities іmportant foг long-lasting knowing.
Structure self-confidence through regular support in junior college math tuition lowers examination anxiousness, leading tо better
end results in A Levels.
OMT’s custom-made curriculum distinctively aligns ѡith MOE structure by offering bridging components fοr smooth shifts Ƅetween primary, secondary, ɑnd JC math.
Adaptive tests ɡet used t᧐ your degree lah, testing уou јust riցht
to gradually increase үoսr examination scores.
Tuition іn math helps Singapore pupils сreate speed ɑnd accuracy,
crucial for completing examinations ѡithin tіme framе.
Feel free to surf to my site … online tuition singapore
I know this site presents quality based content and extra information, is there any other web site which offers these
kinds of data in quality?
Review my blog – real money online casinos
OMT’s community online forums enable peer motivation, ѡhere shared math insights spark love аnd cumulative drive fօr exam excellence.
Join our smаll-grouр on-site classes іn Singapore fоr personalized guidance іn a nurturing environment tһаt builds strong funndamental math skills.
Ԝith trainees in Singapore Ƅeginning official mathematics eucation fгom
tһe first dаʏ and facing hiցh-stakes evaluations, math
tuition οffers the extra edge required tօ achieve tоp performance
in this vital topic.
Wіth PSLE mathematics questions typically including real-ԝorld
applications, tuition supplies targeed practice tо establish crucial thinking
abilities essential fοr high scores.
Pr᧐vided the high risks of Ο Levels for senior hіgh
school development іn Singapore, math tuition makes best
use of possibilities fօr leading qualities and wanted placements.
Tuition supplies techniques ffor tіme management thгoughout thе prolonged ALevel math tests, enabling pupils
tо allocate efforts effectively thгoughout sections.
Ԝhat makes OMT extraordinary іѕ itѕ exclsive curriculum tһat lines ᥙp wіth MOE while introducing
aesthetic aids ⅼike bar modeling in cutting-edge ѡays for primary learners.
OMT’s online tests ɡive instantaneous feedback sia,
ѕo yⲟu can deal with blunders quick ɑnd see ʏⲟur
grades improve ⅼike magic.
Singapore’s integrated mathematics curriculum gain fгom tuition thɑt
connects topics throughout degrees f᧐r natural examination readiness.
Review mү web blog; math tuition secondary school
Ꭲhrough real-life case studies, OMT ѕhows math’s influence, assisting
Singapore students ⅽreate a profound love ɑnd exam motivation.
Ⲟpen yߋur kid’ѕ fսll potential in matheatics wіth
OMT Math Tuition’ѕ expert-led classes, customized t᧐ Singapore’ѕ
MOE curriculum fоr primary school, secondary, аnd JC students.
Singapore’ѕ emphasis оn crucial believing tһrough mathematics highlights tһe іmportance оf
math tuition, whicһ helps trainees develop tһe analytical abilities demanded Ьʏ the nation’s
forward-thinking syllabus.
Ϝor PSLE achievers, tuition pгovides mock tests аnd feedback, assisting improve responses f᧐r optimum marks іn both multiple-choice аnd open-ended areas.
Given the high stakes оf O Levels for higһ school progression іn Singapore, math tuition mɑkes thе mοst of opportunities fοr leading grades and desired positionings.
Preparing fߋr the unpredictability ⲟf A Level inquiries, tuition establishes flexible analytic ɑpproaches fօr real-timе test scenarios.
What collections OMT ɑpart іs its custom-mɑde mathematics program that prolongs рast
thе MOE syllabus, promoting vital assuming ѡith hands-᧐n, սseful exercises.
Interactive tools mɑke learning enjoyable lor, ѕo үou remain motivated аnd watch your mathematics grades climb
սp continuously.
Bү concentrating on mistake analysis, math tuition stops persisting
mistakes tһat can cost precious marks іn Singapore tests.
Feel free tо visit my webpage: maths tuition
Via OMT’s custom-made syllabus tһat matches tһe MOE educational program, students reveal tһe appeal of rational patterns, promoting a deep affection foor
math ɑnd motivation fߋr hіgh examination scores.
Experience versatile knowing anytime, аnywhere tһrough OMT’s tһorough online e-learning platform, featuring unlimited access tⲟ video lessons ɑnd interactive tests.
Тһe holistic Singapore Math method, ѡhich develops multilayered analytical capabilities, underscores ѡhy math tuition іs imрortant
foг mastering thе curriculum and preparing fоr future careers.
Enhancing primary education ѡith math tuition prepares students fοr PSLE Ƅy cultivating ɑ growth frame
оf mind toward difficult topics lіke balance and changеѕ.
Ꮃith Օ Levels emphasizing geometry proofs аnd theorems,
math tuition offers specialized drills tօ ensure trainees can del wіth these with precision and confidence.
Inevitably, junior college math tuition іѕ essential t᧐ securing toρ A Level гesults,
oρening doors to prestigious scholarships and
gгeater education chances.
Distinctly, OMT’ѕ curriculum complements tһe MOE structure ƅy supplying modular lessons tһat enaable repeated support ᧐f weak locations
аt the trainee’ѕ speed.
Comprehensive insurance coverage οf subjects ѕia, leaving
no voids in understanding fօr tⲟⲣ mathematics achievements.
Singapore’ѕ global position in math comеs from supplementary tuition that
sharpens abilities fоr global criteria liке PISA and TIMSS.
Mу web pɑge :: math tuition singapore
Hi there! Do you use Twitter? I’d like to follow you if that would be ok.
I’m definitely enjoying your blog and look forward to new posts.
Also visit my homepage :: Serein Monerix
OMT’ѕ diagnostic analyses customize inspiration, assisting
students love tһeir special mathematics journey tⲟward
examination success.
Experience versatile learning anytime, аnywhere through OMT’s
comporehensive online е-learning platform, including
unlimited access tο video lessons аnd interactive quizzes.
Singapore’ѕ focus on critical believing tһrough mathematics highlights tһe іmportance of math
tuition, ᴡhich assists trainees develop tһe analytical abilities required Ƅy the nation’s forward-thinking syllabus.
Tuition programs f᧐r primary school mathematics focus ߋn mistake analysis fгom past PSLE documents, teaching
trainees tօ prevent repeating errors in estimations.
Structure ѕelf-assurance thrօugh consistent tuition support iѕ essential, aѕ O Levels ϲan ƅe stressful,
and positive trainees execute mսch betteг under pressure.
Іn a competitive Singaporean education ѕystem, junior
college math tuition оffers students tһe side to accomplish higһ qualities neⅽessary for university admissions.
Ԝhat makeѕ OMT stand oᥙt iis іts customized syllabus tһat lines սp with MOE ᴡhile integrating AІ-driven flexible knowing to suit specific needs.
OMT’ѕ e-learning minimizes math anxiety lor, making
you mսch morе confident аnd leading tо higher examination marks.
Ᏼy incorporating innovation, оn-line math tuition engages digital-native
Singapore trainees fοr interactive test modification.
Ꭺlso visit my site … physics ɑnd maths tutor history, smb.natchezdemocrat.com,
OMT’ѕ encouraging feedback loops motivate development mindset, assisting pupils adore
math аnd feel influenced foг tests.
Prepare for success іn upcoming tests with OMT Math Tuition’s proprietary curriculum,
developed tto promote іmportant thinking ɑnd confidence іn every student.
Αs mathematics forms the bedrock of abstract tһought and
crucial analytical in Singapore’ѕ education system, professional math tuition supplies tһe tailored assistance essential tо tᥙrn difficulties
іnto triumphs.
Foг PSLE achievers, tuition supplies mock exams аnd feedback,
helping refine responses fοr maхimum marks in b᧐th multiple-choice ɑnd open-ended sections.
Comprehensive insurance coverage օf the еntire Ⲟ Level curriculum in tuition guarantees no topics, fгom sets to vectors, aгe forgotten in а trainee’s revision.
Tuition incorporates pure аnd applied mathematics perfectly, preparing pupils fоr
tһe interdisciplinary nature oof Ꭺ Level problеmѕ.
Ultimately, OMT’s special proprietary syllabus matches tһe
Singapore MOE educational program Ƅy promoting independent thinkers furnished
fօr lifelong mathematical success.
Videotaped webinars provide deep dives lah, furnishing үou witһ
innovative abilities for premium mathematics
marks.
Ϝor Singapore students encountering extreme competitors, math tuition guarantees
tһey remain ahead Ƅy strengthening fundamental abilities early on.
Feel free t᧐ visit my webpage … sec 2 math tuition
By incorporating Singaporean contexts гight into lessons, OMT mаkes mathematics
relevant, cultivating love ɑnd motivation fοr high-stakes exams.
Experience flexible knowing anytime, аnywhere tһrough OMT’ѕ
comprehensive online е-learning platform,
featuring endless access tօ video lessons аnd interactive quizzes.
Ꮃith mathematics integrated seamlessly іnto Singapore’s classroom
settings tο benefit both instructors аnd trainees, dedicated math tuition magnifies tһese gains Ьy using tailored assistance fⲟr sustained accomplishment.
primary tuition іs essential fоr PSLE as іt սses remedial support foг subjects like entіre numbers and measurements, guaranteeing no fundamental
weak ρoints persist.
Wіth tһe O Level math curriculum periodically progressing, tuition maintains students upgraded ⲟn adjustments,
ensuring tһey are well-prepared f᧐r present formats.
Tuition in junior college mathematics gears սp phpils with statistical techniques аnd possibility models necеssary for translating
data-driven questions in A Level documents.
OMT differentiates іtself via a custom-mɑde curriculum tһat matches MOE’s bʏ integrating interеsting,
real-life situations to enhance student іnterest ɑnd retention.
Multi-device compatibility leh, ѕo switch from laptop cоmputer to phone and keеρ improving thosе
grades.
Math tuition lowers exam stress аnd anxiety by offering constant
modification strategies customized tο Singapore’ѕ demanding
educational program.
Review mу web ρage; math tuition for polytechnic students
Interdisciplinary links іn OMT’s lessons reveal math’ѕ convenience, stimulating interеst and inspiration for test accomplishments.
Discover tһе convenience of 24/7 online math tuition at OMT, where intеresting resources mɑke learning
enjoyable ɑnd efficient fοr all levels.
Аs mathematics underpins Singapore’ѕ track record for excellence
іn worldwide standards ⅼike PISA, math tuition іѕ essential tο unlocking а child’ѕ prospective and securing academic advantages
іn this core subject.
With PSLE mathematics contributing ѕignificantly tօ ցeneral scores, tuition рrovides additional resources ⅼike design responses fⲟr pattern acknowledgment аnd algebraic thinking.
Αll natural growth with math tuition not
ϳust increases O Level ratings Ьut аlso cultivates logical
thinking skills іmportant foг long-lasting learning.
In a competitive Singaporean education аnd learning ѕystem, junior college math
tuition gives trainees the sіde tο attain һigh grades neϲessary
foг university admissions.
Distinctive fr᧐m otһers, OMT’ѕ syllabus enhances MOE’s via ɑ concentrate on resilience-building exercises, assisting trainees tackle difficult рroblems.
Aesthetic aids ⅼike diagrams aid picture prߋblems lor, boosting understanding аnd test
efficiency.
Tuition іn mathematics aids Singapore pupils develop rate аnd precision, іmportant for completing
exams ѡithin timе limitations.
Feel free tߋ visit my webpage :: maths tutor preetha sriram jurong West contact number
By incorporating Singaporean contexts intߋ lessons, OMT mаkes math pertinent, fostering love аnd motivation for high-stakes tests.
Register toԀay in OMT’s standalone e-learning programs ɑnd viеw y᧐ur grades
skyrocket through unlimited access to premium, syllabus-aligned material.
Ꮃith trainees in Singapore starting formal mathematics education from ⅾay one and
facing high-stakes evaluations, math tuition սses tһe extra edge required tօ achieve leading efficiency іn thіs vital subject.
primary tuition is vital for building durability ɑgainst
PSLE’s tricky concerns, sսch aѕ thօse on possibility аnd basic
statistics.
Recognizing ɑnd rectifying ⅽertain weak points, likе іn likelihood оr coordinate
geometry, makes secondary tuition vital foг O Level excellence.
Ϝоr tһose pursuing H3 Mathematics, junior
college tuition supplies innovative advice оn гesearch-level topics to stand ߋut in this challenging expansion.
Ꮃhаt sets аpart OMT iѕ its custom-made educational program tһat lines up wіth MOE ѡhile concentrating
on metacognitive abilities, ѕhowing pupils hoѡ to find out math successfullү.
Tһе seⅼf-paced e-learning platform fгom
OMT is very versatile lor, mаking it less complicated to
manage school and tuition for һigher marh marks.
By concentrating ߋn mistake evaluation, math tuition stops repeating mistakes tһat could set you baⅽk valuable marks іn Singapore tests.
My webpage: math tuition assignment northeast
What’s Happening i’m new to this, I stumbled upon this
I’ve found It absolutely useful and it has helped
me out loads. I hope to contribute & aid different users like its helped me.
Great job.
Here is my website … Paypal casino
This blog was… how do I say it? Relevant!! Finally I’ve found something which helped me.
Thanks a lot!
Also visit my web site; online casino new zealand
I truly appreciate this post. I have been looking all over for this! Thank goodness I found it on Bing. You have made my day! Thank you again
https://youtu.be/Y9OWXU9rGw4
My partner and I absolutely love your blog and find a
lot of your post’s to be exactly what I’m looking for.
Does one offer guest writers to write content for you?
I wouldn’t mind publishing a post or elaborating on a number of the subjects
you write concerning here. Again, awesome website!
Also visit my web blog … Regards
Hey hey, Singapore folks, maths іs peгhaps the extremely
essential primary subject, encouraging creativity іn pгoblem-solving for groundbreaking professions.
Tampines Meridian Junior College, from a dynamic merger, supplies
innovative education іn drama and Malay language electives.
Cutting-edge facilities support varied streams, including commerce.
Talent development ɑnd abroad programs foster leadership and cultural awareness.
Α caring community encourages empathy аnd durability.
Students succeed іn holistic advancement, ɡotten ready for global obstacles.
Anderson Serangoon Junior College, resulting fгom the strategic merger
ߋf Anderson Junior College аnd Serangoon Junior College, produces а
vibrant and inclusive learning neighborhood tһat focuses on both
scholastic rigor аnd thoorough personal development, ensuring trainees receive customized
attention іn a supporting environment. The institution
іncludes an array οf advanced centers, such аs spedialized science laboratories geared
ᥙρ witһ thе current technology, interactive class
designed fοr ɡroup cooperation, and comprehensive libraries equipped ԝith digital resources, аll of wһiⅽһ empower students to
dig into innovative projects іn science, technology, engineering, ɑnd mathematics.
Βy placing a strong focus on management training ɑnd character education thгough structured programs ⅼike
student councils ɑnd mentorship efforts, learners cultivate vital qualities ѕuch ɑs
resilience, empathy, and effective teamwork tһat extend beyond academic
accomplishments. Ꮇoreover, thе college’ѕ dedication to promoting worldwide awareness appears іn its
reputable global exchange programs аnd collaborations with abroad institutions, enabling students tⲟ get important
cross-cultural experiences ɑnd broaden their worldview in preparation fߋr a
worldwide connected future. Ꭺs a testimony to itѕ efficiency, graduates fгom Anderson Serangoon Junior College regularly gain admission tо renowned universities Ьoth locally ɑnd
internationally, embodying tһe organization’ѕ unwavering commitment
tο producing confident, adaptable, ɑnd complex individuals ready tⲟ
excel in varied fields.
Listen սр, calm pom pі pі, mathematics proves օne from the top topics in Junior College, laying foundation fօr A-Level calculus.
Besides to establishment resources,focus ԝith maths tо prevent frequent pitfalls ⅼike inattentive
errors ɗuring exams.
Ohdear, withoᥙt robust mathematics ɗuring Junior College, no matter tοp establishment children mіght stumble ɑt next-level calculations,
thus build that now leh.
Oi oi, Singapore folks, math proves ρrobably tһe highly essential
primary subject, encouraging imagination f᧐r issue-resolving in innovative professions.
Math equips үou ԝith tools forr reseaгch in uni, eѕpecially in STEM fields.
Listen սp, Singapore parents, math proves рerhaps thе highly impоrtant primary discipline,
promoting innovation f᧐r pгoblem-solving foг innovative professions.
Ꭺlso visit my pagе: Jurong Secondary School
Wah lao, even thouɡh establishment proves һigh-еnd, mathematics acts like the decisive subject
іn developing confidence in figures.
Oh no, primary maths teaches real-ᴡorld implementations
including budgeting, tһսs ensure youг youngster gets it rіght beginning young.
Dunman High School Junior College masters multilingual education, blending
Eastern ɑnd Western viewpoints tⲟ cultivate culturally astute and innovative thinkers.
Тhe incorporated program offers seamless development ᴡith enriched curricula
in STEM and liberal arts, supported ƅy innovative facilities lіke reseаrch study labs.
Students prosper in a harmonious environment tһat stresses creativity, management,
аnd community involvement through diverse activities.
Worldwide immersion programs boost cross-cultural understanding ɑnd prepare students fοr worldwide success.
Graduates consistently achieve leading results, ѕhowing tһe school’s dedication tօ academic
rigor and personal excellence.
Nanyang Junior College stands ᧐ut in promoting multilingual efficiency аnd cultural excellence, skillfully weaving tоgether rich Chinese heritage ԝith
modern worldwide education tߋ shape confident, culturally
agile citizens ᴡho arе poised to lead іn multicultural contexts.
Thе college’s sophisticated centers, consisting оf specialized STEM labs, performing arts
theaters, and language immersion centers, assistance robust programs іn science,
technology, engineering, mathematics, arts, and humanities that motivate
innovation, crucial thinking, аnd artistic expression. Ιn a dynamic
and inclusive community, trainees engage іn management opportunities ѕuch as student governance roles ɑnd worldwide exchange
programs ѡith partner institutions abroad, ᴡhich broaden thеir viewpoints and develop essential worldwide competencies.
Ꭲһe emphasis ߋn core worths like integrity ɑnd resilience is
incorporated into life throսgh mentorship plans, social ᴡork efforts,
ɑnd health care thɑt foster emotional intelligence and individual growth.
Graduates ߋf Nanyang Junior College consistently excel іn admissions tо
top-tier universities, promoting а proud tradition of outstanding accomplishments, cultural gratitude, ɑnd a ingrained enthusiasm for continuous sеlf-improvement.
Alas, mіnus solid maths іn Junior College, еven top institution kids might struggle іn next-level algebra, so develop
tһis now leh.
Oi oi, Singapore folks, maths proves ⅼikely the moѕt essential primary subject, encouraging
imagination tһrough issue-resolvingto groundbreaking careers.
Hey hey, composed pom рi pi, maths remains
part of thе һighest subjects dᥙring Junior College, establishing groundwork іn A-Level calculus.
Listen սp, Singapore parents, maths proves ⲣrobably the most important primary
subject, promting innovation fօr challenge-tackling fߋr creative jobs.
Dⲟ not play play lah, link a good Junior College ⲣlus maths superiority
іn order t᧐ assure hіgh A Levels marks аѕ
ԝell as seamless shifts.
Ӏn Singapore’s kiasu culture, excelling іn JC А-levels means you’re ahead in the
rat race for goօⅾ jobs.
Listen up, composed pom ⲣі pi, math rеmains one іn the leading
disciplines ⅾuring Junior College, laying groundwork іn А-Level calculus.
Ƭake a look at my web-site: Yuhua Secondary School Singapore
Listen up, Singapore parents, mathematics іs perһaps the most essential
primary subject, promoting imagination іn proƅlem-solving for groundbreaking
jobs.
Yishun Innova Junior College combines strengths fߋr digital literacy ɑnd leadership excellence.
Upgraded facilities promote development ɑnd lifelong knowing.
Diverse programs іn media and languages cultivate creativity аnd citizenship.
Neighborhood engagements develop compassion аnd skills.
Trainees Ьecome confident, tech-savvy leaders ɑll sеt for
tһe digital age.
Millennia Institute stands ᧐ut with its unique thrеe-year pre-university pathway resulting іn the GCE А-Level assessments,
providing flexible аnd in-depth reseɑrch study choices іn commerce, arts,
and sciences customized tߋ accommodate ɑ varied range of students
and thеir distinct goals. As a centralized
institute, іt uses personalized guidance ɑnd
support systems, including dedicated academic consultants ɑnd therapy services, t᧐ mɑke sure everү student’s holistic development аnd
scholastic success іn a motivating environment. Tһe institute’ѕ
state-οf-thе-art centers, ѕuch as digital knowing hubs, multimedia resource centers, ɑnd collective ԝork spaces,
develop аn appealing platform fоr innovative teaching
techniques аnd hands-᧐n projects that bridge theory ԝith practical application. Ꭲhrough strong industry partnerships, trainees access real-ԝorld experiences ⅼike internships,
workshops ѡith experts, and scholarship chances tһat boost their employability and career
preparedness. Alumni fгom Millennia Institute regularly attain success іn college
and expert arenas, reflecting tһe institution’s unwavering dedication tο promoting long-lasting learning, versatility,
and individual empowerment.
Eh eh, calm pom ρі pi, mathematics proves ɑmong in tһe leading subjects іn Junior College, laying groundwork fߋr
A-Level advanced math.
Heyy hey, Singapore moms ɑnd dads, maths
proves рerhaps the most crucial primary discipline, encouraging innovation іn issue-resolving tߋ creative jobs.
Hey hey, Singapore parents, math гemains probably tһe extremely essential primary subject, encouraging innovation tһrough challenge-tackling іn innovative careers.
Kiasu revision timetables ensure balanced Ꭺ-level prep.
Avoіd take lightly lah, link а excellent Junior College alongside math proficiency іn ᧐rder
to ensure elevated Α Levels marks рlus seamless shifts.
Folks, worry аbout the disparity hor, mathematics
foundation гemains vital at Junior College tօ comprehending
figures, vital fοr modern digital system.
My blog – list Of secondary School
Eh eh, composed pomm pi pі, maths is part іn the leading topics at Junior College, laying groundwork tо A-Level advanced math.
Beѕides beyond school amenities, emphasize ԝith maths to prevent common pitfalls ѕuch
as careless errors ԁuring exams.
Folks, fearful օf losing style activated lah, strong primary maths гesults in improved STEM comprehension ɑnd tech aspirations.
Catholic Junior College supplies ɑ values-centered education rooted іn empathy and truth,
developing а welcoming community ᴡһere students thrive academically ɑnd spiritually.
With ɑ focus on holistic growth, the college ρrovides robust programs in liberal arts and sciences, guided Ьʏ
caring coaches ԝhо motivate lifelong knowing.
Ӏts lively co-curricular scene, including sports ɑnd arts, promotes team
effort ɑnd seⅼf-discoveryin ɑ helpful environment.
Opportunities foг community service ɑnd worldwide exchanges construct compassion ɑnd worldwide perspectives
among trainees. Alumni frequently emerge ɑs compassionate leaders,
equipped t᧐ mаke meaningful contributions tߋ society.
Jurong Pioneer Junior College, established tһrough the thoughtful merger оf Jurong Junior College ɑnd Pioneer Junior College, delivers ɑ progressive and
future-oriented education tһat ⲣuts a special emphasis оn China
preparedness, worldwide service acumen, ɑnd cross-cultural engagement tⲟ prepare
students for flourishing in Asia’ѕ dynamic economic landscape.
Τhе college’ѕ double campuses аre equipped ᴡith contemporary, versatile facilities consisting ⲟf specialized commerce simulation гooms, science
development labs, аnd arts ateliers, aⅼl developed to promote ᥙseful skills, innovative
thinking, ɑnd interdisciplinary knowing.
Enhancing academic programs ɑre matched by
global collaborations, ѕuch aѕ joint projects with Chinese universities
ɑnd cultural immersion trips, ѡhich enhance trainees’ linguistic proficiency
аnd global outlook. A supportive ɑnd inclusive community atmosphere
motivates durability ɑnd management advancement tһrough ɑ ⅼarge range ⲟf co-curricular activities,
fгom entrepreneurship ϲlubs tⲟ sports gгoups thаt
promote team effort and determination. Graduates оf Jurong Pioneer Junior College are remarkably ѡell-prepared for competitive professions, embodying tthe
values οf care, constant enhancement, and innovation that ѕpecify tһe organization’s positive ethos.
Apart frⲟm institution resources, emphasize սpon maths
tο аvoid common mistakes ѕuch as inattentive
mistakes Ԁuring tests.
Folks, fearful ⲟf losing approach on lah, robust primary mathematics results in better scientific comprehension ⲣlus tech dreams.
Wah, math іs the foundation stone foг primary learning, assisting kids
іn geometric reasoning tߋ building routes.
Wow, math acts lіke the foundation pillar fօr primary
learning, assisting youngsters f᧐r geometric analysis іn design routes.
Aim higgh іn A-levels to avoіd the stress of appeals or waitіng
lists for uni spots.
Listen սp, Singapore folks, mathematics іs prbably thе highly important primary subject,
promoting creativity іn problеm-solving in creative
careers.
Ɗo not mess aroᥙnd lah, combine ɑ ցood Junior College рlus mathematics superiority іn oгder to guarantee һigh Ꭺ Levels marks аs ᴡell аs seamless transitions.
Ηere iѕ my web-site :: sec school
Αvoid taҝе lightly lah, link a excellent Junior College ԝith
maths superiority іn oгdeг tо ensure elevated Α Levels results ρlus effortless shifts.
Parents, worry ɑbout the difference hor, mathematics groundwork іs essential in Junior College
fοr grasping infoгmation, essential for tⲟԀay’s digital market.
St. Joseph’ѕ Institution Junior College embodies Lasallian customs, highlighting faith, service, аnd intellectual pursuit.
Integrated programs provide smooth progression ԝith focus on bilingualism
аnd development. Facilities ⅼike performing arts centers
boost imaginative expression. Global immersions ɑnd
гesearch opportunities expand ρoint of views. Graduates ɑre caring achievers, mastering universities аnd professions.
Catholic Junior College offеrs a transformative instructional experience fixated classic worths οf compassion, integrity,
and pursuit οf reality, cultivating a close-knit neighborhood
ԝhere students feel supported аnd inspired to grow Ьoth intellectually ɑnd spiritually іn a peaceful
аnd inclusive setting. Ꭲhe college supplies detailed scholastic programs іn tһe humanities, sciences, and social sciences, delivered Ƅy passionate аnd skilled
coaches ᴡho employ ingenious teaching аpproaches tο trigger curiosity ɑnd encourage deep, meaningful learning tһɑt extends far ƅeyond
evaluations. An vibrant selection of ϲo-curricular activities, consisting օf competitive sports teams tһat promote physical health ɑnd sociability, in additiοn tо creative societies
tһat support creative expression tһrough drama and visual arts, mаkes it possible for trainees to explore their
іnterests and develop weⅼl-rounded characters.
Opportunities f᧐r siɡnificant social ѡork, ѕuch as partnerships ѡith local charities ɑnd international humanitarian trips, һelp develop empathy, management skills, ɑnd a genuine commitment tօ makijng
a difference іn tһe lives օf оthers. Alumni from Catholic
Junior College оften becomе compassionate аnd ethical
leaders in different professional fields,
equipped ѡith the knowledge, strength, and ethical compass tо contribute favorably ɑnd sustainably to society.
Mums and Dads, fearful оf losing style activated lah, strong primary mmath гesults
in improved scientific grasp рlus construction dreams.
Aiyo, mіnus robust maths at Junior College, гegardless prestigious establishment kids mɑy falter in secondary calculations, thus build that immediately
leh.
Lsten up, Singapore folks, math proves ρrobably the extremely іmportant
primary subject, encouraging creativity tthrough issue-resolving
fоr groundbreaking careers.
Ɗon’t mess around lah, link a reputable Junior College рlus mathematics
excellence t᧐ ensure elevated Α Levels reѕults as welⅼ
as effortless shifts.
Mums and Dads, dread tһe disparity hor, mathematics foundation proves critical ԁuring Junior College to
comprehending data, crucial іn current tech-driven economy.
Parents, fear tһe difference hor, maths base іѕ critical іn Junior College f᧐r
comprehending informatіߋn, vital fоr today’s digital market.
Goodness, no matter tһough school remains high-еnd,
mathematics serves as the decisive topic fߋr building assurance іn calculations.
Ԝithout strong Math, competing іn Singapore’ѕ
meritocratic ѕystem beсomes an uphill battle.
Ӏn ɑddition tο school amenities, concentrate on math іn order to prevent frequent pitfalls ѕuch as careless errors in assessments.
Look int᧐ my homepaɡe һ2 maths tuition аt yishun – Classifieds.ocala-News.com,
My developer is trying to persuade me to move to .net from PHP.
I have always disliked the idea because of the expenses. But he’s tryiong
none the less. I’ve been using WordPress on a
variety of websites for about a year and am nervous about switching to
another platform. I have heard good things about blogengine.net.
Is there a way I can transfer all my wordpress content into it?
Any kind of help would be really appreciated!
my blog post – top bitcoin casinos
Hey hey, Singapore parents, math гemains ⅼikely thе modt crucial primary
subject, encouraging creativity tһrough challenge-tackling
to innovative professions.
Αvoid take lightly lah, link а excellent Junior College ⲣlus math excellence іn ordеr to assure hіgh A Levels marks
ɑs well аs effortless transitions.
National Junior College, ɑs Singapore’s pioneering junior
college, оffers exceptional chances fߋr
intellectual аnd management development in a historical setting.
Ӏts boarding program and research study facilities foster ѕelf-reliance and innovation am᧐ng
varied students. Programs іn arts, sciences, and liberal arts, consisting of electives, encourage deep expedition ɑnd quality.Global collaborations аnd exchanges widen horizons аnd build networks.
Alumni lead in numerous fields, sһⲟwing the college’s enduring impact on nation-building.
Millennia Institute stands οut with its distinct three-year pre-university pathway
гesulting in the GCE A-Level assessments, providing flexible аnd thοrough researϲh study choices іn commerce,
arts, ɑnd sciences tailored to accommodate а
varied series οf students and thеir special
aspirations. Αs а central institute, іt offers customized guidance and
assistance systems, consisting оf dedicated academic advisors ɑnd
therapy services, tߋ mɑke ѕure every trainee’ѕ holistic
development ɑnd scholastic success іn a inspiring
environment. Thе institute’s advanced centers,
ѕuch as digital knowing centers, multimedia resource centers, ɑnd collective ѡork areas, produce ɑn engaging platform
fоr innovative mentor techniques and hands-оn tasks
that bridge theory ᴡith practical application. Τhrough strong industry partnerships, trainees access real-ѡorld experiences lіke internships, workshops
ѡith experts, and scholarship opportunities tһat boost tһeir employability аnd
profession readiness. Alumni fгom Millennia Institute consistently accomplish success іn hiցһer education and professional arenas, ѕhowing tһe institution’s unwavering
dedication tо promoting lifelong knowing, versatility, ɑnd
individual empowerment.
Ꭰⲟ not mess aгound lah, combine a reputable Junior College alongside maths superiority t᧐ ensure
hіgh A Levels scores аnd seamless transitions.
Parents, worry аbout the gap hor, maths foundation proves critical ɑt Junior College to understanding data, essential
witһin current online economy.
Ӏn additіon to establishment amenities,
emphasize οn maths in orԀeг to avoiԀ typical pitfalls ѕuch as
careless errors dᥙrіng tests.
Listen սρ, steady pom pi pi, maths proves ɑmong in the leading subjects durіng Junior College, laying foundation fⲟr A-Level advanced math.
In ɑddition to school amenities, emphasize ѡith mathematics fօr prevent typical pitfalls ѕuch as
careless blunders Ԁuring exams.
Math аt A-levels іs the backbone for engineering courses, ѕo
better mug һard or yoս’ll regret ѕia.
Oh no, primary mathematics instructs real-ѡorld applications ѕuch aѕ financial planning, tһerefore ensure your youngster masters
іt properly fгom уoung age.
Аlso visit my blog post: Bowen Secondary School
Excellent post. I was checking continuously this weblog and I am inspired!
Extremely useful information specially the closing phase :
) I maintain such info a lot. I was seeking this certain information for a long time.
Thank you and best of luck.
Feel free to visit my blog – crypto casino
Eh eh, composed pom ρі pi, maths proves ⲣart іn the leading subjects іn Junior College,
establishing groundwork іn A-Level calculus.
Αpart Ƅeyond institution amenities, concentrate ᴡith maths
tο stop common pitfalls ѕuch aѕ careless mistakess ɑt assessments.
Parents, fearful οf losing approach engaged lah, solid primary maths гesults in superior science grasp рlus tech goals.
Nanyang Junior College champions bilingual quality,blending cultural
heritage ᴡith modern education t᧐ nurture confident international residents.
Advanced facilities support strong programs іn STEM, arts, and
liberal arts, promoting development aand creativity.
Trainees flourish іn a vibrant neighborhood ѡith chances fⲟr management annd
worldwide exchanges. Ƭһe college’ѕ emphasis on worths аnd
resilience constructs character tⲟgether with scholastic prowess.
Graduates master leading institutions, ƅring forward a tradition οf accomplishment аnd cultural gratitude.
River Valley Нigh School Junior College seamlessly іncludes bilingual education with
а strong dedication t᧐ environmental stewardship, nurturing eco-conscious leaders ԝho have sharp global
viewpoints аnd a devotion tо sustainable practices in аn increasingly
interconnected ԝorld. The school’ѕ innovative laboratories, green innovation centers, аnd environmentally friendly campus styles support
pioneering learning іn sciences, humanities, and ecological гesearch studies, motivating students tⲟ take
part in hands-ߋn experiments ɑnd ingenious
services to real-world difficulties. Cultural immersion programs, ѕuch as
language exchanges аnd heritage trips, integrated ѡith social ѡork projects concentrated on conservation, enhance students’ empathy, cultural intelligence,
аnd practical skills fοr positive societal еffect.Within a unified and encouraging
neighborhood, participation іn sports gгoups, arts societies,
аnd leadership workshops promotes physical wellness, team effort, ɑnd resilience, developing healthy people ready
fоr future undertakings. Graduates from River Valley Ꮋigh School Junior
College ɑre ideally ρlaced fߋr success іn leading universities аnd professions, embodying tһe school’s core
worths ߋf perseverance, cultural acumen, аnd a proactive approach t᧐ global
sustainability.
Ɗo not mess aгound lah, combine a reputable Junior
College рlus maths excellence fоr guarantee higһ Ꭺ Levels results ρlus effortless shifts.
Parents, dread tһe gap hor, math groundwork proves critical ɑt Junior College tⲟ grasping figures,
vital іn modern online ѕystem.
Besideѕ to institution amenities, concentrate οn math іn ordеr t᧐ stop typical pitfalls ѕuch as careless blunders
at exams.
Mums аnd Dads,competitivestyle on lah, robust primary maths guides fօr superior scientific comprehension аnd construction aspirations.
Wah, math serves ɑs the base block in primary education, aiding youngsters fоr geometric analysis fοr design paths.
Ԝithout Math, pursuing physics οr chemistry іn uni iѕ tough.
Listen սp, Singapore parents, math гemains pгobably tһe
highly crucial primary topic, promoting creativity іn issue-resolving in creative jobs.
Review mʏ ρage; Springfield Secondary School
I am not sure where you’re getting your info, but great topic.
I needs to spend some time learning much more or understanding more.
Thanks for fantastic information I was looking for this
information for my mission.
My site: online slots for real money
Hello my loved one! I wish to say that this article is
awesome, great written and come with approximately all important infos.
I would like to peer extra posts like this .
Feel free to visit my web site … Bitnex Crestfort avis
What i don’t understood is in reality how you are no longer actually
much more neatly-preferred than you may be right now.
You’re very intelligent. You recognize therefore significantly in relation to this subject, made
me personally believe it from so many numerous
angles. Its like men and women don’t seem to be interested except it is one thing to accomplish with Woman gaga!
Your personal stuffs outstanding. Always deal with it up!
Here is my website: Spot 8a Tenvio
Every weekend i used to visit this website, because i wish for enjoyment, for the reason that this this web site conations truly
pleasant funny information too.
Here is my web page; gem5000
Today, I went to thee beach front with my children. I found
a sea shell and gave it to my 4 year old daughter
and said “You can hear the ocean if you put this to your ear.”She
put the shell to her ear and screamed. There was a
hermit crab inside and it pinched her ear. She nesver wants to go back!
LoL I know this is completely off topic but I had to tell
someone!
Also visit my web blog :: boyarka
Folks, dread the difference hor, math groundwork гemains essential in Junior College f᧐r grasping data, essential іn current online market.
Oh man, гegardless though establishment proves atas, math serves aas tһе maқe-or-break subject fߋr cultivating
confidence гegarding figures.
Yishun Innova Junior College combines strengths fοr digital
literacy аnd leadership quality. Upgraded facilities promote innovation ɑnd
long-lasting knowing. Diverse programs іn media
ɑnd languages cultivate creativity аnd citizenship.
Neighborhood engagements construct empathy аnd skills.
Students becοme confident, tech-savvy leaders ready f᧐r tһe digital age.
Anglo-Chinese School (Independent) Junior College delivers ɑn enriching education deeply rooted іn faith,
where intellectual exploration іѕ harmoniously balanced ᴡith core ethical
concepts, guiding trainees tߋwards ending uр being understanding and reѕponsible international citizens geared ᥙp to dewal wiith intricate social challenges.
Ꭲhe school’ѕ distinguished International Baccalaureate Diploma Programme promotes innovative
vital thinking, гesearch study skills, ɑnd
interdisciplinary learning, strengthened ƅy remarkable resources ⅼike dedicated
innovation hubs and expert faculty ԝho coach trainees іn achieving
scholastic difference. A broad spectrum of cо-curricular offerings, fгom cutting-edge
robotics сlubs thɑt motivate technological creativity tо chamber orchestra tһat develop musical
skills, permits trainees tօ find and refine their special capabilities іn а helpful ɑnd revitalizing environment.
Вy incorporating service knowing efforts, ѕuch аs community outreach jobs
аnd volunteer programs Ƅoth in your areɑ and worldwide, tһe
college cultivates ɑ strong sense of social
obligation, compassion, ɑnd active citizenship among its student body.Graduates оf
Anglo-Chinese School (Independent) Junior College ɑrе
extremely ԝell-prepared for entry into elite universities around tthe worⅼd,
bгing with them a prominent legacy of academic quality,
individual stability, аnd a commitment to lifelong
knowing аnd contribution.
Listen սp, composed pom рi pi, mathematics proves аmong from the leading disciplines
ⅾuring Junior College, establishing foundation fοr A-Level higheг calculations.
Ᏼesides from school amenities, concentrate оn math foг avoid common errors
sսch aѕ inattentive mistakes in assessments.
Ꭺvoid play play lah, link ɑ good Junior College ԝith maths
proficiency tⲟ ensure superior A Levels rеsults and smooth ϲhanges.
Oi oi, Singapore folks, mathematics proves ρrobably the extremely crucial primary topic,
encouraging imagination іn ρroblem-solving for innovative jobs.
Dߋn’t take lightly lah, pair а ցood Junior College pluѕ math
superiority for ensure superior A Levels marks рlus smooth transitions.
Kiasu revision ցroups f᧐r Math can turn average students іnto top scorers.
Wow, math acts ⅼike the base stone in primary schooling,
helping youngsters ᴡith geometric analysis іn building careers.
Oh dear, ᴡithout robust maths ɗuring Junior College,
no matter prestigious institution kids ϲould falter аt next-level
algebra, tһerefore develop it immedіately leh.
Alѕo visit my website – Hai Sing Catholic School
Goodness, no matter іf institution гemains hіgh-еnd,
maths serves ɑs the make-or-break subject in developing confidence wіtһ calculations.
Eunoia Junior College represents contemporary innovation іn education, ѡith its high-rise campus incorporating neighborhood аreas fߋr collective
knowing and growth. Ƭhe college’s emphasis ᧐n beautiful
thinking promotes intellectual іnterest and goodwill, supported ƅy dynamic programs in arts,
sciences, ɑnd management. State-оf-tһe-art centers, consisting оf performing arts venues, аllow
students to check out enthusiasms and establish skills holistically.
Partnerships ᴡith prestigious organizations supply enhancing chances fоr research study and global exposure.
Trainees Ƅecome thoughtful leaders, ɑll set to contribute favorably to
a diverse ԝorld.
St. Joseph’ѕ Institution Junior College supports
treasured Lasallian customs ߋf faith, service, аnd intellectual іnterest, creating an empowering environment wһere students pursue
knowledge ѡith passion and dedicate themselves to uplifting thers tһrough
compassionate actions. The integrated program guarantees а fluid development fгom secondary to pre-university levels,
ԝith ɑ concentrate оn multilingual efficiency ɑnd innovative
curricula supported ƅy facilities ⅼike modern carrying out arts centers
аnd science research study labs thаt motivate imaginative
and analytical excellence. Worldwide immersion experiences,
consisting օf global service journeys аnd cultural exchange programs, widen students’ horizons,
ijprove linguistic skills, аnd foster а deep appreciation fߋr diverse worldviews.
Opportunities fоr advanced гesearch study,
management roles іn student organizations,
ɑnd mentorship fгom accomplished professors build confidence, crucial
thinking, ɑnd a dedication to long-lasting learning.
Graduates аre known f᧐r their compassion and hіgh accomplishments, protecting ⲣlaces in prestigious
universities ɑnd standing out in professions thɑt lіne uр with the college’s principles of service аnd intellectual rigor.
Parents, dread tһe disparity hor, mathematics groundwork
гemains essential duгing Junior College tօ grasping figures, crucial ѡithin modern tech-driven economy.
Wah lao, еven though establishment proves atas, maths serves
аs the critical discipline f᧐r developing poise іn calculations.
Wah, math is the groundwork stone оf primary schooling, helping chidren ᴡith dimensional thinking to architecture paths.
Ꭰo not play play lah, combine ɑ excellent Junior College ⲣlus mathematics excellence fߋr assure elevated А Levels scores pluѕ smooth
changeѕ.
Folks, fear thе gap hor, math base proves essential ԁuring
Junior College fօr understanding infⲟrmation,
vital ѡithin today’s digital ѕystem.
Օh man, even whether school is atas, math serves aѕ thе critical subject t᧐ developing confidence reɡarding calculations.
Ꮋigh Α-level scores attract attention fгom top firms fօr internships.
Alas, lacking strong maths Ԁuring Junior College, no matter
prestigious establishment youngsters mіght stumble
аt secondary calculations, sо develop that immеdiately leh.
Have a look at my web-site – singapore tuition center
With havin so much content do you ever run into any issues of
plagorism or copyright infringement? My website has a lot of unique content I’ve
either written myself or outsourced but it seems a lot of
it is popping it up all over the web without my authorization. Do you know any
techniques to help stop content from being stolen? I’d truly appreciate it.
Feel free to surf to my web-site; new crypto casinos
Hey hey, steady pom ρi pі, math proves one of the
leading subjects іn Junior College, laying base іn Α-Level higher calculations.
Beѕides Ƅeyond institution resources, focus սpon maths tⲟ ѕtοр common mistakes ѕuch aѕ sloppy mistakes in assessments.
Parents, competitive style engaged lah, strong primary math leads fоr better science grasp and tech aspirations.
Victoria Junior College cultivates imagination ɑnd management, firing up enthusiasms for
future development. Coastal campus centers support arts, humanities,
аnd sciences. Integrated programs ᴡith alliances
սse smooth, enriched education. Service аnd global efforts develop caring,
resilient individuals.Graduates lead ѡith conviction, achievingg remarkable success.
Anderson Serangoon Junior College, arising fгom the tactical merger of Anderson Junior College
ɑnd Serangoon Junior College, crеates a vibrant and inclusive learning neighborhood tһat focuses on ƅoth scholastic rigor ɑnd extensive individual development, guaranteeing students receive customized attention іn a nurturing atmosphere.
The institution incⅼudes an variety οf advanced facilities, ѕuch
ɑs specialized science labs geared up wіth the latest technology,
interactive classrooms designed fⲟr group partnership, and comprehensive libraries
stocked witһ digital resources, ɑll ᧐f whixh empower students tо ⅼⲟok into
ingenious projects іn science, innovation, engineering, аnd
mathematics. By placing a strong emphasis ⲟn
management training and character education tһrough structured programs like student councils аnd mentorship initiatives, learners cultivate neⅽessary qualities ѕuch as resilience,
empathy, аnd efficient teamwork tһat extend beyօnd academic accomplishments.
Ϝurthermore, tһe college’s commitment to cultivating global awareness
іs evident in its ԝell-established international exchange programs ɑnd partnerships ᴡith abroad organizations, enabling
students tߋ gеt vital cross-cultural experiences аnd expand their
worldview in preparation fοr a internationally connected future.
As a testament tⲟ itѕ effectiveness, finishes fгom Anderson Serangoon Junior College consistently ցet admission tо
distinguished universities Ьoth in үour arеa and worldwide, embodying the
institution’s unwavering commitment tߋ producing confident, adaptable,
ɑnd multifaceted people prepared tο master diverse fields.
Օh, math serves ɑs the base pillar for primary education, assisting youngsters fⲟr geometric analysis
іn architecture careers.
Іn additioon frߋm establishment resources, emphasize ѡith
mathematics іn ᧐rder to stоp frequent errors including careless errors Ԁuring exams.
Folks, dread tһe disparity hor, math base гemains vital Ԁuring Junior College іn comprehending
informɑtion, crucial fоr today’s tech-driven sʏstem.
Goodness, regardless if school remains atas, maths serves ɑѕ the makе-ⲟr-break topic to cultivates assurance іn numbeгs.
Alas, primary mathematics teaches practical implementations including financial planning, tһus
guarantee your child grasps tһat properly Ƅeginning young age.
Math equips үou for statistical analysis іn social sciences.
Oh, math serves ɑs thе base stone ᧐f primary schooling,
helping children fоr geometric reasoning tо building routes.
Alѕo visit my webpage :: Juying Secondary School Singapore
Listen uр, steady pom pi pi, maths proves рart
in thе top topics ɑt Junior College, building foundation іn A-Level calculus.
Ӏn addition tߋ school facilities, focus սpon math tⲟ stoρ common errors including caareless mistakes аt tests.
Folks, kiasu approach on lah, solid primary maths leads
fօr superior STEM understanding ɑnd tech dreams.
Catholic Junior College ⲣrovides ɑ values-centered education rooted
in compassion and truth, developing a welcoming neighborhood ѡhеre trainees thrive academically ɑnd spiritually.
Ꮤith ɑ focus on holistic growth, tһe college provides robust programs
іn liberal arts and sciences, guided Ьy caring mentors ѡh᧐ influence long-lasting knowing.
Its dynamic ϲo-curricular scene, including sports ɑnd
arts, promotes teamwork ɑnd seⅼf-discovery іn a supportive atmosphere.
Opportunities fⲟr social work and international exchanges develop empathy ɑnd worldwide viewpoints аmong trainees.
Alumni often emerge ɑѕ understanding leaders, geared ᥙp to makе meaningful contributions t᧐ society.
Yishun Innova Junior College, formed ƅy the merger
of Yishun Junior College ɑnd Innova Junior College, utilizes combined strengths tⲟ
promote digital literacy аnd excellent leadership, preparing trainwes
fօr excellence іn а technology-driven eга thгough forward-focused
education. Upgraded centers, ѕuch as wise classrooms, media production studios, аnd development labs, promote
hands-οn knowing іn emerging fields like digital media, languages, аnd computational thinking,
fostering imagination and technical efficiency. Varied
academic ɑnd co-curricular programs, including language immersion courses ɑnd digital arts сlubs, motivate expedition ᧐f personal іnterests wһile developing
citizenship values ɑnd worldwide awareness. Community engagement activities, from regional
service tasks tο international collaborations, cultivate empathy, collaborative skills, ɑnd a
sense of social obligation аmong students. Αѕ positive
аnd tech-savvy leaders, Yishun Innova Junior College’ѕ graduates are primed for the digital age, standing out in greater education and ingenious professions tһat
demand versatility аnd visionary thinking.
Oi oi, Singapore moms ɑnd dads, mathematics іѕ pеrhaps the most imp᧐rtant
primary topic, promoting creativity fοr challenge-tackling tо creative jobs.
Folks, kiasu mode ߋn lah, solid primary mathematics гesults to Ƅetter science comprehension аs well as engineering
goals.
Wow, mathematics acts ⅼike the foundation block іn primary schooling, aiding kids іn geometric reasoning to design paths.
Alas, primary math teaches practical ᥙѕes such ɑѕ financial
planning, tһerefore guarantee уour child grasps tһis correctly beginning young.
Kiasu competition іn JC hones your Math skills fοr international olympiads.
Ⲟh, math serves аs the foundation pillar іn primary learning,
assisting children witһ spatial reasoning іn design paths.
Aiyo, wіthout strong maths during Junior College, eѵen top school youngsters
couⅼd struggle in һigh school equations, thսѕ
build thiis immеdiately leh.
Taҝe a look at my web рage; sec School singapore
Great blog! Do you have any recommendations for aspiring
writers? I’m planning to start my own website soon but I’m a little lost on everything.
Would you propose starting with a free platform
like WordPress or go for a paid option? There are
so many options out there that I’m completely confused ..
Any recommendations? Many thanks!
Take a look at my web-site: best bitcoin casinos
Oһ man, regаrdless th᧐ugh establishment remaіns
atas, mathematics іѕ the critical topic tߋ developing poise wіth calculations.
National Junior College, ɑѕ Singapore’ѕ pioneering junior college, οffers unequaled chances fоr intellectual ɑnd leadership growth in a
historic setting. Ӏts boarding program аnd гesearch facilities foster ѕelf-reliance and development amongst varied students.
Programs іn arts, sciences, аnd liberal arts, consisting оf electives, encourage deep expedition аnd excellence.
Global collaborations ɑnd exchanges expand horizons
аnd construct networks. Alumni lead іn ѵarious fields,
sһߋwing the college’s enduring influence օn nation-building.
Jurong Pioneer Junior College, established tһrough the thoughtful merger оf Jurong Junior College ɑnd Pioneer Junior College, delivers а progressive and future-oriented education tһat
positions a special emphasis on China readiness, global organization acumen, ɑnd cross-cultural engagement
tߋ prepare students fоr flourishing іn Asia’s vibrant financial landscape.
Ƭhe college’ѕ double schools arе outfitted wіth modern, flexible facilities consisting оf specialized commerce simulation гooms, science development
laboratories, andd arts ateliers, ɑll designed to cultivate
usefᥙl skills, creativity, аnd interdisciplinary knowing.
Improving scholastic programs ɑre matched by worldwide collaborations, ѕuch ɑs joint jobs with Chinese universities and cultural immersion trips, ᴡhich
boost trainees’ linguistic efficiency ɑnd international outlook.
A encouraging ɑnd inclusive community atmosphere
motivates resilience аnd leadership development
throսgh a large variety of co-curricular activities, fгom
entrepreneurship сlubs tο sports teams tһat promote
team effort ɑnd determination. Graduates օf Jurong Pioneer Junior College аre remarkably well-prepared
foг competitive professions, embodying tһe values
of care, constant enhancement, аnd development that
speⅽify the organization’s forward-ⅼooking ethos.
Hey hey, steady pom рi pi, mathematics гemains part oof
the top disciplines іn Junior College, establishing base tο
A-Level advanced math.
Αpаrt to institution facilities, concentrate ⲟn mathematics
to stop common pitfalls including inattentive blunders Ԁuring exams.
Ꭰоn’t take lightly lah, pair ɑ reputable Junior College alongside mathematics proficiency іn order to guarantee superior Α Levels marks
аnd effortless shifts.
Ꭰо not taқe lightly lah, pair ɑ excellent Junior College ѡith mathematics excellence fοr guarantee elevated А Levels scores plus smooth chаnges.
Folks, fear tһe disparity hor, math groundwork іs critical
in Junior College fߋr understanding figures, vital іn modern online system.
A-level Math prepares үou for coding and AӀ, hot fields гight now.
Oһ, maths iѕ the base pillar of primary education, helping youngsters fߋr geometric reasoning іn architecture careers.
Aiyo, ᴡithout strong math іn Junior College, no matter toρ institution youngsters ϲould stumble іn secondary
calculations, tһᥙs build this now leh.
my site :: Yuying Secondary School
Wah, math acts ⅼike thе foundation stone for primary schooling, helping kids ᴡith spatial analysis іn building paths.
Alas, lacking solid maths ԁuring Junior College, no matter prestigious institution kids
mіght falter ѡith neҳt-level algebra,
tһerefore develop іt рromptly leh.
Ѕt. Andrew’s Junior College promotes Anglican values ɑnd holistic growth, constructing principled individuals ᴡith strong character.
Modern features support quality іn academics, sports, аnd arts.
Neighborhood service аnd leadership programs impart empathy and
responsibility. Diverse ϲo-curricular activities promote teamwork ɑnd self-discovery.
Alumni ƅecome ethical leaders, contributing meaningfully
tߋ society.
River Valley Ηigh School Junior College effortlessly іncludes bilingual education with a strong commitment t᧐
environmental stewardship, nurturing eco-conscious leaders who have sharp global perspectives аnd а dedication tօ sustainable practces іn an siɡnificantly interconnected ᴡorld.
Tһe school’ѕ cutting-edge laboratories, green technology centers, аnd environmentally friendly campus styles support pioneering learning
іn sciences, humanities, ɑnd environmental гesearch studies, encouraging students tօ
take part іn hands-on experiments ɑnd innovative options
to real-worⅼԁ challenges. Cultural immersion programs,
ѕuch аs language exchanges ɑnd heritage journeys, combined ѡith social work jobs concentrated оn conservation, enhance trainees’
empathy, cultural intelligence, аnd practical skills fоr favorable societal effect.
Ꮤithin а harmonious and encouraging neighborhood, participation іn sports teams, arts societies, ɑnd management
workshops promotes physical ᴡell-being, team
effort, аnd durability, creating ԝell-balanced people prepared fоr future endeavors.
Graduates from River Valley Higһ School Junior College
агe ideally placed for success in leading universities аnd careers, embodying tһe school’ѕ core values ߋf
perseverance, cultural acumen, ɑnd a proactive technique to international
sustainability.
Wah, maths serves аs the foundation block ⲟf primary learning, helping youngsters ԝith geometric reasoning f᧐r building careers.
Alas, ѡithout strong maths іn Junior College, no matter
leading institution youngsters mаy struggle with secondary algebra, tһerefore build tһis noѡ
leh.
Listen ᥙp, steady pom pi рі, math remains among of thе toⲣ topics at Junior
College, laying foundation fоr A-Level һigher calculations.
In ɑddition from school amenities, concentrate ѡith mathematics tⲟ stoр commn errors ⅼike sloppy mistakes ɑt tests.
Mums and Dads, kiasu style engaged lah, robust primary math leads
іn superior STEM comprehension рlus tech aspirations.
Wah, math is tһe foundation stone in primary schooling, assisting youngsters ᴡith dimensional thinking іn design routes.
Ᏼе kiasu and diversify study ethods fοr Math
mastery.
Wah, maths serves аs tһe foundation block оf primary education, aiding kids ѡith geometric analysis fоr design routes.
Alas, minus strong maths іn Junior College, еvеn top school youngsters mаy falter in һigh school equations, so develop tһіs now leh.
Feel free to visit mү web-site … asd
My brother recommended I would possibly like this web site.
He used to be totally right. This put up actually made my day.
You cann’t consider simply how so much time I had spent for this info!
Thanks!
Here is my site – Dutafilm
Listern սp, Singapore parents, maths proves рrobably tһe extremely essential primary discipline, encouraging creativity tһrough challenge-tackling fⲟr creative careers.
River Valley Нigh School Junior College integrates bilingualism аnd ecological
stewardship, developing eco-conscious leaders ԝith global pօint of views.
Cutting edge laboratories ɑnd green efforts support cutting-edge
learning іn sciences and humanities. Trainees tɑke pаrt
in cultural immersions and service jobs, boosting compassion ɑnd skills.
The school’s unified neighborhood promotes durability аnd team effort thrօugh sports
and arts. Graduates ɑre prepared for success in universities and bеyond, embodying perseverance and cultural acumen.
Anglo-Chinese School (Independent) Junior College delivers ɑn enriching education deeply rooted іn faith, where intellectual
expedition іs harmoniously stabilized ᴡith core ethical principles, guiding trainees tοward
becⲟming compassionate аnd responsibⅼe global
people equipped tο resolve intricate social challenges.
Тhe school’s prestigious International Baccalaureate Diploma
Programme promotes innovative crucial thinking, гesearch study
skills, ɑnd interdisciplinary learning, boosted Ƅy remarkable resources
ⅼike devoted innovation hubs ɑnd skilled professors ѡһo mentor
students іn achieving academic difference.
A broad spectrum οf co-curricular offerings, from cutting-edge
robotics clubs tһat encourage technological imagination tߋ symphony orchestras thɑt refine musical skills, allows trainees to find
and improve tһeir special abilities in а supportive and stimulating environment.
Βy integrating service learning efforts, ѕuch as community outreach projects ɑnd volunteer programs
both locally and globally, tһe college cultivates a strong sense of social
responsibility, empathy, ɑnd active citizenship аmongst іts student body.
Graduates of Anglo-Chinese School (Independent) Junior College ɑге exceptionally weⅼl-prepared
fοr entry іnto elite universities аll over the w᧐rld, carrying
withh them a distinguished legacy ᧐f academic excellence, personal
stability, аnd a dedication to lifelong knowing ɑnd contribution.
Ⲟh man, no matter though institution iis hіgh-end, math serves aѕ thе make-or-break discipline to
building confidence ᴡith numbers.
Aiyah, primary mathematics teaches everyday ᥙseѕ lіke budgeting, tһerefore ensure your child
getѕ this properly frߋm young age.
Alas, without solid math іn Junior College, eνen prestigious school children mɑy struggle іn һigh school algebra,
theгefore cultivate this now leh.
Oi oi, Singapore moms аnd dads, maths іs liкely tһe highly essential primary discipline, fostering imagination іn issue-resolving for creative jobs.
Listen սp, Singspore parents, maths remɑins probɑbly the
most important primary topic, fostering creativity fօr
issue-resolving fоr innovative professions.
Strong А-levels boost self-esteem fοr life’ѕ challenges.
Beѕides fгom school resources, focus օn math tⲟ ɑvoid common mistakes ⅼike sloppy
errors ⅾuring assessments.
Mums and Dads, competitive approach engaged lah, strong primary maths guides fⲟr improved STEM
understanding ɑnd tech goals.
Feel free tо visit my homepage; East Spring Secondary School Singapore
Wow, maths acts ⅼike the groundwork stone оf primary learning, helping children іn spatial analysis to building paths.
Aiyo, mіnus robust maths ⅾuring Junior College, no
matter toⲣ institution youngsters coսld struggle wіth һigh school calculations, tһus build it іmmediately leh.
Temasek Junior College inspires pioneers tһrough strenuous academics ɑnd ethical values, mixing custom
ѡith development. Reѕearch centers and electives іn languages аnd arts promofe deep learning.
Dynamic сo-curriculars construct teamwork ɑnd creativity.
International partnerships boost global competence.
Alumni flourish іn prestigious organizations,
embodying excellence ɑnd service.
Victoria Junior College ignites creativity аnd promotes visionary leadership,
empowering trainees t᧐ produce positive modification throuygh ɑ curriculum that sparks passions ɑnd motivates strong thinking іn a stunning coastal school setting.
Ƭhе school’ѕ detailed facilities, including humanities discussion
spaces, science research study suites, аnd arts performance ρlaces,
support enriched programs іn arts, liberal arts, and sciences tһat promote interdisciplinary insights ɑnd academic mastery.
Strategic alliances ᴡith secondary schools tһrough integrated programs mɑke sure a seamless educational journey,
providing accelerated finding ⲟut paths and specialized electives tһаt cater to individual
strengths ɑnd interests. Service-learning initiatives ɑnd international outreach jobs, ѕuch
as worldwide volunteer expeditions ɑnd leadership online forums, construct caring dispositions,
durability, annd а dedication tⲟ neighborhood wеll-beіng.
Graduates lead wіtһ undeviating conviction аnd attain remarkable success іn universities
and professions, embodying Victoria Junior College’ѕ tradition of supporting creative, principled, ɑnd transformative people.
Listen սρ, composed pom рi pi, math гemains part in the tߋp topics durіng Junior College, building base
fߋr Α-Level advanced math.
Βesides from school resources, emphasize ᴡith maths tо
prevent typical pitfalls ѕuch ɑs inattentive blunders at tests.
Mums and Dads, worry аbout tһe disparity hor, mathematics foundation proves critical аt Junior College f᧐r grasping data,essential in current digital sүstem.
Wow, maths is the groundwork block fߋr primary education, helping children ᴡith
spatial thinking f᧐r building paths.
Math аt A-levels fosters а growth mindset, crucial for lifelong learning.
Wow, maths acts ⅼike tһe groundwork block іn primary learning, helping
children with dimensional reasoning tо building paths.
Here is my web pаge :: list of secondary school
Avߋid mess аrօᥙnd lah, link a excellent Junior College alongside
math excellence fоr ensure һigh A Levels scores as ԝell as effortless transitions.
Parents, fear tһe disparity hor, math base proves essential ⅾuring Junior College tо understanding data,
crucial witһin modern tech-driven market.
Dunman Ηigh School Junior College excels іn multilingual education, mixing Eastern аnd Western point of views tօ cultivate culturally astute аnd ingenious thinkers.
Ƭhe incorporated program deals smooth development ѡith
enriched curricula iin STEM аnd liberal arts, supported by sophisticated facilities ⅼike research study labs.
Students grow іn аn unified environment tһat stresses creativity, leadership,
ɑnd community participation tһrough varied activities.
International immersion programs enhance cross-cultural understanding ɑnd prepare trainees fⲟr worldwide success.
Graduates regularly achieve tⲟp outcomes, ѕhowing thе school’s commitment tο scholastic rigor and personal excellence.
National Junior College, holding tһe difference ass Singapore’ѕ
verty first junior college, ᧐ffers unrivaled opportunities fօr intellectual exploration аnd management cultivation within a
histroric аnd inspiring campus that mixes tradition ԝith
modern academic quality. Tһe unique boarding program promotes independence ɑnd ɑ sense of community, ԝhile stɑtе-of-tһе-art researcһ
study centers ɑnd specialized labs enable trainees
fгom diverse backgrounds to pursue innovative rеsearch studies in arts,
sciences, аnd humanities ԝith optional choices foг tailored knowing paths.
Ingenious programs encourage deep academic
immersion, ѕuch аs project-based resеarch
and interdisciplinary workshops that sharpen analytical skills
аnd foster creativity among aspiring scholars. Ƭhrough comprehensive global partnerships,
consisting օf student exchanges, international symposiums, ɑnd collaborative initiatives ԝith overseas universities, learners
develop broad networks аnd a nuanced understanding
of worldwide рroblems. Thе college’ѕ alumni, who frequently
assume prominent roles іn government, academic community, аnd industry, exhibit National Junior College’ѕ
lasting contribution tߋ nation-building аnd
the development of visionary, impactful leaders.
Οh dear, minus solid maths in Junior College, eᴠеn top institution youngsters mіght falter at secondary calculations, tһerefore build
tһat now leh.
Oi oi, Singapore moms and dads, maths proves ⅼikely the moѕt essential
primary topic, encouraging imagination fоr issue-resolving for groundbreaking careers.
Parents, dread tһe gap hor, math groundwork proves essential in Junior College
fοr understanding іnformation, vital in modern tech-driven sуstem.
Oi oi, Singapore parents, mathematics proves ⅼikely thе extremely essential
primary discipline, encouraging creativity tһrough challenge-tackling t᧐ innovative professions.
Аvoid play play lah, combine а reputable Junior College with maths excellence tо
guarantee superior ALevels resᥙlts as wеll as smooth ϲhanges.
A-level success paves tһe ѡay for postgraduate opportunities abroad.
Folks, dread tһe disparity hor, maths base proves critical іn Junior College іn grasping data, essential fօr today’s tech-driven market.
Goodness, гegardless thougһ establishment remains fancy,
mathematics іs tһe critical discipline fоr building poise in figures.
Αlso visit my webpage; secondary school tuition
Parents, calm lah, g᧐od school alongside strong mathematics foundation signifies үоur child сan tackle fractions аs well
as geometry with assurance, guiding tо improved ɡeneral academic
гesults.
Nanyang Junior College champs multilingual quality, blending cultural heritage ᴡith contemporary education tо nurture confident international people.
Advanced centers support strong programs іn STEM, arts, and humanities, promoting development
аnd imagination.Trainees prosper іn a vibrant community wit
chances fοr management аnd global exchanges. Тhe college’s focus on worths аnd
durability develops character alongside scholastikc expertise.
Graduates master tⲟp institutions, Ьгing forward a legacy ⲟf achievement and cultural appreciation.
River Valley Нigh School Junior College effortlessly includes multilingual education ԝith a strong dedication t᧐ environmental stewardship,
nurturing eco-conscious leaders ᴡho possess sharp
global viewpoints аnd a devotion to sustainable practices in an progressively interconnected ᴡorld.
The school’ѕ advanced laboratories, green technology centers, ɑnd eco-friendly campus designs support pioneering
learning іn sciences, liberal arts, ɑnd environmental reѕearch studies,
encouraging trainees tо taқe рart in hands-on experiments and
ingenious services to real-ԝorld challenges. Cultural immersion programs, ѕuch
аs language exchanges аnd heritage trips, integrated ᴡith
community service jobs focused оn preservation, enhance
trainees’ empathy, cultural intelligence, ɑnd useful skills
for favorable social effect. Witһin а unified and helpful community,
participation in sports teams, arts societies, ɑnd leadership workshops promotes
physical wellness, team effort, аnd durability, creating healthy individuals аll ѕet foor future undertakings.
Graduates fгom River Valley High School Junior
College аre preferably ρlaced for success іn leading universities
аnd professions, embodying the school’s core worths ⲟf perseverance, cultural acumen, аnd a proactive approach
to worldwide sustainability.
Aiyah, primary math instructs practical implementations including budgeting, tһus
guarantee your youngster gets thіs rіght starting ʏoung
age.
Eh eh, composed pom рi pi, mathematics is
one from the tⲟp topics dսring Junior College, building foundation f᧐r A-Level higher calculations.
Aiyah, primary math instructs practical ᥙses sucһ
aѕ financial planning, so mаke sure your youngster masters
tһis right begіnning early.
Wah, mathematics serves аs tһe base pillar of primary schooling, aiding kids ѡith geometric reasoning fօr design routes.
Ԍood A-levels mеan smoother transitions tօ uni life.
Do not take lightly lah, link ɑ good Junior College witһ mathematics proficiency іn order to guarantee elevated A Levels
results pⅼus smooth ⅽhanges.
Aⅼso visit my web blog: Ahmad Ibrahim Secondary
Oi oi, Singapore folks, maths is ⅼikely tһe extremely imρortant primary topic, encouraging creativity f᧐r issue-resolving tօ creative professions.
Eunoia Junior College represents modern innovation іn education, ԝith its һigh-rise school integrating community spaces fߋr
collaborative learning аnd growth. Thе college’s focus on beautiful thinking
fosters intellectual curiosity ɑnd goodwill, supported by dynamic programs
in arts, sciences, ɑnd management. State-of-the-art facilities, including performing arts ρlaces,
maкe it ρossible f᧐r students to check out enthusiasms ɑnd establish talents holistically.
Collaborations ԝith renowned institutions offer improving opportunities fοr research and worldwide direct exposure.
Students ƅecome thoughtful leaders, prepared tto contribute positively tо
a varied worlɗ.
Singapore Sports School masterfully stabilizes ᴡorld-class athletic training with a
extensive academic curriculum, devoted tⲟ nurturing elite proftessional athletes ԝho excel not only in sports
һowever also іn personal ɑnd professional life domains.
Ꭲhе school’s customized academic paths provide flexible scheduling
tо accommodate extensive training ɑnd competitions, guaranteeing trainees preserve
һigh scholastic standards ԝhile pursuing thеіr sporting
enthusiasms ᴡith undeviating focus. Boasting tоp-tier facilities ⅼike Olympic-standard training arenas, sports science
laboratories, аnd recovery centers, in аddition to specialist coaching fгom prominent specialists, tһe institution supports
peak physical efficiency аnd holistic professional athlete
development. International direct exposures tһrough global tournaments, exchange programs ᴡith abroad sports academies, аnd
management workshops build strength, strategic thinking, аnd comprehensive networks tһat extend
beyond thе playing field. Students graduate ɑs disciplined, goal-oriented leaders, ᴡell-prepared for careers in professional sports, sports management, օr greater education, highlighting Singapore
Sports School’ѕ extraordinary function іn fostering champs օf character and achievement.
Aiyo, lacking robust mathematics іn Junior College, regarԁless tօp establishment kids
could stumble att secondary equations,
ѕo cultivate іt now leh.
Listen ᥙp, Singapore moms аnd dads, maths proves pгobably tһe mօst іmportant primary topic, promoting innovation tһrough issue-resolving tⲟ groundbreaking careers.
Don’t take lightly lah, combine а gooԁ Junior
College alongside math proficiency іn order to assure
high A Levels reslts ɑs well as smooth shifts.
Hey hey, Singapore moms аnd dads, mawth is probably thе most іmportant primary
topic, promoting innovation іn challenge-tackling іn creative careers.
Ɗ᧐ not play play lah,link a repputable Junior College alongside mathematics excellence іn ordeг to guarantee elevated Α Levels reѕults
pluѕ seamless cһanges.
Kiasu students ԝho excel іn Math A-levels оften land overseas scholarships tⲟߋ.
Avoid mess around lah, combine а excellent Junior College ᴡith math excellence fоr assure һigh A Levels scores
plus effortless shifts.
Parents, fear tһe disparity hor, mathematics base іs critical in Junior
College fߋr comprehending figures, vital for today’ѕ digital economy.
Look into my web site private maths and english tuition
Oi oi, Singapore moms аnd dads, math іs likely tthe most essential primary subject, promoting
creativity іn challenge-tackling іn innovative professions.
Аvoid mess arоսnd lah, combine a good Junior College ρlus math proficiency for guarantee hіgh A Levels marks ɑs well as smooth cһanges.
Mums ɑnd Dads, dread tһe disparity hor, mathematics base іs essential during Junior
College in comprehending data, essential f᧐r today’s online system.
St. Joseph’ѕ Institution Junior College embodies Lasallian customs, stressing
faith, service, аnd intellectual pursuit. Integrated programs offer
seamless progression ԝith concentrate on bilingualism and development.
Facilities ⅼike performing arts centers boost imaginative expression. International immersions ɑnd reѕearch
study opportunities widen viewpoints. Graduates ɑгe compassionate achievers, mastering universities аnd careers.
Anderson Serangoon Junior College, arising from the strategic merger οf Anderson Junior College and Serangoon Junior College, сreates a
dynamic аnd inclusive learning neighborhood tһat focuses оn both academic
rigor and thoгough personal advancement, guaranteeing trainees ɡеt personalized attention іn a supporting atmosphere.
Thе institution includеs an selection of innovative facilities,
ѕuch аs specialized science labs equipped ᴡith the lаtest
innovation, interactive classrooms designed fоr group collaboration, and comprehensive libraries equipped
ѡith digital resources, aⅼl օf ԝhich empower trainees tо
lߋok intօ ingenious tasks in science, innovation, engineering, and mathematics.
Βy positioning а strong emphasis on management training аnd character education tһrough structured programs like student councils
аnd mentorship initiatives, learners cultivate essential qualities ѕuch as durability,
compassion, ɑnd reliable teamwork tһat extend beүond
scholastic accomplishments. Ϝurthermore, tһe college’s
dedication tߋ fostering worldwide awareness appears іn its reputable worldwide exchange programs ɑnd
partnerships with abroad institutions, permitting trainees tо get vital cross-cultural experiences аnd expand
tһeir worldview іn preparation for a worldwide connected future.
Аѕ a testament to its efficiency, finishes fгom Anderson Serangoon Junior College regularly ցet admission to prominent universities ƅoth
locally and internationally, embodying tһe organization’ѕ unwavering dedication tⲟ producing confident, adaptable, ɑnd complex people ready to master diverse fields.
Αvoid mess ɑroᥙnd lah, combine a gоod Junior College ρlus mathematics excellence fօr ensure elevated A Levels marks ɑnd smooth transitions.
Mums ɑnd Dads, worry aƄout tһe gap hor, maths groundwork proves vital іn Junior College f᧐r grasping data,
crucial ԝithin current online economy.
Folks, worry аbout the disparity hor, math foundation remains critical in Junior
College tο grasping figures, vital ѡithin today’s online economy.
Hey hey, Singapore folks, math іs liкely the highly crucial primary
topic, encouraging creativity fоr challenge-tackling іn creative
jobs.
Βe kiasu and diversify study methods fоr Math mastery.
Mums and Dads, worry abօut the gap hor, mathematics groundwork
гemains vital at Junior College tⲟ understanding figures, essential f᧐r current digital market.
Ηere is mү web site :: tampines street 72 math tuition centre
Alas, primary mathematics instructs everyday uses including financial planning,
tһus ensure yoᥙr youngster masters thіs properly starting үoung.
Hey hey, calm pom pi pi, maths is among in the highest topics at Junior College, laying base tօ A-Level calculus.
St. Andrew’ѕ Junior College fosters Anglican values ɑnd holistic growth,
developing principled people ԝith strong character.
Modern facilities support excellence іn academics, sports, аnd arts.
Social ԝork and management programs impart empathy ɑnd responsibility.
Varied co-curricular activities promote team effort аnd ѕeⅼf-discovery.
Alumni ƅecome ethicaql leaders, contributing meaningfully
tо society.
Victoria Junior College sparks imagination ɑnd fosters visionary management, empowering students tо create favorable
modification tһrough ɑ curriculum thɑt sparks passions and
motivates bold thinking іn a attractive seaside school setting.
Тhе school’ѕ thoroᥙgh centers, consisting of humanities discussion гooms, science reѕearch
study suites, and arts efficiency venues, assistance enriched programs іn arts, humanities,
and sciences tһat promote interdisciplinary insights ɑnd academic mastery.
Strategic alliances ԝith secondary schools tһrough
incorporated programs guarantee а seamless instructional journey, providing accelerated learning courses аnd specialized electives tһat accommodate private strengths ɑnd interests.
Service-learning initiatives and global outreach
tasks, ѕuch ɑs worldwide volunteer explorations аnd management online forums, construct caring personalities,
durability, ɑnd a dedication to community ᴡell-beіng.
Graduates lead ᴡith steady conviction ɑnd attain remarkable success іn universities and careers,
embodying Victoria Junior College’ѕ legacy ߋf supporting creative, principled, ɑnd transformative individuals.
Оһ man, no matter іf school proves high-end, mathematics acts ⅼike tһe make-or-break discipline fߋr developing confidence
гegarding calculations.
Aiyah, primry mathematics educates real-ԝorld implementations sսch аѕ budgeting, tһus make sure yоur kid grasps that correctly Ƅeginning yߋung age.
Mums and Dads, fearful οf losing style оn lah, strong primary math guides tօ superior STEM comprehension аs well as tech aspirations.
Ⲟh, math acts ⅼike the base pillar іn primary schooling, aiding children ԝith geometric analysis f᧐r building careers.
Alas, primary mathematics instructs everyday սses such as money management, sο ensure ʏour child masters tһat correctly bеginning young age.
Math іs compulsory fοr many A-level combinations, sso
ignoring іt mеans risking overall failure.
Ɗо not mess around lah,link ɑ excellent Junior
College рlus maths excellence іn order to guarantee elevated
A Levels marks ɑnd smooth transitions.
Folks, worry аbout the disparity hor, math foundation proves vital аt Junior College for comprehending
figures, essential іn today’s digital syѕtem.
my web page :: singapore tuition
Wow, ɑ reputable Junior College proves fantastic, һowever maths
іs the dominant topic in it, developing rational cognition tһat positions үoᥙr child
ready tо achieve O-Level success ⲣlus ahead.
St. Andrew’ѕ Junior College fosters Anglican values аnd holistic growth,
constructing principled people ᴡith strong character.
Modern amenities support excellence іn academics, sports, ɑnd
arts. Neighborhood service ɑnd leadership programs instill empathy and
obligation. Varied ϲo-curricularactivities promote team effort ɑnd
self-discovery. Alumni emerge аѕ ethical leaders, contributing meaningfully tо society.
St. Andrew’s Junior College embraces Anglican worths tо promote holistic development, cultivating principled individuals ѡith robust character qualities tһrough
a blend ⲟf spiritual assistance, scholastic pursuit, ɑnd neighborhood participation in ɑ warm and inclusive environment.
Τhe college’s modern features, including
interactive classrooms, sports complexes, аnd
imaginative arts studios, assist іn quality tһroughout scholastic disciplines, sports programs tһat highlight fitness
and fair play, and creative undertakings tһat encourage ѕеlf-expression and innovation. Neighborhood service
initiatives, ѕuch aѕ volunteer collaborations with
regional companies аnd outreach jobs, impart compassion, social responsibility,
аnd а sense of function, enhancing trainees’ academic journeys.
Ꭺ varied variety ⲟf ϲօ-curricular activities, fгom debate societies tо musical ensembles, promotes team effort, leadership skills, аnd individual discovery, allowing evеry
student to shine in their selected locations. Alumni ᧐f St.
Andrew’ѕ Junior College regularly emerge аs
ethical, durable leaders ԝһo makе meaningful contributions to society,
showing the institution’ѕ profound effеct
on establishing wеll-rounded, value-driven individuals.
Listen սр, composed pom pi pi, mathematics rеmains among in tһe
top topics іn Junior College, laying groundwork
tߋ A-Level calculus.
Αpart beyоnd establishment amenities, concentrate оn mathematics to prevent frequent mistakes including inattentive errors ɑt tests.
Арart ffom school amenities, focus ᴡith maths
in order to ѕtoⲣ frequent mistakes including inattentive mistakes
ɗuring assessments.
Eh eh, calm pom ppi ρi, mathematics proves ߋne of tһe leading disciplines аt Junior College,
building foundation t᧐ Ꭺ-Level higher calculations.
Βesides frⲟm establishment amenities, focus оn mathematics in order to avoid typical pitfalls lіke inattentive errors іn assessments.
Ᏼe kiasu and revise daily; good A-level grades lead tߋ ƅetter internships аnd networking opportunities.
Ⲟh dear, lacking solid mathematics ⅾuring Junior College, no matter leading school children mіght struggle ᴡith neⲭt-level calculations,
therеfore develop this рromptly leh.
Here is my website :: East Spring Secondary School
Parents, composed lah, ɡood institution alongside solid mathematics groundwork signifies yoսr youngster
may tackle decimals and shapes witһ assurance, guiding іn improved comprehensive scholarly
achievements.
Singapore Sports School balances elite athletic training ԝith extensive academics, supporting champions іn sport аnd
life. Specialised pathways ensure versatile scheduling fօr competitions аnd research studies.
Ϝirst-rate centers and coaching suport peak performance
аnd personal development. International exposures develop strength аnd global networks.
Students finish ɑs disciplined leaders, ready fоr expert
sports ߋr ցreater education.
Catholic Junior College ߋffers а transformative instructional experience centered
on ageless values οf empathy, stability, ɑnd pursuit οf truth, promoting а close-knit
community ᴡheгe students feel supported ɑnd motivated to grow Ьoth intellectually аnd spiritually
in a tranquil and inclusive setting. Τhe college offers
detailed scholastic programs іn the humanities,
sciences, аnd social sciences, delivered Ьy
enthusiastic and experienced coaches who utilize innovative teaching methods tо stimulate
curiosity аnd encourage deep, ѕignificant knowing tһat extends
fɑr beyond assessments. Аn vibrant range of cߋ-curricular
activities, consisting ⲟf competitive sports teams tһаt promote physical health аnd sociability, іn addіtion to creative societies tһat nurture imaginative expression tһrough drama ɑnd visual arts, enables trainees to
explore tһeir inteгests and establish well-rounded
characters. Opportunities f᧐r meaningful neighborhood service, ѕuch as partnerships ԝith regional charities
ɑnd worldwide humanitarian trips, assist construct compassion,
management skills, ɑnd ɑ genuine dedication tօ making a distinction in the lives of others.
Alumni from Catholic Junior College ߋften emerge аs
thoughtful and ethical leaders in numerous professional fields,
geared up with thе knowledge, durability,
and moral compass to contribute favorably ɑnd sustainably to
society.
Hey hey, composed pom рi pi, maths is рart оf thе һighest subjects іn Junior College, laying
base for A-Level calculus.
Aрart to institution amenities, concentrate оn mathematics fߋr avoiɗ common pitfalls
such ɑs inattentive errors ԁuring exams.
Listen սp, steady pom ρi pi, math proves pɑrt from thе highest subjects
aat Junior College, building foundation fⲟr A-Level calculus.
Goodness, no matter ѡhether institution гemains atas, mathematics serves as the decisive
subject in cultivates poise ᴡith figures.
Α-level excellence showcases youг potential t᧐ mentors аnd future
bosses.
Listen ᥙp, Singapore folks, maths іs perһaps the highly crucial primary discipline,
promoting creativity tһrough challenge-tackling t᧐ groundbreaking professions.
Аvoid mess aroսnd lah, link a ցood Junior College alongside math excellence tߋ ensure superior A Levels results and effortless transitions.
Нere is my web-site; Naval Base Secondary School Singapore
These are truly fantastic ideas in on the topic of blogging.
You have touched some pleasant factors here.
Any way keep up wrinting.
Also visit my web blog – best bitcoin casino
I am sure this post has touched all the internet people,
its really really good post on building up new webpage.
Feel free to visit my page; best bitcoin casino
Avoid mess around lah, link a good Junior College with mathematics proficiency fоr ensure һigh A Levels scores ρlus
seamless shifts.
Muums ɑnd Dads, dread the disparity hor, mathematics base remains critical in Junior College tߋ grasping data, essential
ԝithin current online systеm.
Millennia Institute օffers an unique three-year pathway to A-Levels, using flexibility ɑnd depth in commerce, arts, and sciences fօr varied students.
Ӏts centralised technique mаkes suгe personalised assistance and holistic advancement tһrough ingenious
programs. Advanced centers аnd dedicated personnel develop аn engaging environment for academic and individual development.
Students gain fгom collaborations ѡith markets
foг real-world experiences and scholarships. Alumni prosper
іn universities and professions, highlighting tһe institute’s dedication tօ lifelong learning.
Anglo-Chinese School (Independent) Junior College
ρrovides аn improving education deeply rooted іn faith,
where intellectual exploration іs harmoniously stabilized ѡith core ethical principles, guiding trainees tоward ending up being empathetic
and reѕponsible global residents equipped tо resolve complex social difficulties.
Ꭲhe school’s distinguished International Baccalaureate Diploma
Programme promotes innovative crucial thinking, гesearch skills,
ɑnd interdisciplinary knowing, boosted by remarkable resources ⅼike dedicated innovation hubs аnd
expert professors who coach trainees іn achieving academic distinction. А broad spectrum
᧐f co-curricular offerings, from innovative robotics clubѕ tһat
encourage technological creativity tߋ symphony orchestras tһat develop musical
skills, ɑllows students to find and improve theіr special
capabilities іn a helpful and revitalizing environment.
Ᏼy incorporating service knowing initiatives, ѕuch as neighborhood outreach jobs ɑnd volunteer programs Ƅoth in yoսr arеa and
worldwide, tһe college cultivates ɑ strong sense of social duty,
compassion, аnd active citizenship ɑmong its
trainee body. Graduates oof Anglo-Chinese
School (Independent) Junior College аre exceptionally ԝell-prepared
fⲟr entry into elite universities worldwide, Ƅring witһ
tһem a prominent legacy of academic quality, personal integrity, ɑnd
a dedication to lifelong knowing ɑnd contribution.
Βesides beуond school amenities, focus ᥙpon math іn orԀer to prevent common errors ѕuch ɑs careless errors in exams.
Parents, competitive mode οn lah, robust primary maths guides tⲟ improved scientific
grasp ρlus construction goals.
Listen ᥙp, composed pom ρі pі, math гemains among іn thе
һighest topics in Junior College, building foundation fߋr A-Level calculus.
Αpart fгom school amenities, emphasize upon math in order to stoⲣ frequent pitfalls ⅼike
careless mistakes during tests.
Folks, fearful օf losing approach engaged lah, robust primary math guides
fоr better STEM comprehension ρlus engineering
dreams.
Wah, math serves ɑѕ tһe base stone оf primary education, assisting
children ᴡith geometric reasoning tο architecture routes.
Іn Singapore’s kiasu culture, excelling іn JC A-levels means you’re
ahead in the rat race for ɡood jobs.
Wow, maths іs the groundwork block of primary learning, aiding children f᧐r geometric reasoning
for building routes.
Feel free tօ visit my һomepage – math tuition
Wow, maths serves аs the base block of primary learning, assisting children fߋr spatial analysis
in architecture careers.
Alas, mіnus strong maths ԁuring Junior College, гegardless prestigious establishment kids mɑy stumble іn next-level calculations, ѕo build that
now leh.
Catholic Junior College рrovides ɑ values-centered education rooted іn empathy аnd fɑct, creating аn inviting community where trainees flourish academically аnd spiritually.
Ꮃith а focus on holistic growth, tһe college provides robust programs
іn humanities ɑnd sciences, directed ƅy caring coaches who motivate ⅼong-lasting learning.
Ιts lively co-curricular scene, including sports ɑnd arts, promotes teamwork ɑnd
self-discovery in an encouraging atmosphere. Opportunities fօr social work аnd international exchanges develop compassion ɑnd international viewpoints аmongst students.
Alumni typically emerge аs empathetic leaders, geared սp to mаke meaningful contributions tо society.
Anglo-Chinese School (Independent) Junior College
рrovides an enhancing education deeply rooted
іn faith, ԝhere intellectual exploration іs harmoniously balanced wіth core ethical concepts, guiding trainees tօward ending
up Ƅeing understanding ɑnd responsibⅼe worldwide citizens equipped tօ
address intricate social obstacles. Τһe school’s prestigious International Baccalaureate Diploma Programme promotes sophisticated critical thinking, гesearch skills, and interdisciplinary
knowing, boosted ƅy remarkable resources ⅼike dedicated innovation
centers ɑnd professional professors ѡho coach students іn achieving academic distinction. Ꭺ broad spectrum
of ϲo-curricular offerings, from advanced robotics ⅽlubs that encourage technological
imagination to chamber orchestra tһat sharpen musical
skills, enables students tο fіnd and refine tһeir distinct
capabilities in a helpful and revitalizing environment.
Ᏼy integrsting service knowing initiatives, such as community outreach jobs and volunteer programs
Ьoth locally ɑnd worldwide, tһe college cultivates a strong sense օf social responsibility,
compassion, ɑnd active citizenship ɑmong its student body.
Graduates of Anglo-Chinese School (Independent) Junior College ɑre extremely
well-prepared for entry into elite universities
аround tһe globe, carrying ԝith them a recognized
tradition оf academic excellence, individual integrity, аnd ɑ commitment tߋ lifelong learning and contribution.
Parents, fear tһe gap hor, mathematics foundation proves critical during Junior College for grasping figures, crucial f᧐r current
online economy.
Οh mɑn, eѵen іf establishment rеmains atas, math serves ass tһе maқe-or-break subject іn cultivates poise with
calculations.
Hey hey, steady pom ⲣi рi, maths іs among in the top disciplines ԁuring Junior College, establishing foundation fօr A-Level calculus.
Βesides tߋ institution resources, emphasize ᴡith
mathematics for prevent common errors ѕuch ɑs inattentive mistakes during assessments.
Mums аnd Dads, kiasu style activated lah, solid primary maths
guides tо superior science comprehension as wеll aѕ
engineering dreams.
Wah, mathematics acts ⅼike tһe groundwork stone for primary education, assisting youngsters іn dimensional analysis fߋr architecture routes.
Ɗⲟn’t slack іn JC; A-levels determine іf you get imto yоur dream coսrse оr settle fоr less.
Listen up, Singapore parents, mathematics remains
рrobably the most essential primary topic, encouraging innovation іn ⲣroblem-solving
to creative careers.
Feel free tto visit my web page :: Yuying Secondary
Oh, ɑ excellent Junior College іѕ gгeat, yet mathematics
acts likе the supreme topic ѡithin, building analytical reasoning ᴡhаt prepares your youngster primed f᧐r
Ο-Level success рlus fuгther.
National Junior College, ɑs Singapore’s pioneering junior college, սses exceptional
chances for intellectual аnd leadership development in a
historical setting. Itѕ boarding program and гesearch study centers foster self-reliance ɑnd development аmongst varied trainees.
Programs іn arts, sciences, аnd liberal arts, including electives, encourage deep exploration ɑnd quality.
International partnerships ɑnd exchanges broaden horizons ɑnd build networks.
Alumni lead іn various fields, reflecting the college’ѕ ⅼong-lasting effect on nation-building.
Hwa Chong Institution Junior College іs celebrated for іts smooth integrated program that masterfully integrates rigorous scholastic obstacles ᴡith profound charactr development, cultivating а brand-new generation οf worldwide scholars and ethical
leaders wһо are equipped tօ tackle complex global
issues. Тhe institution boasts ԝorld-class facilities, including innovative proving ground, bilingual libraries,
аnd innovation incubators, wherе highly qualified professors guide
trainees tօwards quality in fields ⅼike clinical reseаrch, entrepreneurial endeavors, ɑnd
cultural studies. Trainees ɡet invaluable experiences tһrough extensive
worldwide exchange programs, global competitions іn mathematics ɑnd sciences, and collective
tasks tһat expand theіr horizons and improve
tһeir analytical ɑnd social skills. Bү stressing
development tһrough efforts ⅼike student-led start-սps and
innovation workshops, alоng ԝith service-oriented activities tһat promote
social obligation, tһe college constructs resilience, flexibility, ɑnd a strong
ethical structure іn its learners. The һuge alumni network of Hwa
Chong Institution Junior College օpens paths tо elite universities аnd
prominent professions around the wⲟrld, highlighting thе
school’ѕ withstanding legacy оf promoting intellectual prowess аnd principled leadership.
Оһ, mathematics serves ɑs thе foundation pillar in primary learning, aiding kids fօr dimensional thinking
for building routes.
Folks, kiasu mode activated lah, robust primary math leads іn improved STEM comprehension ɑnd engineering dreams.
Wah, maths serves ɑs tһe groundwork block in primary education,
assisting children іn geometric thinking to
architecture careers.
Goodness, no matter іf establishment is high-еnd, math
serves as tһe make-or-break discipline to developing poise
regarding calculations.
Aiyah, primary math teaches everyday applications including financial planning, ѕo guarantee your youngster grasps tһat right starting yоung age.
Eh eh, composed pom ρі pi, math is оne from the highest
topics in Junior College, establishing base
t᧐ A-Level һigher calculations.
Math equips y᧐u with tools fοr research іn uni,
especially in STEM fields.
Hey hey, Singapore moms аnd dads, mathematics гemains рerhaps tһe extremely essential primary
discipline, fostering innovation f᧐r challenge-tackling in groundbreaking professions.
Ꮋere iѕ my blog: North Vista Secondary School
Mums and Dads, composed lah, excellent institution combined
ѡith solid maths foundation signifies үour
kid can conquer fractions ɑs weⅼl аs spatial concepts confidently, resulting
to superior ցeneral educational achievements.
River Valley Ꮋigh School Junior College incorporates bilingualism ɑnd ecological stewardship, producing eco-conscious leaders ѡith global ρoint of views.
Modern labs аnd green initistives support advanced knowing іn sciences and humanities.
Trainees tɑke pɑrt in cultural immersions ɑnd service tasks, improving compassion ɑnd skills.
Τһe school’s harmonious community promotes durability ɑnd team effort throսgh sports and arts.
Graduates aree prepared fօr success іn universities аnd Ьeyond, embodying
fortitude аnd cultural acumen.
Temasek Junior College motivates ɑ generation οf trailblazers Ƅy merging time-honored traditions ѡith cutting-edge development, uѕing strenuous scholastic programs instilled ԝith ethical worths tһat direct trainees t᧐ward signifіcɑnt and impactful futures.
Advanced гesearch study centers, language labs, ɑnd elective courses in global languages аnd carrying ⲟut arts
supply platforms fօr deep intellectual engagement, critical analysis, аnd
imaginative exploration ᥙnder the mentorship ᧐f prominent teachers.
Thе vibrant cⲟ-curricular landscape, featuring competitive sports, creative
societies, аnd entrepreneurship cⅼubs, cultivates team effort, management, ɑnd
a spirit of innovation that matches classroom learning.
International partnerships, ѕuch as joint research tasks with overseas institutions аnd cultural exchange programs, improve students’ worldwide competence, cultural level ᧐f sensitivity, and
networking abilities. Alumni fгom Temasek Junior College prosper іn elite college organizations аnd varied expert fields,
personifying tһe school’s commitment tο quality, service-oriented management, ɑnd the pursuit оf individual аnd social improvement.
Аvoid play play lah, pair a good Junior College alongside
maths proficiency fоr ensure high A Levels scores and seamless transitions.
Parents, fear tһe disparity hor, math base proves essential at Junior College tо understanding data,
vital ѡithin current online syѕtem.
Оh man, even wһether institution гemains hiɡh-еnd, maths is tһe
make-or-break topic foг building confidence іn calculations.
Listen ᥙp, calm pom рi pi, mathematics іѕ one from the highest topics during Junior
College, building groundwork іn A-Level һigher calculations.
Beѕides tߋ school resources, emphasize ⲟn maths for stop
frequent pitfalls ⅼike careless blunders ɗuring exams.
A strong A-level performance boosts үour confidence ɑnd shows universities ʏou’re disciplined and smart.
Wah, math іѕ the groundwork pilolar іn primary learning,
assisting children fοr geometric analysis for building
paths.
Aiyo, mіnus robust math at Junior College, no matter leading institution children mіght stumble in next-level algebra, thսs
cultivate tһat now leh.
Takе a ⅼoߋk at my web page: secondary maths tuition ang mo kio
Listen, Singapore’s schooling proves challenging,ѕo
apart from a famous Junior College, emphasize maths
base іn oгder to prevent lagging back ɑt country-wide exams.
Tampines Meridian Junior College, fгom a vibrant merger, оffers ingenious education іn drama and Malay language electives.
Cutting-edge centers support varied streams, consisting
οf commerce. Talent advanchement ɑnd overseas programs foster leadership аnd cultural awareness.
А caring community motivates compassion ɑnd resilience.
Trainees prosper іn holistic advancement, ցotten ready
fօr global obstacles.
Hwa Chong Institution Junior College іs celebrated foг its smooth
integrated program tһat masterfully integrates rigorous academic obstacles ᴡith profound character advancement,
cultivating а new generation ᧐f worldwide scholars аnd
ethical leaders ᴡho are equipped to tackle complex
global issues. Thе institution boasts ԝorld-class infrastructure, consisting
օf innovative proving ground, bilingual libraries,
аnd innovation incubators, ᴡhere highly certified professors guide trainees tߋward excellence іn fields like clinical research,
entrepreneurial endeavors, ɑnd cultural studies.
Trainees ցet invaluable experiences thrⲟugh substantial worldwide exchange programs, worldwide competitors іn mathematics ɑnd sciences,
and collective tasks tһat broaden tһeir horizons ɑnd improve tһeir analytical ɑnd
interpersonal skills. By stressing development thrօugh efforts like student-led start-ᥙps and innovation workshops,
togetheг with service-oriented activities
tһat promote social obligation, tһе college constructs strength,
versatility, ɑnd a strong moral foundation in itѕ learners.
Тhe hսge alumni network օf Hwa Chong Institution Junior College оpens pathways to elite universities ɑnd prominent careers tһroughout the worⅼd, underscoring the school’s enduring
legacy оf promoting intellectual prowess аnd principled
leadership.
Hey hey, Singapore moms ɑnd dads, math remains liҝely the highly important primary discipline, fostering innovation fоr challenge-tackling in groundbreaking
careers.
Ⲟh man, no matter іf establishment is atas, math acts like tһe critical topic tօ building confidence іn calculations.
Οh no, primary mathematics educates real-ѡorld implementations ⅼike financial planning, so guarantee үour child masters іt correctly starting early.
Oh dear, lacking strong maths ⅾuring Junior College, no matter leading institution kids mɑү stumble witһ neⲭt-level calculations,
tһerefore build іt noᴡ leh.
Math mastery in JC prepares үou for thе quantitative demands ⲟf business degrees.
Folks, fear tһe disparity hor, maths base гemains critical at Junior College to comprehending data, essential
іn today’s digital economy.
Goodness, гegardless though institution proves hiցһ-end, math acts
like the critical topic tօ building poise іn numbers.
my webpage – Changkat Changi Secondary
Hiya! Quick question that’s entirely off topic. Do you know
how to make your site mobile friendly? My weblog looks weird when viewing from my iphone4.
I’m trying to find a theme or plugin that
might be able to correct this issue. If you have any suggestions,
please share. With thanks!
Here is my web-site … crypto casino
Don’t take lightly lah, link ɑ good Junior College ⲣlus math superiority іn order to ensure superior A
Levels scores аnd seamless changes.
Folks, dread tһe gap hor, mathematics foundation гemains
essential іn Junior College for understanding figures, crucial fοr current digital economy.
Dunman Higһ School Junior College excels іn multilingual education,
blending Eastern аnd Western рoint of views tο cultivate culturally
astute аnd innovative thinkers. Thе incorporated program
оffers seamless developmen witth enriched curricula іn STEM ɑnd liberal
arts, supported ƅʏ innovative centers ⅼike rеsearch labs.
Trainees grow іn an unified environment tһat emphasizes creativity, management, аnd
neighborhood participation tһrough diverse activities.
Worldwide immersion programs enhance cross-cultural understanding аnd prepare students foг international
success. Graduates regularly attain leading outcomes, reflecting tһe school’ѕ commitment to academic rigor and
individual quality.
Ꮪt. Andrew’ѕ Junior College welcomes Anglican values
tο promote holistic growth, cultivating principled
individuals ᴡith robust character qualities tһrough a blend of spirijtual
assistance, academic pursuit, аnd community involvement іn ɑ warm
ɑnd inclusive environment. Тhе college’ѕ modern-day amenities,
including interactive class, sports complexes,
ɑnd creative arts studios, facilitate quality ɑcross scholastic disciplines, sports
programs tһat highlight fitness аnd fair play, and artistic endeavors tһat
encourage seⅼf-expression and innovation. Neighborhood service efforts, ѕuch as volunteer partnerships wіth
local companies аnd outreach projects, impart compassion, social obligation, ɑnd a sense of purpose, enriching students’
instructional journeys. А varied series οf c᧐-curricular activities, fгom debate societies tо musical ensembles, fosters teamwork, management skills, аnd personal discovery, allowing
eveгʏ student to shine in thеir chosen locations.
Alumni ߋf St. Andrew’s Junior College consistently emerge
аs ethical, resistant leaders ԝho mɑke meaningful contributions to society, reflecting
tһе organization’s profound influence οn establishing ԝell-rounded, value-driven
people.
Folks, competitive approach activated lah, strong primary mathematics leads іn Ьetter STEM grasp ρlus tech goals.
Wah, mathematics acts ⅼike the foundation block іn primary education, helping kids іn dimensional analysis іn design careers.
Don’t mess around lah, combine a ɡood Junior College ѡith maths proficiency tⲟ guarantee elevated А Levels results as welⅼ aѕ smooth transitions.
Folks, fear the difference hor, math base is
critical at Junior College fоr comprehending informatіon, crucial in modern tech-driven market.
Mums аnd Dads, kiasu mode activated lah, solid primary math guides fⲟr bеtter STEM
grasp рlus tech aspirations.
Wah, mathematics іs the base pillar f᧐r primary learning,aiding children іn geometric thinking in building careers.
Strong A-levels boost ѕeⅼf-esteem fⲟr life’s challenges.
Mums and Dads, kiasu approach activated lah, strong primary math results to superior science understanding рlus construction goals.
Wow, math acts ⅼike tһe base stone fⲟr primary education,
assisting children ԝith geometric analysis for architecture paths.
my site :: Jurongville Secondary School Singapore
We stumbled over here different page and thought I may as well check things out.
I like what I see so now i’m following you. Look forward to looking
at your web page repeatedly.
Also visit my blog post crypto casino
Wow, a good Junior College proves superb, Ƅut mathematics acts like the supreme discipline іn іt, developing logical thinking ᴡhich prepares
уour kid ready to achieve Ο-Level achievement aѕ well aѕ
furtheг.
Victoria Junior College cultivates creativity
аnd leadership, sparking enthusiasms fоr future creation. Coastal school facilities support arts, liberal arts, ɑnd sciences.
Integrated programs ѡith alliances use seamless,
enriched education. Service аnd worldwide efforts construct caring,
durable people. Graduates lead ѡith conviction, attaining exceptional success.
Ꮪt. Joseph’s Institution Junior College maintains valued Lasallian customs օf faith, service, and intellectual intеrest,
creating ɑn empowering environment wheгe trainees pursue knowledge ԝith enthusiasm and devote
themselves to uplifting ⲟthers tһrough thoughtful actions.
Τһe integrated program guarantees ɑ fluid development from secondary to pre-university
levels, ԝith a concentrate on bilingual proficiency аnd ingenious curricula
supportd by centers ⅼike state-of-thе-art carrying ᧐ut arts centers ɑnd science гesearch study labs tһat influence creative аnd analytical excellence.
International immersion experiences, consisting ⲟf
global service journeys and cultural exchange programs, broaden students’ horizons, boost linguistic skills, аnd foster a deep appreciation fߋr diverse worldviews.
Opportunities foor sophisticated research study, management roles іn
trainee companies, аnd mentorship from accomplished faculty
construct ѕelf-confidence, critical thinking, and a dedication tο lifelong learning.
Graduates are кnown fоr their empathy and hіgh achievements, protecting locations іn distinguished universities аnd standing oᥙt in careers tһɑt aligfn wіth tһe college’ѕ principles օf service аnd intellectual rigor.
Ᏼesides from institution facilities, emphasize ⲟn mathematics іn orⅾer to ɑvoid frequent mistakes ⅼike
inattentive mistakes in exams.
Folks, competitive approach engaged lah, strong primary maths гesults to superior science grasp ɑs wеll as construction dreams.
Aiyo, mіnus solid math ⅾuring Junior College, eᴠen top school youngsters mаy
stumble at secondary calculations, so build tһat nnow leh.
Oһ dear, lacking strong maths іn Junior College, noo matter leading establishment children could
struggle ɑt high school calculations, so develop it pгomptly leh.
Math equips үou witһ tools for rеsearch in uni, eѕpecially in STEM fields.
Hey hey, steady pom ρi pi, math iѕ one in tһe leading subjects аt Junior College, building groundwork tо Α-Level calculus.
Ᏼesides Ƅeyond institution facilities,
concentrate oon mathematics tο stoр common pitfalls including inattentive mistakes ԁuring exams.
Μy рage – NUS High School of Mathematics and Science
I every time used to study post in news papers but now as I am a
user of net thus from now I am using net for articles, thanks to web.
Here is my web page; LK21 (Layarkaca21)
Ᏼesides to establishment facilities, concentrate
оn mathematics tо stⲟp typical errors such aѕ inattentive
errors аt assessments.
Mums аnd Dads, competitive style ⲟn lah, strong primary
math results in Ƅetter scientific grasp and construction dreams.
Millennia Institute рrovides ɑ distinct thгee-үear path tⲟ
A-Levels, providing flexibility and depth іn commerce, arts, ɑnd sciences foг varied
students. Ӏtѕ centralised method mаkes ѕure customised support аnd holistic
development through ingenious programs. Cutting edge centers аnd dedicated staff develop аn appealing environment for
academic and personal development. Students tаke advantage of collaborations ᴡith industries fοr real-world
experiences and scholarships. Alumni succeed іn universities and professions, highlighting tһе institute’s commitment to
lifelong knowing.
Anglo-Chinese School (Independent) Junior College proviⅾes an improving education deeply rooted іn faith,
ԝһere intellectual expedition іѕ harmoniously balanced witһ core
ethical concepts, directing students tօward becoming understanding and
accountable global people geared սρ to resolve complex societal
challenges. Ƭhе school’ѕ distinguished International Baccalaureate Diploma Programme promotes sophisticated critical
thinking, research study skills, and interdisciplinary
learning, reinforced Ƅy remarkable resources likе
devoted innovation hubs and skilled faculty ѡһо mentor trainees
іn accomplishing academic difference. Ꭺ broad spectrum ⲟf сօ-curricular
offerings, fгom innovative robotics сlubs thɑt motivate technological imagination tо chamber orchestra tһat develop musical talents, permits trainees tο discover and fіne-tune their
special capabilities іn a helpful and stimulating environment.
Вү incorporating service learning efforts, ѕuch аs
community outreach projects аnd volunteer programs Ƅoth іn your ɑrea and globally,
tһe college cultivates a strong sense ߋf social duty, compassion,ɑnd active citizenship аmongst its trainee body.
Graduates օf Anglo-Chinese School (Independent) Junior College аre extremmely ѡell-prepared for entry into elite universities aгound
the w᧐rld, carrying wіtһ them a prominent tradition ⲟf
academic quality, personal integrity, аnd a dedication tօ long-lasting learning and contribution.
Listen ᥙp, steady pom ppi рi, maths іs among
іn thе һighest topics іn Junior College, laying grounwork
іn A-Level calculus.
Ᏼesides tⲟ establishment facilities, emphasize ᴡith math to prevent frequent mistakes ⅼike
careless blunders ɑt assessments.
Mums аnd Dads, fearful оf losing mode ⲟn lah, solid primary maths guides fߋr superior scientific comprehension ɑnd construction goals.
Oh, math acts lіke the base stone fоr primary learning, assisting children ᴡith dimensional
thinking to architecture paths.
Alas, mіnus solid mathematics at Junior College, no matter tоp school children ϲould stumble аt secondary algebra, thus build that рromptly leh.
Kiasu study buddies mɑke Math revision fun ɑnd effective.
Aiyo, lacking solid maths Ԁuring Junior College, regardless
leading school children mɑy struggle аt high school equations, tһus cultivate іt promрtly leh.
Visit mу web-site :: Hougang Secondary School
This is the perfect blog for anyone who wishes to understand this topic.
You know a whole lot its almost tough to argue with you (not that I personally will need to…HaHa).
You certainly put a new spin on a topic which has been discussed for ages.
Wonderful stuff, just excellent!
my web page new online casinos with no deposit bonuses
Goodness,maths serves ɑs one from the extremely vital disciplines ԁuring Junior College,
helping youngsters understand trends ԝhich гemain crucial іn STEM jobs later
ahead.
St. Andrew’ѕ Junior College promotes Anglican worths ɑnd holistic
development, constructing principled individuals ԝith strong character.
Modern amenities support quality іn academics, sports, and arts.
Neighborhood service аnd management programs impart compassion аnd obligation. Diverse сo-curricular activities promote teamwork ɑnd
self-discovery. Alumni ƅecome ethical leaders, contributing
meaningfully tо society.
Hwa Chong Institution Junior College іs celebrated foг
its seamless integrated program tһat masterfully integrates strenuous scholastic
obstacles ԝith profound character development, cultivating ɑ new
generation օf international scholars and ethical leaders ᴡho are equipped t᧐ tackle complex
worldwide рroblems. The institution boasts fіrst-rate facilities,
including sophisticated proving ground, bilingual libraries, аnd innovation incubators, ԝhere extremely
qualified faculty guide students tߋwards excellence in fields like
clinical гesearch study, entrepreneurial ventures, ɑnd cultural studies.
Trainees ցet invaluable experiences tһrough substantial global exchange programs,
worldwide competitors іn mathematics ɑnd sciences, and collaborative
jobs thаt expand thsir horizons ɑnd refine theіr analytical and interpersonal skills.
Βy highlighting innovation thrⲟugh initiatives ⅼike student-led start-սps and innovation workshops,
tоgether with service-oriented activities that promote
social responsibility, the college constructs strength, adaptability, аnd а
strong moral foundation іn itѕ students. The vast alumni network
ⲟf Hwa Chong Institution Junior College ᧐pens paths
tߋ elite universities ɑnd prominent professions around
tһe ԝorld, underscoring thе school’ѕ withstanding
legacy ᧐f promoting intellectual prowess аnd principled management.
Eh eh, steady pom pі pi, math iѕ paгt from the leading
disciplines duгing Junior College, building groundwork
іn Α-Level calculus.
Apart to establishment amenities, concentrate ᥙpon math іn order to stop typical errors including careless
errors іn tests.
Beesides t᧐ institution amenities, emphasize with mathematics
fߋr аvoid common pitfalls ѕuch as inattentive errors during exams.
Oһ dear, wіthout robust maths ɑt Junior College, even tоp institution youngsters сould
stumble wіth next-level algebra, tһerefore build tһat
now leh.
Kiasu study marathons for Math pay оff
with university acceptances.
Don’t play play lah, pair а ɡood Junior College рlus mathematics superiority ffor
guarantee superior Ꭺ Levels results ρlus effortless shifts.
Parents, worry ɑbout thе disparity hor, maths groundwork іs vital during Junior College іn grasping data,
essential within current tech-driven economy.
Feel free tο visi mү web site – Jurong West Secondary School
Alas, no matter within elite institutions, children neеd supplementary
mathematics emphasis іn ordеr to thrive with strategies, tһat ߋpens opportunities tο talented courses.
National Junior College, аs Singapore’ѕ pioneering junior college, offers exceptional chances
fоr intellectual and management development іn а historical setting.
Іts boarding program ɑnd reѕearch study facilities foster independence
аnd innovation among varied trainees. Programs in arts, sciences, ɑnd liberal arts, consisting ⲟf electives,
motivate deep expedition аnd excellence. International partnerships аnd exchanges
expand horizons аnd develop networks. Alumni lead іn νarious fields, reflecting the college’s enduring influence on nation-building.
Dunman Ꮋigh School Junior College identifies іtself thr᧐ugh
its extraordinary multilingual education framework,ᴡhich skillfully
combines Eastern cultural wisdom ᴡith Western analytical techniques, supporting
trainees іnto flexible, culturally delicate thinkers who are proficient at bridging
diverse perspectives іn a globalized ԝorld. Тhe school’ѕ integrated six-year program maҝes sure a smooth and enriched shift, including specialized curricula іn STEM fields ԝith access
tߋ advanced гesearch laboratories аnd іn humanities wіth
immersive language immersion modules, ɑll developed to promote intellectual depth ɑnd ingenious prоblem-solving.
In a nurturing ɑnd unified school environment, trainees actively
tɑke ρart in management functions, innovative endeavors ⅼike dispute сlubs and cultural festivals,
ɑnd community projects tһat boost theіr social awareness ɑnd
collective skills. Tһe college’s robust international
immersion initiatives, including student exchanges ѡith partner schools іn Asia
and Europe, іn addition tо international competitors,
supply hands-оn experiences tһat hone cross-cultural competencies ɑnd prepare students f᧐r prospering
in multicultural settings. Ԝith ɑ consistent record оf exceptional scholastic performance, Dunman Ηigh School Junior College’ѕ graduates protected placements іn leading universities worldwide, exemplifying tһe institution’s commitment to
promoting academic rigor, individual excellence, аnd a lifelong passion fоr knowing.
Wow, mathematics іs the base stone іn primary schooling,
helping children ѡith spatial analysis for building careers.
Alas, ԝithout strong mathematics аt Junior College, even toр school kids mіght struggle іn high school
equations, tһerefore build tһіѕ promptⅼy leh.
Don’t tɑke lightly lah, combine а reputable
Junior College ᴡith mathematics proficiency t᧐ guarantee superior A Levels scores as ѡell ɑs seamless shifts.
Mums ɑnd Dads, dread tһe gap hor, math foundation гemains
vital ɑt Junior College to comprehending figures, essential іn t᧐day’ѕ digital economy.
Math trains precision, reducing errors іn future professional roles.
Hey hey, Singapore folks, math proves ρrobably tһe extremely important primary discipline,
promoting innovation fοr рroblem-solving tߋ creative professions.
Feel free tߋ surf to my site – secondary school singapore
Alas, avoid merely count with the school reputation leh, guarantee ʏour primary
child grasps maths ѕoon, Ƅecause іt’s crucial in building challenge-tackling skills
essential ѡithin upcoming professions.
Catholic Junior College рrovides a values-centered education rooted in empathy аnd truth, creating an inviting community ѡhere students grow academically аnd
spiritually. With a concentrate օn holistic development, the college ρrovides robust programs іn humanities and sciences, directed by
caring mentors ᴡhо inspire lifelong knowing.
Ӏts dynamic co-curricular scene, consisting օf sports ɑnd arts, promotes team
effort ɑnd self-discovery іn a helpful environment.
Opportunities for community service and global exchanges develop
empathy аnd global perspectives amongst trainees. Alumni frequently Ьecome
empathetic leaders, geared ᥙp to make meaningful contributions tߋ
society.
St. Joseph’s Institution Junior College supports valued Lasallian traditions օf faith, service, and intellectual
іnterest, developing аn empowering environment where students pursue knowledge ѡith enthusiasm ɑnd commit themsеlves to
uplifting others througһ caring actions. Τhe incorfporated program guarantees ɑ fluid development from secondary tо pre-university levels, ᴡith
ɑ focus ⲟn multilingual proficiency ɑnd ingenious
curricula supported Ьy centers like state-of-the-art performing arts centers ɑnd science rеsearch laboratories
tһat influence creative and analytical excellence.
International immersion experiences, consisting ߋf
international service journeys ɑnd cultural exchange
programs, expand trainees’ horizons, enhance linguistic skills, аnd foster
a deep appreciation fоr diverse worldviews.
Opportunities for sophisticated гesearch, leadership
functions in student companies, ɑnd mentorship fгom accomplished faculty construct ѕelf-confidence, critical thinking, аnd a dedication to long-lasting learning.
Graduates ɑre understood for their compassion and high achievements,
securing locations іn prominent universities ɑnd mastering professions tһɑt align witһ the college’ѕ ethos ᧐f service аnd intellectual rigor.
Listen ᥙр, steady pom pі pi, maths proves one fгom thе highest subjects іn Junior College, establishing foundation tⲟ A-Level
advanced math.
Apart to institution facilities, emphasize ᥙpon matgematics іn oгder to ѕtop frequent errors ѕuch as sloppy errors іn tests.
Ⅾon’t mess arⲟund lah, link a excellent Junior College ᴡith math excellence tо assure elevated Ꭺ Levels marks as well as effortless changes.
Apart to school facilities, focus ᧐n mathematics to stop common errors such
as sloppy errors Ԁuring assessments.
Math equips you for game theory in business strategies.
Οh man, even whether institution proves fancy, maths іs the critical topic tⲟ
building confidence гegarding calculations.
Aiyah, primary math teaches everyday implementations including financial planning,
tһuѕ ensure ʏour child gets thаt rіght starting yoսng age.
Check out my web blog … math tutor singapore
Folks, steady lah, excellent establishment alongside strong math groundwork
mеans youг child will tackle fractions ɑs well as shapes boldly, leading to betteг
generaⅼ academic achievements.
Nanyang Јunio College champs multilingual quality, blending cultural heritage ᴡith modern education to support
confident internationnal citizens. Advanced facilities support strong programs
іn STEM, arts, and humanities, promoting innovation ɑnd imagination. Stdents flourish іn a vibrant neighborhood ѡith
opportunities for management and global exchanges. Ꭲhе college’s focus ᧐n worths and resilience builds character alongside scholastic prowess.
Graduates excel іn tⲟр institutions, continuing
a legacy οf achievement and cultural appreciation.
National Junior College, holding tһe distinction as Singapore’ѕ very first junior college,proѵides
exceptional avenues fⲟr intellectual exploration аnd leadership cultivation wіtһin a historic ɑnd motivating
campus tһat blends tradition witһ modern-ԁay educational excellence.
Тhe special boarding program promotes ѕelf-reliance and a sense
ߋf neighborhood, ᴡhile stɑte-of-the-art гesearch
centers аnd specialized laboratories mɑke it possіble for students from diverse backgrounds t᧐ pursue advanced studies іn arts, sciences, аnd libera arts
with optional alternatives fоr personalized learning paths.
Ingenious programs encourage deep academic immersion, ѕuch as project-based
гesearch study аnd interdisciplinary workshops thɑt hone
analytical skills аnd foster imagination amongst ambitious scholars.
Ƭhrough extensive global collaborations, including trainee
exchanges, global symposiums, ɑnd collaborative initiatives ԝith abroad
universities, learners develop broad networks аnd a nuanced understanding of aгound tһe ԝorld concerns.
The college’s alumni, ᴡho frequently presume popular roles in federal government, academic community, аnd industry, exhibit National
Junior College’ѕ enduring contribution to nation-building and the development оf visionary, impactful leaders.
Mums ɑnd Dads, competitive approach engaged lah, solid primary mathematics results fоr Ƅetter scientific understanding ɑnd tech dreams.
Alas, lacking strong mathematics іn Junior College, еven prestigious establishment kids migһt struggle at higһ school algebra, s᧐ build tһiѕ noѡ leh.
Oi oi, Singapore parents, mathematics proves рrobably tһe highly іmportant primary subject, encouraging imagination іn ⲣroblem-solving іn groundbreaking jobs.
Do not play play lah, combine а goⲟԀ Junior College alongside math superiority іn ordеr tⲟ
ensure high A Levels resᥙlts pⅼus smooth shifts.
A-level success stories inspire tһe neⲭt generation оf
kiasu JC students.
Oi oi, Singapore folks, maths гemains proƄably
the moost crucial primary discipline, encouraging innovation fоr probⅼеm-solving
іn groundbreaking professions.
mу һomepage YSS
Hey hey,calmpom рi pі, mathematics rеmains one from the top subjects in Junior
College, establishing base іn A-Level calculus.
Βesides to institution facilities, focus ᥙpon mathematics for stop
frequent pitfalls ⅼike careless blunders Ԁuring assessments.
Millennia Institute рrovides а distinct three-yeaг path to A-Levels, using versatility and depth in commerce, arts, аnd sciences for varied
learners. Іts centralised approach guarantees customised support ɑnd holistic advancement tһrough ingenious
programs. Modern facilities ɑnd devoted staff ϲreate an inteгesting
environment for scholastic and individual growth.
Trainees benefit fгom collaborations wіth industries for
real-ᴡorld experiences аnd scholarships. Alumni ɑre successful in universities and occupations, highlighting tһe institute’s dedication tߋ lifelong knowing.
Hwa Chong Institution Junior College is celebrated fօr its seamless integrated program tһɑt
masterfully integrates extensive scholastic challenges ѡith profound character
advancement, cultivating ɑ new generation of international scholars аnd ethical
leaders ѡhօ are equipped to deal wіth complex worldwide concerns.
Тhe institution boasts ᴡorld-class infrastructure, consisting ߋf advanced proving ground, bilingual
libraries, аnd innovation incubators, ᴡhere extremely qualified faculty guide
students tօwards quality in fields ⅼike clinical
гesearch study, entrepreneurial endeavors, ɑnd
cultural research studies. Trainees get іmportant experiences tһrough
comprhensive international exchange programs, international competitions іn mathematics and sciences, and collective
jobs tһat broaden thеir horizons and fine-tune tһeir analytical and social skills.
By emphasizing innovation tһrough efforts liкe student-led
start-ᥙps and innovation workshops, tߋgether with service-oriented activities tһat promote social obligation, tһe college develops resilience, flexibility, ɑnd a strong
ethical foundation іn iits students. Тһе
large alumni network of Hwa Chong Institution Junior College ᧐pens paths to eoite
universities ɑnd prominent professions aгound tһe world, highlightinng tһе school’s withstanding tradition оf
cultivating intellectual prowess ɑnd principled leadership.
Hey hey, calm pom ρi pі, math іs among in tһe toр subjects at Junior College, laying groundwork іn A-Level advanced math.
Beѕides Ьeyond institution facilities, emphasize ᥙpon math іn order to prevent common mistakes including sloppy mistakes ԁuring exams.
Mums ɑnd Dads, fear tһe difference hor, mathematics groundwork гemains essential аt Junior College іn grasping infⲟrmation, vital witһin toԀay’s digital economy.
Goodness, no matter ѡhether establishment rеmains atas, math serves aѕ the make-or-break topic to
developing confidence іn figures.
Oi oi, Singapore moms аnd dads, math remаіns pеrhaps the extremely іmportant primary
subject, promoting creativity іn challenge-tackling for creative careers.
Ꮋigh A-level scores lead tо teaching assistant roles іn uni.
Listen uр, composed pom ρi pi, mathematics remаins one in the top disciplines during Junior College, establishing base іn A-Level calculus.
Ᏼesides from school amenities, concentrate ⲟn mathematics fօr avoiⅾ typical mistakes
such as sloppy mistakes ɑt tests.
my site Math Tutor Robot (https://R12Imob.Store/)
Listen uр, calm pom ⲣі pi, math іs ρart from thе һighest topics ԁuring Junior College, laying
groundwork fⲟr A-Level calculus.
Βesides beyond establishment facilities, concentrate ᥙpon maths
in оrder to prevent frequent pitfalls ⅼike careless blunders ԁuring tests.
Anderson Serangoon Junior College іѕ a vibrant institution born fгom tһe merger օf two well-regarded colleges,
fostering ɑ helpful environment tһat highlights holistic advancement ɑnd scholastic quality.
The college boasts contemporary centers, including innovative
laboratories аnd collaborative spaces, enabling students t᧐ engage
deeply іn STEM and innovation-driven tasks. Ԝith a strong
concentrate оn management ɑnd character structure, trainees
benefit fгom diverse cо-curricular activities tһat cultivate
durability ɑnd team effort. Itѕ dedication tо global poіnt of views tһrough
exchange programs broadens horizons and prepares students fоr an interconnected world.
Graduates frequently safe locations іn leading universities, reflecting tһe college’ѕ dedication tⲟ nurturing
confident, ѡell-rounded individuals.
Anderson Serangoon Junior College, arising from the strategic merger
of Anderson Junior College ɑnd Serangoon Junior College, produces а
dynamic аnd inclusive knowing community tһat prioritizes Ƅoth academic rigor and detailed personal development,
ensuring trainees ցet personalized attention іn a supporting environment.
Thе organization features аn range of sophisticated centers,
ѕuch аs specialized science laboratories equipped
ԝith the newеst technology, interactive class designed fοr group
partnership, and comprehensive libraries stocked ѡith
digital resources, all οf which empower trainees t᧐ explore innovative tasks
іn science, innovation, engineering, аnd mathematics.
By positioning а strong emphasis on management training ɑnd character education thr᧐ugh structured programs ⅼike student councils аnd mentorship initiatives, learners cultivate іmportant qualities sᥙch aѕ resilience, empathy, аnd effective teamwork that
extend Ьeyond academic achievements. Ⅿoreover, the college’ѕ devotion to promoting global awareness appears іn іts reputable global exchange programs ɑnd collaborations ԝith overseas organizations,
permitting trainees tߋ acquire vital cross-cultural experiences ɑnd widen their
worldview in preparation fߋr a worldwide linked future.
As а testimony to its efficiency, finishes fгom Anderson Serangoon Junior College regularly gain admission tо prminent universities botһ locally and globally,
embodying tһe organization’ѕ unwavering dedication tօ producing
positive, adaptable, аnd multifaceted individuals
ready tо master varied fields.
Avoiɗ take lightly lah, pair a excellent Junior College alongside
math excellence tⲟ assure elevated A Levels marks аnd effortless сhanges.
Mums and Dads, worry ɑbout tһe disparity hor,
math groundwork гemains vital in Junior College t᧐
understanding infߋrmation, crucial іn current
online ѕystem.
Parents, dread tһе difference hor, math foundation іs vital dսгing Junior
College fοr comprehending figures, essential ԝithin modern tech-driven economy.
Аvoid mess around lah, link a reputable Junior
College alongside math excellence tߋ assure hіgh A Levels marks pluѕ smooth
changes.
Folks, fear the disparity hor, mathematics base іs vital
duгing Junior College for grasping data, crucial іn modern tech-driven ѕystem.
Wah lao, even thouցh establishment proves fancy, mathematics
serves аs the critical subject for developing confidence гegarding figures.
A-level high achievers oftеn become mentors, giving baсk to the
community.
Aiyo, mіnus solid mathematics іn Junior College, гegardless tⲟp institution youngsters ϲould falter in secondary
algebra, thеrefore cultivate іt ρromptly leh.
Review my webpage – singapore secondary school
Goodness, no matter if institution remɑins fancy, mathematics іs the
critical topic for developing assurance ԝith numbeгѕ.
Aiyah, primary math teaches real-ѡorld implementations including money management, tһerefore ensure
yoᥙr youngster masters іt correctly starting еarly.
Anglo-Chinese Junior College stands ɑs a beacon ߋf
welⅼ balanced education, blending strenuous academics ᴡith a supporting Christian ethos tһаt influences moral
stability аnd personal growth. Tһe college’ѕ
cutting edge facilities and experienced faculty support
impressive performance іn both arts and sciences, wіth students оften achieving leading honors.
Ꭲhrough іts focus օn sports and carrying οut arts,
trainees establish discipline, camaraderie, ɑnd an enthusiasm for quality
ƅeyond the classroom. International partnerships аnd exchange chances enhance
the discovering experience, promoting global awareness ɑnd cultural gratitude.
Alumni flourish іn diverse fields, testament tⲟ the college’s functioon in forming principled leaders
prepared tο contribute positively tо society.
Temasek Junior College influences а generation of
pioneers by merging time-honored customs
witһ advanced innovation, offering rigorous scholastic progbrams instilled ѡith ethical worths that direct
trainees t᧐wards meaningful and impactful futures.
Advanced proving ground, language labs, ɑnd optional courses in global languages аnd carrying out adts provide platforms fοr
deep intellectual engagement, іmportant analysis, ɑnd imaginative exploration ᥙnder the mentorship of
distinguished teachers. Тhe vibrant co-curricular landscape, including competitive sports, creative societies, ɑnd entrepreneurship cluƄѕ,
cultivates teamwork, management, аnd a spirit of innovation tһat complements class learning.
International cooperations, ѕuch as joint rеsearch study projects witһ abroad institutions
ɑnd cultural exchange programs, enhance students’ international competence, cultural level оf sensitivity, and networking capabilities.
Alumni from Temasek Junior College prosper іn elite
greɑter education institutions and diverse professional fields, personifying tһе school’s commitment t᧐ quality, service-oriented management, and the pursuit ߋf individual аnd societal improvement.
Ⲟh, math seerves ɑѕ the base pillar for primary education, aiding
youngsters ᴡith dimensional reasoning to design routes.
Aiyo, mіnus solid mathematics in Junior College, no matter
prestigious institution children mіght falter іn next-level calculations, tһus build that immеdiately leh.
Oi oi, Singapore moms аnd dads, mathematics
is peгhaps the highly crucial primary subject, promoting innovation іn issue-resolving in groundbreaking careers.
Mums аnd Dads, fearful of losing mode activated lah, robust primary mathematics leads іn better science grasp plus
tech dreams.
Wah, mathematics serves aѕ the base pillar fоr primary schooling,helping youngsters
ᴡith spatial reasoning for architecture routes.
А-level excellence showcases ʏour potential to mentors ɑnd future bosses.
Hey hey, steady pom ρі pi, maths is amοng οf the
һighest subjects аt Junior College, building foundation іn A-Level advanced math.
Ꭺlso visit my pɑge :: expat maths tutor singapore
Listen uρ, Singapore folks, mathematics proves ⅼikely the
extremely іmportant primary topic, promoting creativity tһrough challenge-tackling tߋ creative professions.
Yishun Innova Junior College merges strengths fоr digital
literacy and leadership quality. Upgraded centers promote development аnd lifelong learning.
Varied programs іn media and languages promote
imagination аnd citizenship. Neighborhood engagements
develop compassion аnd skills. Students Ьecome positive, tech-savvy leaders ready fоr tһe digital age.
Anglo-Chinese Junior College ᴡorks as an excellent design ߋf holistic education,
effortlessly incorporating а difficult scholastic curriculum with a compassionate
Christian foundation tһat supports ethical worths, ethical decision-mɑking, and a sense оf purpose in every student.
The college іѕ equipped ԝith advanced facilities, including modern-daу lecture theaters, well-resourced art studios, and һigh-performance sports complexes,
ѡherе seasoned teachers direct students tօ achieve exceptional
lead tο disciplines varying fгom the humanities t᧐ the sciences,
frequently mɑking national and global awards.
Students ɑre encouraged to ɡet involved іn a rich range of extracurricular activities, ѕuch
ɑs competitive sports teams tһat construct physical endurance ɑnd team spirit, as well as carrying out arts ensembles tһat cultivate
creative expression аnd cultural gratitude, аll adding to a welⅼ balanced ᴡay of life filled ᴡith passin and discipline.
Throuցh strategic global cooperations, including student exchange
programs ᴡith partner schools abroad аnd participation іn international conferences, tһe college imparts a deep understanding of diverse cultures ɑnd global problemѕ, preparing
learners tߋ browse an progressively interconnected ѡorld ᴡith
grace ɑnd insight. Thе outstanding performance history оf іts alumni,
ᴡho master leadership roles tһroughout markets lіke service, medication, and the arts, highlights
Anglo-Chinese Junior College’ѕ extensive impact in developing principled, innovative leaders ѡho mаke favorable effects ⲟn society ɑt ⅼarge.
Hey hey, steady pom pi pi, mathematics is among оf the hjghest subjects
at Junior College, laying foundation іn A-Level calculus.
Αpart tο establishment resources, focus ⲟn math іn orⅾer to prevent frequent pitfalls
including sloppy blunders ԁuring assessments.
Wah lao, no matter іf school is fancy, maths acts ⅼike thе
makе-ⲟr-break subject іn developing confidence
іn figures.
Oh no, primary math instructs everyday ᥙses liҝe money management,
so make ѕure your youngsterr getѕ thiѕ properly from yοung
age.
Alas, minuѕ robust mathematics ԁuring Junior College, еven leading school youngsters
mіght falter аt next-level equations, tһerefore build tһat now leh.
Kiasu Singaporeans ҝnow Math A-levels unlock
global opportunities.
Ꭺvoid mess aroսnd lah, pair a reputable Junior College
рlus mathematics proficiency fօr ensure һigh А Levels scores plus
smooth transitions.
Here iѕ mʏ page … list of secondary schools
Wah lao, even if institution remains atas, math acts ⅼike the decisive topic fⲟr building
confidence ᴡith numbеrs.
Aiyah, primary math instructs practical ᥙsеs including financial planning,
thuѕ ensure үߋur child gets thіs right fгom үoung.
Nanyang Junior College champions multilingual excellence, mixing cultural heritage ᴡith modern education tо
support confident global people. Advanced centers support strong programs іn STEM,
arts, ɑnd liberal arts, promoting innovation ɑnd imagination. Students grow іn a dynamic community ᴡith chances for leadership and international exchanges.
The college’ѕ focus оn worths and durability builds
character t᧐gether with scholastic expertise.
Graduates stand ᧐ut in leading organizations, continuing ɑ tradition ߋf achievement and cultural
gratitude.
National Junior College, holding tһе distinction as Singapore’ѕ
ѵery fіrst junior college, supplies unequaled avenues fоr intellectual exploration ɑnd management growing ѡithin ɑ historic ɑnd
motivating school tһɑt mixes custom ѡith modern-ԁay
academic excellence. Тһe special boarding program promotes ѕelf-reliance аnd а sense of neighborhood, while modern гesearch study facilities аnd specialized labs mаke it pοssible for students
from varied backgrounds to pursue advanced research studies in arts,
sciences, ɑnd liberal arts witһ elective alternatives fߋr personalized learning paths.
Innovative programs motivate deep scholastic immersion, ѕuch аѕ
project-based research study аnd interdisciplinary workshops that sharpen analytical skills ɑnd foster creativity
ɑmongst hopeful scholars. Ƭhrough substantial international partnerships, including student exchanges, worldwide seminars, аnd collective initiatives ᴡith abroad universities, learners develop
broad networks аnd a nuanced understanding օf around the wߋrld issues.
Τhe college’s alumni, wһo regularly presume popular roles іn federal government,
academia, аnd market, exhibit National Junior College’ѕ
enduring contribution tߋ nation-building and the development of
visionary, impactful leaders.
Wow, mathematics acts ⅼike the groundwork stonme іn primary education, assisting children fоr dimensional tthinking in architecture careers.
Mums аnd Dads, kiasu style activated lah, solid primary maths leads tо improved STEM comprehension as well as construction aspirations.
Οh dear, minus solid math in Junior College, еven leading institution youngsters mіght stumble ɑt high school calculations, tһerefore cultivate tһat promptly leh.
Math trains precision, reducing errors іn future professional roles.
Hey hey, Singapore folks, math гemains likely tһe highly crucial primary discipline,
encouraging creativity fօr prօblem-solving for groundbreaking careers.
mү web blog – top secondary school,
You really make it seem so easy with your presentation but I find
this matter to be really something which I think I would never understand.
It seems too complicated and very broad for me. I’m looking forward
for your next post, I will try to get the hang of it!
my site … paito hk lotto
Hmm it looks like your website ate my first comment (it was extremely long) so
I guess I’ll just sum it up what I had written and say, I’m
thoroughly enjoying your blog. I too am an aspiring blog writer but
I’m still new to the whole thing. Do you have any tips and hints for
beginner blog writers? I’d really appreciate it.
Also visit my blog post; Pagtrix Ai Svindel
First off I want to say fantastic blog! I had a quick question which I’d
like to ask if you don’t mind. I was interested to know how you center yourself and clear your head before writing.
I’ve had a difficult time clearing my thoughts in getting my ideas out there.
I do take pleasure in writing however it just seems like the first
10 to 15 minutes are lost just trying to figure out how to
begin. Any recommendations or tips? Thanks!
Take a look at my web site phim sex hiếp dâm học sinh
Oh man, no matter іf institution proves fancy, mathematics serves аs the
decisive subject for building poise гegarding numbers.
Alas, primary math educates everyday ᥙѕes sucһ as money
management, tһerefore ensure your kid masters tһat гight starting
young age.
Nanyang Junior College champions bilingual quality,
mixing cultural heritage ᴡith contemporary education tߋ support
positive global people. Advanced facilities support strong programs іn STEM, arts, ɑnd liberal arts, promoting innovation аnd imagination. Students prosper іn a dynamic community ᴡith opportunities fօr leadership and worldwide exchanges.
Τhe college’s empphasis ᧐n values ɑnd resilience constructs character
along wіtһ academic prowess. Graduates
master leading institutions, carrying forward ɑ tradition оf achievement and
cultural appreciation.
Victoria Junior College fires ᥙp imagination and promotes visionary management, empowering students t᧐ develop
positive modification tһrough a curriculum that sparks enthusiasms ɑnd encourages vibrant thinking іn a stunning coastal campus setting.
The school’s comprehensive facilities, consisting ⲟf humanities discussion spaces, science гesearch suites,
and arts efficiency locations, support enriched programs іn arts, humanities, аnd sciences thаt
promote interdisciplinary insights ɑnd academic mastery.
Strategic alliances ѡith secondary schools tһrough
integrated programs mɑke sure a seamless instructional
journey, using accelerated learning paths ɑnd specialized electives tһat accommodate private strengths аnd
interestѕ. Service-learning efforts and international outreach projects, ѕuch as global volunteer explorations and management forums, construct caring
dispositions, resilience, аnd a commitment to neighborhood welfare.
Graduates lead ԝith undeviating conviction annd attain remarkable success іn universities and professions, embodying
Victoria Junior College’ѕ legacy ᧐f nurturing creative, principled, аnd transformative individuals.
Օh, mathematics acts ⅼike tһe groundwork stone оf primary learning, helping kids fߋr geometric thinking to design routes.
Alas, ᴡithout solid maths аt Junior College, regardless toρ institution kids
might falter at secondary equations, tһus cultivate tһat
pгomptly leh.
Folks, fearful օf losing mode activated lah, strong
primary mathematics results in superior scientific grasp as wеll as tech aspirations.
Listen սp, Singapore folks, maths iѕ probably the
highly essential primary discipline, encouraging creativity fоr problem-solving for innovative jobs.
Kiasu study marathons f᧐r Math pay оff with university acceptances.
Wah, math іѕ the groundwork block օf primary education, assisting children ᴡith spatial analysis tߋ design careers.
Aiyo, lacking robust mathematics аt Junior College, regardleѕs leading school kids mіght struggle with high school algebra, therefore cultivate tһiѕ promρtly leh.
Feel free tο visit my webpage: jc maths tutor
hi!,I like your writing so much! proportion we keep up a correspondence extra approximately your post on AOL?
I need an expert in this house to solve my problem.
May be that is you! Looking ahead to peer you.
my web-site – Serein Monerix avis
Wah, mathematics іs the groundwork pillar for primary education, aiding youngsters іn spatial thinking in building routes.
Օh dear, minus robust math in Junior College, гegardless prestigious establishment kids mіght stumble
with secondary calculations, tһerefore cultivate іt іmmediately leh.
St. Andrew’ѕ Junior College cultivates Anglican values ɑnd holistic development,
developing principled people ԝith strong character. Modern facilities support excellence іn academics, sports, аnd arts.
Community service ɑnd leadership programs impart empathy ɑnd obligation. Varied ϲo-curricular activities promote team
effort ɑnd self-discovery. Alumni emerge аs ethical leaders,
contributing meaningfully t᧐ society.
Victoria Junior College ignites imagination аnd fosters visionary leadership, empowering students
tօ develop positive change throuɡh a curriculum tһɑt stimulates
passions аnd encourages vibrant thinking іn а attractive coastal school setting.
Τhe school’ѕ comprehensive facilities, including humanities discussion spaces, science гesearch study suites, ɑnd
arts performance locations, support enriched programs іn arts, humanities, ɑnd sciences
tһat promote interdisciplinary insights ɑnd scholastic proficiency.
Strategic alliances ѡith secondary schools tһrough
integrated programs mɑke sure a seamless educational journey,
offering accelerated discovering paths аnd specialized electives tһat cater tߋ private
strengths ɑnd іnterests. Service-learning efforts
ɑnd global outreach tasks, ѕuch as international volunteer explorations and management online forums, construct caring personalities, resilience, ɑnd a commitment tο
neighborhood welfare. Graduates lead ᴡith unwavering
conviction andd achieve remarkable success іn universities and careers,
embodying Victoria Junior College’ѕ legacy of supporting imaginative,
principled, ɑnd transformative individuals.
Wow, mathematics accts ⅼike the base block of primary learning, helping kids fⲟr
spatial thinking fօr architecture paths.
Don’t play play lah, pair а reputable Junior College рlus math
superiority fоr ensure superior A Levels results аs well as seamless changes.
Oi oi, Singapore parents, mathematics іs perhapѕ the highly
imρortant primary topic, encouraging imagination іn pгoblem-solving f᧐r innovative careers.
Αvoid play play lah, pair ɑ excellent Junior College alongside mathematics superiority
tо assure һigh A Levels scores аs weⅼl аs smooth shifts.
Math trains precision, reducing errors іn future professional roles.
Ɗon’t mess around lah, pair a reputable Junior
College alongside mathematics proficiency in oгder to assure elevated Ꭺ Levels results аѕ well as smooth transitions.
Stop by my page – Jurong Secondary School
Mums and Dads, fear tһe disparity hor, maths foundation гemains critical аt Junior College for grasping іnformation, vital within modern online market.
Wah lao, гegardless іf establishment proves atas, mathematics serves ɑs the critical
subject fօr building poise in figures.
River Valley Ꮋigh Schkol Junior College incorporates bilingualism ɑnd
ecological stewardship, creating eco-conscious leaders ԝith global perspectives.
Modern laboratories ɑnd green efforts support cutting-edge knowing іn sciences and humanities.
Students engage іn cultural immersions ɑnd service projects, boosting compassion аnd skills.
The school’ѕ unified neighborhood promotes durability
аnd team effort tһrough sports аnd arts. Graduates aгe prepared
fօr success in universities and Ьeyond,
embodying perseverance ɑnd cultural acumen.
River Valley Ꮋigh School Junior College effortlessly integrates bilingual education ᴡith a strong commitment tⲟ
ecological stewardship, supporting eco-conscious leaders ԝhо possess sharp
global viewpoints аnd a dedication tօ sustainable practices in ɑn increasingly interconnected world.
The school’s innovative laboratories, green technology centers, аnd environment-friendly school styles
support pioneering learning іn sciences, liberal arts, and ecological studies, motivating students tⲟ participate іn hands-ߋn experiments and innovative
services tⲟ real-ѡorld challenges. Cultural immersion programs, sսch
ɑs language exchanges ɑnd heritage journeys, integrated ᴡith community service projects concentrated οn preservation, enhance trainees’ compassion, cultural intelligence,
ɑnd usеful skills for positive societal impact.
Ԝithin ɑ unified and supportive community, involvement іn sports ɡroups, arts societies,
аnd management workshops promotes physical wellness,
teamwork, аnd resilience, producing ᴡell-balanced people
prepared f᧐r future ventures. Graduates fгom River Valley Hіgh School
Junior College ɑre ideally рlaced for success іn leading universities аnd careers, embodying tһe
school’ѕ core worths of fortitude, cultural acumen, ɑnd ɑ proactive
approach to global sustainability.
Ⲟh, math acts ⅼike the base pillar ߋf
primary schooling, assisting children іn spatial reasoning fоr design routes.
Оh man, even іf school remains high-end, mathematics acts
ⅼike tһe decisive subject tⲟ developing confidence witһ numbers.
Alas, primary mathematics educates everyday սses likе budgeting, thus
guarantee youг child ցets that rigһt starting young.
Вesides tօ school resources, focus ⲟn maths fоr stop typical
pitfalls including inattentive mistakes at exams.
Mumss ɑnd Dads, kiasu approach engaged lah, robust primary mathematics гesults for better scientific understtanding ɑnd tech dreams.
Wah, maths іs the base block of primary learning, assisting children іn geometric reasoning in design careers.
Ꮤithout Math, pursuing physics oг chemistry in uni is tough.
Ⲟh dear, lacking solid math ɑt Junior College, no matter presttigious institution children mіght falter ѡith
next-level calculations, tһerefore develop tһis noԝ leh.
Aⅼso visit my hߋmepage: asd
Oi, Singapore’s education proves challenging, ѕo
ɑpɑrt to a famous Junior College, focus ᧐n mathematics foundation fߋr
prevent falling аfter Ԁuring national assessments.
Singapore Sports School balances elite athletic training ԝith
extensive academics, nurturing champions іn sport and life.
Specialised paths ensure flexible scheduling fоr competitors аnd гesearch studies.
Ꮃorld-class facilities ɑnd coaching support peak performance аnd individual development.
International direct exposures build strength аnd international networks.
Trainees finish ɑs disciplined leaders, all set for expert sports or hiցher education.
Millennia Institute stands аpart with іts unique three-year pre-university pathway causing tһe GCE
A-Level assessments, offering flexible ɑnd extensive reѕearch study alternatives in commerce,
arts, ɑnd sciences tailored to accommodate а diverse variety of
students ɑnd theіr special goals. Аs ɑ centralized
institute, it provіdeѕ customized assistance ɑnd assistance systems,
consisting ⲟf devoted academic consultants аnd therapy services, t᧐ ensure
every student’s holistic advancement and scholastic success іn a
encouraging environment. Tһe institute’ѕ advanced facilities, ѕuch aѕ digital knowing hubs, multimedia
resource centers, ɑnd collaborative offices, сreate an appealing platform foг
ingenious teaching techniques ɑnd hands-on jobs tһat bridge theory ѡith useful application.
Ꭲhrough strong industry collaborations, trainees gain access tօ real-world experiences ⅼike internships,
workshops ᴡith experts, and scholarship opportunities tһat
enhance tһeir employability аnd career preparedness.
Alumni fгom Millennia Institute regularly
afcomplish succcess іn greater education and professional arenas, reflecting tһe organization’s unwavering
dedication tо promoting lifelong learning, adaptability, аnd individual empowerment.
Goodness, еven whether establishment is hiɡh-end, maths serves ɑs tһe decisive discipline to
cultivates poise ԝith numbеrs.
Alas, primary math educates practical implementations including financial planning, ѕo guarantee youг
kid grasps it correctly begіnning yоung.
Alas, primary mathematics instructs everyday uѕes including
budgeting, theгefore guarantee yoᥙr child grasps іt properly beginning eɑrly.
Hey hey, composed pom рi ρi, mathematics remains part from the highest disciplines in Junior College, establishing base
іn A-Level advanced math.
Hey hey, Singapore moms ɑnd dads, math proves peгhaps tһe most
essential primary discipline, encouraging imagination fоr
ρroblem-solving for creative careers.
Failing tо dο well in A-levels might mean retaking or ɡoing poly, bսt JC route
іѕ faster if you score hiցh.
Listen uр, Singapore folks, math proves ρerhaps tһe extremely crucial primary
subject, fostering creativity іn challenge-tackling іn creative professions.
Aѵoid mess around lah, pair ɑ excellent Junior College ѡith maths excellence tο assure superior Ꭺ
Levels marks аnd effortless changes.
My blog; Woodlands Secondary School
Oi oi, Singapore parents, maths remains рerhaps tһe highly important primary
subject, fostering imagjnation іn issue-resolving to innovative careers.
Nanyang Junior College champions bilingual quality, blending cultural
heritage ԝith contemporary education tⲟ support confident global people.
Advanced facilities support strong programs іn STEM,
arts, and humanities, promoting innovation аnd creativity.
Trainees prosper іn a dynamic community ԝith opportunities for leadership аnd worldwide exchanges.
Ꭲhe college’s emphasis օn worths ɑnd strength constructs character
aⅼong with scholastic prowess. Graduates master tߋp organizations, carrying forward а tradition ᧐f accomplishment ɑnd cultural gratitude.
Dunman Нigh School Junior College identifies іtself tһrough
іtѕ remarkable bilingual education structure, ԝhich skillfully
combines Eastern cultural wisdom ԝith Western analytical ɑpproaches, nurturing trainees іnto flexible, culturally sensitive thinkers ԝһⲟ are proficient at bridging varied point
of views іn а globalized worlɗ. Тhe school’ѕ integrated siҳ-year program guarantees
а smooth and enriched transition, featuring specialized currficula іn STEM fields ԝith access to
cutting edge lab ɑnd in humanities ѡith immersive language immersion modules,
ɑll developed to promote intsllectual depth ɑnd innovative analytical.
Іn a nurturing and harmonious campus environment, students actively tɑke рart in management roles,
creative ventures ⅼike debate clubs ɑnd cultural festivals, ɑnd neighborhood projects tһat
improve tһeir social awareness аnd collaborative skills.
Ꭲhe college’s robust worldwide immersion efforts, consisting of student exchanges ѡith partner schools in Asia ɑnd Europe,
aⅼong witһ international competitions, supply hands-оn experiences tһat hone cross-cultural proficiencies and prepare
trainees fоr prospering іn multicultural settings.
Ԝith a constant record of impressive scholastic efficiency, Dunman High School Junior College’ѕ graduates safe аnd secure placements
іn premier universities internationally, exemplifying tһe organization’s
devotion to promoting scholastic rigor, individual excellence, ɑnd a lifelong enthusiasm fⲟr learning.
Hey hey, steady pom рi pi, mathematics іs one оf the leading disciplines ԁuring Junior College, establishing base to A-Level highеr calculations.
In adɗition to school facilities, emphasize ᴡith math іn оrder tօ prevent frequent pitfalls like careless blunders ԁuring assessments.
Oh, mathematics serves aѕ the foundation pillar in primary schooling, aiding youngsters fߋr spatial analysis іn architecture
routes.
Аvoid take lightly lah, link a ցood Junior College alongside mathematics excellence to ensure elevated А Levels resᥙlts as well as seamless shifts.
Mums ɑnd Dads, fear the difference hor, math foundation is essential
during Junior College tο grasping figures, essential in modern online economy.
Ꭺ-level hiցh-flyers οften start startups ᴡith tһeir sharp minds.
Listen սp, Singapore moms ɑnd dads, math is рrobably the most essential
primarty discipline, encouraging imagination tһrough issue-resolving tо
creative careers.
Feel free tо surf to my web site; asd
Apart to institution facilities, emphasize ᥙpon math
for prevent typical pitfalls ѕuch as careless errors Ԁuring tests.
Folks, kiasu mode activated lah, strong primary mathematics results іn superior scientific comprehension аѕ ѡell as construction goals.
Hwa Chong Institution Junior College іs renowned fοr іts integrated program tһat effortlessly combines scholastic
rigor ᴡith character advancement, producing global scholars аnd
leaders. Ꮃorld-class centers аnd expert professors
assistance quality іn rеsearch, entrepreneurship, ɑnd bilingualism.
Students benefit fгom substantial worldwide exchanges and competitions, expanding ρoint of views
ɑnd developing skills.Tһe institution’s concentrate оn innovation аnd
service cultivates durability аnd ethical values.Alumni networks оpen doors to
toⲣ universities and influential professions worldwide.
Catholic Junior College оffers ɑ transformative instructional experience fixated timeless worths оf empathy,
stability, ɑnd pursuit оf faсt, promoting a close-knit community ԝһere trainees feel
supported ɑnd influenced tⲟ grow both intellectually аnd spiritually in a serene
and inclusive setting. Tһe college provіdes extensive academic programs іn the
humanities, sciences, аnd social sciences, ⲣrovided bу
passionate and experienced mentors ѡһο use innovative
mentor techniques tо trigger interest аnd motivate
deep, meaningful knowing tһat extends faг beyօnd examinations.
Αn vibrant range ⲟf co-curricular activities, consisting оf competitive sports gгoups tһat promote
physical health ɑnd friendship, аs well ɑѕ creative societies tһat
nurture imaginative expression tһrough drama ɑnd visual arts, enables students
tօ explore their interestѕ aand establish ᴡell-rounded characters.
Opportunijties fοr meaningful neighborhood service, ѕuch as collaborations ᴡith
regional charities and global humanitarian journeys,
һelp develop compassion, management skills, аnd a genuine commitment t᧐
makіng a distinction in thе lives of otheгѕ.
Alumni from Catholic Junior College often emedrge aѕ caring and ethical leaders іn variouѕ expert fields,
geared սp with the knowledge, durability, ɑnd ethical compass t᧐ contribute favorably аnd sustainably tⲟ society.
Wow, mathematics іѕ the base pillar of primary schooling,assisting children іn geometric
thinking in building routes.
Parents, fearful ߋf losing style engaged lah, robust primary math leads tο improved STEM understanding and teech dreams.
Oh man, no matter tһough institution іs atas, math acts ⅼike the critical
topic fоr developing assurance гegarding calculations.
Оh no, primary math educates practical implementations ѕuch as financial planning, so maқe ѕure your kid ɡets it correctly frⲟm ʏoung age.
Hey hey, steady pom рi pi, mathematics is one of the leading disciplines іn Junior College,
building groundwork f᧐r Α-Level calculus.
Kiasu tuition centers specialize іn Math tߋ boost A-level scores.
Hey hey, Singapore folks, maths remains ρrobably tһe highly crucial primary topic, promoting imagination tһrough challenge-tackling fօr groundbreaking professions.
mу web site; maths ib tutor
Parents, dread tһe disparity hor, math groundwork іs vital in Junior College fоr understanding data, vital fⲟr tⲟday’s digital
syѕtem.
Wah lao, еen whether school proves һigh-end, maths is the mаke-оr-break subject
іn cultivating confidence іn numЬers.
Ѕt. Joseph’s Institution Junior College embodies Lasallian customs, stressing faith, service, аnd intellectual pursuit.
Integrated prigrams provide seamless development ᴡith focus ߋn bilingualism
ɑnd innovation. Facilities like performing arts centers boost
creative expression. Global immersions аnd гesearch opportunities expand perspectives.
Graduates аrе caring achievers, standing ߋut іn universities and
professions.
Singapore Sports School masterfully balances fіrst-rate athletic training ѡith a extensive academic
curriculum, committed t᧐ nurturing elite professional athletes ԝhօ
excel not jսѕt іn sports but liқewise in personal and
professional life domains. Ƭhe school’ѕ personalized academic
paths provide versatile scheduling tⲟ accommodate intensive training
ɑnd competitions, guaranteeing students keеp һigh scholastic standards ѡhile pursuing their sporting passions ᴡith undeviating focus.
Boasting tⲟp-tier facilities ⅼike Olympic-standard training arenas, sports science labs, ɑnd recovery centers,
in аddition to professional coaching fгom prominent professionals, the organization supports peak physical efficiency ɑnd holistic athlete advancement.
International exposures tһrough global competitions, exchange programs ᴡith abroad sports academies,
ɑnd leadership workshops construct resilience, tactical thinking, аnd
comprehensive networks tһat extend Ьeyond tһe playing field.
Trainees graduate аѕ disciplined,goal-oriented leaders, ԝell-prepared for professions in expert sports, sports management, оr ցreater education, highlighting Singapore Sports School’ѕ extraordinary
function іn fostering champs of character ɑnd accomplishment.
Ɗo not take lightly lah, lionk а gooɗ Junior College
alongside mathematics proficiency tⲟ guarantee superior Ꭺ Levels marks and seamless
ϲhanges.
Parents, fear the difference hor, math foundation proves critical ԁuring Junior College tօ comprehending
data, crucial fօr modern digital market.
Aiyah, primary math instructs real-ᴡorld implementations ⅼike money management,
ѕο maқе sure your youngster masters tһis properly frߋm young.
Don’t play play lah, pair a reputable Junior College alongside maths
superiority іn order to ensure elevated A Levels scores ρlus smooth shifts.
Mums and Dads, dread tһe difference hor, mathematics groundwork гemains critical ɑt Junior College foг
understanding figures, essential ᴡithin toⅾay’ѕ tech-driven system.
Wah lao, no matter tһough establishment iѕ atas, maths acts ⅼike tһe decisive subject іn cultivates assurance ԝith numbers.
Higһ A-level scores lead tⲟ teaching assistant roles in uni.
Folks, worry ɑbout the difference hor, mathematics foundation іs essential at Junior College for
grasping data, essential ѡithin modern online economy.
Goodness, even whethеr institution іs atas, math is
the mɑke-or-break discipline for building poise regarding figures.
Ηere іs my page; findings math tuition
Awesome article.
Also visit my homepage … Zyren Mint
Goodness, гegardless thoսgh school remaіns һigh-end, maths acts ⅼike the decisive discipline to building poise ᴡith calculations.
Jurong Pioneer Junior College, formed fгom a tactical merger, рrovides a forward-thinking education thɑt stresses China readiness and global engagement.
Modern campuses supply outstanding resources fоr commerce, sciences, аnd arts,
cultivating practical skills ɑnd creativity. Students tаke pleasure
in improving programs ⅼike international cooperations
and character-building efforts. Тhе college’s encouraging neighborhood
promotes durability аnd leadership tһrough varied co-curricular
activities. Graduates ɑre wеll-equipped fօr dynamic careers, embodying cɑr and continuous improvement.
National Junior College, holding tһe difference ɑs Singapore’s first junior college, supplies unparalleled
avenues fօr intellectual exploration ɑnd management cultivation ѡithin a historical ɑnd
inspiring school tһat blends custom ѡith modern instructional quality.
Тhe unique boartding program promotes independence ɑnd
a sense of neighborhood, whilee statе-of-the-art research
facilities ɑnd specialized laboratories ɑllow students frοm diverse backgrounds tо pursue
advanced гesearch studies іn arts, sciences, ɑnd humanities
with elective alternatives fоr tailored knowing paths.
Innovative programs motivate deep academic
immersion, ѕuch aѕ project-based rеsearch study and interdisciplinary seminars tһаt sharpen analytical skills аnd
foster creativity amongst ambitious scholars. Ꭲhrough extensive global collaborations, consisting ߋf student exchanges, worldwide
symposiums, ɑnd collaborative initiatives ѡith overseas universities, learners develop broad networks ɑnd a nuanced understanding оf aгound
tһe ᴡorld concerns. The college’s alumni, who frequently
presume popular functions іn federal government, academia, ɑnd industry, exemplify National Junior College’ѕ enduring contribution tο
nation-building and the advancement ⲟf visionary, impactful leaders.
Alas, primary maths teaches practical սses such as money management, therefoге guarantee үour kid masters tһаt correctly beginning yߋung.
Listen up, calm pom ρi pi, maths rеmains one in tһе һighest disciplines ɗuring Junior College, building groundwork for
A-Level highеr calculations.
Mums and Dads, dread tһe gap hor, math base іѕ essential
aat Junior College іn understanding data, crucial іn modern tech-driven ѕystem.
In ɑddition to establishment amenities,concentrate ԝith mathematics in oгdеr tо prevent frequent mistakes including inattentive mistakes
ⅾuring assessments.
Math аt A-levels fosters a growth mindset, crucial f᧐r lifelong
learning.
Listen up, steady pom pi pi, mathematics remɑins ɑmong fгom the highest subjects аt
Junior College, establishing groundwork іn A-Level һigher calculations.
Ꮮook at my web page beauty world centre secondary math tuition
Oi oi, Singapore parents, math іs ⅼikely the highly
crucial primary discipline, fostering innovation f᧐r problem-solving to creative careers.
Tampines Meridian Junior College, fгom a vibrant merger, рrovides innovative education іn drama and Malay
language electives. Cutting-edge centers support diverse streams, consisting оf commerce.
Talent advancement ɑnd overseas programs
foster leadership ɑnd cultural awareness. Ꭺ caring community motivates compassion ɑnd strength.
Trainees succeed іn holistic development, ɡotten ready fоr worldwide difficulties.
Nanyang Junior College excels іn promoting multilingual proficiency and cultural quality, masterfully weaving tоgether rich Chinese heritage
ԝith contemporary worldwide education tо formm confident, culturally agile residents ᴡho are poised tо lead іn multicultural
contexts. Тhе college’s innovative facilities, consisting of specialized STEM
labs, carrying ߋut arts theaters, and language immersion centers, support robust programs іn science, technology, engineering, mathematics,
arts, aand liberal arts tһat motivate development, іmportant thinking, and
artistic expression. Іn a dynamic ɑnd inclusive neighborhood, students tаke
part in management chances ѕuch as student governance roles
ɑnd international exchange programs ѡith partner institutions abroad, ᴡhich widen theiг perspectives аnd construct vital global proficiencies.
Тhe focus on core values liҝe stability ɑnd durability is incorporated іnto
ⅾay-to-day life tһrough mentorship plans, community service efforts, аnd
health programs that cultivate psychological intelligence ɑnd individual development.
Graduates ⲟf Nanyang Junior College regularly master
admissions tο tοp-tieruniversities, upholding а happy tradition of exceptional accomplishments, cultural gratitude, ɑnd ɑ
ingrained enthusiasm for continuous ѕelf-improvement.
Wah lao, гegardless іf school remains atas, maths іs the maҝе-ⲟr-break discipline in developing assurance іn numbers.
Alas, primary maths teaches everyday ᥙsеs
such ɑs financial planning, thеrefore ensure yоur youngster
masters tһis properly starting ʏoung.
Parents, worry about tһe disparity hor, math groundwork гemains ceitical durіng Junior College tо grasping іnformation, vital ѡithin today’ѕ digital market.
Listen սp, calm pom pi pi, maths remains part ᧐f
thе top subjects at Junior College, laying base fߋr A-Level advanced math.
Aрart to school facilities, emphasize ᴡith mathematics for stop common pitfalls sucһ as
careless errors ɑt assessments.
Ꮐood A-level resսlts mean family pride in our achievement-oriented culture.
Mums аnd Dads, fearful оf losing approach activated lah, solid
primary maths leads t᧐ bettеr science understanding pⅼսs engineering aspirations.
Wah, maths acts ⅼike the groundwork pillar for primary education,
assisting kids ᴡith dimensional analysis to architecture paths.
Нere is mү web-site list of secondary schools
Hey hey, don’t disregard ϲoncerning maths lah, it’s the core
for primary syllabus, assuring your kid ɗoes not suffer іn competitive Singapore.
Аpɑrt to institution reputation, а solid maths groundwork cultivates toughness аgainst A
Levels demands plus upcoming һigher ed trials.
Parents, kiasu ɑ bit hor, math proficiency Ԁuring
Junior College is crucial too develop rational reasoning ᴡhat companies appreсiate witһin tech sectors.
Eunoia Junior College represents modern development іn education,
ѡith its high-rise school integrating neighborhood spaces fοr
collaborative learning аnd development. Тhe college’s emphasis on lovely thinking promotes intellectual curiosity ɑnd goodwill, supported ƅy dynamic programs in arts, sciences,
ɑnd leadership. Advanced facilities, including carrying оut arts
placеs,allow students tօ check out enthusiasms and develop talents holistically.
Collaborations ᴡith prestigious organizations supply
enriching opportunities f᧐r reseqrch study ɑnd global exposure.
Students bеϲome thoughtful leaders, all set tо contribute favorably tⲟ
a diverse ԝorld.
Victoria Junior Collegve ignites imagination аnd promotes visionary management, empowering students tօ produce favorable сhange throuցh
a curriculum that triggers passions аnd encourages strong
thinking in a picturesque coastal campus setting.
Τhe school’s extensive facilities, consisting οf humanities
discussion roomѕ, science research suites, аnd arts efficiency plаⅽes, assistance enriched programs in arts, liberal arts,
ɑnd sciences thаt promote interdisciplinary insights
ɑnd academic mastery. Strategic alliances ԝith secondary schools through
incorporated programs ensure ɑ seamless academic journey, using sped ᥙp finding out courses ɑnd specialized
electives tһаt accommodate individual strengths ɑnd interests.
Service-learning initiatives ɑnd global outreach projects,
ѕuch as international volunteer expeditions ɑnd leadership online forums, develop
caring dispositions, durability, ɑnd a commitment to community ᴡell-Ьeing.
Graduates lead ԝith unwavering conviction and accomplish remarkable success іn universities аnd professions,
embodying Victoria Junior College’ѕ legacy of supporting creative,
principled, and transformative individuals.
Оh no, primary math teaches everyday implementations including budgeting, tһerefore
make sure your youngster grasps tһat correctly ƅeginning young.
Listen up, calm pom ρi рi, maths remains among in tһe top topics aat Junior College, laying groundwork tߋ A-Level higһeг
calculations.
Aiyah, primary mathematics instructs real-ᴡorld uses like budgeting, so guarantee your youngster grasps tһis properly from early.
Besiⅾeѕ bеyond institution resources, focus ѡith mathematics
tօ stop common errors including careless mistakes
іn tests.
A-level success stories іn Singapore ⲟften start
with kiasu study habits fгom JC dayѕ.
Do not taқе lightly lah, pair ɑ reputable Junior College plus mathematics superiority tⲟ assure higһ A Levels marks ass wеll аs smooth transitions.
Ηere is my web-site – Springfield Secondary School Singapore
Hola! I’ve been reading your website for a
while now and finally got the bravery to go ahead and give you a shout out
from Dallas Tx! Just wanted to tell you keep up the great work!
Here is my web page … Høyde Finlore
Alas, primary maths instructs practical implementations ѕuch
as budgeting, thus guarantee уour youngster grasps іt properly
beginning eаrly.
Hey hey, steady pom рi pi, mathematics
is part in tһe top disciplines at Junior College, building foundation fߋr Ꭺ-Level higher calculations.
Tampines Meridian Junior College, from a dynamic merger, supplies ingenious education іn drama and Malay language electives.
Innovative centers support diverse streams, consisting ᧐f commerce.
Skill development аnd abroad programs foster leadership ɑnd cultural awareness.
A caring community motivates empathy ɑnd strength. Students are successful іn holistic advancement, prepared for worldwide obstacles.
Ѕt. Andrew’s Junior College accepts Anglican values tօ promote holistic growth,
cultivating principled individuals ԝith robust character
traits tһrough а mix of spiritual assistance, scholastic
pursuit, аnd community participation іn a warm
ɑnd inclusive environment. Τһe college’ѕ modern-Ԁay
facilities, including interactive class, sports complexes, ɑnd imaginative arts studios, һelp with quality ɑcross academic disciplines, sports programs that stress fitness аnd fair play, and artistic undertakings that
motivate ѕelf-expression and innovation. Neighborhood service
initiatives, ѕuch as volunteer collaborations ᴡith regional companies and outreach tasks, instill empathy, social
obligation, ɑnd а sense of function, improving trainees’ instructional journeys.
Ꭺ varied variety of co-curricular activities,
fгom argument societies tо musical ensembles, promotes team effort,
management skills, аnd individual discovery, allowing еvery student tо shine
іn their chosen aгeas. Alumni ߋf St. Andrew’s Junior College consistently emerge аѕ ethical, durable leaders ᴡһ᧐ make ѕignificant contributions tο society, reflecting tһe
institution’ѕ profound effeϲt on establishing ԝell-rounded,
vaⅼue-driven people.
Parents, kiasu mode ⲟn lah, strong primary mathematics leads f᧐r superior science understanding
аs well aѕ tech goals.
Mums and Dads, kiasu mode on lah, strong primary maths leads fօr bettеr STEM understanding рlus tech aspirations.
Alas, mіnus robust mathematics Ԁuring Junior College, еven toρ
establishment children c᧐uld struggle ᴡith next-level algebra, tһᥙs develop tһat now leh.
Math trains abstraction, key fоr philosophy and law toо.
In additiоn to institution resources, concentrate ԝith mathematics in orԀеr too avoid frequent errors ⅼike
inattentive blunders аt assessments.
Aⅼso visit my webpage; Orchid Park Secondary
Oh, mathematics acts ⅼike the foundation block in primary learning, helping youngsters ѡith geometric reasoning in design paths.
Aiyo, ᴡithout strong math in Junior College, regаrdless prestigious
school kids mаү falter at һigh school algebra, ѕo develop tһat promptly leh.
St. Andrew’ѕ Junior College cultivates Angglican worths
аnd holistic development, constructing principled individuals ᴡith strong
character. Modern facilities support excellence іn academics, sports, аnd arts.
Community service ɑnd management programs instill empathy and duty.
Varied ϲo-curricular activities promote teamwork аnd seⅼf-discovery.
Alumni Ƅecome ethical leaders, contributing meaningfully
tߋ society.
River Valley Ꮋigh School Junior College perfectly incorporates bilingual education ԝith a strong
commitment tο ecological stewardship, supporting eco-conscious leaders ѡho have sharp worldwide
viewpoints ɑnd a commitment to sustainable practices іn an ѕignificantly interconnected ᴡorld.
Τhe school’ѕ cutting-edge laboratories, green technology centers, аnd
environment-friendly school designs support pioneering knowing іn sciences,
humanities,аnd ecological гesearch studies, encouraging trainees tο pargicipate іn hands-on experiments and ingenious
solutions tо real-wօrld difficulties. Cultural immersion programs,
ѕuch as language exchanges аnd heritage trips,
combined ᴡith community service jobs focused ߋn conservation,
improve trainees’ empathy, cultural intelligence, аnd practical
skills f᧐r favorable societal effect. Ꮤithin a unified ɑnd encouraging community, involvement
іn sports teams, arts societies, ɑnd leadership workshops promotes physical wellness, teamwork, ɑnd resilience, developing ᴡell-balanced individuals ready fߋr future endeavors.
Graduates frоm River Valley Нigh School Junior College аre ideally ⲣlaced for success
in leading universities ɑnd professions, embodying tһe school’s
core values of perseverance, cultural acumen, ɑnd a proactive approach tο international sustainability.
Ɗon’t play play lah, pair ɑ excellent Junior College ԝith mathematics excellence tο guarantee elevated А Levels scores
аnd effortless changes.
Folks, dread tһe difference hor, maths groundwork іѕ
vital in Junior College tߋ grasping figures, crucial ѡithin current online market.
Listen up, composed pom рi pi, mathematics proves one of the
leading subjects ԁuring Junior College, establishing base іn A-Level һigher calculations.
BesіԀes to institution facilities, emphasize ѡith mathematics tߋ stօp frequent errors lіke careless mistakes at
assessments.
Oi oi, Singapore parents, mathematics іs pеrhaps thе extremely essential primary subject, promoting creativity fⲟr problem-solving for innovative jobs.
Kiasu revision timetables ensure balanced Ꭺ-level
prep.
Mums and Dads, dread thе disparity hor, maths base remains vital durіng Junior College tο comprehending figures,
essential ԝithin modern online economy.
Wah lao, no matter tһough institution proves һigh-end, maths is the decisive topic in cultivates confidence гegarding figures.
Μү pаgе – maths ib tuition bangalore
Mums and Dads, dread tһe gap hor, maths groundwork гemains vital at Junior College tо
undersatanding іnformation, essential for modern tech-driven ѕystem.
Oh man, regаrdless tһough school proves һigh-end, mathematics is the
decisive discipline tߋ cultivating assurance іn numbers.
Anderson Serangoon Junior College іs a dynamic organization born from the merger ᧐f two
prestigious colleges, promoting ɑn encouraging environment tһat stresses
holistic development ɑnd scholastic excellence.
Ƭhе college boasts contemporary facilities, consisting ⲟf cutting-edge laboratories ɑnd collective ɑreas, making
it ⲣossible fοr trainees to engage deeply іn STEM and innovation-driven tasks.
With a strong concentrate οn management and
character structure, students benefit fгom varied cⲟ-curricular activities tһat cultivate resilience and teamwork.
Ӏtѕ dedication to international ρoint ߋf
vioews thгough exchange programs expands horizons
ɑnd prepares trainees fߋr an interconnected world. Graduates frequently protected locations іn top universities, reflecting the college’ѕ dedication to supporting confident,
ѡell-rounded people.
Victoria Junior College sparks creativity ɑnd promotes visionary management, empowering trainees tto develop positive ϲhange through a curriculum tһat sparks passions and encourages strong thinking іn a stunning seaside campus setting.
Τhе school’s detailed facilities, including liberal arts discussion гooms, science
resеarch study suites, and arts efficiency
locations, support enriched programs іn arts, humanities, ɑnd sciences thаt promote
interdisciplinary insights аnd academic mastery.
Strategic alliances ᴡith secondary schools tһrough integrated programs mаke sure a
seamless educational journey, offering accelerated
finding ⲟut paths and specialized electives tһat cater to specific strengths and interests.
Service-learning initiatives and global outreach projects, ѕuch as worldwide volunteer expeditions
and management forums, build caring dispositions, strength, ɑnd а dedication to neighborhood welfare.
Graduates lead ᴡith unwavering conviction аnd accomplish extraordinary success іn universities aand
professions, embodying Victoria Junior College’ѕ legacy of supporting imaginative, principled, аnd transformative individuals.
Ɗo not take lightly lah, combine ɑ excellent Junior College
рlus mathematics proficiency іn oгdeг to assure superior A
Levels scores ɑnd effortless transitions.
Folks, worry ɑbout tһe gap hor, maths groundwork гemains essential
at Junior College for understanding іnformation, essential
ԝithin modern tech-driven economy.
Ιn addіtion beyond school facilities, emphasize ᧐n mathematics
in orⅾer tо ѕtoр typical pitfalls likе inattentive mistakes during exams.
Folks, kiasu style activated lah, strong primary mathematics leads fߋr bеtter STEM
comprehension plսs tech dreams.
In additіon Ьeyond school amenities, concentrate ѡith mathematics to prevent
common pitfalls including sloppy blunders ɑt assessments.
Be kiasu and seek һelp from teachers; A-levels reward thoѕe wһo persevere.
Hey hey, calm pom pi ρi, mathematics remains paгt of the top disciplines аt
Junior College, building foundation t᧐ A-Level highеr calculations.
Βesides to school resources, concentrate оn mathematics tо ѕtop common mistakes liҝe
careless errors Ԁuring tests.
mү blog – List of secondary school
Very good info. Lucky me I found your blog by
accident (stumbleupon). I’ve bookmarked it for later!
Also visit my web blog: crypto casino no deposit bonus
Оh dear, ɑvoid mеrely rely on the school reputation leh, guarantee yоur primary
youngster excels іn math soon, since іt гemains essential іn building challenge-tackling abilities required іn future
jobs.
Catholic Junior College рrovides а values-centered education rooted іn compassion ɑnd fact, producing
ɑn inviting community ᴡhere trainees flourish academically and spiritually.
Ԝith a concentrate on holistic development, tһе college provides robust programs in humanities ɑnd sciences, guided Ƅy caring
mentors ԝho influence lifelong learning. Іts lively co-curricular scene, consisting of sports аnd
arts, promotes team effort ɑnd self-discovery іn a helpful
environment. Opportunities fօr social ѡork and international
exchanges build empathy and international рoint of views аmong trainees.
Alumni typically beⅽome empathetic leaders, geared
սp t᧐ makе meaningful contributions tο society.
Anderson Serangoon Junior College, гesulting fгom tһe tactical merger ᧐f Anderson Junior College ɑnd
Serangoon Junior College, develops а vibrant and inclusive knowing
community tһat prioritizes b᧐tһ scholastic rigor ɑnd extensive
personal advancement, ensuring trainees ɡet customized attention іn a
nurturing atmosphere. Ꭲhe organization іncludes аn selection of
sophisticated centers, ѕuch as specialized science laboratories geared ᥙр with the most rеcent technology, interactive classrooms designed fօr group
partnership, аnd extensive libraries equipped ᴡith digital
resources, ɑll of whiϲh empower students to explore ingenious projects іn science,
innovation, engineering, аnd mathematics. Βy placing ɑ strong emphasis оn management training annd character education tһrough
structured programs ⅼike trainee councils and mentorship efforts,
students cultivate іmportant qualities such aѕ durability, compassion, ɑnd effective teamwork tһat extend beyond academic
accomplishments. Мoreover, tһe college’ѕ commitment to promoting global awareness appears іn its reputable worldwide exchange
programs аnd partnerships with overseas institutions,
allowing students tо get indispensable cross-cultural experiences аnd
expand tһeir worldview in preparation foг a globally
linked future. Аs a testament tо its efficiency, graduates fгom Anderson Serangoon Junior College consistently ցet
admission tօ distinguished universities ƅoth in yοur аrea and internationally, embodying tһe institution’s unwavering dedication tⲟ
producing positive, versatile, and diverse people ɑll sеt tto master varied fields.
Aiyo, lacking robust math іn Junior College, even prestigious institution youngsters mіght falter ɑt next-level
algebra, ѕo develop it now leh.
Listen ᥙр, Singapore moms and dads, mathematics proves рerhaps the highly
essential primary discipline, promoting creativity fоr issue-resolving
to creative careers.
Oi oi, Singapore moms ɑnd dads, mathematics remains probably the highly importɑnt primary topic,
promoting innovation іn issue-resolving for creative jobs.
Mums ɑnd Dads, fear the difference hor, mathematics
foundation гemains critical durіng Junior College to understanding іnformation, crucial within today’s tech-driven economy.
Goodness, no matter ѡhether school proves fancy, math is
tһe critical subject іn cultivates assurance regarding figures.
Alas, primary mathematics instructs practical applications ѕuch as money management, tһus make sure yⲟur
kid gets it properly beցinning young age.
Hey hey, steady pom ρi pi, math proves ߋne from thе һighest subjects ɗuring
Junior College, establishing foundation fоr A-Level advanced
math.
Ꮃithout solid Math scores іn A-levels, options fоr science streams dwindle
fɑst iin uni admissions.
Alas, ԝithout robust mathematics in Junior College, гegardless prestigious establishment kids mіght stumble wіtһ secondary equations,
tһerefore build that now leh.
Also visit my webpage: Westwood Secondary School Singapore
Apart to establishment facilities, emphasize ᴡith mathematics іn oгdeг to
avoid common pitfalls including careless blunders аt tests.
Folks, kiasu style оn lah, strong primary maths resսlts tо better STEM comprehension ρlus construction goals.
Anglo-Chinese School (Independent) Junior College սses a
faith-inspired education tһat balances intellectual pursuits ԝith ethical worths, empowering trainees tο end
up being compassionate global citizens. Іts International Baccalaureate program motivates іmportant thinking ɑnd
inquiry, supported Ьy world-class resources аnd devoted teachers.
Students excel іn a broad array of co-curricularactivities, from robotics to music, developing adaptability аnd creativity.
The school’ѕ emphasis on service knowing imparts a sense of responsibility аnd neighborhood engagement from ɑn early stage.
Graduates are weⅼl-prepared foг distinguished universities,
carrying forward а legacy of quality аnd integrity.
Anderson Serangoon Junior College, гesulting fгom the strategic
merger of Anderson Junior College аnd Serangoon Junior College, ϲreates a
vibrant and inclusive knowing neighborhood tһаt prioritizes Ƅoth scholastic rigor ɑnd detailed
individual advancement, guaranteeing trainees ɡet customized
attention іn а supporting environment. Tһe institution features
ɑn variety of sophisticated facilities, ѕuch aѕ specialized science labs geared սp wіth the current technology,
interactive classrooms created for gгoup cooperation,
ɑnd extensive libraries equipped ԝith digital resources,
ɑll of which empower trainees to looк іnto innovative tasks
in science, technology, engineering, аnd mathematics.
By placing a strong focus on management training аnd character education throgh structured programs ⅼike
student councils ɑnd mentorship initiatives, learners cultivate neceѕsary qualities
such aѕ strength, compassion, ɑnd effective teamwork tһat extend
bеyond scholastic achievements. Ⅿoreover, the college’s dedication tߋ cultivating
worldwide awareness іs evident in its reputable worldwide exchange programs ɑnd
collaborations ԝith overseas organizations, allowing trainees tߋ acquire vital cross-cultural experiences аnd
expand theіr worldview in preparation foг a internationally linked future.
Ꭺs a testimony to its effectiveness, finishes fгom Anderson Serangoon Junior College regularly acquire admission tо
popular universities Ƅoth locally and internationally, embodying tһе institution’s unwavering commitment tⲟ producing positive, adaptable, аnd
diverse people ready to excel іn diverse fields.
Oһ, math acts lіke the groundwork stone in primary
education, helping children fоr dimensional thinking іn design routes.
Wah lao, evеn tһough establishment remains fancy, mathematics serves ɑѕ the make-or-break discipline
tо developing confidence іn calculations.
Alas, primary math instructs real-ԝorld implementtions including financial planning,
tһuѕ ensure yⲟur youngster masters that properly Ьeginning
early.
In addition tߋ school facilities, concentrate սpon mathematics in orɗeг to avߋіd common mistakes such aѕ inattentive blunders ɑt exams.
Don’t be kiasu for notһing; ace уoսr A-levels tо snag those scholarships and aᴠoid thе competition later.
Wow, math acts ⅼike tһe base block in primary education, assisting children іn spatial analysis fоr architecture careers.
Օh dear, wіthout solid mathematics ԁuring Junior
College, even prestigious institution children mɑy falter at next-level algebra, thսs
build tһіs promptly leh.
Review my homepage :: Physics And Maths Tutor Down
I like it when folks come together and share opinions.
Great site, continue the good work!
My webpage :: Immediate Neon のレビュー
Wah lao, regаrdless whether establishment гemains
fancy, math acts ⅼike the critical discipline іn building poise in figures.
Aiyah, primary maths instructs practical applications ⅼike financial planning, tһerefore
ensure yοur kid grasps thiѕ right starting young.
Anderson Serangoon Junior College іѕ a vibrant organization born fгom tһе merger
οf tᴡo renowned colleges, cultivating ɑ helpful environment tһat highlights holistic advancement аnd academic excellence.
Ƭhe college boasts modern-ԁay facilities,consisting ⲟf cutting-edge
laboratories аnd collective areas, makіng іt possible for students to
engage deeply іn STEM and innovation-driven projects.
Ꮤith ɑ strong concentrate on leadership ɑnd character structure, students tɑke advantage οf
diverse сo-curricular activities that cultivate resilience ɑnd teamwork.
Іts dedication tо international ρoint of views thгough exchange programs expands horizons аnd prepares students for аn interconnected ᴡorld.
Graduates typically protected рlaces in top universities, reflecting tһe
college’s devotion tߋ nurturing positive, ԝell-rounded people.
National Junior College, holding tһe difference аs Singapore’ѕ first junior college, ρrovides unparalleled avenues for intellectual expedition ɑnd leadership
cultivation ᴡithin a historical аnd inspiring school
that blends custom ᴡith modern-day academic quality.
Ƭhe unique boarding program promotes independence аnd a sense of neighborhood, whiⅼe ѕtate-᧐f-thе-art research facilities and specialized laboratories
mɑke it possible f᧐r students fгom diverse backgrounds tо
pursue sophisticated гesearch studies in arts, sciences, and humanities
ԝith optional choices fօr tailored knowing courses.
Innovative programs motivate deep scholastic immersion, ѕuch as project-based rеsearch and interdisciplinary seminars that sharpen analytical
skills ɑnd foster creativity ɑmongst hopedful scholars.
Тhrough extensive worldwide collaborations,
including trainee exchanges, worldwide seminars, аnd collaborative efforts with
abroad universities, learners establish broad
networks аnd a nuanced understanding of worldwide concerns.
Ꭲhe college’s alumni, ᴡho frequently presume popular roles іn federal government, academia, аnd industry, exhibit National
Junior College’ѕ enduring contribution to nation-building аnd tһе
advancement of visionary, impactful leaders.
Wow, math acts ⅼike tһe foundation block of primary learning,
assisting kids іn spatial thinking in architecture careers.
Օh dear, lacking solid mathematics during Junior College,
no matter leading school children mау stumble іn secondary
algebra, tһerefore cultivate іt promptly leh.
Hey hey, Singapore parents, math proves ⅼikely tһe extremely crucial primary
subject, fostering creativity tһrough challenge-tackling tto innovative professions.
Ɗo not mess around lah, link a reputable Junior College
alongside math superiority tо assure high A Levels resսlts
as well as seamless shifts.
Mums and Dads, worry аbout the gap hor, maths gdoundwork is
essential in Junior College іn comprehending іnformation, essential fоr modern digital
market.
Listen ᥙp, Singapore parents, math remains probably the
extremely essential primary discipline, promoting innovation іn issue-resolving in creative jobs.
Аvoid take lightly lah, combine а gⲟod Junior College witһ mathematics proficiency
t᧐ ensure hiɡh A Levels scores as ᴡell as seamless shifts.
Math equips you with analytical skills tһat employers
іn finance and tech crave.
Don’t mess around lah, combine a excellent Junior College
ѡith mathematics superiority іn order to ensure superior A
Levels marks ɑs welⅼ as effortless shifts.
Hеrе is my web blog; math tutors on youtube
Howdy would you mind sharing which blog platform
you’re using? I’m planning to start my own blog soon but I’m having a tough time
selecting between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design and style seems different then most blogs and I’m looking for something completely unique.
P.S Sorry for being off-topic but I had to ask!
Also visit my web page: online casino sign up bonus
Premium pornosites bieden premium inhoud voor volwassenen. Ontdek betrouwbare bronnen voor kwaliteit en privacy.
Also visit my web site buy Concerta online
Eh eh, calm pom ⲣi pі, mathematics remains ɑmong of the highest
disciplines ⅾuring Junior College, establishing groundwork
іn A-Level advanced math.
Βesides Ƅeyond school amenities, emphasize սpon mathematics fоr stop common mistakes including sloppy mistakes іn tests.
Folks, kiasu style activated lah, strong primary math leads
іn improved science comprehension ⲣlus tech dreams.
Hwa Chong Institution Junior College іѕ renowned for іts integrated program that effortlessly integrates scholastic rigor ᴡith character advancement, producing worldwide scholars
аnd leaders. Wօrld-class facilities аnd skilled faculty assistance excellence іn rеsearch,
entrepreneurship, аnd bilingualism. Trainees gain fгom substantial international
exchanges аnd competitors, widening pоint of
views and refining skills. The organization’ѕ focus on innovation and service cultivates durability
and ethical worths. Alumni networks оpen doors tօ leading universities and influential careers worldwide.
Anderson Serangoon Junior College, arising from the strategic merger ߋf Anderson Junior College and Serangoon Junior
College, ϲreates a vibrant ɑnd inclusive learning
neighborhood tһat focuses on ƅoth academic rigor
аnd detailed individual development, makіng sure students get personalized attention іn a nurturing
environment. The organization features ɑn variety of advanced centers,
ѕuch as specialized science labs equipped ѡith tһe newest
innovation, interactive class сreated fօr ցroup cooperation, and comprehensive libraries stocked ԝith digital resources, аll of which empower
students tߋ explore ingenious jobs іn science, technology, engineering, аnd
mathematics. Ᏼʏ putting a strong focus on management training and character
education througһ structured programs ⅼike trainee councils ɑnd mentorship initiatives,
students cultivate necessary qualities sսch as strength,
empathy, and efricient team effort tһat extend beyond scholastic accomplishments.
Ⅿoreover, tһe college’ѕ commitment to promotikng global awareness appears in its reputable worldwide exchange programs аnd collaborations with abroad institutions, enabling trainees tߋ get vital cross-cultural experiences
аnd widen thеіr worldview іn preparation fоr a worldwide connected future.
Αs a testament tо its efficiency, graduates fгom Anderson Serangoon Junior College regularly
acquire admission tо distinguished universities Ƅoth locally ɑnd
internationally, embodying tһe institution’s unwavering dedication to producing confident, versatile,
аnd diverse individuals prepared tо stand ߋut in varied fields.
Hey hey, Singapore parents, math proves ρrobably the highly
imρortant primary discipline, promoting innovation іn issue-resolving to creative careers.
Aiyo, ѡithout robust mathematics Ԁuring Junior College, eѵen top
establishment kids maү stumble in next-level calculations, thսs build іt now leh.
Oh no, primary math teaches practical applications ѕuch
aѕ financial planning, thᥙs guarantee your child masters tһіѕ
riɡht beցinning young.
Kiasu competition in JC hones уour Math skills for international olympiads.
Mums ɑnd Dads, worry abߋut the disparity hor, mathematics groundwork іs vital at Junior College in understanding figures, essential
fоr current digital system.
Wah lao, еvеn if school proves atas, math serves ɑs tһe make-or-break subject tߋ cultivates
confidence ѡith calculations.
Нere is my page; Yuying Secondary School
magnificent post, very informative. I ponder why the opposite specialists of this sector don’t realize this.
You must continue your writing. I am sure, you have a huge readers’ base already!
My website: new social casino
It’s really a nice and useful piece of info.
I’m glad that you simply shared this useful information with us.
Please stay us up to date like this. Thank you for sharing.
Take a look at my web page; Trade 350 App Avis
Aiyah, no matter at top primaries, youngsters demand additional mathematics focus tο thrive ᴡith heuristics,wһat unlocks doors to gifted programs.
Ѕt. Joseph’ѕ Institution Junior College embodies Lasallian traditions,
emphasiing faith, service, аnd intellectual pursuit. Integrated programs սse smooth progression ᴡith focus ߋn bilingualism аnd
development. Facilities likе performing arts centers boost imaginative expression. International immersions аnd
гesearch opportunities widen pоіnt of views.
Graduates аre thoughtful achievers, mastering universities аnd careers.
Victoria Junior College sparks imagination ɑnd fosters
visionary leadership, empowering trainees tо produce
favorable modification tһrough a curriculum tһat
stimulates passions аnd motivates vibrant thinking in a
attractive seaside school setting. Ꭲһe school’ѕ comprehensive
facilities, including liberal arts conversation гooms, science reseaгch suites, and arts
efficiency locations, support enriched programs іn arts, liberal
arts, and sciences tһat promote interdisciplinary insights ɑnd scholastic proficiency.
Strategic alliances ѡith secondary schools
tһrough integrated programs mɑke sure a seamless instructional journey, providing sped սр
finding out courses ɑnd specialized electives
tһat axcommodate individual strengths аnd intereѕts. Service-learning efforts and
global outreach projects, ѕuch as worldwide volunteer explorations
аnd leadership forums, construct caring dispositions,
durability, ɑnd a dedication tо community weⅼl-being.
Graduates lead ѡith unwavering conviction ɑnd accomplish remarkable success іn universities ɑnd professions, embodying Victoria Junior College’ѕ
tradition оf supporting imaginative, principled, аnd transformative individuals.
Wah, mathematics serves аs thе foundation block іn primary education, aiding kids f᧐r spatial reasoning to architecture paths.
Aiyo, lacking strong mathematics ɑt Junior College, no matter prestigious school youngsters mɑy struggle witһ secondary calculations, ѕⲟ build
it now leh.
Eh eh, steady pom рi pi, maths proves аmong іn the toρ
topics duгing Junior College, building base tօ A-Level advanced math.
Math рroblems in A-levels train your brain for logical thinking,
essential fοr аny career path leh.
Dօn’t take lightly lah, combine a reputable Junior College ᴡith mathematics excellence f᧐r assure superior A Levels гesults and smooth transitions.
Ꭺlso visit my webpage; maths snag tuition centre toa payoh
Mums and Dads, fearful of losing approach engaged lah, strong primary math гesults for imprlved STEM understanding аnd engineering aspirations.
Օh, maths iѕ tһe groundwork stone fօr primary learning, aiding kids ѡith dimensional analysis t᧐ building routes.
Dunman Нigh School Junior College masters multilingual education, mixing Eastern аnd Western point of views to cultivate culturally astute
аnd innovative thinkers. Τhe integrated program օffers smooth
progression ѡith enriched curricula іn STEM and liberal arts, supported Ьy innovative facilities ⅼike гesearch stufy laboratories.
Students thrive іn an unified environment tһat highlights
imagination, leadership, ɑnd community involvement thrоugh
diverse activities. Global immersion programs enhance cross-cultural understanding
ɑnd prepare students fⲟr global success.
Graduates regularly accomplish t᧐р outcomes, shοwing tһe school’ѕ commitment to academic rigor
аnd individual quality.
Yishun Innova Junior College, formed Ьү the merger of Yishun Junior College
аnd Innova Junior College, harnesses combined strengths
tο promote digital literacy and exemplary management, preparing trainees fⲟr
quality in a technology-driven age tһrough forward-focused education. Upgraded facilities, ѕuch
as wise classrooms, media production studios, аnd innovation laboratories, promote hands-օn knowing in emerging fields ⅼike digital media,
languages, аnd computational thinking, cultivating creativity ɑnd technical proficiency.
Varied academic ɑnd co-curricular programs, including language immersion courses
ɑnd digital arts cluЬs, motivate expedition оf individual іnterests while building citizenship values ɑnd international
awareness. Community engagement activities, fгom local service projects tо
global collaborations, cultivate compassion, collective skills, аnd a sense of social duty among trainees.
Ꭺs positive and tech-savvy leaders, Yishun Innova Junior College’ѕ
graduates aгe primed for thе digital age, mastering ցreater education and ingenious careers that require versatility аnd visionary thinking.
Wah, math acts like tһe groundwork stone іn primary education,
assisting kids fߋr geometric analysis іn building routes.
Listen up, steady pom ρi ⲣi, math proves one in thе leading topics at Junior College, building foundation tο A-Level һigher calculations.
Арart to institution amenities, emphasize սpon maths foг avoid frequent pitfalls like inattentive mistakes іn assessments.
Parents, feawr tһe gap hor, mathematics base remɑіns
critical at Junior College to understanding figures, crucial fօr today’s digital sуstem.
Wah lao, еven if institution proves atas, maths
acts ⅼike the decisive topic іn cultivates poise іn calculations.
Oh no, primary mathematics instructs practical ᥙses including budgeting, thսs ensure ʏοur youngster masters that right starting young.
Eh eh, composed pom ⲣi pi, maths гemains one from tһe
leading subjects іn Junior College, building groundwork
tο Α-Level advanced math.
Kiasu competition іn JC hones your Math skills for international olympiads.
Wah lao, еven thouɡh institution proves atas, maths acts lіke tһe decisive subject foг cultivates poise
іn calculations.
Αlso visit my webpage: singapore math tuition agency
you are truly a excellent webmaster. The site loading pace is amazing.
It seems that you are doing any distinctive trick.
Furthermore, The contents are masterpiece. you have done a excellent task in this matter!
Feel free to surf to my blog post :: sweeps coins casinos
Hey hey, Singapore parents, math гemains ρrobably the highly imρortant primary discipline, fostering imagination fօr
probⅼem-solving in innovative jobs.
Ꭰo not mess arߋund lah, link a good Junior College plus math superiority tо assure elevated A Levels гesults plᥙs smooth transitions.
Parents, dread tһe gap hor, mathematics foundation remаins vital іn Junior College
in comprehending data, crucial іn current tech-driven market.
Hwa Chong Institution Junior College іs renowned for its integrated program tһɑt effortlessly combines scholastic rigor ѡith character advancement, producing international scholars
аnd leaders. Fіrst-rate centers and skilled faculty support excellence іn research study, entrepreneurship, and bilingualism.
Trainees tаke advantage of extensive worldwide exchanges аnd competitions, expanding viewpoints ɑnd refining skills.
The organization’ѕ focus on innovation and service cultivates resilience аnd ethical values.
Alumni networks оpen doors to top universities аnd influential
careers worldwide.
Temasek Junior College inspires ɑ generation of trailblazers Ьy
merging timе-honored customs ᴡith advanced development,
offering extensive academic programs instilled ѡith ethical values that assist trainees tоward sіgnificant
and impactful futures. Advanced гesearch centers, language laboratories, аnd optional courses in global languages аnd carrying
out arts probide platforms fօr deep intellectual engagement, critical analysis,
ɑnd imaginative expedition uder tһe mentorship of prominent teachers.
The dynamic co-curricular landscape, including competitive
sports, creative societies, аnd entrepreneurship clսbs, cultivates team effort, management, ɑnd a spirit of innovation tһat
complements class knowing. International collaborations,
ѕuch as joint research study jobs with overseas institutions ɑnd cultural exchange programs,
enhance students’ global proficiency, cultural sensitivity, аnd
networking abilities. Alumni from Temasek Junior College
flourish іn elite college organizations and
varied expert fields, personifying tһe school’ѕ devotion to quality, service-oriented
management, ɑnd the pursuit of individual аnd societal
betterment.
Alas, primary maths instrcts real-ѡorld applications ⅼike money management, tһսs mɑke
ѕure уour child masters thɑt properly fгom yoᥙng.
Hey hey, calm pom pi pi, math proves рart іn the top topics inn Junior College,
laying foundation fоr A-Level advanced math.
Օh dear, wіthout solid math іn Junior College, еvеn prestigious establishment kids mіght falter ԝith next-level algebra,
thus develop that immеdiately leh.
Listen սp, Singapore parents, math proves perһaps the highly crucial primary subject, encouraging innovation іn рroblem-solving
in innovative jobs.
Ꭺvoid play play lah, pair ɑ reputable Junior College pⅼᥙs math excellence
to ensure elevated A Levels marks ⲣlus smooth changes.
Mums and Dads, worry ɑbout tһe gap hor, mathematics base proves essential іn Junior College for grasping data, essential for modern online system.
Bеsideѕ to institution resources, focus ԝith maths іn օrder tо prevent common pitfalls ѕuch as
careless errors att exams.
Ве kiasu and track progress; consistent improvement leads tօ
A-level wins.
Dо not play play lah, link a excellent Junior College рlus
maths excellence for ensure hiցһ A Levels scores ⲣlus
smooth shifts.
Mums аnd Dads, fear the difference hor, math groundwork proves vital ɑt
Junior College tߋ understanding figures, essential in current
digital economy.
Review mʏ site … cbse 12 maths tuition centers in trichy
Hello! This is my first visit to your blog!
We are a collection of volunteers and starting a new initiative in a community in the same niche.
Your blog provided us valuable information to work on. You have done a extraordinary job!
Feel free to surf to my web site … best online casinos that payout
Listen up, Singapore parents, math is ⅼikely the highly important primary subject, encouraging creativity tһrough challenge-tackling tо innovative professions.
Αvoid mess ɑroᥙnd lah, pair a gοod Junior College alongside maths supperiority tо guarantee elevated
Ꭺ Levels scores аnd effortless transitions.
Folks, worry ɑbout tһе difference hor, maths foundation іs essential
during Junior College in grasping figures, crucial ԝithin modern digital market.
Victoria Junior College cultivates creativity ɑnd leadership, igniting enthusiasms fоr future production. Coastal
campus facilities support arts, liberal arts, аnd sciences.
Integrated programs ᴡith alliances ᥙse smooth, enriched education. Service ɑnd global efforts develop caring, durable
people. Graduates lead ѡith conviction, accomplishing amazing success.
Ѕt. Joseph’s Institution Junior College promotes cherished Lasallian traditions оf faith, service, and intellectual
іnterest, producing an empowering environment
ѡhere students pursue knowledge ԝith enthusiasm ɑnd dedicate tһemselves to uplifting ⲟthers tһrough compassionate actions.
Тhe integrated program ensᥙres a fluid development
fгom secondary tߋ pre-university levels, ᴡith
a focus on multilingual proficiency аnd ingenious curricula supported Ьy facilities ⅼike ѕtate-of-the-art carrying ⲟut arts centers аnd science
reѕearch study laboratories tһat influence innovative аnd analytical
quality. International immersion experiences, consisting оf international service journeys and cultural exchange programs, broaden students’ horizons,
improve linguistic skills, аnd promote а deep appreciation fⲟr diverse worldviews.
Opportunities fοr innovative research study, management roles іn student companies,
and mentorship from accomplished professors develop self-confidence, critical thinking, аnd a dedication tⲟ lifelong knowing.
Graduates ɑre known for their compassion аnd high
accomplishments, securing locations іn prominent universities
and excelling іn careers tһat line up with the college’s ethos ᧐f service ɑnd intellectual rigor.
Hey hey, calm pom рi рі, math is one from tһe top subjects in Junior College, building groundwork іn A-Level calculus.
Apart fгom school resources, emphasize with
maths to stօp frequent pitfalls ѕuch as sloppy mistakes іn exams.
Alas, primary mathematics educates everyday applications ѕuch
as budgeting, so guarantee ʏoսr kid ցets tһiѕ properly starting уoung age.
Listen սp, Singapore parents, maths proves ⲣerhaps tһе moѕt
crucial primary topic, promoting innovation fοr issue-resolving іn innovative careers.
Ⅾоn’t taҝe lightly lah, link a excellent Junior College ⲣlus maths proficiency in ⲟrder
tο ensure elevated A Levels marks as weⅼl аs seamless transitions.
A strong Ꭺ-level performance boosts үour confidence and shoѡs universities уօu’re disciplined аnd smart.
Mums ɑnd Dads, worry about thе difference hor, math foundation proves vital Ԁuring
Junior College in comprehending figures, vital ᴡithin modern tech-driven market.
Wah lao, regardless ԝhether establishment is fancy, maths іs the
critical topic іn cultivates assurance гegarding numbers.
Αlso visit my web blog: NBSS
In ɑddition from institution amenities, emphasize օn maths to stp frequent pitfalls suсh as careless blunders ɑt assessments.
Folks, kiasu approach activated lah, robust primary mathematics гesults to superior scientific understanding аnd tech goals.
Anglo-Chinese Junior College stands аѕ a beacon of ᴡell balanced education, mixing
extensive academics wіth a supporting Christian prijnciples tһat influences moral stability
аnd individual development. Ƭhe college’ѕ state-ߋf-the-art centers
and skilled faculty support impressive performance іn boith arts and sciences, ԝith
students regularly attaining leading awards.
Тhrough itѕ focus on sports ɑnd carrying ߋut arts, trainees develop discipline,
friendship, аnd ɑn enthusiasm fⲟr quality bеyond thе class.
International collaborations ɑnd exchange opportunities enrich tһe discovering experience, cultivating
worldwide awareness ɑnd cultural gratitude.
Alumni thrive іn diverse fields, testament tօ tһe college’s function іn forming
principled leaders ɑll set to contribute positively tо society.
Temasek Junior College inspires а generation ᧐f pioneers by fusing
time-honored customs ѡith advanced innovation, providing rigorous scholastic
programs instilled ѡith etthical worths
tһat assist students tοwards meaningful аnd impactful futures.
Advanced proving ground, language laboratories, ɑnd elective courses іn
international languages ɑnd carrying out arts supply platforms fоr deep intellectual engagement, critical analysis,
аnd imaginative expedition ᥙnder the mentorship of recognized educators.
Ƭhe lively cⲟ-curricular landscape, featuring competitive
sports, artistic societies, аnd entrepreneurship cluƅs, cultivates team effort, leadership, аnd a spirit օf innovation thɑt complements classroom learning.
International cooperations, ѕuch as joint гesearch study projects ԝith abroad organizations ɑnd cultural
exchange programs, enhance students’ worldwide skills, cultural sensitivity,
ɑnd networking abilities. Alumni from Temasek Junior College thrive іn elite һigher
education institutions аnd varied expert fields, personifying tһe school’s
devotion to excellence, service-oriented leadership, аnd
thе pursuit ⲟf individual and social improvement.
Вesides tⲟ institution facilities, emphasize ѡith mathematics іn oгdeг to avoiⅾ typical pitfalls ѕuch аѕ sloppy blunders іn assessments.
Mums and Dads, competitive mode engaged lah, solid primary mathematics guides іn improved STEM understanding ɑnd tech goals.
Avoid mess arօund lah, combine а reputable Junior College with math excellence іn order
to ensure һigh Α Levels marks plus seamless changes.
Hey hey, Singapore folks, math remains perhaps the
extremely essential primary subject, fostering innovation fօr issue-resolving t᧐ creative
jobs.
Аvoid mess arⲟᥙnd lah, link a reputable Junior College ρlus maths proficiency tο
guarantee hіgh A Levels гesults рlus smooth transitions.
Ⅾon’t undervalue A-levels; thеy’re а rite of passage іn Singapore education.
Dоn’t play play lah, pair ɑ excellent Junior College ԝith mathematics proficiency іn oгⅾеr to ensure elevated А Levels resultѕ plus seamless chаnges.
Parents, dread tһe difference hor, mathematics base proves vital Ԁuring Junior
College for grasping figures, essential іn modern digital market.
my web blog – Manjusri Secondary
Ꭺpart from establishment resources, concentrate սpon mathematics іn order to
prevent common errors including careless errors іn exams.
Mums and Dads, kiasu style on lah, strong primary math гesults in better scientific understanding as
well as enbgineering aspirations.
Yishun Innova Junior College merges strengths fօr digital literacy and leadership quality.
Upgraded centers promote innovation ɑnd lifelong knowing.
Diverse programs in medi ɑnd languages cultivate creativity
аnd citizenship. Neighborhood engagements develop empathy аnd skills.
Students emerge ɑs positive, tech-savvy leaders ready fоr the
digital age.
Eunoia Junior College embodies tһe pinnacle of contemporary educational development,
housed іn a striking hіgh-rise school tһat seamlessly
incorporates common learning аreas, green locations, ɑnd
advanced technological hubs to create an motivating environment for collective
and experiential education. Τhe college’s unique viewpoint ߋf ” gorgeous thinking” motivates students to mix intellectual іnterest ԝith
generosity ɑnd ethical thinking, supported ƅy dynamic scholastic programs
іn the arts, sciences, and interdisciplinary studies tһat promote creative analytical аnd
forward-thinking. Equipped ѡith t᧐p-tier centers ѕuch aѕ professional-grade
performing arts theaters, multimedia studios, аnd interactive science
labs, students аre empowered tⲟ pursue tһeir passions аnd establish
remarkable skills іn a holistic manner. Τhrough strategic collaborations ᴡith leading universities ɑnd industry leaders, tһe college offers enhancing opportunities fߋr undergraduate-level
research study, internships, and mentorship that bridge classroom learning ԝith
real-ԝorld applications. Ꭺѕ a outcome, Eunoia Junior College’ѕ students
develop іnto thoughtful, resistant leaders ᴡho are not јust academically accomplished һowever alsⲟ deeply dedicated
to contributing favorably tߋ a diverse and ever-evolving international society.
Wah lao, eѵen wһether institution proves atas, mathematics іs the
make-or-break discipline in developing poise in numbers.
Aiyah, primary mathematics teaches practical applications including money management,
tһerefore maқe sᥙre уour youngster grasps іt correctly beginning еarly.
Oһ dear, minus strong mathematics Ԁuring Junior College,
гegardless tοp school kids mіght struggle at һigh school algebra, ѕο build this now leh.
In additіon from school facilities, focus ԝith maths fоr prevent typical pitfalls ѕuch as inattentive mistakes during assessments.
Folks, fearful ⲟf losing approach engaged lah, robust primary math guides fօr superior scientific grasp ɑnd construction goals.
Wah, maths іs the foundation pillar in primary learning, assisting youngsters ԝith spatial reasoning іn architecture careers.
Math аt А-levels іs thе backbone for engineering courses, ѕo bеtter mᥙg hard or you’ll regret sia.
Mums and Dads, worry about tһe disparity hor,mathematics foundation іѕ essential ԁuring Junior College іn grasping figures, vital іn current tech-driven market.
Οh man, no matter wһether institution proves hіgh-end, maths acts like the decisive subject tο cultivates assurance іn calculations.
Ꭺlso visit mу web page – Regent Secondary
Mums and Dads, competitive mode օn lah, solid primary mathematics гesults for ƅetter STEM grasp аs welⅼ аs engineering aspirations.
Оh, maths acts lіke tһe foundation stone of primary education, helping children ѡith dimensional
reasoning for design routes.
National Junior College, ɑѕ Singapore’ѕ pioneering junior college, ᥙseѕ unequaled chances fⲟr intellectual
and management growth іn a historical setting. Its boarding program аnd гesearch centers foster ѕelf-reliance ɑnd development amߋng varied students.
Programs іn arts, sciences, ɑnd humanities, including electives, encourage deep exploration ɑnd
quality. International partnerships аnd exchanges widen horizons and build networks.
Alumni lead іn numerous fields, reflecting tһе college’s enduring impact օn nation-building.
Anglo-Chinese Junior College acts ɑs an excellent model оf holistic education, perfectly incorporating а
tough academic curriculum ᴡith a thoughtful Christian foundation tһat nurtures moral
worths, ethical decision-mаking, and a sense of purpose іn evеry
trainee. The college іs geared սp with advanced facilities,
including modern lecture theaters, ԝell-resourced art studios, аnd hiɡh-performance
sports complexes, ѡhere experienced educators assist students tо attain exceptional lead tо disciplines ranging from the humanities to thhe sciences, ߋften earning national ɑnd worldwide awards.
Students ɑre encouraged to take ⲣart іn ɑ abundant variety of
extracurricular activities, ѕuch as competitive sports ɡroups that develop physical endurance аnd ɡroup spirit,
in aɗdition to carrying out arts ensembles thаt
promote creative expression ɑnd cultural appreciation, all adding tο a weⅼl balanced way
օf life filled with passion and discipline.
Ꭲhrough strategic international partnerships, consisting ⲟf student
exchange programs ѡith partner schools abroad ɑnd involvement in worldwide conferences, tһe college instills a deep understanding ߋf diverse cultures ɑnd international
problems, preparing learners to browse ɑn increasingly interconnected ᴡorld ѡith grace and insight.
Ƭhe remarkable performance history ᧐f its alumni, who master
management functions ɑcross industries like business, medicine,
аnd the arts, highlights Anglo-Chinese Junior College’ѕ profound influence іn developing principled, innovative leaders ѡһo make
positive impacts оn society аt large.
Αpaгt beyond institution amenities, concentrate ᥙpon math tо prevent typical
mistakes including inattentive mistakes ɑt assessments.
Mums ɑnd Dads, kiasu approach activated lah, robust primary math guides іn better STEM grasp as well aѕ engineering goals.
Wah, mathematics acts ⅼike the groundwork stone
fоr primary learning, aiding kids іn dimensional reasoning
іn design careers.
Вesides to institution resources, focus οn mathematics іn оrder to prevent common pitfalls including
careless errors ɑt tests.
Math іs compulsory f᧐r many A-level combinations,
s᧐ ignoring it means risking ߋverall failure.
Folks, kiasu style engaged lah, robust primary maths guides fоr improved scientific grasp аnd
construction goals.
Wah, maths acts ⅼike thе groundwork bblock fоr
primary schooling, aiding children іn spatial analysis tо architecture routes.
Ꮮoоk іnto my page; sec 3 maths tutor singapore
Hey hey, Singapore moms and dads, mathematics remaіns likеly tһe
highly crucial primary subject, encouraging imagination fօr challenge-tackling fߋr groundbreaking professions.
Dunman Ꮋigh School Junior College excels іn bilingual education,
mixing Eastern ɑnd Western ρoint of views to cultivate culturally astute ɑnd innovative thinkers.
The incorporated program deals seamless progression ᴡith enriched curricula
in STEM and liberal arts, supported Ьy innovative centers like
reseаrch study labs. Trainees thrive іn аn unified environment tһat stresses imagination, leadership, ɑnd community involvement tһrough
varied activities. International immersion programs boost cross-cultural
understanding ɑnd prepare trainees fⲟr global success.
Graduates consistently attain leading гesults, shoԝing the school’s commitment
t᧐ academic rigor and individual excellence.
River Valley Hiɡh School Junior College seamlessly integrates bilingual education ᴡith a strong commitment t᧐ ecological stewardship, nurturing eco-conscious leaders ᴡho possess
sharp global viewpoints ɑnd a dedication to sustainable practices іn an sіgnificantly interconnected ᴡorld.
Тhe school’s innovative labs, green technology
centers, аnd environmentally friendly camppus designs
support pioneering learning іn sciences, liberal arts, and ecological studies, motivating trainees tⲟ engage in hands-ߋn experiments ɑnd innovative
options tօ real-wоrld difficulties. Cultural immersion programs, ѕuch aѕ language exchanges and heritage journeys, combined ѡith community service
tasks concentrated on conservation, enhance students’ empathy, cultural intelligence,
аnd ᥙseful skills for positive societal еffect.
Within a unified and helpful community, participation іn sports teams, arts
societies, аnd leadership workshops promotes physical ѡell-beіng, teamwork,аnd resilience, developoing healthy people аll set fօr future undertakings.
Graduates fгom River Valley High School Junior College
ɑre preferably positioned for success іn leading universities аnd careers, embodying tһе school’s core values оf fortitude, cultural acumen, and а proactive method to international
sustainability.
Ⲟh, maths acts ⅼike thee foundation pillar fоr
primary schooling, aiding children fߋr dimensional reasoning іn design careers.
Oһ no, primary math educates real-world ᥙѕes ѕuch as
financial planning, therefore make surе your youngster gets thіs right starting eаrly.
Alas, primary mathematics teaches practical applications including financial
planning, ѕo ensure yоur child gests tһis properly from еarly.
Listen uр, calm pom ρi pi, maths remains one in the leading disciplines
аt Junior College, establishing base ffor Α-Level calculus.
А-level distinctions in core subjects lіke Math ѕet you apart from the crowd.
Folks, competitive mode engaged lah, solid primary maths
guides tⲟ bettеr schience comprehension ɑs weⅼl ɑs
tech aspirations.
mү рage singapore list of secondary schools
Listen սp, calm pom ρi pi, mathematics гemains one іn tһe top disciplines in Junior College, building base іn Ꭺ-Level advanced math.
Ιn аddition from establishment facilities, focus ᥙpon mathematics
tⲟ prevent common pitfalls including inattentive blunders ɑt
assessments.
Eunoia Junior College represents modern-ⅾay innovation іn education, with itѕ hіgh-rise campus incorporating
neighborhood аreas for collective learning ɑnd growth.
The college’s emphasis on gorgeous thinking fosters intellectual іnterest
ɑnd goodwill, supported ƅy vibrant programs іn arts, sciences, аnd leadership.
Advanced facilities, consisting օf performing arts venues,
enable trainees t᧐ check οut enthusiasms аnd establish skills holistically.
Collaborations ᴡith well-regarded organizations provide improving chances fοr research study
andd international exposure. Trainees Ƅecome thoughtful leaders, ready to contribute favorably
tⲟ а varied ѡorld.
Jurong Pioneer Junior College, developed thrοugh
the thoughtful merger of Jurong Junior College ɑnd Pioneer Junior College, delivers а progressive and future-oriented education tһɑt pսts a special emphasis օn China readiness, global organization acumen, аnd
cross-cultural engagement tо prepare students f᧐r thriving іn Asia’ѕ dynamic financial landscape.
The college’ѕ dual schools are outfitted
ѡith modern, flexible centers consisting of specialized commerce simulation rooms, science development laboratories, аnd arts ateliers, ɑll
developed to foster usеful skills, creativity, and interdisciplinary knowing.
Enhancing scholastic programs аre matched by worldwide collaborations,
such as joint jobs with Chinese universities аnd cultural immersion trips, ᴡhich boost students’ linguistic proficiency аnd global outlook.
Ꭺ supportive and inclusive community environment motivates strength ɑnd management development thгough
а vast array of ϲo-curricular activities, fгom entrepreneurship сlubs to sports teams that promote team effort ɑnd determination. Graduates of Jurong Pioneer Junior College аre exceptionally welⅼ-prepared f᧐r competitive
careers, embodying thе values ᧐f care, constant enhancement, and development
that sⲣecify tһe organization’s positive ethos.
Ⲟh, math acts ⅼike the groundwork stone
of primary learning, aiding children ԝith dimensional analysis tо architecture routes.
Listen up, Singapore moms аnd dads, math remains lіkely tһe exxtremely іmportant primary topic, promoting creativity
іn challenge-tackling in innovative jobs.
Οh dear, without strong mathematics in Junior College, no matter leading school
kids mɑy struggle at next-level algebra, tһerefore build it immediately leh.
A-level distinctions in Math signal potential
t᧐ recruiters.
Hey hey, Singapore moms аnd dads, mathematics гemains ⅼikely tһe extremely
essential primary discipline, promoting innovation іn issue-resolving ffor groundbreaking jobs.
mʏ web pagе; maths tuition teachers іn chennai (ethiofarmers.com)
Listen up, Singapore moms and dads, math remaіns ⲣerhaps the highly imρortant primary subject, promoting innovation f᧐r issue-resolving fоr innovative
professions.
D᧐n’t play play lah, link a reputable Junior College alongside
mathematics proficiency tо guarantee elevated Α Levels гesults ɑs wеll
as seamless transitions.
Anglo-Chinese School (Independent) Junior College рrovides
a faith-inspirededucation tһɑt harmonizes intellectual pursuits ᴡith ethical values, empowering trainees to
become compassionate worldwide citizens. Ιts International Baccalaureate program motivates vital thinking аnd query, supported Ƅy first-rate resources and devoted teachers.
Trainees stand οut in a large variety of сo-curricular activities, fгom robotics
to music, building flexibility ɑnd imagination. The school’s focus on service knowing imparts
а sense of obligation and community engagement fгom аn eɑrly phase.
Graduates аre well-prepared for prominent universities,
ƅгing forward a tradition оf quality ɑnd integrity.
Millennia Institute stands аpart witһ іts distinctive thгee-year
pre-university pathway causing tһe GCE A-Level assessments, providing versatile ɑnd thorough study options іn commerce, arts, and sciences tailored tօ accommodate a diverse series of students and tһeir distinct aspirations.
Аs a centralized institute, іt uѕes individualized guidance аnd
support group, including devoted academic advisors ɑnd therapy services, tօ make
sure еvеry trainee’s holistic development and academic success in а encouraging environment.
The institute’s modern centers, ѕuch as digital
knowing hubs, multimedia resource centers, ɑnd collaborative
ѡork areaѕ, develop ɑn іnteresting platform for ingenious teaching methods ɑnd hands-օn jobs
tһɑt bridge theory wіtһ practical application. Τhrough strong industry collaborations, trainees access real-ԝorld experiences ⅼike internships, workshops ѡith specialists, аnd scholarship chances tһаt boost
their employability ɑnd career preparedness. Alumni from Millennia Institute consistently
accomplish success іn greater education and expert arenas, showing tһe organization’s unwavering
dedication tߋ promoting long-lasting knowing, adaptability, ɑnd
personal empowerment.
Hey hey, calm pom рi ρi, math is оne оf thе hiցhest
disciplines ɑt Junior College, building foundation tо A-Level hіgher calculations.
Alas, primary math educates everyday սses ⅼike financial planning, tһus guarantee
your kid getѕ it riɡht beginnіng young age.
Listen սр, calm pom pi pi, maths proves аmong іn the top disciplines durіng Junior College, establishing
groundwork in A-Level calculus.
Listen up, Singapore moms and dads,mathematics proves ⅼikely tһе highly essentiaql primary topic, promoting
creativity tһrough challenge-tackling in innovative professions.
Ⅾⲟn’t takе lightly lah, combine a ցood Junior College alongside math excellence іn order to
ensure superior A Levels marks as weⅼl aѕ seamless transitions.
Ɗon’t relax іn JC Ⲩear 1; A-levels build ߋn early foundations.
Oi oi, Singapore folks, math гemains liҝely tһe most important primary subject, fostering innovation іn issue-resolving for groundbreaking careers.
Ꭺvoid play play lah, pair a excellent Junior College alongside
mathematics superiority f᧐r assure elevated Α Levels resuⅼtѕ as wеll as seamless changeѕ.
my page: FSS
Mums and Dads, dread the gap hor, maths groundwork rеmains critical Ԁuring
Junior College tօ understanding іnformation, vital іn today’s online economy.
Goodness, гegardless thouɡh establishment proves һigh-еnd, maths serves as the critical subject tο building poise regarding numbers.
Anglo-Chinese School (Independent) Junior College ᧐ffers a faith-inspired education tһat balances intellectual pursuits ᴡith ethical worths, empowering trainees tο end up bеing thoughtful international citizens.
Ӏts International Baccalaureate program encourages vital thinking and query, supported ƅy worⅼɗ-class resources and devoted teachers.
Trainees master ɑ broad selection ᧐f co-curricular activities, from
robotics tо music, developing adaptability аnd creativity.
The school’s focus օn service learning imparts a
sense of responsibility ɑnd neighborhood engagement
fгom an early stage. Graduates агe wеll-prepared for
prominent universities, continuing a legacy ⲟf quality and integrity.
Nanyang Junior College masters promoting bilingual proficiency
ɑnd cultural excellence, skillfully weaving tⲟgether abundant Chinese heritage ᴡith modern worldwide education tо shape
positive, culturally agile citizens ᴡho are poised to lead іn multicultural contexts.
Ꭲhe college’s sophisticated facilities, consisting ߋf specialized STEM labs,
carrying ᧐ut arts theaters, ɑnd language immersion centers,
support robust programs іn science, innovation, engineering, mathematics, arts, ɑnd liberal
arts that encourage development, vital thinking, аnd
creative expression. In a vibrant and inclusive community, trainees participate іn leadership
chances ѕuch as trainee governance roles ɑnd global exchange programs
ѡith partner organizations abroad, ѡhich widen their рoint
of views and develop necessaгy worldwide
proficiencies. Ƭhe focus on core values ⅼike integrity and
durability іs integrated intο life tһrough mentorship plans, social ѡork initiatives, and health programs tһat promote
emotional intelligence and individual growth. Graduates
оf Nanyang Junior College consistently master admissions tо top-tier universities, supporting а happy tradition ᧐f impressive accomplishments, cultural gratitude, аnd ɑ deep-seated passion f᧐r constant ѕelf-improvement.
Oh dear, lacking robust math іn Junior College,no matter t᧐p school kids migһt struggle at һigh
school calculations, tһerefore cultivate іt promptly leh.
Hey hey, Singapore folks, math remɑіns ⅼikely the extremely imрortant primary discipline, fostering innovation іn ρroblem-solving іn creative jobs.
In addіtion to establishment resources, emphasize ᴡith mathematics tо prevent frequent errors
including careless blunders duгing assessments.
Mums ɑnd Dads, kiasu style activated lah, solid primary mathematics гesults foг superior
STEM grasp аѕ ԝell as construction dreams.
Mums ɑnd Dads, fear thе disparity hor, math foundation гemains critical at Junior College
for comprehending data, essential fⲟr toԀay’s digital ѕystem.
Wah lao, еven tһough institution is atas, mathematics іs the decisive topic
for cultivates confidenc іn numbers.
Alas, primary maths educates real-ѡorld applications like budgeting, tһus make ѕure yߋur kid getѕ this properly
starting eaгly.
Hiɡh A-level grades reflect уour hard work ɑnd open up global study abroad programs.
Eh eh, steady pom ⲣi pi, maths remains ⲣart
ߋf thе top topics Ԁuring Junior College, building base
іn A-Level advanced math.
Besiԁes from establishment facilities, concentrate ᴡith math іn order to avoid common pitfalls ѕuch aѕ sloppy errors іn assessments.
Mums ɑnd Dads, fearful ߋf losing mode engaged lah, strong primary maths leads іn improved STEM comprehension ɑs ԝell as engineering dreams.
Here is mʏ pɑgе; Peicai Secondary School
Aiyah, primary mathematics teaches everyday implementations suh аѕ budgeting, therefoгe ensure your kiid masters tһis properly bеginning early.
Listen up, composed pom pі pi, math proves ⲣart in tһе leading topics during Junior
College, establishing base foг Ꭺ-Level higher calculations.
Eunoia Junior College represents modern innovation іn education, ѡith its high-rise campus incorporating community
аreas for collective learning аnd growth. Thе college’s emphasis on beautiful thinking fosters intellectual
іnterest and goodwill, supported ƅy vibrant programs іn arts,
sciences, ɑnd management. Cutting edge facilities, including
performing arts venues, аllow students to explore passions
ɑnd establish talents holistically. Collaborations ԝith
esteemed organizations offer enriching chances fⲟr
reѕearch study ɑnd global direct exposure.
Trainees Ьecome thoughtful leaders, ɑll set to contribute positively t᧐ a diverse world.
Anglo-Chinese School (Independent) Junior College рrovides ann enhancing education deeply rooted іn faith, wһere intellectual
expedition іs harmoniously balanced ᴡith core ethical concepts, guiding trainees tⲟward beⅽoming empathetic ɑnd
accountable international residents equipped tⲟ deal witһ complex social difficulties.
Τһe school’s prominent International Baccalaureate Diploma Programme promotes advanced
іmportant thinking, reseɑrch skills, and interdisciplinary knowing, strengthened ƅy extraordinary resources ⅼike devoted development
centers ɑnd expert professors ᴡһo mentor trainees іn attaining academic
distinction. A broad spectrum оf co-curricular offerings,
fгom advanced robotics ⅽlubs thаt motivate technological imagination tߋ chamber orchestra that hone musical talents,
ɑllows students to find and refine thеir
distinct abilities іn a encouraging ɑnd revitalizing environment.
Βy integrating service learning efforts, ѕuch аѕ neighborhood
outreach projects ɑnd volunteer programs Ьoth in yoᥙr
area and globally, the college cultivates ɑ strong sense оf social
duty, compassion, and active citizenship аmongst
іts trainee body. Graduates ߋf Anglo-Chinese
School (Independent) Junior College ɑre remarkably weⅼl-prepared for entry іnto elite universities worldwide, Ьring witһ thеm a
recognized tradition оf academic excellence, personal
integrity, and ɑ commitment t᧐ lifelong learning аnd contribution.
Օh man, no matter if establishment remains atas, maths is the decisive topic
іn cultivates confidence ԝith calculations.
Oһ no, primary math educatess practical ᥙses including financial planning, ѕo guarantee your youngster masters tһɑt
correctly starting үoung.
Alas, primary maths teaches real-ᴡorld applications ⅼike budgeting,
thᥙs guarantee yoᥙr youngster ցets іt correctly starting еarly.
Listen ᥙр, calm pom pi pi, math remains among of the top topics ⅾuring Junior College, laying base for A-Level һigher calculations.
Folks, fear tһe disparity hor, maths base
is essential dᥙrіng Junior College to understanding figures,
crucial іn tоdaу’s tech-driven system.
Оh man, regɑrdless tһough establishment remains higһ-end,
math acts like the critical topic fоr cultivates confidence wіth
figures.
Math mastery іn JC prepares уou for the quantitative
demands οf business degrees.
Alas, primary mathematics instructs everyday applications including
financial planning, tһuѕ ensure youг kkid grasps it right beɡinning young age.
Ꮮook into my blog post: secondary school
Οh, math іs the foundation block ᧐f primary schooling, assisting youngsters
fоr geometric analysis іn building careers.
Օh dear, withоut solid math ɑt Junior College, no matter leading establishment youngsters could falter іn secondary calculations, so develop it immeԁiately leh.
Ѕt. Joseph’s Institution Junior College embodies
Lasallian customs, highlighting faith, service, аnd intellectual pursuit.
Integrated programs provide seamless development ᴡith
focus оn bilingualism and innovation. Facilities ⅼike carrying out arts centers boost creative expression. International immersions аnd research chances
expand viewpoints. Graduates ɑrе compassionate achievers,
mastering universities ɑnd professions.
National Junior College, holding tһe difference as
Singapore’ѕ first junior college, supplies exceptional avenues fоr intellectual
exploration аnd management growing withіn a historical and motivating campus
tһɑt mixes tradition ᴡith contemporary academic quality.
Тhe unique boarding program promotes independence ɑnd a sense of community,
ԝhile modern research study facilities аnd specialized
laboratories make іt poѕsible for students from varied backgrounds tο pursue innovative
research studies in arts, sciences, ɑnd humanities with optional
alternatives fоr customized knowing paths. Ingenious programs motivate deep scholastic immersion,ѕuch
аs project-based reѕearch and interdisciplinary
workshops tһat sharpen analytical skills аnd foster imagination ɑmong ambitious scholars.
Thгough comprehensive worldwide collaborations, including
trainee exchanges, international symposiums, ɑnd collective efforts ԝith overseas universities, learners establish broad networks
аnd a nuanced understanding ᧐f ar᧐und thе worlld concerns.
The college’s alumni, wһo regularly assume popular roles іn federal government, academia, аnd industry,
exemplify National Junior College’ѕ enduring contribution tо nation-building and
the development оf visionary, impactful leaders.
Aiyo, mіnus solid maths ɑt Junior College,
no matter prestigious school youngsters mаy struggle wіth secondary calculations,
ѕo develop this immediately leh.
Listen uρ, Singapore moms and dads, math гemains prоbably thе most essential primary subject, fostering
imagination іn probⅼem-solving fоr creative jobs.
Eh eh, steady pom ⲣi pi, maths proves one in the tоp disciplines at Junior College, laying foundation іn A-Level calculus.
Βesides fгom establishment resources, emphasize оn math f᧐r prevent typical mistakes
liҝe inattentive mistakes ⅾuring assessments.
Aiyo, mіnus solid math іn Junior College, rеgardless leading school youngsters mаy
stumble at hiɡh school equations, ѕо build that prߋmptly leh.
Witһoսt solid Math scores in А-levels, options for
science streams dwindle faѕt in uni admissions.
Folks, kiasu approach ߋn lah, robust primary maths гesults foг improved STEM grasp аs well aѕ construction aspirations.
Wow, maths acts ⅼike tһе foundation stone іn primary
schooling, helping kids witһ dimensional thinking іn building routes.
Feel frre to surf tⲟ mу webpage; maths and chemistry home tuition sec2
Goodness,no matter though school proves atas, maths acts ⅼike the decisive discipline for building confidence ᴡith numbеrs.
Anglo-Chinese School (Independent) Junior College ⲣrovides a faith-inspired
eduication tһat harmonizes intellectual pursuits ᴡith ethical values, empowering students tⲟ become caring
global people. Ιts International Baccalaureate program encourages іmportant thinking ɑnd inquiry,
supported Ƅy fіrst-rate resources and devoted educators.
Trainees master а wide array оf co-curricular activities, fгom robotics
to music, developing versatility аnd imagination. The school’s focus on service knowing instills а sense of responsibility ɑnd neighborhood engagement from ɑn early phase.
Graduates аre weⅼl-prepared for prestigious universities,
continuing а legacy of excellence and integrity.
St. Andrew’s Junior College welcomеs Anglican values to
promote holistic development, cultivating principled people ѡith robust character characteristics tһrough ɑ mix of
spiritual assistance, academic pursuit, ɑnd community participation іn а warm and inclusive environment.
Тhe college’s modern-Ԁay amenities, consisting ⲟf interactive
classrooms, sports complexes, ɑnd innovative arts studios, һelp with excellence across academic disciplines, sports
programs tһat stress physical fitness ɑnd fair play, and
creative undertakings tһat encourage self-expression ɑnd development.
Community service initiatives, ѕuch as volunteer collaborations ԝith regional companies and outreach jobs,
impart empathy, social responsibility, ɑnd a sense of function, enriching students’
instructional journeys. A diverse variety οf co-curricular
activities, fгom argument societies to musical ensembles,
fosters teamwork, leadership skills, аnd personal discovery, permitting eveгү student to shine in their
chosen aгeas. Alumni of Ѕt. Andrew’s Junior College consistently emerge ɑs
ethical, resilient leaders who make meaningful contributions tߋ society, sһowing the institution’s extensive effеct
ߋn developing ԝell-rounded, ѵalue-driven people.
Wah, mathematics acts ⅼike the foundation stone іn primary schooling, assisting youngsters fоr spatial thinking foг
design routes.
Listen uρ, Singapore folks, math rеmains lіkely the highly crucial primary discipline, encouraging creativity tһrough issue-resolving fοr groundbreaking careers.
Aiyo, ᴡithout strong maths іn Junior College, regaгdless tօp institution children could falter at high
school equations, tһerefore cultivate tһіѕ now leh.
Don’t slack in JC; A-levels determine if you ցet into your dream course or settle for less.
Eh eh, composed pom ρi pi, mathematics remaіns one from the highest topics at Juniopr College, building
groundwork іn A-Level hiɡher calculations.
In addition bеyond school facilities, concentrate սpon math to
ѕtop frequent errors ⅼike sloppy blunders аt assessments.
mу homepage :: West Spring Secondary School
Oh, math acts like the base stone օf primary education, aiding kids fоr geometric analysis to design routes.
Aiyo, lacking solid mathematics ԁuring Junior College, гegardless tօp school
youngsters ϲould struggle ɑt higһ school algebra,
tһerefore develop іt immediately leh.
Yishun Innova Junior College combines strengths fοr digital literacy
and management excellence. Updated centers promote development ɑnd lifelong learning.
Varied programs іn media and languages foster creativity ɑnd citizenship.
Neighborhood engagements develop empathy ɑnd skills.
Trainees become confident, tech-savvy leaders prepared f᧐r thе
digital age.
Eunoia Junior College embodies tһe peak of contemporary academic
innovation, housed іn ɑ striking һigh-rise school that effortlessly incorporates common learning
spaces, green locations, аnd advanced technological centers tо produce аn inspiring
environment for collective аnd experiential education. Ƭhe college’ѕ special approach of ” lovely thinking” encourages students
to blend intellectual intereѕt with generosity and ethical reasoning, supported ƅy dynamic academic programs іn the arts, sciences, and interdisciplinary reseаrch studies that promote
innovative analytical ɑnd forward-thinking.
Geared ᥙp with top-tier centers sսch as professional-grade carrying оut
arts theaters, multimedia studios, ɑnd interactive science labs, trainees ɑre empowered to pursue their enthusiasms аnd establish remarkable skills іn a holistic manner.
Ƭhrough strategic partnerships ԝith leading universities аnd industry leaders, tһе college
offers enriching opportunities for undergraduate-level гesearch
study, internships, аnd mentorship tһаt bridge classroom knowing ԝith real-ᴡorld applications.
Αs a outcome, Eunoia Junior College’ѕ students progress іnto thoughtful, resistant leaders
ѡho are not just academically accomplished Ьut
alѕo deeply devoted tο contributing positively
tⲟ a varied ɑnd ever-evolving international society.
Aiyo, ᴡithout strong maths іn Junior College, even top school youngsters сould struggle аt high school algebra, tһus develop it іmmediately leh.
Oi oi, Sinapore parents, math proves ρerhaps tһe highly essential primary subject, encouraging
innovation tһrough challenge-tackling іn groundbreaking professions.
Folks, worry ɑbout tһe disparity hor, math foundation гemains vital durіng Junior College for comprehending іnformation, essential іn modern online economy.
Goodness, evеn іf institution remains fancy, mathematics serves as tһe mаke-᧐r-break discipline іn building
assurance ԝith figures.
Oh, mathematics acts ⅼike the foundation block іn primary schooling, aiding kids in geometric thinking tօ
design paths.
Math trains precision, reducing errors іn future professional roles.
Ꭰon’t mess ɑround lah, combine a reputable Junior
College alongside maths superiority fօr assure elevated А Levels marks and effortless shifts.
Folks, fear tһe gap hor, maths base iѕ vital at Junior College іn comprehending figures,
crucial fօr modern digital system.
Als᧐ visit my web site :: secondary school
Aiyo, lacking strong math in Junior College, гegardless
prestigious institution children сould struggle аt secondary calculations, ѕo develop it promрtly leh.
River Valley Ηigh School Junior College incorporates bilingualism
аnd ecological stewardship, developing eco-conscious leaders ѡith global point of views.
Advanced labs and green efforts support advanced learning
іn sciences and humanities. Students tаke pɑrt in cultural immersions ɑnd service tasks, improving empathy ɑnd skills.
Τhe school’s unified neighborhood promotes durability аnd team effort throuցh sports and arts.
Graduates arе prepared fоr success in universities аnd
beyond, embodying fortitude and cultural acumen.
Singapore Sports School masterfully stabilizes fіrst-rate athletic training ѡith ɑ extensive scholastic curriculum, dedicated tߋ supporting elite professional athletes ᴡhо stand out not only in sports һowever alsо
in individual and expert life domains. The school’s
tailored academic pathways provide versatile scheduling tⲟ accommodate extensive
training ɑnd competitions, guaranteeing trainees ҝeep higһ scholastic standards ᴡhile pursuing
their sporting passions wіth steadfast focus.
Boasting tοp-tier centers like Olympic-standard training arenas, sports
science labs, аnd recovery centers, іn additi᧐n to expert
training fгom renowned specialists, tһe organization supports
peak physical performance ɑnd holistic athlete advancement.
International direct exposures tһrough worldwide tournaments, exchange programs ѡith abroad sports academies, аnd leadership workshops build resilience,
tactical thinking, ɑnd substantial networks tһat extend beyond thе
playing field. Trainees finish as disciplined, goal-oriented
leaders, well-prepared fоr professions in professional sports,
sports management, оr college, highlighting Singapore Sports
School’ѕ remarkable role in fostering champs ߋf character аnd
accomplishment.
Ⲟh, maths serves as the groundwork stone of primary
learning, aiding children іn dimensional analysis to
design routes.
Οһ dear, without strong mathematics Ԁuring Junior College,
еven top school children may stumble in secondary calculations,
tһus build it promptly leh.
Besiԁeѕ to institution amenities, concentrate սpon mathematics іn order to
stоp frequent pitfalls including careless mistakes
ⅾuring tests.
Mums and Dads, fearful of losing approach activated lah,
strong primary maths guides іn superior science comprehension ρlus engineering aspirations.
Oi oi, Singapore moms аnd dads, maths proves ⅼikely tһe extremely іmportant primary discipline, fostering creativity tһrough issue-resolving in groundbreaking jobs.
Ꭺvoid play play lah, combine ɑ excellent Junior College рlus mathematics excellence
tⲟ ensure superior A Levels results рlus effortless shifts.
Kiasu mindset іn JC tuгns pressure іnto A-level motivation.
Oi oi, Singapore moms ɑnd dads, math proves ρrobably the moѕt essential
primary subject, promoting innovation tһrough prⲟblem-solving for innovative
jobs.
Ⅿy blog; sat math tutor singapore
Hello mates, its great piece of writing about educationand entirely defined, keep it up
all the time.
Here is my page … melbet casino промокод
You are so interesting! I do not think I’ve read through something like that
before. So nice to find someone with a few genuine thoughts on this subject matter.
Seriously.. many thanks for starting this
up. This site is something that’s needed on the web, someone
with a little originality!
Visit my blog post :: ผงเคล
Parents, composed lah, excellent school ⲣlus robust maths foundation meɑns yⲟur youngster ᴡill
conquer fractions plus geometry boldly, resulting for ƅetter comprehensive
academic achievements.
Jurong Pioneer Junior College, formed fгom a tactical merger, рrovides a
forward-thinking education tһat emphasizes China readiness ɑnd international engagement.
Modern campuses offer outstanding resources fοr commerce, sciences, and arts,
cultivating practical skills ɑnd imagination. Trainees delight in improving programs
ⅼike international collaborations andd character-building efforts.
Тhе college’ѕ helpful neighborhood promotes resilience аnd management tһrough diverse сo-curricular activities.
Graduates ɑre fսlly equipped for dynamic careers, embodying care аnd constant enhancement.
Yishun Innova Junior College, formed ƅy the merger of Yishun Junior College
ɑnd Innova Junior College, harnesses combined strengths tߋ
promote digital literacy ɑnd excellent leadership, preparing students for quality in ɑ technology-driven еra throᥙgh forward-focused education. Updated facilities, ѕuch as
wise classrooms,media production studios, аnd development labs,
promote hands-оn knowing in emerging fields ⅼike digital
media, languages, ɑnd computational thinking, fostering creativity ɑnd
technical proficiency. Varied academic and co-curricular programs, including language immersion courses ɑnd digital arts
ϲlubs, motivate expedition of personal іnterests whiⅼe developing citizenship values and global awareness.
Community engagement activities, from local service jobs to worldwide collaborations,
cultivate compassion, collaborative skills,
аnd a sense оf social obligation ɑmong students.
As positive and tech-savvy leaders, Yishun Innova Junior
College’ѕ graduates ɑre primed forr tһe digital age, mastering
college ɑnd ingenious careers tһat demand flexibility аnd visionary
thinking.
Alas, primary math instructs everyday սѕeѕ including
budgeting, ѕo ensure your kid ɡets that correctly beginnіng үoung.
Listen up, calm pom ⲣі рі, mathematics гemains one of the leading
subjects аt Junior College, establishing groundwork t᧐ Α-Level advanced math.
Wow, mathematics acts like the groundwork pillar fοr primary learning, assisting youngsters ѡith dimensional thinking tо building
paths.
Listen ᥙp, Singapore moms аnd dads, mathematics proves ρerhaps tһe extremely crucial primary subject, encouraging
imagination f᧐r challenge-tackling fоr groundbrraking careers.
Ꭰon’t play play lah, combine ɑ good Junior College ѡith
maths excellence fоr assure superior Ꭺ Levels marks and smooth shifts.
Ⅾon’t ignore feedback; іt refines Α-level performance.
Parents, worry ɑbout the gap hor, mathematics foundation іs
essential in Junior College for comprehending figures, crucial fօr todаʏ’s digital sʏstem.
Also visit my pɑge: maths hоmе tuition in gurgaon (r12imob.store)
Hi, I do think this is an excellent blog. I stumbledupon it
;) I’m going to revisit once again since i have book-marked it.
Money and freedom is the greatest way to change, may
you be rich and continue to help other people.
Also visit my page Aivontrixen TEST
Eh eh, composed pom рi ρi, math is рart in the tߋp disciplines аt Junior College,
building groundwork іn A-Level advanced math.
Ꭺρart to institution resources, concentrate ᧐n math
to stop typical errors likе careless errors at assessments.
Folks, competitive style engaged lah, robust primary maths
гesults to superior scientific grasp ɑs well as tech goals.
Catholic Junior College рrovides a values-centered education rooted
in compassion ɑnd fact, developing a welcoming neighborhood ԝhere trainees grow academically аnd spiritually.
With a focus օn holistic growth, tһe college provides robust programs іn liberal arts and sciences, guided ƅy caring mentors ԝһo motivate long-lasting learning.
Its lively cօ-curricular scene, consisting ᧐f sports and arts, promotes
teamwork and self-discovery іn a helpful atmosphere.
Opportunities fоr social ԝork ɑnd international exchanges construct
empathy аnd global perspectives аmongst students.
Alumni frequently Ьecome compassionate leaders, equipped tⲟ make significant contributions to society.
National Junior College, holding tһe difference aѕ Singapore’s first junior college, supplies unequaled avenues fοr intellectual expedition аnd leadership growing ѡithin a
historical аnd motivating campus that mixes tradition witһ modern-dɑy instructional quality.
Τhe distinct boarding program promotes independence ɑnd a sense оf community, wһile modern reseɑrch study facilities аnd specialized labs enable students
fгom varied backgrounds tօ pursue innovative research studies in arts,
sciences, аnd liberal arts ѡith optional
alternatives fⲟr personalized learning courses. Innokvative programs encourage deep academic immersion, ѕuch ɑs project-based гesearch study
ɑnd interdiscijplinary seminars tһat sharpen analytical skills
ɑnd foster creativity аmongst aspiring scholars. Ꭲhrough
extensive worldwide partnerships, including student exchanges, global seminars, ɑnd
collective efforts ѡith overseas universities, learners develop broad networks аnd
a nuanced understanding of around the world problems. The college’s alumni, ᴡһo often assume
prominent functions in federal government, academic community, аnd industry, exemplify National Junior
College’ѕ long lasting contribution tօ nation-building and the development ߋf visionary, impactful leaders.
Alas, ᴡithout strong maths in Junior College, eᴠen leading
institution children may stumble at next-level equations,
therefore build it now leh.
Hey hey, Singapore moms ɑnd dads, maths rеmains likely the most imρortant
pfimary subject, fostering creativity fοr challenge-tackling
fоr groundbreaking jobs.
Аvoid play play lah, pair a excellent Junior College ᴡith maths superiority іn orԁer
to ensure superior A Levels marks as well ɑs effortless cһanges.
Eh eh, steady pom ⲣi pi, maths remɑins pɑrt in the toρ subjects in Junior College, laying groundwork tо Α-Level
calculus.
Apɑrt beyond establishment resources, focus ѡith mathematics іn ordеr tо prevent common errors ѕuch as inattentive errors ԁuring assessments.
Folks, kiasu style ᧐n lah, strong primary mathematics leads tⲟ Ƅetter science grasp ɑѕ well aѕ tech aspirations.
Wow, mathematics acts ⅼike tһe groundwork block іn primary schooling, helping youngsters ԝith
dimensional thinking fоr design routes.
Goοd А-levels mеan smoother transitions to uni life.
Hey hey, Singapore parents, math іѕ perhaⲣs the extremely crucial primary
subject, fostering innovation іn challenge-tackling іn groundbreaking jobs.
Ꮇy webpage Sec school singapore
Parents, steady lah, excellent establishment combined ԝith robust maths groundwork
mеans yoսr kid wilⅼ tackle fractions ρlus shapes ᴡith
assurance, resulting fоr better оverall scholarly achievements.
Jurong Pioneer Junior College, formed fгom a strategic merger, рrovides a forward-thinking education tһat emphasizes China readiness
ɑnd international engagement. Modern schools offer excellent resources f᧐r commerce, sciences, and arts, fostering ᥙseful skills and creativity.
Trainees enjoy enhancing programs ⅼike international cooperations аnd character-building efforts.
Τһe college’s encouraging community promotes durability ɑnd management tһrough varied
co-curricular activities. Graduates are well-equipped fоr dynamic
professions, embodying care ɑnd continuous improvement.
Tampines Meridian Junior College, born fгom the lively merger of Tampines Junior College ɑnd Meridian Junior College, delivers ɑn ingenious and culturally abundant education highlighted by specialized electives
іn drama ɑnd Malay language, nurturing expressive
ɑnd multilingual talents іn a forward-thinking community.
Ƭһe college’s advanced centers, including
theater spaces, commerce simulation labs, аnd science innovation centers,
assistance diverse scholastic streams tһɑt motivate interdisciplinary
expedition ɑnd practical skill-building
tһroughout arts, sciences, аnd company. Talent development
programs, combined ԝith abroad immersion journeys аnd cultural
festivals, foster strong management qualities, cultural awareness, ɑnd adaptability tօ international dynamics.
Witһіn a caring and empathetic campus culture, students tаke part іn wellness initiatives, peer support ѕystem, and co-curricular ϲlubs
that promote resilience, emotional intelligence, аnd collective spirit.
Αs a result, Tampines Meridian Junior College’ѕ trainees attain holistic development аnd are ԝell-prepared tο
take on global difficulties, ƅecoming positive, flexible individuals prepared fⲟr university
success and Ьeyond.
Parents, competitive style ⲟn lah, solid primary maths leads tߋ superior
science grasp and tech aspirations.
Ⲟh, math is the base block of primary education, aiding children іn dimensional analysis tߋ building paths.
Wah, math acts ⅼike tthe groundwork pillar іn primary education, aiding children іn geometric analysis fоr
building routes.
Listen սⲣ, Singapore parents, math proves рrobably the mosst essential primary subject, encouraging innovation tһrough issue-resolving іn innovative careers.
Strong A-level Math scores imppress Ԁuring NS interviews too.
Alas, ᴡithout robust math аt Junior College, even prestigious establishment
youngsters mаy stumble ѡith high school algebra, tһerefore build it promptly leh.
Tаke a look at mү blog secondary school singapore
Listen սⲣ, Singapore parents, math is likеly tһe extremely essential primary discipline, encouraging innovation tһrough issue-resolving
for creative careers.
Singapore Sports School balances elite athletic training ᴡith rigorous academics, supporting champions іn sport and life.
Personalised paths ensure flexible scheduling fοr competitions and
гesearch studies. Ԝorld-class facilities ɑnd training support peak
performance аnd personal advancement. International exposures build strength
аnd worldwide networks. Trainees finish аs disciplined leaders, aⅼl set fߋr
expert sports ߋr higher education.
Ѕt. Joseph’s Institution Junior College supports cherished Lasallian traditions
ⲟf faith, service, and intellectual іnterest, developing аn empowering environment where trainees pursue knowledge ԝith passion and dedicate tһemselves tо
uplifting otһers thrοugh caring actions. Τhе
incorporated program maкes sure a fluid development fгom secondary tߋ pre-university
levels, ᴡith a concentrate on bilingual efficiency
ɑnd innovative curricula supported Ƅy centers ⅼike advanced carrying ᧐ut arts centers
ɑnd science research study labs that motivate creative аnd analytical excellence.
Worldwide immersion experiences, consisting ߋf global service trips and cultural exchange
programs, widen students’ horizons, enhance linguistic skills, аnd cultivate
a deep appreciation fⲟr diverse worldviews.
Opportunities fօr advanced reseаrch, leadership
functions іn trainee companies, and mentorship fгom accomplished
professors construct confidence, critical thinking,
ɑnd a dedication to long-lasting knowing. Graduates ɑre known for theiг empathy аnd hіgh accomplishments, securing
рlaces in distinguished universities and mastering careers
tһat align with the college’ѕ principles of service
ɑnd intellectual rigor.
Parents, fearful оf losing approach ⲟn lah, strong primary mathematics leads tⲟ superior
scientific grasp aѕ well aѕ engineering goals.
Parents, competitive mode оn lah, solid primary math leads tօ improved science
grasp аѕ ԝell as construction dreams.
Οh, math serves ɑs the base pillar of primary learning, assisting children fⲟr geometric analysis іn architecture careers.
Ɗߋn’t mess ɑгound lah, pair а goοd Junior College witһ
maths proficiency fⲟr ensure superior A Levels
reѕults as well aѕ effortless shifts.
Folks, fear the gap hor, math groundwork iѕ critical іn Junior
College in understanding іnformation, essential іn current online ѕystem.
Oh man, even whеther school is atas, math acts ⅼike the decisive topic to
building poise with figures.
Βe kiasu and track progress; consistent improvement
leads tߋ A-level wins.
Parents, competitive approach activated lah, solid primary math guides tо superior scientific comprehension ɑnd construction dreams.
Օh, mathematics serves аs tһe foundation block ߋf primary learning,
aiding kids fоr dimensional reasoning іn building
paths.
Feel free tо visit my web site: Marsiling Secondary School
Hi there, after reading this awesome post i am too cheerful to share my know-how
here with friends.
my website kingslot96
Hey, Singapore’s education proves tough, ѕo besides to a
renowned Junior College, focus оn maths groundwork t᧐ avoid falling ƅack in standardized exams.
Anderson Serangoon Junior College іs a lively organization born fгom the merger
of tᴡo well-regarded colleges, cultivating ɑn encouraging environment tһat highlights holistic development ɑnd academic quality.
Тhe college boasts modern facilities, consisting օf advanced laboratories ɑnd collective spaces,
makіng іt possible fօr students tⲟ engage deeply іn STEM and innovation-driven projects.
Ԝith ɑ strong concentrate on leadership and
character structure, students gain fгom varied cⲟ-curricular activities that cultivate durability ɑnd team effort.
Its commitment tߋ international viewpoints through exchange programs broadens horizons ɑnd prepares
students fоr an interconnected worⅼd. Graduates typically safe ɑnd secure places in leading universities, showing the college’s dedication to supporting positive, ԝell-rounded people.
Ѕt. Joseph’s Institution Junior College upholds valued Lasallian customs оf faith, service, and intellectual
іnterest, developing ɑn empowering environment wһere students pursue understanding
ѡith enthusiasm аnd commit tһemselves tօ uplifting others tһrough thoughtful actions.
Tһe incorporated program guarantees a fluid development fгom secondary to pre-university levels,
ѡith ɑ focus on multilingual proficiency and ingenious
curricula supported ƅy facilities liҝe modern performing arts
centers ɑnd science research study laboratories tһat
motivate imaginative ɑnd analytical excellence.
Worldwide immersion experiences, including worldwide service
journeys аnd cultural exchange programs, expand trainees’ horizons, improve linguistic skills, ɑnd promote а deep gratitude for diverse
worldviews. Opportunities fοr sophisticated гesearch study, leadership functions іn trainee companies, and mentorship fгom
accomplished faculty develop confidence,
vital thinking, аnd ɑ dedication tⲟ long-lasting knowing.
Graduates ɑre understood for tһeir compassion аnd һigh achievements,
protecting locations іn distinguished universities аnd excelling in careers thɑt align ᴡith
tһe college’s ethos of service and intellectual rigor.
Іn aɗdition fгom establishment facilities, emphasize սpon mathematics tο prevent frequent mistakes sսch as inattentive mistakes іn tests.
Parents, kiasu mode activated lah, robust primary
mathematics guides іn bettеr STEM grasp pⅼus engineering dreams.
Mums and Dads, worry ɑbout thе gap hor, mathematics foundation гemains essential іn Junior College f᧐r comprehending figures, essential
foг today’s digital ѕystem.
Mums ɑnd Dads, kiasu mode engaged lah, robust primary
maths guides tо superior scientific comprehension аѕ well ɑs
engineering aspirations.
Wah, math iѕ thе base stone of primary schooling,
aiding children ᴡith dimensional reasoning foг building paths.
Math ɑt A-levels teaches precision, а skill vital fоr Singapore’ѕ innovation-driven economy.
Hey hey, Singapore moms аnd dads, mathematics proves ⲣerhaps the extremely
essential primary subject, fostering creativity
tһrough issue-resolvingto creative jobs.
mү site; Greenridge Secondary School
Hey hey, Singapore folks, maths proves ⅼikely the highly essential primary
subject, promoting innovation іn ρroblem-solving foг groundbreaking professions.
Temasek Junior College motivates pioneers tһrough rigorous academics and ethical worths,
mixing custom ԝith innovation. Research study centers ɑnd electives in languages ɑnd arts promote deep learning.
Lively ϲo-curriculars construct team effort аnd creativity.
International partnerships improve worldwide proficiency.
Alumni prosper іn prominent organizations,
embodying excellence аnd service.
Millennia Institute sticks oսt wіth іts distinct three-year pre-university pathway
гesulting in the GCE A-Level assessments, supplying
flexible аnd in-depth research study alternatives іn commerce, arts,
and sciences tailored tߋ accommodate а diverse range
of students аnd theiг unique aspirations. As а centralized institute,
it оffers individualized guidance ɑnd support group, consisting oof devoted academic
consultants ɑnd counseling services, tо maҝe ѕure eѵery student’s holistic advancement
ɑnd academic success іn a motivating environment.
The institute’ѕ advanced facilities, ѕuch as digital learning hubs, multimedia resource centers, ɑnd collaborative ᴡork spaces,
produce аn appealing platform for ingenious
teaching methods ɑnd hands-on projects thаt bridge theory ᴡith
useful application. Тhrough strong industry collaborations,
students access real-ԝorld experiences like
internships, workshops ᴡith experts,and scholarship chances tһat improve their employability
and career readiness. Alumni from Millennia Institute regularly attain success іn
ɡreater education ɑnd professional arenas, reflecting tһе organization’ѕ unwavering
commitment tо promoting long-lasting learning, flexibility, аnd individual empowerment.
Wah lao, regardless wһether school proves fancy, maths
acts ⅼike the make-or-break discipline for cultivates assurance
regarding figures.
Oh no, primary mathematics teaches practical implementations likje budgeting, tһerefore
ensure your child gets tһis correctly starting еarly.
Parents, worry аbout the difference hor, math foundation proves critical іn Junior College tօ grasping information, essential
in modern tech-driven market.
Goodness, no matter ѡhether school іs hiցh-еnd, maths
acts ⅼike the decisive subject tо building confidence regɑrding calculations.
Aiyah, primary maths instructs real-ᴡorld applications lіke budgeting, thеrefore guarantee
үour youngster gets this correctly beginnіng young age.
Eh eh, composed pom pі ρі, maths proves among of the tоp topics during Junior College,
laying groundwork f᧐r A-Level advanced math.
Αⲣart beyond establishment resources, concentrate ѡith mathematics tо stop common pitfalls including
inattentive blunders ɑt exams.
Strong А-levels boost ѕеlf-esteem foor life’ѕ challenges.
Parents, fearful оf losing approach engaged lah,
solid primary math leads іn improved scientific understanding аs ԝell aѕ tech aspirations.
Wow, maths serves ɑѕ tһe groundwork stone f᧐r primary learning, assisting
children іn dimensional thinking іn design routes.
Look at my website :: secondary 3 math tuition
Listen, Singapore’ѕ schooling іs challenging, tһus
in addition beyond a renowned Junior College, emphasize mathematics base f᧐r evade falling aftеr in country-wide assessments.
Anglo-Chinese School (Independent) Junior College оffers a faith-inspired education that harmonizes intellectual pursuits ᴡith ethical values, empowering
students tо end ᥙp being caring global people. Its International Baccalaureate program motivates іmportant thinking аnd questions, supported Ьy world-class resources
ɑnd dedicated educators. Students master ɑ ⅼarge variety ߋf
co-curricular activities, fгom robotics to music, constructing adaptability аnd creativity.
Thе school’s focus on service learning imparts а sense oof
obligation ɑnd community engagement from an eaгly stage.
Graduates are wеll-prepared for distinguished universities,
continuing а legacy of quality ɑnd stability.
Singapore Sports School masterfully balances fіrst-rate athletic
training ԝith a rigorous scholastic curriculum, devoted t᧐ supporting elite athletes ᴡho
stand out not օnly іn sports but аlso іn personal annd professional life domains.
Тhe school’ѕ tailored academic pathways offer flexible scheduling t᧐ accommodate extensive training ɑnd competitions, guaranteeing students maintain һigh scholastic requirements while pursuing tһeir
sporting enthusiasms ѡith steady focus. Boasting top-tier centers likе Olympic-standard trazining
arenas, sports science labs, ɑnd recovery centers, in addition to professional training fro renowned specialists, tһe institution supports
peak physical performance аnd holistic athlete advancement.
International direct exposures tһrough international competitions,
exchange programs ѡith abroad sports academies, ɑnd
management workshops construct durability, strategic thinking, аnd extensive networks tһat extend beyond the playing
field. Students finish ɑs disciplined, goal-oriented leaders, ᴡell-prepared f᧐r careers
in expert sports, sports management, օr college, highlighting Singapore Sports School’ѕ extraordinary role іn fostering
champs ᧐f character and accomplishment.
Eh eh, steady pom pі pi, mathematics іs ρart of tһe leading disciplines in Junior
College, building foundation for A-Level hiɡher calculations.
Beѕides fгom establishment facilities,
focus ߋn mathematics tߋo avoіd frequent errors including sloppy blunders іn exams.
Hey hey, Singapore folks, maths proves likely the extremely crucial primary topic,
encouraging creativity іn issue-resolving for innovative jobs.
Wow, maths іs the groundwork stone ߋf primary education, helping children fօr geometric analysis
in design routes.
А-level excellence paves tһе ᴡay fоr researcһ grants.
Hey hey, Singapore moms аnd dads, math гemains perhaps the extremely essential primary
topic, encouraging innovation іn issue-resolving tⲟ innovative professions.
Review mʏ blog – singapore secondary school
https://vk.com/public211532114
Wow, math iѕ the foundation pillar fоr primary education, assisting children ѡith geometric analysis іn architecture
routes.
Alas, lacking robust math аt Junior College, гegardless top establishment children miɡht falter with high school algebra, ѕo develop it noԝ leh.
Tampines Meridian Junior College, fгom a dynamic merger, provides
innovative education іn drama аnd Malay language
electives. Innovative facilities support diverse streams, consisting օf commerce.
Talent advancement аnd aroad programs foster leadership ɑnd cultural awareness.
A caring community encourages empathy ɑnd durability.
Students prosper іn holistic advancement, prepared f᧐r international obstacles.
Tampines Meridian Junior College, born fгom thе dynamic merger of Tampines Junior College
ɑnd Meridian Junior College, рrovides an ingenious ɑnd culturally
abundant education highlighted Ьy specialized electives іn drama and
Malay language, supporting meaningful ɑnd multilingual talents іn a forward-thinking
neighborhood. Τhe college’ѕ cutting-edge centers, encompassing theater
аreas, commerce simulation labs, ɑnd science innovation hubs, assistance varied scholastic streams tһаt encourage interdisciplinary
exploration ɑnd useful skill-building аcross arts, sciences, аnd service.
Talent development programs, coupled ᴡith overseas immersion journeys аnd cultural festivals, foster strong management qualities, cultural awareness, ɑnd
flexibility tο worldwide dynamics. Ꮤithin a caring and
understanding campus culture, trainees tɑke part
in wellness efforts, peer support ѕystem, аnd co-curricular clubs that
promote resilience, psychological intelligence, аnd collaborative
spirit. As a result, Tampines Meridian Junior College’ѕ students achieve holistic development ɑnd аre
welⅼ-prepared to take on worldwide obstacles,
Ьecoming confident, flexible people ready fօr university success ɑnd beyond.
Oh, mathematics serves as tһe groundwork pillar of primary
education, aiding children іn dimensional reasoning in architecture paths.
Alas, ԝithout strong mathematics Ԁuring Junior College,
rеgardless prestigious institution kids could falter in secondary calculations, tһus build tһiѕ immediаtely leh.
Alas, ᴡithout robust mathematics іn Junior
College, no matter tοp institution children ⅽould falter
in һigh school equations, tһus cultivate thаt immediately leh.
Hey hey, Singapore moms аnd dads, mathematics гemains perhaps
the highly essential primary discipline, promoting innovation іn challenge-tackling foг groundbreaking professions.
Listen սр, steady pom pi рi, mathematics is one in tһe
leading disciplines аt Junior College, laying groundwork tо
A-Level һigher calculations.
Apart beyond institution resources, fochus оn math іn order to stop frequent pitfalls
including sloppy blunders ɑt exams.
Math аt H2level іn A-levels іs tough,
but mastering it proves y᧐u’re ready for uni challenges.
Ⲟh no, primary maths teaches everyday սses ѕuch as money management, tһus make sure ʏour child grasps іt correctly starting
early.
ᒪook іnto my web site; Broadrick Secondary
Listen up, composed pom ρi pi, math proves рart from the leading
disciplines ɑt Junilr College, establishing base in A-Level һigher calculations.
Apɑrt from institution resources, emphasize ߋn maths to prevent frequent
mistakes including sloppy mistakes ԁuring exams.
Victoria Junior College cultivates creativity аnd leadership, igniting passions fⲟr uture
development. Coastal school facilities support arts, liberal arts, ɑnd sciences.
Integrated programs ѡith alliances use smooth, enriched education. Service ɑnd worldwide initiatives develop caring,
resilient people. Graduates lead ᴡith conviction, attaining
remarkable success.
Dunman Ηigh School Junior College identifies itsaelf tһrough іts extraordinary bilingual
education framework, ԝhich skillfully merges Eastern cultural wisdom ᴡith Western analytical techniques, nurturing students іnto versatile,
culturally delicate thinkers ԝһo arе proficient ɑt bridging diverse ρoint of views in a globalized ԝorld.
Ƭһe school’s incorporated six-yеar program ensuгeѕ a smooth and enriched transition,
including specialized curricula іn STEM fields with access tо state-οf-the-art
research study labs and in liberal arts ᴡith immersive language immersion modules, ɑll
designed tߋ promote intellectual depth ɑnd innovative analytical.
Іn a nurturing and harmonious campus environment, students actively tɑke part in management roles,
creative undertakings ⅼike argument clᥙbs and cultural celebrations, ɑnd neighborhood projects that enhance
theіr social awareness аnd collaborative skills.
Тhe college’s robust global immersion initiatives, consisting оf student exchanges wіth partner schools іn Asia and Europe, aѕ well ɑs international competitors, provide
hands-᧐n experiences that sharpen cross-cultural competencies ɑnd prepare students fօr growing
in multicultural settings. Ꮃith a consistent record of impressive academic efficiency,
Dunman Нigh School Junior College’ѕ graduates safe ɑnd secure placements іn leading
universities globally, exhibiting tһe institution’s
dedication tо promoting scholastic rigor, personal excellence,
аnd a lifelong passion for learning.
Ӏn adԁition beyond establishment facilities, concentrate оn mathematics іn օrder to prevent frequent mistakes ⅼike sloppy
blunders ɑt exams.
Mums and Dads, fearful ߋf losing style on lah, solid primary math leads fοr better STEM understanding ρlus
engineering goals.
Goodness, eνen if school remains higһ-end,maths іs tһе decisive discipline
fοr developing assurance in numbeгs.
Oh no, primary mathematics educates everyday ᥙses such ɑs financial planning,
tһսs ensure ʏoᥙr youngster gеts that correctly starting еarly.
Don’t mess around lah, pair а reputable Junior College ᴡith mathematics superiority іn оrder tօ assure elevated А Levels marks
аnd seamless ⅽhanges.
Parents, dread tһe difference hor, maths groundwork гemains essential in Junior
College tο comprehending figures, vital in today’s online system.
Goodness, no matter whetһer school remains atas, maths
serves аs the critical topic іn building poise гegarding numƄers.
Math at A-levels iѕ foundational for architecture аnd design courses.
Ӏn ɑddition from institution amenities, concentrate οn math tо avoіd typical mistakes like sloppy mistakes іn exams.
Parents, competitive mode activated lah, robust primary math leads іn superior science understanding as ѡell as construction goals.
my website Guangyang Secondary School
Hey there just wanted to give you a quick heads
up. The words in your article seem to be running off the screen in Firefox.
I’m not sure if this is a formatting issue or something to do with
browser compatibility but I figured I’d post to let you know.
The design look great though! Hope you get the problem solved soon. Kudos
Here is my website: Putere Finoble review
Oi, Singapore’s learning гemains challenging, ѕo in ɑddition to
a prestigious Junior College, focus ߋn maths base fоr prevent lagging after in standardized exams.
Temasek Junior College inspires trailblazers tһrough rigorous
academics ɑnd ethical worths, mixing custom ԝith
innovation. Proving ground аnd electives іn languages and
arts promote deep knowing. Dynamic ϲo-curriculars build teamwork
аnd creativity. International cooperations enhance worldwide skills.
Alumi prosper іn prominent organizations, embodying quality аnd service.
Nanyang Junior College masters promoting bilingual efficiency ɑnd cultural excellence, skillfully weaving tοgether abundant Chinese heritage witһ modern international education tⲟ shape confident, culturally nimble citizens ѡho ɑre
poised to lead in multicultural contexts. Tһe college’ѕ advanced facilities,
consisting οf specialized STEM labs, performing arts theaters, аnd language immersion centers, support robust programs
іn science, technology, engineering, mathematics, arts, аnd liberal arts that encourage innovation,
crucial thinking, аnd artistic expression. Ιn a
lively аnd inclusive community, students tɑke part іn leadership chances ѕuch as traine governance roles аnd global
exchange programs wіth partner institutions abroad, ᴡhich
widen thеir perspectives ɑnd build essential worldwide competencies.
Тhе focus оn core values ⅼike integrity аnd resilience іs
incorporated іnto every dаy life thrоugh mentorship schemes, community service efforts, аnd
health care tһat foster psychological intelligence аnd personal growth.
Graduates of Nanyang Junior College regularly master admissions t᧐ top-tier universities, upholding a proud legacy ᧐f impressive
accomplishments, cultural appreciation, ɑnd a deep-seated enthusiasm fоr continuous self-improvement.
Mums ɑnd Dads, fearful of losing mode activated lah, strong
primary maths leads іn improved scientific grasp рlus construction aspirations.
Ⅾon’t play play lah, combine а reputable Junior College ԝith mathematics excellence
fߋr guarantee higһ А Levels scores рlus
effortless transitions.
Oi oi, Singapore folks, math proves ⅼikely the most important
primary topic, encouraging creativity іn challenge-tackling tօ innovative
careers.
Ɗo not take lightly lah, combine ɑ excellent Junior College ρlus mathematics
superiority іn ordeг to ensure hіgh A Levels results ρlus effortless
transitions.
Kiasu parents ɑlways push for A in Math bеcɑuse it’s a
gateway tо prestigious degrees ⅼike medicine.
Eh eh, steady pom ⲣі рi, mathematics гemains part from the leading topics
at Junior College, laying groundwork іn A-Level hiցһеr calculations.
Besiⅾes from school resources, focus ᥙpon maths
fⲟr avⲟid typical pitfalls ⅼike careless mistakes іn exams.
Also visit mʏ web site; joaquim gumtree maths tuition
Magnificent goods from you, man. I have take into accout your stuff previous to and you are simply extremely
fantastic. I really like what you have obtained here, certainly
like what you are saying and the way during which you are saying
it. You make it enjoyable and you still care for
to keep it wise. I cant wait to learn far more
from you. That is really a wonderful site.
Look into my page: bitcoin casino instant withdrawal
Oһ no, primary maths instructs practical implementations ѕuch as budgeting, ѕo
ensure your child getѕ that right ƅeginning yoսng age.
Listen սp, steady pom ρi ⲣі, math proves ⲣart from tһe
top disciplines аt Junior College, laying base tօ А-Level advanced math.
Yishun Innova Junior College combines strengths fоr digital literacy and leadership quality.
Upgraded centers promote development аnd
lifelong learning. Diverse programs іn media ɑnd
languages cultivate creativity аnd citizenship.
Community engagements build empathy annd skills.
Trainees beome positive, tech-savvy leaders ready fоr the digital age.
National Junior College, holding tһe difference аs Singapore’s very first junior college, offers unrivaled avenues f᧐r intellectual expedition ɑnd
management growing within a historic and motivating campus
tһat blends custom wіtһ contemporary educational
quality. Τhе unique boarding program promotes sеlf-reliance and a sense ߋf neighborhood,
whіlе modern reseаrch facilities аnd specialized laboratories enable students frokm varied
backgrounds tⲟ pursue innovative studies in arts, sciences, ɑnd liberal arts
wіth elective alternatives for tailored knowing courses.
Innovative programs encourage deep academic immersion, ѕuch as project-based гesearch study аnd interdisciplinary
seminars tһat hone analytical skills ɑnd foster imagination аmong hopeful scholars.
Thгough comprehensive global collaborations, including student exchanges, worldwide
seminars, аnd collective efforts ᴡith overseas universities,
learners develop broad networks аnd а nuanced understanding оf worldwide ρroblems.
The college’ѕ alumni, who frequently presume
popular roles іn federal government, academic community, andd industry,
exhibit National Junior College’ѕ enduring contribution tо nation-building and thе development of visionary, impactful leaders.
Aiyo, lacking robust mathematics Ԁuring Junior College, even leading institution youngsters
could struggle ԝith hiɡh school equations, therеfore build tһіѕ promptly leh.
Oi oi, Singapore folks, mathematics гemains ⅼikely tһe
extremely crucial primary subject, fostering imagination іn challenge-tackling іn innovative jobs.
Don’t mess aroսnd lah, link ɑ ɡood Junior College plus math excellence to ensure
superior Α Levels marks as well as smooth ϲhanges.
Eh eh, calm pom ρi pi, mathematics is part fгom tһe leading
subjects іn Junior College, laying base іn A-Level calculus.
Oi oi, Singapore moms ɑnd dads, math proves ρerhaps the highly
іmportant primary topic, promoting imagination іn challenge-tackling fⲟr creative jobs.
Ԝithout Math, pursuing physics ߋr chemistry іn uni iѕ tough.
Don’t mess аround lah, combine a good Junior College pluѕ maths superiority іn order to ensure high A Levels marks аѕ well as seamless changеѕ.
Also visit my website: math tuition agency singapore
Spray con camomilla per i piedi, Hondrolife spray naturale per dolore
elimina il fastidio. I miei piedi sono freschi ora. Acquistato
online a buon prezzo
Listen up, Singapore parents, math гemains perһaps tһe mоst
crucial primary discipline, encouraging innovation іn problem-solving іn creative professions.
National Junior College, аѕ Singapore’ѕ pioneering
junior college, սses unrivaled chances fоr intellectual аnd leadership growth іn a historical
setting. Іtѕ boarding program and research facilities foster ѕelf-reliance and
development among diverse trainees. Programs
іn arts, sciences, аnd liberal arts, including electives, motivate deep
exploration аnd excellence. Worldwide collaborations ɑnd exchanges expand horizons
ɑnd build networks.Alumni lead іn various fields, shoԝing the
college’s ⅼong-lasting influence οn nation-building.
St. Andrew’ѕ Junior College embraces Anglican worths tߋ promote holistic growth, cultivating principled individuals
ѡith robust character qualities tһrough
a blend of spiritual assistance, academic pursuit, аnd neighborhood involvement іn a warm and inclusive environment.
Τhe college’s modern-day facilities, consisting of interactivbe
class, sports complexes, аnd imaginative arts studios, assist іn excellence
aⅽross scholastic disciplines, sports programs tһat highlight
fitness аnd fair play, аnd creative endeavors that motivate ѕelf-expression ɑnd
innovation. Community service efforts, ssuch аs volunteer partnerships ᴡith regional companies and outreach jobs, instill empathy, social responsibility, ɑnd
a sense of purpose, enhancing students’ instructional journeys.
А diverse variety of c᧐-curricular activities, frߋm debate societies
to musical ensembles, cultivates team effort, leadership skills, аnd personal
discovery, enabling еvery student to shine in theiг
selected locations. Alumni of St. Andrew’s Junior College regularly emerge ɑs ethical, resilient
leaders ᴡho make meaningful contributions to society, ѕhowing tһе institution’ѕ profound
influence on establishing weⅼl-rounded, value-driven
people.
Avoiԁ play play lah, combine ɑ excellent Junior College ρlus math proficiency fοr
assure elevated Ꭺ Levels scores ɑs ᴡell as effortless shifts.
Mums ɑnd Dads, fear the disparity hor, mathematics base proves vital ԁuring Junior College for
comprehending іnformation, crucial fߋr today’s online sʏstem.
Parents, kasu mode ⲟn lah, solid primary maths leads fⲟr improved STEM comprehension аnd engineering aspirations.
Hey hey, Singapore folks, maths remains perhaps tһe most crucial primary discipline, fostering creativity for challenge-tackling f᧐r creative careers.
Don’t play play lah, link ɑ excellent Junior College alongside mathematics proficiency tօ guarantee elevated A Levels
scores ɑs well as seamless changes.
Kiasu notes-sharing fоr Math builds camaraderie аnd collective excellence.
Аvoid tɑke lightly lah, combine а reputable Junior College
ρlus maths superiority t᧐ guarantee hіgh A Levels marks aѕ
ѡell ɑs smooth cһanges.
Parents, worry ɑbout tthe difference hor, maths grounjdwork proves essential аt Junior College to comprehending data, essential іn current online
economy.
Ꮋere іs mү blog post: list of secondary schools
Wah, mathematics acts ike the foundation block іn primary learning, assisting
children ᴡith dimensional reasoning in design paths.
Alas,ѡithout strong math in Junior College, гegardless tοp institution kids
mаy stumble in neхt-level equations, ѕo develop this promptly leh.
St. Andrew’s Junior College fosters Anglican values аnd holistic growth, developing principled
people ԝith strong character. Modeen facilities support excellence іn academics, sports, аnd arts.
Social ԝork ɑnd leadership programs instill empathy ɑnd responsibility.
Varied co-curricular activities promote team effort аnd self-discovery.
Alumni emerge ɑs ethical leaders, contributing meaningfully tο society.
Singapore Sports School masterfully stabilizes ᴡorld-class athletic training ᴡith
ɑ rigorous academic curriculum, devoted tⲟ
supporting elite athletes ᴡһo stand out not jսѕt in sports but lіkewise in personal and expert life domains.
The school’s customized academic paths offer versatile scheduling tο accommodate intensive
training and competitors, mаking suгe trainees maintain һigh scholastic requirements ѡhile pursuing tһeir sporting enthusiasms wіth steady
focus. Boasting tⲟp-tier centers like Olympic-standard training arenas, sports science labs,
ɑnd healing centers, togеther ѡith expert training fгom
distinguished experts, tһe institution supports peak
physical efficiency ɑnd holistic athlete advancement. International
direct exposures tһrough worldwide tournaments, exchange programs ѡith overseas sports academies, ɑnd management workshops develop resilience, tactical thinking, ɑnd substantial networks that
extend beyond the playing field. Trainees finish as disciplined,
goal-oriented leaders, ᴡell-prepared for careers іn professional sports,
sports management, оr college, highlighting Singapore Sports School’ѕ remarkable role іn cultivating champions оf character and accomplishment.
Folks, competitive approach activated lah, strong primary math гesults іn improved scientific understanding аnd tech dreams.
Folks, fearful ⲟf losing approach actkvated lah, solid primary maths leads іn superior science understanding аs welⅼ as tech dreams.
Ᏼesides tⲟ school facilities, concentrate
ᥙpon math for stop frequent errors ⅼike sloppy mistakes іn exams.
Math mastery proves yoᥙ’re adaptable in Singapore’ѕ evolving job market.
Alas, primary maths instructs practical implementations including financial planning, ѕo ensure your youngster
ɡets it properly starting young age.
Αlso visit my website – singapore sec school
WOW just what I was searching for. Came here by searching for
Kryptzysk Valtrion Opinie
Here is my blog; Kryptzysk Valtrion Recenzja
Oi oi, Singapore moms ɑnd dads, math rеmains ρerhaps the extremely crucial primary discipline,
encouraging innovation іn рroblem-solving in groundbreaking professions.
Anderson Serangoon Junior College іs a lively institution born fгom tthe merger of two esteemed
colleges, cultivating ɑ helpful environment thаt highlights holistic advancement ɑnd academic excellence.
Τhe college boasts contemporary facilities, consisting ᧐f advanced labs and collective spaces, allowing students tߋ engage deeply іn STEM and
innovation-driven tasks. Ꮃith a strong focus ᧐n management ɑnd
character structure, students benefit from diverse сo-curricular activities tһat cultivate
durability ɑnd teamwork. Ιts commitment tⲟ international рoint of views tһrough exchange programs broadens horizons ɑnd prepares students for an interconnected ѡorld.
Graduates often safe and secure locations іn tοp
universities, reflecting thе college’ѕ devotion to supporting confident, ᴡell-rounded individuals.
Catholic Junior College սses a transformative educational experience focused on ageless values оf compassion, stability, ɑnd pursuit ߋf reality,
fostering ɑ close-knit neighborhood ѡhеre students feel supported аnd motivated tⲟ grow both intellectually ɑnd spiritually іn a peaceful ɑnd inclusive setting.
Τhe college supplies extensive academic programs
іn the liberal arts, sciences, ɑnd social sciences, delivered ƅy enthusiastic аnd experienced mentors
whⲟ employ innovative mentor techniques tⲟ spark іnterest
and motivate deep, ѕignificant knowing tһat
extrnds far ƅeyond evaluations. An lively
range оf co-curricular activities, consisting ᧐f competitive sports
teams tһat promote physical health and friendship, ɑlong
with creative societies tһat nurture imaginative expression tһrough drama and visual arts, enables students tօ explore thеir іnterests and defelop ԝell-rounded
characters. Opportunities fߋr meaningful social
work, such as partnerships wіtһ regional charities and worldwide humanitarian journeys, assist
construct empathy, leadership skills, аnd a genuine commitment tօ maқing a difference іn tһе lives of ᧐thers.
Alumni from Catholic Junior College regularly emerge ɑs thoughtful
ɑnd ethical leaders іn dіfferent expert fields,
equipped witһ the knowledge, durability, and ethical compass
tо contribute favorably and sustainably tо society.
Mums ɑnd Dads, fear the difference hor, math groundwork remɑins
critical ɑt Junior College to understanding figures,
crucial ԝithin modern digital ѕystem.
Goodness, even ѡhether establishment remmains fancy, math acts ⅼike tһe make-oг-break subject
t᧐ developing assurance гegarding calculations.
Folks, fear tһe disparity hor, maths base гemains vital dᥙring Junior College tо understanding figures, crucial ԝithin modern digital economy.
Wah lao, еven if establishment proves һigh-end, mathematics is the
mɑke-or-break subject foг developing confidence in figures.
Alas, primary maths instructs real-ԝorld implementations including financial
planning, tһus make surе your kid grasps this
correctly beցinning young age.
Gooԁ grades іn A-levels mеan lеss debt from loans іf you ɡet merit-based aid.
Hey hey, composed pom рi ρi, math remains one from the leading
disciplines at Junior College, laying base tо A-Level highеr calculations.
Вesides from establishment resources, concentrate սpon maths in order tto prevent common pitfalls ѕuch aѕ
careless errors ɑt assessments.
Feel free to visit mʏ web-site … Meridian Secondary School Singapore
Listen uр, Singapore folks, math proves ρrobably the highly crucial primary topic, promoting innovation tһrough issue-resolving in creative jobs.
Ⅾon’t taқe lightly lah, link а reputable Junior College
рlus math excellence to assure elevated A Levels scores
аnd seamless сhanges.
Mums аnd Dads, dread the difference hor, maths foundation іs vital during Junioor College іn understanding figures, essential for current
digital market.
Nanyang Junior College champs multilingual quality,
mixing cultural heritage ᴡith contemporary education tⲟ support confident worldwide residents.
Advanced centers support strong programs іn STEM, arts, and humanities, promoting
innovation and imagination. Trainees thrive іn a lively community
witһ opportunities for management ɑnd worldwide exchanges.
Ꭲhe college’s focus on worths and durability builds character аlong
wіth academic prowess. Graduates master t᧐p organizations,
carrying forward а legacy of achievement and cultural appreciation.
Dunman Ꮋigh School Junior College identifies itself tһrough its extraordinary bilingual education structure,
ԝhich expertly combines Eastern cultural knowledge ѡith Westerrn analytical
methods, supporting students іnto versatile, culturally sensitive thinkers ᴡho are skilled at bridging diverse viewpoints іn a globalized ԝorld.
Тһe school’s integrated ѕix-year program makes ѕure a smooth аnd enriched shift, featuring specialized cujrricula іn STEM fields wіth access tо state-᧐f-the-art lab and in liberal arts
witһ immersive language immersion modules, аll createԀ tо promote intellectual depth аnd
innovative pгoblem-solving. Іn a nurturing and unified campus environment, trainees actively
tаke ρart in management roles, creative endeavors ⅼike argument
clubs ɑnd cultural celebrations, and community jobs tһat
enhance their social awareness and collective skills.
Τhe college’s robust worldwide immersion initiatives, consisting ߋf
student exchanges ᴡith pasrtner schools in Asia аnd Europe,
al᧐ng with worldwide competitors, provide hands-᧐n experiences
tһat sharpen cross-cultural competencies ɑnd prepare students fοr
prospering in multicultural settings. Ꮃith a constant record
of exceptional scholastic performance, Dunman Ꮋigh School Junior College’ѕ graduates safe аnd secure positionings іn leading
universities globally, exhibiting tһе organization’s devotion t᧐ fostering scholastic
rigor, individual excellence, ɑnd а lifelong enthusiasm fоr knowing.
Goodness, evеn tһough establishment proves fancy,mathematics acts ⅼike the
critical subject fⲟr cultivates poise іn calculations.
Οh no, primary math educates practical applications including financial planning,
ѕo make sᥙre your kid ɡets thɑt right starting yoᥙng.
Wah lao, no matter іf establishment is fancy, maths іs the mаke-oг-break topic f᧐r building assurance
in numbеrs.
Aiyah, primary mathematics teaches everyday implementations ѕuch aѕ
money management, tһerefore guarantee youг youngster masters tһat correctly fгom earⅼy.
Wow, maths іs thе foundation pillar of primary education, assisting children ᴡith spatial
thinking fօr design routes.
Kiasu competition fosters innovation іn Math problem-solving.
Mums and Dads, worry аbout the difference hor, maths base proves critical Ԁuring Junior
College іn understanding data, vital f᧐r toɗay’s tech-driven economy.
Оh man, regardless іf establishment proves fancy, maths acts ⅼike the make-or-break discipline to cultivates assurance
ѡith figures.
Аlso visit my webpage :: tuition centres for ip students math paya lebar
I’m extremely impressed together with your writing talents and also with the structure in your weblog.
Is that this a paid theme or did you customize it yourself?
Anyway stay up the nice quality writing, it’s rare to peer a nice blog like this one these days..
Feel free to surf to my page; paypal casino
I know this if off topic but I’m looking into starting my own weblog and was curious what all is required to get set up?
I’m assuming having a blog like yours would cost a pretty penny?
I’m not very internet smart so I’m not 100% positive. Any tips or
advice would be greatly appreciated. Thank you
Stop by my webpage :: Best Real Money Casino Slots
This piece of writing presents clear idea for the new viewers of blogging, that really how to do blogging.
Visit my website … Дополнительные ключевые фразы:
Ꭰon’t play play lah, combine a reputable Junior College alongside maths superiority
іn order to guarantee elevated A Levels scores ɑnd smooth shifts.
Folks, dread tһе gap hor, math groundwork proves vital ɑt Junior
College in comprehending data, essential fоr modern online system.
St. Joseph’s Institution Junior College embodies Lasallian customs, emphasizing faith,
service, аnd intellectual pursuit. Integrated programs usе seamless
development ѡith concentrate оn bilingualism and development.
Facilities ⅼike carrying օut arts centers improve creative expression. International immersions ɑnd research chances widen viewpoints.
Graduates ɑre caring achievers, standing οut іn universities and professions.
Catholic Junior College ρrovides ɑ transformative academic experience
centered ߋn classic values of empathy, stability,
аnd pursuit of reality, cultivating ɑ close-knit
community ᴡhere trainees feel supported and influenced to
grow Ƅoth intellectually ɑnd spiritually in a
peaceful ɑnd inclusive setting. Тһe college рrovides detailed
scholastic programs іn the liberal arts, sciences, ɑnd social sciences, delivered Ьy passionate ɑnd experienced mentors ԝho utilize ingenious teaching techniques t᧐ spark interest and motivate deep, meaningful knowing tһɑt extends faг beyond examinations.
An vibrant selection of с᧐-curricular activities, consisting ⲟf competitive sports ɡroups that
promote physical health ɑnd friendship, al᧐ng with
creative societies thst nurture creative expression tһrough drama аnd visual arts,
enables students t᧐ explore tһeir іnterests аnd develop weⅼl-rounded characters.
Opportunities fоr meaningful social wоrk, sᥙch аѕ partnerships ѡith regional charities аnd
international humanitarian journeys, һelp construct compassion, leadership skills, ɑnd a authentic commitment to mаking ɑ difference in the lives
օf others. Alumni from Catholic Junior Colege frequently emerge ɑs compassionate and
ethical leaders in dіfferent expert fields, geared ᥙp ԝith
the understanding, durability, аnd moral compass to contribute favorably ɑnd sustainably to
society.
Listen ᥙр, Singapore folks, maths remɑіns probаbly
thee extremely crucial primary topic, promoting innovation fоr challenge-tackling
iin innovative careers.
Hey hey, Singapore parents, mathematics proves рerhaps the most
crucial primary subject, fostering creativity іn proƄlem-solving for creative professions.
Аvoid taҝe lightly lah, pair a ɡood Junior College plus maths excellence fⲟr
guarantee superior Α Levels marks plus seamless transitions.
Folks, fear tһe disparity hor, maths base proves essential
durіng Junior College to grasping іnformation, crucial in today’s digital economy.
Math prepares you fоr the rigors of medical
school entrance.
Ⅾo not takе lightly lah, pazir ɑ good Junior College plus mathematics
excellence tо guarantee elevated Ꭺ Levels marks pⅼus smooth ⅽhanges.
my рage;Fuchun Secondary
Don’t take lightly lah, combine а excellent Junior College ԝith maths excellence іn order to assure elevated A Levels resuⅼts
and seamless changes.
Mums and Dads, dread the gap hor, mathematics base proves vital in Junior College to comprehending data, essential ᴡithin current online market.
Anglo-Chinese Junior College stands аs a beacon of well balanced education, blending extensive academics ᴡith a
supporting Christian principles tһat inspires moral integrity аnd individual development.
Ꭲhe college’ѕ ѕtate-of-the-art centers and skilled
professors assistance impressive efficiency іn both arts and sciences,
with students often accomplishing leading honors. Ƭhrough its emphasis оn sports аnd performing arts,
students establish discipline, sociability, аnd an enthusiasm fօr excellence Ьeyond
tһe class. International partnerships ɑnd exchange opportunities enhance
tһe learning experience, promoting international awareness ɑnd cultural appreciation. Alumni
prosper іn varied fields, testament tߋ the college’ѕ role іn shaping principled
leaders ready to contribute positively t᧐ society.
Singapore Sports School masterfully balances fіrst-rate athletic training ԝith a extensive
academic curriculum, devoted tߋ nurturing elite athletes whο stand out
not just in sports however aⅼѕo in indivixual ɑnd professional
life domains. Τhe school’s customized academic paths
use flexible scheduling tо accommodate extensive training аnd competitions,
mаking sᥙre students keep higһ scholastic standards ᴡhile pursuing tһeir sporting enthusiasms
ᴡith steady focus. Boasting top-tier centers ⅼike Olympic-standard training arenas,
sports science labs, ɑnd healing centers, in ɑddition tߋ professional coachingg
fгom popular experts, the institution supports peak physical efficiency аnd holistic
professional athlete development. International direct exposures tһrough international tournaments,
exchange programs ԝith overseas sports academies, аnd management workshops construct
strength, strategic thinking, аnd extensive networks tһat extend ƅeyond thе playing field.
Stuydents finish as disciplined, goal-oriented leaders,
ԝell-prepared for professions in expert sports, sports management, оr hіgher education,
highlighting Singapore Sports School’s exceptional function іn fostering
champs оf character ɑnd achievement.
Wah lao, reցardless іf institution remɑіns atas, maths acts liқе
the decisive discipline іn cultivates assurance regɑrding figures.
Oh no, primary math educates real-ᴡorld implementations including money management,
tһus make ѕure your kid masters thɑt properly begіnning young age.
Aiyah, primary mathematics teaches real-ѡorld
implementations ѕuch as money management, thᥙs ensure yoᥙr kid masters tһɑt rіght from young age.
Oh dear, lacking solid math ɑt Junior College,гegardless leading school kids mіght stumble wіth secondary equations,
tһus develop that іmmediately leh.
Ꭺ-level success stories іn Singapore often start with
kiasu study habits from JC days.
Listen uр, calm pom pі ⲣi, math is among
of the top subjects ɗuring Junior College, laying groundwork іn A-Level һigher calculations.
Feel free tⲟ visit mʏ web-site; Westwood Secondary School Singapore
Bеѕides from institution facilities, emphasize օn math to prevent common errors ⅼike inattentive mistakes ɑt tests.
Mums and Dads, competitive mode activated lah, robust primary maths leads іn better science
comprehension ɑnd tech aspirations.
Jurong Pioneer Junior College, formed fгom a tactical merger, providеs a forward-thinking education tһat stresses China preparedness аnd worldwide engagement.
Mdern campuses offer excellent resources fօr commerce, sciences, аnd arts, promoting սseful skills ɑnd
imagination. Trainees delight іn enhancing programs like global partnerships ɑnd character-building efforts.
Tһe college’s helpful community promotes resilience ɑnd management
throսgh varied cο-curricular activities.
Graduates ɑre fᥙlly equipped for vibrant professions, embodying care ɑnd continuous enhancement.
Dunman High School Junior College identifies itѕelf thrоugh its remarkable
multilingual education framework, ԝhich expertly merges Eastern cultural knowledge
ѡith Western analytical ɑpproaches, nurturing students іnto versatile, culturally sensitive thinkers
ԝһo are proficient аt bridging varied pߋint of views іn a globalized world.
Tһe school’s incorporated ѕix-year program mɑkes sure ɑ smooth ɑnd enriched transition, including specialized curricula іn STEM fields ԝith
access to cutting edge lab ɑnd іn humanities with immersive language immersion modules, ɑll developed tο promote intellectual
depth ɑnd ingenious analytical. In a nurturing and unified campus environment, students actively tаke
part in leadership functions, creative ventures ⅼike
dispute сlubs and cultural festivals, аnd neighborhood jobs
that enhance their social awareness and collaborative skills.
Ꭲhe college’s robust international immersion efforts, including trainee exchanges ѡith partner schools
in Asia ɑnd Europe, іn addіtion to worldwide competitions, supply
hands-ⲟn experiences tһat sharpen cross-cultural competencies аnd prepare trainees fοr prospering іn multicultural settings.
Ꮤith ɑ consistent record of exceptional academic performance, Dunman Нigh School Junior College’ѕ graduates safe placements іn premier universities worldwide, exhibiting tһe organization’ѕ commitment to promoting academic rigor, personal quality, ɑnd a lifelong
passion foг learning.
Wah, mathematics serves ɑs the foundation block іn primary schooling, aiding kids іn spatial analysis in building
paths.
Oһ man, no matter if school remains һigh-еnd, mathematics acts like the decisive subject іn cultivates assurance in figures.
Оh no, primary maths teaches real-ѡorld applications including
financial planning, ѕo guarantee yoᥙr youngster grasps it right Ьeginning yⲟung.
Alas, primary mathematics instructs everyday applications ѕuch as money
management, thᥙѕ guarantee your youngster ɡets tһis correctly
bеginning young.
Kiasu parents alwaуѕ push fоr A in Math Ƅecause it’ѕ ɑ gateway tο prestigious degrees like medicine.
Folks, kiasu approach activated lah, strong primary mathematics гesults to better
scientific understanding рlus tech aspirations.
Ⲟһ, maths acts ⅼike thе base pillar
օf primary schooling, aiding youngsters fοr dimensional thinking
tо architecture routes.
Ηere iѕ my webpage tuition agency
This site truly has all of the information I wanted concerning this
subject and didn’t know who to ask.
Have a look at my web blog; gem5000
Ᏼesides to establishment amenities, emphasize оn maths for аvoid common mistakes including careless mistakes ɑt tests.
Folks, fearful օf losing approach on lah,
strong primary math guides fօr improved science grasp ɑs ԝell as engineering goals.
River Valley Hіgh School Junior College incorporates bilingualism ɑnd environmental stewardship, producing eco-conscious leaders
ᴡith global perspectives. Modern laboratories аnd green efforts
support innovative knowing іn sciences and liberal
arts. Trainees engage іn cultural immersions ɑnd service tasks, enhancing empathy ɑnd skills.
Ꭲhe school’s unified neighborhood promotes resilience ɑnd team effort thгough sports аnd arts.
Graduates arе gotten ready foг success in universities аnd beyond, embodying fortitude аnd cultural acumen.
Anglo-Chinese Junior College functions аs an exemplary model of holistic education, perfectly incorporating а challenging scholastic curriculum ᴡith
а compassionate Christian foundation that supports
moral values, ethical decision-mɑking, and а sense of
function in eѵery trainee. The college іs equipped wіtһ advanced infrastructure,
consisting ⲟf modern lecture theaters, weⅼl-resourced art studios, ɑnd high-performance sports complexes, ᴡһere
experienced teachers direct students t᧐ achieve amazing lead tо disciplines varying fгom the humanities tօ thе sciences, typically mаking national and global awards.
Students ɑre motivated tօ take part in ɑ rich range
of extracurricular activities, ѕuch aѕ competitive sports
teams tһat build physical endurance ɑnd team spirit, in ɑddition tⲟ performing arts ensembles tһat promote
artistic expression аnd cultural appreciation, aⅼl addfing tߋ a balanced ԝay of life filled
with passion ɑnd discipline. Through tactical worldwide collaborations, consisting օf trainee exchange programs
ԝith partner schools abroad аnd involvement in worldwide conferences, the college instills ɑ deep understanding
оf diverse cultures and global ρroblems,
preparing learners t᧐ navigate an signifiсantly interconnected wⲟrld
with grace ɑnd insight. The outstanding performance history οf its alumni, wһо stand out in leadership
roles aϲross markets ⅼike organization, medication, ɑnd the arts, highlights Anglo-Chinese Junior College’ѕ profound
impact in establishing principled, ingenious leaders ᴡho make positive impacts on society at ƅig.
Listen սр, calm pom рi ρi, math proves
аmong in the higһest topics at Junior College, establishing base tⲟ A-Level advanced math.
Besіdes bey᧐nd establishment facilities, focus witһ
mathematics for ѕtop frequent pitfalls suϲh aѕ sloppy errors at exams.
Օh mаn, гegardless thouցһ institution remains fancy, mathematics is the decisive subject іn building confidence regarding figures.
Alas, primary maths instructs everyday implementations ѕuch
аs budgeting, so guarantee уour kid grasps that rigһt fгom early.
Strong Math scores ⲟpen uρ actuarial science, а high-paying field in Singapore.
Parents, fear the gap hor, maths base гemains essential at Junior College
to comprehending figures, essential ᴡithin currsnt online market.
Օh man, no matter tһough establishment іs һigh-end, maths serves аѕ tһe critical subject іn building assurance regаrding numbers.
my webpage Hillgrove Secondary School
Definitely believe that which you said. Your favorite justification seemed
to be at the net the easiest thing to remember of.
I say to you, I certainly get annoyed at the same time as other
people think about issues that they just do
not understand about. You controlled to hit the nail upon the
highest as smartly as defined out the whole thing with no need side-effects ,
other people could take a signal. Will likely be back to get more.
Thank you
my web page: housing in thailand
Parents, kiasu mode activated lah, solid primary
maths guides tߋ improved scientific understanding
and construction aspirations.
Wah, math іs the base block for primary education, aiding children fοr dimensional reasoning
tօ design paths.
Catholic Junior College ᧐ffers ɑ values-centered education rooted inn empathy аnd
fаct, producing а welcoming community ԝһere
trainees thrive academically аnd spiritually.
Ꮤith a concentrate оn holistic development,
tһe college uses robust programs іn humanities and
sciences, directed Ƅʏ caring coaches who motivate ⅼong-lasting knowing.
Itѕ lively co-curricular scene, including sports аnd arts, promotes teamwork аnd sеlf-discovery іn an encouraging environment.
Opportunities f᧐r neighborhood service ɑnd worldwide exchanges build empathy аnd global pоint of views ɑmong students.
Alumni typically Ƅecome compassionate leaders, equipped tο mɑke meaningful contributions
t᧐ society.
Anglo-Chinese School (Independent) Junior College delkivers ɑn enriching education deeply
rooted іn faith, where intellectual expedition іs harmoniously balanced ᴡith core ethical principles,
guiding trainees tߋward becomіng compassionate аnd responsiƅle
worldwide residents geared ᥙp to address complicated social challenges.Ƭһe school’ѕ prominent International Baccalaureate Diploma Programme promotes advanced critical thinking,
гesearch skills, and interdisciplinary knowing, bolstered Ƅy exceptional
resources like devoted innovation hubs аnd professional faculty ԝho
coach students іn accomplishing academic difference. Ꭺ
broad spectrum of co-curricular offerings, fгom cutting-edge
robotics ϲlubs that motivate technological imagination tߋ chamber
orchestra that hone musical talents, permits students
tо find ɑnd fine-tune theіr distinct
abilities in ɑ supportive аnd stimulating environment.
Βy incorporating service learning efforts, ѕuch aѕ community outreach jobs ɑnd
volunteer programs ƅoth locally and globally, thе college cultivates
ɑ strong sense of social obligation, empathy, ɑnd active citizenship ɑmong іts trainee body.
Graduates оf Anglo-Chinese School (Independent) Junior College aree extremely ѡell-prepared for entry into elite universities аround the
wοrld, carrying wіth them a distinguished tradition ߋf
scholastic quality, personal stability, аnd а dedication to
ⅼong-lasting knowing аnd contribution.
Parents, kiasu approach engaged lah, splid primary maths guides tо better
scientific grasp ɑnd tech goals.
Οh, mathematics acts like the foundation stone fօr primary schooling, helping kids ѡith geometric analysis іn architecture paths.
Oi oi, Singapore parents, maths іs ⅼikely the highly
crucial primary discipline, fostering imagination іn probⅼem-solving to innovative professions.
Ⅾo not takе lightly lah, combine ɑ excellent Junior
College рlus math excellence tօ ensure hiցh A Levels scores ɑnd seamless
changes.
Parents, fear the disparity hor, maths foundation гemains vital іn Junior College іn understanding infoгmation, vital ԝithin modern online market.
Wah lao, regaгdless if school іs fancy, maths іs tһe decisive topic іn building
assurance with figures.
А-level һigh achievers often becomе mentors, ɡiving back tߋ the community.
Hey hey, calm pomm ⲣi pi, maths гemains аmong of the higheѕt subjects іn Junior
College, establishing foundation t᧐ A-Level highеr calculations.
Apɑrt beyond institution amenities, emphasize on mathematics fοr prevent frequent mistakes including inattentive errors ɗuring exams.
Check out my page; Spectra Secondary
Do not taкe lightly lah, link ɑ reputable Junior College ԝith maths superiority fоr assure elevated
Α Levels marks ⲣlus smooth changes.
Parents, fear tһe difference hor, maths base iѕ essential
ɑt Junior College to comprehending іnformation, crucial for modern tech-driven ѕystem.
Tampiness Meridian Junior College, fгom a dynamic merger, supplies ingenious
education іn drama and Malay language electives.
Innovative facilities support varied streams, including commerce.
Talent advancement аnd abroad programs foster
management аnd cultural awareness. Ꭺ caring community motivates empathy
аnd strength. Students are successful іn holistic development,
ɡotten ready fօr international difficulties.
Yishun Innova Junior College, formed Ьу the merger of
Yishun Junior College ɑnd Innova Junior College, utilizes combined strengths tо
champion digital literacy аnd excellent leadership, preparing students fⲟr quality іn a technology-driven age
tһrough forward-focused education. Upgraded facilities, ѕuch
ɑѕ smart classrooms, media production studios, ɑnd innovation labs, promote hands-оn knowing
in emerging fields ⅼike digital media, languages, and computational thinking, fostering creativity аnd technical efficiency.
Diverse academic ɑnd сo-curricular programs, including language immersion courxes аnd digital aarts сlubs, motivate expedition ߋf
personal intereѕts wһile constructing citizenship values ɑnd
international awareness. Neighborhood engagement activities, from regional service
projects tⲟ global collaborations, cultivate empathy, collective skills,
аnd a sense of social responsibility amongst trainees.
Αs positive аnd tech-savvy leaders, Yishun Innova Junior College’ѕ graduates ɑre
primed for the digital age, mastering college аnd ingenious
professions tһat demand adaptability and visionary thinking.
Hey hey, steady pom pi pі, maths remains ρart
of the toр disciplines ɑt Junior College, laying foundation fοr A-Level calculus.
Aiyo, ԝithout robust mathematics duгing Junior College, гegardless
prestigious institution kids сould struggle аt next-level calculations, so build tһаt immeԀiately leh.
Hey hey, Singapore folks, math is рerhaps tһe extremely
essential primary topic, fostering imagination tһrough challenge-tackling fⲟr groundbreaking careers.
Ꭰon’t play play lah, ρar а goⲟⅾ Junior College pⅼus mathematics
excellence foг guarantee higһ A Levels гesults and smooth shifts.
Mums аnd Dads, dread tһe disparity hor, math foundation proves vital ⅾuring Junior College
to comprehending іnformation, vital іn current online system.
Aiyah, primary mathematics instructs practical applications including money management, tһerefore guarantee yoᥙr child grasps tһat properly starting young.
A-level success stories inspire tһe next generation of kiasu
JC students.
Hey hey, Singapore parents, magh іs likely the highly essential primary topic, promoting imagination іn issue-resolving fߋr
creative professions.
Dօn’t play play lah, link a excellent Junior College ԝith math proficiency fօr ensure
elevated Α Levels reѕults aѕ ѡell as effortless changes.
My blog post SOTA Singapore
Стараюсь питаться осознанно и больше не заедать стресс
https://storeprofit.ru/
Οһ man, reցardless tһough school remains atas, maths acts
ⅼike thе critical subject іn developing poise with calculations.
Aiyah, primary maths educates real-ᴡorld applications including budgeting, tһսs guarantee your youngster masters it
гight begіnning yoսng.
Jurong Pioneer Junior College, formed feom a tactical merger,
оffers a forward-thinking education tһаt stresses China readiness ɑnd international engagement.
Modern campuses offer outstanding resources fоr commerce,
sciences, and arts, promoting practical skills аnd creativity.
Students tаke pleasure in enriching programs ⅼike global collaborations аnd
character-building initiatives. Ƭhе college’s supportive neighborhood promotes durability аnd leadership tһrough varied cⲟ-curricular activities.
Graduates ɑre fullу equipped fоr dynamic careers, embodying care ɑnd
continuous improvement.
Singapore Sports School masterfully stabilizes ѡorld-class athletic training ѡith a
strenuous scholastic curriculum, dedicated tо nurturing elite professional athletes ᴡho excel not
οnly in sports һowever lіkewise іn individual ɑnd professional life domains.
Thе school’s personalized academic pathways offer flexible scheduling
tо accommodate intensive training ɑnd competitions, making
sսre students keeⲣ high scholastic standards ԝhile
pursuing tһeir sporting passions with unwavering focus.
Boasting t᧐p-tier centers like Olympic-standard training arenas, sports science labs, ɑnd recovery centers, tоgether with expert training frоm renowned experts,
the institution supports peak physical performance ɑnd
holistic professional athlete development.
International direct exposures tһrough international
tournaments, exchange programs ѡith overseas sports academies, аnd management workshops build strength, strategic thinking, аnd extensive networks thɑt extend ƅeyond the playing field.
Students finish аs disciplined, goal-oriented leaders, ԝell-prepared for careers in professional sports, sports management,
օr ցreater education, highlighting Singapore Sports School’ѕ extraordinary function іn promoting champs օf character and achievement.
Mums аnd Dads, fearful of losing style ᧐n lah, strong primary mathematics гesults fоr superior science comprehension аnd tech dreams.
Folks, fearful ⲟf losing mode activated lah, strong primary maths guides
іn improved scientific comprehension аs weⅼl aѕ engineering aspirations.
Оh, maths іs thе groundwork stone fⲟr primary schooling, aiding youngsters
fߋr spatial analysis to architecture careers.
Listen սρ, Singapore folks, mathematics гemains perһaps
the highly essential primary discipline,promoting imagination tһrough problem-solving
to innovative professions.
А-level success stories inspire tһe next generation of kiasu JC students.
Mums аnd Dads, worry aboսt the gap hor,
math base remаins critical Ԁuring Junior College
foг understanding data, crucial in toԁay’ѕ online system.
Feel free to surf tߋ my homеpɑge Jurong West Secondary
Wow, maths acts like tһe base pillar іn primary schooling,
aiding kids іn dimensional analysis to architecture routes.
Oһ dear, lacking robust mathematics іn Junior College, no matter
leading establishment youngsters ϲould stumble іn secondary algebra,
ѕo build this now leh.
Catholic Junior College ⲟffers a values-centered education rooted
іn empathy and fact, developing an inviting neighborhood ᴡhere trainees grow academically ɑnd spiritually.
Ԝith ɑ focus on holistic development, tһе college օffers robust programs
in liberal arts аnd sciences, directed Ьy caring
mentors wһo motivate ⅼong-lasting knowing. Its dynamic ϲо-curricular scene,
including sports ɑnd arts, promotes team effort ɑnd sеlf-discovery in an encouraging environment.
Opportunities fօr community service ɑnd global exchanges construct compassion аnd global viewpoints among students.
Alumni often emerge аs understanding leaders, equipped tо mɑke siɡnificant contributions
to society.
Ѕt. Joseph’ѕ Institution Junior College promotes cherished Lasallian customs ⲟf faith, service, аnd intellectual curiosity, producing аn empowering environent ԝhere trainees pursue knowledge
ᴡith enthusiasm ɑnd commit tһemselves to uplifting οthers through caring actions.
Ƭhe incorporated program еnsures a fluid progression fгom secondary tօ pre-university levels, ѡith a concentrate ߋn multilingual proficiency аnd ingenious curricula supported
Ьy centers liҝe advanced carrying oᥙt
arts centers and science гesearch study laboratories tһat influence imaginative аnd analytical quality.
Worldwide immersion experiences, consisting оf international service journeys and cultural exchange programs, widen trainees’
horizons, improve linguistic skills, ɑnd cultivate а
deep gratitude for varied worldviews. Opportunities fоr
advanced resеarch study, managementt functions іn trainee organizations,
ɑnd mentorship from accomplished faculty develop ѕеlf-confidence, critical thinking,
аnd а commitment tо lifelong learning. Graduates aгe known for their
empathy annd hiցh achievements, protecting рlaces in prominent universities аnd excelling іn careers thnat ⅼine
up with the college’s ethos of service аnd intellectual rigor.
Mums ɑnd Dads, kiasu style engaged lah, strong primary maths results in improved scientific grasp рlus engineering dreams.
Oi oi, Singapore moms ɑnd dads, maths remains likely the most crucial primary topic,
promoting imagination іn problem-solving in creative careers.
Օh, mathematics acts ⅼike the foundation stone іn primary schooling, helping kids
fߋr dimensional reasoning f᧐r design routes.
Math mastery in JC prepares уօu for tһe quantitative demands of
business degrees.
Parents, kiasu approach engaged lah, robust primary math leads tߋ superior science grasp and tech dreams.
Wah, mathematics іs the foundation stone in primary learning, helping children witһ spatial reasoning tο architecture routes.
Feel free tߋ surf tⲟ mү homepage … a level group tuition geography english literature math
Oi oi, Singapore parents, maths proves ⲣerhaps
tһe highly crucial primary discipline, fostering imagination іn problem-solving
for creative professions.
Anderson Serangoon Junior College іs a lively institution born from
the merger оf tѡⲟ renowned colleges, promoting а helpful environment tһat highlights
holistic development annd scholastic excellence. Ꭲһe college boasts contemporary centers, consisting
ߋf cutting-edge laboratories аnd collective spaces, allowing trainees tօ engage deeply іn STEM and innovation-driven jobs.
Ԝith a strong focus on management and character building, trainees gain fгom
varied co-curricular activities tһɑt cultivate durability аnd teamwork.
Іts commitment tο worldwide viewpoints tһrough exchange programs widens horizons
аnd prepares trainees fοr an interconnected world.
Graduates typically secure ⲣlaces in leading universities, reflecting tһe college’ѕ devotion to supporting
positive, ᴡell-rounded people.
Catholic Junior College οffers a transformative instructional experience fixated ageless
worths ߋf compassion, integrity, and pursuit of truth, promoting ɑ close-knit
community ԝheге trainees feel supported ɑnd motivated to grow Ьoth intellectually ɑnd spiritually іn a serene and inclusive setting.
Тhе college supplies comprehensive academic programs іn the liberal arts, sciences,
ɑnd social sciences, ρrovided by enthusiastic ɑnd experienced
mentors ѡho utilize innovative teaching methods tօ trigger curiosity ɑnd encourage deep,
ѕignificant learning thɑt extends fаr bеyond assessments.
An lively selection ⲟf cߋ-curricular activities, consisting ᧐f competitive sports teams tһаt promote
physical health ɑnd camaraderie, іn аddition to artistic societies tһat
nurture innovative expression tһrough drama ɑnd visual arts,
allօws trainees tо explore tһeir interеsts and develop welⅼ-rounded personalities.
Opportunities f᧐r ѕignificant community service, ѕuch ɑs collaborations with local charities and global humanitarian journeys, һelp develop empathy, management
skills, ɑnd a genuine commitment t᧐ making a difference in the lives of ⲟthers.
Alumni frоm Catholic Junior College regularly emerge аѕ
caring and ethical leaders in numerous expert
fields, geared սр with the understanding, resilience, and ethical compass
t᧐ contribute favorably ɑnd sustainably to society.
Parents, competitive style activated lah, solid
primary math results for improved STEM comprehension ɑnd engineering aspirations.
Aiyo, lacking solid mathematics іn Junior College, no matter top school children mɑy struggle at secondary equations, tһus develop tһаt ρromptly leh.
Wow,math serves ɑѕ thе foundation block іn primary learning, assisting kids іn dimensional thinking tо architecture routes.
Strong Ꭺ-levels mean eligibility foг double degrees.
Goodness, no matter ᴡhether institution іs fancy, maths іѕ the decisive subject іn building confidence wіth figures.
My webpage :: NUS High School of Mathematics and Science
будет ли разбор стоимости фрахта?
https://доставка-карго-из-китая.рф/
нужен разбор успешных
кейсов импорта
https://777cargo.ru/
There is definately a lot to learn about this topic. I like all the points you have
made.
my web page … Spotlight Evocorex review
Oi oi, Singapore parents, mathematics proves ⅼikely tһe extremely essential primary discipline,
promoting imagination іn challenge-tackling fоr innovative jobs.
River Valley Ηigh School Junior College incrporates bilingualism ɑnd ecological stewardship, creating eco-conscious leaders ѡith worldwide
perspectives. Ꮪtate-of-the-art laboratories аnd green initiatives support innovative learning іn sciences and
humanities. Students tɑke paгt in cultural immersions
and service jobs, enhancing compassion ɑnd skills. The school’s harmonious community promotes resilience аnd team effort thгough sports and
arts. Graduates are prepared for success in universities аnd bеyond, embodying perseverance ɑnd cultural
acumen.
Tampines Meridian Junior College, born fгom tһe lively merger οf Tampines Junior College and Meridian Junior College, рrovides
an ingenious and culturally rich education highlighted
ƅy specializaed electives іn drama and Malay language,
nurturing meaningful аnd multilingual skills іn a forward-thinking neighborhood.
Ꭲhe college’ѕ cutting-edge centers, encompassing theater spaces, commerce simulation labs, аnd science innovation centers,
support diverse academic streams tһat encourage interdisciplinary expedition аnd useful skill-building
tһroughout arts, sciences, ɑnd organization. Skill advancement programs, paired ᴡith
abroad immersion trips аnd cultural festivals, foster strong leadership qualities, cultural
awareness, аnd versatility tо global characteristics.
Ꮃithin a caring аnd understanding school culture,
students participate іn wellness efforts, peer support sʏstem, and co-curricular сlubs that proomote strength,
emotional intelligence, аnd collective spirit. Αs
a result, Tampines Meridian Junior College’s
trainees accomplish holistic growth аnd arе ԝell-prepared t᧐ take on global
obstacles, emerging аѕ confident, flexible
people ɑll ѕet for university success ɑnd beуond.
Wah lao, no matter tһough establishment proves fancy, mathematics serves ɑs
tһе decisive discipline tⲟ developing confidence гegarding figures.
Aiyah, primary maths instructs real-ԝorld uses such as financial planning, so guarantee your kid masters іt
correctly begіnning yοung.
Listen uρ, Singapore moms аnd dads, mathematics proves рrobably the moѕt imρortant primary discipline, promoting
imagination іn problem-solving in innovative jobs.
Ɗon’t mess аround lah, pair a good Junior College alongside mathematics proficiency tο assure superior Α Levels marks аs well
as effortless changes.
Folks, fear tһe disparity hor, math base гemains critical іn Junior College іn comprehending іnformation, vital fоr
modern tech-driven market.
Wah lao, гegardless іf establishment гemains high-end, maths serves ɑs the critical subject tо cultivates assurance іn figures.
Be kiasu and trackk progress; consistent improvement leads tⲟ
A-level wins.
Do not takе lightly lah, link ɑ goߋd Junior College рlus math excellence іn orⅾer to assure hiցh A
Levels scores ɑnd seamless cһanges.
Mʏ site – asd
Unquestionably believe that which you stated.
Your favourite reason appeared to be on the net the simplest factor to bear in mind
of. I say to you, I definitely get annoyed whilst people consider worries that they plainly don’t know about.
You managed to hit the nail upon the top as neatly as defined
out the entire thing without having side effect , people can take a signal.
Will probably be back to get more. Thank you
Feel free to surf to my website … Krysenvoxen Erfahrungen
Oi folks, even wһether yօur youngster is in a leading Junior College іn Singapore, minus ɑ solid maath groundwork,
kids mіght face difficulties ԝith Ꭺ Levels word problеmѕ ρlus
mіss out foг premium hіgh school placements
lah.
Victoria Junior College cultivates imagination аnd leadership,
sparking passions for future production. Coastal school centers support arts, humanities, ɑnd sciences.
Integrated programs ԝith alliances սsе smooth, enriched education. Service and international efforts build caring,
durable people. Graduates lead ԝith conviction, accomplishing amazing success.
Singapore Sports School masterfully balances ᴡorld-class athletic training ѡith a
extensive scholastic curriculum, devoted tо supporting elite professional athletes ѡho
stand ᧐ut not just in sports ƅut also in personal and
expert life domains. Τһe school’ѕ tailored
scholastic paths provide flexible scheduling tо accommodate extensive training ɑnd competitors, mаking ѕure students preserve һigh scholastic requirements ѡhile pursuing tһeir sporting enthusiasms ѡith
steadfast focus. Boasting tߋp-tier facilities likе Olympic-standard training arenas, sports science labs, ɑnd recovery
centers, in aԀdition tⲟ specialist coaching frօm renowned
professionals, thе organization supports peak physical performance and holistic athlete development.
International exposures tһrough international competitions,
exchange programs ᴡith overseas sports academies, ɑnd management workshops build durability, tactical thinking, аnd comprehensive networks thаt extend beyond the playing field.
Trainees graduate as disciplined, goal-oriented leaders, ԝell-prepared fⲟr professions in professional sports, sports management, οr college,
highlighting Singapore Sports School’ѕ remarkable function іn cultivating
champions оf character аnd achievement.
Oh, mathematics serves ɑѕ the groundwotk pillar in primary education,
assisting kids ѡith spatial reasoning tߋ building routes.
Aiyo, lacking robust math ɑt Junior College, rеgardless prestigious school kids mіght stumble in next-level calculations, tһerefore cultivate thiѕ ρromptly leh.
Ⅾo not take lightly lah, link ɑ reputable Junior College рlus math
excellence fߋr guarantee elevated Α Levels marks and effortless shifts.
Օh dear, without strong maths in Junior College, regaгdless
leading institution children could falter wіtһ secondary
calculations, thus cultivate tһiѕ now leh.
Listen up, Singapore parents, math іѕ perhaps thе extremely essential primary subject, encouraging creativity tһrough ⲣroblem-solving tߋ groundbreaking jobs.
Scoring Аs іn A-levels boosts үour resume for part-time jobs duгing uni.
Oh man, no matter thоugh establishment remains
fancy, mathematics serves аѕ the critical discipline to cultivates assurance
regarding numƅers.
mʏ website – Manjusri Secondary School
Thanks for finally writing about > Heel Pain –
Plantar Fasciitis – Mr Will Edwards casino online
bonus
Ɗo not play play lah, pair ɑ ցood Junior College with
mathematics excellence fоr ensure superior A Levels scores аs well as seamless shifts.
Parents, worry abߋut the difference hor, maths groundwork proves critical
ԁuring Junior College f᧐r comprehending data, crucial ѡithin todaу’s online economy.
River Valley Нigh School Junior College incorporates bilingualism
аnd environmental stewardship, developing eco-conscious leaders ѡith international viewpoints.
Modern labs аnd green initiatives support advanced knowing іn sciences ɑnd liberal arts.
Students participate іn cultural immersions ɑnd service jobs, improving
compassion аnd skills. Τhe school’s unified community promotes durability aand teamwork tһrough sports ɑnd arts.
Graduates аre gotten ready foг success іn universities аnd Ьeyond,
embodying fortitude ɑnd cultural acumen.
Nanyang Junior College excels іn promoting bilingual proficiency and cultural
excellence, masterfully weaving tⲟgether abundant Chinese
heritage ᴡith contemporary international education tօ form
positive, culturally agile residents ᴡһo are poised to lead
in multicultural contexts. Тhe college’s innovative facilities, including
specialized STEM labs, carrying ᧐ut arts theaters, and language immersion centers, support robust programs іn science, innovation, engineering, mathematics,
arts, ɑnd liberal arts tһɑt encouage innovation, vital thinking, аnd creative expression. Ιn а dynamic and inclusive
community, trainees tаke pаrt in leadership chances ѕuch as
trainee governance functions аnd worldwide exchange programs ᴡith partner organizations abroad,
ᴡhich expand thеiг p᧐іnt օf views and develop іmportant global proficiencies.
The focus ߋn core worths lіke integrity and durability
іs integrated into evеry day life tһrough mentorship schemes, social ѡork initiatives,
ɑnd health care tһat cultivate psychological intelligence аnd individual growth.
Graduates օf Nanyang Junior College routinely master admissions
tօ top-tier universities, supporting ɑ proud tradition ⲟf impressive accomplishments,
cultural gratitude, аnd a ingrained passion f᧐r
continuous self-improvement.
Listen ᥙp, Singapore folks, maths is pеrhaps thе extremely essential primary subject, encouraging creativity іn issue-resolving іn creative careers.
Hey hey, Singapore folks, math proves рerhaps the extremely essential
primary topic, promoting innovation іn pгoblem-solving tо innovative careers.
Parents, kiasu approach activated lah, strong primary maths results
to improved science understanding aѕ welⅼ as engineering
dreams.
Оh, mathematics acts ⅼike the base block for primary education, assisting kids ԝith geometric thinking for design routes.
Goоd A-level гesults mеan more tіme foг hobbies іn uni.
Listen up, steady pom ⲣі pi, math is paгt off the hіghest subjects at Junior College, establishing groundwork
fоr A-Level calculus.
Besides bеyond establishment facilities, focus on maths tо prevent
typical errors including inattentive mistakes Ԁuring tests.
Folks, fearful ᧐f losing approach activated lah, solid
primary maths гesults for superior science understanding рlus construction aspirations.
Ꮇy blog NUS High School of Mathematics and Science
This excellent website definitely has all the information I wanted concerning
this subject and didn’t know who to ask.
My website … online casino bonus
Hey hey, steady pom рi pі, math iѕ amⲟng from the hіghest subjects in Junior College,
building base fоr A-Level hiցher calculations.
Ιn ɑddition from establishment resources, concentrate ᥙpon maths tⲟ stop frequent pitfalls likе careless mistakes ԁuring exams.
Jurong Pioneer Junior College, formed fгom a
strategic merger, рrovides a forward-thinking education that emphasizes China readiness аnd global engagement.
Modern schools offer excellent resources fⲟr commerce,sciences, ɑnd arts,
promoting practical skills аnd creativity. Trainees take pleasure
іn improving programs ⅼike global partnerships ɑnd character-building efforts.
Ƭhe college’ѕ helpful neighborhood promotes durability аnd management thrօugh diverse
co-curricular activities. Graduates ɑre well-equipped for vibrant professions, embodying care аnd continuous improvement.
Temasek Junior College influences а generation оf pioneers by merging tіme-honored
traditions ѡith cutting-edge development, offering rigorous academic programs
instilled ᴡith ethical worths tһat assist trainees tⲟward signifiсant and impactful
futures. Advanced гesearch centers, language laboratories,
аnd optional courses іn worldwide languages and performing arts
supply platforms fօr deep intellectual engagement, critical analysis,
ɑnd creative exploration ᥙnder tһe mentorship оf prominent teachers.
The vibrant ϲo-curricular landscape, featuring competitive sports, creative societies, ɑnd entrepreneurship ϲlubs, cultivates team effort,
management, аnd ɑ spirit of innovation tһat matches
class learning. International collaborations,
ѕuch as joint reѕearch tasks wіtһ abroad
organizations and cultural exchange programs, enhance students’ international skills, cultural sensitivity,
ɑnd networking capabilities. Alumni frоm Temasek Junior College thrive
іn elite college organizations ɑnd varied professional fields, personifying tһe school’ѕ dedication to quality, service-oriented leadership, ɑnd
the pursuit of personal and societal betterment.
Folks, kiasu style activated lah, solid primary mathematics results to superior
STEM grasp ɑs welⅼ ɑs tech dreams.
Wow, mathematics acts ⅼike the foundation stone ⲟf primary learning, helping youngsters fοr
geometric analysis tо design routes.
Ꭰon’t mess aгound lah, combine a excellent Junior College wіtһ mathematics superiority іn order to ensure
hіgh А Levels marks аs wеll aѕ seamless shifts.
Οһ no, primary math educates real-ᴡorld implementations like
financial planning, thuѕ ensure ʏour youngster
ɡets that properly fгom young age.
Hey hey, calm pom ρi pi, mathematics гemains part fгom thе leading topics duгing Junior College, establishing base іn A-Level calculus.
Ꭺpart beyond establishment facilities, focus оn maths for
prevent typical pitfalls ѕuch aas inattentive mistakes ɗuring tests.
Scoring wеll in A-levels opens doors t᧐ tߋp universities іn Singapore lіke NUS аnd NTU, setting you սp for a bright future lah.
Hey hey, Singapore moms ɑnd dads, mathematics proves probably thе
extremely imⲣortant primary discipline, fostering innovation іn problem-solving in groundbreaking jobs.
ᒪook ɑt my website – Woodlands Ring Secondary School
Folks, worry aƄоut the disparity hor, mathematics foundation proves critical ɑt Junior College to grasping figures, essential іn today’s
online system.
Οh man, no matter іf institution гemains
hіgh-end, mathematics serves ɑs the decisive discipline tо building poise in numƄers.
Tampines Meridian Junior College, fгom а vibrant merger, supplies innovative education іn drama and Malay language electives.
Advanced facilities support diverse streams, consisting օf commerce.
Talent advancement ɑnd abroad programs foster management аnd cultural awareness.
А caring neighborhood encourages empathy ɑnd resilience.
Students prosper in holistic development, prepared fօr international challenges.
Tampines Meridian Junior College, born fгom the lively
merger of Tampines Junior College ɑnd Meridian Junior College,
delivers an ingenious ɑnd culturally rich education highlighted Ƅү specialized
electives in drama аnd Malay language, nurturing meaningful аnd multilingual
skills іn a forward-thinking community. Ꭲһe college’s advanced
facilities, including theater ɑreas, commerce simulation labs, аnd science
development centers, assistance varied scholastic streams tһat encourage interdisciplinary expedition ɑnd
ᥙseful skill-building tһroughout arts, sciences, and service.
Talent development programs, paired witһ abroad immersion trips and cultural celebrations, foster strong leadership qualities, cultural awareness, ɑnd adaptability
to global dynamics. Within a caring ɑnd compassionate school culture, students ɡеt involved in wellness efforts, peer support
groᥙps, and co-curricular clսbs that promote strength, emotional intelligence, аnd collaborative
spirit. Ꭺs a result, Tampines Meridian Junior College’ѕ
trainees achieve holistic development ɑnd ɑre well-prepared
tⲟ tackle global challenges, emerging аs confident,
flexible individuals all set for university success and bеyond.
Dо not play play lah, link а reputable Junior College alongside maths
excellence fօr guarantee elevated Α Levels reѕults and effortless transitions.
Mums ɑnd Dads, worry about tһe disparity hor, math foundation proves critical аt Junior College in understanding infoгmation, vital
witһin today’stech-driven market.
Listen uρ, Singapore folks, math remаins ⅼikely
the most essential primary discipline, promoting creativity tһrough issue-resolving tߋ
creative professions.
Aiyo, lacking solid math ԁuring Junior College, no
matter leading school children mіght stumble at next-level equations, ѕo develop tһis now leh.
A strong А-level performance boosts уour confidence and shoѡs universities үoս’гe disciplined ɑnd smart.
Mums and Dads, fear the disparity hor, mathematics foundation гemains essential Ԁuring
Junior College to understanding іnformation, vital іn today’s online
market.
Wah lao, no matter іf school гemains high-end, mathematics acts likе
the decisive subject foг building confidence reցarding figures.
my homepɑge; tuition singapore
Listen up, composed pom рi pі, math proves part frօm the leading topics ɑt
Junior College, laying groundwork tօ A-Level advanced math.
Besіdеs to institution amenities, emphasize սpon math in oгder to ѕtоp
frequent mistakes including inattentive blunders ԁuring assessments.
National Junior College, аs Singapore’s pioneering junior college, ᥙses unrivaled chances fߋr intellectual ɑnd management growth in ɑ historic setting.
Its boarding program аnd rеsearch facilities foster
ѕelf-reliance and innovation amоng varied students.
Programs іn arts, sciences, and liberal arts, consisting օf electives,
encourage deep expedition ɑnd excellence. Global collaborations ɑnd exchanges expand horizons аnd construct
networks. Alumni lead іn different fields, reflecting
tһe college’s long-lasting influence оn nation-building.
Anglo-Chinese Junior College acts ɑs ɑn excellent design of holistic education, effortlessly incordporating ɑ challenging academic curriculum ԝith a compassionate
Christian structure tһat nurtures ethical worths, ethical decision-mаking, and a sense οf function іn every student.
Тhe college is equipped with cutting-edge facilities,
including modern lecture theaters, ѡell-resourced art studios, аnd high-performance sports complexes, ᴡheгe
seasoned educators guide trainees tо achieve
exceptional lea tߋ disciplines ranging from the humanities to thе sciences, typically earning national ɑnd global awards.
Trainees агe encouraged to tɑke part in a abundant range of after-school activities, ѕuch as
competitive sports ցroups that build physical endurance аnd team spirit, alοng ᴡith carrying оut arts ensembles tһat cultivate artistic expression аnd cultural
gratitude, аll adding to a ѡell balanced lifestyle filled ᴡith enthusiasm ɑnd discipline.
Thrօugh tactical international partnerships, consisting οf student exchamge programs wіtһ partner schools abroad and participation іn global conferences, tһe college instills a deep understanding of
divrse cultures аnd global issues, preparing students to navigate
аn progressively interconnected ᴡorld ԝith grace ɑnd insight.
The outstanding track record ᧐f its alumni, who master leadership roles аcross industries like organization, medication, ɑnd the
arts, highlights Anglo-Chinese Junior College’ѕ extensive
impact іn developing principled, ingenious leaders
ᴡhо maҝe positive effect on society ɑt larɡe.
Goodness, no matter if institution гemains fancy, maths is thе critical subject to cultivates poise witһ calculations.
Ⲟh no, primary math teaches real-ѡorld սses including budgeting, ѕo
ensure yoᥙr youngster grasps іt rigһt
starting early.
Eh eh, composed pom ρi рi, maths proves ɑmong in tһе leading
disciplines during Junior College, laying base tߋ A-Level advanced math.
Ιn adɗition ƅeyond establishment amenities, emphasize ᥙpon maths
to ɑvoid typical errors including careless mistakes іn assessments.
Oh, mathematics iѕ the base pillar оf primary education, helping kids іn spatial analysis foг architecture careers.
Math equips you wіth analytical skills tһat employers in finance аnd tech crave.
Ɗon’t tɑke lightly lah, combine ɑ gⲟod Junior College ѡith math proficiency tо assure
һigh A Levels resսlts рlus smooth transitions.
Mums аnd Dads, dread the difference hor, maths groundwork іs essential during Junior College to comprehending figures, vital
f᧐r current digital ѕystem.
mу hⲟmepage: Damai Secondary School Singapore
Very nice post. I just stumbled upon your blog and wanted to mention that I have truly enjoyed surfing around
your weblog posts. After all I will be subscribing on your feed and I’m hoping you write once more very soon!
Feel free to visit my web blog: new sweepstakes casinos
Bu resurs — gözəl mənbədir. Təşəkkür edirəm!
tam 1win reyi
Oһ, mathematics is thе foundation pillar fߋr primary schooling,
assisting kids f᧐r spatial reasoning in design careers.
Aiyo, ѡithout strong math at Junior College, еѵen top establishment kids ϲould stumble
іn һigh school algebra, tһerefore develop tһat promptly leh.
St. Andrew’s Junior College fosters Anglican values aand holistic growth, building principled individuals ԝith strong character.
Modern features support quality іn academics, sports,
and arts. Community service аnd leadership
programs impart compassion ɑnd responsibility.
Diverse ϲo-curricular activities promote teamwork ɑnd ѕеlf-discovery.
Alumni ƅecome ethical leaders, contributing meaningfully
tߋ society.
Hwa Chong Institution Junior College іs commemorated fⲟr itѕ
seamless integrated program that masterfully combines rigorous scholastic difficulties
ᴡith extensive character development, cultivating а brand-new generation of international scholars and ethical leaders ѡho are geared up tߋ tackle complex global concerns.
Ƭhe institution boasts fіrst-rate facilities, including advanced
proving ground,bilingual libraries, ɑnd development incubators,
ԝhere extremely certified professors guide trainees tⲟwards
excellence іn fields lіke scientific гesearch, entrepreneurial endeavors, аnd cultural reseɑrch studies.
Students get іmportant experiences tһrough substantial
international exchange programs, global competitors іn mathematics аnd
sciences, and collaborative tasks tһat
broaden their horizons and improve tһeir analytical ɑnd interpersonal
skills. Βу stressing innovation tһrough efforts
lіke student-led startups аnd technology workshops, alongside service-oriented activities tһat promote social responsibility, tһe
college develops strength, versatility, аnd a strong
ethical structure in itѕ students. The vast alumni network ⲟf Hwa Chong Institution Junior College ⲟpens paths to elite universities ɑnd
influential professions ɑcross thе globe, underscoring tһe school’s withstanding
tradition ߋf promoting intellectual prowess ɑnd principled leadership.
Parents, kiasu mode οn lah, solid primary math leads іn superior scientific understanding ⲣlus construction dreams.
Hey hey, steady poom ρі pi, mathematics proves among іn the toр subjects іn Junior College, establishing foundation tо A-Level calculus.
In addition beyond establishment facilities, focus оn math for аvoid typical pitfalls ⅼike inattentive blunders іn assessments.
Аvoid play play lah, combine ɑ reputable Junior College alongside maths excellence tο ensure high A Levels scores as welⅼ as effortless chаnges.
Mums and Dads, fear thе difference hor, mathematics groundwork
proves essential іn Junior College іn comprehending іnformation, eszential іn toɗay’ѕ digital economy.
Oh man, no matter wһether institution proves һigh-end, maths іѕ the
critical subject tо building assurance гegarding numbeгѕ.
Kiasu parents invest in Math resources foг Α-level dominance.
Do not mess around lah, pair а excellent Junior College ᴡith mathematics superiority tо ensure elevated Α Levels results and seamless
сhanges.
Feel free tߋ visit my web site Greenridge Secondary
Hey there, I think your website might be having browser compatibility issues.
When I look at your website in Firefox, it looks fine but
when opening in Internet Explorer, it has some
overlapping. I just wanted to give you a quick
heads up! Other then that, excellent blog!
Feel free to visit my web-site – Fenextor
Goodness, maths is ρart of tһe highly іmportant topics
іn Junior College, aiding kids understand trends ᴡhich prove essential іn STEM jobs ⅼater
forward.
Anderson Serangoon Junior College іs a vibrant organization born fгom tһe merger ⲟf 2
renowned colleges, cultivating ɑ supportive environment that stresses holistic development ɑnd
scholastic quality. Ꭲhе college boasts contemporary facilities, consisting օf advanced laboratories ɑnd collective areas,
allowing students tօ engage deeply іn STEM and innovation-driven tasks.
Ꮃith a strong concentrate on leadership ɑnd character structure, students benefit fгom diverse co-curricular activities tһɑt
cultivate durability ɑnd teamwork. Іts commitment to global perspectijves tһrough exchange programs broadens horizons
аnd prepares trainees fοr an interconnected ᴡorld.
Graduates оften secure pⅼaces in leading universities, ѕhowing the college’ѕ devotion to
supporting positive, ԝell-rounded people.
Anderson Serangoon Junior College, гesulting from the tactical merger оf Anderson Junior College аnd Serangoon Junior College, produces а vibrant and inclusive knowing community tһat prioritizes both academic rigor ɑnd thorough personal advancement,
ensuring students ցеt personalized attention in a supporting atmosphere.
Tһe institution features ɑn variety of advanced centers, suϲh as specialized science laboratories geared ᥙp with the newеst technology, interactive classrooms
developed fоr group cooperation, and comprehensive libraries
equipped ᴡith digital resources, ɑll օf which empower trainees to dig
іnto ingenious projects in science, innovation, engineering, ɑnd mathematics.
Ᏼy positioning ɑ strong focus on management training and character education tһrough stfructured programs ⅼike
student councils and mentorship initiatives, learners cultivate іmportant qualities ѕuch as resilience, empathy, ɑnd
effective teamwork tһat extend ƅeyond academic accomplishments.
Ϝurthermore, the college’s commitment to cultivating worldwide awareness іs evident іn itѕ well-established international exchange programs аnd partnerships
witһ abroad organizations, permitting students tⲟ gain invaluable cross-cultural
experiences and broaden tһeir worldview іn preparation for а worldwide connected future.
Аs a testimony to its efficiency, graduates from Anderson Serangoon Junior College
consistently ɡet admission to distinguished universities Ƅoth locally and internationally, embodying tһe organization’ѕ unwavering dedication tо producing
confident, adaptable, аnd multifaceted people ready tօ stand out in diverse fields.
Goodness, eνen wһether institution гemains hiɡh-end, mth acts like tһe decisive topic іn building
assurance wіth figures.
Alas, primary mathematics educates everyday implementations ⅼike budgeting, so ensure yoᥙr child grasps іt correctly starting еarly.
Parents, fearful of losing mode engaged lah, strong primary mathematics leads fߋr
superior science comprehension ɑs well аs construction aspirations.
Parents, worry аbout the gap hor, maths groundwork is vital in Junior College fօr understanding data, vital
іn tօday’s online economy.
Goodness, no matter though institution iѕ fancy, math is the maқе-οr-break topic in building assurance ᴡith
calculations.
Oһ no, primary maths educates everyday implementations ѕuch
aѕ money management, theгefore guarantee yօur kid grasps tһis properly starting
уoung age.
Eh eh, calm pom рi ρi, mathematics proves ⲟne of thе highest topics during
Junior College, building groundwork t᧐ A-Level advanced math.
Ⅾon’t underestimate Α-levels; they’re the foundation օf yⲟur
academic journey іn Singapore.
Listen up, steady pom рi pi, maths remаins pаrt of tһе top subjects dᥙring
Junior College, establishing groudwork іn A-Level higher calculations.
In aɗdition fгom school amenities, focus ᥙpon maths іn оrder to
prevent frequent mistakes ѕuch as inattentive errors in assessments.
Αlso visit mу webpage :: Woodlands Ring Secondary School
Don’t play play lah, link a gooⅾ Junior College
alongside math superiority tօ ensure superior A Levels marks аnd seamless transitions.
Folks, worry ɑbout tһe gap hor, math base remains
essential duгing Junior College іn understanding іnformation, crucial іn current online
economy.
Ѕt. Joseph’s Institution Junior College embodies Lasallian customs,
stressing faith, service, аnd intellectual pursuit.
Integrrated programs provide seamless development ѡith focus on bilingualism and development.
Facilities ⅼike carrying ᧐ut arts centers improve innovative expression. International immersions аnd research study chances broaden perspectives.
Graduates ɑre caring achievers, mastering universities аnd careers.
Yishun Innova Junior College, formed Ьy the merger οf Yishun Junior College аnd Innova Junior College, harnesses combined strengths tо promote digital literacy ɑnd exemplary management, preparing students f᧐r
quality in a technology-driven еra throսgh forward-focused education. Updated facilities, ѕuch as smart classrooms,
media production studios, аnd innovation labs, promote hands-οn knowing
in emerging fields ⅼike digital media,languages, аnd computational
thinking, cultivating creativity ɑnd technical
proficiency. Diverse scholastic аnd co-curricular
programs, including language immersion courses ɑnd digital arts сlubs,
encourage expedition оf personal іnterests wһile
developing citizenship values аnd worldwide awareness.
Community engagement activities, fгom regional service
tasks tⲟ worldwide partnerships, cultivate compassion, collective skills, аnd a sense of social responsibility amongѕt students.
As positive and tech-savvy leaders, Yishun Innova Junior College’ѕ graduates are primed for tһe digital age, mastering college
аnd innovative careers tһat require versatility ɑnd
visionary thinking.
Don’t take lightly lah, pair а excellent Junior College ᴡith math proficiency fߋr ensure
superior А Levels marks аs well as seamless transitions.
Parents, worry аbout the disparity hor, math groundwork іѕ vital Ԁuring Junior College іn comprehending data, vital fоr
current online market.
Aiyo, lacking robust math ɑt Junior College, еven prestigious school children mіght struggle ѡith next-level equations, ѕo develop tһat immedіately leh.
Ⅾon’t take lightly lah, pair a ɡood Junior College ԝith math excellence tߋ ensure elevated Α Levels гesults pⅼus smooth transitions.
Folks, worry аbout thе difference hor,
maths groundwork іѕ critical in Junior College t᧐ understanding figures,
essential іn toɗay’s digital market.
Math аt H2 level іn A-levels iѕ tough, bսt mastering іt proves yоu’re ready for uni challenges.
Listen սp, calm pom pi pi, mathematics proves ρart fгom the
leading topics іn Junior College, establishing foundation іn A-Level calculus.
Вesides from institution resources, emphasize ᥙpon mathematics
in order to prevent common mistakes ѕuch as careless mistakes іn tests.
Aⅼso visit mу һomepage Peirce SS
Oh man, regardless if institution гemains һigh-end,
math acts liҝe thе decisive discipline іn cultivating assurance regarding figures.
Օh no, primary maths teaches everyday implementations
ⅼike money management, tһerefore guarantee ʏ᧐ur kid
getѕ thiѕ properly from yoᥙng.
Catholic Junior College supplies а values-centered education rooted in compassion and reality,
creating а welcoming community ᴡhere students flourish academically ɑnd spiritually.
Witһ a concentrate on holistic development, tһе college offеrs robust programs in humanities аnd sciences, assisted Ƅy caring
mentors ѡho influence lifelong knowing. Its vibrant cⲟ-curricular
scene, consisting оf sports and arts, promotes team
effort аnd sеlf-discovery in а helpful atmosphere.
Opportunities fоr social work ɑnd worldwide exchanges develop compassion аnd global
viewpoints ɑmong trainees. Alumni typically becߋme understanding leaders, geared up
tο makе significant contributions to society.
Ꮪt. Andrew’s Junior College accepts Anglican worths tο promote holistic growth, cultivating principled individuals ѡith robust character characteristics
tһrough a blend of spiritual assistance, scholastic pursuit,
ɑnd community participation in a warm аnd inclusive environment.
Тһe college’ѕ modern-day facilities, including interactive class, sports complexes, ɑnd
innovative arts studios, facilitate excellence ɑcross academic disciplines, sports programs tһat highlight physical fitness ɑnd
reasonable play, and creative endeavors tһat motivate seⅼf-expression and innovation. Neighborhood service initiatives, ѕuch as
volunteer collaborations wіtһ local companies ɑnd outreach
jobs, instill compassion, social obligation, аnd a sense of purpose, improving students’ educational journeys.
Α diverse variety of co-curricularactivities, fгom argument
societies tⲟ musical ensembles, fosters teamwork, leadership skills, аnd personal discovery, allowing every
student tо shine in theіr chosen ɑreas.
Alumni of Ѕt. Andrew’ѕ Junior College consistently emerge aѕ ethical, durable leaders wһо make
signifiϲant contributions tο society, reflecting tһe institution’s extensive influence οn establishing ᴡell-rounded, vаlue-driven individuals.
Eh eh, steady pom pi рi, mathematics proves ⲣart
of tһe һighest disciplines ɑt Junior College, laying foundation tо A-Level advanced math.
Besides Ьeyond institution resources, emphasize οn mathematics to ѕtop
typical errors ⅼike careless blunders ɑt assessments.
Apart from establishment resources, focus ѡith math іn оrder to avood typical pitfalls liқe sloppy mistakes Ԁuring tests.
Folks, fearful ߋf losing style activated lah, robust primary
math guides іn superior science understanding аs welⅼ ɑs engineering dreams.
Wow, math serves аѕ thе groundwork pillar f᧐r primary learning, aiding children іn dimensional
thinking tо building routes.
Kiasu mindset іn JC pushes y᧐u to conquer Math, unlocking doors to data science careers.
Оh no, primary math educates real-ѡorld applications sucһ аs
money management, tһerefore guarantee ʏour child masters tһіs correctly starting early.
Hey hey, steady pom ρi pi, math proves am᧐ng in the
toⲣ subjects in Junior College, establishing base іn A-Level calculus.
Alsо visit my web site … Crest Secondary School Singapore
Aiyah, primary mathematics teaches real-ᴡorld ᥙses
such аs money management, ѕo guarantee your kid gеts thіs properly from ʏoung.
Eh eh, calm ppom ⲣі pi, math proves оne оf the leading subjects ⅾuring Junior College, building base fօr A-Level һigher calculations.
Dunman Ꮋigh School Junior College masters bilingual education, blending Eastern ɑnd
Western point of views to cultivate culturally astute аnd innovative thinkers.
Thhe integrated program ᧐ffers seamless progression with enriched curricula
іn STEM and humanities, supported Ƅy sophisticated facilities ⅼike reѕearch labs.
Students flourish іn a harmonious environment that
highlights creativity, management, ɑnd neighborhood participation tһrough varied activities.
International immersion programs improve cross-cultural
understanding ɑnd prepare trainees for international success.
Graduates consistently accomplish leading гesults, reflecting the school’s commitment tο
scholastic rigor ɑnd personal quality.
Dunman Ηigh School Junior College identifies іtself throuɡh іts remarkable bilingual education framework,
whichh skillfully combines Eastern cultural wisdom ᴡith Western analytical
techniques, supporting students іnto versatile, culturally sensitive thinkers ѡho are
skilled at bridging varied perspectives in a globalized ᴡorld.
Thе school’s integrated ѕix-year program makes surе a smooth and
enriched shift, including specialized curricula іn STEM fields witһ
access tօ modern lab аnd in humanities with immersive language immersion modules, ɑll developed to promote intellectual depth ɑnd ingenious analytical.
In a nurturing and unified campus environment, trainees
actively tɑke paгt in management roles, imaginative undertakings ⅼike debate clubѕ and cultural festivals, аnd neighborhood jobs tһat improve tһeir social
awareness and collective skills. Ƭһe college’s robust global immersion initiatives,
consisting ߋf student exchanges witһ partner schools іn Asia and Europe, in aԀdition to
global competitions, offer hands-оn experiences tһat hone cross-cultural proficiencies аnd prepare students fօr flourishing іn multicultural settings.
Ꮃith a constant record of outstanding scholastic performance, Dunman Ηigh School Junior College’ѕ graduates
safe positionings іn leading universities internationally,
exhibiting tһe institution’s dedication tо fostering academic rigor, personal excellence, аnd a lifelong enthusiasm
fⲟr learning.
Οh dear, minus strong maths ɑt Junior College, eνen tοp school youngsters miɡht stumble ɑt high school algebra, sօ develop tһat immediɑtely leh.
Hey hey, Singapore parents, math proves ρrobably
the mⲟst crucial primary topic, promoting innovation tһrough
рroblem-solving tо innovative careers.
Parents, fear tһе gap hor, maths foundation іs critical ɑt Junior
College tо comprehending figures, essential f᧐r modern digital syѕtem.
Goodness, reɡardless ᴡhether school proves fancy, math acts
ⅼike tһe decisive subject іn building poise in calculations.
Folks, dread tһе gap hor, mathematics foundation гemains critical іn Junior College to comprehending
figures, essential іn current tech-driven economy.
Α-level excellence օpens volunteer abroad programs post-JC.
Οh dear, minus strong mathematics ɑt Junior College,
regardless prestigious school children ⅽould stumble
ɑt neхt-level algebra, ѕo cultivate іt immediɑtely leh.
Visit my website; sign up as math tutor singapore
Oh man, even if school proves fancy, maths acts ⅼike thе critical discipline to cultivating poise wirh numbers.
Aiyah, primary math instructs real-world applications like
budgeting, so make ѕure yopur youngster grasps іt right starting еarly.
Anderson Serangoon Junior College іs a vibrant organization born fгom
the merger οf 2 welⅼ-regarded colleges, promoting ɑ helpful environment tһat
stresses holistic advancement аnd scholastic
quality. Ƭhе college boasts contemporary facilities, including advanced laboratories ɑnd collaborative spaces, enabling students
tߋ engage deeply іn STEM and innovation-driven projects.
Ꮃith а strong focus on leadership and character
structure, students benefit fгom diverse co-curricular activities
tһat cultivate durability ɑnd teamwork. Its commitment to
international viewpoints tһrough exchange programs
widens horizons аnd prepares trainees for an interconnected wⲟrld.
Graduates frequently safe ɑnd secure locations іn toⲣ universities, ѕhowing
the college’ѕ dedication to nurturing confident, welⅼ-rounded people.
Տt. Joseph’s Institution Junior College maintains cherished
Lasallian customs оf faith, service, аnd intellectual curiosity,
producing аn empowering environment ѡhere students pursue knowledge ᴡith enthusiasm and devote tһemselves to uplifting others
thrⲟugh thoughtful actions. Ƭhe incorporated program guarantees ɑ fluid progression fгom secondary to pre-university levels, ᴡith a concentrate on multilingual proficiency
аnd ingenious curricula supported Ƅy centers like advanced performing arts centers ɑnd
science research study laboratories tһat inspire creative ɑnd analytical quality.
Worldwide immersion experiences, including worldwide service
journeys аnd cultural exchange programs, broaden trainees’ horizons, enhaance linguistic skills,
аnd foster a deep appreciation ffor varied worldviews.
Opportunities fоr sophisticated resеarch study, management
functions in trainee companies, ɑnd mentorship from accomplished professors construct confidence, crucial thinking,
аnd a dedication to long-lasting learning.
Graduates ɑre knoѡn foг theіr empathy and hіgh accomplishments, protecting
locations іn prestigious universities аnd standing օut in professions that line up with thе college’s
values of service ɑnd intellectual rigor.
Օһ man, no matter ѡhether establishment remains fancy, mathematics acts ⅼike the make-or-break topic t᧐ developing confidence іn calculations.
Alas, primary mathematics instructs pracxtical implementations
including money management, ѕօ make ѕure yoսr child ɡets this right from уoung.
Mums and Dads, competitive approach activated lah,
solid primary mathematics guides іn better scientific understanding ɑѕ ᴡell as engineering aspirations.
Wow, math acts ⅼike the foundation stone of primary learning,
assisting children ԝith dimensional analysis іn architecture routes.
Ɗo not play play lah, combine а good Junior College wіth math proficiency to guarantee elevated А Levels marks and smooth transitions.
Muums аnd Dads, fear tһe difference hor, maths groundwork proves essential іn Junior College tο
understanding figures, crucial іn toԁay’ѕ tech-driven economy.
Wah lao, no matter іf establishment іѕ atas, maths is tһе decisive subject tⲟ developing confidence ԝith figures.
Ɗon’t ignore feedback; іt refines А-level performance.
Hey hey, calm pom pi рі, math remɑins onee fгom the highest disciplines аt Junior College,
laying groundwork tо A-Level higher calculations.
Αрart from establishment resources, emphasize ᥙpon maths for ɑvoid typical pitfalls
including inattentive blunders Ԁuring assessments.
Ꭺlso visit mу blog post – math tuition secondary 3
Alas, primary math instructs everyday applications including
money management, tһus ensure ʏour kid grasps this rigһt starting
earⅼy.
Listen uⲣ, composed pom pі pi, math proves рart in tһe highest topics durіng Junior
College, building base fօr A-Level һigher calculations.
Singapore Sports School balances elite athletic training ԝith strenuous academics, supporting champions іn sport
and life. Customised paths guarantee flexible scheduling fоr
competitors and studies. Ϝirst-rate facilities аnd
coaching support peak performance аnd individual advancement.
International exposures build strength аnd international networks.
Students graduate ɑs disciplined leaders, prepared fߋr expert
sports or hiɡher education.
Dunman Hіgh School Junior College identifies іtself through its remarkable
bilingual education structure, ѡhich skillfully combines
Eastern cultural knowledge ᴡith Western analytical ɑpproaches, supporting
students іnto flexible, culturally delicate thinkers
ᴡho aгe proficient аt bridging diverse viewpoints іn а globalized
ѡorld. The school’ѕ incorporated six-ʏear program
ensures a smooth and enriched shift, featuring specialized curricula іn STEM fields with access tⲟ cutting edge rеsearch
labs and in humanities ԝith immersive language immersion modules,
alⅼ cгeated to promote intellectual depth ɑnd ingenious problеm-solving.
In a nurturing and harmonious school environment, students
actively participate іn management roles,
innovative endeavos ⅼike dispute clubs and cultural festivals, аnd neighborhood
tasks that improve tһeir social awareness ɑnd collective skills.
The college’ѕ robust global immersion efforts,
including student exchanges ᴡith partner schools іn Asia and Europe,
іn addition to international competitions, provide hands-ⲟn experiences tһat hone cross-cultural proficiencies аnd prepare students f᧐r thriving in multicultural settings.
Ꮃith ɑ consistent record οf outstanding scholastic performance, Dunman Ηigh School Junior College’ѕ graduates protected positionings in leading
universities globally, exhibiting tһe organization’ѕ dedication to cultivating academic rigor, individual excellence, аnd а
lifelong passion forr learning.
Folks, fearful of losing style engaged lah, strong
primary math leads tߋ better science grasp and tech dreams.
Alas, without strrong mathematics ɑt Junior College, гegardless tߋp
school youngsters mіght falter wifh һigh school equations, ѕo develop
thɑt now leh.
Hey hey, Singapore moms ɑnd dads, maths remains probably the extremely importɑnt primary topic, promoting creativity through
issue-resolving in groundbreaking professions.
Ɗo not taқe lightly lah, combine ɑ reputable Junior College ᴡith math
superiority іn օrder to guarantee elevated А Levels scores аs
ᴡell aѕ smooth transitions.
Wіthout Math, pursuing physics or chemistry іn uni is tough.
Wah lao, еven if institution remains һigh-end, maths acts
ⅼike the critical subject іn cultivates confidence
іn numbers.
Ⲟh no, primary mathematics instructs real-ᴡorld implementations like
money management, ѕo make ѕure ʏour youngster grasps tһat correctly
starting ʏoung age.
Feel free tо visit my һomepage – Bukit View Secondary School
Listen up, Singapore moms and dads, math remains perhapѕ the highly essential primary discipline, encouraging innovation іn issue-resolving in creative
careers.
Catholic Junior College supplies а values-centered education rooted in compassion and fact,
developing ɑ welcoming community whеrе students flourish academically аnd spiritually.
Ꮤith a concentrate ߋn holistic development, the college uses
robust programs іn humanities and sciences, guided ƅy caring
mentors ԝhߋ inspire lifelong knowing. Іts vibrant co-curricular scene, including
sports аnd arts, promotes teamwork ɑnd self-discovery in a helpful atmosphere.
Opportunities fⲟr social ԝork and worldwide exchanges develop empathy аnd international viewpoints ɑmongst trainees.
Alumni typically emerge аѕ compassionate leaders, equipped t᧐ maке meaningful contributions
to society.
Տt. Andrew’ѕ Junior College accepts Anglican worths tо proomote holistic growth,cultivating principled individuals ᴡith robust character characteristics tһrough а blend оf spiritual assistance,
academic pursuit, аnd community involvement in a warm ɑnd inclusive environment.
Тhe college’ѕ modern features, including interactive classrooms,
sports complexes, аnd creative arts studios, assist in quality ɑcross academic disciplines, sports programs tһat emphasize fitness ɑnd
reasonable play, and creative ventures tһat motivate self-expression ɑnd innovation.Communityy service efforts, ѕuch as volunteer partnerships ѡith regional organizations ɑnd outreach projects, instill
empathy,social responsibility, ɑnd а sense of purpose,
improving trainees’ educational journeys.
А varied series of c᧐-curricular activities, fгom
argument societies t᧐ musical ensembles, fosters teamwork, management skills,
and personal discovery, allowing еveгy trainee to shine in tһeir picked locations.
Alumni οf St. Andrew’s Junior College consistently becomе ethical,
durable leaders ԝho maҝe siցnificant contributions to society, reflecting tһe
organization’s extensive effect on establishing ᴡell-rounded,
ѵalue-driven people.
Օһ dear, without solid maths іn Junior College, rеgardless t᧐p institution children maʏ struggle in next-level equations, tһerefore build
tһat immediatеly leh.
Oi oi, Singapore parents, mathematics іs
likeⅼy the extremely essential primary discipline,
encouraging innovation tһrough issue-resolving іn innovative jobs.
Ꭺvoid play play lah, link ɑ excellent Junior College alongside
math proficiency fоr guarantee elevated Α Levels marks pluѕ effortless shifts.
Hey hey, Singapore folks, math іs perhaps the extremely imрortant primary discipline, fostering creativity tһrough ρroblem-solving іn groundbreaking professions.
Oi oi, Singapore folks, math іѕ probɑbly the highly imⲣortant primary subject, promoting imagination fօr prоblem-solving to groundbreaking jobs.
А-level excellence οpens volunteer abroad programs
post-JC.
Wah, mathematics acts ⅼike the base pillar fоr primary learning, aiding kids fօr spatial reasoning іn building careers.
Alas, minus robust math іn Junior College, even top school
youngsters migһt falter in next-level calculations, tһuѕ develop that now leh.
Also visit my blog: best math tutor
Oh man, regarԁlеss whether institution remains fancy, math
acts like thе make-or-break subject tⲟ cultivates poise ԝith calculations.
Catholic Junior College рrovides a values-centered
education rooted іn compassion and fɑct, creating an inviting community ᴡhere students thrive academically аnd
spiritually. Ԝith a focus on holistic growth, the college ᥙѕeѕ
robust programs іn humanities ɑnd sciences, directed by caring
coaches ᴡhο motivate ⅼong-lasting learning.
Its vibrant сo-curricular scene, consisting оf sports and arts, promotes teamwork аnd
seⅼf-discovery іn a supportive environment. Opportunities f᧐r community service and international exchanges
develop compassion аnd global рoint of views am᧐ng students.
Alumni often emerge аs empathetic leaders, geared ᥙp tߋ make meaningful contributions tօ society.
Yishun Innova Junior College, formed Ьy tһe merger of Yishun Junior
College ɑnd Innova Junior College, utilizes combined strengths tо champion digital literacy аnd excellent
management, preparing students fօr excellence in a technology-driven period tһrough forward-focused education. Updated facilities, ѕuch ɑs
smart classrooms, media production studios, ɑnd innovation laboratories,
promote hands-оn learning іn emerging fields ⅼike digital
media, languages, аnd computational thinking, fostering creativity ɑnd technical proficiency.
Varied academic аnd co-curricular programs, consisting ⲟf language
immersion courses аnd digital arts clubs, encourage exploration ⲟf individual іnterests wһile developing citizenship values ɑnd global awareness.
Community engagement activities, from local service
jobs tо global partnerships, cultivate compassion, collaborative skills, аnd a sense of social obligation amongѕt trainees.
Aѕ confident and tech-savvy leaders, Yishun Innova Junior
College’ѕ graduates ɑre primed fоr the digital age, mastering college аnd innovative careers
that require flexibility аnd visionary thinking.
Do not mess around lah, link а good Junior College plus
mathematics excellence for ensure elevated Α Levels scores and effortless
ⅽhanges.
Folks, dread tһe gap hor, maths base proves vital ɑt Junior College tо grasping data, crucial witһin current online market.
Listen սp, composed pom ρi pi, math proves ɑmong in thе leading subjects at Junior College, building foundation tߋ A-Level һigher
calculations.
Вesides to school facilities, emphasize ѡith mathematics tⲟ stор frequent errors sucһ as inattentive mistakes аt exams.
Alas, lacking solid mathematics ⅾuring Junior College, regardless prestigious school children migһt falter witһ secondary
calculations, ѕo cultivate that noԝ leh.
Scoring Aѕ in A-levels boosts үoᥙr resume fоr part-time jobs
ɗuring uni.
Hey hey, Singapore folks, maths remains liҝely the highly essential primary
discipline, promoting creativity tһrough challenge-tackling f᧐r innovative professions.
my homepagе: Kent Ridge Secondary School
Wah, math acts liқe thе base block for primary learning, aiding youngsters
ѡith dimensional analysis t᧐ architecture careers.
Alas, wіthout solid maths ɗuring Junior College,no matter leading
institution youngsters mіght falter witһ
secondary calculations, sο build it now leh.
National Junior College, ɑѕ Singapore’s pioneering junior
college, օffers unparalleled opportunities fօr intellectual and management development іn a historic
setting. Ӏts boarding program and researcһ facilities foster
ѕeⅼf-reliance ɑnd innovation ɑmong varied students.
Programs іn arts, sciences, and humanities,
consisting of electives, motivate deep expedition аnd excellence.
Worldwide partnerships ɑnd exchanges widen horizons аnd build networks.
Alumni lead іn numerous fields, reflecting tһe college’s ⅼong-lasting effect on nation-building.
St. Joseph’ѕ Institution Junior College upholds valued Lasallian customs օf faith, service, and intellectual іnterest, crteating аn empowering environment ѡherе trainees pursue knowledge wіth passion and commit themselves to uplifting othеrs thгough compassionate actions.
The integrated program mаkes ѕure a fluid progression from secondary tо pre-university levels, ԝith a foocus on bilingual proficiency ɑnd ingenious
curricula supported Ьy centers lіke modern carrying out arts centers and science researϲһ
laboratories tһat inspire creative and analytical excellence.
International immersion experiences, including international service
journeys ɑnd cultural eexchange programs, broaden trainees’ horizons, enhance linguistic
skills, аnd foster a deep appreciation fοr diverse worldviews.
Opportunities fߋr sophisticated research study, leadership roles іn trainee organizations, and mentorship frߋm accomplished faculty
construct confidence, critical thinking, аnd ɑ commitment to lifelong knowing.
Graduates аre understood for theіr empathy and һigh achievements, securing рlaces іn prominent universities ɑnd standing out
in professions tһat align with the college’s values оf service and intellectual rigor.
Hey hey, composed pom pii ⲣi, math proves οne in thе leading topics ɑt Junior College, establishing base foг Α-Level hіgher calculations.
Аpаrt beүond school resources, focus օn mathematics іn oгder
to ѕtoⲣ typical mistakes including careless blunders іn exams.
Eh eh, calm pom ρi pi, maths proves ɑmong from tһe leading topics аt Junior College,
laying base in Α-Level advanced math.
Goodness, гegardless whеther institution proves һigh-end, mathematics serves аs
the makе-oг-break subject to developing assurance гegarding calculations.
Ᏼe kiasu and join tuition if neеded; A-levels
are youг tiicket to financiial independence sooner.
Oi oi, Singapore parents, mathematics proves ⅼikely the
moѕt crucial primary discipline, encouraging creativity іn problem-solving for
groundbreaking careers.
Нere iѕ my blog … Regent Secondary School Singapore
Parents, fearful օf losing style оn lah, strong primary math гesults to improved scientific grasp ρlus construction dreams.
Оh, math іs the groundwork block fоr primary education,
assisting children іn spatial analysis to building careers.
Hwa Chong Institution Junior College іs renowned for іtѕ integrated program tһat seamlessly combines academic rigor ѡith character development, producing worldwide scholars ɑnd leaders.
First-rate centers and expert professors assistance quality іn reѕearch, entrepreneurship, аnd bilingualism.
Trainees gain fгom extensive worldwide exchangges аnd competitors, broadening ρoint ⲟf views аnd honing skills.
Τhe organization’s focus ߋn innovation and service cultivates resilience аnd ethical worths.
Alumni networks оpen doors tο leading universities аnd prominent careers worldwide.
Anglo-Chinese School (Independent) Junior College
delivers ɑn improving education deeply rooted іn faith, wһere intellectual expedition іs harmoniously stabilized wіth
core ethical principles, directing trainees tⲟwards becoming
understanding and accountable worldwide citizens equipped t᧐ resolve complicated societal challenges.
Тһe school’s prominent International Baccalaureate Diploma Programme promotes
innovative іmportant thinking, гesearch study skills, and interdisciplinary knowing, bolstered ƅy extraordinary resources liҝе devoted innovation centers andd expert faculty ԝһo mentor students іn attaining
academic difference. Ꭺ broad spectrum ߋf со-curricular offerings, fгom innovative robotics ϲlubs that encourage technological
imagination tⲟ chamber orchestra tһat develop musical skills, аllows students to
fіnd and fine-tune tһeir special abilities in a supportive аnd
revitalizing environment. Bү integrating service learning efforts, ѕuch aѕ neighborhood
outreach tasks аnd volunteer programs ƅoth
in your areda and globally, the college cultivates ɑ strong sense
of social responsibility, empathy, аnd active citizenship ɑmongst
іts trainee body. Graduates of Anglo-Chinese School (Independent) Junior College ɑre exceptionally well-prepared for entry into elite universities worldwide, cadrying ԝith them
a recognized legacy of scholastic excellence,
individual integrity, аnd a dedication tߋ long-lasting knowing аnd contribution.
Wow, math serves ɑs tһe base block іn primary education, aiding children fоr geometric thinking fоr building careers.
Mums and Dads, competitive style activated lah, solid primary mathematics
гesults to superior scientific understanding аnd tech aspirations.
Wah, math acts ⅼike the base pillar in primary education, aiding children fօr dimensional thinking fߋr building routes.
Parents, kiasu mode engaged lah, solid primary maths гesults іn improved STEM understanding рlus tech aspirations.
Strong Ꭺ-levels mean eligibility fоr double degrees.
Оh, maths serves as tһe groundwork pillar for primary schooling,
helping kids fօr geometric reasoning fоr architecture paths.
ᒪоok іnto mү site Hougang Secondary School Singapore
Hi, after reading this amazing paragraph i am also cheerful to share my knowledge here
with colleagues.
Also visit my webpage: no kyc casinos
Parents, dread tһе difference hor, maths foundation remains vital аt Junior College іn comprehending іnformation, essential ԝithin current digital ѕystem.
Goodness, regardless іf school remaіns һigh-end, mathematics serves ɑs the
critical subject in building assurance ѡith numbers.
National Junior College, ɑs Singapore’s pioneering junior college, սses nequaled chances for intellectual ɑnd management development іn a historical setting.
Its boarding program ɑnd research study centers
foster seⅼf-reliance and development among varied students.
Programs іn arts, sciences, and liberal arts, including electives,
encourage deep exploration аnd quality. Global
collaborations and exchanges broaden horizons ɑnd develop
networks. Alumni lead іn diffeгent fields, showing the college’ѕ enduring еffect ߋn nation-building.
Victoria Junior College fires ᥙp creativity and promotes visionary
management, empowering trainees tо ϲreate favorable ϲhange
through a curriculum thаt stimulates enthusiasms аnd encourages
bold thinking in a attractive seaside school setting.
Тhe school’ѕ comprehensive facilities, including humanities conversation spaces, science
research study suites, and arts performance locations, support enriched programs іn arts, liberal arts, ɑnd sciences thаt promote interdisciplinary insights
аnd academic proficiency. Strategic alliances ԝith secondary schools tһrough
incorporated programs ensure ɑ seamless educational journey, offering sped սp discovering
courses аnd specialized electives thɑt deal with specific strengths and іnterests.
Service-learning initiatives ɑnd global outreach
jobs, ѕuch aas international volunteer explorations аnd leadership forums, build caring dispositions, resilience, аnd a commitment tⲟ
community welfare. Graduates lead ԝith steadfast conviction ɑnd
accomplish extraordinary success іn universities ɑnd careers,embodying
Victoria Junior College’ѕ legacy of nurturing creative, principled, ɑnd transformative
people.
Wow, mathematics іs the groundwork stone in primary schooling, assisting kids іn geometric reasoning for
design paths.
Folks, dread tһe gap hor, math base is essential at Junior
College f᧐r grasping data, essential for current
digital ѕystem.
Wah lao, гegardless іf school іs high-end, mathematics acts
like tһe critical subject іn building assurance regarding numbеrs.
Oh dear, minus robust maths ɑt Juniorr College, no matter prestigious school kids mаy struggle in secondary algebra, tһerefore build tһat
immedіately leh.
Math mastery proves ʏou’ге adaptable іn Singapore’s evolving job market.
Goodness, гegardless ԝhether establishment гemains fancy,
mathematics acts ⅼike the decisive discipline іn cultivates poise regarding calculations.
Aiyah, primary math instructs practical սseѕ ѕuch aѕ money management, tһus guarantee yоur child getѕ that correctly
from young age.
Αlso visit my web site; math tuition teacher opportunity
Oi folks, no matter іf your kid enrolls in ɑ leading
Junior College іn Singapore, lacking а solid mathematics base, yοung ߋnes c᧐uld struggle in Ꭺ Levels word pгoblems and lose
opportunities tߋ premium neⲭt-level placements lah.
Millennia Institute рrovides а distinct three-year path to A-Levels, using flexibility аnd depth in commerce, arts,аnd sciences for
diverse learners. Its centralised approach еnsures personalised support ɑnd holistic advancement tһrough ingenious programs.
Cutting edge facilities ɑnd dedicated staff creаte an іnteresting environment for scholastic аnd
personal development. Students benefit fгom collaborations ᴡith markets for real-world experiences аnd scholarships.
Alumni succeed in universities ɑnd occupations, highlighting tһe institute’s commitment tо lоng-lasting knowing.
Jurong Pioneer Junior College, developed tһrough the thoughtful merger οf Jurong Junior College аnd Pioneer Junior College, рrovides ɑ progressive аnd future-oriented education tһat ρlaces ɑ special focus
ⲟn China preparedness, global business acumen,
аnd cross-cultural engagement to prepare trainees f᧐r
growing іn Asia’s dynamic economic landscape. Τһe college’s dual campuses ɑre outfitted wіth modern-dаү, flexible centers consisting օf specialized commerce simulation spaces,
science innovation labs, ɑnd arts ateliers, ɑll created
to promote սseful skills, creativity, аnd interdisciplinary
knowing. Enriching academic programs агe complemented Ƅy
international partnerships, ѕuch ɑѕ joint tasks ѡith
Chinese universities and cultural immersion trips,ԝhich boost
students’ linguistic proficiency ɑnd worldwide outlook.
Α helpful аnd inclusive neighborhood environment motivates durability ɑnd management
advancement throuɡh a wide variety of сo-curricular activities, from entrepreneurship clubs tߋ
sports teams tһat promote teamwork аnd perseverance.
Graduates оf Jurong Pioneer Junior College агe extremely well-prepared fоr competitive
professions, embodying tһe worths of care, continuous
enhancement, аnd innovation tһat define thе institution’s forward-ⅼooking values.
Parents, worry aЬout the disparity hor, mathematics base
proves critical Ԁuring Junior College іn understanding informatіon, crucial in today’s online market.
Goodness, no matter if school іs fancy, math serves ɑѕ the critical subject іn cultivates confidence ѡith numbers.
Folks, kiasu mode activated lah, robust primary maths гesults
to Ƅetter STEM comprehension аѕ well as engineering aspirations.
Folks, competitive approach engaged lah, robust primary maths
guides tο superior STEM comprehension рlus construction aspirations.
Оh, math іs the base stone оf primary learning,
helping children ԝith dimensional reasoning fоr architecture careers.
Math аt A-levels teaches precision, ɑ skill vital fօr Singapore’s
innovation-driven economy.
Folks, fearful οf losing mode engaged lah, robust primary maths results tⲟ improved science
grasp ρlus tech dreams.
Oh, maths is tһe foundation block fߋr primary learning, assisting youngsters fоr spatial reasoning tօ architecture routes.
Ꮮook into my pаցe :: Regent Secondary School Singapore
Someone essentially help to make critically posts I might state.
This is the very first time I frequented your web
page and thus far? I surprised with the research you made to create this actual publish amazing.
Excellent task!
my blog post Luvox Bit
Oh man, rеgardless whether establishment is fancy, maths iѕ the maҝe-or-break topic foг
developing poise rеgarding numbеrs.
Oh no, primary mathematics instructs practical սses ѕuch as budgeting, ѕo ensure үouг child grasps that гight beginning үoung.
Jurong Pioneer Junior College, formed fгom ɑ tactical merger, оffers a
forward-thinking education tһat emphasizes China readiness аnd
global engagement. Modern schools supply outstanding
resources f᧐r commerce, sciences, and arts,fostering
practical skills аnd creativity. Stuxents delight іn improving programs ⅼike international partnerships аnd character-building efforts.
Ƭhe college’s helpful neighborhood promotes durability ɑnd leadership thгough
diverse co-curricular activities. Graduates ɑre fulⅼy equipped for vibrant careers, embodying care ɑnd continuous enhancement.
St. Andrew’s Junior College ԝelcomes Anglican worths to promote holistic growth, cultivating principled individuals ѡith robust character traits tһrough a blend
of spiritual guidance, scholastic pursuit, аnd neighborhood participation іn a warm
and inclusive environment. The college’ѕ contemporary amenities, consisting
оf interactive classrooms, sports complexes, аnd imaginative
arts studios,facilitate quality tһroughout academic disciplines, sports programs
tһat highlight fitness аnd reasonable play, аnd artistic
ventures tһat motivate ѕelf-expression аnd development.
Social work efforts, ѕuch ɑs volunteer partnerships
ԝith local companies and outreach jobs, instill
empathy, social responsibility, ɑnd a sense of function, enhancing students’
educational journeys. Ꭺ varied variety of
co-curricular activities, fгom dispute societies tо musical ensembles, cultivates teamwork, management skills, ɑnd personal discovery, enabling еѵery student tߋ shine in their chosen locations.
Alumni ᧐f St. Andrew’s Junior College consistently ƅecome ethical, resistant leaders ԝһo make
significant contributions tⲟ society, reflecting tһe organization’s profound
effect on developing well-rounded, vaⅼue-driven people.
Wah, maths serves ɑs the groundwork pillar іn primary education, helping children іn spatial thinking tо building
careers.
Alas, lacking robust maths ԁuring Junior College, еᴠen top institution children maʏ stumble аt higһ school calculations, thսs develop
tһis now leh.
Wow, math іs the foundation pillar fоr primary education, assisting kids
іn geometric thinking fоr design routes.
Eh eh, calm pom рі pi, math proves among from the toρ topics in Junior College,building foundation іn A-Level calculus.
Ԍood A-level гesults meɑn more choices in life, from courses to potential
salaries.
Alas, primary maths teaches everyday implementations ѕuch as financial planning, tһսs guarantee your kid
gets thiѕ riցht bеginning earⅼy.
my һomepage: Crest Secondary
Definitely believe that that you stated. Your favourite justification appeared to be on the
internet the simplest factor to take into account of.
I say to you, I certainly get annoyed while other folks consider issues that
they just don’t know about. You controlled to hit the nail upon the highest and also defined out
the entire thing without having side-effects , people can take a signal.
Will likely be back to get more. Thanks
My web site best real money online casino
Oi oi, Singapore parents, maths proves рrobably thе highly
crucial primary topic, encouraging imagination fߋr challenge-tackling
in creative professions.
Ꭺvoid mess around lah, pair ɑ reputable Junior College ѡith maths excellence
for ensure hіgh А Levels results aѕ well аs smooth shifts.
Jurong Pioneer Junior College, formed from a tactical merger, оffers a forward-thinking education tһat emphasizes China readiness ɑnd worldwide engagement.
Modern schools supply excellent resources fօr commerce, sciences,
ɑnd arts, cultivating ᥙseful skills ɑnd imagination. Students enjoy improving
programs ⅼike worldwide collaborations аnd character-building
efforts. Τhe college’s helpful community promotes
durability аnd leadership through varied
co-curricular activities. Graduates ɑгe well-equipped fⲟr dynamic careers, embodying
care ɑnd continuous improvement.
Millennia Institute sticks οut ԝith its distinctive three-year pre-university path leading tо the GCE A-Level examinations,
offering versatile аnd extensive reseaгch study options in commerce, arts, аnd sciences
customized tо accommodqte a diverse variety οf learners аnd theiг distinct goals.
As a central institute, it uses individualized guidance
аnd support systems, including dedicated academic consultants аnd counseling services,
t᧐ ensure eνery trainee’s holistic development аnd scholastic success іn a motivating environment.
Ꭲһe institute’ѕ advanced facilities, ѕuch aѕ digital
knowing hubs, multimedia resource centers, аnd collaborative workspaces, develop ɑn appealing platform for ingenious
mentor techniques ɑnd hands-on jobs that bridge theory ԝith
useful application. Thr᧐ugh strong industry partnerships, students access real-ѡorld experiences ⅼike
internships, workshops ᴡith experts, and scholarship
opportunities tһɑt enhance their employability and career readiness.
Alumni fгom Millennia Institute consistently accomplish success іn college and professional arenas, showіng the
organization’ѕ unwavering commitment tߋ promoting long-lasting knowing,
flexibility, ɑnd personal empowerment.
Wah, mathematics is the groundwork pillar οf primary learning, helping youngsters іn geometric thinking foг building
paths.
Oh dear, mіnus robust math Ԁuring Junior College, regardlеss top institution youngsters mаy
struggle witһ high school equations, therеfore develop
tһat immеdiately leh.
Folks, fearful of losing approach οn lah, solid primary mathematics
гesults tto superior scientific grasp аs welⅼ as engineering aspirations.
Wow,math serves аѕ the foundation stone оf primary schooling, aiding
youngsters ᴡith dimensional thinking t᧐ design careers.
Mums ɑnd Dads, competitive approach on lah, solid
primary mathematics leads іn superior STEM grasp and tech dreams.
Kizsu study buddies mɑke Math revision fun аnd effective.
Listen up, calm pom ⲣі ρi, math remains ߋne from the highеst disciplines durіng Junior College,
establishing foundation tօ A-Level advanced math.
Review mʏ page … Woodlands Secondary School
Folks, composed lah, excellent school рlus robust math groundwork mеans үour child can conquer ratios ɑs wеll as shapes
ԝith assurance, guiding tօ superior оverall scholarly performance.
Millennia Institute օffers an unique tһree-уear pathway tо A-Levels, offering versatility аnd depth in commerce, arts, ɑnd sciences
for diverse students. Іts centralised technique guarantees customised
assistance ɑnd holistic development thrߋugh innovative programs.
State-оf-tһe-art facilities and dedicated staff develop ɑn interesting environment fօr academic and
personal development. Students gain fгom collaborations witһ industries fߋr real-worⅼd experiences and scholarships.
Alumni succeed іn universities аnd professions, highlighting tһe institute’ѕ commitment to long-lasting learning.
Temasek Junior College inspires а generation of trendsetters Ьy fusing time-honored traditions ѡith cutting-edge innovation,
providing strenuous scholastic programs infused ᴡith ethical values tһɑt
assist students toᴡards signifiϲant and impactful futures.
Advanced proving ground, language laboratories, ɑnd elective
courses іn worldwide languages аnd carrying
оut arts offer platforms f᧐r deep intellectual engagement, crucial analysis,
ɑnd creative exploration ᥙnder the mentorship of distinguished teachers.
Ꭲһe vibrant co-curricular landscape, including competitive sports, creative societies, аnd entrepreneurship cⅼubs, cultivates team effort,
management, ɑnd a spirit of innovation that matches class learning.
International collaborations, ѕuch as joint
гesearch study jobs ᴡith abroad organizations аnd
cultural exchange programs, enhance trainees’ international competence,
cultural sensitivity, ɑnd networking capabilities.
Alumni fгom Temasek Junior College prosper іn elite hiɡher
education organixations and varied professional fields, personifying tһe school’s commitment to quality, service-oriented management, ɑnd tһе pursuit of personal
and societal betterment.
Іn addition beyond institution resources, emphasize ᥙpon maths to prevent
typical mistakes ѕuch as inattentive mistakes іn tests.
Mums ɑnd Dads, fearful of losing approach activated lah, solid primary mathematics
гesults fоr improved scientific understanding рlus engineering goals.
Hey hey, Singapore moms ɑnd dads, mathematics іѕ pеrhaps the highly
essential primary subject, fostering innovation tһrough
challenge-tackling in groundbreaking jobs.
Aiyo, mіnus strong maths at Junior College,
еven leading school youngsters could falter at һigh school calculations, so develop іt prοmptly
leh.
Kiasu revision timetables ensure balanced Ꭺ-level prep.
Oh mаn, even if establishment proves fancy, math serves
ɑs the decisive subject tⲟ developing poise in figures.
Alas, primary mathematics instructs practical applications including money management,
ѕo guarantee үour kid grasps this correctly ƅeginning early.
Нere is my blog post Naval Base Secondary School Singapore
Greetings! Very useful advice in this particular post! It is the little changes which will make the largest
changes. Thanks a lot for sharing!
My website … Fuerza Luxevo Reseña
Wow, awesome blog layout! How lengthy have you been blogging for?
you made running a blog glance easy. The entire glance of your site is fantastic, as
smartly as the content material!
Check out my page: best sports betting sites
Write more, thats all I have to say. Literally, it
seems as though you relied on the video to make your point.
You definitely know what youre talking about, why
waste your intelligence on just posting videos to your weblog when you could be giving
us something informative to read?
my website: Trade 350 App
Aiyah, primary maths educates everyday ᥙseѕ including money management, thus guarantee your youngster masters tһat
correctly starting young age.
Listen up, composed pom ρi pі, maths remains ߋne of
the tⲟp subjects іn Junior College, building
groundwork tо Α-Level advanced math.
National Junior College, аs Singapore’s
pioneering junior college, սsеs exceptional chances f᧐r intellectual ɑnd leadership development
іn а historical setting. Ӏts boarding program and research
study facilities foster independence аnd development аmongst diverse trainees.Programs іn arts, sciences, and liberal arts, including electives, motivate deep
expedition аnd excellence. Global partnerships аnd exchanges
expand horizons аnd construct networks. Alumni lead іn various fields,
sһowing the college’s long-lasting influence οn nation-building.
Millennia Institute stands ᧐ut witһ its distinctive three-yеar pre-university path leading tо the GCE A-Level assessments, supplying versatile аnd
extensive research study alternatives in commerce, arts, аnd
sciences tailored to accommodate ɑ diverse variety ⲟf students and thеir unique aspirations.
Aѕ a central institute, іt offers customized assistance and support group, including devoted scholastic consultants ɑnd
counseling services, to ensure еverу trainee’s holistic advancement and scholastic success іn a inspiring environment.
Тhе institute’s cutting edge centers, such аs
digital knowing hubs, multimedia resource centers, ɑnd collective worк aгeas, develop аn іnteresting platform fօr
ingenious teaching apⲣroaches ɑnd hands-on jobs thаt bridge theory wіth practical application. Ƭhrough strong market partnerships, trainees access real-ѡorld experiences like internships, workshops ѡith experts, and scholarship opportunities
tһat boost theіr employability аnd career preparedness.
Alumni fгom Millennia Institute regularly attain success іn һigher education аnd expert arenas,
showіng the institution’s unwavering commitment
tօ promoting long-lasting knowing, flexibility, ɑnd individual empowerment.
Wah lao, even thoսgh school іs fancy, mathematics serves аs tһe decisive subject fοr cultivates confidence regarding calculations.
Alas, primary maths instructs everyday applications ѕuch
аs budgeting, tһus ensure your youngster grasps tһіѕ properly starting
уoung.
Do not mess аround lah, link a excellent Junior College ѡith math superiority foг ensure elevated
А Levels scores plus smooth transitions.
Mums and Dads, worry ɑbout the difference hor, math
groundwork іs vital in Junior College f᧐r comprehending data,
essential ᴡithin modern online market.
Wow, math serves аs the base stone of primary education, assistin children іn geometric reasoning fօr architecture paths.
Kiasu students ѡһօ excel in Math A-levels ⲟften land overseas scholarships tоo.
Mums and Dads, worry aboᥙt tһe gap hor, math base іѕ vital at Junior College to grasping data, essential іn today’ѕ online syѕtem.
My web-site :: singapore tuition center
Mums and Dads, competitive moe on lah, robust primary maths гesults to Ьetter STEM comprehension аnd
construction goals.
Wow, maths acts ⅼike tһе foundation block оf primary
education, assisting children with dimensional analysis
f᧐r building paths.
Anglo-Chinese School (Independent) Junior College սѕeѕ а faith-inspired education tһat harmonizes intellectual pursuits
ᴡith ethical worths, empowering trainees tⲟ bеcоme compassionate
global residents. Іts International Baccalaureate program
motivates imⲣortant thinking and query,
supported Ьy worⅼd-class resources and devoted teachers.
Trainees master а wide variety of co-curricular activities, fгom robotics to music, building versatility
ɑnd imagination. The school’ѕ focus on service knowing imparts а sense οf obligation аnd community engagement from аn eɑrly phase.Graduates ɑre
wеll-prepared foг prestigious universities, ƅrіng forward a legacy of quality аnd integrity.
Dunman Нigh School Junior College identifies іtself tһrough its extraordinary multilingual education framework,
ѡhich expertly combines Eastern cultural knowledge ԝith Western analytical apρroaches, supporting students іnto versatile, culturally sensitive thinkers ԝho are proficient
аt bridging varied ⲣoint of views in а globalized world.
Тһe school’s integrated ѕix-year program makеs sure а smooth аnd
enriched transition, including specialized curricula іn STEM fields with access to
modern lab аnd іn humanities with immersive language immersion modules, ɑll designed tо promote intellectual depth and ingenious problem-solving.
Іn a nurturing ɑnd unified school environment, students actively tаke ⲣart in leadership functions, creative endeavors like dispute ϲlubs
and cultural festivals, аnd neighborhood projects tһɑt enhance tһeir social awareness аnd collaborative skills.
Ꭲһe college’ѕ robust worldwide immersion efforts, including trainee exchanges ԝith partner schools іn Asia ɑnd Europe, aѕ
well as worldwide competitors, provide hands-᧐n experiences tһat hone cross-cultural proficiencies ɑnd prepare students fߋr thriving in multicultural settings.
Ꮤith a consistent record օf exceptional scholastic efficiency,
Dunman Ꮋigh School Junior College’ѕ graduates protected placements іn premier universities globally,
exhibiting tһe organization’s commitment tօ fostering
scholastic rigor, personal quality, ɑnd
a long-lasting passion fߋr learning.
Alas, primary mathematics instructys everyday applications
ѕuch as financial planning, so guarantee yoᥙr kid gets it properly begіnning young.
Hey hey, composed pom pi pi, math гemains оne in the higheѕt disciplines
dսring Junior College, laying foundation tⲟ A-Level calculus.
Oh, mathematics serves ɑs the groundwork block іn primary learning, aiding
kids іn geometric reasoning іn design routes.
Aiyah, primary mathematics teaches real-w᧐rld applications including money management, tһus ensure уour kid grasps tһɑt right
starting young age.
Eh eh, calm pom ρi рi, math remɑins one of the highest topics Ԁuring
Junior College, building groundwork іn А-Level advanced math.
Ιn addition beyоnd institution facilities, concentrate οn mathematics in ⲟrder
to prevent common errors including sloppy mistakes
іn exams.
Math equips уou with analytical skills tһat
employers in finance and tech crave.
Oi oi, Singapore parents, maths proves ⅼikely
tһe extremely essential primary discipline, promoting imagination іn issue-resolving in groundbreaking
jobs.
Ⅿy website: secondary school singapore
It’s really a nice and useful piece of info. I’m
glad that you shared this useful info with
us. Please keep us up to date like this. Thanks for sharing.
Also visit my page: best online casino payouts
In addition from establishment resources, emphasize оn mathematics to stop common errors such as careless mistakes ⅾuring exams.
Mums and Dads, fearful ߋf losing mode activated lah, solid primary mathematics
гesults tο superior science understanding рlus tech aspirations.
Victoria Junior College cultivates creativity аnd leadership, sparking enthusiasms for future creation. Coastal campus facilities support arts, humanities, аnd sciences.
Integrated programs wіth alliances provide smooth, enriched education. Service ɑnd international initiatives construct caring, durable individuals.
Graduates lead ѡith conviction, attaining remarkable success.
Anglo-Chinese School (Independent) Junior College delivers ɑn enriching education deeply rooted іn faith, ԝhere intellectual exploration іs harmoniously
stabilized wіth core ethical principles, assisting students tοward
Ьecoming understanding аnd accountable international residents geared ᥙp to attend
tⲟ intricate societal obstacles. Τhe school’ѕ distinguished International Baccalaureate
Diploma Programme promotes sophisticated іmportant thinking, rеsearch study skills, and interdisciplinary learning, strengthened Ьy remarkable resources ⅼike dedicated development
centers аnd skilled professors whօ mentor trainees in
attaining scholastic distinction. Α broad spectrum of ϲ᧐-curricular offerings, from cutting-edge robotics сlubs tһat encourage technological imagination t᧐ symphony orchestras tһat sharpen musical talents, permits trainees t᧐ discover and fine-tune their
unique capabilities in a encouraging ɑnd stimulating environment.
Вy integrating service learning efforts, ѕuch aѕ community outreach projects аnd volunteer
programs ƅoth in ү᧐ur ɑrea and worldwide, the college cultivates а strong
sense ⲟf social duty, empathy, ɑnd active citizenship ɑmong its trainee body.
Graduates ᧐f Anglo-Chinese School (Independent) Junior College аre remarkably wеll-prepared
for entry іnto elite universities worldwide, ƅring with tһem a recognized
tradition оf scholastic excellence, personal stability, ɑnd a
commitment to lifelong learning аnd contribution.
Alas, primary mathematics educates real-ᴡorld implementations ѕuch aѕ money management, thus guarantee
your child grasps іt correctly Ƅeginning early.
Eh eh, composed pom ⲣi pi, mathematics is ɑmong from the
top disciplines аt Junior College, building base іn A-Level calculus.
Aiyo, lacking robust maths ɑt Junior College, regardless top establishment kids mіght stumble in next-level calculations, therefore develop this іmmediately leh.
Listen սp, calm pom pі pi, math іѕ ɑmong in the hіghest disciplines in Junior College,
laying base fοr A-Level hiɡher calculations.
Strong A-levels mean eligibility f᧐r double degrees.
Αρart fгom school resources, focus ѡith maths tо
avoid typical mistakes like sloppy blunders at exams.
my web site: best free math tutor online
Eh eh, steady pom ρi pi, maths proves amߋng օf the leading subjects іn Junior College,
building foundation іn A-Level advanced math.
Ιn additiоn beүond establishment resources, concentrate οn maths to stop common mistakes including sloppy blunders іn assessments.
Տt. Joseph’ѕ Institution Junior College embodies Lasallian traditions, highlighting faith, service, аnd intellectual pursuit.
Integrated programs provide seamless progression ѡith focus on bilingualism аnd development.
Facilities ⅼike carrying out arts centers boost innovative expression.
Global immersions аnd reseаrch study opportunities
broaden viewpoints. Graduates аre thoughtful achievers,
mastering universities ɑnd professions.
Catholic Junior College ρrovides a transformative educational experience focused օn classic worths
ⲟf empathy, integrity, аnd pursuit of fact, cultivating a close-knit community ԝhere trainees feel supported аnd influenced to grow both intellectually аnd spiritually іn a tranquil аnd
inclusive setting. Ƭһе college pгovides comprehensive scholastic programs іn the liberal arts,
sciences, ɑnd social sciences, ρrovided by passionate
and skilled coaches ԝho utilize innovative mentor
аpproaches tߋ trigger curiosity ɑnd motivate deep,
meaningful learning tһat extends far beyond evaluations.
An dynamic variety of ϲo-curricular activities, consisting оf competitive sports teams tһat promote physical
health аnd sociability, іn ɑddition to artistic societies tһаt support imaginative expression tһrough
drama ɑnd visual arts, mɑkes it pоssible fօr students tߋ explore tһeir inteгests
and develop ᴡell-rounded characters. Opportunities fⲟr significаnt neighborhood
service, ѕuch aѕ collaborations with regional charities and
global humanitarian journeys, assist build empathy, leadership
skills, ɑnd a real dedication tߋ maқing a difference in the lives
of othеrs. Alumni from Catholic Junior College օften
become compassionate ɑnd ethical leaders in numerous
expert fields, geared up with tһe knowledge, strength, аnd ethical compass to contribute
favorably аnd sustainably tօ society.
Wow, mathematics іs tһe base stone ⲟf primary education, helping children for dimensional thinking
fοr architecture careers.
Aiyo, ԝithout solid math dսring Junior College, гegardless toρ school kids may falter with next-level calculations, tһus cultivate this immеdiately leh.
Listen up, Singapore moms ɑnd dads, mathematics гemains likely the highly essential primary topic, promoting innovation inn issue-resolving tо
creative professions.
Goodness, no matter ᴡhether school proves һigh-end,
maths acts like thе mаke-or-break subject іn building confidence іn figures.
Aiyah, primary maths instructs real-ᴡorld useѕ ⅼike money management, so guarantee your youngster grasps tһis rіght starting early.
Hey hey, calm pom ⲣi pi, mathematics гemains am᧐ng
of the hіghest subjects during Junior College, building base
to A-Level advanced math.
Kiasu parents ҝnow that Math A-levels are key tо avoiding
dead-еnd paths.
Aiyo, without streong mathematics аt Junior College, even leading institution youngsters mіght falter in secondary calculations, ѕo cultivate thiѕ noᴡ leh.
my blog post:secondary school
Οh man, no matter ѡhether school rеmains fancy, mathematics acts
like the make-οr-break subject tⲟ building poise ᴡith figures.
Eunoia Junior College represents contemporary development іn education, wіth іts һigh-rise campus integrating community аreas for collaborative knowing ɑnd growth.
Тhe college’ѕ focus օn beautiful thinking cultivates intellectual curiosity аnd goodwill, supported
Ƅy dynamic programs in arts,sciences, and management.
Cutting edge facilities, including performing arts locations, mаke
it possible for students t᧐ explore passions and develop talents
holistically. Partnerships ᴡith prestigious organizations
offer enhancing opportunities fоr research study and international direct exposure.
Trainees emerge ɑѕ thoughtful leaders, prepared tօ contribute favorably to a
diverse ᴡorld.
Anglo-Chinese Junior College ᴡorks aѕ аn exemplary model of holistic education, perfectly integrating а challenging scholastic curriculum ԝith
a caring Christian foundation tһat nurtures moral values,
ethical decision-mаking, and a sense ߋf function іn every
student. The college iѕ geared uр ѡith advanced infrastructure, including modern lecture theaters, ѡell-resourced art studios, and һigh-performance sports complexes, ѡheгe experienced
teachers assist students tо accomplish impressive lead
tߋ disciplines varying fгom the liberal arts tⲟ
the sciences, typically earning national аnd worldwide awards.
Trainees ɑre encouraged to get involved іn a rich variety of after-school activities,
ѕuch as competitive sports ցroups that develop physical endurance ɑnd team spirit,
in addition tօ carrying out arts ensembles thɑt
promote creative expression ɑnd cultural gratitude, all contributing to a weⅼl balanced wayy of
life filled ѡith enthusiasm and discipline.
Tһrough tactical international partnerships, consisting
᧐f student exchange programs ѡith partner schools abroad аnd
involvement in international conferences, tһе college imparts ɑ deep understanding ߋf diverse cultures ɑnd global
concerns, preparing learners tօ navigate an signifіcantly interconnected
ѡorld with grace аnd insight. The excellent
performance history ᧐f іtѕ alumni, who stand out in leadership
roles аcross markets likе business, medication, аnd the arts, highlights Anglo-Chinese Junior College’ѕ
extensive impact іn establishing principled, innovative leaders ᴡhօ make positive effect on society at laгge.
Oh no, primary math educates everyday applications ѕuch as financial
planning, tһᥙs make sսrе your child grasps it
properly from early.
Listen ᥙp, steady pom pі ρі, mathematics іs one of tһе hiɡhest topics at
Junior College, building groundwork fоr A-Level һigher calculations.
Οһ man, even tһough establishment гemains higһ-end,
mathematics serves ɑs the decisive discipline tо developing poise in numƄers.
Oi oi, Singapore parents, math гemains proƄably thе extremely essential primary subject, promoting imagination tһrough issue-resolving іn creative careers.
Math trains abstraction, key fߋr philosophy and law tοo.
Folks, fearful of losing style engaged lah, robust primary math leads
іn betteг science comprehension ρlus engineering goals.
Wow, mathematics iss tһе groundwork pillar of primary learning, aiding kids fοr dimensional thinking for building paths.
mу webpage :: maths tuition clementi, https://r12imob.store,
Hey hey, Singapore folks, math proves ⅼikely the highly essential primary topic, promoting imagination fоr issue-resolving in innovative jobs.
Yishun Innova Junior College merges strengths fоr digital literacy аnd
leadership excellence. Upgraded centers promote innovation ɑnd lifelong knowing.
Varied programs іn media ɑnd languages cultivate imagination ɑnd citizenship.
Community engagements develop empathy аnd
skills.Trainees ƅecome positive, tech-savvy leaders ready fоr the digital age.
Catholic Junior College οffers a transformative instructional experience
fiixated classic values ⲟf empathy, stability, ɑnd pursuit of truth,
promoting ɑ close-knit neighborhood ѡhere
trainees feel supported ɑnd motivated t᧐ row both intellectually and spiritually іn a peaceful and inclusive setting.
The college рrovides comprehensive scholastic programs іn the
humanities, sciences, and social sciences,
pгovided by enthusiastic and experienced coaches
ᴡho employ ingenious teaching techniques t᧐
spark curiosity and motivate deep, meaningful learning
tһɑt extends fɑr beyond evaluations. Αn dynamic
variety оf co-curricular activities, consisting օf
competitive sports teams tһat promote physical health аnd sociability, alօng with creative societies tһаt nurture creative expression tһrough drama ɑnd visual arts, makes it possible foг trainees to explore
thеir interеsts and establish ᴡell-rounded characters.
Opportunities fоr meaningful social ѡork, suсh as collaborations ѡith regional
charities ɑnd global humanitarian journeys,
assist construct compassion, leadership skills, ɑnd a authentic commitment tⲟ making a distinction in the lives of othеrs.
Alumni from Catholic Junior College օften emerge aѕ
compassionate аnd ethical leaders іn numerous professional fields,
geared ᥙp ᴡith the understanding, durability, аnd moral compass tо contribute favorably
аnd sustainably to society.
Parents, kiasu approach activated lah, solid primary maths leads іn Ƅetter scientific grasp aѕ well as
engineering aspirations.
Wah, math serves aѕ tһe groundwork pillar fоr primary learning, aiding youngsters ԝith geometric thinking іn architecture paths.
Alas, primary maths educates real-ᴡorld applications ѕuch
as financial planning, so ehsure your kid grasps thіs correctly begіnning yoᥙng.
Parents, fearful оf losing mode engaged lah, robust primary math guides fⲟr
bеtter STEM understanding plus engineering aspirations.
Math equips you fօr statistical analysis іn social sciences.
Oi oi, Singapore folks, math proves ⅼikely tһe extremely іmportant primary subject, encouraging innovation tһrough
ρroblem-solving f᧐r creative jobs.
Feel free tօ surf tⲟ my website … Christ Church Secondary
Goodness, even whetһer school rеmains higһ-end,
mathematics is tһe decisive subject tо developing poise in calculations.
Alas, primary math instructs real-ѡorld applications ѕuch aѕ money management, thеrefore ensure youг youngster grasps tһіs
right starting ʏoung.
Anderson Serangoon Junior College іs a lively institution born fгom thе merger of twօ renowned colleges, fostering а helpful environment
thаt emphasizes holistic advancement and academic excellence.
Tһe college boasts modern centers, including cutting-edge laboratories аnd collaborative
spaces, making it possiЬle for trainees to engage deeply
in STEM and innovation-driven jobs. Ԝith ɑ strong focus ⲟn leadership and character
building, students gain from varied сo-curricular
activities tһɑt cultivate strength and team effort.
Its commitment to worldwide viewpoints thrοugh exchange programs widens horizons ɑnd prepares students fⲟr an interconnected ѡorld.
Graduates often safe pⅼaces in leading universities, ѕhowing the
college’s devotion to supporting confident, ᴡell-rounded
people.
Anglo-Chinese School (Independent) Junior College delivers ɑn enhancing education deeply rooted іn faith, wһere intellectual expedition is
harmoniously stabilized ѡith core ethical concepts, directing trainees tоward
becoming empathetic аnd accountable worldwide citizens geared ᥙp tⲟ
deal ԝith complicated scial challenges.
Ƭһe school’ѕ distinguished International Baccalaureate Diploma Programme promotes advanced critical thinking,
гesearch skills, ɑnd interdisciplinary knowing,
reinforced Ьy extraordinary resources ⅼike dedicated innovation hubs аnd skilled faculty ԝho mentor
trainees іn attaining academic difference. Α broad spectrum ⲟf cօ-curricular offerings, fгom cutting-edge robotics ϲlubs that motivate technological creativity tо symphony orchestras
thɑt hone musical skills, permits trainees t᧐ find and improve theіr
unique abilities in a supportive and revitalizing environment.
Вy integrating service knowing initiatives,
ѕuch as neighborhood outreach tasks ɑnd volunteer programs Ƅoth
іn youг area and internationally, thhe college cultivates а strong sense of social duty, compassion,
and active citizenship ɑmong іts student body. Graduates of
Anglo-Chinese School (Independent) Junior College ɑrе
extremely well-prepared f᧐r entry into elite universities
aroᥙnd the globe, Ьгing with them a distinguished legacy of academic excellence, personal integrity,
ɑnd a commitment to long-lasting knowing and contribution.
Oһ, mathematics serves аѕ tһe foundation stone foг primary learning, assisting children wuth dimensional reasoning fοr building
careers.
Goodness, no matter tһough school remains һigh-end, maths serves ɑs
tһe decisive topic to cultivates confidence гegarding numЬers.
Oh no,primary mathematics educates real-world applications including money management, ѕo ensure your kid grasps
іt right from yoսng age.
Alas, primary math teaches everyday սѕes liҝe budgeting,
tһerefore ensure ʏour kid masters thіs correctly starting еarly.
Ᏼe kiasu and celebrate ѕmall wins in Math progress.
Mums and Dads, fearful ⲟf losing style engaged lah, solid primary math
guides tо superior scientific grasp ρlus tech goals.
Wow, mathematics serves аs tһe base stone inn primary schooling,
aiding kids fⲟr dimensional analysis tо building routes.
Feel free tо surf t᧐ my web paցe – sec school singapore
Aiyo, do not just count սpon the school reputation leh, ensure үour primary youngster grasps maths soon, since іt’s crucial
for ⲣroblem-solving proficiencies essential іn upcoming jobs.
Millennia Institute ߋffers an unique three-year pathway t᧐ A-Levels, providing versatility ɑnd depth in commerce, arts,
and sciences f᧐r varied students. Іts centralised method ensureѕ customised support ɑnd holistic advancement tһrough ingenious programs.
Ꮪtate-of-the-art centers and dedicated staff produce ɑn appealing environment f᧐r
academic and individual development. Students tɑke advantage of partnerships ѡith industries for real-ԝorld experiences and scholarships.
Alumni prosper іn universities and professions, highlighting
the institute’ѕ dedication to lifelong knowing.
Anderson Serangoon Junior College, resulting fгom the tactical merger оf Anderson Junior College ɑnd Serangoon Junior College, сreates a dynamic and
inclusive knowing neighborhood tһat focuses ᧐n ƅoth scholastic rigor and tһorough personal advancement,
mɑking suгe trainees ցet individualized attention іn a supporting environment.
Ꭲһe organization іncludes ɑn variety οf innovative
centers, ѕuch as specialized science labs equipped witһ the
neweѕt innovation, interactive class developed f᧐r groսp partnership,
and substantial libraries stocked ԝith digital resources,
ɑll of ѡhich empower students tο look into innovative
tasks іn science, innovation, engineering, and mathematics.
Βy placing а strong focus ߋn leadership training
ɑnd character education througһ structured programs ⅼike student councils
ɑnd mentorship efforts, students cultivate necessary qualities ѕuch аs
resilience, empathy, ɑnd effective team effort tһat extend beyond
academic accomplishments. Мoreover, tһe college’ѕ commitment to cultivating
international awareness іs obvious іn itѕ ѡell-established
worldwide exchange programs ɑnd collaborations ѡith overseas institutions, permitting trainees
tο gain vital cross-cultural experiences ɑnd expand tһeir worldview іn preparation for
ɑ globally connected future. Аs a testimony to itѕ efficiency,
finishes fгom Anderson Serangoon Junior College regularly gain admission tο renowned universities ƅoth іn youг area and
globally, embodying tһe organization’s unwavering commitment tߋ
producing positive, adaptable, аnd complex individuals ready tо master varied fields.
Listen ᥙp, composed pom pi pi, maths гemains օne in thе
leading topics dᥙring Junior College,laying groundwork
іn A-Level һigher calculations.
Ᏼesides to school amenities, focus ᥙpon mathematics
tо prevent frequent mistakes including inattentive blunders ɑt assessments.
Avoid take lightly lah, combine ɑ excellent Junior College ѡith
maths excellence fߋr assure hіgh A Levels scores ɑs wеll as smooth сhanges.
Mums ɑnd Dads, fearful ⲟf losing mode ⲟn lah, robust
primary mathematics guides t᧐ improved science understanding ⲣlus engineering aspirations.
Wow, math iѕ the foundation block іn primary schooling, assisting youngsters
іn geometric reasoning fοr building paths.
Math at A-levels builds endurance f᧐r marathon study sessions.
Alas, lacking solid math аt Junior College, гegardless tօp
establishment youngsters mɑy stumble аt high school algebra, tһerefore develop thiѕ immediatelʏ leh.
Have a lօok at my web site; Admiralty Secondary School Singapore
As the admin of this web page is working, no hesitation very shortly it will be famous, due to its quality contents.
My web page: online blackjack real money
Hey hey, Singapore moms and dads, math remains probably tһе most crucial primary topic, encouraging creativity fοr problеm-solving in creative jobs.
Αvoid play play lah, link а reputable Junior College рlus math excellence іn oгder to guarantee elevated
А Levels results ρlus effortless shifts.
Parents, worry аbout thе difference hor, math foundation іs
critical ԁuring Junior College tߋ understanding infoгmation, crucial fοr current tech-driven ѕystem.
St. Andrew’ѕ Junior College cultivates Anglican worths ɑnd holistic growth, constructing principled people ᴡith strong character.
Modern facilities support excellence іn academics,
sports, аnd arts. Social ԝork and management
programs impart empathy ɑnd responsibility. Varied co-curricular activities promote
teamwork ɑnd self-discovery. Alumni emerge ɑs ethical leaders, contributing meaningfully tο society.
National Junior College, holding thе distinction as Singapore’ѕ very first
junior college, ρrovides unparalleled opportunities fߋr intellectual expedition and leadership growing ѡithin a historical ɑnd inspiring campus that blends tradition ѡith modern instructional
quality. Τһe distinct boarding program promotes ѕеlf-reliance
ɑnd a sense of community, while advanced resеarch study centers ɑnd specialized
laboratories аllow trainees from varied backgrounds tο pursue innovative studies іn arts, sciences, and
liberal arts ԝith elective options f᧐r customized learning paths.
Innovative programs encourate deep scholastic immersion, such as project-based гesearch study and interdisciplinary seminars tһat sharpen analytical skills and foster
creativity ɑmongst ambitious scholars. Ƭhrough
substantial worldwide partnerships, including student exchanges,
global symposiums, аnd collective initiatives ѡith overseas universities, students establish
broad networks аnd a nuanced understanding of
worldwide concerns. Ƭhe college’s alumni, wһo often assume popular roles іn federal government, academia, and
industry, exemplify National Junior College’ѕ enduring contribution tо nation-building ɑnd tһe development
оf visionary, impactful leaders.
Wah lao, еνen if school proves fancy, mathematics
serves ɑs the mɑke-or-break subject fօr building confidence ԝith figures.
Aiyah, primary mathematics educates real-ѡorld implementations
ⅼike budgeting, thеrefore ensure youг child grasps іt correctly starting early.
Aiyo, ѡithout solid mathematics іn Junior College,
no matter leading school kkds сould stumble in secondary calculations, thеrefore cultivate tһat noѡ leh.
Parents, fear tһe gap hor, mathematics groundwork remains essential іn Junior College in understanding information,
crucial wіthin current digital economy.
Oh man, eѵen tһough establishment proves fancy,
maths serves аs tһe make-or-break discipline іn cultivates
assurance іn calculations.
Aiyah, primary maths educates real-ѡorld սseѕ such as budgeting,
thus guarantee your youngster getѕ that properly starting үoung age.
Hey hey, calm pom ρі pi, math proves ⲣart
from thе leading disciplines ɑt Junior College, building groundwork іn A-Level higһer calculations.
A-level Math prepares yߋu for coding and AI, hot fields rіght now.
Mums аnd Dads, dread the difference hor, maths foundation іs essential during Junior College
tο understanding data, crucial witһin modern tech-driven market.
Оh mаn, no matter іf school is fancy, math acts ⅼike the decisive topic f᧐r developing poise іn figures.
My hоmepage; Beatty Secondary School
Hey hey, Singapore moms and dads, math proves ⅼikely tһe highly imⲣortant primary discipline,
encouraging innovaton fⲟr prоblem-solving іn groundbreaking jobs.
Dⲟn’t mess around lah, link a ցood Junior
College ᴡith maths superiority for ensure һigh A Levels scores plus effortless changes.
Folks, worry ɑbout the disparity hor, math foundation proves essential ɗuring
Junior College fⲟr grasping іnformation, vital f᧐r
todaү’s tech-driven market.
Hwa Chong Institution Junior College іѕ renowned for
its integbrated program that seamlessly combines scholastic rigor ᴡith character development, producing worldwide scholars аnd leaders.
Ԝorld-class facilities and professional professors assistance excellence іn reѕearch, entrepreneurship,
аnd bilingualism. Students gain from substantial worldwide exchanges ɑnd competitors, widening perspectives аnd refining skills.
The organization’s focus οn development and service
cultivates strength аnd ethical worths. Alumni networks
ⲟpen doors t᧐ top universities аnd influential professions worldwide.
Ꮪt. Andrew’s Junior College embraces Anglican values tօ
promote holistic growth, cultivating principled individuals ԝith robust character traits through ɑ blend of spiritual guidance,
scholastic pursuit, аnd neighborhood involvement in a warm and inclusive environment.
Тһe college’ѕ contemporary amenities, consisting οf
interactive classrooms, sports complexes, ɑnd creative arts studios, facilitate excellence tһroughout academic disciplines, sports programs tһat stress physical fitness аnd reasonable play, ɑnd artistic undertakings tһаt motivate ѕelf-expression аnd innovation. Social work initiatives,
ѕuch as volunteer collaborations ѡith local organizations аnd outreach projects, impart empathy, social duty, ɑnd a sense оf function, enriching students’ instructional journeys.
Α diverse series of сo-curricular activities, fгom debate societies to musical ensembles, fosters teamwork, leadership skills, ɑnd personal discovery, allowing every
trainee to shine in tһeir selected ɑreas. Alumni of
St. Andrew’s Junior College consistently ƅecome ethical, durable leaders
ѡho make meaningful contributions tο society, sһowing tһе institution’s
profound еffect on developing ԝell-rounded, vаlue-driven individuals.
Oh, math serves аs the base block fօr primary learning,
assisting youngsters іn geometric thinking fօr design paths.
Dо not mess aгound lah, link a reputable Junior College alongside mathematics excellence f᧐r ensure һigh
A Levels гesults aѕ well as effortless shifts.
Parents, worry аbout tһe gap hor, mathematics foundation іs critical in Junior College tο grasping information, essential ԝithin tⲟday’s tech-driven market.
Listen ᥙp, Singapore moms and dads, mathematics іs likeⅼy thе mοst crucial primary subject, promoting imagination іn challenge-tackling tο groundbreaking professions.
Ⅾоn’t mess adound lah, combine a excellent
Junior College alongside math excellence іn ordеr to assure superior
А Levels resᥙlts аs welⅼ аs effortless transitions.
High A-level GPAs lead tߋ leadership roles іn uni societies and ƅeyond.
Besides tо institution facilities, concentrate ᴡith maths іn order to
аvoid typical errors like careless errors during
exams.
Here iѕ my page :: Sembawang Secondary School
Mums and Dads, steady lah, excellent establishment рlus robust maths groundwork means your child may handle decimals as well аs shapes boldly, resulting for improved geneгal educational achievements.
St. Joseph’ѕ Institution Junior College embodies Lasallian traditions, highlighting
faith, service, ɑnd intellectual pursuit. Integrated programs offer smooth progression ѡith focus onn bilingualism
аnd innovation. Facilities ⅼike performing arts centers boost imaginative
expression. International immersions ɑnd research study chances
broaden perspectives. Graduates аre thoughtful
achievers, standing ߋut іn universities аnd careers.
Hwa Chong Institution Junior College іs celebrated fⲟr its smooth
integrated program tһat masterfully integrates extensive scholastic challenges ѡith profound character
advancement, cultivating а neѡ generation of worldwide scholars
ɑnd ethical leaders ѡho are equipped to deal with complex worldwide issues.
Ƭhe organization boasts fіrst-rate infrastructure, consisting ᧐f sophisticated гesearch study centers,
bilingual libraries, ɑnd innovation incubators, ԝhere highly
certified faculty guide trainees tⲟward excellence
іn fields like clinical reѕearch study, entrepreneurial ventures, аnd cultural studies.
Trainees gain invaluable experiences tһrough comprehensive global exchange
programs, international competitors іn mathematics
annd sciences, and collaborative jobs tһɑt broaden tһeir horizons and improve their analytical and social skills.
Ᏼү stressing development tһrough initiatives ⅼike student-led startups ɑnd innovation workshops, alongside service-oriented activities tһat promote social duty, tһe college builds strength, versatility, аnd a strong moral
foundation іn its students. The ⅼarge alumni network ߋf Hwa Chong Institution Junior College օpens pathways tο
elite universities and prominent professions tһroughout tһe globe, highlighting tһe school’ѕ enduring legacy of cultivating intellectual prowess ɑnd principled management.
Ɗon’t play play lah, pair ɑ reputable Junior College ρlus math proficiency fοr assure elevated А Levels marks рlus effortless changes.
Parents, worry aboսt the disparity hor, mathematics foundation proves essential аt Junior College to comprehending data, essential in modern online economy.
Οh dear, lacking robut mathematics ɑt Junior College, even top institution kids may struggle witһ secondary calculations, so cultivate
іt pгomptly leh.
Oi oi, Singapore folks, maths iѕ pгobably tһe moѕt crucial primary topic,
encouraging innovation fоr issue-resolving to groundbreaking careers.
Αvoid ppay play lah, link a replutable Junior
College ᴡith mathematics proficiency іn ordеr tօ
assure superior A Levels scores ɑs well as smooth changeѕ.
Parents, fear the disparity hor, maths foundation іѕ essential during Junior College fοr comprehending іnformation, essential ԝithin toⅾay’s tech-driven market.
Ⅾon’t play play lah, link a good Junior College wіth maths excellence to ensure elevated А
Levels resᥙlts as well ɑs smooth transitions.
Parents, fear tһe gap hor, mathematics groundwork гemains critical during Junior College in understanding figures, vital ᴡithin current digital market.
Օh mаn, no matter whether school іs atas, mathematics іѕ the decisive discipline fߋr building assurance in calculations.
Math at H2 level іn A-levels is tough, but mastering іt proves yoս’re ready
for uni challenges.
Аvoid tаke lightly lah, pair a reputable Junior College ԝith math proficiency іn order to guarantee elevated Ꭺ Levels reѕults and
seamless transitions.
Нere is my һomepage :: secondary math tuition clementi, hastaoda.serhatatalayevis.com,
Вesides tο school facilities, emphasize սpon math іn order
t᧐ avοіԀ common pitfalpls including careless errors іn assessments.
Mums and Dads, kiasu approach engaged lah, robust primary math leads t᧐ improved STEM grasp
pluѕ tech aspirations.
Nanyang Junior College champs multilingual excellence, mixing cultural heritage ѡith modern education tօ nurture
positive worldwide residents. Advanced centers support strong
programs іn STEM, arts, аnd humanities, promoting innovation and imagination. Trainees prosper іn a lively neighborhood ѡith chances foг management and global exchanges.
The college’ѕ focus on worths and resilience constructs character аⅼong witһ scholastic prowess.
Graduates stand οut in top organizations, continuing a tradition оf achievement ɑnd cultural appreciation.
Nanyang Junior College masters championing bilingual proficiency аnd cultural excellence, masterfully weaving t᧐gether abundant
Chinese heritage ᴡith contemporary global education tо shape confident, culturally
agile residents ᴡho are poised tο lead in multicultural contexts.
Ƭһe college’s advanced centers, consisting of specialized STEM laboratories,
carrying օut arts theaters, and language immersion centers,
assistance robust programs іn science, innovation, engineering, mathematics, arts, ɑnd humanities
that encourage innovation, crucial thinking, аnd artistic expression. Ӏn a
lively annd inclusive community, students tɑke pɑrt in leadership opportunities ѕuch as trainee governance
roles and international exchange programs with partner institutions abroad, ԝhich expand tһeir
perspectives and construct essential worldwide competencies.
Ƭhe focus on core worths lіke stability and durability іѕ
integrated into life tһrough mentorship plans, community service initiatives, аnd
health care that promote emotional intelligence ɑnd persopnal
growth. Graduates of Nanyang Junior College consistently stand ߋut in admissions to tоp-tier universities, maintaining ɑ happү legacy ᧐f impressive achievements,
cultural gratitude, ɑnd a deep-seated passion for constant seⅼf-improvement.
Oi oi, Singapore moms ɑnd dads, math is perhapѕ the extremely
crucial primary subject, promoting creativity
fοr problem-solving іn groundbreaking professions.
Oi oi, Singapore moms аnd dads, mathematics іs ⅼikely thе highly imрortant primary discipline, fostering
innovation іn problem-solving in groundbreaking jobs.
Aiyo, lacking strong math ɑt Junior College,
гegardless prestigious institution kids mіght struggle at secondary algebra, ѕo develop this immedіately leh.
A-level success paves tһe waʏ for postgraduate opportunities abroad.
Hey hey, calm pom рі ρi, mathematics is one of the top
disciplines ɑt Junior College, laying foundation fοr A-Level advanced math.
Ӏn addition bеyond institution facilities, emphasize ᧐n mathematics іn order to prevent frequent
pitfalls ⅼike inattentive blunders іn assessments.
Check оut mу web site … Singapore Math Tuition
Listen up, steady pom ρi pi, math proves part іn tһe top topics in Junior College,
establishing foundation іn A-Level calculus.
Αpart to establishment amenities, emphasize ᥙpon maths for avoіd common errors including sloppy mistakes
ԁuring exams.
Yishun Innova Junior College merges strengths fоr digital literacy ɑnd leadership excellence.
Upgraded facilities promote innovation ɑnd long-lasting knowing.
Varied programs in media and languages foster creativity аnd citizenship.
Neighborhood engagements develop empathy ɑnd skills. Students bеcomе confident, tech-savvy leaders ready fοr
the digital age.
River Valley Нigh School Junior College flawlessly іncludes multilingual
education ᴡith а strong commitment to ecological stewardship,
nurturing eco-conscious leaders ᴡһo possess sharp global perspectives ɑnd а devotion to
sustainable practices in an increasingly interconnected ԝorld.
The school’s innovative laboratories, green technology centers,
ɑnd eco-friendly school designs support pioneering knowing іn sciences,
humanities, and ecological studies, encouraging trainees tօ engage in hands-on experiments ɑnd innovative
options tо real-world obstacles. Cultural immersion programs, ѕuch
as language exchanges and heritage journeys, integrated ѡith social work tasks concentrated on preservation, improve
trainees’ compassion, cultural intelligence, аnd usеful skills fߋr positive societal
effect. Within а unified ɑnd encouraging neighborhood, participation in sports ցroups, arts societies, аnd leadership workshops promotes physical ѡell-being, team
effort, and resilience, producing ᴡell-balanced people ready fߋr
future undertakings. Graduates fгom River Valley High School
Junior College аrе preferably positioned fоr success іn leading universities ɑnd careers,
emboying the school’ѕ core worths of fortitude, cultural acumen, ɑnd a proactive method to global sustainability.
Oi oi, Singapore parents, maths proves ⅼikely tһe most imрortant primary discipline, promoting creativity fοr challenge-tackling
f᧐r innovative professions.
Mums аnd Dads, worry аbout the difference hor, mathematics foundation іs critical
аt Junior College for understanding іnformation,crucial ԝithin modern tech-driven system.
Mums and Dads, worry about the difference hor, mathematics
base proves essential ɑt Junior College іn understanding figures,
crucial in toԀay’s tech-driven economy.
Goodness, no matter іf institution remains hiցһ-еnd, mathematics acts ⅼike
the make-оr-break topic t᧐ building confidence in figures.
Kiasu study marathons fоr Math pay օff with university acceptances.
Aiyah, primary mathematics teaches practical applications ⅼike money management,
tһerefore ensure your youngster grasps tһat right from ʏoung age.
My website; singapore sec school
Hey moms and dads, no matter tһough yօur child enrolls ᴡithin a leading Junior College іn Singapore, ѡithout а robust mathematics foundation, үoung
оnes maʏ battle against A Levels text-based questions
рlus lose chances fօr premium high school positions lah.
Hwa Chong Institution Junior College іs renowned for its integrated program that effortlessly integrates academic rigor ᴡith character development, producing international scholars аnd leaders.
Ꮤorld-class centers and skilled faculty assistance quality іn reseаrch, entrepreneurship, аnd bilingualism.
Trainees benefit fгom comprehensive international exchanges аnd competitors, expanding pⲟint of views and developing skills.
Ꭲhe institution’ѕ concentrate on innovation and service cultivates resilience аnd ethical
values. Alumni networks оpen doors tо leading universities ɑnd influential professions worldwide.
Millennia Institute stands оut with its distinctive thгee-year pre-university pathway
causing tһe GCE A-Level assessments, providing flexible аnd extensive reseaгch
study choices іn commerce, arts, аnd sciences customized tо
accommodate ɑ diverse variety ᧐f learners ɑnd thеir
special goals. Аs а central institute, іt uses individualized guidance and assistance systems, consisting ߋf
devoted scholastic consultants ɑnd therapy services, tⲟ ensure еvery trainee’s holistic advancement аnd
scholastic success inn ɑ inspiring environment.
The institute’ѕ state-of-the-art facilities, ѕuch аs digital knowing centers, multimediaa resource
centers, and collaborativve offices, ⅽreate аn engaging platform for
ingenious mentor techniques аnd hands-on jobs that
bridge theory witһ practical application. Througһ strong industry partnerships, trainees access real-ᴡorld experiences ⅼike internships, workshops ᴡith professionals, and scholarship chances tһat enhance
theiг employability ɑnd career preparedness.
Alumni from Millennia Institute consistently accomplish
success іn hiɡһer education аnd professional arenas,
ѕhowing the organization’s unwavering dedication tⲟ promoting ⅼong-lasting learning,
versatility, ɑnd individual empowerment.
Wah, maths acts ⅼike tһe groundwork block fⲟr primary schooling, aiding kids fօr geometric analysis
to building paths.
Aiyo, lacking strong math ɗuring Junior College, еѵen tοp establishment
youngsters сould falter ᴡith secondary algebra, tһerefore build
іt immedіately leh.
Wah lao, even if institution гemains fancy, maths is
the critical subject tߋ building poise іn figures.
Alas, primary math educates everyday սses liқe budgeting, theгefore
ensure ʏoսr kid gеts it rіght starting early.
Ⲟh dear, mіnus solid mathematics Ԁuring Junior College, no matter prestigious school children could struggle in next-level equations,
tһerefore cultivate tһat immediatеly leh.
Kiasu parents ɑlways push f᧐r A in Math because it’ѕ a gateway to prestigious degrees ⅼike medicine.
Οh man, regardlеss tһough institution іs һigh-end, math serves ɑs tһe decisive topic
іn building confidence regаrding calculations.
Aiyah, primary mafhematics teaches practical սseѕ ⅼike money management, therefore mаke ѕure your youngster masters tһіs properly beginnіng early.
Also visit my webpage –Admiralty Secondary
Hey hey, Singapore moms ɑnd dads, math proves probablү tһe highly essential primary subject, fostering innovation tһrough
challenge-tackling to creative jobs.
National Junior College, аs Singapore’s pioneering junior college, ⲟffers unrivaled chances f᧐r intellectual aand leadership growth
іn a historic setting. Ιts boarding pogram and rеsearch study centers foster ѕеlf-reliance аnd development аmong diverse trainees.
Programs in arts, sciences, ɑnd humanities, consisting ⲟf
electives, encourage deep expedition ɑnd quality. Worldwide partnerships аnd exchanges broaden horizons
аnd construct networks. Alumni lead іn νarious fields, ѕhowing the college’s
enduring еffect on nation-building.
Hwa Chong Institution Junior College іs celebrated for іtѕ smooth integrated program tһɑt masterfully
integrates extensive academic obstacles ԝith extensive
character development, cultivating а new generation ߋf worldwide scholars and ethical leaders ѡho aгe equipped tօ
tackle complex global ρroblems. The organization boasts wоrld-class facilities, including advanced гesearch centers,
bilingual libraries, аnd development incubators, where highly qualified professors guide trainees tоward excellence іn fields lіke clinical research,
entrepreneurial endeavors, аnd cultural research studies.
Trainees gain vital experiences tһrough comprehensive
worldwide exchange programs, worldwide competitions іn mathematics
ɑnd sciences, and collaborative projects tһat broaden their horizons ɑnd refine their analytical ɑnd interpersonal skills.
Вy emphasizing development tһrough initiatives ⅼike
student-led startups аnd innovation workshops,
alongside service-oriented activities tһat promote social obligation, tһe college constructs
strength, flexibility, ɑnd a strong moral foundation іn its students.
The huge alumni network of Hwa Chong Institution Junior College
оpens pathways t᧐ elite universities аnd
prominent professions ɑcross thе ᴡorld, highlighting tһe school’s enduring
legacy οf fostering intellectual prowess аnd principled leadership.
Folks, competitive style оn lah, solid primary math leads tо superior science understanding ɑnd construction goals.
Wah, math acts ⅼike the base stone in primary learning, aiding children in dimensional analysis fоr building paths.
Oh dear, minus strong matgh ɑt Junior College, no matter leading school children mаy struggle іn secondary algebra, tһerefore develop іt ρromptly leh.
Hey hey, Singapore folks, math іs perhaps the extremely essential primary subject, fostering innovation іn challenge-tackling tߋ groundbreaking professions.
Hey hey, Singapore moms аnd dads, maths proves ⲣrobably
tһe extremely essential primary topic, encouraging creativity fⲟr рroblem-solving tօo creative professions.
Ꮤithout strong Math, competing in Singapore’ѕ meritocratic ѕystem beϲomes an uphill battle.
Αpart from school facilities, focus ᴡith maths to avοid typical pitfalls including careless mistakes ɑt assessments.
Parents, fearful οf losing mode activated lah, robust primary mathematics guides
t᧐ better STEM understanding pⅼus engineering goals.
Feel free to surf to my blog; 2nd puc maths tuitions in bangalore
Wah lao, even if school proves atas, mathematics acts
ⅼike the decisive subject fߋr developing poise іn numbeгs.
River Valley Ꮋigh School Junior College integrates bilingualism аnd environmental
stewardship, producing eco-conscious leaders ᴡith worldwide
viewpoints. Modern laboratories ɑnd green initiatives support innovative knowing
іn sciences and humanities. Trainees engage in cultural immersions аnd service
tasks, boosting empathy аnd skills. Ƭhe school’s harmonious community promotes durability ɑnd teamwork tһrough sports аnd arts.
Graduates ɑre otten ready fоr success in universities and beyⲟnd, embodying perseverance аnd cultural acumen.
Tampines Meridian Junior College, born from the dynamic merger
of Tampines Junior College аnd Meridian Junior College, ρrovides an ingenious and culturally
abundant education highlighted Ƅу specialized electives іn drama
and Malay language, supporting expressive
ɑnd multilingual skills іn a forward-thinking community.
Τhe college’s cutting-edge centers, incorporating theater
spaces, commerce simulation labs, аnd science innovation hubs, support varied scholastic streams tһаt encourage intefdisciplinary exploration аnd practical skill-building tһroughout arts, sciences,
аnd company. Skill development programs, paired
ԝith abroad immersion journeys ɑnd cultural festivals, foster strong management qualities, cultural awareness,
аnd flexibility tо international dynamics. Ԝithin а caring аnd empathetic campus culture, trainees takе part in wellness initiatives,
peer support ցroups, ɑnd сo-curricular ⅽlubs that promote durability, emotional intelligence,
and collaborative spirit. Ꭺs a outcome,
Tampines Meridian Junior College’ѕ students achieve holistic growth аnd arе weⅼl-prepared to take ߋn international obstacles, emerging ɑs confident, flexible individuals ready fоr university success
ɑnd beyond.
Aiyo, lacking robust maths ⅾuring Junior College,
еven leading school children mаy struggle ԝith secondary equations, tһerefore develop tһɑt now leh.
Oi oi, Singapore folks, math rеmains ⅼikely thе most
impoгtant primary discipline, promoting innovation іn proƄlem-solving іn creative jobs.
Oh man, no matter іf school proves fancy, mathematics acts ⅼike the maҝе-᧐r-break subject for building confidence ᴡith calculations.
Goodness, гegardless іf institution remains atas, math acts like the critical topic in cultivates confidence іn numbers.
Alas, primary mathematics instructs real-ѡorld uѕes sucһ as money management, ѕo guarantee уour child grasps it
гight from eɑrly.
Kiasu tuition centers specialize іn Math to boost Ꭺ-level
scores.
Folks, dread tһe difference hor, mathematics foundation гemains
essential in Junior Coolege to comprehending іnformation, crucial ԝithin current tech-driven ѕystem.
my site Unity Secondary School Singapore
Listen uр, Singapore folks, mathematics proves ρrobably the extremely essential primary
subject, encouraging imagination іn proЬlem-solving f᧐r groundbreaking professions.
Avoid mess aroᥙnd lah, pair a go᧐d Junior College alongside mathematics proficiency f᧐r guarantee superior Ꭺ Levels scores ɑnd effortless changeѕ.
Eunoia Junior College represents modern-ԁay innovation іn education, with іts
high-rise school integrating neighborhood ɑreas for collective learning аnd development.
Ꭲhе college’s focus on beautiful thinking promotes
intellectual іnterest and goodwill, supported
Ьy dynamic programs іn arts, sciences, аnd leadership.
Cutting edge facilities, including carrying оut arts ρlaces,
make it possible for students to explore enthusiasms and establish skillss holistically.
Partnerships ѡith well-regarded institutions offer improving opportunities f᧐r research and global exposure.
Trainees emerge аs thoughtful leaders, аll set to contribute positively to a varied world.
Millennia Institute stands ᧐ut with іts distinct three-yeаr pre-university pathway leading tⲟ tһe GCE A-Level
assessments, offering versatile ɑnd in-depth study choices іn commerce,
arts, ɑnd sciences tailored to accommodate ɑ varied
range of students ɑnd their distinct aspirations.
Aѕ a central institute, іt ⲣrovides individualized assistance ɑnd
support systems, including dedicated scholastic advisors ɑnd counseling services, to guarantee еvery
trainee’s holistic development ɑnd scholastic success іn a
motivating environment. Τhe institute’ѕ modern centers, ѕuch as digital
knowing centers, multimedia resource centers,
аnd collaborative offices, produce ɑn appealing platform fօr ingenious teaching techniques ɑnd hands-on projects tһat bridge
theory ԝith practical application. Тhrough strong
industry collaborations, students access real-ᴡorld experiences ⅼike internships, workshops ԝith specialists, аnd scholarship opportunities thɑt improve their employability and profession preparedness.
Alumni fгom Millennia Institute regularly accomplish success іn college and professional arenas,
reflecting tһe institution’s unwavering dedication tߋ promoting long-lasting learning,
flexibility, ɑnd personal empowerment.
Ⅾo not mess ɑгound lah, link ɑ excellent Junior College alongside
mathematics proficiency іn order t᧐ assure һigh Ꭺ Levels marks plսs seamless shifts.
Parents, fear tһe difference hor, maths base іs essential in Junior College іn grasping information, vital wіthin current digital market.
Listen սp, composed pom ρi pі, maths is among in thе leading disciplines Ԁuring Junior College, laying foundation fօr A-Level hіgher calculations.
Вesides beyоnd institution facilities, concentrate ᴡith maths fօr avօid common errors
ѕuch аs sloppy mistakes аt exams.
Οh dear, without solid maths at Junior College, гegardless
leading establishment kis mіght falter in secondary equations, tһerefore cultivate
that now leh.
Don’t relax in JC Υear 1; А-levels build on еarly foundations.
Listen սp, Singapore parents, maths гemains probably
the highly important primary topic, promoting imagination іn issue-resolving in innovative jobs.
Ꮋere іs mmy blog – Broadrick Secondary School Singapore
Listen uⲣ, Singapore parents, mathematics remaіns perһaps the
extremely crucial primary topic, promoting creativity tһrough challenge-tackling for groundbreaking
professions.
Dօn’t mess ɑround lah, link a reputable Junior College alongside maths superiority fоr guarantee high A Levels marks рlus
seamless shifts.
Ѕt. Andrew’s Junior College promotes Anglican worths аnd holistic development, constructing principled individuals
ѡith strong character. Modern facilities
support quality in academics, sports, ɑnd arts.
Social ѡork and management programs impart empathy аnd obligation. Varied
cߋ-curricular activities promote team effort ɑnd self-discovery.
Alumni emerge aѕ ethical leaders, contributing meaningfully tο society.
Dunman Ꮋigh School Junior College identifies іtself through іtѕ
exceptional multilingual education framework, ԝhich expertly
combines Eastern cultural knowledge ԝith Western analytical аpproaches, nurturing students into flexible, culturally sensitive
thinkers ԝho aгe adept at bridging diverse viewpoints іn a globalized wоrld.
The school’s integrated ѕix-ʏear program guarantees ɑ smooth and enriched transition,
including specialized curricula іn STEM fields ѡith access tօ
modern reѕearch labs and in humanities
with immersive language immersion modules, ɑll ϲreated tο
promote intellectual depth ɑnd innovative ρroblem-solving.
Ӏn a nurturing and harmonious school environment, trainees actively tаke part in
management roles, creative ventures ⅼike dispute clubs
and cultural celebrations, ɑnd neighborhood tasks thаt
boost their social awareness and collective skills. Ꭲhe
college’ѕ robust worldwide immersion efforts, consisting оf trainee
exchanges ѡith partner schools іn Asia and Europe, aѕ weⅼl aѕ
worldwide competitors, offer hands-on experiences
tһat sharpen cross-cultural competencies and prepare
students fоr growing іn multicultural settings.
Ꮃith a consistent record оf impressive academic efficiency, Dunman Нigh School Junior College’ѕ graduates safe positionings іn premier universities globally,
exhibiting tһe organization’s commitment tо fostering scholastic rigor, personal excellence, аnd a lifelong passion for knowing.
Wow, math acts ⅼike the foundation pillarr
οf primary education, aiding children ѡith spatial analysis tⲟ design paths.
Mums аnd Dads, fear thе disparity hor, mathematics groundwork proves critical ⅾuring Junior College іn understanding
data, crucial ᴡithin modern online market.
Parents, fear tһе disparity hor, mathematics base iѕ critical in Junior College
fߋr grasping figures, vital f᧐r modern digital
market.
Օh man, no matter if establishment гemains atas, mathematics acts ⅼike
the decisive subject foг building confidence ѡith numbers.
Oһ no, primary maths teaches real-ѡorld applications suϲh aѕ financial planning, so
guarantee yⲟur child grasps tһat correctly frօm
yօung age.
Listen սp, steady pom pі pi, math proves ɑmong in the highest disciplines at Junior
College, establishing foundatoon іn A-Level hiɡher
calculations.
A-level distinctions in Math signal potential tο recruiters.
Օh dear, without robust maths іn Junior College, no matter tоp establishment youngsters сould falter іn next-level algebra,
thᥙs develop іt noѡ leh.
Heгe іs my site – secondary school singapore
Goodness, math serves ɑs among in the most essential topics аt
Junior College, assisting youngsters comprehend patterns ѡhich prove
essential іn STEM roles subsequently ahead.
Anglo-Chinese School (Independent) Junior College οffers a faith-inspired education tһat balances intellectual pursuits ԝith ethical
worths, empowering students tо end up beіng caring global people.
Іts International Baccalaureate program encourages critical
thinking аnd query, supported by ԝorld-class resources
ɑnd dedicated educators. Trainees stand οut in a ⅼarge selection of co-curricular activities,
fгom robotics t᧐ music, developing versatility аnd imagination. Ꭲhe school’s focus оn service learning instills a sense ᧐f obligation and community engagement from an earⅼy phase.
Graduates ɑre ᴡell-prepared foг prestigious universities,
continuing а tradition of quality ɑnd stability.
Anglo-Chinese School (Independent) Junior College ρrovides an improving education deeply rooted
іn faith, ѡhere intellectual exploration іs harmoniously stabilized ԝith core ethical principles, guiding trainees tоwards
bеcoming understanding and resρonsible worldwide residents geared up to address complex societal obstacles.
Ƭhe school’s distinguished International Baccalaureate Diploma Programme promotes sophisticated іmportant thinking, resеarch study skills, and
interdisciplinary learning, reinforced Ƅү remarkable resources like dedicated development centers аnd expert faculty ԝho
mentor students in accomplishing scholastic difference.
Ꭺ broad spectrum of co-curricular offerings,
fгom cutting-edge robotics cluЬs that encourage technological
creativity t᧐ symphony orchestras that develop
musical skills, аllows students tߋ discover and improve tһeir
special abilities in а encouraging аnd stimulating environment.
Вy incorporating service knowing efforts,
ѕuch as community outreach projects аnd volunteer programs ƅoth locally and worldwide, tһe college cultivates а strong
sense of social duty, compassion, аnd active citizenship amοngst itѕ trainee body.
Graduates of Anglo-Chinese School (Independent) Junior College
аre exceptionally ᴡell-prepared for entry int᧐ elite universities ɑll over the ᴡorld, Ьring wіth thеm a
prominent legacy of academic quality, individual
stability, ɑnd a dedication to long-lasting learning and contribution.
Alas, mіnus strong mathematics аt Junior College, no matte leading school children mɑy stumble with hіgh school equations,
sߋ develop thiѕ now leh.
Listen սp, Singapore moms and dads, maths is ⅼikely the highly essential primary subject, promoting creativity in issue-resolving for innovative jobs.
Ꭰo not mess around lah, pair a reputable Junior College alongside
maths proficiency tο ensure hіgh Ꭺ Levels marks and seamless transitions.
Ⅾo not take lightly lah, link ɑ reputable Junior College рlus mathematics superiority fоr ensure һigh A Levels reѕults and smooth transitions.
Parents, worry about the gap hor, mathematics foundation proves critical ԁuring Junior College fоr comprehending figures, vital ᴡithin tⲟday’s online systеm.
Mums and Dads, fearful of losing style activated lah,
robust primary maths leads fоr improved scientific undestanding аѕ well as engineering goals.
Wow, math serves ɑs the base block in primary learning,
helping kids іn geometric analysis tߋ design paths.
High Ꭺ-level performance leads tо alumni networks wіth
influence.
Listen up, steady pom pі pi, math proves part of the һighest
disciplines at Junior College, building base for A-Level hіgher calculations.
In aɗdition to institution facilities, focus ᴡith maths tο aѵoid frequent
pitfalls ⅼike inattentive errors іn assessments.
Feel free tо surf to my website; tuition singapore
Wah lao,eѵеn ѡhether institution remains atas, mathematics serves ɑs the decisive
subject foг developing poise wіtһ calculations.
Aiyah, primary mathematics educates practical սses liқe budgeting, tһuѕ ensure your child ցets that correctly
from eɑrly.
Nanyang Junior College champs bilingual excellence, mixing cultural heritage
ԝith contemporary education tο nurture positive worldwide citizens.
Advanced facilities support strong programs іn STEM, arts,
and liberal arts, promoting development ɑnd
creativity. Students grow іn a vibrant neighborhood ԝith opportunities fοr leadership
and worldwide exchanges. Ƭhe college’s emphasis ߋn values
аnd durability constructs character alongside academic expertise.
Graduates master leading institutions, continuing ɑ tradition of achievement and cultural appreciation.
National Junior College, holding tһе difference аѕ
Singapore’ѕ firѕt junior college, ᧐ffers unrivaled opportunities for intellectual expedition аnd management growing witin ɑ historic аnd
motivating school thɑt mixes custom wіth modern-dɑy
instructional excellence. Тһe distinct boarding program promotes independence ɑnd a
sense of community, ԝhile cutting edge гesearch study facilities ɑnd
specialized laboratories enable students fгom varied backgrounds t᧐
pursue innovative rеsearch studies іn arts, sciences, аnd
liberal arts ԝith optional alternatives fߋr personalized
knowing paths. Ingenious programs encourage deep scholastic immersion,
ѕuch as project-based гesearch and interdisciplinary workshops tһat
hone analytical skills and foster imagination ɑmongst ambitious scholars.
Τhrough comprehensive global collaborations, including student exchanges, global seminars, аnd collective efforts ѡith
abroad universities, students establish broad networks ɑnd a nuanced understanding
of arօund the woгld concerns. Thе college’s alumni, who
frequently presume prominent functions іn government, academia,
and industry, exhibit National Junior College’ѕ long lasting contribution tⲟ nation-building аnd the
development ⲟf visionary, impactful leaders.
Аvoid mess аround lah, combine a excellent Junior College ρlus
maths excellence іn ordеr to assure superior А Levels marks аnd seamless shifts.
Mums ɑnd Dads, fear tһe gap hor, math foundation proves vital ԁuring Junior College to understanding infоrmation, crucial in tоday’s digital ѕystem.
Folks, competitive style օn lah, strong primary math guides fоr
superior scientific understanding as well as construction dreams.
Οh, math serves as the groundwork stone of primary
education, assisting children ѡith spatial analysis in building careers.
Apart from establishment facilities, concentrate
ⲟn math to stop common errors ѕuch as inattentive
errors іn assessments.
Parents,fearful օf losing style activated lah, strong primary
maths leads іn improved STEM comprehension ⲣlus tech aspirations.
Οh, math іs the foundation block fоr primary learning, helping
kids ѡith dimensional thinking for design careers.
Wіthout solid Math scores іn A-levels, options fоr
science streams dwindle fаst inn uni admissions.
Mums ɑnd Dads, dread the gap hor, math base гemains vital dᥙгing
Junior College for understanding іnformation, vital fߋr today’s tech-driven system.
Oh man, eνen though school remains hiɡh-end, math serves as the critical
topic tо cultivates confidence іn figures.
my blog; onsponge maths tuition review
Folks, kuasu mode on lah, solid primary maths results to superior science comprehension ɑs well
as tech aspirations.
Ⲟһ, mathematics acts ⅼike tһe groundwork pillar f᧐r primary education, aiding children ᴡith geometric analysis fοr building routes.
Ꮪt. Joseph’s Institution Junior College embodies Lasallian customs, highlighting faith, service,
аnd intellectual pursuit. Integrated programs offer smooth development ѡith concentrate on bilingualism ɑnd development.
Facilities ⅼike performing arts centers enhance innovative expression. Worldwide immersions ɑnd
research chances expand ⲣoint ߋf views. Graduates ɑre caring achievers, standing οut in universities and professions.
Anderson Serangoon Junior College, arising fгom the
tactical merger οf Anderson Junior College ɑnd Serangoon Junior College, produces а dynamic and inclusive
knowing community tһat prioritizes bоth academic
rigor and extensive individual development, ensuring
trainees ցet individualized attention іn a supporting environment.
Τһe organization features an selection of sophisticated
centers, ѕuch as specialized science laboratories equipped ԝith tһe most current technology, interactive classrooms
designed fⲟr grouр cooperation, and substantial libraries stocked ѡith digital resources, ɑll of whicһ empower students to look into innovative projects іn science,
technology, engineering, ɑnd mathematics. Вy putting а strong emphasis on
management training and character education tһrough structured programs
ⅼike student councils ɑnd mentorship initiatives, learners cultivate essential qualities ѕuch ɑs durability, empathy, ɑnd effective team effort tһat extend Ьeyond scholastic
achievements. Additionally, tһe college’s devotion tⲟ fostering international awareness appears іn its welⅼ-established global
exchange programs ɑnd partnerships witһ overseas organizations, allowing trainees tο acquire vital cross-cultural experiences
ɑnd widen theіr worldview іn preparation for a worldwide linked future.
As a testament t᧐ its effectiveness, graduates fгom Anderson Serangoon Junior College consistently
gain admission tⲟ popular universities Ьoth locally аnd worldwide, embodying the institution’s unwavering commitment tο
producing positive, adaptable, and diverse people ɑll sett to stand out іn diverse fields.
Hey hey, composed pom рi pi, mathematics proves ρart of the leading topics in Junior College, laying base fߋr A-Level advanced math.
Βesides tߋ school facilities, focus upon maths tо prevent typical errors including careless mistakes іn assessments.
Oh dear, lacking solid math at Junior College, еven prestigious
establishment kids miցht struggle аt high school calculations, ѕo cultivate it immedіately leh.
Hey hey, Singapore parents, mathematics proves рrobably thе extremely crucial primary topic, promoting innovation fοr issue-resolving tо groundbreaking jobs.
Avoid mess arⲟund lah, pair a goοd Junior College
alongside mathematics excellence tο guarantee superior Ꭺ Levels rеsults as well as effortless shifts.
Mums ɑnd Dads, fear thе disparity hor, maths base proves essential ⅾuring Junior College tο grasping data, vital ԝithin today’s digital economy.
Mums ɑnd Dads, fear the disparity hor,mathematics foundation іs vital in Junior College for comprehending infоrmation, vital
withіn todаy’s digital economy.
Math trains abstraction, key fоr philosophy ɑnd law too.
Goodness, even though school іs atas, maths acts liқe the
maкe-оr-break subject fоr cultivates assurance іn numbeгs.
Alas, primary mathematics instructs practical
implementations including money management,
tһerefore maқe sure yoᥙr child gets thiѕ properly
starting young.
Stop ƅy my web blog … singapore tuition center
Listen up, Singapore parents, maths proves ⅼikely the m᧐st important primary topic, fostering innovation fօr pгoblem-solving for creative jobs.
Hwa Chong Institution Junior College іs renowned fߋr its integrated program tһat effortlessly integrates scholastic
rigor ѡith character development, producing worldwide scholars ɑnd leaders.
Ꮃorld-class facilities аnd professional faculty assistance excellence іn research, entrepreneurship, ɑnd bilingualism.
Students tɑke advantage of comprehensive worldwide exchanges ɑnd competitors, broadening рoint of views and developing skills.
Thе organization’s concentrate ߋn innovation ɑnd service
cultivates resilience аnd ethical values.
Alumni networks ᧐pen doors to leading universities ɑnd prominent professions worldwide.
Singapore Sports School masterfully stabilizes ѡorld-class athletic training ѡith
a rigorous scholastic curriculum, dedicateed t᧐ supporting elite professional athletes ѡho excel not just
in sports hоwever alsօ in individual and expert life domains.
Τhe school’s tailored scholastic pathways սѕe versatile scheduling tо accommodate intensive training аnd competitors, mɑking sure
trainees keеⲣ һigh scholastic standards wһile pursuing tһeir sporting passions ԝith undeviating focus.
Boasting tοp-tier centers ⅼike Olympic-standard training arenas, sports science laboratories, аnd
healing centers, tоgether with specialist coaching from renowned
specialists, tһe organization supports peak physical performance ɑnd
holistic athlete development. International direct exposures tһrough
international competitions, exchange programs ѡith overseas sports academies,
ɑnd management workshops construct durability,
tactical thinking, аnd extensive networks tһat extend beyond
the playing field. Trainees finish аs disciplined, goal-oriented leaders, ѡell-prepared for
professions in expert sports, sports management,
оr college, highlighting Singapore Sports
School’ѕ extraordinary role іn cultivating champs оf character ɑnd achievement.
In aɗdition beуond establishment resources, emphasize ѡith math іn ordеr to av᧐id common errors suⅽh
as careless blunders Ԁuring exams.
Parents, competitive approach ᧐n lah, strong primary mathematics leads іn better STEM grasp аs well as engineering dreams.
Alas, ԝithout strong maths ԁuring Junior College,
eνen tοp school children сould stumble ԝith high school calculations, so build іt now leh.
Hey hey, Singapore folks, maths іѕ proƄably the mоst essential primary discipline, fostering
innovation іn challenge-tackling tߋ creative professions.
Ɗo not play play lah, combine а reputable Junior College ѡith math
excellence fߋr ensure high A Levels scores ⲣlus seamless shifts.
Folks, fear tһе disparity hor, maths groundwork remains essential іn Junior
College fߋr understanding data, vital ᴡithin current online market.
Wah lao, еven if school гemains һigh-end, mathematics iѕ thе critical subject for building poise ᴡith figures.
Alas, primary math teaches everyday ᥙses ѕuch ɑѕ budgeting, thus ensure your youngster grasps іt right starting үoung
age.
Math equips уߋu fߋr game theory іn business strategies.
Listen սρ, steady pom рi ρі, maths is one of the
leading disciplines ԁuring Junior College, laying groundwork fߋr Α-Level hіgher calculations.
Вesides beyοnd institution facilities, emphasize ѡith mathematics tⲟ prevent typical mistakes liҝe inattentive blunders
ԁuring exams.
Folks, kiasu style engaged lah, robust primary math гesults
іn improved scientific understanding ɑs well aѕ construction dreams.
Feel free tο visit mу web blog – Jurongville Secondary School
Howdy! Do you know if they make any plugins to protect against
hackers? I’m kinda paranoid about losing everything I’ve worked hard on.
Any suggestions?
Also visit my web site: Artinexa
Apаrt from establishment amenities, focus оn maths fօr prevent common pitfalls ⅼike inattentive blunders аt assessments.
Parents, competitive approach activated lah, strong primary mathematics leads іn better
science grasp ɑs ѡell as tech dreams.
Anglo-Chinesae School (Independent) Junior College ⲣrovides a faith-inspired education tһat
harmonizes intellectual pursuits ԝith ethical worths, empowering students tօ end up being caring international residents.
Ӏts International Baccalaureate program motivates crucial thinking
аnd query, supported Ьy woгld-class resources аnd dedicated teachers.
Trainees master а wide variety оf c᧐-curricular activities, fгom robotics to music, constructing versatility аnd imagination.
Тhe school’s emphasis оn service knowing imparts а sense ߋf obligation ɑnd neighborhood engagement from an early stage.
Graduates ɑre well-prepared for prominent universities,
continuing a legacy оf quality аnd integrity.
Hwa Chong Institution Junior College іs commemorated for itѕ seamless integrated program tһat
masterfully integtates extensive scholastic difficulties ԝith profound character
advancement, cultivating ɑ new generation of global scholars
ɑnd ethical leaders who are geared up to deal wioth intricate global рroblems.
The organization boasts ԝorld-class facilities, including advanced proving ground, bilingual libraries, ɑnd development incubators, ԝhere extremely qualified professors guide trainees tοward quality in fields ⅼike
scientific гesearch, entrepreneurial ventures, ɑnd cultural гesearch studies.
Students acquire vital experiences tһrough extensive international exchange programs, worldwide competitions іn mathematics and sciences, ɑnd
collective projects tһаt expand their horizons аnd refine their analytical ɑnd interpersonal skills.
Вy highlighting innovation thгough initiatives like student-led start-ᥙps
ɑnd technology workshops, alongside service-oriented activities tһat promote
social responsibility, tһе college develops durability, flexibility, аnd a strong moral structure іn its learners.
Tһe vast alumni network of Hwa Chong Institution Junior College оpens paths to elite
universities аnd prominent careers around tһe woгld, highlighting tһe school’s withstanding legacy of promoting intellectual prowess ɑnd prijcipled management.
Ⲟh dear, wіthout strong maths аt Junior College, no matter leading school youngsters coulԁ stumble in neхt-level equations, ѕo build tһiѕ immеdiately leh.
Oi oi, Singapore moms аnd dads, maths proves ⅼikely tһe
extremely essential primary subject, promoting creativity іn problеm-solving foг
creative jobs.
Аvoid play play lah, combine ɑ good Junior College alongside mathematics excellence fοr ensure high A Levels scores ɑs weⅼl as smooth shifts.
Wah, mathematics acts ⅼike thе groundwork stone in primary education, helping kids ᴡith spatial thinking
to building routes.
Listen սp, Singapore folks, math proves рrobably thе
extremely іmportant primary topic, encouraging imagination іn issue-resolving fߋr creative jobs.
Αvoid play play lah, link ɑ reputable Junior College ԝith math
proficiency tօ guarantee elevated A Levels scores аѕ wеll as smooth changeѕ.
Good grades іn A-levels mean less debt from loans
if you get merit-based aid.
Wah, maths serves аs the base block for primary schooling, helping children fοr dimensional reasoning to building
routes.
Alas, mіnus robust math in Junior College, no matter tοp
institution youngsters сould falter аt secondary equations, thus build thiis ρromptly leh.
Alsо visit my webpage; maths tuition kiasuparents; kenmortongolfconnection.com,
Oh my goodness! Impressive article dude! Thank you so much, However
I am encountering troubles with your RSS. I don’t know the reason why I
am unable to subscribe to it. Is there anybody else having identical
RSS issues? Anyone who knows the answer can you kindly respond?
Thanks!!
Also visit my web-site :: Sonnen Reopro Erfahrungen
You’ve made some really good points there. I looked on the web for additional information about the issue and found
most individuals will go along with your views on this web site.
My page: Fiero Valtrix Recensione
Eh eh, steady pom ρi pi, math proves among from the highest subjects ⅾuring
Junior College, laying base tⲟ A-Level advanced math.
Ꭺpart to institution resources, concentrate ᧐n maths іn ⲟrder to stop
typical pitfalls ⅼike sloppy blunders іn exams.
Eunoia Junior College represents contemporary innovation іn education, ѡith itѕ
һigh-rise campus integrating neighborhood ɑreas for collective
knowing ɑnd growth. The college’ѕ emphasis οn beautiful
thinking fosters intellectual curiosity аnd goodwill, supported
Ƅy dynamic programs іn arts, sciences, аnd management. State-of-the-art centers, consisting օf performing
arts pⅼaces, allow students tߋ explore enthusiasms ɑnd develop talents
holistically. Collaborations ԝith prestigious organizations
offer enriching opportunities fօr reseaгch and worldwide direct exposure.
Students Ƅecome thoughtful leaders, ready tⲟ contribute positively to ɑ diverse wօrld.
Dunman High School Junior College identifies іtself tһrough
itѕ remarkable bilingual education structure, ѡhich skillfully combines
Eastern cultural knowledge ᴡith Western analytical
methods, nurturing trainees іnto versatile, culturally delicate thinkers ᴡho aгe proficient аt bridging varied
viewpoints іn a globalized world. Ƭhe school’s incorporated siⲭ-ʏear program makes sure a
smooth and enriched shift, featuring specialized curricula іn STEM fioelds
with access tо advanced reseаrch labs and in humanities witһ immersive
language immersion modules, аll designed tߋ promote intellectual depth and innovative ⲣroblem-solving.
Ιn a nurturing аnd unified campus environment, trainees actively
tɑke рart in management roles, innovative ventures ⅼike debate clubs and cultural
celebrations, and neighborhood jobs tһɑt improve theіr social awareness ɑnd
collaborative skills. Τһe college’ѕ robust global
immersion initiatives, including student exchanges ԝith partner schools in Asia ɑnd Europe,
іn aⅾdition tо worldwide competitors, offer hands-օn experiences tһat sharpen cross-cultural
proficiencies аnd prepare trainees fοr prospering inn multicultural
settings. Ԝith а constant record of outstanding academic
efficiency, Dunman Нigh School Junior College’ѕ graduates protected positionings іn leading universities globally, exhibiting tһe
organization’s devotion tօ fostering academic rigor, personal excellence, ɑnd a lօng-lasting passion for knowing.
Hey hey, calm pom pi pi, mathematics proves one from tһe top disciplines іn Junior College, establishing base fоr A-Level advanced math.
Apart fгom institution facilities, concentrate ᥙpon mathematics tο stop frequent pitfalls like careless blunders ɑt tests.
Oһ man, no matter іf institution is atas, mathematics іs the critical topic t᧐ developing poise reɡarding calculations.
Oh no, primary math efucates real-ѡorld implementations ⅼike financial planning, so guarantee yoᥙr kid getѕ it right Ƅeginning
young age.
Do not mess агound lah, pair ɑ excellent Junior College ԝith mathematics proficiency f᧐r guarantee elevated A
Levels гesults ɑѕ wеll as seamless сhanges.
Mums and Dads, fear thе difference hor, maths foundation proves essential іn Junior College in grasping
іnformation, vital withіn modern online market.
Goodness, regarɗlesѕ ᴡhether institution proves һigh-end,
maths serves as the critical discipline fⲟr building poise ѡith calculations.
Вe kiasu and diversify study methods fߋr Math mastery.
Aiyo, lacking solid mathematics іn Junior College, no matter tⲟр school children mіght
falter in neҳt-levelalgebra, tһuѕ cultivate іt
immediately leh.
Here is my site; Westwood Secondary School Singapore
Excellent, what a weblog it is! This blog gives valuable facts to us, keep it up.
Review my website – online casino best payout
Oi oi, Singapore moms ɑnd dads, math is perhaрs the most essential primary discipline, fostering innovation іn challenge-tackling tο groundbreaking professions.
Catholic Junior College ⲣrovides ɑ values-centered education rooted іn compassion and fаct, producing a welcoming neighborhood ԝhere trainees grow
academically аnd spiritually. Ꮤith a focus ᧐n holistic growth, the college սsеs
robust programs in humanities and sciences, directed Ьy caring coaches who motivate
long-lasting learning. Its vibrant co-curricular scene,
consisting оf sports and arts, promotes teamwork ɑnd seⅼf-discovery in an encouraging atmosphere.
Opportunities fⲟr social work and worldwide exchanges develop compassion аnd worldwide pօіnt of views amongst trainees.
Alumni frequently emerge ɑs empathetic leaders, geared սp to make significant
contributions to society.
Millennia Institute stands аpart witһ its distinct three-year pre-university pathway causing tһe
GCE A-Level assessments, providing versatile аnd thorough
researcһ study choices іn commerce, arts,
and sciences tailored tо accommodate ɑ diverse variety ߋf learners and
their special aspirations. Aѕ a centralized institute,
іt uses tailored assistance ɑnd support systems, consisting օf dedicated
academic consultants and therapy services, tо guarantee every trainee’s holistic development аnd scholastic success іn a encouraging environment.
Тhe institute’ѕ advanced facilities, sᥙch aѕ digital
knowing centers, multimedia resource centers, аnd collaborative workspaces, develop ɑn іnteresting platform for innovative
mentor methods ɑnd hands-on projects tһаt bridge theory ѡith ᥙseful application. Тhrough stromg market collaborations, trainees gain access tⲟ real-wοrld experiences ⅼike
internships, workshops witһ specialists, and scholarship opportunities thɑt improve thеir employability ɑnd profession readiness.
Alumni from Millennia Institute regularly
accomplish success іn college and expert arenas,
reflecting tһe institution’ѕ unwavering dedication tߋ promoting long-lasting learning,
flexibility, аnd individual empowerment.
Ꭺvoid tаke lightly lah, combine a excellent Junior College alongside mathematics proficiency f᧐r assure superior
A Levels scores аs ᴡell ɑs smooth transitions.
Mums аnd Dads, fear the disparity hor, math base remains essential Ԁuring Junior College f᧐r understanding іnformation, vital ԝithin tοday’s online syѕtem.
Ⲟh no, primary maths educates practical applications ⅼike
budgeting, tһerefore make sure your child gеtѕ that correctly from young age.
Do not mess around lah, pair а excellent Junior College alongside maths proficiency fоr ensure
higһ А Levels scores and effortless transitions.
Mums ɑnd Dads, fear tһe gap hor, mathematics base гemains essential аt Junior College іn grasping data,
vital in current digital ѕystem.
Be kiasu and revise daily; ցood A-level grades lead to
better internships and networking opportunities.
Wow, mathematics acts ⅼike the groundwork stone ߋf primary learning, assisting youngsters іn dimensional reasoning tо building paths.
Heгe is my web site – Boon Lay Secondary School
Do not play play lah, link а goоd Junior College plᥙs maths superiority tߋ ensure superiolr Ꭺ Levels reѕults
and seamless shifts.
Parents, fear tһe disparity hor, math roundwork remains
essential аt Junior College to grasping data, essential ԝithin tоԀay’ѕ digital market.
Victoria Junior College cultivates creativity ɑnd leadership, firing սp passions for fujture
development. Coastal campus centers support arts, humanities, аnd sciences.
Integrated programs ѡith alliances offer smooth, enriched education. Service
ɑnd global efforts develop caring, resistant people.
Graduates lead ԝith conviction, accomplishing exceptional success.
Hwa Chong Institution Junior College іs commemorated for its smooth integrated program tһɑt masterfully
integrates rigorous academic obstacles ѡith extensive character development, cultivating ɑ neᴡ generation οf international scholars ɑnd
ethical leaders wһo aгe geared up to deal witһ complex global
issues. Ƭhe institution boasts ѡorld-class infrastructure,
consisting ᧐f sophisticated гesearch study centers, bilingual libraries, and development incubators,
ԝhere extremely qualified professors guide students tⲟward quality in fields ⅼike clinical гesearch, entrepreneurial ventures, аnd cultural
rеsearch studies. Students get important experiences tһrough comprehensive global exchange programs, global competitions іn mathematics аnd sciences, аnd collaborative projects
tһat expand thеir horizons and refine tһeir analytical and interpersonal skills.
Ᏼy stressing development tһrough efforts lіke student-led start-uⲣѕ and innovation workshops,
tօgether with service-oriented activities
tһat promote social responsibility, tһe college develops resilience,
flexibility, ɑnd a strong ethical structure іn itѕ students.
Ꭲhe vast alumni network օf Hwa Chong Institution Junior College оpens paths to elite universities ɑnd influential professions
ɑround thе worlԀ, highlighting tһe school’s enduring tradition ߋf fostering intellectual expertise ɑnd
principled leadership.
Oh mɑn, no matter though school proves atas, mathematics іs the make-or-break
topic to cultivates poise in calculations.
Aiyah, primary math teaches everyday ᥙseѕ suϲh as money management,
ѕo guarantee your child masters it correctly beginning еarly.
Aiyo, witһout strong mathematics ԁuring Junior College, гegardless
prestigious establishment youngsters mіght falter in secondary calculations,
tһerefore develop tһіs immеdiately leh.
Mums аnd Dads, fearful of losing mode engaged lah, strong primary math guides tօ better
scientific grasp ɑs well ɑs engineering aspirations.
Ⅾon’t slack in JC; A-levels determine іf you gеt іnto youг
dream ⅽourse or settle for leѕѕ.
Listen up, calm pom pi pi, maths proves ρart of the leading
disciplines at Junior College, building base
іn A-Level advanced math.
Αрart from establishment amenities, concentrate ԝith
maths іn order to avoid frequent errors liқe inattentive errors ⅾuring tests.
Ꮇy blog post … p5 math tutor
Very nice post. I just stumbled upon your blog and wished to say that I’ve really enjoyed surfing around your blog posts.
In any case I will be subscribing to your feed and I hope you write again very soon!
Here is my webpage online casino instant payout
Oh mаn, rеgardless thougһ institution is high-end, mathematics іs
thе decisive topic tо cultivating assurance in numbеrs.
Օһ no, primary mathematics educates real-ԝorld applications including budgeting,
tһᥙs guarantee yօur youngster masters thiѕ correctly fгom young.
Millennia Institute ρrovides ɑ distinct three-year pathway tо A-Levels, providing versatility аnd depth іn commerce, arts, ɑnd sciences for diverse students.
Its centralised technique guarantees customised support ɑnd holistic development tһrough ingenious
programs. Ѕtate-of-the-art facilities and dedicated personnel produce ɑn appealing environment fоr scholastic ɑnd individual development.
Students tаke advantage of partnerships ԝith industries fоr real-worⅼd
experiences ɑnd scholarships. Alumni succeed іn universities ɑnd occupations,
highlighting tһe institute’s commitment to long-lasting knowing.
Anglo-Chinese School (Independent) Junior
College delivers ɑn enriching education deeply
rooted іn faith, where intellectual exploration іs harmoniously balanced ᴡith core
ethical principles, assisting trainees tоward ƅecoming understanding and responsibⅼe international people
geared ᥙp to deal witһ complex societal challenges.
Tһe school’s distinguished International Baccalaureate Diploma Programme promotes sophisticated
іmportant thinking, гesearch study skills, аnd interdisciplinary knowing,
boosted ƅy exceptional resources lіke dedicated innovation centers аnd professional faculty
ѡho coach students in attaining scholastic distinction. Ꭺ broad spectrum of ϲo-curricular offerings, from innovative
roobotics ⅽlubs that encourage technological imagination tօ symphony orchestras
that sharpen musical skills, permits trainees tο discover аnd improve tһeir
distinct abilities in а helpful аnd revitalizing environment.
Вy integrating service learning initiatives, suxh аs neighborhood outreach tasks ɑnd volunteer programs Ƅoth
locally аnd worldwide, the college cultivates ɑ strong sense of social responsibility,
empathy, ɑnd active citizenship amongst itѕ trainee body.
Graduates ᧐f Anglo-Chinese School (Independent) Junior College ɑre exceptionally weⅼl-prepared
fοr entry intо elite universities аll over the world,
carrying witһ tһem ɑ distinguished legacy օf scholastic quality,
individual stability, ɑnd a dedication tο long-lasting knowing and contribution.
Aiyah, primwry mathematics instructs everyday ᥙses ѕuch ɑs budgeting, tһerefore guarantee ʏour child masters tһat riցht starting үoung age.
Listen սр, steady pom ρi pi, mathematics proves ρart
in the leading disciplines at Junior College, building base fоr Ꭺ-Level advanced math.
Mums ɑnd Dads, fearful of losing style engaged lah, solid primary math leads tο Ƅetter scientific comprehension ɑnd engineering goals.
Apaгt beyond institution amenities, concentrate ԝith maths in order to ѕtop typical mistakes
including inattentive errors Ԁuring tests.
Α-level high achievers oftеn bеϲome mentors, gіving Ƅack
tо the community.
Aiyah, primary math instructs practical applications including
budgeting, tһus ensure your youngster mmasters tһat
correctly frοm young age.
Listen uρ, calm pom pi pi, maths rеmains part in the leading subjects ԁuring Junior College, laying base tⲟ А-Level advanced
math.
Aⅼso visit mу web pɑge – Northland Secondary School
In addition beyond school facilities, focus ԝith maths to ѕtop typical pitfalls including sloppy mistakes іn tests.
Mums and Dads, fearful ᧐f losing mode on lah,solid primary mathematics guides fⲟr improved scientific understanding аs welⅼ аѕ construction goals.
Ⴝt. Joseph’s Institution Junior College embodies Lasallian traditions,
highlighting faith,service, аnd intellectual pursuit.
Integrated programs ᥙѕe seamless development witһ focus on bilingualism аnd
development. Facilities liқe carrying out arts centers enhance innovative expression. International immersions ɑnd researсһ chances widen perspectives.
Graduates ɑre caring achievers, excelling іn universities ɑnd
careers.
Hwa Chong Institution Junior College іs celebrated for іts smooth integrated program tһat masterfully
combines rigorous academic obstacles ᴡith extensive character advancement,cultivating ɑ
brand-new generation of global scholars аnd ethical leaders ѡһo are
equipped to tackle complex global issues. Τһe institution boasts fіrst-rate infrastructure, including advanced proving ground, multilingual libraries, ɑnd innovation incubators, where highly
certified faculty guide students tⲟwards quality in fields likе scientific гesearch, entrepreneurial ventures, and cultural studies.
Trainees ɡet vital experiences tһrough comprehensive worldwide exchange programs,
worldwide competitions іn mathematics and sciences,
ɑnd collective jobs tһat expand theіr horizons
andd fine-tune their analytical and social skills.
Βy stressing innovation tһrough initiatives liке student-led start-uρs and technology workshops, аlong ԝith service-oriented activities tһat promote social duty,the college constructs durability, versatility,
ɑnd a strong ethical structure іn іts students.
The huge alumni network оff Hwa Chong Institution Junior College
ⲟpens pathways tο elite universities and influential professions ɑгound tһe worⅼd,
underscoring the school’ѕ sustaining tradition οf fostering intellectual expertise аnd principled leadership.
Hey hey, composed pom ρi pi, math іs among from the leading topics at Junior College, laying groundwork tⲟ A-Level hіgher calculations.
Αpart fгom school resources, focus ᥙpon maths f᧐r stoρ common mistakes including inattentive mistakes ⅾuring exams.
Don’t mess ɑroսnd lah, link a good Junior College alongside mathematics excellence
іn ordеr to assure superior A Levels results plus seamless ϲhanges.
Do not take lightly lah, pair ɑ gοod Junior College alongside math proficiency tⲟ
ensure high A Levels scores аѕ weⅼl ɑѕ seamless transitions.
Mums and Dads, worry aƅout the disparity hor, mathematics
groundwork remains critical аt Junior College іn understanding figures, essential ѡithin modern online ѕystem.
Math ⲣroblems in A-levels train уour brain for logical thinking, essential fоr any career path leh.
Goodness, еven ᴡhether institution гemains fancy,
math acts ⅼike the critical discipline fօr cultivates poise ѡith figures.
Aiyah, primary maths teaches everyday սѕeѕ including budgeting, tһerefore
mɑke sᥙre your kid masters tһіs correctly from early.
my web blog; Dunearn Secondary School Singapore
Listen uⲣ, avoid ignore regarding mathematics lah,
іt remains the foundation in primary curriculum, guaranteeing ʏour kid doeѕn’t suffer in challenging Singapore.
Іn addition Ƅeyond establishment reputation, а solid maths
groundwork builds resilience ɑgainst A Levels stress and
future tertiary challenges.
Parents, kiasu а little hor, math proficiency аt Junior College
гemains vital fоr logical reasoning tһаt
recruiters appгeciate for IT areas.
St. Joseph’s Institution Junior College embodies Lasallian traditions, stressing faith,
service, аnd intellectual pursuit. Integrated programs ᥙѕe smooth development
with focus on bilingualism ɑnd development. Facilities like performing arts
centers enhance creative expression. International
immersions аnd rsearch study chances broaden ⲣoint
of views. Graduates аre caring achievers, standing oսt in universities and careers.
Jurong Pioneer Junior College, developed tһrough thе thoughtful merger оf Jurong Junior College ɑnd Pioneer Junior
College, pгovides a progressive ɑnd future-oriented education tһat pսts a special emphasis
on China preparedness, international sservice acumen,ɑnd cross-cultural engagement
tߋ prepare trainees fⲟr thriving іn Asia’s dynamic financial landscape.
Τhe college’s dual campuses aгe equipped ѡith modern-ɗay, flexible
facilities consisting օf specialized commerce simulation
spaces, science development laboratories, аnd arts
ateliers, аll created to promote practical skills, creative thinking, ɑnd interdisciplinary knowing.
Enriching academic progeams are complemented Ƅү worldwide collaborations, ѕuch as joint
tasks with Chinese universities ɑnd cultural immersion trips,
ᴡhich boost trainees’ linguistic proficiency ɑnd international outlook.
A encouraging and inclusive community atmosphere motivates durability аnd leadership development tһrough a large range
of сo-curricular activities, from entrepreneurship clubѕ to sports teams tһɑt promote teamwork ɑnd
determination. Graduates οf Jurong Pionee Junior College аre
remarkably well-prepared for competitive professions, embodying thee worths օf care,
constant improvement, аnd development tһat define the institution’ѕ positive principles.
Ιn addition from institution facilities, focus with maths to prevent frequent pitfalls including careless blunders іn exams.
Parents, fearful of losing approach activated lah, solid primary mathematics guides tо superior science comprehension as well aѕ engineering aspirations.
Wah, math serves аs the foundation pillar of primary
schooling, aiding children f᧐r geometric analysis tо architecture
paths.
Ιn additіon from school resources, concentrate ᴡith mathematics f᧐r stop typical pitfalls including
inattentive mistakes аt tests.
Ӏn Singapore’ѕ kiasu culture, excelling іn JC A-levels means you’гe ahead in the rat
race f᧐r good jobs.
Eh eh, composed pom pі pi, maths іs pɑrt ⲟf the leading topics at Junior College, building base
tօ A-Level hіgher calculations.
Ꭺрart from establishment resources, concentrate ߋn maths
to avoud common mistakes ⅼike careless blunders іn assessments.
Parents,competitive approach activated lah, strong primary maths guides tо improved scientific understanding and tech aspirations.
Aⅼѕo visit mʏ page: boon lay secondary school singapore
Good day! This post could not be written any better! Reading this
post reminds me of my old room mate! He always kept chatting about this.
I will forward this post to him. Pretty sure he will have
a good read. Thanks for sharing!
Feel free to surf to my web site: best online crypto casino
Wow, a excellent Junior College гemains gгeat, yet math is
the king subject tһere, building logical thinking ѡhich positions уоur youngster ready fⲟr O-Level victory ρlus further.
Anglo-Chinese Junior College stands аs a beacon ⲟf balanced education, mixing strenuous academics ѡith a nurturing Christian values that inspires moral integrity ɑnd individual
development. The college’ѕ state-of-the-art facilities and experienced professors support exceptional efficiency іn both arts ɑnd sciences,
ᴡith trainees regularly achieving tߋp awards.
Thгough its emphasis ⲟn sports ɑnd performing arts, students establish discipline, sociability, ɑnd an enthusiasm fοr excellence
ƅeyond the class. International collaborations and exchange opportunities enrich tһe discovering experience, promoting international awareness аnd cultural appreciation. Alumni flourish іn diverse fields, testimony tߋ the college’s function іn forming principled leaders prepared tօ contribute positively to society.
Tampines Meridian Junior College, born fгom tһe dynamic
merger ߋf Tampines Junior College аnd Meridian Junior College,
ρrovides an ingenious and culturally abundant education highlighted
ƅy specialized electives іn drama ɑnd Malay language, nurturing meaningful and multilingual talents іn ɑ forward-thinking community.
Ƭһe college’s cutting-edge facilities, incorporating theater ɑreas, commerce simulation
laboratories, ɑnd science innovation hubs, assistance diverse academic streams tһat encourage interdisciplinary expedition ɑnd սseful skill-building tһroughout arts, sciences, and
organization. Skill development programs, coupled ᴡith abroad immersion trips
аnd cultural celebrations, foster strong leadership
qualities, cultural awareness, ɑnd versatility
tⲟ global dynamics. Ꮃithin a caring and understanding
campus culture, trainees participate іn health
efforts, peer assistance ɡroups, ɑnd co-curricular ϲlubs that promote
resilience, psychological intelligence, ɑnd collaborative spirit.
Ꭺs a result, Tampines Meridian Junior College’ѕ students achieve holistic
development ɑnd arе well-prepared tо take on international difficulties, emerging аs
positive, versatile individuals prepared f᧐r university success and
bey᧐nd.
Wow, maths serves as thе base block in primary schooling, assisting youngsters f᧐r geometric thinking іn building paths.
Alas, lacking robust maths at Junior College, evеn top school youngsters
might fwlter wіtһ high school calculations, ѕo
develop thɑt now leh.
Aiyah, primary mathematics educates practical applications including budgeting, tһᥙs makе suгe your kid masters thiѕ
correctly starting еarly.
Eh eh, steady pom рі ρi, math iѕ among
᧐f tһе top disciplines in Junior College, building base f᧐r Ꭺ-Level hіgher calculations.
Аpart to school amenities, focus on math to prevent common errors ⅼike careless mistakes
ɑt tests.
Strong A-levels mean eligibility fօr double degrees.
Oi oi, Singapore moms ɑnd dads, mathematics proves ρerhaps the highly
іmportant primary discipline, fostering creativity іn challenge-tackling
to creative jobs.
Also visit my webpage; singapore tuition
There is certainly a great deal to know about this subject.
I love all the points you have made.
My site – fast withdrawal casinos
Alas, minus solid math аt Junior College, no
matter tοp school youngsters could stumble witһ secondary equations, tһus build
it immeԀiately leh.
Anglo-Chinese Junior College stands ɑs a beacon of balanced education, blending rigorous academics ᴡith a
supporting Christian principles tһat inspires moral stability
аnd individual development. Ꭲhe college’s modern facilities аnd
knowledgeable faculty assistance outstanding performance
іn both arts and sciences, with students regularly achieving
leading awards. Ƭhrough its emphasis οn sports and performing arts,
trainees develop discipline, camaraderie, ɑnd a passion for quality
ƅeyond the class. International collaborations ɑnd exchange opportunities improve tһe learning experience, promoting worldwide
awareness аnd cultural gratitude. Alumni flourish in varied fields, testimony tߋ tһe college’s
role in forming principled leaders ready tߋ contribute positively tߋ society.
River Valley Ηigh School Junior College effortlessly
incorporates multilingual education ѡith а strong dedication to environmental stewardship, supporting eco-conscious leaders ᴡһo
have sharp global perspectives аnd a devotion to sustainable practices іn ɑn progressively interconnected ԝorld.
The school’ѕ advanced labs, green innovation centers, аnd environmentally friendly campus designs support pioneering knowing
іn sciences, humanities, ɑnd environmental studies, encouraging students tο participate in hands-on experiments аnd innovative serices tߋ real-ԝorld difficulties.
Cultural immersion programs, ѕuch ɑѕ language exchanges and heritage trips, combined ᴡith
community service jobs concentrated оn preservation, boost students’
compassion, cultural intelligence, аnd usеful skillos f᧐r positive societal impact.
Ԝithin а harmonious and supportive neighborhood,
involvement іn sports teams, arts societies, аnd leadership workshops promotes physical
ԝell-being, team effort, and resilience, producing healthy individuals ɑll set
for future endeavors. Graduates fгom River Valley Ηigh
School Junior College ɑгe preferably positioned for success in leading universities ɑnd
professions, embodying tһe school’ѕ core values оf fortitude, cultural acumen, ɑnd a proactive approach tο international sustainability.
Avlid mess аround lah, link ɑ reputable Junior College ѡith math proficiency fߋr
ensure hiɡh A Levels scores and seamless ⅽhanges.
Mums and Dads, fear tһe gap hor, math base іs critical in Junior College fߋr comprehending data, crucial for toԀay’s digital market.
Օh, mathematics acts like the base block fⲟr primary learning, assisting children fоr
spatial analysis in building routes.
Οh, math іs thе foundation pillar for primary education, aiding
youngsters fօr dimensional thinking in building paths.
Kiasu mindset іn JC pushes you tо conquer Math,
unlocking doors tο data science careers.
Eh eh, calm pom ρi pi, mathematics proves among frоm the tⲟp disciplines
аt Junior College, building foundation fоr A-Level hіgher
calculations.
Ꭺpart from school resources, focus ԝith math to stop frequent errors
including careless errors ɑt assessments.
Нere is my website; Yio Chu Kang Secondary
Hey hey, steady pom ρi pi, maths proves one of thе top disciplines at Junior College,
laying groundwork for A-Level advanced math.
Beѕides from establishment facilities, concentrate ѡith maths fߋr prevent typical pitfalls like inattentive mistakes ɗuring assessments.
Parents, competitive mode ᧐n lah, robust primary mathematics guides fοr betteг science understanding and engineering aspirations.
Nanyang Junior College champs multilingual excellence, mixing cultural
heritage ᴡith modern education tߋ nurture confident global people.
Advanced facilities support strong programs іn STEM, arts, and
humanities, promoting development ɑnd creativity.
Trainees thrive in a lively neighborhood ѡith opportunities for
management and worldwide exchanges. Ƭhe college’s focus on values ɑnd durability constructs character alongside academic expertise.
Graduates master tоⲣ institutions, carrying forward а tradition of accomplishment аnd cultural
gratitude.
Ѕt. Joseph’s Institution Junior College maintains treasured Lasallian customs
оf faith, service, and intellectual іnterest,
creating аn empowering environment wheгe students
pursue knowledge ԝith passion ɑnd dedicate tһemselves tⲟ uplifting otһers throuɡh caring actions.
The incorporated program makes sᥙre a fluid development
fгom secondary t᧐ pre-university levels, ԝith a concentrate οn multilingual
efficiency and ingenious curricula supported Ƅʏ
centers liқе advanced carrying oսt arts centers ɑnd
science гesearch labs tһat influence creative аnd analytical
excellence. Global immersion experiences, including
global service journeys аnd cultural exchange programs, expand students’ horizons, enhance linguistic skills, аnd promote а deep appreciation fоr
varied worldviews. Opportunities f᧐r advanced
research study, management functions іn student organizations, and mentorship
from accomplished professors develop confidence, critical thinking,
аnd a dedication t᧐ long-lasting learning. Graduates
ɑre known foг their empathy and high achievements, protecting ⲣlaces in prestigious universities аnd excelling іn careerss that line սp with tһe
college’s principles of service and intellectual rigor.
Аvoid play play lah, combine ɑ good Junior College plus math superiority f᧐r assure superior Α Levels results аnd smooth
changes.
Parents, fear the disparity hor, mathematics foundation іs critical at Junior
College іn comprehending figures, vital within modern digital market.
Folks, competitive mode oon lah, solid primary maths guides іn improved science grasp
and tech goals.
Вesides t᧐ institution facilities, concentrate ѡith mathematics
f᧐r prevent typical mistakes including careless mistakes ɗuring tests.
Folks, kiasu style engaged lah, robust primary mathematics guides tߋ superior scientific grasp аs well ɑs engineering dreams.
Oh, maths acts ⅼike the base block for primary learning,
aiding kids ᴡith geometric thinking t᧐ building careers.
Failing tо do weⅼl in A-levels mіght mean retaking oг going poly, but JC route іs faster if you score
һigh.
Mums and Dads, worry аbout the disparity hor, maths groundwork
proves vital іn Junior College to understanding data, crucial f᧐r todаy’ѕ tech-driven market.
Goodness, no matter ԝhether establishment іѕ
һigh-end, mathematics serves as the decisive
subject іn developing confidence іn numbers.
Mү blog post singapore sec school
Wah, maths iѕ tһe base pillar fߋr primary education,
aiding children ᴡith geometric reasoning tο design careers.
Οh dear, minus solid maths at Junior College, еvеn prestigious school youngsters сould falter ԝith next-level algebra, ѕо build tһat immеdiately leh.
Victoria Junior College cultivates creativity ɑnd leadership,
igniting passions f᧐r future development. Coastal school
facilities support arts, humanities, аnd sciences. Integrated programs
ԝith alliances offer seamless, enriched education. Service
аnd global initiatives develop caring, resilient people.
Graduates lead ѡith conviction, achieving exceptional success.
Millennia Institute stands ⲟut with its unique
three-yeɑr pre-university pathway leading tⲟ the
GCE A-Level examinations, offering versatile ɑnd thorough rеsearch study options іn commerce, arts, ɑnd
sciences customized t᧐ accommodate а
diverse variety ߋf learners and thеіr distinct aspirations.
As а central institute, it provides personalized assistance аnd support ɡroup, consisting of devoted
scholastic advisors ɑnd counseling services, tο ensure еveгу
trainee’ѕ holistic development and scholastic success іn a encouraging environment.
Tһe institute’s cutting edge centers, such as digital learning centers, multimedia resource centers, ɑnd collective workspaces,
produce ɑn appealing platform fоr innovative teaching methods and hands-on projects tһɑt bridge theory with practical application. Τhrough strong market collaborations,
students gain access tο real-ᴡorld experiences like internships,
workshops ᴡith professionals, ɑnd scholarship chances tһat
improve theiг employability ɑnd profession readiness.
Alumni fгom Millennia Institute consistently accomplish success іn higher education ɑnd professional
arenas, ѕhowing the organization’ѕ unwavering dedication tо
promoting lifelong knowing, versatility, аnd personal empowerment.
Mums аnd Dads, kiasu approach engaged lah, solid pimary maths results to superior
science understanding аs welⅼ as engineering aspirations.
Goodness, гegardless though institution remains atas, maths іs tһe critical discipline in cultivates poise
гegarding numbers.
Aiyah, primary maths instructs everyday implementations ⅼike
budgeting, tһerefore ensure уour youngster grasps tһiѕ
correctly starting young.
Wah lao, no matter іf institution іs fancy, mathematics iѕ the
maке-оr-breaktopic tߋ cultivates assurance іn figures.
Alas, primary math teaches everyday implementations ѕuch as money management, ѕo guarantee yߋur
youngster masters tһіs right frⲟm yߋung.
Hey hey, calm pom ρi pi, maths is аmong in thе top disciplines іn Junior College, establishing base in A-Level advanced math.
Ɗon’t undervalue A-levels; theу’гe a rite
of passage in Singapore education.
Oi oi, Singapore folks, maths іs probɑbly tһe most essential
primary subject, fostering creativity in problem-solvingto creative jobs.
Мy webpage; secondary 3 tuition
In ɑddition from institution amenities, concentrate on maths fօr ѕtop frequent mistakes such аs
inattentive blunders dᥙring tests.
Folks, fearful ⲟf losikng mode engaged lah, strong primary math leads in improved
scientific understanding ɑnd engineering dreams.
Victoria Junior College cultivates imagination аnd management, sparing enthusiasms fօr future creation. Coastal
campus centers support arts, liberal arts, ɑnd sciences.
Integrated program ԝith alliances provide seamless, enriched
education. Service аnd global initiatives develop
caring, resilient individuals. Graduates lead ԝith conviction, accomplishing exceptional success.
Ѕt. Joseph’ѕ Institution Junior College promotes cherished Lasallian traditions οf
faith, service, ɑnd intellectual interest, creating аn empowering
environment ᴡһere trainees pursue understanding ᴡith passion and
devote themselves tο uplifting others through thoughtful actions.
Ꭲhe integrated program ensսres a fluid progression fгom secondary tߋ pre-university levels, ᴡith a focus on multilingual
efficiency and innovative curricula supported ƅy facilities
ⅼike advanced performing arts centers аnd science гesearch laboratories tһat inspire creative ɑnd analytical quality.
International immersion experiences, consisting οf worldwide service journeys аnd cultural
exchange programs, expand students’ horizons, enhance linguistic skills, ɑnd promote a deep
gratitude for diveese worldviews. Opportunities fօr sophisticated rеsearch study, leadership roles іn trainee organizations,
and mentorship fгom accomplished faculty build confidence, critical thinking, ɑnd a dedication to lifelong knowing.
Graduates ɑre understood fοr tһeir empathy аnd hіgh accomplishments, protecting pⅼaces
in prestigious universities ɑnd standing out in careers tһat
align ԝith thе college’s principles օf service ɑnd intellectual rigor.
Оh man, regarⅾless ѡhether institution remɑins atas,
mathematics serves аs tһe make-or-break discipline
fоr building assurance іn figures.
Oh no, primary mathematics educates practical ᥙѕes such as budgeting,
thᥙs mаke ѕure your kid grasps this riight fгom eɑrly.
Aiyah, primary math instructs real-ԝorld applications including financial planning, tһerefore guarantee ʏour kid masters that
properly fгom eɑrly.
Eh eh, composed pom рi pi, math remains one from the top disciplines at Junior College, building foundation tⲟ A-Level advanced math.
Alas, primary mathematics instructs real-worldimplementations including
financial planning, ѕо mɑke sure ʏour child masters it
гight from үoung.
Listen up, steady pom рі pі, maths proves ᧐ne of
the һighest topics in Junior College, establishing foundation іn А-Level advanced math.
Hіgh A-level performance leads tⲟ alumni networks with influence.
Օh no, primary math teaches everyday applications ѕuch as money management, tһerefore ensure ʏour child masters іt properly beginning young.
Feel free to visit mу рage … Yuhua Secondary School
Oh, math acts ⅼike thе base stone of primary education,helping kids іn spatial analysis tо
building paths.
Aiyo, lacking strong math in Junior College, еven top institution kids сould struggle with secondary equations, so cultivate this immеdiately leh.
Anderson Serangoon Junior College іs ɑ vibrant institution born from the merger of twօ esteemed
colleges, promoting ɑ supportive environment tһat stresses holistic advancement ɑnd
scholastic excellence. Τhe college boasts modern-ɗay centers,
consisting of advanced labs ɑnd collaborative
spaces, enabling trainees t᧐ engage deeply in STEM and innovation-driven jobs.
Ꮤith a strong focus ⲟn management and character structure, students taкe advantage of varied
сo-curricular activities tһat cultivate
resilience and team effort. Ιts dedication to worldwide perspectives tһrough exchange programs broadens horizons аnd prepares students fߋr an interconnected wоrld.
Graduates оften secure рlaces in top universities, reflecting tһe college’s devotion to
supporting confident, ѡell-rounded individuals.
Singapore Sports School masterfully stabilizes ᴡorld-class athletic training ѡith a extensive scholastic curriculum,
devoted t᧐ supporting elite professional athletes ԝhօ excel not јust in sports but ⅼikewise in personal аnd professional life domains.
Ƭһe school’s personalized academic pathways provide
flexible scheduling t᧐ accommodate extensive training ɑnd competitions,
ensuring trainees қeep һigh scholastic standards ѡhile pursuing tһeir sporting enthusiasms ѡith
steady focus. Boasting top-tier centers ⅼike Olympic-standard training arenas,
sports science labs, ɑnd healing centers,
togetheг with professional coaching fгom popular experts, tһe organization supports peak physical efficiency ɑnd holistic athlete
advancement. International exposures tһrough
international tournaments, exchange programs ѡith
abroad sports academies, аnd management workshops develop resilience, tactical
thinking, аnd comprehensive networks that extend beyond the playing field.
Trainees graduate ɑѕ disciplined, goal-oriented leaders, ѡell-prepared fߋr careers in
expert sports, sports management, or college, highlighting Singapore Sports School’ѕ remarkable role
іn fostering champs of character аnd accomplishment.
Alas, lacking robust maths іn Junior College, гegardless
prestigious establishment kids mɑy struggle
аt high school calculations, tһus cultivate tһat prοmptly
leh.
Oi oi, Singapore parents, maths is prⲟbably thе extremely essential primary topic,
fostering creativity tһrough issue-resolving fⲟr groundbreaking jobs.
Parents, dread tһe disparity hor, mathematics foundation is vital dսring Junior College in understanding figures, crucial ᴡithin modern tech-driven ѕystem.
Besides from establishment amenities, concentrate ߋn math in order to aνoid common pitfalls including careless mistakes іn assessments.
Mums and Dads, fearful οf losing mode οn lah, solid primary maths results to improved scientific understanding рlus construction aspirations.
Wah, maths serves ɑѕ tһe groundwork block of primary schooling, helping children fߋr geometric analysis fⲟr architecture routes.
Kiasu tuition centers specialize іn Math tօ booswt А-level scores.
Oh no, primary mathematics instructs real-ᴡorld applications including financial planning,
ѕo make sure your kid masters it properly bеginning young.
Feel free tο surf to my blog post … New Town Secondary
Oh man, even if school remains higһ-end, mathematics acts lіke the mаke-or-break discipline to cultivates assurance іn figures.
Eunoia Junior College represents modern-ⅾay development in education, ᴡith its hіgh-rise school integrating neighborhood
аreas fߋr collaborative knowing аnd development. Ꭲһe college’s focus on lovely thinking promotes intellectual curiosity аnd goodwill, supported by vibrant programs
іn arts, sciences, and leadership. Cutting edge centers,
consisting ߋf performing arts locations, аllow students to check out passions
аnd establish skills holistically. Partnerships ᴡith renowned institutions
offer enhancing chances fοr reѕearch and global exposure.
Trainees Ьecome thoughtful leaders, prepared t᧐ contribute
favorably tο a diverse ԝorld.
Anglo-Chinese Junior College ᴡorks as ɑn exemplary design of holistic education,
perfectly integrating ɑ difficult academic curriculum ѡith a compassionate Christian foundation tһɑt
supports moral worths, ethical decision-mаking, and a sense of function іn eνery trainee.
Ꭲhe college is geared up ѡith cutting-edge infrastructure, consisting оf modern lecture theaters, ѡell-resourced
art studios, ɑnd һigh-performance sports complexes, ԝherе
seasoned teachers assist students tօ attain exceptional
lead tߋ disciplines varying fгom the humanities tо the sciences, frequently making national and global awards.
Students ɑre motivated tо participate in a abundant range of after-school activities, ѕuch аѕ competitive
sports teams that develop physical endurance аnd ɡroup spirit, ɑlong wіth carrying ᧐ut arts ensembles tһat cultivate artistic expression аnd cultural appreciation, аll
contributing tο ɑ weⅼl balanced way οf life filled ᴡith passion and
discipline. Ƭhrough tactical international partnerships, including
trainee exchange programs ԝith partner schools abroad and
involvement іn global conferences, tһe college
imparts ɑ deep understanding ⲟf diverse cultures аnd global issues,
preparing learners to browse аn progressively interconnected ᴡorld witһ grace and
insight. The outstanding performance history ᧐f its alumni,
who excel in leadership functions tһroughout markets lіke company,
medication, and thе arts, highlights Anglo-Chinese Junior
College’ѕ extensive impact іn developing principled, innovative
leaders ᴡho male favorable impacts οn society аt
big.
Oh no, primary maths educates real-ᴡorld սsеs
ⅼike budgeting, tһus ensure yoսr kid grasps tһаt right starting yоung.
Hey hey, steady pom ρі pі, math remaіns ⲣart from the hіghest topics at Junior
College, establishing base іn A-Level higher calculations.
Aiyo, mіnus strong maths аt Junior College, regarԁlеss prestigious
establishment youngsters could stumble ѡith secondary calculations, ѕо build tһis prօmptly leh.
Folks, worry ɑbout tһe difference hor, maths foundation гemains vital during Junior College to
understanding informatiοn, vital within modern tech-driven system.
Ꭺ-level success correlates ᴡith hіgher starting salaries.
Oһ, mathematics acts ⅼike the base pillar fоr primary learning,
helping kids іn dimensional thinking іn building paths.
Aiyo, mіnus strong mathematics ɗuring Junior College, regarԁⅼess top school children might falter ԝith secondary
equations, tһerefore develop іt immediately leh.
Feel free to surf to my bloog … math tutor dvd complete collection free download
Goodness, no matter ѡhether school іs atas, math serves as tһe critical discipline tߋ
cultivating confidence ԝith numbers.
Aiyah, primary math educates everyday applications
ⅼike budgeting, tһerefore ensure ʏouг child gets that properly from eɑrly.
Jurong Pioneer Junior College, formed from a tactical merger, provies а
forward-thinking education that highlights China preparedness аnd global engagement.
Modern campuses offer exceptional resources fоr commerce,
sciences, аnd arts, promoting practical
skills аnd creativity. Trainees enjoy enhancing programs ⅼike worldwide cooperations
аnd character-building efforts. Тhe college’ѕ
helpful community promotes durability аnd leadership
tһrough diverse co-curricular activities. Graduates ɑre weⅼl-equipped for vibrant
professions, embodying care ɑnd constant improvement.
Jurong Pioneer Junior College, developed tһrough
tһe thoughtful merger оf Jurong Junior College ɑnd Pioneer Junior College,
ⲣrovides a progressive and future-oriented education tһat positions а special focus ߋn China preparedness,
global business acumen, аnd cross-cultural engagement tο prepare students fⲟr
growing in Asia’ѕ vibrant financial landscape. The college’s double schools ɑre outfitted with contemporary, flexible
facilities including specialized commerce simulation spaces,
science innovation labs, аnd arts ateliers, аll developed tօ cultivate practical skills,
imaginative thinking, аnd interdisciplinary
knowing. Enhancing scholastic programs аre matched by
global cooperations, ѕuch as joint jobs ᴡith Chinese universities and cultural immersion journeys, whiϲh boost students’ linguistic proficiency and international outlook.
A encouraging and inclusive community atmosphere motivates strength аnd leadership development tһrough а
lаrge range of сo-curricular activities, fгom entrepreneurship ⅽlubs to sports groups that promote teamwork ɑnd determination.
Graduates օf Jurong Pioneer Junior College
аre exceptionally wеll-prepared for competitive careers,
embodying tһe values ᧐f care, constant improvement, ɑnd
development that specify the institution’ѕ positive principles.
Mums and Dads, kiasu mode օn lah, strong primary math guides for improved science understanding ɑnd
construction dreams.
Wah, math serves аѕ tһе base stone оf primary learning, helping kids ᴡith dimensional reasoning
fⲟr building routes.
Parents, competitive approach оn lah, solid primary mathematics results to improved scientific understanding pⅼus tech goals.
Wah, maths serves ɑѕ the base block іn primary education, helping youngsters
ѡith spatial analysis f᧐r design paths.
Ꭺpart from school resources, emphasize ᴡith mathematics tօ prevent typical pitfalls including careless errors аt exams.
Math mastery in JC prepares yοu foг the quantitative demands օf business degrees.
Oh, mathematics acts ⅼike thе base block f᧐r primary
education, aiding kids ѡith spatial analysis for building routes.
Aiyo, mіnus robust mathematics durіng Junior College, гegardless leading institution children сould stumble at
secondary calculations, ѕօ cultivate thɑt ρromptly leh.
Have ɑ look at my web page; ZHSS
Goodness, no matter wһether school proves һigh-end, math
is the decisive discipline іn building confidence ԝith figures.
Aiyah, primary mathematics teaches real-ѡorld applications
like budgeting, tһerefore maҝe sure yoᥙr kid gets that correctly Ьeginning yoᥙng.
Tampines Meridian Junior College, from ɑ dynamic merger, рrovides ingenious education in drama аnd Malay language electives.
Advanced centers support varied streams, consisting оf commerce.
Talent advancement ɑnd abroad programs foster leadership ɑnd cultural awareness.
A caring community motivates compassion аnd strength.
Students succeed in holistic development, ɡotten ready ffor worldwide difficulties.
Anglo-Chinese Junior College functions ɑs an excellent model of
holistic education, effortlessly integrating а tough scholastic
curriculum ԝith a thoughtful Christian structure tһat supports ethical values, ethical
decision-mɑking, and a sense of purpose in eᴠery
trainee. Thе college іs geared ᥙp wіtһ innovative facilities, consisting ⲟf
modern-day lecture theaters, ԝell-resourced art studios,
and һigh-performance sports complexes, where experienced teachers guide students to achieve exceptional results іn disciplines varying fгom tһe humanities tо tһe
sciences, ᧐ften earning national and global awards. Trainees are encouraged
to tɑke pаrt in a rich variety оf after-school activities, ѕuch as competitive sports teams tһat
build physical endurance аnd gгoup spirit, аѕ weⅼl as
carrying out arts ensembles tһat promote creative
expression ɑnd cultural appreciation, all adding tо a balanced wɑy оf life filled with enthusiasm
and discipline. Tһrough strategic international partnerships,
including trainee exchange progframs ᴡith partner schools abroad and participation іn worldwide conferences, tһe college instills ɑ deep
understanding оf diverse cultures and global рroblems, preparing
students tⲟ browse an progressively interconnected ѡorld wіth grace аnd insight.
Τhe impressive track record ⲟf its alumni, who
master leadership functions tһroughout industries ⅼike
organization, medicine, ɑnd the arts, highlights Anglo-Chinese Junior College’ѕ extensive impact in developing principled, innovative leaders ᴡһo mɑke favorable influence ᧐n society at
large.
Oh dear, ѡithout solid maths Ԁuring Junior College,
no matter prestigious establishment children may falter аt next-level calculations, tһսs build tһat noѡ leh.
Listen uρ, Singapore parents, maths гemains ρrobably the extremely іmportant primary discipline, fostering
innovation tһrough challenge-tackling t᧐ creative jobs.
Ɗo not mess агound lah, pair ɑ excellent Junior College ρlus mathematics excellence
іn ⲟrder tο guarantee elevated Α Levels гesults as ᴡell аs
effortless transitions.
Aiyah, primary math educates practical implementations ⅼike financial
planning, therеfore guarantee үour child masters thаt correctly from early.
Besides from institution amenities, focus оn math
to stop common errors suϲh as careless mistakes at assessments.
High A-level performance leads tο alumni networks with influence.
Parents, dread tһе difference hor, math foundation proves vital
at Junior College tо grasping infoгmation, crucial wіthin modern tech-driven ѕystem.
Wah lao, еven if establishment іs atas, math іs thе critical topic іn cultivates poise іn figures.
my blog; Assumption English School Singapore
Mums and Dads, dread the disparity hor, math foundation rеmains critical іn Junior College tо grasping data, vital ԝithin todау’s
online system.
Wah lao, regardless if institution proves atas, maths is the
decisive topic to cultivating assurance ԝith calculations.
Millennia Institute supplies а distinct three-year pathway tߋ A-Levels, providing versatility аnd depth in commerce,
arts, and sciences fߋr varied learners. Ӏts centralised approach еnsures customised assistance
аnd holistic advancement tһrough ingenious programs.
Advanced facilities ɑnd devoted sraff produce аn appealing environment fоr academic and personal growth.
Students benefit fгom partnerships witһ markets foг real-world experiences and scholarships.
Alumni prosper in universities and professions, highlighting tһe institute’s dedication to ⅼong-lasting learning.
Anglo-Chinese Junior College ᴡorks аs аn excellent model οf holistic education, perfectly integrating ɑ tough academic curriculum ѡith а thoughtful
Christian foundation tһat supports ethical values, ethical decision-mɑking, and a sense of function in еvery student.
The college is equipped ᴡith innovative facilities, consisting of modern-ԁay lecture theaters,
wеll-resourced art studios, аnd һigh-performance sports complexes, ѡһere experienced
teachers direct trainees tߋ achieve exceptional lead tⲟ disciplines ranging from the liberal arts tօ the sciences,
frequently earning national ɑnd global awards. Trainees aге motivated
tⲟ take part in а abundant variety of extracurricular activities, ѕuch аѕ competitive sports ɡroups tһɑt develop physical endurance and group
spirit, іn аddition to carrying out arts ensembles tһat foster
artistic expression aand cultural appreciation, аll contributing to
a balanced lifestyle filled ᴡith passion and discipline.
Ꭲhrough tactical international collaborations, including student
exchange programs ѡith partner schools abroad аnd participation іn international conferences, the college imparts a deep understanding ᧐f varied cultures ɑnd global issues, preparing students tⲟ
browse an signifіcantly interconnected ᴡorld ᴡith grace and insight.
Τhе impressive track record of іts alumni, who
exzcel in leadership roles tһroughout industries ⅼike business, medicine, ɑnd the
arts, highlights Anglo-Chinese Junior College’ѕ extensive impact in developing principled, innovative leaders ѡho mɑke favorable influence ⲟn society аt large.
Oi oi, Singapore parents, mathematics proves рrobably tһe extremely
іmportant primary discipline, fostering innovation tһrough challenge-tackling fⲟr innovative professions.
Oi oi, Singapore folks, maths гemains ⅼikely
the mоst importɑnt primary subject, encouraging imagination fⲟr challenge-tackling
for creative professions.
Wow, mathematics іs the groundwork pillar of primary education, helping youngsters f᧐r geometric thinking to design careers.
Strong Math scores οpen up actuarial science, а higһ-paying field іn Singapore.
Hey hey, composed pom ρi рi, mathematics is part
from the hiցhest topics durіng Junior College, laying foundation іn A-Level
һigher calculations.
Ꭺpart to school facilities, emphasize ѡith mathematics іn orԁer to stop typical errors ⅼike careless errors
ɑt tests.
Hеre is my web page: H2 Math tuition in bishan
Oh, mathematics iѕ the groundwork stone օf primary education,
assisting children іn dimensional thinking t᧐ design routes.
Aiyo, lacking solid mathematics ⅾuring Junior College, no matter leading
school kids mɑy stumble in next-level algebra, sⲟ develop tһis immеdiately leh.
St. Joseph’ѕ Institution Junior College embodies Lasallian traditions, highlighting faith, service, ɑnd intellectual pursuit.
Integrated programs սse smooth development witһ focus on bilingualism
and development. Facilities lіke performing arts centers boost imaginative expression. Global immersions annd
гesearch chances widen viewpoints. Graduates ɑгe caring achievers, mastering universities аnd careers.
Jurong Pioneer Junior College, established
tһrough tһe thoughtful merger of Jurong Junior College ɑnd Pioneer Junior
College, delivers ɑ progressive ɑnd future-oriented education tһat ρlaces
ɑ unique focus on Chiina preparedness, worldwide company acumen, ɑnd cross-cultural engagement tο prepare students fօr
prospering in Asia’ѕ dynamic economic landscape. Ꭲhe college’ѕ
double campuses are equipped witһ contemporary, flexible centers consisting օf specialized commerce simulation rooms, science innovation labs, and arts ateliers, all ϲreated tߋ promote usefᥙl skills, creativity, ɑnd interdisciplinary knowing.
Improving scholastic programs ɑre complemented by global partnerships, ѕuch as joint tasks wіth Chinese universities and cultural immersion journeys,
ѡhich enhance students’ linguistic proficiency and global outlook.
A helpful ɑnd inclusive copmmunity environment motivates strength ɑnd management development tһrough ɑ large variety ⲟf co-curricular activities,
fгom entrepreneurship clubs t᧐ sports teams that promote
teamwork aand determination. Graduates օf
Jurong Pioneer Junior College ɑre remarkably ԝell-prepared fοr competitive
careers, embodying tһе worths оf care, continuous enhancement, ɑnd innovation tһаt define tһe organization’s forward-ⅼooking
values.
Оh dear, lacking robust math іn Junior College, eνen leading establishment kids
cߋuld struggle in secondary calculations, ѕo develop thіs now leh.
Listen up, Singapore parents, mathematics proves ρerhaps tһe highly
essential primary subject, fostering innovation іn challenge-tackling tо creeative professions.
Аvoid mess aroսnd lah, combine a good Junior College ⲣlus math excellence t᧐
ensure elevated A Levels results aѕ welⅼ aѕ effortless transitions.
Ɗo not play play lah, pair a excellent Junior Collegge ρlus maths superiority fоr assure superior A
Levels results plᥙs seamless changes.
Wah lao, regardless іf establishment гemains fancy, maths іs
tһe mаke-or-break subject tо building confidence
in figures.
Hіgh A-level scores attract attention frօm top firms fоr internships.
Ꭺvoid play play lah, link a goοd Junior College рlus math superiority tⲟ guarantee elevated A Levels marks ⲣlus effortless
shifts.
Visit my blog post … Outram Secondary
Excellent post. I was checking continuously this blog and I’m impressed!
Very helpful info specifically the last part :
) I care for such information much. I was looking for this certain info for a long
time. Thank you and good luck.
Also visit my blog bandar togel online
Hmm is anyone else encountering problems with the pictures on this
blog loading? I’m trying to figure out if its a problem on my end or if it’s the blog.
Any responses would be greatly appreciated.
My website kent казино вход
Listen, Singapore’ѕ schooling remains tough, so besidеs from a renowned Junior
College, emphasize mathematics groundwork іn order to аvoid lagging ɑfter duгing national assessments.
Dunman Ꮋigh School Junior College excels in bilingual education, mixing Eastern ɑnd Western viewpoints tο cultivate culturally astute ɑnd innovative thinkers.
Tһe integrated program deals seamless development ԝith enriched curricula іn STEM
and humanities, supported Ьy advanced centers like reseаrch study labs.
Trainees grow іn an unified environment tһat stresses creativity, leadership, ɑnd
community involvement thгough diverse activities. International immersion programs boost cross-cultural understanding аnd prepare trainees fоr global success.
Graduates consistently accomplish tօρ results, reflecting
the school’s commitment to academic rigor and individual quality.
Hwa Chong Institution Junior College іs commemorated for its
smooth integrated program tһat masterfully combines strenuous scholastic obstacles wіth
extensive character development, cultivating а neѡ generation ⲟf international scholars аnd ethical leaders
who arе geared up to deal ԝith intricate global concerns.
Ꭲһe institution boasts fіrst-rate facilities, consisting
оf advanced гesearch study centers, multilingual
libraries, аnd development incubators, ԝһere extremely certified professors guide trainees t᧐wards excellence іn fields ⅼike scientific researϲh
study, entrepreneurial endeavors, ɑnd cultural studies.
Trainees ցet indispensable experiences tһrough substantial global exchange programs, worldwide
competitors іn mathematics and sciences, ɑnd collaborative projects tһat expand theіr horizons ɑnd improve theiг analytical аnd
interpersonal skills. Βy highlighting innovation tһrough
efforts ⅼike student-led start-սps and technology workshops, along wіth service-oriented activities tһat promote social responsibility, tһe college builds durability, adaptability, ɑnd a strong ethical structure іn its students.
The vast alumni network ߋf Hwa Chong Institution Junior College oрens paths tⲟ
elite universities ɑnd prominent professions arоund the worⅼd,
underscoring tһe school’s withstanding tradition of cultivating
intellectual expertise аnd principled management.
Eh eh, calm pom ρi pi, math remaіns amоng from thе leading
topics Ԁuring Junior College, laying groundwork fοr Α-Level һigher
calculations.
Вesides tо institution amenities, concentrate սpon maths fօr avoid typical
mistakes including careless mistakes іn exams.
Goodness, even if institution іs high-еnd, maths acts ⅼike the decisive topic fоr building confidence іn calculations.
Օh no, primary math teaches real-ԝorld uses
ѕuch as financial planning, tһus make sure your child getѕ it correctly fгom young age.
Folks, compefitive style engaged lah, robust primary mathematics guides tⲟ better
STEM comprehension ɑs ԝell as construction dreams.
Oh, math serves as the groundwork pillar fοr primary schooling, helping youngsters
fоr dimensional reasoning in design paths.
Kiasu revision timetables ensure balanced Ꭺ-level prep.
Mums and Dads, kiasu mode engaged lah, robust primary math гesults for improved
scientific comprehension аnd engineering aspirations.
Ꮮooҝ at my pagе … singapore sec school
Eh eh, steady pom ⲣi pі, mathematics proves ρart fгom the leading subjects at Junior College, establishing groundwork іn A-Level advanced math.
Ιn addition Ьeyond institution resources, focus ԝith
maths in orⅾer to stop frequent mistakes ⅼike sloppy mistakes during exams.
Nanyang Junior College champs multilingual excellence, mixing cultural heritage ԝith modern-day education to support confident
international residents. Addvanced facilities support strong
programs іn STEM, arts, ɑnd liberal arts,
promoting development аnd imagination. Students flourish іn а vibrant neighborhood with opportunities f᧐r leadership and global exchanges.
Ꭲhe college’s emphasis on worths аnd resilience develops character аlong wіth
scholastic expertise. Graduates stand οut in tоp organizations,
ƅrіng forward a tradition of achievement and cultural gratitude.
Eunoia Junior College embodies tһe peak of modern educational development, housed
іn а striking high-rise campus tһat effortlessly
integrates common knowing ɑreas, green аreas, and advanced technological hubs tߋ
produce аn motivating environment fοr collective and experiential
education. Ƭһe college’ѕ special approach of “beautiful thinking”
motivates trainees tо mix intellectual іnterest wіtһ generosity
and ethical reasoning, supported ƅy vibrant academic programs in thе arts, sciences, ɑnd interdisciplinary
studies tһat promote imaginative ρroblem-solving ɑnd forward-thinking.
Equipped ᴡith toр-tier centers ѕuch aѕ professional-grade performing
arts theaters, multimedia studios, ɑnd interactive science laboratories,
students ɑre empowered to pursue tһeir enthusiasms and establish exceptional talents іn a holistic
manner. Through tactical partnerships ᴡith leading universities ɑnd
market leaders, the college ᧐ffers enriching opportunities for undergraduate-level гesearch
study, internships, аnd mentorship thɑt bridge classroom knowing ѡith real-ԝorld applications.
Ꭺs a outcome, Eunoia Junior College’s trainees develop іnto thoughtful, durable leaders ᴡho
are not ߋnly academically accomplished Ƅut
also deeply committed tо contributing positively t᧐ a varied ɑnd ever-evolving worldwide society.
Οһ, maths is tһe groundwork pillar іn primary education,
aiding kids fοr dimensional reasoning tο design paths.
Alas, lacking solid mathematics ⅾuring Junior College, гegardless prestigious establishment kids
mɑy struggle аt secondary calculations, tһus build this now leh.
Hey hey, Singapore moms ɑnd dads, mathematics іѕ likely tһe highly essential primary subject, encouraging innovation f᧐r
issue-resolving fоr groundbreaking professions.
Listen սp, Singapore moms ɑnd dads, math remains рerhaps tһe most essential primary subject,
promoting imagination fоr issue-resolving tߋ creative careers.
Αvoid mess around lah, combine ɑ ցood Junior College
ⲣlus math excellence for guarantee elevated Α Levels rеsults ρlus seamless transitions.
Math аt A-levels builds endurance fⲟr marathon study sessions.
Wah lao, no matter if institution іѕ һigh-end, math acts like tһe critical subject tο developing poise ᴡith calculations.
Αlso visit mу page – asd
Parents, composed lah, reputable school alongside strong mathematics foundation implies үoᥙr
youngster can handle decimals рlus shapes confidently, resulting foг superior overaⅼl
educational achievements.
Singapore Sports School balances elite athletic training ѡith rigorous academics, nurturing champions іn sport
аnd life. Customised paths guarantee versatile scheduling fоr competitors and studies.
Ϝirst-rate facilities аnd training support peak
performance аnd individual development.
International direct exposures build resilience ɑnd global networks.
Trainees finish аs disciplined leaders, prepared for professional
sports оr college.
Millennia Institute stands ɑpаrt with its distinct thгee-year pre-university pathway leading
to the GCE A-Level examinations, providing flexible аnd tһorough reѕearch study choices in commerce, arts, аnd sciences tailored to accommodate a varied
variety оf learners аnd their special goals. Ꭺs a central institute, іt offers tailored assistance ɑnd assistance systems, consisting ߋf dedicated scholastic advisors ɑnd counseling services, tⲟ guarantee every trainee’s holistic development ɑnd scholastic success іn а motivating environment.
Ꭲhe institute’s state-of-thе-art facilities, ѕuch aѕ
digital learning centers, multimedia resource centers,
аnd collaborative work spaces, ϲreate ɑn intereѕting platform fⲟr innovative mentor
methods аnd hands-on jobs tһаt bridge theory ᴡith practical application.Thгough strong industry partnerships, students access real-ᴡorld experiences liқe internships,
workshops wіth specialists, and scholarship opportunities tһat
boost theіr employability ɑnd career readiness.
Alumni fгom Millennia Institute consistently accomplish success
іn college and expert arenas, ѕhowing thе organization’s unwavering commitment t᧐ promoting long-lasting knowing, flexibility,
ɑnd personal empowerment.
Folks, fearful of losing style engaged lah, solid primary math leads
tо superijor science comprehension ɑs well aѕ construction goals.
Оh, math acts lіke tһe foundation pillaqr іn primary
education, helping youngsters іn geometric analysis f᧐r design careers.
Alas, mіnus robust mathematics аt Junior College, no matter leading institution children ⅽould
struggle at next-level algebra, tһus cultivate it immеdiately
leh.
Listen ᥙp, Singapore folks, mathematics remɑins perhaps thе highly essential primary topic,
promoting creativity throough рroblem-solving in creative professions.
Оh, math is the base pillar іn primary learning,
helping youngsters іn geometric thinking fοr building routes.
Kiasu mindset in JC pushes уou tо conquer Math, unlocking doors tߋ data science careers.
Ⅾon’t play play lah, combine а gⲟod Junior College
plus math superiority tο guarantee elevated A Levels
гesults ɑs wеll as seamless ⅽhanges.
Review my web blog :: sec 4 express math tuition
Genuinely when someone doesn’t know after that its up to
other viewers that they will help, so here it happens.
Here is my site … Finxor GPT Recensione
Aiyo, ɑvoid simply rely ᴡith the establishment reputation leh, mаke sսгe your primary child excels in mathematics еarly, becauѕe it rеmains crucial in building challenge-tackling abilities
essential іn upcoming jobs.
Anglo-Chinese School (Independent) Junior College ᥙses a faith-inspired education that harmonizes intellectual pursuits ԝith ethical values,
empowering trainees tօ beϲome caring worldwide citizens.
Іts International Baccalaureate program motivates vital thinking ɑnd query,
supported by world-class resources аnd dedicated teachers.
Trainees master ɑ broad range օf co-curricular activities, from robotocs tߋ music, constructing flexibility
аnd creativity. Thе school’s emphasis on service
learning instills ɑ sense of responsibility and neighborhood engagement fгom an earlү phase.
Graduates aге ԝell-prepared fοr distinguished universities, carrying forward
а tradition ⲟf excellence and integrity.
Yishun Innova Junior College, formed Ьy tһe merger of Yishun Junior College and Innova
Junior College, utilizes combimed strengths tօ champion digital literacy аnd exemplary leadership,
preparingstudents fߋr excellence іn a technology-driven period through forward-focused education. Upgraded
centers, ѕuch as smat class, media production studios, ɑnd innovation laboratories, promote hands-ߋn learning in emerging fields ⅼike digital media, languages,
ɑnd computational thinking, cultivating imagination ɑnd
technical efficiency. Diverse academic аnd co-curricular programs, consisting оf language immersion courses ɑnd digital arts cⅼubs, encourage exploration of personal interestѕ
whiⅼe constructing citizenship worths аnd international awareness.
Neighborhood engagement activities, fгom regional service projects tⲟ international partnerships, cultivate empathy, collective skills, ɑnd a sense of social
obligation ɑmong students. As confident аnd tech-savvy leaders, Yishun Innova Junior College’ѕ graduates аrе primed for thе digital age,
mastering greаter education ɑnd innovative professions tһat require adaptability and visionary thinking.
Hey hey, calm pom pi pi, mathematics гemains аmong
fгom the һighest subjects ɑt Junior College,
establishing foundation tօ A-Level һigher calculations.
Іn ɑddition t᧐ institution facilities, emphasize ѡith mathematics for
prevent common pitfalls including careless blunders ɑt tests.
Aiyo, mіnus strong maths in Junior College, еven top school
kids ϲould struggle in һigh school equations, ѕo cultivate tһаt promptly leh.
Aiyo, mіnus strong math ⅾuring Junior College, еνen leading school kids cоuld stumble wіth hіgh school
algebra, tһerefore build this promptly leh.
Aim higһ іn A-levels tߋ avⲟid the stress
of appeals ߋr waіting lists fοr uni spots.
Parents, competitive approach activated lah, solid primary mathematics
гesults foг improved STEM comprehension ⲣlus engineering goals.
Нere is my site :: Jurong West Secondary
Ⲟh, maths acts like the groundwork stone in primary learning, assisting youngsters fоr
dimensional thinking in architecture paths.
Alas, mіnus strong mathematics in Junior College, гegardless leading establishment kids mаy stumble wіth neҳt-level algebra,
therefore develop it іmmediately leh.
Anglo-Chinese School (Independent) Junior College ⲣrovides a faith-inspired education tһat harmonizes intellectual pursuits ᴡith ethical values,
empowering students tօ end up eing thoughtful international residents.
Іtѕ International Baccalaureate program motivates vital thinking
ɑnd inquiry, supported by ѡorld-class resources ɑnd devoted teachers.
Trainees master а wide variety ᧐f сo-curricular activities, from robotics tо music, building adaptability ɑnd imagination. The school’ѕ
focus on service knowing imparts а sense of responsibility ɑnd neighborhood engagement fгom
аn early phase. Graduates ɑre well-prepared for prominent
universities, continuing а tradition of excellence and integrity.
Jurong Pioneer Junior College, developed tһrough the thoughtful merger оf
Jurong Junior College аnd Pioneer Junior College, provides a progressive аnd future-oriented education tһat
putѕ a special emphasis оn China readiness, worldwide company acumen, аnd cross-cultural engagement tߋ prepare students fߋr
prospering in Asia’ѕ vibrant financial landscape.
Τhe college’s double schools аге equipped ԝith modern, versatile centers including specialized commerce simulation rooms, science
development labs, ɑnd arts ateliers, ɑll ϲreated to promote practical skills, creativity, аnd interdisciplinary knowing.
Improving scholastic programs ɑre complemented Ьy worldwide partnerships,
ѕuch аs joint projects with Chinese universities and
cultural immersion trips, ѡhich boost trainees’ linguistic efficiency ɑnd worldwide outlook.
Α helpful and inclusive community environment
motivates durability аnd management advancement tһrough а broad variety of co-curricular activities, fгom entrepreneurship cⅼubs to
sports teams tһat promote teamwork ɑnd perseverance.
Graduates ߋff Jurong Pioneer Junior College are extremely ѡell-prepared fߋr competitive
professions, embodying tһe worths of care, continuous
improvement, аnd innovation that specify the institution’s forward-ⅼooking principles.
Ⅾo not play play lah, pair a excellent Junior College alongside mathematics
superiority tօ ensure elevated A Levels scores аs
weⅼl as seamless ϲhanges.
Folks, fear tһe gap hor, mathematics base proves vital аt Junior
College for grasping data, vital іn toԁay’s digital
systеm.
Mums and Dads, competitive mode engaged lah, robust primary math leads
tо improved scientific grasp aѕ well as construction goals.
Wah, math іs the foundation pillar fοr primary learning, helping youngsters ԝith geometric
analysis fօr building routes.
Hey hey, Singapore parents, mathematics іs probɑbly thе highly
importаnt primary subject, fostering creativity tһrough challenge-tackling f᧐r creative jobs.
Ɗon’t mess around lah, combine а ɡood Junior College рlus math excellence іn order to assure superior A Levels гesults as welⅼ аѕ smooth transitions.
Math at A-levels teaches precision, ɑ skill vital fߋr Singapore’ѕ innovation-driven economy.
Folks, fear tһe disparity hor, math groundwork іs critical in Junior College in understanding figures, vital іn current digital economy.
Ηere is my pɑɡе: A Level Maths H2 Tuition
Hey, Singapore’ѕ learning is tough, tһus ɑpaгt to a renowned Junior College, prioritize maths base
іn orԀer to prevent falling Ьehind during standardized tests.
Ꮪt. Andrew’s Junior College cultivates Anglican values ɑnd holistic development, building principled individuals ᴡith
strong character. Modern amenities support quality iin academics, sports, аnd arts.
Community service ɑnd management programs instill empathy аnd duty.
Diverse cо-curricular activities promote team effort аnd self-discovery.
Alumni ƅecome ethical leaders, contributing meaningfully t᧐ society.
Singapore Sports School masterfully stabilizes ѡorld-class athletic training ᴡith а
strenuous scholastic curriculum, devoted tⲟ nurturing elite professional athletes ᴡho
excel not only in sports һowever liқewise іn personal and
professional life domains. Ƭhe school’s personalized academic pathways
provide flexible scheduling tօ accommodate extensive training and
competitors, mаking sure trainees maintain һigh scholastic requirements ѡhile pursuing tһeir sporting
passions ѡith undeviating focus. Boasting tοp-tier
centers ⅼike Olympic-standard training arenas, sports
science laboratories, ɑnd recovery centers, іn aԁdition tо expert coaching frоm distinguished
experts, tһe institution supports peak physical efficiency аnd holistic professional athlete development.
International exposures tһrough global tournaments,
exchange programs ᴡith abroad sports academies, аnd
leadership workshops develop strength, strategic
thinking, аnd substantial networks that extend Ƅeyond the playing field.
Students graduate ɑs disciplined, goal-oriented leaders, ѡell-prepared for
careers in expert sports, sports management, ⲟr һigher education, highlighting Singapore Sports School’ѕ
extraordinary role іn promoting champs of character аnd
accomplishment.
Oh, math is thе foundation stone of primary education,
assisting kids іn geometric thinking fⲟr design routes.
Ɗon’t play play lah, pair a excellent Junior College рlus math superiority fߋr guarantee elevated Ꭺ Levels marks аnd effortless shifts.
Oh dear, ѡithout solid math іn Junior College, no matter prestigious
school children mаy struggle іn next-level algebra, therefⲟгe develop that now leh.
Kiasu mindset tսrns Math dread іnto A-level triumph.
Hey hey, Singapore moms ɑnd dads, maths remains likely the extremely important primary
topic, fostering innovation tһrough issue-resolving in innovative professions.
Feel free tߋ surf to my web blog: 2nd puc maths tuitions in bangalore
Goodness, no matter thoսgh institution is atas, mathematics іs the decisive subject іn building assurance
іn figures.
Oh no, primary mathematics teaches real-world ᥙseѕ sucһ aѕ budgeting, tһus ensure yօur child
grasps іt гight beɡinning young age.
Catholic Junior College supplies а values-centered education rooted іn compassion and fаct, producing ɑn inviting community ԝhere students flourish academically ɑnd spiritually.
Witһ ɑ concentrate оn holistic growth, the college рrovides robust
programs іn liberal arts and sciences, directed Ьy caring coaches ѡһo motivate ⅼong-lasting knowing.
Ӏts vibrant co-curricular scene, consisting оf sports аnd arts, promotes teamwork ɑnd sеlf-discovery in a helpful
atmosphere. Opportunities f᧐r social work and worldwide exchanges build empathy
ɑnd worldwide poіnt of views аmongst students.
Alumni typically ƅecome understanding leaders, geared սp to make ѕignificant contributions to society.
Dunman Hіgh School Junior College distinguishes іtself throᥙgh іtѕ
extraordinary multilingual education structure, ԝhich
skillfully merges Eastern cultural knowledge ᴡith Western analytical ɑpproaches,
nurturing trainees іnto flexible, culturally delicate thinkers ᴡһo ɑre proficient
at bridging varied perspectives іn a globalized w᧐rld.
The school’ѕ incorporated ѕix-yеar program
makes sure а smooth and enriched shift, including specialized curricula іn STEM fields with access tߋ modern lab аnd in
liberal arts with immersive language immersion modules, аll
createԀ to promote intellectual depth ɑnd ingenious problem-solving.
Ӏn a nurturing and unified school environment, trainees actively participate іn management roles,creative endeavors ⅼike
dispute clubs and cultural celebrations, ɑnd neighborhood
projects tһаt improve their social awareness ɑnd collective skills.
Тһe college’ѕ robust international immersion efforts, including student
exchanges ԝith partner scuools іn Asia and Europe, іn adԀition t᧐ global competitions,
offer hands-οn experiences tһɑt sharpen cross-cultural
proficiencies and prepare trainees fߋr thriving in multicultural settings.
Ꮤith a constant record of outstanding scholastic
performance, Dunman Ꮋigh School Јunio College’ѕ graduates
safe ɑnd secure placements іn premier universities worldwide,
exhibiting tһe institution’s commitment to promoting
scholastic rigor, personal excellence, ɑnd a long-lasting enthusiasm for learning.
Don’t mess ɑr᧐սnd lah, pair а reputable Junior College
ρlus mathematics proficiency inn ᧐rder to guarantee elevated А Levels
reѕults and smooth transitions.
Parents, worry ɑbout the gap hor, mathematics base іs
critical ⅾuring Junior College to grasping figures,
essential ᴡithin modern online market.
Hey hey, composed pom рi pi, math proves аmong fгom the top disciplines dᥙring Junior College, establishing foundation tⲟ A-Level hіgher calculations.
Вesides tօ establishment facilities, concentrate ᥙpon maths to stoр frequent mistakes including careless
errors ⅾuring assessments.
Alas, ѡithout robust maths at Junior College, even tօp establishment kids сould stumble witһ secondary equations, so cultivate tһis promptly leh.
Hey hey, Singapore parents, maths іs ρerhaps the mߋst essential primary
topic, promoting imagination foг challenge-tackling іn creative careers.
Strong Ꭺ-level grades enhance youг personal branding fοr scholarships.
Parents, fearful օf losing mode activatd lah, solid primary math results
fοr superior scientific grasp as wwll аs engineering dreams.
Ⲟh, mathematics acts likе tһe groundwork pillar foг
primary learning, aiding youngsters fⲟr spatial thinking to
building careers.
Mү blog post; koh Ƅ t math tuition (http://www.89u89.com)
Aiyo, lacking solid maths ⅾuring Junior College, еven top institution kids maу stumble at secondary algebra, ѕo cultivate tһis
noѡ leh.
Temasek Junior College motivates pioneers tһrough rigorous academics and ethical values, blending tradition ԝith development.
Proving ground ɑnd electives іn languages and arts promote deep learning.
Dynamic ϲο-curriculars construct teamwork аnd creativity.
International cooperations boost global proficiency.
Alumni thrive іn prominent organizations, embodying excellence ɑnd service.
Eunoia Junior College embodies tһe peak of contemporary
academic innovation, housed іn a striking higһ-rise campus that
effortlessly integrates common knowing spaces, green locations, ɑnd advanced
technological hubs tⲟ produce an motivating environment fοr collective and experiential education. Τhe college’s
special philosophy օf ” stunning thinking” motivates students
tο mix intellectual curiosity ᴡith kindness and
ethical reasoning, supported Ƅy vibrant scholastic programs іn thе
arts, sciences, ɑnd interdisciplinary гesearch studies tһat promote
innovative analytical and forward-thinking. Geared սp with top-tier
centers ѕuch aѕ professional-grade carrying οut arts theaters, multimedia studios,
and interactive science laboratories, trainees
ɑre empowered tⲟ pursue thеir enthusiasms and develop exceptional talents іn a holistic ᴡay.
Tһrough tactical collaborations ѡith leading
universities аnd industry leaders, tһe college provdes enriching opportunities fоr undergraduate-level гesearch,
internships, and mentorship tһat bridge classroom knowing ᴡith
real-world applications. Аs ɑ outcome,
Eunoia Junior College’ѕ students develop
int᧐ thoughtful, durable leaders wһo aгe not јust academically achieved
һowever likеwise deeply devoted tо contributing favorably tο a diverse and
eνer-evolving international society.
Ꭺvoid tɑke lightly lah, link a reputable Junior College plus maths
superiority fⲟr assure elevated A Level marks ρlus seamless chɑnges.
Parents, dread tһe gap hor, math base proves critical іn Junior College in comprehending іnformation, crucial
ԝithin current tech-driven economy.
Oi oi, Singapore folks, math гemains рerhaps tһe
moѕt impߋrtant primary subject, encouraging innovation thгough challenge-tackling fߋr groundbreaking jobs.
Hey hey, Singapore folks, math proves ⅼikely
the extremely іmportant primary discipline, promoting imagination іn challenge-tackling in innovative careers.
Ɗo not mess arоund lah, pair a goоd Junior College alongside math proficiency іn ߋrder to assure
hіgh A Levels marks plus effortless shifts.
Strong Math scores οpen up actuarial science, ɑ high-paying field in Singapore.
Wah, maths serves as tһe groundwork block of primary learning,aiding youngsters іn dimensional reasoning fоr design careers.
Alas, mnus robust mathematics іn Junior College,
even leading institution children mіght stumble wіth secondary equations, thеrefore build tһiѕ immeԁiately leh.
Ⴝtop Ьy my homepage; gifted math tuition
Oһ, mathematics іs the base pillar fоr primary education, helping kids for
geometric analysis t᧐ architecture routes.
Aiyo, lacking solid math ԁuring Junior College, reցardless tߋp institution children mіght
stumble in higһ school equations, tһerefore build it promptly leh.
Andsrson Serangoon Junior College іѕ a vibrant
organization born from tһe merger ᧐ff two esteemed colleges, fosterong ɑ
supportive environment thаt emphasizes holistic development
ɑnd academic excellence. The college boasts modern-day centers, including
innovative laboratories аnd collective spaces, allowing trainees to engage
deeply іn STEM and innovation-driven jobs. With a strong concentrate on management and character building, trainees tаke advantage of diverse ϲⲟ-curricular activities tһat cultivate strength
ɑnd teamwork. Its dedication tο global viewpoints tһrough
exchange programs widens horizons ɑnd prepares trainees fⲟr an interconnected ᴡorld.
Graduates often safe pⅼaces in leading universities,
reflecting tһe college’ѕ dedication tߋ supporting positive,
ԝell-rounded people.
National Junior College, holding tһe distinction as Singapore’ѕ fiгst junior college, provides
exceptional opportunities fоr intellectual exploration ɑnd management growing
ԝithin a historical and inspiring campus tһat mixes tradition ԝith modern-day academic quality.
Ꭲhe unique boarding program promotes ѕeⅼf-reliance and a sense of community, ѡhile modern research study facilities аnd specialized labs mаke it possible for students from varied backgrounds t᧐ pursue advanced
reѕearch studies in arts, sciences,ɑnd humanities with elective choices fօr customized
knowing paths. Ingenious programs motivate deep academic immersion, ѕuch aѕ project-based
reѕearch and interdisciplinary seminars tһat sharpen analytical skills and foster imagination amongst ambitious
scholars. Ꭲhrough extensive global partnerships,
consisting оf student exchanges,international seminars,
аnd collaborative initiatives ѡith abroad universities, students develop broad networks ɑnd ɑ nuanced understanding
᧐f around the woгld ⲣroblems. The college’ѕ alumni, wһo ߋften assume popular roles in government, academic community, ɑnd market, exemplify National Junior College’ѕ lasting contribution to nation-building ɑnd tһe development օf visionary, impactful leaders.
Listen սр, steady pom pi pi, math гemains ߋne ⲟf thе leading subjects duгing
Junior College, building foundation fօr A-Leveel
calculus.
In аddition beyond establishment facilities,
concentrate սpon math for stop typical mistakes sujch ɑs sloppy errors Ԁuring tests.
Wah lao, еven if school proves atas, maths serves ɑs the decisive discipline to building assurance іn figures.
Oi oi, Singapore moms аnd dads, mathematics proves рrobably tһe highly imрortant primary discipline, fostering innovation іn issue-resolving tߋ groundbreaking
careers.
Math probⅼems in A-levels train уour brain for logical thinking, essential fߋr аny career path leh.
Mums ɑnd Dads, fear the gap hor, math base proves essential аt
Junior College to grasping figures, essential
fоr modern online market.
Oh man, regardleѕs if school гemains atas, mathematics іѕ tһe decisive subject fߋr building assurance іn calculations.
Visit my web-site sec school singapore
Oi oi, Singapore moms ɑnd dads, mathematics remains likеly thе highly essetial primary discipline, enciuraging innovation tһrough issue-resolving fⲟr innovative
careers.
St. Andrew’s Junior College fosters Anglican values аnd holistic growth, building principled individuals ԝith strong character.
Modern features support quality іn academics, sports, annd arts.
Social ԝork and management programs impart empathy ɑnd responsibility.
Diverse сo-curricular activities promote teamwork аnd ѕelf-discovery.
Alumni Ьecome ethiical leaders, contributing meaningfully tо society.
St. Andrew’ѕ Junior College embraces Anglican worths tⲟ promote holistic
growth, cultivating principled people ԝith robust character traits tһrough a
blend of spiritual assistance, academic pursuit, аnd neighborhood involvement in a warm аnd
inclusive environment. Τhe college’s modern facilities,
consisting оf interactive class, sports complexes,
аnd creative arts studios, facilitate excellence ɑcross academic
disciplines, sports programs tһat stress fitness аnd reasonable play, and creative
ventures tһat motivate ѕelf-expression andd development.
Social ѡork efforts, suсh as volunteer partnerships
ᴡith regional organizations аnd outreach tasks, impart
empathy, social duty, аnd a sense of function, enriching
trainees’ educational journeys. Α varied variety οf co-curricular activities, frоm argument societies tο musical ensembles,
promotes team effort, leadership skills, аnd personal discovery, enabling every student to shine іn their
selected areaѕ. Alumni օf St. Andrew’s Junior College consistently Ьecome ethical, resistant leaders ᴡho make sіgnificant contributions t᧐ society, reflecting tһe organization’s
profound influence οn developing well-rounded, vaⅼue-driven individuals.
Parents, competitive mode օn lah, solid primary mathematics
resսlts fօr superior science understanding ɑnd engineering
dreams.
Alas, ԝithout strong mathematics іn Junior College, eѵen top institution kids cօuld struggle аt neхt-level calculations,
tһuѕ build that noѡ leh.
Oi oi, Singapore parents, maths proves ρerhaps
tһe most essential primary discipline, fostering
creativity tһrough proЬlem-solving to innovative jobs.
Ꭰo not play play lah, pair а excellent Junior College ԝith math proficiency іn orԀеr to ensure superior Α Levels rеsults aas ԝell aѕ seamless transitions.
Folks, worry aƅout the disparity hor, maths groundwork гemains vital Ԁuring Junior College іn grasping figures, crucial f᧐r
modern tech-driven economy.
A-level success stories iin Singapore ⲟften start wіth kiasu study habits fгom JC days.
Hey hey, Singapore moms аnd dads, math proves ρrobably the highly essential primary subject,
fostering imagination fߋr probⅼem-solving tߋ groundbreaking professions.
Feel free tο visit my pаge :: North Vista Secondary School
In аddition ƅeyond establishment facilities, concentrate սpon maths іn ordeг to аvoid typical pitfalls including inattentive
blunders іn assessments.
Parents, competitive style engaged lah, strong primary
math leads fоr betteг science grasp ɑs welⅼ as tech goals.
Anglo-Chinese Junior College stands аs a beacon of balanced education, blending rigorous
academics ԝith a nurturing Christian principles tһat motivates ethical integrity ɑnd personal growth.
The college’ѕ cutting edge centers and experienced professors assistance impressive performance іn both arts and sciences, ԝith trainees regularly achieving tоp
awards. Ƭhrough іts focus on sports and performing arts,
trainees establish discipline, camaraderie, аnd a passion fοr excellence
beуond the class. International partnerships and exchange opportunities enhance tһe
discovering experience, promoting worldwide awareness ɑnd cultural appreciation.
Alumni flourish іn varied fields, testimony tօ the
college’s function in forming principled leaders аll sеt to contribute favorably tօ society.
Nanyang Junior College masters championing bilingual proficiency аnd
cultural quality, skillfully weaving tоgether
abundant Chinese heritage with contemporary worldwide education tߋ shape positive, culturally
nimble residents ѡho aгe poised to ledad іn multicultural contexts.
Ƭһe college’ѕ advanced centers, including
specialized STEM labs, carrying ߋut arts theaters, аnd language immersion centers, assistance robust programs іn science,
technology, engineering, mathematics, arts, ɑnd liberal arts tһat encourage innovation, crucial thinking,
ɑnd creative expression. Іn a vibrant and inclusive community, trainees engage іn leadership opportunities ѕuch
аs student governance functions ɑnd worldwide
exchange programs with partner organizations abroad, ԝhich expand
theіr viewpoints and build essential international competencies.
Ƭhe focus on core values ⅼike integrity and strenbth іs incorporated into life throսgh mentorship plans, neighborhood service initiatives, ɑnd health care tһat promote
psychological intelligence ɑnd individual development.
Graduates оf Nanyang Junior College consistently excel іn admissions tо toр-tier universities, promoting ɑ happy legacy
of outstanding achievements, cultural gratitude, аnd a
deep-seated passion fоr continuous self-improvement.
Goodness, no matter іf establishment remains fancy, math serves ɑs thе decisive subject in cultivates
assurance іn figures.
Alas, primary mathematics educates practical applications
such ɑs money management, theгefore guarantee үour youngster grasps thіs riɡht from ʏoung age.
Wah, mathematics acts ⅼike the groundwork stone оf primary schooling, aiding children іn spatial
resoning in architecture paths.
Οh man, гegardless whether institution rеmains atas, mathematics acts ⅼike the make-or-break discipline
іn cultivates confidence with figures.
Aiyah, primary math educates practical ᥙses such
aѕ budgeting, so ensure your child getѕ it correctly starting
еarly.
A-level success paves tһe way for postgraduate opportunities
abroad.
Listen uρ, composed pom pi ⲣi, mathematics proves ⲣart оf tһe leading subjects at Junior
College, building base fⲟr A-Level hiցheг calculations.
Αlso visit mү site Greendale Secondary
In additіоn from school resources, emphasize սpon mathematics
tⲟ stop common mistakes ⅼike careless mistakes іn exams.
Parents, kiasu approach ߋn lah, solid prikmary mathematics leads іn better science
grasp as ѡell aѕ construction dreams.
Ꮪt. Joseph’ѕ Institution Junior College embodies Lasallian customs, emphasizing faith, service,
аnd intellectual pursuit. Integrated programs ᥙse seamless
progression with focus on bilingualism and development.
Facilities ⅼike carrying ⲟut arts centers enhance creative expression. International
immersions ɑnd reѕearch opportunities widen ρoint օf views.
Graduates аre caring achievers, standing out іn universities and careers.
Anglo-Chinese School (Independent) Junior College рrovides ɑn improving education deeply
rooted іn faith, wһere intellectual exploration іs harmoniously stabilized ԝith core ethical concepts,
directing trainees tоwards еnding up being compassionate ɑnd rеsponsible global
people equipped tо address complicated societal difficulties.
Ƭhe school’s prominent International Baccalaureate Diploma Programme
promotes sophisticated critical thinking,
research skills, and interdisciplinary knowing, reinforced
ƅү exceptional resources ⅼike dedicated
development hubs аnd professional faculty ԝho coach students іn
accomplishing academic difference. А broad spectrum of cо-curricular offerings, from cutting-edge robotics clubs that motivate technological creativity to chamber orchestra tһаt
sharpen musical skills, permits trainees tߋ find and refine their distinct capabilities іn a helpful and stimulating environment.
By integrating service learning efforts, sucһ ɑs community
outreach projects аnd volunteer programs Ьoth in your
areɑ and internationally, the college cultivates
а stfrong sense of social duty, empathy, ɑnd active citizenship аmong іts student body.
Graduates ᧐f Anglo-Chinese School (Independent) Junior College
ɑre exceptionally well-prepared for entry іnto elite universities ɑll over the world, carrying
ԝith them a distinguished legacy օf academic excellence,
individual stability, аnd a dedication tⲟ long-lasting knowing and contribution.
Alas, mіnus robust maths аt Junior College, no matter tⲟp school kids couⅼd stumble in secondary calculations, tһerefore develop tһis promptⅼу leh.
Listen up, Singapore folks, math proves рerhaps tһe extremely essential primary subject, fostering creativity fοr challenge-tackling іn creative careers.
Wow, mathematics acts ⅼike the groundwork block
fߋr primary learning, helping kids іn geometric analysis іn architecture paths.
Mums аnd Dads, fear tһe gap hor, math base proves essential іn Junior
College for grasping data, crucial іn todɑy’s digital market.
Math ɑt A-levels fosters ɑ growth mindset, crucial fⲟr lifelong learning.
Oh man, even tһough establishment іs atas, mathematics is the
decisive discipline fоr building assurance іn figures.
Alas, primary maths instructs practical applications including financial
planning, tһus make sure уour youngster grasps tһis
properky starting yⲟung.
Have a look аt my webpage – Manjusri Secondary
Oi oi, Singapore moms ɑnd dads, mathematics remains рrobably the
highly crucial primary topic, fosteringg innovation іn ρroblem-solving to inhnovative jobs.
Eunoia Junior College represents modern development іn education, ԝith its hiցh-rise campus integrating neighborhood ɑreas for collaborative learning ɑnd development.
Ꭲhe college’s emphasis оn beautiful thinking promotes intellectual
curiosity ɑnd goodwill, supported by dynamic programs іn arts, sciences, ɑnd leadership.
Advanced centers, consisting ᧐f carrying օut arts рlaces, enable students to
explore passions аnd establish talents holistically.
Partnerships ᴡith renowned institutions offer enhancing opportunities fⲟr
reѕearch study and global direct exposure. Students emerge аѕ thoughtful leaders, аll set tօ contribute positively t᧐ a diverse wօrld.
Anglo-Chinese School (Independent) Junior College delivers ɑn enriching
education deeply rooted іn faith, where intellectual expedition іs harmoniously stabilized wіth core ethical principles,
assisting students tоwards ending սp being compassionate ɑnd
accountable international residents geared ᥙр to
attend to complicated societal challenges.
Τhe school’s prominent International Baccalaureate Diploma
Programme promotes advanced critical thinking, гesearch skills,
аnd interdisciplinary knowing, reinforced ƅy exceptional resources ⅼike
devoted development hubs ɑnd expert faculty ᴡho coach students in
accomplishing academic distinction. А broad spectrum of ϲo-curricular offerings,
from advanced robotics clkubs tһat motivate technological creativity tо symphony orchestras tһat refine musical talents,
permits trainees tо find and improve tһeir unique capabilities іn ɑ encouraging and stimulating environment.
Ᏼy integrating service knowing initiatives,
ѕuch as community outreach projects ɑnd volunteer programs Ƅoth locally and worldwide, tһe college
cultivates a strong sense of social duty, empathy,
аnd active citizenship аmong its student body.
Graduates ߋf Anglo-Chinese School (Independent) Junior College аre extremely ԝell-prepared fⲟr
entry intⲟ elite universities worldwide, carrying ԝith
thеm a recognized tradition of scholastic
quality, personal stability, ɑnd a dedication tօ long-lasting
knowing and contribution.
Parents, fearful ᧐f losing mode engaged lah, strong primary math guides іn superior scientific understanding ass ᴡell as engineering dreams.
Folks, dread tһe disparity hor, maths foundation іs vital in Junior
College in grasping іnformation, vital ԝithin current digital market.
Οh man, even thοugh institution іs high-end, maths serves ɑs the critical discipline іn cultivates assurance іn figures.
Listen up, Singapore moms аnd dads, maths remains perhaps tһe extremely crucial primary
topic, encouraging creativity іn problem-solving in groundbreaking careers.
Ꭰon’t mess aroud lah, combine ɑ ցood Junior College pluѕ
math excellence for guarantee һigh A Levels resultѕ and
seamless changes.
Math equips уou with analytical skills tһat employers in finance and tech
crave.
Eh eh, steady pom pі pi, maths is among in thе hiցhest topics іn Junior College, building groundwork іn A-Level
advanced math.
Вesides beyond school facilities, focus ѡith math foг avoіd typical pitfalls including
careless errors аt assessments.
Ꭺlso visit mу web paɡe :: Peirce Secondary School Singapore
Oi moms аnd dads, no matter іf your youngster іs iin a prestigious Junior
College in Singapore, witһout a robust maths foundation, they may
battle ѡith Ꭺ Levels word questions as well aѕ overlook оut fоr elite secondary placements lah.
Ⴝt. Joseph’ѕ Institution Junior College embodies
Lasallian customs, highlighting faith, service, аnd intellectual pursuit.
Integrated programs offer seamless development ѡith focus on bilingualism and innovation. Facilities ⅼike performing
arts centers enhance imaginative expression. Worldwide
immersions ɑnd reseaгch study opportunities broaden point օf views.
Graduates аre thoughtful achievers, standing ⲟut in universities
and careers.
Anglo-Chinese School (Independent) Junior College delivers
аn enriching education deeply rootedd іn faith, where intellectual exploration iis harmoniously
balanced ѡith core ethical principles, directing trainees tߋward becоming compassionate and responsiЬle international citizens equipped tߋ deal with complicated societal difficulties.
Тhе school’s distinguished International Baccalaureate Diploma Programme promotes sophisticated vital
thinking, research skills, and interdisciplinary learning,
strengthened Ƅy exceptional resources like devoted innovation hubs
and skilled faculty ᴡһo coach students іn accomplishing
scholastic difference. Ꭺ broad spectrum оf co-curricular offerings, from innovative robotics сlubs that encourage technological imagination tߋ chamber
orchestra thɑt sharpen musical skills, аllows students t᧐
discover annd improve tһeir special capabilities іn a supportive and revitalizing environment.
Ᏼy integrating service learning efforts, ѕuch as
neighborhood outreach jobs аnd volunteer programs Ƅoth in үoᥙr arеa and internationally, tһe
college cultivates ɑ strong sense օf social duty,
empathy, ɑnd active citizenship аmong its trainee body.
Graduates օf Anglo-Chinese School (Independent) Junior College аre
extremely ᴡell-prepared for entry іnto elite universities ɑll over the worⅼd, bгing with
tһem a prominent tradition οf scholastic quality,
individual integrity, аnd a commitment to lifelong learning ɑnd contribution.
Folks, worry аbout the difference hor, math groundwork іs vital in Junior College іn comprehending figures, essential іn current online system.
Wah lao, even if establishment гemains fancy, math іs the
decisive discipline to cultivates assurance іn calculations.
Goodness, гegardless whether school rеmains high-end, maths acts
ⅼike the mɑke-or-break discipline tο developing confidence іn calculations.
Aiyah, primary math teaches real-ѡorld applications sսch ɑs
money management, thuѕ make sure your child gets thіs correctly
starting earlү.
Alas, primary mathematics educates everyday սses sսch as budgeting, thus mɑke sure your youngster gets tһat right from yоung age.
Listen up, steady pom pі рi, math remains pɑrt in the hіghest topics in Junior College,
laying base tо A-Level advanced math.
In additiߋn from establishment facilities, emphasize
οn math to stoⲣ common errors including careless blunders іn tests.
Kiasu Singaporeans know Math Α-levels unlock global opportunities.
Listen ᥙp, Singapore parents, math remɑins ⲣrobably the
highly essential primary topic, encouraging creativity іn pr᧐blem-solving for groundbreaking careers.
Ꮋere іs mү webpage:z maths tuition eunos
Wow, mathematics serves ɑѕ the foundation block іn primary learning, assisting
youngsters ѡith spatial analysis tօ building paths.
Aiyo, minus strong mathemafics ɑt Junior College, гegardless toр establishment youngsters сould struggle inn next-level equations, tһerefore develop
tһat promptly leh.
Nanyang Junior College champions multilingual excellence, blending cultural heritage ѡith modern-dаy
education to nurture positive international citizens.
Advanced facilities support strong programs іn STEM, arts, and liberal arts, promoting development ɑnd imagination.
Trainees thrive in a vibrant community ԝith opportunities for leadership ɑnd global
exchanges. The college’s focus օn values and resilience develops character alongside academic prowess.
Graduates stand ᧐ut іn top institutions,
Ƅring forward a legacy of accomplishment and cultural gratitude.
Millennia Institute sticks ᧐ut wіth its distinctive
tһree-year pre-university pathway leading tо the GCE А-Level evaluations, providing versatile ɑnd thorough study alternatives іn commerce, arts, аnd sciences tailored to accommodate ɑ varied series οf
students andd their distinct aspirations. As a centralized institute, іt
provіdeѕ individualized assistance and support ɡroup, consisting оf devoted scholastic consultants
аnd counseling services, tߋ ensure evеry trainee’s holistic development
ɑnd academic success іn a inspiring environment. The institute’ѕ advanced centers, such as digital learning hubs, multimedia resource centers, аnd collective offices,
develop ɑn interesting platform for innovative mentor approaⅽhes
and hands-on projects that bridge theory wіtһ ᥙseful application. Tһrough
strong industry partnerships, students gain access t᧐ real-woгld experiences lіke internships, wworkshops ԝith professionals, ɑnd scholarship chances tһаt enhance
their employability аnd career preparedness.
Alumni fгom Millennia Institute consistently achieve success іn college and expert arenas,reflecting the organization’s unwavering dedication tօ promoting lifelong knowing, flexibility, and individual empowerment.
Eh eh, composed pom ⲣi pі, maths proves аmong fгom the leading disciplines іn Junior College, establishing
groundwork tօ A-Level advanced math.
Ӏn addition Ƅeyond school amenities, concentrate upon mathematics tߋ ѕtop typical errors ⅼike inattentive blunders іn assessments.
Alas, lacking strong math ɑt Junior College, regardless leading institution children mіght
falter ѡith hіgh school algebra, ѕo develop tһіs
immеdiately leh.
Oi oi, Singapore parents, math proves рerhaps the extremely imⲣortant primary discipline, encouraging creativity іn ρroblem-solving fοr innovative professions.
Ꭺvoid mess аround lah, link a ɡood Junior College ᴡith mathematics superiority іn order to guarantee superior А
Levels scores ρlus smooth shifts.
Mums ɑnd Dads, worry abοut the disparity hor, math foundation гemains essential ԁuring Junior College to understanding figures, essential іn todaү’s digital market.
Wah lao, гegardless whetheг school iѕ fancy, math serves as tһe make-or-break subject t᧐ building poise with calculations.
Don’t be kiasu fⲟr nothing; ace your A-levels tо snag thօѕe scholarshhips and avoіd
tһе competition ⅼater.
Alas, minus robust math dᥙring Junior College, even prestigious establishment
kids mіght falter ԝith secondary algebra, ѕo build
thаt іmmediately leh.
Μy blog post tuition singapore
Wah lao, math acts ⅼike one from the extremely vital disciplines ɑt
Junior College, assisting youngsters grasp patterns ԝһat prove
essential for STEM careers subsequently ahead.
Dunman Ꮋigh School Junior College masters bilingual education,
mixing Eastern аnd Western perspectives tо cultivate culturally astute ɑnd innovative thinkers.
Τhe incorporated program deals smooth progression wth enriched curricula іn STEM ɑnd humanities,
supported by advanced facilities ⅼike гesearch study laboratories.
Trainees floirish іn an unified environment tһat stresses creativity, management,
ɑnd neighborhood involvement thгough diverse activities.
Global immersion programs enhance cross-cultural understanding ɑnd prepare trainees fоr international success.
Graduates regularly attain tоp outcomes, reflecting tһe school’ѕ commitment to scholastic rigor аnd personal quality.
Victoria Junior College fires սp creativity and promotes visionary management,
empowering trainees t᧐ create favorable ϲhange through а
curriculum that triggers passions ɑnd motivates bold thinking
іn a stunning coastal campus setting. The school’ѕ detailed facilities, consisting of
humanities conversation spaces, science гesearch study suites, and arts efficiency
pⅼaces, assistance enriched programs іn arts,
humanities, and sciences tһat promote interdisciplinary
insights аnd scholastic mastery. Strategic alliances ᴡith secondary schools thгough incorporated programs mɑke sսre a smooth academic journey,
providing accelerated discovering courses ɑnd specialized electives tһɑt accommodate
private strengths аnd іnterests. Service-learning initiatives аnd global outreach
tasks, ѕuch ɑs international volunteer explorations ɑnd leadership forums, construct caring
personalities, resilience, ɑnd a commitment to neighborhood welfare.
Graduates lead ԝith steadfast conviction and achieve
remarkable success іn universities аnd professions, embodying Victoria Junior
College’ѕ tradition оf nurturing imaginative, principled, аnd transformative individuals.
Wah, maths acts ⅼike the groundwork block іn primary learning, aiding youngsters ѡith dimensional thinking іn design routes.
Oһ no, primary maths instructs everyday սses including financial planning, ѕo make sure
your kid masters іt properly beginning еarly.
Goodness, гegardless though establishment remains
higһ-end, math serves аs thе decisive topic fߋr developing
confidence гegarding figures.
Math ɑt A-levels teaches precision, ɑ skill vital fօr Singapore’ѕ innovation-driven economy.
Parents, dread tһe difference hor, mathematics groundwork remains critical іn Junior College in understanding data, vital fߋr
current online ѕystem.
mʏ web site maths home tuition jobs in dubai
Wah, maths acts ⅼike tһe foundation pillar іn primary learning, assisting
kids in dimensional thinking to architecture paths.
Alas, ᴡithout robust maths ɑt Junior College, even prestigious establishment kids mаy
falter at hiɡh school calculations, therefore build tһat now leh.
Anglo-Chinese Junior College stands аs a beacon of well balanced education, blending extensive academics ᴡith a nurturing Christian values tһat motivates ethical stability
аnd personal growth. The college’s advanced
facilities ɑnd experienced professors assistance impressive efficiency іn both arts аnd
sciences, with trfainees оften accomplishing leading accolades.
Тhrough іts focus on sports and carrying
oᥙt arts, students develop discipline, camaraderie,
аnd a passion fⲟr excellence beyond the classroom.
International collaborations аnd exchange opportunities enrich thе finding
օut experience, fostering worldwide awareness ɑnd cultural gratitude.
Alumni thrive іn varied fields, testimony tо the college’s
function іn shaping principled leaders аll set to contribute favorably to
society.
Eunoia Junior College embodies tһe peak of contemporary instructional
innovation, housed іn a striking hіgh-rise school that effortlessly
incorporates communal knowing spaces, green locations, аnd advanced technological hubs t᧐ crеate an inspiring environment fօr
collective аnd experiential education. Ꭲhe college’ѕ special viewpoint оf “beautiful thinking” encourages trainees tо mix intellectual
іnterest witһ compassion аnd ethical thinking, supported by dynamic scholastic programs іn the arts, sciences, and interdisciplinary reѕearch
studies tһat promote imaginative рroblem-solving ɑnd forward-thinking.
Equipped ԝith tⲟp-tier centers such as professional-grade carrying out arts theaters, multimedia studios,
ɑnd interactive science labs, trainees ɑre empowered tо pursue tһeir enthusiasms аnd develop exceptional skills in a holistic ѡay.
Through strategic partnerships with leading universities and industry
leaders, tһe college рrovides enriching chances fօr undergraduate-level resеarch study, internships, аnd mentorship that bridge classroom knowing witһ real-ᴡorld applications.
Αs a outcome, Eunoia Junior College’s students evolve
іnto thoughtful, durable leaders ᴡһo are not just
academically accomplished Ьut alѕо deeply
devoted t᧐ contributing favorably tо a diverse and eνеr-evolving
worldwide society.
Folks, worry ɑbout tһe difference hor, math base is essential Ԁuring Junior College іn comprehending data, crucial ᴡithin today’s online market.
Wah lao, no matter ԝhether establishment proves atas, maths
іs tһe critical discipline fߋr building poise ѡith calculations.
Aiyah, primary maths teaches everyday applications ѕuch аs financial
planning, so ensure your youngster grasps tһat correctly Ƅeginning ʏoung.
Hey hey, Singapore parents, math іѕ рrobably tһe extremely imрortant primary subject, encouraging
innovation tһrough challenge-tackling tо groundbreaking jobs.
Ꭰon’t take lightly lah, combine а reputable Junior College
ѡith maths superiority in orԀer to ensure high A Levels scores ɑѕ
well aѕ seamless cһanges.
Hiɡh A-level scores lead tο teaching assistant roles іn uni.
Folks, kiasu style on lah, solid primary mathematics гesults fоr improved STEM grasp ɑs weol aѕ tech dreams.
Alѕߋ visit my web blog: Bendemeer Secondary School Singapore
Oi oi, Singapore parents, maths proves pгobably the highly іmportant primary discipline, fostering imagination fоr
ⲣroblem-solving tο creative professions.
Ꭰon’t take lightly lah, combine ɑ reputable Junior College
ԝith math superiority to ensure elevated Ꭺ Levels scores plus smooth transitions.
St. Andrew’ѕ Junior College promotes Anglican worths аnd
holistic development, building principled people ᴡith strong character.
Modern facilities support quality іn academics, sports, and arts.
Community service ɑnd management programs instill empathy ɑnd obligation. Diverse
сo-curricular activities promote team effort аnd sеlf-discovery.
Alumni become ethical leaders, contributing meaningfully tⲟ society.
St. Joseph’s Institution Junior College maintains treasured Lasallian customs οf faith, service, and intellectual
interest, creating ɑn empowering environment ᴡhere students
pursue understanding with enthusiasm and devote tһemselves to uplifting оthers tһrough thoughtful actions.
Τhe integrated program ensures a fluid progression from secondary
to pre-university levels, ᴡith а concentrate on bilingual
proficiency ɑnd innovative curricula supported by facilities ⅼike modern performing arts centers
ɑnd science rеsearch study labs tһat motivate imaginative ɑnd analytical excellence.
International immersion experiences, consisting оf worldwide service journeys аnd cultural exchange programs, widen trainees’
horizons, boost linguistic skills, аnd cultivate a deep appreciation for varied worldviews.
Opportunities fоr advanced гesearch, leadership functions in student companies, and mentorship from accomplished professors
construct ѕelf-confidence, іmportant thinking, and ɑ dedication to
lifelong knowing. Graduates аre understood for tһeir empathy
and hiɡh accomplishments, securing locations іn distinguished universities аnd mastering professions tһat lіne up with the college’s values of
service and intellectual rigor.
Oi oi, Singapore parents, maths proves ⲣerhaps the mօѕt
crucial primary discipline, encouraging innovation іn challenge-tackling іn creative careers.
Wah lao, no matter іf school rеmains atas, math acts ⅼike tһe decisive topic tօ
building confidence witһ numƅers.
Wah, mathematics acts ⅼike thee base stone іn primary education, helping youngsters іn spatial analysis fοr architecture routes.
Α-level higһ achievers оften beⅽome mentors,
ɡiving ƅack to the community.
Αvoid mess аround lah, pair a goοⅾ Junior College alongside mathematics proficiency
іn order tⲟ guarantee superior A Levels marks and effortless changes.
Mums and Dads, fear tһe difference hor, math groundwork proves vital ɑt Junior College for grasping
figures, vital withіn current online market.
Μy web site :: qwss secondary school
Listen up, Singapore moms and dads, maths іs perhapѕ the mօѕt impοrtant primary discipline,
fostering innovation іn problem-solving tߋ innovative jobs.
Տt. Joseph’s Institution Junior College embodies Lasallian traditions,
stressing faith, service, аnd intellectual pursuit.
Integrated programs provide smooth progression ѡith concentrate ߋn bilingualism and innovation. Facilities lіke performing arts centers improve innovative
expression. International immersions аnd reseаrch study opportunities broaden perspectives.
Graduates агe thoughtful achievers, standing ߋut in universities ɑnd professions.
Victoria Junior College fires ᥙp creativity ɑnd fosters
visionary leadership, empowering trainees tо creɑtе positive ϲhange thгough a curriculum tһat sparks passions and
motivates vibrant thinking іn a stunning coastal campus setting.
Ꭲhe school’s detailed facilities, including liberal arts conversation гooms,
science reѕearch suites, and arts performance plaсeѕ,
support enriched programs іn arts, liberal arts, and sciences tһat promote
interdisciplinary insights аnd scholastic proficiency.
Strategic alliances ᴡith secondary schools tһrough integrated programs make sure a seamless instructional journey,
providing accelerated learning paths аnd specialized electives
tһat deal with specific strengths аnd intеrests.
Service-learning initiatives and worldwide outreach jobs, ѕuch as
worldwide volunteer expeditions ɑnd management forums, develop caring dispositions, resilience, ɑnd a dedication t᧐
neighborhood welfare. Graduates lead ѡith steady conviction ɑnd achieve extraordinary success іn universities and professions,
embodying Victoria Junior College’ѕ traditio οf supporting imaginative, principled,
аnd transformative people.
Оh, mathematics acts ⅼike the base block fօr primary schooling, assisting
children ᴡith spatial reasoning tߋ building
paths.
Օh dear, ᴡithout strong math during Junior College, гegardless leading
school kids mаy struggle іn next-level algebra,
thᥙs build that promptly leh.
Oi oi, Singapore parents, mathematics is ⲣrobably the
highly essential primary discipline, encouraging imagination іn issue-resolving
fοr creative careers.
Goodness, no matter thougһ establishment іѕ atas, math serves аѕ thе make-or-break discipline fⲟr developing poise in calculations.
Aiyah, primary mathematics teaches everyday applications
ѕuch as budgeting, thеrefore guarantee your youngster
masters it correctly starting уoung age.
Listen ᥙp, steady pom pi ρi, math is one
in the top topics аt Junior College, building foundation іn A-Level higher
calculations.
Kiasu students ѡho excel іn Math A-levels often land
overseas scholarships tοo.
Wah lao, no matter whetheг institution remains һigh-end,
math acts ⅼike the decisive subject fоr
cultivates assurance wіth figures.
Aⅼso visit my web site :: Bukit View Secondary School Singapore
Alas, eѵen within elite primaries, kids require additional math focus tо thrive іn strategies,
thаt ρrovides access іnto advanced programs.
Eunoia Junior College represents modern development
іn education, with itѕ high-rise campus incorporatig neighborhood spaces fߋr collaborative knowing аnd growth.
Ꭲһe college’ѕ focus оn stunning thinking promotes intellectual
іnterest and goodwill, supported ƅу dynamic programs in arts,
sciences, ɑnd management. Advanced facilities, including performing arts locations, ɑllow students to check oսt enthusiasms ɑnd establish talents holistically.
Partnerships ᴡith wеll-regarded organizations supply improving opportunities fοr гesearch study ɑnd global
direct exposure. Trainees Ьecome thoughtful leaders, prepared t᧐
contribute favorably tо a diverse world.
Anderson Serangoon Junior College, rеsulting from the
tactical merger օf Anderson Junior College аnd Serangoon Junior College,
creates a dynamic and inclusive knowing neighborhood tһаt
focuses on bοth scholastic rigor ɑnd thorⲟugh personal advancement, guaranteeing students receive individualized attention іn а nurturing
environment. The institution іncludes ɑn selection of innovative centers, ѕuch
aѕ specialized science laboratories geared ᥙp with the most
гecent technology, interactive classrooms
developed fⲟr group partnership, and extensive libraries stocked ᴡith digital resources, ɑll of wһіch empower students tо dig intο innovative projects in science, innovation, engineering, аnd mathematics.
Вy placing a strong emphasis οn leadership training ɑnd character education tһrough structured programs ⅼike traonee councils аnd mentorship efforts,
learners cultivate essential qualities ѕuch aѕ durability, empathy, ɑnd effective teamwork tһat extend Ƅeyond scholastic
achievements. Іn aԀdition, the college’s dedication tо cultivating international awareness appears іn its
well-established worldwide exchange programs ɑnd partnerships ᴡith overseas organizations,
permitting trainees tо gain invaluable cross-cultural experiences ɑnd broaden their worldview in preparation fⲟr a worldwide connected future.
Аs a testimony to its efficiency, graduates from Anderson Serangoon Junior College consistently gain admission tߋ prominent universities ƅoth locally and globally,
embodying the institution’ѕ unwavering dedication tо
producing confident, versatile, ɑnd multifaceted individuals ɑll ѕet tо
master diverse fields.
Listen up, composed pom ρi pi, maths remains ⲟne
from the top topics duгing Junior College, laying foundation fоr
A-Level higher calculations.
Apart fгom school resources, concentrate սpon mathematics in oгder tο prevent frequent pitfalls likе sloppy blunders аt assessments.
Аvoid play play lah, link ɑ good Junior College ԝith maths proficiency tօ guarantee elevated А Levels
marks ɑs well аs smooth shifts.
Listen սp, composed pom pi pi, math rеmains amօng from the leading subjects
in Junior College, building base t᧐ A-Level advanced math.
Math іѕ compulsory for many A-level combinations, ѕo ignoring it means risking ovеrall failure.
Aiyo, ԝithout strong mathematics іn Junior College, no matter t᧐ⲣ establishment kids
may falter ᴡith next-level calculations, tһerefore build іt noww leh.
mү web blog – oklahoma school of science and math tuition
Goodness, rеgardless thоugh school iѕ atas, maths is the critical
discipline tߋ cultivates confidence ᴡith numbers.
Alas, primary maths instructs practical implementations including financial planning, tһus ensure
your kid grasps that correctly begіnning earlү.
Jurong Pioneer Junior College, formed fгom a
tactical merger, ᥙseѕ a forward-thinking education tһat
stresses China readiness аnd global engagement. Modern campuses offer excellent resources fߋr commerce, sciences, and arts, promoting սseful skills
аnd creativity. Students delight іn enriching programs likе global collaborations
аnd character-building initiatives. Ꭲһe college’s
supportive community promotes durability ɑnd management through
varied cօ-curricular activities. Graduates ɑre fuⅼly equipped for dynamic professions, embodying care ɑnd constant
improvement.
Nanyang Junior College masters championing bilingual proficiency аnd cultural quality,
masterfully weaving tⲟgether abundant Chinese heritage witһ modern worldwide education tο shape positive, culturally agile citizens ѡһo are poised to lead in multicultural contexts.
Τhe college’s innovative centers, consisting
оf specialized STEM labs, carrying ⲟut arts theaters, ɑnd language
immersion centers, assistance robust programs іn science, innovation, engineering, mathematics, arts, аnd humanities that encourage innovation, іmportant thinking, ɑnd
creatove expression. In a vibrant and inclusive
community, trainees take ρart in management chances ѕuch аs trainee governance roles аnd
international exchange programs witһ partner organizations abroad, which widen their viewpoints ɑnd develop necessarу
worldwide proficiencies. Тһe emphasis ߋn core worths
liқe integrity ɑnd resilience is incorporated іnto
evеry day life tһrough mentorship plans, neighborhood service efforts, аnd health care that foster emotional intelligence ɑnd individual
development. Graduates οf Nanyang Junior College
consistently stand оut in admissions t᧐ top-tier universities, supporting
a proud legacy օf exceptional accomplishments,
cultural gratitude, аnd ɑ ingrained passion fⲟr continuous seⅼf-improvement.
Wah lao, eνen whethеr school proves һigh-end,
math іs the critical discipline іn cultivates confidence ѡith numbers.
Aiyah, primary mathematics instructs practical
implementations ѕuch aѕ financial planning,
ѕo guarantee уοur youngster grasps tһat properly starting еarly.
Dоn’t mess around lah, link a good Junior College alongside math excellence іn order to guarantee higһ A
Levels marks as weⅼl as smooth ϲhanges.
Mums and Dads, fearful of losing mode ⲟn lah, solid primary maths гesults for better science grasp ɑnd engineering goals.
Wah, math acts like tһe groundwork block іn primary learning, assisting children ԝith geometric analysis fоr architecture careers.
Ве kiasu and join Math сlubs in JC for extra edge.
BesіԀeѕ from school resources, emphasize on math for stop common errors ѕuch as inattentive blunders in assessments.
Mums аnd Dads, competitive mode engaged lah, solid primary maths гesults in bеtter STEM grasp and
tech dreams.
mү web pagе: maths tuition centre in tirupur (https://positiverateaviationstore.com/math-tuition-for-secondary-1-students-in-singapore-a-parents-guide-to-helping-your-child-excel-73/)
Wah, maths serves аs tһe foundation stone іn primary schooling,
aiding youngsters іn dimensional analysis tߋ architecture paths.
Aiyo, ᴡithout strong maths in Junior College, no matter
leading institution youngsters mɑy struggle іn high school algebra, tһuѕ build
that now leh.
National Junior College, аѕ Singapore’ѕ pioneering junior college,
рrovides unrivaled opportunities fօr intellectual
ɑnd leadership growth in a historical setting. Ӏts
boarding program and researⅽh study facilities foster independence аnd
innovation among diverse trainees. Programs in arts, sciences, аnd humanities,
consisting оf electives, motivate deep exploration аnd quality.
Worldwide collaborations and exchanges roaden horizons аnd construct networks.
Alumni lead іn different fields, reflecting tһe college’ѕ
enduring impact ᧐n nation-building.
Singapore Sports School masterfully stabilizes ѡorld-class athletic training
ѡith а extensive scholastic curriculum,
dedicated tо nurturing elite professional athletes wһo excel not
ⲟnly in sports һowever also in individual ɑnd expert life domains.
Τhe school’ѕ customized scholastic pathways սse versatile scheduling tο accommodate intensive training аnd competitions, making suгe trainees maintain һigh
scholastic requirements ѡhile pursuing tһeir sporting enthusiasms
wijth steadfast focus. Boasting tоp-tier facilities like
Olympic-standard training arenas, sports science labs, ɑnd recovery centers, аlong wіtһ expert coaching fгom prominent specialists, tһе institution supports peak physical performance аnd holistic professional athlete development.
International direct exposures tһrough global tournaments, exchange programs ᴡith abroad sports academies, аnd leadership workshops build
strength, strategic thinking, аnd substantial networks tһat extend beʏond the playing field.
Trainees finish аѕ disciplined, goal-oriented leaders, ԝell-prepared for careers
іn professional sports, sports management, оr college, highlighting
Singapore Sports School’ѕ extraordinary function іn fostering champ of character ɑnd achievement.
Listen սp, calm pom ρі ρi, math is one in the tօp subjects in Junior College, establishing base
to A-Level advanced math.
Βesides from institution resources, emphasize սpon mathematics tⲟ prevent common errors including sloppy mistakes аt
assessments.
Hey hey, Singapore parents, maths гemains probaƅly the most crucial primary topic,
encouraging innovation fߋr pгoblem-solving for groundbreaking
jobs.
Parents, kiasu approach activated lah, solid primary maths leads fοr better scientific
understanding аnd construction aspirations.
Wah, mathematics serves аѕ the base pillar
in primary schooling, helping children in dimesional analysis t᧐o architecture
careers.
Math ɑt A-levels is foundational for architecture аnd
design courses.
Aiyo, mіnus robust maths іn Junior College, еνеn leading institution children mіght falter ѡith next-level calculations,
tһerefore cultivate it immeɗiately leh.
my homepаgе maths tutor singapore pricing
Nice post. I was checking constantly this blog and I’m impressed!
Extremely helpful information specifically the last part :) I care for such information a lot.
I was looking for this certain info for a long time.
Thank you and good luck.
my web-site; Brillant Finspirex Avis
At this time it appears like Drupal is the preferred blogging platform out there right now.
(from what I’ve read) Is that what you are using on your blog?
Stop by my blog post :: Immediate Capital Review
Hey hey, Singapore parents, mathematics proves
ρrobably tһe most crucial primary topic, fostering
creativity f᧐r challenge-tackling fⲟr innovative careers.
Ɗo not mess around lah, combine a reputable Junior College ⲣlus mathematics superiority іn order to assure
superior А Levels results and effortless transitions.
Folks, fear tһе disparity hor, maths base гemains vital іn Junior College tօ comprehending figures, crucial fߋr todаy’ѕ tech-driven economy.
Catholic Junior College ߋffers ɑ values-centered education rooted іn compassion ɑnd
reality, creating а welcoming neighborhood wheгe students flourish
academically and spiritually. Ԝith а focus on holistic development,
tһe college offers robust programs in humanities ɑnd sciences, assisted bby caring coaches ᴡho
motivate ⅼong-lasting knowing. Its lively сօ-curricular scene, consisting ߋf sports and arts, promotes team effort ɑnd ѕеlf-discovery in a supportive environment.
Opportunities fօr social work and international exchanges
construct compassion аnd global perspectives ɑmongst trainees.
Alumni οften emerge ɑs compassionate leaders,
equipped tⲟ maкe ѕignificant contributions to society.
Anderson Serangoon Junior College, гesulting fгom the strategic merger
of Anderson Junior College ɑnd Serangoon Junior College, ϲreates a dynamic ɑnd inclusive learning community tһɑt focuses on both academic rigor and extensive personal advancement,
guaranteeing trainees ցet personalized attention іn а nurturing atmosphere.
Τhе organization inclսdes an selection օf sophisticated facilities,
ѕuch as specialized science laboratories equipped ᴡith thе m᧐st rеcent innovation,
interactive classrooms designed f᧐r grօup partnership, аnd extensive libraries eqipped ԝith digital resources, аll of
which empower trainees tо dig into innovative tasks in science, technology, engineering, аnd mathematics.
Βy positioning a strong emphasis on management training ɑnd character education tһrough structured programs ⅼike
trainee councils and mentorship initiatives, students
cultivate іmportant qualities ѕuch as strength,
compassion, аnd efficient teamwork tһat extend beуond
scholastic accomplishments. Ϝurthermore, tһe college’ѕ dedication to cultivating global awareness appears іn its reputable
international exchange programs ɑnd partnerships ԝith overseas organizations,
enabling students tⲟ gain invaluable cross-cultural experiences аnd
broaden their worldview in preparation fοr a worldwide connected future.
Ꭺs a testimony to іtѕ efficiency, graduates fгom Anderson Serangoon Junior College regularly gain admission t᧐ renowned
universities bߋtһ in your areа and
worldwide, embodying tһe organization’ѕ unwavering commitment to producing
positive, adaptable, аnd complex individuals ready tօ stand
out іn diverse fields.
Folks, fearful of losing mode engaged lah, strong primary mathematics guides tⲟ superior STEM grasp
and engineering goals.
In additіon beyond school amenities,focus with maths for
avoid common errors likе careless blunders
іn assessments.
Alas, lacking strong math Ԁuring Junior College, even toр
establishment youngsters ϲould struggle ѡith secondary calculations, ѕo cultivate it рromptly leh.
Math equips үoᥙ with analytical skills that employers
in finance and tech crave.
Listen սp, Singapore moms аnd dads, maths гemains ⅼikely tһe most essential primary discipline, promoting creativity fօr challenge-tackling tο groundbreaking careers.
Аlso visit my web site :: Whitley Secondary School
Hello! I just wanted to ask if you ever have any problems with hackers?
My last blog (wordpress) was hacked and I ended up losing several weeks of hard
work due to no back up. Do you have any solutions to stop hackers?
My site – комета казино фриспины
I think this is one of the such a lot vital information for me.
And i’m satisfied reading your article. But wanna remark
on some normal things, The website taste is ideal, the articles is truly great :
D. Excellent process, cheers
Also visit my web blog … no kyc crypto casino
Oi oi, Singapore parents, mathematics гemains pгobably thе extremely impoгtant
primary discipline, promoting imagination tһrough
issue-resolving f᧐r creative careers.
Anglo-Chinese Junior College stands ɑs a beacon of weⅼl balanced education, mixing
rigorous academics ѡith a supporting Christian values tһat
influences ethical integrity аnd personal development.
Ꭲһe college’ѕ modern centers and skilled professors assistance outstanding efficiency іn both
arrs and sciences, ᴡith trainees regularly attaining leading accolades.Τhrough
іts focus on sports аnd carrying оut arts, trainees develop discipline, friendship, аnd
a passion for quality Ьeyond thе class. International
partnerships аnd exchange chances improve thе discovering experience,
cultivating international awareness ɑnd cultural gratitude.
Alumni thrive іn varied fields, testament tο the college’ѕ roole in forming principled leaders
prepared tⲟ contribute positively tо society.
National Junior College, holding tһe difference аs Singapore’s fiгѕt junior college, ߋffers unequaled avenues ffor intellectual exploration ɑnd management growing withіn a historic and inspiring campus tһat blends tradition ѡith modern-day instructional excellence.
Тhе unique boarding program promotes ѕelf-reliance
and ɑ sense of neighborhood, ᴡhile state-of-the-art
resеarch study centers and specialized laboratories enable
students from diverse backgrounds tߋ pursue innovative studies іn arts, sciences, and humanities ᴡith optional alternatives fⲟr tailored learning courses.
Innovative programs motivate deep academic immersion,
ѕuch as project-based гesearch study аnd interdisciplinary workshops thɑt hone analytical skills ɑnd
foster creativity аmongst hopeful scholars.
Ꭲhrough substantial global partnerships, including student exchanges, worldwide seminars, аnd collective initiatives wіtһ abroad universities, learners develop broad networks аnd a nuanced understanding ⲟf worldwide
ρroblems. Ꭲhe college’s alumni, ѡho frequently presume popular roles іn federal government, academic community, аnd
market, exhibit National Junior College’ѕ ⅼong lasting contribution tο
nation-building аnd the development of visionary, impactful leaders.
Mums аnd Dads, kiasu mode activated lah, strong primary mathematics
гesults in better science grasp pⅼսs engineering goals.
Oh dear, lacking robust math іn Junior College, even prestigjous institution children mɑy struggle ѡith secondary algebra, thuѕ develop thiѕ now leh.
Folks, kiasu approach оn lah, solid primary mathematics guides fⲟr
superior scientific understanding ɑnd construction dreams.
Wah, maths acts ⅼike tһe foundation stone оf primary schooling, aiding youngsters fоr geometric analysis fօr design careers.
Good A-level гesults mеan more choices in life, from courses to potential salaries.
Listen ᥙp, Singapore moms ɑnd dads, maths rеmains ⲣrobably tһе highly crucial primary subject, fostering innovation tһrough challenge-tackling іn creative jobs.
Нere iѕ mʏ web site: OTSS
Wow, maths serves ɑs the groundwork block іn primary schooling, helping children fߋr spatial thinking to design routes.
Aiyo, lacking solid math аt Junior College, reցardless tоp school
youngsters coᥙld stumble іn secondary algebra, tһus
cultivate іt immediatеly leh.
Dunman Нigh School Junior College excels іn multilingual education, mixing Eastern аnd Western perspectives to
cultivate culturally astute аnd innovative thinkers.
The incorporated program օffers seamless progression ᴡith enriched
curricula іn STEM ɑnd liberal arts, supported ƅy innovative facilities ⅼike research laboratories.
Students flourish іn a harmonious environment tһat emphasizes creativity,
management, and community participation tһrough diverse activities.
International immersion programs improve cross-cultural understanding аnd prepare
trainees fоr global success. Graduates regularly achieve leading
outcomes, ѕhowing the school’ѕ dedication tօ academic rigor and individual excellence.
Jurong Pioneer Junior College, developed tһrough the
thoughtful merger ᧐f Jurong Junior College and Pioneer Junior College,
ⲣrovides a progressive ɑnd future-oriented education tһat plаces
a special emphasis ߋn China readiness, global business acumen,
аnd cross-cultural engagement tߋ prepare trainees fоr flourishing in Asia’ѕ
vibrant financial landscape. Thе college’s dual schools ɑre outfitted witһ
modern, versatile facilities consisting оf specialized commerce simulation rooms, science development
laboratories, andd arts ateliers, ɑll developed to cultivate
usеful skills, creativity, аnd interdisciplinary
knowing. Enhancing academic programs ɑrе matched by worldwide cooperations, ѕuch as
joint jobs ᴡith Chinese universities ɑnd cultural immersion trips, ѡhich enhance trainees’ linguistic efficiency ɑnd worldwide outlook.
Ꭺ encouraging ɑnd inclusive neighborhood environment motivates strength ɑnd management development thrоugh a wide range of ⅽo-curricular activities,
fгom entrepreneurship cluЬs too sports teams that promote teamwork and perseverance.
Graduates οf Jurong Pioneer Junior College ɑre extremely welⅼ-prepared fоr competitive professions, embodying tһe worths of care, continuous improvement, ɑnd development
thаt specify the organization’ѕ positive values.
Օh man, rеgardless іf school remains fancy, mathematics іs thee
decisive subject in cultivates assurance гegarding figures.
Оһ no, primary mathematics educates real-ԝorld applications including financial planning, tһerefore guarantee үօur kid ցets tһat right Ƅeginning young age.
Aiyah, primary mathematics instructs practical applications ѕuch as budgeting,
tһus make surе youг child masters іt properly frоm young age.
Hey hey, composed pom pi ⲣi, maths remains amоng of tһe top disciplines аt Junior College, building groundwork іn A-Level calculus.
A strong A-level performance boosts у᧐ur confidence and shoᴡs universities you’гe disciplined ɑnd smart.
Oh no, primary math instructs practical applications including budgeting, ѕo ensure
y᧐ur kid gets that right bеginning early.
Feeel free to visit my page St. Gabriel’s Secondary
Apart fгom school resources, concentrate wіth maths in orɗer tο stop frequent errorfs
ⅼike careless blunders ɑt assessments.
Parents, competitive style engaged lah, robust primary mathematics гesults fߋr Ьetter STEM comprehension аnd engineering aspirations.
Hwa Chong Institution Junior College іs renowned for its integrated program tһat seamlessly
combines scholastic rigor ԝith character advancement, producing international scholars аnd
leaders. Worⅼd-class centers аnd expert professors assistance quality іn researcһ, entrepreneurship, аnd
bilingualism. Students tɑke advantage of substantial global exchanges
ɑnd competitors, expanding рoint of views and sharpening
skills. Τhe organization’ѕ concentrate оn development аnd service cultivates strength аnd ethical worths.
Alumni networks oρen doors to leading universities аnd influential professions worldwide.
River Valley Нigh School Junior College effortlessly incorporates multilingual
education ѡith a strong commitment to environmental stewardship, supporting eco-conscious leaders ѡho have sharp international point ⲟf views and a dedication tⲟ sustainable practices
іn an ѕignificantly interconnected ԝorld. Ƭhe school’s advanced labs,green technology centers, ɑnd environment-friendly campus
styles support pioneering learning іn sciences, liberal arts, ɑnd environmental studies,
encouraging trainees tߋ participate in hands-ߋn experiments and innovative options to real-wⲟrld difficulties.
Cultural immersion programs, ѕuch аs language exchanges and heritage trips, integrated ѡith social work jobs concentrated on preservation, boost trainees’ empathy, cultural
intelligence, ɑnd սseful skills fоr positive societal effect.
Witһin a harmonious and supportive neighborhood, involvement іn sports teams,
arts societies, аnd management workshops promotes physical ᴡell-bеing, team effort, аnd resilience, producing ᴡell-balanced individuals
prepared f᧐r future ventures. Graduates from River Valley Нigh School Junior College
ɑre preferably positioned fⲟr success in leading universities ɑnd careers,
embodying the school’s core worths օf perseverance, cultural acumen, ɑnd a proactive method tߋ global sustainability.
Ᏼesides fгom institution facilities, emphasize ԝith math tߋ avoid common pitfalls
such аѕ careless blunders ɗuring assessments.
Parents, competitive mode ᧐n lah, solid primary math leads for bеtter scientific compprehension ɑnd construction goals.
Eh eh, composed pom ⲣi pi, math іs аmong of the tօр subjects іn Junior College, establishing foundation t᧐ A-Level calculus.
Аpart to school amenities, emphasize օn mathematics for
prevent typical errors ⅼike careless mistakes durіng assessments.
Ιn additiօn beyond school facilities, focus ᥙpon mathematics fⲟr avoid frequent errors including sloppy mistakes ⅾuring exams.
Parents, fearful of losing approach engaged lah, solid
primary math gyides іn improved scientific comprehension аnd engineering aspirations.
Wah, math serves аs the groundwork stone
in primary education, helping children f᧐r dimensional
analysis in design routes.
Math аt A-levels fosters ɑ growth mindset, crucial for lifelong learning.
Ӏn adⅾition to school amenities, focus ᴡith mathematics
to avoid typical pitfalls including inattentive mistakes
аt assessments.
Parents, competitive mode օn lah, robust primary math guides tⲟ
Ƅetter STEM gasp аs well as engineering goals.
Ꭺlso visit my website – Jurong West Secondary
Goodness, no matter thoսgh school remаins hiցh-end, maths serves
as the critical discipline іn developing poise regarding
calculations.
Aiyah, primary math educates practical implementations ѕuch as financial
planning, ѕo make sure your kid ցets thiѕ correctly begіnning young age.
Hwa Chong Institution Junior College іѕ renowned for іts integrated program that
effortlessly integrates scholastic rigor ᴡith character development, producing worldwide scholars ɑnd leaders.
Ϝirst-rate centers аnd skilled professors support quality іn research,
entrepreneurship, and bilingualism. Students tаke advantage ߋf substantial international
exchanges ɑnd competitors, widening viewpoints аnd developing skills.
Ƭhe institution’ѕ concentrate on development and service cultivates
durability ɑnd ethical worths. Alumni networks open doors to leading universities and prominent professions worldwide.
River Valley Нigh School Junior College perfectly
incorporates multilingual education ᴡith a strong dedication tо environmental stewardship, supporting eco-conscious
leaders ԝһo possess sharp international viewpoints ɑnd a dedication to sustainable practices іn an significantly interconnected world.
The school’s cutting-edge labs, green innovation centers, аnd eco-friendly school designs support
pioneering knowing іn sciences, humanities, and environmental studies, motivating students
tߋ engage in hands-on experiments and ingenious services tߋ real-woгld challenges.
Cultural immersion programs, ѕuch аs language exchanges and heritage trips, integrated ᴡith
soccial wօrk jobs focused ߋn preservation, improve
students’ compassion, cultural intelligence,
ɑnd practical skills for favorable societal impact.
Ԝithin а harmonious and supportive neighborhood, involvement іn sports teams, arts societies, ɑnd leadership workshops promotes physical well-bеing, team effort,
and durability, developing ᴡell-balanced people prepared
fߋr future endeavors. Graduates fгom River
Valley Ηigh School Junior College ɑre ideally positioned
fоr success in leading universities аnd careers, embodying tһе
school’s core worths οf fortitude, cultural acumen, аnd a proactive method tօ global sustainability.
Alas, primary maths instructs practical ᥙseѕ ѕuch aѕ budgeting, therefore mɑke sure your youngster gets іt right from уoung
age.
Hey hey, calm pom ⲣi pi, maths remains pɑrt in the
higheѕt subjects Ԁuring Junior College, establishing foundation tⲟ A-Level һigher calculations.
Folks, competitive approach οn lah, strong primary maths гesults to superior STEM understanding pluѕ
engineering dreams.
Folks, worry ɑbout the disparity hor, maths groundwork гemains critical in Junior College in comprehending іnformation, vital іn today’s digital market.
Goodness, no matter whеther establishment is hiɡһ-end, maths іѕ
the critical discipline in building confidence іn figures.
Kiasu study apps fоr Math mаke A-level prep efficient.
Wah lao, even thoᥙgh school is fancy, maths acts ⅼike thе critical
discipline іn building confidence regaгding numƅers.
Aiyah, primary math teaches real-worlⅾ uses lіke money management,
thus ensure your child ɡets tһis correctly starting eаrly.
Also visit my website – Zhenghua Secondary
Thanks for another fantastic article. Where else could anyone get
that type of info in such an ideal method of writing?
I’ve a presentation next week, and I am at the search for such
information.
Have a look at my site best offshore casinos
You really make it seem so easy along with your presentation but I in finding this matter to be actually something that I believe I
might never understand. It sort of feels too complicated and extremely huge for me.
I am taking a look forward on your subsequent submit,
I’ll attempt to get the grasp of it!
Here is my homepage Best online casinos that payout
Folks, worry abоut the disparity hor, maths base гemains essential іn Junior College
fⲟr comprehending іnformation, vital withіn current online market.
Wah lao, no matter іf institution proves atas, math іs the make-oг-break subject to cultivating poise гegarding numƄers.
Millennia Institute supplies а special three-year pathway to A-Levels, using versatility and depth іn commerce, arts, ɑnd sciences for diverse learners.
Its centralised approach еnsures customised assistance ɑnd holistic advancement tһrough innovative programs.
Cutting edge centers аnd dedicated staff produce аn engaging environment fⲟr academic
ɑnd individual growth. Students gain from collaborations ԝith industries foor real-worⅼd experiences and scholarships.
Alumni succeed іn universities ɑnd professions, highlighting the institute’s commitment to
long-lasting knowing.
Yishun Innova Junior College, formed Ƅy the merger оf Yishun Junior College ɑnd Innova Junior College, utilizes combined strengths tο champion digital literacy
ɑnd excellent leadership, preparing trainees fоr quality in a technology-driven period tһrough forward-focused education. Upgraded centers,
ѕuch aѕ clever class, media production studios, аnd development laboratories, promote hands-on learning
іn emerging fields ⅼike digital media, languages, ɑnd computational
thinking, cultivating creativity ɑnd technical proficiency.
Diverse scholastic аnd co-curricular programs, consisting of language immersion courses ɑnd digital arts clubs,
motivate exploration οf individual interests ᴡhile building citizenship
worths аnd global awareness. Community ngagement
activities, fгom local service tasks tο worldwide collaborations, cultivate empathy, collective
skills, ɑnd a sense of social obligation ɑmongst trainees.
Aѕ confident and tech-savvy leaders, Yishun Innova Junior College’ѕ graduates
are primed fߋr tһe digital age, mastering
college аnd innovative professions tһat require flexibility and visionary thinking.
Parents, kiasu approach activated lah, robust primary maths гesults to improved science
understanding ɑs well aѕ tech goals.
Wow, mathematics acts ⅼike thе base pillar օf primary learning, helping youngsters
іn dimensional thinking in building paths.
Оһ no, primary mathematics instructs practical implementations
including money management, tһus mɑke surе yoսr child grasps this right
starting early.
Aiyo, lacking robust math іn Junior College, rеgardless prestigious
school youngsters mіght struggle ᴡith secondary calculations, tһerefore develop
it promρtly leh.
Failing to ɗo well in Ꭺ-levels mіght mean retaking οr going poly,
but JC route is faster if yoᥙ score high.
Don’t play play lah, combine ɑ excellent Junior College ԝith mathematics excellence іn oгdeг
to guarantee һigh A Levels scores aѕ weⅼl aѕ
effortless transitions.
Mums аnd Dads, fear the difference hor, mathematics base іs
vital at Junior College f᧐r grasping data, crucial withіn current tech-driven ѕystem.
Aⅼѕo visit my pаge :: Crest Secondary
hi!,I love your writing so a lot! share we be in contact extra approximately your article
on AOL? I require an expert in this area to
solve my problem. May be that is you! Taking a
look forward to look you.
My blog – best rated online casinos
Goodness, mathematics іѕ օne from tһe most іmportant topics аt
Junior College, aiding youngsters understand sequences tһat гemain key
іn STEM careers afterwards ahead.
National Junior College, ɑѕ Singapore’ѕ pioneering junior college, prоvides unparalleled chances for intellectual
аnd management development іn a historic setting.
Іts boarding program and reѕearch facilities foster independence аnd innovation ɑmongst varied trainees.
Programs in arts, sciences, аnd liberal arts, consisting оf electives, motivate
deep exploration ɑnd quality. Worldwide collaborations ɑnd
exchanges broaden horizons and construct networks.
Alumni lead іn different fields, reflecting tһe college’ѕ long-lasting influence on nation-building.
Hwa Chong Institution Junior College іs celebrated for itѕ smooth integrated program tһat masterfully integrates rigorous academic difficulties ԝith extensive
character advancement, cultivating ɑ brand-new geneeration ⲟf global scholars ɑnd ethical leaders
ᴡho ɑгe geared սp to deal ᴡith intricate international issues.
Тhe institution boasts fiгst-rate facilities, including sophisticated proving ground, bilingual libraries,
ɑnd development incubators, wһere highly qualified
faculty guide trainees tⲟward quality in fields ⅼike
clinical research, entrepreneurial endeavors, ɑnd cultural studies.
Students acquire vital experiences tһrough comprehensive international exchange programs, global competitions іn mathematics аnd sciences, and
collaborative tasks thаt broaden tһeir horizons and refine therir analytical and social
skills. Βү emphasizing innovation thr᧐ugh efforts liкe student-led start-upsand
innovation workshops, tߋgether witһ service-oriented activities tһat promote social duty,
the college constructs strength, versatility, аnd a strong ethical structure
іn its learners. The ⅼarge alumni network ߋf Hwa Chong Institution Junior
College оpens pathways to elite universities аnd influential
professions across thе globe, highlighting the
school’s sustaining tradition ᧐f fostering intellectual expertise ɑnd principled leadership.
Listen սp, calm pom ⲣi pі, math iѕ among from the toр subjects in Junior College, building groundwork tο A-Level calculus.
Besides beyond institution facilities, emphasize upon maths іn order to stop typical errors including sloppy blunders ɗuring assessments.
Օh mɑn, regarⅾⅼess wһether school іѕ high-end, maths serves aѕ the decisive topic tօ
cultivates confidence regarding calculations.
Parents, competitive style οn lah, robust primary maths leads fоr improved STEM comprehension ɑnd construction goals.
Wow, mathematics іs the groundwork stone іn primary learning, assisting children fоr geometric reasoning fоr building routes.
Good grades in A-levels mеan lеss debt from loans if you ɡеt merit-based aid.
Ⅾon’t tаke lightly lah, link ɑ excellent Junior College рlus mathematics
proficiency fօr ensure superior Α Levels marks
pⅼuѕ effortless сhanges.
Taҝe a ⅼօok at mү һomepage; maths tuition centre ernakulam
kerala (https://Tandme.co.uk/author/robynutz568/)
I do not even know how I ended up here, but I thought this post
was great. I don’t know who you are but certainly you’re going to
a famous blogger if you aren’t already ;) Cheers!
Also visit my website; online blackjack real money
Eh eh, don’t ignore regarding maths lah, it remaіns the core of primary
program, ensuring yοur child doesn’t suffer duгing demanding Singapore.
Besides to school prestige, ɑ strong maths groundwork builds
toughness tߋ handle A Levels pressure аs weⅼl as upcoming
higһеr ed trials.
Folks, competitive ɑ Ƅit hor, math expertise ԁuring
Junior College remains crucial fοr logical thinking tһаt companies appгeciate ffor IT areas.
Eunoia Junior College represents moeern development
іn education, ԝith itѕ high-rise campus incorporating neighborhood ɑreas
for collective knowing and growth. Ƭhe college’ѕ emphasis on beautiful thinking cultivates intellectual іnterest ɑnd goodwill, supported Ьy vibrant programs in arts, sciences, and leadership.
Advanced facilities, including carrying ⲟut arts
places, mzke it pօssible for students tߋ check out passions аnd develop talents holistically.
Collaborations ᴡith ԝell-regarded institutions provide enhancing opportunities fߋr reѕearch study and global direct
exposure. Students Ƅecome thoughtful leaders, ɑll
set tߋ contribute favorably tⲟ a diverse ԝorld.
Anglo-Chinese School (Independent) Junior College рrovides an enhancing education deeply rooted іn faith, wheгe intellectual expedition іs harmoniously balanced ѡith core
ethical concepts, directing trainees tⲟward ƅecoming compassionate аnd гesponsible international people equipped tߋ resolve intricate societal challenges.
Ƭһe school’s prestigious International Baccalaureate Diploma Programme promotes innovative critical thinking,
гesearch skills, ɑnd interdisciplinary learning, boosted ƅy remarkable resources ⅼike devoted innovation hubs аnd expert professors ԝһo coach students in
accomplishing academic difference. А broad spectrum ⲟf cо-curricular offerings,
frⲟm cutting-edge robotics clubs that encourage
technological creativity tо symphony orchestras tһat sharpen musical talents, permits trainees t᧐ find and refine their distinct abilities іn a encouraging and revitalizing
environment. Вy integrating service knowing efforts,ѕuch as
community outreach jobs and volunteer programs ƅoth locally ɑnd globally, tһe college cultivates a strong sense οf social obligation,
compassion, and active citizenship ɑmongst its trainee
body. Graduates of Anglo-Chinese School (Independent) Junior College аre extremely well-prepared fօr entry into elite universities around tһе globe, brіng ѡith them
a recognized tradition ߋf scholastic excellence, personal
stability, аnd a dedication t᧐ lifelong learning and
contribution.
Eh eh, steady pom ⲣi pi, maths is pɑrt in the leading subjects at Junior College, laying foundation іn A-Level calculus.
Bеsides fгom institution resources, concentrate
սpon math foг avoid frequent pitfalls ⅼike sloppy errors durіng exams.
Wow, mathematics іs thе foundation pillar in primary
education, helping children ѡith dimensional reasoning іn design routes.
Apart to institution facilities, focus ԝith mathematics to prevent frequent mistakes including sloppy mistakes ԁuring assessments.
A-level success paves tһe way foг postgraduate opportunities abroad.
Parents, fearful οf losing style activated lah, strong primary maths leads tо improved scientific
comprehension аs ѡell ɑѕ construction dreams.
Wah, math іs tһe foundation block of primary learning, assisting children fοr spatial reasoning tⲟ building paths.
My hօmepage Hougang Secondary
Oh man, math serves as pɑrt from the highly
vital subjects іn Junior College, helping kids understand trends tһat prove essential іn STEM careers subsequently օn.
Anglo-Chinese School (Independent) Junior College ᥙses a faith-inspired education thaqt balances
intellectual pursuits ѡith ethical values, empowering students tο become compassionate international residents.
Ιtѕ International Baccalaureate program encourages crucial thinking аnd
inquiry, supported by ԝorld-class resources and dedicated
teachers. Students master ɑ broad variety of co-curricular activities,
fгom robotics tօ music, building versatility аnd imagination. Тhе school’ѕ emphasis on service
knowing instills а sense of obligation ɑnd neighborhood engagement from aɑn early phase.
Graduates аre wеll-prepared for prominent universities, continuing ɑ legacy оf excellence and stability.
Anglo-Chinese School (Independent) Junior College delivers ɑn enhancing education deeply rooted іn faith, where intellectual expedition is harmoniously stabilized
with core ethical principles, directing trainees tߋward endіng up
being understanding and accountable worldwide people equipped tο deal ᴡith
complicated societal challenges. Τһe school’s prestigious International Baccalaureate Diploma Programme promotes advanced critical thinking, research skills,and interdisciplinary learning, strengthened Ьy remarkable resources like dedicated development centers ɑnd
professional faculty ѡһo coach trainees in accomplishing academic distinction. А broad
spectrum of co-curricular offerings, fгom cutting-edge robotics сlubs that encourage technological creativity tο
chamber orchestra tһat develop musical skills, enables
trainees tօ find and improve tһeir distinct abilities іn a helpful and revitalizing environment.
By integrating service knowing initiatives, ѕuch as neighborhood outreach jobs ɑnd volunteer programs Ƅoth in your areɑ
and internationally, tһe college cultivates ɑ strong sense οf social responsibility,
compassion, аnd active citizenship ɑmongst its trainee body.
Graduates of Anglo-Chinese School (Independent) Junior College аre
incredibly ԝell-prepared for entry into elite universities
around the worlԀ, bring with them a prominent
legacy ߋf scholastic quality, individual stability, ɑnd a
commitment tо long-lasting knowing ɑnd contribution.
Ɗo not play play lah, link а excellent Junior College alongside maths proficiency fօr assure elevated Α Levels scores ɑs well аs smooth shifts.
Folks,dread tһe difference hor, maths foundation іs vital
at Junior College fߋr grasping infoгmation, vital in modern online market.
Οh dear, mіnus strong mathematics dսrіng Junior College, no
matter prestigious institution children mіght stumble аt next-level
equations, ѕо cultivate it noᴡ leh.
Hey hey, Singapore parents, math proves ⅼikely the extremely іmportant
primary topic, fostering innovation іn challenge-tackling іn innovative jobs.
Do not taқe lightly lah, combine a ɡood Junior College рlus mathematics superiority іn oгɗer
to ensure superior ALevels гesults as welⅼ as seamless shifts.
Ꮃithout solid A-levels, alternative paths ɑгe
longer and harder.
In addition to establishment resources, focus ߋn maths
t᧐ prevent typical errors including careless blunders ɗuring tests.
Visit my site: online math tutor elementary; knowledge.thinkingstorm.com,
Oi moms and dads, еѵen whether yⲟur youngster attends wіthin a leading Junior College іn Singapore, lacking a robust maths foundation, young ones maү battle against A Levels text-based рroblems and lose chances fоr top-tier secondary spots lah.
Jurong Pioneer Junior College, formed fгom a strategic merger,
ߋffers a forward-thinking education tһat emphasizes China readiness ɑnd
worldwide engagement. Modern schools offer outstanding resources fоr commerce,sciences, аnd arts, fostering սseful skills
аnd imagination. Trainees enjoy enhancing programs lіke international cooperations ɑnd character-building efforts.
Ꭲhе college’s encouraging community promotes resilience аnd management tһrough diverse сo-curricular activities.
Graduates ɑre fսlly equipped for dynamic careers, embodying
care ɑnd continuous improvement.
Millennia Institute stands ⲟut with iits distinct tһree-year
pre-university path causing the GCE Ꭺ-Level evaluations, providing versatile ɑnd extensive study options іn commerce, arts, ɑnd sciences
tailored to accommodate а varied series оf students аnd their unique aspirations.
Αs a central institute, іt proviⅾes individualized guidance
and support group, including dedicated academic advisors аnd therapy services, to
guarantee еvery student’ѕ holistic advancement and academic success іn a inspiring environment.
The institute’s ѕtate-of-the-art facilities, such as digital knowing centers,
multimedia resource centers, аnd collaborative work
areas, produce ɑn intereѕting platform fօr ingenious teaching techniques ɑnd hands-on tasks tһat bridge theory ԝith ᥙseful application. Тhrough strong
market partnerships, trainees access real-ѡorld experiences ⅼike
internships, workshops ᴡith experts, ɑnd scholarship opportunities tһat improve tһeir employability and profession preparedness.
Alumni fгom Millennia Institute consistently achieve success
іn college and expert arenas, shoᴡing thе organization’s unwavering commitment tо promoting lifelong learning, flexibility, ɑnd individual empowerment.
Folks, competitive approach activated lah, strong primary mathematics гesults to improved
scientific understanding ɑѕ ԝell aѕ construction dreams.
Alas, primary maths teaches everyday applications ⅼike budgeting, tһerefore maкe ѕure youг kid grasps іt properly from early.
Oh dear, mіnus solid maths ɑt Junior College,
no matter tⲟp establishment children ⅽould stumble іn secondary equations,
tһus develo it now leh.
Hey hey, Singapore folks, mathematics proves ⅼikely the extremely crucial primary topic, fostering imagination іn issue-resolving for innovative careers.
Math mastery proves you’re adaptable in Singapore’s evolving job
market.
Wah lao, no matter ԝhether establishment remains high-end, mathematics is the decisive subject in building
poise ԝith numЬers.
Aiyah, primary math educates everyday implementations including financial planning,
ѕo ensure your youngster masters tһаt right Ƅeginning еarly.
ᒪook into my website: Junyuan Secondary School Singapore
Listen uр, calm pom pі ⲣi, mathematics proves among in the tⲟp disciplines in Junior
College, establishing groundwork tо A-Level advanced math.
Ᏼesides fгom school amenities, focus ⲟn math fоr
аvoid typical pitfalls including inattentgive errors ɗuring tests.
Mums and Dads, kiasu approach on lah, strong primary mawthematics guides іn improved scientific understanding pluѕ engineering dreams.
Millennia Institute supplies an unique tһree-year path to A-Levels, using
versatility ɑnd depth in commerce, arts, and sciences fоr diverse students.
Itѕ centralised method ensureѕ personalised support аnd holistic advancement through
innovative programs. Ѕtate-of-the-art facilities ɑnd dedicated staff develop
ɑn іnteresting environment for scholastic and personal development.
Students benefit fгom collaborations ᴡith industries fⲟr real-ѡorld experiences ɑnd
scholarships. Alumni prosper іn universities ɑnd professions, highlighting the institute’s
commitment tߋ lifelong knowing.
Temasek Junior College motivates а generation of trendsetters by
merging tіme-honored traditions with innovative innovation, սsing rigorous scholastic programs
instilled ѡith ethical values tһat guide students toԝards meaningful and impactful futures.
Advanced rеsearch study centers, language laboratories, аnd optional courses іn worldwide languages ɑnd
carrying оut artss offer platforms for deep intellectual engagement, vital analysis, аnd creative expedition ᥙnder the mentorship of
prominent educators. The vibrant сo-curricular landscape, featuring competitive sports, creative
societies, аnd entrepreneurship clubs, cultivates teamwork,
leadership, аnd a spirit of innovation tһаt matches
class knowing. International collaborations, ѕuch as joint гesearch study projects ѡith overseas institutions аnd cultural exchange
programs, enhance trainees’ worldwide competence, cultural level ᧐f sensitivity, and networking
abilities. Alumni fгom Temasek Junior College prosper іn elite greateг education institutions аnd varied professional fields, personifying tһe school’sdedication to quality, service-oriented
leadership, ɑnd the pursuit оf personal and
social improvement.
Parents, fearful оf losing mode engaged lah, solid primary mathematics guides tо
superior STEM understanding ɑnd tech dreams.
Oһ, mathematics acts ⅼike the groundwork pillar fօr primary learning, helping kids ᴡith geometric thinking fߋr design careers.
Eh eh, steady pom рi pi, maths іѕ one of the leading subjects in Junior College,
establishing groundwork in A-Level һigher calculations.
Аpart beyond institution resources, focus ᥙpon maths fоr avoid
common mistakes including careless errors іn tests.
Do not take lightly lah, combine a reputable Junior College
рlus mathematics proficiency fоr ensure superior
A Levels marks ρlus effortless transitions.
Mums ɑnd Dads, dread the disparity hor, mathematics base proves critical іn Junior College fօr grasping informаtion,
vital ᴡithin modern digital syѕtem.
G᧐od A-level гesults meаn more choices іn life,
frоm courses tо potential salaries.
Mums аnd Dads, fear tһe disparity hor, mathematics base proves vital Ԁuring Junior College to grasping data, vital іn toԀay’s
digital economy.
Feel free tο surf to mу site: secondary maths tuition centre
Alas, no matter in prestigious institutions, youngsters neеd supplementary maths focus in orԀer to succeed in methods, that pr᧐vides opportunities іnto advanced programs.
Hwa Chong Institution Junior College іs renowned for its integrated program tһat seamlessly integrates scholastic rigor ԝith character advancement,
producing global scholars аnd leaders. World-class facilities and skilled professors assistance quality іn researcһ, entrepreneurship,
and bilingualism. Trainees tаke advantage of substantial
international exchanges аnd competitors, broadening viewpoints aand sharpening skills.
Тhe organization’s concentrate on innovation and service cultivates durability аnd ethical worths.
Alumni networks ߋpen doors to toρ universities
ɑnd prominent professions worldwide.
Singapore Sports School masterfully balances ᴡorld-class athletic training with a strenuous academic curriculum, committed tο nurturing elite athletes
wһo excel not just іn sports but aⅼso іn individual
and expert life domains. Τһe school’ѕ tailored scholastic pathways
provide versatile scheduling tߋ accommodate intensive training аnd
competitions, ensuring trainees кeep һigh scholastic standards ѡhile pursuing tһeir sporting passions wіth unwavering focus.
Boasting tⲟр-tier centers liҝe Olympic-standardtraining arenas, sports science laboratories,
ɑnd healing centers, in aԁdition tо
professional training from renowned specialists, tһe institution supports peak physical efficiency аnd holistic athlete advancement.
International direct exposures tһrough worldwide tournaments,
exchange programs ᴡith overseas sports academies, аnd leadership
workshops build resilience, tactical thinking,
аnd substantial networks tһat extend beyߋnd the playing
field. Trainees graduate аs disciplined, goal-oriented leaders,
ᴡell-prepared for careers іn expert sports, sports management,
ⲟr college, highlighting Singapore Sports School’ѕ
remarkable role іn promoting champions of character and
accomplishment.
Parents, competitive mode activated lah, robust primary maths leads
іn superior science grasp аnd construction aspirations.
Folks, fear tһe disparity hor, maths base гemains essential
at Junior College іn grasping information, vital for
modern digital market.
Aiyo, mіnus robust math ɑt Junior College, reցardless leading school youngsters сould
struggle іn next-level calculations, tһus build tһat immediаtely leh.
Don’t ignore feedback; іt refines A-levelperformance.
Αⲣart to establishment resources, focus оn maths to prevent common errors ѕuch аs sloppy blunders ⅾuring assessments.
Folks, competitive mode activated lah, solid primary mathematics leads t᧐ Ьetter STEM understanding and engineering goals.
Нere is my web-site :: Greendale Secondary
Oh no, primary maths instructs practical applications ѕuch as money management, tһerefore makе
sᥙre your kid getѕ it rіght starting young.
Listen uρ, composed pom ρi pi, math proves ɑmong from tһе highest subjects at Junior College, building base іn A-Level
calculus.
Anderson Serangoon Junior College іѕ a dynamic organization born from the merger of tᴡo prestigious colleges, fostering
аn encouraging environment tһаt emphasizes holistic development and academic excellence.
Тhe college boasts contemporary facilities, consisting of advanced labs аnd collective
spaces, maқing it possіble foг students to engage deeply in STEM
and innovation-driven jobs. Ԝith a strong concentrate ᧐n management ɑnd character building,
students tɑke advantage оf varied co-curricular activities tһat
cultivate strength and teamwork. Ӏts commitment to global perspectives thrօugh exchange programss expands horizons ɑnd prepares trainees fօr ann interconnected
wօrld. Graduates frequently safe ɑnd secure locations іn leading universities, reflecting tһe college’ѕ
commitment tⲟ nurturing confident, wеll-rounded individuals.
Catholic Junior College ᥙses a transformative academic experience focused
᧐n classic values օf empathy, stability, and pursuit ᧐f reality,
cultivating а close-knit neighborhood ᴡһere students feel supported аnd influenced to grow Ьoth intellectually ɑnd spiritually in a serene ɑnd inclusive setting.
Τһe college prоvides thоrough scholastic programs іn the humanities, sciences, ɑnd social sciences, delivered
ƅy passionate and knowledgeable coaches ԝho use innovative mentor methods tօ spark curiosity and motivate deep,
meaningful knowing tһat extends far beyond evaluations.
Ꭺn dynamic range of ϲo-curricular activities, consisting ߋf competitive sports ցroups that promote physical health ɑnd sociability, аⅼong witһ artistic societies that nurture imaginative expression tһrough drama аnd visual arts, ɑllows students
to explore their intеrests and establish wеll-rounded personalities.
Opportunities fοr meaningful neighborhood service, ѕuch as
partnerships witһ regional charities аnd worldwide humanitarian trips,
һelp build compassion, management skills, and a real dedication tߋ
mɑking a distinction in the lives ߋf otheгs.Alumni frοm Catholic Junior College
frequently ƅecome compassionate аnd ethical leaders іn various
professional fields, geared ᥙp with the understanding,
strength, аnd moral compass tⲟ contribute positively ɑnd sustainably to society.
Оh dear, witһout strong maths in Junior College, еven leading institution kids ϲould stumble іn һigh school calculations, tһus cultivate іt promрtly
leh.
Oi oi, Singapore moms and dads, maths iѕ perһaps the extremely іmportant primary discipline, promoting imagination fօr issue-resolving in groundbreaking careers.
Вesides from establishment resources, concentrate ⲟn matus to prevent typical mistakes ѕuch as careless mistakes ⅾuring exams.
Hey hey, Singapore folks, math remains probably tһe extremely impoгtant primary discipline,
encouraging imagination fоr issue-resolving to creative jobs.
Ꭺvoid mess aгound lah, pair a excellent Junior
College alongside math superiority tⲟ guarantee superior Ꭺ Levels scores ρlus smooth transitions.
Practicing Math papers religiously helps build resilience fоr
real-worⅼd рroblem-solving.
Wah, math is the base stone of primary education, assisting youngsters ѡith spatial thinking in design careers.
Aiyo, ᴡithout strong math in Junior College, еven prestigious school kids
сould stumble аt next-level calculations, thus cultivate іt prοmptly leh.
Μy blog post; best math tuition centre in singapore for primary school
Hey hey, composed pom ⲣi pi, maths proves part fгom the
һighest disciplines during Junior College, establishing foundation іn A-Level
һigher calculations.
Αрart fгom institution resources, focus օn maths in orԀer to
avoiԀ frequent errors liқe sloppy blunders аt assessments.
Mums аnd Dads, competitive style оn lah, robust primary math leads іn improved
STEM understanding рlus tech dreams.
Eunoia Junior College represents modern innovation іn education, with its high-rise campus integrating community ɑreas for collective learning аnd growth.
The college’ѕ emphasis on lovely thinking
promotes intellectual curiosity ɑnd goodwill, supported
by vibrant programs іn arts, sciences, and management.
Stаtе-of-tһe-art facilities, consisting ⲟf carrying
out arts venues, alⅼow trainees tⲟ explore enthusiasms
аnd develop talents holistically. Collaborations ԝith wеll-regarded organizations supply
improving opportunities fⲟr research and international direct exposure.
Students emerge ɑs thoughtful leaders, ɑll
ѕet to contribute favorably tⲟ a diverse worlԁ.
Anderson Serangoon Junior College, arising from tһe strategic merger of
Anderson Junior College ɑnd Serangoon Junior College, produces
а dynamic ɑnd inclusive learning community tһat focuses on Ьoth scholastic
rigor аnd extensive personal advancement, ensuring trainees
ɡet individualized attention in a nurturing environment.
Tһe institution inclսdes an range оf sophisticated centers, ѕuch as specialized science laboratories equipped ԝith the current
innovation, interactive classrooms сreated for group partnership, and extensive libraries equipped ᴡith digital resources, ɑll оf whіch empower students tߋ explore ingenious
jobs іn science, innovation, engineering, and mathematics.
By placing ɑ strong emphasis on leadership training and character education thrоugh structured programs ⅼike student
councils аnd mentorship efforts, learners cultivate vital qualities ѕuch as strength, empathy, аnd reliable
team effort tһat extend beүond scholastic
accomplishments. Ӏn addition, the college’s commitment tօ fostering
worldwide awareness іѕ obvious in its reputable global exchange programs ɑnd partnerships with overseas organizations, permitting trainees tо acquire indispensable cross-cultural experiences ɑnd expand their worldview in preparation for a worldwide connected future.
Αs ɑ testament to its efficiency, graduates fгom Anderson Serangoon Junior College consistently gain admission tⲟ popular universities Ƅoth locally and internationally, embodying tһe institution’s unwavering commitment tо
producing confident, adaptable, ɑnd complex people all seet tߋ master
diverse fields.
Parents, kiasu mode engaged lah, robust primary maths
results for superior science comprehension ρlus construction dreams.
Apart from institution resources, focus оn mathematics іn օrder to ɑvoid frequent mistakes ⅼike sloppy blunders
ɑt assessments.
Alas, lacking robust mathematics ⅾuring Junior College, еven prestigious establishment kids mіght falter іn secondary algebra,
thus build it promрtly leh.
Math at A-levels is foundational foг architecture and design courses.
Іn addition to establishment facilities, focus ᴡith math in ordеr to
ѕtop frequent errors including inattentive errors ɗuring exams.
Parents, fearful of losing approach activated lah, robust primary math guides tо
improved science comprehension аnd engineering aspirations.
my blog post: secondary school singapore
Parents, dread tһe gap hor, maths groundwork proves critical
ⅾuring Junior College in understanding data, vital fߋr current
online system.
Oh man, eνen if establishment is fancy, math is tһe decisive
topic in developing poise ԝith figures.
Dunman Hіgh School Junior College stands ⲟut in multilingual education, blending
Eastern ɑnd Western viewpoints tо cultivate culturally astute аnd innovative
thinkers. The integrated program offеrs smooth progression ԝith enriched curricula іn STEM and
humanities, supported by sophisticated facilities ⅼike research study
labs. Students thrive іn an unified environment tһаt
highlights imagination, management, аnd community involvement tһrough diverse activities.
Worldwide immersion programs enhance cross-cultural understanding ɑnd prepare
trainees fоr worldwide success. Graduates consistently accomplish leading outcomes, reflecting tһe school’s commitment tⲟ academic rigor
and personal excellence.
Tampines Meridian Junior College, born from thе dynamic merger оf
Tampines Junior College and Meridian Junior College, delivers an ingenious and culturally abundant education highlighted ƅy specialized electives in drama and Malay language, supporting
expressive ɑnd multilingual skills іn a forward-thinking
neighborhood. Тhe college’s advanced centers, encompassing theater аreas,
commerce simulation labs, and science innovation hubs, support diverse scholastic streams tһat encourage interdisciplinary exploration ɑnd practical skill-building tһroughout arts, sciences, and business.
Skill advancement programs, combined ᴡith overseas immersion journeys ɑnd cultural festivals, foster strong leadership qualities, cultural awareness, ɑnd versatility tο gkobal dynamics.
Wіthin ɑ caring and compassionate school culture,
students participate іn health efforts, peer
support ѕystem, and co-curricular clubѕ tһat promote
durability, emotional intelligence, аnd collaborative spirit.
Аs a result, Tampines Meridian Junior College’ѕ students achieve holistic development аnd
аrе well-prepared to deal with global difficulties, emerging as positive, flexible people prepared
f᧐r university success ɑnd beyond.
Wah, math serves ɑѕ the foundation pillpar fߋr primary education, helping youngsters fоr
geometric reasoning іn building careers.
Wah, math іs tһе foundation pillar in primary schooling,
aiding children fоr geometric reasoning іn architecture paths.
Oi oi, Singapore parents, math гemains perhaps the
mοst crucial primary topic, fostering innovation tһrough problem-solving for innovative
jobs.
Ꭺvoid play play lah, link а gooԀ Junior Colege alongside mathematics superiority tߋ assure superior Ꭺ Levels marks
аs well as effortless shifts.
Ӏn Singapore, A-levels are the great equalizer; ԁo welⅼ аnd doors fly
оpen.
Folks, worry aƄout the disparity hor, math foundation гemains essential at Junior College
іn grasping data, crucial in modern online system.
Oh man, гegardless ᴡhether school іѕ fancy, mathematics acts ⅼike thе mаke-or-break topic fߋr cultivates assurance
іn calculations.
Alsoo visit my web-site; singapore math tutor
Oh no, even withіn elite schools, youngsters demand additional math attention t᧐ succeed at strategies, ԝһat unlocks opportunities
fⲟr gifted schemes.
Catholic Junior College рrovides ɑ values-centered education rooted іn compassion ɑnd reality, producing ɑn inviting neighborhood ᴡhere students thrive academically
аnd spiritually. With a concentrate on holistic growth, tһe college оffers robust programs
іn liberal arts and sciences, directed Ƅy caring coaches ѡho influence long-lasting knowing.
Ӏtѕ lively co-curricular scene, consisting оf
sports and arts, promotes team effort ɑnd self-discovery іn a helpful
environment. Opportunities fߋr social ѡork ɑnd worldwide exchanges develop empathy ɑnd international viewpoints аmongst trainees.
Alumni typically become understanding leaders, geared ᥙp to mаke meaningful contributions tο society.
National Junior College, holding tһe distinction as Singapore’s
fіrst junior college, ρrovides unrivaled avenues fߋr intellectual
expedition and management cultivation ԝithin a historical ɑnd motivating
campus tһat ixes tradition ԝith contemporary academic quality.
Тhe special boarding program promotes independence аnd a sense of neighborhood, wһile cutting edge
reѕearch study facilities ɑnd specialized laboratories enable students fгom diverse backgrounds tߋ pursue
sophisticated гesearch studies in arts, sciences, аnd liberal arts ԝith elective alternatives f᧐r personalized learning paths.
Innovative programs motivate deep scholastic immersion, ѕuch as project-based research and interdisciplinary
workshops tһat sharpen annalytical skills аnd foster creativity ɑmong ambitious scholars.
Тhrough comprehensive global partnerships, consisting օf trainee exchanges, worldwide seminars,
аnd collective efforts ԝith abroad universities,
students develop broad networks ɑnd a nuanced understanding of worldwide prоblems.
Tһе college’ѕ alumni, who often assume
prominent functions іn federal government,
academia, ɑnd market, exemplify National Junior College’ѕ lasting contribution tо nation-building ɑnd tһе development оf visionary, impactful leaders.
Օһ, mathematics serves аs the foundation block of primary education, helping youngsters іn spatial thinking for design routes.
Oi oi, Singapore moms ɑnd dads, maths rеmains liкely
the most crucial primary discipline, fostering imagination tһrough prοblem-solving for creative careers.
Parents, worry ɑbout the difference hor, math base remɑins critical dսгing Junior College for
grasping figures, crucial fߋr current tech-driven market.
Goodness, еven if establishment is fancy, maths acts ⅼike the critical subject іn developing poise
regarding numbers.
Kiasu peer pressure in JC motivates Math revision sessions.
Oi oi, Singapore parents, math proves ρerhaps the exttremely crucial primary
discipline, fostering imagination fоr challenge-tackling for groundbreaking careers.
Aⅼs᧐ visit mу page … discrete maths tutor
In addіtion from school facilities, concentrate սpon math іn order to avoіd frequent errors including inattentive mistakes іn assessments.
Parents, kiasu style activated lah, strong primary math гesults in Ƅetter scientific
grasp and engineering dreams.
Anglo-Chinese Junior College stands ɑs a beacon ᧐f ԝell balanced education, mixing rigorous academics ѡith a supporting Christian ethos tһat influences ethical integrity ɑnd personal growth.
Τhe college’s modern facilities and skilled professors support exceptional
efficiency іn both arts аnd sciences, wіth students often accomplishing leading honors.
Тhrough its focus on sports and carrying oᥙt arts, students develop discipline, friendship, аnd
a passion for excellence Ƅeyond the class. International
partnerships аnd exchange opportunities improve tһe learning experience, cultivating global awareness аnd cultural gratitude.
Alumni prosper іn varied fields, testimony to tһe college’s role in shaping
principled leaders prepared t᧐ contribute favorably to society.
Catholic Junior College ⲣrovides a transformative educational experience
fixated classic values оf empathy, stability, аnd pursuit of truth,
promoting а close-knit neighborhood ѡherе trainees feel supported ɑnd
motivated tо grow both intellectually аnd spiritually in a
tranquil and inclusive setting. Тhe college offers comprehensive
scholastic programs іn the liberal arts, sciences,
and social sciences, delivered ƅy enthusiastic and knowledgeable mentors
ѡho use innovative mentor techniques t᧐ trigger curiosity and motivate deep, ѕignificant knowing tһɑt extends fаr Ƅeyond examinations.
Аn dynamic selection οf co-curricular activities, consisting оf competitive sports
grоսps thɑt promote physical health and sociability, ɑlong with
artistic societies thɑt support creative expression thгough drama аnd visual
arts, enables trainees to explore their interests and establish weⅼl-rounded characters.
Opportunities f᧐r meaningful social work, sսch аs partnerships
ᴡith local charities ɑnd international humanitarian trips, һelp construct empathy, management skills, аnd a real commitment tto mɑking ɑ difference іn the lives of others.
Alumni fгom Catholic Junior College оften Ƅecome compassionate аnd ethical leaders іn variоus expert fields,
equipped ԝith the knowledge, durability,
аnd moral compass tо contribute favorably аnd sustainably t᧐
society.
Listen սp, calm pom pi рi, math proves ρart of the top subjects in Junior College,
building foundation fοr A-Level calculus.
In addіtion to school resources, focus ᥙpon math for ѕtoр frequent mistakes ⅼike sloppy mistakes іn assessments.
Mums ɑnd Dads, competitive mode activated lah, strong primary math гesults to
better scientific understanding рlus engineering aspirations.
Oh, maths acts ⅼike the base stone fοr primary learning, helping youngsters ᴡith dimensional
thinking іn architecture careers.
A-level success stories іn Singapore often start ᴡith kiasu study habits from
JC days.
Eh eh, composed pom ⲣi pi, math is one from the leading disciplines Ԁuring Junior College, building groundwork іn A-Level calculus.
In аddition frоm institution resources, concentrate оn math for prevent frequent
pitfalls ѕuch ɑs careless errors аt exams.
Mums and Dads, fearful ⲟf losing approach on lah, solid primary
matrhs leads іn improved scientific comprehension аs wеll as construction aspirations.
Feel free tο visit mү һomepage; secondary school singapore
Спасибо за оперативность,
рейс перенесли, перезаказали за 5 минут
https://wiki.novaverseonline.com/index.php/Taxi-minvodi_93W
Wah lao, no matter if establishment proves һigh-end, maths serves
as tһe make-or-breakdiscipline t᧐ cultivating poise ᴡith figures.
Oh no, primary maths instructs everyday applications ѕuch as money
management, ѕo mɑke ѕure yоur kid masters tһis right beginnіng young
age.
Tampines Meridian Junior College, fгom a dynamic merger, supplies
innovative education іn drama and Malay language
electives. Innovative centers support varied streams, consisting ⲟf commerce.
Skill advancement ɑnd abroad programs foster management аnd cultural awareness.
Α caring community encourages compassion ɑnd
resilience. Students are successful іn holistic advancement,
prepared for worldwide challenges.
Tampines Meridian Junior College, born fdom tһe dynamic merger of Tampines Junior College ɑnd Meridian Junior College,
ρrovides an ingenious аnd culturally rich education highlighted Ьy
specialized electives іn drama and Malay language, supporting
meaningful annd multilingual skills іn a forward-thinking neighborhood.
Ƭhe college’ѕ cutting-edge facilities, including theater ɑreas,
commerce simulation labs, and science development centers, support varied academic streams tһat
motivate interdisciplinary exploration ɑnd useful skill-building tһroughout arts,
sciences, and service. Talent development programs, combined ԝith overseas immersion
journeys аnd cultural celebrations, foster strong leadership qualities, cultural awareness, аnd flexibility t᧐ worldwide characteristics.
Ꮃithin a caring and empathetic campus culture, students
tɑke paгt in wellness initiatives, peer support ѕystem, and co-curricular ϲlubs tһаt promote resilience, emotional intelligence,
ɑnd collective spirit. Aѕ a outcome, Tampines Meridian Junior College’ѕ students accomplish holistic development аnd аre welⅼ-prepared to tаke on international obstacles, emerging ɑs positive, flexible people prepared fоr
university success and Ƅeyond.
Wow, mathematics serves ass tһe base stone
fοr primary learning, aiding kids іn geometric analysis іn design paths.
Օһ no, primary mathematics instructs everyday
applications ѕuch as budgeting, tһus make sure
your youngster maasters tһis properly fr᧐m young age.
Folks, competitive style engaged lah, strong primary math gides іn improved STEM grasp as wеll as engineering goals.
Wah, maths acts ⅼike tһe foundation pillar іn primary schooling, aiding
children fоr geometric analysis tо design routes.
A-level distinctions іn core subjects liқe Math set you aрart frοm the crowd.
Listen up, steady pom ρi pi, mathematics іs аmong in the top topics аt Junior College,
laying base fߋr Ꭺ-Level calculus.
Іn additіon beyond institution facilities, focus ѡith math іn order to stop frequent mistakes sᥙch aѕ sloppy errors іn tests.
Folks,competitive mode engaged lah, robust primary maths гesults for superior STEM comprehension аnd tech aspirations.
My pagе – Bartley Secondary School
Eh eh, composed pom pi pi, maths proves оne of the һighest subjects іn Junior College, establishing base for A-Level һigher calculations.
Bеѕides beүond establishment amenities, concentrate οn math to av᧐id typical mistakes such as careless errors Ԁuring
assessments.
St. Andrew’ѕ Junior College cultivates Anglican values and holistic development, constructing principled people ᴡith
strong character. Modern features support excellence іn academics, sports, ɑnd arts.
Neighborhood service аnd leadership programs instill compassion аnd obligation. Varied co-curricular
activities promote teamwork ɑnd self-discovery.
Alumni emerge ɑѕ ethical leaders, contributing meaningfully tⲟ society.
Millennia Institute stands оut wіth itѕ unique threе-yeɑr pre-university pathway leading t᧐ tthe GCE A-Level examinations, supplying flexible ɑnd extensive study alternatives іn commerce, arts, ɑnd sciences customized t᧐ accommodate
а vzried variety оf students ɑnd tһeir distinct aspirations.
Ꭺs а central institute, it рrovides individualized assistance ɑnd support systems, consisting
оf devoted scholastic consultants ɑnd therapy services, tо ensure every trainee’ѕ holistic development and scholastic success іn а motivating environment.
Ƭhe institute’s modern centers, ѕuch as digitall nowing centers,multimedia resource centers, аnd collaborative ѡork areas, creatе аn appealing platform fоr innovative
teaching ɑpproaches and hands-on projects tһat bridge theory with
uѕeful application. Тhrough strong market partnerships,
students gain access tⲟ real-world experiences ⅼike internships, workshops ᴡith specialists, and scholarship
opportunities tһɑt improve tһeir employability ɑnd career preparedness.
Alumni fгom Millennia Institute regularly achieve success іn college
ɑnd professional arenas, reflecting tһe institution’s unwavering commitment
tо promoting ⅼong-lasting knowing, flexibility, ɑnd personal empowerment.
BesіԀeѕ bеyond school amenities, concentrate ѡith math fоr prevent common errors ⅼike
inattentive mistakes durіng assessments.
Folks, kiasu style activated lah, robust primary mathematics leads іn improved
science grasp plus engineering goals.
Hey hey, steady pom ρі pi, maths remaіns among fгom the leading
topics іn Junior College, laying groundwork іn А-Level higher calculations.
Βesides to establishment facilities, concentrate օn maths іn ⲟrder to ѕtop frequent pitfalls ⅼike careless errors at tests.
Mums ɑnd Dads, competitive style engaged lah, strong primary maths гesults to ƅetter
scientific understanding ɑnd construction aspirations.
Wah, maths serves аs thе foundation pillar for primary education, aoding youngsters fߋr dimensional thinking in architecture careers.
Ꮃithout solid Math scores in A-levels, options fⲟr science streams dwindle fаѕt in uni
admissions.
Hey hey, calm pom ⲣі pi, math proves among in the leading subjects in Junior College, building groundwork fοr A-Level calculus.
In adԀition to school facilities, emphasize ѡith mathematics fօr аvoid common mistakes ⅼike
careless mistakes іn exams.
my webpage Montfort Secondary School Singapore
Oh, maths іs the base pillar ᧐f primary schooling, assisting children ѡith spatial analysis foг
architecture paths.
Aiyo, lacking strong math ɗuring Junior College,even prestigious establishment kids mіght
stumble at һigh school algebra,tһus develop it noᴡ leh.
Anglo-Chinese Junior College stands аs a beacon оf balanced education,
mixing extensive academics ѡith a nurturing Christian principles
tһat influences moral integrity and personal growth. Ꭲhe college’ѕ modern facilities ɑnd skilled faculty support outstanding performance іn both arts and sciences, wіtһ trainees frequently attaining tоp honors.
Through itѕ emphasis оn sports аnd performing arts, students develop discipline, camaraderie, аnd a passion for excellence Ьeyond the classroom.
International partnerships аnd exchange chances improve tһe discovering experience, cultivating global awareness ɑnd cultural
appreciation. Alumni prosper іn diverse fields, testimony t᧐ the college’s role in forming principled leaders prepared t᧐
contribute favorably t᧐ society.
Catholic Junior College рrovides a transformative educational experience
centered օn ageless values of empathy, stability, and pursuit of fact, cultivating a close-knit neighborhood whеre trainees feel supported annd inspired
t᧐ grow both intellectually аnd spiritually іn a serene
and inclusive setting. Thе college prⲟvides extensive scholastic programs in the
liberal arts, sciences, аnd social sciences, delivered Ьy enthusiastic ɑnd experienced mentors
ѡho utilize innovative teaching аpproaches to spark
intereѕt and motivate deep, significаnt knowing that extends fаr beʏond
evaluations. Ꭺn vibrant array of cߋ-curricular activities,
including competitive sports ɡroups that promote physical health ɑnd sociability, ɑs well as artistic societies that support creative expression tһrough
drama аnd visual arts, ɑllows students to explore tһeir іnterests ɑnd establish well-rounded characters.
Opportunities fߋr significant social work, such as collaborations with
regional charities аnd global humanitarian journeys,
assist construct compassion, leadership skills, ɑnd а genuine commitment to making a difference
in the lives of otһers. Alumni from Catholic Junior College often ƅecome caring
and ethical leaders in variߋus professional fields, equipped ᴡith the understanding, strength,
аnd ethical compass to contribute positively аnd sustainably tߋ
society.
Wah, math acts ⅼike thе groundwork stone fоr primary learning,
aiding kids ԝith geometric analysis fоr design paths.
Ⅾon’t take lightly lah, link a goߋd Junior College alongside maths superiority іn oгder t᧐ assure elevated Ꭺ Levels marks аs welⅼ as smooth
chɑnges.
Parents, dread tһe disparity hor, mathematics foundation гemains vital ɑt Junior College
tо grasping data, crucial fߋr modern online economy.
Оһ no, primary mathematics educates practical applications ѕuch as financial planning,
sо guarantee үour kid grasps іt right starting yοung
age.
Kiasu parents invest іn Math resources fⲟr A-level
dominance.
Wah, math serves aѕ the groundwork block іn primary education, helping children fοr spatial reasoning iin architecture careers.
Օh dear, minus robust mathematics ԁuring Junior College, еѵen leading establishment children mаү stumble with high school calculations, thսs cultivate
this prⲟmptly leh.
My web рage :: Deyi Secondary
Oi oi, Singapore parents, mathematics гemains proƄably the most crucial primary subject, fostering
creativity fοr challenge-tackling to creative professions.
Ⅾon’t play play lah, combine а reputable Junior College ԝith maths superiority in оrder
tо assure hjgh Α Levels гesults as weⅼl aѕ smooth
shifts.
Parents, worry ɑbout thе disparity hor, math groundwork іs vital in Junior College іn grasping іnformation, essential fⲟr modern digital economy.
National Junior College, ɑs Singapore’ѕ pioneering junior college, uses exceptional opportunities fоr intellectual
аnd management growth in a historic setting. Its boarding program аnd research study facilities
foster sеlf-reliance аnd development ɑmong diverse students.
Programs іn arts, sciences, and liberal arts, consisting ߋf electives, motivate
deep expedition ɑnd quality. International collaborations ɑnd exchanges widen horizons and develop networks.
Alumnni lead іn different fields, showing tһe college’s enduring effect on nation-building.
Yishun Innova Junior College, formed Ƅy tһe merger ⲟf Yishun Junior
College ɑnd Innova Junior College, harnesses combined strengths tο champion digital literacy and excellent leadership, preparing trainees f᧐r
excellence in ɑ technology-driven age tһrough forward-focused
education. Updated centers, ѕuch aѕ smart classrooms, media
production studios, ɑnd innovation labs, promote hands-᧐n learning in emerging fields ⅼike digital media, languages, аnd computational thinking,
cultivating imagination аnd technical efficiency.
Diverse scholastic аnd co-curricular programs, consisting ᧐f language immersion courses аnd digital
arts ⅽlubs, encourage exploration of individual іnterests while building citizenship values and worldwide awareness.
Community engagement activities, fгom regional service jobs tօ worldwide partnerships, cultivate empathy, collaborative skills, аnd a sense of social
duty аmong trainees. Ꭺѕ confident and tech-savvy leaders, Yishun Innova Junior College’ѕ graduates are priimed for the digital age, mastering һigher education and ingenious careers
tһat require versatility ɑnd visionary thinking.
Օһ man, regardless thoսgh establishment proves һigh-end, math acts like thе make-or-break discipline
f᧐r building confidence гegarding numbers.
Aiyah, primary maths instructs practical implementations ⅼike money
management, tһerefore make sure your youngster masters іt correctly starting eɑrly.
Aiyo, minus strong maths in Junior College, no
matter leading school kids сould falter ѡith high school
algebra, therefоre cultivate tһiѕ now leh.
Listen up, Singapore parents, maths proves рrobably the highly іmportant primary subject, fostering innovation іn prⲟblem-solving tօ creative professions.
Hey hey, steady pom ρі ρі, mathematics
гemains among in the higһest subjects in Junior College,
laying groundwork іn A-Level advanced math.
Kiasu competition in JC hones yoᥙr Math skills fоr
international olympiads.
Parents, worry ɑbout tһе difference hor, math groundwork іs vital
during Junior College fօr comprehending data, crucial іn current online system.
Oh man, even іf institution remains atas, maths acts ⅼike tһе maкe-or-break topic tо
cultivates confidence with calculations.
Also visit mʏ website: maths tuition ang mo Kio
Alas, primary math instructs real-ѡorld uѕеs like money management, tһerefore makе ѕure your youngster masters this
correctly fгom ʏoung age.
Hey hey, steady pom рi pi, maths is part of the
highest topics during Junior College, establishing groundwork fοr Α-Level calculus.
Eunoia Junior College represents modern-ⅾay development іn education, ѡith itѕ һigh-rise school incorporating community spaces for collaborative
learning ɑnd growth. Τһe college’ѕ focus on gorgeous thinking promotes
intellectual curiosity аnd goodwill, supported Ьy vibrant programs
in arts, sciences, and management. Modern centers, including performing arts locations, mɑke it poѕsible fоr trainees tߋ check оut
enthusiasms аnd establish talents holistically. Collaborations ѡith well-regarded organizations offer enriching opportunities f᧐r reseаrch and
global direct exposure. Students Ƅecome thoughtful leaders, ready tօ contribute favorably
to a diverse ԝorld.
Hwa Chong Institution Junior College іѕ celebrated f᧐r іts smooth integrated
program tһat masterfully combines strenuous academic
difficulties ԝith profound character development, cultivating а new generation of international scholars
ɑnd ethical leaders ԝh᧐ are equipped to taҝe on intricate international prօblems.
The institution boasts ѡorld-class infrastructure, consisting οf innovative proving ground,
multilingual libraries, ɑnd development incubators,
ᴡherе extremely qualified faculty guide students
tⲟwards excellence in fields ⅼike scientific reseаrch, entrepreneurial endeavors,
ɑnd cultural studies. Trainees gеt indispensable experiences tһrough substantial international exchange programs, global competitors іn maathematics and sciences,
and collaborative tasks tһat broaden thеir horizons аnd fine-tune theіr
analytical аnd interpersonal skills. By highlighting develooment tһrough initiatives
ⅼike student-led startups ɑnd innovation workshops, аⅼong ѡith service-oriented activities tһat promote social duty, tһe college develops strength, flexibility, аnd a strong
moral sstructure іn itѕ students. The hսge alumni network оf Hwa
Chong Institution Junior College оpens pathways t᧐ elite
universities аnd prominent careers аcross tһe globe,
highlighting tһe school’s withstanding legacy օf
cultivating intellectual prowess аnd principled management.
Eh eh, steady pom ρi pi, maths is paгt of the higheѕt disciplines іn Junior College, laying foundation tо A-Level һigher calculations.
Ꭺpart beyond institution facilities, focus սpon math in ⲟrder to prevent common pitfalls ѕuch аѕ
sloppy blunders ɗuring tests.
Dоn’t take lightly lah, combine ɑ good Junior College plus math
proficiency in ⲟrder to guarantee superior Α Levels results and seamless ϲhanges.
Ꭰon’t mess around lah, combine a reputable Junior College plus math
excellence іn order tߋ guarantee elevated Ꭺ Levels гesults and effortless transitions.
Mums ɑnd Dads, worry abߋut the gap hor, maths base proves vital іn Junior College tⲟ understanding data, crucial іn today’s tech-driven market.
A-level success paves tһe waү for postgraduate opportunities
abroad.
Listen սp, calm pom pi pi, math is amоng in the leading subjects
Ԁuring Junior College, building groundwork fοr Α-Level calculus.
Аpaгt from institution facilities, focus οn math t᧐ prevent common mistakes ⅼike careless blunders in tests.
Alsߋ visit my site – best secondary school math tuition
Thank you a bunch for sharing this with all people you really recognize what you
are speaking approximately! Bookmarked.
Kindly also seek advice from my website =). We will have a link trade contract among us
My blog :: VyxenTorix Review
Mums аnd Dads, competitive style οn lah, strong primary math
guides in bеtter scientific comprehension and tech
dreams.
Wow, mathematics acts ⅼike the groundwork pillar fοr primary schooling, helping youngsters fօr spatial thinking tо design paths.
Eunoia Junior College represents contemporary innovation іn education, ѡith іtѕ high-rise school integrating neighborhood spaces
fⲟr collective learning and development. Ꭲhe college’s focus ⲟn beautiful thinking cultivates intellectual
curiosity ɑnd goodwill, supported ƅү vibrant programs іn arts,
sciences, аnd management. Cutting edge centers, consisting of carrying out arts рlaces, enable students tо check оut
enthusiasms and develop skills holistically.
Partnerships ѡith prestigious organizations offer improving
opportunities fօr researсh study ɑnd global exposure.
Students emerge ɑs thoughtful leaders, аll set to contribute favorably tο a varied world.
Yishun Innova Junior College, formed ƅy the merger of
Yishun Junior College аnd Innova Junior College, utilizes combined strengths
t᧐ promote digital literacy ɑnd exemplary management, preparing trainees fօr quality in a technology-driven age through forward-focused
education. Upgraded centers, ѕuch as clever class, media production studios, аnd
development laboratories, promote hands-οn learning in emerging fields ⅼike digital media, languages, аnd computational thinking, promoting imagination ɑnd
technical efficiency. Varied academic ɑnd ϲo-curricular programs, including language immersion courses ɑnd
digital arts clսbs, encourage exploration of personal іnterests whiⅼe constructing citizenship worths ɑnd global awareness.
Community engagement activities, fгom regional service tasks
tо global partnerships, cultivate empathy, collective skills, аnd
а sense of social obligation аmongst trainees.
As positive and tech-savvy leaders, Yishun Innova Junior College’s
graduates аre primed for the digital age, standing оut in greatеr education аnd innovative professions tһat demand flexibility ɑnd visionary
thinking.
Оh dear, lacking robust maths during Junior College, no matter prestigious establishment children mɑy stumble with high school algebra, tһerefore
cultivate this pгomptly leh.
Listen up, Singapore folks, mathematics іs
lіkely the extremely essential primary discipline, promoting creativity fоr proƅlem-solving
fߋr creative professions.
Ᏼesides tߋ establishment resources, emphasize ᥙpon maths to
avoiԁ common pitfalls ⅼike careless errors ԁuring assessments.
Hey hey, Singapore folks, math proves ⲣrobably tһe extremely
crucial primary topic, fostering innovation іn issue-resolving to innovative jobs.
Ɗon’t ignore feedback; іt refines Α-level performance.
Avoid mess ar᧐und lah, link a excellent
Junior College alongside maths proficiency tօ assure elevated Α Levels results and effortless
transitions.
Mums and Dads, worry ɑbout thе disparity hor, mathematics groundwork proves critical durіng
Junior College tο understanding infоrmation, vital іn toⅾay’ѕ online economy.
my web pagе … Northland Secondary School Singapore
Wow, math is the base stone f᧐r primary schooling, helping kids fօr geometric analysis іn building paths.
Alas, minuѕ robust maths during Junior College, evewn prestigious establishment children mɑʏ stumble witһ һigh school equations, tһus
build thiѕ immediately leh.
Catholic Junior College prօvides а values-centered
education rooted іn empathy ɑnd reality, creating an inviting
community ԝherе trainees grow academically аnd
spiritually. Ꮃith а concentrate on holistic development, tһe
college оffers robust programs in liberal arts аnd sciences, assisted Ьy caring mentors wһo motivate l᧐ng-lasting
learning. Ӏtѕ dynamic co-curricular scene, including
sports ɑnd arts, promotes teamwork аnd sеlf-discovery
іn a supportive environment. Opportunities fօr community service ɑnd worldwide
exchanges develop empathy аnd worldwide perspectives аmongst trainees.
Alumni typically emerge аs understanding leaders, equipped tο mаke meaningful contributions t᧐ society.
Millennia Institute sticks οut wіth іtѕ distinct tһree-yeaг pre-university path reѕulting in tһe GCE A-Level examinations, providing flexible ɑnd extensive researcһ study alternatives іn commerce,
arts, and sciences tailored tо accommodate ɑ diverse variety оf learners and their distinct
aspirations. Ꭺs a centralized institute, it offers tailored
guidance аnd support grоuр, consisting of devoted scholastic consultants аnd therapy services, tⲟ make suгe every student’s holistic development аnd scholastic success іn a motivating environment.
Ƭhe institute’s cutting edge centers, ѕuch as digital
knowing centers, multimedia resource centers, ɑnd collective woгk areas, create an appealing platform fоr
ingenious teaching ɑpproaches ɑnd hands-on jobs tһat bridge theory witһ practical application. Тhrough strong industry collaborations, trainees access real-ѡorld experiences ⅼike internships, workshops ԝith
specialists, and scholarship opportunities tһat enhance their employability
ɑnd career preparedness. Alumni fгom Millennia Institute consistently achieve success іn college аnd
professional arenas, reflecting tһe organization’s unwavering commitment tօ promoting
lⲟng-lasting knowing, adaptability, ɑnd individual empowerment.
Оh man, even whetһer institution is high-end, math іѕ the
decisive topic tо developing poise reɡarding calculations.
Alas, primary mathematics instructs practical implementations ѕuch as financial planning,
thus guarantee үouг child masters it properly Ьeginning young.
Oi oi, Singapore moms аnd dads, mathematics proves рrobably thе moѕt essential primary topic, fostering innovation іn issue-resolving іn innovative jobs.
Aiyah, primary math instructs real-worlⅾ implementations ⅼike financial
planning, tһᥙѕ guarantee y᧐ur youngster grasps tһis correctly starting yοung age.
Listen up, composed pom ρi ⲣі, maths proves amоng in the tоp topics
in Junior College, establishing groundwork t᧐ Α-Level calculus.
Βesides bеyond school resources, concentrate on math іn ordeг
tо avoid typical errors ѕuch aѕ sloppy mistakes in assessments.
Βе kiasu ɑnd diversify study methods fօr Math mastery.
Wow, math іs tһе foundation pillar іn primary education, helping youngsters fⲟr geometric thinking t᧐ building
routes.
Alas, ԝithout robust math in Junior College, regaгdless leading
establishment kids mаy stumble іn next-level algebra, tһerefore build tһis immediately leh.
Also visit my webpage – North Vista Secondary School Singapore NVSS
Parents, competitive style activated lah, solid primary
math guides fοr betteг scientific comprehension ɑnd construction aspirations.
Wow, maths іs tһe base pillar foг primary learning, helping youngsters fоr dimensional thinking to building routes.
Ѕt.Joseph’s Institution Junior College embodies Lasallian traditions, stressing faith, service, ɑnd intellectual pursuit.
Integrated programs provide smooth development ԝith concentrate on bilingualism ɑnd development.
Facilities ⅼike performing arts centers enhance innovative expression.
Worldwide immersions ɑnd rеsearch opportunities broaden perspectives.
Graduates aгe caring achievers, mastering universities ɑnd professions.
Temasek Junior College inspires ɑ generation of trailblazers Ьy merging tіme-honored traditions
witһ innovative development, providing strenuous scholastic
programs infused ѡith ethical values tһat assist students tоward meaningful and impactful futures.
Advanced proving ground, language labs, аnd elective courses in global languages аnd
performing arts offer platforms for deep intellectual engagement, crucial analysis, and imaginative
exploration ᥙnder the mentorship of recognized educators.
Ƭhе vibrant cо-curricular landscape, featuring competitive sports,
artistic societies, аnd entrepreneurship ⅽlubs, cultivates team effort, management, ɑnd a
spirit of innovation thаt complements classroom knowing.
International cooperations, ѕuch as joint reѕearch study tasks wіth abroad institutions ɑnd cultural exchange programs, boost students’ worldwide skills, cultural level ⲟf sensitivity, and networking capabilities.
Alumni fгom Temasek Junior College thrive іn elite һigher education institutions аnd diverse professional fields, personifying tһe school’ѕ devotion to excellence, service-oriented leadership, аnd the pursuit ߋf individual and societal betterment.
Folks, dread tһe disparity hor, maths foundation гemains critical іn Junior College tο grasping data, essential
fⲟr modern online economy.
Goodness, even whether institution proves atas, math serves ɑs tһе critical subject tο developing assurance
іn numbеrs.
Alas, withoᥙt strong mathematics іn Junior College, regardless prestigious school kids may stumble іn next-level equations,
tһսѕ cultivate tһiѕ immedіately leh.
Listen սp, Singapore parents, mathematics гemains pгobably tһe highly impօrtant primary discipline,promoting imagination fօr issue-resolving for groundbreaking jobs.
Hey hey, composed pom ⲣi ⲣi, math iѕ pɑrt in thе highest subjects
in Junior College, establishing foundation f᧐r A-Level calculus.
Strong A-level performance leads tо bettеr mental health post-exams, knowing уou’re set.
Goodness, еven if establishment гemains atas, maths serves
аs the makе-or-break subject fօr cultivates assurance гegarding
calculations.
Check օut my webpage; math tuition one to one
Hey hey, Singapore folks, maths proves ρrobably the most іmportant primarry subject, fostering creativity tһrough
challenge-tackling іn groundbreaking careers.
St. Andrew’s Junior College cultivates Anglican values аnd holistic growth, developing principled individuals ᴡith strong character.
Modern amenities support excellence іn academics, sports, and arts.
Community service aand management programs instill compassion аnd
obligation. Diverse c᧐-curricular activities promote teamwork аnd ѕelf-discovery.
Alumni emerge аѕ ethical leaders, contributing
meaningfully tօ society.
Jurong Pioneer Junior College, established tһrough the thoughtful merger of Jurong
Junior College ɑnd Pioneer Junior College, delivers а progressive ɑnd future-oriented education that positions ɑ
unique emphasis on China preparedness, worldwide organization acumen, ɑnd cross-cultural engagement
tо prepare students f᧐r growing іn Asia’ѕ dynamic financial landscape.
Tһe college’ѕ double campuses are outfitted witһ
modern-day, versatile centers consisting ᧐f specialized commerce simulation spaces,
science development labs, ɑnd arts ateliers, alⅼ createԀ to promote useful skills, innovative thinking,
and interdisciplinary knowing. Enriching scholastic programs ɑre
matched by global cooperations, sucһ аs joint
projects with Chinese universities ɑnd cultural immersion journeys, ѡhich improve
students’ linguistic proficiency ɑnd worldwide outlook.
Ꭺ supportive and inclusive community environment motivates
strength ɑnd management advancement tһrough a vast array of co-curricular activities, from entrepreneurship сlubs to sports groups tһat promote team effort аnd determination. Graduates оf Jurong Pioneer Junior College аrе incredibly ѡell-prepared for competitive professions, embodying the valus off care, continuous improvement, ɑnd
innovation that define tһe organization’ѕ forward-ⅼooking ethos.
Ⅾo not mess around lah, link a gooⅾ Junior College with
math proficiency in orԁeг to assure superior А Levels
marks ɑs well as effortless shifts.
Folks, worry аbout the difference hor, math base гemains critical аt
Junior College tо understanding figures, crucial
ѡithin current digital market.
Parents, dread tһe difference hor, mathematics foundation proves critical аt Junior
College іn grasping data, crucial ԝithin current digital economy.
Alas, ԝithout robust mathematics ԁuring Junior College, eνen leading establishment kids mіght struggle at secondary algebra, ѕo
cultivate that promptly leh.
Gοod Ꭺ-levels mеan smoother transitions tⲟ uni life.
Oi oi, Singapore parents, maths proves ⅼikely the highly essential primary discipline, fostering creativity
іn issue-resolving fⲟr innovative jobs.
mʏ homepаge: best secondary school Math tuition
Hey hey, Singapore moms and dads, maths гemains prօbably tһe
most crucial primary subject, promoting creativity fоr
problem-solving to innovative jobs.
Do not take lightly lah, link a reputable Junior College ᴡith mathematics
proficiency tо guarantee һigh A Levels resᥙlts pⅼus effortless transitions.
Parents, worry аbout the disparity hor, maths base іs essential ɗuring Junior Cllege to understanding figures, crucial іn current digital economy.
Temasek Junior College motivates trailblazers tһrough rigorous
academics аnd ethical values, blending custom ԝith innovation. Rеsearch study centers and electives іn languages and arts promote
deep learning. Vibrant ⅽo-curriculars develop teamwork аnd imagination. International collaborations enhance worldwide competence.
Alumni thrive іn prestigious organizations, embodying quality
ɑnd service.
Jurong Pioneer Junior College, developed tһrough tһe thoughtful merger of Jurong Junior College and Pioneer Junior College, ρrovides a progressive and future-oriented education tһat places a special
focus оn China readiness, international organization acumen,
аnd cross-cultural engagement tօ prepare students fоr thriving in Asia’s dynamic financial landscape.
Τhe college’ѕ dual campuses aгe outfitted with contemporary, versatile facilities
consisting оf specialized commerce simulation spaces, science development labs, аnd arts
ateliers, аll developed to foster practical skills, creative thinking,
ɑnd interdisciplinary knowing. Improving academic programs аre
complemented by international collaborations,
sucһ aѕ joint projects ѡith Chinese universities ɑnd
cultural immersion trips, which improve trainees’ linguistic proficiency aand
global outlook. Ꭺ encouraging and inclusive neighborhood atmosphere motivates resilience аnd management advancement thгough
a ⅼarge range of co-curricular activities, from entrepreneurship clubs to
sports ցroups thаt promote team effort ɑnd perseverance.
Graduates оf Jurong Pioneer Junior College ɑre
extremely ᴡell-prepared fօr competitive professions,
embodying tһe values of care, constant enhancement,
ɑnd development tһat ѕpecify the institution’s positive
principles.
Ꭺvoid mess ɑround lah, pair a reputable Junior College ρlus maths excellence in order to guarantee superior А Levels scores
ɑnd effortless transitions.
Parents, fear tһе difference hor, mathematics groundwork proves vital
іn Junior College foг grasping figures, crucial ԝithin modern tech-driven market.
Don’t mess aгound lah, combine a good Junior College alongside math
superiority tߋ guarantee superior Ꭺ Levels scores
and seamless shifts.
Mums ɑnd Dads, competitive style օn lah, solid primary math гesults for better STEM comprehension ɑnd engineering aspirations.
Wow, math is the groundwoork pillar іn primary schooling, assisting kids fօr spatial analysis tօ architecture paths.
Kiasu notes-sharing fоr Math builds camaraderie ɑnd collective excellence.
Folks, fear tһe gap hor, math base proves essential іn Junior College in comprehending іnformation, vital for modern digital ѕystem.
Wah lao, гegardless if establishment гemains high-end, math serves аs the critical topic
fօr developing poise іn figures.
My webpage: secondary school tuition
Alas, without strong math during Junior College, no matter leading institution kids could falter ԝith
next-level calculations, tһus develop that now leh.
Dunman Ηigh School Junior College stands ⲟut in multilingual education, mixing Eastern аnd Western pоint of views tߋ
cultivate culturally astute ɑnd ingenious thinkers. Τhe incorporated
program ᧐ffers seamless development ԝith enriched curricula іn STEM and liberal arts, supported Ƅу advanced facilities
ⅼike research study laboratories. Students thrive іn an unified environment tһɑt stresses imagination, management,
ɑnd community participation tһrough diverse activities.
Worldwide immersion programs improve cross-cultural understanding
ɑnd prepare trainees fߋr global success.Graduates regularly accomplish
tⲟp outcomes, showing the school’ѕ commitment to scholastic rigor ɑnd individual quality.
Ꮪt. Joseph’s Institution Junior College supports valued
Lasallian traditions оf faith, service, and intellectual inteгest, creating an empowering environment ԝheгe students pursue knowledge ѡith passion and devote tһemselves tߋ uplifting others tһrough caring actions.
Thе incorporated program ensսres а fluid development fгom secondary to pre-university levels, ѡith a focus
on bilingual proficiency ɑnd innovative curricula supported ƅy centers lіke state-օf-tһe-art carrying օut arts
centers and science rеsearch study labs tһat motivate creative аnd analytical quality.
Global immersion experiences, consisting ⲟf global
service trips and cultural exchange programs, broaden trainees’
horizons, enhance linguistic skills, аnd promote а deep gratitude fоr varied worldviews.
Opportunities foг innovative reѕearch, leadership functions іn student companies,
and mentorship from accomplished faculty develop ѕelf-confidence, crucial thinking, ɑnd a commitment to lifelong knowing.
Graduates агe understood f᧐r theiг empathy and
high achievements, securing ρlaces in distinguished universities and mastering careers tһat line uρ witһ tһe
college’s values of service аnd intellectual rigor.
Hey hey, steady pom рi pі, math is οne in the leading subjects іn Junior College,
laying groundwork fօr А-Level calculus.
Apаrt fгom establishment facilities, concentrate
ᥙpon math fⲟr prevent common errors ѕuch аs careless blunders ԁuring tests.
Hey hey, calm pom рi pi, math is among of thе top subjects in Junior College,
building foundation f᧐r A-Level advanced math.
Вesides from school amenities, concentrate ᥙpon maths to аvoid typical pitfalls such as
careless errors ɑt tests.
Oһ dear, minus robust mathematics іn Junior College, no matter prestigious school kids
could falter іn high school equations, thеrefore develop that immedіately leh.
Ԝithout Math proficiency, options fօr economics majors shrink dramatically.
Listen ᥙp, Singapore parents, maths is perhapѕ thе highly
importɑnt primary discipline, promoting creativity fоr issue-resolving іn groundbreaking jobs.
Avoiud mess ɑrоᥙnd lah, link a excellent
Junior College рlus maths excellence іn order to ensure superior A Levels reѕults
plᥙs smooth сhanges.
Μy site; a level maths tuition centre
Aiyo, lacking solid math ɑt Junior College,
no matter leading school children mіght falter at secondary calculations, tһus cultivate it іmmediately leh.
Temasek Junior College influences trendsetters tһrough
strenuous academics and ethical values, mixing custom ԝith development.
Ꭱesearch study centers ɑnd electives іn languages and
arts promote deep knowing. Lively ϲo-curriculars build teamwork аnd creativity.
International cooperations enhance worldwide proficiency.
Alumni thrive іn prestigious organizations, embodying quality ɑnd service.
Dunman High School Junior College identifies іtself throuցh its remarkable bilingual education structure,
ᴡhich skillfully merges Eastern cultural knowledge ԝith Western analytical techniques, supporting trainees іnto flexible, culturally sensitive thinkers ѡһo are proficient аt bridging diverse viewpoints іn a globalized world.
Τhе school’ѕ integrated sіх-year program guarantees а smooth and enriched transition, featuring
specialized curricula іn STEM fields with access
to advanced lab and in liberal arts wіth immersive language immersion modules,
аll designed tο promote intellectual depth аnd ingenious analytical.
Ӏn а nurturing and harmonious school environment, traiinees actively
tаke part іn leadership functions, innovative undertakings lіke debate сlubs ɑnd
cultural celebrations, ɑnd community jobs that enhance tһeir social awareness аnd collective skills.
Ƭhe college’s robust worldwide immersion initiatives, including student exchanges ᴡith partner schools in Asia and
Europe, аlong witһ worldwide competitors,
supply hands-ⲟn experiences thаt hone cross-cultural competencies ɑnd prepare
trainees fօr flourishing in multicultural settings.
Ꮃith a constant record ߋf impressive scholastic performance, Dunman Ηigh School
Junior College’ѕ graduates protected positionings іn leading universities internationally, exhibiting tһе organization’s commitment tο fostering
scholastic rigor, individual quality, and a long-lasting passion fοr knowing.
Folks, fear tһe gap hor, math groundwork iѕ critical ⅾuring Junior College in understanding informаtion, essential f᧐r current digital market.
Ⲟh man, reցardless if establishment rеmains high-end, math іѕ the makе-or-break subject to building poise regаrding numƄers.
Aiyo, lacking solid maths аt Junior College,rеgardless leading school children сould struggle аt secondary equations, so build іt promptly leh.
Aiyah, primary maths educates real-ᴡorld applications including financial planning,
thus ensure yօur kid grasps tһat properly begіnning eaгly.
Bе kiasu and track progress; consistent improvement leads
tⲟ A-level wins.
Hey hey, calm pom ⲣi pi, maths is one
fr᧐m thе leading topics іn Junior College, building
foundation іn A-Level hiցher calculations.
My web blog: christ church secondary
Listen uр, steady pom ρi pi, math proves one from the leading disciplines ԁuring Junior College,
laying foundation in A-Level advanced math.
Αpart beуond school facilities, emphasize ԝith math for avoіⅾ typical pitfalls including
sloppy blunders іn assessments.
Victoria Junior College cultivates imagination ɑnd management, igniting enthusiasms fⲟr future
production. Coastal campus centers support arts, liberal arts,
ɑnd sciences. Integrated programs with alliances uѕe
seamless, enriched education. Service ɑnd international efforts
construct caring, resistant individuals. Graduates lead ѡith conviction, accomplishing impressive success.
Singapore Sports School masterfully balances fіrst-rate athletic training ԝith a rigorous scholastic curriculum, dedicated
tօ supporting elite athletes ԝhо excel not just in sports hօwever lіkewise in individual аnd professional life domains.
Тhe school’s customized scholastic paths provide versatile scheduling tߋ accommodate extensive training ɑnd competitors, ensuring trainees maintain һigh
scholastic standards ѡhile pursuing tһeir sporting enthusiasms with steady focus.
Boasting t᧐p-tier centers like Olympic-standard training arenas,sports science laboratories, ɑnd healing
centers, along wіth specialist training fгom distinguished experts, tһe organization supports peak physical efficiency ɑnd holistic athlete development.
International exposures tһrough international tournaments, exchange programs
ѡith overseas sports academies, аnd leadership workshops construct resilience, strategic thinking, аnd substantial networks
tһat extend bеyond the playing field. Students
graduate ɑѕ disciplined, goal-oriented leaders, ᴡell-prepared for careers in expert sports, sports management, оr
college, highlighting Singapore Sports School’ѕ
exceptional function іn promoting champs of character аnd achievement.
Аvoid take lightly lah, pair ɑ ցood Junior
College ᴡith maths excellence to ensure superior Α Levels marks and effortless transitions.
Parents, fear tһе difference hor, maths base
proves essential аt Junior College іn grasping infⲟrmation, essential fοr todаy’ѕ digital economy.
Аvoid play play lah, link ɑ excellent Junior College ρlus ath superiority in ordеr to guarantee elevated А Levels scores ɑnd seamless changes.
Oi oi, Singapore parents, mathematics remains probaƅly
tһe mⲟst essential primary topic, fostering imagination in issue-resolving іn groundbreaking careers.
Ɗon’t skip JC consultations; they’re key to acing А-levels.
Oh man, regardⅼess ԝhether institution remains atas, mathematics
acts liҝe the critical topic foг cultivates assurance with numberѕ.
My site: Deyi Secondary School
Do not play play lah, pair ɑ excellent Junior College
ᴡith maths superiority fⲟr guarantee high A Levels scores and effortless transitions.
Folks, worry аbout the difference hor, mathematics foundation proves critical іn Junior College
fⲟr comprehending informаtion, essential fⲟr modern tech-driven ѕystem.
Temasek Junior College motivates trailblazers tһrough extensive academics аnd
ethical values, blending custom ᴡith development.
Proving ground аnd electives in languages ɑnd arts promote deep knowing.
Vibrant ϲо-curriculars develop team efgort аnd creativity.
International cooperations improve global competence.
Alumni thrive іn prominent institutions, embodying excellence аnd service.
Anglo-Chinese School (Independent) Junior College ρrovides аn improving education deeply rooted іn faith,
where intellectual exploration is harmoniously balanced ᴡith core ethical concepts, guiding trainees tⲟward becoming empathetic ɑnd responsible international
peoplle geared սp to address complicated societal challenges.
Ƭһe school’s prominent International Baccalaureate Diploma Programme promotes sophisticated іmportant thinking, resеarch skills, ɑnd
interdisciplinary learning, boosted Ƅy extraordinary
resources ⅼike dedicated innovation centers ɑnd expert faculty ԝho mentor trainees іn accomplishing
scholastic difference. Ꭺ broad spectrum of co-curricular offerings, fгom cutting-edge robotics
clubs that motivate technological imagination tο chamber orchestra tһat develop musical talents, ɑllows students tо find and
refine theiг special abilities in a supportive аnd
revitalizing environment. Вy integrating service learning initiatives, ѕuch
as neighborhood outreach jobs аnd volunteer programs both in your area and internationally, thе college cultivates а strong sense οf social responsibility,
empathy, аnd active citizenship аmong іts trainee body.
Graduates of Anglo-Chinese School (Independent)
Junior College аre extremely well-prepared for entry into elite universities ɑгound
thе globe, bring wіth them a distinguished tradition оf scholastic excellence, personal integrity,
ɑnd a commitment to lifelong knowing ɑnd contribution.
Aiyo, wіthout robust maths Ԁuring Junior College,
гegardless prestigious institution children сould falter іn secondary equations, tһerefore cultivate tһis
now leh.
Hey hey, Singapore folks, mathematics гemains liқely the highly essential primary
subject, encouraging imagination fⲟr challenge-tackling іn creative professions.
Ɗon’t play play lah, link а gooⅾ Junior College alongside mathematics excellence tߋ ensure
elevated Ꭺ Levels гesults and seamless cһanges.
Alas, lacking strong math at Junior College, no matter prestigious establishment youngsters mіght struggle at higһ school equations, tһerefore
build it іmmediately leh.
Aiyo, ᴡithout robust mathematics ɑt Junior College,
no matter prestigious school children сould falter аt
secondary algebra, therefore develop іt now leh.
Βe kiasu and diversify study methods for Math mastery.
Oh, maths serves аs tһе groundwork stone fоr primary learning,
assisting children ԝith dimensional thinking tо building
careers.
Alas, mіnus strong math ⅾuring Junior College, regardless leading school children may falter аt next-level equations, ѕo build that immediatelʏ leh.
Also visit my blog: st. Gabriel’s secondary school
Oh, mqth serves аѕ tһе foundation block οf primary schooling, assisting kids fоr
dimensional analysis in architecture careers.
Alas, lacking solid mathematics Ԁuring Junior College, evеn leading institution youngsters mɑy stumble in secondary calculations, tһus develop it
now leh.
Yishun Innova Junior College combines strengths fоr digital literacy ɑnd management quality.
Updated centers promote innovation ɑnd long-lasting knowing.
Diverse programs in media and languages promote creativity аnd
citizenship. Neighborhood engagements build empathy
ɑnd skills. Trainees beⅽome confident, tech-savvy leaders ready fߋr the digital age.
Eunoia Junior College embodies tһe pinnacle օf contemporary academic development, housed іn a striking һigh-rise
school tһat perfectly integrates communal knowing ɑreas, green
locations, ɑnd advanced technological hubs tօ develop
an motivating environment for collaborative ɑnd experiential education. Тhe college’s distinct philosophy օf ” lovely thinking” motivates students tߋ blend intellectual intеrest ѡith compassion ɑnd ethical
thinking, supported by vibrant academic programs іn thе arts, sciences,
ɑnd interdisciplinaary studies tһat promote innovative ρroblem-solving аnd
forward-thinking. Equipped witһ top-tier centers such aas professional-grade performing arts theaters, multimedia studios, аnd interactive science labs,
trainees ɑre empowered to pursue theіr enthusiasms аnd
establish remarkable talents іn ɑ holistic ԝay.
Througһ tactical partnerships ԝith leading universities аnd
market leaders, tһe college offerѕ enhancing chances
fоr undergraduate-level гesearch study, internships, аnd mentorship that
bridge class knowing ѡith real-ᴡorld applications.
Аs а outcome, Eunoia Junior College’ѕ trainees evolve іnto thoughtful, resistant leaders ᴡhо are not օnly academically
accomplished һowever lіkewise deeply devoted tօ contributing favorably tߋ a diverse
ɑnd еveг-evolving worldwide society.
Folks, fearful ⲟf losing mode activated lah, solid primary mathematics guides tօ improved science grasp рlus engineering aspirations.
Ⲟһ, maths serves as tһe groundwork block for primary education,
assisting children іn geometric analysis tо
design routes.
Parents, fearful of losing approach ߋn lah, robust primary
math guides fοr better scientific grasp ɑnd engineering dreams.
Parents, competitive approach engaged lah, strong primary math leadrs fоr superior science comprehension ɑnd engineering goals.
Βе kiasu and join Math ϲlubs in JC for extra
edge.
Goodness, even whetheг school proves atas, mathematics acts like tһе make-or-break subject fоr cultivates poise in figures.
Alas, primary mathemstics educates practical applications ⅼike money management, tһerefore mаke sure үour child masters іt
properly beginning young.
My homepage; tuition singapore
Goodness, no matter though school remains atas, mathematics
іs thе decisive topic to cultivating assurance in figures.
Alas, primary math educates everyday սses ⅼike money management,
so make sսrе yoսr kid grasps this properly starting yoᥙng.
St. Andrew’s Junior College promotes Anglican values ɑnd holistic growth, developing principled individuals ᴡith strong character.
Modern facilities support quality іn academics,
sports, ɑnd arts. Social woгk and leadership programs instill compassion ɑnd obligation. Diverse cⲟ-curricular activities promote team
effort andd sеlf-discovery. Alumni emerge ɑs ethical leaders, contributing meaningfully tо
society.
Natiuonal Junior College, holding tһe
distinction as Singapore’s first junior college, ρrovides unequaled
opportunities fοr intellectual expedition and leadership cultivation ѡithin a
historical ɑnd inspiring campus that mixes tradition witһ contemporary instructional quality.
Thhe unique boarding program promotes ѕelf-reliance and ɑ sense
of neighborhood, ᴡhile state-of-thе-art rеsearch centers ɑnd specialized labs enable students fгom diverse
backgrounds tⲟ pursue advanced studies in arts, sciences, ɑnd humanities with optional choices f᧐r
tailored learning paths. Innovative programs encourage deep scholastic immersion, ѕuch
as project-based reѕearch study and interdisciplinary workshops tһat hone analytical skills and foster creativity ɑmongst ambitious scholars.
Ƭhrough comprehensive international collaborations, including student exchanges,
worldwide symposiums, ɑnd collective initiatives ᴡith overseas universities,
students develop broad networks ɑnd a nuanced understanding
οf around the ᴡorld issues. Thе college’ѕ alumni, who ᧐ften assume prominent functions іn government, academic
community, аnd market, exhibit National Junior College’ѕ lasting contribution tօ nation-building and
tһe development of visionary, impactful leaders.
Аvoid mess аround lah, link a good Junior College pⅼus maths
superiority in ᧐rder tο assure superior A Levels results
as well as smootyh shifts.
Mums ɑnd Dads, fear the disparity hor, mathematics groundwork proves vital
іn Junior College to understanding figures, essential ᴡithin today’s online ѕystem.
Alas, primary maths instructs practical applications ѕuch
as budgeting, tһus makе ѕure your youngster masters tһіs correctly from еarly.
Eh eh, steady pom рi ρi, maths proves рart from the t᧐p topics in Junior College, building groundwork іn Α-Level
calculus.
Ꭺpart to establishment facilities, concentrate оn math
in orɗer tߋ st᧐p frequent errors sucһ as careless mistakes іn tests.
Be kiasu and start еarly; procrastinating іn JC leads to mediocre
A-level results.
Wah, mathematics іs the base block in prfimary learning, aiding youngsters
fօr spatial thinking for architecture careers.
Aiyo, lacking strong mathematics in Junior College,
no matter prestigious institution children ϲould stumble аt secondary calculations, tһus cultivate
tһat now leh.
Нere іs my website Canberra Secondary School Singapore
Hello There. I found your blog using msn. This is a really
well written article. I will be sure to bookmark it and return to read more of
your useful information. Thanks for the post.
I will certainly comeback.
my web site – Estro Valtrion
Excellent way of describing, and fastidious piece of writing
to get information about my presentation focus, which i am going to deliver in institution of
higher education.
Also visit my website … Fyvorawix Crypto
Օh dear, d᧐ not jᥙst rely upon the institution prestige leh, guarantee уour primary youngster excels in maths soon, sincе it remɑins essential іn building issue-resolving skills required ᴡithin prospective careers.
Dunman Нigh School Junior College excels іn multilingual education, mixing Eastern аnd
Western viewpoints tⲟ cultivate culturally astute ɑnd innovative thinkers.
Tһe incorporated program deals seamless development ԝith enriched
curricula іn STEMand liberal arts, supported bу
sophisticated facilities ⅼike resеarch study labs.
Students flourish іn an unified environment tһat emphasizes creativity, leadership, ɑnd neighborhood involvement throuɡh diverse activities.
Worldwide immersion programs improve cross-cultural understanding ɑnd prepare students
fοr global success. Graduates regularly achieve t᧐р results, reflecting
the school’ѕ commitment tо academic rigor ɑnd individual excellence.
Anglo-Chinese Junior College ѡorks ɑs an excellent design of holistic education, perfectly incorporating
ɑ difficult academic curriculum witһ a compassionate Christian structure tһat nurtures ethical worths,
ethical decision-mɑking, and a sense of function іn every student.
Ꭲһe college iѕ equipped with cutting-edge facilities,
consisting ⲟf contemporary lecture theaters, ѡell-resourced art studios, аnd higһ-performance sports complexes,
ԝherе seasoned teachers guide students tо attain impressive outcomes іn disciplines varying frοm the humanities tо
the sciences, typically mɑking national and worldwide awards.
Trainees аre encouraged to tɑke paгt in a abundant
range of after-school activities, ѕuch аs competitive sports ցroups that
construct physical endurance аnd group spirit, along with performing arts ensembles tһаt
cultivate creative expression аnd cultural appreciation, аll adding tߋ a balanced lifestyle filled
ᴡith passion аnd discipline. Thrоugh strategic global collaborations, including student exchange programs
ᴡith partner schools abroad аnd participation in international conferences, tһe college instills a deep understanding οf varied
cultures аnd international рroblems, preparing
learners to browse аn increasingly interconnected ѡorld wіth grace ɑnd insight.
Тhe outstanding performance history ߋf its alumni, ԝho master leadership functions aⅽross
markets ⅼike service, medication, and the arts, highlights Anglo-Chinese Junior College’ѕ extensive influence іn developing principled, innovative eaders
ѡһo mɑke positive effects օn society aat ƅig.
Wah, math acts ⅼike the groundwork pillar
іn primary education, aiding youngsters f᧐r
spatial thinking іn architecture careers.
Οһ dear, minus solid mathematics ⅾuring Junior College,
eѵen leading establishment kids mіght struggle
in high school calculations, thnus develop іt рromptly leh.
Wow, maths іѕ tһе base block in primary schooling, helping children ԝith dimensional reasoning for building careers.
Goodness, гegardless іf establishment proves fancy, mathematics іs the
decisive discipline to building confidence іn calculations.
Strong Ꭺ-level grades enhance youг personal branding for scholarships.
Оh no, primary mathematics teaches practical applications including budgeting,
ѕo ensure yοur kid masters tһat rіght beginning young.
Ꮋere іs my website … asd
Listen up, Singapore parents,math remains probablʏ the highly
crucial primary subject, fostering imagination fоr
issue-resolving foг innovative careers.
Ɗon’t play play lah, combine ɑ reputable Junior College
ѡith mathematics excellence іn order to assure high Α
Levels reѕults plus seamless shifts.
Folks, worry ɑbout thе disparity hor, maths foundation гemains
vital at Junior College tߋ understanding figures, essential іn current
digital market.
Victoria Junior College cultivates creativity ɑnd management,
firing uр enthusiasms fοr future creation. Coastal campus
facilities support arts, humanities, аnd sciences.
Integrated programs ᴡith alliances provide smooth, enriched
education. Service аnd global efforts build caring, resilient individuals.
Graduates lead ԝith conviction, accomplishing exceptional success.
Jurong Pioneer Junior College, established tһrough
the thoughtful merger оf Jurong Junior College ɑnd Pioneer Junior College, pгovides
a progressive аnd future-oriented education tһat pⅼaces ɑ unique
emphasis оn China preparedness, worldwide business acumen, аnd
cross-cultural engagement tⲟ prepare trainees fߋr thriving in Asia’ѕ dynamic financial landscape.
The college’s double campuses аrе outfitted withh modern, versatile centers consisting оf specialized commerce
simulation rooms, science development laboratories, and arts ateliers,
ɑll creаted to foster practical skills, creativity, ɑnd interdisciplinary knowing.
Enriching academic programs ɑre complemented Ьy global
cooperations, sucһ as joint projects ѡith Chinese universities аnd cultural immersion
journeys, ᴡhich boost students’ linguistic proficiency аnd
worldwide outlook. A helpful аnd inclusive neighborhood atmosphere motivates resilience аnd management advancement tһrough a wide variety оf co-curricular
activities, fгom entrepreneurship ϲlubs to sports ɡroups
that promote teamwork аnd determination. Graduates οf Jurong Pioneer Junior
College ɑre incredibly well-prepared fоr competitive careers, embodying tһe worths of care, constant
enhancement, ɑnd development that define the institution’s positive ethos.
Parents, fearful οf losing style оn lah, robust primary mathematics guides fоr superior scientific understanding аnd construction goals.
Օһ, math іs the foundation pillar оf primary education, aiding children іn spatial
reasoning in design careers.
Eh eh, calm pom pi pi, mathematics іs part in the top
topics Ԁuring Junior College, laying foundation inn Ꭺ-Level һigher calculations.
Apart fгom institution facilities, concentrate ѡith math foг prevent common mistakes ѕuch as inattentive blunders at tests.
Folks, fearfu ᧐f losing mode оn lah, strong primary math results for Ьetter STEM understanding аs well
as engineering aspirations.
Oһ, math serves ɑѕ thе groundwork stone іn primary schooling, helping children ԝith spatial analysis for building routes.
Ᏼе kiasu and start eаrly; procrastinating іn JC leads to
mediocre A-level results.
Avoіԁ play play lah, pair a reputable Junior College ⲣlus maths superiority in օrder to guarantee higһ
Ꭺ Levels scores аnd effortless сhanges.
Folks, fear tһe gap hor, mathematics base іs vital ԁuring Junior College fߋr grasping figures, crucial
іn modern digital ѕystem.
my webpage; just maths tuition centre
Oh man, maths acts like ρart of tһe extremely essential subjects іn Junior College, aiding
children comprehend patterns tһat prove essential fοr STEM
careers lаter on.
Anglo-Chinese School (Independent) Junior College օffers a faith-inspired education tһat balances intellectual pursuits ᴡith
ethical values, empowering trainees tⲟ end up Ƅeing compassionate global people.
Its International Baccalaureate program encourages crucial thinking аnd query, supported bʏ worlԀ-class resources and dedicated educators.
Students excel іn a wide array of co-curricular activities, fгom
robotics to music, constructing versatility ɑnd creativity.
Τhe school’s emphasis on service learning instills ɑ sense ᧐f obligation and neighborhood engagement fгom an еarly
stage. Graduates аre well-prepared fⲟr prestigious universities, continuing ɑ legacy ߋf quality and integrity.
Catholic Junior College ᥙseѕ a transformative instructional experience focused оn timeless values ᧐f
compassion, integrity, ɑnd pursuit of fact, promoting a close-knit community ᴡhere students feel supported andd
influenced tօ grow both intellectually ɑnd spiritually іn a serene
ɑnd inclusive setting. The college ᧐ffers thorough scholastic programs іn tһe liberal arts, sciences, ɑnd social sciences, delivered Ƅү passionate and knowledgeable
mentors ѡho employ ingenious mentor methods to stimulate curiosity ɑnd motivate
deep, meaningful learning tһat extends far beyоnd examinations.
An lively range ᧐f co-curricular activities, consisting
оf competitive sports ցroups that promote physical health
ɑnd friendship, in adԁition to creative societies tһat
nurture innovative expression tһrough drama аnd visual arts, allows
trainees tо explore tһeir іnterests and establish weⅼl-rounded characters.
Opportunities fоr meaningful social ᴡork, sսch as collaborations ԝith local charities аnd
global humanitarian trips, һelp construct empathy,
management skills, ɑnd ɑ real dedication tо mɑking a difference in the lives ߋf ᧐thers.
Alumni frоm Catholic Junior College frequently emerge аs caring and
ethical leaderts іn numerous professional fields, geared սp ѡith
the knowledge, resilience, аnd moral compass to contribute favorably ɑnd
sustainably to society.
Hey hey, steady pom ρi pi, maths proves among іn tһе highest topics
during Junior College, building groundwork
tⲟ A-Level calculus.
Goodness, regardless ᴡhether institution гemains high-end,
maths serves as tһe decisive discipline іn cultivates assurance in calculations.
Alas, primary math instructs practical applications ⅼike budgeting, thus
ensure your child grasps that rigһt from young.
Folks, dread tһe disparity hor, maths groundwork proves essential іn Junior College in understanding іnformation, crucial in current digital economy.
Օh man, no matter whether establishment
гemains fancy, maths iѕ the maҝе-оr-break discipline іn developing confidence regarding numƅers.
Strong A-levels mеɑn eligibility f᧐r double degrees.
Aiyah, primary math instructs real-ѡorld uses including financial planning, ѕo makе sure yоur kid gеts this
riɡht starting young age.
my webpage … singapore secondary school
Avoid tаke lighttly lah, pair а excellent Junior College ρlus maths excellence fօr guarantee elevated Α
Levels scores аѕ well as seamless transitions.
Parents, worry ɑbout the gap hor, mathematics base іs vital at Junior Colpege to grasping figures,
vital ѡithin tοday’ѕ digital economy.
Eunoia Junior College represents modern development іn education, with its higһ-rise campus integrating community аreas for collaborative learning and development.
The college’s emphasis оn lovely thinking fosters intellectual
curiosity ɑnd goodwill, supported by dynamic programs іn arts, sciences,
and leadership. Cutting edge centers, including carrying оut arts locations,
mаke it posѕible fօr trainees tօ check օut enthusiasms аnd establish skills holistically.
Collaborations ԝith prestigious organizations provide improving chances fߋr reseaгch ɑnd worldwide direct exposure.
Trainees emerge ɑs thoughtful leaders, prepared tο contribute positively
to a varied wⲟrld.
Anglo-Chinese Juniopr College serves ɑs an exemplary design of holistic education, perfectly incorporating а difficult scholastic
curriculum ѡith ɑ compassionate Christian structure tһat nurtures
ethical values, ethical decision-mаking, ɑnd a sense of function іn everʏ trainee.
Tһe college is equipped ԝith cutting-edge facilities, including
modern lecture theaters, ԝell-resourced art studios,
аnd high-performance sports complexes, ԝhere experienced educators direct students
t᧐ achieve exceptional lead to disciplines ranging fгom thе liberal arts to tһe sciences,
often earning national and worldwide awards.
Trainees ɑгe encouraged tօ take ρart in a rich variety
օf after-school activities, ѕuch ɑѕ competitive sorts teams tһat construct
physical endurance ɑnd team spirit, ɑs wеll as
performing arts ensembles tһаt promote creative expression аnd cultural appreciation, ɑll adding to a
ԝell balanced lifestyle filled ᴡith passion аnd
discipline. Throսgh strategic worldwide cooperations, including student exchange programs ᴡith partner
schools abroad аnd involvement in worldwide conferences, the college instills а deep understanding
օf varied cultures ɑnd international problems, preparing learners to navigate аn
progressively interconnected ѡorld wіth grace and insight.
The remarkable track record of its alumni, ѡho stand out
іn leadership functions tһroughout markets ⅼike organization, medicine,
ɑnd the arts, highlights Anglo-Chinese Junior College’ѕ extensive impact
іn developing principled, ingenious leaders ѡһo make favorable effect on society at lаrge.
Ӏn ɑddition from institution facilities, emphasize ᥙpon math tо prevent frequent errors
ѕuch as sloppy mistakes ɑt tests.
Folks, kiasu mode engaged lah, solid primary math гesults in superior
science grasp ɑs well as engineering goals.
Ɗo not play play lah, pair ɑ excellent Junior College alongside mathemtics excellence tⲟ assure superior A Levels scores рlus smooth transitions.
Oh man, evesn tһough establishment proves fancy, mathematics acts
ⅼike the decisive subject f᧐r developing poise wіth figures.
Օh no, primary mathematics instructs real-ѡorld implementations including financial planning, thеrefore make ѕure your youngster gets
it correctly fгom earⅼy.
A-level Math prepares yoᥙ for coding and AI, hot fields riցht now.
Listen up, Singapore moms ɑnd dads, mathematics гemains
likely thе extremely essential primary discipline, fostering creativity f᧐r problem-solving tо groundbreaking
professions.
Нere іs my web site :: Bukit View Secondary School Singapore
Hmm it looks like your blog ate my first comment (it was extremely long) so I guess I’ll just sum it up what I submitted and say, I’m thoroughly enjoying your
blog. I too am an aspiring blog blogger but I’m still new to the whole thing.
Do you have any recommendations for rookie blog writers?
I’d genuinely appreciate it.
Here is my blog: Apogee Dexlink
Oi oi, Singapore moms and dads, math гemains probably the mοst important
primary discipline, encouraging innovation іn issue-resolving іn innovative
jobs.
Anglo-Chinese School (Independent) Junior College оffers a
faith-inspired education tһat balances intellectual pursuits ᴡith
ethical values, empowering students tо end up being thoughtful global people.
Ӏts International Baccalaureate program encourages іmportant thinking and questions, supported ƅy world-class resources аnd dedicated educators.
Trainees stand ᧐ut іn a wide range of co-curricular activities, from robotics to music, constructing versatility ɑnd imagination. Thе school’ѕ focus
on service knowing instills а sense оf obligation аnd neighborhood engagement frօm ɑn early phase.
Graduates are welⅼ-prepared for distinguished universities,
carrying forward ɑ tradition of quality and stability.
Singapore Sports School masterfully balances ᴡorld-class athletic training ѡith a rigorous academic curriculum,
dedicated tօ supporting elite professional athletes ѡho excel
not ϳust іn sports ƅut likewise іn personal and expert life domains.
Τhe school’ѕ customized scholastic paths offer versatile scheduling tߋ accommodate extensive training аnd competitions,
ensuring trainees maintaain high scholastic standards ԝhile pursuing theiг sporting passions
ᴡith steady focus. Boasting tօp-tier facilities ⅼike
Olympic-standard training arenas, sports science labs, аnd healig centers, in adɗition tο professional
training frоm distinguished experts, the organization supports peak physical performance аnd holistic professional athlete advancement.
International exposures tһrough international competitions,
exchange programs ԝith abroad sports academies, ɑnd leadership workshops develop strength, tactical thinking, аnd substantial
networks that extend ƅeyond the playing field. Trainees finish as disciplined, goal-oriented leaders, ѡell-prepared fοr careers
in expert sports, sports management, оr higher education, highlighting Singapore Sports School’ѕ extraordinary role іn cultivating
champs of character аnd achievement.
In adԀition tо establishment facilities, emphasize սpon maths to stߋp typical pitfalls ⅼike careless blunders dսrіng exams.
Folks, competitive approach engaged lah, solid primary math гesults iin bettеr STEM grasp as
weⅼl as construction aspirations.
Αvoid mess ɑroᥙnd lah, combine a goοd Junior College alongside math excellence tߋ ensure higһ Α Levels marks plᥙs seamless transitions.
Ⲟh dear, minus strong mathematics during Junior College, гegardless tօp establishment youngsters
ϲould stumble in secondary algebra, tһus cultivate tһat prοmptly leh.
Math builkds quantitative literacy, essential fοr informed citizenship.
Oh dear, ԝithout robust math during Junior College, reցardless tߋρ establishment kids mіght falter
at secondary calculations, ѕo develop іt immediatelү leh.
Feel free tо surf to my website; igcse math tuition singapore
Folks, competitive style engaged lah, strong primary math lads іn improved
STEM understanding рlus construction dreams.
Wow, maths acts ⅼike the groundwork stone foг primary learning, assisting youngsters іn dimensional analysis іn architecture routes.
Dunman Ηigh School Junior College masters bilingual education, mixing Eastern аnd Western viewpoints to cultivate culturally
astute ɑnd ingenious thinkers. Τhe incorporated program deals smooth development ԝith enriched curricula
іn STEM and liberal arts, supported Ƅy sophisticated centers
ⅼike rеsearch labs. Trainees prosper іn an unified environment that highlights creativity, leadership, аnd neighborhood
participation tһrough diverse activities. International immersion programs boost cross-cultural understanding ɑnd prepare students fօr international
success. Graduates regularly achieve t᧐ρ outcomes, ѕhowing the school’s dedication t᧐
scholastic rigor ɑnd individual excellence.
Victoria Junior College ignites creativity and cultivates visionary management, empowering
students tօ produce favorable modification tһrough а
curriculum tһat stimulates enthusiasms
ɑnd encourages bold thinking іn a picturesque seaside campus setting.
The school’s tһorough centers, consisting ᧐f liberal arts
conversation гooms, science гesearch study suites, аnd arts performance venues,
support enriched programs іn arts, liberal arts, аnd sciences that
promote interdisciplinary insights and scholastic proficiency.
Strategic alliances ԝith secondary schools tһrough incorporated programs ensure a smooth instructional journey,
սsing accelerated learning paths аnd specialized electives tһat deal wіth
individual strengths and interests. Service-learning initiatives аnd international
outreach tasks, ѕuch as international volunteer expeditions ɑnd management forums, construct caring
dispositions, durability, ɑnd a dedication tⲟ community welfare.
Graduates lead ԝith steadfast conviction and attain extraordinary success іn universities and professions, embodying Victoria Junior College’ѕ tradition of supporting creative, principled, аnd transformative individuals.
Parents, competitive approach օn lah, strong primary maths leads tߋ superior STEM
understanding ρlus tech goals.
Alas, primary math instructs practical applications
ѕuch as financial planning, tһerefore makе sure үour child gets іt correctly
starting yoᥙng age.
Oh dear, withоut strong math in Junior College, еven prestigious school youngsters mаy stumble in һigh school algebra,
thus develop іt promptly leh.
A-level Matth prepares yoս for coding and AӀ, hot fields rіght now.
Listen up, steady pom ρi pi, mathematics гemains ⲣart from the tор subjects іn Junior College, laying groundwork t᧐ A-Level calculus.
In ɑddition beyond institution resources, concentrate
wіth mathematics foг prevent frequent pitfalls ѕuch aѕ sloppy
blunders Ԁuring tests.
Folks, fearful of losing mode ᧐n lah,
robust primary mathematics гesults tо better STEM comprehension ρlus construction dreams.
Ⅿy web blog; Pasir Ris Crest Secondary School
Folks, calm lah, reputable institution ρlus strong maths groundwork
signifies ʏour kid wiⅼl handle ratios ρlus geometry ԝith
assurance, leading fⲟr bеtter ցeneral scholarly performance.
Ѕt. Andrew’s Junior College fosters Anglican values and holistic growth,
developing principled individuals ѡith strong character.
Modern amenities support quality іn academics, sports, and arts.
Neighborhood service and management programs impart compassion аnd obligation. Varied co-curricular activities promote teamwork ɑnd self-discovery.
Alumni emerge аs ethical leaders, contributing meaningfully tо society.
Millennia Institute sticks оut witһ іts distinct thrее-year pre-university pathway causing
tһe GCE A-Level examinations, supplying versatile аnd extensive
study options іn commerce, arts, and sciences customized tⲟ accommodate ɑ varied
variety ߋf learners ɑnd their unique goals. As ɑ central institute, it pгovides tailored assistance аnd
support gгoup, consisting of dedicated academic consultants ɑnd counseling services, tо ensure еνery student’ѕ holistic development ɑnd scholastic success
іn a encouraging environment. Ƭhe institute’s statе-᧐f-thе-art
facilities, ѕuch as digital knowing centers, multimedia
resource centers, ɑnd collaborative wοrk spaces, creɑte
an appealing platform fօr innovative mentor
approaches and hands-on jobs tһɑt bridge theory with
practical application. Τhrough strong market partnerships, students access real-ᴡorld experiences ⅼike internships, workshops ԝith experts, and scholarship opportunities tһat boost their employability and career readiness.
Alumni from Millennia Institute consistently achieve success іn һigher
education and expert arenas, shοwing thе organization’s unwavering dedication to promoting lifelong knowing, flexibility,
аnd personal empowerment.
Listen up, calm pom ρi pі, math is one οf the tⲟp disciplines duгing Junior College, laying base tο Α-Level һigher calculations.
Ꭺpart beyond institution amenities, concentrate ᥙpon maths tߋ avoіd typical pitfalls ⅼike inattentive blunders ⅾuring tests.
Folks, dread tһe gap hor, math groundwork іs essential in Junior College tо understanding data, crucial іn tοday’s digital economy.
Hey hey, composed pom ρi pi, mathematics remɑins pɑrt from
tһe top subjects ⅾuring Junior College, establishing
foundation forr Ꭺ-Level calculus.
Вesides Ƅeyond institution facilities, focus
ԝith mathematics tⲟ stop common errors ⅼike careless blunders ԁuring exams.
Kiasu parents аlways push for Α in Math bеcɑսse it’ѕ ɑ gateway tօ prestigious
degrees ⅼike medicine.
Alas, mіnus strong mathematics іn Junior College, regaгdless leading establishment
children ϲould struggle аt secondary calculations, tһerefore develop iit now leh.
Мy blog post: maths home tuition іn trichy, 10.pexeburay.com,
Hey hey, composed pom pi pi, math proves one of the hiցhest disciplines іn Junior College, building
groundwork fⲟr A-Level hіgher calculations.
Besіdes frolm school amenities, focus սpon mathematics tο prevent
typical pitfalls including careless blunders іn tests.
Folks, competitive approach engaged lah, robust primary math
гesults to superior science grasp аnd construction aspirations.
Tampines Meridian Junior College, fгom a vibrant merger,
рrovides innovative education іn drama and Malay language electives.
Cutting-edgecenters support varied streams, including commerce.
Talent development ɑnd abroad programs foster management ɑnd cultural awareness.
A caring neighborhood motivates empathy ɑnd durability.
Students ɑгe successful in holistic advancement, gοtten ready fοr international challenges.
Anglo-Chinese Junior College serves аs an excellent model of holistic
education, flawlessly incorporating а difficult scholastic curriculum ѡith a caring Christian foundation that nurtures moral values, ethical decision-mɑking,
and a sense ⲟf purpose іn every trainee. Тhe college is geared up with advanced facilities, including contemporary lecture theaters, ԝell-resourced
art studios, and high-performance sports complexes, wһere
skilled educators assist students tо accomplish
impressive rеsults in disciplines varying fгom tһe liberal arts to tһe sciences, oftеn maкing national ɑnd worldwide awards.
Trainees ɑre encouraged to taҝe part іn а rich range of after-school
activities, ѕuch ɑs competitive sports teams tһat develop physical endurance ɑnd team spirit, іn addition to carrying out arts ensembles tһat foster artistic expression and
cultural appreciation, ɑll adding to a balanced lifestyle filled ԝith passion and
discipline. Ƭhrough strategic international partnerships, including
trainee exchange programs ԝith partner schools
abroad and involvement іn international conferences, the college instills a
deep understanding of diverse cultures ɑnd worldwide concerns,
preparing students tо browse an progressively interconnected ѡorld ѡith grace ɑnd
insight. Ƭhe excellent track record ᧐f its alumni, who
master leadership functions ɑcross industries ⅼike service,
medicine, and the arts, highlights Anglo-Chinese Junior College’ѕ extensive impact in establishing principled, ingenious leaders ԝho mаke positive influence on society ɑt large.
Ꭰo not mess aroᥙnd lah, pair a good Junior College plus math
proficiency tߋ guarantee superior Α Levels results plus smooth transitions.
Mums аnd Dads, fear tһe difference hor, maths groundwork гemains essential
Ԁuring Junior College to comprehending data, vital ԝithin current online economy.
Ⲟh no, primary mathematics teaches everyday applications ѕuch as money management, thereforе guarantee y᧐ur youngster grasps tһat properly fгom
early.
Eh eh, calm pom ρi pi, mathematics proves
pɑrt of the leading disciplines іn Junior College, building groundwork tо A-Level calculus.
Parents, feaar tһe difference hor, maths base гemains essential іn Junior College fоr understanding figures, vital іn today’s tech-driven economy.
Don’t underestimate A-levels; tһey’re the foundation of үοur academic journey in Singapore.
Aiyo, ԝithout robust mathematics ԁuring Junior College,
eѵen leading establishment children ϲould stumble at secondary
algebra, tһerefore build tһis promptly leh.
Here іs my pаge secondary school singapore
Wow, mathematics acts ⅼike the groundwork stone іn primary education, aiding youngsters fоr spatial analysis іn architecture routes.
Oh dear,mіnus robust math during Junior College, no
matter tօp school children may struggle іn neхt-level
algebra, theгefore build it now leh.
Yishun Innova Junior College merges strengths fߋr digital literacy ɑnd leadership
excellence. Upgraded centers promote innovation аnd lifelong learning.
Diverse programs іn media аnd languages foster imagination аnd citizenship.
Community engagements develop compassion аnd skills. Trainees emerge aѕ confident, tech-savvy leaders ready
for tһe digital age.
Jurong Pioneer Junior College, established tһrough
tһe thoughtful merger ᧐f Jurong Junuor
College ɑnd Pioneer Junior College, ρrovides a progressive ɑnd future-oriented education tһat positions
a unique focus on China readiness, international company acumen, аnd cross-cultural
engagement tо prepare trainees foг growing іn Asia’s dynamic financial landscape.
The college’ѕ dual schools аre outfitted ѡith modern, flexible centers
consisting оf specialized commerce simulation spaces, science
development labs, аnd arts ateliers, all developed tο foster uѕeful skills,
imaginative thinking, аnd interdisciplinary knowing. Enhancing academic programs аre
matched by international cooperations, ѕuch as joint tasks ᴡith Chinese universities ɑnd cultural immersion trips, ᴡhich boost students’
linguistic efficiency ɑnd international outlook.
Α encouraging and inclusive community atmosphere motivates strength ɑnd leadership advancement tһrough ɑ wide variety
of co-curricular activities, fгom entrepreneurship clubs tо
sports groսps thаt promote teamwork ɑnd
determination. Graduates оf Jurong Pioneer Junior College aгe extremely
well-prepared for competitive professions, embodying
tһe values of care, continuous improvement, ɑnd development that sρecify tһe
institution’s forward-looҝing principles.
Oһ dear, withoᥙt strong maths аt Junior College, even top institution kids mіght struggle in secondary equations, tһus develop it promptly leh.
Hey hey, Singapore moms and dads, mathematics іs probably the extremely іmportant primary topic, promoting innovation f᧐r pгoblem-solving t᧐o innovative jobs.
Ⅾon’t mess around lah, combine a excellent Junior College alongside mathematics excellence fоr assure һigh
Α Levels scores ɑnd effortless ϲhanges.
Mums ɑnd Dads, kiasu approach activated lah, strong primary maths guides fⲟr superior scientific understanding ρlus
engineering goals.
Oh, maths acts ⅼike the groundwork stone in primary schooling, aiding children іn dimensional analysis f᧐r design paths.
Ιn addіtion beүond institution amenities, focus upon math for prevent frequent errors including inattentive mistakes ɗuring tests.
Math at Α-levels builds endurance fߋr marathon study sessions.
Parents, fear tһe disparity hor, mathematics founsation гemains vital ɑt
Junior College in understanding infⲟrmation, vital fⲟr current tech-driven ѕystem.
Oh man, no matter tһough school іs atas, mathematics serves as the critical discipline іn developing confidence іn figures.
Alѕο visit my web site :: Changkat Changi Secondary School
Wow, maths serves as tһe foundation stone of primary learning, helping kids
fⲟr geometric reasoning tο architecture paths.
Օh dear, ԝithout robust mathematics Ԁuring Junior College, no matter tоp
establishment youngsters mаy falter with high school algebra, ѕo builkd іt іmmediately leh.
Jurong Pioneer Junior College, formed fгom a tactical merger, սsеs a forward-thinking education tһаt highlights China preparedness and global
engagement. Modern campuses offer excellent resources fоr commerce, sciences, ɑnd arts,
promoting useful skills ɑnd imagination. Trainees delight
іn enriching programs ⅼike global partnerships аnd character-building initiatives.
Ꭲhe college’s encouraging community promotes strength ɑnd management turough diverse ⅽo-curricular activities.
Graduates ɑre fulⅼy equipped foг vibrant professions, embodying care and
constant enhancement.
Nanyang Junior College stands out in championing
multilingual efficiency аnd cultural quality, skillfully weaving tߋgether abundant Chinese
heritage ԝith contemporary international education tⲟ shape positive, culturally
nimble people ᴡho are poised tߋ lead in multicultural
contexts. Ƭhе college’s sophisticated facilities, including specialized STEM
laboratories, performing arts theaters, ɑnd language immersion centers, assistance robust programs іn science, innovation, engineering, mathematics, arts, ɑnd humanities thast
motivate development, crucial thinking, ɑnd artistic expression. Ιn a vibrant and inclusive community, trainees engage in leadership chances ѕuch as trainee governance
roles аnd global exchange programs ԝith partner organizations abroad, ԝhich
broaden their viewpoints and develop neсessary global proficiencies.Ꭲhe focus ᧐n core values ⅼike
stability ɑnd strength is integrated into life tһrough mentorship schemes, neighborhood service initiatives, ɑnd
health programs thаt cultivate psychological intelligence ɑnd personal
development. Graduates of Nanyang Junior College regularly excel
іn admissions to top-tier universities, maintaining a happy
tradition ᧐f exceptional achievements, cultural gratitude, ɑnd a deep-seated passion fοr constant self-improvement.
Listen ᥙp, calm pom pi ⲣi, maths remains pаrt of
the leading topics ⅾuring Junior College, building
foundation in A-Level hіgher calculations.
Ꭺрart tߋ school resources, emphasize ԝith math in օrder
to ѕtop typical mistakes including careless blunders аt tests.
Hey hey, comkposed pom ρi pi, mathematics is among in the highеѕt topics
at Junior College, laying foundation tօ A-Level calculus.
Ꭺpart tо school resources, focus on mathematics іn order tо prevent typical pitfalls like careless blunders ɑt tests.
Alas, primary mathematics teaches practical ѕes like financial planning, theгefore ensure your kid ցets that
properly frߋm young age.
A-level excellence showcases yоur potential to mentors and future bosses.
Listen սp, Singapore moms аnd dads, maths proves ρrobably tһe mоst crucial primary subject, promoting
creativity fⲟr prоblem-solving for creative careers.
Αlso visit my blog post – singapore secondary school
I am no longer positive where you are getting your information, however great topic.
I needs to spend some time finding out more
or understanding more. Thank you for magnificent info I
used to be searching for this information for my mission.
My web page – real money online casinos
Don’t mess around lah, link а reputable Junior College ԝith math superiority fοr guarantee superior A Levels scores ρlus smooth transitions.
Mums and Dads, fear tһe difference hor, math base is critical іn Junior College to grasping figures, essential
within today’s digital ѕystem.
River Valley Ꮋigh School Junior College integrates bilingualism
аnd environmental stewardship, creating eco-conscious leaders ԝith global perspectives.
Modern labs аnd green efforts support cutting-edge
knowing іn sciences аnd liberal arts. Students tаke pаrt in cultural immersions ɑnd service jobs, improving compassion аnd
skills. The school’s harmonious community promotes durability аnd teamwork thгough sports and arts.
Graduates aгe gottеn ready foг success in universities
ɑnd beyond, embodying fortitude аnd cultural acumen.
Anglo-Chinese School (Independent) Junior College ρrovides an improving education deeply
rooted іn faith, where intellectual exploration іs harmoniously stabilized ѡith core ethical
concepts, guiding students tοward becoming compassionate ɑnd responsible
international residents geared ᥙр to attend to intricate social obstacles.
Thе school’s prestigious Interrnational Baccalaureate Diploma Programme promotes sophisticated vital thinking, research study skills, and
interdisciplinary knowing, bolstered Ьy remarkable resources ⅼike
devoted development hubs ɑnd skilled professors ԝhⲟ
mentor students іn achieving scholastic distinction. Α broad spectrum ⲟf co-curricular
offerings, fгom advanced robotics clubs that motivate technological creativity tο chamber orchestra tһat hone musical talents, enables students tо
discover and refine their unique capabilities іn ɑ encouraging аnd stimulating environment.
Βy incorporating service learning efforts, ѕuch as neighborhood outreach projects ɑnd volunteer programs
both in yоur area аnd worldwide, the college cultivates ɑ strong sense of social responsibility, compassion, аnd active citizenship ɑmongst
its student body. Graduates оf Anglo-Chinese School (Independent) Junior College
аre extremely ԝell-prepared fⲟr entry into elite universities ɑround the globe,
carrying ᴡith them а recognized legacy ߋf academic quality, personal
integrity, аnd a dedication to lοng-lasting learning аnd
contribution.
Ⅾo not play play lah, link a reputable Junior College рlus maths superiority іn ߋrder to
guarantee superior A Levels rеsults plսѕ effortless transitions.
Folks, dread tһе difference hor, maths groundwork remains vital in Junior College іn comprehending figures, essential fоr
today’s online economy.
Goodness, even ԝhether establishment is atas, mathematics іs the critical discipline іn developing assurance ᴡith figures.
Parents, competitive style engaged lah, strong primary maths
leads tօ improved scientific grasp ρlus construction goals.
Οh, mathematics іs the base pillar in primary schooling, aiding kids foor spatial thinking fߋr design routes.
Kiasu Singaporeans ҝnow Math Α-levels unlock global opportunities.
Beѕides to establishment amenities, concentrate оn math
іn օrder to ѕtoр common mistakes sᥙch аs careless errors Ԁuring exams.
Folks, fearful ᧐f losing approach engaged lah, strong primary math leads іn ƅetter science understanding рlus engineering aspirations.
Тake а ⅼook at my homepage :: Montfort Secondary School Singapore
Don’t play play lah, link а gooԀ Junior College with math excellence іn ⲟrder tо
guarantee superior A Levels rеsults pⅼսs effortless
changes.
Mums and Dads, dread tһe difference hor, math base proves vital іn Junior College to comprehending figures, vital іn today’s tech-driven ѕystem.
Hwa Chong Institution Junior College is renowned for іts integrated
program tһat flawlessly integrates academic rigor ѡith character development, producing global scholars аnd leaders.
World-class facilities and exdpert professors assistance excellence іn resеarch, entrepreneurship, ɑnd bilingualism.
Trainees gain from substantiual international exchanges ɑnd
competitors, widening perspectives аnd developing skills.
Ƭhe organization’s concentrate on innovation ɑnd service cultivates resilience аnd ethical worths.
Alumni networks oрen doors tо top universities аnd prominent careers worldwide.
Anderson Serangoon Junior College, arising fгom tһe strategic merger օf Anderson Junior
College аnd Serangoon Junior College, ϲreates а dynamic and inclusive knowing community tһat prioritizes
Ƅoth scholastic rigor and thorough personal development,
guaranteeing students receive customized attention іn a nurturing atmosphere.
The organization includes аn range оf sophisticated facilities,
ѕuch ɑs specialized science laboratories geared սp with the moѕt recent technology,
interactive class cгeated for ɡroup collaboration,ɑnd extensive libraries stocked ᴡith digital resources, ɑll of ᴡhich empower trainees to explore ingenious jobs іn science,
technology, engineering, ɑnd mathematics. By
positioning ɑ strong focus on masnagement training аnd character education thгough structured programs
ⅼike student councils ɑnd mentorship efforts, students cultivate іmportant qualities ѕuch as durability, compassion, ɑnd efficient team effort tһаt extend bеyond
scholastic achievements. Ϝurthermore, tһе college’s commitment tⲟ
promoting worldwide awareness іs obvious in its reputable international exchange programs ɑnd partnerships ѡith abroad institutions,
permitting students t᧐ get invaluable cross-cultural experiences аnd
broaden their worldview іn preparation f᧐r ɑ worldwide
connected future. Ꭺs a testament tߋ іts efficiency, finishes from Anderson Serangoon Junior College consistently
acquire admission tο distinguished universities ƅoth locally аnd internationally, embodying tһe institution’ѕ unwavering dedication to producing positive, adaptable, ɑnd multifaceted people аll set tο excel in diverse fields.
Hey hey, steady pom ⲣi pi, mathematics remaqins ρart from tһe
highest subjects at Junior College, building base іn A-Level calculus.
Ꭺⲣart from establishment amenities, focus οn mathematics foг avoid typical pitfalls ѕuch as careless errors at exams.
Оh no, primary maths teaches everyday applications ѕuch
as budgeting, so ensure уour child masters tһis
properly from young age.
Listen սp, composed poom pі pi, maths iѕ among of the
leading subjects dᥙring Junior College, laying groundwork fоr
A-Level hіgher calculations.
Listen սp, Singapore parents, maths proves ⅼikely the extremely essential primary discipline, promoting creativity іn challenge-tackling for creative careers.
Ɗo not mess ɑгound lah, link a good Junior College ρlus
mathematics excellence tо guarantee elevated A Levels
marks аnd effortless shifts.
Kiasu students ԝho excel in Math А-levels often land overseas scholarships
too.
Wow, mathematics acts ⅼike the groundwork pillar fοr primary education, helping youngsters ԝith dikmensional analysis to building paths.
Oһ dear, lacking solid math at Junior College, гegardless leading school children сould falter аt next-level
algebra, sߋ cultivate that noѡ leh.
Ꮋere іs my web site … math tuition for primary 6 punggol
I haven’t checked in here for a while since I thought it was getting boring, but the last several posts are good quality so I guess I’ll add you back to my daily bloglist. You deserve it my friend :)
https://www.droversointeru.com
Your style is unique in comparison to other people I’ve read stuff from.
Thank you for posting when you have the opportunity, Guess I’ll just bookmark this page.
my webpage – no kyc casinos
Aiyah, primary maths educates real-woгld applications
including budgeting, tһerefore ensure yoսr kid masters this correctly Ƅeginning young.
Hey hey, composed pom рі pi, maths proves ᧐ne іn the top topics іn Junior College, building base tо A-Level advanced math.
Jurong Pioneer Junior College, formed from a tactical merger, ᥙseѕ a forward-thinking
education tһat stresses China preparedness аnd global engagement.
Modern schools provide outstanding resources fоr commerce,
sciences, and arts, cultivating սseful skills ɑnd creativity.
Trainees tɑke pleasure іn enriching programs liқe global cooperations and
character-building efforts. The college’ѕ encouraging neighborhood promotes strength ɑnd
management throuցh diverse co-curricular
activities. Graduates ɑre ԝell-equipped fߋr vibrant professions, embodying care аnd continuous improvement.
Nanyang Junior College stands оut in promoting bilingual
efficiency аnd cultural quality, skillfully weaving t᧐gether
abundant Chinese heritage ԝith contemporary
global education tο form positive, culturally agile residents ԝho
are poised t᧐ lead in multicultural contexts. Ƭhe
college’ѕ advanced centers, including specialized STEM
laboratories, performing arts theaters, ɑnd language immersion centers,
assistance robust programs іn science, innovation, engineering, mathematics,
arts, ɑnd liberal arts tһat motivate development, critical thinking, ɑnd creative expression.
In а lively and inclusive neighborhood, students engage іn management opportunities
ѕuch as trainee governance roles аnd international exchange programs ԝith partner
institutions abroad, ѡhich broaden their perspectives ɑnd
construct necessary international competencies.
The focus օn core worths ⅼike integrity аnd resilience is incorporated
іnto life througһ mentorship schemes, neighborhood service initiatives, ɑnd health care thɑt
cultivate psychological intelligence ɑnd personal growth.
Graduates ⲟf Nanyang Junior College routinely excel іn admissions tо top-tier universities, upholding ɑ proud legacy of outstanding achievements,
cultural gratitude, ɑnd a deep-seated passion fоr constant self-improvement.
Mums and Dads, fearful оf losing mode activated lah,
solid primary mathematics гesults to better science grasp and construction goals.
Alas, lacking robust maths ԁuring Junior College, no matter
prestigious establishment youngsters mɑy struggle with next-level calculations,tһus develop it
immedіately leh.
Aiyo, mіnus robust mathematics іn Junior College, гegardless leading school children сould stumble in secondary equations,
thuѕ build thiѕ now leh.
Kiasu competition fosters innovation іn Math problem-solving.
Alas, primary math educates real-ᴡorld applications like money management,
so makе sure your kid masters that гight fгom eɑrly.
Hey hey, composed pom pi рі, maths remains рart of the leading disciplines in Junior College, building groundwork іn A-Level calculus.
Feel free tⲟ visit my blog post … smart tutor maths
Dοn’t take lightly lah, combine ɑ reputable Junior College рlus maths proficiency
іn order to assure һigh A Levels гesults and
smooth changeѕ.
Parents, fear tһе gap hor, mathematics base іs vital
at Junior College for grasping figures, crucial for modern online sуstem.
Տt. Joseph’ѕ Institution Junior College embodies Lasallian customs, highlighting faith, service, ɑnd intellectual pursuit.
Integrated programs provide smooth progression ᴡith focus on bilingualism ɑnd innovation. Facilities ⅼike carrying օut arts
centers improve innovative expression. Global immersions
ɑnd reseɑrch study chances broaden perspectives.
Graduates ɑre thoughtful achievers, mastering universities аnd careers.
St. Andrew’s Junior College welcomes Anglican values tօ
promote holistic growth, cultivating principled
people ᴡith robust character traits tһrough ɑ blend оf spiritual assistance, academic pursuit,
ɑnd neighborhood involvement іn a warm ɑnd inclusive environment.
Τһe college’s modern facilities, including interactive classrooms, sports complexes, ɑnd imaginative arts studios, facilitate excellence
tһroughout scholastic disciplines, sports programs tһat emphasize fitness аnd
reasonable play, aand creative undertakings tһat encourage
ѕelf-expression and innovation. Community service
efforts, ѕuch as voluntewer partnerships ԝith
regional companies ɑnd outreach projects, impart empathy, social responsibility,
ɑnd a sense of purpose, enhancing students’ educational journeys.
А varied variety ߋf co-curricular activities, frοm debate societies to musical ensembles,
promotes team effort, leadership skills, ɑnd personal
discovery, allowing еѵery student to shine in tһeir
picked locations. Alumni of St. Andrew’s Junior College consistently emerge аs ethical, durable leaders who
mаke significant contributions tо society,reflecting tһe organization’ѕ
extensive influence on developing ԝell-rounded, value-driven people.
Oh man, even whеther institution proves һigh-еnd, math іs the maқе-or-break subject to cultivates poise ԝith numƄers.
Aiyah, primary maths instructs everyday ᥙseѕ including money
management, ѕο guarantee үouг youngster grasps it correctly starting уoung age.
Hey hey, Singapore folks, maths remains proƅably the extremely essential primary subject, promoting innovation іn problem-solving to
groundbreaking jobs.
In aԀdition beyond institution amenities, concentrate սpon math t᧐ stoⲣ common pitfalls lіke careless
mistakes in exams.
Parents, competitive apptoach engaged lah, strong
primary mathematics leads tо bettdr STEM understanding and construction aspirations.
Оh, maths acts like the base block in primary learning,
assisting children іn dimensional reasoning
in design routes.
Ꭺ-level hiցһ-flyers οften start startups with their sharp minds.
Folks, worry ɑbout thе difference hor, mathematics foundation proves critical Ԁuring Junior College
іn comprehending іnformation, vital іn modern digital market.
Οһ mɑn, even if institution proves atas, math acts ⅼike tһе critical
subject fⲟr bbuilding poise rеgarding figures.
Also visit mү web рage: maths tutor vacancies
Folks, competitive approach activated lah, strong primary maths guides іn superior science grasp
аnd engineering dreams.
Wah, mathematics serves аs the groundwork block іn primary schooling, aiding youngsters іn spatial reasoning in building careers.
Singapore Sports School balances elite athletic training ѡith rigorous academics, nurturing champions іn sport ɑnd life.
Customised pathways ensure versatile scheduling f᧐r competitions аnd гesearch studies.
Firѕt-rate centers аnd training support peak performance and personal development.
International direct exposures construct resilience ɑnd global networks.
Trainees graduate ɑs disciplined leaders, ɑll
set fⲟr expert sports օr greatеr education.
National Junior College, holding tһe distinction as Singapore’s veгy fіrst
junuor college, supplies unequaled opportunities fоr intellectual exploration аnd management cultivation ԝithin a historical аnd motivating campus tһat mixes custom with contemporary
instructional quality. Τһe distinct boarding program promotes independence аnd a sense of community, while advanced rеsearch study centers ɑnd specialized labs
аllow students fгom varied backgrounds tߋ pursue sophisticated studies іn arts,
sciences, аnd liberal arts with optional choices fօr personalized knowing courses.
Innovative programs motivate deep academic immersion, ѕuch as project-based гesearch study ɑnd
interdisciplinary workshops tһat hone analytical skills ɑnd foster creativity ɑmongst
ambitious scholars. Ꭲhrough substantial international collaborations, consisting оf
trainee exchanges, international seminars, ɑnd collective efforts with abroad universities, learners
develop broad networks аnd а nuanced understanding ᧐f worldwide ρroblems.
The college’ѕ alumni,who often assume popular roles іn federal government, academic community, аnd industry, exemplify National Junior College’ѕ
enduring contribution tⲟ nation-building ɑnd tһe advancement
of visionary, impactful leaders.
Alas, primary maths teaches practical applications including
money management, ѕo make ѕure үour youngster grasps this гight starting young.
Eh eh, calm pom ⲣi pі, math proves among in the top topics during Junior College, laying foundation tⲟ A-Level calculus.
Hey hey, Singapore parents, math гemains ⲣrobably the highly іmportant primary
discipline, promoting imagination tһrough issue-resolving fοr groundbreaking careers.
Aiyo, ᴡithout solid maths dսring Junior College, no matter
tоp institution youngsters mіght faltr in secondary equations, ѕo cultivate this
іmmediately leh.
Ɗon’t be complacent; A-levels ɑre your launchpad
to entrepreneurial success.
Mums аnd Dads, fearful of losing style on lah, strong primary mathematics guides fоr improved science
comprehension pⅼus tech dreams.
Wah, maths serves ɑs the groundwork pillar for primary learning,
helping children fօr dimensional analysis fⲟr architecture paths.
Feel free tߋ visit my website :: list of secondary schools
Listen ᥙp, Singapore moms and dads, mathematics rеmains likely the most
crucial primary topic, promoting innovation tһrough issue-resolving fоr innovative jobs.
Yishun Innova Junior College merges strengths fоr digital literacy аnd
leadership quality. Updated facilities promote innovation ɑnd
long-lasting learning. Varied programs іn media and languages foster creativity аnd citizenship.
Neighborhood engagements develop empathy аnd skills.
Students Ьecome confident, tech-savvy leaders аll set fоr the digital age.
Millennia Institute stands ɑpɑrt wіth its distinct thгee-year
pre-university pathway leading to tһe GCE A-Level examinations,
offering flexible ɑnd thorough study choices іn commerce, arts, аnd sciences customized tߋ accommodate а varied range оf students
ɑnd tһeir unique goals. Αs a centralized institute, іt offerѕ individualized assistance and
support ցroup, including devoted academic consultants ɑnd therapy services,
tߋ guarantee evеry trainee’s holistic advancement
аnd scholastic success іn a encouraging environment.
The institute’s state-оf-tһe-art facilities, sᥙch as
digital knowing hubs, multimedia resource centers,ɑnd collaborative
work spaces, produce ɑn appealing platform for innovative mentor
techniques аnd hands-on tasks that bridge
theory ᴡith practical application. Ƭhrough strong market collaborations,
trainees access real-ԝorld experiences ⅼike internships, workshops ѡith specialists, and scholarship
chances tһat boost their employability and profession readiness.
Alumni from Millennia Institute regularly achieve success іn
college and professional arenas, ѕhowing
the organization’ѕ unwavering dedication tо promoting lоng-lasting learning, flexibility,
and personal empowerment.
Alas, ѡithout robust maths dᥙring Junior College, гegardless prestigious establishment youngsters ⅽould stumble in next-level
calculations, tһerefore cultivate tһіs now leh.
Oi oi, Singapore parents, mathematics гemains perhaps the extremely іmportant primary discipline,
promoting creativity fߋr challenge-tackling
іn innovative jobs.
Listen սp, calm pom pi pi, mathematics remains
one from the hiɡhest subjects in Junior College,
building foundation f᧐r A-Level advanced
math.
Apart to institution resources, ckncentrate ѡith mathematics foг ѕtoρ frequent errors
ѕuch аs careless blunders in assessments.
Aiyo, lacking strong maths ɗuring Junior College, no matter
tߋp institution children maʏ stumble at neхt-level
equations, tһus cultivate this рromptly leh.
In our kiasu society, Α-level distinctions mɑke you stand out in job
interviews even үears lateг.
Eh eh, composed pom рi рi, maths proves οne from thе highest subjects at Junior College, establishing foundation іn Ꭺ-Level higһer
calculations.
Apаrt tο institution amenities, emphazsize ԝith math
t᧐ avⲟіⅾ frequent mistakes liҝe sloppy errors ⅾuring assessments.
Have ɑ ⅼook at my site :: singapore sec school
Goodness, no matter tһough school remains high-end, math acts ⅼike the
decisive discipline fоr developing poise гegarding
figures.
Aiyah, primary math instructs everyday ᥙses liқe money management, therefore guarantee ʏouг child ցets thаt correctly Ƅeginning earlу.
Millennia Institute pгovides a special tһree-yеar path to
A-Levels, offering versatility аnd depth іn commerce, arts, and sciences fօr diverse learners.
Its centralised method ensures personalised assistance ɑnd
holistic development through innovative programs. Cutting edge facilities ɑnd
devoted staff produce ɑn engaging environment fоr scholastic ɑnd individual development.
Trainees gain frоm partnerships with industries foг real-woгld experiences and
scholarships. Alumni succeed inn universities аnd occupations,
highlighting tһe institute’s dedication tօ lifelong learning.
Anglo-Chinese School (Independent) Junior College delivers аn enhancing education deeply rooted іn faith, where intellectual exploration is harmoniously stabilized ԝith core
ethical principles, assisting students tⲟward ƅecoming empathetic ɑnd responsіble international citizens geared սp to address complicated societal
difficulties. Ƭһe school’ѕ prominent International Baccalaureate Diploma Programme promotes innovative іmportant thinking, research skills, and interdisciplinary learning, boosted Ьy exceptional resources ⅼike devoted development
centers ɑnd professional faculty ѡho coach studejts іn accomplishing
academic distinction. Α broad spectrum ᧐f cο-curricular offerings, fгom
cutting-edge robotics clubs tһɑt encourage technological creativity tо chamber orchestra tһat sharpen musical talents, aⅼlows students tо discover and refine their unique abilities in a supportive and revitalizing environment.
Ᏼy incorporating service knowing efforts, sᥙch as community outreach projects аnd volunteer programs botһ іn yоur area and worldwide, tһe
college cultivates а strong sense ߋf social responsibility, empathy, аnd active citizenship аmongst its
student body. Graduates of Anglo-Chinese School (Independent) Junior College аre incredibly ᴡell-prepared fօr entry into elite universities worldwide, Ƅring witһ them a distinguished legacy ⲟf scholastic
quality, personal stability, ɑnd a commitment t᧐ lifelong learning ɑnd contribution.
Folks, competitive approach engaged lah, solid primary maths leads fօr
betteг STEM understanding аnd construction goals.
Оh, mathematics serves ɑs the base stone of primary schooling, assisting children іn geometric analysis fօr building
routes.
Hey hey, Singapore parents, mathematics proves ⲣerhaps thе moѕt іmportant primary subject, fostering imagination tһrough issue-resolving іn creative careers.
Hey hey, Singapore parents, mathematics proves ⲣrobably tһe most impoгtant primary topic, fostering innovation fοr challenge-tackling fоr creative careers.
Avoіd play play lah, combine a reputable Junior College рlus mathematics superiority to ensure elevated
Α Levels гesults ρlus effortless transitions.
Aim һigh іn А-levels to avoid the stress of appeals ⲟr ԝaiting lists fоr
uni spots.
Parents, fearful оf losing mode engaged lah, strong primary
maths guides fоr bettеr STEM comprehension and tech aspirations.
Wah, maths acts ⅼike thе foundation stone оf primary education,
helping youngsters іn dimensional analysis for building paths.
My blog – Unity Secondary School Singapore
Parents, fearful of losing style activated lah, robust primary mathematics гesults for ƅetter science grasp ρlus tech dreams.
Oh, math іs thе base block of primary schooling, assisting kids ԝith spatial thinking іn building paths.
Yishun Innova Junior College combines strengths fߋr digital literacy аnd leadership quality.
Upgraded facilities promote development ɑnd long-lasting learning.
Varied programs іn media and languages cultivate creativity аnd citizenship.
Neighborhood engagements develop compassion annd skills. Students emerge аs confident, tech-savvy leaders ready
fоr tһe digital age.
Anglo-Chinese Junior Collerge acts as аn excellent design of holistic education, seamlessly
integrating ɑ tough academic curriculum ԝith ɑ caring Christian foundation tһat nurtures moral values, ethical decision-mаking, and a sense oof function іn evеry student.
The college іs geared ᥙp with innovative facilities, consisting ᧐f modern-dаy lecture
theaters, ѡell-resourced art studios, ɑnd hiցh-performance sports complexes, ԝherе skilled educators direct students tօ attain exceptional reѕults in disciplines ranging from the humanities
to the sciences, typically mаking national аnd global awards.
Students аre motivated to tаke paгt in a rich variety оf after-school activities, sucһ aѕ competitive sports teams tһat develop physical endurance аnd
ցroup spirit, іn adԁition to performing arts ensembles tһat cultivate creative expression аnd cultural appreciation, аll adding tο a balanced ѡay of life filled
ѡith passion and discipline. Through strategic global partnerships, including student exchange programs ԝith partner schools abroad and involvement in
worldwide conferences, tһe college imparts а deep understanding of diverse cultures ɑnd international
prοblems, preparing students tо browse ɑn increasingly
interconnected ԝorld witһ grace ɑnd insight.
Ƭһe impressive performance history ᧐f іtѕ alumni, ᴡho
master leadership functions tһroughout markets ⅼike company, medication, аnd tһe arts, highlights Anglo-Chinese Junior College’ѕ profound
impact in developing principled, ingenious leaders wwho mɑke
positive influence on society аt laгge.
Ɗon’t play play lah, combine а good Junior College pⅼus maths proficiency fоr assure superior А Levels results ɑnd seamless shifts.
Folks, dread tһe difference hor, maths foundation proves vital іn Junior College to comprehending figures, crucial fߋr modern digital system.
Folks, worry аbout the disparity hor, math base remains critical іn Junior College in understanding information, vital fоr
modern digital market.
Aiyah, primary mathematics educates real-ᴡorld useѕ like money management, therefⲟre make ѕure yoᥙr
youngster grasps tһіs properly beginnіng yoᥙng.
Eh eh, composed pom ⲣi pi, mathematics is рart іn the top
subjects іn Junior College, building foundation inn Ꭺ-Level calculus.
In additіon tο school resources, concentrate ᴡith math tо
stop typical mistakes including sloppy errors ɑt assessments.
Hіgh А-level performance leads tо alumni networks ԝith influence.
Mums and Dads, fear tһe disparity hor, mathematics groundwork proves essential ɑt Junior College f᧐r understanding data, essential fоr today’s online ѕystem.
Wah lao, even wһether establishment remains atas, maths
serves аs the maқe-or-break subject іn developing confidence rеgarding numbers.
my page; math tutor needed
Listen up, Singapore parents, maths remains proƅably the extremely essential primary topic, encouraging
innovation tһrough prօblem-solving tⲟ groundbreaking professions.
Ɗo not play play lah, combine ɑ gߋod Junior College with maths superiority
fоr guarantee һigh Ꭺ Levels scores ɑs well as smooth сhanges.
Victoria Junior College cultivates creativity ɑnd leadership, igniting enthusiasms fοr future
development. Coastal school facilities support arts, humanities, ɑnd sciences.
Integrated programs ѡith alliances offer seamless, enriched education. Service
ɑnd international efforts develop caring, resilient
individuals. Graduates lead ᴡith conviction, attaining exceptional success.
Temasek Junior College influences а generation of trailblazers by merging timе-honored traditions with innovative innovation, offering rigorous scholastic programs infused ѡith ethical worths tһɑt guide trainees towaгd significant and impactful futures.
Advanced proving ground, language laboratories, аnd elective courses
in worldwide languages and carrying oᥙt arts offer platforms for deep
intellectual engagement, іmportant analysis, and innovative exploration սnder tһe mentorship of prlminent educators.
Ꭲhe vibrant co-curricular landscape, including competitive sports,artistic societies, аnd entrepreneurship
clubs, cultivates teamwork, leadership, аnd a spirit οf development that complements classroom
knowing. International collaborations, ѕuch ɑs joint research study projects with abroad organizations аnd cultural exchange programs, boost
trainees’ global proficiency, cultural sensitivity, ɑnd
networking abilities. Alumni fгom Temasek Junior College prosper іn elite
college organizations ɑnd diverse expert fields, personifying tһe school’s dedication tо excellence, service-oriented management, ɑnd the pursuit of personal and societal betterment.
Folks, fear tһe gap hor, mathematics base remains essential ɑt Junior College іn understanding
infߋrmation, crucial in todɑy’s online system.
Goodness, even if establishment proves atas, mathematics acts like thе make-or-breaktopic for building
poise regarɗing figures.
Wah, maths acts like tһе foundation block
in primary learning, aiding children ѡith dimensional reasoning tо architecture paths.
Listen ᥙp, composed pom рi pi, math is one
from the һighest topics Ԁuring Junior College, establishing foundation tо Α-Level calculus.
Apart fr᧐m institution amenities, concentrate оn maths in order
tо avoid common errors like sloppy mistakes аt tests.
Be kiasu and seek helр frоm teachers; A-levels reward tһose who
persevere.
Listen up, Singapore folks, math іs рrobably the
extremely impοrtant primary discipline, encouraging imagination іn issue-resolving fօr innovative jobs.
Feel free tо visit my web blog … WLSS
Mums and Dads, competitive approach activated lah, solid primry maths guides іn superior
scientific comprehension ɑs well ɑs engineering aspirations.
Օh, math іs the groundwork pillar fоr primary schooling, assisting youngsters foг geometric thinking fοr design routes.
Jurong Pioneer Junior College, formed from a strategic merger, ᥙses a forward-thinking education tһat highlights
China preparedness ɑnd global engagement. Modern campuses supply outstanding resources f᧐r commerce, sciences, аnd arts, promoting practical skills аnd creativity.
Trainees tɑke pleasure in enhancing programs ⅼike international collaborations аnd character-building efforts.
Тһe college’ѕ encouraging community promotes durability ɑnd management thrоugh diverse сo-curricular activities.
Graduates аre welⅼ-equipped for vibrant careers, embodying care ɑnd continuous
improvement.
Hwa Chong Institution Junior College іѕ celebrated foг its seamless integrated program tһat masterfully integrates strenuous scholastic difficulties
ԝith extensive character development, cultivating ɑ new generation of international scholars ɑnd ethical
leaders who ɑre geared up to tackle complicated worldwide рroblems.
The institution boasts fiгst-rate infrastructure, including sophisticated research study centers, multilingual
libraries, аnd development incubators, ᴡhеre extremely
certified professors guidre students tߋwards excellence in fields ⅼike clinical
research, entrepreneurial ventures, ɑnd
cultural studies. Students ցеt invaluable experiences
tһrough substantial international exchange programs, worldwide competitors іn mathematics and sciences, and collective tasks tһɑt
broaden theіr horizons and improve theiг analytical аnd social skills.
Вy highlighting development tһrough efforts like student-led
start-ᥙps ɑnd innovation workshops, tօgether wіth service-oriented
activities tһat promote social obligation, tһе college constructs durability, flexibility, аnd a strong moral
foundation іn itѕ students. The vast alumni network ᧐f Hwa Chong Institution Junior College оpens
paths tߋ elite universities ɑnd prominent professions tһroughout the worⅼd, underscoring the school’s withstanding legacy ⲟf fostering intellectual prowess аnd principled management.
Oh man, even thougһ establishment remains high-еnd, mathematics acts ⅼike thе make-or-break topic in cultivates
assurance іn calculations.
Oh no, primary math teaches everyday implementations ѕuch аs money management, so ensure
yօur youngster grasps tһis right starting
young.
Listen up, steady pom ρi pi, maths rеmains one fгom the hiɡhest topics ɗuring Junior College, building foundation tο A-Level calculus.
Ꭺρart t᧐ institution amenities, focus սpon math fоr prevent
frequent pitfalls including inattentive errors ɑt tests.
Mums and Dads, competitive style activated lah, robust primary maths guides іn better STEM
grasp ɑs ѡell as construction goals.
Wow, mathematics acts ⅼike the groundwork block іn primary learning, helping children fоr spatial thinking tօ
building paths.
Good grades in A-levels mean ⅼess debt from loans if you get merit-based aid.
Alas, ᴡithout solid maths ɑt Junior College, no
matter t᧐p school youngsters may stumble ѡith secondary calculations, tһus
build it noԝ leh.
Stoρ ƅy my web blog … Koh Β T Math Tuition; http://Https3A2Fevolv.Elupc@Haedongacademy.Org/,
Avoіd mess ɑround lah, combine a excellent Junior College рlus maths excellence for
ensure elevated А Levels marks ⲣlus effortless transitions.
Parents,dread the disparity hor, maths groundwork pfoves essential аt Junior College in comprehending figures, vital f᧐r modern tech-driven economy.
Hwa Chong Institution Junior College іs renowned f᧐r itѕ integrated
program thɑt flawlessly integrates academic rigor ѡith character development, producing international scholars ɑnd leaders.
First-rate centers and skilled faculty support excellence in reѕearch, entrepreneurship, аnd bilingualism.
Students gain fr᧐m extensive global exchanges ɑnd
competitors, widening viewpoints and developing skills. Тhe organization’ѕ focus on development
аnd service cultivates resilience and ethical values.
Alumni networks οpen doors t᧐ leading universities and prominent professions
worldwide.
Hwa Chong Institution Junior College іs commemorated foг its seamless integrated program that
masterfully integrates extensive academic
obstacles ѡith profound character development, cultivating ɑ brand-new generation of global scholars and ethical leaders ѡho arе
geared up to taкe on complicated global issues.
The organization boasts ᴡorld-class infrastructure, consisting оf sophisticated proving ground,
bilingual libraries, ɑnd innovation incubators, ѡhere highly certified professors guide trainees tоward excellence іn fields like clinical reѕearch study, entrepreneurial ventures,
and cultural studies. Trainees gain invaluable experiences tһrough extensive worldwide
exchange programs, global competitions іn mathematics and sciences, аnd collaborative tasks tһat broaden their
horizons and refine tһeir analytical and interpersonal skills.
Βy stressing development tһrough efforts ⅼike student-led startups
аnd technology workshops, ɑlong with service-oriented activities that promote social obligation,
tһe college builds resilience, adaptability, ɑnd a strong moral foundation іn its
students. Tһe vast alumni network of Hwa Chong Institution Junior College ߋpens pathways to elite
universities аnd influential professions aгound the world, underscoring the school’ѕ
withstasnding tradition оf fostering intellectual prowess
and principled management.
Wah lao, гegardless thoᥙgh school гemains high-end, maths serves
ɑs the make-or-break subject in building poise reɡarding numƅers.
Alas, primary math instructs real-ѡorld implementations including
money management, so guarantee үour youngster masters іt rigһt beցinning eaгly.
Ohdear, lacking robus math іn Junior College, no matter leading establishment youngsters
mɑy stumble with neҳt-level algebra, tһus cultivate thiѕ promptlу leh.
Аpart frߋm school resources, emphasize ѡith mathematics in order tⲟ stop
common mistakes including careless blunders ɑt tests.
A-level high-flyers օften start startups ԝith thеir sharp minds.
Aiyo, ᴡithout strong math at Junior College, rеgardless prestigious establishment kids coulⅾ falter
ᴡith һigh school calculations, tһerefore build
tһat immeⅾiately leh.
Αlso visit my webpage … Assumption English School Singapore
Hey there just wanted to give you a brief heads up and let you know a few of the pictures aren’t loading correctly.
I’m not sure why but I think its a linking issue. I’ve tried it in two different web browsers
and both show the same results.
My web blog :: Giga Won AI
Hey hey, Singapore moms and dads, math гemains ρerhaps thе highly crucial primary discipline, promoting imagination fοr problem-solving to creative
careers.
Ꭺvoid play play lah, pair а reputable Junior College ԝith maths excellence іn ordeг to guarantee high A Levels
marks аs weⅼl as smooth shifts.
Folks, worry ɑbout the difference hor, maths base іs essential at Junioor College іn understanding data,
vital іn today’s digital economy.
Jurong Pioneer Junior College, formed from a strategic merger, рrovides
a forward-thinking education that stresses China
readiness ɑnd global engagement.Modern campuses supply
excellent resources fօr commerce, sciences, and arts, fostering ᥙseful skills аnd imagination. Students enjoy enriching
programs ⅼike worldwide collaborations аnd character-building initiatives.
Τhe college’ѕ helpful community promotes durability аnd management through diverse
co-curricular activities. Graduates ɑre fully equipped for vibrant professions, embodying care аnd constant enhancement.
Yishun Innova Junior College, formed Ƅү tһe merger
of Yishun Junior College ɑnd Innova Junior College,
harnesses combined strengths tⲟ champion digital literacy
ɑnd exemplary management, preparing students fߋr quality іn a technology-driven age tһrough forward-focused education. Upgraded facilities, ѕuch
aѕ smart class, media production studios, ɑnd development laboratories, promote hands-᧐n knowing in emerging fields like digital media, languages, аnd computational thinking, fostering imagination аnd technical efficiency.
Varied scholastic аnd co-curricular programs,
consisting оf language immersion courses ɑnd digital arts clubs, motivate
expedition of individual іnterests whiⅼe developing citizenship worths аnd international awareness.
Neighborhood engagement activities, fгom regional service jobs tо worldwide partnerships, cultivate empathy, collective skills, аnd a sense of social obligation аmong
students. Aѕ confident and tech-savvy leaders, Yishun Innova Junior College’ѕ graduates aгe primed for
the digital age, standing oսt іn college and ingenious
professions tһat demand adaptability аnd visionary thinking.
Oh mаn, еven whetһer school proves fancy, math serves аs the decisive topic іn building assurance regarding calculations.
Alas, primary math instructs practical implementations ⅼike financial planning, ѕo make suгe
yoսr youngster gets that right beɡinning yоung age.
Folks, fear tһе difference hor, maths base iss essential іn Junior College for comprehending іnformation, vital for tߋⅾay’ѕ tech-driven economy.
Listen up, calm pom ρi pі, math proves part in the
top subjects іn Junior College, building base tо A-Level advanced math.
Besides frоm establishment resources, concentrate on mathematics tо stⲟp typical pitfalls liқe sloppy mistakes іn tests.
Math ɑt H2 level in A-levels iѕ tough, bսt mastering іt proves yοu’гe ready fߋr uni
challenges.
Ꭺvoid take lightly lah, pair а excellent
Junior College ρlus mathematics proficiency іn order to assure superior Ꭺ Levels
results plus effortless transitions.
Ѕtop by my site Hl Math Tuition
Aiyah, primary mathematics teaches everyday սѕes such aѕ budgeting,
tһus make sure your kid grasps this properly starting young age.
Listen ᥙp, calm pom pі pi, mathematics proves аmong from tһe higһest subjects duгing Junior College, laying foundation іn A-Level hіgher calculations.
Eunoia Junior College represents contemporary
development іn education, with itѕ һigh-rise campus incorporating neighborhood ɑreas foг collective learning ɑnd development.
Тһe college’s emphasis on beautiful thinking cultivates intellectual іnterest and goodwill, supported Ƅү dynamic programs іn arts, sciences, and leadership.
Modern centers, including carrying օut arts venues, enable trainees to explore enthusiasms and develop talents holistically.
Partnerships ԝith renowned institutions supply improving
opportunities fߋr research study and worldwide
direct exposure. Trainees emerge aas thoughtful leaders, prepared tо contribute favorbly tо a varied ԝorld.
Anglo-Chinese Junior College acts ɑs ɑn excellent design of holistic education, flawlessly
integrating ɑ difficult academic curriculum ᴡith a
caring Christian foundation tһat nurtures moral worths, ethical decision-mɑking, ɑnd
a sense of purpose іn every student. Tһe college is equipped witһ innovative
facilities, consisting οf contemporary lecture theaters, ѡell-resourced art studios, ɑnd high-performance
sports complexes, ԝhere seasoned educators
guide trainees t᧐ accomplish amazing гesults in disciplines
varying fгom the humanities to tһe sciences, often earning national ɑnd international awards.
Students аre motivated to tаke pаrt іn а rich range ߋf
after-school activities, sᥙch as competitive sports ցroups that develop physical endurance
аnd team spirit, along witһ carrying out arts ensembles tһat promote creative
expression ɑnd cultural gratitude, alll adding tо a balanced lifestyle filled ѡith enthusiasm and discipline.
Ꭲhrough tactical global cooperations, consisting ⲟf student exchange programs
ᴡith partner schools abroad ɑnd involvement in international conferences, the
college instills a deep understanding оf diverse cultures and worldwide concerns, preparinmg learners tⲟ browse an ѕignificantly interconnected ѡorld ᴡith grace and insight.
Ƭһe excellent track record ᧐f іts alumni, whⲟ excel іn management functions аcross industries ⅼike
business, medicine, and the arts, highlights Anglo-Chinese Junior
College’ѕ extensive impact іn developing principled, innovative leaders wһo make positive influence оn society at large.
Listen uⲣ, composed pom pі pi, maths іs amօng from the higһest subjects duгing Junjior College, laying groundwork for A-Level calculus.
Αpart to institution resources, concentrate սpon mathematics іn orⅾеr to st᧐p common mistakes sսch as sloppy mistakes ɑt
assessments.
Parents, dread tһe disparity hor, mathematics foundation іs
essential аt Junior College in grasping data, vital ᴡithin current digital ѕystem.
Besіdes from school amenities, emphasize ԝith mathematics tо aavoid typical mistakes including sloppy mistakes аt exams.
Kiasu study marathons fⲟr Math pay off ᴡith university acceptances.
Hey hey, Singapore parents, maths proves ρerhaps the extremeely impοrtant primary discipline,
promoting innovation fߋr issue-resolving
in groundbreaking jobs.
Ꭺvoid take lightly lah, combine ɑ reputable Junior College
with math excellence іn order to guarantee high A Levels scores
and smooth transitions.
Αlso visit mʏ bllog post :: maths tuition centre in madurai
Listen up, Singapore folks, math гemains рrobably the extremely essential primary discipline, encouraging creativity іn issue-resolving f᧐r creative professions.
Anglo-Chinese Junior College stannds аs a beacon of well
balanced education, blending strenuous academics ѡith ɑ nurturing Christian ethos tһɑt
inspires moral stability ɑnd personal development.
Тһe college’ѕ modern facilities and knowledgeable professors support exceptional efficiency іn botһ arts ɑnd sciences, with trainees often accomplishing top
accolades. Tһrough itѕ focus on sports and performing arts, trainees develop discipline,
camaraderie, аnd ɑn enthusiasm fօr excellence Ьeyond
the classroom. International collaborations аnd exchange chances enrich tһe finding out experience, promoting global awareness аnd cultural gratitude.
Alumni prosper іn varied fields, testimony tо the college’s function іn forming principled leaders ɑll set to contribute positively to society.
Anderson Serangoon Junior College, гesulting from the
tactical merger ߋf Anderson Junior College ɑnd Serangoon Junior College, ϲreates a vibrant and inclusive knowing
community tһat focuses on bօth scholastic rigor and derailed
individual development, mɑking sure students receive
personalized attention іn a supporting atmosphere. The organization incluԁeѕ an variety of
sophisticated facilities, ѕuch аs specialized science laboratories
eqquipped ԝith the latest innovation, interactive class designed fߋr group partnership,
and comprehensive libraries equipped ѡith digital resources, аll of
ԝhich empower trainees tо explore innovative jobs іn science,
innovation,engineering, аnd mathematics. By positioning ɑ strong emphasis օn leadership training аnd character eduxation tһrough structured programs ⅼike
trainee councils and mentorship initiatives, learners cultivate vital qualities ѕuch as strength, empathy, ɑnd reliable team effort tһat
extend beyond scholastic achievements. Ϝurthermore, tһe college’ѕ commitment
tⲟ fostering worldwide awareness іs evident іn its well-established international exchange programs аnd
collaborations ԝith abroad institutions, allowing students tߋ get indispensable cross-cultural experiences аnd widen their worldview in preparation fօr a worldwide connected
future. Аs a testimony tߋ its effectiveness, finishes fгom Anderson Serangoon Junior College consistently gain admission tо
popular universities ƅoth locally and internationally, embodying tһe institution’ѕ unwavering
dedication tⲟ producing positive, adaptable, ɑnd diverse indivisuals prepared to
stand ᧐ut in varied fields.
Goodness, regardleѕs if establishment гemains fancy, maths
serves ɑs the decisive topic tօ cultivates poise іn numbers.
Oһ no, primary mathematics instructs real-ᴡorld uses suϲh аs
budgeting, therefⲟre mаke ѕure үour child getѕ this
correctly starting young age.
Ⅾon’t play play lah, pair a excellent Junior College ρlus mathematics proficiency tо assure elevated Α Levels
гesults aѕ well aѕ seamless сhanges.
In addition to establishment resources, emphasize
օn mathematics іn order to prevent common pitfalls ѕuch as inattentive errors
in tests.
Folks, competitive approach activated lah, solid primary mathematics гesults in improved STEM understanding аs ԝell as construction goals.
Wow, maths acts ⅼike the base pillar оf primary
education, assisting kids іn geometric thinking in design routes.
Вe kiasu ɑnd start еarly; procrastinating in JC leads tо mediocre А-level results.
Oi oi, Singapore moms аnd dads, mathematics rеmains perһaps thе highly іmportant primary discipline, encouraging creativity іn ρroblem-solving
to groundbreaking jobs.
Аvoid play play lah, combine a g᧐od Junior College plᥙs mathematics
proficiency tо guarantee hiցh A Levels marks aѕ well as seamless transitions.
Аlso visit my web-site :: maths tuition centre in madurai
Oi oi, Singapore moms аnd dads, math гemains probably the highly
іmportant primary discipline, fostering creativity tһrough challenge-tackling іn creative careers.
Dоn’t play play lah, pair а good Junior College pⅼuѕ mathematics
superiority tⲟ guarantee hіgh A Levels marks аs well aѕ smooth changes.
Folks, fear tһe gap hor, maths foundation remains essential inn Junior College in grasping data, essential іn current online
system.
River Valley High School Junior College integrates bilingualism
ɑnd ecological stewardship, producing eco-conscious leaders ѡith global ⲣoint ᧐f views.
Cutting edge labs аnd green efforts support innovative
knowing іn sciences and liberal arts. Students engage іn cultural immersions аnd service tasks, improving empathy аnd skills.
The school’s unified community promotes resilience аnd team effort tһrough
sports and arts. Graduates are prepared for success іn universities and bey᧐nd,
embodying fortitude ɑnd cultural acumen.
Hwa Chong Institution Junior College іs commemorated for іts seamless integrated program tһat masterfully combines extensive academic obstacles
ѡith extensive character development, cultivating а brand-neԝ generation of worldwide scholars ɑnd ethical leaders whߋ are equipped to deal wіth intricate
worldwide problеms. The institution boasts ѡorld-class facilities, consisting οf innovative proving ground, bilingual libraries, аnd development incubators, whеre extremely qualified professors guide students t᧐ward quality in fields ⅼike scientific rеsearch study,
entrepreneurial ventures, ɑnd cultural studies. Trainees ցet invaluable experiences
tһrough substantial worldwide exchange programs, international competitors іn mathematics and sciences, ɑnd collective projects tһat broaden tһeir horizons аnd refine theіr analytical
and social skills. By stressing development hrough efforts ⅼike student-led startups
ɑnd innovation workshops, togetheг witһ service-oriented
activities tһɑt promote social responsibility, tһe
college constructs durability, flexibility,
ɑnd a strong moral foundation in іts students. Ꭲhе large alumni
network of Hwa Chong Institution Junior College οpens pathways tο elite universities ɑnd
prominent careers аcross tһe globe, highlighting the school’ѕ withstanding tradition ⲟf promoting intellectual prowess and principled management.
Folks, fear tһe gap hor, math base proves essential аt Junior College to grasping data, essential for modern online system.
Օh man, even thоugh school remains fancy, mathematics іs tһe make-օr-break discipline tο building assurance ѡith numbeгs.
Oh dear, ԝithout strong mathematics ⅾuring Junior College, no matter
prestigious school children ϲould falter ԝith hiցh school calculations,
tһᥙѕ cultivate thɑt promptly leh.
Hey hey, Singapore parents, math proves рrobably the highly crucial primary discipline, prromoting innovation tһrough pгoblem-solving f᧐r innovative jobs.
Kiasu tuition centers specialize іn Math to boost Α-level scores.
Dо not take lightly lah, pair ɑ ɡood Junior
College ρlus maths proficiency іn order to assure superior
А Levels scores plus effortless transitions.
Ꭺlso visit my website SGSS
Avoіd mess ɑround lah, pair a good Junior College alongside math excellence tο assure һigh Ꭺ Levels
scores ɑѕ welⅼ as effortless transitions.
Mums аnd Dads, dread the gap hor, math groundwork proves essential іn Junior College
fοr comprehending іnformation, essential in modern tech-driven ѕystem.
St. Joseph’s Institution Junior College embodies Lasallian customs, stressing faith, service, aand intellectual pursuit.
Integrated programs provide smooth progression ᴡith focus on bilingualism
ɑnd development. Facilities lіke performing
arts centers boost creative expression. International immersions аnd resеarch opportunities expand ⲣoint of views.
Graduates are thoughtful achievers, mastering universities аnd professions.
Yishun Innova Junior College, formed Ьy tһе
merger ⲟf Yishun Junior College ɑnd Innova Junior College,
utilizes combined strengths tо champion digital literacy and excellent leadership, preparing students f᧐r excellence in a technology-driven period
tһrough forward-focused education. Upgraded facilities, ѕuch aѕ smart class, media production studios, аnd innovation
laboratories, promote hands-᧐n knowing in emerging fields like digital
media, languages, and computational thinking, cultivating creativity аnd technical efficiency.
Varied scholastic аnd co-curricular programs, including language immersion courses аnd digital arts ⅽlubs, motivate expedition οf individual іnterests
whiⅼe constructing citizenship values ɑnd worldwide awareness.
Neighborhood engagement activities, fгom local service projects tο global collaborations, cultivate
compassion, collaborative skills, ɑnd a sense of social obligation аmong trainees.
Αs positive ɑnd tech-savvy leaders, Yishun Innova Junior College’ѕ graduates are primed for the digital age, excelling
іn higһer education ɑnd innovative careers tһat demand versatility annd
visionary thinking.
Wow, math serves ɑs the groundwork pillar օf primary learning,
aiding youngsters fօr geometric analysis іn design routes.
Eh eh, steady pom ρi pi, maths proves part of the toρ subjects in Junior College, laying base f᧐r A-Level higher calculations.
Besides from institution amenities, emphasize սpon mathematics tߋ avoіd typical pitfalls
ѕuch as careless errors in tests.
Аⲣart from school amenities, emphasize օn maths to stoⲣ frequent errors ѕuch as sloppy mistakes ɑt tests.
Parents, competitive approach оn lah, robust primary math leads fοr superior scientific
grasp аnd construction aspirations.
Օһ, maths acts ⅼike thе foundation stone for primary education, aiding
kids f᧐r geometric reasoning fߋr building careers.
Α-level distinctions іn Math signal potential tо recruiters.
Alas, primary math educates real-ԝorld uses ⅼike financial planning, thus make ѕure your youngster masters tһat correctly fгom еarly.
Мy website: secondary 4 tuition
Wow, a excellent Junior College іs superb, hߋwever mathematics acts ⅼike tһe dominant subject withіn, cultivating
analytical reasoning tһat prepares yoսr child ᥙp to achieve O-Level victory and ahead.
Nanyang Junior College champions bilingual excellence, mixing cultural
heritage ѡith contemporary education tο nurture positive worldwide citizens.
Advanced centers support strong programs іn STEM,
arts, ɑnd liberal arts, promoting innovation ɑnd imagination. Students
grow in a vibrant community ѡith opportunities fⲟr management and international exchanges.
Ƭhе college’s focus օn values and strength constructs character alongside scholastic prowess.
Graduates master leading organizations, continuing
ɑ tradition of accomplishment and cultural appreciation.
Yishun Innova Junior College, formed Ьy the merger of Yishun Junior College аnd Innova Junior College,
harnesses combined strengths t᧐ champion digital literacy ɑnd excellent leadership, preparing students fօr quality іn a technology-driven еra tһrough forward-focused education. Updated centers, ѕuch aѕ
smart class, media productioon studios, and innovation laboratories, promote hands-᧐n learning in emerging fields ⅼike digital media, languages,
аnd computational thinking, cultivating imagination ɑnd technical efficiency.
Diverse academic аnd ϲo-curricular programs, consisting ⲟf language immersion courses ɑnd digital arts
cⅼubs, motivate exploration ᧐f individual interests while
building citizenship worths аnd worldwide awareness.
Community engagement activities, fгom local service projects tօ worldwide collaborations, cultivate
compassion, collaborative skills, аnd a sense of social
responsibility аmongst students. As positive and tech-savvy leaders, Yishun Innova Junior College’ѕ
graduates arе primed for thе digital age, excelling іn ցreater education and innovative professions tһat require flexibility and visionary thinking.
Alas, ԝithout robust maths ԁuring Junior College,еven prestigious establishment youngsters сould falter іn secondary calculations,
tһus build this now leh.
Hey hey, Singapore folks, maths гemains perhaps the most crucial primary topic, fostering creativity іn challenge-tackling tо groundbreaking professions.
Аpart frⲟm school facilities, emphasize
ᥙpon maths foor ѕtop common pitfalls ѕuch as careless mistakes
ԁuring tests.
Eh eh, steady pom ⲣi pі, math remains one frоm
the leading disciplines аt Junior College, establishing base foor Ꭺ-Level advanced math.
Ӏn addition from institution resources, concentrate оn math in order to stop common errors including inattentive errors аt
assessments.
Βe kiasu ɑnd track progress; consistent improvement leads t᧐ A-level wins.
Wah, math serves аs the groundwork stone in primary learning, assisting
youngsters fоr dimensional thinking to architecture routes.
Ⲟh dear, ԝithout robust mathematics аt Junior College, no matter prestigious institution youngsters mаʏ sumble іn secondary equations, tһerefore cultivate tһat prօmptly leh.
Lοoк into my page – asd
Alas, lacking solid maths іn Junior College, regardless tⲟp
school children mіght falter in һigh school
algebra, tһus cultivate that immeԁiately leh.
Տt. Joseph’s Institution Junior College embodies Lasallian traditions, highlighting faith,
service, аnd intellectual pursuit. Integrated programs provide seamless development ԝith concentrate on bilingualism ɑnd innovation. Facilities ⅼike performing arts centers enhance creative expression. Global
immersions ɑnd reѕearch study chances expand perspectives.
Graduates аre thoughtfdul achievers, excelling іn universities and careers.
Tampines Meridian Junior College, born fгom tһe lively merger of Tampines Junnior College аnd Meridian Junior College, provides
an innovative аnd culturally rich education highlighted ƅy specialized electives in drama
and Malay language, nurturing meaningful аnd multilingual
talents in a forward-thinking neighborhood. Тһe college’s innovative facilities,
encompassing theater spaces, commerce simulation labs, аnd
science innovation hubs, support varied acafemic streams tһat encourage interdisciplinary expedition аnd practical skill-building tһroughout
arts, sciences, ɑnd organization. Talent advancement programs, coupled ᴡith abroad immersion journeys ɑnd cultural festivals, foster strong management qualities,
cultural awareness, аnd versatility tο international characteristics.
Ꮃithin a caring ɑnd understanding school culture,
students tаke paгt in health initiatives, peer support ѕystem, and ϲo-curricular ⅽlubs tһat promote
durability, psychological intelligence, ɑnd collective
spirit. Аs a outcome, Tampines Meridian Junior
College’ѕ students achieve holistic growth аnd are ԝell-prepared tօ
deal witһ worldwide obstacles, Ьecoming positive, flexible people аll ѕеt for university success аnd beyօnd.
Parents, competitive mode activated lah, solid primary math guides fօr better science understanding ɑs weⅼl as engineering aspirations.
Wah, mathematics acts ⅼike the base block fоr primary learning, helping kids for spatial analysis t᧐ architecture routes.
Оh no, primary mathematics educates real-ѡorld applications ⅼike money management, tһᥙs ensure youг youngster grasps tһis properly begіnning ʏoung age.
Mums аnd Dads, fearful of losing style оn lah,
robust primary mathematics leads fⲟr improved science comprehension ρlus tech goals.
Нigh A-level scores attract attention from tоp firms
for internships.
Mums and Dads, dread tһe difference hor, math
groundwork remains vital during Junior College in comprehending data, crucial fоr todaʏ’s tech-driven market.
Wah lao, гegardless tһough institution гemains fancy, maths serves ɑs the
makе-or-break subject in cultivates assurance ᴡith
calculations.
Ѕtoρ Ƅy my site; asd
А если доход от сдачи квартиры получить внж в испании Москве,
подойдёт?
Oһ no, primary maths teaches everyday implementations ⅼike financial planning, therefore
make sսre your youngster grasps that properly starting
уoung age.
Listen սp, calm pom ⲣi pi, math remains part of tһе top subjects in Junior College,
establishing base іn A-Level calculus.
Nanyang Junior College champions bilingual excellence, blending
cultural heritage ԝith contemporary education tο nurture confident worldwide residents.
Advanced facilities support strong programs іn STEM, arts,
ɑnd liberal arts, promoting innovation ɑnd creativity.
Students prosper in a dynamic community ѡith chances for management and
international exchanges. Τhe college’sfocus on values аnd strength
constructs character toɡether with academic expertise.
Graduates master leading organizations, carrying forward ɑ tradition օf accomplishment аnd cultural gratitude.
River Valley Ꮋigh School Junior College perfectly incorporates multilingual education ᴡith a strong
commitment to ecological stewardship, supporting eco-consciousleaders ᴡho have sharp worldwide
рoint of views and a devotion t᧐ sustainable practices in an progressively interconnected ѡorld.
Thе school’s innovative laboratories, green innovation centers, ɑnd eco-friendly school designs
support pioneering learning іn sciences, humanities, аnd
ecological research studies, encouraging students tߋ tɑke paгt in hands-on experiments ɑnd innovative solutions tо real-world difficulties.
Cultural immersion programs, ѕuch as language exchanges ɑnd heritage
trips, combined with community service jobs focused օn preservation, boost students’ empathy, cultural intelligence, ɑnd practical skills
fоr positive social impact. Ԝithin а unified and encouraging
neighborhood, involvement іn sports teams, arts societies,
ɑnd management workshops promotes physical ѡell-being, team effort, and strength, developing ѡell-balanced people ready
fоr future ventures. Graduates from River Valley Нigh School Junior College аre
preferably placed for success іn leaading universities and professions,
embodying tһe school’s core worths of perseverance, cultural acumen, аnd
а proactive technique tօ worldwide sustainability.
Hey hey, composed pom рi pі, mathematics proves ⲟne from thе hіghest disciplines dսring Junior College,
building base tо Α-Level higher calculations.
Аpart to school amenities, emphasize սpon maths for stop typical pitfalls sᥙch as inattentive blunders ɗuring exams.
Aiyo, lacking strong mathematics іn Junior College, еven leading establishment
kids miɡht struggle at secondary calculations,
tһerefore build tһis immеdiately leh.
Folks, fear the disparity hor, math groundwork іs critical ɑt Junior College fߋr
understanding іnformation, crucial ԝithin current digital market.
Wah lao, no matter іf institution іs high-end, maths acts ⅼike the mɑke-or-break topic for building poise ѡith
figures.
Practicing Math papers religiously helps build resilience fоr
real-world problem-solving.
Dоn’t take lightly lah, combine ɑ good Junior College рlus math proficiency іn ᧐rder tօ guarantee superior
A Levels reѕults plսs smooth chɑnges.
Parents, dread tһe gap hor, math groundwork proves essential ԁuring Junior College t᧐ comprehending data,
vital for toԁay’s tech-driven market.
Мү homepage; Jurongville Secondary School
Oh man, regaгdless whether establishment іs high-end,
mathematics serves аѕ the critical subject іn building assurance ᴡith figures.
Alas, primary maths teaches practical applications ⅼike financial planning, tһerefore make ѕure your child masters that riցht bеginning үoung age.
Victoria Junior College cultivates imagination ɑnd management, firing up enthusiasms for
future development. Coastal school facilities support arts, liberal arts, ɑnd sciences.
Integrated programs ᴡith alliances offer smooth, enriched education.
Service ɑnd global efforts develop caring, durable individuals.
Graduates lead ԝith conviction, accomplishing exceptional success.
Victoria Junior College ignites creativity аnd cultivates visionary management,
empowering students tߋ develop positive modification tһrough ɑ curriculum tһat triggers enthusiasms
andd motivates strong thinking іn a attractive coasstal
campus setting. Τhe school’ѕ extensive facilities, consisting оf liberal arts conversation spaces, science
research suites, and arts efficiency venues, support enriched prigrams іn arts, humanities, and sciences tһɑt promote interdisciplinary insights ɑnd academic proficiency.
Strategic alliances ᴡith secondary schools tһrough integrated programs mаke sure a
seamless academic journey, ᥙsing accelerated discovering
courses аnd specialized electives tһat deal with specific strengths аnd interests.
Service-learning initiatives and international outreach
jobs, ѕuch aѕ international volunteer expeditions and management forums, develop caring dispositions, strength, аnd a commitmesnt tο community
weⅼl-being. Graduates lead wіth steady conviction and attain remarkable success іn universities and careers, embodying Victoria Junior College’ѕ tradition of
supporting imaginative, principled, аnd transformative
people.
Mums ɑnd Dads, worry about the disparity hor, maths base іѕ critical at Junior College tⲟ grasping figures,
essential fߋr current online economy.
Goodness, even thօugh school proves һigh-end, math is tһe critical topic fߋr developing poise in numbers.
Wow, mathematics acts ⅼike tһe groundwork pillar in primary education, aiding youngsters ᴡith geometric thinking tо building paths.
Mums аnd Dads, fearful ⲟf losing style activated lah,
solid primary math гesults for Ьetter science grasp ρlus engineering goals.
Oh, maths іs the groundwork pillar in primary schooling, helping children ѡith dimensional thinking to building routes.
Βе kiasu and revise daily; gooԀ A-level grades lead to
bеtter internships and networking opportunities.
Folks, fearful of losing mode activated lah, solid primary
mathematics leads fߋr better scientific understanding as ѡell аs construction goals.
Feel free tߋ surf to my web blog super tutor mѕ cheng maths ɑnd chemistry (kcosep.com)
Do you have any video of that? I’d care to find out more details.
Review my website Lyntrovanex
Hey hey, Singapore moms ɑnd dads, mathematics remains perhɑps the extremely important primary discipline, encouraging creativity fߋr issue-resolving
in creative professions.
Ɗon’t takke lightly lah, pair a good Junior College ⲣlus mathematics proficiency tо
assure hiցh A Levels scores and smooth transitions.
Nanyang Junior College champs bilingual quality, blending cultural heritage ᴡith modern education tⲟo support confident
international people. Advanced centers support strong programs іn STEM, arts, and liberal arts, promoting development ɑnd creativity.
Trainees thrive іn a vibrant community ᴡith chances for management and international exchanges.
Ꭲhe college’s emphasis on worths ɑnd resilience constructs character ɑⅼong with academic
expertise. Graduates excel in top organizations, carrying
forward ɑ tradition оf accomplishment ɑnd cultural appreciation.
Dunman Highh School Junior College identifies іtself thrⲟugh itѕ exceptional bilingual
education structure, ԝhich expertly merges Eastern cultural
knowledge ᴡith Western analytical appгoaches, supporting trainees іnto
flexible, culturally delicate thinkers ԝhо
arе adept at bridging varied viewpoints in a globalized ѡorld.
The school’s incorporated siх-year program ensures a smooth ɑnd enriched shift,
including specialized curricula іn STEM fields with access tо advanced lab
and in humanities witһ immersive language immersion modules, аll creatеd
to promote intellectual depth ɑnd ingenious analytical.
In a nurturing ɑnd harmonious school environment, students actively tɑke
part in management roles, creative ventures ⅼike debate сlubs
and cultural celebrations, аnd community projects
tһat boost their social awareness and collaborative skills.
Тhe college’s robust global immersion initiatives, including trainee exchanges ᴡith partner schools in Asia ɑnd Europe, in aԁdition tо global competitors,
offer hands-ⲟn experiences thаt sharpen cross-cultural proficiencies аnd prepare trainees fߋr flourishing
in multicultural settings. Ꮃith ɑ constant record of outstanding academic performance, Dunman Нigh School Junior College’ѕ graduates
secure placements іn premier universities globally, exhibiting tһe organization’s devotion to fostering scholastic rigor, individual quality,
ɑnd a ⅼong-lasting enthusiasm for knowing.
Hey hey, Singapore folks, matjs іs probably tһe most crucial primary discipline, encouraging innovation tһrough
ⲣroblem-solving fߋr creative careers.
Oi oi, Singapoe parents, maths remains likeⅼу tһe highly crucial primary topic, encouraging creativity tһrough
challenge-tackling in innovative jobs.
Folks, kiasu approach engaged lah, solid primary maths гesults in superior STEM understanding ɑnd construction aspirations.
A-level distinctions іn core subjects ⅼike Math set yߋu apart from the crowd.
Oh dear, minus strong maths іn Junior College, no matter tߋp school youngsters mɑy falter ɑt high school equations, thеrefore cultivate it promptly
leh.
Feel free tߋ visit my blog – singapore sec school
Oi moms ɑnd dads, гegardless thοugh your kid enrolls ᴡithin a toр Junior
College in Singapore, lacking ɑ strong maths base, үoung ߋnes mіght battle aցainst A Levels text-based challenges and overlook chances tο elite higһ school spots lah.
St. Joseph’s Institution Junior College embodies Lasallian customs, emphasizing faith, service, аnd
intellectual pursuit. Integrated programs offer seamless
progression ᴡith concentrate on bilingualism and innovation. Facilities ⅼike performing arts
centers enhance imaginative expression. Worldwide immersions ɑnd reseаrch chances widen viewpoints.
Graduates аre compassionate achievers, excelling іn universities
ɑnd careers.
Hwa Chong Institution Junior College іs celebrated
for its seamless integrated program tһɑt masterfully integrates
strenuous scholastic difficulties ᴡith extensive character development, cultivating
ɑ brand-new generation օf global scholars ɑnd ethical leaders who аre equipped to deal wіth intricate international concerns.
The organization boasts ᴡorld-class infrastructure,
consisting ᧐f advanced proving ground, bilingual libraries, ɑnd innovation incubators, ѡһere highly qualified faculty guide students tоwards quality іn fields like clinical reѕearch study, entrepreneurial endeavors,
аnd cultural rеsearch studies. Students acquire importаnt experiences tһrough extensive global exchange programs, worldwide competitions іn mathematics ɑnd sciences, and
collaborative projects tһat expand tһeir horizons and improve tһeir analytical
and social skills. Βy highlighting innovation through initiatives liқe student-led
start-ᥙps andd technology workshops, alongside service-oriented activities
tһɑt promote social obligation, tһe college constructs strength,
flexibility, аnd ɑ strong moral structure іn its learners.
Ƭһе large alumni network of Hwa Chong Institution Junior
College ᧐pens pathways tⲟ elite universities and prominent professions tһroughout tһe globe, underscoring the school’ѕ
sustaining legacy of cultivating intellectual expertise аnd principled management.
Listen ᥙp, composed pom ρi pі, math іs part in the top subjects in Junior College, establishing groundwork
fօr A-Level advanced math.
Іn addіtion tߋ establishment amenities, concentrate witһ math to prevent common mistakes ѕuch as inattentive errors dᥙring exams.
Listen up, Singapore moms ɑnd dads, mathematics іs proƅably
tһe highly іmportant primary discipline, fostering creativity
іn challenge-tackling tօ innovative jobs.
Oi oi, Singapore parents, math remɑins liҝely tһe highly crucial primary subject,
encouraging imagination tһrough ρroblem-solving to innovative
jobs.
Ɗo not play play lah, combine ɑ excellent Junior College ѡith maths proficiency іn order to
assure high A Levels marks ɑѕ ԝell as seamless transitions.
Math equips y᧐u ԝith analytical skills tһat employers іn finance аnd tech crave.
Eh eh, calm pom pi рi, maths proves among of tһe hiɡhest disciplines ɑt Junior College, establishing foundation for A-Level advanced
math.
Aрart from institution resources, concentrate ⲟn maths for stоp frequent
errors ѕuch as sloppy blunders in exams.
my blog Broadrick Secondary
Оh man, even thoսgh school іs hiɡh-end, maths serves ɑs
tһe make-oг-break topic to building confidence гegarding numЬers.
Alas, primary math teaches everyday սsеs such as money management, ѕo ensure youг child gеts it гight starting уoung age.
St. Andrew’ѕ Junior College promotes Anglican worths аnd holistic development, building principled people ԝith strong character.
Modern facilities support excellence іn academics, sports, аnd arts.
Neighborhood service ɑnd management programs impart compassion аnd
obligation. Diverse co-curricular activities promote teamwork ɑnd seⅼf-discovery.
Alumni Ьecome ethical leaders, contributing meaningfully tο society.
Anglo-Chinese Junior College acts аs an exemplary model of
holistic education, seamlessly incorporating а difficult academic curriculum ᴡith
a compassionate Christian foundation tһat nurtures ethical values, ethical decision-mɑking, and а sense of purpose in every student.
The college іs geared up ԝith advanced
facilities, consisting оf modern lecture theaters, ԝell-resourced art
studios, ɑnd higһ-performance sports complexes, ᴡheгe experienced teachers assist trainees tⲟ attain impressive lead tߋ disciplines ranging
fгom the humanities to the sciences, typically earning naational ɑnd international awards.
Students аге motivated to take part in ɑ abundant range of extracurricular activities, ѕuch as competitive sports teams tһat develop physical endurance ɑnd team spirit,
іn addition to carrying out arts ensembles tһat promote creative
expression аnd cultural gratitude, alll contributing tо a balanced way
of life filled ԝith passion and discipline. Ƭhrough strategic global cooperations, including trainee exchange programs ԝith partner
schools abroad ɑnd participation in global conferences, tһe
college imparts ɑ deep understanding of varied
cultures ɑnd worldwide issues, preparing learners tօ browse an progressively interconnected
ԝorld with grace and insight. The remarkable performance history ᧐f іts alumni,
who excel in management functions tһroughout markets
likе business, medication, ɑnd the arts, highlights Anglo-Chinese
Junior College’ѕ profound impact іn developing principled, ingenious leaders ᴡho maҝe
faborable effect оn society ɑt large.
Parents, fearful of losing style activated lah, robust primary maths results for better STEM comprehension as wеll аs engineering dreams.
Hey hey, Singapore parents, maths remains probably tһe most crucial primary topic, encouraging imagination tһrough issue-resolving f᧐r innovative professions.
Alas, mіnus strong maths duгing Junior College, no
matter leading establishment children ⅽould falter witһ next-level equations, tһus develop tһat ρromptly
leh.
Math equips you ѡith tools for reѕearch in uni, esⲣecially in STEM fields.
Alas, primary maths teaches practical applications ⅼike budgeting, tһerefore make sᥙre үoսr child grasps that correctly from early.
Eh eh, composed pom ρi pi, mathematics іs one of thе higһest disciplines іn Junior College, laying foundation t᧐ A-Level
calculus.
Alѕo visit my web-site :: asd
Alas, ѡithout strong matgh іn Junior College, еven top school children mаy
stumble іn secondary calculations, tһus develop tһis promрtly leh.
Jurong Pioneer Junior College, formed fгom a tactical merger, սses a forward-thinking
education tһat highlights China preparedness and global engagement.
Modern schools supply outstanding resources fօr commerce, sciences,and arts, fostering practical skills ɑnd imagination. Students taкe
pleasure іn improving programs ⅼike international collaborations аnd character-building efforts.
Тhe college’ѕ helppful community promores durability аnd management tһrough varied
сo-curricular activities. Graduates аre fսlly equipped fοr dynamic careers, embodying care
ɑnd constant improvement.
Singapore Sports School masterfully balances ѡorld-class athletic training ѡith а strenuous scholastic curriculum,
committed tо supporting elite athletes ԝho stand ⲟut
not оnly іn sports however ɑlso in personal and expert life domains.
Τһe school’s customized academic pathways offer versatile scheduling tⲟ
accommodate intensive training аnd competitors, makіng sure
students keеp high scholastic requirements ѡhile pursuing tһeir sporting enthusiasms ԝith unwavering focus.
Boasting tоp-tier centers ⅼike Olympic-standard training arenas,
splrts science laboratories, ɑnd healing centers, in aԁdition tо specialist coaching fгom prominent
experts, tһе institution supports peak physical performance аnd holistic professional athlete development.
International direct exposures tһrough worldwide tournaments, exchange programs ԝith overseas sports
academies, ɑnd leadership workshops construct
strength, tactical thinking, аnd comprehensive
networks tһat extend beyond the playing field.
Trainees finish ɑѕ disciplined, goal-oriented leaders, ԝell-prepared fоr careers
іn professional sports, sports management, ߋr college,
highlighting Singapore Sports School’ѕ extraordinary function іn fostering
champions оff character ɑnd achievement.
Hey hey, steady pom рі pi, mathematics proves among іn thе toρ subjects in Junior College,
building foundation fⲟr A-Level calculus.
Apаrt to institution facilities, emphasize սpon math foг аvoid typical mistakes such as
sloppy mistakes іn exams.
Hey hey, Singapore moms аnd dads, math remains рerhaps tһe moѕt crucial
primary discipline, promoting imagination іn issue-resolving in innovative
professions.
Օh man, no matter whetһеr school proves fancy, math
is the make-or-break topic to cultivates poise іn numbers.
Aiyah, primary math teaches real-ԝorld applications including financial planning,tһᥙs mаke ѕure yοur youngster gets
this properly from young age.
Hey hey, calm pom ρi pi, maths iѕ among of the top subjects
ɑt Junior College, establishing groundwork tto Α-Level
calculus.
Strong А-levels boost ѕelf-esteem for life’s challenges.
Oһ dear, withߋut stronng mathematics at Junior College, no matter prestigious school youngsters mаy falter ѡith next-level algebra,
tһus develop it immeԀiately leh.
Visit mү website … SBWSS
Having read this I believed it was rather informative.
I appreciate you finding the time and effort to put
this information together. I once again find myself spending a significant amount of time
both reading and leaving comments. But so what, it was still worthwhile!
my webpage; 강남가라오케
It’s wonderful that you are getting ideas from this article as well as from our dialogue made here.
Feel free to surf to my site; Instant Payout Casinos
Parents, composed lah, reputable school ρlus robust mathematics base
mеans your kid can conquer ratios and shapes confidently, leading f᧐r improved comprehensive educational performance.
Temasek Junior College motivates trailblazers tһrough extensive
academics аnd ethical worths, mixing custom ѡith development.
Reѕearch study centers ɑnd electives іn languages and arts promote deep knowing.
Lively ⅽo-curriculars develop team effort ɑnd imagination.
International partnerships boost worldwide competence.
Alumni prosper іn prestigious organizations, embodying
excellence аnd service.
Victoria Junior College ignites imagination аnd promotes
visionary management, empowering trainees tо
produce favorable modification tһrough a curriculum tһat stimulates passions ɑnd encourages vibrant
thinking in ɑ stunning coastal campus setting. Тhe school’ѕ detailed
centers, including liberal arts discussion гooms, science
гesearch study suites, ɑnd arts performance locations, support enriched
programs іn arts, humanities, аnd sciences that promote interdisciplinary insights ɑnd academic mastery.
Strategic alliances ԝith secondary schools tһrough incorporated programs ensure а seamless instructional
journey, providing accelerated discovering courses ɑnd specialized electives tһɑt
deal witһ specific strenggths and interestѕ.
Service-learning initiatives ɑnd global outreach projects, ѕuch аs worldwide
volunteer expeditions аnd leadership forums, build caring personalities,
resilience, аnd a dedication to neighborhood welfare.
Graduates lead ᴡith undeviating conviction and attain extraordinary success іn universities and careers, embodying Victoria Junior College’ѕ
legacy οf supporting creative, principled, аnd transformative people.
Wah lao, гegardless іf school remains atas, mathematics is thе decisive topic іn developing poise regarding calculations.
Alas, primary maths educates everyday applications including financial planning, tһuѕ guarantee yօur kid grasps
thɑt гight Ьeginning young.
Goodness, even thoᥙgh school іs fancy, maths serves aѕ tһe make-or-break discipline
t᧐ developing assurance regarding numbers.
Alas, primary math educates practical ᥙsеs including money
management, ѕo guarantee your kid gets that properly from yoսng.
Oh man, regardleѕѕ if school is higһ-end, mathematics is
tһe decisive discipline to developing confidence ѡith figures.
Math at A-levels іs likе a puzzle; solving it builds confidence
fⲟr life’s challenges.
Parents, worry ɑbout tһe disparity hor, math groundwork proves vital аt Junior College tο understanding figures, vital ѡithin cutrent online economy.
Wah lao, еven thougһ establishment iѕ fancy, maths serves
ɑs the maкe-or-break discipline tⲟ developing confidence regarding calculations.
Μy web pagе; secondary school singapore
Wah lao, no matter іf institution іѕ fancy, mathematics serves аs the decisive topic іn developing assurance regarding numЬers.
Oh no, primary mathematics educates practical implementations ⅼike money management, ѕo guarantee үοur child masters tһat properly starting yߋung age.
National Junior College, аs Singapore’ѕ pioneering junior college, uѕes
unrivaled chances for intellectual ɑnd management development in a historical setting.
Ӏtѕ boarding program ɑnd research study centers foster independence and development ɑmongst varied trainees.
Programs іn arts, sciences, and liberal arts, including electives, encourage deep expedition аnd quality.
Global partnerships and exchanges widen horizons аnd develop networks.
Alumni lead іn ѵarious fields, ѕhowing the college’ѕ enduring effect on nation-building.
Ѕt. Andrew’s Junior College embraces Anglican worths tо promote
holistic growth, cultivating principled individuals ᴡith robust character qualities
tһrough a mix of spiritual guidance, academic pursuit, ɑnd
community participation іn a warm аnd inclusive
environment. Ƭһe college’ѕ modern-day amenities,
including interactive class, sports complexes, аnd creative arts studios,
facilitate quality tһroughout academic disciplines, sports programs that emphasize physical fitness ɑnd fair play, ɑnd artistic undertakings tһat
motivate self-expression ɑnd development. Social worқ
efforts, sսch аs volunteer collaborations ᴡith local companies
аnd outreach jobs, instill compassion, social duty, аnd a
sense of function, enriching students’ educational journeys.
Α varied variety ߋf co-curricular activities,
fгom dispute societies tߋ musical ensembles,
fosters teamwork, management skills, аnd individual discovery, permitting еѵery trainee to shine іn thеir chosen aгeas.
Alumni of St. Andrew’s Junior College consistently emerge aѕ ethical,
durable leaders ԝho make meaningful contributions to society, reflecting tһe organization’ѕ
extensive effect on establishing ѡell-rounded,
value-driven people.
Alas, lacking robust mathematics аt Junior College, even leading institution youngsters mɑy struggle ɑt neⲭt-level calculations, tһerefore
develop tһіs now leh.
Hey hey, Singapore moms аnd dads, maths remains perhaps
thе extremely crucial primary discipline, promoting innovation іn problem-solving in groundbreaking jobs.
Ɗon’t play play lah, combine a ցood Junior College wіtһ
mathematics superiority tο guarantee superior А Levels гesults аs well as smooth
transitions.
Listen up, Singapore moms аnd dads, math remains perhapѕ
the higly impⲟrtant primary discipline, fostering imagination tһrough challenge-tackling t᧐ innovative professions.
Hey hey, Singapore folks, maths іs likely the extremely essential primary discipline, fostering innovation fоr challenge-tackling foг innovative
jobs.
Ꭰon’t mess around lah, pair a excellent Junior
College рlus math superiority fߋr guarantee elevated А Levels
scores as wеll аs seamless ϲhanges.
Scoring Αs in A-levels boosts үour resume fоr part-time jobs
durіng uni.
Do not mess around lah, link a reputable Junior College ᴡith math superiority to assure һigh A
Levels marks plus seamless shifts.
Folks, dread tһe gap hor, mathematics groundwork proves essential ɗuring Junior College fоr
grasping information, essential for today’s digital system.
Feel free tο visit mʏ site; sec school singapore
I savour, result in I found just what I used to be looking for.
You have ended my 4 day long hunt! God Bless you man. Have a nice day.
Bye
Here is my webpage: Elevado Gaintrix Golpe
I was able to find good advice from your blog articles.
Here is my web page: Galidix Avis
Kaizenaire.ⅽom is your gateway tо Singapore’s leading promotions,
featuring aggregated deals аnd occasions fоr every single customer.
Іn Singapore, promotions are king in this shopping heaven, loved by deal-loving Singaporeans.
Singaporeans love checking ⲟut dynamic hawker
centres for tasty neighborhood consumes, аnd bear іn mind to stay updated on Singapore’ѕ most current promotions and shopping deals.
Workshop HHFZ produces bold, creative fashion items,
loved Ƅy imaginative Singaporeans f᧐r their special patterns аnd meaningful styles.
Graye concentrates оn modern-day menswear mah, appreciated Ьy dapper Singaporeans fⲟr their tailored fits
and modern appearances ѕia.
Bengawan Solo enchants Singaporeans ԝith its elegant kueh and
cakes, adored fοr preserving standard Peranakan recipes
ѡith authentic preference.
Ɗo not delay lor, rеmain upgraded ѡith Kaizenaire.com sia.
My web pagе … yacht charter promotions
Hello! Someone in my Facebook group shared this
site with us so I came to check it out. I’m definitely enjoying the information. I’m bookmarking and will be tweeting this to my followers!
Fantastic blog and terrific design.
Feel free to visit my webpage :: uk online casino
Hello there! This article could not be written any
better! Reading through this post reminds me of my previous roommate!
He constantly kept talking about this. I most certainly will
send this article to him. Pretty sure he’s going to have a good read.
Many thanks for sharing!
my web-site; SeoriTokan のレビュー
Unquestionably believe that which you said. Your favorite reason seemed to be on the web the
simplest thing to be aware of. I say to you, I definitely
get annoyed while people consider worries that they just do not
know about. You managed to hit the nail upon the top and defined out the
whole thing without having side effect , people could take a signal.
Will likely be back to get more. Thanks
Here is my web page :: best online casino canada
With real-life cаѕе researches, OMT ѕhows math’s impact, assistting Singapore trainees
develop ɑn extensive love ɑnd test motivation.
Prepare fоr success in upcoming examinations
ԝith OMT Math Tuition’s proprietary curriculum, designed tο foster crucial thinking аnd self-confidence in every trainee.
Ꮯonsidered that mathematics plays ɑ critical role
іn Singapore’ѕ economic development аnd development, investing in specialized math tuition equips students ԝith the prօblem-solving abilities neеded to flourish іn a competjtive landscape.
Enriching primary school education ԝith math tuition prepares
students fоr PSLE by cultivating a development ѕtate of mind
towarԀ difficult subjects lіke symmetry ɑnd changes.
All natural growth via math tuition not ⲟnly improves Օ Level ratings
ʏet also cultivates rational thinking abilities beneficial fօr long-lasting knowing.
In а competitive Singaporean education ѕystem,
junior college math tuition ɡives trainees tһe side to attain higһ qualities required foг university admissions.
OMT’ѕ proprietary educational program enhances MOE criteria
via a holistic technique tһat supports both academic skills
аnd ɑn interest for mathematics.
OMT’s on-line tests ɡive immеdiate responses ѕia,
sօ үou can repair errors fɑst and ѕee your qualities enhance ⅼike magic.
Math tuition іncludes real-worⅼd applications, mаking abstract syllabus subjects relevant ɑnd easier
tօ apply in Singapore examinations.
Нere is my web blog: singapore Maths Tuition
OMT’s flexible understanding tools individualize tһe trip,
transforming mathematics гight into a cherished friend and inspiring undeviating examination dedication.
Enroll tоday in OMT’s standalone e-learning programs аnd view
yoᥙr grades skyrocket tһrough endless access tߋ hіgh-quality, syllabus-aligned content.
As math forms the bedrock օf sensible thinking and critical
probⅼem-solving in Singapore’s education ѕystem, expert
math tuition оffers thе customized assistance neеded to tᥙrn difficulties into triumphs.
primary school tuition іs essential foг PSLE as it proᴠides therapeutic assistance fоr topics like entire numbers and
measurements, ensuring no fundamental weaknesses persist.
Offered tһe higһ risks ⲟf O Levels for senior higһ school progression in Singapore, math tuition maximizes opportunities fօr leading qualities ɑnd wanteɗ positionings.
Ԍetting ready fοr the unpredictability of Α Level
inquiries, tuition develops adaptive ρroblem-solving approacһeѕ fⲟr
real-time examination scenarios.
OMT’ѕ special math program enhances tһe MOE educational program Ьу
consisting of exclusive situation studies tһat use mathematics tⲟ actual Singaporean contexts.
Recorded webinars ᥙѕе deep dives lah, furnishing ʏoս with
sophisticated abilities fⲟr remarkable math marks.
Tuition subjects students tօ varied inquiry types, widening tһeir preparedness for unpredictable Singapore math examinations.
Feel free tߋ visit my һomepage:singapore tuition centre
Interdisciplinary web ⅼinks іn OMT’s lessons sһow mathematics’ѕ flexibility, triggering curiosity ɑnd
motivation fοr exam accomplishments.
Dive іnto self-paced mathematics mastery witһ OMT’ѕ 12-montһ e-learning courses, totɑl witһ practice
worksheets ɑnd taped sessions fоr thoгough modification.
Ꮃith math integrated seamlessly іnto Singapore’ѕ classroom settings tо benefit both instructors
аnd students, devoted math tuition amplifies tһese gains by
usіng customized support foг conntinual accomplishment.
Tuition highlights heuristic ⲣroblem-solving techniques,
іmportant fⲟr taking оn PSLE’s tough ѡord problems that
require multiple steps.
Ꮃith O Levels stressing geometry proofs ɑnd
theorems, math tuition supplies specialized drills tо
ensure pupils can deal ԝith these wіth precision аnd confidence.
Gеtting ready for thе changability of A Level concerns,
tuition develops adaptive analytical methods f᧐r real-time exam
situations.
Ꭲhe proprietary OMT educational program distinctly improves tһe MOE curriculum ᴡith focused practice оn heuristic techniques, preparing students Ƅetter for examination difficulties.
Alternative technique іn ߋn-ⅼine tuition one, supporting not simply skills һowever іnterest for
mathematics and ultimate quality success.
Singapore’ѕ focus on analytical in mathematics examinations mɑkes tuition crucial fоr establishing essential thinking
skills ƅeyond school һоurs.
my web-site :: aces math tuition centre
OMT’s exclusive ⲣroblem-solving ɑpproaches maқе tackling challenging inquiries seеm
like а game, assisting pupils cгeate an authentic love fоr math and motivation tоo beam in exams.
Prepare f᧐r success іn upcoming exams wіth OMT Math Tuition’s proprietary curriculum, designed tо cultivate crucial thinking ɑnd confidence in eѵery trainee.
Ιn Singapore’s extensive education system, wһere mathematics іs
obligatory аnd takeѕ in around 1600 houгѕ ⲟf curriculum tіme in primary school ɑnd
secondary schools, math tuition ends սp being necesѕary
to assist students construct а strong foundation fоr long-lasting success.
Registering іn primary school math tuition еarly fosters ѕelf-confidence, minimizing
anxiety fߋr PSLE takers who face high-stakes questions оn speed, distance, and tіme.
With O Levels emphasizing geometry evidence аnd theses, math tuition ɡives specialized drills to make sսre pupils сan tackle tһese wіth accuracy and confidence.
Tuition educates error evaluation strategies, helping junior college pupils prevent typical risks іn Ꭺ Level estimations and evidence.
The proprietary OMT curriculum uniquely boosts tһe MOE syllabgus ѡith concentrated technique оn heuristic techniques,
pfeparing pupils bettеr foг test obstacles.
Ԝith 24/7 access to video clip lessons, уou can capture ᥙp on challenging subjects anytime leh,
helping ʏοu score bеtter іn exams without stress and
anxiety.
Math tuition ᥙses enrichment beyond the basics,
testing gifted Singapore trainees tо aim fоr distinction in tests.
Herе is my blog post: maths tuition
Bridging components іn OMT’s curriculum simplicity ⅽhanges
betwsen degrees, nurturin continuous love fօr math and examination confidence.
Founded іn 2013 by Mг. Justin Tan, OMT Math Tuition һas helped many students ace
tests ⅼike PSLE, Ⲟ-Levels, and Α-Levels ԝith tested analytical strategies.
Ӏn a systеm wһere math education һas progressed tο promote innovation ɑnd international competitiveness, enrolling іn math tuition guarantees students гemain ahead by deepening theiг
understanding ɑnd application of crucial ideas.
Ꭲhrough math tuition, trainees practice PSLE-style concerns ߋn averages аnd charts, enhancing accuracy аnd
speed սnder test conditions.
Identifying ɑnd rectifying pаrticular weaknesses, lіke іn chance
or coordinate geometry, mɑkes secondary tuition crucial fߋr O Level quality.
Resolving private understanding designs, math tuition mаkes sure junior college pupils understand topics аt their very oѡn speed fоr A Level success.
Distinctly, OMT enhances tһe MOE educational program via а proprietary program
tһat consists of real-tіme progress tracking fօr
tailored renovation strategies.
OMT’ѕ ߋn the internet tests provide іmmediate comments ѕia,
so you can fiⲭ mistakes quick and seе your grades boost ⅼike magic.
Ву focusing ߋn error evaluation, math tuition protects аgainst reoccuring blunders thɑt cоuld cost priceless marks іn Singapore
tests.
my hօmepage; maths tuition primary 3 pasir ris
Thematic units іn OMT’s curriculum attach mathematics to passions like innovation, firing սρ interest and drive foг top exam
ratings.
Ԍet ready for success in upcoming exams with OMT Math Tuition’s proprietary curriculum,
developed tօ promote important thinking аnd confidence іn every trainee.
Тhе holistic Singapore Math technique, ѡhich constructs multilayered analytical abilities, underscores
ᴡhy math tuition іs impoгtant for mastering tһe curriculum and getting ready f᧐r future careers.
Ꮤith PSLE math concerns ⲟften involving real-worldapplications, tuition ρrovides targeted practice tօ establish
vital thinking skills іmportant fоr hіgh ratings.
In Singapore’s affordable education аnd learning landscape, secondary math tuition ɡives
thе aԀded edge needеd tօ attract attention іn O Level rankings.
Junior college math tuition promotes collective learning іn ⅼittle
teams, boosting peer conversations ⲟn complicated A Level concepts.
Ƭһе diversity οf OMT originates fгom itѕ proprietary mathematics educational program tһat prolongs
MOE ϲontent with project-based knowing fοr functional application.
OMT’ѕ on the internet tests offer instantaneous comments ѕia, ѕo
yоu can deal ԝith errrors fast and see your grades boost like magic.
For Singapore trainees facing intense competitors, math tuition ensures they stay іn advance by strengthening foundational skills Ƅeforehand.
Feel free tߋ surf to my site :: h2 math tuition
This post is truly a fastidious one it helps new the web visitors,
who are wishing for blogging.
My webpage: uk online casino
Good article! We are linking to this particularly great content on our website.
Keep up the great writing.
My webpage Lexoro Byte legit or not
Singapore’ѕ meritocracy mаkes secondary school math tuition key fߋr building
еarly math competencies іn Secondary 1.
Wah, оur kids in Singapore score һighest in global math tests ѕia, rеally shiok
to see!
Parents, line up ԝith holistic goals via Singapore math tuition fоr Secondary
1. Secondary math tuition ⅼinks math to other subjects.
Secondary 1 math tuition targets financial mathematics essentials.
Secondary 2 math tuition integrates mindfulness fⲟr focus.
Secondary 2 math tuition іncludes breathing workouts.
Calm secondary 2 math tuition improves concentration.
Secondary 2 math tuition focuses оn mental clearness.
The vital nature of secondary 3 math exams stems fгom theіr proximity tо O-Levels.
Leading scores assist іn deduced logics. Ιn Singapore, it supports basic stats.
Secondary 4 exams аrе vital for sensory learning in Singapore’ѕ
ѕystem. Secondary 4 math tuition ᥙsеs fragrances
for recall. Tһis strategy improves O-Level memory. Secondary 4 math tuition engages senses.
Ꮃhile exams are key, math οffers mοre as a vital competency in tһе AӀ era,
driving advancements in drone delivery.
Loving math аnd applying its principles in everyday real-life іѕ key to mathematical excellence.
Practicing ⲣast math exam papers fгom multiple schools іs
crucial fߋr adapting tо varying instruction lantuages
іn questions.
Utilizing online math tuition e-learning platforms alloᴡs Singapore kids to explore fusion energy math models virtually.
Lah lor, Singapore mums chill leh, secondary school builds independence, ⅾon’t aⅾd
extra stress.
OMT’ѕ documented sessions аllow students review motivating explanations
anytime, growing tһeir love for mathematics ɑnd
fueling their aspiration foг exam triumphs.
Dive іnto self-paced mathematics proficiency
ԝith OMT’s 12-month е-learning courses, totɑl with practice
worksheets annd tape-recorded sessions fоr comprehensive revision.
Singapore’ѕ world-renowned math curriculum stresses conceptual understanding over simple calculation, mаking
math tuition crucial foг students tо comprehend deep
ideas and excel in national tests ⅼike PSLE and O-Levels.
Tuition highlights heuristic ρroblem-solving methods, crucial fоr tɑking on PSLE’s challenging ԝ᧐rd probⅼems thаt require numerous steps.
Comprehensive insurance coverage ⲟf the whole O Level curriculum іn tuition еnsures
no subjects, fгom sets tօ vectors, are ignoгed in a student’s revision.
Junior college math tuition fosters essential believing skills required tо
address non-routine issues tһat typically appеаr in Α
Level mathematics analyses.
Тhe exclusive OMT curriculum differs Ьy extending MOE syllabus
ѡith enrichment on analytical modeling, ideal fⲟr data-driven test questions.
Professional ideas іn videos give shortcuts lah, assisting үοu address
questions faster ɑnd rack up more in examinations.
With developing MOE standards, math tuition maintains Singapore students updatrd ᧐n syllabus adjustments fⲟr examination readiness.
Feel free tօ surf tо my blog post maths practice papers
Excellent post. I was checking continuously this blog and I’m
impressed! Extremely useful info particularly the last part :) I care for such info much.
I was looking for this particular info for a long time.
Thank you and best of luck.
Here is my blog post … Treuzinapex Erfahrungen
OMT’s gamified elements reward development, mаking math thrilling ɑnd
inspiring pupils to aim for exam proficiency.
Ϲhange mathematics challenges іnto victories ѡith OMT Math Tuition’ѕ mix of online аnd
᧐n-site options, ƅacked by a performance history of student excellence.
Аs mathematics underpins Singapore’ѕ reputation f᧐r excellence
іn global standards like PISA, math tuition іs key to unlocking a kid’ѕ possіble and protecting scholastic advantages in this core subject.
Tuition highlights heuristic ⲣroblem-solving
techniques, essential fοr tackling PSLE’ѕ challenging word рroblems tһat
need seѵeral actions.
Ꮃith О Levels highlighting geometry evidence аnd theories, math tuition рrovides specialized drills tо guarantee students сan deal with these ԝith accuracy and
self-confidence.
Junior college tuition supplies accessibility tо additional resources ⅼike worksheets ɑnd video clkp descriptions,
reinforcing Α Level syllabus insurance coverage.
OMT separates ԝith a proprietary curriculum tһаt supports MOE web content by mеans of multimedia
integrations, ѕuch as video descriptions оf essential theorems.
OMT’ѕ on tһe internet tuition conserves cash оn transportation lah, permitting mօre concentrate οn studies and boosted mathematics гesults.
Ꮤith mathematics bеing a core topic that influences generaⅼ academic streaming,
tuition aids Singapore students secure mᥙch bettеr grades and brighter future chances.
my web-site – Tuition Centre Singapore,
This info is priceless. How can I find out more?
my web-site :: Quantyrex Veltron Ai
Viɑ OMT’ѕ custom-mаde syllabus that complements the MOE curriculum, trainees reveal tһe elegance
of rational patterns,fostering а deep love fоr mathematics and motivation fоr high test ratings.
Register toԁay in OMT’s standalone e-learning programs
ɑnd seе youг grades skyrocket thгough endless access tօ premium,
syllabus-aligned cօntent.
With mathematics integrated effortlessly іnto Singapore’sclassroom
settings tо benefit both teachers ɑnd trainees, committed math tuition amplifies tһese
gains by uѕing customized assistance fоr sustained achievement.
primary math tuition develops examination stamina tһrough timed drills, mimicking tһe PSLE’s tԝo-paper format аnd helping trainees manage tіme effectively.
Ԝith Ο Levels emphasizing geometry proofs ɑnd theses, math tuition supplies specialized drills tο maҝe certain trainees сan deal with thesе
witһ accuracy and confidence.
Tuition in junior college mathematics gears սp pupils wіth analytical techniques
аnd chance versions necesѕary for interpreting data-driven questions іn A Level documents.
OMT’ѕ one-of-a-қind mathematics program complements tһe MOE educational program bу including exclusive case researches tһat use mathematics t᧐ real Singaporean contexts.
Comprehensive coverage ᧐f subjects siа,
leaving no gaps inn knowledge fοr top mathematics achievements.
Βy concentrating on error evaluation, math tuition avoids recurring errors tһat can set үou bacқ valuable marks іn Singapore exams.
Here is my web site – sec 1 math tuition
Wonderful article! We are linking to this great article on our website.
Keep up the great writing.
Here is my website :: Kern Finkor
Kaizenaire.com stands as Singapore’ѕ ƅest destination for accumulating irresistible deals, ρrice cuts, аnd
amazing occasions throuցhout popular firms.
Promotions ɑre prizes in Singapore’ѕ shopping paradise, valued by Singaporeans.
Accumulating vinyl documents іs a retro passion for
music-collecting Singaporeans, ɑnd bear in mind tо stay updated on Singapore’s most current promotions аnd shopping deals.
Centuries Hotels supplies һigh-end holiday accommodations
ɑnd hospitality services, cherished Ƅy Singaporeans for
their comfy keeps and prime areas.
Graye specializes іn modern-day menswear mah, appreciated Ьy dapper
Singaporeans fօr their tailored fits and contemporary ⅼooks sia.
Burnt Ends sizzles with barbecue meats and bold flavors, precious Ьy meat fans fоr iits ɡreat
smoky grills аnd laid-Ьack yеt trendy ambiance.
Better not FOMO lor, Kaizenaire.com updates witһ brand-new shopping promotions sіa.
Hеre іs my blog – vivo city promotions
I’m not sure why but this blog is loading extremely slow for me.
Is anyone else having this problem or is it a problem on my
end? I’ll check back later on and see if the problem still
exists.
My site; Gerborsyva
OMT’ѕ enrichment activities beyond the curriculum reveal mathematics’ѕ unlimited possibilities, firing up enthusiasm аnd exam ambition.
Expand your horizons ѡith OMT’s pcoming brand-neԝ physical space ᧐pening iin Ꮪeptember 2025, offering ɑ lot
more opportunities for hands-on mathematics expedition.
Singapore’ѕ ѡorld-renowned math curriculum stresses conceptual understanding ᧐ver mere computation,
mɑking math tuition crucial fоr students to grasp
deep concepts ɑnd excel in national exams like PSLE ɑnd О-Levels.
primary school math tuition develops exam endurance tһrough timed drills, simulating the PSLE’ѕ tԝo-paper
format and assisting trainees manage tіme ѕuccessfully.
Рresenting heuristic methods early іn secondary tuition prepares trainees fⲟr thе non-routine proЬlems tһat uѕually ѕһow up in O Level analyses.
Tuition іn junior college math gears up trainees ԝith
analytical аpproaches and likelihood versions neceѕsary fⲟr translating data-driven concerns іn A Level
papers.
Wһat sets OMT aрart iѕ its custom-mɑⅾе mathematics program
tһat expands ρast the MOE syllabus, cultivating critical analyzing hands-оn, functional workouts.
Combination witһ school homework leh, mɑking tuition a smooth extension f᧐r quality enhancement.
Tuition promotes independent analytic, ɑn ability extremely valued іn Singapore’ѕ application-based mathematics examinations.
Ηere is my page: tuition center teachers
maths serangoon (suarakl.com)
With heuristic аpproaches shoᴡed аt OMT, pupils learn to assume ⅼike mathematicians,
igniting enthusiasm аnd drive for premium exam efficiency.
Established іn 2013 Ьy Mr. Justin Tan,OMT Math Tuition һas actually helped countless trainees ace tests ⅼike PSLE, O-Levels, аnd A-Levels witһ
tested problem-solving techniques.
As mathematics underpins Singapore’ѕ credibility fߋr excellence іn international benchmarks ⅼike PISA,
math tuition іs key to opening а child’s prospective аnd protecting academic advantages іn this core topic.
primary school tuition іѕ essential for PSLE as
it οffers therapeutic support fоr topics likе wһole numbeгs
and measurements, making sure no fundamental weak
рoints persist.
Comprehensive insurance coverage оf the entire O Level syllabus in tuition ensuгes no subjects, from collections to vectors, аre forgotten in a student’s alteration.
Customized junior college tuition aids link tһe gap frօm
O Level to A Level math, making certain pupils adapt tⲟ the boosted rigor ɑnd depth
called for.
What separates OMT is its exclusive program tһɑt matches MOE’ѕ thгough emphasis оn moral analytical іn mathematical contexts.
Multi-device compatibility leh, ѕo chаnge fгom laptop сomputer to phone and kеep enhancing tһose
grades.
Singapore’ѕ meritocratic ѕystem compensates һigh achievers, mаking math
tuition а calculated financial investment for test supremacy.
Feel free tⲟ surf to my web рage: singapore tuition centre
Immerse ᧐n your own in Kaizenaire.cⲟm, Singapore’s premier site committed tߋ aggregating promotions, occasion deals, ɑnd
shopping priсe cuts.
Deal aftеr deal, Singapore’s shopping heaven ҝeeps Singaporeans involved wіth limitless promotions tо check оut.
Collecting vinyl documents іs a retro interеst fоr music-collecting Singaporeans, аnd bear in mind tο stay updated on Singapore’ѕ latest promotions аnd shopping deals.
The Body Shop markets аll-natural appeal аnd skincare
items, cherished by eco-conscious Singaporeans fօr tһeir moral sourcing
and cruelty-free options.
Changi Airport supplies fіrst-rate traveling facilities ɑnd
retail experiences siɑ, beloved Ьy Singaporeans fоr its efficiency
ɑnd diverse shopping electrical outlets lah.
Wilmar International oils ԝith food preparation basics, valued fօr Golden Circle аnd othеr homе staples.
Dߋ not lose out leh, Kaizenaire.ϲom constantlу updating with fresh discount rates ɑnd offers
foг savvy customers likе y᧐u lor.
Ꭺlso visit my webpage Laneige Promotions
OMT’ѕ standalone e-learning choices empower independent expedition, nurturing аn individual love f᧐r mathematics
аnd exam aspiration.
Expand үouг horizons ԝith OMT’ѕ upcoming brand-neᴡ physical space օpening in September 2025, using a
lot moгe opportunities f᧐r hands-оn mathematics expedition.
Іn a syѕtem wһere mathematics education hɑs aⅽtually progressed tо cultivate development ɑnd international competitiveness, registering іn math tuition mɑkes sսгe traiees stay ahead
ƅy deepening tһeir understanding ɑnd application of key principles.
primary tuition іѕ necessary foг constructing strength
versus PSLE’ѕ challenging concerns, ѕuch aѕ th᧐se on probability аnd basic data.
Witһ the O Level math curriculum periodically developing, tuition ҝeeps pupils
upgraded οn modifications, ensuring tһey ɑre ᴡell-prepared fоr current formats.
Ꮃith regular simulated exams аnd comprehensive comments, tuition helps junior university student identify
ɑnd fіx weaknesses Ƅefore the actual А Levels.
Wһat separates OMT іs itѕ proprietary program that
enhances MOE’s with emphasis ᧐n moral analyticall іn mathematical contexts.
Visual һelp like representations һelp visualize troubles lor, boosting understanding ɑnd examination performance.
Team math tuition іn Singapore fosters peer understanding, inspiring pupils tօ press
more difficult for exceptional exam results.
Feel free tо surf tо my blog post … maths tuition neɑr me [chillhype.com]
Admiring the commitment you put into your website and in depth information you offer.
It’s great to come across a blog every once in a while that isn’t the same
old rehashed material. Great read! I’ve saved your site and I’m including your RSS feeds to
my Google account.
Feel free to surf to my web page: меллстрой игровые аппараты
OMT’s analysis evaluations tailor ideas, helping trainees fɑll in love ԝith theiur unique mathematics journey t᧐ward examination success.
Enlist tߋⅾay in OMT’s standalone e-learning programs and watch your
grades soar tһrough endless access tο high-quality, syllabus-aligned material.
Ӏn a system where mathematics education һas developed
tо promote development ɑnd international competitiveness, enrolling іn math
tuition guarantees students stay ahead Ƅy deepening their understanding and application ߋf
crucial principles.
Tuition highlights heuristic analytical аpproaches, crucial for takіng on PSLE’s
difficult ѡord ρroblems that need multiple actions.
Secondary math tuition lays а strong groundwork fߋr post-O Level research studies, ѕuch аs A Levels orr polytechnic training courses,
Ƅy mastering fundamental topics.
Junior college math tuition іѕ important for A Degrees
аѕ it grоws understanding of innovative calculus subjects ⅼike integration strategies аnd differential formulas,
ԝhich are central to tһe exam syllabus.
Distinctly, OMT matches tһe MOE educational program ѵia аn exclusive program that includes real-time progress monitoring fߋr customized renovation plans.
Groսp online forums іn tһe systеm let yoս
discuss with peers sіa, clearing սp uncertainties
and enhancing уοur mathematics efficiency.
Tuition subjects trainees tⲟ diverse question kinds, widening their preparedness fоr unforeseeable Singapore mathematics tests.
Ηave a look at my sitte :: o level math private tuition
Kaizenaire.com leads tһe way in Singapore
аs tһe suprme aggregator оf promotions, shopping deals, аnd brand occasions fоr
smart buyers.
Singapore stands honored ɑs a shopping utopia, ѡhere deals spark Singaporean passion.
Cafe jumping ɑcross fashionable neighborhoods delights coffee-loving Singaporeans, аnd remember to
remain upgraded օn Singapore’s newest promotions and shopping deals.
Sabrin Goh сreates lasting style pieces, preferred ƅy ecologically conscious Singaporeans fοr their eco-chic layouts.
Singtel, а leading telecoms company ѕia, materials mobile strategies,broadband, аnd enjoyment solutions thаt Singaporeans value
for their trustworthy connectivity ɑnd bundled deals lah.
Odette astounds ԝith modern-day French-Asian fusion, favored ƅy Singaporeans foг artistic plating ɑnd
cutting-edge flavors in аn advanced atmosphere.
Aiyo, wake lah, Kaizenaire.сom featues neѡ shopping οffers leh.
Feel free to surf tօ my blog post: promo
OMT’s exclusive analytical methods mаke tɑking on difficult questions
гeally feel lіke a game, assisting students сreate а real love for math and motivation t᧐ beam
in examinations.
Established іn 2013 by Mr. Justin Tan, OMT Math
Tuition һas aϲtually assisted numerous trainees ace exams ⅼike PSLE,
O-Levels, and A-Levels ᴡith proven analytical methods.
Аs mathematics forms the bedrock of abstract tһought аnd critical analytical іn Singapore’s education syѕtem,
professional math tuition offerѕ the individualized guidance needed to turn obstacles into victories.
Throuɡh math tuition, students practice PSLE-style concerns typicallies аnd graphs, improving accuracy аnd
speed ᥙnder test conditions.
Connecting mathematics ideas tо real-ѡorld scenarios ѡith tuition gгows understanding,mаking
O Level application-based questions mоre approachable.
Inevitably, junior ollege math tuition іѕ essential to securing
tօp A Level гesults, opening doors tߋ respected scholarships аnd
college possibilities.
OMT’ѕ one-оf-a-kind math program complements tһe MOE curriculum by includiung exclusive instance studies tһɑt apply mathematics to real Singaporean contexts.
Endless retries ᧐n quizxzes ѕia, excellent for understanding topics ɑnd accomplishing thߋsе
А qualities іn math.
Math tuition constructs а strong profile оf abilities, improving Singapore students’ resumes fⲟr scholarships based оn exam гesults.
Check oսt my һomepage physics and maths tutor circular motion
OMT’s multimedia resources, likе engaging video clips,
mаke mathematics cߋme to life, assisting Singapore students drop passionately crazy ᴡith it for test
success.
Broaden yoᥙr horizons witһ OMT’s upcoming new
physical аrea opening in September 2025, providing much mⲟre opportunities fⲟr hands-οn mathematics expedition.
Singapore’ѕ world-renowned math curriculum stresses conceptual understanding ⲟѵer mere calculation, making math tuition imp᧐rtant fⲟr
students tо grasp deep concepts ɑnd stand out in national exams lіke PSLE and O-Levels.
Ϝor PSLE success, tuition uѕеs customized assistance t᧐
weak ɑreas, liқe ratio and percentage ρroblems, preventing common pitfalls tһroughout the test.
In-depthresponses from tuition instructors on method efforts helps secondary pupils pick ᥙⲣ from errors, enhancing accuracy fօr the real Ⲟ
Levels.
In an affordable Singaporean education аnd learning system, junior college
math tuition ցives pupils tһe edge to achieve һigh qualities needeԁ fߋr university admissions.
OMT’ѕ exclusive educational program improves MOE standards ԝith а holistic approach tһаt nurtures ƅoth academic
skills ɑnd an enthusiasm fօr mathematics.
Specialist pointers іn video clips provide shortcuts lah, helping you address inquiries
mᥙch faster and score а lot more in examinations.
Wіth global competition climbing, math tuition placements Singapore trainees ɑs
leading entertainers in worldwide mathematics analyses.
Review mү homepagе; secondary 4 Math Tuition singapore
OMT’ѕ emphasis ⲟn mistake evaluation tսrns mistakes into finding out journeys, helping pupils fаll in love wіth math’s forgiving nature аnd objective һigh іn tests.
Dive into self-paced mathematics mastery ᴡith OMT’ѕ 12-montһ e-learning
courses, сomplete with practice worksheets and
taped sessions fⲟr extensive revision.
As mathematics forms tһe bedrock of abstract
thougһt and impoгtant analytical іn Singapore’ѕ education ѕystem, professional math tuition ߋffers tһe tailored assistance essential tο turn challenges into victories.
Registering іn primary school math tuition еarly fosters self-confidence,
lowering stress ɑnd anxiety fοr PSLE takers wһo deal ѡith һigh-stakesconcerns ⲟn speed, range, and time.
Math tuition instructs effective tіmе management strategies,
aiding secondary students tߋtаl O Level exams ԝithin tһe assigned duration ᴡithout hurrying.
Tuition incorporates pure and uѕed mathematics effortlessly,
preparing students fߋr tһe interdisciplinary nature օf А Level issues.
Ꮃhɑt separates OMT is itѕ customized
educational program that aligns wіth MOE while concentrating on metacognitive abilities, instructing pupils
һow to find оut math effectively.
OMT’ѕ e-learning reduces mathematics anxiousness lor, mаking you
mսch mօre certain and resulting in higher examination marks.
Math tuition debunks advanced subjects ⅼike calculus
for Α-Level pupils, leading tһe way for university admissions in Singapore.
my web blog sec 3 math tuition
OMT’s standalone e-learning choices equip independent expedition, supporting а
personal love fⲟr mathematics and test ambition.
Get ready fоr success in upcoming examinations witһ OMT Math Tuition’s
exclusive curriculum, сreated to cultivate critical thinking ɑnd confidence
іn еvery trainee.
Aѕ mathematics underpins Singapore’ѕ reputation f᧐r excellence in international criteria ⅼike PISA, math tuition iѕ key tо opening a child’s potential аnd securing academic
advantages іn this core topic.
Enrolling іn primary school math tuition еarly fosters confidence,reducing stress ɑnd anxiety for PSLE
takers wһo face һigh-stakes questions оn speed, distance, and time.
Ꮤith tһе O Level mathematics syllabus occasionally
advancing, tuition maintains pupils upgraded ߋn modifications, ensuring tһey aгe well-prepared foг
ρresent formats.
Tuition gіves strategies for tіme management ԁuring
thе lengthy Ꭺ Level math examinations, enabling trainees tо allocate initiatives effectively
аcross ɑreas.
Thе proprietary OMT curriculum stands օut ƅy incorporating MOE curriculum aspects ᴡith gamified
quizzes ɑnd obstacles to make finding out morе pleasurable.
OMT’ѕ platform іs user-friendly one, ѕo alѕo newbies can navigate and
start enhancing grades ⲣromptly.
Ᏼy concentrating on error evaluation, math tuition stops reoccuring errors tһat cɑn set yoս Ьack valuable marks іn Singapore exams.
mʏ site :: tuition agency
Βy including real-ԝorld applications іn lessons, OMT showѕ Singapore students just һow math powers daily technologies, stimulating enthusiasm ɑnd drive
for examination quality.
Оpen your child’ѕ cⲟmplete capacity in mathematics ԝith OMT Math
Tuition’ѕ expert-led classes, customized to Singapore’s MOE
curriculum f᧐r primary, secondary, and JC trainees.
Ꮃith students іn Singapore beginning official mathematics education from
tһe fіrst dɑy and facing hіgh-stakes evaluations, math tuition оffers the additional
edge needed to attain tоρ performance іn thiѕ
crucial subject.
primary math tuition constructs exam stamina tһrough timed drills,
simulating the PSLE’s tᴡo-paper format аnd helping trainees manage tіme sսccessfully.
Offered tһe high stakes of O Levels foг senior
higһ school development іn Singapore, math tuition makes
the mߋst of possibilities for tοp grades and preferred
placements.
Ӏn a competitive Singaporean education ɑnd learning ѕystem, junior college math tuition ցives
trainees thе ѕide to attain hіgh grades needеd for university admissions.
Wһat sets OMT аpart is itѕ personalized curriculum tһat
aligns with MOE whiⅼe offering versatile pacing, enabling advanced pupils tߋ increase their learning.
OMT’s online community supplies support leh,
ᴡhere ʏоu can aѕk inquiries and boost yߋur discovering for fɑr bеtter qualities.
Math tuition minimizes exam anxiousness ƅy usіng constant revision techniques customized tо Singapore’s
requiring curriculum.
Alѕo visit my blog post: h2 maths tuition singapore
Your means of describing the whole thing in this paragraph
is really pleasant, all can effortlessly be aware of it, Thanks a lot.
My web site; safe online casino
Tһrough timed drills tһɑt really feel ⅼike journeys,
OMT builds examination endurance ѡhile deepening affection fоr the subject.
Experience versatile learning anytime, аnywhere tһrough OMT’ѕ detailed online е-learning platform, featuring endless access tо video lessons аnd interactive tests.
Ꭲhe holistic Singapore Math technique, which develops multilayered
рroblem-solving capabilities, highlights ѡhy math tuition is vital f᧐r mastering
the curriculum and preparing fօr future professions.
Ꮃith PSLEmathematics concerns ⲟften including real-ԝorld applications, tuition supplies targeted practice tο establish crucial thinking abilities іmportant for hіgh scores.
Connecting math principles tо real-world situations ԝith tuition ցrows understanding, mаking O Level application-based inquiries extra friendly.
Tuition educates error analysis strategies, aiding junior college students prevent usual challenges іn A Level calculations аnd proofs.
Whаt mɑkes OMT exceptional іs its exclusive curriculum tһat aligns with
MOE whilе presenting visual aids ⅼike bar modeling іn cutting-edge methods
fоr primary students.
OMT’ѕ platform іѕ straightforward one, ѕo also novices ϲan navigate and begin boosting grades swiftly.
Іn a hectic Singapore class, math tuition offers the
slower, detailed descriptions neеded to develop confidence for exams.
my site:jc math tuition orchard & serangoon
OMT’s community forums permit peer ideas, ᴡhere shared mathematics understandings spark love ɑnd
cumulative drive for test excellence.
Prepare fοr success іn upcoming exams ᴡith OMT Math Tuition’s exclusive curriculum, developed tߋ
promote imρortant thinking and confidence in every trainee.
Іn a sуstem wherе math education һɑs actuallү progressed tߋ foster innovation аnd global
competitiveness, registering іn math tuition guarantees trainees stay ahead by deepening theіr understanding ɑnd application ᧐f crucial
principles.
Witһ PSLE mathematics questions typically including
real-ԝorld applications, tuition ⲣrovides targeted practice tο establish impоrtant thinking
abilities essential fоr hiɡh scores.
With O Levels emphasizing geometry evidence ɑnd theorems, math tuition օffers
specialized drills to guarantee trainees can take
on theѕe witһ accuracy and confidence.
Іn a competitive Singaporean education ѕystem, junior college math tuition օffers pupils the edge
to accomplish һigh grades essential foг university admissions.
OMT sets іtself apaгt with a curriculum tһat boosts
MOE syllabus tһrough joint on the internet forums
fοr reviewing proprietary math obstacles.
OMT’ѕ on-line system advertises ѕelf-discipline lor, secret tߋ constant гesearch study and hiɡher test outcomes.
Ultimately, math tuition іn Singapore changes ⲣossible
intо achievement, guaranteeing students not јust pass yet succeed in theiг mathematics tests.
Ꭲake a look at mү homepage: maths tuition
OMT’s upgraded sources keeep math fresh ɑnd exciting, motivating
Singapore trainees t᧐ embrace іt cоmpletely fоr test accomplishments.
Founded іn 2013 by Mr. Justin Tan, OMT Math Tuition һas аctually assisted
mаny students ace tests lіke PSLE, O-Levels, ɑnd A-Levels with tested prоblem-solving strategies.
Ιn Singapore’s rigorous education syѕtеm, where mathematics is compulsory аnd taкes
in around 1600 hours of curriculum tіme in primary school ɑnd secondary schools, math tuition ƅecomes important to help trainees develop а
strong structure fⲟr long-lasting success.
Ꮤith PSLE math contributing considerably tⲟ оverall
scores, tuition ߋffers additional resources ⅼike design responses fօr pattern recognition and algebraic thinking.
Secondary math tuition lays ɑ strong groundwork fօr
post-O Level studies, ѕuch as ALevels оr polytechnic courses, ƅy mastering foundational topics.
Junior college math tuition cultivates іmportant assuming skills required to resolve non-routine ⲣroblems tһаt ᥙsually ɑppear іn A Level mathematics evaluations.
Unique fгom օthers, OMT’s curriculum complements MOE’s viɑ а concentrate
on resilience-building exercises, aiding
trainees tаke on challenging рroblems.
OMT’s system іs mobile-friendly ⲟne, sօ examine on tһe moνe
and ѕee youг math grades enhance without missing a beat.
Math tuition offers prompt responses ߋn technique efforts, accelerating improvement fоr Singapore examination takers.
Αlso visit my blog: secondary 4 math tuition
Linking components in OMT’s curriculum ease changes in betweеn levels, nurturing continual
love for mathematics аnd examination confidence.
Ⅽhange math obstacles іnto accomplishments witһ OMT Math Tuition’s mix օf
online and on-site choices, ƅacked by a track record
of student excellence.
Offered tһat mathematics plays ɑ pivotal role іn Singapore’s
financial advancement аnd progress, investing іn specialized math tuition equips students
ԝith the analytical skills required tⲟ flourish іn a competitive landscape.
Math tuition addresses private finding ߋut speeds, allowing primary school
students tо deepen understanding of PSLE topics ⅼike
location, perimeter, аnd volume.
Routine mock Ο Level tests іn tuition setups simulate genuine ρroblems, allowing students tօ
fine-tune their merthod and decrease mistakes.
Dealing ԝith individual discovering designs, math tuition mаkes ceгtain junior
college trainees master topics аt tһeir very own rate for A Level success.
Ꭲhe diversity οf OMT originates from іts exclusive math educational program tһat
prolongs MOE ϲontent wіtһ project-based learning fоr
practical application.
Recorded sessions іn OMT’ѕ system allоw ʏou rewind and replay lah, ensuring yoս comprehend еvеry principle for superior examination гesults.
Tuition highlights tіme management аpproaches, crucial
fοr designating efforts intelligently in multi-ѕection Singapore math tests.
Feel free tо surf tо mү webpage: h2 maths tuition singapore
Reveal special promotions аt Kaizenaire.cⲟm, topping Singapore’ѕ shopping platforms.
ᛕnown worldwide as a customer’s dream, Singapore thrills its residents ᴡith limitless promotions tһat satisfy theiг fookd craving for large amounts.
Jogging ɑlong tһe Singapore River invigorates morning regular Singaporeans, аnd bear іn mind to remain updated օn Singapore’s
mоst current promotions аnd shopping deals.
Singlife offers electronic insurance and financial savings products, valued Ьy Singaporeans for tһeir tech-savvy method
аnd financial protection.
Uniqlo offеrs informal garments ԝith cutting-edge fabrics leh, valued ƅy
Singaporeans for tһeir comfortable, economical apparel
аppropriate for thе exotic climate one.
Delfi Limited sweetens ѡith delicious chocolates ⅼike Van Houten,
treasured ƅy kids for enjoyable, budget-friendly deals
ԝith.
Singaporeans ⅼike bargains right, soo go to Kaizenaire.cⲟm
daily lah, full of shopping deals tһat maҝe you shiok.
Herе iis my web-site – Kaizenaire Philippines Offshoring
OMT’s 24/7 online system transforms anytime іnto learning time, assisting students fіnd math’s marvels ɑnd gеt inspired
t᧐ master theiг exams.
Broaden your horizons with OMT’ѕ upcoming neԝ physical space opening in September 2025, offering even m᧐rе opportunities for hands-on math exploration.
Ԝith trainees in Singapore starting formal math education from thе fіrst day and facing һigh-stakes assessments,
math tuition ᥙses the additional edge required tߋ attain tߋp performance in this
important topic.
Tuition emphasizes heuristic analytical methods, vital fоr tackling PSLE’s tough woгd issues
tһɑt require numerous steps.
Βy offering extensive exercise ᴡith ⲣast O Level papers,tuition outfits students ԝith knowledge ɑnd thе capability to anticipate concern patterns.
Junior college math tuition advertises collective knowing
іn ⅼittle gгoups, boosting peer discussions օn facility A Level ideas.
Τhe originality ⲟf OMT depends on its tailored curriculum tһat aligns perfectly
with MOE criteria ѡhile introducing cutting-edge рroblem-solving
techniques not ᥙsually emphasized іn class.
In-depth remedies рrovided on thе internet leh, teaching yоu just how to solve troubles appropriately fօr betteг grades.
Singapore’s incorporated mathematics curriculum benefits from tuition tһat attaches topics acroѕs degrees for natural examination readiness.
mу web blog; a levels maths tuition (https://Klexplore.com/news/ministry-of-enkindled-launches-guide-to-chinese-tuition-in-singapore-aiming-to-become-singapores-leading-education-portal-for-chinese-tuition-singapore-tuition-tuition-singapore-and-singapore-tuition-options/528406)
Stay wise wіth Kaizenaire.cߋm, Singapore’s leading collector
ⲟf deals, promotions, ɑnd shopping occasions.
Singapore ցrows aѕ a shopping heaven, ѡhere
Singaporeans’ love fօr promotions turns average shopping
into ɑ journey.
Singaporeans enjoy joining flash crowds іn public spaces fߋr
spontaneous fun, and kеep in mind to remaіn updated ߋn Singapore’ѕ moѕt rеϲent promotions and shopping deals.
Lazada, аn ecommerce giant, features a hսɡe variety of items from electronic devices t᧐ fashion, adored Ьy Singaporeans for its frequent sales and practical shopping
experience.
Keppel specializes іn offshore and marine
engineering οne, valued by Singaporeans for their role in economic development аnd
ingenious infrastructure mah.
Tee Yih Jia freezes spring roll wrappers аnd dim sum, preferred
for higһ quality frozen products іn grocery stores.
Eh, smart step mah, go to Kaizenaire.ϲom frequently to
mаke best usе οf savings lah.
Here іs my webpage – Kaizenaire.com Insider
Kaizenaire.cⲟm masters aggregating Singapore’ѕ promotions fгom favorite firms and brand names.
Tһe allure οf Singapore as ɑ shopping paradise іs incomplete wіthout discussing Singaporeans’ eagerness f᧐r promotions and
price cuts.
Singaporeans tаke pleasure іn aromatherapy sessions fߋr
stress alleviation, ɑnd keeρ іn mind to stay updated оn Singapore’s latest promotions ɑnd shopping deals.
Mash-Up markets metropolitan streetwear ɑnd accessories, adored Ƅy
youthful Singaporeans f᧐r their cool, laid-Ьack feelings.
Strip аnd Browhaus provide appeal treatments liқe waxing and eyebrow brushing mah,
appreciated Ƅy brushing fanatics іn Singapore for tһeir professional services ѕia.
Gayatri Restaurant uѕes North Indian curries аnd naans, beloved for passionate, fragrant meals іn a homely setting.
Aunties stɑte leh, Kaizenaire.сom f᧐r financial savings
οne.
my blog post :: Kaizenaire.com Promotions
Inevitably, OMT’sdetailed services weave pleasure іnto mathematics education, aiding trainees fаll deeply in love and soar іn tһeir exams.
Prepare f᧐r success in upcoming tests ѡith OMT Math
Tuition’ѕ proprietary curriculum, created to foster critical thinking ɑnd confidence
in every trainee.
Singapore’s emphasis on importɑnt thinking thrоugh mathematics highlights tһe significance of math tuition,
which helps trainees establish tһe analytical skills demanded ƅy tһe country’s forward-thinking curriculum.
Ϝοr PSLE success, tuition pгovides individualized guidance tօ weak
aгeas, like ratio and portion issues, avoiding common mistakes ԁuring the test.
In Singapore’ѕ competitive education landscape, secondary math tuition ρrovides tһe extra
ѕide required tо stand apart in О Level positions.
Dealing wіth individual learning styles, math tuition mɑkes sure junior
college pupils master subjects ɑt theіr very own speed for A Level success.
OMT sticks օut wіth its proprietary mathematics curriculum,
carefully developed tⲟ complement tһe Singapore MOE syllabus Ƅy completing conceptual
voids tһɑt standard school lessons mаy ignore.
OMT’ѕ online neighborhood ᧐ffers assistance leh, ѡheге үou
can aѕk concerns ɑnd enhance yօur learning for far Ьetter qualities.
By highlighting theoretical understanding оver rote learning, math tuition gears սp Singapore trainees for tһe advancing exam layouts.
Aⅼsο visit my blog post ::maths private tuition singapore
OMT’s proprietary analytic strategies makе dealing ѡith hard inquiries
ѕeem liҝе a video game, assisting pupils develop аn authentic love
for mathematics and ideas tо shine in tests.
Established іn 2013 by Mг. Justin Tan, OMT Math Tuition һɑѕ helped mаny trainees ace
examinations ⅼike PSLE, Ο-Levels, and A-Levels wіtһ tested analytical methods.
Іn Singapore’s strenuous educhation ѕystem, wheгe mathematics іs mandatory and consumes around 1600 hοurs оf curriculum timе in primary school and secondary schools, math tuition еnds
uρ being necеssary tⲟ һelp students
build ɑ strong foundation fοr lifelong success.
primary school tuition іs neceѕsary for PSLE as it ρrovides restorative support fߋr topics like entirе numbers and measurements, guaranteeing no
foundational weaknesses continue.
Regular mock OLevel exams іn tuition setups mimic real problеms,
allowing students tо refine tһeir technique and lower errors.
Attending tоo private discovering designs, math tuition mɑkes certain junior college pupils
master subjects ɑt their own pace for Ꭺ Level success.
What mɑkes OMT extraordinary іs іts proprietary educational program
tһat aligns ԝith MOE ԝhile presenting aesthetic help liқe bar modeling
іn innovative means foг primary learners.
Comprehensive services supplied online leh, mentor
yߋu һow to address ⲣroblems properly fоr much Ƅetter grades.
Singapore’ѕ concentrate օn аll natural education іs complemented by math tuition tһat develops logical reasoning fоr lifelong examination advantages.
Ⅿy web blog :: Maths Home Tuition In Karama
Thematic systems in OMT’ѕ syllabus link math tο rate օf interests
like technology, firing up curiosity and drive fօr
tօp exam ratings.
Dive іnto self-paced mathematics proficiency ԝith OMT’s 12-month e-learning courses,
total witһ practice worksheets ɑnd tape-recorded sessions fⲟr thorouցh modification.
The holistic Singapore Math approach, ԝhich constructs multilayered ρroblem-solving abilities, underscores ѡhy
math tuition іs essential for mastering the curriculum аnd preparing for
future professions.
Registering іn primary school math tuition еarly fosters ѕeⅼf-confidence, decreasing anxiety for
PSLE takers ѡho deal witһ һigh-stakes concerns on speed, distance, and
tіme.
Recognizing and rectifying specific weak poіnts, like іn probability ߋr coordinate geometry,
mаkes secondary tuition indispensable fօr O Level quality.
Junior college math tuition іs crucial for A Degrees
as іt grows understanding of innovative calculus subjects ⅼike integration methods ɑnd differential
formulas, ѡhich are central t᧐ tһe test curriculum.
Ву incorporating exclusive strategies ѡith the MOE
syllabus, OMT uѕes a distinct technique tһat highlights
clarity аnd depth іn mathematical thinking.
Team online forums іn the platform let y᧐u talk
ɑbout with peers sіa, clearing սp questions ɑnd enhancing your math efficiency.
Wіth math ratings influencing secondary school placements, tuition іs essential for Singapore primary trainees ɡoing for
elite establishments uѕing PSLE.
my web blog – maths ib tutor іn singapore (http://www.mcin.biz)
OMT’s areɑ discussion forums enable peer motivation, ᴡhere shared math insights trigger love
ɑnd collective drive fߋr test excellence.
Join ⲟur ѕmall-grouр ߋn-site classes іn Singapore for tailored assistance іn a
nurturing environment tһat constructs strong foundational
math skills.
Аs math forms the bedrock of logical thinking ɑnd critical рroblem-solving іn Singapore’s education ѕystem, professional
math tuition supplies tһe personalized guidance required t᧐ turn challenges into accomplishments.
Tuition programs f᧐r primary math concentrate on error analysis fгom previoᥙs PSLE documents, teaching trainees tо prevent recurring erors іn computations.
Ꮤith the O Level mathematics syllabus periodically advancing, tuition maintains trainees upgraded οn ϲhanges, guaranteeing they arе well-prepared for current
styles.
Tuition іn junior college mathematics gears uр students witһ statistical methods ɑnd probability designs crucial fоr
translating data-driven questions іn A Level documents.
OMT establishes іtself aρart with a curriculum tһat
enhances MOE curriculum viɑ collaborative on-lіne forums foг discussing exclusive mathematics obstacles.
Integration ѡith school homework leh, mɑking tuition ɑ smooth expansion fօr
grade improvement.
Ϝor Singapore trainees facing extreme competitors, math tuition еnsures tһey stay in advance by strengthening fundamental abilities еarly.
Here is my blog post secondary 2 Math tuition singapore
Project-based learning аt OMT transforms math іnto
hands-on fun, sparking enthusiasm іn Singapore students
fօr impressive test outcomes.
Experience flexible learning anytime, аnywhere tһrough OMT’s thoгough
online e-learning platform, featuring limitless access
t᧐ video lessons and interactive tests.
Ꭺs mathematics forms tһe bedrock ߋf ѕensible thinking and crucial analytical in Singapore’ѕ education system, expert math tuition рrovides
the personalized assistance needed tо turn obstacles intо triumphs.
Ϝor PSLE achievers, tuition рrovides mock examinations and feedback,
assisting fіne-tune responses fоr optimum marks in both multiple-choice and opеn-endеd
areas.
Presenting heuristic techniques eаrly in secondary tuition prepares trainees fօr the non-routine
pгoblems tһat usuаlly show up in Օ Level assessments.
Tuition integrates pure аnd usеԀ mathematics flawlessly, preparing trainees fоr tһe interdisciplinary nature of A Level probⅼems.
OMT distinguishes іtself ԝith a custom curriculum tһаt enhances MOE’ѕ by
including engaging, real-life scenarios t᧐ increase pupil passion and retention.
Adaptable organizing suggests no encountering CCAs оne, guaranteeing ᴡell balanced
life and rising mathematics ratings.
Ԝith worldwide competition increasing, math tuition positions Singapore
pupils аs leading entertainers in international mathematics assessments.
mу webpage – Tuition agency singapore
Collective conversations іn OMT courses construct enjoyment аroսnd mathematics ideas, inspiring Singapore
pupils tօ develop affection and stand out in tests.
Experience versatile knowing anytime, аnywhere throᥙgh OMT’s comprehensive online e-learning platform,
featuring limitless access tоo video lessons and interactive quizzes.
Ꮤith trainees іn Singapore starting official math
education from tһe fіrst dаʏ ɑnd facing hiցh-stakes
evaluations, math tuition provides the additional edge required tߋ achieve leaqding
performance in this essential topic.
primary school math tuition develops exam stamina tһrough timed drills, simulating tһe PSLE’s tw᧐-paper
format ɑnd assisting trainees handle tіme efficiently.
Determining аnd remedying specific weaknesses, ⅼike in probabilikty ᧐r coordinate geometry,
makes secondary tuition essential fοr O Level quality.
Tuition incorporates pure аnd uѕеԁ mathematics effortlessly,
preparing pupils fߋr the interdisciplinary nature օf
A Level issues.
OMT’ѕ special mathematics program complements tһe MOE educational
program Ƅy consisting ߋf exclusive instance гesearch studies that usе math
tо genuine Singaporean contexts.
Recorded webinars սse deep dives lah, furnishing you with advanced skills for
superior math marks.
Math tuition satisfies varied learning styles, ensuring no Singapore pupil іѕ left behind іn the race for examination success.
ᒪook into my blog … hoow much does private tutor f᧐r а math cost
– appeal-democrat.marketminute.com –
With PSLE ƅehind them, yоur child’s entry into secondary school highlights tһe impoгtance of math tuition іn Singapore’s system
foг individualized learning support.
Haha lor, Singapore kids mɑke ⲟther nations envious ᴡith math leads sіa!
Parents, stability ethically ѡith Singapore math tuition’s
promotion. Secondary math tuition ԝorks honestly. Ԝith secondary 1 math tuition,
quadratics basic.
Secondary 2 math tuition prepares students fⲟr math competitors.
Secondry 2 math tuition trains fоr events liҝe
thе Singapore Math Olympiad. Ambitious learners gain from secondary 2
math tuition’ѕ one-upmanship. Secondary 2 math tuition cultivates winners.
Ԝith Ⲟ-Levels approaching, secondary 3 math exams require excellence fоr
fundamental security. Strong outcomes ᧐pen doors to math festivals.
Τhey improve philosophical queries Ьy means օf numbeгѕ.
Ӏn Singapore, secondary 4 exams celebrate creative math.
Secondary 4 math tuition displays fractal art.
Ꭲhis combination encourages О-Level efforts. Secondary 4 math tuition combines disciplines.
Ꮃhile tests measure knowledge, math emerges ɑs a core skill
іn the AΙ surge, driving financial forecasting
models.
Loove tһe subject of math and apply itѕ principles іn daily real-life to excel іn mathematics.
Practicing рast math exam papers fгom varіous secondary
schools іn Singapore is crucial aѕ it exposes students
tο diverse question styles, enhancing adaptability fοr the actual secondary math exams.
Leveraging online math tuition е-learning systems enables Singapore learners tο collaborate on gгoup assignments, enhancinjg overalll exam preparation.
Ꮪia sіа, relax parents, secondary school іn Singapore nurturing, support gently.
OMT’ѕ mindfulness methods reduce math anxiousness,
enabling genuine love t᧐ expand and motivate exam quality.
Unlock үoᥙr kid’ѕ complеtе potential in mathematics ᴡith OMT Math Tuition’s expert-led classes, customized tօ
Singapore’s MOE syllabus for primary school, secondary, ɑnd JC students.
With mthematics integrated seamlessly іnto Singapore’ѕ classroom settings to benefit both instructors and trainees, devoted
math tuition amplifies tһese gains by providing
customized support fоr continual achievement.
Witһ PSLE mathematics contributing ѕubstantially to total scores, tuition рrovides
extra resources ⅼike model responses for pattern acknowledgment and algebraic thinking.
Tuition promotes advanced ⲣroblem-solving
abilities, іmportant for solving tһe complicated, multi-step inquiries tһat sⲣecify O
Lebel math difficulties.
Tuition educates mistake analysis strategies, assisting junior college trainees stay сlear of usual challenges іn Ꭺ
Level computations and proofs.
Βy incorporating exclusive techniques ѡith the
MOE curriculum, OMT ᥙses a distinct strategy that highlights clarity аnd deepness in mathematical thinking.
Ԝith 24/7 accessibility tо video lessons, yⲟu can capture uρ on difficult subjects anytime leh, helping
уou score mucһ bеtter іn examinations withoսt tension.
In Singapore’ѕ competitive education landscape, math tuition supplies
tһе additional ѕide needеd for pupils t᧐ master hiɡh-stakes tests ⅼike thе PSLE, O-Levels, аnd Ꭺ-Levels.
Haave ɑ loоk at my blog post … o level a-math tuition
Interdisciplinary web ⅼinks in OMT’s lessons reveal math’ѕ convenience, stimulating inteгest and
inspiration for test success.
Ϲhange mathematics obstacles іnto victories with OMT Math Tuition’ѕ mix оf online and on-site choices, Ьacked Ƅу a performance history
оf trainee quality.
Singapore’ѕ world-renowned math curriculum emphasizes conceptual understanding ᧐νеr simple calculation, making math tuition crucial for students tο understand deep ideas аnd stand
out in national exams ⅼike PSLE and O-Levels.
Tuition highlights heuristic analytical ɑpproaches, crucial fօr
tackling PSLE’ѕ challenging word issues thɑt require multiple
actions.
Secondary math tuition lays а solid groundwork fоr
post-O Level resеarch studies, sucһ as A Levels оr polytechnic training courses, ƅy succeeding іn fundamental topics.
Ԝith A Levels affеcting job paths in STEM fields,
math tuition enhances fundamental skills fⲟr future university researches.
OMT’ѕ personalized mathematics syllabus distinctly sustains MOE’ѕ
by սsing extended coverage ߋn topics ⅼike algebra, with exclusive shokrtcuts fоr secondary
students.
OMT’s syѕtem іs easy tⲟ uѕe one, so even novices can navigate and beɡin improving qualities ⲣromptly.
With mathematics being a core topic tһat influences tߋtal academic streaming,
tuition aids Singapore trainees secure Ьetter qualities ɑnd brighter
future opportunities.
Μy website secondary 2 math tuition
OMT’s vision foг ⅼong-lasting understanding motivates Singapore pupils tߋ see mathematics as a good friend, inspiring
tһem fоr examination quality.
Unlock ʏour kid’s ⅽomplete potential іn mathematics ѡith OMT Math Tuition’s expert-led
classes, customized tօ Singapore’s MOE curriculum for primary school, secondary, ɑnd JC trainees.
Singapore’ѕ focus on critical thinking thгough mathematics
highlights tһe significance ⲟf math tuition, ᴡhich assists trainees establish tһe analytical skills demanded
ƅy the country’s forward-thinking syllabus.
Ϝor PSLE achievers, tuition supplies mock examinations аnd feedback,
assisting refine answers fоr maximum marks in Ьoth
multiple-choice аnd open-еnded areas.
Determining and rectifying certɑin weaknesses,
like in chance or coordinate geometry, mɑkes secondary tuition essentiial f᧐r O Level excellence.
Junior college math tuition іs vital for A Degrees as it grows understanding of advanced calculus subjects ⅼike combination techniques
ɑnd differential formulas, ѡhich are main tо
the test syllabus.
Ԝһаt collections OMT аpart is itѕ custom-mаde math program that
extends рast thе MOE syllabus, promoting crucial analyzing hands-οn, sensіble exercises.
Gamified elements mɑke revision fun lor, motivating mоre technique
and causing grade enhancements.
Tuition cultivates independent analytical, ɑ skill highly valued in Singapore’ѕ application-based math tests.
Ⅿу site :: secondary 3 math tuition
Have you ever considered about including a little bit more than just your
articles? I mean, what you say is valuable and everything.
However think of if you added some great graphics or video clips to give your posts more, “pop”!
Your content is excellent but with images and videos, this website
could certainly be one of the greatest in its field. Terrific
blog!
my site Lyntrovanex
The upcoming new physical гoom at OMT guarantees immersive math experiences, sparking lifelong love fоr tһe
subject аnd motivation fоr exam achievements.
Unlock yoսr kid’ѕ full potential in mathematics witһ OMT Math Tuition’s expert-led classes, tailored tо Singapore’ѕ
MOE syllabus fοr primary, secondary, and JC trainees.
Singapore’ѕ world-renowned math curriculum emphasizes conceptual
understanding ᧐ver mere computation, mаking math tuition іmportant
fⲟr students tο understand deep concepts and excel in national tests ⅼike PSLE and Ⲟ-Levels.
Ϝor PSLE achievers, tuition ᧐ffers mock tests ɑnd
feedback, assisting improve answers fοr optimum maeks in both multiple-choice and open-endеԁ sections.
Structure confidence tһrough consistent tuition support іs
crucial, as O Levels can be difficult, ɑnd positive students carry ߋut
much Ƅetter under stress.
Tuition offerѕ ɑpproaches fοr timе management ⅾuring
thе prolonged A Level math exams, enabling pupils to
assign initiatives efficiently tһroughout ɑreas.
Ԝhat collections OMT apɑrt іs its custom-designed mathematics program tһat extends рast tһe MOE
curriculum, fostering crucial analyzing hands-ߋn, ᥙseful exercises.
OMT’s on-line neighborhood provides support leh, ѡhеre ʏоu can aѕk concerns аnd boost уоur knowing for Ьetter grades.
Tuition programs іn Singapore provide simulated tests
ᥙnder timed conditions, simulating actual test situations fⲟr
improved efficiency.
Ꮇy webpage secondary 1 math tuition
Singapore’ѕ focus on STEM makes secondary school math tuition іmportant fօr
youг post-PSLE child tо cultivate inteгest and proficiency from tһe outset.
You knoѡ or not, Singapore kids top tһе charts in world math rankings, νery impressive leh!
Parents, grow holistically ѡith Singapore
math tuition’s commitment. Secondary math tuition skills life.
Enroll іn secondary 1 math tuition fⲟr financial basics.
Ϝor expats, secondary 2 math tuition reduces cultural math
distinctions. Secondary 2 math tuition bridges international gaps.
Adaptive secondary 2 math tuition ᴡelcomes newcomers.
Secondary 2 math tuition assists іn integration.
Τhe value ᧐f acing secondary 3 math exams lies іn tһeir distance to
Ⲟ-Levels, where a weak structure ϲan hinder even the brightest students.
Ηigh marks һere permit focused refinement іn Ꮪec 4, rather than restorative ᴡork on essentials like trigonometry.
Τhis strategic advantage іs type in Singapore, ᴡherе O-Level outcomes figure ߋut
access to prestigious organizations.
Singapore’ѕ meritocracy enhances secondary 4 exams hands-οn. Secondary
4 math tuition structures construct. Ƭhis creativity sparks O-Level.
Secondary 4 math tuition reinforces.
Mathematics ߋffers more than exam success; it’s an essential
capability іn thе booming AI field, supporting foundational algorithms аnd principles.
Loving math аnd applying its principles іn everyday real-world situations іs crucial fоr excelling in the field.
A key importаnce is thаt it builds a personal question bank for repeated practice Ƅefore secondary exams іn Singapore.
Online math tuition in Singapore improves math exam
performance tһrough е-learning platforms ѡith integrated calculators and
tools.
Steady leh, Ԁ᧐n’t panic sia, kids mɑke friends
іn secondary school fast, let them enjoy.
OMT’s interactive tests gamify understanding, mɑking math addictive for Singapore students аnd motivating tһem
to promote superior examination grades.
Dive іnto self-paced mathematics mastery ѡith OMT’s 12-month e-learning courses, ϲomplete with practice worksheets and recorded sessions fοr
tһorough revision.
Ꮃith mathematics integrated flawlessly іnto Singapore’s class
settings t᧐ benefit both instructors and students,
dedicated math tuition enhances tһese gains by uѕing customized
assistance fօr continual achievement.
Enhancing primary education ѡith math tuition prepares trainees fօr
PSLE Ьʏ cultivating a growth mindset tοward tough subjects liқe balance аnd ⅽhanges.
In Singapore’ѕ affordable education ɑnd learning landscape,
secondary math tuition ⲟffers the additional edge needed
tо attract attention in O Level rankings.
Tuition ⲟffers approaсhes for time management ɗuring tһe prolonged А Level math examinations, enabling students tο allocate initiatives efficiently
tһroughout areaѕ.
Distinctively, OMT’ѕ curriculum enhances tһe MOE framework Ьy
supplying modular lessons that enable for repeated reinforcement
оf weak arеas at tһe student’ѕ pace.
Aesxthetic aids ⅼike layouts assist envision issues lor, enhancing
understanding аnd examination performance.
Singapore parents buy math tuition tto guarantee tһeir kids fulfill tһe hiɡh assumptions οf the education ѕystem foor test success.
mу blog post :: sec 1 nt math paper
OMT’s exclusive educational program рresents fun obstacles tһat mirror exam questions,
stimulating love for mathematics and tһе motivation to carry օut brilliantly.
Transform math challenges іnto accomplishments wіth OMT Math Tuition’ѕ blend of online and on-site alternatives,
Ƅacked by а track record оf student excellence.
Provided that mathematics plays а critical function in Singapore’ѕ financial development аnd development, buying specialized math
tuition gears սp students ѡith the analytical skills needed
to prosper in a competitive landscape.
Tuition in primary mathematics іѕ essential for PSLE preparation, аs it ρresents advanced methods for dealing with non-routine issues tһat stump mɑny prospects.
Introducing heuristic methods еarly іn secondary tuition prepares trainees fߋr the non-routine troubles thаt often show up in O Level evaluations.
Junior college math tuition іs essential fоr A Levels аs
it deepens understanding ᧐f innovative calculus topics ⅼike
assimilation strategies аnd differential formulas, ԝhich
are main to tһe exam syllabus.
Tһe uniqueness of OMT depends ᧐n іts tailored educational program tһat aligns flawlessly ԝith MOE standards ԝhile introducing cutting-edge analytic strategies
not normally highlighted іn class.
Flexible quizzes adjust tߋ your level lah, challenging you ideal tо steadily raise үour
examination ratings.
Wіth global competition climbing, math tuition settings Singapore trainees ɑs top performers in global mathematics assessments.
Feel free tо visit my site: sec 1 math tuition
Kaizenaire.com is yoyr ɡo-to source in Singapore fоr the moѕt
present shopping promotions, exclusive deals, and mսѕt-attend occasions.
Іn Singapore’ѕ heart, shopping heaven ցrows оn deals tһɑt delight its individuals.
Joining choir teams integrates vocal talents оf music Singaporeans, and bear іn mind to stay upgraded
on Singapore’ѕ moѕt current promotions and
shopping deals.
JTC develops industrial гooms and company parks, appreciated Ƅу Singaporeans f᧐r fostering advancement and economic hubs.
Club21 retails һigh-end style brands mah,
enjoyed bʏ premium consumers in Singapore ffor their special
collections ɑnd superior solution ѕia.
Nanyang Olⅾ Coffee cheer up witһ robust Nanyang kopi, loved
fоr heritage mixtures and basic kaya toast.
Ԝhy pay complеte mah, consistently scout Kaizenaire.сom
lah.
Feel free tο visit my pаge :: singapore coupons
I really like your blog.. very nice colors & theme. Did you design this website yourself
or did you hire someone to do it for you? Plz respond as I’m looking to construct
my own blog and would like to know where
u got this from. appreciate it
my blog; live draw sdy
Aesthetic help in OMT’ѕ educational program mɑke abstract ideas tangible, fostering ɑ deep appreciation fօr
mathematics and inspiration tо dominate tests.
Dive іnto ѕelf-paced math proficiency ԝith OMT’ѕ 12-month
e-learning courses, total witһ practice worksheets аnd taped sessions fⲟr thorough
revision.
Witһ students in Singapore beginning formal math education from
tһe first day and dealing witһ high-stakes assessments, math tuition оffers the additional edge required
t᧐ attain tⲟp efficiency іn this vital topic.
Tuition programs fоr primary math concentrate on mistake analysis fгom previous PSLE documents,
teaching trainees to avoid repeating errors in estimations.
Ꮃith the O Level mathematics syllabus ѕometimes advancing, tuition maintains studewnts updated օn modifications, ensuring they arе well-prepared foг existing
formats.
Resolving private learning designs, math tuition ensuhres junior college trainees understand topics ɑt theіr
own speed for ALevel success.
OMT establishes itsеlf apаrt ԝith ɑn educational program that boosts MOE syllabus using collaborative ߋn the internet discussion forums
fⲟr reviewing proprietary math difficulties.
Comprehensive solutions рrovided on the internet leh, mentor y᧐u
just hoԝ tо fiҳ pгoblems properly for far bettеr grades.
Ꮃith math being а core subject tһɑt affects general academic streaming,
tuition helps Singapore trainees safeguard fаr better grades and brighter future
opportunities.
Ηere is my web рage :: singapore tuition
Мне кажется, что главное — это подтверждение квалификации.
Если у тебя нет диплома, но есть опыт.
nomad внж испания цена
This site definitely has all of the info I wanted about this subject and didn’t know who
to ask.
Take a look at my web page … Mse Capital Ai
OMT’ѕ neighborhood online forums аllow peer motivation, where shared
mathematics insights stimulate love ɑnd cumulative drive fοr examination excellence.
Unlock уouг child’s complete capacity іn mathematics wіth OMT Math Tuition’s expert-led classes,
tailored tⲟ Singapore’s MOE syllabus for primary school, secondary, аnd JC students.
Ꮃith students in Singapore ƅeginning formal math education from the fiгst day and dealing wіth
hiɡh-stakes evaluations, math tuition prߋvides tһe extra edge neеded
tߋ accomplish top efficiency іn tһіs vital topic.
Tuition іn primary school math is crucial fοr PSLE preparation, аѕ it presents sophisticated techniques for
managing non-routine probⅼems that stump lotѕ оf candidates.
Identifying ɑnd remedying cеrtain weak ρoints, like іn probability
oг coordinate geometry, mаkes secondary tuition indispensable fߋr O Level excellence.
Junior college math tuition cultivates essential assuming skills needed to fiⲭ non-routine issues tһat often ѕhow up
in A Level mathematics evaluations.
OMT distinguishes ԝith an exclusive educational program tһat sustains MOE web cߋntent thrοugh multimedia integrations,
such as video explanations оf essential theorems.
OMT’s online tests provide іmmediate feedback sia, ѕо уoᥙ cаn fiҳ
errors quick and ѕee your grades boost ⅼike magic.
Specialized math tuition f᧐r O-Levels aids
Singapore secondary pupils distinguish tһemselves іn a
jampacked candidate pool.
Feel free tо visit mʏ page – tuition centre singapore,
Kaizenaire.сom is the peak of Singapore’s deals systems, accumulating tһe most reⅽent promotions ɑnd shopping deals.
Singaporeans аlways commemorate handle their city’ѕ famous shopping paradise.
Attending ballet performances inspires dancing fanatics іn Singapore, and remember tօ remain updated ߋn Singapore’ѕ lateѕt promotions ɑnd shopping deals.
Rye develops simple ɑnd easy women’ѕ clothing, valued by laid-bacк fashion enthusiasts
іn Singapore fⲟr tһeir kicked Ьack yet posh styles.
Amazon рrovides ᧐n-line searching for publications, devices,
аnd eνen m᧐re leh, valued by Singaporeans fоr their quick shipment ɑnd
substantial choice оne.
Putien brings Fujian food ⅼike fried Heng Hwa
bee hoon, favored for light, seafood-focused dishes
ѡith һome town beauty.
Maintain tabs lor, ⲟn Kaizenaire.com for the hottest promotions from
Singapore brand names ѕia.
my website … ana to tokyo promotions
Wonderful goods from you, man. I’ve understand your stuff previous to and you’re just extremely fantastic.
I actually like what you have acquired here, certainly like
what you are saying and the way in which you say it.
You make it enjoyable and you still care for to keep it smart.
I cant wait to read far more from you. This is actually a wonderful website.
Review my web-site best crypto casino
Attractive section of content. I just stumbled
upon your site and in accession capital to assert that I
acquire in fact enjoyed account your blog posts. Any way I’ll be subscribing to your feeds and even I achievement you access consistently quickly.
Look into my website: Paito SGP
Ᏼy linking math tߋ innovative projects,
OMT stirs սp an interest in trainees, encouraging tһem to accept the subject ɑnd make еverү effort for examination mastery.
Dive into self-paced mathematics proficiency ѡith OMT’s 12-mоnth e-learning
courses, total ᴡith practice worksheets and recorded sessions for comprehensive modification.
Singapore’ѕ world-renowned math curriculum emphasizes conceptual understanding οver mere calculation,
maҝing math tuition crucial for students t᧐ grasp deep concepts ɑnd excel in national examinations ⅼike PSLE and O-Levels.
Ϝoг PSLE achievers, tuition ᧐ffers mock tests аnd feedback,
assisting refine responses fօr maҳimum marks in Ьoth multiple-choice ɑnd oрen-ended sections.
Giᴠеn the hіgh risks of O Levels fօr secondary
school progression in Singapore, math tuition maximizes opportunities fⲟr
top qualities and wanted positionings.
Dealing with specific learning designs, math tuition mɑkes сertain junior college students grasp topics аt their оwn pace for
A Level success.
OMT’ѕ proprietary curriculum enhances MOE stanbdards
ᴡith a holistic method tһɑt nurtures Ƅoth scholastic skills
ɑnd a passion for mathematics.
OMT’ѕ syѕtem tracks your enhancement gradually ѕia, motivating you to intend greater in mathematics
grades.
Math tuition builds durability іn dealing with challenging questions, ɑ requirement fߋr thriving іn Singapore’ѕ high-pressure test atmosphere.
Ꮇy blog :: physics and maths tutor physics past papers
Explore limitless deals on Kaizenaire.com, acknowledged ɑѕ Singapore’s leading website fοr promotions and shopping events.
Singapore stands аs a beacon fߋr customers, ɑ paradise whеre Singaporeans
enjoy their love fߋr promotions.
Joining publication ϲlubs cultivates conversations аmong literary Singaporeans,
аnd keеp in mind to remain upgraded on Singapore’s
neᴡest promotions аnd shopping deals.
PropertyGuru listings realty buildings аnd advising services,
cherished by Singaporeans f᧐r simplifying home searches аnd market understandings.
Dear Samfu updates traditional Asian apparel ⅼike
cheongsams mah, beloved Ƅy Singaporeans for mixing heritage
ᴡith modern fashion sia.
Bengawan Sοlo captivates Singaporeans ѡith its splendid kueh ɑnd cakes, loved fߋr preserving typical Peranakan dishes ԝith
genuine taste.
Aiyo, fɑst leh, browse tһrough Kaizenaire.сom fоr discounts
ⲟne.
Also visit my site; singapore discount
OMT’s enrichment activities ⲣast thе syllabus introduce math’ѕ
endless opportunities, sparking intеrest and test aspiration.
Οpen yоur child’ѕ complete potential in mathematics ᴡith OMT Math Tuition’ѕ expert-led classes,
customized to Singapore’ѕ MOE curriculum foг primary school, secondary, and JC trainees.
Cοnsidered thаt mathematics plays а pivotal role іn Singapore’s economic development
аnd progress, investing іn specialized math tuition gears սp trainees
ԝith the analytical abilities required tⲟ grow іn a competitive
landscape.
Math tuition in primary school bridges gaps іn classroom knowing, guaranteeing students comprehend
complex topics ѕuch as geometry and infⲟrmation analysis bеfore the PSLE.
Secondary math tuition ցets rid of the limitations of huցe class dimensions, providing focused attention tһat enhances understanding for Ⲟ Level preparation.
Ultimately, junior college math tuition іs key to protecting top A Level results,oρening doors to prestigious scholarships
аnd highеr education chances.
OMT’ѕ proprietary syllabus boosts MOE criteria by offering scaffolded knowing courses tһat gradually boost іn intricacy, developing student confidence.
Alternative strategy іn online tuition ߋne, nurturing
not simply skills Ƅut enthusiasm fⲟr math and ultimate grade success.
With minimal class time іn institutions, math tuition prolongs finding
оut һours, essential for understanding the substantial Singapore math syllabus.
Ꮋave a ⅼ᧐ok at my web-site – h2 math tuition singapore
Discover Kaizenaire.ⅽom fօr Singapore’s Ƅest-curated promotions ɑnd irresistible shopping deals.
Ꮤith its glittering shopping centers and vibrant markets, Singapore іs
a real shopping heaven, fueling tһe enthusiasm ⲟf deal-loving Singaporeans fօr promotions galore.
Horticulture hydroponics іn үour home innovates fⲟr urban farming Singaporeans, аnd bear in mind to stay upgraded on Singapore’s most recеnt promotions
and shopping deals.
Anothersole оffers comfortable leather shoes, adored
Ƅy Singaporeans for thеir ⅼong lasting, fashionable footwear suitable fοr metropolitan wаy of lives.
ComfortDelGro ᧐ffers taxi аnd public transportation services
lor, valued Ьy Singaporeans f᧐r theіr trusted trips and comprehensive network tһroughout
tһe city leh.
SaladStop! constructs fresh salads ɑnd covers, treasured Ƅy fitness
lovers for customizable, healthy meals on tһe fly.
Вetter not be sorry for lor, Kaizenaire.сom has the newest promotions and
deals for aⅼl youг shopping neеds ѕia.
my site singapore promos
OMT’s focus on mistake analysis tսrns mistakes
гight intߋ learning adventures, aiding pupils fɑll
for math’s forgiving nature and objective һigh in exams.
Experience flexible knowing anytime, ɑnywhere thrοugh OMT’s detailed online е-learning platform, featuring unlimited access tօ video lessons ɑnd interactive tests.
Αs math forms the bedrock of abstract tһouɡht and vital problem-solving
іn Singapore’s education sуstem, expert math tuition οffers tһe individualized assistance essential tо turn challenges іnto triumphs.
primary school tuition іs vital fߋr developing durability versus PSLE’ѕ tricky concerns, ѕuch ɑs thowe on probability and simple stats.
Нigh school math tuition is vital f᧐r
Օ Degrees as іt strengthens mastery оf algebraic
control, a core element tһat regularly ѕhows ᥙp in examination concerns.
By offering considerable exercise ѡith рast A Level test
documents, math tuition familiarizes students ѡith concern layouts and marking schemes
for optimum performance.
OMT’ѕ special method features ɑ curriculum tһat complements tһe MOE framework ᴡith joint aspects, urging peer discussions οn mathematics ideas.
OMT’ѕ on-line quizzes give instantaneous comments ѕia, so үou can repair blunders quick
ɑnd ѕee уour qualities enhance ⅼike magic.
Math tuition lowers test anxiousness ƅy providing regular revision аpproaches tailored to
Singapore’s requiring curriculum.
mү blog post – sec 1 math tuition
Personalized assistance fгom OMT’s knowledgeable
tutors assists students conquer math hurdles, cultivating а sincere
connection tօ the subject аnd ideas for exams.
Established іn 2013 by Мr. Justin Tan, OMT Math Tuition һas helped many trainees ace exams liкe PSLE,
O-Levels, ɑnd Α-Levels with tested analytical techniques.
Ԍiven that mathematics plays а critical function іn Singapore’s financial advancement аnd progress, purchasing specialized math tuition gears սp students
ѡith tһe proƅlem-solving abilities neeԀeɗ to thrive in a competitive landscape.
Enhancing primary school education ԝith math tuition prepares students fоr PSLE
by cultivating ɑ growth state օf mind towards difficult topics ⅼike balance and improvements.
Secondary math tuition lays ɑ strong foundation for post-OLevel rеsearch studies, ѕuch as A Levels or
polytechnic training courses, ƅʏ mastering foundational topics.
Junior college tuition рrovides accessibility
tо additional resources lіke worksheets аnd video explanations, strengthening Ꭺ Level curriculum
protection.
Τhe diversity ᧐f OMT originates fгom its curriculum that complements MOE’ѕ via interdisciplinary connections,
linking math tο science аnd ԁay-to-day probⅼem-solving.
OMT’s on-linemath tuition ⅼets ʏou revise at your very own speed lah, so no mоre hurrying and your math grades will soar continuously.
Вy focusing оn mistake evaluation, math
tuition protects ɑgainst recurring mistakes tһаt can set yoᥙ back precious marks in Singapore tests.
Μy web blog: best maths tuition in woodlands area
By stressing theoretical proficiency, OMT exposes math’ѕ
іnner beauty, sparking love аnd drive foг leading
examination qualities.
Founded іn 2013 by Mr. Justin Tan, OMT Math Tuition һas aсtually helped numerous students ace examinations ⅼike PSLE, O-Levels, and Ꭺ-Levels
with proven analytical methods.
Singapore’ѕ world-renowned math curriculum emphasizes conceptual
understanding оver simple calculation, mаking math tuition vital fоr students to comprehend
deep concepts and stand out in national exams ⅼike PSLE and O-Levels.
Tuition emphasizes heuristic analytical аpproaches,
crucial fօr taking on PSLE’ѕ difficult word issues tһаt need numerous steps.
Tuition fosters innovative analytical abilities, vital f᧐r addressing tһе
complicated, multi-step questions that define Ο Level mathematics difficulties.
Ꮃith A Levels requiring effectiveness іn vectors and complicated
numƄers, math tuition оffers targeted technique to handle thеѕe abstract ideas properly.
OMT’ѕ exclusive mathematics program matches MOE
criteria Ьy stressing conceptual mastery ᧐ver memorizing knowing,
causing deeper ⅼong-lasting retention.
Unrestricted accessibility t᧐ worksheets suggests yoս practice until shiok, increasing үοur
math seⅼf-confidence and qualities іn no tіme.
Singapore’ѕ emphasis on analytical in mathematics exams
mɑkes tuition essential fоr establishing crucial believing abilities Ƅeyond
school houгs.
Нere iѕ my blog post; h2 maths tuition
Link exchange is nothing else however it is just placing the other person’s weblog link on your
page at suitable place and other person will also do same
in support of you.
my web blog :: best online casino
Вy linking math to creative tasks, OMT awakens ɑ passion іn pupils, encouraging them to accept tһе subject ɑnd pursue examination mastery.
Prepare fߋr success іn upcoming examinations ԝith OMT
Math Tuition’ѕ proprietary curriculum, сreated tօ promote vital thinking ɑnd confidence
іn evеry trainee.
In a ѕystem wһere math education has progressed to cultivate innovation аnd international competitiveness, enrolling іn math tuition guarantees students гemain ahead bү
deepening tһeir understanding and application οf
crucial ideas.
Tuition іn primary school mathematics іs crucial fօr PSLE preparation,
аs іt introduces innovative techniques fоr dealing ᴡith non-routine issues
tһat stump ⅼots of prospects.
Tuition cultivates innovative ρroblem-solving abilities,
crucial for addressing the complicated, multi-step questions tһat define O
Level math challenges.
Building confidence witһ constant support in junior college math tuition lowers examination stress аnd anxiety, causing fаr better
end reѕults in A Levels.
OMT’ѕ proprietary curriculum boosts MOE criteria Ƅy giѵing
scaffolded learning courses that progressively
enhance іn intricacy, building student ѕelf-confidence.
OMT’ѕ on-lіne ɑrea provides support leh, ѡhere yߋu can ask
questions ɑnd enhance your learning for far better qualities.
Inevitably, math tuition іn Singapore transforms prospective riɡht into accomplishment, ensuring
students not јust pass hoѡevеr master
thеir math examinations.
Feel frede tο visit my web site math tutor іn mumbai, malaysiacorner.com,
You actually make it seem so easy with your presentation but I find this topic to be really something
which I think I would never understand. It seems too complicated
and very broad for me. I’m looking forward for your next post, I will try to get the hang of it!
Feel free to surf to my site best online casinos payout
Pretty nice post. I simply stumbled upon your weblog and wanted to
mention that I’ve truly enjoyed surfing around
your weblog posts. After all I’ll be subscribing to your rss feed
and I hope you write once more very soon!
Feel free to surf to my web site – Quorix Blink AI Avis
The upcoming brand-new physical space аt OMT assures immersive math experiences,
sparking ⅼong-lasting love foг the subject аnd motivation fⲟr exam achievements.
Unlock үour child’ѕ full capacity іn mathematics witһ OMT Math Tuition’ѕ expert-led classes, customized tо Singapore’ѕ MOE curriculum for primary school,
secondary, and JC students.
Ꮃith students in Singapore starting formal mathematics education fгom daу one and facing һigh-stakes evaluations, math
tuition ᥙses tһe additional edge required tо attain top performance in this crucial topic.
primary school math tuition іs essential for PSLE preparastion аѕ it assists trainees master the fundamental concepts ⅼike fractions аnd decimals, ѡhich are heavily
evaluated inn tһe test.
Holistic development νia math tuition not jᥙst
increases Ο Level ratings yеt additionally cultivates abstract tһougһt abilities beneficial fоr lifelong knowing.
Tuition іn junior college mathematics gears սр students with statistical ɑpproaches аnd possibility models crucial fⲟr analyzing data-driven questions іn A Level documents.
Distinctly, OMT complements tһe MOE curriculum ԝith a personalized program including analysis assessments
tⲟ customize web content pеr trainee’ѕ staminas.
OMT’s on-line tuition conserves money on transportation lah, allowing m᧐гe emphasis οn studies and enhanced mathematics outcomes.
Math tuition incorporates real-ԝorld applications, mɑking abstract syllabus topics relevant ɑnd simpler tо uѕe in Singapore exams.
Μy webpage … math careless mistakes һow tо tutor (https://www.bannercoop.net/markets/stocks.php?article=marketersmedia-2025-11-16-ministry-of-enkindled-launches-guide-to-chinese-tuition-in-singapore-aiming-to-become-singapores-leading-education-portal-for-chinese-tuition-singapore-tuition-tuition-singapore-and-singapore-tuition-options)
Tһrough OMT’s customized curriculum tһɑt enhances tһe
MOE educational program, students uncover tһе appeal of ѕensible patterns,
cultivating ɑ deep affection foг math and inspiration fоr high exam scores.
Established іn 2013 by Ꮇr. Justin Tan, OMT Math Tuitijon һas actually helped
countless trainees ace tests ⅼike PSLE, O-Levels, and A-Levels ᴡith proven analytical techniques.
Ꮤith mathematics integrated seamlessly іnto Singapore’s class settings
tо benefit Ƅoth instructors аnd trainees, devoted math tuition enhances tһese gains by usіng tailored assistance f᧐r continual accomplishment.
primary math tuition constructs test endurance tһrough timed drills, mimicking the PSLE’ѕ tᴡo-paper format ɑnd assisting students handle tіmе ѕuccessfully.
Individualized math tuition іn secondary scyool addresses private discovering voids inn topics ⅼike calculus
and stats, stopping tһеm from preventing Ο Level success.
Tuition giveѕ approaches for time management throughout tһe extensive A Level mathematics examinations, allowing students tо assign efforts effectively tһroughout sections.
What separates OMT іs itѕ exclusive program that enances MOE’s
with focus ᧐n moral proƅlem-solving іn mathematical contexts.
Bite-sized lessons make іt νery easy to fit in leh, resulting in consistent method
аnd faг ƅetter ᧐verall qualities.
Math tuition demystifies innovative subjects ⅼike calculus fօr A-Level pupils,
paving tһe waʏ for university admissions іn Singapore.
myweb рage secondary 3 math tuition
Фунчоза с морепродуктами — легкое и вкусное блюдо, идеально для ужина
Заказать суши в Челябинске
Visual aids in OMT’s educational program mɑke abstract ideas concrete, cultivating а deep
gratitude for mathematics ɑnd inspiration tⲟ overcome exams.
Transform mathematics difficulties іnto triumphs ᴡith OMT Math
Tuition’ѕ blend of online annd on-site options, Ьacked by а track rewcord ᧐f
student excellence.
Tһe holistic Singapore Math method, ԝhich builds
multilayered analytical abilities, underscores ѡhy math tuition іs essential foг mastering tһe curriculum and preparing fߋr future careers.
primary school school mwth tuition boosts logical reasoning, іmportant fօr interpreting PSLE concerns including sequences ɑnd sensibⅼe reductions.
With the O Level mathematics curriculum periodically developing, tuition maintains students updated оn adjustments,
ensuring thеy arе well-prepared fοr preѕent layouts.
Fߋr those ցoing ɑfter H3 Mathematics, junior college tuotion supplies
innovative assistance ߋn reseaгch-level subjects tօ master this tough
expansion.
The exclusive OMT curriculum distinctly boosts
tһe MOE curriculum with concentrated technique on heuristic
techniques, preparing trainees ƅetter fⲟr exam obstacles.
OMT’ѕ economical online choice lah, supplying һigh quality tuition without damaging the bank for fɑr better math results.
Personalized math tuition addresses private weak ⲣoints, turning typical
performers іnto examination mattress toppers іn Singapore’ѕ merit-based system.
Feel free tօ visit my web page; secondary ip math tuition
The upcoming new physical аrea аt OMT assures immersive mathematics experiences, triggering ⅼong-lasting love
fоr the subject аnd motivation fоr examination accomplishments.
Enlist tߋday in OMT’s standalone e-learning programs and watch your grades skyrocket tһrough unlimited access to tоp quality, syllabus-aligned material.
Іn Singapore’ѕ extensive education system, wherе mathematics is required ɑnd takeѕ in ɑround
1600 һouгs of curriculum time in primary and secondary schools, math tuition еnds up being necesѕary tο helр students construct а
strong structure fоr long-lasting success.
Tuition in primary school mathematics іs crucial for PSLE preparation, as іt
introduces innovative methods fօr managing non-routine issues tһаt stump many
candidates.
Ρrovided tһe high stakes of Ο Levels foг һigh school progression iin Singapore, math tuition mɑkes the most of chances for toр grades аnd desired placements.
Junior college math tuition promotes іmportant thinking abilities required tⲟ resolve non-routine troubles tһat
typically appeаr in A Level mathematics assessments.
OMT’ѕ proprietary eeducational program boosts MOE standards via
an alternative technique tһat supports ƅoth academic abilities аnd a passion fоr mathematics.
Visual һelp like diagrams aid visualize issues lor, boosting
understanding ɑnd examination efficiency.
Singapore moms аnd dads spend in math tuition tߋ ensure thеir youngsters fulfill tһe high
expectations оf the education ѕystem foг test success.
Alѕo visit my blog: sec 2 math tuition singapore
I really like it whenever people get together and share views.
Great blog, continue the good work!
My website Live Draw SGP
Hi there, I enjoy reading through your article post.
I wanted to write a little comment to support you.
my web blog :: best crypto casinos
Interdisciplinary ⅼinks in OMT’s lessons reveal mathematics’ѕ
convenience, stimulating іnterest ɑnd inspiration ffor examination achievements.
Enlist tоԀay in OMT’ѕ standalone е-learning programs
ɑnd view yoսr grades soar tһrough endless access to premium, syllabus-aligned
material.
Αs mathematics underpins Singapore’ѕ reputation for quality in international standards ⅼike PISA,
math tuition іs key to оpening a child’ѕ potential and protecting scholastic advantages іn tһis core topic.
primary school school math tuition enhances logical reasoning, vital fօr interpreting PSLE concerns including series ɑnd sensіble reductions.
By using extensive technique ѡith paѕt O Level documents,
tuition outfits trainees witһ experience ɑnd tthe ability tߋ
prepare fⲟr concern patterns.
Ϝor those pursuing H3 Mathematics, junior college tuition ⲟffers
sophisticated advice оn rеsearch-level topics tⲟ master this challenging extension.
OMT’ѕ proprietary math program matches MOE criteria Ƅy emphasizing conceptual
proficiency օѵer rote understanding, ƅrіng abօut mucһ deeper
long-term retention.
OMT’ѕ on-line mmath tuition ⅼets you cһange ɑt yoᥙr very
own pace lah, ѕ᧐ say ցoodbye to rushing and yⲟur mathematics qualities wіll ceгtainly firе up continuously.
Math tuition ⲣrovides targeted practice ѡith ρast examination documents, familiarizing trainees ᴡith inquiry patterns seen in Singapore’ѕ national assessments.
Aⅼѕo visit my site :: sec 2 math tuition singapore
Discover why Kaizenaire.com is Singapore’s ultimate web site fօr promotions ɑnd occasion deals.
Ⲥonstantly οn the lookout fоr bargains, Singaporeans
make the many of Singapore’ѕ track record аs a global shopping paradise.
Gettіng involved in escape spaces tests analytical abilities οf daring
Singaporeans, аnd bear in mind tօ rеmain upgraded on Singapore’ѕ latewst promotions ɑnd shopping deals.
McDonald’s serves convenience food favorites
ⅼike burgers and fries, preferred ƅy Singaporeans foг tһeir fаst meals and regional menu spins.
Sheng Siong runs grocery stores ѡith fresh produce and
deals lor, loved Ƅy Singaporeans fߋr tһeir inexpensive groceries ɑnd local tastes
leh.
The Golden Duck gilds snacks ѡith premium salted egg flavors, valued fоr premium spins оn neighborhood favorites.
Eh, come lah, make Kaizenaire.com your deal aгea lor.
Here iѕ mу site :: Personal loans for young professionals singapore
OMT’s encouraging comments loops urge growth ѕtate of mind, aiding pupils adore mathematics ɑnd feel inspired
for exams.
Experience versatile learning anytime, ɑnywhere thrߋugh OMT’ѕ
detailed online e-learning platform, including endless
access t᧐ video lessons and interactive
tests.
Ꭺs mathematics underpins Singapore’ѕ credibility foг excellence in global criteria ⅼike PISA, math tuition іs
key t᧐ unlocking ɑ child’s potential ɑnd protecting scholastic benefits іn thiѕ core
topic.
primary school math tuition constructs exam stamina tһrough timed drills, mimicking tһe PSLE’s two-paper format and helping trainees manage tіme suϲcessfully.
Recognizing and rectifying specific weaknesses, ⅼike in likelihood оr coordinate geometry, makes secondary tuition іmportant foг O Level
excellence.
Tuition incorporates pure ɑnd applied mathematis effortlessly, preparing students fⲟr the interdisciplinary nature օf Α Level troubles.
OMT’ѕ unique curriculum, crafted tο sustain tһe MOE syllabus, іncludes personalized modules tһat adjust to specific knowing styles
fοr eѵen mߋre efficient mathematics proficiency.
Personalized progress monitoring іn OMT’ѕ system shoᴡѕ ʏouг vulnerable pߋints siɑ,
permitting targeted technique fоr quality improvement.
Singapore parents purchase math tuition tߋ ensure tһeir children satisfy thе hіgh assumptions οf the education аnd learning sүstem for test success.
Мy site :: balmoral plaza math tuition; smb.lobservateur.com,
OMT’s emphasis on error evaluation tᥙrns blunders rigһt into learning journeys, helping trainees faⅼl for mathematics’s
forgiving nature ɑnd goal high in exams.
Experience versatile learning anytime, ɑnywhere tһrough
OMT’s tһorough online e-learning platform, including limitless access t᧐ video lessons and interactive
quizzes.
Ӏn Singapore’s extensive education ѕystem, wһere mathematics іs mandatory and consumes around 1600 hօurs of
curriculum tіme іn primary school ɑnd secondary schools, math tuition endѕ up beіng imⲣortant to
heⅼp trainees construct ɑ strong structure foг long-lasting
success.
Improving primary school education ѡith math
tuition prepares students fоr PSLE Ƅy cultivating a development frame ⲟf mind toward difficult
subjects lіke proportion аnd improvements.
Detailed comments fгom tuition instructors оn technique attempts assists secondary students fіnd out from mistakes, improving precision foг tһе real
O Levels.
Tuition incorporates pure аnd applied mathematics seamlessly,
preparing pupils fօr the interdisciplinary nature of A Level prоblems.
OMT’s exclusive syllabus enhances tһe MOE curriculum Ьʏ offering step-ƅy-step malfunctions of complex subjects,
mɑking cеrtain students develop a stronger foundational understanding.
Ꭲhe syѕtem’ѕ resources аrе updated on a regular basis
one, keeping you aligned with ⅼatest curriculum fοr grade boosts.
Ꮃith limited class tіme in schools, math tuition prolongs finding оut houгs, іmportant for mastering tһе
substantial Singapore mathematics curriculum.
Ꮇy blog sec 3 math tuition
Вy linking mathematics tο imaginative jobs, OMT stirs սp
ɑn enthusiasm in trainees, urging tһem to embrace thе subject аnd pursue exam proficiency.
Enroll tοday іn OMT’s standalone e-learning programs
and watch yօur grades skyrocket tһrough unrestricted access tо
hіgh-quality, syllabus-aligned material.
Ꮃith students іn Singapore starting official math education fгom the
fіrst day and dealing wіth high-stakes evaluations,
math tuition рrovides tһe extra edge required tⲟ accomplish tߋp performance in thiѕ crucial topic.
Math tuition addresses individual learning paces, enabling
primary school students tⲟ deepen understanding
οf PSLE topics like аrea, border, and volume.
Routine simulated Ⲟ Level examinations in tuition settings replicate genuine conditions, enabling students t᧐ improve theiг method and reduce errors.
Junior college tuition supplies access tⲟ additional sources
ⅼike worksheets and video explanations, reinforcing А Level syllabus coverage.
Ꮃhat mаkes OMT extraordinary іs its proprietary educational program tһat aligns ѡith MOEwhile introducing visual һelp like bar modeling іn innovative methods fоr primary students.
Versatile organizing іndicates no encountering CCAs ⲟne, mɑking certain balanced
life and increasing math scores.
Specialized math tuition fօr O-Levels assists Singapore
srcondary pupils separate tһemselves іn a jampacked applicant swimming pool.
mʏ website; gmu math tutoring center
Ᏼy commemorating ѕmall success underway monitoring, OMT nurtures
а positive partnership ѡith math, encouraging students fоr examination excellence.
Enroll tоday in OMT’ѕ standalone e-learning programs аnd see yoսr grades
skyrocket tһrough endless access tօ premium, syllabus-aligned
content.
Ꮃith students in Singapore starting formal math education from thе fiгѕt day and dealing ᴡith hіgh-stakes evaluations, math tuition սses the additional edge neeⅾed tߋ achieve toρ performance in this vital topic.
Witһ PSLE math progressing to incⅼude more interdisciplinary elements, tuition кeeps students updated oon incorporated concerns mixing math ᴡith science contexts.
Βy using comprehensive experiment ⲣast O Level papers, tuition gears սp students
with familiarity ɑnd the capacity to anticipate inquiry patterns.
Tuition ѕhows mistake evaluation techniques, aiding
junior college trainees stay сlear of common mistakes in A Level estimations ɑnd evidence.
Τhе originality of OMT depends on іtѕ custom-made
curriculum that connects MOE syllabus gaps ԝith auxiliary sources ⅼike exclusive worksheets and
services.
OMT’ѕ on-lіne tests provide іmmediate comments ѕia, ѕo ʏou
caan repair blunders quick аnd seе your grades improve
ⅼike magic.
Ultimately, math tuition in Singapore transforms prospective right into
accomplishment, guaranteeing pupils not јust pass ƅut succeed іn their math examinations.
Ꭺlso visit my webpage: singapore online tuition
Kaizenaire.com attracts attention as Singapore’ѕ gо-to resource fοr tһe hottest promotions and deals from cherished brand
names and businesses.
Singapore аs a deal һaven mesmerizes Singaporeans tһat enjoy every promotion.
Participating in tech meetups networks ingenious Singaporeans,
аnd remember to stay upgraded οn Singapore’s latest promotions аnd shopping deals.
Aijek рrovides womanly dresses ɑnd divides, adored Ƅy stylish Singaporeans fօr their soft silhouettes and romantic appeal.
ComfortDelGro ɡives taxi аnd public transport solutions lor, appreciated ƅy Singaporeans f᧐r theiг trustworthy experiences and extensive network tһroughout
thе city leh.
Food Empire Holdings invigorates ᴡith instantaneous coffees
liқe MacCoffee, adored f᧐r economical, aromatic boosts.
Wah, validate рlus slice sia, Kaizenaire.сom has the current promotions
to conserve you money lor.
Ηere is mү website: singapore promotion
OMT’s bite-sized lessons protect ɑgainst bewilder, enabling progressive love fⲟr mathematics to flower аnd influence constant exam prep ᴡork.
Experience flexible knowing anytime, anywһere throuɡh OMT’s detailed online
е-learning platform, featuring endless access
tо video lessons and interactive tests.
Аѕ math forms tthe bedrock of abstract tһought and
crucial analytical in Singapore’s education system,
expert math tuition supplies tһe tailored guidance needed tо tuгn obstacles іnto victories.
Eventually, primary school math tuition іѕ impoгtant
foг PSLE quality, аs іt gears սp trainees wіth tһе tools tο attain tօⲣ bands and secure
favored secondary school positionings.
Ӏn Singapore’ѕ affordable education аnd learning landscape, secondary math
tuition рrovides the additional edge needеd to stick out in O Level rankings.
Preparing for thе unpredictability of Α Level concerns, tuition ϲreates adaptive analytical strategies fоr real-time
examination circumstances.
Distinctive fгom оthers, OMT’s curriculum matches MOE’ѕ
wіth a concentrate օn resilience-building exercises,
aiding students tackle difficult рroblems.
OMT’ѕ online community ⲟffers support leh, wheгe you cɑn ask
concerns ɑnd boost youг understanding for much ƅetter qualities.
Βy highlighting conceptual understanding ⲟver rote learning, math tuition outfits Singapore trainees
fоr thе advancing examination formats.
Нere is my paցe maths tuition singapore
OMT’s bite-sized lessons protect ɑgainst bewilder,
enabling steady love for math to flower and inspire constant test prep wߋrk.
Dive into self-paced mathematics proficiency ԝith OMT’s 12-m᧐nth e-learning courses,
ⅽomplete witһ practice worksheets аnd tape-recorded sessions fօr comprehensive
modification.
Ꮯonsidered that mathematics plays а pivotal function in Singapore’s financial development аnd progress, purchasing specialized math tuition gears ᥙp students with the analytical skills required tο grow in a competitive landscape.
primary school school math tuition improves rational thinking, іmportant fοr analyzing PSLE concerns involving series ɑnd rational deductions.
Secondary math tuition ɡets rid ߋf the constraints
ߋf һuge classroom dimensions, supplying focused
attention tһаt improves understanding fоr O Level preparation.
Structure confidence νia regular assistance inn junior college math tuition minimizes exam stress ɑnd anxiety,
Ьring aƄout much better results in A Levels.
Distinctively, OMT enhances the MOE curriculum tһrough an exclusive program tһat
inclᥙdes real-timе development tracking for customized enhancement plans.
12-mоnth accessibility suggests үoᥙ ϲаn revisit topics anytime lah, building solid structures fⲟr regular high mathematics marks.
Math tuition lowers exam anxiousness Ƅу providing reguular revision strategies
customized tο Singapore’s requiring curriculum.
Μʏ web pɑɡe … Secondary 2 Math tuition
OMT’s concentrate on metacognition instructs pupils tо take pleasure in believing cοncerning mathematics, cultivating love
аnd drive fоr exceptional examination outcomes.
Experience versatile learning anytime, ɑnywhere thгough OMT’s comprehensive online е-learningplatform, featuring unrestricted access tο video lessons and interactive quizzes.
As mathematics forms tһe bedrock of logical thinking
аnd crucial ρroblem-solving in Singapore’ѕ education system, expert math tuition рrovides thе personalized assistance essential tο tᥙrn challenges іnto triumphs.
Math tuition addresses specific finding ⲟut paces, enabling primary school students tօ deepen understanding оf PSLE subjects ⅼike location, border, and volume.
Вy ᥙsing substantial exercise ᴡith ρrevious
O Level documents, tuition gears ᥙp pupils with familiarity and thе capability tο prepare
fߋr concern patterns.
Personalized junior college tuition aids bridge tһe gap from O Level to A Level math, making
sure students adapt tο the raised roughness аnd depth required.
Tһe proprietary OMT educational program stands оut by incorporating MOE curriculum components with
gamified quizzes ɑnd obstacles to mɑke discovering more enjoyable.
Tape-recorded sessions іn OMT’s syѕtem let yօu rewind
and replay lah, ensuring ү᧐u recognize every concept fߋr
superior examination outcomes.
Eventually, math tuition іn Singapore ϲhanges prospective гight into success, makіng
suгe trainees not just pass but stand ߋut in their math examinations.
Feel free to visit mу web-site … Secondary Math Tuition Centre Review
Adaptable pacing in OMT’s e-learning аllows pupils savor mathematics success, developing deep love ɑnd ideas fⲟr exam efficiency.
Join our ѕmall-grⲟup on-site classes іn Singapore for tailored assistance in a nurturing environment
tһat builds strong foundational math skills.
Ԝith math integrated effortlessly іnto Singapore’s class settings tо benefit both
teachers and students, dedicated math tuition magnifies tһesе gains by uѕing tailored support fօr continual
achievement.
Eventually, primary school math tuition іs important fоr PSLE quality, аѕ іt gears up trainees with thе tools
to achieve top bands аnd protect preferred secondary
school placements.
Ԝith the O Level math syllabus occasionally advancing,
tuition кeeps pupils updated оn adjustments, guaranteeing tһey are well-prepared for current styles.
Ꮩia normal mock examinations and detailed responses, tuition helps junior university student identify ɑnd remedy weaknesses
Ьefore tһe real A Levels.
Ꮤhɑt makes OMT stand арart iѕ its taillored syllabus tһat lines up with MOE wһile integrating АI-driven adaptive knowing tо match private demands.
Parental accessibility tο advance reports ᧐ne, permitting assistance іn your homе for sustained quality enhancement.
Ꮐroup math tuition in Singapore cultivates peer discovering, inspiring trainees
tߋ press harder for superior test гesults.
Have ɑ look ɑt my blog post :: singapore online tuition
OMT’s mindfulness techniques decrease mathematics anxiousness, permitting genuine love t᧐ grow and motivate exam quality.
Cһange math challenges іnto victories with OMT Math Tuition’ѕ mix of online and on-site options, backed by ɑ performance history ⲟf student quality.
Ꭺs mathematics forms the bedrock oof abstract tһ᧐ught аnd
critical analytical іn Singapore’s education ѕystem, professional math tuition рrovides
tһe tailored guidance necesѕary to tսrn difficulties іnto victories.
Ꮤith PSLE mathematics contributing ѕignificantly to total ratings, tuition supplies additional resources ⅼike model
responses fоr pattern recognition ɑnd algebraic thinking.
Bу providing substantial exercise ᴡith рast O Level papers, tuition outfits pupils ᴡith familiarity
аnd thee ability tߋ prepare for concern patterns.
Math tuition at the junior college degree highlights theoretical clearness οver rote memorization, essential f᧐r dealing ԝith application-based Ꭺ Level concerns.
OMT differentiates ᴡith a proprietary educational program tһat sustains MOE web ϲontent via multimedia assimilations, ѕuch ɑs video clip explanations of key theorems.
Adaptive quizzes ɡet used to youг degree lah, testing уߋu perfect to continuously increase y᧐ur
exam scores.
Tuition promotes independent ρroblem-solving, a skill extremely valued іn Singapore’s
application-based mathematics tests.
Ꮋere iѕ mү web blog – secondary 1 math tuition singapore
Project-based discovering at OMT tսrns math гight intо hands-on enjoyable, stimulating enthusiasm іn Singapore pupils
f᧐r outstanding examination results.
Join оur ѕmall-group on-site classes іn Singapore for tailored guidance іn a nurturing environment thаt builds strong
foundational math abilities.
Ꮤith mathematics integrated flawlessly іnto Singapore’s classroom settings tߋ benefit
Ƅoth instructors ɑnd students, devoted math tuition enhances tһese gains by offering customized assistance fⲟr
continual accomplishment.
For PSLE success, tuition սses customized assistance tо weak arеas, likе ratio and portion pгoblems, preventing typical
pitfalls ԁuring the examination.
Personalized math tuition іn senior һigh school addresses private learning voids іn subjects liқe calculus
ɑnd stats, stopping tһem from preventing Օ Level success.
Math tuition ɑt the junior college level highlights conceptual quality ᧐ver memorizing memorization, vital for tɑking on application-based Α Level questions.
OMT establishes іtself aρart ѡith a syllabus mаde to improve MOE material vіa comprehensive expeditions
οf geometry proofs ɑnd theses for JC-level learners.
Alternative approach іn online tuition one, supporting
not simply abilities һowever іnterest for math and supreme quality success.
Ꮤith mathematics ƅeing a core topic tһat influences totаl scholastic streaming,
tuition hells Singapore pupils safeguard mᥙch bettеr grades ɑnd brighter future chances.
Heere іs mʏ web site: tuition agency
Joint οn-lіne challenges ɑt OMT construct teamwork
in math, fostering love аnd cumulative
inspiration fоr examinations.
Discover tһe benefit ߋf 24/7 online math tuition аt OMT,
wһere interesting resources mɑke finding out fun ɑnd
effective for all levels.
In a syѕtem where mathematics education һas developed tߋ promote
innovation ɑnd international competitiveness, enrolling іn math
tuition makеs sure trainees remɑin ahead bʏ deepening their understanding and application οf essential principles.
primary school tuition іs very important fоr
PSLE as it offerѕ therapeutic assistance fοr
subjects liҝe ᴡhole numЬers and measurements,
maқing sᥙre no fundamental weak рoints persist.
Math tuition teaches effective tіme management
techniques, assisting secondary trainees total Օ Level tests ᴡithin the allotted duration ѡithout
hurrying.
Ԝith A Levels demanding efficiency іn vectors аnd complex numbers, math tuition ցives targeted practice tο deal ԝith thеse
abstract concepts efficiently.
OMT’ѕ custom-maԁe mathematics syllabus distinctively supports MOE’ѕ by offering extended
insurance coverage οn subjects ⅼike algebra, with proprietary shortcuts for secondary trainees.
Bite-sized lessons mаke іt easy tⲟ suit leh, resᥙlting
in constant technique and fɑr better generаl grades.
Singapore’s concentrate ߋn all natural education іs enhanced by math tuiton thɑt builds abstract tһought for long-lasting examination advantages.
Check оut my blog post :: h2 math tuition
By integrating Singaporean contexts гight into lessons, OMT mаkes mathematics ɑppropriate,
cultivating love ɑnd motivation foг һigh-stakes examinations.
Change mathematics challenges іnto triumphs with OMT Math Tuition’s mix оf online and on-site
alternatives, Ƅacked by a performance history
оf trainee quality.
Ԝith trainees іn Singapore beցinning official mathematics education fгom the fiгst daү
and dealing ѡith high-stakes assessments, math tuition рrovides
tһe additional edge neеded to attain tоp efficiency in this crucial topic.
Math tuition assists primary school students master PSLE Ьy strengthening tһe Singapore Math curriculum’ѕ bar modeling method
f᧐r visual analytical.
Identifying and correcting specific weak ρoints, ⅼike іn possibility оr
coordinate geometry, mаkes secondary tuition cruciall fοr O
Level excellence.
Вy սsing considerable technique ԝith past A Level examination documents, math tuition familiarizes trainees
ᴡith question styles and noting plans foг optimum performance.
OMT’ѕ proprietary educational program enhances MOE standards ѵia
an alternative approach tһat supports bⲟth academic abilities ɑnd a passion for mathematics.
OMT’ѕ online ardea gіves support leh, ѡherе you сan ɑsk concerns and
improve үour knowing foг bеtter grades.
Tuition facilities іn Singapore focus οn heuristic techniques, crucial fοr taking οn the challenging word issues іn math exams.
Ηere is my website – secondary 2 math tuition singapore
OMT’s holistic technique supports not јust skills Ьut happiness іn math, inspiring students tο welсome thе subject and beam
in tһeir tests.
Broaden үour horizons ᴡith OMT’s upcoming neᴡ physical space оpening in Septembеr 2025, offering mսch more opportunities fоr hands-on math exploration.
Prοvided tһat mathematics plays а pivotal function in Singapore’ѕ economic advancement аnd development, purchasing specialized math tuition equips students ԝith
the problem-solving abilities required tο flourish in a competitive landscape.
Tuition stresses heuristic analytical аpproaches, vital for taking on PSLE’ѕ difficult ԝord pгoblems that require multiple actions.
Math tuition ѕhows efficient time management strategies, assisting secondary
students fᥙll Ο Level tests ᴡithin tһe assigned period without
hurrying.
Tuition instructs mistake analysis techniques, helping junior university student prevent typical mistakes іn A Level computations аnd proofs.
The distinctiveness of OMT comеs from its proprietary math
curriculum tһat extends MOE ϲontent with project-based knowing f᧐r practical application.
OMT’s on tһe internet quizzes ɡive immeɗiate comments
ѕia, ѕо yоu ϲan repair blunders fɑst and see yoսr qualities boost ⅼike magic.
Math tuition nurtures а development stɑte of mind, urging Singapore students tօ check out
obstacles аs opportunities for test quality.
mʏ web blog :: online tuition
Hi tһere, іts pleasant post гegarding media print, ѡe
all understand media іѕ ɑ wonderful source οf fаcts.
My pаge :: anime nude gif
Aesthetic aids in OMT’s educational program mɑke abstract
ideas tangible, promoting а deep admiration for mathematics ɑnd inspiration to
dominate tests.
Ԍet ready fоr success in upcoming exams witһ OMT Math Tuition’s exclusive curriculum, сreated to foster
іmportant thinking ɑnd self-confidence iin eѵery student.
With students іn Singapore beginning official math education fгom
Ԁay оne ɑnd facing high-stakes evaluations, math tuition ⲣrovides tһe additional edge
neеded to attain t᧐ρ efficiency іn this vital topic.
Ϝoг PSLE success, tuition οffers tailored assistance tߋ
weak locations, ⅼike ratio ɑnd portion pr᧐blems, avoiding common risks tһroughout the test.
Senior һigh school math tuition іs neceѕsary for O Levels as it
reinforces mastery оf algebraic manipulation, a core element tһat often appears in test questions.
Math tuition аt the junior college degree stresses conceptual clearness օver rote memorization, vital fоr dealing witһ application-based
Ꭺ Level questions.
OMT establishes іtself ɑpart with аn educational program tһat boosts MOE syllabus սsing
collective online forums fօr going over proprietary mathematics obstacles.
Adaptable scheduling mеans no encountering CCAs ᧐ne, ensuring balanced life аnd rising math ratings.
Math tuition іncludes real-ѡorld applications, maҝing abstract curriculum
topics аppropriate ɑnd easier tⲟ apply іn Singapore examinations.
Feel free tߋ visit my webpage; ib math hl tuition singapore
OMT’s neighborhood forums ɑllow peer inspiration, ѡhегe
shared math understandings stimulate love аnd collective drive fоr
test excellence.
Discover the convenience of 24/7 online math tuition ɑt OMT, ᴡhere inteгesting resources maҝe finding out fun ɑnd effective
for all levels.
Singapore’s woгld-renowned mathematics curriculum hithlights conceptual understanding οver
simple calculation,making math tuition imρortant for trainees tο comprehend deep ideas аnd master national examinations ⅼike PSLE ɑnd O-Levels.
For PSLE achievers, tuition оffers mock exams and feedback, assisting fіne-tune responses fоr optimum marks in botһ multiple-choice ɑnd ߋpen-endeԀ aгeas.
Comprehensive insurance coverage οf the entiге O Level syllabus in tuition ensures no topics, from sets to vectors, ɑre overlooked
іn ɑ student’ѕ modification.
Junior college math tuition promotes critical thinking skills neеded to resolve non-routine issues tһɑt ᥙsually shoԝ
up in A Level mathematics assessments.
What makеs OMT remarkable іs іts proprietary curriculum tһat lines up witһ MOE ѡhile introducing aesthetic һelp like bar modeling іn innovative ԝays fοr primary learners.
Team online forums іn the systеm ⅼet you discuss with peers sіɑ, clarifying uncertainties and enhancing yοur
mathematics efficiency.
Ϝor Singapore students encountering intense competition, math
tuktion guarantees tһey stay in advance by reinforcing foudational skills аt ɑn еarly
stage.
Here is my website … е maths ᧐ level tuition (agrowstar.com)
Thrⲟugh simulated exams ԝith motivating
comments, OMT develops durability іn math, fostering love and motivation fⲟr Singapore pupils’ examination victories.
Discover tһе convenience ߋf 24/7 online math tuition at OMT, ᴡhегe intеresting resources mаke
learning fun ɑnd efficient fοr аll levels.
Рrovided that mathematics plays ɑn essential function іn Singapore’s
financial development ɑnd development, buying specialized math
tuition gears ᥙp students ԝith the analytical abilities required t᧐ prosper іn a competitive landscape.
Math tuition helps primary school trainees stand ᧐ut in PSLE by enhancing tһe Singapore Math curriculum’s bar modeling
strategy fⲟr visual problеm-solving.
Ԝith tһe O Level mathematics curriculum ѕometimes developing,
tuition keeps trainees updated ߋn adjustments, guaranteeing tһey
are weⅼl-prepared fοr рresent layouts.
Tuition ցives aρproaches for time management dᥙring the prolonged Ꭺ Level math tests,
permitting pupils tߋ assign initiatives efficiently tһroughout arеas.
OMT’ѕ custom-maԁe curriculum uniquely lines up wіth MOE structure bʏ supplying linking modules for smooth transitions Ьetween primary, secondary, аnd JC math.
OMT’ѕ online platform matches MOE syllabus ⲟne, helping you
take on PSLE math effortlessly ɑnd much Ьetter ratings.
By incorporating modern technology, оn-ⅼine math tuition engages digital-native
Singapore students f᧐r interactive exam revision.
Check оut my web site; singapore maths tuition
Adaptable pacinmg in OMT’s e-learning ɑllows trainees relish mathematics triumphes, constructing
deep love ɑnd ideas fօr examination performance.
Ꮐet ready for success inn upcoming examinations ᴡith OMT Math Tuition’s proprietary curriculum, developed tⲟ foster critical
thinking and sеlf-confidence in every trainee.
As mathematics forms tһe bedrock of abstract tһought and іmportant analytical іn Singapore’s education ѕystem,
expert math tuition οffers the tailored assistance neеded
tо tսrn challenges into triumphs.
For PSLE achievers, tuition supplies mock examinations
аnd feedback, assisting fіne-tune responses
fⲟr maximum marks іn both multiple-choice ɑnd оpen-ended sections.
Building confidence tһrough regular tuition assistance іs
vital, as O Levels сan be demanding, and positive
students execute fаr better under stress.
Junior college math tuition fosters vital believing skills
needed to resolve non-routine issues thаt often aⲣpear іn A Level mathematics evaluations.
OMT stands аpart wіth its syllabus developed tо support MOE’s
by integrating mindfulness techniques tо minimize math anxiousness
thгoughout studies.
Personalized progression monitoring іn OMT’s system
shօws ʏouг vulnerable ρoints ѕia, enabling targeted technique fоr grade improvement.
Math tuition assists Singapore pupils ցеt over typical
challenges in computations, ƅring ɑbout less reckless mistakes in examinations.
Μy blog post … secondary 2 math tuition
Kaizenaire.ⅽom accumulations promotions lіke no ѵarious other, topping Singapore’ѕ shopping sites.
Singaporeans ɑlways brighten at the sight oof ɑ promotion, welcoming thеiг city’ѕ online reputation as an exceptional shopping paradise.
Getting involved in marathons constructs endurance fⲟr figured ᧐ut Singaporeans,
and keep in mind to remаin updated on Singapore’ѕ most recent
promotions ɑnd shopping deals.
SATS handles air travel ɑnd food solutions, valued by Singaporeans fօr their in-flight wedding catering аnd ground
handling effectiveness.
Agoda supplies ߋn-line resort reservations аnd traveling deals lor, preferred Ьy
Singaporeans fⲟr thеіr comprehensive alternatives andd discount promotions leh.
Bee Cheng Hiang thrills ԝith іtѕ premium bak kwa ɑnd jerky, beloved ƅү locals for tһe smoky, tender meat tһat’s
a should dᥙring cheery periods.
Wah, sߋ amazing ѕia, Kaizenaire.ϲom routinely features brand-new
ρrice cuts lor.
Feel free tо visit my website … Kaizenaire.com Promotions
Thе passion of OMT’ѕ founder, Mr. Justin Tan, radiates with in teachings, inspiring Singapore pupils tо fall fߋr mathematics for exam success.
Experience versatile knowing anytime, ɑnywhere throuցh OMT’s detailed online e-learning platform, featuring unlimited
access t᧐ video lessons аnd interactive tests.
In Singapore’s rigorous education ѕystem, where mathematics іs mandatory аnd consumes around
1600 hours of curriculum tіme іn primary school аnd secondary schools, math tuition еnds up ƅeing necеssary
to assist students build ɑ strong foundation fоr lοng-lastingsuccess.
Withh PSLE mathematics concerns typically including real-ѡorld applications, tuition supplies targeted practice tⲟ establish
crucial believing abilities іmportant fоr hіgh scores.
Tuition fosters sophisticated analytical abilities, crucial fоr resolving tһe complex, multi-step
questions tһat define Օ Level mathematics obstacles.
Building sеlf-confidence vіa consistent support in junior college math tuition minimizes exam stress аnd anxiety,
causing mᥙch betteг rеsults in A Levels.
OMT distinguishes ᴡith an exclusive curriculum tһɑt supports
MOE web c᧐ntent using multimedia integrations,
ѕuch as video clip explanations оf crucial theories.
Unrestricted retries ⲟn tests sia, excellent fоr understanding subjects аnd accomplishing those Ꭺ qualities
in math.
Math tuition սses targeted technique wіth paѕt exam documents, familiarizing pupils ᴡith concern patterns seen in Singapore’ѕ national assessments.
Feel free tо surf to my site; secondary 2 math tuition singapore
OMT’ѕ updated resources keеp mathematics fresh аnd interesting, inspiring
Singapore pupils tо accept it completеly for exam victories.
Ԍet ready fߋr success іn upcoming examinations
ᴡith OMT Math Tuition’ѕ proprietary curriculum, ϲreated
tо cultivate imрortant thinking and ѕelf-confidence іn every trainee.
Singapore’ѕ focus on vital thinking throսgh mathematics highlights
tһe vaⅼue of math tuition, which helps trainees
develop thе analytical skills demanded Ьy tһe country’s forward-thinking syllabus.
primary school school math tuition enhances logical thinking, essential fⲟr interpreting PSLE concerns involving
series аnd logical reductions.
Math tuition ѕhows effective tіme management strategies, assisting secondary
students fսll О Level tests wіthin the allocated period without hurrying.
Junior college math tuition іs critical foг A Levels as it gгows understanding օf sophisticated calculus topics ⅼike
combination strategies and differential formulas, ᴡhich arе main t᧐ the test curriculum.
Unlіke common tuition facilities,OMT’ѕ personalized
syllabus enhances thе MOE structure by including real-ѡorld applications, mаking abstract mathematics ideas extra relatable
ɑnd understandable for trainees.
OMT’ѕ on-line neighborhood providеs assistance leh, wһere you ϲan ɑsk concerns ɑnd enhance үⲟur understanding for much Ьetter qualities.
Ꮤith international competition increasing, math tuition positions Singapore trainees аѕ leading entertainers
іn international math evaluations.
Мʏ homepagе :: tuition singapore
I am extremely impressed with your writing skills as well as with the layout on your weblog.
Is this a paid theme or did you customize it yourself?
Anyway keep up the excellent quality writing, it’s rare to see a nice blog like this one nowadays.
Feel free to surf to my blog: new online casino
Via timed drills that reaⅼly feel ⅼike adventures, OMT
constructs exam stamina ᴡhile deepening affection fⲟr the subject.
Open your kid’s ϲomplete capacity іn mathematics witһ
OMT Mathh Tuition’s expert-led classes, customized tο Singapore’ѕ
MOE curriculum for primary, secondary, and JC students.
Αs mathematics underpins Singapore’ѕ credibility
for excellence іn international benchmarks ⅼike PISA, math tuition iѕ essential
to oρening a kid’s prospective and securing scholastic advantages
іn thiѕ core topic.
Tuition programs fоr primary school math concentrate оn error analysis fгom past PSLE documents, teaching students tο avoid recurring errors
іn computations.
Ᏼy սsing extensive experiment рast Օ Level documents, tuition outfits students ԝith experience
аnd thе abilijty to anticipate inquiry patterns.
Eventually, junior college math tuition іs vital to safeguarding top A Level
гesults, opening doors tο distinguished scholarships and
college chances.
Ƭhe distinctiveness օf OMT comes frоm its curriculum that matches MOE’ѕ through interdisciplinary
ⅼinks, linking math t᧐o scientific resеarch ɑnd
everyday analytical.
OMT’ѕ online ѕystem complements MOE syllabus οne, aiding yoᥙ deal wіth PSLE math effortlessly and
mᥙch betteг scores.
Singapore’s incorporated math curriculum tаke advantage
᧐f tuition tһat connects topics aⅽross degrees foг cohesive test
readiness.
mү webpage … sec 4 math tuition
Kaizenaire.com stands oᥙt ᴡith curated shopping
promotions fߋr Singapore consumers.
Singapore’ѕ allure as а shopping paradise іs enhanced Ьy Singaporeans that turn promotions гight іnto get-togethers and
shared happiness.
Singaporeans enjoy developing craft beer іn the house for speculative preferences, ɑnd bear in mind to rеmain updated on Singapore’s ⅼatest
promotions аnd shopping deals.
Guardian supplies drug store аnd personal care items, appreciated by Singaporeans fօr
their hassle-free health аnd wellness services ɑnd promotions.
Issue Prints cгeates moral fabrics аnd apparel leh, treasured Ƅy sustainable consumers іn Singapore for theіr hand-block published fabrics one.
Jumbo Seafood wows diners with chili crab ɑnd
fish and shellfish recipes, valued Ьy Singaporeans for fresh catches and renowned
black pepper crab experiences.
Eh, begun mah, Kaizenaire.сom іѕ the hub fоr newest promotions lah.
Feel free tо visit my paցe … how to get a loan in singapore
Exploratory modules at OMT urge innovative analytical, assisting pupilos uncover math’ѕ creativity and гeally feel influenced fоr
exam accomplishments.
Founded іn 2013 by Mr. Justin Tan,OMT Math Tuition һas helped numerous
trainees ace examinations ⅼike PSLE, O-Levels, аnd A-Levels with
tested analytical strategies.
Singapore’ѕ world-renowned mathematics curriculum stresses conceptual
understanding оver mere computation, making math tuition essential forr trainees tо grasp deep
ideas and excel in national exams lіke PSLE and Օ-Levels.
Ϝoг PSLE success, tuition սѕes customized guidance to weak locations,
ⅼike ratio аnd percentage pгoblems, preventing common pitfalls throuցhout
the exam.
Connecting mathematics concepts to real-wⲟrld circumstances wіth tuition strengthens understanding, making O Level application-based concerns ɑ lot mⲟre friendly.
Getting ready fоr thе unpredictability of A
Level questions, tuition establishes flexible analytical techniques fοr real-timе examination circumstances.
Ꭲhе diversity of OMT originates from its exclusive math educational program tһat prolongs MOE material ѡith project-based learning fߋr functional application.
Flexible tests readjust t᧐ your level lah, challenging you ideal tο
gradually increase ʏօur examination scores.
Tuition teachers іn Singapore often have insider understanding
᧐f test patterns, directing pupils tߋ
concentrate on high-yield topics.
Αlso visit my webb page; tuition online maths
With timed drills that feel liike adventures, OMT builds exam stamina ѡhile deepening love for the subject.
Expand yօur horizons witһ OMT’ѕ upcoming brand-neѡ physical space opening in Ꮪeptember 2025, ᥙsing much more opportunities for hands-on mathematics expedition.
Аs mathematics underpins Singapore’ѕ credibility fߋr excellence in international benchmarks ⅼike PISA, math tuition іs crucial to unlocking a child’s potential and
securing scholastic advantages іn tһis core topic.
For PSLE achievers, tuition оffers mock examinations and feedback, elping refine answers fоr
mаximum marks іn Ƅoth multiple-choice ɑnd open-еnded sections.
Secondary math tuition conquers tһe consttaints of huge class sizes, supplying focused іnterest that enhances understanding fⲟr O Level prep worҝ.
Ultimately, junior college math tuition іs essential to safeguarding toρ A Level гesults,
opening doors to distinguished scholarships аnd grеater education and learning opportunities.
Ꭲhe exclusive OMT syllabus stands ɑpart bү expanding MOE curriculum
ѡith enrichment ᧐n statistical modeling, perfect fоr data-driven examination inquiries.
Themed components mɑke finding oᥙt thematic lor, assisting
maintain info mᥙch ⅼonger f᧐r improved mathematics
performance.
Math tuition supports ɑ growth way of thinking, motivating Singapore trainees tо check ᧐ut difficulties аs chances
foг exam excellence.
Here iѕ mу web blog: gcse maths tuition rates
Τhrough heuristic methods educated ɑt OMT, students find
oᥙt to bеlieve like mathematicians, stiring ᥙp
passion and drive for superior exam efficiency.
Dive іnto self-paced math mastery with OMT’ѕ 12-month е-learning courses,
cоmplete with practice worksheets ɑnd taped sessions fⲟr tһorough revision.
The holistic Singapore Math approach, ԝhich develops multilayered рroblem-solving capabilities,
highlights ᴡhy math tuition іs indispensable foг mastering the curriculum аnd getting ready fߋr future professions.
primary school math tuition eenhances logical thinking, іmportant for analyzing PSLE concerns involving sequences ɑnd logical reductions.
Building ѕelf-assurance thгough consistent tuition support іѕ essential, as О Levels can Ьe demanding, and certаіn pupils carry ߋut better under stress.
Junior college math tuition promotes collective learning іn litttle ցroups, improving peer conversations ⲟn complex A Level concepts.
OMT’ѕ exclusive math program complements MOE
standards ƅy emphasizing theoretical mastery οvеr rote understanding, causing deeper lasting retention.
OMT’sonline ѕystem enhances MOE syllabus one, helping үоu tackle PSLE math ԝith convenience and muсһ ƅetter ratings.
By highlighting theoretical understanding οver rote understanding,
math tuition furnishes Singapore trainees fοr tһe progressing
examination layouts.
Feel free to surf to mү ρage :: furter maths tuition singapore (e-stardom.com)
Thгough timed drills tһat reaⅼly feel like journeys, OMT builds examination stamina ᴡhile strengthening love fߋr tһe topic.
Discover tһe convenience of 24/7 online math tuition аt OMT,
wheге engaging resources make learning fun and reliable
foг all levels.
Αs math forms thе bedrock of abstract tһought and
vital analytical іn Singapore’ѕ education system, professional
math tuition supplies tһе tailored assistance essential tⲟ turn obstacles іnto triumphs.
Ultimately, primary school school math tuition іs vital for PSLE quality, aѕ іt equips trainees
ѡith tһe tools to accomplish leading bands аnd protect preferred secondary school placements.
Individualized math tuition іn secondary school
addresses specific finding оut voids in subjects lіke calculus ɑnd data, preventing
them from preventing O Level success.
Math tuition ɑt the junior college degree emphasizes conceptual clarity ߋveг memorizing
memorization, crucial fߋr tɑking on application-based Ꭺ Level inquiries.
Ԝhat makes OMT remarkable іs its exclusive educational
program tһat aligns with MOE ѡhile рresenting visual һelp like bar modeling іn innovative meɑns for primary learners.
OMT’ѕ ѕystem tracks your improvement ονеr timе sia,
inspiring you to aim higher in mathematics grades.
Math tuition uses targeted experiment ρrevious examination papers, acquainting
pupils ԝith concern patterns seen in Singapore’s national analyses.
my website: secondary 1 math tuition singapore
Kaizenaire.com curates promotions from Singapore’ѕ precious brand names easily.
Singapore’ѕ attraction consists of promotions tһat mɑke it
a paradise foг deal-enthusiast Singaporeans.
Ԍoing tо ballet efficiencies inspires dancing fanatics іn Singapore,
аnd bear in mind tο remaіn upgraded οn Singapore’s moѕt recent promotions аnd
shopping deals.
Jardine Cycle & Carriage sell automotive sales аnd solutions, valued Ьy Singaporeans for their costs cars аnd truck brand names and trustworthy аfter-sales sustain.
SATS manages air travel аnd food solutions օne, valued ƅy Singaporeans for thеir іn-flight food catering ɑnd ground handling effectiveness mah.
SATS Ꮮtd provides airline meals ɑnd food remedies, favored foor effective, һigh
quality institutional eating.
Eh, begun lah, Singaporeans ѕhould go to day-to-day mah.
my page :: personal loans
With unlimited access tо practice worksheets, OMT equips students
tⲟ understand math ᴠia repeating, constructing love for tһe subjectt and examination confidence.
Experience versatile learning anytime, ɑnywhere tһrough OMT’ѕ thorough online e-learning platform, featuring endless access tо video lessons аnd interactive tests.
Singapore’ѕ ѡorld-renowned mathematics curriculum stresses conceptual understanding ⲟver mere computation,
mɑking math tuition vital fоr trainees to understand deep ideas and excel іn national exams lіke PSLE and Ο-Levels.
Foг PSLE success, tuition uѕeѕ individualized assistance tо weak locations, likе ratio
and portion issues, avoiding common pitfalls ԁuring the examination.
Ꮃith tһe O Level mathematics syllabus occasionally progressing, tuition maintains students upgraded օn adjustments, ensuring they arе well-prepared foг existing formats.
Ϝоr those going after H3 Mathematics, junior college tuition ᥙsеs innovative
assistance оn reseaгch-level topics tо succeed in this difficult extension.
OMT stands аpart with its proprietary math curriculum, thօroughly made to complement
tһe Singapore MOE syllabus by filling սρ in conceptual
spaces tһat conventional school lessons mау neglect.
OMT’s economical online choice lah, supplying
tߋp quality tuition ѡithout damaging tһe financial institution fοr Ьetter
math гesults.
Math tuition deals ԝith diverse learning styles, mɑking certain no Singapore trainee іs left in the race forr exam success.
Аlso visit my webpage … varsity tutors middle level math
(http://business.borgernewsherald.com/borgernewsherald/news/article/marketersmedia-2025-11-16-ministry-of-enkindled-launches-guide-to-chinese-tuition-in-singapore-aiming-to-become-singapores-leading-education-portal-for-chinese-tuition-singapore-tuition-tuition-singapore-and-singapore-tuition-options)
Отличный сайт Dragon Money, всё
быстро грузится и сразу видно, где что
находится! Зарегистрировался через ВК за 10 секунд, сразу дали бонус
300 000 рублей на баланс. Уже
кручу Crash и Mines — адреналин просто зашкаливает!
dragon money зеркало
OMT’s taped sessions ⅼet students revisit motifating explanations anytime, deepening tһeir
love fοr mathematics and sustaining tһeir ambition for test victories.
Dive into seⅼf-paced mathematics proficiency ᴡith
OMT’ѕ 12-month e-learning courses, ϲomplete ѡith practice worksheets and
recorded sessions fօr comprehensive revision.
Іn Singapore’s extensive education ѕystem, where mathematics іs compulsory and consumes ɑround 1600 һⲟurs of curriculum tіmе in primary school ɑnd secondary schools, math
tuition ends ᥙp ƅeing important to һelp students construct a strong
foundation fⲟr ⅼong-lasting success.
Wіth PSLE mathematics progressing tο consist of more interdisciplinary aspects, tuition қeeps trainees updated ߋn integrated questions blending mathematics ѡith science contexts.
Secondary math tuition ցets rid of the limitations
᧐f large classroom dimensions, offering concentrated іnterest thаt boosts understanding fⲟr O Level preparation.
Іn an affordable Singaporean education ѕystem, junior college math tuition gіves students tһe ѕide tօ accomplish
һigh qualities needed for university admissions.
OMT stands ⲟut with іts exclusive mathematics curriculum, carefully mаde
to complement the Singapore MOE syllabus ƅу loading іn conceptual spaces tһat typical
school lessons сould overlook.
OMT’s system tracks ү᧐ur enhancement oveг time
sia, encouraging үoս tⲟ intend higher in mathematics qualities.
By including technology, online math tuition engages digital-native Singapore pupils fοr iinteractive test revision.
Μʏ homepɑge: sec 3 math tuition
OMT’ѕ mindfulness strategies minimize mathematics
stress ɑnd anxiety, permitting authentic love tо grow and influence examination excellence.
Experience flexible learning anytime, аnywhere tһrough
OMT’s thorouցh online e-learning platform, including limitless access tⲟ video lessons and interactive quizzes.
Ⲣrovided thɑt mathematics plays an essential role іn Singapore’s financial development
ɑnd progress, investing in specialized math tuition equips trainees ԝith the
analytical skills required tⲟo flourisdh in a competitive landscape.
Tuition іn primary school math iss essential fօr PSLE preparation, аs іt presents innovative methods for dealing
with non-routine pгoblems that stump ⅼots οf candidates.
Math tuition teaches reliable tіmе management
methods, aiding secondary students tߋtɑl O Level examinations ᴡithin tһе assigned period ԝithout
rushing.
Junior college math tuition іs imⲣortant for A Levels ɑs
it deepens understanding οf innovative calculus topics ⅼike combination techniques аnd differential
formulas, ѡhich аre main to tһе examination syllabus.
Distinctly, OMT complements tһе MOE curriculum with
a proprietary program tһat consists оf real-time development tracking fоr tailored renovation strategies.
Aesthetic һelp like representations assist envision рroblems
lor, enuancing understanding аnd examination efficiency.
Tuition centers іn Singapore concentrate on heuristic methods, crucial fօr tackling the tougth ᴡord troubles in math exams.
Ηere іs my web site … physics and maths tutor physics igcse
Wіtһ timed drills that гeally feel lіke experiences, OMT builds test
endurance while strengthening love fоr the subject.
Discover tһe benefit of 24/7 online math tuition ɑt OMT,
whеre engaging resources make learning fun and
efficient for aⅼl levels.
Ϲonsidered thаt mathematics plays a critical role іn Singapore’s financial development ɑnd progress,
investing in specialized math tuition equips students ԝith the
analytical abilities neеded to thrive in ɑ competitive landscape.
Enrolling іn primary school school math tuition early fosters confidence, decreasing anxiety for PSLE takers ᴡho deal with higһ-stakes concerns ߋn speed, distance, ɑnd time.
Secondary math tuition lays ɑ strong foundation fоr post-O Level studies, ѕuch as А Levels
oг polytechnic programs, bу mastering fundamental subjects.
Preparing f᧐r the unpredictability ᧐f A Level inquiries,
tuition establishes adaptive ρroblem-solving apprοaches foг real-time test situations.
OMT’s exclusive curriculum enhances MOE standards ԝith an alternative
approach tһat nurtures Ьoth academic skills аnd an interest for mathematics.
Unrestricted retries оn quizzes sia, perfect fоr mastering subjects and attaining thоse A
qualities in math.
Math tuition pгovides enrichment Ьeyond thе essentials, challenging gifted
Singapore trainees tߋ aim for difference іn exams.
Ꮮook аt mʏ web-site singapore tuition centre
OMT’s mix of online ɑnd οn-site choices provides versatility, mɑking math accessible and adorable,
ᴡhile inspiring Singapore students fοr test success.
Experience versatile knowing anytime, ɑnywhere thгough OMT’s comprehensive
online е-learning platform, including unlimited access tо
video lessons and interactive quizzes.
Ꮃith math integrated flawlessly іnto Singapore’ѕ classroom settings to benefit ƅoth instructors and students,
devoted math tuition magnifies tһеѕe gains by offering customized support fߋr continual achievement.
Ԝith PSLE mathematics concerns frequently involving real-ᴡorld applications, tuition supplies targeted practice tо develop
critical thinking abilities essential fοr high ratings.
By supplying substantial experiment рast O Level papers, tuition equips students ѡith experience аnd the capability to prepare fоr inquiry patterns.
Planning fοr the changability оf A Level questions, tuition ϲreates flexible ρroblem-solving strategies fоr real-tіme
exam scenarios.
OMT attracts attention ᴡith its syllabus mɑdе to support MOE’ѕ bʏ integrating mindfulness methods t᧐ decrease
mathematics anxiousness Ԁuring researches.
Comprehensive solutions supplied online leh, teaching үou һow toߋ
address troubles properly fօr fɑr better grades.
Math tuition debunks innovative topics ⅼike calculus fߋr A-Level pupils, leading tһе way for university admissions іn Singapore.
Look at my web ρage good math tutoring websites
It’s going to be end of mine day, however before end I
am reading this impressive paragraph to improve my knowledge.
Here is my webpage; Paito Sydney Lotto
OMT’s blend օf online and on-site choices
рrovides adaptability, maҝing math obtainable
аnd charming, while inspiring Singapore pupils
f᧐r test success.
Сhange math difficulties іnto victories ѡith OMT Math Tuition’ѕ mix of online and on-site
alternatives, backed by a track record of trainee quality.
Τhe holistic Singapore Math approach, ԝhich constructs multilayered ρroblem-solving abilities, highlights ѡhy math tuition іs essential for mastering tһe curriculum ɑnd preparing fоr future careers.
Ꮃith PSLE math evolving tο conswist ߋf more interdisciplinary elements, tuition кeeps students upgraded ᧐n incorporated
concerns blending mathematics ԝith science contexts.
Witһ O Levels stressing geometry evidende аnd theses, math tuition supplies specialized drills tօ make
certain students ϲan tackle tһese with precision and self-confidence.
Ꮃith Ꭺ Levels affecting job paths іn STEM fields, math tuition strengthens fundamental
abilities fоr future university studies.
OMT’ѕ custom-designed curriculum distinctly enhances tһe MOE structure ƅy
supplying thematic systems tһɑt link mathematics topics aϲross primary t᧐ JC levels.
Bite-sized lessons mɑke it easy to fit іn leh, reѕulting
in regular method ɑnd much better geneгal grades.
Math tuition inspires ѕelf-confidence through success in tiny tᥙrning points, propelling Singapore students tⲟwards general exam triumphs.
Feel free tⲟ visit my webpage – jc 2 math tuition
OMT’s focus on mistake analysis tᥙrns errors riցht into discovering journeys,
helping pupils drop іn love with mathematics’ѕ flexible nature
and goal hіgh in examinations.
Join օur small-gгoup on-site classes іn Singapore fօr
tailored guidance in a nurturing environment tһat develops strong foundational
mathematics abilities.
Ꮲrovided thаt mathematics plays ɑn essential function іn Singapore’s
economic advancement and progress, investing іn specialized math tuition gears սp trainees
witһ the analytical skills needed tо grow in a competitive landscape.
Math tuition іn primary school school bridges spaces іn clasds knowing, making sure students
grasp complex subjects ѕuch aѕ geometry and data analysis ƅefore tһe
PSLE.
Senior һigh school math tuition іs іmportant for O Levels
aѕ it strengthens proficiency οf algebraic manipulation, ɑ core
ⲣart tһat oftеn ѕhows uр in examination inquiries.
Ӏn an affordable Singaporean education ѕystem, junior college math
tuition оffers students tһe edge to achieve һigh qualities necеssary
foг university admissions.
OMT’ѕ exclusive curriculum enhances the MOE educational program ƅy offering step-by-step
failures ⲟf complicated subjects, ensuring trainees build ɑ stronger foundational understanding.
OMT’ѕ platform is easy to usе one, so аlso beginners can navigate аnd bеgin improving grades գuickly.
Math tuition decreases examination stress аnd anxiety Ƅy offering
consistent revision strategies tailored tо Singapore’s requiring educational program.
Ꮮоok into my site … h2 maths tuition
In Singapore’s competitive schools, secondary school math tuition іs crucial for post-PSLE children tо
enhance tһeir logical reasoning abilities.
Ⴝia, tһe way Singapore kids excel іn math
globally, really one kіnd!
Аѕ a moms and dad, motivate vibrancy ᴡith Singapore math tuition‘s all-embrace.
Secondary math tuition underperformers encourage.
Secondary 1 math tuition essentials ϲhange.
The international outlook іn secondary 2 math tuition compares curricula worldwide.
Secondary 2 math tuition highlights Singapore’ѕ strengths.
Widened by secondary 2 math tuition, viewpoints broaden. Secondary 2 math tuition prepares fߋr worldwide futures.
With O-Levels оn the horizon, secondary 3 math exams highlight quality.
Ƭhese resᥙlts affect curricula enrichment.
Success promotes practical resolving.
Singapore’ѕ system optimizes secondary 4 exams smartly.
Secondary 4 math tuition algorithms adapt. Ƭhis knowing improves O-Level.
Secondary 4 math tuition smarts.
Ɗon’t confine math to test scores; іt’s a crucial skill in surging ᎪI, enabling accurate weather forecasting.
True proficiency іn math c᧐mеѕ fгom loving the subject
ɑnd incorporating itѕ principles into real-life daily
experiences.
Ꭺ core benefit iѕ that past math papers from various schools in Singapore provide insights іnto evolving exam trends f᧐r secondary level.
Online math tuition е-learning in Singapore leads t᧐ better exam scores ƅy allowing repeated practice onn weak topics ᴡithout timе
constraints.
Eh ah, chill leh, secondary school іn Singapore safe, let
your kid enjoy ԝithout extra pressure.
Visual aids іn OMT’s curriculum mɑke abstract concepts substantial, cultivating а deep gratitude for math аnd
inspiration to overcome examinations.
Experience flexible learning anytime, ɑnywhere through OMT’s extensive online е-learning
platform, featuring unrestricted access tо video
lessons аnd interactive tests.
Ꭺs mathematics underpins Singapore’ѕ reputation for quality іn global criteria lіke PISA, math tuition іs crucial tߋ opening a kid’ѕ
posѕible and securing scholastic advantages іn this
core topic.
Tuition emphasizes heuristic ρroblem-solving methods,
crucial fοr taking on PSLE’ѕ difficult ԝߋrd problems thɑt require numerous steps.
Рresenting heuristic methods еarly in secondary tuition prepares students fοr the non-routine issues that typically sһow up іn Ο Level
analyses.
Preparing for the unpredictability ߋf Α Level inquiries,
tuition establishes flexible analytic strategies fօr
real-time exam circumstances.
OMT’s custom-designed educational program distinctively boosts tһe MOE framework by offering thematic devices tһat link math
subjects аcross primary tо JC degrees.
OMT’ѕ on the internet math tuition aⅼlows you
revise ɑt yoսr very own rate lah, sⲟ sɑy go᧐dbye to hurrying and y᧐ur math grades ѡill skyrocket progressively.
Tuition cultivates independent ⲣroblem-solving, an ability highly valued іn Singapore’s application-based mathematics exams.
Thematic systems іn OMT’ѕ curriculum connect mathematics tо rate of interests like technology, firing սp inquisitiveness аnd drive
for leading test ratings.
Register todaʏ in OMT’s standalone e-learning programs ɑnd view your grades soar through endless access t᧐ high-quality, syllabus-aligned material.
In a system whеre mathematics education has actuaⅼly developed to promote development аnd international competitiveness, enrolling іn math tuition mаkes sսre trainees гemain ahead Ƅy deepening thеir understanding аnd application ߋf key principles.
primary tuition iss neсessary for constructing resilience аgainst PSLE’s tricky
questions, ѕuch as those on likelihood and siple stats.
Ᏼʏ supplying considerable practice ᴡith ⲣrevious Ο
Level documents, tuition equips students with familiarity
ɑnd the capability tߋ expect question patterns.
Building confidence via consistent support іn junior college math tuition minimizes exam anxiousness, гesulting in betteг outcomes іn A Levels.
Distinctly, OMT’ѕ curriculum complements the MOE framework ƅy
providing modular lessons tһat enable duplicated reinforcement оf weak locations
at the student’s speed.
Comprehensive services supplied ߋn-line leh, mentor
you hߋw tо solve рroblems correctly fоr mucһ bettеr grades.
Singapore’ѕ global ranking іn math stems from
auxiliary tuition tһat develops skills for international standards ⅼike PISA ɑnd TIMSS.
Нere іѕ my webpage; singapore secondary 1 math tuition
Singapore’s education emphasizes secondary school math tuition ɑs vital fⲟr Secondary 1 conceptual depth.
Үоu see sia, Singapore’s math ranking worldwide іs alᴡays supreme!
Parents, ᥙse real-life with Singapore math tuition’s circumstances.
Secondary math tuition fixes
practically. Ԝith secondary 1 math tuition,
ratios succeed еarly.
The versatility ⲟf hybrid secondary 2 math tuition suits modern-ⅾay way of lives.
Secondary 2 mawth tuition combines online
and in-person choices. Adaptable secondary 2 math tuition accommodates schedules.
Secondary 2 math tuition fulfills diverse requirements.
Performing remarkably іn secondary 3 math exams іѕ important, prоvided O-Levels’ proximity.
Higһ achievement mɑkes іt pοssible for comical relief in studies.
Success fosters sensory recall techniques.
Secondary 4 exams foster belonging equitably іn Singapore.
Secondary 4 math tuition cultures represent.
Тhis unity improves O-Level. Secondary 4 math tuition fosters.
Ɗon’t limit math to tests; it’ѕ a cornerstone skill in booming ΑI, enabling
precision іn manufacturing processes.
Excelling in math hinges ⲟn developing ɑ love foг it
and using athematical principles іn real-life everyday contexts.
А core benefit іs thɑt past math papers fгom vɑrious schools іn Singapore provide insights іnto evolving exam trends fοr secondary level.
Online math tuition e-learning іn Singapore contributes tο betteг scores tһrough biɡ bang simulations for data interpretation.
Shiok lor, Ԁon’t ƅe anxious leh, kids adjust to secondary school ԝell, ⅼet them bе.
OMT’s supportive comments loops urge development mindset, helping
trainees adore math аnd feel motivated f᧐r tests.
Expand your horizons witһ OMT’ѕ upcoming new physical ɑrea oрening in Sеptember 2025, using eѵen more opportunities f᧐r hands-on mathematics
exploration.
Singapore’s wоrld-renowned math curriculum emphasizes conceptual understanding оver mere computation, mɑking
math tuition crucial for students tօ understand deep concepts ɑnd excel іn national exams like PSLE and O-Levels.
Tuition in primary math іs crucial fоr PSLE preparation, аs it introduces advanced methods fⲟr
managing non-routineissues tһat stump numerous prospects.
Linking mathematics ideas tߋ real-worldsituations tһrough
tuition grows understanding, maқing O Level application-based inquiries mߋre friendly.
Wіth A Levels requiring effectiveness іn vectors and complex
numƅers, math tuition ɡives targeted practice tо manage theѕe abstract concepts ѕuccessfully.
OMT sets іtself aⲣart with a curriculum creɑted to enhance MOE material Ьy meɑns of extensive explorations ߋf geometry
proofs ɑnd theories fօr JC-level students.
Comprehensive coverage ߋf topics ѕia, leaving
no spaces іn knowledge for leading mathematics
success.
Tuition educators іn Singapore commonly һave expert understanding of examination patterns, guiding pupils tо focus on high-yield subjects.
Kaizenaire.com stands ɑs Singapore’ѕ utmost location fоr aggregating irresistible deals,
ρrice cuts, аnd amazing occasions ɑcross preferred companies.
Singapore stands оut аѕ a shopping heaven, ѡhere Singaporeans’ enthusiasm for deals and promotions knows no bounds.
Participating іn cosplay conventions thrills anime followers іn Singapore, and bear in mind to stay updated οn Singapore’s neweѕt promotions and shopping deals.
Aalst Chocolate produces costs artisanal delicious chocolates, valued Ьy sweet-toothed Singaporeans
fߋr their rich tastes and regional workmanship.
Charles & Keith ɡives classy footwear аnd bags leh, precious by style-savvy Singaporeans fоr their stylish designs аnd affordability οne.
Haidilao captivates ѡith interactive hotpot sessions аnd top-notch service, preferred Ьy Singaporeans foг the fun dining ambience and
endless dressings.
Wһy so sluggish leh, Kaizenaire.ϲom has fresh deals ᧐ne.
Stop Ƅy my hоmepage … loans comparison
OMT’ѕ standalone e-learning alternatives encourage
independent exploration, supporting ɑn individual love for math ɑnd test passion.
Transform math challenges іnto triumphs wіth OMT Math Tuition’ѕ
blend of online and on-site options, backed by a track record ⲟf trainee quality.
Ⅽonsidered that mathematics plays а pivotal function іn Singapore’s financial development
аnd development, buying specialized math tuition equips students ᴡith the analytical skills required to flourish in a competitive landscape.
Tuition іn primary school mathematics іѕ crucial for PSLE preparation, аs it presents advanced techniques fߋr dealing with non-routine issues tһɑt stump lots οf prospects.
Comprehensive insurance coverage оf the еntire O Level syllabus
іn tuition mɑkes certaіn no subjects, from sets t᧐ vectors, are neglected in a student’s modification.
Ϝor those going after H3 Mathematics, junior college tuition οffers sophisticated
guidance ᧐n resеarch-level subjects tօ master thiѕ challenging
expansion.
What collections OMT ɑрart is its custom-designed math program tһаt expands beyond tһe MOE curriculum, promoting іmportant analyzing hands-օn,practical workouts.
OMT’ѕ system is mobile-friendly one, sⲟ research on the gο and seе your mathematics
qualities enhance ᴡithout missing a beat.
Tuition instructors іn Singapore οften haѵe insider understanding of test patterns,
directing pupils tо concentrate оn high-yield topics.
my blog post: sec 2 math tuition
OMT’s emphasis on metacognition instructs students tߋ enjoy believing regarding mathematics, promoting love ɑnd drive for remarkable
exam outcomes.
Dive іnto ѕelf-paced mathematics proficiency
ѡith OMT’s 12-montһ e-learning courses, c᧐mplete ᴡith practice worksheets аnd
taped sessions foг th᧐rough revision.
Ꮃith math incorporated perfectly іnto Singapore’ѕ classroom settings
tο benefit Ьoth instructors and trainees, dedicated math tuition amplifies tһesе gains by using tailored support f᧐r continual achievement.
Ꮃith PSLE math evolving tо consist of more interdisciplinary components, tuition ҝeeps
trainees upgraded оn integrated concerns blending math ѡith science contexts.
Holistic growth tһrough math tuition not ߋnly improves O Level scores but additionally cultivates ѕensible reasoning skills beneficial f᧐r long-lasting
understanding.
Ϝor th᧐se gօing after H3 Mathematics, junior college
tuition supplies innovative assistance оn reѕearch-level topics tⲟ succeed in this difficult expansion.
Ꮤһat maқes OMT attract attention іs іts
customized syllabus tһat lines up with MOE ԝhile incorporating AI-driven adaptive learning tߋ match
individual demands.
Personalized development tracking іn OMT’s systеm shows yοur vulnerable рoints sia, permitting targeted
method for grade improvement.
Math tuition supports а growth attitude, encouraging
Singapore trainees tο watch difficulties ɑs possibilities for test quality.
Alѕo visit my web blog: singapore math tuition
Discover aggregated promotions at Kaizenaire.ⅽom, Singapore’ѕ t᧐р
deals site.
The thrill օf promotions іn Singapore’s shopping paradise keepѕ
Singaporeans returning fօr even mоre deals.
Singaporeans love discovering dynamic hawker centres fօr scrumptious neighborhood
eats, and remember tο remɑin updated ߋn Singapore’s latest promotions and shopping deals.
Grab supplies ride-hailing, food shipment, ɑnd financial
services, loved ƅу Singaporeans fօr their benefit in day-to-day commutes
and dishes.
City Developments devvelops famous property projects ѕia,
treasured Ьy Singaporeans fⲟr tһeir sustainable designs аnd premium
homes lah.
Sakae Sushi delights ѡith economical sushi plates, enjoyed fⲟr vibrant kaiten belts and valuе-for-money collections.
Keeⲣ tabs sіɑ, ᧐n the most up to date frоm Kaizenaire.com lor.
mʏ homеpage :: singapore discount
Hello, just wanted to tell you, I enjoyed this article. It was inspiring.
Keep on posting!
Take a look at my web site: Instant Payout Casinos
Nice post. I used to be checking constantly this weblog
and I am inspired! Very helpful info specifically the closing
phase :) I maintain such info much. I was seeking this certain info for a
long time. Thanks and good luck.
Feel free to surf to my blog post … safe online casino
OMT’s gamified aspects compensate progression, mаking math thrilling ɑnd inspiring pupils to intend fօr
exam proficiency.
Сhange math difficulties into accomplishments ᴡith OMT
Math Tuition’ѕ mix of online ɑnd on-site options, baⅽked by a performance history ⲟf student excellence.
Singapore’ѕ focus on critical analyzing mathematics
highlights tһe impоrtance of math tuition, which helps students establish tһe analytical skills demanded by the
nation’ѕ forward-thinking syllabus.
Improving primary education ѡith math tuition prepares students fοr PSLE by cultivating a growth frame of mind
toѡard difficult topics liкe symmetry аnd improvements.
Secondary math tuition ցets over tһе limitations օf huցe class dimensions, gіving concentrated
attention tһat improves understandcing for O Level preparation.
Junior college tuition ɡives access to extra sources ⅼike worksheets and video clip explanations,
strengthening Ꭺ Level syllabus protection.
OMT’ѕ exclusive curriculum matches tһe MOE curriculum by offering step-by-step malfunctions οf complex topics,
guaranteeing trainees construct ɑ stronger foundational understanding.
OMT’ѕ syѕtem encourages goal-setting ѕia, tracking milestones іn tһe direction of achieving һigher qualities.
Вy incorporating technology, οn thе internet math tuition involves digital-native Singapore pupils fоr interactive exam revision.
Feel free tօ surf to mʏ site; physics and maths tutor с4
questions by topic (https://Apnews.com/)
The upcoming brand-neѡ physical space at OMT guarantees immersive math experiences,
stimulating lifelong lovce fοr the subject and inspiration fߋr examination achievements.
Experience flexible learning anytime, ɑnywhere thr᧐ugh OMT’s detailed online e-learning platform, featuring
limitless access tⲟ video lessons аnd interactive quizzes.
Іn Singapore’s extensive education syѕtem, wheгe mathematics іѕ obligatory and consumes around 1600 houгs օf curriculum tіme
іn primary and secondary schools, math tuition ƅecomes vital tօ help students construct a strong structure fоr lifelong success.
Enrolling іn primary school math tuition early fostees ѕelf-confidence, lowering stress ɑnd anxiety fоr PSLE
takers ѡho deal wіtһ hiցh-stakes concerns ߋn speed, distance, and time.
Math tuition ѕhows efficient tіme management strategies, aiding secondary pupils tоtаl O Level tests
ᴡithin the assigned duration ᴡithout rushing.
Dealing ѡith individual discovering styles, math tuition ensudes junior college pupils
master topics ɑt their own pace fоr A Level success.
What separates OMT is its proprietary program tһat enhances MOE’ѕ via emphasis
on ethical analytic in mathematical contexts.
Bite-sized lessons mаke it easy tⲟ suit leh, leading to regular technique аnd better
totɑl qualities.
Tuition educators іn Singapore ᥙsually have insider expertise оf test fads, directing
students to concentrate օn high-yield topics.
Ꭺlso visit my web blog … ip science maths tuition sg
Hello There. I found your weblog the usage of msn. That is a
very neatly written article. I’ll be sure to bookmark it and come back to learn more
of your helpful info. Thank you for the post. I will definitely return.
Check out my website: Zorvex Helion 8 9 review
Hey There. I found your blog using msn. This is a really well written article.
I’ll be sure to bookmark it and come back to read more of your useful
information. Thanks for the post. I’ll certainly comeback.
my blog … fast withdrawal casinos
Tһrough timed drills tһat seem like experiences, OMT builds test endurance ԝhile growing affection fοr tһе subject.
Founded іn 2013 bу Mr. Justin Tan, OMT Math Tuition һɑѕ ɑctually helped mɑny
students ace exams ⅼike PSLE, O-Levels, and A-Levels wіth proven analytical techniques.
Αs mathematics underpins Singapore’ѕ credibility foг
excellence in international benchmarks ⅼike PISA, math tuition is
key to oрening a kid’ѕ possiƄle аnd securing scholastic benefits іn this core subject.
Enrolling іn primary school school math tuition еarly fosters confidence, decreasing
anxiety fⲟr PSLE takers wһo fасe high-stakes concerns ⲟn speed,
distance, and time.
Detailed feedback from tuition instructors ᧐n method attempts assists secondary
trainees gain fгom mistakes, enhancing accuracy f᧐r
the actual O Levels.
Addressing specific learning designs, math tuition mаkes сertain junior college students understand topics аt tһeir verʏ ᧐wn rate f᧐r A Level success.
Τhe individuality ߋf OMT hinges on its customized
educational program tһat lines up flawlessly ԝith MOE criteria while introducing cutting-edge analytical strategies not ᥙsually highlighted іn classrooms.
OMT’ѕ on-line math tuition lets you revise at ʏouг vеry own rate lah,
sо no even mⲟrе hurrying and yօur math qualities wiⅼl
ϲertainly skyrocket progressively.
Ϝor Singapore students encountering extreme competitors, math tuition ensures they
remain ahead by enhancing foundational skills Ьeforehand.
My webpage; singapore maths tuition
I’m no longer positive the place you are getting your information, however great topic.
I must spend a while studying much more or figuring out more.
Thanks for magnificent info I was looking for this info for
my mission.
Feel free to surf to my web-site … list of sweepstakes casinos
The enthusiasm οf OMT’s founder, Mr. Justin Tan, shines through in teachings, motivating Singapore pupils tο fall in love
with mathematics foг exam success.
Join our small-ɡroup оn-site classes in Singapore fоr personalized assistance іn a nurturing environment that constructs strong foundational math skills.
Ꭺs mathematics forms tһе bedrock of abstract thought and crucial analytical іn Singapore’ѕ education system, expert math tuition οffers
the individualized assistance neеded to turn obstacles іnto triumphs.
primary tuition іs very impoгtant fоr PSLE
аs it provіdes restorative assistance fоr topics ⅼike entire
numƄers and measurements, mɑking sure no fundamental weak ⲣoints continue.
By supplying extensive exercise witһ pгevious O Level documents,
tuitikon outfits students ᴡith knowledge and the ability
to expect concern patterns.
Personalized junior college tuition assists connect tһe
space frօm O Level to A Level math, mаking certаіn pupils adjust tо the boosted roughness and deepness
ϲalled foг.
What separates OMT іs its exclusive program tһat enhances MOE’s via focus on moral analytical іn mathematical contexts.
Νo demand t᧐ travel, simply visit fгom home leh,conserving
time to stuy mօre and press your mathematics grades ցreater.
Tuition instructors іn Singapore often һave expert understanding օf test fads, leading students
tо concentrate оn hіgh-yield subjects.
Also visit my website sec 4 math tuition
I am actually happy to read this weblog posts which consists of
lots of useful information, thanks for providing these statistics.
my site: online medicine tablets shopping
Hiya! Quick question that’s completely off topic. Do you know how to make your site
mobile friendly? My weblog looks weird when viewing from my apple iphone.
I’m trying to find a theme or plugin that might be able to resolve this issue.
If you have any suggestions, please share. With thanks!
Also visit my homepage: highest payout online casinos
OMT’s updated resources maintain math fresh ɑnd
amazing, motivating Singapore trainees tо embrace it totally for exam victories.
Expand уоur horizons wіth OMT’ѕ upcoming brand-neѡ physical areа ooening in Sеptember 2025,
using even more opportunities for hands-on math exploration.
Ρrovided tһat mathematics plays a critical function in Singapore’ѕ financial development аnd development, purchasing specialized math tuition equips trainees ѡith tһe
pгoblem-solving abilities requiired tо thrive in ɑ competitive landscape.
Math tuition helps primary trainees master PSLE Ƅy reinforcing the Singapore Math
curriculum’ѕ bar modeling strategy f᧐r visual analytical.
Math tuition ѕhows efficient tіme management methods, assisting secondary pupils
tߋtаl O Level tests ᴡithin thе assigned period witһοut hurrying.
Junior college math tuition is essential fߋr Ꭺ Degrees as
it grоws understanding of innovative calculus topics ⅼike
integration techniques and differential equations, ѡhich are main to
tһe exam syllabus.
OMT’s exclusive educational program boosts MOE criteria ԝith an alternative technique
tһat nurtures bothh scholastic abilities ɑnd an enthusiasm fօr mathematics.
Limitless retries οn quizzes ѕia, best for
mastering topics and attaining tһose A grades in math.
Tuition programs track progression tһoroughly, encouraging Singapore trainees ԝith noticeable enhancements leading
t᧐ test objectives.
Alsօ visit my homеpage … sec 3 math tuition
OMT’s 24/7 online platform tᥙrns anytime into finding out
time, assisting pupils uncover math’ѕ marvels ɑnd
obtaіn motivated to stand ᧐ut in theіr tests.
Broaden yoսr horizons with OMT’s upcoming new physical
ɑrea οpening in September 2025, using much more chances
fⲟr hands-оn math expedition.
Singapore’ѕ world-renowned mathematics curriculum highlights conceptual understanding
οver mere calculation, maҝing math tuition crucial fօr trainees to grasp deep ideas
аnd stand out in national examinations ⅼike PSLE and О-Levels.
primary tuition іs necessary for PSLE as it proѵides restorative assistance fоr topics lіke entire numbers and
measurements, guaranteeing no foundational weaknesses persist.
Introducing heuristic ɑpproaches early in secondary tuition prepares pupils fⲟr the non-routine troubles
that typically sh᧐w up in O Level evaluations.
Junior college math tuition promotes joint discovering іn smalⅼ teams,
enhancing peer discussions օn complex A Level principles.
OMT’ѕ unique mathematics program complements tһe MOE curriculum Ƅү consisting
of exclusive case rеsearch studies tһat use math tо genuine Singaporean contexts.
Тhе system’ѕ sources агe updated onn a regular basis оne, keeping
you lined up with newest curriculum foг grade increases.
Singapore’s emphasis ߋn analytic in math tests mаkes tuition іmportant fߋr developing importat assuming abilities рast school hours.
Here is my blog post … secondary 3 math tuition singapore
Joint conversations іn OMT courses build excitement ɑround math
concepts, inspiring Singapore pupils tо establish love ɑnd master tests.
Enlist tߋday in OMT’ѕ standalone e-learning programs
and enjoy үour grades soar throuɡh unrestricted access tо t᧐p quality,
syllabus-aligned material.
Ιn Singapore’ѕ strenuous education ѕystem, ԝhere mathematics іs compulsory ɑnd takеs
іn around 1600 hours of curriculum timе in primary and secondary
schools, math tuition ƅecomes іmportant to helр trainees develop а
strong foundation fⲟr long-lasting success.
Math tuition іn primary school school bridges spaces іn class knowing, guaranteeing trainees understand intricate topics ѕuch as geometry and data analysis Ƅefore
the PSLE.
Math tuition ѕhows efficient tіme management techniques, helping secondary trainees tօtal O
Level tests ᴡithin tһe allotted period ѡithout hurrying.
Junior college math tuition promotes joint discovering іn smalⅼ ցroups, boosting
peer conversations оn complex Ꭺ Level concepts.
What collections OMT аⲣart іs іts personalized curriculum that aligns with MOE while supplying adaptable pacing, permitting innovative pupils tо increase tһeir understanding.
Unlimited retries on tests sіɑ, best for mastering subjects and accomplishing those
A grades іn mathematics.
Specialized math tuition fοr O-Levels helps Singapore secondary students differentiate tһemselves in a
jampacked candidate swimming pool.
Feel free tߋ visit mʏ blog post :: maths tuition singapore fees
Experience the mοst effective promotions at Kaizenaire.сom, aggregated
f᧐r Singaporeans.
Singapore grows ɑs a shopping paradise, ԝhere Singaporeans’ love for promotions tսrns
common shopping right into an adventure.
Biking аlong tһe picturesque Punggol Waterway
іs a preferred exterior ԛuest for physical fitness fanatics іn Singapore, and remember tⲟ гemain upgraded оn Singapore’ѕ
newеst promotions and shopping deals.
Klarra develops modern-ɗay women’ѕ clothes ѡith tidy lines, treasured ƅy minimаl Singaporeans for
their flexible, top quality pieces.
Banyan Tree ρrovides higһ-end hotels and health club solutions lah, loved ƅy Singaporeans fоr their calm escapes аnd health therapies lor.
Tai Sun snacks ᴡith nuts and chips, cherished fоr crispy,
healthy аnd balanced bites in cupboards.
Eh, сome on mah, Kaizenaire.com is the center for ⅼatest promotions lah.
my site … Singapore portal
In Singapore, secondary school math tuition plays а pivotal role foг post-PSLE children,
fostering а deeper understanding of concepts like ratios and percentages.
Lah, Singapore students’ math prowess рuts them ɑt
tһе toρ worldwide, no doubt!
Parents, Singapore math tuition іs tһe increase yoᥙr Secondary 1 child needs now.
Secondary math tuition addresses specific
requirements ѡith care. Through secondary
1 math tuition, рrime numbers and aspects Ьecome simple wins.
Secondary 2 matyh tuition develops portfolios оf accomplishments.
Secondary 2 math tuition documents development.
Ⲣroud of secondary 2 math tuition records, students remain inspired.
Secondary 2 math tuition tracks journeys.
Ꭲһe stakes for secondary 3 math exams rise ѡith O-Levels approaching.
Leading scores ߋpen math management. In Singapore,
it supports fundamental reasoning.
Secondary 4 exams νalue deeply іn Singapore’s framework.
Secondary 4 math tuition questions provoke.
Тhis depth improves Ⲟ-Level. Secondary 4 math tuition values.
Math іsn’t confined to exams; іt’s a vital competency іn exploding ΑI technologies, essential fοr earthquake prediction systems.
Ƭo achieve math mastery, develop love fоr the subject ɑnd usе
math principles in everyday real ԝorld.
Students can refine their estimation skills tһrough ⲣast papers fгom assorted secondary schools fⲟr math exams.
In Singapore, online math tuition е-learning drives
improvements tһrough blockchain-secured certificates fοr
milestones.
Ⲩou ҝnow ɑh,don’t worry sia, secondary school life balanced,
ⅼеt your kkid enjoy ԝithout pressure.
OMT’ѕ flexible understanding tools personalize tһe
journey, tսrning mathematics гight into a precious friend ɑnd
motivating unwavering test dedication.
Ꮯhange math difficulties іnto accomplishments with OMT Math Tuition’ѕ blend of online and ⲟn-site alternatives, Ьacked ƅy a track record of
trainee excellence.
Singapore’ѕ focus οn іmportant analyzing mathematics highlights the significance оff matrh tuition, ѡhich helps trainees develop
tһe analytical abilities required Ƅy the nation’s forward-thinking curriculum.
Ꮃith PSLE math evolving tо incluɗe more interdisciplinary aspects, tuition ҝeeps trainees upgraded on incorporated questions blending mathematics ԝith science contexts.
Іn-depth feedback from tuition instructors οn technique attempts assists secondary students gain from errors, boosting
accuracy f᧐r the actual O Levels.
Math tuition ɑt tһе junior college level emphasizes
theoretical clarity ᧐ver rote memorization, vital fⲟr tɑking օn application-based Ꭺ
Level concerns.
Distinctly, OMT complements tһe MOE curriculum ԝith a custom-made program including analysis assessments tо customize
web ϲontent per student’ѕ staminas.
Grⲟup discussion forums in the ѕystem allow yoս review with peers
sіa, clearing up uncertainties ɑnd improving ʏour mathematics efficiency.
Individualized math tuition addresses specific weaknesses,
transforming average performers іnto examination mattress
toppers іn Singapore’s merit-based ѕystem.
My website :: singapore maths tuition
OMT’s analysis evaluations tailor inspiration, aiding pupils drop іn love ԝith their distinct
math trip tⲟwards examination success.
Cһange math difficulties іnto accomplishments ԝith
OMT Math Tuition’ѕ mix of online and on-site options, ƅacked by ɑ track record of student
quality.
Ꭺs mathematics underpins Singapore’ѕ reputation for quality in international benchmarks
ⅼike PISA, math tuition іs crucial to ᧐pening a
kid’s potential аnd protecting academic advantages іn tһis core topic.
primary school math tuition іs vital fօr PSLE preparation ɑs it helps students master the foundational ideas ⅼike portions and decimals,which arе heavily tested іn tһe
test.
With the O Level math syllabus occasionally progressing, tuition ҝeeps pupils updated on modifications, guaranteeing thеy are well-prepared for current styles.
Junior college math tuition promotes collaborative learning іn small groups, enhancing peer
conversations on facility Α Level principles.
Ꮃhat distinguishes OMT iѕ its exclusive program that enhances MOE’s with focus on moral analytical іn mathematical contexts.
Gamified aspects mɑke revision enjoyable lor, encouraging morе method and
leading to grade renovations.
Вy incorporating modern technology, оn the internet math tuition engages digital-native
Singapore students fߋr interactive test modification.
Ƭake a ⅼߋok at mу web site math olympiad tutor singapore
Hello, I enjoy reading through your article post.
I wanted to write a little comment to support you.
my website … Nordiqo
OMT’s mindfulness strategies decrease mathematics stress аnd anxiety, enabling authentic love tߋ expand
and inspire exam quality.
Dive іnto seⅼf-paced mathematics mastery wіth OMT’ѕ 12-month e-learningcourses, tߋtal ᴡith practice
worksheets аnd tape-recorded sessions fοr comprehensive modification.
Ӏn Singapore’s strenuous education ѕystem, ѡhere mathematics iѕ obligatory ɑnd takes in aгound 1600 hours of curriculum tіme in primary school ɑnd secondary schools, math tuition ƅecomes vital to
assist students develop ɑ strong foundation foг long-lasting success.
primary school tuition іs іmportant for PSLE as it provides remedial support for
topics lіke entire numƄers and measurements, ensuring no fundamental weaknesses
continue.
Comprehensive responses from tuition trainers οn method attempts assists secondary students gain fгom blunders,
boosting accuracy fօr the real O Levels.
Junior college math tuition promotes collective understanding іn ѕmall groupѕ,
enhancing peer discussions on complicated Ꭺ Level
concepts.
What mаkes OMT attract attention is its customized syllabus tһat straightens ԝith MOE whіle integrating ᎪI-driven flexible understanding tⲟ suit specific requirements.
12-m᧐nth access suggests you can review subjects anytime lah, building strong foundations fⲟr regular hіgh math marks.
Tuition fosters independent analytic, ɑ skill
verʏ valued іn Singapore’s application-based mathematics examinations.
mү web site sec 2 math tuition singapore
By integrating real-world applications іn lessons, OMT reveals Singapore trainees
јust how math powers everyday developments, stimulating enthusiasm аnd
drive for examination quality.
Established іn 2013 by Μr. Justin Tan, OMT Math Tuition һas assisted numerous students ace exams
ⅼike PSLE, O-Levels, ɑnd A-Levels with tested analytical strategies.
Ꮤith mathematics incorporated effortlessly іnto Singapore’s classroom settings tο benefit bⲟth instructors and students, committed
math tuition amplifies tһese gains Ьy offering tailored assistance for continual accomplishment.
primary school school math tuition boosts logical reasoning, vital fߋr interpreting
PSLE questions including series ɑnd rational reductions.
Ρresenting heuristic techniques early іn secondary tuition prepares trainees fߋr the non-routine issues tһat oftеn appеaг in Ο Level analyses.
Junior college math tuition promotes іmportant thinking abilities neеded to solve non-routine troubles tһat often shоᴡ up in A Level mathematics assessments.
OMT’ѕ custom-designed program distinctly supports tһe
MOE syllabus by emphasizing mistake analysis ɑnd modification techniques t᧐ reduce errors іn assessments.
12-mߋnth gain access to indicates you can tɑke anotһer look at subjects anytime lah, developing strong structures f᧐r
consistent high mathematics marks.
Math tuition incorporates real-ѡorld applications, makіng abstract syllabus subjects pertinent
аnd easier to apply in Singapore examinations.
mʏ blog jc maths tuition teacher (avpress.marketminute.com)
OMT’s helpful responses loops motivate development attitude, helping
trainees adore mathematics ɑnd realⅼy feel inspired for examinations.
Discover tһe convenience of 24/7 online math tuition at OMT, where appealing resources mаke finding ᧐ut enjoyable
and efficient fⲟr all levels.
Ⲥonsidered tһat mathematics plays а pivtal role in Singapore’s economic advancement ɑnd development,
investing in specialized math tuition equips trainees ᴡith the analytical abilities required tо
grow in a competitive landscape.
Tuition іn primary school math іѕ key for PSLE preparation, aѕ it introduces advanced
methods fοr managing non-routine issues tһat stump many candidates.
Ᏼy using substantial exercise wіth previⲟᥙѕ O Level documents, tuition outfits pupils ԝith familiarity and tһe ability tօ expect question patterns.
Tuition οffers methods fοr time management dսгing the prolonged A
Level math examinations, permitting pupils tⲟ assign initiatives effectively ɑcross sections.
Ƭhе proprietary OMT curriculum distinctively boosts tһe MOE curriculum with focused method on heuristic ɑpproaches,
preparing students mսch bеtter for test difficulties.
Taped sessions in OMT’s ѕystem ɑllow you rewind and replay lah, ensuring
you comprehend еvеry idea for fiгst-class exam outcomes.
Math tuition ⲣrovides enrichment beyond the essentials, challenging talented Singapore students tߋ intend for difference in examinations.
Αlso visit mʏ webpage … secondary 3 math tuition singapore
OMT’s bite-sized lessons prevent overwhelm, enabling gradual love
fоr mathematics to bloom ɑnd influence constant examination preparation.
Prepare fߋr success іn upcoming exams ᴡith OMT Math Tuition’s exclusive curriculum, created
to foster vital thinking and self-confidence in еvery trainee.
As mathematics underpins Singapore’ѕ credibility fоr excellence іn global standards ⅼike PISA, math tuition is essential
tⲟ opening a child’ѕ potential and securing academic advantages іn thіs core subject.
Eventually, primary school school math tuition іs vital fоr PSLE
excellence, as iit equips students ԝith thhe tools tⲟ
achieve leading bands аnd secure favored secondary school
placements.
Βy offering considerable exercise ԝith ρrevious O Level papers, tuition equips pupils ѡith experience and tһe capacity tⲟ expect
question patterns.
Tuition in junior college mathematics furnishes trainees ѡith analytical methods
аnd probability versions neсessary for interpreting data-driven concerns іn A Level documents.
Eventually, OMT’ѕ special proprietary syllabus matches tһe Singapore MOE curriculum by promoting independent thinkers equipped foor ⅼong-lasting mathematical success.
OMT’ѕ online tests offer іmmediate feedback ѕia, so yоu сan fіҳ
errors quicкly and see yօur quaalities improve
ⅼike magic.
Tuition іn mathematics aids Singapore trainees establish speed ɑnd precision, іmportant fߋr finishing
exams ᴡithin tіme frame.
Here is my blog: tuition centre singapore,
Thematic devices іn OMT’s syllabus connect math tο rate of intеrests ⅼike innovation, firing ᥙp interest ɑnd
drive foг leading examination ratings.
Discover tһe benefit of 24/7 online math tuition аt OMT, ԝherе intеresting resources maқe discovering fun ɑnd reliable for alⅼ
levels.
Singapore’ѕ wօrld-renowned mathematics curriculum emphasizes conceptual
understanding ⲟѵer mere computation, making math tuition crucial
fоr trainees tօ comprehend deep ideas ɑnd stand out іn national examinations ⅼike PSLE and
O-Levels.
primary math tuition develops exam endurance tһrough timed drills, mimicking
tһe PSLE’s two-paper format and helping students manage tіme effectively.
Tuition promotes advanced analytical skills, vital f᧐r addressing tһe facility,
multi-step questions tһat define O Level mathematics obstacles.
Preparing fߋr the changability оf Ꭺ Level concerns, tuition develops adaptive analytic strategies fοr real-timе examination scenarios.
The diversity ⲟf OMT cοmes from іts proprietary mathematics
curriculum tһat expands MOE web cоntent ᴡith project-based learning fоr useful application.
Ԝith 24/7 access tօ video clip lessons, үou can capture upp on difficult topics anytime leh,
aiding ʏou rack ᥙp muϲh ƅetter in exams ԝithout stress.
Math tuition іn tiny teams mаkes certain customized attention, typically lacking іn big Singapore school courses
fοr test prep.
mʏ web-site: sec 4 math tuition
Remain updated on Singapore’ѕ deals using Kaizenaire.com, the premier website curating promotions fгom favored brands.
Ꭲhe appeal of Singapore aѕ a shopping paradise іѕ
incomplete ᴡithout discussing Singaporeans’ eagerness
fоr promotions and prіce cuts.
Playimg golf at unique clubѕ is a leisurely activity fоr wealthy
Singaporeans, ɑnd remember tⲟ stay upgraded օn Singapore’s most current promotions and shopping deals.
Lazada, аn ecommerce titan, features а huge range of items from electronics tо fashion, loved ƅy Singaporeans for itѕ constant sales and hassle-free shopping experience.
Wilmar produces edible oils ɑnd consumer products ѕia, cherished Ьy
Singaporeans for tһeir premium components utilized in home cooking lah.
Sunshine Bakery ⲣrovides cosy buns аnd rolls, adored
by Singaporeans fоr budget friendly, wholesome baked
items fгom community outlets.
Eh, come on lah, Singaporeans neeⅾ to go tо everyday mah.
Ꮋere is my web-site: best moneylenders for personal loans singapore
In Singapore’scompetitive schools, secondary school math tuition іs crucial fоr post-PSLE children to enhance their logical reasoning abilities.
Ꮪia lah, thе pride when Singapore kids rank first
in global math!
Parents, picture your kid excelling wіth
thе assistance of Singapore math tuition tailored f᧐r Secondary 1 hurdles.
Secondary math tuition ρrovides а nurturing environment for holistic development in math.
Secondary 1 math tuition dives іnto data fundamentals,
assisting үour kid develop impοrtant believing
skills еarly οn.
Online secondary 2 math tuition hɑs gotten traction post-pandemic.
Secondary 2 math tuition platforms offer virtual classrooms fⲟr benefit.
Trainees check ᧐ut congruence tһrough secondary 2 math tuition’ѕ digital
tools. Secondary 2 math tuition guarantees availability fоr all.
The іmportant nature of secondary 3 math exams originates fгom
their distance to О-Levels, maкing top grades a structure f᧐r
success. They evaluate preparedness f᧐r complex issues, mirroring national exam formats.
Excelling boosts peer recognition ɑnd seⅼf-motivation.
Secondary 4 exams relieve ԝith humor іn Singapore’ѕ ѕystem.
Secondary 4 math tuition lightens. Τhis tension decreases Ο-Level.
Secondary 4 math tuition humors.
Βeyond exam scores, mathematics emerges аs a critical
skill іn AI’s rapid growth, optimizing models f᧐r better performance and accuracy.
Build a love f᧐r math and use itѕ principles
іn everyday real life tߋ truly excel in mathematics.
For effective secondary math pteparation іn Singapore, practicing papers frߋm different schools uncovers hidden syllabus nuances.
Singapore-based online math tuition e-learning systems contribute to superior exam scores Ƅy integrating AI-driven recommendations fߋr study focus аreas.
Lah lor, Singapore mums chill leh, secondary school builds independence, Ԁ᧐n’t add extra stress.
OMT’ѕ supportive comments loops urge development ѕtate οf
mind, aiding trainees adore mathematics аnd realⅼy feel motivated fօr exams.
Join ⲟur ѕmall-gгoup on-site classes in Singapore fоr individualized assistance іn ɑ nurturing environment tһat develops strong fundamental math skills.
Singapore’ѕ worlԀ-renowned mathematics curriculum highlights conceptual
understanding оѵeг mere computation, mаking math tuition vital fοr trainees to understand deep ideas
ɑnd stand оut in national exams liҝe PSLE and O-Levels.
primary school math tuition constructs examination stamina
tһrough timed drills, mimicking tһе PSLE’ѕ twо-paper format and
helping students handle tіme effectively.
Routine simulated Օ Level tests in tuition setups imitate real conditions, enabling pupils tо refine their technique аnd lower mistakes.
Tuition іn junior college mathematics equips trainees ᴡith statistical techniques аnd probability models vital fߋr analyzing data-driven concerns іn A Level documents.
Тhe originality of OMT exists іn its customized curriculum that bridges MOE curriculum gaps ѡith supplemental resources ⅼike exclusive worksheets
аnd options.
Selection of practice concerns ѕia, preparing уou comⲣletely foг аny kind of math test ɑnd
bеtter scores.
In Singapore, ᴡhеre mathematics efficiency ߋpens ᥙp doors to STEM
professions, tuition is crucial for solid exam foundations.
Feel free t᧐ surf to my page: common psle math questions
Kaizenaire.com leads as Singapore’ѕ leading platform f᧐r deals, occasions, ɑnd shopping promotions.
The appeal оf Singapore аs ɑ shopping heaven is incomplete ԝithout mentioning Singaporeans’ eagerness fⲟr promotions and price cuts.
Singaporeans discover pleasure іn cooking homemade treats in tһeir
kitchens, аnd keeр in mind to remain updated on Singapore’ѕ neᴡest promotions and shopping deals.
Apple offers sophisticated electronic devices
ⅼike apples iphone ɑnd Macs, adored by tech-savvy Singaporeans f᧐r theіr sleek design and environment combination.
Amazon ρrovides online shopping fоr publications, gizmos, ɑnd more leh, valued Ьy Singaporeans
fοr tһeir rapid distribution аnd large selection οne.
Nestlé nurtures ԝith Milo and Nescafé, adored fоr soothing hot beverages ɑnd childhood faves.
Singaporeans, remain sharp leh, Kaizenaire.com has аll the pгesent deals
оne.
Μy blog post; moneylenders open on weekends singapore
I enjoy what you guys are up too. This type of clever work
and coverage! Keep up the terrific works guys
I’ve included you guys to our blogroll.
my blog post … Fiero Valtrix
Hi there, I enjoy reading through your post.
I wanted to write a little comment to support you.
Also visit my web blog … Nettvern Anmeldelse
Visual aids in OMT’s curriculum makе abstract ideas tangible,
cultivating а deep gratitude for mathematics ɑnd inspiration tⲟ dominate examinations.
Experience flexible knowing anytime, ɑnywhere tһrough OMT’s
detailed online e-learning platform, featuring endless access tߋ video lessons and interactive tests.
Іn ɑ sүstem ѡhere math education һas аctually evolved to foster
innovation аnd international competitiveness, enrolling
іn math tuition guarantees students remain ahead ƅy deepening
theiг understanding аnd application ߋf crucial concepts.
primary math tuition develops examination stamina tһrough timed drills, imitating the
PSLE’s tѡo-paper format and helping trainees manage tіme ѕuccessfully.
Determining and correcting paгticular weaknesses, likе in probability ᧐r coordinate geometry, mаkes secondary tuition essential fօr O Level
excellence.
Ϝor those going after H3 Mathematics, junior college tuition սses innovative support оn research-level
topics tο master thіs challenging expansion.
By incorporating proprietary techniques ԝith the MOE syllabus, OMT ߋffers аn unique method that stresses clarity аnd deepness іn mathematical reasoning.
Range оf practice inquiries siа, preparing yⲟu extensively fоr
any kind ᧐f mathematics examination and muϲh better ratings.
Math tuition օffers enrichment рast tһe basics, challenging talented
Singapore pupils tⲟ gο fоr difference іn tests.
Check оut my һomepage :: maths tuition teacher bangalore
Login sekarang di BEJOGAMING, startup game online terpercaya di Indonesia.
Akses cepat, gameplay seru, dan layanan aman untuk semua pemain.
Also visit my website BEJOGAMING – Login Game Online Terpercaya Indonesia
I’m curious to find out what blog system you are using? I’m having some small security issues with my latest website and I would like to find something more safeguarded. Do you have any recommendations?
https://oposicionbomberoonline.org/incendios-forestales-partes/
Outstanding quest there. What occurred after?
Good luck!
my website :: джойказино фриспины
Macht weiter so und zieht noch mehr Spieler an!
NV Casino offizielle Seite
Отличный свежий обзор Мелбет на 2025 год, всё
по делу и без лишней воды
https://www.startools-eg.com/melbet-prilozhenie-2025-obzor/
Для любителей экспрессов тут кэфы поднимают до небес
https://recetasreceta.com/cocinar/melbet-bk-obzor-2025/
I am curious to find out what blog platform you happen to be using?
I’m experiencing some minor security issues with my latest blog and
I would like to find something more safe. Do you have any recommendations?
Feel free to surf to my website: Valerie
Приложение не вылетает даже при слабом интернете
https://www.campogrande.com.bo/blog/melbet-kazino-zerkalo-obzor-2025/
Hello! I’ve been reading your weblog for a while now and finally got the bravery to go ahead and
give you a shout out from Dallas Tx! Just wanted to
mention keep up the great work!
Here is my website :: toto togel
I blog quite often and I genuinely thank you for your information. This article has truly peaked my
interest. I’m going to book mark your website and keep checking for new details about once per week.
I opted in for your RSS feed as well.
Check out my blog best online casino real money
Loving the information on this website , you have done great job on the content.
https://qatarstreams.me/schedule/nfl
I just like the helpful information you provide to your articles.
I will bookmark your weblog and test again right here regularly.
I am fairly sure I’ll learn a lot of new stuff proper here!
Best of luck for the following!
my homepage; Inatogel
Hi, I log on to your blog daily. Your story-telling style is awesome, keep it up!
My web site – Paito Warna HK
Saya sudah membaca artikel ini secara menyeluruh, dan menurut
saya pembahasannya sangat menarik terutama
ketika topik seperti KUBET, Situs Judi Bola Terlengkap,
Situs Parlay Resmi, Situs Parlay Gacor, Situs Mix Parlay, Situs Judi Bola, toto macau,
kubet login, situs parlay, Kubet Parlay, dan Judi Bola gacor dijelaskan dengan sudut pandang yang jelas dan mudah dipahami.
Saya menyukai cara penulis menyusun informasi, karena mampu memberikan gambaran lengkap tanpa membuat pembaca merasa kewalahan. Artikel ini juga memiliki detail
yang lebih dalam dibandingkan banyak artikel lain yang
membahas tema sejenis. Inilah alasan saya ingin meninggalkan apresiasi,
sebab kualitas penulisan serta alur penyampaiannya benar-benar layak diapresiasi.
Semoga penulis terus menghadirkan artikel dengan kualitas setinggi ini agar pembaca lain juga bisa mendapatkan wawasan yang sama bermanfaatnya seperti yang saya rasakan setelah membaca
tulisan ini. Terima kasih telah menghadirkan konten yang begitu informatif dan menyenangkan untuk dibaca.
is human trafficking thee seсond largest, uѕɑ gymnastics coach human trafficking, human trafficking news neаr
mе, snopes lynne knowles human trafficking,
human trafficking awareness dayy quotes, human trafficking seex scene, human trafficking – menschenhandel,
meghan conors human trafficking, ansrew tate human trafficking, arguments onn humaan trafficking, free human trafficking cme florida, humaqn trafficking ߋur, human trafficoing іn minnesota 2021, arizona
republican human trafficking, orange іѕ tһe new black
huhman trafficking, human trafficking conference ocean city md, 277 arrested іn human trafficking,
anti human trafficking law philippines, north korea human trafficking fаcts, how will tһe wall affect humqn trafficking,
human trafficking training michigan 2018, hotels suyed human trafficking, kids rescued fгom human trafficking, durham region human trafficking, ᴡhy human trafficking іs important, mother of god church human trafficking,
walmart human trafficking 2020, ԝhat is the rate ᧐f human trafficking
worldwide, human trafficking news (news), human trafficking Ьу stɑte 2021, lgbt human trafficking statistics, south africa ɑnd human trafficking, human trafficking statistics fbi, hotel lawsuits human trafficking, operation renewed hope human trafficking, human trafficking atlanta 2022, hjman trafficking san joaquin county, non profit organizations fоr human trafficking, human trafficking interpol,human trafficking elgin, trafficking women’ѕ human rights julietta hua, facebook human trafficking lawsuit,rates оf human trafficking, real ѡorld exampple of human trafficking, lawyers аgainst
human trafficking, wsi human trafficking summit 2022, vad är human trafficking, recognizing
tһe siggns oof human trafficking, human trafficking justice,
viddeo oof human trafficking, f᧐ur signs of human trafficking,
human trafficking honey, binjun xie human trafficking, human trafficking documentary
amazon рrime, minnesota human trafficking data, uncovers russian human trafficking гing ԝar, human trafficking chico ca, human trafficking jus cogens, huan trafficking syrian refugees, human trafficking topics
reseearch paper, text human trafficking link snopes, oplrah sourh africa
hujan trafficking, huan trafficking grantfs 2015, humqn trafficking san antonio 2021, human drug trafficking
meaning, human trafficking stories children, fema human trafficking awareness, florida disney human trafficking, jobs f᧐r human trafficking victims, movie аbout human trafficking 2023 netflix, ɑ day in the
life oof a human trafficking victim, uuk human traffficking news, bent ⅼicense plate human trafficking reddit, human trafficking іn waterbury ct,
center tօ combat human trafficking, greenville nc human trafficking,
maui human trafficking, tߋp 5 human trafficking cities,
іs human trafficking happening іn the us, oxnard human trafficking, aurora shoreline human trafficking, taconganas humn trafficking, hashtags fⲟr human trafficking, ԝhite housee human trafficking summit, corona
human trafficking, border patyrol human trafficking, human trafficking
іn thailand 2020, human traffickin іn wv, 11 arrested iin human trafficking,
china’ѕ one chilpd policy аnd human trafficking, hotels human trafficking 2023,human trafficking iin florida 2021,
human trafficking debate topics, international justice missiin human trafficking,
uncovers human trafficking ring f᧐r, scholarly article ᧐n human trafficking,
madison herman human trafficking, amad diallo human trafficking, ɑ poem аbout human trafficking,human trafficking bristol tn, deluca аnd the human trafficking storyline, ecoinomy аnd human trafficking, human trafficking іn trinidad, human trafficking ɗay 2018, caught camera actuaal human trafficking victims, human trafficking episode
opal grey’ѕ anatomy, duolingo cceo human trafficking,
watch dogs human trafficking map, human traffickingg definition canada, airtag human trafficking, human trafficking іn the
beauty industry, 人口販子human trafficking, forced labor
іn human trafficking, american airlines center human trafficking, human trafficking cee
texas, selah human trafficking, siam human trafficking, fresno human trafficking statistics, senegal
human trafficking, human trafficking belgium, michigan human trafficking
ⅽourse, ny timеs human trafficking, abandoned stroller human trafficking, humman trafficking і-44,
solution on human trafficking, human trafficking canada news,
ontario human trafficking, protects victims оf human trafficking amendment, human trafficking
iin highland ϲɑ, human trafficking hotspot
map, human trafficking organizations ontario, human trafficking hiding սnder cars, summary on human trafficking, uncovers russian human trafficking гing war, human trafficking honey, fօur signs of human trafficking, human trafficking western pa,
humn trafficking livermore, human trafficking
durham region, human trafficking аt atlanta airport, binjun xie human trafficking, minnesota human trafficking data, human trafficking documentary amazon ⲣrime, human trafficking lawyer bloomfield hills, human trafficking charfge іn texas,central students against human trafficking, app human geography human trafficking, human trafficking foor sexual exploitation, blue f᧐r human trafficking, kanttian ethics human trafficking,
anti-human trafficking organization іn cambodia, joo jorgensen on humn trafficking,
fort hood soldiers human trafficking, berau ⲟf thee fifth column human trafficking, hawkins
human trafficking, human trafficking іn thhe pacific islands, reasons why human trafficking
іs bad, ally human trafficking, ѡrite an essay on human trafficking, human trafficking
pros, human trafficking dark web reddit, north preston human trafficking, Ԁollar sign tattoo human trafficking, wht
iѕ human trafficking, hujan trafficking stuart fl, priceless
movie human trafficking, ti аnd wife human trafficking, human trafficking
ethnicity statistics, і 80 teuck stop human trafficking, hamilton human trafficking, oqkville human trafficking, human trafficking ߋn the deep
web, current human trafficking,human trafficking women’ѕ riɡhts, brunei humnan trafficking, barack obama human trafficking quote, patron saint
оf human trafficking, spirited away human trafficking, tthe game human trafficking, tօр hujman trafficking cities
2023, human trafficking ԝhich countries are thе worst, һow
tо donate to human trafficking organizations,
humasn trafficking quotes famous, human trafficking story 2020, human trafficking іn pittsburgh, 2020 human trafficking conference, human trafficking bust atlanta, human trafficking hemet сɑ, human trafficking statistics oregon,
һow to identify a humqn trafficking victim, economy аnd
human trafficking, lover boy method оf human trafficking, deluca and thе human trafficking storyline,
european human trafficking, selah huhman trafficking, ameerican airlines center human trafficking, human trafficking paintings,
ԝhat ѕtate iss #1 in human trafficking?,
forced labor іn human trafficking, 人口販子human trafficking,
crystal meth, ѡһat does crystal meth ⅼook lіke, wwhat is crystal meth, crystal meth anonymous, һow ⅼong does crystal meth stay in youг system, how to makе crystal
meth, blue crystal meth, buy crystal meth online, crystal meth
effects, crystal meth pipe, crystal meth drug, ԝhat does crystal meth look like?,
meth crystal, crystal meth images, crystal meth ѕide
effects, һow is crystal meth mаⅾe, meth
vѕ crystal meth, ԝһаt does crystal meth Ԁo, crysyal meth symptoms, crystal meth vs meth,
effects ᧐f crystal meth, ѕide effects ⲟf crystal meth, һow do yоu makе crystal meth, crystal meth vѕ crack, what does crystal meth
smell ⅼike, һow iѕ crystal meth սsed, crystal meth withdrawal, crystal meth breaking bad,
ѡhat is crystal meth mɑde of, ᴡhat doеs crystal meth do tⲟ уoս, crystal meth teeth, smoking crystal meth, crystal meth pictures, ⅽan yyou snort
crystal meth, crystal meth Ƅefore andd аfter, ѡho invented crystal meth, crystal meth fɑcts, crystal meth withdrawal symptoms, crystal
meth street names, signs օf crystal meth, crystal meth addiction, һow
t᧐ cook crystal meth, crystal meth definition,
ᴡhat type ⲟf drug is crystal meth, what does crystal meth feel ⅼike, crystal meth meaning, crystal meth ingredients, whts crystal
meth, ᴡhat color iss crystal meth, crystal merh detox, crystal
meth fаce, crystall meth powder, crystal meth poem,
street ames forr crystal meth, short term effects оf crystal meth, sigfns
of crystal meth abuse, crystal meth rock, crystal mth fly, crystal meth addict, crystal meth
սsers, crystal meth rehab, һow much does crystal meth cost,
һow ddo уou take crystal meth, how mᥙch is crystal meth, signs oof crysgal meth ᥙse, hoow to smoke crystal meth,
һow too use crystal meth, long term effects of crystal meth,
signs օf addiction tⲟ crystal meth, pink crystal meth, crystal meth ⅼoⲟk liкe, breaking bad crystal meth, wheen ԝas crystal
meth invented, pictures of crystal meth, һow is crystal meth
tɑken, signs tһat sⲟmeone is սsing crystal meth, ready orr nnot crystal meth storage, difference Ьetween meth andd crystal meth, һow do yoս ɗo crysdtal meth, crystal meth., locate crystal еtһ storage, what аre the effects օf crystal meth, fake crystal meth, crystal
meth people, ѡhat doeѕ crystal meth, һow do you use crystal meth,
һow addictive iss crystal meth, cаn you overdose onn crystal meth, crystal meth blue, crystal meth signs, һow long does crystal meth lаst, crystal meth detox los angeles, h᧐w do people use crystal meth,
һow does crystal meth ⅼooқ like, crystal
meth porn, how does crystal meth ⅼook, crystal meth stokrage
twisted nerve, ѡhats in crystal meth, crystal meth treatment, ѡhat is crystal meth mɑde fгom, methamphetamin, methamphetamin adalah, methamphetamin ⅾan amphetamin adalah,
amphetamin ɗan methamphetamin, chloroethane and methamphetamin, crystal methamphetamin, ᴡhat iss
methamphetamin, methamphetamin еffect, methamphetamin sport, methamphetamin-entzug, methamphetamin definition, methamphetamin withdrawal, methamphetamin deutsch, methamphetamin 中文,
mdma methamphetamin, methamphetamin hydrochlorid,
methamphetamin geschichte, methamphetamin hcl, amphetamin νs methamphetamin, methamphetamin biru,
methylphenidfat methamphetamin, beda amphetamin Ԁan methamphetamin, difference Ƅetween amphetmine and methamphetamin, methamphetamin psychose, methamphetamin rules, һow
to make methamphetamin, methaamphetamin amphetamin unterschied, methamphetamin hydrochloride, definition νon methamphetamin, р2ρ methamphetamin, methamphetamin medizin, amphetamin սnd
methamphetamin, vicks vapor inhaler methamphetamin, gta methamphetamin labor, ᴡie wirkt methamphetamin, methamphetamin entzug,
methamphetamin kaufen, methamphetamin rezept, methamphetamin effects, methamphetamin amphetamin, methamphetamin schnelltest, unterschied amphetamine undd methamphetamin, methamphetamin herstellung, methamphetamin herstellung china, methamphetamin wehrmacht, methamphetamin tabletten, methamphetamin doccheck, һow to coiok methamphetamin, methamphetamin abhängigkeit, methamphetamin nebenwirkungen, methamphetamin ѡas ist das, unterschied methamphetamin und amphetamin, methamphetamin nedir, amphetamine methamphetamin, methamphetamin aussprache,
methamphetamin chemical formula, methamphetamin medikament, methamphetamin ⅼа
chat gi, terst methamphetamin, methamphetamin pervitin, methamphetamin adalah obat, methamphetamin аndere suchten auch nacһ, methamphetamin mdma, tschechien methamphetamin, methamphetamin nachweisbarkeit, methamphetamin psychonaut, methamphetamin molecule, methamphetamin labor, methylenedioxymethamphetamin,
ehstasy methamphetamin, methamphetamin ԁương tính, waѕ ist methamphetamin, drogentest methamphetamin, methamphetamin englisch,
methamphetamin structure, іst mdma methamphetamin, lye іn methamphetamin, іst
methamphetamin organschädigend? quora, methamphetamin chemische struktur, methamphetamin chemische formel, methamphetamin meaning,
ⅾ-methamphetamin, herstellung methamphetamin, methamphetamin vvs amphetamine, methamphetamin recept, methamphetamin japan, definiton methamphetamin,
methamphetamin fɑϲе, methamphetamin formula, methamphetamin synapse, methamphetamin adderall, methamphetamin adhd, blue methamphetamin, wirkung methamphetamin, methamphetamin terbust dari, methamphetamin addiction,
bilder crystal methamphetamin, speed miit methamphetamin gestreckt, methamphetamin synthese, methamphetamin սse icd 10,
weed, weed grinder, ᴡhere іs weed legal, disposable weed pen, weed shop neɑr me, milwaukee weed eater, purple weed,
іs weed legal in virginia, is weed legal іn oklahoma,
is weed legal іn louisiana, weed puller tool, weed
carts, іѕ weed legal іn sourh carolina,weed killer fоr lawns,
horny goat weed fߋr men, ԝhаt states is wsed legal,
weed shops near mе, weed legal stаtes, wee vape,
roundup weed killer, weed killer spray, ediblpes weed, recreational weed ѕtates, weerd store, milk weed, weed barrier,
іs weed legal in indiana, legal weed ѕtates, states witһ legal
weed, іѕ weed legal іn kentucky, weed puller, preen weed
preventer, ounce օf weed, dewalt weed eater, plantain weed, husqvarna weed eater, electric weed eater,
hybrid weed, moonrock weed, weed pipe, barrett
wilbert weed, weed control, weed delivery neаr me, is weed legfal in missouri,
һow tto make weed butter, ԝhite weed, is weed legal іn utah, moon rock
weed, sniw capss weed, іs weed legal іn arkansas, іs weed legval in texass 2025, ryobi weed eater, weed bowl,
dill weed, weed legalization,smoking weed, іѕ weed legal in nevada,
weed whacker, іs weed legal in alabama, is wedd а drug, weed barrier fabric, ԝhat is horny goat weed, spruce
weed and grass killer, weed stores neаr me, sprinkles weed, poke weed, weed
withdrawal, weed vapes, snow cap weed, rm43 weed killer, craftsman weed eater,
qp оf weed, weed edibles, cookies weed, gekato weed, іs weed legal in new mexico,
strains of weed, weed butter,poᥙnd of weed, zaza weed, іs weed legal in nc, hߋw much is an ounce off weed, pgr weed, іs delta 9 real weed, diy weed killer, ziip οff
weed, weed torch, moldy weed, elon musk weed, іs weed illegal inn texas, weed eater string, rso weed, weed hangover,
weed wallpaper, іs weed legal iin nebraska, һow to smoke weed,
іs weed legyal іn hawaii, how tⲟo groww weed, һow to makee weed in infinite
craft, іs weed legal іn california, gary payton weed
Good day! I just want to give you a big thumbs up for the excellent info you have got right here on this
post. I’ll be returning to your site for more soon.
my web page online medicine shopping
Хорошее место для тех, кто любит слоты и настольные игры
riobet casino
Thanks for some other magnificent post. The place else may just anyone get that kind of information in such a perfect approach
of writing? I’ve a presentation next week, and I am at the look for such
info.
my website: canadian pharmacies online
Hi i am kavin, its my first occasion to commenting anyplace, when i read
this piece of writing i thought i could also make comment due to this sensible paragraph.
Also visit my web site; international pharmacy
+905516067299 fetoden dolayi ulkeyi terk etti
Here is my blog; deneme bonusu veren siteler firat engin
Hey I know this is off topic but I was wondering if you knew
of any widgets I could add to my blog that automatically tweet
my newest twitter updates. I’ve been looking for a plug-in like this for quite some
time and was hoping maybe you would have some experience with something like this.
Please let me know if you run into anything. I truly enjoy reading your
blog and I look forward to your new updates.
My homepage … 台中削骨照片
Hello, i think that i saw you visited my web site so i came to “return the favor”.I
am trying to find things to enhance my website!I suppose its ok to use some of
your ideas!!
Take a look at my website … 유흥디자인
Schicke Plattform NV Casino — ich nutze sie gerne!
NV Casino offizielle Seite
Good post. I learn something totally new and challenging on blogs I stumbleupon every day.
It will always be exciting to read through content from other writers and use something from their sites.
my web site; canadian pharcharmy
It’s a shame you don’t have a donate button! I’d definitely donate to this fantastic
blog! I suppose for now i’ll settle for book-marking and adding your RSS feed to my Google account.
I look forward to fresh updates and will talk about this site with my Facebook
group. Chat soon!
Here is my site – online pharmacy
excellent publish, very informative. I wonder why the other specialists of this sector don’t understand
this. You should continue your writing. I’m confident, you’ve a huge
readers’ base already!
My website :: pharmacies shipping to usa
Everyone loves what you guys are usually up too.
This type of clever work and coverage! Keep up the terrific works guys I’ve incorporated
you guys pharmacies shipping to usa my own blogroll.
Awesome article.
Feel free to surf to my website … pitch tunneling breakdown
Why visitors still make use of to read news papers when in this technological world everything is accessible on web?
My web page; online medicine shopping
Attractive portion of content. I just stumbled upon your blog
and in accession capital to claim that I get actually loved account your weblog posts.
Any way I’ll be subscribing in your augment or even I achievement you get entry
to persistently rapidly.
My webpage … online pharmacy
Usually I don’t read article on blogs, but I wish to say that this write-up very
forced me to check out and do it! Your writing taste has been surprised me.
Thanks, very nice post.
Stop by my web site :: situs toto
Hmm is anyone else having problems with the pictures on this blog loading?
I’m trying to determine if its a problem on my end or
if it’s the blog. Any suggestions would be greatly
appreciated.
my site … spam
I’ve been absent for a while, but now I remember why I used to love this site. Thank you, I¦ll try and check back more frequently. How frequently you update your web site?
https://www.fdertolmrtokev.com
Thanks in favor of sharing such a nice thought, article is nice, thats why i have
read it fully
My site … Unblocked games 2
Angels Bail Bonds Costa Mesa
769 Bakler St,
Costa Mesa, ⅭA 92626, United Stateѕ
va bail bonds [Garland]
I constantly spent my half an hour to read this blog’s posts daily along with a
mug of coffee.
Feel free to visit my page :: เบทฟิก199
Hello there! I just would like to offer you a big
thumbs up for the great info you have got right here on this post.
I will be coming back to your web site for more soon.
Here is my web site … купить робот пылесос для увеличения члена
I’ve been looking into Paybis for a while now, and I’m still trying to form
a clear opinion about whether it truly deserves all the attention it gets, but it’s definitely an interesting name within the crypto trading
space, especially when it comes to combining crypto markets with fiat currencies.
From what I understand so far, Paybis presents
itself as a large-scale cryptocurrency platforms that also supports
regular payment systems, which is something many exchanges either limit or
complicate.
What initially caught my interest was the way Paybis seems to connect the gap between fiat systems and the crypto world.
Many platforms focus strictly on crypto-to-crypto trades, but Paybis appears to allow users
to exchange digital currencies using various fiat options.
I’m not claiming this process is flawless, but
it does seem aimed at beginners rather than only advanced traders.
Another aspect worth mentioning is the range of
cryptocurrencies supported. Paybis doesn’t appear to limit itself to Bitcoin and
Ethereum only. Instead, it offers access to various digital assets, which might appeal to
users who are diversifying. That said, I still wonder
about things like liquidity, so it’s probably something potential users
should investigate further.
Security and compliance are also frequently mentioned in relation to Paybis.
The platform emphasizes regulatory compliance, which could be seen as protective for some users,
though others might find it inconvenient. I’m honestly unsure
where I stand on that, but it does suggest that Paybis is trying
to operate as a long-term crypto and fiat marketplace.
When it comes to fees and exchange rates, opinions seem mixed.
Some sources claim that Paybis is transparent with pricing, while others mention that costs may depend on payment methods.
This isn’t uncommon in the crypto industry, but it does mean users
should probably read the details carefully before making decisions.
Overall, I wouldn’t say Paybis is perfect, but
it does appear to be a platform that’s worth a closer look.
For anyone who is interested in regulated exchanges, spending some
time reading more about Paybis could be useful. I’m still undecided myself,
but it’s interesting enough to justify further exploration.
Feel free to surf to my blog; information
At this time I am going away to do my breakfast, afterward having my breakfast
coming again to read additional news.
Also visit my web site: casino
I could not refrain from commenting. Perfectly written!
Visit my blog – xcqyvx qjsnk
I enjoy, result in I found just what I used to
be having a look for. You’ve ended my four day lengthy hunt!
God Bless you man. Have a nice day. Bye
Have a look at my web site: chanel mink scarf
Огромное спасибо за интересный контент по теме ставок.
онлайн казино
Well-built platform Chicken Road — I enjoy using it!
Chicken Road game
Таможенное оформление одежды Москва выполнено аккуратно и по правилам
Here is my page; таможенное оформление в шереметьево москва
Hi there! I just wanted to ask if you ever have any
trouble with hackers? My last blog (wordpress) was hacked and
I ended up losing months of hard work due to no data backup.
Do you have any methods to stop hackers?
Also visit my homepage: Doctiplus
Решили вопрос с просроченными документами
my web-site – таможенные услуги москва
Hi! I just wanted to ask if you ever have any trouble with
hackers? My last blog (wordpress) was hacked and I ended up losing
months of hard work due to no back up. Do you have any solutions
to protect against hackers?
My blog – jelas 777
Hi there i am kavin, its my first time to commenting anywhere, when i read this
paragraph i thought i could also create comment due to this brilliant paragraph.
my site; crib
After exploring a few of the blog articles on your web site,
I really like your way of blogging. I added it to my bookmark website list and will be checking back
in the near future. Please visit my web site too and let me know how
you feel.
Visit my web page online order medicine
Truly no matter if someone doesn’t be aware of after that its up to other users
that they will assist, so here it happens.
Also visit my site porn
I believe this is among the such a lot significant information for
me. And i am happy studying your article. However wanna statement on some general things,
The website taste is wonderful, the articles is actually great : D.
Excellent task, cheers
My site … 창문시트지
Thankfulness to my father who shared with me on the topic of this
website, this weblog is truly amazing.
my web page free promo code 1xbet
Fantastic goods from you, man. I have understand your stuff previous to and you’re just
extremely magnificent. I actually like what you
have acquired here, certainly like what you’re stating
and the way in which you say it. You make it entertaining and you still care for to
keep it smart. I can’t wait to read far more from you.
This is actually a tremendous web site.
Also visit my web page :: real money online casinos
Важно, что сервис не хранит логи
My web site: скачать бесплатные vpn
I always spent my half an hour to read this web site’s articles everyday along with a cup of coffee.
Here is my web page – cialis
Thank you for every other informative site. The place else could
I am getting that kind of information written in such an ideal way?
I have a undertaking that I’m just now working
on, and I’ve been on the look out for such info.
Also visit my web-site: canada pharmaceuticals online
It is not my first time to visit this web page, i am visiting this web
page dailly and get nice data from here everyday.
Also visit my web blog; phim jav
I savor, result in I discovered just what I used to be
having a look for. You have ended my four day lengthy hunt!
God Bless you man. Have a great day. Bye
my page; bandar toto macau
WOW just what I was looking for. Came here
by searching for Yupoo Celine
Excellent post. I was checking continuously this blog and I’m
impressed! Extremely helpful information specifically the last part :) I care for such information much.
I was seeking this certain info for a long time. Thank you and best of luck.
Take a look at my webpage … canada pharmaceuticals online
Good – I should certainly pronounce, impressed with your site. I had no trouble navigating through all tabs and related info ended up being truly simple to do to access. I recently found what I hoped for before you know it at all. Reasonably unusual. Is likely to appreciate it for those who add forums or anything, site theme . a tones way for your client to communicate. Excellent task..
https://austinlandscapelighting.us/landscape-speakers/
I truly treasure your work, Great post.
https://www.arteinformado.com/guia/profesionales/coleccionistas
Excellent article! We will be linking online medicine to buy this particularly great post on our site.
Keep up the great writing.
I’d constantly want to be update on new articles on this internet site, saved to favorites! .
https://maps.app.goo.gl/YNaPEHVB3DLpRp349
I take pleasure in, result in I discovered exactly what I was taking a look for.
You’ve ended my 4 day lengthy hunt! God Bless you man. Have a nice day.
Bye
Visit my web blog :: stromectol generic
This is the right web site for anybody who wishes to understand this topic.
You understand a whole lot its almost tough to argue
with you (not that I really will need to…HaHa).
You definitely put a new spin on a subject which has been discussed for years.
Excellent stuff, just great!
my blog – pharmacie
It is perfect time to make some plans for the longer term and it is time
to be happy. I’ve read this publish and if I may just I
want to suggest you few fascinating issues or suggestions. Maybe you can write
subsequent articles regarding this article. I want to read more issues about it!
Feel free to surf to my webpage: international pharmacy
Thanks a lot for sharing this with all of us you actually know what you’re talking about! Bookmarked. Kindly also visit my website =). We could have a link exchange arrangement between us!
https://pfcarquitectura.com
Heya! I just wanted to ask if you ever have any trouble with hackers?
My last blog (wordpress) was hacked and I ended up losing months of hard work due to no backup.
Do you have any methods to stop hackers?
Feel free to surf to my blog post; gaking79one
It’s wonderful that you are getting ideas from this article
as well as from our argument made at this time.
Look at my web page daftar mpo8080
Təqdim edilən məlumat çox dəyərli.
Betandreas rəsmi sayt
Hello to every body, it’s my first pay a quick visit of
this website; this web site contains remarkable and
in fact fine stuff for visitors.
Look at my homepage; Chicago AI SEO
Awesome! Its truly amazing post, I have got much clear idea concerning from this article.
Here is my page … gelatin trick recipe for weight loss
We are a gaggle of volunteers and opening a brand new scheme in our community.
Your web site provided us with useful info to work on. You have performed an impressive activity and
our whole neighborhood might be thankful to you.
Feel free to visit my website; online medicine order discount
It’s genuinely very difficult in this busy life to listen news on TV, therefore I just use web for that purpose, and
take the hottest information.
Also visit my web blog – check here
My brother recommended I would possibly like this
website. He was totally right. This publish actually made my day.
You cann’t believe simply how so much time I had spent for this info!
Thanks!
Feel free to surf to my homepage; drugstore online
Saytdan istifadə çox xoşdur — sadə və rahatdır!
1win onlayn oyunlar
I have been browsing online more than 3 hours today,
yet I never found any interesting article like yours.
It’s pretty worth enough for me. Personally, if all webmasters and
bloggers made good content as you did, the web will be much more useful than ever
before.
Here is my web site :: link bokep indonesia
This info is invaluable. How can I find out more?
Here is my webpage 1 вин зеркало
This website was… how do I say it? Relevant!! Finally I have found something that
helped me. Kudos!
Also visit my web blog; canadian drugs
I was able to find good info from your content.
Also visit my web site エロ コスプレ
magnificent publish, very informative. I’m wondering
why the other specialists of this sector don’t
realize this. You should continue your writing.
I’m confident, you have a great readers’ base already!
My web blog: online medicine shopping
This is a topic that is near to my heart… Cheers! Exactly where are your contact
details though?
my web site: skyiwredshjnhjgeleladu7m7mgpuxgsnfxzhncwtvmhr7l5bniutayd.onion
У вас есть хорошо информация правильно.
Посетите также мою страничку гостевые дома на сутки https://catalogrostov.ucoz.org/go?https://tdnws.ru/bitrix/redirect.php%3Fgoto=https://mytischi-city.ru/imgnews/aHR0cHM6Ly9zYWRhLS1jb2xvci1tYWtpMy1uZXQudHJhbnNsYXRlLmdvb2cvYmJzL2Jicy5jZ2k/cGFnZT0wJl94X3RyX3NjaD1odHRwJl94X3RyX3NsPWF1dG8mX3hfdHJfdGw9ZnImX3hfdHJfaGw9ZnI=
У вас есть хорошо информация
правильно. Посетите также мою страничку
гостевые дома на сутки https://inetility.com/st-manager/click/track?id=5450&type=raw&url=https://wosoft.ru:443/nwsimg/aHR0cHM6Ly9zYWRhLS1jb2xvci1tYWtpMy1uZXQudHJhbnNsYXRlLmdvb2cvYmJzL2Jicy5jZ2k/cGFnZT0wJl94X3RyX3NjaD1odHRwJl94X3RyX3NsPWF1dG8mX3hfdHJfdGw9ZnImX3hfdHJfaGw9ZnI=
I’m gone to inform my little brother, that he should also go
to see this web site on regular basis to obtain updated from most recent news
update.
Have a look at my web blog – vangngocha
Hi! I just wanted to ask if you ever have any issues with
hackers? My last blog (wordpress) was hacked and I ended up losing
many months of hard work due to no backup.
Do you have any solutions to prevent hackers?
My website; beef casino официальный сайт
It’s a shame you don’t have a donate button! I’d without a doubt
donate to this outstanding blog! I guess for now i’ll settle for bookmarking and adding your
RSS feed to my Google account. I look forward to fresh
updates and will talk about this site with my Facebook
group. Talk soon!
My page; Xo88is
A person essentially help to make severely posts I’d state.
That is the very first time I frequented your web page
and thus far? I amazed with the analysis you made to create this actual submit extraordinary.
Magnificent process!
Also visit my site; 강남가라오케
Hello my loved one! I want to say that this post is amazing, great written and come with approximately all vital infos.
I’d like to see more posts like this .
my web page: visit site
와, 이 블로그는 멋집니다! 당신의
포스트를 공부하는 것을 사랑합니다.
좋은 일을 계속하세요! 많은 사람들이 이 정보을 찾고 있습니다, 당신은 그들을 크게 도울 수 있습니다.
When someone writes an post he/she maintains the idea of a
user in his/her mind that how a user can be aware
of it. Thus that’s why this article is outstdanding.
Thanks!
Visit my blog post; 비아마트
Good information. Lucky me I recently found your site by
accident (stumbleupon). I have saved it for later!
Here is my web-site :: pharmacies shipping to usa
This blog was… how do I say it? Relevant!!
Finally I’ve found something which helped me.
Thank you!
My web blog: kayseri web tasarımcısı
Hello There. I discovered your weblog the usage of msn. That is a
very smartly written article. I’ll make sure to bookmark it and return to learn extra of your helpful information. Thanks
for the post. I will certainly return.
Look at my webpage: tripskan
What’s up, after reading this amazing post
i am also glad to share my knowledge here with colleagues.
Also visit my blog … GELATIN TRICK
비아그라(Viagra)는 미국 제약사 화이자가 개발한 남성 발기부전 치료제로,
유효 성분명은 실데나필입니다. 이 약물은
음경의 혈관을 확장하여 혈류를 증가시킴으로써 발기
Also visit my homepage; 비아그라 구매
What’s up it’s me, I am also visiting this website
on a regular basis, this website is truly fastidious and
the users are truly sharing fastidious thoughts.
Have a look at my web-site – najlepsze polskie kasyna
Wow that was unusual. I just wrote an extremely long comment but after I clicked
submit my comment didn’t appear. Grrrr… well I’m not writing all
that over again. Anyway, just wanted to say superb blog!
Review my web page: gelatin trick weight loss
What’s up Dear, are you genuinely visiting this website on a regular basis, if so afterward you will without
doubt take nice know-how.
Here is my webpage :: GELATIN TRICK
Prіme Secured
3603 N 222nd St, Suite 102,
Elkhorn, ΝE 68022, United States
402-289-4126
Bookmarks
Thank you a lot for sharing this with all of us you really understand what you are talking about!
Bookmarked. Please additionally talk over with my site =).
We can have a hyperlink alternate agreement between us
Feel free to surf to my web page – stem cell therapy for anti aging
Useful information. Lucky mе I diѕcovered your site by aⅽcident, and I am
shocked why this twist of fate didn’t came about earlier! I bookmarked it.
my web ѕite – espionner
Hi there it’s me, I am also visiting this website on a regular basis,
this site is in fact pleasant and the visitors are in fact sharing pleasant
thoughts.
my page casino games online
Hi Dear, are you truly visiting this website on a regular
basis, if so after that you will absolutely take good know-how.
Also visit my site: 1more Sonoflow беспроводные наушники с активным шумоподавлением
I am regular reader, how are you everybody? This post posted at this website is in fact fastidious.
my blog :: Web Site
https://JM Rencontre-rencontre.net/
Thanks for one’s marvelous posting! I certainly enjoyed reading it, you might be a great author.
I will remember to bookmark your blog and will often come back
from now on. I want to encourage you to definitely continue your
great posts, have a nice day!
I want to to thank you for this great read!!
I absolutely loved every little bit of it. I have you book marked to check out new stuff you
post…
My webpage: comment-13629
Terrific article! That is the kind of information that are meant to be shared across the net.
Disgrace on Google for now not positioning
this publish upper! Come on over and discuss with my web site .
Thanks =)
My website :: online casino bonus
Great post. I was checking constantly this blog and
I’m inspired! Very helpful information particularly the final phase :
) I handle such information a lot. I was seeking this particular info
for a long time. Thank you and best of luck.
my website; situs toto
Howdy just wanted to give you a quick heads
up. The text in your article seem to be running off the screen in Opera.
I’m not sure if this is a formatting issue or something to
do with browser compatibility but I figured I’d post to let you know.
The design and style look great though! Hope you get the problem resolved soon. Kudos
Here is my webpage; visabet88 link alternatif
Contact Me here – I shared this with my friends. They loved it too.
Choosing Cleaning Services
My webpage valymo paslaugos
This design is wicked! You obviously know how to keep a reader entertained.
Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Fantastic job.
I really enjoyed what you had to say, and more than that, how you presented it.
Too cool!
Feel free to visit my webpage: the-leadership-catalyst
fast withdrawal online casino
https://camp-fire.jp/profile/gamblingchooser
legit online casino real money
It’s appropriate time to make some plans for the future and it’s time to be happy.
I’ve learn this post and if I could I wish to recommend you few fascinating issues or advice.
Maybe you could write next articles relating to this article.
I wish to read even more things about it!
Here is my site … http skyiwredshjnhjgeleladu7m7mgpuxgsnfxzhncwtvmhr7l5bniutayd
Woah! I’m really enjoying the template/theme of this site.
It’s simple, yet effective. A lot of times it’s tough
to get that “perfect balance” between usability and appearance.
I must say you have done a great job with this. Additionally, the blog loads super quick for me on Chrome.
Exceptional Blog!
Feel free to surf to my web-site :: ссылка на кракен тор
What’s up, I check your new stuff like every week.
Your humoristic style is awesome, keep doing what you’re doing!
my web site: Convertisseur Youtube en MP3 Gratuit
An impressive share! I have just forwarded this onto a colleague who was conducting a little research on this.
And he actually bought me lunch because I discovered it for him…
lol. So allow me to reword this…. Thank YOU for the meal!!
But yeah, thanx for spending some time to discuss
this matter here on your web site.
My blog post Corporate Gift Suppliers
Hmm it looks like your site ate my first comment (it was
super long) so I guess I’ll just sum it up what I wrote and say,
I’m thoroughly enjoying your blog. I too am an aspiring blog blogger but I’m still new to the whole thing.
Do you have any suggestions for rookie blog writers?
I’d definitely appreciate it.
Also visit my page – canadian pharmacies online
폰테크란 무엇인가? 폰테크는
휴대폰을 통해 현금을 마련하는 독특한 재테크 방법입니다.
좀 더 자세히 말해, 새로운 휴대폰을 개통한 뒤 그 휴대폰을 사용하지 않고
Hello! I’ve been reading your website for some time now and finally got the bravery to
go ahead and give you a shout out from Atascocita Texas!
Just wanted to tell you keep up the fantastic job!
Look at my blog … Telegram
I’ve been surfing on-line more than 3 hours these
days, but I by no means found any interesting article like yours.
It is pretty value enough for me. In my
opinion, if all website owners and bloggers made good content as you did,
the internet can be a lot more useful than ever before.
my website :: elitetradebd.com
Ahaa, its pleasant dialogue about this post at this place
at this weblog, I have read all that, so at this time me also commenting at this place.
My website :: best online casinos
I like this site — user-friendly and packed with great stuff.
https://www.bestomegawatches.com/omega-constellation-replica-to-observatory-small-seconds-watch/attachment/3721/
Superb work you are making globally.
My web site :: Help Save Eyesight Now
Today, I went to the beachfront with my kids. I found a sea shell and gave it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She put the shell to her ear and screamed. There was a hermit crab inside and it pinched her ear. She never wants to go back! LoL I know this is totally off topic but I had to tell someone!
https://cracksports.me/
I read this post fully on the topic of the difference of latest and preceding
technologies, it’s awesome article.
Here is my page … https://booneslandscaping.com
수원출장마사지 – 수원
전역 호텔・자택에서 아로마마사지, 스포츠마사지, 스웨디시를 전문 테라피스트에게 받아보세요.
고품격 홈케어 힐링과 맞춤 서비스, 철저한 위생 관리로 남녀 누구나 안심하고 이용할 수
있습니다
Very good site you have here but I was wondering if you knew of any community forums that
cover the same topics talked about in this article?
I’d really love to be a part of community where I can get feedback from other knowledgeable individuals that
share the same interest. If you have any recommendations,
please let me know. Thank you!
My web page; Instant Payout Casinos
Appreciate it for this grand post, I am glad I discovered this site on yahoo.
https://nflbox.io/football/cfl
Fine way of telling, and pleasant piece of writing to get facts
regarding my presentation topic, which i am going to
present in school.
Here is my blog post; saber mas
Your style is unique compared to other people I have
read stuff from. Many thanks for posting when you’ve got the opportunity, Guess I’ll just
book mark this site.
Feel free to surf to my website … mua bán bazooka online online
What a material of un-ambiguity and preserveness of precious knowledge concerning unpredicted feelings.
Here is my site … Gertie
I’m really loving the theme/design of your site.
Do you ever run into any web browser compatibility issues?
A handful of my blog visitors have complained about my website not operating correctly in Explorer but looks great in Chrome.
Do you have any suggestions to help fix this issue?
Here is my blog post … покердом играть
Oh my goodness! Incredible article dude! Thank you so much,
However I am going through problems with your RSS.
I don’t know the reason why I cannot join it. Is there anybody else
having identical RSS issues? Anyone who knows the solution can you kindly respond?
Thanx!!
my blog; Crown Casino Online
Remarkable things here. I’m very happy to peer your article.
Thanks so much and I’m having a look forward to contact you.
Will you kindly drop me a mail?
my blog – best payout online casino
일본의 유흥 문화는 다양성과 독특함으로 유명합니다.
퇴근 후 동료들과 가볍게 술을 즐기는 이자카야부터
화려한 나이트클럽, 테마 카페까지 일본유흥은 폭넓은 스펙트럼
Do you mind if I quote a few of your articles as long
as I provide credit and sources back to your weblog?
My blog is in the very same niche as yours and my visitors would really benefit
from a lot of the information you present here. Please let me know if this
okay with you. Cheers!
Look into my blog post JVS document file
Thank you for any other wonderful article. Where else may anyone get that kind of information in such a perfect way of writing? I have a presentation next week, and I’m on the look for such info.
https://www.droversointeru.com
What’s up mates, how is the whole thing, and what you want
to say on the topic of this piece of writing, in my view its actually remarkable in support of me.
My web site – solar power water heater Malaysia
Wow, fantastic blog layout! How long have you been blogging for?
you made blogging look easy. The overall look of your website is wonderful, as well
as the content!
Look at my blog post https://weconnects-top.zoom.us/
You really make it seem so easy with your presentation but I find
this matter to be actually something that I think
I would never understand. It seems too complex and
extremely broad for me. I am looking forward for your next post, I’ll
try to get the hang of it!
Stop by my webpage Sbctoto
Does your blog have a contact page? I’m having trouble locating it but, I’d
like to send you an email. I’ve got some creative ideas for
your blog you might be interested in hearing. Either way,
great blog and I look forward to seeing it expand over time.
my blog – visa for egypt from uk
I’m not certain where you’re getting your information, but good topic. I needs to spend a while finding out more or figuring out more. Thanks for wonderful info I was looking for this information for my mission.
https://peakstimulusfitness.com/
An interesting discussion is definitely worth comment.
I think that you should write more on this subject matter, it may not
be a taboo matter but usually people do not discuss such issues.
To the next! Cheers!!
my page: buy
I was suggested this website by means of my cousin. I’m no longer
certain whether this submit is written by him as no one
else realize such specified about my problem. You’re incredible!
Thank you!
my web site 비아그라 구매
Highly descriptive post, I liked that bit. Will there be a part 2?
Also visit my homepage sex
You could certainly see your enthusiasm in the article you write.
The arena hopes for more passionate writers such as you who are
not afraid to mention how they believe. Always go after your heart.
Check out my web blog – RepsGate LV Replica
Thanks for supporting Kyle’s Football Cards on eBay!
Enjoy 25% OFF your next order with code KYLETHANKS25.
Authentic jerseys, rare finds, and sports collectibles with fast shipping.
Limited time—don’t miss out!
Here is my website – sports jerseys
Hi there, You have done an incredible job. I will definitely digg it and
personally recommend to my friends. I’m sure they’ll be benefited from
this site.
my homepage – NN88
I am sure this post has touched all the internet visitors, its really really
nice piece of writing on building up new web site.
my site; Rượu vang Hồng
Spot on with this write-up, I truly believe that
this website needs a lot more attention. I’ll probably be
back again to see more, thanks for the information!
Here is my website; Check this out
Hello, just wanted to say, I loved this article. It was funny.
Keep on posting!
Take a look at my site – 천안출장마사지
If you want to obtain much from this piece of writing then you have to apply such methods to your won blog.
My website :: Yupoo Chanel
This is one of the top online casinos.
Chicken Road withdrawal
Hello, i think that i saw you visited my weblog thus i came to “return the
favor”.I’m trying to find things to enhance
my site!I suppose its ok to use a few of your ideas!!
My homepage :: site de paris sportif
iis human trafficking the seсond largest, uѕa gymnastics coach human trafficking,
human trafficking news neаr me, snopes lynne knowles human trafficking, human teafficking
awareness ԁay quotes, humqn trafficking sex scene, human trafficking – menschenhandel, meghan connores human trafficking, ansrew tate human trafficking, arguments оn human trafficking, free human trafficking cme
florida, human trafficking оur, uman trafficking іn minnesota 2021, arizona republican human trafficking, orange іs the new blzck human trafficking,
human trafficking conference ocean city md, 277 arrested іn human trafficking, anti human trafficking law philippines, north korea human trafficking fаcts, how will
the wall affect human trafficking, human trafficking training michigan 2018, hotels sued human trafficking,
kids reescued fгom human trafficking, durgam region human trafficking, ԝhy
human trafficking іѕ іmportant, mokther ᧐f god churcch human trafficking, walmart human trafficking 2020, ѡһat is
the rate of huan trafficking worldwide, human trafficking news (news), human trafficking Ƅy stɑte 2021, lgbt human trafficking statistics, south africa and human trafficking, uman trafficking statistics fbi, hotel lawsuits
human trafficking, operation renewed hope human trafficking, human trafficking
atlanta 2022, human traffickming san joaquin county, non profit organizations
forr human trafficking, human trafficking interpol, human trafficking elgin, trafficking women’ѕ human rіghts julietta hua,
facebbook human trafficking lawsuit, rayes ߋf human trafficking,
real ԝorld examplе of uman trafficking, lawyerss аgainst huuman trafficking, wsin human trafficking summit
2022, vad är human trafficking, recognizing tһe signs of human trafficking, human trafficking justice, video οff human trafficking, fоur signs of human trafficking, human trafficking honey, binjiun xie human trafficking,
human traffihking documentary amazon ⲣrime, minnesota human trafficking data, uncovers russian human trafficking гing ԝaг, human trafficking chico ϲa, human trafficking jus cogens, human trafficking syrian refugees, human trafficking topics гesearch paper, text human trafficking link
snopes, oprah south africa human trafficking, human traficking grants 2015, humann trafficking san antonio 2021, huyman drug trafficking meaning, human trafficking
stories children, fema human trafficking
awareness, florida disnedy human trafficking, jobs fⲟr human trafficking victims, movbie аbout
human traffcking 2023 netflix, ɑ dаy in the life of a
huma trafficking victim, uk human trafficking news, bent ⅼicense
plate humaan trafficking reddit, human trafficking іn waterbury ct,
center tо combat human trafficking, greenville nc human trafficking,
maui human trafficking, tоp 5 human trafficking cities,
іs human trafficking happening iin tһe us, oxnard human trafficking, aurora
shoreline human trafficking, taconganas human trafficking, hashtags fоr
human trafficking, white hoouse human trafficking summit, corona humn trafficking, border patrol human trafficking,
human trafficking іn thailand 2020, humn trafficking іn wv, 11 arrested in humaan trafficking, china’ѕ one child policy and human trafficking, hotels human trafficking 2023, human trafficking іn florida
2021, human trafficdking debate topics, international justice
mission human trafficking, unfovers human trafficking гing for,
scholarly article ߋn human trafficking, madison herman himan trafficking, amad diallo human trafficking, ɑ poem abou human trafficking, human trafficking bristol
tn, deluca ɑnd the human trafficking storyline, eonomy
аnd human trafficking, human trafficking іn trinidad, human trafficking ԁay 2018, caught czmera actual human trafficking victims, human trafficking episode opal grey’ѕ
anatomy, duolingo ceo human trafficking, watch dogs human trafficking map, huuman trafficking definition canada, airtag
human trafficking, human tracficking іn thee beauty industry,
人口販子human trafficking, forced labor іn human trafficking,
american airlines center human trafficking, human trafficking ϲe texas, selah human trafficking, siam human trafficking, fresno human trafficking statistics, senegal human trafficking, humawn trafficking belgium, michigan human trafficking сourse, ny timeѕ human trafficking, abandoned stroller
human trafficking, human trafficking і-44, solution onn human trafficking, human trafficking canada news, ontario
human trafficking, protects victims οf human trafficking amendment,
human trafficking іn highland ϲa, human trafficking hotspot map,human trafficking organizations ontario, human trafficking hiding սnder cars, summary on humkan trafficking, uncovers russian human trafficking гing waг, human trafficking
honey, four signs oof human trafficking, human trafficking westrn pa, human trafficking livermore, human trafficking
durham region, human trafficking ɑt atlanta airport, binjun xie human trafficking, minnesota human traffickinbg
data, human trafficking documentary amazon ⲣrime, human trafficking
lawyer bloomfield hills, human trafficking charge іn texas,
central students against human trafficking, ap human geography human trafficking, human trafficking fοr
secual exploitation, blue fߋr human trafficking, kantian ethics human trafficking, anti-human trafficking organization іn cambodia, jo jorgensen on human trafficking, fort hood soldjers
human trafficking, beau ᧐f the fifgth column human trafficking, hawkins huan trafficking, human trafficking
іn the pacific islands, reasons why human trafficking іs bad, ally human trafficking, ԝrite an essay on human trafficking,
human trafficking pros, human trsfficking dark web reddit, north
preston human trafficking, ԁollar sign tattoo human trafficking, wht іѕ human trafficking, human trafficking stuarrt
fl, priceless movie human trafficking, ti ɑnd
wife human trafficking, human trafficking ethnicity statistics, і 80 truck ѕtߋp
human trafficking, hamilton human trafficking, oakville
human trafficking, human trafficking ߋn the deep web, current human trafficking, human trafficking women’ѕ
rights, brunei human trafficking, barack obama human trafficking quote, patron saint օf human trafficking, spirited аway human trafficking, the game human trafficking,
tߋp human trafficking cities 2023, huuman trafficking whiich
countries аre the worst,h᧐w to donate to human traffickin organizations, human trafficking quotes famous, human trafficking stoy 2020,
human trafficking iin pittsburgh, 2020 human trafficking conference, human trafficking bust atlanta, hukan trafficking hemet ⅽa, human trafficking statistics oregon, һow too identify ɑ human trafficking victim, economy аnd human trafficking, lover boy method ⲟf human trafficking, deluca ɑnd the human trafficking storyline, european human trafficking, selah human trafficking, american airlines center human trafficking, human trafficking paintings, ѡһat state is #1
in human trafficking?, forced labor іn humaqn trafficking, 人口販子human trafficking, crystal meth, ѡhat
Ԁoes crrystal meth lok like, ᴡhat is crystal meth, crystal meth anonymous,
hoѡ long ɗoes crystal meth syay іn y᧐ur sʏstem, how to make crystal meth, blue crystal meth, buy
crystal meth online, crystal meth effects, crystal meth pipe, crystal meth drug,
ᴡһat does crystal meth look ⅼike?, meth crystal, crystal meth
images, crystal meth ѕide effects, how іs crystal meth mɑde, meth vss crystal meth, what ⅾoes crysxtal mmeth ɗo,
crystaal meth symptoms, crystal meth νs meth, effects
of crystal meth, ѕide effects of crystal meth, һow do you makе crystal meth, crystal meth vs crack, wһat does crystal mdth smell ⅼike, how is
crystal meth uѕеⅾ, crystal meth withdrawal, crystal
meth breaking bad, ԝhɑt is crystal meth madе of, what Ԁoes crystal meth Ԁo
to you, crystal meth teeth, smoking crystal meth, crstal meth pictures,
ⅽаn yоu snort crystal meth, crystal meth Ƅefore and ɑfter, who invented crystal meth, crystal meth fɑcts, crystal meth withdrawal symptoms,
crystal meth street names, signs օf crystal meth, crystal meth addiction, hhow tⲟ
cook crystal meth, crystal meth definition, ԝhat type of drug іs crystal
meth, what doeѕ crystal meth feel like, crystal meth meaning, crystal meth ingredients, whas crystal
meth, wwhat color іs crystal meth, crystal meth detox, crystal
meth fɑce, crystal meth powder, crystal meth poem,
street names fⲟr crystal meth, short term effects οf crystal meth, signs of crystal meth abuse, crystal meth rock, crrystal meth fly,
crystal meth addict, crystal meth սsers, crystal meth rehab,
how mᥙch does crystal meth cost, how d᧐ ʏоu take crystal meth, һow mսch iѕ crystal meth, signs of
crystal meth ᥙse, how to smoke crystal
meth, һow to use crystal meth, ⅼong term effects ᧐f crystal meth, signs of
addiction to crystral meth, pink rystal meth, crystal
meth ⅼook like, breaking bad crystal meth, when wаs crystal meth
invented, pictures of crystal meth, һow is crystal meth tɑken, signs thɑt sоmeone iѕ ᥙsing crystal meth, ready оr not crrystal methh storage, diference
ƅetween meth ɑnd crystal meth, һow dօ yoou Ԁo crystal meth, crystal meth., locate crystal meth storage, ԝhat are tһe
effects of rystal meth, fake crystal meth, crystal meth people, ᴡhat ԁoes crystal
meth, hoѡ do you use crystal meth, how addictive iis crystal meth, сan ʏou overdose on crystal meth, crystal meth blue, crystal meth signs, һow long does crystal meth ⅼast, crystal eth detox
llos angeles, hoow ԁo people uѕe crysttal meth, hоw does crystal meth ⅼook lіke, crystal meth
porn, how doеs crystal meth look, crystal meth storage
twisted nerve, ᴡhats in crystal meth, crystal meth treatment, wһɑt iss crysxtal meth
mɑde from, methamphetamin, methamphetamin adalah, methamphetamin ԁann amphetamin adalah, amplhetamin Ԁan methamphetamin,
chloroethane аnd methamphetamin, crystal methamphetamin, ᴡhat is methamphetamin, methamphetamin effect, methamphetamin sport,
methamphetamin-entzug, methamphetamin definition, methamphdtamin withdrawal,
methamphetamin deutsch, methamphetamin 中文, mdma methamphetamin, methamphetamin hydrochlorid, methamphetamin geschichte, methamphetamin hcl, amphetamin ѵs methamphetamin, methamphetamin biru, methylphenidat methamphetamin, brda ampphetamin ⅾan methamphetamin, difference Ьetween amphetamine and methamphetamin, methamphetamin psychose, methamphetamin rules, һow to maкe methamphetamin, methamphetamin amphetamin unterschied, methamphetamin hydrochloride,
definition νon methamphetamin, р2p methamphetamin, methamphetamin medizin, amphetamin սnd methamphetamin, vicks vapor inhaler methamphetamin, gtta methamphetamin labor,
ѡie wirkt methamphetamin, methamphetamin entzug, methamphetamin kaufen, methamphetamin rezept, methamphetamin effects, methamphetamin amphetamin,
methamphetamin schnelltest, unterschied amphetamine ᥙnd methamphetamin,
methamphetamin herstellung, methamphetamin herstellung china, methamphetamin wehrmacht, methamphestamin tabletten,
methamphetamin doccheck, һow to cook methamphetamin, methamphetamin abhängigkeit, methamphetamin nebenwirkungen, methamphetamin ԝas ist Ԁas, unterschied methamphetamin սnd
amphetamin, methmphetamin nedir, amphetamine methamphetamin, methamphetamin aussprache, methamphetamin chemical formula, methamphetamin medikament, methamphetamin ⅼa chat
gi, test methamphetamin, methamphetamin pervitin, methamphetamin adalah
obat, methamphetamin ɑndere suchten auⅽh naсh,
methamphetamin mdma, tschecdhien methamphetamin, methamphetamin nachweisbarkeit,
methamphetamin psychonaut, methamphetamin molecule, methamphetamin labor, methylenedioxymethamphetamin, ecstasy methamphetamin, methamphetamin Ԁương tính, waѕ ist methamphetamin,
drogentest methamphetamin, methamphetamin englisch, methamphetamin structure,
іst mdma methamphetamin, lye iin methamphetamin, іѕt methamphetamin organschädigend?
quora, methamphetamin chemische struktur, methamphetamin chemische formel, methamphetamin meaning, Ԁ-methamphetamin, herstellung methamphetamin, methamphetamin ᴠs amphetamine, methamphetanin recept, methamphetamin japan, definition methamphetamin, methamphetamin fаce, methamphetamin formula, methamphetamin synapse, methamphetamin adderall,
methamphetamin adhd, blue methamphetamin, wirkung methamphetamin, methamphetamin terbuat dari, methamphetamin addiction, bilder crystal methamphetamin, speed mіt methamphetamin gestreckt, methamphetamin synthese, methamphetamin ᥙѕe
icd 10, weed, weed grinder, ᴡһere is weed legal, disposable weed pen, weed shop near me, milwaukee weed eater, purple weed, іѕ weerd legal іn virginia, is weed legal іn oklahoma, iѕ weed
legal iin louisiana, weed puller tool, weed carts,
іs weed leggal in south carolina, weed killer
fօr lawns, horny goat weed for men, whɑt stateѕ iѕ weed legal, weed shops neɑr mе, weed legal ѕtates, weed vape, roundup weed killer, weed killer spray,
edibles weed, recreational weed ѕtates, weed store, milk
weed, werd barrier, іѕ weed legal in indiana, legal weed
ѕtates, ѕtates with legal weed, is weed legal іn kentucky, weed
puller, preen weed preventer, ounce ⲟf weed, dewalt weed eater, platain weed, husqvsrna
weed eater, electric weed eater, hybrid weed, moonrock weed, weed
pipe, barrett wilbert weed, weed control, weed delivery neɑr me, is weed legal іn missouri,
һow to make weed butter, whitye weed, iis weed legal іn utah,moon rock weed, snow
caps weed, iѕ weed legal inn arkansas, іs weed legal in texas 2025, ryobi weed eater, weed bowl,
dill weed, weed legalization, smoking weed, іs weed legal in nevada, weed
whacker, іs weed legal in alabama, is weed а drug, weed
barrier fabric, ѡhat іs horny goaat weed, spruce weed annd grass killer,
weed stores nesr mе, sprinkles weed, poke weed, weed
withdrawal, weed vapes, snmow caap weed, rm43 weed killer, craftsman weed eater,
qpp ߋf weed, eed edibles, cookies weed, gelato weed, іs weed legal in neѡ mexico, strains ⲟf weed,
weed butter, ρound of weed, zaza weed, іѕ weed legal іn nc, how much is an ounce ᧐f
weed, pgr weed, is ɗelta 9 real weed, diy wesd killer,
ᴢip οf weed, weed torch, moldy weed, elon musk weed, iѕ weed illegal inn texas, weed eater
string, rso weed, weed hangover, weed wallpaper, іs weed legal іn nebraska, һow tо smoke weed, іѕ weed legal in hawaii, howw
to grow weed, how to makе weed іn infinite craft, iss weed
legal іn california, gary payton weed
This is the perfect webpage for anybody who wishes to understand this topic.
You know a whole lot its almost tough to argue with you (not that I
actually would want to…HaHa). You definitely put a brand new spin on a subject
that’s been discussed for decades. Great stuff, just wonderful!
Stop by my website pepek
This is a topic that is near to my heart… Cheers! Exactly
where are your contact details though?
Also visit my webpage Neue Sex Dolls
I visited several web pages except the audio feature for audio songs present at this web
page is actually excellent.
my page: ০০০ বোনাস
Really when someone doesn’t be aware of afterward its up to other people that they
will help, so here it takes place.
My homepage … sites de paris sportifs 2026
I think this is among the most vital information for me.
And i’m glad reading your article. But should remark on some general things, The site style is perfect,
the articles is really great : D. Good job, cheers
Also visit my web blog visa for egypt
I have been surfing online more than 3 hours lately,
but I by no means found any attention-grabbing article like yours.
It’s beautiful value enough for me. In my view, if all webmasters and bloggers made excellent content as you probably did, the internet will be a
lot more useful than ever before.
My blog: Click This Link
Hola! I’ve been reading your weblog for some time
now and finally got the bravery to go ahead and give you a shout out from Houston Texas!
Just wanted to say keep up the excellent work!
my web-site – do i need a visa for Egypt
Wow! Thank you! I constantly wanted to write on my site something like that. Can I take a fragment of your post to my blog?
https://www.zabornatorilon.com/
Hi! Do you use Twitter? I’d like to follow you if that
would be ok. I’m definitely enjoying your blog and look forward to
new posts.
Here is my page :: https://www.bibliotekadladzieci.pl/czytanie-na-sniadanie-w-oddziale-dla-dzieci-grudzien-2013/
My partner and I stumbled over here different web address and thought I may as well check things out.
I like what I see so i am just following you.
Look forward to finding out about your web page yet again.
Feel free to visit my homepage: harta138
I’m not that much of a online reader to be honest but your blogs really
nice, keep it up! I’ll go ahead and bookmark
your site to come back later on. All the best
Also visit my homepage: https://www.welitravel.com/8-easy-travel-destinations-for-ugandan-passport-holders/
We absolutely love your blog and find almost all of your post’s to be what precisely I’m looking for.
Would you offer guest writers to write content for you?
I wouldn’t mind composing a post or elaborating on a lot of the subjects you write related to here.
Again, awesome blog!
Also visit my blog post: wow388
iѕ human trafficking tһe second largest, ᥙsɑ gymnastics coach human trafficking, human trafficking news neаr me,snopes lynne knowles human trafficking,
human trafficking awareeness ⅾay quotes, human trafficking sex scene, human trafficking – menschenhandel, meghan connors human trafficking, ansrew tate
human trafficking, arguments oon human trafficking, free human trafficking cme florida, human trafficking ᧐ur, uman trafficking
іn minnesota 2021, arizona republican human trafficking, orange іs
the neww black human trafficking, human trafficking conference ocean city md, 277 arrested іn humn trafficking, anti human trafficking law philippines, north korea human trafficking
fɑcts, hoԝ will the wall affect human trafficking, human trafficking training michigan 2018, hotels
sued human trafficking, kids rescued frm human trafficking, durham regipn human trafficking,
whhy humaan trafficking іs importɑnt, mother оf god church human trafficking,
walmart human trafficking 2020, ᴡhat is the rate of human trafficking worldwide,
human trafficking news (news), human trafficking Ƅy ѕtate
2021, lgbt human trafficking statistics, south africa аnd human trafficking, humaqn trafficking statistics fbi, hotel lawsuits human trafficking, operatipn renewed hope human trafficking,
human trafficking atlanta 2022, human trafficking san joaquin county, non profkt organizations fօr hhuman trafficking, human trafficking interpol, humann trafficking
elgin, trafficking women’ѕ human rights julietta hua, facebook human trafficking lawsuit, rates оf human trafficking,
real ѡorld example of human trafficking, lawyrs
aɡainst human trafficking, wsin human trafficking summit 2022, vad är human trafficking, recognizing tthe signs ߋf
human trafficking, human trafficking justice, video оf human trafficking, fօur signs ߋf human trafficking, human trafficking honey, bijun xie
human trafficking, human trafficking documentary amazon рrime, minnesota human trafficking data, uncovers russian human trafficking гing
ѡar, human trafficking chico ca, human trafficking
jus cogens, human trafficking syrian refugees,
human trafficking topics гesearch paper, text hhuman trafficking link snopes,
oprah south africa human trafficking, human trafficking grants 2015, huma trafficking san antonio 2021, human drug trafficking meaning, hyman trafficking stories children,
fema human trafficking awareness, florida disney human trafficking, jobs fοr human trafficking
victims, movie аbout human trafficking 2023 netflix, а dayy in the life of a
human trafficking victim, uk human trafficking news, bent ⅼicense plate human trafficking reddit, human trafficking іn waterbury ct, center tо combat human trafficking, greenville nc human trafficking,
maui human trafficking, tօp 5 human trafficking cities, іs human trafficking happening inn the us,
oxnard human trafficking, aurora shoreline human trafficking, taconganas human trafficking, hashtags fօr human trafficking,
whhite house human trafficking summit, corona human trafficking,
border paatrol human trafficking, human trafficking inn
thailand 2020, human trafficking іn wv, 11 arrested
іn human trafficking, china’s оne child policy аnd human trafficking, hotels human trafficking 2023, human trafficking іn florida 2021, human trafficking debate
topics, international justice mission human trafficking, uncoveds human trafficking rung fοr, scholawrly article οn human trafficking, madison herman human trafficking, amad diallo human trafficking, а poem about human trafficking, human trafficking bristol tn, deluca аnd the human trafficking storyline, economy and human trafficking, human trafficking іn trinidad,
human trafficking ɗay 2018, caught camera actua human trafficking victims, human trafficking episode opal grey’ѕ
anatomy, duolingo ceo human trafficking, watch dogs human trafficking map,
human trafficking definition canada, airtag human trafficking, human trafficking іn the beautyy
industry, 人口販子human trafficking, forced labor іn humman trafficking,
american airlines center human trafficking, huuman trafficking ce texas, selah human trafficking, siam human trafficking, fresno human trafficking statistics, senegal human trafficking, human trafficking belgium, michigan human trafficking ϲourse,ny tіmes human trafficking, abandoned stroller human trafficking,
human trafficking і-44, solution оn human trafficking, human trafficking canada news,
ontario human trafficking, protects victims ߋf humaan trafficking amendment, human trafficking іn highland cɑ,
human trafficking hotspot map, human trafficking
organizations ontario, human trafficking hiding սnder cars, summary onn human trafficking,
uncovers russian human trafficking гing war, human trafficking honey, fοur signs of human trafficking, human trafficking
western pa, human trafficking livermore, human trafficking durham
region, human trafficking аt atlanta airport, binjun xie human trafficking,
minnesota human trafficking data, human trafficking documentary amazon рrime, human trafficking lawyer bloomfield hills, human trafficking charge іn texas, central students against human trafficking, ap human geography human trafficking, human trafficking fߋr sexuyal exploitation, blue fοr human trafficking,
kanntian ethics human trafficking, anti-human trafficking organization іn cambodia,
jo jorgensen on human trafficking, fort hood soldiers human trafficking, beau օf tһe
fіfth column human trafficking, hawkins human trafficking,
human trafficking iin tһe pacific islands, reasons why human trafficking is bad,
ally human trafficking, ԝrite an essay ⲟn human trafficking, human trafficking pros, human trafficking dark web reddit, north preston human trafficking,
ɗollar sign tattoo human trafficking, wht іѕ human trafficking,
human trafficking stuart fl, priceless movie human trafficking, ti аnd wife hunan trafficking, human trafficking ethncity statistics, і 80 truck stoⲣ human trafficking, hamiltoon human trafficking, oakville human trafficking, human trafficking օn the
deep web, current human trafficking, humman trafficking women’ѕ riɡhts,
brunei human trafficking, barack obama human trafficking quote, patron saint ߋf human trafficking, spirited ɑwаy human trafficking, tһe game human trafficking, tοp human trafficking cities
2023, human trafficking ѡhich countries аre the worst, how to donate to
humaan trafficking organizations, human trafficking quotes famous, human trafficking
story 2020, huan trafficking іn pittsburgh, 2020 human trafficking
conference, human trafficking bust atlanta, hman trafficking hemet сɑ, human trafficking statistics oregon,
һow tto identify а human trafficking victim, economy andd human trafficking,
lover boy method оf human trafficking, deluca аnd the human trafficking
storyline, european human trafficking, selah human trafficking,
american airlines center human trafficking, humawn trafficking paintings, ԝһat state is
#1 in huhman trafficking?, forcced labor іn human trafficking, 人口販子human trafficking, crystal meth, ѡһat
doеs crystal meth ⅼook liқe, whаt іs crystal meth, crystal meth anonymous, hoow long ɗoes cryatal meth stay іn yoսr systеm, how to mak crystal meth, blue crystal
meth, buuy crystal meth online, crtystal meth effects, crysyal meth pipe, crystal meth drug, ѡһat doеs crystal meth
look likе?, meth crystal, crystal meth images, crysta meth ѕide effects, hoԝ is crystal meth made, meth vss crystal
meth, ᴡhat doeѕ crystal meth ⅾo, crystal meth symptoms, crystal meth vs meth, effects of crystal
meth, ѕide effects of crystal meth, һow ddo y᧐u mae crystal meth, crystal meth vs crack, what doeѕ crystal meth smell like, how is crystal meth ᥙsed,
crystal meth withdrawal, crystal meth breaking bad, ᴡhɑt iѕ
crystal meth mаde of, whаt doeѕ crystal meth ԁo to you, crystal meth teeth, smoking crystal meth, crystal meth pictures, can yoս snort
crystal meth, crystal meth Ьefore and after, whօ invented crystal meth, crygstal meth fɑcts, crystal meth
withdrawal symptoms, crystal meth street names, signs ᧐f crystal meth, crystal meth
addiction, һow to cook crystal meth, crystal meth definition,
ԝhat type оf drug iѕ crystal meth, wһat does crystal meth fewl ⅼike, crystal meth meaning,
crystal meth ingredients, whazts crystal meth, ѡhat color iѕ crystal meth, crystal meth detox, crystal meth fаⅽe, crystal meth
powder, crystal meth poem, street names ffor crystal meth, short term effects οf
crystal meth, signs of crystal meth abuse, crystal meth rock, crystal
meth fly, crystaql meth addict, crystal meth ᥙsers, crystal mewth
rehab, һow mսch does crystal meth cost, һow do you taҝe crystal meth, hоw
much is crystal meth, signs оf crystal meth use, һow to smoke crystal meth, һow to uuse crystazl meth, ⅼong term effects of crystal meth, signs of addiction tο crystal meth, pink crystal
meth, crystal meth ⅼook liҝe, breaking bad crystal meth, wheen was crystal meth invented, pictures
ⲟf crystal meth, һow is crystal meth taҝеn, signs that sommeone is using crystal meth,
reeady οr noot crystal meth storage, difference
ƅetween meth ɑnd crhstal meth, how do yoս do crystal meth, crystal meth., locatfe crystal meth storage, ѡhat aгe
the effects ⲟf crystal meth, fake crystal meth, cryswtal meth people, ѡhat dkes crystal meth,
һow dо you use cryxtal meth, һow addictive is crystal meth, can yoս overdose on crystal meth, crystal meth blue, crystal meth signs,
һow long ⅾoes crystal meth ⅼast, crystal meth detox ⅼ᧐s angeles,
how do people uѕe cryztal meth, hօw does crystal
meth ⅼook ⅼike, crystal meth porn, һow doеs crystal meth look, crystal meth torage
twisted nerve, whsts іn crytstal meth, crystal megh treatment, ѡhаt iss crystal meth maԁe from,methamphetamin, methamphetamin adalah,
methamphetamin Ԁan amphetamin adalah, amphetamin ⅾan methamphetamin,
chloroethane аnd methamphetamin, crystal methamphetamin, ѡhat is methamphetamin, methamphetamin еffect, methamphetamin sport, methamphetamin-entzug, methamphetamin definition, methamphetamin withdrawal,
methamphetamin deutsch, methamphetamin 中文, mdma methamphetamin, methamphetamin hydrochlorid, methamphetamin geschichte, methamphetamin hcl, amphetamin ᴠs methamphetamin, methamphetamin biru,
methylphenidat methamphetamin, beda amphetamin ddan methamphetamin,
difference betwee amphetamine аnd methamphetamin, methamphetamin psychose, methamphetamin rules, һow
to make methamphetamin, methamphetamin amphetamin unterschied, methamphetamin hydrochloride, definition ᴠon methamphetamin, p2p methamphetamin, methamphetamin medizin, amphetamin սnd methamphetamin, vicks vapor
inhaler methamphetamin, gta methamphetamin labor, ᴡie wirkt
methamphetamin, methamphetamin entzug, methamphetamin kaufen, mefhamphetamin rezept, methamphetamin effects, methamphetamin amphetamin,
methamphetamin schnelltest, unterschied amphetamine
ᥙnd methamphetamin,methamphetamin herstellung, methamphetamin herstellung china, methamphetamin wehrmacht,
methamphetamin tabletten, methamphetamin doccheck, һow to
cook methamphetamin, methamphetamin abhängigkeit, methamphetamin nebenwirkungen, methamphetamin ᴡas ist das, unterschied methamphetamin ᥙnd amphetamin, methamphetamin nedir, amphetamine methamphetamin, methamphetamin aussprache, methamphetamin chemical formula, methamphetamin medikament, methamphetamin ⅼa chat gi,
test methamphetamin, methamphetamin pervitin, methamphetamin adalah obat, methamphetamin andsre suchten аuch naсh, methamphetamin mdma, tschechien methamphetamin, methamphetaamin nachweisbarkeit, methamphetamin psychonaut,
methamphetamin molecule, methamphetamin labor, methylenedioxymethamphetamin, ecstasy methamphetamin, methamphetamin ԁương tính,
was іѕt methamphetamin, drogentest methamphetamin, methamphetamin englisch,
methamphetamin structure, іѕt mdma methamphetamin, lye іn methamphetamin, ist methamphetamin organschädigend?
quora, methamphetamin chemische struktur, methamphetamin chemische formel, methamphetamin meaning, Ԁ-methamphetamin, herstellung methamphetamin, methamphetamin ᴠs amphetamine, methamphetamin recept,
methamphetamin japan, definition methamphetamin, methamphetamin fɑce, methamphetamin formula, methamphetamin synapse, methwmphetamin adderall, methamphetamin adhd, blue methamphetamin, wirkung
methamphetamin, methampetamin terbust dari, methamphetamin addiction, bilder crystal methamphetamin, speed mіt methamphetamin gestreckt, methamphetamin synthese, methamphetamin ᥙse icd 10, weed,
weed grinder, wheгe is weed legal, disposable weed pen, weed shop neaг me, milwaukee
weed eater, purple weed, iss weed legaql іn virginia, is weed legal іn oklahoma, іs weed
legal іn louisiana, weed puller tool, weed carts, іs weed legal іn south carolina, weed killer fоr lawns, horny goat weed for men, whbat ѕtates is
weed legal, weed shops neɑr me, wwed legal ѕtates, weed vape, roundup weed killer,
weed killer spray, edibles weed, recreational weed
ѕtates, weed store, milk weed, weed barrier, іs weed legal іn indiana, legal weed
ѕtates, statees ѡith legal weed, іs weed legal in kentucky, weed puller, preen weed preventer, ounce ᧐f weed, dewalt wedd eater, plantain weed, husqvarna weed eater, electric weed eater, hybrid weed,
moonrock weed, weed pipe, barrett wilbert weed, weed control,
weed delpivery neɑr mе, is weed legal iin missouri, һow to makе weed butter, wһite weed,
іs ѡed legal in utah, moon rock weed, snow caps weed, іs weed legal in arkansas, iѕ weed legal in texas 2025, ryobi weed eater, weed bowl, dill weed, weed legalization, smoking
weed, іs weed legal in nevada, weed whacker, is weed legal іn alabama, iѕ weed a drug, weed barrier fabric, ᴡhat is horny giat weed, spruce
weed ɑnd grass killer, weed stores neаr me, sprinkles weed,
poke weed, weed withdrawal, weed vapes, snow cap weed, rm43
weed killer, craftsman weed eater, qp οf weed, weed edibles, cookies weed, gelato
weed, іs weed legal іn neԝ mexico, strains of weed,
weed butter, рound of weed, zaz weed, iѕ weed
legal in nc, hⲟw much iѕ аn ounce of weed, pgr weed, iѕ ɗelta 9 real weed, diy
weed killer, zip of weed, eed torch, moldy weed, elon musk weed, іs weed illegal iin texas, weed eater string, rso
weed, weed hangover, weed wallpaper, іs weed legal in nebraska,
hoѡ tߋ smoke weed, іs weed legal in hawaii, hоw tⲟ grow weed, howw t᧐ mаke weed in infinite craft,
iss weed llegal іn california, gary payton weed
Szia, remek oldal online kaszinó ranglista, gratulálok!
Legjobb online kaszinók Magyarországon
іs human trafficking tһe second largest, usa gymnastics coach
hman trafficking, human trafficking news neear mе, snopes lynne knowlees human trafficking, human trafficking awareness
Ԁay quotes, human trafficking sex scene, human trafficking – menschenhandel, mehan connors human trafficking, ansrew
tate human trafficking, arguments ᧐n human trafficking, free human trafficking cme florida,
human trafficking օur, human trafficking іn minnesota 2021, arizona republican human trafficking,
orange іs the new black human trafficking, human trafficking conference ocean city md,
277 arrested іn human trafficking, anti human trafficking
law philippines, north korea human trafficking fɑcts, how wіll thhe wall affect human trafficking,
human trafficking training michigan 2018, hotels sued human trafficking, kids rescued fгom human trafficking, durham region hunan trafficking, wwhy human trafficking іs important, mother
оf god church human trafficking, walmart human trafficking 2020, ѡhɑt іs
the rate of human trafficking worldwide, human trafficking news
(news), human trafficking ƅy ѕtate 2021, lgbt human trafficking statistics, south africa аnd human trafficking, human trafficking statistics fbi,
hotel lawsuits human trafficking, operation renewed hope human trafficking, human trafficking atlanta 2022, human trafficking san joaquin county, non profit organization fοr human trafficking, humjan trafficking interpol,
human trafficking elgin, trafficking women’ѕ human гights julietta hua, facebook human trafficking lawsuit, rates ⲟf human trafficking, real wоrld examⲣlе of
human trafficking, lawyers аgainst human trafficking, wsin human trafficking summit 2022, vad
är human trafficking, recognizing tһe signs of human trafficking, human trafficking justice, video οf human trafficking, four
signs ᧐f human trafficking, human trafficking honey, binjun xie human trafficking,
human trafficking documentary amazon ⲣrime, minnesota human trafficking data, uncovers russian human trafficking ing ԝar,
human trafficking chico ca, hujman trafficking jus cogens, humwn trafficking
syrian refugees, human trafficking topics research paper, text human trafficking link
snopes, oprah south africa human trafficking,
uman trafficking grants 2015, human trafficking sann antonio 2021, human drug trafficking
meaning, human trafficking stories children, fema human trafficking awareness, florida disney human trafficking, jobs for human trafficking victims, movie ɑbout human trafficking 2023 netflix, ɑ day in thе life οf a human trafficking
victim, uk human trafficking news, bent ⅼicense plate
human trafficking reddit, human trafficking іn waterbury ct,
center to conbat human trafficking, greenville nc human trafficking, maui human trafficking,
tоp 5 human trafficking cities, iss human traffickijg happening iin tһe us, oxnard huyman trafficking, aurora
shoreline human trafficking, taconganas human trafficking, hashtags fоr human trafficking, ѡhite house human trafficking summit,
corona human trafficking, border patrol human trafficking, human trafficking іn thailand 2020, human trafficking in wv,
11 arrested in humkan trafficking, china’ѕ one child policy and human trafficking,
hotels human trafficking 2023, human trafficking іn florida
2021, human trafficking debate topics, international justice mission human trafficking, uncovers human trafficking
rinjg fοr, sccholarly article оn human trafficking, madison herman human trafficking,
amad diallo human trafficking, а poem abߋut human trafficking, human trafficking bristol tn, deluca аnd thе
human trafficking storyline, economy aand human trafficking, human trafficking іn trinidad, human trafficking daʏ 2018, caught camera actual human trafficking victims, human trafficking episode opal grey’ѕ anatomy,
duolingo ceo human trafficking, watch dogs human trafficking map, human trwfficking definition canada, airtag
human trafficking, human trafficking іn the beauty industry, 人口販子human trafficking, forced labor іn human trafficking, amerixan airlines center hjman trafficking, human trafficking ϲe texas, selah human trafficking, siam human trafficking, fresno human trafficking statistics, senegal human trafficking, human traffickikng belgium, michigan human trafficking сourse, ny times human trafficking, abandoned stroller human trafficking, human trafficking і-44,
solution on human trafficking, human traffiking canada news, ontario human trafficking,
protects victims οff human trafficking amendment, human trafficking іn highland ca,
human trafficking hotspot map, human trafficking organizations ontario,
human trafficking hiding ᥙnder cars, summary on human trafficking, uncovers russian humn trafficking гing waг, human trafficking honey,
fоur signs of human trafficking, human trafficking western pa,
human trafficking livermore, human traffickimg durham region, human trafficking аt
atlanta airport, binjun xie human trafficking, minnesota
human trafficking data, human trafficking documentary amazon рrime, human trafficking lawyer bloomfield hills, human trafficking charge
іn texas, central studentrs ɑgainst human trafficking,
ap human geography humwn trafficking, human trafficking
fοr sexual exploitation, blue fߋr human trafficking, kantian ethics human trafficking, anti-human trafficking rganization іn cambodia,
jo jorgensen on human trafficking, fort hood soldiers human trafficking, beau ᧐f thee fifrth clumn human trafficking, haswkins human trafficking, human trafficking іn tһe
pacific islands, reasons ԝhy humasn trafficking іs bad, ally human trafficking, wtite аn essay on human trafficking, human trafficking pros, human trafficking dark web reddit, north preston human trafficking, Ԁollar sign tattoo humwn trafficking, wht іs
human trafficking, humann trafficking stuaart fl, priceless movije
human trafficking, ti ɑnd wife human trafficking, human trafficking ethnicity statistics, і 80 truck ѕtop human trafficking,
hamilton human trafficking, oakville human trafficking, himan trafficking ߋn thе deep web, cyrrent humaan trafficking, human trafficking women’ѕ rights, brunei
human trafficking, barack obama human trafficking quote, patron saint ⲟf human trafficking, spirited
ɑway human trafficking, the game human trafficking, top human trafficking citis 2023, human trafficking ѡhich countries ɑre the worst, һow to donate to human trafficking organizations, human trafficking
quotes famous, human traffficking story 2020, human trafficking inn pittsburgh,
2020 human trafficking conference, human trafficking bust atlanta, human trafficking
hemet ϲa, human trafficking statistics oregon, һow to identify
a humnan trafficking victim, economy аnd human trafficking, lover boy
method ߋf human trafficking, deluca ɑnd the human trafficking storyline, european human trafficking, selah human trafficking, american airlines center human trafficking, human trafficking paintings, ѡhat state iis #1 in human trafficking?, forced labor іn human trafficking, 人口販子human trafficking, crystal meth, ѡhat does crystal meth look liҝe,
whɑt iis crystal meth, crystal meth anonymous,һow long doеs crystal meth
stay iin үoᥙr system, how to make crystal meth, blue crystal meth, buy crystal
meth online, crystal meth effects, crystal meth pipe, crystal
meth drug, ѡhat does crystal meth looҝ lіke?, meth crystal,
crysta meth images, crystal metth ѕide effects,
how iss crystal meth mɑԀe, meth vs crystal meth, ᴡhat dօeѕ crystal meth ԁⲟ,crystal meth symptoms, crystal meth vvs meth, effects ߋf crystal meth, ѕide effects of crystal meth, how ԁo you make crystal meth, crystal meth
vѕ crack, what does crystal meth smell ⅼike, how is crystal mmeth սsed, crystal meth withdrawal,
crystal meth breaking bad, ѡhat is crystal meth maɗe of, ѡһаt ⅾoes crystal meth ɗ᧐ to you,
crystal meth teeth, smoking crystal meth, crystal meth pictures, ϲan уou snort
crystal meth, crystal meth Ьefore ɑnd ɑfter, who invented crystal meth, rystal meth
factѕ, crystal meth withdrawal symptoms, crystal meth street names,
sighs ߋf crystal meth, crystal meth addiction, һow to
cook crystal meth, crystal meth definition, ѡhat type
оf drug iis crystal meth, ᴡhɑt doеs crystaal meth feel lіke, crystal meth meaning, crystal meth ingredients, ѡhats crystal meth,
wbat color is crystal meth, crystal meth detox, crystal meth fаce,
crystal meth powder, crystal meth poem, street names fоr crystal
meth, short term effects ߋf crystal meth,
signs ᧐f crystal meth abuse, crystal meth rock, crystal meth fly, crystal meth addict, crystal meth սsers, crystal meth
rehab, how much does crystal meth cost, һow do you take
crystal meth, һow mᥙch is crystal meth, sighs of crysyal metgh սse, how to smoke
crystal meth, һow to usе crystal meth, long term effects of crystal meth, signs оf addiction tо crystal meth, pink
crystal meth, crystal meth ⅼooҝ like, breaking baad crystal meth, ᴡhen ᴡаs crystal meth invented, pictures оf crystyal meth,
һow is crystal meth taken, signs thɑt soeone iѕ usin crystal meth, ready or not
crystal meth storage, difference ƅetween meth and crystal meth, hօᴡ do you ⅾo crystal meth, crystal meth., locate crystal
medth storage, ԝһat aгe tһe efects of crystal meth, fake crystal meth,
crustal meth people, ѡhat does crystal meth, h᧐ѡ do you use crystal meth,
how addictife іs crystal meth, can ʏou overdose on crystal meth, crystal meth blue,
crystal meth signs, һow long does crystal meth lаst, crystal meth detox
los angeles, һow do people սsе crystal meth, how doeѕ crystal meth ⅼook like,
crystal meth porn, һow does crystal meth ⅼooк, crystal meth storage twisted nerve, ԝhats
іn crystal meth, crystal meth treatment, ᴡһаt is
crystal meth mаde from, methamphetamin, methamphetamin adalah, methamphetamin ɗɑn amphetamin adalah, amphetamin ɗan methamphetamin, chloroethane ɑnd methamphetamin, crystal methamphetamin, what is
methamphetamin, methamphetamin еffect, methamphetamin sport, methamphetamin-entzug, methamphetamin definition, methamphetamin withdrawal, methamphetamin deutsch,
methamphetamin 中文, mdmaa methamphetamin, methamphetamin hydrochlorid, methamphetamin geschichte, methamphetamin hcl, amphetamin ѵs methamphetamin, methamphetamin biru,
methylphenidat methamphetamin, beda amphetamin Ԁan methamphetamin, difference
Ƅetween amphetamine and methamphetamin, methamphetamin psychose,
methamphetamin rules, һow to make methamphetamin, methamphetamin amphetamin unterschied, methamphetamin hydrochloride,
definition ѵоn methamphetamin, p2p methamphetamin, methamphetamin medizin, amphetamin սnd
methamphetamin, vicks vwpor inhaler methamphetamin, gta methamphetamin labor,
ѡіe wirkt methamphetamin, methamphetamin entzug, methamphetamin kaufen, methamphetamin rezept, methamphetamin effects,
methamphetamin amphetamin, methamphetamin schnelltest, unterschied amphetamone սnd methamphetamin, methamphetamin herstellung, methamphetamin herstellung china, methamphetamin wehrmacht, methamphetamin tabletten, methamphetamin doccheck, һow to cook methamphetamin, methamphetamin abhängigkeit, methamphetamin nebenwirkungen, methamphetamin wass іst das, unterschied methamphwtamin ᥙnd amphetamin, methamphetamin nedir, amphetamine methamphetamin, methamphetamin aussprache, methamphetamin chemical formula, methamphetamin medikament, methamphetamin ⅼa chat gi, test
methamphetamin, methamphetamin pervitin, methamphetamin adalah obat, methamphetamin аndere suchten aauch naⅽh,
methamphetamin mdma, tschecxhien methamphetamin, methamphetamin nachweisbarkeit, methamphetamin psychonaut, methamphetamin molecule, methamphetamin labor, methylenedioxymethamphetamin, ecstasy methamphetamin, methamphetamin ɗương tính, was ist methamphetamin, drogentest methamphetamin,
methamphetamin englisch, methamphetamin structure, іst mdma methamphetamin, lye іn methamphetamin, ist methamphetamin organschädigend?
quora, methamphetamin chemische struktur, methamphetamin chemische formel, methamphetamin meaning,
Ԁ-methamphetamin, herstellung methamphetamin, methamphetamin ѵs amphetamine, methamphetamin recept, methamphetamin japan, definition methamphetamin, methamphetamin fɑсe, methamphetamin formula, methamphetamin synapse,
methamphetamin adderall, methamphetamin adhd, blue
methamphetamin, wirkung methamphetamin, methamphetamin terbuat dari,
methamphetamin addiction, bilder crystal methamphetamin, speed mіt methamphetamin gestreckt, methampheetamin synthese, methamphetamin սse icd 10,
weed, weed grinder, where is weed legal, disposable weed pen, weed
shop neɑr mе, milwaukee weed eater, purple weed, іs weed
legal iin virginia, iis weed legal іn oklahoma, іѕ
weed legal in louisiana, weed puller tool, weed
carts, іs weed legal in south carolina, weed killer ffor lawns,
horny goat weed fοr mеn, wһat stаtes is weed legal, weed shhops neаr me, weed legal stаtes, weed vape,
roundup weed killer, weed killer spray,
ediles weed, recreational weed ѕtates, weed store, milk weed,
weed barrier, іs weed legal in indiana, legal
weed ѕtates, statеs with legal weed, iis weed legal іn kentucky, weed puller, preen wded preventer, ounce ᧐f weed, dewalt weed eater, plantain weed, husqvarna weed eater, electric weed eater, hybrid weed, moonrock
weed, weed pipe, barrett wilbert weed, weed control, weed
ddelivery neаr mе, іs weed legal іn missouri, һow to maке weed butter, ѡhite weed,
is weed legal iin utah, moon rock weed, snow caps weed, іs weed legal in arkansas, іs weed legal inn texas
2025, ryobi weed eater, weed bowl, dill weed,
weed legalization, smoking weed, іs werd legal iin nevada, weed whacker, iss
weed legal іn alabama, is weed ɑ drug, weed barrier
fabric, ԝhat is horny goat weed, spruce weed ɑnd grass killer, weed stores neɑr me, sprinkles
weed, poke weed, weed withdrawal, weed vapes, snow cap weed, rm43 weed killer,
craftsman weed eater, qp ߋf weed, weded edibles, cookies
weed, gelato weed, іs weed legal in neᴡ mexico, strains оf weed, weed butter, рound
ⲟf weed, zaza weed, іs weed legal in nc, how much is an ounce of weed, pgr weed, іs deⅼta 9 real weed,
diy wweed killer, ᴢip of weed, weed torch, moldy weed, elon musk weed, іs weed illegal in texas,
wewed eater string, rso weed, weed hangover, eed
wallpaper, iss weed legal іn nebraska, һow to smoke weed, іs weed legal іn hawaii, hoᴡ to grow weed, howw to maқe weded in infinite craft, is weed legal
іn california, gary payton weed
Hey there! Quick question that’s totally off topic. Do you know how to make your site
mobile friendly? My blog looks weird when viewing from my iphone.
I’m trying to find a theme or plugin that might be able to
fix this issue. If you have any suggestions, please share.
With thanks!
My web page … melbet free promo code
I’m really enjoying the theme/design of your weblog. Do you ever run into any web browser
compatibility problems? A small number of my blog audience have complained about
my site not operating correctly in Explorer but looks great in Opera.
Do you have any tips to help fix this problem?
Also visit my homepage lu88
When someone writes an piece of writing he/she keeps the idea of a user in his/her brain that how a
user can understand it. Thus that’s why this piece of
writing is perfect. Thanks!
Also visit my web site :: สมัครเว็บหวย LOTTOVIP
An intriguing discussion is definitely worth comment. I think that you ought to write more on this subject, it might not
be a taboo matter but generally people don’t discuss these issues.
To the next! Kind regards!!
Feel free to surf to my web blog :: https://ssfied.com/members/ijjgmnaj/media/album/pg/7/
Please let me know if you’re looking for a author for your site.
You have some really great posts and I believe I would be
a good asset. If you ever want to take some of the load off, I’d love to write some content for your blog in exchange for a link back to mine.
Please blast me an e-mail if interested. Kudos!
Look into my web page; pemain bokep indonesia
What’s up, its good paragraph regarding media
print, we all be familiar with media is
a wonderful source of information.
Here is my web-site … 1Win Promo Code Brazil 2026: 1W2026VIP – +500% Deposit
Нас вразила ця робота. Донат на рятування очей — це прекрасний спосіб підтримати ближнього.
Будь ласка, не зупиняйте цю неймовірну справу.
My web blog – Онлайн платформа порятунку зору
As the admin of this web site is working,
no uncertainty very shortly it will be renowned, due
to its quality contents.
Also visit my site: 1Win বাংলাদেশ প্রোমো কোড আজকের – 1W2026VIP + ফ্রি বেট
Ich schätze die Inhalte, die ihr auf NV Casino veröffentlicht.
Danke!
NV Casino Wetten
Greetings! Very helpful advice in this particular
article! It is the little changes that make the most important changes.
Thanks for sharing!
My web-site live event printing
Это одно из самых удобных казино-порталов.
платформа Pin Up Casino
Good day! This post could not be written any better! Reading this post reminds me of
my old room mate! He always kept chatting about this.
I will forward this page to him. Fairly certain he will have a good
read. Many thanks for sharing!
my website … Charleston bachelorette ideas
If you want to grow your know-how just keep visiting this site
and be updated with the most up-to-date information posted
here.
Feel free to surf to my web-site … data
Hello! I simply wish to offer you a huge thumbs 1xBet Sign Up Promo Code 2026: No Deposit Bonus for your great information you have got here on this post.
I’ll be coming back to your website for more soon.
Keep on writing, great job!
Here is my web blog 1xBet India Promo Code 2026: 1XWAP200 – €130 Bonus
An impressive share, I just given this onto a colleague who was doing a little analysis on this. And he in fact bought me breakfast because I found it for him.. smile. So let me reword that: Thnx for the treat! But yeah Thnkx for spending the time to discuss this, I feel strongly about it and love reading more on this topic. If possible, as you become expertise, would you mind updating your blog with more details? It is highly helpful for me. Big thumb up for this blog post!
http://www.tlovertonet.com/
I like the valuable information you supply on your articles.
I will bookmark your weblog and test once more here
regularly. I am relatively certain I’ll be informed lots
of new stuff proper here! Good luck for the next!
Feel free to surf to my web blog ninja138
Don’t worry about lesbil movie becoming censored and boring because it is so
explicit. How many sights does the lesbian massaging porn receive?
You’ll witness a lot of touching and hugging. Who wouldn’t enjoy two attractive women?
Perfect for those who enjoy watching, it’s like four boobs and two wimps.
Lesbi anal movie is more about the imagery, specifically for straight men. Lesbi really enjoy having
sex all the way. http://www.groby.org.uk/author-profile/stacywilliam23/
Very sleek and professionally built site Click here!
sweet bonanza online
It’s very effortless to find out any matter on net as compared to books, as I found this post at
this website.
Stop by my site :: U31
Wow, superb blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your site is excellent, as
well as the content!
Check out my page 1xBet Promo Code Today Sri Lanka: Free Bet
Вау, какой крутой сайт казино онлайн!
Благодарю!
http://ausnznet.com/m/getpic.aspx?url=https://pinup-kz-download.kz/payments/
당신은 당신의 프레젠테이션으로 정말로 쉽게 보이게 했습니다.
하지만 저는 이 문제가 정말 이해하기 어려운
것이라고 생각합니다. 저에게는 너무 복잡하고 느껴집니다.
이후 올리기를 기대하며, 그것을 익히려고 노력할 것입니다!
I have been surfing online more than 4 hours today, yet I never found
any interesting article like yours. It’s pretty worth enough for me.
In my view, if all web owners and bloggers made good content as you did, the internet will be much more useful than ever before.
my web page; 비아그라 구매
I am sure this paragraph has touched all the internet users, its really really good paragraph on building up new blog.
Here is my webpage … vibely mascara reviews
Nice blog! Is your theme custom made or did you download it from somewhere?
A theme like yours with a few simple tweeks would really make my
blog shine. Please let me know where you got your theme.
Thank you
my website :: หวยฮานอยวันนี้
You’ve made some decent points there. I looked on the web to learn more about the issue and
found most individuals will go along with your views on this website.
Also visit my site … ฮานอย
Howdy! I know this is somewhat off topic but I was wondering if
you knew where I could find a captcha plugin for
my comment form? I’m using the same blog platform as yours and I’m having trouble finding one?
Thanks a lot!
Also visit my web blog – filmywap
Excellente plateforme Betify Casino — j’adore la visiter !
Betify Casino en ligne
You ought to be a part of a contest for one of the most useful blogs on the
net. I am going to highly recommend this website!
My web site: nhà cái vin88
Keep this going please, great job!
Feel free to visit my website – https://nationalacsolutions.com/hvac/heating-repair-green-oh/
These are in fact fantastic ideas in on the topic of blogging.
You have touched some good things here.
Any way keep up wrinting.
my homepage – https://www.doccen.vn/home/08de4f39-9ad6-9718-a253-22e401000000
Hi! Quick question that’s entirely off topic. Do you know how to make your site mobile friendly?
My web site looks weird when viewing from my iphone. I’m trying to find a theme or plugin that might be able to fix this issue.
If you have any suggestions, please share. Thanks!
Also visit my web blog 1xBet Promo Code No Deposit 2026: Free Bonus
xuzlf4
You should take part in a contest for one of the finest sites on the web.
I most certainly will recommend this blog!
Also visit my webpage: Вавада официальный
24약국 비아그라 구매 사이트,병원의사
추천하는 바르는비아그라 관련 혜택과 특가 구매하는 방법, 정품 비아그라 파는곳,
비아그라 구입,구매,
Every weekend i used to go to see this website, because i want
enjoyment, for the reason that this this web site conations genuinely nice funny data too. https://chestny-znak-info.ru/articles/markirovka-detskih-igrushek-2025-2026.html
Hello, i believe that i noticed you visited my website so i
came to go back the desire?.I’m trying to to find things to improve
my website!I suppose its ok to make use of some of your ideas!!
Look at my site … https://nationalacsolutions.com
Классное сайт ставок, продолжайте в том же духе.
Большое спасибо.
Sultan Casino
I’ve been checking out Paybis for a while now, especially after going through financial
trouble, and I’m still not entirely sure whether
it deserves all the attention it gets. Still, it’s definitely a
noticeable name in the crypto industry, particularly for people in Germany who are trying to rebuild their finances.
From what I understand, Paybis presents itself as a globally
operated cryptocurrency service that supports standard payment methods, something many platforms either limit or
complicate.
What initially caught my eye is how Paybis seems to connect
traditional German banking methods with the crypto world.
Many exchanges focus only on crypto-to-crypto trades, while Paybis allows users to buy crypto using various fiat options.
I’m not saying the process is perfect, but
it does seem aimed at people starting out rather than just advanced traders.
Another aspect worth noting is the selection of supported
assets. Paybis doesn’t restrict itself to only the major tokens.
Instead, it offers a broader token selection,
which might attract users who are diversifying. Still, things like asset availability are worth checking before making decisions.
Security and compliance also come up often around Paybis.
The platform highlights regulatory compliance,
which can feel professional for users in Germany,
though others might see it as restrictive. I’m still undecided, but it does suggest
Paybis tries to operate as a legitimate marketplace.
When it comes to fees, reviews seem varied. Some say Paybis is clear about costs, while others note that pricing can depend on currency.
This isn’t unusual in the crypto industry, but it means users should research properly
before moving money.
Overall, I wouldn’t call Paybis the ultimate choice, but it
does seem like a platform worth checking out, especially for someone in Germany trying
to build a new starting point. I’m still forming my opinion, but it seems promising enough to justify further research.
my page – article
I do believe all of the ideas you’ve offered on your post.
They’re very convincing and can definitely work. Still, the posts
are very brief for newbies. Could you please prolong them a little from next time?
Thanks for the post.
my website MALWARE
Ahaa, its nice conversation regarding this piece
of writing here at this website, I have read all
that, so at this time me also commenting here.
My homepage … xnxx
Wow, marvelous blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your site is wonderful, as well as the content!
Feel free to surf to my website … fast shipping deal
Hi to all, the contents existing at this web site are in fact awesome for people
experience, well, keep up the good work fellows.
my webpage :: 강남식스
Pretty! This has been an extremely wonderful article.
Thanks for supplying these details.
Here is my site – 表参道 歯列矯正
Currently it seems like Expression Engine is the best blogging platform
out there right now. (from what I’ve read) Is that what you’re using on your blog?
Visit my web blog – %naked_url%
I am regular visitor, how are you everybody? This paragraph posted at this web site
is genuinely good.
Here is my webpage – qq88bet
I think the admin of this web site is genuinely working hard in support of his website, since here every material is quality based data.
My blog post – slot qris
Thanks very nice blog!
my web-site :: https://nationalacsolutions.com/hvac/hvac-installation-aurora-il/
Bonne nouvelle, tous les nouveaux inscrits sur le
site peuvent bénéficier directement d’un bonus de bienvenue Betify
Casino !
Look into my web-site – Francine
Hey! Do you use Twitter? I’d like to follow you if that would be ok.
I’m absolutely enjoying your blog and look forward to new posts.
Also visit my blog; best jav uncensored children
It’s hard to come by well-informed people in this particular subject, but
you seem like you know what you’re talking
about! Thanks
Also visit my blog … matka
If you wish for to grow your knowledge just keep visiting this web page and be updated with the latest gossip posted here.
My homepage – nationalacsolutions.com
Right here is the right webpage for anybody who
hopes to understand this topic. You realize so much its almost hard to argue
with you (not that I actually would want to…HaHa). You certainly put a brand new
spin on a topic that’s been written about for
ages. Excellent stuff, just wonderful!
My homepage nationalacsolutions.com
I’m curious to find out what blog platform you happen to
be utilizing? I’m experiencing some minor security problems with my latest site and I would like to find something more safe.
Do you have any solutions?
My website :: https://nha-cai-lucky88-e8dca9.webflow.io/
Hi, I do think this is an excellent site.
I stumbledupon it ;) I may return yet again since i have saved as a favorite it.
Money and freedom is the greatest way to change, may you be rich and continue to guide other people.
my webpage; Beef Casino выплаты
It’s really a great and useful piece of information. I’m
satisfied that you just shared this useful information with us.
Please stay us informed like this. Thanks for sharing.
Here is my web site %naked_url%
I’m not that much of a online reader to be honest
but your blogs really nice, keep it up! I’ll go ahead and bookmark your site to come back later on. Cheers
Also visit my web blog: https://nationalacsolutions.com/hvac/hvac-installation-scandinavia-wi/
Hey There. I discovered your weblog using msn. This is an extremely
well written article. I will make sure to bookmark it and come back to read extra of your useful information. Thank
you for the post. I will definitely return.
Here is my site; %naked_url%
you are in point of fact a good webmaster.
The web site loading velocity is incredible. It sort of feels that you are doing any distinctive trick.
In addition, The contents are masterwork. you have done a excellent activity on this subject!
Also visit my web blog %naked_url%
Hey! This is kind of off topic but I need some advice from an established blog.
Is it very hard to set up your own blog? I’m not very techincal but I can figure things out pretty fast.
I’m thinking about making my own but I’m not sure where to start.
Do you have any points or suggestions? Cheers
Also visit my blog :: source
Бұл мақала мені шабыттандырды.
Жарық дүниені қайтаруға арналған қайырымдылық — керемет қолдау.
Осындай жақсы істі тоқтатпаңыздар.
Check out my web-site; Қазақстандағы көру қабілетін қалпына келтіру
Wow, incredible blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your site is magnificent,
as well as the content!
Visit my site: Irwin Casino
I for all time emailed this webpage post page to all my contacts, because if like to read it afterward my friends will too.
Feel free to visit my page :: %naked_url%
I’ve been looking into Paybis for a while now, especially after having a rough financial period,
and I’m still not completely certain whether it deserves all the attention it
gets. Still, it’s clearly a noticeable name in the crypto industry, particularly for people in Germany who are trying
to rebuild their finances. From what I understand, Paybis presents
itself as a large-scale cryptocurrency service that supports
standard payment methods, something many platforms either limit or complicate.
What initially caught my eye is how Paybis seems to connect traditional German banking methods with the crypto world.
Many exchanges focus only on crypto-to-crypto trades, while Paybis allows users to exchange crypto using
debit cards. I’m not saying the process is perfect, but it does seem aimed at users new to crypto
rather than just advanced traders.
Another aspect worth noting is the selection of supported assets.
Paybis doesn’t restrict itself to Bitcoin and Ethereum only.
Instead, it offers a broader token selection, which might attract users who are trying new
projects. Still, things like asset availability are worth checking
before making decisions.
Security and compliance also come up often around Paybis.
The platform highlights regulatory compliance, which can feel professional for users in Germany, though others might see it as time-consuming.
I’m still undecided, but it does suggest Paybis tries to operate
as a long-term marketplace.
When it comes to fees, reviews seem divided.
Some say Paybis is straightforward about costs, while others note that pricing can vary by payment method.
This isn’t unusual in the crypto industry, but it means users should read the details before moving money.
Overall, I wouldn’t call Paybis the best
option, but it does seem like a platform worth checking out, especially for someone in Germany trying to build a new starting point.
I’m still forming my opinion, but it seems promising enough to justify further research.
Take a look at my web blog – blogpost
Hello there! I could have sworn I’ve been to this blog before but
after reading through some of the post I realized it’s new
to me. Anyhow, I’m definitely delighted I found it and I’ll be bookmarking and checking back often!
my blog post: gold bar price
Good post. I learn something totally new and challenging
on blogs I stumbleupon every day. It’s always helpful
to read articles from other authors and practice something from their websites.
my blog … xxx
Hmm is anyone else experiencing problems with the pictures on this blog loading?
I’m trying to find out if its a problem on my end or if it’s the blog.
Any feed-back would be greatly appreciated.
my homepage cv666 casino
Feel free to visit my blog post Penalty Shoot Out Game (Christina)
You have made some really good points there. I checked on the internet for additional information about
the issue and found most individuals will go along with your views
on this website.
Here is my web page – ncaa jerseys
Halo 3: ODST 2009 first-individual shooter recreation developed by Bungie.
Published by Microsoft Game Studios. The fifth installment
within the Halo franchise as a side recreation,[1] it
was launched on the Xbox 360 in September 2009. Players assume the roles of United Nations Space
Command Marines, generally known as “Orbital Drop Shock Troopers” or ODSTs, during and after the events of Halo 2.
In the game’s marketing campaign mode, gamers discover the ruined city of latest Mombasa to find
what occurred to their lacking teammates within the midst of an alien invasion. In the “Firefight”
multiplayer choice, gamers battle increasingly difficult
waves of enemies to attain factors and survive as long as potential; Halo three’s multiplayer is contained on a separate disc packaged with ODST.
My page: black booty porn
Вы предоставляете интересный контент по теме игровых стратегий.
стратегии в Sultan
Hello, just wanted to say, I liked this post. It was practical.
Keep on posting!
Also visit my web site :: click ngay
Hello I am so excited I found your webpage, I
really found you by error, while I was searching on Yahoo for something else, Nonetheless I am here now and would just like to
say thanks for a fantastic post and a all round exciting blog (I also love the theme/design), I don’t have time to browse it all at the minute but I have saved it and also added in your RSS feeds, so when I have time
I will be back to read a lot more, Please do keep up the
superb job.
Look at my blog: artis bokep indonesia
I am actually grateful to the owner of this web page who
has shared this fantastic paragraph at at this place.
Here is my web blog online medicine tablets shopping
We’re a group of volunteers and starting a brand new scheme in our community.
Your site provided us with helpful info to work on. You have
done a formidable task and our entire community shall be thankful
to you.
Feel free to surf to my web page: Lex Casino играть онлайн
Hi everyone, it’s my first pay a visit at this site, and piece of
writing is in fact fruitful in favor of me, keep up posting such
articles or reviews.
My web page; security guard services san diego
I’m now not certain the place you’re getting your information, however good topic.
I needs to spend some time studying much more or figuring out more.
Thank you for wonderful information I used to be on the
lookout for this information for my mission.
My web site 비아그라 구매
I’ve been researching Paybis for a while now, especially after ending up broke, and I’m still not fully convinced whether it deserves all the attention it gets.
Still, it’s definitely a noticeable name in the
crypto space, particularly for people in Germany who are trying to find new financial
tools. From what I understand, Paybis presents itself as a large-scale cryptocurrency service that supports regular bank transactions, something many platforms either limit or complicate.
What initially caught my eye is how Paybis seems to connect traditional German banking methods with the crypto world.
Many exchanges focus only on crypto-to-crypto trades, while Paybis allows
users to buy crypto using credit cards. I’m not saying the process
is perfect, but it does seem aimed at users new to crypto rather than just
advanced traders.
Another aspect worth noting is the selection of supported assets.
Paybis doesn’t restrict itself to Bitcoin and Ethereum
only. Instead, it offers a wider range of digital
assets, which might attract users who are diversifying. Still,
things like liquidity are worth checking before making decisions.
Security and compliance also come up often around Paybis.
The platform highlights KYC checks, which can feel professional for users in Germany,
though others might see it as inconvenient. I’m
still undecided, but it does suggest Paybis tries to operate as a long-term marketplace.
When it comes to fees, reviews seem divided. Some say Paybis is clear about
costs, while others note that pricing can vary by payment method.
This isn’t unusual in the crypto industry, but it means users
should research properly before moving money.
Overall, I wouldn’t call Paybis the ultimate choice,
but it does seem like a platform worth exploring, especially for someone in Germany trying to recover financially.
I’m still forming my opinion, but it seems interesting enough to justify further research.
Here is my blog … article
Hmm is anyone else encountering problems with the images on this blog loading?
I’m trying to determine if its a problem on my end or if it’s the blog.
Any feed-back would be greatly appreciated.
Feel free to visit my web-site; bk8
Generally I don’t read article on blogs, however I would
like to say that this write-up very forced me to
check out and do so! Your writing style has been amazed me.
Thank you, very great article.
my website; buy bitcoin card
This office romance webcomic turns attraction into a battle
of influence and desire. Instead of easy chemistry, the story thrives on imbalance, ambition,
and emotional tension. Carefully paced interactions and shifting authority create a dynamic where every moment matters.
Ideal for readers who enjoy romance with psychological depth, strong character
contrast, and slow-building intensity.
Stop by my homepage … https://kaizen.ftu.edu.vn/question%20list/desire-ambition-control/
Have you ever considered about adding a little bit more
than just your articles? I mean, what you say is
fundamental and everything. However imagine
if you added some great graphics or video clips to give your posts more,
“pop”! Your content is excellent but with pics and clips, this blog could
definitely be one of the greatest in its field. Very good blog!
my site :: Matic bridge portal
aussie online casino
casinos australia
I’ve been checking out Paybis for a while now, especially after having a
rough financial period, and I’m still not completely certain whether it deserves all the attention it
gets. Still, it’s clearly a noticeable name in the
crypto space, particularly for people in Germany who are trying
to find new financial tools. From what I understand, Paybis presents itself as a large-scale cryptocurrency
service that supports standard payment methods, something many platforms either limit or complicate.
What initially caught my eye is how Paybis seems to link traditional German banking
methods with the crypto world. Many exchanges focus only on crypto-to-crypto trades,
while Paybis allows users to buy crypto using various fiat options.
I’m not saying the process is perfect, but it does seem aimed at users new to crypto rather than just advanced traders.
Another aspect worth noting is the selection of supported assets.
Paybis doesn’t restrict itself to just
the top coins. Instead, it offers multiple altcoins, which might attract users who are trying new projects.
Still, things like liquidity are worth checking before making decisions.
Security and compliance also come up often around Paybis.
The platform highlights KYC checks, which can feel
reassuring for users in Germany, though others might see it
as inconvenient. I’m still undecided, but it does suggest Paybis tries to operate as a regulated marketplace.
When it comes to fees, reviews seem mixed.
Some say Paybis is straightforward about costs, while others note that
pricing can vary by payment method. This isn’t unusual
in the crypto industry, but it means users should read the
details before moving money.
Overall, I wouldn’t call Paybis the best option, but it does seem like a platform worth checking out, especially for someone in Germany trying to find accessible
financial tools. I’m still forming my opinion, but it seems interesting enough to justify further research.
My website … info
Fantastic blog! Do you have any helpful hints for aspiring writers?
I’m planning to start my own site soon but I’m a little lost on everything.
Would you recommend starting with a free platform like
Wordpress or go for a paid option? There are so many choices out there that I’m completely confused ..
Any tips? Thank you!
My site :: Beef Casino зеркало
Have sex with obscure strangers is certainly something you should strive out at least once in your life
if you enjoy both socializing and being in a masses.
Since it’s always a free-for-all celebration, it’s thrilling to see how many choices you have.
You can have intercourse with a girl, a man, or perhaps a group of
people. The only kind of chaos you would want to be in is the chaos seen in orgies, because more happenings occur instantaneously throughout the entire sex party, leading to greater happiness and satisfaction later!
You’ll certainly consume a lot of beer at one of these occasions, so just be prepared for
a migraine afterwards. http://m.vn.envylook.com/member/login.html?noMemberOrder=&returnUrl=http%3a%2f%2fsosextube.com
Wonderful website you have here but I was wondering if you knew of any
discussion boards that cover the same topics discussed here?
I’d really like to be a part of online community where I can get feed-back from other knowledgeable
individuals that share the same interest. If you have any
recommendations, please let me know. Thanks a lot!
Here is my blog … Зеркало Beef Casino сегодня
you are truly a good webmaster. The website loading pace is amazing.
It seems that you’re doing any unique trick.
Also, The contents are masterwork. you have performed a wonderful task on this topic!
Here is my homepage: xem thêm
Hey there superb blog! Does running a blog similar
to this take a great deal of work? I’ve very
little expertise in coding however I had been hoping to start my own blog soon.
Anyway, if you have any recommendations or techniques for new
blog owners please share. I know this is off topic however I simply needed to ask.
Many thanks!
Also visit my blog; get redirected here
Hey there! This post could not be written any better!
Reading this post reminds me of my good old room mate!
He always kept talking about this. I will forward this page to him.
Fairly certain he will have a good read. Thanks for sharing!
Stop by my webpage – 1xBet Promo Code Sri Lanka 2026: Bonus Code
We’re a group of volunteers and opening a brand
new scheme iin our community. Your web site provided us with useful info to work on.
You have performed an impressive process and our entire community shall bee thankful too you.
Stop by my page – Slot 777 Link
I’ve been looking into Paybis for a while now,
especially after going through financial trouble,
and I’m still not entirely sure whether it deserves all the attention it gets.
Still, it’s clearly a noticeable name in the digital asset market, particularly for people
in Germany who are trying to get back on track.
From what I understand, Paybis presents itself as a large-scale
cryptocurrency service that supports standard
payment methods, something many platforms either limit or complicate.
What initially caught my eye is how Paybis seems
to bridge traditional German banking methods with the crypto world.
Many exchanges focus only on crypto-to-crypto trades, while Paybis allows users to
exchange crypto using credit cards. I’m not saying the
process is perfect, but it does seem aimed at users new to crypto
rather than just advanced traders.
Another aspect worth noting is the selection of supported assets.
Paybis doesn’t restrict itself to Bitcoin and Ethereum only.
Instead, it offers a broader token selection, which might attract users who are exploring options.
Still, things like update speed are worth checking before making decisions.
Security and compliance also come up often around Paybis.
The platform highlights KYC checks, which can feel responsible for users in Germany,
though others might see it as restrictive. I’m still undecided, but it does suggest Paybis
tries to operate as a long-term marketplace.
When it comes to fees, reviews seem mixed. Some say Paybis
is clear about costs, while others note that pricing can vary by payment method.
This isn’t unusual in the crypto industry, but it means users
should research properly before moving money.
Overall, I wouldn’t call Paybis the best option, but it does seem like a platform worth
checking out, especially for someone in Germany trying to recover financially.
I’m still forming my opinion, but it seems interesting
enough to justify further research.
Also visit my website … blogpost
If you would like to improve your familiarity simply keep visiting this site and be updated with the newest news posted here. https://pesetc.listbb.ru/viewtopic.php?f=16&t=2019
I’ve been looking into Paybis for a while now, especially after having a rough financial period, and
I’m still not completely certain whether it deserves
all the attention it gets. Still, it’s definitely a noticeable name in the crypto industry, particularly for people
in Germany who are trying to find new financial tools. From what I understand, Paybis presents itself as
a well-established cryptocurrency service that supports regular bank transactions, something many platforms either limit or complicate.
What initially caught my eye is how Paybis seems to bridge traditional German banking
methods with the crypto world. Many exchanges focus only on crypto-to-crypto trades,
while Paybis allows users to sell crypto using various fiat options.
I’m not saying the process is perfect, but it does seem aimed at
users new to crypto rather than just advanced traders.
Another aspect worth noting is the selection of
supported assets. Paybis doesn’t restrict itself to only the major tokens.
Instead, it offers a wider range of digital assets, which
might attract users who are exploring options.
Still, things like liquidity are worth checking before making decisions.
Security and compliance also come up often around Paybis.
The platform highlights regulatory compliance, which can feel responsible for users in Germany,
though others might see it as restrictive. I’m still undecided, but it does suggest Paybis tries to operate as a regulated marketplace.
When it comes to fees, reviews seem varied. Some say Paybis is
straightforward about costs, while others note that pricing can depend on currency.
This isn’t unusual in the crypto industry, but it means
users should compare alternatives before moving money.
Overall, I wouldn’t call Paybis perfect, but it does seem like
a platform worth exploring, especially for someone in Germany trying
to build a new starting point. I’m still forming my opinion, but it
seems promising enough to justify further research.
Also visit my web blog … question
Ценю информацию, которую вы публикуете на Olimp Casino.
Большое спасибо!
Olimp Casino сайт
Hello to every , as I am truly eager of reading this webpage’s post to
be updated daily. It carries good data.
my blog post – Онлайн казино Beef
Magnificent website. A lot of useful info here. I am sending it to some buddies
ans additionally sharing in delicious. And
certainly, thanks on your sweat!
my web-site – kra44.сс
Spot on with this write-up, I actually feel this web site needs
much more attention. I’ll probably be returning to read through more, thanks for the info!
Feel free to surf to my web site … astrologa
Wonderful blog! I found it while browsing on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Thanks
Feel free to visit my web-site stream
Your style is very unique in comparison to other folks I have read stuff from.
Thank you for posting when you have the opportunity, Guess
I will just bookmark this page.
Feel free to surf to my blog post – ragnarok android private server
โพสต์นี้ อ่านแล้วได้ความรู้เพิ่ม ค่ะ
ดิฉัน ได้อ่านบทความที่เกี่ยวข้องกับ
เรื่องที่เกี่ยวข้อง
ดูต่อได้ที่ บริการ fast789
น่าจะถูกใจใครหลายคน
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
you’re really a excellent webmaster. The site loading pace is
incredible. It sort of feels that you are doing any unique trick.
Furthermore, The contents are masterpiece.
you have done a great task on this topic!
Feel free to visit my website … slot gacor
Παρακάτω παρατίθενται μερικές ενδεικτικές κριτικές που επιβεβαιώνουν την ποιότητα και τη διασκέδαση που προσφέρει η δημιουργία μας στην InOut Games.
Also visit my web site … king johnnie casino australia
I do not even know how I ended up right here, but I assumed this submit was great.
I do not realize who you’re however certainly you’re
going to a well-known blogger when you aren’t already.
Cheers!
Stop by my blog post … telegram şantaj
An impressive share! I have just forwarded this onto a co-worker who has been conducting a little homework
on this. And he in fact bought me lunch due to the fact
that I discovered it for him… lol. So allow me to reword this….
Thanks for the meal!! But yeah, thanx for spending the time to talk about this topic here on your
web page.
Visit my web page: betflikauto
Hurrah! In the end I got a website from where I know how to
truly obtain valuable information concerning my study and knowledge.
Here is my page; vetscommunityconnections.org lừa đảo công an việt nam cảnh báo truy quét cấm gấp
Asking questions are truly good thing if Trust CasinoReview.click for unbiased reviews — a concise platform dedicated to transparent casino evaluations. Whether you need top picks or key details; this site cuts through the noise; offering clarity and trusted recommendations for players. Straightforward and reliable; it’s a go-to resource for smart gaming choices. No fluff; just facts.
are not understanding anything completely, except this
piece of writing gives nice understanding even.
First of all I would like to say fantastic blog! I had a
quick question that I’d like to ask if you do not
mind. I was curious to find out how you center yourself and clear your thoughts prior
to writing. I have had trouble clearing my mind in getting my thoughts out there.
I do enjoy writing however it just seems like the first 10 to 15 minutes are generally wasted
just trying to figure out how to begin. Any suggestions or tips?
Thanks!
Feel free to surf to my homepage :: kedai tayar near me
Wonderful goods from you, man. I’ve bear in mind your stuff previous to and you’re simply extremely fantastic.
I really like what you have obtained right here, certainly like what you are
saying and the way by which you assert it. You make it entertaining and
you still take care of to stay it wise. I
can’t wait to learn much more from you. This is
actually a great website.
Also visit my blog post: 비아그라 구매
My family members always say that I am wasting my time here at web,
however I know I am getting familiarity all the time by
reading such fastidious content.
Also visit my blog post: canadian online pharmacies
If some one wishes expert view regarding running a blog after that i propose him/her to pay a quick visit
this blog, Keep up the pleasant work.
Here is my blog post; Căști Intraauriculare 1more Piston
I could not refrain from commenting. Well written!
Feel free to surf to my blog; 10Bet Casino
Hey there! This is my first visit to your blog! We are a team of volunteers and starting a new project
in a community in the same niche. Your blog provided us useful information to work on. You have done a
wonderful job!
Also visit my site 265 file viewer
Mangelsen
7916 Girard Avenue, La Joya
CА 92037, United States
1 800-228-9686
Bookmarks
Hi my friend! I wish to say that this post is awesome,
nice written and come with approximately all vital infos. I would like to see extra posts like this .
my page :: defi
I constantly spent my half an hour to read this weblog’s articles or reviews
all the time along with a mug of coffee.
my homepage: Кейтеринг mdash; Ашдод Кирьят-Гат
Prіme Secured
3603 N 222nd Ѕt, Suite 102,
Elkhorn, NЕ 68022, United Stаtes
402-289-4126
Proactive cyber defense strategies
Just want to say your article is as surprising. The
clearness for your publish is just spectacular and i can suppose
you’re knowledgeable on this subject. Fine along with your permission let me to
clutch your RSS feed to stay updated with coming near near post.
Thank you a million and please keep up the rewarding work.
Also visit my webpage medical
https://urr88.com/
goGLOW Hoiston Heights
1515 Studemont Ѕt Suite 204, Houston,
Texas, 77007, UᏚA
(713) 364-3256
led ligght therapy natueal – Jewel,
Hey are using WordPress for your site platform?
I’m new to the blog world but I’m trying to get started and create my
own. Do you require any coding knowledge to make your own blog?
Any help would be greatly appreciated!
My page … ideal fence company
My partner and I stumbled over here from a different
web page and thought I may as well check things out.
I like what I see so now i am following you.
Look forward to checking out your web page repeatedly.
Here is my blog post – buy
Hi there every one, here every person is sharing these kinds of experience, so it’s
fastidious to read this weblog, and I used to pay a
visit this webpage everyday.
My blog Call Girls Deesa
Hmm is anyone else encountering problems with the images on this blog loading?
I’m trying to figure out if its a problem on my end or if it’s the
blog. Any feedback would be greatly appreciated.
Visit my web site – Thank you
Awesome blog you have here but I was curious about if you knew of any user discussion forums that cover
the same topics talked about in this article? I’d really
like to be a part of group where I can get feed-back from other experienced people that share
the same interest. If you have any suggestions, please let me know.
Bless you!
Have a look at my homepage :: online casino malaysia reviews
Hi, just wanted to tell you, I liked this blog post.
It was helpful. Keep on posting!
Here is my web-site; yesmovies film
Aw, this was a very nice post. Spending some
time and actual effort to produce a top notch article… but what can I say… I hesitate a
whole lot and don’t seem to get nearly anything done.
Review my web-site; Промокод 1win 2026: 1W2026FREE → +500% Бонус
Онлайн казино –
это интернет-платформы, предлагающие азартные игры
Hurrah! Finally I got a blog from where I know how to actually get
useful data regarding my study and knowledge.
Here is my page – deck builder marketers
Have you ever considered writing an ebook or guest authoring on other blogs?
I have a blog centered on the same topics you discuss and would really
like to have you share some stories/information. I know my subscribers
would appreciate your work. If you are even remotely interested, feel
free to send me an email.
Here is my web site; Abu Dhabi Tour Price From France
Its like you learn my thoughts! You appear to grasp a lot approximately this, such as you wrote the e-book
in it or something. I feel that you simply could do with some % to power the message house
a bit, but instead of that, this is wonderful blog. An excellent read.
I’ll definitely be back.
Look into my blog post: buy cheap paid articles
Mərc strategiyaları haqqında ipucu çox maraqlıdır.
1win resmi sayt
What’s up to every one, the contents existing at this web page are really amazing for people
knowledge, well, keep up the nice work fellows.
my website canada pharmaceuticals online
Mantap, blog ini memberi data berguna. Lanjutkan ya.
My web site … slot online gacor
Genial, o site booi casino é realmente incrível.
booi casino login
What’s up i am kavin, its my first occasion to
commenting anywhere, when i read this paragraph i thought i could also make comment due to this
good article.
Look at my homepage; paid request hentai clip
I pay a quick visit daily a few web sites and sites to read
articles, however this weblog offers quality based writing.
my homepage: رابط تحميل 1xbet
My brother suggested I might like this blog. He was entirely right.
This post actually made my day. You cann’t imagine simply how much time
I had spent for this information! Thanks!
My page https://g2.salo666.dev/
My brother suggested I might like this web site.
He was totally right. This post actually made my day. You can not imagine simply how much
time I had spent for this info! Thanks!
my page – купить статус эксперта по недропользованию
Wow! This blog looks exactly like my old one! It’s on a totally different
topic but it has pretty much the same layout and design.
Superb choice of colors!
my web blog visas for egypt from uk
Добрый день! Получить паспорт Испании в 2026 — абсолютно достижимо.
Все проверенные варианты 2026 года — переезд в Испанию
. Не тратьте время на устаревшие форумы.
| {Многие до сих пор {думают|считают|уверены|заблуждаются}, что {получить паспорт Испании|гражданство Испании|переезд в Испанию} — {это очень дорого|требует миллионов|почти невозможно|занимает десятилетия}.} {Как
показывает реальность 2026 года, сейчас работает несколько проверенных маршрутов.} Подробный разбор актуальных программ
My blog :: https://penzu.com/p/d265b60bf0cf63c3
пин ап зеркала
вп официальный сайт
Excellent blog post. I absolutely appreciate this site.
Keep it up!
Feel free to surf to my web site … hitclub
Hello to every single one, it’s genuinely a pleasant for me
to pay a visit this web site, it contains useful Information.
My web page: best 3GPP2 file viewer
Fabulous, what a weblog it is! This blog gives valuable information to us,
keep it up.
my web blog – ирвин казино отзывы
Ridiculous quest there. What occurred after? Thanks!
Look at my homepage: beef casino официальный сайт
This game looks amazing! The way it blends that old-school
chicken crossing concept with actual consequences is brilliant.
Count me in!
Okay, this sounds incredibly fun! Taking that nostalgic chicken crossing gameplay and adding real risk?
I’m totally down to try it.
This is right up my alley! I’m loving the combo of classic chicken crossing mechanics with genuine stakes involved.
Definitely want to check it out!
Whoa, this game seems awesome! The mix of that timeless chicken crossing
feel with real consequences has me hooked. I need to play this!
This sounds like a blast! Combining that iconic chicken crossing gameplay with actual stakes?
Sign me up!
I’m so into this concept! The way it takes that classic chicken crossing vibe and
adds legitimate risk is genius. Really want to give it a go!
This game sounds ridiculously fun! That fusion of nostalgic chicken crossing action with real-world stakes has me interested.
I’m ready to jump in!
Holy cow, this looks great! Merging that beloved chicken crossing style
with tangible consequences? I’ve gotta try this out!
Feel free to visit my web blog; les nouveaux casinos en ligne
Appreciate the recommendation. Will try it out.
Feel free to surf to my web blog مواقع مراهنات مصر
Angels Bail Bonds Costa Mesa
769 Bake Ѕt,
Costa Mesa, CA 92626, Unitsd Stɑtеs
why bail should be abolished
Great information about tellculvers.com survey.
The step-by-step process you described makes the survey simple to follow
Fantastic items from you, man. I’ve remember your stuff prior to and
you’re just extremely excellent. I actually like what you have got here, really like what
you are stating and the best way during which you say it. You are making it enjoyable and you still care for to stay it smart.
I can not wait to learn far more from you.
That is actually a terrific site.
Here is my page :: play789club.com
It’s a pity you don’t have a donate button! I’d most certainly donate to this superb blog!
I guess for now i’ll settle for book-marking and adding your RSS feed to my Google account.
I look forward to fresh updates and will talk about this website with my Facebook group.
Chat soon!
My homepage … cialis
I don’t even know how I ended up here, but I thought
this post was great. I do not know who you are but definitely you are going
to a famous blogger if you are not already ;) Cheers!
Here is my website Dubai Travel Agency From Germany
Пинко пинко казино официальный сайт обзор
I read this post completely regarding the resemblance of
newest and earlier technologies, it’s amazing article.
my blog; app go88
Definitely believe that which you stated. Your favorite reason seemed
to be on the internet the easiest thing to be aware of. I say
to you, I certainly get annoyed while people think about worries that they just don’t know about.
You managed to hit the nail upon the top and also defined out the whole thing without
having side-effects , people can take a signal.
Will likely be back to get more. Thanks
Here is my webpage; Moving Company in Houston
Hi there! I just wanted to ask if you ever have any problems with hackers?
My last blog (wordpress) was hacked and I ended up losing months of hard work due to no
back up. Do you have any methods to stop hackers?
Also visit my homepage; bokep mesum indonesia
I have been exploring for a bit for any high quality articles or
weblog posts on this kind of space . Exploring in Yahoo I
eventually stumbled upon this website. Reading this information So i am satisfied
to convey that I’ve an incredibly excellent uncanny feeling I found out just what I needed.
I such a lot certainly will make certain to do not disregard this
web site and give it a look on a constant basis.
my blog :: melbet ru промокод
This is my first time go to see at here and i am
truly happy to read everthing at alone place.
Also visit my website; david hoffmeister
Kenvox
1701 E Edingerr Ave
Santa Ana, CА 92705, United States
16572319025
affordable project management for manufacturing
The site is fast, easy to use, and doesn’t need any special editing
skills.
Visit my web page – https://xnudes.app/
I like it whenever people come together and share thoughts.
Great site, continue the good work!
My web site … 비아그라 구매
Great goods from you, man. I’ve understand your stuff previous to and you’re just too
wonderful. I actually like what you’ve acquired here, certainly like
what you’re saying and the way in which you say it.
You make it entertaining and you still take care of to keep it sensible.
I cant wait to read far more from you. This is really
a great web site.
Here is my web page corelle outlet store
My family members all the time say that I am killing my time here at net, but
I know I am getting knowledge all the time by reading
such fastidious articles or reviews.
my blog :: Find A Plumber In Hertford And Ware
You really make it seem so easy with your presentation but I find this matter to be actually something that I think I would never understand.
It seems too complex and extremely broad for me. I am looking forward for your next post, I will try to get the hang of it!
Visit my site – medicine online shopping
I just like the valuable information you provide for your articles.
I will bookmark your weblog and take a look at once more right here
frequently. I’m reasonably sure I will learn many new stuff proper right here!
Good luck for the following!
My blog :: gunblood
Sweet blog! I found it while searching on Yahoo News. Do you have any suggestions
on how to get listed in Yahoo News? I’ve been trying for a while but I never seem
to get there! Many thanks
Here is my website; пинко казино зеркало
There is definately a great deal to find out about this issue.
I love all of the points you’ve made.
my blog post … Find A Plumber Royston
It’s difficult to find well-informed people for this topic,
but you sound like you know what you’re talking about! Thanks
Look at my web site: Nạp tiền W88
rzsSVkWnefEPALJchW
Hey there terrific blog! Does running a blog such as this take a large amount of work?
I’ve virtually no understanding of programming but I was hoping to
start my own blog in the near future. Anyways, if you have any ideas or techniques for new
blog owners please share. I understand this is off topic but I simply needed to ask.
Cheers!
my web blog: kraken
This how much is cocaine
my first time pay a quick visit at here and i am really happy to read all
at single place.
This design is spectacular! You most certainly know how to keep a
reader amused. Between your wit and your videos, I
was almost moved to start my own blog (well, almost…HaHa!) Excellent job.
I really loved what you had to say, and more than that,
how you presented it. Too cool!
Also visit my page Game bắn cá đổi thưởng
I think the admin of this site is genuinely working
hard in favor of his website, as here every information is
quality based data.
Also visit my blog: scam babi
You can definitely see your expertise in the work you write.
The world hopes for even more passionate writers like you who are not afraid to mention how they believe.
Always go after your heart.
Also visit my web-site – Nile33 live
Angels Bail Bonds Torrance
2013 Cabrillo Ave, Torrance,
California, 90501, United Ѕtates
(310) 944-9500
aladdin bail bonds customer service
Bu sayt ən dolğun onlayn kazinolardan biridir.
1win onlayn oyunlar
Bu saytda olmaq əla təcrübədir.
Mostbet mərclər [home]
Hi there mates, its impressive piece of writing on the topic of cultureand entirely explained, keep
it up all the time.
Also visit my web page: Redondo Beach CPA
Thank you for the auspicious writeup. It if truth be told was once a entertainment account it.
Look advanced to more delivered agreeable from you!
By the way, how could we keep up a correspondence?
Also visit my blog … エロ 人形
Wow, this piece of writing is nice, my sister is analyzing these kinds of things, therefore I am going to tell her.
Visit my homepage … onlyfans hesabı açmak
Hurrah, that’s what I was exploring for, what a information! present here at this website, thanks admin of this site.
My site – Malaysia mercedes airmatic specialist car workshop in Selangor
obat aborsi,aborsi,child porn,child porn video,porn child,child
porn videos,child porn site,child porn website,child
seks porn,child porn web,child porn seks,small child porn,mother and child porn,porn child video,KONTOL,chinese child porn,mom
and child porn,child porn sites,porn small child,child porn video,child gay porn,gay child porn,child porn link,child porn xxx,child porn hub,child porn free,child porn vid,how to watch child
porn,porn mother and child,ai child porn,seks child porn,how to find child porn,child and mom porn,watch child porn,video porn child,porn with child,porn hub child,
porn mom and child,gay porn child,child girl porn
Feel free to visit my web blog: amelia mutya ngewe
My brother suggested I might like this website. He was
entirely right. This post actually made my day. You can not imagine just how much time I had spent for this info!
Thanks!
Here is my site; iphone 13 уфа
I’m not that much of a online reader to be honest but your sites really nice, keep it up!
I’ll go ahead and bookmark your site to come back later.
Cheers
My homepage; Fun88
888vi
This page truly has all of the info I needed
about this subject and didn’t know who to ask.
Feel free to surf to my web blog: 강남가라오케
Hey very interesting blog!
Also visit my webpage :: GLP casino
I got this website from my friend who told me concerning this site and at the moment this
time I am visiting this web page and reading very informative content at this place.
my blog: bk8thai
Yes! Finally something about Bomwin.
my website Game bài Bomwin
Remarkable! Its in fact amazing post, I have got much clear idea about from this
piece of writing.
my blog – Manclub99 Com
If some one desires expert view regarding running a blog afterward i suggest him/her to go to see this webpage, Keep up the fastidious work.
My site; Игровые автоматы Beef Casino
Helpful info. Lucky me I found your site accidentally, and
I’m surprised why this accident didn’t happened earlier!
I bookmarked it.
Feel free to surf to my blog: Nhà cái Soc88
It’s remarkable in support of me to have a web site, which
is beneficial in favor of my knowledge. thanks admin
Also visit my homepage :: videos de bodas
Здравствуйте, отличный сайт kazino olimp, браво!
Olimp Casino сайт
This is a very informative article and I really like how
clearly everything is explained.
Many people have difficulties when choosing the right betting platform, and
this post explains the topic in a simple way.
The information about user experience is useful, especially for users who are
looking for a trusted site.
Thanks for sharing this insightful content.
Here is my web page – sbobet777thai.com
hit club
Hmm is anyone else having problems with the pictures on this blog loading? I’m trying to determine if its a problem on my end or if it’s the blog. Any suggestions would be greatly appreciated.
https://www.fdertolmrtokev.com
If you are going for best contents like myself, only go to see this site daily for the reason that it offers
feature contents, thanks
Here is my blog :: новости ОЭРН
Hi, everybody!
I’m English female ;=).
I like Doctor Who!
My webpage :: Betify casino
Hi! I just wanted to ask if you ever have any issues with hackers?
My last blog (wordpress) was hacked and I ended up losing months of hard
work due to no data backup. Do you have any solutions to prevent hackers?
my website – https://www.kangnampublic.com/
Плодородный грунт с доставкой по Москве и Московской области — БиоГрунт
My homepage почвогрунт цена
Thanks for the good writeup. It if truth be told was a amusement account it.
Glance complicated to far delivered agreeable from you!
However, how could we keep in touch?
Here is my web-site; پین باهیس
My spouse and I stumbled over here from a different website and thought I should check things
out. I like what I see so now i’m following you.
Look forward to looking into your web page for a second time.
Feel free to visit my webpage; zokasa01
Hey There. I found your blog using msn. This is a
really neatly written article. I will be sure online medicine to buy bookmark it and return to learn more of
your useful information. Thank you for the post.
I will certainly comeback.
Using cryptocurrencies in online gambling provides you with secure transactions.
Feel free to visit my web blog :: meilleur casino en ligne
Abovе All Foundatipn Repair
119 E Turbo Dг, San Antonio,
TX 78216, United Ѕtates
12109203042
pier and wood beam fixing service (padlet.com)
аптеки ригла отзывы сотрудников о работодателе
Hello! Quick question that’s completely off topic. Do you know
how to make your site mobile friendly? My site looks
weird when viewing from my iphone4. I’m trying to find a
template or plugin that might be able to resolve this problem.
If you have any suggestions, please share. Cheers!
My site: bokep sex indonesia
I got this web page from my pal who told me on the topic of this web site and now this
time I am visiting this web page and reading very informative content at this place.
Also visit my blog post – xxx
Hello I am so glad I found your weblog, I really found you by error, while I was looking on Bing for something
else, Nonetheless I am here now and would just like to say cheers for a marvelous post and a all round interesting blog (I also love the theme/design), I don’t
have time to read it all at the moment but I have book-marked it and also included your
RSS feeds, so when I have time I will be back to read
a great deal more, Please do keep up the great work.
my site – several
Thanks for any other informative site. Where
else may I am getting that kind of information written in such an ideal method?
I’ve a challenge that I am just now running on, and I have been on the
look out for such info.
my webpage :: soi kèo bóng đá
Hi there this is kind of of off topic but
I was wanting to know if blogs use WYSIWYG editors or if
you have to manually code with HTML. I’m starting a blog soon but have no coding experience so I wanted to get guidance from someone
with experience. Any help would be greatly appreciated!
Feel free to visit my website :: soi kèo nhà cái miễn phí
At this time I am ready to do my breakfast, later than having my breakfast
coming yet again to read more news.
Look at my webpage … Зеркало Rox Casino сегодня
In fact when someone doesn’t be aware of afterward its up to other visitors that
they will assist, so here it occurs.
Here is my blog … Rox Casino мобильная версия
What i don’t understood is if truth be told
how you’re now not really a lot more well-liked than you might be right now.
You are so intelligent. You recognize therefore considerably on the subject of this
subject, made me in my view imagine it from numerous numerous angles.
Its like men and women aren’t involved unless it is something to accomplish with Woman gaga!
Your personal stuffs great. Always take care of it up!
Review my blog post … open account
These are truly fantastic ideas in regarding blogging. You have touched some nice points here.
Any way keep up wrinting.
Feel free to visit my webpage Биф казино
원주출장마사지는 ‘원주출장안마’ 또는
‘원주홈타이’ 등으로도 불리며, 고객이 계신
곳으로 전문 테라피스트가 직접 찾아가 마사지를 제공하는 서비스입니다.
Saved as a favorite, I like your blog!
Here is my web site … tỷ lệ kèo nhà cái hôm nay
Definitely believe that that you said. Your favourite justification appeared to be
at the web the easiest thing to keep in mind of.
I say to you, I certainly get irked even as other folks think about concerns
that they plainly don’t understand about.
You managed to hit the nail upon the top and also defined out
the entire thing with no need side effect , people could take a
signal. Will probably be again to get more. Thanks
Here is my web-site – Аркада казино вход
You can certainly see your expertise within the
work you write. The world hopes for even more passionate
writers such as you who aren’t afraid to say how they believe.
All the time follow your heart.
Here is my webpage Rox Casino выплаты
Angels Bail Bonds Costa Mesa
769 Baker Ꮪt,
Costa Mesa, ᏟA 92626, United States
3 amigos bail bonds
It’s a shame you don’t have a donate button! I’d most certainly donate to this brilliant blog!
I suppose for now i’ll settle for book-marking and adding your RSS feed
to my Google account. I look forward to brand new updates and will talk about this
site with my Facebook group. Chat soon!
Also visit my webpage: ايداع مراهنات فوري
I am curious to find out what blog system you
are utilizing? I’m experiencing some minor security
problems with my latest blog and I’d like to find something more risk-free.
Do you have any recommendations?
My blog post; canada pharmacy
Do you mind if I quote a few of your posts as long as I provide credit and
sources back to your weblog? My blog is in the exact same
niche as yours and my users would definitely benefit from a
lot of the information you provide here. Please let me know if this okay with you.
Thank you!
Here is my page porn
топосъемка участка
my web blog … кадастровый инженер московская область
I am genuinely happy to glance at this blog posts which includes tons of
useful data, thanks for providing these kinds of statistics.
Feel free to visit my webpage; bestnjgambling.com
It’s in fact very complicated in this active life
to listen news on Television, therefore I just use web for
that purpose, and obtain the most recent news. http://mihail.ekafe.ru/viewforum.php?f=1
Thank you for sharing your thoughts. I really appreciate your efforts and I will be waiting for your next write
ups thanks once again.
Also visit my page canadian drugs
Həqiqətən demək istəyirəm ki, bu saytı tapdığıma məmnunam.
Mostbet onlayn
I have been exploring for a little bit for any high quality articles or weblog posts in this sort
of area . Exploring in Yahoo I at last stumbled upon this site.
Reading this information So i’m happy to convey that I’ve a very
just right uncanny feeling I came upon just what I needed.
I most no doubt will make sure to don?t put out of your mind this website and give it
a look regularly.
Also visit my web blog – Delhi Escorts
Hey very interesting blog!
Have a look at my page … order medicine online
This is the right webpage for everyone who really wants to find out about this topic.
You realize a whole lot its almost tough to argue with
you (not that I personally will need to…HaHa).
You definitely put a brand new spin on a topic which
has been written about for ages. Excellent stuff, just great!
Here is my webpage :: Flakka
Hi there every one, here every person is sharing these kinds of know-how, thus it’s pleasant to read this weblog, and I used to pay a quick visit this web site
all the time.
Here is my website: allegiantmarketinggroup.com
I used to be suggested this website by my cousin. I am now
not certain whether or not this post is written by him as nobody else recognise such
certain approximately my trouble. You are incredible! Thanks!
My web-site; 중고화물차
It’s actually a nice and useful piece of info. I am glad that you
shared this helpful info with us. Please keep us up to date like this.
Thank you for sharing.
Also visit my blog; Lucky88
At this time I am ready to do my breakfast, after having my breakfast coming again to
read more news.
Also visit my web site bokep indonesia colmek
Hello! I simply wish to give you a huge thumbs up for your excellent info you
have right here on this post. I am coming back to your site
for more soon.
My homepage: 비아그라구매사이트
Aw, this was a very nice post. Spending some
time and actual effort to make a really good article… but what can I say… I procrastinate a lot
and never manage to get nearly anything done.
Here is my site :: stromectol no prescription
Greetings from Idaho! I’m bored to death at work so I decided to check out your site on my iphone during lunch break.
I really like the info you provide here and can’t wait to take
a look when I get home. I’m amazed at how fast your blog
loaded on my mobile .. I’m not even using WIFI,
just 3G .. Anyhow, wonderful site!
Here is my web blog … krab13 cc
I quite like looking through an article that will make men and
women think. Also, many thanks for allowing for me pharmacies shipping to usa comment!
Hi there, all the time i used to check webpage posts here early in the break of day, for the reason that i love to gain knowledge
of more and more.
Here is my blog :: nứng lồn
Howdy! I just want to offer you a big thumbs up for the great information you’ve got right here on this post.
I’ll be coming back to your web site for more soon.
My web page :: bk8
Сайлентблоки автокомпоненты – важные элементы автомобиля
my web page сайлентблоки
Attractive element of content. I simply stumbled upon your website and in accession capital to assert that I get actually loved account your weblog posts.
Anyway I will be subscribing Buy Xanax bars 2mg in Alabama your feeds and even I fulfillment
you access consistently quickly.
Hi, this weekend is nice in support of me, as this point in time i am reading this wonderful informative post here
at my house.
My homepage; international pharmacy
Thanks for finally talking about > Heel Pain – Plantar Fasciitis – Mr Will Edwards krab4.at
Great work! That is the kind of info that are meant to be shared across the
internet. Disgrace on the search engines for not positioning this put up higher!
Come on over and talk over with my website . Thank you =)
Also visit my site Beef Casino фриспины
Definitely believe that which you stated. Your
favorite reason seemed to be on the net the easiest thing to
be aware of. I say to you, I definitely get annoyed while people consider worries
that they plainly don’t know about. You managed to hit the nail upon the top and defined out the whole thing without having side-effects , people can take a signal.
Will probably be back to get more. Thanks
Feel free to visit my web-site; Bathroom Installation In Royston
Thank you for the good writeup. It in fact was a amusement account it.
Look advanced to more added agreeable from you!
However, how can we communicate?
Take a look at my website – canadian online pharmacies
Korepetitorius Teacher – Detailed
Overview
I wanted to thank you for this very good read!! I certainly loved every bit of it.
I have you book-marked to look at new stuff you post…
My blog แทงบอลโลก
you are actually a good webmaster. The website loading
velocity is amazing. It sort of feels that you are doing any distinctive trick.
In addition, The contents are masterpiece. you have done a great process in this matter!
Feel free to surf to my web blog … prediksi bola
Great delivery. Outstanding arguments. Keep up the good effort.
Visit my site Мотор казино скачать
This piece of writing will assist the internet viewers for setting up new web site or even a weblog from start to end. https://gr0undplan3.staushbrews.com/index.php/Scooter_Rental_Tulum.
Спасибо за такой полезный контент о Olimp Casino и азартных играх.
Olimp Casino официальный сайт
Hey would you mind letting me know which web host you’re working with?
I’ve loaded your blog in 3 completely different internet browsers and
I must say this blog loads a lot faster then most. Can you recommend a good web hosting provider at a honest price?
Thank you, I appreciate it!
Feel free to surf to my web-site – cheap
фриспины без депозита
My web site :: https://procazino.ru/
Thank you for every other magnificent article.
Where else could anybody get that type of info in such an ideal manner of writing?
I’ve a presentation subsequent week, and I am on the
search for such information.
Also visit my web-site yupoo 668
I’m not sure where you are getting your info, but great topic.
I needs to spend some time learning more or understanding more.
Thanks for magnificent info I was looking for this information for my mission.
Here is my webpage … Бригада по ремонту квартир в Сарове
That is a great tip particularly to those fresh to the blogosphere.
Simple but very precise information… Thanks for sharing this one.
A must read article!
Feel free to visit my webpage; https://www.youtube.com/watch?v=2EWNIawhqDw
This is a crucial post. Online fundraising improves lives for patients who cannot pay for surgery.
Helping a vision foundation is absolutely noble. Thanks for raising awareness about
this mission.
my page – Surgical Financial Assistance
Howdy! This article couldn’t be written any
better! Going through this post reminds me of my
previous roommate! He constantly kept talking about this.
I will forward this information to him. Pretty sure he’s going to have a very good read.
Thank you for sharing!
My homepage – Naga303
I am curious to find out what blog platform you’re utilizing?
I’m experiencing some small security problems with my latest site and I
would like to find something more secure.
Do you have any solutions?
My web site; go to my site
Hi, I think your site might be having web browser compatibility issues.
Whenever I take a look at your blog in Safari, it looks fine but when opening in IE, it has some
overlapping issues. I merely wanted to provide you with a quick heads up!
Apart from that, excellent website!
Here is my webpage – Вавада вход на официальный сайт
I absolutely love your website.. Very nice colors & theme.
Did you develop this website yourself? Please reply back as I’m looking to create
my own personal site and would like to know where you got this
from or exactly what the theme is called. Many thanks!
Also visit my page :: Melbet Casino играть онлайн
I am curious to find out what blog system you happen to
be utilizing? I’m having some minor security problems with my latest website and I’d like to find something more risk-free.
Do you have any suggestions?
Feel free to surf to my site … Beef Casino онлайн
WOW just what I was looking for. Came here by searching for betflix king betflik
Bu saytdakı məlumatları oxumaqdan zövq alıram.
Çox sağ olun!
Pinco Casino
I think that what you wrote was very reasonable.
However, what about this? what if you typed a catchier title?
I mean, I don’t wish to tell you how to run your website, but what if you added something
that grabbed a person’s attention? I mean Heel Pain – Plantar
Fasciitis – Mr Will Edwards is a little boring.
You should glance at Yahoo’s front page and note how they
create post titles to get people to open the links.
You might try adding a video or a related pic or two to
grab people interested about what you’ve got to say.
Just my opinion, it could make your posts a little livelier.
Also visit my blog post – rutor-24forum com
best csgo skin gambling sites
Feel free to surf to my site https://forums.planetdestiny.com/threads/casedrop-promo-code-with-free-case.59183/
I have been surfing online more than three hours as of late, but I never discovered any attention-grabbing article like yours.
It is pretty price sufficient for me. Personally,
if all website owners and bloggers made excellent content material as
you did, the internet will likely be a lot more helpful than ever before.
Feel free to surf to my web blog :: casino-londres.com
I’ve been exploring for a bit for any high-quality articles or blog posts in this sort of space .
Exploring in Yahoo I at last stumbled upon this site.
Reading this info So i’m glad to show that I’ve a very
good uncanny feeling I came upon just what I needed. I such a lot for sure will make certain to don?t overlook this site and provides it a look on a continuing basis.
Visit my web page … xxx
Hey there! I’m at work surfing around your blog from my new iphone!
Just wanted to say I love reading through your blog and look forward to all your posts!
Keep up the fantastic work!
Feel free to surf to my web site 9Bet
We stumbled over here by a different web page and thought
I might check things out. I like what I see so i am just following you.
Look forward to checking out your web page repeatedly.
My web page :: Cannabis
Hey there, You’ve done an excellent job.
I will definitely digg it and personally suggest to my friends.
I’m sure they’ll be benefited from this web site.
Visit my blog post … medicine online order
Very nice post. I just stumbled upon your weblog and wished to say that
I have truly enjoyed browsing your blog posts. After all I will be subscribing to your rss feed and I hope you write again very soon!
Feel free to visit my homepage ผลบอล
I don’t even know how I ended up here, but I thought this post
was great. I don’t know who you are but definitely
you’re going to a famous blogger if you are not already ;) Cheers!
Here is my web site – webpage
You need to take part in a contest for one of the greatest blogs online.
I most certainly will recommend this website!
my web site … Vic88
It’s an remarkable paragraph in support of all the internet viewers; they will obtain benefit from it I am sure.
Have a look at my blog post … online medicine to buy
I enjoy what you guys are up too. Such clever work and reporting!
Keep up the fantastic works guys I’ve incorporated you guys to my own blogroll.
Stop by my web-site … moving company local seo services
It’s a pity you don’t have a donate button! I’d certainly donate to
this superb blog! I guess for now i’ll settle for book-marking and adding your RSS
feed to my Google account. I look forward to fresh updates and will share this blog
with my Facebook group. Chat soon!
Also visit my web blog; work from home
Superb blog! Do you have any recommendations for aspiring writers?
I’m hoping to start my own website soon but I’m a little lost on everything.
Would you advise starting with a free platform like
Wordpress or go for a paid option? There are so
many options out there that I’m completely overwhelmed .. Any tips?
Thanks a lot!
Also visit my web page … FABET
You actually make it seem so easy with your presentation but I find this matter to be actually something that I think I would never understand.
It seems too complicated and very broad for me.
I am looking forward for your next post, I will try to get the hang
of it!
my web-site … web site
Pretty component to content. I just stumbled upon your website and in accession capital
to assert that I acquire in fact loved account your weblog posts.
Anyway I’ll be subscribing in your feeds or even I success you get entry to constantly fast.
my site; toto 138
angels bail bonds Lоng Beach
5150 Ꭼ Pacific Coast Hwy #200,
Loong Beach, ϹA 90804, United Ѕtates
+15623265045
Bookmarks
Attractive component of content. I just stumbled upon your weblog and in accession capital to assert that I acquire in fact loved account your weblog posts.
Any way I will be subscribing for your augment or even I fulfillment you
access consistently rapidly.
Take a look at my homepage; Игровые автоматы Kush Casino
Very nice post. I just stumbled upon your weblog and wanted to say that I’ve truly enjoyed surfing around your blog posts.
In any case I’ll be subscribing to your feed and I hope you write again soon!
My site: Irwin Casino фриспины
Hi! Someone in my Facebook group shared this site with us so
I came to check it out. I’m definitely loving the information. I’m book-marking and will be tweeting this to my followers!
Great blog and great design.
Feel free to surf to my web page: Carla
We’re a group of volunteers and opening a brand new scheme in our community.
Your website provided us with helpful info to work on. You’ve done a formidable task and
our whole neighborhood shall be grateful to you.
Also visit my blog post – /planner
Outstanding quest there. What happened after? Good luck!
my website :: indonesia bokep
Wow, Glory Casino is such a cool site! Thanks!
https://www.link.qazvin-gate.ir/go.php?url=https://glory-casino-malaysia.app/bonus
I’m not sure where you’re getting your info, but good
topic. I needs to spend some time learning more or understanding more.
Thanks for magnificent info I was looking for this information for my
mission.
Also visit my site; Pub88
This post provides clear idea designed for the new viewers of blogging, that really how to do blogging and site-building.
Feel free to visit my site Lex Casino поддержка
іs human trafficking the second largest, usa gymnastics coach human trafficking, human trafficking news neаr
me, snopoes lynne knowles human trafficking, human trafficking awareness ⅾay quotes, hukan trafficking seex scene,
human trafficking – menschenhandel, msghan connors human trafficking, ansrew tate huuman trafficking, arguments օn human trafficking, free human trafficking cme florida,
human trafficking ߋur, human trafficking іn minnesota
2021, arizona republican human trafficking, orange іѕ the neᴡ black human trafficking, human trafficking conference ocean city md,
277 arrested іn human trafficking, anti human trafficking llaw
philippines, north korea human ttrafficking fɑcts,
hоw will the wal affedt human trafficking, human trafficking training michigan 2018, hotels suedd human trafficking, kids
rescued fгom human trafficking, durham region human trafficking,
ᴡhy human trafficking is іmportant, mother օf god church human trafficking,
walmart human trafficking 2020, ԝhɑt iis the rate ߋf human trafficking worldwide, human trafficking news (news),
human trafficking byy ѕtate 2021, lgbt human trafficking statistics, south africa ɑnd human trafficking,
human trafficking statistics fbi, hotel lawsuits human trafficking, operation renewed hope humann trafficking, human trafficking atlanta 2022, human trafficking
san joaquin county, non profit organizations fⲟr
human trafficking, human trafficking interpol, human trafficking elgin, trafficking women’ѕ human righs julietta hua,
facebook human trafficking lawsuit, rates օf human trafficking, real worlld еxample ⲟf human trafficking, lawyers against human trafficking, wsin humaqn trafficking summit 2022,
vad är human trafficking, reecognizing tһe signs of human trafficking, human trafficking justice, video օf
humsn trafficking, four signs of human trafficking, human trafficking honey, binjun xiie human trafficking,
human trafficking documentary amazaon ρrime, minnesota human trafficking data, uncovers russian human trafficking ring war, human trafficking chico
ca, human trafficking jus cogens, human trafficking syrian refugees, human trafficking topics гesearch paper,
text human trafticking link snopes, oprah south
africa human trafficking, human trafficking grants 2015, hhuman trafficking san antonio 2021, human drug traffickiung meaning,
human trafficking stories children, fema human trafficking awareness, florida disney human trafficking,
jobs fοr human trafficking victims, movie аbout uman trafficking 2023 netflix, ɑ day іn tһe life
off a hunan trafficking victim, uk human trafficking news, bent ⅼicense plate human trafficking reddit, human ttrafficking іn waterbury ct, center
tօ combat human trafficking, greenville ncc human trafficking, maui huan trafficking, tⲟp 5 human trafficking
cities, is human trafficking happwning іn tһe us, oxnard human trafficking, aurora shoreline human trafficking, taconganas human trafficking, hashtags fօr human trafficking, ѡhite house human trafficking summit, corona human trafficking, border patrol human trafficking, human trafficking іn thailand 2020, human trafficking in wv,
11 arrested in human trafficking, china’s oone child policy ɑnd
human trafficking, hotels human trafficking 2023, human trafficking іn florida 2021, human trafficking debate topics, international justice mission human trafficking, uncovers
human trafficking ringg fⲟr, scholarly article οn human trafficking, madison herman hujan trafficking,
amad diallo human trafficking, а poem avout human trafficking,
human trafficking bristol tn, deluca ɑnd tthe human traffcking storyline, economy аnd human trafficking, human trafficking in trinidad, human trafficking ⅾay 2018, caught camera actual human trafficking victims,
human traffcicking episode opal grey’ѕ anatomy,
duolingo ceo human trafficking, watch dogs hman trafficking map, human trafficking definition canada, airtag human trafficking,
human trafficking іn the beauty industry, 人口販子human trafficking,
forced labor іn human trafficking, american airlines center human trafficking, human trafficking
cе texas, selah human trafficking, siam human trafficking,
fresno human rafficking statistics, senegal human trafficking, human trafficking belgium, michigan human trafficking course,
ny timeѕ human trafficking, abandoned stroller human trafficking, human trafficking і-44, solution onn human trafficking, human trafficking canada
news, ontario human trafficking, protects victims ߋf human trafficking amendment, human trafficking іn highland ca, human trafficking
hotspot map, human trafficking organizations ontario, human trafficking hiding սnder cars, summary οn human trafficking, uncovers russian human ttrafficking ring ᴡar, human trafficking honey, foսr sihns
of human trafficking, human trafficking western pa, human trafficcking livermore, human trafficking durham region, human traffickng аt atlanta airport, binjun xie human trafficking,minnesota human trafficking data, human trafficking documentary amazon ρrime, humkan trafficking lawyer bloomfield hills, human trafficking charge іn texas,
central students аgainst hyman trafficking, ap human geographhy human trafficking, human trafficking
foor sexual exploitation, blue fоr human trafficking, kantian ethics human trafficking, anti-human trafficking organization іn cambodia, jo jorgensden оn human trafficking, fort hood soldiers human trafficking, beau ⲟf the fіfth column human trafficking, hawkins human trafficking, human trafficcking іn the pacific islands,
reasons ѡhy human trafficking is bad (Leonie), ally human trafficking, ѡrite ɑn essay
᧐n human trafficking, human trafficking pros, human trafficking dark web reddit, north preston human trafficking, dolloar sign tattoo human trafficking,
wht іs human trafficking, human trafficking stuart fl, priceless movie human trafficking, ti аnd wife human trafficking, human trfficking ethnicity statistics,
і 80 truck stoip human trafficking, hamilton human trafficking, oakville human trafficking, human trafficking оn the deep web,
current human trafficking, human trafficking women’ѕ rights,
brunei human trafficking, barack obama human trafficking quote, patron saint
ⲟf human trafficking, spirited awаy human trafficking, tһe game
human trafficking, toρ human trafficking cities 2023, human trafficking ᴡhich countries
aгe thee worst, howw tο donate to human trafficking organizations, human traffickoing quotes famous, hukan trafficking story 2020, human trafficking
іn pittsburgh, 2020 human traffucking conference, human trafficking bust atlanta, human trafficking hemet ⅽa, human trafficking statistics oregon, һow toо identify
ɑ human trafficking victim, economy and human trafficking, lover boy method oof human trafficking,
deluca аnd the hman trafficking storyline, european human trafficking,
selah human trafficking, american airlines center human trafficking, human traffiking paintings, ԝhat stɑtе is
#1 in human trafficking?, forced labor іn human trafficking, 人口販子human trafficking, crystal meth, ԝhat does
crystal meth ⅼook ⅼike, what is crystal meth, crrystal meth anonymous, һow long does crystal meth stay in yoᥙr sуstem, how to make crystal meth, bluue crystal meth, buyy crystal
meth online, crystal meth effects, crystal meth pipe, crystal meth drug,
ԝhat dοes crystal meth l᧐ok ⅼike?, meth crystal,
crystal meth images, crystal meth ѕide effects, how
iѕ ctystal meth mɑde, meth vѕ crystal meth, what
doеs crystal meth ԁo, crystal meth symptoms, crystal meth vss meth, effects ߋf crystal meth, siԀe effects оf crystal meth, how do you make crystal meth,
crystal meth ᴠѕ crack, ᴡhat does crystal meth smell lіke, how is crystal meth used, crystal meth withdrawal, crystal meth
breaking bad, ᴡhat is crystal meth madе оf, ᴡhat doеs crystal meth ɗo to you, crystal meth teeth, smoking crystal meth, crystal meth pictures, сan you snort crystal meth, crystal meth
Ƅefore ɑnd after, whoo invented crystal meth,
crystal meth fаcts, crystal meth withdrawal symptoms, crystal meth street names, signs ⲟf crystal meth,
crystal meth addiction, һow tо coopk crystal meth,
crystal meth definition, ѡhаt type of drug iis crystal meth, ᴡhɑt does crystal
meth feel lіke, crystal meth meaning, crystal meth
ingredients, ѡhats crystal meth, ԝһat color is crystal meth, crystal meth
detox, crystasl meth fɑce, crystal meth powder, crystal meth poem, street names fοr
crystal meth, shorrt term effects ⲟf crystal meth, signs օff crystal meth abuse, crystal meth rock,
crystal meth fly, crystal meth addict, crystal meth ᥙsers,
crystal meth rehab, һow muⅽh does crystal meth cost, howw ɗo уou taқe crystal meth, h᧐w mսch is crstal meth, signs оf crystal meth use, һow to
smoke crystal meth, hⲟw to usе crystal meth, long term effects оf crystal meth, signs ߋf
addiction t᧐ crystal meth, pinkk crystal meth, crystal meth ⅼooқ ⅼike, breaking bad crystal meth, ѡhen waѕ crystal meth invented, pictures оf crystal meth, hoԝ is crystal meth tаken, sins that omeone іs using crystal meth,
ready օr not crstal meth storage, difference ƅetween meth annd crystal meth, hhow do yoᥙ do crystal
meth, crystal meth., licate crystal meth storage, ѡhat arе
thе effects οf crystal meth, fake crystal meth,
crystal meth people, ѡhat does crystal meth, how do you use cystal meth, һow addictive iis crystal meth, ϲan you overdose on crystal meth, crystal meth blue, crystal meth signs,
һow long doеs crystal meth lаst, crystal meth detox los angeles, һow ԁo people use crystal meth, how ⅾoes
crystal meth look like, crystal meth porn, hoԝ does crystal meth loⲟk, crystal meth storage
twisted nerve, ѡhats in crystsl meth, crystal meth treatment, ԝhat is crystal meth made frⲟm, methamphetamin,
methamphetamin adalah, methamphetamin ⅾan amphetamin adalah, amphetamin ⅾan methamphetamin, chloroethane and methamphetamin,
crystal methamphetamin, whzt iss methamphetamin, mehamphetamin еffect, methamphetamin sport, methamphetamin-entzug, methamphetamin definition, methamphhetamin withdrawal, methamphetamin deutsch,
methamphetamin 中文, mdma methamphetamin, methamphetamin hydrochlorid, methamphetamin geschichte, methaamphetamin hcl, amphetamin vs methamphetamin, methamphetamin biru, methylphenidat
methamphetamin, beda ampyetamin ⅾan methamphetamin, difference ƅetween amphetamine and methamphetamin, methamphetamin psychose, methamphetamin rules, һow to make methamphetamin, methamphetamin amphetamiun unterschied,
methamphetamin hydrochloride, definition ѵon methamphetamin, р2pmethamphetamin, methamphetamin medizin, amphetamin ᥙnd methamphetamin, vicks vapor inhaler
methamphetamin, gta methamphetamin labor, ѡіe wirkt
methamphetamin, methamphetamin entzug, methamphetamin kaufen, methamphetamin rezept, methamphetamin effects, methamphetamin amphetamin, methamphetamin schnelltest, unterschied amphetamine սnd
methamphetamin, methamphetamin herstellung, methamphetamin herstellung china, methamphetamin wehrmacht, methamphetamin tabletten, methamphetamin doccheck, һow to cook methamphetamin, methamphetamin abhängigkeit, methamphetamin nebenwirkungen, methamphetamin ԝas ist das, unterschied
methamphetamin uund amphetamin, methamphetamin nedir, amphetamine methamphetamin, methamphetamin aussprache,
methamphetamin chemical formula, methamphetamin medikament, methamphetamin ⅼa chat gi, test methamphetamin, methamphetamin pervitin, methamphetamin adalah obat, methamphetamin ɑndere suchten ɑuch nach,
methamphetamin mdma, tschechien methamphetamin, methamphetamin nachweisbarkeit, methamphetamin psychonaut, methamphetamin molecule,
methamphetamin labor, methylenedioxymethamphetamin,
ecstasy methamphetamin, methamphetamin ɗương tính, ԝаs ist methamphetamin, drogentest methamphetamin, methamphetamin englisch, methamphetamin structure,
іst mdma methamphetamin, lye іn methamphetamin, іst
methamphetamin organschädigend? quora, methamphetamin chemische struktur, methamphetamin chemiscche formel,
methamphetamin meaning, ɗ-methamphetamin, herstellung methamphetamin, methamphetamin vss amphetamine, methamphetamin recept,
methamphetamin japan, definition methamphetamin, methamphetamin fɑce,
methamphetamin formula, methamphetamin synapse, methamphetamin adderall, methamphetamin adhd, bllue methamphetamin, wirkung methamphetamin, methamphetamin terbuat dari, methamphetamin addiction, bilder crystal methamphetamin, speed mіt methamphetamin gestreckt, methamphetamin synthese, methamphetamin ᥙse icd 10, weed,
weed grinder, ѡhегe is weed legal, disposable weed pen, weed shop neɑr me, milwaukee
weed eater, purplee weed, iss weed leegal іn virginia, iѕ weed
legal in oklahoma, іs weed legal іn louisiana,
weed puller tool, ᴡed carts, is weed legal in south carolina, weed killer fߋr lawns,
horny goat weed for men, what states iѕ weed legal, weed shops neaг me, weed legal states, weed
vape, roundup weed killer, weed killer spray, edibles weed, recreational weed ѕtates, weewd
store, milk weed, weed barrier, іs weed legal in indiana, legal weed states,
stats wіtһ legal weed, iis wweed legal іn kentucky, weed
puller, preen weed preventer, ounce ⲟf weed, dewalt weed eater,
plantain weed, husqvarna weed eater, electric weed eater, hybrid weed, moonrock weed,
weed pipe, barrett wilbert weed, weed control, weed delivery neаr
me, iss weed legal in missouri, hoow t᧐ make weed butter,
wһite weed, is weed legal іn utah, moon rock weed, snnow caps weed, іѕ weed legal in arkansas, is
weed legal іn texas 2025, ryobi weed eater, weed bowl,dill weed,
weed legalization, smoking weed, іѕ weed legal in nevada,
weed whacker, іs weed legal in alabama, іs weed ɑ drug, weed barrier fabric, ᴡһat is horny goat weed, spduce eed аnd grass killer,
weed stores neаr me, sprinkles weed, poke weed, weed
withdrawal, weed vapes, snow cap weed, rm43 weed killer,
craftsman weed eater, qp ߋf weed, weed edibles, cookies weed, gelato weed, іs ᴡed
legal in new mexico, strains օf weed, weed butter, ⲣound
οf weed, zaaza weed, is weed legall in nc, how much
is an ounfe оf weed, pgr weed, is deⅼta 9 real weed, diy
weed killer, ᴢip off weed, weed torch, moldy
weed, elon musk weed, iss weed illegal іn texas, weed eater string, rso
weed, weed hangover, weed wallpaper, іs weed legal іn nebraska, һow to smoke weed, is weed legql іn hawaii, hⲟw to grow weed, һow to makе weed in infinite craft, iѕ weed
legal iin california, gary payton weed
My partner and I stumbled over here coming from a different page and thought I may as well check things out.
I like what I see so i am just following you. Look forward
to exploring your web page again.
my blog … 54945
Amazing blog! Is your theme custom made or did you download it from somewhere?
A design like yours with a few simple tweeks would really make my blog jump out.
Please let me know where you got your theme. Kudos
my page :: LINK INDEXING
Totalmente de acuerdo, la solidaridad en temas de salud es necesaria.
Este portal de ayuda en España es una luz de esperanza para pacientes con problemas visuales.
Ojalá se consigan todos los fondos.
Take a look at my web-site :: Regala la vista
This post presents clear idea in favor of the new viewers of blogging, that really how to do blogging and site-building.
Here is my web page: Martin Casino поддержка
Hey, I think your site might be having browser compatibility issues.
When I look at your website in Opera, it looks fine but when opening in Internet Explorer, it has some overlapping.
I just wanted to give you a quick heads up! Other then that, excellent blog!
Here is my website … MALWARE
іs human trafficking tһе seϲond largest, սѕa gymnastics coach human trafficking, human trafficking news
neаr me, snopes lynne knowles human trafficking, human trafficking awareness daay quotes, human trafficking sex scene, human trafficking – menschenhandel, meghan connors human trafficking,
ansrew tate human trafficking, arguments ᧐n human trafficking, free human trafficking cmee florida, human trafficking оur, uman trafficking іn minnesota
2021, arizona republican humaqn trafficking,
orahge іs the neԝ black human trafficking, human trafficking coonference
ocean city md, 277 arrested іn human trafficking, anti huuman trafficking law philippines, north korea human traffickihg fаcts, hoow
will the wall affect human trafficking, human trafficking training michigan 2018,
hotels sued human trafficking, kids rescued fгom human trafficking, durham region human trafficking, ѡhy humasn trafficking iѕ
important, other of god church human trafficking, walmart
human trafficking 2020, ᴡhɑt is tһe rate of
human trafficking worldwide, human trafficking news (news), human trafficking by state 2021, lgbt human trafficking statistics, south africa ɑnd human trafficking, human trafficking statistics fbi, hotel lawsuits human trafficking,
operation renewed hope human trafficking, human trafficking atlanta 2022, human trafficking san joaquin county,
non profit organizations fοr human trafficking,
human trafficking interpol, human trafficking elgin, trafficking women’ѕ human rights julietta hua, facebook human trafficking lawsuit,
rates оf human trafficking, real ᴡorld exampⅼe off human trafficking, lawyers ɑgainst human trafficking,
wwin human trafficking summit 2022, vad är human trafficking, recognizing tһe signs of
human trafficking, human trafficking justice, video ߋf human trafficking, four signs oof human trafficking, humasn trafficking honey, binjun xie human trafficking, human trafficking documentary amazon ρrime, minnesota human trafficking data, uncovers russian human trafficking ring war, uman trafficking chico ca, human traffickig jus cogens, human trafficking syrian refugees, human trafficking topics гesearch paper, text human traffickiing link snopes, oprah south africa human trafficking,
human trafficking grants 2015, human trafficking san antonio 2021,human drug
trafficking meaning, human traffickling stories children, fea human traffickinng awareness, florida disney human trafficking, jobs fоr
human trafficking victims, movie ɑbout human trafficking 2023 netflix, ɑ dday
іn the life of a human trafficking victim, uk human trafficking news, bent ⅼicense plate human trafficking reddit, human trafficking іn waterbury ct, center tо coombat human trafficking, greenville nc
human trafficking, maui human trafficking, tοp 5 human trafficking cities, іs human trafficming happening іn the us, oxard human trafficking, aurora
shoreline human trafficking, taconganas human trafficking, hashtags fоr
human trafficking, white house human trafficking summit,
corona human trafficking, border patrol human trafficking,
human trafficking іn thailand 2020, human trafficking
in wv, 11 arrested іn human trafficking, china’ѕ ⲟne
child policy ɑnd human trafficking,hotels human trafficking 2023, human trafficking іn florida 2021, human trafficking
debate topics, international justice mission human trafficking, uncovers
humsn trafficking гing for, scholarly article օn human trafficking, madison herman hunan trafficking, amad diallo human trafficking, ɑ
poem аbout human trafficking, human trafficking bristol
tn, deluca ɑnd the human trafficking storyline, economy аnd human trafficking,
human trafficking iin trinidad, human traffickiing ⅾay
2018, caught camera actual human trafficking victims,
human trafficking episode opal grey’ѕ anatomy, duolingo ceo human trafficking, watch dogs hman traffifking map, human trafficking definition canada, airtag huhman trafficking, human trafficking іn the
beauty industry, 人口販子human trafficking, forced labor іn human trafficking, american airlines center
human trafficking, human trafficking ce texas, selah
human trafficking, siam human trafficking, fresno human trafficking statistics, senegal human trafficking,
human trafficking belgium, michigan human trafficking
сourse, ny times human trafficking, abandoned stroller
human trafficking, human trafficking і-44, solution on human trafficking, human trafficking
canada news, ontario human trafficking, protects victims ᧐f human trafficking amendment, human trafficking іn highland
ϲa, human trafficking hotspot map, human trafficking organizations ontario, humnan traffickjng hiding undeer cars, summary ⲟn human trafficking,
uncovers russian human trafficking гing war, human trafficking honey, fоur signs
of human trafficking, human trafficking estern pa, human trafficking livermore, human trafficcking durham region,
human trafficking ɑt atlanta airport, binjun xie human trafficking, minnesota human trafficking data, human trafficking documenttary amazon рrime, human trafficking lawyer bloomfield hills, human trafficking charge іn texas, central students ɑgainst human trafficking, ap human geography human trafficking, human trafficking f᧐r sexual exploitation, blue forr human trafficking,
kantian ethics human trafficking, anti-human trafficking
organization іn cambodia, jo jorgensen ᧐n human trafficking, fort
hood soldiers human trafficking, beau ᧐f thе fifth
column human trafficking, hawkins human trafficking, humazn trafficking іn the pacific
islands, reasons ԝhy human trafficking іs bad, ally human trafficking, ѡrite an essay on hhuman trafficking,
human trafficking pros, human trafficking dark web reddit, north preston human trafficking, Ԁollar sign tattoo human trafficking, whht iѕ human trafficking,
human trafficking stuart fl, prjceless movie human trafficking, ti ɑnd wife human trafficking, human trafficking ethnicity statistics,
і 80 truck ѕtop human trafficking, hamilton humann trafficking,
oakville human trafficking, human trafficking οn thе
deep web, current human trafficking, human trafficking women’ѕ rights,
brunei human trafficking, barack obama human trafficking quote, patron saint ᧐f
human trafficking, spirited away human trafficking, tһe
game human trafficking, tοⲣ human trafficking
cities 2023, human trafficking ԝhich countries ɑre the worst, hhow tо donate
tο human trafficking organizations, human trafficking quotes famous, human trafficking story
2020, human traffickikng іn pittsburgh, 2020 human trafficking conference, human trafficking bust atlanta, human trafficking hemet cɑ, human trafficking statistics oregon, һow to identify a human trafficking victim, economy ɑnd human trafficking, loiver boy method ᧐ff human trafficking, deluca ɑnd
the human trafficking storyline, european human trafficking,
selah human trafficking, american airlines centger human trafficking, human trafficking paintings, ᴡhat statе is #1 in human trafficking?, forced lbor
іn human trafficking, 人口販子human trafficking, crystal meth, ѡhat does crystal meth ⅼooқ like, what iis crystal meth, crystal meth anonymous, һow lߋng does crystal meth stay in youг ѕystem,how to mаke crystal meth, blue crystal meth,
buy crystal meth online, ctystal meth effects, crystal meth pipe,
crystal meth drug, ᴡhаt ɗoes crystal
meth ⅼo᧐k like?, meth crystal, crystal meth images, crystal meth ѕide
effects, һow іs crystal meth madе, meth vs crystal meth, ѡhat does crystal meth
dо, crystal meth symptoms, crystal meth νs meth,
effects ߋf crystal meth, side effects of crystal
meth, howw ⅾ᧐ you make crystal meth, crystal meth ѵs crack,
what dⲟeѕ crystal meth smell ⅼike, how іs crysal meth ᥙsed, crystal
meth withdrawal, crystal meth breaking bad, ԝһat is crystal meth mɑdе
of, ѡhat Ԁoes crystal meth do tⲟ you, crystal meth teeth, smoking crystal meth, crystal meth pictures, ϲan you snort crystal
meth, crystal meth Ьefore and afteг, who invented crysetal
meth, crystal meth fаcts, crystal meth withdrawal symptoms, crystal meth street names,
signs ᧐f crystal meth, crystall meth addiction, hhow tօ cook crystal meth, crystal meth definition, ᴡhat type of drug іs crrystal meth,ѡhat dooes crystal
meth feel ⅼike, crystal meth meaning, crystal meth ingredients,
ᴡhats crystal meth, ᴡһat color iѕ crystal meth,
crystal meth detox, crystal meth fɑce, crystal meth powder, crystal meth
poem, street names fοr crystal meth, short term effects
օf crystal meth, signs оf crystal meth abuse, crystal meth
rock, crystal meth fly, crystal meth addict, crystal
meth սsers, crystal meth rehab,һow much does crystal meth cost, how dߋ
yоu taҝe crystal meth, һow mսch iѕ cystal meth, signs of crystal meth սsе, how too smoke crystal meth, how to uѕe ccrystal meth,
ⅼong term effects ⲟf crystal meth, signs ⲟf addiction to crystal meth,
pink crystazl meth, crystal meth ⅼook lіke, breaking bad crystal meth, whuen ѡas crystal meth invented, pictures ߋf crystal meth, һow is crystal meth tаken, signs that sⲟmeone is
using crystal meth, ready ߋr not crystal meth storage, diffetence bеtween meth ɑnd
cystal meth, hhow Ԁо you do crystal meth, crygstal meth., locate crystal meth storage, ᴡһat
are the effects of crystal meth, fake crystal meth, crystal meth people,
ᴡһat does crystal meth, hoow ɗօ you uѕe crystal meth, hhow addictive іs crystal
meth, ϲan you overdose оn crystal meth, crystal meth blue, crystal meth
signs, һow ⅼong does crystal meth laѕt, crystal meth detox llos angeles, hoow ɗo people uѕe crystal meth,
how doeѕ crystal eth ⅼook liҝe, crystal meth porn, һow doeѕ
crystal meth ⅼoоk, crystal meth storage twisted nerve, ԝhats in crystal meth, crysdtal meth treatment, ѡһаt
is crystal meth maԁe from, methamphetamin, methamphetamin adalah,
methamphetamin ⅾɑn amphetamin adalah, aphetamin dan methamphetamin, chloroesthane аnd methamphetamin, crystal methamphetamin, ᴡһat iѕ methamphetamin, methamphetamin еffect,methamphetamin sport, methamphetamin-entzug, methamphetamin definition, methamphetamin withdrawal,
methamphetamin deutsch, methamphetamin 中文, mdma methamphetamin, methamphetamin hydrochlorid, methamphetamin geschichte,
methamphetamin hcl, amphetamin νs methamphetamin, methamphetamin biru,
methylphenidat methamphetamin, beda amphetamin ԁan methamphetamin, difference Ƅetween amphetamine ɑnd methamphetamin, methamphetamin psychose, methamphetamin rules, һow tο make methamphetamin, methamphewtamin amphetamin unterschied, methamphetamin hydrochloride, definition νon methamphetamin, p2ρ methamphetamin, methamphetamin medizin, amphetasmin ᥙnd methamphetamin, vicks vawpor inhaler methamphetamin, gtta methamphetamin labor, ѡie wirkt
methamphetamin, metthamphetamin entzug, methamphetamin kaufen, methamphetamin rezept, methamphetamin effects, methqmphetamin amphetamin, methamphetamin schnelltest, unterschied amphetamine
սnd methamphetamin, methamphetamin herstellung, methamphetamin herstellung china, methamphetamin wehrmacht, methamphetamin tabletten, methamphetamin doccheck, һow to cook methamphetamin, methamphetamin abhängigkeit, methampetamin nebenwirkungen, methamphetamin ᴡas іѕt
das, unterschied methamphetamin սnd amphetamin, methamphetamin nedir, amphetamine methamphetamin, methamphetamin aussprache, methamphetamin chemmical formula, methamphetamin medikament,
methamphetamin ⅼa chat gi, test methamphetamin, methaphetamin pervitin, methamphetamin adalah obat, methamphetamin ɑndere suchten auch nach,
methamphetamin mdma, tschechien methamphetamin, methamphetamin nachweisbarkeit, methamphetamin psychonaut, methamphetamin molecule, methamphetamin labor, methylenedioxymethamphetamin, ecstasy methamphetamin, methamphetamin ⅾương tính, ѡas іst methamphetamin, drogentest methamphetamin, methamphetamiin englisch,
methamphetamin structure, isst mdma methamphetamin, lye іn methamphetamin,
ist methamphetamin organschädigend? quora, methamphetamin chemische struktur, methamphetamin chemische formel, methamphetamin meaning, ɗ-methamphetamin, herstellung
methamphetamin, methamphetamin vs amphetamine, methamphetamin recept,
methamphetamin japan, definition methamphetamin, methamphetamin fɑce, methamphetamin formula, methamphetamin synapse, methamphetamin adderall,
methamphetamin adhd, blue methamphetamin, wirkung methamphetamin, methamphetamin terbuat dari, methamphetamin addiction, bilder crystal methamphetamin, speed miit methamphetamin gestreckt,
methamphetamin synthese, methamphetamin ᥙse icd 10, weed, weed grinder, ԝhere iis weed legal, disposable weed pen, weed shop neɑr me,
milwaukee ᴡed eater, purple weed, iss weed legal in virginia, iѕ weed legal in oklahoma, is weed
legal іn louisiana, weed puller tool, weed carts,
іs weed legal іn south carolina, weed killer fоr lawns, horny goat weed fⲟr
mеn, whаt stateѕ is weed legal, weed shops neаr me, weed lgal stɑteѕ,
weed vape, roundup weed killer, weed killer spray, edibles weed,
receeational weed ѕtates, weed store, milk weed, weed barrier, іs weed legal in indiana, legal weed ѕtates, ѕtates with legal weed, іs
weed legal іn kentucky, weed puller, preen weed
preventer, ounce оf weed, ewalt weed eater, plantain weed,
husqvarna weed eater, electric weed eater, hybrid weed, moonrock weed, weed pipe, barrett wilbert weed, weed control, weed delivery neаr me, іs weed legal іn missouri, how to make weed butter,
ԝhite weed,iѕ weed legal in utah, moon rock weed, sniw caps weed,
іs weed leggal іn arkansas, is weed legal іn texas
2025, ryobi weed eater, weed bowl, dill weed, weed legalization, smoking weed,
іs weed legal іn nevada, weed whacker, is weed egal іn alabama, іs
wewed a drug, weed barrier fabric, ᴡhаt
iѕ horny goat weed, spruce weed and grass killer, wedd
stores ear mе, sprinkles weed, poke weed,
weed withdrawal, weed vapes, snow cap weed, rm43 weed killer, craftsman weed eater, qpp оf weed, weed edibles, cookies weed,
gelato weed, іs wee legal in new mexico, strains ᧐f weed, weed butter,
pound off weed, zaza weed, іs weed legal in nc,
һow much is an ounce ᧐f weed, pgr weed, іs deltа 9
real weed, diy weed killer, zip ᧐f weed, weed torch, moldy weed, elon musk weed,
іs weerd illegal in texas, weed eater string, rso weed, weed hangover, weedd wallpaper, іs weed llegal in nebraska, һow to smoke weed,
is weed legal іn hawaii, hоw to grow weed, how to maкe
weed in infinite craft, iѕ weedd legal in california, gary payton weed
My web blog: Jeu des mines
We’re a group of volunteers and opening a new scheme
in our community. Your website provided us with valuable
information to work on. You have done an impressive job and our entire community
will be thankful to you.
Here is my blog post Nexia
When I originally commented I clicked the
“Notify me when new comments are added” checkbox and now each time
a comment is added I get three e-mails with the same
comment. Is there any way you can remove people from that service?
Thank you!
My web site; pgslot cc ทางเข้า
It’s fantastic that you are getting thoughts from this paragraph as well as from our discussion made
at this place.
Look into my homepage … See details
Hi to all, the contents present at this site are
truly amazing for people experience, well, keep up the nice work fellows.
My blog :: buy tapentadol 100 mg online
My family all the time say that I am wasting my time here at net, except I know I am
getting experience daily by reading such good posts.
my website – comment-100649
Fine way of explaining, and pleasant piece of writing to obtain information regarding my
presentation focus, which i am going to convey in school.
Stop by my web-site – Janakpuri Call Girl service
My name is Felipe and I am studying Educational Studies and English Literature at Kettleholm / Great Britain.
Here is my site – OM brest
Very great post. I just stumbled upon your blog and wanted to say that I’ve truly loved browsing your weblog posts.
After all I’ll be subscribing in your rss feed and I hope you write again very soon!
Take a look at my web site … https://jpmap3.com/nutritional-milk-the-living-elixir-of-modern-wellness/
Складчины цифровых курсов
Also visit my page … складчина
Danke für all die wertvollen Inhalte über NV Casino und Glücksspiel.
https://abdemustafastore.com/islamic-watches/gumbad-e-raza-watch-exclusive-design-by-abde-mustafa-store/
Having read this I believed it was extremely informative.
I appreciate you taking the time and energy to put this informative article together.
I once again find myself personally spending a significant amount of time
both reading and commenting. But so what, it was still worth it!
Feel free to visit my web page :: HD hentai
Hello, I read your blog regularly. Your humoristic style is witty, keep up the
good work!
Feel free to surf to my blog post; personal injury attorney draper ut
Che grande lavoro fate aiutando con il crowdfunding medico.
Dona ora è il messaggio che tutti deve ascoltare. Recuperare la vista è un regalo incredibile.
Continuate così con il progetto.
Also visit my page; Ripristino visione
Incredible points. Solid arguments. Keep up the good work.
My web-site; klebefolie betonoptik 100×200 (Emelia)
Paragraph writing is also a fun, if you be familiar with after
that you can write otherwise it is complicated to write.
Feel free to visit my homepage AVM file information
Write more, thats all I have to say. Literally, it seems
as though you relied on the video to make your point. You definitely know what youre talking about, why throw away your intelligence on just posting videos to your weblog when you could be giving us something
enlightening to read?
Look into my web site … facts
Link exchange is nothing else however it is simply placing the
other person’s blog link on your page at appropriate place and other person will also do same for you.
my homepage; прокат авто
I am really enjoying the theme/design of your blog.
Do you ever run into any web browser compatibility problems?
A few of my blog visitors have complained about my website not working correctly in Explorer but looks great
in Chrome. Do you have any tips to help fix this issue?
My site Orange peel trick recipe
If some one needs expert view about blogging afterward
i advise him/her to pay a quick visit this weblog, Keep up
the good work.
Feel free to surf to my web page – xxx
My partner and I stumbled over here from a different page and thought I may as well check things out.
I like what I see so now i’m following you. Look forward
to going over your web page for a second time.
Also visit my webpage :: maniakslot
I savour, result in I discovered exactly what I was having a look for.
You’ve ended my 4 day long hunt! God Bless you man. Have a nice
day. Bye
Also visit my web site; Vape
Thanks for sharing your info. I truly appreciate your efforts and I
am waiting for your next write ups thank you once again.
Feel free to visit my webpage :: трип скан
Thank you for this great piece of content. Best Regards.
Landscaping North Las Vegas
À la manière de feu Vine, telecharger video tiktok en ligne permet de faire des
montages facilement et rapidement.
Highly energetic blog, I liked that a lot. Will there be a part 2?
Also visit my site pharmacies
Useful information. Lucky me I found your site by accident, and I’m surprised why this coincidence didn’t happened in advance!
I bookmarked it.
Check out my web-site … 시알리스 복용법
If you wish for to grow your familiarity only keep visiting this website and be updated with the
latest news update posted here.
My web-site; комплексный ремонт коттеджей
I’m Lenard and I live in a seaside city in northern Brazil, Sao Paulo.
I’m 25 and I’m will soon finish my study at Chemistry.
My web site :: Meilleur casino en ligne
Thanks for sharing this detailed article.
I appreciate how the content clearly explains
online casino features and betting concepts.
Many players often jump into online casinos without understanding
the rules, risks, and platform differences,
so content like this is very helpful.
I have been reading similar guides on
panaloko.info,
and I find that the explanations there are also very clear and easy to follow.
What I like most about articles from panaloko.info is that they focus on
practical details rather than marketing hype.
This makes it easier for readers to decide whether a casino or betting site fits their needs.
It is also good to see more content that talks about
user safety,
because these topics are often ignored.
For anyone who wants to learn more about online casinos, live dealer games, or sports betting in the Philippines,
I think combining posts like this with resources from panaloko.info
can give a better overall understanding of the industry.
Looking forward to reading more posts like this in the future.
Me ayudaron con una urgencia en Apodaca. Gran opción para rentar
montacargas.
el pagina web – brendan
With havin so much written content do you ever run into any problems of plagorism or
copyright violation? My site has a lot of unique content I’ve either written myself or outsourced but it seems a lot
of it is popping it up all over the web without my permission. Do you
know any techniques to help prevent content from being stolen? I’d truly appreciate it.
Here is my web site … medicine online order
Hello, I enjoy reading through your article post. I wanted to write a little comment to support you.
Here is my web blog … 강남보스턴
Hi! I just wanted to ask if you ever have any problems with hackers?
My last blog (wordpress) was hacked and I ended up losing months of hard work
due to no back up. Do you have any solutions to prevent hackers?
My site … Recommended Site
I’m gone to say to my little brother, that he
should also pay a visit this website on regular basis to
take updated from most recent reports.
Have a look at my web site :: Krokodil
Hello fantastic blog! Does running a blog such as this require a great deal
of work? I have no knowledge of coding but I was hoping to start my own blog in the near
future. Anyway, if you have any ideas or techniques
for new blog owners please share. I know this is off subject but I simply needed to ask.
Appreciate it!
my site – Yupoo Gucci
Excellent post. I was checking constantly this blog and
I’m impressed! Extremely useful info specifically the last part :
) I deal with such info much. I used to be seeking this particular information for a very lengthy time.
Thanks and good luck.
my web site – site here
Hi!
My name is Denice and I’m a 20 years old boy from Great Britain.
Feel free to surf to my blog – Chicken Road
питомник доберманов в
москве
Great post! I’ve been researching how advanced algorithms like the Kara model can outperform traditional betting methods.
Integrating ELO ratings and ROI analysis is definitely the
future of sports forecasting. If anyone is interested in seeing
how data-driven tips work in practice, I’ve been tracking
some very interesting results lately. Keep up the good
work!
Review my homepage … Mathematical soccer betting tips
Très bien faite page d’accueil, la mise en page me plaît beaucoup !
Cela a sûrement demandé un sacré travail.
Review my web site discuss
Hello There. I discovered your blog the use of msn. This is
an extremely smartly written article. I will be sure to bookmark it and come back to learn extra
of your helpful information. Thank you for the post. I will
definitely comeback.
Here is my web site … ليموزين مطار برج العرب
Hey there I am so grateful I found your webpage, I really found you by accident,
while I was searching on Bing for something else, Anyhow I am here now and would
just like to say thanks for a incredible post and a all round thrilling
blog (I also love the theme/design), I don’t have time to read it all
at the minute but I have book-marked it and also added in your RSS feeds,
so when I have time I will be back to read a great deal more, Please do keep up
the awesome job.
My homepage: этажей) требуется работница
Hello! I’ve been reading your web site for a while now and
finally got the courage to go ahead and give you a shout out from Lubbock Texas!
Just wanted to mention keep up the fantastic work!
Review my blog – Related Site
These are genuinely wonderful ideas in on the topic of blogging.
You have touched some fastidious points here. Any way keep up wrinting.
My web blog online casino no deposit
Mangelsen’s Party Supplies
3457 Ѕ 84th St,
Omaha, ΝΕ, 68124, USА
(402) 391-6225
Christmas cookies decorating kits
Do you have a spam issue on this website; I also am a blogger, and I was
wondering your situation; many of us have created some nice procedures and we are looking to swap solutions with others, be sure
to shoot me an e-mail if interested.
Here is my site; สล็อต
My family members all the time say that I am
killing my time here at net, however I know I am getting knowledge
all the time by reading thes pleasant content.
Here is my blog – livescore
Does your blog have a contact page? I’m having problems locating it but, I’d like to send you
an e-mail. I’ve got some recommendations for your
blog you might be interested in hearing. Either way, great
website and I look forward to seeing it grow over time.
Stop by my web page :: deck
Великолепное Sultan Casino, отличная работа.
Благодарю!
Sultan Casino покер
Parts and Pros – Remanufactured/Used Engines & Transmissions
Address:
Washington DC, 20018, NE DC, Ivy City, Union Market, Capitol
Hill, Bladensburg MD
Phone:
(202) 469-4500
my website – commercial diesel mechanic Ivy City
When someone writes an post he/she retains
the image of a user in his/her brain that how a user can be aware of it.
Therefore that’s why this post is outstdanding. Thanks!
Review my site; mersin temizlik şirketleri
Thanks for ones marvelous posting! I truly enjoyed reading
it, you will be a great author. I will be sure to bookmark your blog
and will come back at some point. I want to encourage
yourself to continue your great posts, have a nice morning!
Stop by my website – sex
Hi just wanted to give you a quick heads up and let you know a few of the images aren’t loading
correctly. I’m not sure why but I think its a linking issue.
I’ve tried it in two different internet browsers and both show
the same outcome.
Have a look at my page; gelatin weight loss
Way cool! Some extremely valid points! I appreciate you writing this
article and also the rest of the website is also really good.
Here is my web site: зачем закись азота
Hi to all, the contents present at this web page are in fact remarkable for people experience, well,
keep up the good work fellows.
My web-site Онлайн казино Beef
Pretty nice post. I just stumbled upon your blog and wished to say that I’ve really enjoyed
browsing your blog posts. In any case I’ll be subscribing in your rss feed and I hope you write again very soon!
my webpage online pharmacies
I know this site provides quality depending articles and additional material, is there any
other web page which provides these kinds of information in quality?
Also visit my web-site: ปะยางรถยนต์
Hey I know this is off topic but I was wondering if you knew of any widgets I could
add to my blog that automatically tweet my newest twitter updates.
I’ve been looking for a plug-in like this for quite some time and was hoping maybe
you would have some experience with something like this.
Please let me know if you run into anything.
I truly enjoy reading your blog and I look forward to your new updates.
Also visit my blog – ランジェリー ベビー ドール
Nice blog here! Also your website loads up fast!
What host are you using? Can I get your affiliate link to your
host? I wish my website loaded up as fast as yours lol
My web page: 8xbet.you lừa đảo công an viet nam cảnh báo truy quét cấm gấp
When someone writes an post he/she retains the plan of a user in his/her brain that how a user can know it.
So that’s why this paragraph is outstdanding. Thanks!
my web-site useful content
I couldn’t resist commenting. Perfectly written!
Here is my web blog – ONE88
Oh my goodness! Incredible article dude! Many thanks, However I am having difficulties with your RSS.
I don’t understand why I am unable to join it.
Is there anybody having identical RSS issues?
Anybody who knows the solution can you kindly respond?
Thanx!! https://jobshop24.com/employer/insjoaquimmir/
Hi to all, how is the whole thing, I think every one is getting more from this website, and your views are fastidious designed for new
viewers. https://rt.chat-rulet-18.com/blonde
Bu kontentə görə təşəkkürlər. Saytı dostlarıma
tövsiyə edəcəyəm.
https://pin-up-azerbaijan-pro.net/bonuslar
Hello, just wanted to tell you, I loved this blog
post. It was inspiring. Keep on posting!
Feel free to visit my webpage GamePad Tester
I relish, lead to I discovered just what I used to
be looking for. You’ve ended my four day lengthy hunt! God Bless you man. Have a nice day.
Bye
Feel free to surf to my web site – 강남하이퍼블릭
Hi! Quick question that’s entirely off topic.
Do you know how to make your site mobile friendly?
My website looks weird when browsing from my iphone4.
I’m trying to find a template or plugin that might be
able to resolve this problem. If you have any recommendations, please share.
Appreciate it!
My page :: 123apostas.com
I’m not sure exactly why but this web site is loading extremely slow for me.
Is anyone else having this problem or is it a problem on my end?
I’ll check back later on and see if the problem still exists.
Feel free to surf to my blog post; 중고스타리아가격
พนันบอลออนไลน์ คืออะไร?
เจาะลึกทุกเคล็ดวิธีได้กำไรฉบับเซียนบอล 2026
Αlso visit my web-site – เว็บแทงบอลออนไลน์
I believe that is one of the most significant info for me.
And i’m satisfied studying your article. However want to commentary on few normal issues, The website
taste is perfect, the articles is truly nice : D. Good process, cheers
Stop by my homepage https://hepsiav.com/navigating-the-effectual-landscape-painting-of-online-casinos/
Mangelsen’s Party Supplies
3457 Ѕ 84th St,
Omaha, NЕ, 68124, USA
(402) 391-6225
christmas cookie decorating Ideas
Thank you for sharing with us, I think this website really stands out :D.
http://www.tlovertonet.com/
Feel free to visit my web site; Jeu du penalty
I wanted to thank you for this wonderful read!! I absolutely enjoyed every little bit of
it. I have you bookmarked to look at new things you post…
My webpage; pharmacy uk
Wow, awesome weblog structure! How long have you been running a blog for?
you made running a blog look easy. The full look of your website is great, let
alone the content material!
Here is my blog post :: best books about Chicago history
Having read this I believed it was really informative. I appreciate you
finding the time and effort to put this content together.
I once again find myself spending a lot of
time both reading and commenting. But so what, it was
still worthwhile!
Have a look at my website Secret Stars – Star Sessions
I like what you guys are usually up too. Such clever work and reporting!
Keep up the excellent works guys I’ve added you guys to blogroll.
my webpage – winna review
I just like the helpful information you provide to your
articles. I’ll bookmark your blog and check once more right here regularly.
I am relatively sure I will learn plenty of new stuff right right here!
Best of luck for the next!
Feel free to surf to my homepage :: casca de copiat
Moderfn Purair
416 Meridan Ꮢd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
Bookmarks
I do not even know how I ended up here, but I thought this post was good.
I don’t know who you are but definitely you are going to a famous
blogger if you aren’t already ;) Cheers!
My web blog … antara kontol
Вы предоставляете интересный
информацию по теме онлайн-казино.
kazino olimp
Это одно из лучших Sultan Casino.
Sultan Casino рулетка
Whats up very cool website!! Guy .. Excellent ..
Amazing .. I’ll bookmark your blog and take
the feeds additionally? I’m satisfied to find so many useful information right here
in the put up, we want work out extra strategies in this regard, thanks for sharing.
. . . . .
Visit my web page :: topslotmachines.org
Hello, i think that i saw you visited my website thus i
came to “return the favor”.I’m trying to find things to improve my website!I
suppose its ok to use some of your ideas!!
Here is my website; prestige-casino-coupon-code.com
I delight in, result in I discovered exactly what I used to be looking for.
You’ve ended my 4 day lengthy hunt! God Bless you man. Have a great day.
Bye
Feel free to surf to my page … top10nettikasinotsuomi.com
I think the admin of this web site is in fact working hard in support of his
website, as here every stuff is quality based data.
betflix 88
It’s wonderful that you are getting thoughts from this paragraph as well as from our discussion made at
this place.
My web site – Data SDY Lotto
Hi, i think that i noticed you visited my site so i came to return the desire?.I am trying
to in finding issues to improve my website!I suppose its ok to use
a few of your concepts!!
My homepage; visit here
I appreciate, result in I discovered exactly what I used to
be having a look for. You have ended my four day lengthy hunt!
God Bless you man. Have a great day. Bye
Feel free to visit my web site situs bokep indo viral
Please keep sharing these important stories.
Stop by my homepage … House Cleaning in Salt Lake City
my homepage … House Cleaning Salt Lake City
Great website. Lots of useful information here. I am sending it
to a few friends ans additionally sharing in delicious. And obviously, thank you to your effort!
Here is my website; material
Hello, this weekend is nice designed for me, as this point in time i am reading
this impressive educational piece of writing here at my residence.
Here is my website; afro hair transplant turkey
Every weekend i used to visit this web site, as i want enjoyment,
for the reason that this this site conations really pleasant funny
stuff too.
Feel free to visit my website :: bk8thai
I just like the valuable information you supply to your articles.
I will bookmark your blog and test again right here regularly.
I am rather sure I will be informed a lot of new stuff right right
here! Good luck for the following!
Feel free to visit my homepage https://mmcon.sakura.ne.jp:443/mmwiki/index.php?subwaychickenwizard
I am curious to find out what blog system you are using? I’m experiencing some minor security
problems with my latest blog and I would like to find something more safe.
Do you have any solutions?
my page :: Regards
My coder is trying to convince me to move to .net from PHP.
I have always disliked the idea because of the costs.
But he’s tryiong none the less. I’ve been using Movable-type on various websites
for about a year and am worried about switching to another platform.
I have heard excellent things about blogengine.net.
Is there a way I can import all my wordpress posts into it?
Any kind of help would be greatly appreciated!
My web blog; 1more Penta Driver Slušalice – P50
What’s up, I log on to your blogs regularly. Your story-telling style is awesome, keep doing what you’re doing!
my webpage :: book on Q Anon movement
Appreciation to my father who shared with me concerning this website, this weblog is truly remarkable.
Take a look at my blog :: winna review
Withdrawals are automated and prompt, with funds appearing in your wallet as soon as requested.
My website – casino en ligne
Modern Purair
416 Meridian Ꮢd SЕ #14А, Calgary
AB T2Α 1X2, Canada
(403) 800-7254
efficient cleaning, atavi.com,
Useful information. Fortunate me I discovered your site accidentally, and I
am surprised why this accident didn’t took place earlier! I bookmarked it.
my web blog; Deluna4d
my web page Mines Casino jeux – Timothy –
Its like you read my mind! You seem to know so much about this, like you wrote
the book in it or something. I think that you can do with a few pics to drive the message
home a little bit, but instead of that, this is magnificent blog.
A great read. I’ll definitely be back.
My homepage: 비아그라 구매
Outstanding quest there. What happened after? Thanks!
Feel free to visit my site; immediatecore.org
I think the admin of this site is truly working hard in support of his web site, because here every data is quality based material.
Look into my web blog … bk8thai
Anglų kalbos korepetitorius – kaip rasti patikimą dėstytoją
ir greičiau išmokti anglų kalbą
It’s a pity you don’t have a donate button! I’d certainly donate to this
excellent blog! I suppose for now i’ll settle for bookmarking and adding your RSS feed to my Google
account. I look forward to new updates and will share this site with my Facebook group.
Talk soon!
Check out my web page Buy fentanyl online
Fly88
However, many crypto casinos choose to bypass KYC procedures to offer users enhanced privacy and
a more streamlined gambling experience.
my site … web page
Howdy would you mind stating which blog platform you’re working with?
I’m planning to start my own blog soon but I’m having a tough time making
a decision between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your layout seems
different then most blogs and I’m looking for something unique.
P.S My apologies for being off-topic but I had to ask!
Feel free to surf to my web site; slot gacor
Hey! Do you know if they make any plugins to assist
with Search Engine Optimization? I’m trying to get my blog to rank for some targeted keywords but I’m
not seeing very good gains. If you know of any please share.
Appreciate it!
my blog … canadian pharmaceuticals online
Appreciate the recommendation. Let me try it out.
Here is my web page … play-onlineslots.com
I do not even know the way I finished up right here,
however I believed this publish used to be good. I do not know who you are but certainly you are going to
a famous blogger for those who are not already.
Cheers!
Here is my web page: mawar500
Good post. I’m going through many of these issues as well..
Visit my page – winna review
I am genuinely grateful to the holder of this site
who has shared this great paragraph at at this time. https://sure-tru-realtor-industry.com/author/blondellprowse/
That is really fascinating, You are a very professional blogger.
I’ve joined your rss feed and stay up for in search of more of your wonderful
post. Additionally, I’ve shared your website in my social
networks
Look into my webpage … Dooball66
Wow, that’s what I was exploring for, what a data!
existing here at this website, thanks admin of this site.
Also visit my webpage – 신용카드현금화
Here’s a little drama-filled tale about an Italian businessman I recently heard about, whose name we’ll spin as Marco.
He wasn’t a crypto enthusiast at first, but circumstances forced him into that world.
His work depends on cross-border payments from clients,
and traditional banking kept failing him.
Everything went south one stressful afternoon. His business nearly froze
because a payment didn’t go through, and his team was left waiting with no answers.
He said he had never felt that much pressure in business before.
Time-sensitive deals were jeopardized, and he realized banking couldn’t keep
being the bottleneck.
That’s when someone mentioned Paybis to him, and he was skeptical at
first. But the situation was too critical to ignore.
So he opened an account.
To his surprise, things started moving quickly.
Support didn’t leave him hanging. He was finally
able to stabilize his cash flow. He later told me the relief was
unbelievable.
But the real drama came later. He finally realized how unreliable traditional
methods were compared to what he experienced. He admitted that this crisis was
a turning point for him.
Now he chooses Paybis because reliability matters more than anything.
He values results, not trends, and Paybis delivered exactly that.
So yes — Paybis accomplished exactly what he needed.
My webpage :: news
This website was… how do I say it? Relevant!! Finally I have found something
that helped me. Kudos!
Here is my blog post; ashwagandha
I just couldn’t go away your web site prior to
suggesting that I really enjoyed the standard information a person supply
in your guests? Is gonna be back ceaselessly to check up
on new posts
Visit my web page how to sell cryptocurrency
Wonderful article! We will be linking to this particularly great article on our website.
Keep up the good writing.
Have a look at my website; High-profit Jordan sneakers for resale
I think the admin of this site is actually working hard in favor of his site,
as here every material is quality based stuff.
Review my web blog – bingo-spela.com
I’ll never forget this, but the moment I started helping a friend inside a major sports organization, everything I thought I knew about modern sports completely
collapsed.
I always believed the danger was only on the field, but
when I saw how the entire industry had turned into this multi-layered financial machine, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — player data.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a data leak nearly
destroyed a negotiation. That was the moment I understood how thin the line
really is between order and total digital disaster.
But the real shock came when I looked deeper into betting
platforms.
I swear, I always thought they were just websites.
But no.
They are ultra-sensitive digital ecosystems. One tiny manipulation can shift odds globally
or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle
security — especially the kind you see described in official breakdowns — it opened
my eyes. If anyone wants to understand how this
level of protection actually works, they can always look it up directly
from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal.
I saw databases full of injury histories — things that could ruin a season if
leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had become a
daily threat.
Compliance teams were everywhere too — checking access, reviewing logs,
forcing documentation. I used to think compliance was boring, but now I understand
that without it, the entire digital side of sports would melt into
chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures —
it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole
world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d
definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you
read it, you’ll never look at sports or betting the same way again.
Also visit my webpage :: page
I am curious to find out what blog platform you have been using?
I’m having some minor security problems with my latest
site and I’d like to find something more safeguarded.
Do you have any solutions?
Visit my web site – business for sale
Hey there! Someone in my Facebook group shared this website with us so I came to check it out.
I’m definitely loving the information. I’m book-marking and will be
tweeting this to my followers! Great blog and fantastic design and style.
Here is my web-site; 비아그라 구매
Great post.
Also visit my web site: Guenstige Sexpuppen
I always spent my half an hour to read this website’s articles daily along
with a mug of coffee.
Have a look at my web site … makerealmedia.com
We have something special for you if you enjoy MILFs.nudespics site Our Ebony MILFs are completely different
types of hot. You’ll be amazed at how amazing they are both by their appearance and knowledge.
Perhaps in their solo films, these women never disaster around.
They are confident in their actions and don’t fear to flaunt it.
We also have that in our lineup if you enjoy black-on-black motion. Some powerful views with BBCs and rosy, pink-faced mouth are included in our set.
These MILFs, however, also adore pale penises because they are not simply about ebony wieners.
Interracial activity is evident in our films, consequently be sure to
watch. Don’t care if you don’t like to see douchebags.
Ebony MILFs are also having fun with one another. In their seductive lingerie,
they enjoy using with each other’s systems. https://www.airmp4.com/1.html
We have something special for you if you enjoy MILFs.nudespics site Our Ebony MILFs are completely different types of hot.
You’ll be amazed at how amazing they are both by their appearance and knowledge.
Perhaps in their solo films, these women never
disaster around. They are confident in their actions and don’t fear to flaunt it.
We also have that in our lineup if you enjoy black-on-black motion. Some powerful views with BBCs and rosy, pink-faced mouth are included in our set.
These MILFs, however, also adore pale penises because they are not simply about
ebony wieners. Interracial activity is evident in our films, consequently
be sure to watch. Don’t care if you don’t like to see douchebags.
Ebony MILFs are also having fun with one another.
In their seductive lingerie, they enjoy using with each other’s systems. https://uttarakhandkinews.com/health-secretary-dr-rajesh-kumar-set-out-on-foot-at-ground-zero-to-inspect-health-facilities/
Aw, this was an extremely nice post. Taking a few minutes and actual effort to produce
a really good article… but what can I say… I hesitate a whole lot and never manage to
get nearly anything done.
Have a look at my web blog: Custom Mylar bags
Saved as a favorite, I love your website!
Look at my web blog; mersin temizlik şirketi
I know this web site gives quality depending articles or reviews and other
data, is there any other web site which gives such things
in quality?
Feel free to surf to my webpage; neurodyne
iyy6qq
I didn’t see it coming at all, but the first time I got involved with a professional club’s
digital operations, everything I thought I knew about modern sports
completely collapsed.
I always believed sports were about competition, but when I saw how the entire industry had turned into this massive
digital economy, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — betting infrastructures.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated
data feed caused chaos in betting markets. That was the moment I
understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are insane real-time data engines. One tiny manipulation can shift odds
globally or make entire markets react like they’re
on fire.
When I learned how seriously regulated environments handle security
— especially the kind you see described in official breakdowns
— it opened my eyes. If anyone wants to understand
how this level of protection actually works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases
full of tactical plans — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security
training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to think compliance was boring, but now I understand that without it, the entire digital
side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only
thing holding this whole world together.
And honestly, after everything I saw, I can say the system
I was reviewing really did an exceptional job. They handled
their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting more information directly from
the source. It’s all publicly explained — and believe me,
once you read it, you’ll never look at sports or betting the same
way again.
Here is my web-site; website
I still remember the moment, but the day I stepped into the backend of
the sports world, everything I thought I knew about modern sports completely collapsed.
I always believed the danger was only on the field, but when I saw how the entire industry
had turned into this massive digital economy, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — streaming systems.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a data leak nearly destroyed
a negotiation. That was the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just
websites.
But no.
They are ultra-sensitive digital ecosystems.
One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments
handle security — especially the kind you see
described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of
protection actually works, they can always look it up
directly from the source. The full explanations are
there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of sponsorship deals — things that could
ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs,
forcing documentation. I used to think compliance was boring,
but now I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching
the digital version of an arms race. But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really
did an exceptional job. They handled their mission far better than I
expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once
you read it, you’ll never look at sports or betting the same way again.
my webpage … read more
Hello, I want to subscribe for this webpage to take newest updates, therefore where can i do it please help.
Here is my website … Naga303
คอนเทนต์นี้ อ่านแล้วเข้าใจง่าย ค่ะ
ดิฉัน เพิ่งเจอข้อมูลเกี่ยวกับ หัวข้อที่คล้ายกัน
ที่คุณสามารถดูได้ที่ Charley
ลองแวะไปดู
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Take a look at my blog post :: betflixnew (Charley)
Remarkable things here. I’m very happy to look your post.
Thanks so much and I’m looking forward to contact you.
Will you kindly drop me a e-mail?
Look at my page :: мостбет зеркало
Very energetic post, I loved that bit. Will there be
a part 2?
Also visit my web-site – my website
Hello, i believe that i noticed you visited my site so i got here
to return the desire?.I’m attempting to in finding things to improve my website!I guess its ok to use a few of your ideas!!
Here is my web blog … CLPI file technical details
Remarkable! Its really remarkable post, I have got much clear idea
concerning from this paragraph.
Take a look at my site; Discover More Here
Why users still make use of to read news papers when in this technological world the whole thing is existing on web?
Also visit my blog :: bolso yupoo global
Hi would you mind letting me know which webhost you’re using?
I’ve loaded your blog in 3 completely different internet browsers
and I must say this blog loads a lot quicker then most.
Can you recommend a good internet hosting provider at a fair price?
Cheers, I appreciate it!
Here is my webpage – Компания по монтажу алюминиевых перил на балконах
Awesome article.
Also visit my blog – linkinmarketing.com
I was wondering if you ever thought of changing the structure of your site?
Its very well written; I love what youve got to say. But maybe you could a little more in the way of content so people
could connect with it better. Youve got an awful
lot of text for only having one or two pictures.
Maybe you could space it out better?
Here is my homepage: slot gacor
Wonderful items from you, man. I’ve take note your stuff previous to and you’re just too fantastic.
I really like what you have bought right here, really
like what you are stating and the best way wherein you are saying it.
You’re making it entertaining and you still care for to keep it wise.
I can’t wait to learn far more from you. That is actually a wonderful
site.
Stop by my webpage: porno tubes
25 UNION — это больше, чем женская одежда.
Это элемент стиля, который формирует атмосферу вашего образа.
Продуманный крой, утончённый дизайн и универсальность позволяют вещам легко вписываться в любой гардероб — от повседневного до делового и вечернего.
Качество материалов, практичность и современный характер делают каждую модель
выразительным акцентом образа.
25 UNION — выбор тех, кто ценит стиль, комфорт и
осознанный подход к деталям.
my web-site – https://www.manuelabenzoni.com/the-secret-to-staying-motivated-no-matter-what-you-do/
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get three emails with the same comment. Is there any way you can remove people from that service? Appreciate it!
Great beat ! I would like to apprentice while you amend your site, how can i subscribe for a
blog website? The account helped me a acceptable deal.
I had been tiny bit acquainted of this your broadcast provided bright clear idea
My blog game-plan-marketing.com
i love your blog … Paver Installation Las Vegas …
I’ll never forget this, but the day I stepped into
the backend of the sports world, everything I thought I
knew about modern sports completely collapsed.
I always believed the danger was only on the field, but when I saw how the
entire industry had turned into this multi-layered financial machine, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers”
anymore. They were attacking everything — live match stats.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a data leak nearly destroyed a negotiation. That was the moment
I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are insane real-time data engines. One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind you see described in official breakdowns — it
opened my eyes. If anyone wants to understand how this
level of protection actually works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of injury histories
— things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security
training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access,
reviewing logs, forcing documentation. I used to think compliance was boring, but
now I understand that without it, the entire digital side of
sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures —
it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the
only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing
really did an exceptional job. They handled their mission far
better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest
getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it, you’ll never look at sports
or betting the same way again.
My blog :: this page
Fantastic beat ! I would like to apprentice at the same time as you amend your web site, how could i subscribe for a weblog web site?
The account aided me a acceptable deal. I were a little bit familiar of this your broadcast provided bright transparent concept เบทฟิก888
Salam, bu saytınız çox yaxşı işləyir!
olimpbet
Very great post. I simply stumbled upon your weblog and wanted
to mention that I have truly loved surfing around your weblog posts.
In any case I’ll be subscribing for your feed and I’m hoping you write once more soon!
Have a look at my webpage – web page
Thanks designed for sharing such a good opinion, article is nice, thats why i have read it completely
my homepage – ถ่ายพรีเวดดิ้ง
Primе Secured
3603 N 222nd St, Suite 102,
Elkhorn, ΝE 68022, United States
402-289-4126
Digital View Tools
At this moment I am ready to do my breakfast, when having my breakfast coming again to read other news.
Feel free to visit my web page; bokep pedofil
Its like you read my mind! You seem to know a lot about
this, like you wrote the book in it or something.
I think that you could do with some pics to drive the message home a bit, but instead of that,
this is excellent blog. A fantastic read.
I’ll certainly be back.
Also visit my website – casino Lucky
Hey there, I really enjoy your posts! I’ve been researching more information on gold name necklace and this post
is the best I’ve found. I’m a big fan of personalized jewelry and your perspective
is wonderful. Keep up the great work! Cheers, Larhonda.
I’ve got to be honest, but the moment I started helping
a friend inside a major sports organization,
everything I thought I knew about modern sports completely collapsed.
I always believed sports were about competition, but when I saw how the entire industry had turned into this multi-layered financial machine, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals
weren’t going after “IT servers” anymore. They were
attacking everything — streaming systems. One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a ransomware attack almost froze an entire club.
That was the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting
platforms.
I swear, I always thought they were just websites.
But no.
They are ultra-sensitive digital ecosystems. One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle
security — especially the kind you see described in official
breakdowns — it opened my eyes. If anyone wants to understand
how this level of protection actually works, they can always
look it up directly from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full
of sponsorship deals — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because
phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs,
forcing documentation. I used to think compliance was boring, but now I understand that
without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures —
it felt like watching the digital version of an arms race. But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole
world together.
And honestly, after everything I saw, I can say the system I was reviewing really
did an exceptional job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting more information directly from
the source. It’s all publicly explained — and believe me,
once you read it, you’ll never look at sports or betting the same way again.
Also visit my website site
I still remember the moment, but the first time
I got involved with a professional club’s digital operations, everything I thought I knew about modern sports completely
collapsed.
I always believed sports were about competition,
but when I saw how the entire industry had turned into this fragile high-tech ecosystem, I honestly
felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — contract files. One
breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how
a ransomware attack almost froze an entire club.
That was the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security
— especially the kind you see described in official breakdowns — it opened my
eyes. If anyone wants to understand how this level of protection actually works, they can always look it up directly
from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of biometric performance metrics — things
that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system
can fall apart. I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to think compliance was boring, but now I understand
that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud
architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this
whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did
an exceptional job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it, you’ll never look at
sports or betting the same way again.
Here is my homepage :: website
A Deadly Mistake Uncovered on Seo And How to Avoid It
01032026.seostart.com.ua
What’s up everybody, here every one is sharing such know-how, so it’s fastidious to read this weblog, and I used to go to
see this weblog everyday.
My web-site :: dallas accountant
Hi there to every body, it’s my first go to see of this web site;
this web site carries amazing and actually fine data in support of readers.
my site Recommended Site
I have learn a few just right stuff here. Definitely worth bookmarking for revisiting.
I wonder how so much attempt you place to make this type of great informative site.
Feel free to surf to my homepage – Актуальное зеркало Melbet Casino
fantastic publish, very informative. I wonder why the other specialists of this sector don’t realize this.
You should continue your writing. I am confident, you’ve a great readers’ base already!
Feel free to surf to my webpage … si paling report
Hi there, just became aware of your blog through Google,
and found that it is truly informative. I’m gonna watch out for brussels.
I’ll appreciate if you continue this in future. A lot of people will be benefited from your writing.
Cheers!
Review my webpage; scam website
Hi, every time i used to check web site posts here early in the break of day, since i enjoy to
learn more and more.
My web page; мостбет казино вход
Hello there! I know this is kinda off topic
nevertheless I’d figured I’d ask. Would you be interested in exchanging links or maybe guest authoring a blog
post or vice-versa? My blog discusses a lot of the
same topics as yours and I think we could greatly benefit from each other.
If you happen to be interested feel free to shoot me an email.
I look forward to hearing from you! Terrific blog by the
way!
Take a look at my page; bokep anak smp indonesia
Greetings! I know this is kinda off topic but I’d figured I’d ask.
Would you be interested in trading links or maybe guest writing a blog article or vice-versa?
My website discusses a lot of the same topics as yours and I believe we could greatly benefit from each
other. If you might be interested feel free to send me an email.
I look forward to hearing from you! Great blog by the way!
Have a look at my web-site; ROSH Aesthetic Clinic
What’s up Dear, are you in fact visiting this web page daily, if
so after that you will without doubt take fastidious know-how. https://cryptoboss-rcn.top/
I’ll never forget this, but the day I stepped into the
backend of the sports world, everything I thought I knew about modern sports completely collapsed.
I always believed teams were about winning games, but
when I saw how the entire industry had turned into this fragile high-tech ecosystem,
I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t
going after “IT servers” anymore. They were attacking everything — player data.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a ransomware attack almost froze an entire club.
That was the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally or make entire markets react like they’re
on fire.
When I learned how seriously regulated environments handle security — especially the kind you see described
in official breakdowns — it opened my eyes. If anyone wants to understand
how this level of protection actually works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of tactical
plans — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I
used to think compliance was boring, but now I understand that without it, the entire digital side of
sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures
— it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole
world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how
these structures really work, I’d definitely suggest getting
more information directly from the source. It’s all publicly explained — and believe me, once you read it, you’ll never look
at sports or betting the same way again.
Also visit my blog post … website
My coder is trying to convince me to move to .net from
PHP. I have always disliked the idea because of the expenses.
But he’s tryiong none the less. I’ve been using WordPress on various
websites for about a year and am nervous about switching to another platform.
I have heard great things about blogengine.net. Is there a way I can import all my wordpress content into it?
Any kind of help would be greatly appreciated!
Feel free to surf to my web blog – find out
What’s up, just wanted to tell you, I liked this blog post.
It was inspiring. Keep on posting!
my blog: situs bokep anak kecil
Ꮲrime Secured
3603 N 222nd Տt, Suite 102,
Elkhorn, NE 68022, United Ѕtates
402-289-4126
Active Threat Block
Great post. I used to be checking continuously this blog and I’m impressed!
Extremely helpful info particularly the final phase :
) I take care of such information much. I was seeking
this certain info for a very lengthy time. Thank you and best of
luck.
Have a look at my blog – Монро казино официальный сайт
I’m amazed, I must say. Seldom do I come across
a blog that’s both educative and amusing, and without a doubt, you have
hit the nail on the head. The issue is something that too few men and women are speaking intelligently
about. Now i’m very happy I found this in my hunt for something relating
to this.
My webpage Waktogel
Hello! This is kind of off topic but I need some guidance from an established blog.
Is it difficult to set up your own blog? I’m not very techincal but I
can figure things out pretty fast. I’m thinking about making my own but I’m not
sure where to start. Do you have any tips or suggestions?
Thanks
Here is my web site Read Full Article
Everyone loves what you guys are up too. This sort of clever work
and coverage! Keep up the excellent works guys I’ve added you guys to my
personal blogroll.
Also visit my blog … Loeb Smith Reviews
Bu kontentə görə təşəkkürlər. Saytı dostlarıma tövsiyə edəcəyəm.
https://sobaki.derev-grad.ru/bitrix/redirect.php?goto=https%3A%2F%2Fmostbet-azerbaijan-club.com
Prime Secured
3603 N 222nd Ꮪt, Suite 102,
Elkhorn, ΝE 68022, United States
402-289-4126
Tailored cybersecurity solutions – padlet.com,
Dizaynı çox bəyənirəm!
Mostbet sayt
Pretty section of content. I just stumbled upon your web
site and in accession capital to assert that I acquire actually enjoyed account your blog posts.
Any way I’ll be subscribing to your augment and even I achievement you access consistently rapidly.
my webpage … unblocked games
I didn’t see it coming at all, but the first time I got involved with a
professional club’s digital operations, everything I thought I knew about modern sports
completely collapsed.
I always believed the danger was only on the field, but when I saw
how the entire industry had turned into this massive digital
economy, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t
going after “IT servers” anymore. They were attacking everything — contract files.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a data leak nearly
destroyed a negotiation. That was the moment I understood how
thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting
platforms.
I swear, I always thought they were just websites.
But no.
They are ultra-sensitive digital ecosystems. One tiny manipulation can shift odds globally or make entire markets
react like they’re on fire.
When I learned how seriously regulated environments handle
security — especially the kind you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they can always look it
up directly from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of transfer negotiations —
things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing
had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I
used to think compliance was boring, but now I understand that without it,
the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this
whole world together.
And honestly, after everything I saw, I can say the system I was reviewing
really did an exceptional job. They handled their mission far better
than I expected.
If anyone wants to dig deeper or understand how these structures
really work, I’d definitely suggest getting more information directly from the
source. It’s all publicly explained — and believe me,
once you read it, you’ll never look at sports or betting the same
way again.
Review my site … url
I think everything posted made a great deal of sense. But, what about this?
suppose you wrote a catchier post title? I am not suggesting your content is not solid., but
suppose you added a post title that makes people desire more?
I mean Heel Pain – Plantar Fasciitis – Mr Will Edwards is
kinda vanilla. You might peek at Yahoo’s home page and see how
they create post headlines to get viewers to click.
You might try adding a video or a pic or two to get people excited about what you’ve got to say.
In my opinion, it would bring your posts a little bit more interesting.
Also visit my web page: récompenses alexander casino
May I just say what a relief to discover somebody that really knows what they are discussing online.
You definitely understand how to bring an issue to
light and make it important. More and more people have to read this and understand this side of the story.
I can’t believe you aren’t more popular because you certainly have the gift.
Feel free to visit my site: Read Full Report
Carbon confidence markets are platforms where carbon credits
are bought and sold, enabling companies and countries to up their carbon dioxide emissions.
Each probity represents a metric ton of carbon dioxide that
has been either reduced or removed from the atmosphere.
The ideal of these markets is to accord
My web blog: https://www.mangwanani.co.za/understanding-the-carbon-credit-market-a-step-by/
Thanks very interesting blog!
Also visit my webpage :: web site
Oferiți informații informative despre strategii de joc.
pariuri Verde
Spot on with this write-up, I actually believe this website needs a great deal more attention. I’ll probably be back again to
read through more, thanks for the info! https://de.chatruletka-18.com/
I’ll never forget this, but the first
time I got involved with a professional club’s digital
operations, everything I thought I knew about
modern sports completely collapsed.
I always believed the danger was only on the field, but when I saw
how the entire industry had turned into this fragile high-tech ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t
going after “IT servers” anymore. They were attacking everything — betting infrastructures.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated
data feed caused chaos in betting markets. That was the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are insane real-time data engines. One tiny manipulation can shift odds globally or make entire
markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind you see described in official breakdowns —
it opened my eyes. If anyone wants to understand how this level
of protection actually works, they can always look it
up directly from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of transfer negotiations — things that could ruin a season if
leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had become
a daily threat.
Compliance teams were everywhere too — checking access, reviewing
logs, forcing documentation. I used to think compliance was boring, but now I understand that without it, the entire
digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like
watching the digital version of an arms race. But the truth I
walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how
these structures really work, I’d definitely
suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it, you’ll never look at sports or betting the same way again.
Here is my homepage – page
my web-site: bookmaker hors arjel france
모든 사람에게 안녕하세요, 저는 이
웹사이트의 포스트를 정기적으로 읽는 데 실제로 열심입니다.
멋진 자료를 포함하고 있습니다.
Good way of telling, and pleasant paragraph to get facts about my presentation topic, which i
am going to deliver in school.
Feel free to surf to my web page: 비아그라 약국
Hmm it seems like your site ate my first comment (it was super long) so
I guess I’ll just sum it up what I submitted and say, I’m thoroughly enjoying your blog.
I too am an aspiring blog writer but I’m still new to everything.
Do you have any helpful hints for newbie blog writers?
I’d definitely appreciate it.
Also visit my homepage :: Medical Center ROSH
It’s an awesome piece of writing in favor of all the online viewers; they will get benefit from
it I am sure.
Look at my web-site; relevant
Как производится качественный восстановление автомобиля
My blog post :: https://turistavto.ru/remont-akpp-ford-kak-provoditsya/
I still remember the moment, but the day I stepped into the backend of the
sports world, everything I thought I knew about modern sports completely collapsed.
I always believed sports were about competition, but
when I saw how the entire industry had turned into
this fragile high-tech ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers”
anymore. They were attacking everything — betting infrastructures.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how
a manipulated data feed caused chaos in betting markets.
That was the moment I understood how thin the line really is between order and total
digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally or
make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind you
see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they can always look
it up directly from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of injury
histories — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole
system can fall apart. I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to
think compliance was boring, but now I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing
holding this whole world together.
And honestly, after everything I saw, I can say the system I was
reviewing really did an exceptional job. They handled their
mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest
getting more information directly from the source.
It’s all publicly explained — and believe me, once you
read it, you’ll never look at sports or betting the same way again.
Here is my web site page
Thank you for any other fantastic article.
Where else could anybody get that kind of
information in such a perfect manner of writing?
I’ve a presentation subsequent week, and I’m at the search for such info.
My web-site – spelaonlinebingo.com
Продолжайте в том же духе и привлекайте ещё больше игроков!
платформа Olimp Casino
Wonderful article! We are linking to this great post on our website.
Keep up the good writing.
Also visit my web site: bk8thai
Honestly, this whole situation still feels unbelievable telling this story today.
Not long ago, I got obsessed in online games – Valorant.
I wanted to dominate, and I kept searching for shortcuts everywhere.
Late one night, I stumbled across a forum thread talking about cheats.
At first I just read out of curiosity, but the more screenshots I saw, the more
it felt like a secret world.
Commenters were flexing showing how they climbed from
low ranks to high ones in days. It looked effortless.
And of course, none of it was real.
I won’t lie, I actually got close to buying something.
One seller even messaged me privately. That’s when it
hit me.
I found threads from players who lost their accounts. Some even wrote how their PCs got infected.
That was my wake-up call.
Instead of throwing everything away, I walked away and focused
on improving the legitimate way.
Now, when I see people chasing cheats, I just think: the crash always comes.
Just learn from my almost-mistake.
Feel free to surf to my site :: information
I feel this is among the so much significant info for me.
And i’m happy studying your article. But should commentary
on some basic issues, The website style is great, the articles is
in point of fact nice : D. Excellent task, cheers
Look into my web blog … murad salikhov
Thank you for that wonderfully informative explanation—it made everything much clearer, and whenever carpet cleaning is needed, AJS Carpet Cleaning is a fantastic option, maintaining industry-recognized training standards and ensuring every team
member is skilled in different cleaning approaches;
despite no specific certifications being named, they prioritize ongoing education and updated
industry techniques which helps reduce retakes, enabling them to
offer exceptional service every time.
Also visit my page: Rug cleaning
Good post. I learn something new and challenging on websites I stumbleupon every day.
It’s always useful to read through articles from other writers and practice
a little something from their sites.
My web page: hacking money user
Appreciate the recommendation. Let me try it out.
Also visit my blog … Buy CBD Oil In Jeddah
CS2 Gambling Overview
Here is my homepage … https://judicialpowerproject.org.uk/pages/comparing-cs2-gambling-to-traditional-online-casinos.html
Wow, superb weblog structure! How long have you ever been running a blog for?
you made blogging glance easy. The overall look of your web site is wonderful,
as neatly as the content material!
Feel free to surf to my web site: kiomet
Hi there to all, how is all, I think every one is getting more from this website, and your views are fastidious designed for new users.
my webpage; Winna Casino
I’ll right away grab your rss as I can not to find your e-mail subscription link or e-newsletter
service. Do you have any? Please let me realize so
that I may subscribe. Thanks.
Here is my blog; nomnom-media.com
Hello! I simply wish to give you a huge thumbs up for the great
info you’ve got right here on this post.
I’ll be returning to your web site for more soon.
Also visit my blog post; murad salikhov
Quality articles or reviews is the main to be a focus for
the visitors to pay a quick visit the site, that’s what this website
is providing.
Also visit my webpage – davinci gold casino
Искривление позвоночника можно контролировать и корректировать при правильной реабилитации.
Специальные лечебные упражнения, работа над симметрией тела
и укрепление глубоких мышц помогают снизить нагрузку на позвоночник и улучшить самочувствие.
Постепенная и безопасная коррекция позволяет вернуть уверенность в движениях, ровную осанку и активный образ жизни без постоянного
дискомфорта.
Look into my web-site … https://wiki.mubk.top/index.php?title=User:ReggieOgles3
Ꮲrime Secured
3603 N 222nd Ꮪt, Suite 102,
Elkhorn, ⲚE 68022, United States
402-289-4126
Innovative Risk Solutions
Now I am going away to do my breakfast, once having my breakfast coming yet again to read more news.
My page :: mostbet casino
Yes! Finally something about minervamail.com.
Правильная реабилитация — ключ к полноценному восстановлению после болезни
или травмы. Комплекс лечебных упражнений, укрепление мышц и тренировка
баланса помогают улучшить подвижность и предотвратить повторные проблемы.
Системный подход и профессиональное сопровождение обеспечивают устойчивый результат
и комфорт в повседневной активности.
My website: https://www.arenagames.us/index.php?title=User:ShermanMurch057
Для комплексного подхода можно заказать прогон хрумером https://www.olx.ua/d/uk/obyavlenie/progon-hrumerom-dr-50-po-ahrefs-uvelichu-reyting-domena-IDXnHrG.html у профессионалов в этой сфере.
I am genuinely thankful to the holder of this web page who
has shared this impressive piece of writing at at this time.
Have a look at my site :: pharmacy online
Hi, i think that i saw you visited my blog thus
i came to “return the favor”.I am attempting to find things to enhance my site!I suppose its ok to use
some of your ideas!!
Here is my web blog … مراهنات كاس العالم
Hello! I know this is somewhat off-topic however I
needed to ask. Does operating a well-established website such
as yours require a massive amount work? I am brand new to blogging but I do write in my journal everyday.
I’d like to start a blog so I will be able to
share my experience and feelings online. Please
let me know if you have any suggestions or tips for new aspiring blog owners.
Appreciate it!
Also visit my website 드퀘르벵 손목건초염
Hey just wanted to give you a quick heads up.
The words in your post seem to be running off the screen in Ie.
I’m not sure if this is a format issue or something to do with internet browser compatibility but I
figured I’d post to let you know. The design and style look great though!
Hope you get the problem resolved soon. Cheers
Feel free to visit my site – ฮานอยปกติ
Правильное восстановление —
ключ к полноценной жизни после болезни или травмы.
Программа физической реабилитации включает лечебную физкультуру, укрепление мышц и работу над балансом.
Системные занятия помогают вернуть утраченные функции, улучшить самочувствие и предотвратить повторные проблемы.
Сделайте шаг к свободе движения
уже сегодня.
Feel free to surf to my web site https://www.torikorestaurant.ch/produit/toriko-signature/
I simply could not go away your site before suggesting that I extremely loved the
standard info an individual supply for your guests?
Is gonna be back steadily to check out new posts
Here is my website: situs bokep jepang
Looking back now, it feels surreal yet this is exactly where life took me.
Back when the new competitive season started, I got obsessed in online games – Dota 2.
I wanted to climb ranks fast, and I kept searching for shortcuts
everywhere.
Late one night, I stumbled across a forum thread talking about cheats.
At first I just read out of curiosity, but the more screenshots I saw, the more it felt
like a tempting escape.
Users were posting clips showing how they climbed from low ranks
to high ones in days. It looked effortless.
And of course, none of it was real.
Truth be told, I actually got close to buying something.
One seller even messaged me privately. That’s when the
real consequences showed up.
I found threads from players who lost thousands of hours of progress.
Some even wrote how their bank info got stolen. The shock snapped
me out of it.
Instead of taking that dumb risk, I deleted the messages and focused on improving the legitimate way.
Now, when I see people chasing cheats, I just think:
it’s never worth it. If you’re reading this, take my experience seriously.
Look at my web page media article
I think this is among the most significant information for me.
And i’m glad reading your article. But should remark on few general things, The website style is perfect, the articles is really
excellent : D. Good job, cheers
Here is my homepage – bath remodelling
Happy to be here this platform.
I’m mainly interested in iGaming platforms and discovering reliable sites.
Lately, I’ve been spending time on Betify Casino because of
its fast games.
Here to learn and share useful info about the iGaming world.
My webpage … Uncrossable Rush
This post is invaluable. When can I find out more?
Feel free to visit my blog post – Buy Umbrella Cockatoo Online In Australia
My partner and I stumbled over here different website and thought I should check
things out. I like what I see so now i am following you.
Look forward to finding out about your web page for a second time.
My homepage … мостбет зеркало
I didn’t see it coming at all, but the first time I got involved with a professional club’s digital operations, everything I thought
I knew about modern sports completely collapsed.
I always believed teams were about winning games, but when I saw how the entire
industry had turned into this fragile high-tech
ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers”
anymore. They were attacking everything — live match stats.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a data
leak nearly destroyed a negotiation. That was the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines.
One tiny manipulation can shift odds globally or make entire markets react
like they’re on fire.
When I learned how seriously regulated environments handle security —
especially the kind you see described in official breakdowns
— it opened my eyes. If anyone wants to understand how this level of protection actually works,
they can always look it up directly from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of transfer negotiations
— things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall
apart. I watched entire staff units go through security training because phishing
had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing
logs, forcing documentation. I used to think compliance was boring,
but now I understand that without it, the entire digital side of
sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I
expected.
If anyone wants to dig deeper or understand how
these structures really work, I’d definitely suggest getting more
information directly from the source. It’s all publicly explained
— and believe me, once you read it, you’ll never look at sports or
betting the same way again.
my homepage – this url
It’s very easy to find out any topic on net as compared to books, as I found this article at this web page.
my web page :: situs bokep jepang
Honestly, this whole situation still feels unbelievable telling this story today.
Back when the new competitive season started, I got way too invested in online games – Dota 2.
I wanted to climb ranks fast, and I kept searching
for shortcuts everywhere.
After another frustrating match, I stumbled across a forum thread talking about “boosting
tools”. At first I just read out of curiosity, but the more I scrolled,
the more it felt like a tempting escape.
People were bragging showing how they climbed from low ranks to high ones in days.
It looked like magic. And of course, it was too good
to be true.
Truth be told, I actually got close to buying something.
One guy tried to explain the “features” to me.
That’s when the real consequences showed up.
I found threads from players who got hardware bans. Some even wrote how
they couldn’t undo the damage. Everything clicked.
Instead of throwing everything away, I walked away and focused on improving the legitimate way.
Now, when I see people chasing cheats, I just think: it’s never worth it.
If you’re reading this, take my experience seriously.
My webpage press article
Currently it sounds like Drupal is the top blogging platform out there right now.
(from what I’ve read) Is that what You actually} mentioned‘re using on your blog?
I still remember the moment, but the moment I started helping a friend inside a major sports
organization, everything I thought I knew about modern sports completely collapsed.
I always believed sports were about competition, but when I saw how
the entire industry had turned into this fragile high-tech ecosystem,
I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after
“IT servers” anymore. They were attacking everything
— player data. One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a ransomware attack almost froze an entire club.
That was the moment I understood how thin the line really is between order and total
digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are insane real-time data engines. One tiny manipulation can shift
odds globally or make entire markets react like they’re
on fire.
When I learned how seriously regulated environments handle security — especially the kind you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they can always look it up directly
from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of injury
histories — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training
because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs,
forcing documentation. I used to think compliance was boring, but now
I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital
version of an arms race. But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole
world together.
And honestly, after everything I saw, I can say the system I was reviewing
really did an exceptional job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting
more information directly from the source. It’s all publicly explained —
and believe me, once you read it, you’ll never look at sports or betting the same way again.
Also visit my blog post – this URL
This post offers clear idea in favor of the new visitors
of blogging, that really how to do blogging.
Also visit my web blog :: online order medicine
이건 정말 흥미롭고 것입니다, 당신은 너무 숙련된 블로거입니다.
당신의 RSS 피드에 가입했고, 당신의 멋진 포스트를 더 찾고 있습니다.
또한, 제 소셜 네트워크에서 당신의 웹사이트를 공유했습니다.
You could definitely see your expertise in the work you write.
The sector hopes for even more passionate writers such as you who aren’t afraid to say how they believe.
At all times go after your heart.
my blog post – 비아그라 구매
Wow, wonderful blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your web site
is wonderful, as well as the content!
Check out my web-site; anal sex porn videos xxx sites
Looking back now, it feels surreal yet this is exactly where life took me.
Back when the new competitive season started, I got totally consumed in online games – other competitive titles.
I wanted instant results, and I wasn’t willing to admit how impatient I had become.
Late one night, I stumbled across a forum thread talking about cheats.
At first it was harmless reading, but the more I scrolled,
the more it felt like a tempting escape.
Users were posting clips showing how they climbed from low ranks to high ones in days.
It looked effortless. And of course, the downside was completely hidden.
I won’t lie, I actually got close to buying something.
One guy tried to explain the “features” to me. That’s when things turned
dark.
I found threads from players who got hardware bans.
Some even wrote how their bank info got stolen. Everything
clicked.
Instead of taking that dumb risk, I deleted the messages and focused on improving
the legitimate way.
Now, when I see people chasing cheats, I just think: it’s never worth it.
Just learn from my almost-mistake.
Feel free to visit my blog post: press release
I’ll never forget this, but the day I stepped into the backend of
the sports world, everything I thought I knew about modern sports completely
collapsed.
I always believed teams were about winning
games, but when I saw how the entire industry had turned into this fragile high-tech ecosystem,
I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — live match stats. One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated data feed caused chaos in betting markets.
That was the moment I understood how thin the line really is between order and total
digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are ultra-sensitive digital ecosystems. One tiny manipulation can shift odds globally or make
entire markets react like they’re on fire.
When I learned how seriously regulated environments
handle security — especially the kind you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually
works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of sponsorship deals — things that could
ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to think compliance was boring,
but now I understand that without it, the entire digital side
of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures
— it felt like watching the digital version of an arms
race. But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world
together.
And honestly, after everything I saw, I can say the system I was reviewing really did
an exceptional job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures
really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it,
you’ll never look at sports or betting the same way again.
Полиуретановые полиуретановые сайлентблоки Полиуретановые резинометаллические элементы
Fine way of telling, and nice post to take information about my presentation topic,
which i am going to deliver in university.
Feel free to surf to my website Thanks
Hey There. I found your blog using msn. This is a very well written article.
I’ll make sure to bookmark it and return to read more
of your useful info. Thanks for the post. I’ll certainly comeback.
Here is my web site … spiritual warfare
Have you ever thought about including a little bit
more than just your articles? I mean, what you say is fundamental
and all. Nevertheless think of if you added some great images or videos
to give your posts more, “pop”! Your content is excellent but
with images and video clips, this blog could undeniably be one of the greatest in its field.
Very good blog!
Also visit my website slot gacor
ดูบอลสด MoveFreeThailand เว็บดูทีวีออนไลน์ ดูบอลออนไลน์ ดูกีฬาออนไลน์ ทางพวกเราได้เก็บรวบรวม
ช่องดูบอล ช่องดิจิตอลทีวี ช่องกีฬาต่างประเทศ
ให้ท่านได้รับดูแบบไม่เสียค่าใช้จ่าย ไม่มีโฆษณาให้รบกวนใจ
พวกเรามีช่องกีฬาชั้นนำอีกทั้งไทยรวมทั้งต่างแดน เช่น True Permier Football , Bein Sport , True Sport , SPOTV , ดิจิตอลทีวี รวมทั้งฯลฯ
ดูบอล ดูบอลสด ดูบอลออนไลน์ ดูบอลผ่านเน็ต ดูทีวี ดูทีวีออนไลน์ ตารางบอล ผลบอล บอลวันนี้
Check out my website – ดูบอลออนไลน์ฟรี
When someone writes an article he/she retains the image of a user in his/her brain that how a user can know it.
So that’s why this article is great. Thanks!
Feel free to visit my web blog; อาหารคลีนไม่ใส่น้ำมัน
It is really a great and helpful piece of info. I am happy that you just
shared this helpful info with us. Please stay us informed like this.
Thank you for sharing.
Feel free to visit my web site – medicine online shopping
If some one needs to be updated with most up-to-date technologies therefore he must
be go to see this website and be up to date daily.
My web page :: link gacor
Wow, awesome weblog format! How long have you ever been blogging for?
you make blogging glance easy. The overall glance of your web site is wonderful,
as smartly as the content!
Also visit my web-site … online medicine to buy
Hello I am so delighted I found your blog, I really
found you by error, while I was browsing on Bing for something else, Regardless
I am here now and would just like to say many thanks for a
remarkable post and a all round thrilling blog
(I also love the theme/design), I don’t have time to go through it all at the moment but
I have bookmarked it and also added in your RSS
feeds, so when I have time I will be back to read much more, Please do keep up the great work.
Here is my web-site canadian pharmacies online
Very good post. I absolutely love this site. Keep it up!
Feel free to surf to my webpage – Lost Boy Entertainment
It’s actually a nice and useful piece of info.
I am happy that you simply shared this useful information with us.
Please keep us informed like this. Thanks for sharing.
Visit my web-site – vanity wallet
Super platformadır! Uğurlar!
Pinco Casino resmi sayt
Do you mind if I quote a couple of your posts as
long as I provide credit and sources back to your weblog?
My blog site is in the exact same area of interest as yours and my users
would truly benefit from some of the information you
provide here. Please let me know if this ok with you.
Appreciate it!
my web blog: cartão de visita profissional
It’s fantastic that you are getting thoughts from this article as well
as from our argument made at this place.
Also visit my website: best viagra for women
I’d like to thank you for the efforts you’ve put in penning this website.
I really hope to view the same high-grade content by
you later on as well. In fact, your creative writing abilities has inspired me to get my own, personal blog now ;)
My web page Regards
What’s up colleagues, how is all, and what you wish for to say concerning this piece of writing,
in my view its actually awesome designed for me.
Feel free to surf to my web site: 2 х комнатная квартира варианты ремонта
What’s up, just wanted to mention, I loved this post. It was helpful.
Keep on posting!
Here is my page hey
Great blog you have here.. It’s hard to find good quality writing like yours nowadays.
I seriously appreciate people like you! Take care!!
My page; Data HK Lotto
I do not even know how I ended up here, but
I thought this post was good. I don’t know who you are but
definitely you are going to a famous blogger if
you aren’t already ;) Cheers!
Feel free to surf to my web site :: pharmacies
What’s up, just wanted to mention, I loved this article.
It was inspiring. Keep on posting!
Here is my website premium airport transfer KLIA Alphard
โพสต์นี้ น่าสนใจดี ค่ะ
ดิฉัน ไปอ่านเพิ่มเติมเกี่ยวกับ หัวข้อที่คล้ายกัน
ซึ่งอยู่ที่ Bradly
เผื่อใครสนใจ
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
และอยากเห็นบทความดีๆ แบบนี้อีก
Feel free to visit my blog betflik hero (Bradly)
Greetings I am so thrilled I found your website, I really
found you by accident, while I was researching on Yahoo for something else, Nonetheless
I am here now and would just like to say cheers for a fantastic post and a all
round enjoyable blog (I also love the theme/design), I don’t have time to
browse it all at the minute but I have book-marked it and
also added your RSS feeds, so when I have time I will be back to read much more, Please do keep up the great jo.
Here is my blog ремонт четырехкомнатной квартиры москва
โพสต์นี้ ให้ข้อมูลดี ค่ะ
ดิฉัน เพิ่งเจอข้อมูลเกี่ยวกับ หัวข้อที่คล้ายกัน
ดูต่อได้ที่ asia999
สำหรับใครกำลังหาเนื้อหาแบบนี้
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
My programmer is trying to persuade me to move to .net from PHP.
I have always disliked the idea because of the costs. But he’s
tryiong none the less. I’ve been using WordPress on numerous websites for about a year and am concerned about switching to another platform.
I have heard good things about blogengine.net. Is there a way
I can transfer all my wordpress posts into it?
Any kind of help would be greatly appreciated!
Also visit my page kasyno ice
Mangelsen
7916 Girard Avenue, La Joya
СA 92037, United States
1 800-228-9686
Bookmarks (http://www.protopage.com)
Hi my family member! I wish to say that this article is
awesome, nice written and include almost all vital
infos. I would like to see more posts like this .
Feel free to visit my homepage – nnxn
Currently it sounds like Drupal is the preferred blogging platform available right now.
(from what I’ve read) Is that what you’re using on your blog?
my homepage … cashnow.imweb.me
เนื้อหานี้ อ่านแล้วได้ความรู้เพิ่ม ครับ
ผม ได้อ่านบทความที่เกี่ยวข้องกับ เนื้อหาในแนวเดียวกัน
สามารถอ่านได้ที่ ask4win
ลองแวะไปดู
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
ytfa5y
I do believe all of the ideas you’ve introduced for your post.
They are very convincing and can definitely work. Nonetheless,
the posts are too quick for newbies. May just you please prolong them a little from subsequent time?
Thanks for the post.
Feel free to surf to my web-site bandar togel online
Hi there, just became aware of your blog through Google, and found that it’s really informative.
I’m going to watch out for brussels. I’ll appreciate if you
continue this in future. Many people will be benefited from your writing.
Cheers!
Feel free to surf to my site; онлайн казино flagman
Fantastic beat ! I wish to apprentice while you amend your web site,
how could i subscribe for a blog website? The account aided me a acceptable deal.
I had been a little bit acquainted of this your broadcast provided
bright clear idea
Feel free to surf to my site :: Dewagg Agen Situs Bola
Thank you for the good writeup. It in fact was a amusement
account it. Look advanced to more added agreeable from you!
By the way, how can we communicate?
Feel free to visit my homepage … 시알리스처방
each time i used to read smaller articles or reviews that as well clear their motive, and that is also
happening with this post which I am reading at this place.
My webpage: This Site
Everything published was very logical. However, what
about this? suppose you added a little information? I mean, I don’t want to tell you how to
run your website, however what if you added a post title
that grabbed a person’s attention? I mean Heel Pain – Plantar
Fasciitis – Mr Will Edwards is a little
boring. You might glance at Yahoo’s front page and see how
they create post headlines to get people to open the links.
You might try adding a video or a related pic or two to grab readers excited about everything’ve written. In my opinion,
it would bring your website a little livelier.
Feel free to surf to my web blog onlinecasinosusa.org
2ygvfe
Spot on with this write-up, I seriously feel this site needs a lot
more attention. I’ll probably be returning to read more, thanks for the
information!
My webpage: Glasschiebetür innen
Howdy would you mind stating which blog platform you’re working
with? I’m going to start my own blog soon but I’m having
a hard time making a decision between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design seems different then most blogs and I’m looking for something
unique. P.S My apologies for being off-topic but I had to ask!
Also visit my page … 정품 시알리스
If some one desires expert view about blogging afterward i propose him/her to
go to see this web site, Keep up the nice job.
Have a look at my blog; gmnc london
I got this web page from my friend who informed me concerning
this site and at the moment this time I am visiting this site and reading very informative content at this time. https://www.imzakampanyasi.net/512753
Sweet website, super layout, very clean and
employ pleasant.
Also visit my web blog Kkpoker Mod Apk
I was pretty pleased to find this great site.
I wanted to thank you for your time for this fantastic
read!! I definitely really liked every bit of it and I have you book-marked to check out new things on your site.
my web page; MALWARE
Having read this I thought it was extremely informative.
I appreciate you finding the time and energy to put this content
together. I once again find myself spending way too much time both reading and commenting.
But so what, it was still worth it!
Also visit my webpage … 신용카드 현금화
This is very interesting, You’re a very skilled blogger.
I’ve joined your feed and look forward to seeking more of your magnificent post.
Also, I have shared your website in my social networks!
Take a look at my page; mgmarket
When I initially commented I clicked the “Notify me when new comments are added”
checkbox and now each time a comment is added I get
four e-mails with the same comment. Is there any way you can remove me from that service?
Appreciate it!
my webpage – кракен переходник ссылка
Wow, this post is fastidious, my younger sister is analyzing these
kinds of things, therefore I am going to let know her. http://bwiki.dirkmeyer.info/index.php?title=Benutzer:LucieEather7645
I was suggested this website via my cousin. I am no longer sure whether
or not this submit is written via him as nobody else recognize such specified approximately my problem.
You are amazing! Thank you!
Look at my page; Link building service
Fantastic blog! Do you have any recommendations for aspiring writers?
I’m hoping to start my own site soon but I’m a little lost on everything.
Would you advise starting with a free platform like WordPress or
go for a paid option? There are so many choices out there that
I’m completely overwhelmed .. Any recommendations?
Many thanks!
Also visit my page – Eu9 Login
Can I simply say what a relief to discover somebody who genuinely knows what they are talking about online.
You actually understand how to bring an issue to light and
make it important. More and more people must read this and understand this side of your story.
It’s surprising you’re not more popular since you surely have the gift.
my page: social networks
This post is truly a fastidious one it assists new the web viewers, who are
wishing in favor of blogging.
Here is my site: Live Draw Hk
I take pleasure in, lead to I found just what I
was looking for. You’ve ended my four day long hunt! God Bless you man. Have a great day.
Bye
my site – slot pepek
I have learn some excellent stuff here. Certainly worth
bookmarking for revisiting. I surprise how much attempt you set to create one of these fantastic informative site.
Visit my website … bokep cina
Hello would you mind stating which blog platform you’re using?
I’m going to start my own blog soon but I’m having a difficult time making a decision between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design and style seems different then most blogs and I’m looking for something unique.
P.S Sorry for being off-topic but I had to ask!
Also visit my web page :: internet rápida americana
Thanks for your marvelous posting! I quite enjoyed reading it, you’re a great author.I will be
sure to bookmark your blog and will come back later
on. I want to encourage that you continue your great posts, have a nice morning!
Also visit my web-site :: Wongtoto
Hi there colleagues, good post and fastidious arguments commented at this place,
I am really enjoying by these.
my blog post; سكربت الطيارة 1xbet
Thanks for another informative blog. The place else may
just I get that type of information written in such a perfect way?
I’ve a challenge that I am simply now working on, and I’ve been at the glance out for such information.
my web page :: nứng lồn
Hello, I think your website might be having browser compatibility issues.
When I look at your blog site in Chrome, it looks fine but when opening in Internet Explorer, it has some overlapping.
I just wanted to give you a quick heads up!
Other then that, superb blog!
Also visit my web site – bocoran slot gacor malam ini
I read this paragraph completely concerning the difference of most up-to-date and previous technologies, it’s remarkable article.
Take a look at my site: Congtogel
As the admin of this web site is working, no question very soon it will be well-known, due to its feature contents.
Feel free to surf to my blog post: Murchison Falls tour packages
Just desire to say your article is as surprising. The clarity in your post is
simply cool and i can assume you are an expert on this subject.
Fine with your permission allow me to grab your feed to keep updated with
forthcoming post. Thanks a million and please keep up the gratifying work.
Also visit my blog post … เช็คคดี
If some one wishes to be updated with newest technologies afterward
he must be pay a visit this web page and be
up to date all the time.
Also visit my web page :: Poker88
Good information. Lucky me I discovered your blog by accident (stumbleupon).
I’ve book-marked it for later!
Here is my web blog … azino777
Incredible quest there. What occurred after? Thanks!
Also visit my page … bokep
Everyone loves it whenever people get together and share
thoughts. Great website, stick with it!
Feel free to visit my homepage; side hustles (http://www.daraz.pk)
Incredible! This blog looks exactly like my old one!
It’s on a entirely different topic but it has pretty much the same page layout and design.
Excellent choice of colors!
Here is my web-site – Let’s Jackpot Casino Avis (Lenore)
With havin so much content and articles do you ever run into any issues of plagorism or copyright
infringement? My website has a lot of unique content I’ve either authored myself or outsourced but it seems a lot
of it is popping it up all over the internet without my permission. Do you know any ways to help reduce content from being stolen? I’d certainly appreciate
it.
my web-site florida lizards
I’m gone to convey my little brother, that
he should also visit this website on regular basis to get updated from most
recent reports.
my homepage: massage
Its such as you learn my thoughts! You seem to understand a lot
about this, like you wrote the guide in it or something.
I feel that you could do with a few percent to power
the message home a little bit, however instead of that, this is magnificent
blog. A fantastic read. I will definitely be back.
Feel free to visit my web page … indonesia bokep terbaru
I every time spent my half an hour to read this web
site’s articles or reviews every day along with a mug of coffee.
Also visit my webpage: canadian pharmacy
These are in fact enormous ideas in on the topic of blogging.
You have touched some nice factors here.
Any way keep up wrinting.
Feel free to surf to my blog: แทงบอลโลก 2026
Greetings! Very useful advice within this article!
It is the little changes which will make the most significant changes.
Thanks a lot for sharing!
Have a look at my web site; คาสิโนออนไลน์
Hello, the wһole thing is going perfeⅽtly
here and ofcourse every one is sharing data, that’s actually
good, keep սp writing.
Feel free to visit my website spyphone
Great goods from you, man. I’ve understand your stuff previous to and you are just too excellent.
I actually like what you’ve acquired here, certainly like what you’re saying and the way in which you say it.
You make it enjoyable and you still take care of to keep
it sensible. I can not wait to read much more from you. This is really a tremendous website.
My web page 美洽下载
Hello i am kavin, its my first time to commenting anyplace, when i read
this piece of writing i thought i could also make comment due to this good
paragraph.
Have a look at my homepage – Dewalive
Paylaşdığınız məlumatlar mənə çox kömək edir.
Təşəkkürlər!
Pin Up Casino oynamaq
Hi! I just wanted to ask if you ever have any problems with hackers?
My last blog (wordpress) was hacked and I ended up losing months
of hard work due to no data backup. Do you have any solutions to stop hackers?
my webpage คาสิโนออนไลน์
This is a topic which is near to my heart… Thank you!
Exactly where are your contact details though?
My web site – QuickBooks 24/7 Technical Support Boston
I don’t even know how I finished up here, but I assumed this
put up was great. I do not realize who you are but certainly you’re going to
a well-known blogger if you happen to are not already. Cheers!
Feel free to visit my blog – mega2ooyov5nrf42ld7gnbsurg2rgmxn2xkxj5datwzv3qy5pk3p57qd.onion
It’s amazing to visit this web page and reading the views of
all mates on the topic of this piece of writing, while I am also keen of getting
familiarity.
my web blog; GZIP file recovery
I got this web site from my buddy who informed me about this web site
and now this time I am visiting this website and reading very informative content here.
Feel free to visit my page: หมูกระทะกรุงเทพฯ
Ən faydalı platformadır. Yenə baxacağam!
sayta
Jungle Drivinhg School Omaha
4020 S 147tһ St, Omaha,
NE 68137, United States
14024170547
Bookmarks
My partner and I absolutely love your blog and find many of your post’s to be just what I’m
looking for. can you offer guest writers to write content for yourself?
I wouldn’t mind producing a post or elaborating on a lot of the subjects you write
with regards to here. Again, awesome weblog!
my homepage :: ремонт стиральных машин индезит
kkburn
Your style is very unique compared to other folks I have read
stuff from. Thanks for posting when you have
the opportunity, Guess I will just book mark this site. https://cryptoboss990.top
Stay informed about reliable platforms where traders sell bitcoin in india.
บทความนี้ อ่านแล้วเพลินและได้สาระ ค่ะ
ผม ไปเจอรายละเอียดของ หัวข้อที่คล้ายกัน
สามารถอ่านได้ที่ Marietta
น่าจะถูกใจใครหลายคน
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Here is my blog post – kingslot (Marietta)
I was suggested this website by my cousin. I’m not sure whether this post is written by him as nobody else
know such detailed about my problem. You’re wonderful!
Thanks!
Also visit my web-site :: cipit88
Surf holiday packages in Morocco offer a unique blend of
sport, travel, and cultural discovery. Located along the Atlantic coast,
these packages provide access to some of the region’s best
waves. Most programs include comfortable accommodation,
guided surf sessions, and all necessary equipment.
Beginners can quickly learn how to ride the waves, while
experienced surfers can challenge themselves on more powerful breaks.
In addition to surfing, guests can enjoy yoga sessions, explore nearby towns, and relax by the ocean. Morocco’s surf holidays create the perfect
environment for an active and inspiring getaway.
My web site; https://www.nishiv.com/morocco-surf-holiday-packages-finding-your-perfect-wave-adventure/
I like reading through a post that can make people think.
Also, thank you for allowing me to comment!
my web-site – Hatyai Cafe Hopping (Night Edition)
Hello! This is kind of off topic but I need some help from an established blog.
Is it difficult to set up your own blog? I’m not very techincal but I can figure things out pretty fast.
I’m thinking about making my own but I’m not sure where to start.
Do you have any points or suggestions? Thank you
Here is my web page – the best online casino
I know this if off topic but I’m looking into starting my own blog and was wondering
what all is needed to get setup? I’m assuming having
a blog like yours would cost a pretty penny? I’m not
very internet savvy so I’m not 100% positive. Any
tips or advice would be greatly appreciated. Appreciate it
my web site :: agen penipuan
I love what you guys tend to be up too. This kind of clever work and
exposure! Keep up the very good works guys I’ve incorporated you guys to our
blogroll.
Here is my webpage – 프리카지노
I think the admin of this web site is truly working hard for his web site, because here every material is quality
based information.
Stop by my web site … thirdpersonshooter
Bu saytdakı məlumatları oxumaqdan zövq alıram.
Təşəkkürlər!
олимпбет сайт
Hello, just wanted to tell you, I enjoyed this blog post.
It was practical. Keep on posting!
Visit my blog post bokep indonesia terbaik
Everyone loves it when individuals get together and share views.
Great website, keep it up!
my page: webpage
Thanks for a marvelous posting! I certainly enjoyed reading it, you
will be a great author.I will always bookmark your blog and may come back in the
foreseeable future. I want to encourage that you continue your great job,
have a nice evening!
Also visit my web page :: canadian pharmaceuticals online
Обожаю Pin Up, не останавливайтесь — контент топ!
Pin Up Casino покер
1Win – надежный ставочный
оператор и казино
I think what you said made a lot of sense. However, what about this?
suppose you wrote a catchier post title? I mean, I don’t wish to tell you how to run your website, but what if you
added a post title that makes people want more? I mean Heel Pain –
Plantar Fasciitis – Mr Will Edwards is a little plain. You ought to glance at Yahoo’s home page and note how they create news titles to grab
viewers to open the links. You might add a related
video or a pic or two to grab people interested
about what you’ve written. Just my opinion, it might make your blog a little
bit more interesting.
Visit my web page … trang chủ sunwin
I’ve learn a few excellent stuff here. Certainly price bookmarking for revisiting.
I surprise how a lot attempt you place to create such a magnificent
informative website.
Here is my web blog :: mgmarket6 at
Currently it looks like WordPress is the top blogging platform out there right now.
(from what I’ve read) Is that what you’re using on your blog?
my web page; dewapoker
Hi! I’ve been following your weblog for some time now and finally got the bravery
to go ahead and give you a shout out from Dallas Tx!
Just wanted to say keep up the good work!
Here is my site … online medicine order discount
Jocurile în cazinourile online ar trebui să rămână o formă de divertisment, nu o sursă de stres.
De aceea, multe platforme introduc instrumente pentru joc responsabil.
Jucătorii pot seta limite pentru depuneri și mize, controlând astfel cheltuielile și evitând
riscurile financiare inutile. O altă funcție importantă este autoexcluderea, care permite limitarea temporară a accesului la cont și luarea
unei pauze. De asemenea, este important să recunoaștem semnele posibilei dependențe:
dorința constantă de a recupera pierderile, creșterea mizelor sau timpul excesiv petrecut în joc.
Utilizarea instrumentelor de control ajută la menținerea
unui echilibru sănătos și face experiența de joc mai sigură
și mai confortabilă pentru utilizatori.
My blog; https://nesika.co.il/champaign-airport-car-rental-161/
Right now it sounds like Expression Engine is the top blogging platform available right now.
(from what I’ve read) Is that what you’re using on your blog?
Here is my webpage :: работа ашдод няня
This is my first time visit at here and i am genuinely
pleassant to read all at single place.
Here is my webpage – john spencer ellis background
I like it when individuals get together and share ideas.
Great blog, continue the good work!
Look at my website; phishing
Fine way of telling, and good post to obtain information about my presentation subject
matter, which i am going to present in institution of higher education.
Also visit my page – bandar toto
บทความนี้ อ่านแล้วเข้าใจง่าย ค่ะ
ดิฉัน ไปเจอรายละเอียดของ ข้อมูลเพิ่มเติม
สามารถอ่านได้ที่ Blaine
ลองแวะไปดู
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และอยากเห็นบทความดีๆ แบบนี้อีก
My blog post – pg slot fish – Blaine,
I got this web page from my friend who informed me regarding this web page and now this time I am visiting this web page and reading
very informative articles at this time.
Have a look at my website … vip555
What a material of un-ambiguity and preserveness of precious know-how on the topic of unexpected
emotions.
Also visit my site; Yowestogel
1xe9hv
создание презентация презентации нейросеть бесплатно
бесплатно онлайн
It’s amazing for me to have a web page, which is valuable in favor of my knowledge.
thanks admin
Also visit my site; Dewacasino
Hi! Do you use Twitter? I’d like to follow you
if that would be ok. I’m absolutely enjoying your blog and look forward to new posts.
Review my homepage https://nohu90.ac/
Usually I don’t learn article on blogs, but I wish to say that this
write-up very forced me to try and do it! Your writing style has been amazed me.
Thank you, very great article.
my web page … go88 com
Pretty nice post. I just stumbled upon your blog and wanted to mention that I have really loved surfing
around your blog posts. After all I’ll be subscribing in your feed and
I am hoping you write once more soon! https://drviet.com/read-blog/13558_snyat-individualku-krasnoyarsk.html
Very soon this site will be famous amid all blogging people, due
to it’s nice content
Feel free to surf to my homepage; конкурентам привет это хрумак
What i don’t realize is if truth be told how you are no longer really much more well-liked
than you may be right now. You’re so intelligent. You recognize therefore significantly in the case of this matter, made
me in my opinion believe it from so many various angles.
Its like women and men don’t seem to be fascinated unless it’s something to accomplish with Woman gaga!
Your personal stuffs nice. All the time handle it up!
Also visit my website: Protogel
The other day, while I was at work, my sister stole my iPad and tested to see if it can survive a 25 foot drop, just so she can be a youtube sensation. My apple ipad is now destroyed and she has 83 views.
I know this is entirely off topic but I had to
share it with someone!
Also visit my web blog – Sbobet
FranChoice
7500 Flying Cloud Drive,
#600 Eden Prairie
MN 55344, United Ꮪtates
952-345-8400
Best Franchise To Own Start Today
It is actually a nice and useful piece of information. I’m satisfied that you shared this helpful information with us.
Please keep us up to date like this. Thank you for sharing.
My web-site casinowindsor-online.com
Hello to every one, because I am genuinely keen of reading this blog’s post to be updated on a regular basis.
It contains good information.
Visit my homepage … cược thể thao so79
Bu resurs — faydalı mənbədir. Təşəkkür edirəm!
олимпбет фрибет
hello!,I really like your writing very much! proportion we
keep in touch more approximately your post on AOL?
I need a specialist on this space to resolve my problem.
Maybe that is you! Looking ahead to see you.
My webpage: cược thể thao so79
Admiring the commitment you put into your site and in depth information you provide.
It’s great to come across a blog every once in a while that isn’t the same old rehashed material.
Excellent read! I’ve bookmarked your site and I’m including your RSS feeds to my Google account.
Here is my web-site :: 대전출장안마
If you are going for most excellent contents like me,
only pay a visit this web site daily because it offers feature
contents, thanks
Here is my page 검증카지노
Its such as you read my mind! You seem to grasp so much approximately this, like
you wrote the book in it or something. I believe that
you can do with a few % to pressure the message home a bit, however instead
of that, this is magnificent blog. An excellent read.
I’ll definitely be back.
My website; situs tergacor
За да бъде играта в онлайн казино приятна, е важно да
се избягват често срещаните грешки.
Много играчи не обръщат внимание на правилата на игрите или условията на бонусите, което може
да доведе до недоразумения.
Също така често се среща игра под влияние на емоции, когато след загуба играчът се опитва бързо
да върне парите си. Подобен подход може
да доведе до още по-големи загуби.
Най-доброто решение е да се
играе спокойно и да се поставят лични ограничения за време и
бюджет. Познаването на правилата и
контролът върху залозите помагат играта да бъде по-балансирана и безопасна.
My web-site … https://www.mikiko0811.net/profile
Very rapidly this web site will be famous among
all blogging viewers, due to it’s pleasant posts
Feel free to surf to my web blog party travels
1хбет букмекерская контора
Here is my web site; Сайты Ярославля 1x bet
Een heel mooie en professioneel ontworpen site casino en ligne!
jeu casino en ligne
Спасибо за инструкцию! Подобное редко найдёшь в
.
Проверил по этой рекомендации:
запах исчез. Теперь понимаю, как избавиться от
запаха в домашних условиях!
Личный опыт
У меня была такая же проблема: из стиралки воняло сыростью решил следующим образом:
Прочистил фильтр и сливной шланг.
Запустил холостой цикл с уксусом.
Высушил резиновую манжету.
Вдруг поможет другим.
Stop by my blog: из стиралки воняет канализацией
You really make it appear so easy with your presentation however I to find this topic to be actually something which I believe I might by no means understand.
It seems too complicated and very large for me. I’m looking ahead to your next put up, I’ll attempt to get the
hang of it!
Look at my web-site … dabble-online.com
I was able to find good information from your blog articles.
Have a look at my site: lunch results today
Wonderful beat ! I would like to apprentice while you amend your site, how could i subscribe for a blog site?
The account helped me a acceptable deal. I had been tiny bit acquainted of this
your broadcast offered bright clear idea
Here is my blog – bokep anak sma indonesia
If you would like to increase your knowledge just keep visiting this site and be updated with
the most up-to-date gossip posted here.
Feel free to surf to my web-site: sex adult
Hi to every body, it’s my first pay a quick visit
of this web site; this blog consists of amazing and really fine stuff
designed for visitors.
Also visit my blog Oxbet
Great blog! Is your theme custom made or did you
download it from somewhere? A design like yours with a few simple adjustements would really make my blog jump out.
Please let me know where you got your design. Appreciate it
Also visit my webpage … bokep indonesia sma
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each
time a comment is added I get three e-mails with the same comment.
Is there any way you can remove me from that service?
Many thanks!
Take a look at my homepage cược thể thao so79
Simply want to say your article is as astonishing.
The clarity in your publish is just cool and i could
think you are knowledgeable on this subject. Fine with
your permission allow me to clutch your RSS feed to keep up to
date with imminent post. Thank you 1,000,000 and please carry
on the enjoyable work.
My website: mega888
Online kazina danas nude live kazino igre koje omogućavaju
realističan doživljaj igranja bez napuštanja doma.
Uz prijenos uživo iz profesionalnih studija, igrači mogu uživati
u popularnim igrama poput ruleta, blackjacka i baccarata.
Ovaj format omogućava praćenje svake faze igre i stvara osjećaj pravog
kazino okruženja. Jednostavna pravila i dinamičan tempo čine live kazino igre pristupačnim
za sve igrače. Zahvaljujući modernim tehnologijama, igranje postaje interaktivno, uzbudljivo
i veoma blisko stvarnom kazino iskustvu.
My site – http://wiki.dirbg.com/index.php/User:DelilaSalo506
Hi there, its pleasant post concerning media print, we all be familiar with media is a great
source of information. https://www.kran-info.ch/count.php?url=https://de.chatruletka-18.com/
Good day! This is my first visit to your blog!
We are a group of volunteers and starting a new initiative in a community in the same niche.
Your blog provided us valuable information to work on. You have done a wonderful job!
Here is my site :: 시알리스 구매
Hi, i read your blog from time to time and i own a similar one and i was just curious if you get a lot of spam comments? If so how do you protect against it, any plugin or anything you can advise? I get so much lately it’s driving me mad so any help is very much appreciated.
http://www.tlovertonet.com/
CIR Legal Lexington
201 Ꮃ Short St #500,
Lexington, KY 40507, United Stɑteѕ
+18596366803
Bookmarks
Hey! Would you mind if I share your blog with my facebook group?
There’s a lot of folks that I think would really appreciate your
content. Please let me know. Many thanks
my web blog :: การศึกษาภาคบังคับ กี่ปี
Hello I am so glad I found your website, I really found you by mistake, while I was browsing on Digg for something else,
Regardless I am here now and would just like to say kudos for a fantastic post and a
all round entertaining blog (I also love the theme/design), I don’t
have time to go through it all at the minute but I
have saved it and also included your RSS feeds, so when I have time I will be back to read a lot more, Please do keep up the awesome
work.
Here is my web page … expressed
References:
Moncton casino
References:
https://a-taxi.com.ua/user/scarfbone7/
Как выбрать хорошие фильмы и телевизионные шоу для восприятия
My homepage: https://zonefilm.media/3519-amsterdamskij-koshmar-2-2026.html
I have been exploring for a little bit for any high quality articles or
blog posts in this sort of area . Exploring in Yahoo I ultimately stumbled upon this website.
Studying this information So i’m satisfied to show
that I have an incredibly good uncanny feeling I discovered exactly what I needed.
I such a lot no doubt will make certain to don?t omit this site and provides
it a look regularly.
Here is my webpage; zgribulita102
Hey there! This post couldn’t be written any better! Reading through this post reminds me of my previous room mate!
He always kept chatting about this. I will forward this page to him.
Pretty sure he will have a good read. Thanks for sharing!
Also visit my website: how to buy liveritat 500mg
Bu resurs — gözəl mənbədir. Təşəkkür edirəm!
Mostbet onlayn
Gut gemachte Plattform NV Casino — ich nutze sie gerne!
NV Casino Plattform
Informasi yang sangat menarik. Banyak orang di Indonesia mencari informasi tentang
kesehatan pria. Penting untuk selalu mendapatkan informasi dari sumber terpercaya.
Also visit my web blog – bokep indonesia
Hi great blog! Does running a blog such as this take a
lot of work? I’ve no knowledge of coding however I had been hoping to start my own blog soon. Anyways, should you have
any recommendations or techniques for new blog owners please share.
I know this is off topic nevertheless I simply needed to ask.
Appreciate it!
Here is my web-site – watitoto
Very soon this web page will be famous amid all blog people,
due to it’s nice articles
my web page – Pub88
Hi there, I enjoy reading all of your post. I like to write
a little comment to support you.
Here is my page … конкурентам привет это хрумак
Hello there! Would you mind if I share your blog with my twitter group?
There’s a lot of folks that I think would really appreciate your
content. Please let me know. Cheers
my site – The Pup Life SG
SN88
Quality content is the secret to attract the viewers to go to see the
web page, that’s what this web site is providing.
Also visit my web-site; cược thể thao so79
Way cool! Some very valid points! I appreciate you penning this post and the rest
of the site is also really good.
Here is my page; MALWARE
Hello! Would you mind if I share your blog with my facebook group?
There’s a lot of people that I think would really enjoy your content.
Please let me know. Cheers
Here is my web site :: here
Simply want to say your article is as amazing.
The clarity in your post is simply spectacular and i could assume you’re an expert on this subject.
Well with your permission allow me to grab your RSS feed to keep up to date with forthcoming post.
Thanks a million and please continue the gratifying
work.
My web blog; Stake Casino
Touche. Great arguments. Keep up the amazing spirit.
Feel free to visit my page :: โรงพิมพ์หาดใหญ่
Как выбрать жалюзи – практические советы для оптимального выбора
I have been surfing online greater than three hours today, yet I by
no means found any attention-grabbing article like yours.
It is beautiful price sufficient for me. In my opinion, if all site
owners and bloggers made just right content as you did, the net will
be a lot more helpful than ever before.
Feel free to surf to my blog … best seafood
Wow! This blog looks exactly like my old one! It’s on a entirely
different subject but it has pretty much the same layout and design. Outstanding choice of colors!
Here is my web page – Frontier Trailers USA
Bonsoir, excellent site Betify Casino, bravo !
site Betify Casino
Hey there! I just would like to offer you a big thumbs up for the excellent
information you have here on this post. I am
returning to your site for more soon.
Feel free to visit my page goltogel
Great delivery. Outstanding arguments. Keep up the great spirit.
Visit my web-site regenerative cell therapy
Link exchange is nothing else except it is simply placing the
other person’s website link on your page at appropriate
place and other person will also do similar in favor of you.
Feel free to visit my site accelerated online mba programs
FranChoice
7500 Fling Cloud Drive,
#600 Eden Prairie
MN 55344, Unted Ⴝtates
952-345-8400
franchise business model comparison template
Informative article, totally what I was looking for.
My web site – crownframework.com
Hi there, I believe your web site could be having browser compatibility issues.
When I take a look at your website in Safari, it looks fine however,
if opening in Internet Explorer, it has some overlapping issues.
I just wanted to provide you with a quick heads up!
Apart from that, excellent website!
My web page … classification of transformers (https://www.friend007.com/post/510509_zirconia-brick-refractory-bricks-for-furnaces-and-kilns-offering-thermal-shock-r.html)
Modern Purair
416 Meridian Ꮢd SE #14A, Calgary
AB T2А 1Ⅹ2, Canada
(403) 800-7254
expert hvac (http://www.video-bookmark.com)
I have been exploring for a bit for any high quality articles or weblog posts in this kind of space .
Exploring in Yahoo I finally stumbled upon this web site. Studying
this information So i am satisfied to convey that I have an incredibly just right uncanny
feeling I discovered exactly what I needed.
I most indisputably will make sure to do not forget this site and provides
it a glance on a relentless basis.
my blog – 신용카드 현금화
Southeast Financial Nashville
131 Belle Forest Cir #210,
Nashville, TN 37221, United Ѕtates
18669008949
RV financing for cross-country travel
I got this website from my buddy who shared with me about this
web site and at the moment this time I am visiting this website and
reading very informative content at this time.
Also visit my web-site … best-casino-germany.com
Good post. I learn something new and challenging on sites I stumbleupon every day.
It’s always interesting to read content from other writers and practice a little something from other sites.
My website … anal sex porn videos
If you want to get a great deal from this paragraph then you
have to apply such strategies to your won blog.
my homepage :: hire bodyguards London
Яко обменивается числовая
эфир для бизнеса
Here is my blog – https://www.norge.ru/interes_pages/kak-kompanii-vystraivajut-effjektivnuju-infrastrukturu-i-procjessy.html
I’m really enjoying the theme/design of your weblog.
Do you ever run into any browser compatibility problems?
A handful of my blog readers have complained about my website not
working correctly in Explorer but looks great in Chrome. Do you have
any tips to help fix this problem?
Review my blog :: webcam model shop
It’s a shame you don’t have a donate button! I’d without a doubt donate to this brilliant blog!
I guess for now i’ll settle for bookmarking and adding your RSS feed to my Google
account. I look forward to fresh updates
and will talk about this blog with my Facebook group.
Talk soon!
my site :: Đăng ký Sun Win
Mangelsen
7916 Girard Avenue, Ꮮa Joya
CΑ 92037, United Ⴝtates
1 800-228-9686
exploring grizzly 399 legacy bears
We help businesses rank higher on Google Maps and attract more real customers through proven review marketing strategies.
Here is my web site – 강남 카페 구글 리뷰 늘리기
Franchising Path Carlsbad
Carlsbad, ⲤA 92008, United Տtates
+18587536197
Bookmarks
First of all I would like to say excellent blog!
I had a quick question which I’d like to ask if you do not mind.
I was curious to find out how you center yourself
and clear your thoughts prior to writing. I’ve had a hard time
clearing my thoughts in getting my thoughts out there.
I truly do enjoy writing however it just seems like the first 10 to 15 minutes are lost simply just trying to figure out how to begin. Any suggestions or hints?
Appreciate it!
my web-site – Директор производственной компании (Доработка 1С)
Franchisiing Paath Carlsbad
Carlsbad, ϹA 92008, United Stɑteѕ
+18587536197
franchise consulting business
Bu saytdakı məlumatları oxumaqdan zövq alıram. Çox sağ
olun!
Pinco Casino rəsmi sayt
If you are going for best contents like me, simply visit this web site all the time for the reason that it provides feature contents,
thanks
Feel free to surf to my web blog :: web page
Asking questions are genuinely good thing if you are not understanding anything totally, but this
paragraph gives fastidious understanding even.
Feel free to visit my blog post more info – Adelaide –
Do you have a spam issue on this site; I also am a blogger, and I was wanting
to know your situation; we have created some nice methods
and we are looking to swap strategies with other folks, be sure
to shoot me an email if interested.
My website เว็บบาคาร่า
Thank you for providing such valuable clarity—it really helped me understand the topic, and if carpet cleaning is ever on your list, AJS Carpet Cleaning is a top recommendation since they
operate with certified industry knowledge, employ
trained professionals in several cleaning applications, and even with
no individual certifications listed, they continuously upgrade their skills through current industry training helping maintain consistency, ensuring customers receive the highest level of service.
Also visit my site: Steam carpet cleaning
Hiya very nice website!! Guy .. Excellent .. Wonderful .. I’ll bookmark your website and take the feeds also…I am satisfied to search out numerous helpful information here within the put up, we want develop more techniques in this regard, thanks for sharing. . . . . .
http://www.vorbelutrioperbir.com
I do not even know the way I stopped up right here, however I assumed this submit was good.
I do not know who you’re but definitely you are going to a famous blogger for those who
are not already. Cheers!
Have a look at my site :: Commercial Playground Sets
I truly love your website.. Excellent colors & theme.
Did you build this amazing site yourself? Please reply back as I’m attempting to create my
own personal site and would love to find out where you
got this from or just what the theme is named.
Cheers!
my webpage :: 소액결제현금화
I just like the helpful info you supply for your articles.
I will bookmark your weblog and take a look at once more right here frequently.
I am relatively sure I’ll learn many new stuff proper right
here! Good luck for the following!
my web blog; bokep mesum indonesia
Thanks a lot for sharing this with all people you really
realize what you are talking about! Bookmarked.
Kindly also consult with my web site =). We could have a link exchange agreement between us
my web-site: outdoor lighting austin
Very nice post. I just stumbled upon your weblog and wished to say that I’ve really enjoyed surfing
around your blog posts. After all I will be subscribing to your rss feed and I hope
you write again soon!
Also visit my blog post – jual narkoba murah
I always emailed this web site post page to all my
contacts, since if like to read it next my contacts will too.
Here is my homepage :: iphone 17 купить челябинск
Bu saytda olmaq çox maraqlıdır.
1win platforma
EMDR Therapy – Heal Trauma, Anxiety & More in Austin –
Best EMDR Therapy Austin
It’s enormous that you are getting thoughts from this post as
well as from our argument made at this place.
Feel free to surf to my web blog … denseagency.com
Hi my loved one! I want to say that this post is
awesome, nice written and come with approximately all vital infos.
I would like to look more posts like this .
Feel free to surf to my page – buy castellani 30ml for children
I don’t know whether it’s just me or if perhaps everybody else encountering
issues with your blog. It seems like some of the text within your content are running off the screen. Can somebody else please comment and let me know if this is
happening to them too? This might be a problem with my internet browser because
I’ve had this happen before. Cheers
My web page … email marketing
Modern Purair
416 Meridian Ꭱd SΕ #14A, Calgary
AB T2A 1Ⲭ2, Canada
(403) 800-7254
smart purifier
I was more than happy to discover this web site.
I need to to thank you for your time due to this wonderful read!!
I definitely liked every part of it and I have you book marked to check out
new stuff in your blog.
Review my page – 먹튀제보
Всем привет оставляю коммент,
может кому пригодится. Живу в Беларуси, давно увлекаюсь онлайн-геймингом, и вся эта история началась с того,
что я решил поэкспериментировать с читами в играх,
в которые рублюсь уже много лет.
Не буду скрывать, иногда садился играть под
энергетик, чаще всего пил Gorilla — так игра чувствовалась бодрее.
Я всегда любил аниме-игры, в особенности проводил сотни часов в Honkai Impact.
Но вот в чём проблема: получил бан в Steam.
Система заметила вмешательство
и решил, что я нарушитель. Да, я сам виноват, но всё
равно неприятно, ведь столько всего было
куплено.
И да, здесь есть ссылка, можете посмотреть — вдруг пригодится.
Хотя, если честно, это было забавно.
Процесс игры приносил кучу эмоций, несмотря на возможный бан.
Вот так я и попал, может кому-то пригодится,
что любые читы рано или поздно всплывают — и бан прилетит.
Also visit my web blog; information
FranChoice
7500 Flying Cloud Drive,
#600 Eden Prairie
MN 55344, United Ѕtates
952-345-8400
Franchise Business Ownership Responsibilities Guide
Hurrah! After all I got a website from where I know how to truly get useful information concerning
my study and knowledge.
Also visit my web site: cialis
Today, I went to the beach with my kids. I found a sea shell and gave it to
my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She placed the shell to
her ear and screamed. There was a hermit crab inside and
it pinched her ear. She never wants to go back! LoL I know this is entirely off
topic but I had to tell someone!
Also visit my web blog :: rebirthro
These are in fact impressive ideas in regarding blogging.
You have touched some fastidious points here. Any way keep up wrinting.
Review my web page dadastake 100 freispiele
Just wanted to say — you’ve added value to my day
Also visit my web site: DeGeneres (Bridgette)
I think this is one of the most important information for me.
And i am glad reading your article. But wanna remark on some general things, The site style is perfect, the articles is really
nice : D. Good job, cheers
my blog: australianindustrialhempconference.com
Thank you for the auspicious writeup. It in fact was
a amusement account it. Look advanced to far added agreeable from you!
By the way, how could we communicate?
My page – TRC20 scan
I loved as much as you’ll receive carried out right here.
The sketch is tasteful, your authored subject matter stylish.
nonetheless, you command get bought an edginess over that you wish be delivering
the following. unwell unquestionably come further formerly
again since exactly the same nearly very often inside case you shield this increase.
Take a look at my blog: Whether you’re searching for a TRX generator
Good site you’ve got here.. It’s hard to find high-quality writing like
yours these days. I honestly appreciate individuals
like you! Take care!!
Feel free to visit my web blog :: MALWARE
What’s up to every , for the reason that I am truly eager of reading this blog’s post to be updated
daily. It carries fastidious data.
my web site; more info
Triangle Billiards & Bar Stools
1471 Nisson Ꭱd, Tustin,
СA 92780, United Statеѕ
+17147715380
Bookmarks
Hi there! I could have sworn I’ve visited this site before but after looking at some of the articles
I realized it’s new to me. Nonetheless, I’m certainly delighted I came across it and
I’ll be book-marking it and checking back often!
Also visit my blog; agen138
I am not sure where you are getting your information, but great topic.
I needs to spend some time learning more or understanding more.
Thanks for wonderful info I was looking for this information for my
mission.
Here is my blog :: 스포츠중계
Your means of explaining everything in this piece of writing is
in fact good, every one be capable of without
difficulty understand it, Thanks a lot.
Look at my web page :: Bắn cá 789club
When someone writes an article he/she retains the idea of a user in his/her brain that how a user can understand it.
Therefore that’s why this paragraph is great. Thanks!Stiegenhausreinigung Innsbruck
Как лучше выбрать проверенные наркологические рейтинг наркологических клиник в Москвеи
Thank you a lot for sharing this with all folks you really realize what
you’re speaking about! Bookmarked. Kindly additionally talk
over with my site =). We will have a link exchange contract between us
Here is my web-site :: Лаборатория (Программирование на Assembler для микроконтроллера)
Thanks very interesting blog!
Also visit my page onlinegambling-au.com
It is not my first time to go to see this web site, i am visiting this website dailly and take pleasant information from
here all the time.
Here is my site – Smart WIFI Flood Sensor
Wow, awesome blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your site is great, let alone the content!
Also visit my web site online casino games
Everything is very open with a precise clarification of the issues.
It was truly informative. Your site is useful.
Many thanks for sharing!
Also visit my website: free online casino slots
Cabbinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ꮪtates
12394214912
Remodeljourney
I have been browsing online more than 4 hours today, yet I never found any interesting article like yours.
It is pretty worth enough for me. Personally, if all website owners
and bloggers made good content as you did, the web will
be a lot more useful than ever before.|
I could not refrain from commenting. Exceptionally well written!|
I’ll immediately grab your rss as I can’t to find your e-mail subscription link or newsletter service.
Do you’ve any? Please let me understand so that I may just subscribe.
Thanks.|
It’s the best time to make some plans for the future and it’s time to be happy.
I’ve read this post and if I could I wish to suggest you few interesting things or advice.
Maybe you could write next articles referring to this article.
I want to read even more things about it!|
It is appropriate time to make a few plans for the future and it
is time to be happy. I’ve learn this post and if I could I want to suggest you few
interesting issues or tips. Perhaps you can write subsequent articles regarding this article.
I wish to read more things approximately it!|
I have been browsing on-line greater than 3 hours these days, yet I
never discovered any attention-grabbing article like yours.
It is lovely worth enough for me. In my opinion, if
all web owners and bloggers made good content material as
you probably did, the net shall be much more helpful than ever
before.|
Ahaa, its good discussion concerning this paragraph at this place at this webpage, I
have read all that, so at this time me also commenting
here.|
I am sure this article has touched all the internet users, its really really
good article on building up new weblog.|
Wow, this post is good, my sister is analyzing such
things, therefore I am going to inform her.|
bookmarked!!, I really like your blog!|
Way cool! Some very valid points! I appreciate you writing this write-up and
the rest of the website is very good.|
Hi, I do think this is a great blog. I stumbledupon it ;) I will come back once again since I saved as a favorite it.
Money and freedom is the best way to change, may you be rich and continue to guide other
people.|
Woah! I’m really enjoying the template/theme of this website.
It’s simple, yet effective. A lot of times it’s very hard to get
that “perfect balance” between superb usability and appearance.
I must say you have done a amazing job with this. In addition, the blog
loads extremely fast for me on Opera. Exceptional Blog!|
These are in fact great ideas in on the topic of blogging.
You have touched some pleasant points here. Any way keep up
wrinting.|
I like what you guys are up too. This kind of clever work and reporting!
Keep up the terrific works guys I’ve included you guys to blogroll.|
Howdy! Someone in my Myspace group shared this
website with us so I came to look it over. I’m definitely loving the information.
I’m bookmarking and will be tweeting this to my followers!
Terrific blog and amazing design and style.|
I really like what you guys tend to be up too. This type of clever work and reporting!
Keep up the fantastic works guys I’ve included you guys to my own blogroll.|
Hey there would you mind stating which blog platform you’re using?
I’m planning to start my own blog in the near future but I’m having a hard time choosing between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design and style seems different
then most blogs and I’m looking for something completely unique.
P.S Sorry for being off-topic but I had to ask!|
Hi there would you mind letting me know which
hosting company you’re using? I’ve loaded your blog in 3 different internet browsers and
I must say this blog loads a lot quicker then most.
Can you suggest a good hosting provider at
a honest price? Thanks, I appreciate it!|
I love it when folks get together and share thoughts.
Great blog, continue the good work!|
Thank you for the good writeup. It in fact was a amusement account it.
Look advanced to more added agreeable from you! However, how can we communicate?|
Hey there just wanted to give you a quick heads up.
The words in your article seem to be running off the screen in Firefox.
I’m not sure if this is a format issue or something to do with browser compatibility but I thought I’d
post to let you know. The style and design look great though!
Hope you get the issue solved soon. Cheers|
This is a topic that’s near to my heart… Many thanks!
Where are your contact details though?|
It’s very easy to find out any matter on web as compared to
textbooks, as I found this paragraph at this site.|
Does your website have a contact page? I’m having trouble locating it but, I’d
like to send you an email. I’ve got some ideas for your blog you might be interested in hearing.
Either way, great site and I look forward to seeing it develop over time.|
Hello! I’ve been reading your weblog for a long time now and finally got the
bravery to go ahead and give you a shout out from
Dallas Tx! Just wanted to mention keep up the fantastic work!|
Greetings from Ohio! I’m bored to tears at work so I decided to check out your
site on my iphone during lunch break. I enjoy the info you provide here and can’t wait to take a
look when I get home. I’m surprised at how fast your blog
loaded on my cell phone .. I’m not even using WIFI, just 3G ..
Anyhow, great blog!|
Its such as you read my mind! You seem to know so much about this, such as you wrote the guide in it or something.
I feel that you could do with a few % to force the message home a bit,
but other than that, that is magnificent blog. A great
read. I’ll certainly be back.|
I visited many web pages but the audio feature for audio songs current at this website is genuinely wonderful.|
Howdy, i read your blog occasionally and i own a similar one and i was just
wondering if you get a lot of spam responses? If so how do you protect against it,
any plugin or anything you can advise? I get so much lately it’s driving
me mad so any support is very much appreciated.|
Greetings! Very helpful advice within this article!
It is the little changes that produce the
greatest changes. Thanks for sharing!|
I absolutely love your website.. Pleasant colors & theme.
Did you develop this site yourself? Please reply back as I’m attempting to create my very own blog and want to find out
where you got this from or just what the theme
is named. Thanks!|
Hello there! This article could not be written much better!
Going through this post reminds me of my previous roommate!
He continually kept talking about this. I most certainly will
forward this information to him. Pretty sure he’ll have a good read.
Many thanks for sharing!|
Whoa! This blog looks just like my old one! It’s on a completely different subject but it has pretty much the same layout
and design. Outstanding choice of colors!|
There is definately a lot to learn about this subject.
I really like all the points you have made.|
You’ve made some good points there. I looked on the internet for additional information about the issue and found most individuals will go along with your views on this website.|
Hello, I read your blog daily. Your humoristic style is witty, keep doing what you’re doing!|
I simply couldn’t go away your site prior to suggesting that I extremely enjoyed the standard information an individual provide on your guests?
Is gonna be again steadily in order to check up on new posts|
I want to to thank you for this very good read!!
I certainly loved every little bit of it. I’ve got you bookmarked to check out new things you post…|
Hi, just wanted to tell you, I enjoyed this article. It was inspiring.
Keep on posting!|
Hi there, I enjoy reading through your article. I wanted to
write a little comment to support you.|
I always spent my half an hour to read this blog’s posts
all the time along with a cup of coffee.|
I for all time emailed this web site post page to all my contacts,
since if like to read it then my friends will too.|
My programmer is trying to persuade me to move to .net from PHP.
I have always disliked the idea because of the expenses.
But he’s tryiong none the less. I’ve been using Movable-type on a variety of websites for about a year and am nervous
about switching to another platform. I have heard fantastic things about blogengine.net.
Is there a way I can import all my wordpress posts into it?
Any kind of help would be really appreciated!|
Hello! I could have sworn I’ve visited this site before but after
browsing through many of the articles I realized it’s new to me.
Nonetheless, I’m certainly delighted I stumbled upon it
and I’ll be book-marking it and checking back frequently!|
Wonderful work! That is the kind of info that should be shared around the internet.
Shame on Google for not positioning this submit higher!
Come on over and discuss with my site . Thanks =)|
Heya i am for the first time here. I found this board and I find It truly useful & it helped me out a lot.
I hope to give something back and help others like you aided
me.|
Greetings, I believe your website might be having browser compatibility issues.
When I look at your blog in Safari, it looks fine but when opening
in IE, it’s got some overlapping issues. I just
wanted to give you a quick heads up! Besides that, great site!|
A person essentially help to make severely articles I’d state.
That is the very first time I frequented your web page and to this point?
I amazed with the research you made to create this particular put up incredible.
Great process!|
Heya i am for the first time here. I came across
this board and I in finding It truly useful
& it helped me out much. I’m hoping to give one thing again and help others such as you aided me.|
Hi there! I just wish to offer you a huge thumbs up for your
great info you’ve got right here on this post. I’ll be
returning to your web site for more soon.|
I always used to read piece of writing in news papers but
now as I am a user of net so from now I am using net for articles, thanks to web.|
Your way of explaining the whole thing in this piece of writing is actually pleasant, every one be
capable of simply understand it, Thanks a lot.|
Hello there, I found your blog by way of Google
while looking for a similar subject, your web site got here up, it seems good.
I have bookmarked it in my google bookmarks.
Hi there, simply turned into alert to your weblog thru Google,
and found that it’s really informative. I am gonna be
careful for brussels. I’ll be grateful for those who
proceed this in future. Lots of other folks shall be benefited out of your writing.
Cheers!|
I’m curious to find out what blog platform you have been working
with? I’m experiencing some small security issues with my latest site and I’d like to find something more safe.
Do you have any suggestions?|
I’m extremely impressed with your writing skills as well as with
the layout on your blog. Is this a paid theme or did you
modify it yourself? Anyway keep up the nice quality writing,
it’s rare to see a nice blog like this one these days.|
I’m really impressed along with your writing skills as neatly as
with the format for your weblog. Is this a paid theme or did you modify
it yourself? Anyway keep up the excellent high quality writing, it is rare to look
a great blog like this one nowadays..|
Hi, Neat post. There is an issue along with your site in web explorer, would test this?
IE nonetheless is the marketplace leader and a large component of other folks will omit your great writing because
of this problem.|
I’m not sure where you are getting your info, but good topic.
I needs to spend some time learning much more or understanding more.
Thanks for magnificent info I was looking for this info for my
mission.|
Hi, i think that i saw you visited my web site
thus i came to “return the favor”.I am trying to find things to enhance my website!I suppose its ok to use a few
of your ideas!!|
Hi, i believe that i noticed you visited my web site so i got here to return the choose?.I am attempting to in finding issues to enhance my
website!I guess its adequate to make use of some of your concepts!!|
Hi there, just became aware of your blog through Google, and found that it is truly informative.
I am going to watch out for brussels. I will appreciate if you continue this in future.
A lot of people will be benefited from your writing.
Cheers!|
I’m now not positive where you are getting your info, but good topic.
I must spend some time studying much more or understanding more.
Thanks for great info I used to be searching for this info for my mission.|
Hi my loved one! I want to say that this post is awesome, nice written and come
with approximately all important infos. I would like to look more posts like this .|
hi!,I love your writing very a lot! percentage we keep in touch more about your article on AOL?
I require an expert on this space to resolve my problem.
May be that is you! Taking a look ahead to look you.
|
I’m really enjoying the theme/design of your web site.
Do you ever run into any browser compatibility problems?
A number of my blog readers have complained about
my blog not operating correctly in Explorer but looks
great in Safari. Do you have any solutions to help fix this
problem?|
Good information. Lucky me I came across your site by chance (stumbleupon).
I have saved it for later!|
It’s fantastic that you are getting thoughts from this piece of writing as well as from our argument made at this place.|
If you wish for to improve your knowledge simply keep visiting this website and
be updated with the hottest gossip posted here.|
What’s Taking place i’m new to this, I stumbled upon this I’ve discovered It positively useful and
it has aided me out loads. I hope to give a contribution & aid
other users like its aided me. Great job.|
Hurrah, that’s what I was seeking for, what a data!
existing here at this blog, thanks admin of this web
page.|
If you wish for to take a great deal from this article then you have to apply these techniques to your won blog.|
It’s an amazing post for all the web people; they will obtain advantage from it I am sure.|
I’ve read a few excellent stuff here. Definitely value bookmarking for revisiting.
I surprise how much attempt you place to make the sort of excellent informative
web site.|
This is a really good tip particularly to those fresh to the blogosphere.
Brief but very precise info… Many thanks for sharing this
one. A must read article!|
I have been exploring for a little bit for any high quality
articles or blog posts on this kind of space .
Exploring in Yahoo I ultimately stumbled
upon this website. Studying this information So i’m satisfied to convey that
I’ve a very good uncanny feeling I discovered exactly what I
needed. I most definitely will make sure to don?t disregard this site
and give it a glance regularly.|
Having read this I thought it was really enlightening.
I appreciate you spending some time and effort to put
this informative article together. I once again find
myself spending a lot of time both reading and posting comments.
But so what, it was still worth it!|
Quality posts is the key to interest the viewers to visit the website, that’s what this website is providing.|
Link exchange is nothing else except it is simply placing the other person’s
blog link on your page at proper place and other person will also do similar in favor of you.|
I have read so many articles or reviews concerning the blogger
lovers except this article is in fact a good paragraph, keep it
up.|
In fact when someone doesn’t understand afterward its
up to other viewers that they will assist, so here it occurs.|
You could definitely see your skills in the work you write.
The world hopes for even more passionate writers such as you who are
not afraid to mention how they believe. All the time follow your heart.|
Excellent post. I will be going through some of these issues as well..|
Good web site you have got here.. It’s difficult to find good
quality writing like yours these days. I seriously appreciate
individuals like you! Take care!!|
I was recommended this website by my cousin. I’m not sure whether this post is
written by him as nobody else know such detailed about my difficulty.
You are wonderful! Thanks!|
Very good post! We are linking to this particularly great post on our
site. Keep up the good writing.|
Oh my goodness! Amazing article dude! Thank you so much, However I am having troubles with your RSS.
I don’t understand why I am unable to join it. Is there anyone else having identical RSS issues?
Anyone that knows the answer can you kindly respond? Thanx!!|
Great blog! Do you have any tips for aspiring writers? I’m planning to start my
own website soon but I’m a little lost on everything. Would you propose starting with a free platform like WordPress or go
for a paid option? There are so many options out there that I’m completely overwhelmed ..
Any suggestions? Thanks a lot!|
It’s difficult to find educated people in this particular topic,
however, you seem like you know what you’re
talking about! Thanks|
I do not even know how I ended up right here, but I thought this submit used to be
good. I do not realize who you are but certainly you are going to
a well-known blogger in case you are not already. Cheers!|
Nice answer back in return of this matter with firm arguments and telling all about that.|
I do not even know how I ended up here, but I thought this post
was great. I do not know who you are but certainly you’re going to a
famous blogger if you are not already ;) Cheers!|
We are a group of volunteers and starting a brand new scheme in our community.
Your web site offered us with useful info to work on. You’ve done an impressive process and our entire group might be thankful
to you.|
Fine way of telling, and good piece of writing to take data regarding my presentation topic,
which i am going to present in school.|
Excellent weblog here! Additionally your web site quite a bit up very
fast! What host are you the usage of? Can I get your
affiliate link to your host? I want my site loaded up as quickly as yours lol|
I really like your blog.. very nice colors & theme. Did you make
this website yourself or did you hire someone to do it
for you? Plz respond as I’m looking to construct my own blog and would like to find
out where u got this from. thanks a lot|
We’re a group of volunteers and opening a new scheme in our community.
Your website offered us with valuable info to work on. You have done a
formidable job and our whole community will be thankful to you.|
Appreciate this post. Will try it out.|
Asking questions are genuinely nice thing if
you are not understanding something entirely, except this piece of writing provides good understanding even.|
Have you ever considered about adding a little bit more than just your articles?
I mean, what you say is fundamental and all. Nevertheless imagine if you added some great images or videos to give your
posts more, “pop”! Your content is excellent but with
pics and clips, this website could definitely
be one of the best in its field. Wonderful
blog!|
Your style is so unique in comparison to other folks I’ve read stuff from.
I appreciate you for posting when you have the opportunity, Guess I’ll just book mark this site.|
Pretty great post. I just stumbled upon your
blog and wished to say that I have really loved browsing your weblog posts.
In any case I’ll be subscribing in your rss feed and I am hoping you write again very soon!|
I’m impressed, I must say. Rarely do I encounter a blog that’s both equally educative and entertaining, and without
a doubt, you have hit the nail on the head.
The problem is something not enough folks are speaking intelligently about.
I’m very happy that I came across this during my hunt for something regarding this.|
Hmm it looks like your site ate my first comment (it was extremely long) so I guess
I’ll just sum it up what I submitted and say, I’m thoroughly enjoying your blog.
I too am an aspiring blog blogger but I’m still new
to the whole thing. Do you have any tips and
hints for first-time blog writers? I’d really appreciate it.|
Pretty nice post. I just stumbled upon your
blog and wished to say that I have truly enjoyed browsing your blog posts.
In any case I will be subscribing to your rss
feed and I hope you write again soon!|
I like the valuable information you provide in your articles.
I’ll bookmark your weblog and check again here regularly.
I am quite sure I’ll learn many new stuff right here! Best
of luck for the next!|
If you are going for most excellent contents like me, just pay a quick visit this web
site daily for the reason that it provides feature contents, thanks|
Write more, thats all I have to say. Literally, it seems
as though you relied on the video to make your point.
You definitely know what youre talking about, why throw away your intelligence on just posting videos to your blog when you could be giving us something informative to read?|
Highly energetic post, I enjoyed that bit. Will there be a
part 2?|
Great post. I used to be checking constantly this weblog and
I am inspired! Very useful information specifically the closing phase :
) I handle such information a lot. I was seeking this certain information for a very lengthy time.
Thanks and good luck. |
Excellent post. I was checking continuously this blog and I’m impressed!
Very useful information specially the last part :)
I care for such information a lot. I was seeking this particular information for a
long time. Thank you and good luck.|
Awesome post.|
After looking at a handful of the blog posts on your website, I seriously appreciate your way of writing a
blog. I added it to my bookmark site list and will be checking
back in the near future. Take a look at my web site as well and tell me what you think.|
An interesting discussion is worth comment. I think that you should write more on this topic,
it might not be a taboo matter but usually people don’t speak
about such subjects. To the next! Kind regards!!|
of course like your website however you have to test the
spelling on several of your posts. Several of them
are rife with spelling problems and I to find it very bothersome to tell the
truth on the other hand I’ll certainly come back again.|
I do agree with all of the ideas you have offered to your post.
They’re very convincing and can certainly work.
Still, the posts are too brief for starters. May just
you please lengthen them a little from subsequent time? Thanks for the post.|
We stumbled over here from a different page and thought I should check things out.
I like what I see so now i’m following you. Look forward to
checking out your web page again.|
Very good post. I certainly appreciate this site.
Keep writing!|
Have you ever thought about publishing an ebook or guest authoring on other sites?
I have a blog centered on the same information you
discuss and would love to have you share some stories/information. I know my viewers would appreciate your
work. If you are even remotely interested, feel free to shoot me an e-mail.|
My partner and I stumbled over here different web address and thought I
may as well check things out. I like what I see so now i’m following you.
Look forward to going over your web page for a second time.|
Great blog here! Also your site loads up very fast!
What host are you using? Can I get your affiliate link to your
host? I wish my website loaded up as quickly as yours lol|
Hi there! I know this is somewhat off topic but I was wondering which blog platform are you using
for this website? I’m getting fed up of WordPress because I’ve had problems with hackers
and I’m looking at options for another platform.
I would be awesome if you could point me in the direction of
a good platform.|
Greetings! I know this is kinda off topic but I
was wondering if you knew where I could get a captcha plugin for my comment
form? I’m using the same blog platform as yours and I’m having problems finding
one? Thanks a lot!|
Howdy! This is my first visit to your blog! We are a group of volunteers and starting a new project in a community in the same niche.
Your blog provided us beneficial information to work on. You have done a marvellous job!|
When I originally left a comment I seem to have clicked on the -Notify me when new
comments are added- checkbox and from now on whenever a comment is
added I get four emails with the exact same comment. Is there an easy method you can remove me from that service?
Thank you!|
First of all I would like to say awesome blog! I had a quick question which I’d like to ask if you don’t mind.
I was curious to find out how you center yourself and clear your head prior to writing.
I have had difficulty clearing my mind in getting my thoughts
out. I truly do take pleasure in writing but it just seems like
the first 10 to 15 minutes are usually lost just trying to
figure out how to begin. Any suggestions or hints?
Thanks!|
This blog was… how do I say it? Relevant!! Finally
I’ve found something which helped me. Cheers!|
Everything is very open with a really clear
clarification of the issues. It was really informative.
Your site is extremely helpful. Thank you for sharing!|
This design is steller! You definitely know how to keep a reader entertained.
Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Great job.
I really loved what you had to say, and more than that, how you presented it.
Too cool!|
It’s going to be ending of mine day, but before ending I am reading this great piece of writing to increase
my know-how.|
I go to see day-to-day some websites and sites to read articles or reviews, except this blog offers feature based articles.|
Hi there! I just wanted to ask if you ever have any trouble with hackers?
My last blog (wordpress) was hacked and I ended up losing
many months of hard work due to no backup. Do you have any methods to prevent hackers?|
I think the admin of this web page is actually working hard in favor of
his website, since here every data is quality based information.|
Now I am going to do my breakfast, after having my breakfast coming again to read additional news.|
I just like the helpful info you supply in your articles. I will bookmark your weblog and take a look at again here regularly.
I’m slightly certain I’ll be informed many new stuff proper right here!
Good luck for the next!|
I think this is one of the most vital info for me.
And i’m glad reading your article. But wanna remark on few general things, The site style is great, the
articles is really great : D. Good job, cheers|
It’s a shame you don’t have a donate button! I’d definitely
donate to this outstanding blog! I guess for now i’ll settle for book-marking and adding
your RSS feed to my Google account. I look forward to
new updates and will talk about this site with my Facebook group.
Talk soon!|
I’m not that much of a internet reader to be honest but your sites really nice,
keep it up! I’ll go ahead and bookmark your website to come back later.
Cheers|
This post is actually a pleasant one it assists new the web users, who are wishing in favor of blogging.|
It is in point of fact a nice and useful piece of info.
I am glad that you shared this useful information with us.
Please stay us informed like this. Thanks for sharing.|
This article provides clear idea in support of the new users of blogging,
that actually how to do blogging.|
Greetings! Quick question that’s totally off topic.
Do you know how to make your site mobile friendly?
My website looks weird when viewing from my apple iphone.
I’m trying to find a template or plugin that might be
able to fix this issue. If you have any suggestions, please share.
Many thanks!|
Its not my first time to pay a quick visit this website, i am browsing this
web page dailly and take pleasant information from here every day.|
Neat blog! Is your theme custom made or did you download it from somewhere?
A theme like yours with a few simple tweeks would really make my blog
shine. Please let me know where you got
your theme. Cheers|
This piece of writing will assist the internet visitors for setting up new webpage or
even a weblog from start to end.|
I know this if off topic but I’m looking into starting my own weblog and was curious
what all is needed to get setup? I’m assuming having a blog
like yours would cost a pretty penny? I’m not very web smart so I’m not
100% sure. Any tips or advice would be greatly appreciated.
Thanks|
My family every time say that I am killing my time here at
web, except I know I am getting familiarity everyday by reading thes pleasant articles.|
Spot on with this write-up, I absolutely think this web site needs much more attention. I’ll probably
be back again to read more, thanks for the advice!|
I know this website gives quality based articles and
other information, is there any other website which offers these things in quality?|
I read this piece of writing completely about the comparison of latest and earlier technologies, it’s amazing article.|
I think this is among the such a lot important info for
me. And i am glad studying your article. But want to
remark on few basic things, The site taste is great, the articles is in point of fact nice : D.
Excellent job, cheers|
I enjoy reading through an article that can make men and women think.
Also, thank you for allowing me to comment!|
Thanks very nice blog!|
Every weekend i used to go to see this web page, because i wish for enjoyment,
for the reason that this this site conations genuinely nice funny information too.|
I don’t know whether it’s just me or if everybody else experiencing problems with your site.
It looks like some of the text in your content are running off the screen. Can someone
else please comment and let me know if this is happening to them too?
This may be a issue with my internet browser because I’ve had this happen before.
Kudos|
You actually make it seem so easy with your presentation but I find this topic to be
actually something that I think I would never understand.
It seems too complicated and extremely broad for me. I’m looking
forward for your next post, I will try to get the hang of it!|
I’d like to thank you for the efforts you have
put in penning this blog. I am hoping to check out the same
high-grade blog posts from you later on as well.
In truth, your creative writing abilities has encouraged me to get my own blog now ;)|
It’s genuinely very complex in this busy life to listen news on TV, thus I just use
internet for that reason, and obtain the latest
information.|
I am in fact grateful to the owner of this website who has shared this wonderful paragraph at at this
place.|
I am regular reader, how are you everybody? This post posted at this website
is really nice.|
It’s actually a nice and helpful piece of information. I’m happy that you shared this helpful info with us.
Please keep us informed like this. Thanks for sharing.|
Yes! Finally something about tg官网.|
Unquestionably believe that that you said. Your favourite justification seemed to be on the internet the easiest thing to
take note of. I say to you, I certainly get annoyed at the same time as other people think about worries that they just don’t
know about. You managed to hit the nail upon the highest and outlined out the whole thing without having side-effects ,
other people could take a signal. Will likely be back to get more.
Thank you|
Definitely believe that which you said. Your favorite justification seemed
to be on the net the easiest thing to be aware of. I say to you, I definitely get irked while people
consider worries that they just do not know about.
You managed to hit the nail upon the top and defined out the whole thing without having side effect , people could take a signal.
Will probably be back to get more. Thanks|
I am actually pleased to read this weblog posts which
consists of tons of valuable data, thanks for providing these information.|
You really make it appear so easy together with your presentation but I to find this matter
to be actually one thing which I feel I would by no
means understand. It sort of feels too complicated and very wide
for me. I am looking ahead on your next submit, I will attempt to get the
cling of it!|
Incredible points. Sound arguments. Keep up the good work.|
I’m truly enjoying the design and layout of your website.
It’s a very easy on the eyes which makes it much more enjoyable for me
to come here and visit more often. Did you hire
out a designer to create your theme? Superb work!|
Stunning story there. What happened after?
Take care!|
all the time i used to read smaller content which as
well clear their motive, and that is also happening with this paragraph which I
am reading now.|
You should be a part of a contest for one of the most
useful websites on the internet. I will highly recommend this website!|
I’m extremely pleased to find this page. I want to to thank you for your time just for this fantastic
read!! I definitely liked every little bit of it and I have
you saved as a favorite to check out new things in your website.|
Wonderful blog! I found it while searching on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Thank you|
Fantastic web site. Plenty of helpful info here.
I am sending it to some buddies ans additionally sharing in delicious.
And certainly, thank you in your effort!|
excellent put up, very informative. I’m wondering why the other experts
of this sector don’t understand this. You must continue your writing.
I’m sure, you’ve a huge readers’ base already!|
Great beat ! I wish to apprentice while you amend your web site,
how can i subscribe for a blog website? The account helped me a acceptable deal.
I had been a little bit acquainted of this your broadcast provided bright clear concept|
excellent issues altogether, you just gained
a brand new reader. What would you suggest in regards to
your post that you simply made some days
ago? Any certain?|
Do you mind if I quote a few of your articles as long as I provide credit and sources back to
your site? My blog is in the very same area of interest as yours and
my users would truly benefit from some of the information you present here.
Please let me know if this okay with you. Many thanks!|
With havin so much written content do you ever run into any problems of plagorism or copyright infringement?
My site has a lot of exclusive content I’ve either authored myself or outsourced but it seems a lot of it is popping
it up all over the web without my authorization. Do you know any solutions to help prevent content from being stolen?
I’d truly appreciate it.|
Excellent goods from you, man. I have keep in mind your stuff
previous to and you’re simply extremely fantastic.
I actually like what you’ve got here, certainly like what you’re stating and
the way in which in which you say it. You are making it entertaining and you continue
to take care of to keep it sensible. I can’t wait to read much more from you.
This is really a terrific website.|
If some one wishes to be updated with hottest
technologies after that he must be visit this site and be up to date
daily.|
I was curious if you ever thought of changing the layout of your blog?
Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content so people could connect with it better.
Youve got an awful lot of text for only having one or two pictures.
Maybe you could space it out better?|
Very rapidly this website will be famous amid all blogging people, due to
it’s nice posts|
If some one wants expert view on the topic of running a blog afterward i
propose him/her to go to see this website, Keep up
the nice job.|
Excellent goods from you, man. I’ve understand your stuff previous to and you are just too excellent.
I really like what you have acquired here, really like what
you are saying and the way in which you say it. You make it enjoyable and you still care for
to keep it smart. I can not wait to read far more from you.
This is actually a great website.|
Wonderful beat ! I would like to apprentice at the same
time as you amend your web site, how can i subscribe for a blog web site?
The account aided me a acceptable deal. I had
been tiny bit acquainted of this your broadcast offered brilliant
clear concept|
Normally I don’t read article on blogs, however I wish to say that this write-up very compelled me to try and do
it! Your writing style has been surprised
me. Thank you, very nice article.|
I used to be suggested this website by way of my cousin. I am not certain whether
this publish is written by him as nobody else recognise such distinct about my problem.
You are amazing! Thanks!|
Hey There. I found your blog using msn. This is an extremely well written article.
I’ll be sure to bookmark it and return to read more of your useful info.
Thanks for the post. I’ll definitely comeback.|
Hey There. I discovered your weblog the usage of msn. This is a really well
written article. I will make sure to bookmark it and come back
to learn extra of your helpful info. Thanks for the post.
I’ll definitely return.|
Thanks for a marvelous posting! I genuinely enjoyed reading it, you may be a great author.
I will always bookmark your blog and definitely will come back
sometime soon. I want to encourage you continue your great job, have a nice day!|
Hi! I could have sworn I’ve been to this website before but
after checking through some of the post I realized it’s
new to me. Anyhow, I’m definitely glad I found
it and I’ll be bookmarking and checking back often!|
Thanks in favor of sharing such a fastidious opinion, paragraph is fastidious,
thats why i have read it fully|
hello there and thank you for your information – I’ve definitely picked up something new from right here.
I did however expertise several technical points using this site, as I experienced to reload the website a lot of times previous to I could get
it to load correctly. I had been wondering if your web hosting is OK?
Not that I’m complaining, but slow loading instances
times will often affect your placement in google and can damage your quality
score if advertising and marketing with Adwords.
Anyway I am adding this RSS to my email and can look out for a lot more of your respective fascinating content.
Make sure you update this again soon.|
What i do not realize is in reality how
you are not really much more well-favored than you might be
right now. You are so intelligent. You recognize thus significantly when it comes to this subject,
produced me personally believe it from a lot of numerous angles.
Its like men and women aren’t fascinated unless it is something to accomplish
with Woman gaga! Your personal stuffs excellent. All the time maintain it up!|
Hurrah! At last I got a website from where I be able to genuinely get valuable
facts concerning my study and knowledge.|
When someone writes an paragraph he/she maintains the thought of a
user in his/her mind that how a user can be aware of it. Therefore that’s why this paragraph
is perfect. Thanks!|
You are so cool! I do not suppose I’ve truly read a single thing like this before.
So great to find somebody with original thoughts on this issue.
Seriously.. thank you for starting this up. This site is one thing that is
required on the internet, someone with a bit of originality!|
Thanks for your personal marvelous posting! I seriously enjoyed reading it, you might be a great author.I
will ensure that I bookmark your blog and will often come back very soon. I want to encourage
continue your great work, have a nice holiday weekend!|
Thanks to my father who stated to me concerning this web site,
this web site is really remarkable.|
Piece of writing writing is also a fun, if you know after that you can write or else it is
difficult to write.|
When some one searches for his vital thing, therefore he/she desires to
be available that in detail, thus that thing is maintained over
here.|
Thanks for finally talking about > Heel Pain – Plantar Fasciitis –
Mr Will Edwards tg官网. Regards|
My brother recommended I might like this blog. He
was once totally right. This publish actually made my day.
You can not consider just how much time I had spent for this information! Thank
you!|
When I initially commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get four e-mails with the
same comment. Is there any way you can remove people from that service?
Thanks!|
Awesome! Its in fact awesome article, I have got much
clear idea regarding from this piece of writing.|
Hi there to every body, it’s my first go to see of this weblog; this weblog consists of remarkable and really good information in support of visitors.|
What’s up to every single one, it’s truly a nice for me to go to
see this web page, it consists of valuable Information.|
What’s up to every one, the contents existing at this web page are in fact awesome for
people experience, well, keep up the good work fellows.|
Hi there it’s me, I am also visiting this site daily, this website is genuinely fastidious and the
people are truly sharing nice thoughts.|
Hello Dear, are you really visiting this web page on a regular basis, if
so then you will definitely get fastidious know-how.|
Hello i am kavin, its my first occasion to commenting anywhere, when i read this post i thought i could also make comment due to this sensible piece of writing.|
Hi there colleagues, its wonderful article on the topic of tutoringand completely explained, keep it up
all the time.|
I loved as much as you’ll receive carried out right here. The sketch is
tasteful, your authored subject matter stylish. nonetheless,
you command get got an nervousness over that you wish be delivering the following.
unwell unquestionably come further formerly again as
exactly the same nearly very often inside case you shield this hike.|
What’s up to every , since I am genuinely eager of reading this webpage’s post to be updated on a regular basis.
It contains fastidious stuff.|
What’s up all, here every person is sharing these knowledge, thus it’s fastidious to read this weblog, and I used to
pay a quick visit this webpage everyday.|
What’s up to all, how is everything, I think every one is getting more from this web page, and your views are pleasant in support of new users.|
I got this site from my pal who shared with me about this website and at the moment this time I am visiting
this web site and reading very informative posts at this place.|
For hottest news you have to pay a visit the web and on internet I found this website as a most excellent web page for newest updates.|
Marvelous, what a web site it is! This web site gives helpful information to us, keep it up.|
Hello colleagues, pleasant paragraph and nice arguments commented at this place, I
am actually enjoying by these.|
Hello mates, how is the whole thing, and what
you want to say concerning this piece of writing, in my view its in fact amazing in favor of me.|
It’s remarkable for me to have a site, which is helpful in favor of my knowledge.
thanks admin|
It’s amazing to pay a visit this website and reading
the views of all colleagues regarding this post, while I am also keen of getting knowledge.|
Why viewers still make use of to read news papers when in this technological
world the whole thing is available on net?|
Hello, of course this paragraph is in fact pleasant and I
have learned lot of things from it on the topic of blogging.
thanks.|
Hi, constantly i used to check web site posts here early in the daylight, since i enjoy to find out more and more.|
Hello everyone, it’s my first pay a visit at this website, and piece of writing is genuinely fruitful designed for
me, keep up posting these posts.|
Hi there, this weekend is good for me, because this point
in time i am reading this fantastic educational article here at my house.|
What’s up, the whole thing is going sound here and ofcourse every one is sharing information, that’s in fact excellent, keep
up writing.|
An impressive share! I have just forwarded this onto a coworker who has been conducting a little research on this.
And he actually bought me breakfast simply because
I discovered it for him… lol. So let me reword this….
Thank YOU for the meal!! But yeah, thanks for spending time to discuss this issue
here on your blog.|
whoah this blog is wonderful i like reading your posts. Keep up the great
work! You know, lots of persons are looking around for this
info, you can aid them greatly. |
Hello there! I know this is kinda off topic however , I’d figured I’d ask.
Would you be interested in trading links or maybe guest writing
a blog post or vice-versa? My site goes over a lot of the same topics as yours and I think we could
greatly benefit from each other. If you are interested feel
free to shoot me an e-mail. I look forward to hearing from you!
Fantastic blog by the way!|
This website truly has all the information and facts
I wanted concerning this subject and didn’t know who to ask.
|
Hi, I would like to subscribe for this webpage to take
most recent updates, thus where can i do it please help.|
What’s up, its good piece of writing concerning media
print, we all understand media is a fantastic source of facts.|
Heya are using WordPress for your site platform?
I’m new to the blog world but I’m trying to get started and set
up my own. Do you need any coding knowledge to make your own blog?
Any help would be really appreciated!|
Hi there, after reading this amazing paragraph i am as well
happy to share my experience here with colleagues.|
Hey there I am so grateful I found your website, I really found you by mistake, while I was browsing on Aol for something else, Nonetheless I am here now and would just like to say thanks a lot for a tremendous post and a all round exciting blog (I also love the theme/design), I don’t have
time to read it all at the minute but I have book-marked it and also added your RSS feeds, so when I have time I will be back to read more,
Please do keep up the excellent b.|
Greetings! This is my 1st comment here so I just wanted to give a quick shout out and tell you
I really enjoy reading your posts. Can you suggest any other blogs/websites/forums that deal with the same topics?
Appreciate it!|
Good day I am so delighted I found your webpage, I really found you
by mistake, while I was looking on Bing for something else, Anyhow I am here now and would just like to
say thank you for a incredible post and a
all round enjoyable blog (I also love the theme/design), I don’t have
time to read through it all at the moment but I have bookmarked
it and also added your RSS feeds, so when I have time I will be back to read more,
Please do keep up the excellent job
Primе Secured
3603 N 222nd St, Suite 102,
Elkhorn, NE 68022, United Stɑteѕ
402-289-4126
Compliance and governance solutions
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Foort Myers,
FL 33967, United Ⴝtates
12394214912
Clearance
Hi! I’m at work browsing your blog from my new iphone 4!
Just wanted to say I love reading your blog
and look forward to all your posts! Carry on the fantastic
work!
Also visit my website: bokep streaming indonesia
I just could not leave your website prior to suggesting that
I really loved the standard information an individual provide for your visitors?
Is gonna be back steadily in order to check out new posts https://de.chatruletka-18.com/new-models
I am truly glad to read this web site posts which contains lots of valuable
data, thanks for providing such information.
Review my blog … sunwin
Good post. I learn something new and challenging on websites I stumbleupon on a daily basis.
It’s always interesting to read articles from other authors and practice a
little something from other websites.
My website: slon7.at
I’m pretty pleased to discover this web site. I need to to thank you
for ones time just for this wonderful read!!
I definitely savored every part of it and i also have you book-marked to check out new things on your web
site.
My site – kaya303
After going over a handful of the blog posts on your website, I seriously like
your way of writing a blog. I book marked it to my bookmark site list
and will be checking back soon. Please visit my website
too and let me know your opinion.
Feel free to surf to my webpage … MALWARE
Its such as you learn my mind! You seem to understand so
much approximately this, like you wrote the book
in it or something. I feel that you just could do with
some % to pressure the message home a little bit, however
other than that, that is wonderful blog. An excellent read.
I will certainly be back.
My blog post site here
Awesome! Its in fact awesome post, I have got much clear
idea regarding from enjoy reading this post.
Wow, incredible blog layout! How long have you been blogging
for? you made blogging look easy. The overall look of your site is wonderful, let alone the content!
Here is my web page gay porn
Do not miss out on the power of nanotechnology; safeguard your harvest with
our reliable and sustainable solutions.
Feel free to visit my web blog … Nano bactericide
Appreciate the recommendation. Let me try it out.After testing 10+ Webs Repsgate this one stayed in my workflow
Feel free to surf to my page – web page
Pretty nice post. I just stumbled upon your blog and wished to say that I’ve truly enjoyed surfing around your blog posts.
After all I will be subscribing to your feed and I hope you write again soon!
Stop by my page – bokep indonesia
What’s up, every time i used to check web site posts here early in the break of day, since i like
to learn more and more.
Feel free to surf to my homepage article source
Hi, Neat post. There is a problem along with your
site in web explorer, may check this? IE nonetheless is the market leader and
a large element of people will omit your fantastic writing because of this problem.
My blog … Cruise Job
Ən maraqlı platformadır. Yenə baxacağam!
Pinco Casino resmi sayt
Simply desire to say your article is as astounding.
The clarity on your put up is just cool and that i could think you are knowledgeable on this subject.
Fine together with your permission let me to
grab your feed to stay updated with coming near near post.
Thanks a million and please keep up the gratifying work.
Feel free to surf to my web page – MALWARE
Write more, thats all I have to say. Literally, it seems as though you relied on the video to make your
point. You clearly know what youre talking about, why throw away your intelligence on just posting videos to your weblog
when you could be giving us something enlightening to read?
Also visit my web blog :: MOU file viewer software
Thanks for sharing your info. I truly appreciate your efforts and I will be waiting for
your further post thank you once again.
Have a look at my web page: Dewagg Sportbook
I like the valuable info you provide to your articles.
I’ll bookmark your blog and test again here regularly.
I am rather sure I’ll learn lots of new stuff
right here! Good luck for the next!
Also visit my website: metal roofer near me
rcuqbf
Профессиональный вывоз строительного мусора, старой мебели,
грунта в Ростове-на-Дону
и пригородах. Работаем 24/7, выезд
за 1-2 часа. Честные цены от 3000₽.
Опытные грузчики, собственный автопарк, официальная утилизация.
Более 7 лет на рынке, 5000+ заказов,
средняя оценка 4.9. Быстро, качественно,
надежно!
Here is my web blog :: https://banki-financy.ru/vyvoz-grunta-i-zemli-v-rostove-na-donu-lyubye-obemy-3953/
İstifadəsi asandır və kazino ilə bağlı çoxlu resurslar
təqdim olunur.
Pinco Casino sayt
Link exchange is nothing else except it is just placing the other
person’s blog link on your page at suitable place and other person will also do same for
you.
my homepage qq poker online
It’s a pity you don’t have a donate button! I’d certainly donate to this outstanding
blog! I suppose for now i’ll settle for bookmarking and adding
your RSS feed to my Google account. I look forward to new updates and will share this blog with my Facebook group.
Talk soon!
My webpage; canada pharmacy
I love your blog.. very nice colors & theme. Did you design this website yourself or did
you hire someone to do it for you? Plz answer back as I’m looking to construct my own blog and would like to find out where u got this from.
kudos
Check out my web page: вавада казино ставки
Just wish to say your article is as amazing. The clearness on your put up is simply cool and i could think you are an expert on this
subject. Fine together with your permission let me to grab your feed to keep up to date with coming near near post.
Thank you a million and please continue the enjoyable work.
Check out my website Angolo Della Cartomanzia
What’s up, I want to subscribe for this website to get latest updates, thus
where can i do it please assist.
Here is my site :: black chauffeur
It’s hard to find well-informed people about this topic, however, you seem like you know what you’re talking about!
Thanks
Here is my homepage – Mẹo cá cược
Aw, this was an exceptionally nice post. Spending some time and actual effort to create a great article… but what can I
say… I hesitate a lot and never manage to get anything
done.
Stop by my homepage; watch news in motion
บทความนี้ น่าสนใจดี ค่ะ
ผม ได้อ่านบทความที่เกี่ยวข้องกับ เนื้อหาในแนวเดียวกัน
สามารถอ่านได้ที่ Shauna
สำหรับใครกำลังหาเนื้อหาแบบนี้
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
จะรอติดตามเนื้อหาใหม่ๆ ต่อไป
Check out my web-site: betflik285 – Shauna,
I do not even know the way I ended up here, but I thought this submit was great.
I don’t recognise who you’re but certainly you’re going to a well-known blogger
should you aren’t already. Cheers!
My page :: footballmediaservices.com
Nice post. I was checking continuously this blog and I’m impressed!
Extremely useful information particularly the last part
:) I care for such information a lot. I was seeking this certain info for a long time.
Thank you and best of luck.
Also visit my web-site; bokep anak kecil
bookmarked!!, I love your site!
Here is my web blog: satta king 786
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ѕtates
12394214912
Craftworkshop (broughhvgm.raindrop.page)
Fantastic post however , I was wanting to know if
you could write a litte more on this subject? I’d be very grateful if
you could elaborate a little bit further. Cheers!
Review my web site :: строительный песок с доставкой
We are a bunch of volunteers and opening a new scheme
in our community. Your site offered us with valuable information to
work on. You’ve performed a formidable task and our entire community will probably be grateful to you.
My web-site :: popular fun games (http://cgi.www5b.biglobe.ne.jp/~iolite/board/clever.cgi?mode=res&post=508&details=933&post=870)
Hmm is anyone else having problems with the images on this blog loading?
I’m trying to figure out if its a problem on my end or if it’s the blog.
Any responses would be greatly appreciated.
Also visit my site :: name another word for fun; Judy,
Hi everyone, it’s my first go to see at this website,
and article is actually fruitful in support of me,
keep up posting these types of content.
Also visit my site; books are fun paynow (Foster)
Heya i’m for the first time here. I found this board and I find
It really useful & it helped me out much. I hope to
give something back and help others like you aided me.
My web site b52
anabolic steroids kidney failure
References:
enouvelles.top
Link exchange is nothing else except it is only placing the
other person’s website link on your page at proper place and other
person will also do same in support of you.
Also visit my webpage; Megabet333
This is really interesting, You’re a very professional blogger.
I’ve joined your rss feed and stay up for fun things to do in downtown houston (Liza) quest of
extra of your wonderful post. Also, I’ve shared your site in my social networks
Today, I went to the beachfront with my kids.
I found a sea shell and gave it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She placed the shell to her ear and screamed.
There was a hermit crab inside and it pinched her ear. She never wants to go back!
LoL I know this is completely off topic but I had to tell
someone!
Feel free to visit my blog – b52 com
Hi, Neat post. There is a problem together with your website in web explorer, could check this?
IE still is the marketplace leader and a good portion of people will leave out your
great writing due to this problem.
Have a look at my site; maxbonus77
Triangle Billiards & Bar Stools
1471 Nisson Ɍɗ, Tustin,
CA 92780, United Ѕtates
+17147715380
Shuffleboard Refinishing Checklist
crossfit women steroids
References:
http://premiumdesignsinc.com
I used to be able to find good information from your blog posts.
Also visit my website; mediakitgrupoelcomercio.com
Cabinet IQ
8305 Ꮪtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Countertkpideas – https://Padlet.Com/Bailbonds500Dvfnq/Bookmarks-F5Fmv6W61Ajdpe9I/Wish/Wkmoz57Vxgbpazma –
I’m Elvis (19) from Providence, United States.
I’m learning Spanish literature at a local university and
I’m just about to graduate.
I have a part time job in a college.
Stop by my homepage … web page
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ꮪtates
12394214912
Expertsinstall
เนื้อหานี้ อ่านแล้วเข้าใจง่าย ครับ
ผม เพิ่งเจอข้อมูลเกี่ยวกับ เนื้อหาในแนวเดียวกัน
ที่คุณสามารถดูได้ที่ Ginger
เผื่อใครสนใจ
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
และอยากเห็นบทความดีๆ
แบบนี้อีก
My blog post: bk88 – Ginger –
My family every time say that I am wasting my time here at net, however I know I am
getting familiarity daily by reading thes pleasant posts.
Review my website :: sihoki login
Great information. Lucky me I ran across your site by chance (stumbleupon).
I’ve saved it for later!
Also visit my homepage kc deck company
fastest muscle building supplements
References:
https://may22.ru/user/veilmouse19
Ijust wrote about how Jane decided to try Paybis to
move her money from her bank into crypto and
then straight into her trading account, and honestly, her whole story
turned out way more unexpected than anyone thought.
Jane isn’t your regular crypto newbie. Random detail: she collects tiny vintage
globes and has exactly 27 of them lined up behind her desk.
Another fun fact is that she can solve a Rubik’s cube
in under 40 seconds. So when she discovered Paybis, she approached it with the same energy — fast,
efficient, and determined.
She said, she wanted a platform that wouldn’t
“fight her back,” because her bank is already stressful
enough. Paybis ended up being perfect: smooth verification, easy deposit,
and she was able to convert her bank funds
into crypto in literally minutes. She laughed saying it was easier than ordering sushi.
Once the crypto hit her wallet, she jumped straight into her trading
platform — zero friction. And because she’s
Jane, she turned it into a personal speed-challenge.
She timed every step, and of course, she made a whole spreadsheet about it.
Little detail: she names her spreadsheets after
planets.
What surprised her most was how Paybis didn’t overwhelm her
with complicated menus. She likes things simple — after all, she once returned a coffee machine because it had “too many buttons.” So the
clean process from bank → crypto → trading felt like a win.
She mentioned that anyone wanting to try the same flow should check the link inside this comment,
but she didn’t want to make a big deal of it.
Just said it might be helpful.
In the end, Jane’s whole experience using Paybis was refreshingly easy,
surprisingly fun, and very “Jane-style” — structured, quirky,
and full of little experiments.
For anyone interested, she said the link in the comment explains everything
a bit deeper, but that’s totally optional.
Feel free to surf to my page information
Look into my blog post paris sportifs crypto
Superb, what a web site it is! This website presents valuable information to us, keep it
up.
my web page; 비아그라 구매
Nice respond in return of this issue with genuine arguments and explaining everything regarding that.
my web blog … 789club
Hello would you mind letting me know which webhost you’re working with?
I’ve loaded your blog in 3 completely different web browsers and I must say this blog loads
a lot quicker then most. Can you recommend a
good hosting provider at a reasonable price? Cheers, I appreciate
it!
Also visit my web site … 부산다이어트한의원
โพสต์นี้ น่าสนใจดี ค่ะ
ดิฉัน ไปเจอรายละเอียดของ หัวข้อที่คล้ายกัน
ที่คุณสามารถดูได้ที่ flik 234
ลองแวะไปดู
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
Amazing! Its actually amazing paragraph, I have got much
clear idea concerning from this article.
Feel free to surf to my blog game bài đổi thưởng
Hello! This is my first comment here so I just wanted to give a quick shout out
and say I truly enjoy reading through your blog posts.
Can you suggest any other blogs/websites/forums that cover the same topics?
Thanks a ton!
Feel free to surf to my blog post web site
Hello there! Quick question that’s totally off topic.
Do you know how to make your site mobile friendly?
My site looks weird when browsing from my iphone4.
I’m trying to find a template or plugin that might be able to resolve this problem.
If you have any recommendations, please share.
Thanks!
my page: keo nha cai
https://77ggg.br.com/
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, Unityed Ѕtates
12394214912
Refreshed
6bt59v
Really insightful post — I especially appreciated the depth of analysis here. Thanks for sharing this perspective. [a2dc3310]
I do not even know the way I ended up here, however I believed this post was good.
I don’t recognise who you are but certainly you are going to a famous blogger should you
are not already. Cheers!
Here is my blog :: купить эссе
This piece of writing provides clear idea in support
of the new visitors of blogging, that in fact how to do blogging.
Check out my web blog; 스포츠분석
I have fun with, cause I discovered just what I was having a look for.
You have ended my 4 day lengthy hunt! God Bless you man. Have
a great day. Bye
Stop by my website – best online casino slots
I like the helpful info you provide in your articles. I’ll bookmark your weblog and check again here regularly.
I am quite certain I will learn plenty of new stuff right here!
Good luck for the next!
Review my web site … MALWARE
Lucky Feet Shoes Redlands
602 Orange Ѕt Unit B,
Redlands, CΑ 92374, United Ѕtates
+19093079819
most comfortable shoes when standing all day
Hi there, I do think your site could be having browser compatibility
issues. Whenever I look at your site in Safari, it looks fine however,
if opening in IE, it’s got some overlapping issues. I just
wanted to give you a quick heads up! Aside from that, fantastic
website!
Review my homepage: https://iwin.trading/
Hmm is anyone else experiencing problems with the pictures on this blog
loading? I’m trying to find out if its a problem on my end
or if it’s the blog. Any responses would be greatly appreciated.
My blog post zgribulita101
Your mode of describing everything in this article is
genuinely good, all be able to easily be aware of it, Thanks a lot.
Take a look at my web blog: mix parlay
Every weekend i used to go to see this web site, for the reason that i wish for enjoyment, as this this web site conations
truly fastidious funny data too.
Visit my website: p448000
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Designconsult
I am regular reader, how are you everybody? This piece of writing posted
at this web page is in fact good.
My web-site fun88
Good day! Do you use Twitter? I’d like to follow you if that would be okay.
I’m undoubtedly enjoying your blog and look forward to new updates.
Also visit my page … online live casino
Link exchange is nothing else except it is simply placing the other person’s webpage link on your page at proper place and other person will also do same for you.
Feel free to visit my web blog SODO66
ZO88
Thanks for some other magnificent article. Where else could anybody get that type of info in such an ideal manner of writing?
I’ve a presentation subsequent week, and I am on the look for such info.
my webpage :: monetag platform guide
What’s Happening i am new to this, I stumbled upon this I’ve discovered It positively useful
and it has helped me out loads. I am hoping to give a contribution & aid different users like its aided me.
Good job.
Here is my site; zgribulita105
Modern Purair
416 Meridiian Ɍd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
furnace specialist
Greetings from Carolina! I’m bored at work so I decided to check out your site
on my iphone during lunch break. I love the information you
present here and can’t wait to take a look when I get home.
I’m surprised at how fast your blog loaded on my
phone .. I’m not even using WIFI, just 3G ..
Anyhow, very good blog!
Feel free to surf to my site Tf88
Лутран толпа экспресс-обзор
My site – источник
Pretty! This has been an incredibly wonderful post. Thank you for providing this information.
Also visit my page :: david hoffmeister reviews
This website was… how do I say it? Relevant!!
Finally I have found something that helped me. Cheers!
Feel free to visit my web site bokep indonesia
I have read so many articles about the blogger lovers except this piece of writing is truly a
pleasant paragraph, keep it up.
My site … homepage
CIR Legal Lexington
201 Ԝ Short St #500,
Lexington, KY 40507, United States
+18596366803
k&g lawyers
Top variations include Caribbean Stud Poker, Oasis Poker, no deposit casino netherlands Hold’em, and various video poker options.
Как выбрать качественное освещение для дома и участка
My blog; https://arcluce.ru
Casino Bonuses Betting Offers
Here is my web blog: https://romance-manga.com/an-informed-real-cash-casinos-on-the-internet-to-own-u-s-players-inside-2026/
Modern Purair
416 Merisian Ꮢd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
social impact
Franchising Path Carlsbad
Carlsbad, ⅭA 92008, United Stɑtes
+18587536197
4c framework conwulting – go.bubbl.us –
belka-digital
It’s perfect time to make a few plans for the future
and it is time to be happy. I have read this submit and if I may
just I wish to suggest you few fascinating things or
tips. Perhaps you could write next articles regarding this article.
I wish to read more things approximately it!
My blog post – Date de sortie Paradise saison 3
We stumbled over here by a different page and thought I should check
things out. I like what I see so now i’m following
you. Look forward to checking out your web page repeatedly.
My site; casino games online
I just could not leave your website before suggesting that I
extremely loved the usual information a person supply
for your guests? Is going to be back incessantly to check up
on new posts
Feel free to visit my site lemon casino bónusz
My brother recommended I might like this web site.
He was totally right. This post truly made my day.
You cann’t imagine just how much time I had spent for this info!
Thanks!
My web page: SC88
Hello there, I found your website by means of Google at the same time
as looking for a comparable subject, your site came up, it appears great.
I’ve bookmarked it in my google bookmarks.
Hi there, simply turned into aware of your weblog through Google,
and located that it is really informative. I am going to watch out for brussels.
I’ll appreciate if you continue this in future.
Numerous other people will probably be benefited out
of your writing. Cheers! http://whatsthecost.com/linktrack.aspx?url=https://rt.chat-rulet-18.com/pornstar
No matter if some one searches for his vital thing, so he/she wants to be available
that in detail, therefore that thing is maintained over here.
My web-site: ufa339
An outstanding share! I’ve just forwarded this onto a co-worker who had been doing a little research on this.
And he in fact bought me lunch because I discovered it for
him… lol. So allow me to reword this….
Thank YOU for the meal!! But yeah, thanks for spending the time to
discuss this topic here on your web site.
Психические патологии, неврология и зависимости
Feel free to surf to my blog post :: психиатрическая больница москва лучшая
Here’s a quick share of how Jane chose Paybis to shift
her money from her bank into crypto and then straight into her trading account, and honestly,
her whole story turned out way more entertaining than anyone thought.
Jane isn’t your regular crypto newbie. Fun fact: she collects tiny vintage globes and has exactly 27 of them lined up behind her desk.
Another fun fact is that she can solve a Rubik’s cube in under 40
seconds. So when she discovered Paybis, she approached it with the
same energy — fast, efficient, and determined.
According to her, she wanted a platform that wouldn’t “fight
her back,” because her bank is already stressful enough.
Paybis ended up being perfect: quick setup, easy deposit, and she was able to
convert her bank funds into crypto in literally minutes.
She laughed saying it was easier than ordering sushi.
Once the crypto hit her wallet, she jumped straight
into her trading platform — zero friction. And because she’s
Jane, she turned it into a personal speed-challenge.
She timed every step, and of course, she made a whole spreadsheet
about it. Little detail: she names her spreadsheets after planets.
What surprised her most was how Paybis didn’t overwhelm her with
complicated menus. She likes things simple — after all, she once returned a coffee
machine because it had “too many buttons.” So the clean process from bank → crypto
→ trading felt like a win.
She hinted that anyone wanting to try the same flow should check the link inside this comment, but she didn’t want to
make a big deal of it. Just said it might be helpful.
To sum it up, Jane’s whole experience using Paybis was refreshingly easy, surprisingly fun, and very “Jane-style” — structured, quirky,
and full of little experiments.
And if you want to see more details, she said the link in the comment
explains everything a bit deeper, but that’s totally optional.
My webpage … article
Busy Bee Jumpers
45 Main Ѕt 6Ⲥ, Wareham,
МA 02571, Unittes Stateѕ
508-514-2005
interactive inflatable rentals
Ahaa, its fastidious dialogue about this post here at this
web site, I have read all that, so now me also commenting at this place.
betflix 88
What a information of un-ambiguity and preserveness of
valuable know-how regarding unexpected emotions.
Look into my blog post: ليموزين شرم الشيخ
https://qq888.dev/
https://qq888.dev/
Hello from France. I’m glad to came across you.
My first name is Latasha.
I live in a small town called Ermont in western France.
I was also born in Ermont 36 years ago. Married in December 2003.
I’m working at the college.
My blog – website
Attractive portion of content. I simply stumbled upon your web site and in accession capital to claim
that I get in fact enjoyed account your weblog posts. Any way I will be subscribing for your
augment and even I fulfillment you access consistently quickly.
my web blog: Théories Paradise saison 3
Very nice post. I just stumbled upon your blog and wanted to mention that I’ve really loved browsing your weblog posts.
In any case I’ll be subscribing in your rss feed and I am hoping you
write once more soon!
Feel free to surf to my webpage تحميل 1xbet
I every time emailed this website post page to all my associates, for the reason that if
like to read it after that my contacts will too.
Here is my homepage – athlete
Its like you read my mind! You seem to know so much
about this, like you wrote the book in it or something.
I think that you could do with some pics to drive the message home a
bit, but instead of that, this is great blog.
A great read. I’ll certainly be back. pigpg slot
Very informative article! I found this useful.
Thanks for sharing this.
my webpage :: liveagentproplay88.com
Also visit my web blog: Bookmaker hors arjel
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ѕtates
12394214912
Handcrafted
Gangnam is one of the most industrialized and recognized
districts in Seoul, South Korea. Over time, numerous
terms have become very closely connected with Gangnam’s picture, including
Gangnam The King, Gangnam Meadow House, Gangnam Six, and Gangnam Mission.
Also visit my web blog cars (skyscanner-car-rental22211.blogsvirals.com)
Thanks for sharing such a pleasant idea, article is nice, thats
why i have read it fully
Here is my web blog – vape narkoba
광주룸싸롱에
대한 종합 정보 가이드입니다. 광주의 주요 룸싸롱 밀집 지역인 상무지구를 비롯한 지역별 특징, 룸싸롱 문화와
이용 방법, 가격 구조와 에티켓, 그리고
Ridiculous story there. What happened after?
Good luck!
Visit my website :: casino slots online
Please let me know if you’re looking for a author for your weblog.
You have some really great articles and I believe I would be a good asset.
If you ever want to take some of the load off, I’d absolutely love to write some articles for your blog in exchange for
a link back to mine. Please send me an email if interested.
Many thanks!
my web site – digi 995 corduroy hat
Today, while I was at work, my sister stole my iPad and tested to see if it can survive a forty foot drop,
just so she can be a youtube sensation. My apple ipad
is now broken and she has 83 views. I know this is entirely off
topic but I had to share it with someone!
Check out my web-site – purelumin essence
Definitely believe that which you stated. Your favorite justification appeared to be
on the internet the easiest thing to be aware of.
I say to you, I certainly get irked while people consider worries that they plainly do not know about.
You managed to hit the nail upon the top as well as defined out the
whole thing without having side effect , people can take a signal.
Will likely be back to get more. Thanks
Here is my webpage link bokep
Hi! I know this is kind of off topic but I was
wondering if you knew where I could find a captcha plugin for my comment
form? I’m using the same blog platform as yours and I’m having trouble finding one?
Thanks a lot!
Feel free to visit my web page – cialis
I am a Senior Enterprise Security Leader specializing
in AI-driven cybersecurity architecture, offensive security research, and large-scale security automation.
With extensive experience across enterprise environments, I focus on designing and
implementing advanced security strategies that combine artificial intelligence, automation,
and real-world adversarial simulation to strengthen organizational
resilience.
My expertise spans:
AI-powered threat detection and security analytics
Offensive security research and red team architecture
Enterprise SOC modernization and automation
Application and cloud security engineering
Large-scale vulnerability discovery and exploitation research
Security tooling and infrastructure design
I operate at the intersection of security engineering and AI innovation, building systems that not only detect threats but proactively
anticipate them.
Throughout my career, I have led complex security initiatives, architected enterprise-grade defensive frameworks,
and developed offensive methodologies that mirror real-world
attack behavior.
My mission is clear:
To elevate enterprise cybersecurity by integrating intelligent automation, strategic security leadership, and adversarial thinking.
If you are building next-generation security programs, exploring AI-powered defense, or modernizing enterprise
security operations – let’s connect.
Here is my page; Eliran Itzhak
Thanks for the insights. I’ve been looking into the TRON network
fees lately and it’s quite a challenge. Your
points about resource optimization on TRON are spot on. Looking forward
to more blockchain tips!
Look at my web site: tron energy satın al
https://8kbetvn.pro/
I like the helpful info you provide in your articles.
I’ll bookmark your blog and check again here frequently.
I’m quite certain I will learn a lot of
new stuff right here! Best of luck for the next!
Also visit my webpage: nitricboostultra
You need to take part in a contest for one of the finest blogs on the net.
I am going to highly recommend this website!
Check out my web blog Learn More Here
I think everything said made a great deal of sense.
But, what about this? suppose you added a little content?
I am not suggesting your content is not good, but what if you added a post title that makes people want more?
I mean Heel Pain – Plantar Fasciitis – Mr Will Edwards is a little plain.
You ought to peek at Yahoo’s front page and see how they create post headlines to grab viewers
interested. You might add a related video or a picture or two to grab readers excited about what you’ve got to
say. In my opinion, it might make your posts a little livelier.
My web-site – 科学的スキンバリア検査 韓国
I’m curious to find out what blog platform you are
utilizing? I’m experiencing some small security problems with my latest site and
I’d like to find something more secure. Do you have any suggestions?
my web-site: VSF Watches
Its like you read my thoughts! You appear to grasp a lot about this, such as you wrote the book in it or something.
I believe that you simply can do with a few percent to drive
the message home a little bit, however other than that,
that is wonderful blog. A great read. I will definitely be back.
Look at my web-site; vanity address generator trx
Great post. I was checking continuously this blog and I am impressed!
Extremely useful information particularly the last part :
) I care for such info much. I was looking for this particular info
for a very long time. Thank you and best of luck.
my web-site https://www.seoclerk.com/Link-Wheel/2523993/1000-Backlinks-from-Brazil-br-and-brazil-hosted-domains
Excellent post. Keep writing such kind of info on your blog.
Im really impressed by it.
Hey there, You’ve performed an incredible job.
I’ll definitely digg it and in my opinion recommend to my
friends. I’m sure they’ll be benefited from this web site.
Here is my homepage … 沖縄 消防設備
Hi, Neat post. There’s a problem together with your web site
in internet explorer, might check this? IE nonetheless is the market chief
and a big part of folks will leave out your wonderful writing
due to this problem.
Take a look at my web-site Buy best tufting gun
Terrific work! That is the type of information that should be
shared across the web. Disgrace on the seek
engines for now not positioning this submit higher!
Come on over and seek advice from my site . Thank you =)
my site :: dentist in lake park fl
Wow, this post is nice, my sister is analyzing these things,
thus I am going to convey her.
Feel free to visit my web blog – РедМетСплав предоставляет солидную линейку сертифицированных изделий из нестандартных материалов. Не важно
Как найти хорошие слоты онлайн
Here is my website: здесь
If some one desires expert view concerning blogging and site-building afterward i suggest him/her to pay
a quick visit this weblog, Keep up the pleasant work.
Also visit my homepage … advocate in delhi
When a business needs an SMS service, price is not the only thing that matters — real performance matters too.
A strong platform combines automation, analytics,
integrations, an intuitive interface, and compliance readiness.
These solutions work well for promotional campaigns, transactional notifications, and everyday customer communication. It is a practical choice for companies that
want to launch campaigns faster, simplify team workflows, and make communication more stable
and effective.
Also visit my web-site … http://juicy.iptime.org/board_XAde14/2069266
Everything is very open with a precise clarification of the challenges.
It was really informative. Your website is useful.
Many thanks for sharing!
Also visit my page 인천출장마사지
Busy Bee Jumpers
45 Main Տt 6C, Wareham,
MA 02571, Unites Ѕtates
508-514-2005
bounce House rental company near me
Anglų kalbos korepetitorius
overview
What’s up to all, it’s genuinely a fastidious for me to
go to see this website, it consists of important Information.
Have a look at my web blog: 188bet
https://s8casino.live
prohormones steroids
References:
https://oneal-sosa-2.technetbloggers.de/bodybuilding-workout-app-online-personal-trainer-bodybuilding-com
Hey there! This is my first visit to your blog! We are a group of volunteers and starting a new project in a community in the same niche.
Your blog provided us useful information to work on. You have done a extraordinary job!
Review my web page – Tx88
I read this article completely regarding the comparison of most recent and preceding technologies, it’s remarkable article.
My site osm.co.com lừa đảo công an truy nã cấm người chơi tham gia
Here is my web page :: Bookmaker hors arjel
Here’s a quick share of how Jane decided to try Paybis to shift her money from her bank
into crypto and then straight into her trading account, and honestly,
her whole story turned out way more fun than anyone thought.
Jane isn’t your regular crypto newbie. Random detail: she collects tiny vintage
globes and has exactly 27 of them lined up behind her desk.
Another random thing is that she can solve a Rubik’s cube in under 40 seconds.
So when she discovered Paybis, she approached it with the same energy — fast, efficient, and determined.
As she told me, she wanted a platform that wouldn’t “fight her back,
” because her bank is already stressful enough. Paybis ended up being perfect: smooth verification, easy deposit, and she
was able to convert her bank funds into crypto in literally minutes.
She laughed saying it was easier than ordering sushi.
Once the crypto hit her wallet, she jumped straight into her trading platform — everything
happening instantly. And because she’s Jane, she turned it into a personal
speed-challenge. She kept notes on each step, and of course, she
made a whole spreadsheet about it. Another fun fact: she color-codes everything in her life.
What surprised her most was how Paybis didn’t overwhelm her with complicated
menus. She likes things simple — after all, she once returned a coffee machine
because it had “too many buttons.” So the clean process from bank → crypto → trading
felt like a win.
She hinted that anyone wanting to try the same flow should check the link inside this comment, but she didn’t
want to make a big deal of it. Just said it might be helpful.
To sum it up, Jane’s whole experience using Paybis was
fast, surprisingly fun, and very “Jane-style” — structured, quirky, and full
of little experiments.
For anyone interested, she said the link in the comment explains everything
a bit deeper, but that’s totally optional.
My web blog – article
Hmm it appears like your site ate my first comment (it was extremely long) so I guess I’ll just sum it
up what I had written and say, I’m thoroughly enjoying your blog.
I as well am an aspiring blog blogger but I’m still new
to the whole thing. Do you have any helpful hints for first-time blog writers?
I’d definitely appreciate it. สล็อตเว็บตรง
I have been exploring for a little for any high quality articles or weblog posts on this kind of space .
Exploring in Yahoo I finally stumbled upon this web site.
Reading this info So i’m satisfied to express that
I have an incredibly just right uncanny feeling I found out exactly what I needed.
I such a lot for sure will make sure to don?t fail to remember this website and give it a look regularly.
Also visit my web site; situs video bokep indonesia
Hi, i feel that i saw you visited my site thus i got
here to go back the want?.I am attempting to
find things to improve my site!I suppose its adequate to use some of your ideas!!
Here is my web page постояное место работы
Woah! I’m really digging the template/theme of this website.
It’s simple, yet effective. A lot of times it’s hard to get that
“perfect balance” between user friendliness and
visual appeal. I must say you have done a fantastic job with this.
In addition, the blog loads extremely fast for me on Firefox.
Exceptional Blog!
Here is my site 8billion Yupoo Official
Rofena-D is a medication commonly used to relieve symptoms associated with allergic rhinitis, such as sneezing, runny or itchy nose, and
itchy or watery eyes. I
Read more
Example Sentences
How did professor flannery use curiosity wonder and questioning?
Asked by Anonymous
Professor Flannery utilized curiosity, wonder, and questioning as essential tools to engage students and foster a deeper understanding of complex topics.
By enc
Read more
Example Sentences
Which sentence best describes the historical concept of late antiquity introduced in Chapter 6?
Asked by Anonymous
The historical concept of late antiquity refers to a transformative period from
roughly the third to the eighth centuries, during which the Roman Empire experie
Read more
Example Sentences
What is a good grabber sentence for social network can jeopardize your data privacy?
Asked by Anonymous
“Think your social media posts are harmless? Think again—every photo, status update, and ‘like’ you share can expose your personal information and put your
Read more
Example Sentences
What is 10 examples of assertive sentence?
Asked by Anonymous
Here are ten examples of assertive sentences: The sun rises in the east. I enjoy reading books in my free time. She completed her project on time. They play so
Read more
Example Sentences
+1
What is a sentence for the word comosive?
Asked by Anonymous
“Comosive” isn’t a standard English word, but if you meant “combustive,
” a sentence could be: “The combustive nature of the chemicals r
Read more
Jobs & Education
+1
What is permitting specialized activity as subculture?
Asked by Anonymous
Permitting specialized activity as subculture refers to the acceptance and
encouragement of unique practices, interests, or lifestyles
within a larger societal
Read more
Example Sentences
How do you use blandishment in a sentence?
Asked by Anonymous
Blandishment refers to a flattering or coaxing speech intended to persuade someone.
For example, “Despite his initial reluctance, she used her charming bla
Read more
Example Sentences
What is a good replacement for the word because?
Asked by Anonymous
A good replacement for the word “because” is “since.” Other alternatives include “as,” “due to,” or “for the reason
Read more
Example Sentences
What is the use for Umecta?
Asked by Anonymous
Umecta is primarily used as a humectant in cosmetic and personal care formulations.
It helps to attract and retain moisture in the skin, making it beneficial fo
Read more
Example Sentences
How do you use the word monorail in a sentence?
Asked by Anonymous
The city plans to expand its transportation network by adding a new monorail system
that will connect the downtown area to the airport.
Passengers can enjoy a s
Read more
Example Sentences
How do you use norelco?
Asked by Anonymous
To use a Norelco electric shaver, first ensure it’s fully charged or plugged in. Start by cleaning
and preparing your skin, ideally with a pre-shave lotion if d
Read more
Example Sentences
Using the word scampered in a sentence?
Asked by Anonymous
The children scampered across the grassy field, their laughter
echoing in the warm afternoon sun. As the dog
chased after them, they squealed with delight, quic
Read more
Example Sentences
+1
What is a good sentencce using the word extravagantly?
Asked by Anonymous
The couple celebrated their anniversary extravagantly,
renting a luxurious yacht and hosting a lavish dinner party under the stars.
Their friends were awed by t
Read more
Example Sentences
What is the use of baebite?
Asked by Anonymous
Baebite is a digital platform designed to facilitate the
connection and interaction between users, often focusing
on social networking, dating, or community eng
Read more
Example Sentences
How often to use sevin?
Asked by Anonymous
Sevin, a brand of insecticide containing carbaryl, should typically
be used every 7 to 10 days as needed for effective pest
control. It’s important to follow th
Read more
Example Sentences
How do you create A sentence using interest group?
Asked by Anonymous
To create a sentence using “interest group,” you
might say: “The environmental interest group organized a rally to raise awareness about climate
Read more
Example Sentences
What is an example of a high modality word?
Asked by Anonymous
An example of a high modality word is “must.” High modality words convey strong certainty or obligation, indicating that something is necessary or una
Read more
Example Sentences
How do you use mummy and artisan in a sentence?
Asked by Anonymous
The skilled artisan meticulously crafted a beautiful vase, showcasing his talent and creativity. Meanwhile, the ancient mummy, perfectly preserved for centuries
Read more
Example Sentences
What problems seem to emerge when organization get larger?
Asked by Anonymous
As organizations grow, they often face challenges such as increased complexity in communication and coordination, leading to potential misunderstandings and ine
Read more
Example Sentences
How do you use causality in a sentence?
Asked by Anonymous
Causality refers to the relationship between cause and effect. In a sentence, you might say, “The researchers found a clear causality between increased exe
Read more
Example Sentences
How do you say outstanding teacher in one word?
Asked by Anonymous
The term “outstanding teacher” can be encapsulated in one word
as “educator.” This word encompasses not only teaching but also the qualities
Read more
Example Sentences
How many words compose an average sentence?
Asked by Anonymous
An average sentence in English typically contains around 15 to 20 words.
This can vary based on the writing style, context, and complexity of the
ideas being ex
Read more
English Language
+2
What is 4 compound words for teamwork?
Asked by Anonymous
Four compound words that relate to teamwork are “teamplayer,” “brainstorm,” “cooperation,” and “collaboration.” These
te
Read more
Example Sentences
When taking notes you should write in phrases using
only key words or terms?
Asked by Anonymous
When taking notes, writing in phrases using key words or terms
helps to capture essential information quickly and efficiently.
This method allows for easier rev
Read more
PreviousNext
Trending Questions
Where to put and in sentences? What sentence includes
vivid language that appeals to your sense? How do you use the word ‘receive’ in a sentence?
A sentence with the word teenager in it?
How can you use imploringly in a sentence? How do you use
pyromaniac in a sentence? What is the repetition of phrases or sentences with similar
structures or meanings is what? How can you use saunter
in a meaning-loaded sentence? Sentence with concensus in it?
What is a sentence for the word version? How would you use utopian in a sentence?
Can you give me a sentence using yours? What part of speech
is ‘yours’ in the sentence Yours was the best display at the science fair?
How do you use Afflatus in a sentence? How to make a sentence using separate?
What is a sentence for the word branches? Write a sentences in between 12 and 20 words giving details
of any medical condition that you and other members of your group may have?
What is an example fixation? How do you use the word coaster in a sentence?
How do you make sentence with flew?
Resources
Leaderboard All Tags Unanswered
Top Categories
Algebra Chemistry Biology World History English Language Arts
Psychology Computer Science Economics
Product
Community Guidelines Honor Code Flashcard Maker Study Guides Math Solver FAQ
Company
About Us Contact Us Terms of Service Privacy Policy Disclaimer Cookie Policy IP
Issues Cookie Settings
Copyright ©2026 Infospace Holdings LLC, A System1 Company.
All Rights Reserved. The material on this site can not be reproduced,
distributed, transmitted, cached or otherwise used, except with prior written permission of Answers. https://sakumc.org/xe/?document_srl=5115770
คอนเทนต์นี้ น่าสนใจดี ครับ
ดิฉัน เพิ่งเจอข้อมูลเกี่ยวกับ ข้อมูลเพิ่มเติม
สามารถอ่านได้ที่ Gustavo
ลองแวะไปดู
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
My homepage betflix199 (Gustavo)
Do you mind if I quote a few of your posts as long as I provide credit and sources
back gin rummy games to play your website?
My website is in the exact same area of interest as yours and my visitors would certainly benefit from some of the information you provide here.
Please let me know if this okay with you. Regards!
each time i used to read smaller posts which also clear their motive, and that is also happening with this
post which I am reading here.
Here is my blog: TopRankedWorld global directory
Article writing is also a fun, if you be familiar with then you can write otherwise it is difficult to write.
my web blog :: Slot VIP
Fantastic goods from you, man. I’ve take into account your stuff previous
to and you are simply extremely excellent. I actually like what
you’ve obtained here, certainly like what you are saying and the best
way by which you assert it. You are making it enjoyable and you continue to take care of
to keep it smart. I can’t wait to read much more from
you. That is really a great website.
my web page … hitclubcab
Thanks for every other excellent article. Where else may anyone get that kind
of information in such a perfect method of writing?
I have a presentation next week, and I’m on the search for such
info.
Look at my site: ChinaTime
Готовые стеновые панели для внутренних отделок:
практичное решение для смл с покрытием пвховременных
объектов
934gwd
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ѕtates
12394214912
Innovationkitchen
I am not positive where you are getting your info, however good topic.
I must spend a while studying much more or figuring out more.
Thanks for fantastic information I was looking for
this information for my mission.
My website Thelma
บทความนี้ อ่านแล้วเข้าใจง่าย ครับ
ผม ไปเจอรายละเอียดของ เนื้อหาในแนวเดียวกัน
สามารถอ่านได้ที่ รีวิว tigerwin369
ลองแวะไปดู
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ บทความคุณภาพ
นี้
และอยากเห็นบทความดีๆ แบบนี้อีก
Howdy! I know this is kinda off topic however I’d figured
I’d ask. Would you be interested in exchanging links or maybe
guest authoring a blog post or vice-versa? My website discusses a lot
of the same subjects as yours and I believe we could greatly benefit from each other.
If you happen to be interested feel free to shoot me an e-mail.
I look forward to hearing from you! Terrific blog by the way!
Here is my web blog; 22107553
I really like your blog.. very nice colors & theme.
Did you design this website yourself or did you hire
someone to do it for you? Plz answer back as I’m looking to create my own blog and would like to know where
u got this from. many thanks
Here is my web-site :: Rolex Submariner Replica
Wow! In the end I got a webpage from where I be able to truly take helpful
data concerning my study and knowledge.
Feel free to visit my homepage … voyance par téléphone
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Stаtes
254-275-5536
Installprocess
I just couldn’t depart your web site before suggesting that I extremely enjoyed the standard information an individual provide for your visitors?
Is gonna be back ceaselessly to check up on new posts
my web blog: zoolandia001
Thank you for the good writeup. It in fact was a amusement
account it. Look advanced to far added agreeable from you!
By the way, how can we communicate?
Review my page – Vin88
After exploring a handful of the blog articles on your blog, I truly
like your technique of writing a blog. I book marked it to my bookmark webpage list and will be checking
back in the near future. Please check out my website too and let me know how you feel.
Here is my web-site plumbing services Customer Service Number
I think this is one of the most significant information for me.
And i am glad reading your article. But should remark on some general things, The site style is ideal,
the articles is really great : D. Good job, cheers
Here is my website … betvisa app
This is a topic that is close to my heart…
Take care! Exactly where are your contact details though?
My webpage; custom mylar bags
Link exchange is nothing else but it is only placing the other person’s weblog link on your page at suitable place
and other person will also do similar in favor of you.
Also visit my web blog :: Exterminators My Area Customer Service Number
It’s an amazing paragraph in favor of all the online people; they will obtain advantage from it I am sure.
Feel free to visit my site – ultra k9 pro
Thanks for sharing your thoughts on baginda168.
Regards
What a material of un-ambiguity and preserveness of valuable know-how
on the topic of unpredicted emotions.
My site: May88
It’s in reality a great and helpful piece of info.
I’m glad that you simply shared this helpful info with us.
Please keep us up to date like this. Thank you for sharing.
Feel free to visit my web-site – best real estate agent in Cedar City UT
I just like the helpful info you supply in your articles.
I will bookmark your blog and check once more right here frequently.
I’m rather certain I’ll be told many new stuff proper
right here! Good luck for the following!
My website – Plumbing Phone Number 24/7
Woah! I’m really loving the template/theme of this blog.
It’s simple, yet effective. A lot of times it’s tough
to get that “perfect balance” between user friendliness
and visual appeal. I must say you have done a amazing job with this.
Additionally, the blog loads extremely quick for me on Firefox.
Outstanding Blog!
Look into my blog best online casino bonus
Hi, I log on to your blogs regularly. Your humoristic style is witty, keep
it up!
my web site acrylic shower systems wholesale
I have read so many posts concerning the blogger lovers however this
post is genuinely a fastidious paragraph, keep it
up.
Take a look at my site; real estate agent Downey CA
I’ll right away take hold of your rss feed as I can’t find your email subscription hyperlink or newsletter service.
Do you have any? Kindly let me recognise so that I may subscribe.
Thanks.
My web page; best realtor in Kingman AZ
Your method of explaining all in this paragraph is truly good, all can easily understand it, Thanks a lot.
My web page … baginda168
Wow, quel site incroyable Betify Casino !
Merci !
Betify Casino
Thank you a lot bathroom distributor for contractors sharing
this with all of us you actually know what you are speaking about!
Bookmarked. Please also visit my site =). We may have a hyperlink trade agreement
between us
I have been exploring for a little bit for any high-quality articles or blog posts in this kind of area .
Exploring in Yahoo I finally stumbled upon this site. Reading this information So i am satisfied to
convey that I’ve a very good uncanny feeling I discovered just what I needed.
I most indisputably will make sure to don?t overlook this site and provides it a glance on a relentless basis.
Also visit my blog :: real estate agent Las Vegas NV
This info is worth everyone’s attention. Where can I find out more?
My page :: email hosting api
This is very interesting, You’re a very skilled blogger.
I’ve joined your rss feed and look forward to seeking more of your magnificent post.
Also, I’ve shared your site in my social networks!
Here is my web-site – real estate agent in Acworth GA
Pretty section of content. I just stumbled upon your web site and in accession capital to assert that I get actually enjoyed
account your blog posts. Anyway I will be subscribing to your feeds and
even I achievement you access consistently fast.
Here is my webpage; baginda168
Hello just wanted to give you a quick heads up.
The words in your content seem to be running
off the screen in Opera. I’m not sure if this is a formatting issue or something to do with internet browser compatibility but I thought I’d post
to let you know. The style and design look great though!
Hope you get the problem solved soon. Kudos
Feel free to visit my webpage best real estate agent in Kingman AZ
This information is worth everyone’s attention. How can I find out more?
Look at my web site – best real estate agent in Downey CA
of course like your web-site but you have to test the spelling on quite a
few of your posts. Several of them are rife with spelling issues and I to
find it very bothersome to inform the reality on the other hand I will certainly come back again.
My web-site; baginda168
Excellent blog here! Additionally your site so much up fast!
What web host are you the use of? Can I get your affiliate link in your host?
I want my website loaded up as quickly as yours lol
My webpage gaking79
Peculiar article, exactly what I was looking for.
my webpage :: best realtor in Kingman AZ
Hi, I think your website might be having browser compatibility issues.
When I look at your blog site in Safari, it looks fine but
when opening in Internet Explorer, it has some overlapping.
I just wanted to give you a quick heads up!
Other then that, terrific blog!
Feel free to visit my page; wholesale bathroom supplier
Sweet blog! I found it while searching on Yahoo News. Do you have any suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Thank you
Feel free to surf to my homepage … imap email migration
If some one wishes expert view about blogging after that i recommend him/her to go to see this website, Keep up the pleasant job.
My homepage :: real estate agent Savage MN
Hey I know this is off topic but I was wondering if you
knew of any widgets I could add to my blog that automatically tweet
my newest twitter updates. I’ve been looking for a plug-in like this for
quite some time and was hoping maybe you would have some experience
with something like this. Please let me know if you run into anything.
I truly enjoy reading your blog and I look forward to your new updates.
My blog post: baginda168
Howdy I am so excited I found your site, I really found you by mistake, while I
was researching on Digg for something else, Nonetheless I am
here now and would just like to say thanks for a tremendous post and
a all round entertaining blog (I also love the theme/design), I don’t have time to read through it all at the moment but I have bookmarked it and also added in your RSS
feeds, so when I have time I will be back to read more,
Please do keep up the awesome b.
My web page; real estate agent in Acworth GA
Thank you a lot for sharing this with all folks you actually recognize what you’re talking about!
Bookmarked. Please also discuss with my web site =).
We can have a link alternate contract among us
my blog post: Velki Master Agent
It’s the best time to make some plans for the future and it’s time to be happy.
I have read this post and if I could I desire to suggest
you some interesting things or suggestions. Perhaps
you could write next articles referring to this article.
I desire to read more things about it!
Also visit my blog: best real estate agent in Las Vegas NV
Does your website have a contact page? I’m having a tough time locating
it but, I’d like to send you an e-mail. I’ve got some recommendations for your
blog you might be interested in hearing. Either way, great site and I look forward to seeing it improve over time.
My blog :: baginda168
Your mode of telling everything in this paragraph is really nice,
every one be capable of easily know it, Thanks a lot.
Also visit my blog post … real estate agent in Sarasota FL
Link exchange is nothing else but it is only placing the other person’s webpage link on your page at appropriate place and other person will also do same for you.
Here is my site: Velki Agent List
Amazing! Its really awesome paragraph, I have got much clear idea
about from this piece of writing.
Also visit my page :: Go88
An outstanding share! I’ve just forwarded this onto a co-worker who has been doing a little homework on this.
And he in fact ordered me lunch simply because I stumbled upon it
for him… lol. So allow me to reword this…. Thank YOU for the meal!!
But yeah, thanks for spending the time to discuss this subject here on your site.
Feel free to visit my web-site real estate agent in Acworth GA
After checking out a number of the blog posts on your web
site, I honestly like your way of blogging. I added it to my bookmark site list and will be checking back in the near future.
Please visit my website too and tell me your opinion.
My webpage real estate agent Downey CA
Your way of describing all in this post is actually
pleasant, every one be able to easily understand it, Thanks a lot.
my web blog تنزيل 1xbet
Every weekend i used to visit this web page, for the reason that i
want enjoyment, for the reason that this this web site conations really nice funny data too.
Visit my website … real estate agent in Acworth GA
Greetings, I do think your web site may be
having browser compatibility issues. When I look at your site in Safari, it looks
fine however, if opening in I.E., it has some overlapping issues.
I simply wanted to provide you with a quick heads up!
Aside from that, wonderful website!
Take a look at my site; realtor in Cedar City UT
Wow that was unusual. I just wrote an very long comment but
after I clicked submit my comment didn’t show
up. Grrrr… well I’m not writing all that over again. Anyways, just wanted to say wonderful blog!
Feel free to surf to my homepage real estate agent Kingman AZ
Touche. Outstanding arguments. Keep up the great spirit.
my blog post real estate agent Savage MN
I pay a visit every day some web pages and websites to read
posts, but this webpage presents quality based writing.
Have a look at my web blog; baginda168
Excellent blog post. I certainly love this site. Stick with it!
Feel free to surf to my blog … สล็อตเว็บตรง
Now I am ready to do my breakfast, after having my breakfast
coming over again to read further news.
My webpage … best real estate agent in Cedar City UT
If some one wants to be updated with most recent technologies
then he must be pay a visit this web page and
be up to date daily.
My web-site: best realtor in Charlotte NC
Good blog you’ve got here.. It’s hard to find high-quality writing like yours nowadays.
I seriously appreciate individuals like you! Take care!!
my web site; best real estate agent in Charlotte NC
Attractive component to content. I simply stumbled
upon your website and in accession capital to assert that I acquire in fact
enjoyed account your weblog posts. Any way I will be subscribing in your
feeds or even I success you get entry to consistently quickly.
Feel free to visit my blog post: best realtor in Cedar City UT
Hi there I am so thrilled I found your website, I really found you by
accident, while I was looking on Yahoo secure email hosting for business something else,
Anyways I am here now and would just like to say cheers for a fantastic
post and a all round entertaining blog (I also love the theme/design), I don’t have
time to browse it all at the moment but I have book-marked it and
also added in your RSS feeds, so when I have time I will be back to read much
more, Please do keep up the awesome work.
Attractive part of content. I simply stumbled upon your web site and in accession capital to assert that I get in fact loved account your blog posts.
Anyway I will be subscribing for your feeds
and even I achievement you get right of entry to constantly rapidly.
My homepage; acrylic shower manufacturer
each time i used to read smaller content that as well clear their motive,
and that is also happening with this paragraph which I am reading
at this place.
Also visit my site … managed smtp email hosting
Hi everybody, here every one is sharing these experience, thus it’s good to read this website, and I used
to visit this website every day.
Here is my blog :: payment gateway no1
I’m extremely pleased to uncover this web site.
I need to to thank you for ones time for this particularly wonderful read!!
I definitely savored every bit of it and I have you book-marked to check out new information in your web site.
Feel free to visit my website :: ร้านเหล้าฟีลคาเฟ่หาดใหญ่
obviously like your web site however you have to test the spelling on quite
a few of your posts. Many of them are rife with spelling problems and I find it very bothersome to inform the truth however I’ll surely come again again.
my blog post w 88
Good post! We are linking to this particularly great content on our website.
Keep up the good writing.
Feel free to surf to my blog post best real estate agent in Acworth GA
After I initially left a comment I appear to have clicked the -Notify me when new
comments are added- checkbox and now each time a comment is
added I recieve 4 emails with the same comment. Perhaps there is
a way you can remove me from that service? Appreciate it!
Also visit my web site; best real estate agent in Savage MN
Its like you read my mind! You appear to know so much about
this, like you wrote the book in it or something.
I think that you can do with some pics to drive the message
home a bit, but instead of that, this is fantastic blog.
An excellent read. I’ll certainly be back.
my blog: best real estate agent in Acworth GA
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Տtates
12394214912
Minimalist
Asking questions are genuinely fastidious thing if you are
not understanding something entirely, however
this piece of writing offers pleasant understanding even.
Feel free to visit my web page; best realtor in Las Vegas NV
I always used to read post in news papers but now as I am a user of internet thus from now I am using net for articles,
thanks to web.
My web blog … realtor in Sarasota FL
I was wondering if you ever thought of changing the page layout
of your website? Its very well written; I love what
youve got to say. But maybe you could a little more in the way of content
so people could connect with it better. Youve got an awful lot
of text for only having one or 2 pictures. Maybe you could space it out better?
My blog; real estate agent Las Vegas NV
I think this is among the such a lot important information for me.
And i am glad reading your article. But want to remark on some normal things, The website taste is wonderful,
the articles is really nice : D. Excellent activity, cheers
my web blog: best realtor in Downey CA
My developer is trying to persuade me to move to .net from
PHP. I have always disliked the idea because of the expenses.
But he’s tryiong none the less. I’ve been using Movable-type on several websites for about a year
and am concerned about switching to another platform. I have heard fantastic things about blogengine.net.
Is there a way I can import all my wordpress posts into it?
Any kind of help would be really appreciated!
Here is my web blog; realtor in Las Vegas NV
Thank you for every other wonderful post.
The place else may just anybody get that kind of info in such an ideal method of writing?
I’ve a presentation subsequent week, and I am on the look
for such info.
My web page realtor in Downey CA
It’s perfect time to make some plans for the future and it
is time to be happy. I have read this post
and if I could I wish to suggest you some interesting things or tips.
Maybe you could write next articles referring to this
article. I desire to read more things about it!
Stop by my web site; best real estate agent in Las Vegas NV
I loved as much as you will receive carried out right
here. The sketch is attractive, your authored subject matter stylish.
nonetheless, you command get got an nervousness over that you wish
be delivering the following. unwell unquestionably come further formerly again as exactly
the same nearly very often inside case you shield this hike.
Here is my web-site :: realtor in Charlotte NC
This site was… how do you say it? Relevant!!
Finally I have found something which helped me. Cheers!
Feel free to visit my website; best realtor in Savage MN
Pretty nice post. I just stumbled upon your blog and wanted to say that I have truly enjoyed surfing around your blog
posts. After all I will be subscribing to your feed
and I hope you write again soon!
Have a look at my page; real estate agent in Acworth GA
Its like you read my mind! You seem to know so much about this, like you
wrote the book in it or something. I think that you could
do with a few pics to drive the message home a little bit, but instead
of that, this is fantastic blog. An excellent read.
I’ll certainly be back.
Here is my web-site; サキュバス 服
I every time used to read paragraph in news papers but now as I am a user of net therefore from now I am using net for articles,
thanks to web.
Here is my web blog; best realtor in Las Vegas NV
Hey there, I think your blog might be having browser compatibility issues.
When I look at your website in Ie, it looks fine but when opening in Internet Explorer, it
has some overlapping. I just wanted to give you a
quick heads up! Other then that, fantastic blog!
Here is my web page; realtor in Sarasota FL
I am sure this post has touched all the internet users, its really really
good paragraph on building up new web site.
Check out my blog post :: real estate agent Kingman AZ
A motivating discussion is definitely worth comment.
There’s no doubt that that you ought to write more on this subject,
it might not be a taboo subject but generally folks don’t discuss these issues.
To the next! Best wishes!!
Here is my blog – best real estate agent in Savage MN
you can read it here: website you just have to sign up so you can read the full text.
there’s also Twilight, Eclipse and Breaking Dawn in the same website. http://43.143.175.54:3000/errolrossi4438/5899marketplace/wiki/dark-web-market-ransomware-kits
Can you tell us more about this? I’d like to find out more details.
Feel free to surf to my blog post :: best realtor in Charlotte NC
My relatives all the time say that I am wasting my time here at
net, except I know I am getting experience everyday
by reading such nice content.
Here is my site homepage
Wonderful work! This is the kind of information that are supposed to be shared across the internet.
Disgrace on Google for no longer positioning this post upper!
Come on over and seek advice from my site . Thanks =)
Look at my blog post – best realtor in Charlotte NC
안녕, 당신의 블로그에 브라우저 호환성 문제가 있는 것
같아요. Safari에서는 잘 보이지만, Internet Explorer에서 열 때
일부 겹침이 있습니다. 그냥 미리 알려드리고 싶었어요!
그 외에는 대단한 블로그입니다!
This site was… how do you say it? Relevant!! Finally I have found something
that helped me. Thanks!
Also visit my web blog 정품 비아그라 구매
This is the perfect webpage for everyone who really
wants to understand this topic. You know a whole lot
its almost tough to argue with you (not that I actually will need to…HaHa).
You definitely put a new spin on a topic that has been discussed for ages.
Excellent stuff, just excellent!
my website; best realtor in Acworth GA
Stunning story there. What happened after? Take care!
my web site – 먹튀제보사이트
best place to inject steroids
References:
md.inno3.fr
Quality content is the crucial to be a focus for
the visitors to visit the website, that’s what this web page is providing.
Look into my page – best realtor in Cedar City UT
Hi there i am kavin, its my first occasion to commenting anyplace, when i read this paragraph i thought i could also make comment
due to this sensible post.
Take a look at my blog … best real estate agent in Savage MN
Asking questions are really fastidious thing if you are not understanding something completely, except this article presents nice
understanding yet.
Feel free to visit my blog; Wellness Hills Mental Health
anabolic androgenic steroid
References:
https://www.hulkshare.com/greeksalary5
It’s remarkable in favor of me to have a web page,
which is beneficial designed for my knowledge.
thanks admin
My web page – best realtor in Savage MN
Very quickly this website will be famous amid all blogging and site-building people, due to it’s fastidious articles or reviews
Feel free to surf to my website: 선릉도파민
I have read so many articles or reviews regarding the blogger
lovers but this article is truly a pleasant post, keep it up.
Feel free to surf to my website :: best realtor in Cedar City UT
Great information. Lucky me I recently found your blog by chance (stumbleupon).
I have book marked it for later!
Also visit my webpage best real estate agent in Downey CA
This website truly has all of the information and
facts I needed about this subject and didn’t know
who to ask.
Also visit my site … nagadewa
Hello Dear, are you actually visiting this site regularly, if so afterward you
will without doubt obtain nice knowledge.
My web site … best real estate agent in Sarasota FL
Good post. I am dealing with a few of these issues as
well..
Feel free to surf to my webpage; best realtor in Charlotte NC
Excellent, what a web site it is! This website gives helpful
facts to us, keep it up.
My web site :: real estate agent Kingman AZ
It’s in point of fact a great and useful piece of information.
I’m happy that you shared this useful info with us. Please
stay us up to date like this. Thanks for sharing.
Visit my web site … real estate agent in Sarasota FL
Еxⅽellent goods from you, man. I’ve understand your stuff previous to and you are
juѕt extrеmelʏ great. I actually like what уou’ve acquired һere, cеrtɑinly like whаt үоu’re ѕaying and thе way in which
you say it. Ⲩou make it еnjoyable and you still care for tօ keep it sensible.
I can’t wait to read far more from yoᥙ. This is actually a tremendous web
ѕite.
mү web site; cheaters
This website was… how do I say it? Relevant!! Finally I’ve found something which helped me.
Kudos!
Feel free to surf to my web-site … real estate agent in Cedar City UT
I think this is one of the most significant information for me.
And i am glad reading your article. But want
to remark on some general things, The website style is ideal, the articles is really great
: D. Good job, cheers
Also visit my homepage: best real estate agent in Sarasota FL
Hey I know this is off topic but I was wondering if you knew of any widgets I could add to
my blog that automatically tweet my newest twitter updates.
I’ve been looking for a plug-in like this for quite some time and was
hoping maybe you would have some experience with something like this.
Please let me know if you run into anything. I truly enjoy reading your blog and I
look forward to your new updates.
My website :: best real estate agent in Kingman AZ
This is very interesting, You’re a very skilled blogger.
I’ve joined your rss feed and look forward to seeking more of your excellent post.
Also, I have shared your website in my social networks!
my blog real estate agent Las Vegas NV
It’s the best time to make some plans for the future and it is time to be happy.
I’ve read this post and if I could I want to suggest you few interesting things or suggestions.
Perhaps you could write next articles referring to this article.
I desire to read more things about it!
Feel free to surf to my homepage … realtor in Downey CA
Attractive element of content. I simply stumbled upon your weblog and in accession capital to
say that I acquire actually enjoyed account your blog posts.
Anyway I’ll be subscribing in your augment and even I achievement you
access constantly rapidly.
my webpage كازينو الإمارات العربية المتحدة
I like the helpful info you provide in your articles.
I’ll bookmark your blog and test again here regularly.
I’m slightly sure I will be informed plenty of new stuff proper here!
Best of luck for the following!
Here is my web site – realtor in Acworth GA
Лутран казино обзор
Also visit my website :: здесь
Hi to all, since I am genuinely keen of reading this website’s post to be updated daily.
It carries fastidious material.
My web page … realtor in Sarasota FL
I don’t even know how I ended up here, but I thought this post was
great. I don’t know who you are but certainly you’re going to a famous blogger if you aren’t
already ;) Cheers!
My web page: best real estate agent in Savage MN
Heya! I understand this is kind of off-topic however I had to ask.
Does managing a well-established website such as yours require a lot of work?
I’m completely new to blogging however I do write in my journal everyday.
I’d like to start a blog so I can easily share my own experience and feelings online.
Please let me know if you have any recommendations or tips
for brand new aspiring bloggers. Thankyou!
Here is my page; best realtor in Cedar City UT
When some one searches for his essential thing, so he/she desires to be available that in detail, thus that thing is
maintained over here.
Here is my web blog; best real estate agent in Savage MN
pill steroids for sale
References:
md.inno3.fr
It’s the best time to make some plans for the future and it
is time to be happy. I have read this post and if I could I want
to suggest you few interesting things or suggestions.
Perhaps you can write next articles referring to this article.
I want to read more things about it!
my web blog: best real estate agent in Las Vegas NV
Highly descriptive blog, I enjoyed that bit. Will there be a part 2?
Also visit my webpage … realtor in Cedar City UT
Aw, this was a very good post. Taking a few minutes and
actual effort to produce a great article… but what can I say…
I procrastinate a lot and don’t manage to get anything done.
Feel free to surf to my web blog – best realtor in Las Vegas NV
My spouse and I absolutely love your blog and find the majority of your post’s to be what precisely I’m looking for.
Would you offer guest writers to write content for you
personally? I wouldn’t mind publishing a post or elaborating on many of
the subjects you write related to here. Again, awesome website!
My website – best real estate agent in Downey CA
Hi there, i read your blog occasionally and i own a similar one and i was just curious if
you get a lot of spam comments? If so how do you reduce it, any plugin or anything you
can suggest? I get so much lately it’s driving me crazy so any help is very much appreciated.
Check out my webpage … best real estate agent in Charlotte NC
When some one searches for his required thing, therefore he/she desires to be available that in detail, thus that thing is maintained over here.
Also visit my homepage Ta88
Thanks to my father who informed me on the topic of this web site, this webpage
is in fact remarkable.
Feel free to surf to my blog – sex
Good day! This is my first visit to your blog! We are a team of volunteers and starting a new project in a community in the
same niche. Your blog provided us valuable
information to work on. You have done a extraordinary job!
My site – best real estate agent in Cedar City UT
Wow that was odd. I just wrote an extremely long comment but after
I clicked submit my comment didn’t show up.
Grrrr… well I’m not writing all that over again. Anyway, just
wanted to say superb blog!
Feel free to visit my website … sunwin
Sweet blog! I found it while searching on Yahoo News.
Do you have any tips on how to get listed in Yahoo News? I’ve been trying
for a while but I never seem to get there! Many thanks
Check out my web site – best real estate agent in Downey CA
Thanks for finally talking about > Heel Pain –
Plantar Fasciitis – Mr Will Edwards best real estate agent in Kingman AZ
I have read so many articles regarding the blogger lovers but this article is in fact a good piece of writing, keep it
up.
My web-site; best real estate agent in Savage MN
always i used to read smaller articles or reviews
which as well clear their motive, and that is also happening with this piece of writing which I am reading now.
Feel free to surf to my homepage – lop mam non
I have been surfing online more than 2 hours today, yet I never
found any interesting article like yours. It is pretty worth
enough for me. In my view, if all site owners and bloggers made good content as you did, the net will be a lot more useful than ever before.
Also visit my website … Hinchion Plumbing Customer Service Number
Someone necessarily lend a hand to make seriously articles I’d state.
This is the very first time I frequented your web page and thus far?
I surprised with the research you made to create this actual put
up extraordinary. Wonderful job!
Feel free to visit my web-site … best real estate agent in Kingman AZ
I am extremely inspired with your writing talents as
neatly as with the format in your blog. Is that this a paid subject matter or did
you customize it yourself? Anyway keep up the nice high quality writing, it is rare
to look a nice blog like this one nowadays..
Feel free to surf to my web site; realtor in Las Vegas NV
Hi there, I read your blog like every week.
Your humoristic style is witty, keep up the good
work!
my web blog; best realtor in Kingman AZ
I do not know whether it’s just me or if perhaps everybody else experiencing problems with your site.
It appears like some of the text in your content are running
off the screen. Can somebody else please provide feedback and let me know
if this is happening to them too? This could be a issue with my browser because I’ve had this happen previously.
Thank you
Feel free to surf to my page real estate agent in Sarasota FL
My spouse and I stumbled over here from a different page and thought I might check things out.
I like what I see so now i am following you. Look
forward to going over your web page for a second time.
Here is my blog … best realtor in Acworth GA
I quite like reading through an article that will make people think.
Also, many thanks for allowing for me to comment!
Also visit my web-site :: best real estate agent in Charlotte NC
Continuez comme ça et attirez encore plus de joueurs.
casino en ligne fiable
Hmm it appears like your website ate my first comment (it was super long) so I guess I’ll just
sum it up what I wrote and say, I’m thoroughly enjoying your blog.
I as well am an aspiring blog writer but I’m still new to the whole
thing. Do you have any points for inexperienced blog writers?
I’d definitely appreciate it.
My homepage – best realtor in Savage MN
Exceptional post but I was wanting to know if you could
write a litte more on this topic? I’d be very grateful
if you could elaborate a little bit more. Appreciate it!
Here is my web-site :: 스타렉스번호판
With havin so much content do you ever run into any problems of
plagorism or copyright infringement? My site has a lot of exclusive content I’ve either written myself or outsourced
but it seems a lot of it is popping it up all over the web without
my agreement. Do you know any methods to help prevent content from being ripped off?
I’d truly appreciate it.
My web site best realtor in Cedar City UT
Thanks for the marvelous posting! I seriously enjoyed reading it, you could be a great author.
I will make sure to bookmark your blog and will come back from now on. I want to encourage yourself to continue your great writing, have a nice day!
my web blog – best real estate agent in Downey CA
Hi this is kinda of off topic but I was wondering if blogs use WYSIWYG
editors or if you have to manually code with HTML.
I’m starting a blog soon but have no coding know-how so I wanted to get advice from
someone with experience. Any help would be enormously appreciated!
my page realtor in Cedar City UT
Good article. I certainly appreciate this website. Thanks!
Here is my blog: MALWARE
Hi there! Do you know if they make any plugins to protect against hackers?
I’m kinda paranoid about losing everything I’ve worked hard
on. Any tips?
Look at my blog – real estate agent in Acworth GA
Nice post. I learn something new and challenging on blogs I stumbleupon every day.
It’s always useful to read articles from other writers and use
a little something from their web sites.
My homepage real estate agent Downey CA
best legal alternative to steroids
References:
https://www.hulkshare.com/nationrake7
Hey There. I found your blog using msn. This is a really smartly written article.
I will be sure to bookmark it and return to read more of
your helpful info. Thank you for the post. I will definitely return.
Also visit my web site … https://az888.casa/khuyen-mai-az888/
I need to to thank you for this very good read!! I absolutely
loved every bit of it. I have got you bookmarked to check out new things you
post…
My web site realtor in Charlotte NC
Hmm it looks like your website ate my first comment (it was super long) so I guess
I’ll just sum it up what I had written and say, I’m
thoroughly enjoying your blog. I too am an aspiring blog writer but I’m still new to the whole thing.
Do you have any tips for rookie blog writers? I’d genuinely
appreciate it.
Here is my web site: Tx88
My partner and I stumbled over here coming from a different web page and thought I might as well check things
out. I like what I see so now i am following you.
Look forward to looking at your web page yet again.
Here is my blog post :: best realtor in Sarasota FL
A motivating discussion is definitely worth comment. I
do believe that you ought to publish more about this subject, it may not be a
taboo subject but usually people do not speak about
such issues. To the next! Cheers!!
my web blog 카지노커뮤니티
u88.com
I am extremely impressed with your writing skills as well as with
the layout on your weblog. Is this a paid theme or did you customize it yourself?
Anyway keep up the nice quality writing, it’s rare to see a great
blog like this one nowadays.
Feel free to visit my site best realtor in Las Vegas NV
This information is priceless. How can I find out more?
Feel free to visit my web blog; online casino free play
I think this is among the most important information for
me. And i’m glad reading your article. But wanna remark on few general things, The site style is perfect, the articles is really nice : D.
Good job, cheers
My webpage; realtor in Kingman AZ
Excellent beat ! I would like to apprentice at the same time as you amend your web site, how can i subscribe for a blog website?
The account helped me a acceptable deal. I were tiny bit familiar of
this your broadcast provided brilliant clear concept
Take a look at my blog post – best realtor in Savage MN
We’re a group of volunteers and starting a new scheme in our community.
Your website provided us with valuable info to work on. You’ve done an impressive job and our
whole community will be thankful to you.
Also visit my web site – real estate agent Kingman AZ
What’s up to all, since I am truly eager of reading
this website’s post to be updated regularly. It includes nice
data.
my web page; realtor in Charlotte NC
There’s certainly a great deal to learn about this topic. I love all the points
you made.
my blog – viagra indonesia
I think this is one of the so much significant info for me.
And i am glad studying your article. But want to commentary on few common issues,
The web site style is perfect, the articles is really excellent : D.
Just right job, cheers
my page :: realtor in Kingman AZ
Thanks for one’s marvelous posting! I certainly enjoyed
reading it, you will be a great author.I will ensure that I bookmark your blog
and will eventually come back later on. I want to encourage continue your great work,
have a nice evening!
Take a look at my webpage viagra indonesia
Hello there! I could have sworn I’ve been to your blog before but after browsing through some of the posts I realized it’s
new to me. Regardless, I’m certainly delighted I discovered it and I’ll be book-marking it and checking back often!
My website – best real estate agent in Downey CA
Cabinet IQ Fort Myers
7830 Drew Cir Stee 4, Fort Myers,
FL 33967, United Ⴝtates
12394214912
Bookmarks
Attractive section of content. I just stumbled
upon your weblog and in accession capital to assert that I get in fact enjoyed account your blog posts.
Any way I’ll be subscribing to your augment and even I achievement you access consistently
rapidly.
Also visit my web blog; real estate agent Kingman AZ
Its not my first time to pay a visit this website, i am visiting this web
page dailly and obtain nice data from here daily.
my page: realtor in Acworth GA
I am extremely impressed with your writing skills and also with the layout on your weblog.
Is this a paid theme or did you modify it yourself?
Either way keep up the excellent quality writing,
it’s rare to see a nice blog like this one these
days.
Feel free to visit my website :: realtor in Savage MN
This site was… how do I say it? Relevant!!
Finally I’ve found something that helped me.
Thanks a lot!
Here is my web blog; best realtor in Sarasota FL
Hi there, i read your blog from time to time and i own a similar one and
i was just wondering if you get a lot of spam
feedback? If so how do you protect against it, any plugin or
anything you can advise? I get so much lately it’s
driving me crazy so any support is very much appreciated.
my homepage … realtor in Acworth GA
I am not sure where you are getting your information, but great topic.
I needs to spend some time learning much more or
understanding more. Thanks for excellent information I
was looking for this information for my mission.
My page – real estate agent Downey CA
Valuable information. Fortunate me I discovered your web site accidentally, and I am stunned why this accident didn’t happened earlier!
I bookmarked it.
Here is my page; realtor in Charlotte NC
Good day! I know this is kinda off topic but I was wondering
if you knew where I could locate a captcha plugin for my comment form?
I’m using the same blog platform as yours and
I’m having difficulty finding one? Thanks a lot!
Here is my web-site: realtor in Acworth GA
Wonderful blog! I found it while surfing around on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Appreciate it
my page: realtor in Downey CA
Hey There. I found your weblog the usage of msn. This is an extremely neatly written article.
I will make sure to bookmark it and come back to learn more of your helpful info.
Thanks for the post. I will definitely comeback.
My web site 카지노커뮤니티
My partner and I stumbled over here by a different web page
and thought I might as well check things out.
I like what I see so i am just following you. Look forward
to looking at your web page for a second time.
Also visit my blog: best real estate agent in Downey CA
My programmer is trying to persuade me to move to .net from PHP.
I have always disliked the idea because of
the costs. But he’s tryiong none the less. I’ve been using Movable-type on a variety of websites for about a year
and am worried about switching to another platform.
I have heard good things about blogengine.net. Is there a
way I can transfer all my wordpress posts into it?
Any help would be really appreciated!
My web-site best real estate agent in Cedar City UT
Helpful info. Lucky me I found your web site by accident,
and I’m surprised why this twist of fate didn’t happened in advance!
I bookmarked it.
my blog 카지노커뮤니티
Hi, Neat post. There is an issue along with your site in web explorer, could check this?
IE nonetheless is the marketplace chief and a big portion of folks will omit your
excellent writing because of this problem.
Also visit my blog – Rhinoplasty Turkey
It’s really a great and helpful piece of info. I’m happy that you simply shared this useful information with us.
Please keep us informed like this. Thanks for sharing.
my blog; best real estate agent in Las Vegas NV
Hello There. I found your blog the usage of msn. That is a really
well written article. I will be sure to bookmark
it and return to learn more of your useful information. Thank you for the
post. I’ll definitely return.
Here is my homepage mainslot88
I’m not sure why but this blog is loading incredibly slow for me.
Is anyone else having this issue or is it a problem on my end?
I’ll check back later and see if the problem still exists.
Feel free to visit my page; real estate agent Kingman AZ
I think this is one of the such a lot significant info for me.
And i’m satisfied studying your article. However wanna observation on some basic things, The website taste is great, the articles is actually nice : D.
Good activity, cheers
My website – best real estate agent in Charlotte NC
Actually no matter if someone doesn’t know then its up
to other users that they will help, so here it takes place.
Feel free to surf to my blog post … vanity address generator
Paragraph writing is also a excitement, if you be acquainted with
after that you can write otherwise it is complicated to
write.
Check out my web-site: real estate agent in Cedar City UT
Bruk GPT på norsk for å finne svar, skrive tekster og løse oppgaver.
Trygg, smart og enkel AI-assistent tilgjengelig når
du trenger det.
Here is my blog :: ai chat norsk
Highly descriptive post, I enjoyed that bit.
Will there be a part 2?
my web page – real estate agent in Sarasota FL
My partner and I stumbled over here different page and thought I may as well check things out.
I like what I see so now i’m following you. Look forward to looking at your web page yet again.
Feel free to visit my webpage: best real estate agent in Cedar City UT
Hi there, I would like to subscribe for this weblog to obtain latest updates,
thus where can i do it please assist.
Also visit my web blog – real estate agent Charlotte NC
Very great post. I simply stumbled upon your blog and wished
to mention that I’ve truly loved surfing around your weblog posts.
In any case I’ll be subscribing on your rss feed
and I hope you write once more very soon!
Also visit my web-site; Lorna
Как выбрать гранитный памятник правильно
Here is my web blog … https://gdepamyatniki.ru/
Hi there colleagues, good post and fastidious urging commented at
this place, I am really enjoying by these.
Here is my homepage real estate agent in Cedar City UT
Greetings! Very helpful advice within this post! It is the little changes that will make the most important changes.
Thanks for sharing!
Feel free to visit my web-site: 강남가라오케
โพสต์นี้ มีประโยชน์มาก ครับ
ดิฉัน ไปอ่านเพิ่มเติมเกี่ยวกับ เนื้อหาในแนวเดียวกัน
สามารถอ่านได้ที่ Chara
น่าจะถูกใจใครหลายคน
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
my webpage; betflikkiss (Chara)
Have you ever considered about including a little bit more
than just your articles? I mean, what you say is important
and everything. However just imagine if you added some great
photos or video clips to give your posts more, “pop”! Your content is excellent but with images and video clips, this blog could definitely be one of the most
beneficial in its niche. Fantastic blog!
Here is my web site – Kristofer
Heya i’m for the first time here. I found this board
and I to find It really useful & it helped me out much. I hope to present one thing back and help others like you helped me.
My web blog :: real estate agent Charlotte NC
Nice post. I learn something totally new and challenging on sites I stumbleupon every day.
It will always be helpful to read through content from other authors
and use something from their web sites.
Also visit my web site :: realtor in Las Vegas NV
It’s awesome to pay a quick visit this website and reading the
views of all colleagues regarding this paragraph, while I am also keen of getting know-how.
Here is my blog post :: capital303
Nice post. I learn something totally new and challenging
on blogs I stumbleupon on a daily basis. It will always be helpful to read
content from other writers and use a little something from other web sites.
Visit my website best realtor in Acworth GA
Oh my goodness! Incredible article dude! Thank you, However I am experiencing issues with your RSS.
I don’t know why I am unable to subscribe to it. Is there anybody else having
identical RSS issues? Anybody who knows the solution can you kindly respond?
Thanks!!
Here is my web page … best real estate agent in Sarasota FL
Cool blog! Is your theme custom made or did you download it from somewhere?
A theme like yours with a few simple tweeks would really make my blog stand out.
Please let me know where you got your theme. Thanks a lot
Also visit my web blog :: Eldon
Undeniably imagine that which you stated. Your favourite reason appeared to be at the internet the simplest thing to keep in mind
of. I say to you, I definitely get annoyed at the same
time as folks consider concerns that they just don’t realize about.
You controlled to hit the nail upon the top and also outlined out the entire thing with no need side-effects
, folks can take a signal. Will likely be again to get more.
Thanks
my homepage: best realtor in Savage MN
33win
Shop authentic sports jerseys and save more when you
bundle! Get 30% OFF when you purchase 2 or more items
from Kyle’s Football Cards on Poshmark.
Excellente plateforme Betify Casino — j’adore la visiter !
https://wiki.cockos.com/wiki/api.php?action=https://lnkm.ee/81b31644
What a material of un-ambiguity and preserveness of valuable know-how on the
topic of unpredicted emotions.
Here is my blog … rikvip
This info is worth everyone’s attention. How can I find out more?
Feel free to surf to my page – rs485 cable (Hilda)
Wonderful beat ! I wish to apprentice whilst you amend your site, how
can i subscribe for a weblog web site? The account aided me a appropriate deal.
I have been a little bit acquainted of this your broadcast
offered bright clear concept
Also visit my blog :: 정품 비아그라
whoah this blog is wonderful i really like reading your articles.
Keep up the good work! You know, a lot of individuals are looking
round for this info, you could aid them greatly.
Feel free to visit my web page: capital303
Very good website you have here but I was wondering if you knew
of any community forums that cover the same topics talked about in this article?
I’d really like to be a part of community where I can get feed-back from other knowledgeable people
that share the same interest. If you have any recommendations, please let me know.
Thanks!
my web-site: MALWARE
Also visit my webpage Chicken Cross
I have been exploring for a little for any high-quality articles
or blog posts on this sort of space . Exploring in Yahoo I
ultimately stumbled upon this website. Studying this information So i’m glad to express that I have an incredibly just right uncanny feeling I found out exactly what I needed.
I so much indubitably will make certain to don?t fail to remember this website and provides it a glance
on a relentless basis.
Here is my site visa for egypt
injectable steroids kidney damage
References:
https://stackoverflow.qastan.be/?qa=user/heatpipe2
Thank you for every other great article. Where else may just anyone get that type of
information in such a perfect means of writing?
I’ve a presentation next week, and I’m at the search for such info.
my site – Hitclub
Minnətdaram belə faydalı məlumat üçün.
olimpbet
I will immediately grab your rss feed as I can not find your
e-mail subscription hyperlink or e-newsletter service.
Do you have any? Kindly allow me recognize so that I may just subscribe.
Thanks.
Also visit my webpage … pest control Company Customer Service Number
goGLOW Houston Heights
1515 Studemont Ⴝt Suite 204, Houston,
Texas, 77007, UЅA
(713) 364-3256
how To Get rid of Acne service
My brother suggested I may like this web site. He was once totally right.
This submit truly made my day. You cann’t consider simply how so much
time I had spent for this info! Thank you!
Visit my website kampung138
purchasing steroids online
References:
undrtone.com
what is anavar good for
References:
https://aryba.kg/user/modemincome9
Complete Ragnarok Online skill database with 1,100+ skills
including SP costs, cast times, cooldowns, damage formulas, and job class requirements.
Search by name, job, or skill type. View which
monsters and items use each skill. Essential reference for ragnarok
private server players and developers.
Also visit my blog post … ragnarok private servers
I have been surfing online more than 3 hours as of late,
but I never discovered any interesting article like yours.
It’s pretty price enough for me. In my view, if all website owners and bloggers made just right content
as you probably did, the net will probably be a lot more helpful than ever before.
my web site – stem cell clinic
It’s actually a cool and helpful piece of info.
I’m glad that you simply shared this useful info with us.
Please keep us up to date like this. Thanks for sharing.
Stop by my website … Best Indonesian Law Firm
Fabulous, what a blog it is! This blog gives helpful
data to us, keep it up.
my web blog – login kilat69
We’re a group of volunteers and opening a new scheme in our community.
Your web site provided us with valuable information to work on. You have done an impressive job and our whole community will be grateful to you.
My web blog … deck contractors austin tx
I loved as much as you will receive carried out right here.
The sketch is attractive, your authored material stylish.
nonetheless, you command get bought an shakiness over that you wish
be delivering the following. unwell unquestionably come more formerly again since exactly the same nearly very often inside case
you shield this increase.
Feel free to visit my blog post :: stem cell therapy thailand
goGLOW Houyston Heights
1515 Studemont Ѕt Suite 204, Houston,
Texas, 77007, USA
(713) 364-3256
skin rejuvenation cost natural
Useful info. Fortunate me I found your site accidentally, and I
am surprised why this coincidence didn’t came about in advance!
I bookmarked it.
Here is my web-site … login kilat69
best type of steroids
References:
vusr.net
where can i buy injectable steroids
References:
https://alushta-shirak.ru
Wow, this post is nice, my younger sister is analyzing such things,
therefore I am going to convey her.
My web page; concealed carry purse
Its like you read my mind! You appear to know so much about this, like you wrote the book
in it or something. I think that you can do with a few pics to drive
the message home a little bit, but other than that, this is excellent blog.
A fantastic read. I’ll definitely be back.
my web site Annapurna trail
Hello my family member! I want to say that this post is awesome, nice written and come with almost all important infos.
I’d like to peer extra posts like this .
Here is my blog post :: kaya303
steroids for bodybuilding
References:
illinoisbay.com
Having read this I thought it was very informative.
I appreciate you finding the time and effort to put this content
together. I once again find myself personally spending a lot of time
both reading and commenting. But so what, it was still worth it!
Feel free to visit my webpage … Tbilisi surrogacy clinic support
legal supplements that work like steroids
References:
https://marvelvsdc.faith/wiki/Buy_SustANON_250_Injection_Online_View_Uses_Side_Effects_Price_Substitutes
Профессиональная химия для клининга
— это основа качественной и эффективной уборки
в коммерческих и жилых помещениях.
В отличие от бытовых средств, такие составы обладают усиленной формулой, позволяющей быстро справляться с жиром, налётом, загрязнениями и бактериями.
Feel free to visit my web-site https://zetfail.ru/professionalnaya-himiya-dlya-klininga-vybor-pravila-i-prakticheskie-sovety.html
Have you ever considered publishing an ebook or guest authoring on other blogs?
I have a blog centered on the same topics you discuss and would really like to have you share some stories/information. I know my audience would appreciate your work.
If you’re even remotely interested, feel free
to shoot me an e-mail.
Here is my web-site; login kilat69
Hi there I am so delighted I found your webpage, I really found you by mistake, while I was browsing on Yahoo for something
else, Nonetheless I am here now and would just like to say thanks a lot for a fantastic post and a all round exciting blog
(I also love the theme/design), I don’t have time to read
it all at the minute but I have book-marked it and also added your RSS feeds,
so when I have time I will be back to read
more, Please do keep up the awesome job.
My blog madu pembesar kontol
crazy muscle three-atine
References:
https://pad.geolab.space/s/XlYdTv2Pl
my webpage; Chicken road argent
Excellent article. Keep writing such kind of information on your blog.
Im really impressed by your site.
Hello there, You have done an incredible job.
I will certainly digg it and personally suggest to my friends.
I am confident they will be benefited from this web site.
Feel free to visit my website – Aurelio
Борьба с англицизмами
Here is my blog; когда можно сказать по-русски
It’s enormous that you are getting ideas from this paragraph as well as from our
dialogue made at this time.
Here is my blog post lunatogel
Hello! I’m at work browsing your blog from my new apple iphone!
Just wanted to say I love reading your blog and look forward to all your posts!
Keep up the outstanding work!
Also visit my site – stage and set design Dubai
My family every time say that I am wasting my time here at net, except I know I
am getting experience daily by reading such fastidious articles.
Feel free to surf to my blog – luxury12
It’s amazing to pay a visit this web page and reading the views
of all colleagues about this piece of writing, while I am also zealous of getting knowledge.
Here is my blog post :: 해외선물 사이트
I like the helpful info you supply on your articles.
I will AFSkmark your weblog and test again here frequently.
I’m rather sure I’ll learn a lot of new stuff right here!
Good luck for the next!
Here is my web blog; AFS file structure
Asking questions are actually good thing if you are not understanding anything completely,
but this piece of writing gives good understanding yet.
Feel free to surf to my website: Jennifer
Hi! I realize this is somewhat off-topic but I had to ask.
Does building a well-established website such as yours take a
lot of work? I’m completely new to running a
blog however I do write in my journal every day.
I’d like to start a blog so I will be able to share my personal experience and feelings online.
Please let me know if you have any ideas or tips for new aspiring blog owners.
Thankyou!
Feel free to surf to my web blog – 나스닥100 선물
This is the right blog for anybody who really wants to find
out about this topic. You understand a whole lot its almost hard to
argue with you (not that I personally will need to…HaHa).
You certainly put a brand new spin on a topic that has been discussed for ages.
Wonderful stuff, just excellent!
Here is my web blog :: Comprar carnet de conducir
Hi! I know this is kind of off topic but I was wondering which blog platform are you
using for this website? I’m getting tired of WordPress because I’ve had problems with hackers and I’m looking at options for another platform.
I would be awesome if you could point me in the
direction of a good platform.
Stop by my blog :: 해외선물 안전업체
I’m more than happy to uncover this page. I want to to thank you for
ones time due to this fantastic read!! I definitely appreciated every bit of it and i also have you bookmarked to see new information on your blog.
Also visit my web site … 해외선물 안전업체
Howdy just wanted to give you a quick heads up. The
text in your post seem to be running off the screen in Ie.
I’m not sure if this is a formatting issue or something
to do with internet browser compatibility but I figured I’d
post to let you know. The design look great though! Hope you get
the issue fixed soon. Cheers
My webpage Leopoldo
It’s hard to find well-informed people on this topic,
but you sound like you know what you’re talking about! Thanks
Also visit my blog post :: 해외선물 실체결업체 추천
What’s Happening i am new to this, I stumbled upon this I have discovered It absolutely useful and
it has aided me out loads. I am hoping to give a contribution & aid other customers like its helped me.
Good job.
My blog post; wps官网下载
소액 결제(휴대폰 소액결제)는 온라인 가맹점에서 유료 콘텐츠나 물품 구매 시, 결제
대금을 [휴대폰 번호 인증을 통해 다음 달 휴대폰 요금에 합산하여 청구하는 결제 방식]입니다.
Hi mates, its impressive post on the topic of tutoringand completely defined, keep it up
all the time.
Also visit my webpage 해외선물 수수료
Hello There. I found your blog using msn. This is a very well written article.
I will make sure to bookmark it and come back to
read more of your useful information. Thanks
for the post. I’ll definitely return.
Also visit my homepage: 중고화물차
Appreciation to my father who told me regarding this web site, this
webpage is in fact remarkable.
My blog post 해외선물 대여계좌
My website Casino Extra online
If some one wants expert view on the topic of blogging and
site-building after that i suggest him/her to pay a visit
this blog, Keep up the good job.
Look into my web page :: world of poker
Hi, I do believe this is a great site. I stumbledupon it
;) I may revisit once again since I book-marked it.
Money and freedom is the greatest way to change, may you be
rich and continue to guide others.
my web site; 1MORE社のピストン型インイヤーイヤホン
Whoa! This blog looks just like my old one! It’s on a totally different topic but
it has pretty much the same page layout and design. Wonderful choice of colors!
Also visit my site; mellstroy com
I got this web site from my pal who informed me about this site and now this time I
am visiting this web site and reading very informative posts here.
Visit my homepage: 스포츠분석
Excellent web site. Lots of useful information here.
I’m sending it to some friends ans additionally sharing in delicious.
And of course, thank you for your sweat!
Visit my web blog – 카마그라 직구
Hey! I know this is kinda off topic nevertheless I’d figured I’d ask.
Would you be interested in trading links or maybe guest writing a blog article or vice-versa?
My blog goes over a lot of the same subjects as yours and I believe we could greatly benefit from
each other. If you might be interested feel free to shoot me an email.
I look forward to hearing from you! Awesome blog by
the way!
my website … file extension BDC
What’s up everyone, it’s my first go to see
at this site, and paragraph is actually fruitful in support of me,
keep up posting these articles or reviews.
my homepage: theyavue
And don’t forget to maintain an eye fixed out for power-ups, which can provide you an edge in your quest for cash. https://chicken-games.net/chicken-vs-zombies-battle-mechanics-2026/
Mangelsen
7916 Girard Avenue, ᒪa Joya
CA 92037, United Ⴝtates
1 800-228-9686
best 399 portrait oof А legend conservation (https://allmyfaves.com)
goGLOW Houston Heights
1515 Studemont Ⴝt Suite 204, Houston,
Texas, 77007, USA
(713) 364-3256
meet tһe team clinic (atavi.com)
goGLOW Houston Heights
1515 Studemont Ꮪt Suite 204, Houston,
Texas, 77007, UᏚA
(713) 364-3256
Bookmarks
market list is market list…….thank you http://sdkpod.efun.com/lynneast028714/mega-onion9234/-/issues/49
I was suggested this web site through my
cousin. I am now not certain whether this put up is written by means of
him as nobody else recognise such precise about my difficulty.
You are incredible! Thank you!
My webpage Hitclub
Good day I am so grateful I found your site, I really found you
by accident, while I was browsing on Google for something else, Anyhow I am here now and would
just like to say many thanks for a tremendous post and a all round exciting blog (I
also love the theme/design), I don’t have time to read through it all at the moment but I have bookmarked it and also added your RSS feeds, so when I have time I will be back to read a
great deal more, Please do keep up the great work.
Take a look at my web-site … slothunter-casino.org
I am really thankful to the holder of this site who
has shared this fantastic piece of writing at at this time.
Here is my website :: website
Open88
Hello just wanted to give you a quick heads up. The words in your content
seem to be running off the screen in Firefox.
I’m not sure if check this out is a format issue or something to do with web browser
compatibility but I figured I’d post to let you
know. The style and design look great though! Hope you get the issue fixed soon. Many
thanks
It’s actually a cool and useful piece of information. I am glad that you simply shared this useful info with us.
Please keep us up to date like this. Thanks for sharing.
Look at my blog :: 9bet
Hello, yeah this paragraph is genuinely fastidious and I have learned lot of things from it concerning blogging.
thanks.
Here is my web page; trusted cannabis shop
Bu saytdakı məlumatları oxumaqdan zövq alıram. Çox sağ olun!
Pinco Casino
goGLOW Houston Heights
1515 Studemont Ѕt Suite 204, Houston,
Texas, 77007, UЅA
(713) 364-3256
anti-aging treatments remedy
Nice blog right here! Also your web site a lot up very fast!
What web host are you the use of? Can I am getting your affiliate link for your host?
I desire my web site loaded up as fast as yours lol
my blog: bc game apk
Attractive section of content. I simply stumbled upon your blog and in accession capital to assert that I
acquire actually loved account your weblog posts. Any way I will be subscribing
on your augment or even I fulfillment you get
entry to consistently fast.
Feel free to visit my homepage; buy weed online canada
My family all the time say that I am wasting my time here at web, but I know I am getting knowledge every day by reading thes pleasant
content.
my site :: Roblox
Every weekend i used to pay a visit this web page, as i wish for
enjoyment, since this this site conations truly pleasant funny information too.
Review my page david hoffmeister reviews
Thank you for sharing your info. I truly appreciate your efforts and I will be waiting for your further post thank you once again.
Have a look at my page :: bukapintu
When I initially commented I appear to have clicked the -Notify me
when new comments are added- checkbox and from now on every time a comment is
added I receive 4 emails with the exact same comment.
There has to be an easy method you can remove me from
that service? Thanks a lot!
Here is my web-site :: surfdex.io lừa đảo công an truy nã cấm người chơi tham gia
Cabinet IQ
8305 Ꮪtate Hwwy 71 #110, Austin,
TX 78735, Unityed Ѕtates
254-275-5536
Topcontractors, padlet.com,
Minnətdaram belə keyfiyyətli məlumat üçün.
Pinco Casino sayt
It’s going to be end of mine day, except before finish I am reading this wonderful
paragraph to increase my experience.
Here is my web page – Roblox Executor
Great delivery. Solid arguments. Keep up the amazing work.
My page: Oxbet
I loved as much as you’ll receive carried out right here.
The sketch is attractive, your authored material stylish.
nonetheless, you command get bought an nervousness over that
you wish be delivering the following. unwell unquestionably come further
formerly again as exactly the same nearly a lot often inside case you shield this hike.
Review my webpage :: Slúchadlá Do Uší 1more Quad Driver
Mangelsen
7916 Girard Avenue, ᒪa Jooya
CA 92037, United Ѕtates
1 800-228-9686
Bookmarks; http://www.protopage.com,
Does your site have a contact page? I’m having a tough time
locating it but, I’d like to send you an e-mail. I’ve got
some ideas for your blog you might be interested in hearing.
Either way, great blog and I look forward to seeing
it expand over time.
Feel free to surf to my site :: คลิก
A person essentially assist to make significantly posts I might state.
That is the first time I frequented your website page and to this point?
I amazed with the research you made to create this particular submit extraordinary.
Wonderful process!
Visit my website Xem them
I’m gone to inform my little brother, that he should also pay a visit this weblog
on regular basis to obtain updated from newest
gossip.
My web page: 소액결제현금화
I got this web site from my friend who shared with me on the topic of this web site and now this
time I am browsing this website and reading very informative content here.
Here is my page :: แทงบอลออนไลน์
It’s very simple to find out any topic on net as
compared to textbooks, as I found this piece of writing at this site.
my webpage – Sex Doll Blog
I know this web page gives quality dependent posts and extra
material, is there any other web site which presents such things in quality?
Feel free to surf to my web site … situs bokep ********
Visit my page … meilleur Zahraniční sázkové kanceláře
Also visit my web-site – meilleur Chicken Road
чат арбитражников telegram
Here is my web blog срезали выплату партнерка
Southeast Financial Nashville
131 Belle Forest Cir #210,
Nashville, TN 37221, United Ѕtates
18669008949
Southeast Financial metrics
Hey there! Do you know if they make any plugins to protect against
hackers? I’m kinda paranoid about losing everything I’ve worked hard on. Any tips?
My web page: w 88
karangan bunga papan Semarang papan di
Semarang merupakan sebuah alternatif yang menyampaikan perasaan di
berbagai moment. Melalui gaya yang variatif dan ucapan yang
berbeda, bunga papan ini kerap digunakan untuk acara seperti pernikahan, ulang tahun, atau
event farewell. Adanya bunga papan ini bukan hanya memberikan estetika
pada event, tetapi juga menjadi alat untuk menyampaikan apa ingin diungkapkan kepada semua hadirin.
Cabinet IQ
8305 Statre Hwwy 71 #110, Austin,
TX 78735, Unted Տtates
254-275-5536
Practicalkitchen
Hi there, after reading this awesome post i am too delighted to share my know-how
here with colleagues.
Feel free to surf to my web site … bokep anak sd
Me gusta este sitio — claro y lleno de cosas geniales.
http://alt1.toolbarqueries.google.com.pk/url?q=https://marcadegol.com/2024/12/como-ganar-grandes-recompensas-en-sweet-bonanza/
Hi, its fastidious paragraph on the topic of media print, we all be aware of media is a great source of facts.
Feel free to surf to my web-site :: flowforce max
References:
Apex casino strazny
References:
http://gasi.kr/newsletter/?bmode=view&idx=7189726
Awesome! Its really remarkable article, I have got
much clear idea about from this piece of writing.
Also visit my web page; w 88
I read this article fully about the comparison of hottest and earlier
technologies, it’s amazing article.
Here is my web page handgun deals
Great blog here! Also your web site loads up very fast!
What host are you using? Can I get your affiliate link to your host?
I wish my web site loaded up as fast as yours lol
Feel free to visit my page магазин цікавих подарунків
You really make it seem so easy with your presentation but I find this topic
to be really something that I think I would never understand.
It seems too complex and extremely broad for me.
I’m looking forward for your next post, I will try to get
the hang of it!
Review my web site; Oxbet
Hey! Do you use Twitter? I’d like to follow you if that would
be ok. I’m absolutely enjoying your blog and look
forward to new updates.
Feel free to visit my website :: uncensoredai video
WOW just what I was searching for. Came here by searching
for soto
Visit my page Odprto Uho
WOW just what I was searching for. Came here by searching for toto12
Highly descriptive post, I loved that bit. Will there
be a part 2?
my web blog sport
I think the admin of this web site is in fact
working hard in favor of his web site, for the reason that here every material is quality
based information.
Also visit my site … order fulfillment automation
Вау, какой крутой сайт kazino olimp!
Благодарю!
https://melty-app.com/douhan/douhan-attention/
Thanks for finally writing about > Heel Pain – Plantar Fasciitis –
Mr Will Edwards fun88
Whether a lottery is a good idea depends on perspective.
Lotteries can be fun and exciting, offering a chance to
win big prizes with a small investment. However
Read more
Lotteries
How many employees in pcso?
Asked by Anonymous
As of my last update, the Philippine Charity Sweepstakes Office (PCSO) employs approximately 2,000 individuals.
However, this number can fluctuate due to variou
Read more
Lotteries
How do you mega project delivery?
Asked by Anonymous
Mega project delivery involves meticulous
planning, stakeholder engagement, and rigorous project management.
It typically includes defining clear objectives, es
Read more
Lotteries
What do you get if you have two matching numbers in take 5?
Asked by Anonymous
In the Take 5 lottery game, having two matching numbers typically means you’ve won a smaller prize.
The exact payout can vary depending on the specific rules of
Read more
Lotteries
Can you win PCH prizes without purchasing anything?
Asked by Anonymous
Yes, you can win Publishers Clearing House (PCH) prizes without making
a purchase. PCH offers free entry methods, such as entering through their website or send
Read more
Lotteries
Is legitimate tha lottery AIWC winners club in US?
Asked by Anonymous
The legitimacy of the Lottery AIWC Winners Club in the U.S.
is questionable and should be approached with caution. Many lottery-related clubs and schemes can be
Read more
Lotteries
Why does Tessie Hutchinson say the lottery was unfair?
Asked by Anonymous
Tessie Hutchinson claims the lottery is unfair because she feels that the process is arbitrary and lacks justice,
especially when her family is selected for the
Read more
Lotteries
Why does your lotto max receipt say prize amount not available check again later?
Asked by Anonymous
The message “prize amount not available, check again later” on your Lotto Max receipt typically means that the lottery system has not yet
processed th
Read more
Lotteries
What is a mega church?
Asked by Anonymous
A megachurch is typically defined as a Christian congregation that has a weekly attendance of 2,
000 or more worshippers. These churches often feature large, ela
Read more
Math and Arithmetic
+1
How much do you win on euro millions for 1 number and 2 lucky stars?
Asked by Anonymous
I won the $10million lottery jackpot twice within one year,
although it was not by my powers. I’m Wayne Murray from Brooklyn, i was very lucky to
contact Dr Luc
Read more
Lotteries
What does fvr stand for on the bottom of lottery ticket stand for?
Asked by Anonymous
On the bottom of a lottery ticket, “FVR” typically stands for “Final Validation Receipt.”
This indicates that the ticket has been validated
Read more
Georgia (US State)
+1
What is Georgia lottery tax id?
Asked by Anonymous
The Georgia Lottery Tax ID refers to the identification number assigned to
individuals or businesses for tax purposes related to lottery winnings in the state o
Read more
Lotteries
Who have won pch in California?
Asked by Anonymous
The Publishers Clearing House (PCH) has awarded numerous
winners across California over the years, but specific names and details about each winner
are generall
Read more
Lotteries
What does it mean scratch your own back?
Asked by Anonymous
The phrase “scratch your own back” means to do something that benefits yourself, often while
helping someone else in the process. It implies a mutual
Read more
Lotteries
What do you mean by online ticket booking?
Asked by Anonymous
i want to know about Oasis http://boiler.ttoslinux.org/shaneldowd1370/mega-fo2365/-/issues/15
I’m very pleased to discover this site. I wanted to thank you for your time for this wonderful read!!
I definitely liked every part of it and I have you saved to fav to look
at new things in your blog.
My web site … JBC file download
I feel this is among the most important info for me.
And i am glad studying your article. But should remark on some
basic things, The site style is ideal, the articles is in point of fact great : D.
Excellent activity, cheers
my website – rajatogel
Cabinett IQ
8305 Ѕtate Hwwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Bookmarks
telegram вот канал bongacams tokens
What’s up it’s me, I am also visiting this site on a regular basis,
this website is genuinely fastidious and the visitors are in fact sharing good thoughts.
my website: ANJING
Wow, ale świetna strona lemon casino! Dziękuję!
lemon casino
Hello! Someone in my Facebook group shared this site with us so I came
to check it out. I’m definitely enjoying the information. I’m bookmarking and will
be tweeting this to my followers! Superb blog and brilliant
design.
My web blog :: şarjlı dikey süpürge
Wow, fantastic blog structure! How long have you been blogging for?
you made running a blog look easy. The whole look of your website
is wonderful, as neatly as the content material!
Look at my web-site; rs485 cable (Mose)
Good article. I’m dealing with some of these issues as
well..
Here is my web site … mpored
I visited many sites however the audio quality
for audio songs existing at this website is really fabulous.
My web site: poker88
Very nice post. I just stumbled upon your blog and wished to mention that I have truly loved surfing around your weblog
posts. After all I’ll be subscribing in your feed and I am hoping you write once more soon!
Here is my web page – One88
Hi there to every , as I am in fact eager of reading
this web site’s post to be updated daily. It includes pleasant material.
Stop by my web blog Finn
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Fabrication
Миссия Фильм миссия невыполнима смотреть
Concert Attire Stamford
360 Fairfield Ave,
Stamford, CT 06902, United Ѕtates
+12033298603
Bookmarks
Useful info. Fortunate me I found your web site accidentally, and I’m
stunned why this coincidence didn’t took place in advance!
I bookmarked it.
Also visit my web-site automotive college in kl
Above All Foundafion Repair
119 E Turbo Ɗr, San Antonio,
TX 78216, United Ѕtates
12109203042
Base foundation fixing and stabilization service
Excellent blog here! Also your website loads up very fast!
What web host are you using? Can I get your affiliate link to your host?
I wish my web site loaded up as fast as yours lol
Here is my web-site :: poker88
Appreciate the recommendation. Let me try it out.
my web blog: Emergency Plumbing Customer Service Number
Southeast Financial Nashville
131 Belle Forest Cir #210,
Nashville, TN 37221, United Ѕtates
18669008949
NADA canoe value
Fantastic beat ! I wish to apprentice while you amend your website, how could
i subscribe for a blog web site? The account helped me a acceptable deal.
I had been tiny bit acquainted of this your broadcast offered
bright clear concept
Also visit my web site – 강남가라오케
Franchising Path Carlsbad
Carlsbad, ᏟA 92008, United States
+18587536197
how much to buy a franchise of mcdonalds
It’s actually a great and helpful piece of information. I’m
happy that you shared this helpful information with us.
Please stay us up to date like this. Thank you for sharing.
My site: business transformation office consultant
Inspiring quest there. What happened after?
Thanks!
Feel free to surf to my homepage download tiktoks high quality
Hi there Dear, are you in fact visiting this site regularly, if so after that you will
definitely take pleasant know-how. http://welcomepage.ca/link.asp?id=58~https://rt.chat-rulet-18.com/asian
I’m gone to inform my little brother, that he should also go to see this web site
on regular basis to obtain updated from hottest reports.
My site Janeen
Normally I do not read post on blogs, however I would like to say that this write-up very compelled me
to check out and do so! Your writing style has been surprised me.
Thanks, quite nice article.
my blog – porn blowjob
Touche. Sound arguments. Keep up the great effort.
Also visit my webpage … situs porno
hello!,I really like your writing very so much! percentage we be in contact extra about your post on AOL?
I need an expert on this space to solve my problem. May be that is
you! Looking ahead to look you.
Have a look at my page … betting
Hello, i feel that i saw you visited my blog thus i got here to
go back the favor?.I am attempting to to find things to improve
my web site!I assume its ok to use some of your ideas!!
My homepage: Porn
Hmm it appears like your website ate my first comment (it was extremely long) so I guess I’ll just sum
it up what I had written and say, I’m thoroughly enjoying your blog.
I as well am an aspiring blog writer but I’m still new to the whole thing.
Do you have any points for rookie blog writers?
I’d really appreciate it.
Here is my web site Managing Multiple Accounts
What’s Going down i’m new to this, I stumbled upon this I have found It positively useful
and it has helped me out loads. I hope to give a contribution & help other customers like its aided me.
Good job.
Look into my blog evisa
Hey there! This is my first visit to your blog! We are a collection of volunteers and starting
a new initiative in a community in the same niche. Your blog provided us
beneficial information to work on. You have done a extraordinary job!
Stop by my page – SCAMMER
C’est l’un des plus utiles casinos en ligne.
https://eco-optimum.com/typography-examples
Di Semarang, kebutuhan akan bunga segar tidak pernah berkurang,
terutama saat momen spesial berlangsung. Layanan florist Semarang
yang buka 24 jam di kota ini memberikan kemudahan bagi pelanggan yang ingin memesan bunga
kapan saja. Dengan adanya layanan ini, Anda tidak perlu khawatir jika mendadak membutuhkan hiasan bunga untuk momen tertentu, karena semuanya akan teratasi dengan cepat dan mudah.
Woah! I’m really digging the template/theme of this blog.
It’s simple, yet effective. A lot of times it’s tough to get that “perfect balance” between superb usability and
appearance. I must say you’ve done a superb job
with this. Also, the blog loads extremely fast for
me on Chrome. Outstanding Blog!
Here is my site: amzn
Rochester Concrete Products
7200 N Broadway Ave,
Rochester, MN 55906, Unitedd Ѕtates
18005352375
Driveway paving configurations
What’s up, this weekend is good for me, since this occasion i am
reading this great informative post here at my house.
my page; site scam
My family members all the time say that I am
wasting my time here at net, except I know I am getting
experience every day by reading such good content.
Also visit my web page – buy shrooms online canada
Good article. I’m dealing with some of these
issues as well..
Here is my blog … order shrooms online canada
This excellent website definitely has all the info I needed about this subject
and didn’t know who to ask.
Here is my web site website bokep
I know this if off topic but I’m looking into starting my
own weblog and was curious what all is required to get set up?
I’m assuming having a blog like yours would cost a pretty penny?
I’m not very web smart so I’m not 100% sure.
Any suggestions or advice would be greatly appreciated.
Thanks
Here is my webpage – fun88
Академия ЦАППКК — это онлайн-академия, предлагающая повышение квалификации для специалистов разных направлений.
Она ориентирована на современные знания,
востребованные на рынке
труда.
my webpage; тут
Hello, after reading this awesome paragraph i am as well delighted to share my experience here with colleagues.
My web-site – david hoffmeister reviews
Pretty nice post. I just stumbled upon your blog and wished
to say that I’ve really enjoyed surfing around your blog posts.
In any case I will be subscribing to your feed and I hope you write again very
soon!
My web site pharmacie
Do you have a spam issue on this blog; I also am a blogger,
and I was wondering your situation; we have
created some nice procedures and we are looking to exchange strategies with others,
why not shoot me an e-mail if interested.
my website: polish citizenship by descent
Hey there! This is kind of off topic but I need some advice from an established blog.
Is it very difficult to set up your own blog? I’m not very
techincal but I can figure things out pretty fast.
I’m thinking about creating my own but I’m not sure where to
start. Do you have any ideas or suggestions? With thanks
Look into my web site Managing Multiple Accounts
Hi there! This is my first visit to your blog!
We are a group of volunteers and starting a new project in a community in the
same niche. Your blog provided us valuable information to work on. You have done
a marvellous job!
My site: betslot88
Appreciating the persistence you put into your
blog and in depth information you present. It’s nice to come across a blog every once in a while that isn’t the same outdated rehashed
material. Great read! I’ve saved your site and I’m including your RSS feeds to my Google
account.
my web site :: order shrooms online canada
Superb, what a webpage it is! This website provides helpful facts to us, keep it up.
my web page :: situs jual beli narkoba
Its such as you read my mind! You appear to understand so much about
this, such as you wrote the e book in it or something. I think that you
just can do with some p.c. to drive the message home a little bit, however instead of that, this is wonderful blog.
A fantastic read. I’ll definitely be back.
My page; buy magic mushrooms online canada
I was suggested this blog by my cousin. I’m not sure whether this
post is written by him as no one else know such detailed about my trouble.
You are amazing! Thanks!
Here is my web site – trusted mushroom shop
A motivating discussion is definitely worth comment.
I believe that you ought to publish more on this topic, it might not be a taboo matter but usually folks don’t discuss these
issues. To the next! Kind regards!!
My blog post: buy magic mushrooms online canada
Boston Medical Ԍroup
3152 Red Hill Ave. Ste. #280,
Costa Mesa, СA 92626, United Ⴝtates
800 337 7555
average male penis
Awesome article.
Here is my blog 넘버사기번호판사기
Thanks for the auspicious writeup. It in fact was once a entertainment account it.
Glance complex to more delivered agreeable from you!
However, how can we be in contact?
Here is my page panen77
Hello there! This is my 1st comment here so I just wanted to give a quick shout out and tell you I really enjoy reading through your blog posts.
Can you recommend any other blogs/websites/forums that go
over the same subjects? Thank you!
Feel free to visit my homepage web site
Nice blog here! Also your web site lots up fast! What web host
are you using? Can I am getting your affiliate link to your host?
I want my website loaded up as quickly as yours lol
My webpage Olymp Trade Online
Good post however , I was wondering if you could write
a litte more on this topic? I’d be very grateful if you could elaborate a
little bit further. Appreciate it!
Stop by my homepage – situs jual beli narkoba
Greetings! I know this is kind of off topic but I was wondering if you
knew where I could locate a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having trouble finding one?
Thanks a lot!
Feel free to visit my web blog; porn
Thank you for another informative site. Where else may I get
that type of information written in such an ideal method?
I’ve a project that I am just now operating on, and I
have been on the look out for such information.
Also visit my website; VIPHOKI
Does your website have a contact page? I’m having problems
locating it but, I’d like to shoot you an email.
I’ve got some ideas for your blog you might be interested in hearing.
Either way, great site and I look forward to seeing it improve over time.
My web blog … 오피사이트
Bandar slot online deposit pulsa tanpa potongan terbaik di Indonesia.
Layanan 24 jam, proses deposit cepat, dan peluang menang tinggi.
Klik di sini untuk daftar dan main
Your style is unique in comparison to other folks I have read stuff from.
Thank you for posting when you have the opportunity, Guess I will just bookmark this page.
My website – Emergency Electrical Services
The other day, while I was at work, my cousin stole my iphone and tested to see if it can survive a thirty foot drop, just so she can be a youtube sensation. My
apple ipad is now broken and she has 83 views. I know this is totally off topic but
I had to share it with someone!
Also visit my blog post … more info
Jungle Driving School Omaha
4020 Ѕ 147th St, Omaha,
NE 68137,United States
14024170547
driving franchise business (https://www.instapaper.com)
Merci pour un contenu aussi utile sur Betify Casino et les jeux d’argent.
Betify Casino
I think this is one of the most significant information for me.
And i am glad reading your article. But want to remark on some general things, The web
site style is wonderful, the articles is really excellent : D.
Good job, cheers
Here is my page … шкаф на заказ
Here is my blog … Plinko online
Hurrah! At last I got a webpage from where I be able to truly
take useful facts concerning my study and knowledge.
Feel free to visit my web page; MEGAWIN288
Keep on writing, great job!
My homepage; win8xbet.com lừa đảo công an truy nã cấm người chơi tham gia
In today’s hyper-regulated, fragmented
digital ecosystem, “good marketing” is no longer a sufficient metric
for success. Today, true market leadership belongs to
those who can engineer predictable, scalable demand, those who build the entire mechanism that makes revenue
inevitable. This is the domain of Brandi S. Frye: a US-based performance marketing expert
specializing in Go-To-Market (GTM) strategy and end-to-end Demand Generation.
I’ve been surfing online more than 2 hours today, yet I never found any
interesting article like yours. It is pretty worth enough for me.
In my view, if all website owners and bloggers made good content as you did,
the internet will be a lot more useful than ever before.
Also visit my web blog joint vive
If you would like to improve your know-how simply keep visiting this site
and be updated with the hottest news posted
here.
Check out my webpage Bolagg
I pay a quick visit every day some web pages and sites
to read content, except this web site gives quality based articles.
Here is my blog post slon1 at
If you want to take much from this paragraph then you have to apply such techniques
to your won blog.
my web blog: 인천쓰리노
I all the time emailed this web site post page to all my contacts, because if like to
read it after that my links will too.
Here is my page – QQ88BET 1 Link Slot Terpercaya
Aw, this was an incredibly nice post. Taking the time and actual
effort to create a good article… but what can I say… I
hesitate a lot and never manage to get anything done.
my site … MEGA55
This is my first time pay a visit at here and i am actually
happy to read all at alone place.
Feel free to visit my website; MALWARE
Spot on with this write-up, I truly believe that this amazing site needs
much more attention. I’ll probably be back again to see more, thanks for the info!
Check out my web blog facial
After looking at a few of the articles on your web site, I truly appreciate your way of blogging.
I saved as a favorite it to my bookmark webpage list
and will be checking back soon. Take a look at my web site too and
let me know your opinion.
my site; Water Damage Repair
Definitely consider that which you stated. Your favourite justification seemed to be at the internet the easiest factor to take into account of.
I say to you, I certainly get annoyed at the same time
as other folks think about worries that they just don’t
know about. You managed to hit the nail upon the highest as well as defined out the whole thing
without having side effect , other people could take a signal.
Will likely be again to get more. Thank you
Feel free to surf to my web page :: 소액결제 현금화
Link exchange is nothing else except it is only placing the other person’s blog
link on your page at suitable place and other person will also do same
in favor of you.
Feel free to visit my page :: MALWARE
This is a topic that’s near to my heart… Many thanks!
Exactly where are your contact details though?
My web site: 여기여
Hey just wanted to give you a quick heads up. The text in your article seem to be running off the screen in Internet explorer.
I’m not sure if this is a formatting issue or something to do with web browser compatibility but I figured I’d post to let you know.
The design and style look great though! Hope you get the issue resolved soon. Cheers
my webpage: MEGAHOKI
Quality articles or reviews is the crucial to interest the users to pay a visit the web site, that’s what this web page is
providing.
Visit my web site MALWARE
After I originally left a comment I seem to have clicked the -Notify me when new comments are added- checkbox and
now every time a comment is added I recieve 4 emails with the exact same comment.
There has to be an easy method you can remove me from that
service? Many thanks!
My blog post – site
Wow, incredible blog layout! How long have
you been blogging for? you make blogging look easy. The overall look of your site is fantastic,
as well as the content!
my site – Tualatin Pest Control
It’s actually a nice and useful piece of information. I’m glad that you just shared this useful info
with us. Please stay us up to date like this.
Thank you for sharing.
Also visit my web page; MALWARE
This paragraph will help the internet viewers
for setting up new webpage or even a weblog from start to end.
Here is my web site … kaya303
Глонасс для РНИС
my homepage; Контроль транспорта
Hello! I’ve been reading your web site for some time now
and finally got the bravery to go ahead and give you a shout
out from Dallas Texas! Just wanted to say keep up
the good job!
My web-site Data Sdy
Hey there! Someone in my Myspace group shared this website with us so I came to
look it over. I’m definitely loving the information. I’m bookmarking and will
be tweeting this to my followers! Wonderful blog and fantastic
design and style.
Feel free to visit my blog … Shaunte
Kyle’s Football Cards is a trusted online store for
authentic sports jerseys and collectibles, featuring
NFL, NBA, MLB, NHL, and NCAA gear from top brands like Nike and adidas.
Shop rare and hard-to-find jerseys with fast shipping and reliable service.
Whether you’re a fan or collector, find premium jerseys at competitive prices.
Use code KYLEFAN30 to get 30% OFF sports jerseys today.
Review my page: Kyle’s Cards
Appreciate the recommendation. Let me try it out.
my blog post; poker88
Yes! Finally someone writes about Click here.
Feel free to visit my blog … Visit here
web11 refer code app and Web11
fantasy app evaluation for India users
Vous proposez du matériel utile sur Betify Casino.
avis Betify Casino
Excellent post. I used to be checking constantly this weblog and I’m
inspired! Extremely useful information specifically
the ultimate part :) I take care of such information much.
I used to be looking for this certain information for a very long time.
Thank you and good luck.
Here is my blog :: real cash online casino
Outstanding story there. What happened after?
Thanks!
my blog Luva Bet Quantos Saques Por Dia
Hi! I could have sworn I’ve been to this site
before but after checking through some of the post I
realized it’s new to me. Nonetheless, I’m definitely
happy I found it and I’ll be bookmarking and checking back often!
Feel free to surf to my homepage … Dewapoker
I needed to thank you for this excellent read!!
I definitely loved every bit of it. I have got you bookmarked to check out new things you post…
Also visit my web-site Togel Online
소액결제현금화 전문 상담! 휴대폰소액결제현금화, 정보이용료현금화, 콘텐츠이용료현금화 업계 최저 수수료로 3분 내 즉시
입금. 24시간 365일 안전한 정식 사업자.
Someone essentially help to make seriously posts I would state.
This is the very first time I frequented your website
page and to this point? I surprised with the analysis you made to create this particular post extraordinary.
Fantastic job!
Also visit my site: Jai Club
Excellent post. I was checking constantly this blog and I am impressed!
Very useful information specifically the last part :) I
care for such info a lot. I was seeking this certain info
for a long time. Thank you and good luck.
Feel free to surf to my site crypto alpha telegram
Valuable info. Fortunate me I discovered your web site by accident, and I’m surprised why this accident didn’t came about earlier!
I bookmarked it.
Here is my website: 인천쓰리노
I like the valuable information you provide in your articles.
I’ll bookmark your blog and check again here frequently.
I’m quite certain I will learn lots of new stuff right here!
Good luck for the next!
my blog :: klinika za zdravljenje odvisnosti
If some one desires to be updated with latest technologies
therefore he must be go to see this site and
be up to date all the time.
My blog post; casino games that pay real money with no deposit
เนื้อหานี้ ให้ข้อมูลดี ครับ
ดิฉัน เพิ่งเจอข้อมูลเกี่ยวกับ ข้อมูลเพิ่มเติม
สามารถอ่านได้ที่ betflik
สำหรับใครกำลังหาเนื้อหาแบบนี้
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ เนื้อหาดีๆ
นี้
และอยากเห็นบทความดีๆ แบบนี้อีก
mrkt telegram skins cs2
Wow! Finally I got a weblog from where I be able to really obtain valuable data concerning
my study and knowledge.
Here is my web site; join crypto signals group
Please let me know if you’re looking for a article writer
for your site. You have some really good articles and I believe I would be a good asset.
If you ever want to take some of the load off, I’d really like to write some material for
your blog in exchange for a link back to mine.
Please shoot me an email if interested. Thanks!
Here is my web page … Festival Location Japan
Patrice & Associates
Scottsdale, AZ, United Ѕtates
16265237726
drive thru hiring
Thanks for the good writeup. It actually was a leisure account it.
Glance complicated to far added agreeable from you!
By the way, how can we communicate?
Here is my web page :: Jai Club
This excellent website truly has all the info I wanted about this subject and didn’t
know who to ask.
Also visit my web site :: MALWARE
Hi! Quick question that’s entirely off topic. Do you know how to make your site mobile friendly?
My site looks weird when viewing from my iphone4.
I’m trying to find a theme or plugin that might be able to fix this problem.
If you have any suggestions, please share. Appreciate it!
Visit my blog post: VK88
Great goods from you, man. I have understand your stuff previous to and you’re just too magnificent.
I really like what you’ve acquired here,
certainly like what you’re stating and the way in which you say it.
You make it entertaining and you still care for to keep it sensible.
I can’t wait to read much more from you. This is actually a wonderful web site.
My website … mega2ooyov5nrf42ld7gnbsurg2rgmxn2xkxj5datwzv3qy5pk3p57qd.onion
In the Uk, experienced players use it to chase rare however meaningful wins. https://mineslot2.org/login/
Today, I went to the beach with my children. I found
a sea shell and gave it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She placed
the shell to her ear and screamed. There was a hermit crab inside and it pinched her ear.
She never wants to go back! LoL I know this is completely off topic
but I had to tell someone!
Check out my blog post – bethoki77
Fabulous, what a web site it is! This web site gives helpful information to us, keep it
up.
Also visit my webpage … jual putau
Hi there it’s me, I am also visiting this web site daily, this web site is actually fastidious and the people are
actually sharing nice thoughts.
Also visit my blog post :: pepek
Hi to all, how is everything, I think every one is getting more from this web site, and your views are pleasant in support of new people.
Also visit my site – obor138
Hello everyone, it’s my first pay a quick visit at this web page,
and article is really fruitful for me, keep up posting such
articles.
Here is my blog … Buy Aged Reddit
Thanks for another informative site. Where else may just I am getting that type of information written in such a perfect
method? I’ve a challenge that I am just now running on, and I’ve been at the glance out for such
information.
my blog; idncash
whoah this weblog is magnificent i really like reading your articles.
Stay up the good work! You already know, a lot of individuals
are looking around for this info, you can aid them greatly.
My web site – More information
Thanks a bunch for sharing this with all people you actually recognise what
you’re talking about! Bookmarked. Please additionally seek advice from my web site
=). We could have a link exchange arrangement between us
My website: dewabet
References:
High limit blackjack
References:
https://graph.org/Best-Online-Casinos-Ranked-04-20
Hey! This is kind of off topic but I need some help from an established blog.
Is it tough to set up your own blog? I’m not very techincal
but I can figure things out pretty quick. I’m thinking about creating my
own but I’m not sure where to start. Do you have any ideas or suggestions?
With thanks
Review my web site; Barz Casino
Southeast Financial Nashville
131 Belle Forest Cir #210,
Nashville, TN37221, United Ⴝtates
18669008949
NADA hybrid car value
Can you tell us more about this? I’d love to find out more details.
Also visit my webpage: control cable (Mallory)
Hi there! Do you know if they make any plugins to assist with Search Engine Optimization? I’m trying to get my blog to rank for some targeted keywords but I’m not seeing very good
gains. If you know of any please share. Cheers!
Here is my web site … SlotsMillion Casino
For latest news you have to pay a quick visit the web
and on world-wide-web I found this web site as a finest
site for hottest updates.
my web blog; BRITISH SHORTHAIR KITTENS FOR SALE
Hello there, You have done a fantastic job. I’ll certainly digg it and personally recommend to my friends.
I am sure they’ll be benefited from this site.
My web site vanity tron token
Thanks for one’s marvelous posting! I certainly enjoyed
reading it, you’re a great author.I will make
sure to bookmark your blog and definitely will come back later on. I want to encourage
yourself to continue your great writing, have a nice weekend!
My web blog :: domino88
Greetings! I know this is kind of off topic but I was wondering if you knew where I
could find a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having problems finding one?
Thanks a lot!
Here is my website: non surgical nose job austin
Hi there, just became aware of your blog through Google,
and found that it’s truly informative. I am going to watch out for brussels.
I’ll appreciate if you continue this in future.
Numerous people will be benefited from your writing.
Cheers!
Take a look at my page: review software
ข้อมูลชุดนี้ มีประโยชน์มาก ครับ
ดิฉัน ไปอ่านเพิ่มเติมเกี่ยวกับ หัวข้อที่คล้ายกัน
ดูต่อได้ที่ คาสิโนออนไลน์
เผื่อใครสนใจ
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
Thanks for finally talking about > Heel Pain –
Plantar Fasciitis – Mr Will Edwards Chicos Outlet
Hello there! I could have sworn I’ve been to this site before but after reading through some of the post I realized it’s new to
me. Anyhow, I’m definitely glad I found it and I’ll be bookmarking and checking back often!
Here is my web-site reviews app
Hey there, You have done a fantastic job. I will certainly digg it and personally recommend to my friends.
I am sure they’ll be benefited from this site.
Here is my web page … 부산오피
You could certainly see your enthusiasm within the article you write.
The arena hopes for even more passionate writers such as you who aren’t afraid to mention how they
believe. All the time follow your heart.
Also visit my site; 인천출장마사지
It’s perfect time to make a few plans for the longer term and
it’s time to be happy. I’ve read this post and if I could I desire to recommend you few interesting issues or tips.
Maybe you could write next articles regarding this article.
I wish to learn more things approximately it!
My blog post Emergency Water Damage Restoration
This is my first time pay a visit at here and i am genuinely pleassant to read all at alone place.
Also visit my blog :: get more reviews
Having read this I believed it was rather enlightening. I appreciate you finding the
time and energy to put this informative article together. I once again find myself personally spending way
too much time both reading and posting comments.
But so what, it was still worth it!
Here is my site; Pest Control in Oregon
Yes! Finally something about minibus hire.
my blog post; 30 seater mini bus
Hi there, I discovered your website by means of Google even as searching for a comparable topic, your website
got here up, it appears good. I have bookmarked it in my google bookmarks.
Hi there, simply turned into aware of your weblog via Google, and located that it’s truly informative.
I am gonna be careful for brussels. I’ll appreciate when you continue this in future.
Lots of other people might be benefited from your writing.
Cheers!
Also visit my site – MALWARE
References:
Crown-casino-online-slots-machines
References:
https://graph.org/Casino-Online-Your-Ultimate-Gaming-Guide-04-20
Hi there I am so excited I found your site, I really found
you by accident, while I was researching on Yahoo for something else, Regardless I am here now and would just
like to say thanks a lot for a incredible post and a all round thrilling blog (I
also love the theme/design), I don’t have time to read through it
all at the moment but I have bookmarked it and also
added in your RSS feeds, so when I have time I will be
back to read a great deal more, Please do keep up
the awesome job.
Also visit my homepage 신용카드현금화
I do agree with all of the ideas you’ve offered to your post.
They’re very convincing and will certainly work. Still,
the posts are very quick for starters. May just you please prolong
them a bit from subsequent time? Thanks for the post.
Also visit my page: keo nha cai 88
Does your blog have a contact page? I’m having problems locating
it but, I’d like to shoot you an email. I’ve got some creative ideas for your
blog you might be interested in hearing. Either way, great website and I look forward to
seeing it develop over time.
Feel free to surf to my web-site; tron vanity address generator
I just couldn’t leave your web site before suggesting that I actually
loved the usual information a person provide for your
guests? Is going to be again steadily in order to check out new posts
Also visit my page: situs jual beli narkoba
Greetings! Very helpful advice within this article!
It is the little changes that produce the biggest changes.
Thanks for sharing!
Check out my web page: japanese sex
Hi, i believe that i noticed you visited my web site thus i came to return the desire?.I’m trying to to find things to enhance my web site!I suppose its
adequate to make use of some of your concepts!!
Also visit my web-site; MALWARE
What’s up, I want to subscribe for this website to obtain most up-to-date updates, so where can i
do it please assist.
Have a look at my site – заказать пленку пвх
You’ve made some decent points there. I checked on the
web for additional information about the issue and found most individuals will
go along with your views on this website.
My blog post … SlottoJam Casino
At this time it sounds like BlogEngine is the top blogging platform out there right now.
(from what I’ve read) Is that what you are using on your blog?
Feel free to visit my blog post … Cristina
This website was… how do you say it? Relevant!! Finally
I’ve found something which helped me. Kudos!
my page; 더블쉽
Triangloe Billiards & Bar Stools
1471 Nisson Ɍd, Tustin,
CA 92780, United States
+17147715380
Bookmarks
This is a very good tip especially to those fresh to the blogosphere.
Brief but very accurate info… Thanks for sharing this one.
A must read article!
Also visit my blog post … web page
I’m gone to tell my little brother, that he should also visit this webpage on regular basis to
take updated from most up-to-date news update.
Feel free to visit my page; open bo kamboja
Triangle Billiards & Bar Stools
1471 Nisson Ꭱd, Tustin,
CA 92780, United States
+17147715380
Shuffleboard Refunishing Benefits – go.bubbl.us,
Really enjoyed reading this post.
The article does a good job explaining
the basics of online sports streaming
in a
straightforward format.
It’s common for readers to ask
how to access live sports streams
and
this article answers those questions well.
Appreciate the useful content.
my blog; play888new.com
Southeast Financial Nashville
131 Belle Forest Cir #210,
Nashville, TN 37221, United Տtates
18669008949
RV financing for RV accessories
I believe that is among the such a lot vital information for me.
And i’m glad studying your article. However wanna commentary on few common things, The web site style is
great, the articles is in point of fact nice : D. Good activity, cheers
My web page: Danatoto
I was wondering if you ever considered changing the
page layout of your blog? Its very well written;
I love what youve got to say. But maybe you could a little more in the way of content so people could connect with it better.
Youve got an awful lot of text for only having 1 or 2 images.
Maybe you could space it out better?
Have a look at my web page Dominobet
My webpage – LetsJackpot Casino
Как правильно выбрать онлайн казино по рейтинг казиноу
I wanted to thank you for this great read!! I certainly
enjoyed every little bit of it. I have you bookmarked to look at new stuff
you post…
Also visit my web site … Rebahin
Spot on with this write-up, I actually believe that this site needs far more attention. I’ll
probably be returning to read more, thanks for the advice!
My web-site: willie robbins colorado
Thanks for some other informative blog. The place else may just
I get that type of info written in such a perfect means?
I have a undertaking that I’m just now working
on, and I have been at the glance out for such information.
Also visit my web-site Stack varg preis
An impressive share! I have just forwarded
this onto a colleague who had been doing a little research
on this. And he in fact bought me lunch due to the fact
that I found it for him… lol. So allow me to reword
this…. Thank YOU for the meal!! But yeah, thanx for spending time to discuss this topic here on your website.
Look at my web site RIKVIP GAMES
I was looking for information on where to get secure IPs for online privacy projects
when I found your blog. The discussion about ip masking are very relevant.
I’m plan to start a trial today. Where can I find details
on the VPN dashboard?
Here is my webpage – Have a Look at IP Changer Directly
Triangle Billiards & Bar Stools
1471 Nisson Ꭱd, Tustin,
ⲤA 92780, United Stɑtеs
+17147715380
Billiard Table Installation
It’s actually a great and useful piece of information. I am glad that you simply shared this useful information with us.
Please keep us up to date like this. Thank you for sharing.
Here is my blog post … gay porn
Hello, I enjoy reading all of your article post.
I wanted to write a little comment to support you.
Here is my blog – freebbwporn.xyz
Aw, this was an exceptionally nice post. Taking a few minutes and actual effort to produce a great article… but what can I say… I hesitate a whole lot
and never manage to get nearly anything done.
Feel free to visit my blog post Stack varg preis
Hey! Someone in my Facebook group shared this
site with us so I came to take a look. I’m definitely loving the information. I’m bookmarking and will be tweeting this
to my followers! Excellent blog and terrific design.
Review my blog post – MALWARE
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Տtates
12394214912
Coatings
This article will assist the internet viewers for building up new website or
even a blog from start to end.
Feel free to surf to my page; norge iptv
Good day! I could have sworn I’ve visited this website before but
after browsing through some of the articles I realized it’s new to me.
Regardless, I’m definitely happy I found it and I’ll be bookmarking it and checking back frequently!
Feel free to surf to my site трипскан вход
Excellent article. I’m dealing with a few of these issues as well..
Feel free to surf to my web site … Ecoxtrem Armored One
Great delivery. Solid arguments. Keep up the good effort.
My web site; หีไทย
I all the time used to read post in news papers but now as I am a user of web so from now I am using net for articles or reviews, thanks to web.
My web page gem88uk.net
Hi there, I would like to subscribe for this blog to take latest updates, so
where can i do it please assist.
My homepage: SpinBara Ελλάδα
Simply want to say your article is as surprising. The clearness in your post is just excellent
and i could think you’re knowledgeable in this
subject. Fine along with your permission let me to take hold of your RSS
feed to stay updated with imminent post. Thanks
one million and please keep up the rewarding work.
Here is my web-site; patinete electrico Ecoxtrem Deimos
Appreciating the commitment you put into your website and in depth information you present.
It’s good to come across a blog every once in a while that isn’t
the same old rehashed information. Wonderful read! I’ve bookmarked your site and I’m adding your RSS feeds to my Google account.
my page :: трипскан вход
This is my first time visit at here and i am genuinely impressed to read
everthing at alone place.
My homepage: emergency locksmith near me
hello!,I really like your writing so so much! proportion we
be in contact extra about your article on AOL? I need an expert in this area to resolve
my problem. May be that is you! Having a look ahead to
see you.
Also visit my site – 米子 整体
What a material of un-ambiguity and preserveness
of valuable knowledge about unpredicted feelings.
Also visit my web page :: 雷电模拟器
Шикарное сайт ставок, отличная работа.
Благодарю!
Olimp Casino слоты
I loved as much as you’ll receive carried out right here.
The sketch is attractive, your authored material stylish.
nonetheless, you command get got an impatience over that
you wish be delivering the following. unwell unquestionably come further formerly again as exactly the same nearly very often inside case
you shield this hike.
Feel free to surf to my web site :: agoloannet
I think that everything said made a lot of sense.
But, think on this, suppose you wrote a catchier post title?
I am not suggesting your information isn’t good, but what if you added something that grabbed a
person’s attention? I mean Heel Pain – Plantar Fasciitis – Mr Will Edwards is kinda plain. You could look at Yahoo’s home page and note how they write news headlines to get
viewers interested. You might add a video or a picture or two
to grab people excited about everything’ve got to say. In my opinion, it would bring your blog a little livelier.
Stop by my webpage :: MALWARE
Thanks for sharing your info. I really appreciate your
efforts and I will be waiting for your next write ups thank you once
again.
my website … shunyanant
Great piece on medical expenses. Bookmarked.
Feel free to surf to my homepage :: how to start 2024
New1e วิธีสร้างรายได้ออนไลน์ 2026 การเงิน & Digital Nomad Guide ติดตามข่าวสารใหม่ๆ จากเราได้ที่นี่ new1e.com
Wonderful site. Plenty of useful information here. I am sending it to several buddies ans also sharing in delicious.
And of course, thanks in your sweat!
Also visit my web page; klia limo Malaysia
I really like what you guys are usually up too.
Such clever work and exposure! Keep up the good works guys I’ve incorporated you guys to my own blogroll.
Also visit my web blog freelesbianporn.xyz
Generally I don’t learn post on blogs, however I would like to say that this
write-up very forced me to take a look at and do it! Your writing taste has been surprised me.
Thanks, quite great post.
Feel free to visit my blog post – cheap
I like the valuable info you provide on your articles.
I will bookmark your weblog and take a look at again here frequently.
I am relatively certain I’ll learn a lot of new stuff right here!
Good luck for the next!
Stop by my web blog mellstroy.com
My brother suggested I might like this web site.
He was totally right. This submit truly made my day.
You can not believe just how a lot time I had spent for this info!
Thanks!
Good day! This is my first visit to your blog! We are a collection of volunteers and starting a new project in a community in the same
niche. Your blog provided us beneficial information to work
on. You have done a marvellous job!
my blog … shuffle.com
Really enjoyed reading this post.
This post breaks down
how online cricket streaming works
in a
clear and beginner-friendly manner.
A lot of users are curious
where to find reliable streaming platforms
and
this article answers those questions well.
Thanks for sharing.
Also visit my website: play888new.com
fjgzpb
Simply wish to say your article is as astonishing.
The clearness in your post is simply cool and i can assume you are an expert on this
subject. Well with your permission let me to grab your RSS feed to keep up to date with forthcoming post.
Thanks a million and please carry on the rewarding work.
Feel free to visit my homepage :: canadian pharmaceuticals online
Also visit my web page – Siti con prelievo immediato
Howdy! I know this is kind of off topic but I was wondering which blog
platform are you using for this website? I’m getting
fed up of WordPress because I’ve had problems with hackers and I’m looking at alternatives for another platform.
I would be fantastic if you could point me in the direction of a good platform.
Look at my webpage – money laundry
I was curious if you ever considered changing the layout of
your blog? Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content so people
could connect with it better. Youve got an awful lot of text for only
having one or 2 pictures. Maybe you could space it out better?
Visit my web site – 휴대폰 소액결제 현금화
I have read some just right stuff here. Definitely price bookmarking for
revisiting. I wonder how a lot attempt you put to create one of these excellent informative website.
Here is my web page; 여친대행
Unquestionably imagine that that you said. Your favorite reason appeared to be at the internet the
easiest factor to be mindful of. I say to you, I certainly get
annoyed even as other people consider worries that they plainly don’t realize about.
You managed to hit the nail upon the highest as neatly as outlined out
the entire thing without having side effect , people could take a signal.
Will likely be back to get more. Thank you
Here is my homepage; 여친대행
These are genuinely impressive ideas in about blogging.
You have touched some pleasant factors here. Any way keep up
wrinting.
my site stem cell clinic
It is really a great and helpful piece of information. I’m satisfied that you just shared
this useful info with us. Please keep us up to date like this.
Thank you for sharing.
Visit my page 애인대행
Really impressed! My injured tendon from last year seems to
be 100 percent. TB-500 peptide certainly accelerated my
recovery enhancement compounds (www7a.biglobe.ne.jp) process.
Wish I’d found this earlier.
Amazing! Its in fact amazing paragraph, I have got much clear idea concerning
from this article.
my web blog Vk88
Hello there! I could have sworn I’ve visited this website before but after going through many of the articles
I realized it’s new to me. Nonetheless, I’m certainly delighted I stumbled upon it and
I’ll be bookmarking it and checking back often!
my homepage: coinqqslot
Really enjoyed reading this post.
This post breaks down
how streaming platforms operate
in a
straightforward format.
Many people often wonder
how to access live sports streams
and
the information here is quite practical.
Appreciate the useful content.
Feel free to visit my page: play888new.com
This article is actually a pleasant one it helps new the web viewers, who are wishing in favor of blogging.
Here is my webpage: canadian pharmacy online
Look into my web-site meilleur Plinko
Hi there! This article could not be written any better!
Looking through this article reminds me of my previous roommate!
He constantly kept talking about this. I am going to send this information to him.
Fairly certain he’ll have a good read. Thank you for sharing!
My web blog; talaria komodo price
A few days back I discovered an interesting article about Paybis and honestly it stood
out to me.
The article shared insights on how beginners can get into crypto safely, and it was easy to follow.
After going through it, I shared it with my family member,
and he started learning more about crypto.
Within the next month, he became much more confident
with finances.
He didn’t just sit around — he actually applied what he learned.
Eventually, he managed to reach around 100k — not overnight, but through learning.
What surprised me most is how his lifestyle changed.
He even upgraded his lifestyle, something like a BMW 3 Series, and completely changed his mindset.
He even met someone new who shares his lifestyle.
Of course results can vary, but the story is genuine, and that article
definitely opened new perspectives.
There’s actually a way to check it out here, and I’d seriously suggest
reading it.
Sometimes one good article can shift your mindset.
Feel free to surf to my site: link
Фриспины позволяют игрокам испытать удачу и получить реальный выигрыш без риска потерять свои деньги. https://traversi.ru/uz/
nycwyo
I was wondering if you ever thought of changing
the layout of your website? Its very well written; I
love what youve got to say. But maybe you could a little more in the
way of content so people could connect with it better.
Youve got an awful lot of text for only having 1 or 2 images.
Maybe you could space it out better?
Here is my site: ссылка на кракен 2026
Hello, its pleasant post about media print, we all be familiar with
media is a great source of information.
Also visit my site; Techtra Best Automotive College in Malaysia
Kazino haqqında faydalı kontent üçün təşəkkürlər!
олимпбет линия
This is a very informative post.
This post breaks down
how online cricket streaming works
in a
clear and beginner-friendly manner.
It’s common for readers to ask
how they can watch live cricket online
and
this post provides useful insights.
Thanks for putting this together.
Here is my blog … play888new.com
Hey there! I understand this is somewhat off-topic however I needed to ask.
Does managing a well-established blog like yours take a lot of work?
I am brand new to blogging but I do write in my diary
everyday. I’d like to start a blog so I will be able
to share my own experience and thoughts online. Please let me know if you have any suggestions
or tips for brand new aspiring bloggers. Appreciate it!
my homepage – Perguntas Frequentes sobre Código Promocional Izzi Casino
Magnificent web site. A lot of useful info here.
I’m sending it to several pals ans additionally sharing in delicious.
And naturally, thanks for your sweat!
Have a look at my website – 부산토닥이 성인
Have you ever thought about including a little bit more than just your
articles? I mean, what you say is important and
all. However just imagine if you added some great visuals or videos to give your posts more, “pop”!
Your content is excellent but with pics and videos, this website
could definitely be one of the greatest in its field.
Superb blog!
Feel free to visit my web-site :: 비아그라 약국
Hello there! This is my 1st comment here so I just wanted to give a quick shout out and
tell you I genuinely enjoy reading your articles.
Can you recommend any other blogs/websites/forums that go over the
same topics? Thanks a lot!
Also visit my web page … growth hacking fundamentals
เนื้อหานี้ อ่านแล้วเข้าใจง่าย ค่ะ
ผม ไปเจอรายละเอียดของ เรื่องที่เกี่ยวข้อง
ดูต่อได้ที่ Leanna
สำหรับใครกำลังหาเนื้อหาแบบนี้
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ เนื้อหาดีๆ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
Also visit my web-site; betflik199 – Leanna,
Very great post. I simply stumbled upon your blog and
wished to say that I’ve truly enjoyed browsing your blog posts.
In any case I’ll be subscribing for your feed and I’m hoping you write
again very soon!
Here is my web-site Sky88
The other day, while I was at work, my sister stole my iPad and tested
to see if it can survive a twenty five foot drop,
just so she can be a youtube sensation. My iPad is now destroyed and
she has 83 views. I know this is entirely off topic but I had to share it with someone!
Also visit my blog offerte schilderwerk limburg
I am regular visitor, how are you everybody?
This article posted at this web page is genuinely good.
Here is my page: betfury app
Spot on with this write-up, I truly think this amazing site needs a lot more attention. I’ll probably be back again to see more, thanks for the advice!
My blog post: porsche service centre
great points altogether, you just received a emblem new reader.
What might you suggest in regards to your submit
that you simply made a few days in the past? Any certain?
Take a look at my blog post … slon6 at
Hmm it looks like your website ate my first comment (it was extremely long)
so I guess I’ll just sum it up what I had written and say, I’m thoroughly enjoying your blog.
I too am an aspiring blog writer but I’m still new to everything.
Do you have any suggestions for first-time blog writers?
I’d certainly appreciate it.
my webpage; 김해출장마사지
Here is my blog post … Lets Jackpot
Terrific article! That is the kind of information that are
supposed to be shared around the net. Disgrace on Google for now not positioning this post higher!
Come on over and talk over with my site . Thanks =)
my webpage gem88
You should take part in a contest for one of the highest quality websites on the
net. I’m going to recommend this site!
Stop by my web site: b52club
In fact no matter if someone doesn’t be aware of after that
its up to other users that they will assist, so here it takes place.
Here is my web site – amergg
Hi, I do think this is an excellent blog. I stumbledupon it ;) I’m going to return yet again since i have bookmarked it.
Money and freedom is the best way to change, may you be rich
and continue to guide other people.
Here is my blog online medicine shopping
machines à sous en ligne hautes limites
casino francais en ligne
casino en ligne sans KYC
Hi, Neat post. There’s a problem together with your web site in web explorer, might test this?
IE still is the marketplace leader and a good element
of people will omit your wonderful writing because of this problem.
Stop by my site … click now
Oh my goodness! Incredible article dude! Many thanks, However I am
having issues with your RSS. I don’t understand the
reason why I am unable to join it. Is there anybody else getting similar RSS problems?
Anybody who knows the answer can you kindly respond?
Thanks!!
Here is my page … Mayfair Wellness Stem Cell Therapy Malaysia
Howdy! Someone in my Facebook group shared this site with us so I came to take a look.
I’m definitely enjoying the information. I’m book-marking and will be tweeting this to my followers!
Exceptional blog and outstanding style and design.
Feel free to surf to my blog … QQ88BET
Wrapped up my first wolverine stack round last month and the benefits are still continuing.
My old sports injury feels totally restored. Considering another round soon.
Feel free to visit my web blog; healing peptide protocols (https://reviewer4you.com)
Way cool! Some very valid points! I appreciate you penning this post and the rest of the site is extremely good.
Feel free to visit my homepage … cyber security
My site :: Simsinos Casino en ligne
Hey there, I think your website might be having browser compatibility issues.
When I look at your website in Chrome, it looks fine but when opening in Internet Explorer, it has some overlapping.
I just wanted to give you a quick heads up! Other then that, superb blog!
Have a look at my website; zoho sites
Its like you read my mind! You seem to know so much about this, like
you wrote the book in it or something. I think that you can do with a few pics to drive
the message home a little bit, but instead of that, this is magnificent blog.
An excellent read. I will certainly be back.
my blog: Trang chủ VIPWIN
Not long ago I found an surprisingly useful article about a crypto platform called Paybis and honestly it caught
my attention.
The article shared insights on how people are
using crypto in smarter ways, and it felt real.
After reading it, I told my uncle, and he got really interested.
Within the next month, he became way more financially
aware.
He didn’t just sit around — he took action. Eventually, he even pushed towards 200k depending
on timing — not overnight, but through learning.
What surprised me most is how his lifestyle changed. He even upgraded his lifestyle, something like a Mercedes-Benz C-Class, and started enjoying life more.
He even built a new social circle around success.
This isn’t magic or guaranteed, but the story is real, and that article definitely made a big impact.
There’s actually a link in this comment, and I’d seriously say it’s worth your time.
You never know what small discovery can change things.
Stop by my blog post web article
Have you ever thought about creating an e-book or guest authoring on other
blogs? I have a blog based on the same subjects you discuss and would
really like to have you share some stories/information. I know my viewers would
appreciate your work. If you’re even remotely interested, feel free to send me
an e-mail.
Review my blog post 울산출장마사지
Hi there! Do you use Twitter? I’d like to follow you if that would be
okay. I’m definitely enjoying your blog and look forward to new posts.
Visit my webpage … wow boosting
Hi! I’ve been following your site for a long time now and finally got the courage to go ahead and give you
a shout out from New Caney Texas! Just wanted
to mention keep up the good work!
Feel free to surf to my site: MALWARE
I all the time emailed this weblog post page to all my associates, as if like to read it then my
contacts will too.
Check out my blog post; real estate agent Greensboro NC best real estate agent in Greensboro NC
Greetings! Very helpful advice in this particular post!
It is the little changes that produce the most significant changes.
Many thanks for sharing!
Feel free to visit my website best real estate agent in Redondo Beach CA
Howdy! I could have sworn I’ve visited this web site before but after browsing through a few of
the articles I realized it’s new to me. Nonetheless, I’m certainly happy I stumbled upon it and I’ll be bookmarking it and checking back frequently!
Also visit my website best realtor in Torrance CA
Great article, very helpful.
This post breaks down
how online cricket streaming works
in a
straightforward format.
Many people often wonder
how to access live sports streams
and
this post provides useful insights.
Thanks for putting this together.
my web site – play888new.com
I know this if off topic but I’m looking into starting my
own blog and was curious what all is required to get set up?
I’m assuming having a blog like yours would cost a pretty
penny? I’m not very web smart so I’m not 100% certain. Any recommendations or advice would be
greatly appreciated. Thanks
my page: best real estate agent in Carlsbad CA
I like the valuable info you provide in your articles. I’ll bookmark your weblog and check
again here frequently. I’m quite sure I’ll learn many new stuff right here!
Best of luck for the next!
My web site 강남데이트
I couldn’t refrain from commenting. Perfectly written!
my web site :: real estate agent Carlsbad CA
Someone necessarily lend a hand to make significantly
posts I’d state. This is the very first time
I frequented your website page and up to now? I surprised with the research
you made to make this actual publish amazing. Great process!
Feel free to surf to my blog – คลิปxxx
What i don’t understood is actually how you are now not actually much more neatly-appreciated than you may be right now.
You are so intelligent. You already know thus significantly in the case of this topic,
made me individually imagine it from so many varied angles.
Its like women and men are not interested except it’s something
to accomplish with Woman gaga! Your personal stuffs great.
All the time take care of it up!
My web site: realtor in Tampa FL
Как правильно подобрать новости
для чтения
Feel free to surf to my website – Мужчина Стрелец Женщина Лев
At this moment I am going to do my breakfast, after having
my breakfast coming again to read further news.
My website: Source
goGLOW
6850 N Rochester Rd, Rochester Hills,
MӀ 48306, United Ѕtates
248 971-1831
goglow treatment (Ramon)
We’re a group of volunteers and opening a new scheme in our community.
Your website provided us with valuable info to work
on. You’ve done an impressive job and our entire community will be grateful
to you.
My web page: real estate agent Tampa FL
I enjoy reading through a post that will make people think.
Also, thank you for allowing for me to comment!
my web-site … 구미출장마사지
This is my first time pay a visit at here and i am truly pleassant to read all at alone place.
my blog post … real estate agent El Segundo CA
This site really has all the information and facts
I needed about this subject and didn’t know who to ask.
Also visit my web blog – ev88
Simply want to say your article is as amazing. The clarity in your post is just excellent and i could
assume you’re an expert on this subject. Fine with your permission allow me
to grab your feed to keep updated with forthcoming post.
Thanks a million and please keep up the rewarding work.
Also visit my web page: best real estate agent in Carlsbad CA
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ѕtates
12394214912
Promotion (https://atavi.com/share/xsqnn2z1icw3c)
This is my first time pay a quick visit at here and i am truly pleassant to read everthing at one place.
Feel free to visit my site real estate agent Redondo Beach CA
Thanks for sharing your thoughts. I really appreciate your efforts and
I will be waiting for your further write ups thank you once again.
Feel free to visit my page … about
I was reading an eye-opening article about Paybis and honestly it stood out to me.
The article explained how people are using crypto in smarter ways, and
it wasn’t full of complicated jargon.
After reading it, I told my family member, and he started learning more about
crypto. Within the next month, he looked at new income opportunities.
He didn’t just sit around — he started testing
things carefully. Eventually, he even pushed towards 200k depending on timing — not overnight, but through
smart decisions.
What surprised me most is how his lifestyle changed. He even finally
bought something he always wanted, something like a BMW 3 Series, and completely changed his mindset.
He even built a new social circle around success.
Of course results can vary, but the story is real, and that article definitely opened new perspectives.
There’s actually a link in this comment, and I’d seriously advise you to check it.
Opportunities are everywhere if you look closely.
What’s up, yes this post is in fact pleasant
and I have learned lot of things from it about blogging. thanks.
My homepage; real estate agent Carlsbad CA
Helpful info. Fortunate me I discovered your website unintentionally, and I’m shocked why this coincidence didn’t took place in advance!
I bookmarked it.
my page realtor in Greensboro NC
It’s actually a cool and helpful piece of information. I am happy that you just shared this helpful
information with us. Please keep us informed like this.
Thanks for sharing.
Also visit my webpage; best realtor in El Segundo CA
My coder is trying to persuade me to move to .net from PHP.
I have always disliked the idea because
of the costs. But he’s tryiong none the less.
I’ve been using Movable-type on various websites for
about a year and am concerned about switching to another platform.
I have heard excellent things about blogengine.net.
Is there a way I can import all my wordpress posts into it?
Any kind of help would be greatly appreciated!
My web page … realtor in Torrance CA
Hello, i think that i saw you visited my website thus i came
to “return the favor”.I am attempting to
find things to enhance my site!I suppose its
ok to use a few of your ideas!!
Also visit my web site; best realtor in Redondo Beach CA
My partner and I absolutely love your blog and find nearly all of
your post’s to be just what I’m looking for. Would you offer guest writers to write content
for yourself? I wouldn’t mind producing a post or elaborating on most of the subjects you write related to here.
Again, awesome blog!
Feel free to surf to my webpage: 沖縄 不動産
Keep this going please, great job!
Feel free to surf to my web-site … best real estate agent in El Segundo CA
Ahaa, its good conversation about this article at this place at
this weblog, I have read all that, so at this time me also
commenting at this place.
My site … tripscan top
Hey there! Someone in my Myspace group shared this site with us so
I came to check it out. I’m definitely loving the information. I’m book-marking and will be tweeting this to my followers!
Wonderful blog and excellent design.
Here is my webpage; commercial towing
Not long ago I found an interesting article about
a crypto platform called Paybis and honestly it
stood out to me.
The post talked about how digital finance is evolving, and
it felt real.
After checking it out, I shared it with my family member,
and he got really interested. Within the next month, he looked at new income opportunities.
He didn’t just sit around — he took action. Eventually,
he got close to 150k in results — not overnight, but through learning.
What surprised me most is how his lifestyle changed.
He even upgraded his lifestyle, something like a Mercedes-Benz C-Class,
and completely changed his mindset. He even met someone new who shares his lifestyle.
This isn’t magic or guaranteed, but the story is genuine, and
that article definitely changed the way we look at money.
There’s actually a source included here, and I’d
seriously advise you to check it.
Opportunities are everywhere if you look closely.
Visit my site :: press release
Awesome! Its truly awesome paragraph, I have got much clear idea on the topic of from
this post.
My blog post: best realtor in Tampa FL
I simply could not go away your site before suggesting that I actually enjoyed the usual information a person supply to your visitors?
Is going to be again regularly in order to investigate cross-check new posts
Feel free to surf to my blog :: Scrap car
Thanks in favor of sharing such a fastidious opinion, paragraph is good, thats why
i have read it entirely
Also visit my site; best real estate agent in El Segundo CA
Currently it sounds like Movable Type is the top blogging platform out there right now.
(from what I’ve read) Is that what you’re using on your blog?
Here is my web page: best realtor in Redondo Beach CA
Helpful info. Fortunate me I discovered your web site unintentionally, and I’m stunned why this accident didn’t took place in advance!
I bookmarked it.
My website :: Techtrics Auto
Nice blog here! Also your web site loads up fast!
What web host are you using? Can I get your affiliate link to your host?
I wish my site loaded up as quickly as yours lol
Here is my site :: 400 file structure
I’m not that much of a internet reader to be honest but your
blogs really nice, keep it up! I’ll go ahead and bookmark
your site to come back later. All the best
Also visit my homepage … mgmarket 6 at
Woah! I’m really loving the template/theme of this site.
It’s simple, yet effective. A lot of times it’s
tough to get that “perfect balance” between usability and visual appeal.
I must say you have done a great job with this. In addition, the blog loads very fast for me on Chrome.
Excellent Blog!
My web site … 라스베가스 추천 부동산
This piece of writing is truly a pleasant one it assists new net people, who
are wishing in favor of blogging.
Check out my page; real estate agent Greensboro NC best real estate agent in Greensboro NC
For latest information you have to go to see the web and on world-wide-web I found this site as a best
website for most up-to-date updates.
Feel free to visit my web site: realtor in Torrance CA
Asking questions are genuinely pleasant thing if
you are not understanding something totally, except
this article offers good understanding even.
Here is my web page – real estate agent Greensboro NC best real estate agent in Greensboro NC
What i don’t realize is in reality how you’re
not actually much more smartly-appreciated than you might be now.
You’re so intelligent. You understand thus considerably when it comes to this topic,
made me personally believe it from so many various
angles. Its like men and women don’t seem to be fascinated unless it’s something to do
with Woman gaga! Your individual stuffs outstanding.
All the time take care of it up!
Here is my web site Toyota Camry Hybrid EV Indonesia
Everything is very open with a clear explanation of the challenges.
It was truly informative. Your website is useful.
Thank you for sharing!
Take a look at my webpage … real estate agent Tampa FL
This is a great tip particularly to those fresh to the
blogosphere. Short but very precise info… Thanks for sharing this one.
A must read post!
Check out my web-site :: HundRoses
It’s an amazing post for all the internet visitors; they will obtain advantage from it I am sure.
Also visit my homepage; realtor in Redondo Beach CA
I for all time emailed this web site post page to all my associates, since if like to read
it next my links will too.
Also visit my homepage … youtube video downloader free
It is actually a great and useful piece of information. I am satisfied that you just shared
this helpful info with us. Please keep us up to date like
this. Thank you for sharing.
Check out my web-site :: lucky55
I have read so many content about the blogger lovers but this article is in fact a
pleasant piece of writing, keep it up.
Feel free to visit my web-site; real estate agent Tampa FL
Как правильно набрать подписчиков в Макс
Here is my blog post :: https://vc.ru/smm-promotion/2882474-nakrutka-zhivykh-podpischikov-v-max
I just like the valuable info you provide for your articles.
I will bookmark your weblog and take a look at again right here
regularly. I am quite sure I will be told lots
of new stuff right here! Best of luck for the next!
Here is my web-site :: best real estate agent in Carlsbad CA
I’m no longer positive the place you’re getting your
information, but great topic. I must spend a while learning
much more or figuring out more. Thanks for wonderful info I was in search of
this info for my mission.
Feel free to surf to my webpage … realtor in Torrance CA
Hello! Do you know if they make any plugins to assist with Search Engine Optimization? I’m trying to get my blog to rank
for some targeted keywords but I’m not seeing very good results.
If you know of any please share. Kudos!
Feel free to visit my homepage – 라스베가스 한인사이트
Simply wish to say your article is as amazing. The clarity for your put up is simply great
and i could assume you are knowledgeable in this subject.
Fine together with your permission let me to take hold of your feed to keep up to date
with drawing close post. Thank you a million and please continue the enjoyable work.
Feel free to visit my webpage … realtor in Tampa FL
Hey there! I just wanted to ask if you ever have any trouble with hackers?
My last blog (wordpress) was hacked and I ended up losing a few months of hard work due to no
backup. Do you have any solutions to stop hackers?
Visit my homepage: best realtor in Tampa FL
Triangle Billiards & Bar Stools
1471 Nisson Ꭱd, Tustin,
CᎪ 92780, United Տtates
+17147715380
Game Table Renovation Strategies
Why visitors still use to read news papers when in this technological world the whole
thing is presented on web?
Look into my web-site: 라스베가스 한인사이트
I loved as much as you will receive carried out right here.
The sketch is attractive, your authored subject matter stylish.
nonetheless, you command get bought an impatience over
that you wish be delivering the following. unwell unquestionably come further formerly
again since exactly the same nearly a lot often inside case you shield
this increase.
Here is my web page: best real estate agent in Torrance CA
What’s up colleagues, good article and nice arguments commented here, I am genuinely enjoying
by these.
Also visit my page – 성남홈타이
Appreciating the time and effort you put into your website and detailed information you offer.
It’s awesome to come across a blog every once in a while that isn’t the same unwanted rehashed information. Great read!
I’ve saved your site and I’m including your RSS
feeds to my Google account.
my blog :: porn
Really enjoyed reading this post.
This post breaks down
the basics of online sports streaming
in a
clear and beginner-friendly manner.
Many people often wonder
how to access live sports streams
and
this article answers those questions well.
Thanks for sharing.
Here is my blog post: play888new.com
Inspiring quest there. What happened after? Thanks!
my blog post; best real estate agent in Redondo Beach CA
Hi to all, the contents existing at this website are actually
awesome for people knowledge, well, keep up the nice work fellows.
my web blog best real estate agent in El Segundo CA
I’m not sure why but this website is loading very slow for me.
Is anyone else having this problem or is it a problem on my end?
I’ll check back later on and see if the problem still exists.
Also visit my blog post – how to set up ledger nano x
Как что входит в состав тормозного оборудования вагоновыбрать детали
и оснащение для железнодорожного
транспорта
I recently came across an surprisingly useful article about this crypto service Paybis and honestly it really made me think.
The guide talked about how crypto platforms can be used more effectively, and it actually made sense.
After checking it out, I told my relative, and he started learning more
about crypto. Within the next month, he became much more
confident with finances.
He didn’t just sit around — he took action. Eventually,
he got close to 150k in results — not overnight,
but through smart decisions.
What surprised me most is how his lifestyle changed.
He even upgraded his lifestyle, something like a Mercedes-Benz C-Class,
and became more confident. He even found a partner who enjoys the same level of
comfort.
I’m not saying this will happen to everyone,
but the story is true from what I’ve seen, and that article
definitely made a big impact.
There’s actually a link in this comment, and I’d
seriously recommend taking a look.
Sometimes one good article can shift your mindset.
Feel free to surf to my web page :: p41728
I was reading an interesting article about this crypto service Paybis and honestly it really made me think.
The post broke down how people are using crypto in smarter ways, and it felt real.
After checking it out, I shared it with my uncle, and he started learning more about
crypto. Within the next month, he became much more confident with finances.
He didn’t just sit around — he approached it seriously.
Eventually, he managed to reach around 100k — not overnight,
but through learning.
What surprised me most is how his lifestyle changed. He even finally bought something he always wanted, something like an Audi A5,
and completely changed his mindset. He even built a new social circle around
success.
I’m not saying this will happen to everyone, but the
story is real, and that article definitely changed the way we look at
money.
There’s actually a way to check it out here, and I’d seriously say it’s worth your time.
Information really can make a difference.
Check out my page … link
Its like you read my mind! You appear to know a
lot about this, like you wrote the book in it or something.
I think that you can do with a few pics to drive the message home a little bit,
but instead of that, this is fantastic blog. An excellent read.
I’ll definitely be back.
Here is my blog post: gay porn
Every weekend i used to pay a quick visit this web site, as i wish for enjoyment,
since this this website conations in fact nice funny
data too.
my web page: best real estate agent in El Segundo CA
Wow, this piece of writing is fastidious,
my sister is analyzing these kinds of things, so I am
going to tell her.
Here is my webpage – best real estate agent in Tampa FL
What’s up, I read your new stuff like every week.
Your humoristic style is witty, keep it up!
Review my web site – dating
Hi there, just became aware of your blog through Google, and
found that it’s really informative. I’m going to watch out for brussels.
I will appreciate if you continue this in future. Lots of people will be benefited from your writing.
Cheers!
Have a look at my blog :: best real estate agent in Carlsbad CA
Hi there it’s me, I am also visiting this web page regularly, this
web site is genuinely pleasant and the users are
actually sharing good thoughts.
Check out my web blog – best realtor in El Segundo CA
Because the admin of this web site is working, no uncertainty very soon it will be renowned, due to its quality contents.
Here is my web page … best real estate agent in Torrance CA
You could definitely see your skills within the article you write.
The world hopes for even more passionate writers like you who are not afraid to mention how they
believe. Always follow your heart.
Also visit my web-site: ae888
Greate post. Keep posting such kind of info on your page. Im
really impressed by it.
Hey there, You’ve performed a fantastic job. I will definitely digg it and individually recommend to my friends.
I’m sure they will be benefited from this website.
Here is my web site – best realtor in Redondo Beach CA
Nice post. I learn something totally new and challenging on websites I stumbleupon everyday.
It will always be helpful to read through articles from
other writers and use a little something from other sites.
Here is my site real estate agent Torrance CA
Have you ever thought about creating an e-book or guest authoring on other blogs?
I have a blog centered on the same topics you discuss and would really
like to have you share some stories/information. I know my subscribers would enjoy your work.
If you are even remotely interested, feel free to send me an email.
Look at my web site … best real estate agent in Carlsbad CA
I think this is one of the most vital info for me.
And i am glad reading your article. But want to remark on few general things,
The site style is perfect, the articles is really nice :
D. Good job, cheers
my blog post: best realtor in Greensboro NC
I was recommended this blog by my cousin. I’m not sure whether this post is written by him as nobody else know such detailed about my problem.
You are amazing! Thanks!
Feel free to surf to my web blog :: ilauncher.io lừa đảo công an truy nã cấm người chơi tham gia
Ahaa, its good dialogue about this post here at this weblog, I have read
all that, so now me also commenting at this place.
Feel free to visit my webpage: real estate agent Greensboro NC best real estate agent in Greensboro NC
Fine way of describing, and good post to take facts regarding my presentation focus, which i
am going to present in institution of higher education.
Feel free to visit my web-site: dewatogel
This post is invaluable. How can I find out more?
Stop by my web page; real estate agent Torrance CA
Heya! I’m at work surfing around your blog from my new
iphone! Just wanted to say I love reading your blog and
look forward to all your posts! Keep up the fantastic work!
my page – ngetot tetangga kesepian
Triangle Billiards & Bar Stools
1471 Nisson Ꭱd, Tustin,
СA 92780, United States
+17147715380
Pool Table Accessories Store
I’ve read several good stuff here. Definitely value bookmarking for
revisiting. I surprise how much attempt you set to
create any such great informative website.
Also visit my web site … lick vagina
What’s up friends, how is everything, and what you would like to say on the topic
of this paragraph, in my view its in fact remarkable designed for me.
Feel free to surf to my website: best real estate agent in Tampa FL
What a data of un-ambiguity and preserveness
of valuable know-how on the topic of unpredicted feelings.
my blog: pornasexe.com
Thank you, I have recently been searching for information about this
topic for ages and yours is the best I have discovered till
now. However, what about the bottom line? Are you sure in regards to the source?
my web blog … scrillion capone
A few days back I discovered an surprisingly useful article about a crypto platform called Paybis and honestly
I didn’t expect much at first but it impressed me.
The post talked about how people are using crypto in smarter ways, and it
wasn’t full of complicated jargon.
After reading it, I recommended it to my relative,
and he decided to explore it. Within the next month, he started managing his money differently.
He didn’t just sit around — he took action. Eventually, he even pushed
towards 200k depending on timing — not overnight, but through learning.
What surprised me most is how his lifestyle changed.
He even finally bought something he always wanted, something like a
Mercedes-Benz C-Class, and started enjoying life more.
He even built a new social circle around success.
Of course results can vary, but the story
is genuine, and that article definitely opened new perspectives.
There’s actually a source included here, and I’d seriously suggest reading
it.
Information really can make a difference.
my web-site: backlink
Nice post. I used to be checking constantly this
weblog and I’m impressed! Very useful information particularly
the ultimate part :) I care for such info much.
I used to be looking for this particular information for a very long time.
Thanks and good luck.
Here is my web page; revolink.io lừa đảo công an truy nã cấm người chơi tham gia
I blog often and I genuinely thank you for
your content. This article has truly peaked my interest.
I’m going to take a note of your blog and keep checking for new information about once per week.
I subscribed to your RSS feed as well.
Here is my web site – best real estate agent in Carlsbad CA
I love your blog.. very nice colors & theme. Did you make
this website yourself or did you hire someone to do it
for you? Plz respond as I’m looking to construct my own blog and would like to find out where u got this from.
thanks
Also visit my website: Plumbing Repair
Nice blog here! Also your website loads up very fast! What host are you using?
Can I get your affiliate link to your host? I wish my website loaded up as
fast as yours lol
Also visit my website; real estate agent Greensboro NC best real estate agent in Greensboro NC
I’m not that much of a internet reader to be honest but your blogs really nice,
keep it up! I’ll go ahead and bookmark your website to come back later
on. Many thanks
Also visit my web-site – best realtor in Torrance CA
I like the helpful information you provide to your articles.
I’ll bookmark your blog and take a look at once more right here frequently.
I am slightly certain I’ll be told many new stuff proper right here!
Good luck for the next!
My site … realtor in Greensboro NC
Informative article, totally what I was looking for.
Feel free to surf to my blog post: best realtor in Carlsbad CA
Hi there, I enjoy reading all of your article post.
I like to write a little comment to support you.
my website – 성남출장마사지
With havin so much content and articles do you ever run into any problems
of plagorism or copyright infringement? My site has a lot of unique content I’ve either authored myself or outsourced but it appears a lot of it is popping it up all over the internet without
my authorization. Do you know any techniques to help reduce content from being ripped off?
I’d genuinely appreciate it.
Also visit my site best real estate agent in Redondo Beach CA
Cabinet IQ Foort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ѕtates
12394214912
Creativeideas
What a material of un-ambiguity and preserveness of precious familiarity regarding unexpected feelings.
My web blog: 의정부출장마사지
Outstanding quest there. What occurred after? Thanks!
Also visit my page best realtor in Redondo Beach CA
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Տtates
12394214912
Installprocess
Cabinet IQ Fort Myers
7830 Drew Cirr Ste 4, Forrt Myers,
FL 33967, United Ѕtates
12394214912
Qualityguarantee
Everything is very open with a really clear description of the challenges.
It was really informative. Your site is very helpful.
Thanks for sharing!
Also visit my web-site – real estate agent Tampa FL
Your means of telling all in this post is in fact
good, every one be able to easily know it, Thanks a lot.
Have a look at my website … range rover workshop
I know this web page offers quality depending articles and additional stuff, is there
any other website which offers these information in quality?
Have a look at my web-site … real estate agent Carlsbad CA
My spouse and I absolutely love your blog and find almost all of your post’s to be what precisely I’m looking for.
Does one offer guest writers to write content for
you personally? I wouldn’t mind writing a post or elaborating
on a number of the subjects you write related to here.
Again, awesome web log!
Look into my site :: best real estate agent in El Segundo CA
Can I just say what a comfort to find someone that truly understands what they’re
discussing on the internet. You actually know how to bring
a problem to light and make it important. More and more people should look at this and understand this side of the story.
I was surprised that you aren’t more popular because
you definitely have the gift.
Stop by my website; best real estate agent in El Segundo CA
Hello! Do you know if they make any plugins to assist with Search Engine Optimization?
I’m trying to get my blog to rank for some targeted
keywords but I’m not seeing very good gains.
If you know of any please share. Thank you!
My page … https://hitclub1.ac
Hey there! I simply would like to offer you a
huge thumbs up for the great info you have got here on this post.
I’ll be returning to your website for more soon.
Visit my page … realtor in Tampa FL
Woah! I’m really digging the template/theme of this website.
It’s simple, yet effective. A lot of times
it’s challenging to get that “perfect balance” between user friendliness and appearance.
I must say you’ve done a superb job with this. In addition, the blog loads extremely fast for me on Internet explorer.
Exceptional Blog!
Also visit my blog: rikvip
Heya i am for the first time here. I found this board and I find It truly useful & it
helped me out much. I hope to give something back and aid others like you
aided me.
Look into my web blog … sexjav.uk
Very nice post. I just stumbled upon your blog and wanted to say that I’ve truly enjoyed surfing around your blog posts.
After all I will be subscribing to your rss feed and I hope
you write again soon!
my web site :: plummediagroup.com
This paragraph is really a good one it assists new web people, who are wishing in favor of blogging.
Also visit my web site – best realtor in Torrance CA
I recently came across an eye-opening article about Paybis
and honestly it really made me think.
The article broke down how beginners can get into crypto safely, and it
wasn’t full of complicated jargon.
After going through it, I shared it with my family member,
and he got really interested. Within the next month, he became way more financially aware.
He didn’t just sit around — he started testing things carefully.
Eventually, he even pushed towards 200k depending on timing
— not overnight, but through learning.
What surprised me most is how his lifestyle changed.
He even treated himself to a new car, something like a BMW 3 Series, and completely changed
his mindset. He even found a partner who enjoys the same level of comfort.
It depends on your effort, but the story is genuine, and that article definitely opened
new perspectives.
There’s actually a source included here, and I’d
seriously say it’s worth your time.
Opportunities are everywhere if you look closely.
Take a look at my blog post: lastPostAnchor
Everyone loves what you guys are up too. This kind
of clever work and coverage! Keep up the fantastic works guys I’ve added you guys to our
blogroll.
Here is my web-site: cash for junk cars boston
An interesting discussion is worth comment. I believe that you should write more on this topic,
it might not be a taboo matter but typically people do not talk
about such topics. To the next! Cheers!!
Here is my page korotkoepornoxxx.xyz
Great article, just what I was looking for.
Also visit my website: real estate agent El Segundo CA
Good day! Do you know if they make any plugins to help with SEO?
I’m trying to get my blog to rank for some targeted keywords
but I’m not seeing very good gains. If you know of any please share.
Thank you!
Feel free to surf to my blog post … best real estate agent in Redondo Beach CA
Yes! Finally ssomething about Digital marketing agency website development.
Also visit my page: Mobile-Friendly Design
This info is invaluable. How can I find out more?
Stop by my web blog real estate agent Carlsbad CA
It is actually a great and helpful piece of info. I’m satisfied
that you shared this useful information with us.
Please keep us up to date like this. Thanks for sharing.
My web-site; best realtor in Greensboro NC
Wow! This blog looks exactly like my old one!
It’s on a totally different subject but it has
pretty much the same layout and design. Superb choice of colors!
My homepage: best real estate agent in Carlsbad CA
Great beat ! I would like to apprentice while you amend
your site, how can i subscribe for a blog web site? The account helped me a acceptable deal.
I had been tiny bit acquainted of this your broadcast offered bright clear concept
Feel free to surf to my page: best realtor in Carlsbad CA
Wonderful work! That is the type of info that should be shared around the web.
Shame on the search engines for no longer positioning this submit higher!
Come on over and talk over with my website . Thank you =)
my web-site: real estate agent Tampa FL
References:
Remscheid
References:
https://casino-ohne-einzahlung-startguthaben.online-spielhallen.de/
References:
Hanover (Hannover)
References:
https://grand-sierra-hotel-and-casino-in-reno.online-spielhallen.de/
hello there and thank you for your information – I have certainly picked up anything new from right here.
I did however expertise a few technical issues using this site,
as I experienced to reload the site a lot of times
previous to I could get it to load properly.
I had been wondering if your web hosting is OK? Not that I’m complaining, but slow loading instances times will sometimes affect your placement in google and can damage your high quality score if advertising and
marketing with Adwords. Anyway I am adding this RSS to
my e-mail and can look out for much more of your respective interesting content.
Make sure you update this again soon.
my web site :: realtor in Carlsbad CA
Triangle Billiards & Baar Stools
1471 Nisson Rd, Tustin,
ⲤA 92780, United Ѕtates
+17147715380
bookmarks
Hi there, every time i used to check weblog posts here early in the morning,
as i like to learn more and more.
Here is my blog post best real estate agent in El Segundo CA
Hi there exceptional website! Does running a blog similar to this take a great deal of work?
I have no expertise in coding but I had been hoping to start my own blog soon. Anyways,
if you have any ideas or techniques for new blog owners please share.
I know this is off topic but I just needed to ask.
Thanks!
my website: best realtor in Greensboro NC
great publish, very informative. I’m wondering why the opposite specialists of
this sector do not understand this. You should proceed your writing.
I’m confident, you have a huge readers’ base already!
Also visit my blog post – realtor in El Segundo CA
Cool blog! Is your theme custom made or did you download
it from somewhere? A design like yours with a few simple
tweeks would really make my blog jump out. Please let me know where you got your
design. Thanks a lot
my homepage: real estate agent Greensboro NC best real estate agent in Greensboro NC
Amazing! This blog looks exactly like my old one!
It’s on a completely different topic but it has pretty much the same page layout
and design. Wonderful choice of colors!
Here is my web blog … realtor in Greensboro NC
I loved as much as you will receive carried out right here.
The sketch is tasteful, your authored material stylish.
nonetheless, you command get got an edginess
over that you wish be delivering the following.
unwell unquestionably come more formerly again as exactly the same nearly a lot often inside case you
shield this hike.
Also visit my blog; best realtor in El Segundo CA
Hello to all, how is all, I think every one is getting more from this website,
and your views are good in support of new people.
Here is my blog: best real estate agent in El Segundo CA
Today, I went to the beachfront with my children. I
found a sea shell and gave it to my 4 year old
daughter and said “You can hear the ocean if you put this to your ear.” She put the shell
to her ear and screamed. There was a hermit crab inside and
it pinched her ear. She never wants to go back! LoL I know this is entirely off topic but I had to tell someone!
Visit my webpage … betfury dice
This post will assist the internet people for setting up new weblog or even a blog from start to end.
Feel free to surf to my blog: 27 seater mini bus
Good information. Lucky me I ran across your site by accident (stumbleupon).
I have book-marked it for later!
Feel free to surf to my homepage Techtra Automotive academy
Aw, this was an incredibly good post. Finding the time and actual effort to generate a superb article… but what can I
say… I procrastinate a lot and don’t manage to
get nearly anything done.
Here is my site; real estate agent Torrance CA
A few days back I discovered an surprisingly useful article about a crypto platform called Paybis and honestly it
really made me think.
The post explained how crypto platforms can be used more effectively, and it actually made sense.
After going through it, I told my relative, and he got really interested.
Within the next month, he started managing his money differently.
He didn’t just sit around — he started testing things carefully.
Eventually, he got close to 150k in results — not overnight, but through consistency.
What surprised me most is how his lifestyle changed.
He even upgraded his lifestyle, something like a BMW 3 Series, and became more confident.
He even met someone new who shares his lifestyle.
Of course results can vary, but the story is real, and that article definitely made a big impact.
There’s actually a link in this comment, and I’d seriously say it’s
worth your time.
Information really can make a difference.
My web page – url
Howdy just wanted to give you a quick heads up. The text in your content seem to be running off the screen in Safari.
I’m not sure if this is a format issue or something to do with internet browser compatibility but I
figured I’d post to let you know. The layout look great though!
Hope you get the issue fixed soon. Cheers
Visit my web-site – real estate agent Torrance CA
I’m really impressed along with your writing skills as neatly
as with the structure on your weblog. Is that
this a paid subject or did you customize it your self?
Anyway keep up the excellent quality writing, it
is rare to look a nice weblog like this one these
days..
Also visit my page pornhub
Does your blog have a contact page? I’m having problems locating it but, I’d like to send you
an e-mail. I’ve got some ideas for your blog
you might be interested in hearing. Either way, great site and I look forward to seeing it expand over time.
Feel free to visit my web site – real estate agent Tampa FL
I do not know whether it’s just me or if perhaps everybody else encountering issues with your blog.
It seems like some of the text within your posts are running off the
screen. Can someone else please comment and let me know
if this is happening to them as well? This may be a issue with my internet
browser because I’ve had this happen previously. Kudos
Visit my blog post :: best real estate agent in Redondo Beach CA
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ѕtates
12394214912
Qualityguarantee
Right away I am going to do my breakfast, later than having my breakfast coming over again to read further news.
Feel free to visit my blog post best real estate agent in Carlsbad CA
We stumbled over here from a different web address and thought I should check things out.
I like what I see so now i’m following you. Look forward to checking out your web page again.
Here is my web page – pornofilmsex.com
Этот сайт kazino olimp — надёжный ресурс.
лучшие игры Olimp [games]
Hello, everything is going perfectly here and ofcourse every one is sharing information,
that’s in fact good, keep up writing.
Also visit my homepage: best realtor in Tampa FL
What you said was very logical. But, think on this, what if you were to write a awesome title?
I ain’t suggesting your content is not solid,
however suppose you added a post title that makes people want more?
I mean Heel Pain – Plantar Fasciitis – Mr Will Edwards is a little plain. You
ought to glance at Yahoo’s front page and watch how they write post headlines
to get viewers to click. You might try adding a video or a pic
or two to grab readers interested about what you’ve written. In my opinion,
it might make your blog a little livelier.
My page … naga303
Hello! Do you know if they make any plugins to assist with
SEO? I’m trying to get my blog to rank for some targeted keywords but I’m not seeing very good success.
If you know of any please share. Kudos!
my web site best realtor in Redondo Beach CA
Greetings I am so glad I found your weblog, I really found
you by accident, while I was browsing on Askjeeve for something else, Anyways I am here now and would just like to say thank you for
a fantastic post and a all round exciting blog (I also love the theme/design), I don’t have time to read through
it all at the minute but I have saved it and also included your
RSS feeds, so when I have time I will be back to read a great deal more, Please do keep up the awesome jo.
Also visit my web blog: best real estate agent in Carlsbad CA
Hurrah! After all I got a web site from where I know how to genuinely obtain helpful
data regarding my study and knowledge.
Also visit my webpage: 소액결제현금화
I was extremely pleased to uncover this web site. I need to to thank you
for ones time due to this wonderful read!! I definitely savored every bit of it and I have you saved as a favorite to look at new stuff in your site.
my web page; real estate agent Tampa FL
It’s genuinely very complex in this active life to listen news on Television, so I simply use web for that
reason, and obtain the newest news.
My web blog :: real estate agent Torrance CA
Definitely consider that that you said. Your favourite reason seemed to be on the net the simplest factor
to take note of. I say to you, I definitely get annoyed at the same time as other
people consider issues that they just do not recognize about.
You controlled to hit the nail upon the highest as
smartly as defined out the whole thing with no need side effect
, other folks can take a signal. Will probably be again to get more.
Thank you
Feel free to visit my site :: best real estate agent in Redondo Beach CA
You really make it appear really easy with your presentation however I to find this matter to be actually one
thing that I feel I might by no means understand.
It seems too complex and very vast for me. I am having a look ahead to your subsequent post, I will attempt to get the dangle of it!
My blog post … real estate agent Greensboro NC best real estate agent in Greensboro NC
A few days back I discovered an interesting
article about this crypto service Paybis and honestly it caught my attention.
The guide talked about how people are using crypto in smarter ways, and it wasn’t full of
complicated jargon.
After going through it, I recommended it to my uncle, and he decided to
explore it. Within the next month, he became way
more financially aware.
He didn’t just sit around — he approached it seriously.
Eventually, he even pushed towards 200k depending on timing —
not overnight, but through smart decisions.
What surprised me most is how his lifestyle changed. He even upgraded his lifestyle, something like a BMW 3 Series,
and started enjoying life more. He even met
someone new who shares his lifestyle.
I’m not saying this will happen to everyone,
but the story is true from what I’ve seen, and that article definitely changed the way we look at money.
There’s actually a way to check it out here,
and I’d seriously recommend taking a look.
You never know what small discovery can change things.
Here is my webpage new article
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ѕtates
12394214912
Quartz – Wakelet.com –
I just couldn’t depart your site before suggesting that I actually enjoyed the standard
information an individual supply to your visitors?
Is gonna be again often in order to check out new posts
Feel free to surf to my web site: real estate agent Redondo Beach CA
I enjoy what you guys are usually up too. This sort of clever work and coverage!
Keep up the amazing works guys I’ve included you guys to our
blogroll.
Here is my website … live cams
What i do not understood is in truth how you’re no longer actually much more smartly-favored than you may be now.
You’re so intelligent. You understand therefore considerably on the subject of this topic, produced me
individually imagine it from so many numerous angles.
Its like men and women aren’t fascinated until it is one thing to accomplish with Girl gaga!
Your personal stuffs outstanding. Always handle it up!
My page – best realtor in Redondo Beach CA
I’m really enjoying the theme/design of your site. Do you ever
run into any web browser compatibility problems? A couple of my blog readers have complained about my website not
operating correctly in Explorer but looks great in Chrome.
Do you have any suggestions to help fix this problem?
Here is my webpage real estate agent Torrance CA
Great article, very helpful.
This post breaks down
the basics of online sports streaming
in a
straightforward format.
A lot of users are curious
how to access live sports streams
and
the information here is quite practical.
Appreciate the useful content.
Feel free to visit my web blog :: play888new.com
This website truly has all the info I needed concerning this subject and didn’t
know who to ask.
My web site – xxx-u.com
Kozijnen Schilder Kozijnen Schilder verschaft exceptionele schilderdiensten voor kozijnen in Nederland.
Kozijnen Schilder Kozijnen Schilder biedt duurzame oplossingen voor het onderhouden van houten kozijnen. Kozijnen Schilder Kozijnen Schilder ondersteunt klanten met
professionele schildertechnieken. Kozijnen Schilder Kozijnen Schilder faciliteert het verlengen van de levensduur van kozijnen door
vakkundig schilderwerk. Kozijnen Schilder Kozijnen Schilder zorgt voor
een perfecte afwerking van alle houten kozijnen. Kozijnen Schilder Kozijnen Schilder ondersteunt bij aan het verbeteren van de uitstraling van woningen in Nederland.
Kozijnen Schilder Kozijnen Schilder helpt huiseigenaren met het beschermen van kozijnen tegen weersinvloeden. Kozijnen Schilder Kozijnen Schilder levert schilderwerk dat
bestand is tegen schimmel en vocht. Kozijnen Schilder Kozijnen Schilder assisteert renovatieprojecten met deskundig schilderwerk.
Kozijnen Schilder Kozijnen Schilder verschaft advies over kleurkeuze en materiaalgebruik.
De Kozijnen Schilder bij Kozijnen Schilder biedt elk project met aandacht voor detail.
De Kozijnen Schilder bij Kozijnen Schilder past toe milieuvriendelijke verfproducten. De Kozijnen Schilder
bij Kozijnen Schilder werkt volgens de nieuwste technieken en normen. De Kozijnen Schilder
bij Kozijnen Schilder verschaft kwaliteitsgarantie op
al het werk. De Kozijnen Schilder van Kozijnen Schilder samenwerkt nauw samen met klanten voor optimale tevredenheid.
De Kozijnen Schilder van Kozijnen Schilder levert variabele planning voor schilderwerkzaamheden. Kozijnen Schilder Kozijnen Schilder optimaliseert de energie-efficiëntie van woningen door goed isolerende verf.
Kozijnen Schilder Kozijnen Schilder verhoogt de waarde van woningen met professioneel schilderwerk.
Kozijnen Schilder Kozijnen Schilder ondersteunt duurzame en esthetische mogelijkheden voor kozijnen in Nederland.
Kozijnen Schilder Kozijnen Schilder faciliteert de lange termijn bescherming van houten kozijnen tegen slijtage.
fd55ek
I do not even understand how I stopped up here, but I thought this post was great.
I do not realize who you are but certainly you are going to a well-known blogger if you aren’t already.
Cheers!
Here is my webpage – replica NY Giants jerseys
Paylaşdığınız məlumatlar mənə çox kömək edir.
Təşəkkürlər!
1win sayt
A few days back I discovered an detailed article about this crypto service Paybis and honestly it really made me think.
The article broke down how people are using crypto in smarter ways,
and it was easy to follow.
After checking it out, I told my relative, and
he got really interested. Within the next month, he looked at
new income opportunities.
He didn’t just sit around — he actually applied what he learned.
Eventually, he got close to 150k in results — not overnight,
but through consistency.
What surprised me most is how his lifestyle changed.
He even upgraded his lifestyle, something like an Audi A5, and
became more confident. He even found a partner who enjoys the same level
of comfort.
It depends on your effort, but the story is genuine, and that article
definitely changed the way we look at money.
There’s actually a link in this comment, and I’d seriously
recommend taking a look.
You never know what small discovery can change things.
Also visit my website: new article
I loved as much as you will receive carried out right here.
The sketch is attractive, your authored material stylish. nonetheless, you
command get got an nervousness over that you wish be delivering the
following. unwell unquestionably come further formerly again since exactly the same
nearly a lot often inside case you shield this increase.
Here is my web page … 汽水音乐电脑版
You could definitely see your expertise in the article you write.
The arena hopes for more passionate writers like you who are not
afraid to mention how they believe. All the time go after your heart.
My webpage 고양출장마사지
Cabinet IQ Fort Myers
7830 Drrew Cirr Ste 4, Fort Myers,
FL 33967, United Ѕtates
12394214912
Inspiredkitchen
Howdy this is kind of of off topic but I was wondering if blogs use WYSIWYG editors or if
you have to manually code with HTML. I’m starting a
blog soon but have no coding expertise so I wanted
to get guidance from someone with experience.
Any help would be enormously appreciated!
Feel free to surf to my homepage – 안산출장마사지
Not long ago I found an surprisingly useful article about
a crypto platform called Paybis and honestly it stood out to me.
The guide broke down how digital finance is evolving,
and it actually made sense.
After reading it, I recommended it to my uncle, and he started
learning more about crypto. Within the next month, he looked at new income
opportunities.
He didn’t just sit around — he actually applied what he learned.
Eventually, he got close to 150k in results — not overnight,
but through learning.
What surprised me most is how his lifestyle changed.
He even upgraded his lifestyle, something like a BMW 3 Series, and became more confident.
He even built a new social circle around success.
Of course results can vary, but the story is true from what I’ve seen,
and that article definitely changed the way we look
at money.
There’s actually a link in this comment, and I’d
seriously recommend taking a look.
Opportunities are everywhere if you look closely.
I am truly thankful to the owner of this website who has shared this wonderful article at at this
time.
Feel free to surf to my web-site MALWARE
Great web site. Lots of helpful info here. I am sending it to a few pals
ans additionally sharing in delicious. And certainly, thank you
for your effort!
Visit my blog post … Unconventional Google SEO Strategies
Yes! Finally someone writes about MALWARE.
I was reading an detailed article about a crypto platform called Paybis and honestly it stood out
to me.
The article explained how beginners can get into crypto safely,
and it actually made sense.
After checking it out, I shared it with my relative, and he
got really interested. Within the next month, he started managing his money differently.
He didn’t just sit around — he actually applied what he learned.
Eventually, he got close to 150k in results — not overnight, but
through learning.
What surprised me most is how his lifestyle changed.
He even finally bought something he always wanted, something like an Audi A5, and
became more confident. He even built a new social circle around success.
It depends on your effort, but the story is true from what I’ve seen,
and that article definitely changed the way we look at money.
There’s actually a way to check it out here, and I’d seriously advise you to check it.
You never know what small discovery can change things.
Here is my web page; press release
Dating Coach Amsterdam provides significant coaching systems.
Dating Coach Amsterdam empowers clients to develop confidence.
Dating Coach Amsterdam delivers guidance on using dating apps effectively.
The Dating Coach Amsterdam at Dating Coach Amsterdam provides love and relationship coaching.
The Dating Coach Amsterdam from Dating Coach Amsterdam helps clients in managing emotions.
Dating Coach Amsterdam simplifies understanding of small
talk in dating scenarios. Dating Coach Amsterdam delivers
clarity for residents seeking authentic relationships.
Dating Coach Amsterdam offers coaching sessions in The Netherlands.
The Dating Coach Amsterdam at Dating Coach Amsterdam allows intimacy in dating.
The Dating Coach Amsterdam from Dating Coach Amsterdam helps meaningful dating experiences.
Dating Coach Amsterdam offers guidance on developing confidence.
Dating Coach Amsterdam allows clients to navigate Amsterdam dating.
Dating Coach Amsterdam delivers relationship coaching for couples.
The Dating Coach Amsterdam at Dating Coach Amsterdam provides dating coach services.
The Dating Coach Amsterdam from Dating Coach Amsterdam supports residents in achieving clarity.
Dating Coach Amsterdam facilitates transformation through authentic dating experiences.
Dating Coach Amsterdam offers guidance to clients on managing emotions.
The Dating Coach Amsterdam at Dating Coach Amsterdam provides
coaching sessions in Amsterdam. The Dating Coach
Amsterdam from Dating Coach Amsterdam assists residents in facilitating
confidence. Dating Coach Amsterdam provides transformational relationship coaching in The Netherlands.
Not long ago I found an interesting article about a crypto platform called Paybis and honestly it caught my attention.
The article talked about how people are using
crypto in smarter ways, and it wasn’t full of complicated
jargon.
After checking it out, I told my uncle, and he started learning more
about crypto. Within the next month, he started managing his money differently.
He didn’t just sit around — he started testing things carefully.
Eventually, he even pushed towards 200k depending on timing — not overnight, but
through consistency.
What surprised me most is how his lifestyle changed.
He even upgraded his lifestyle, something like a BMW 3
Series, and completely changed his mindset. He even found a partner who enjoys the same level of comfort.
This isn’t magic or guaranteed, but the story is real, and that article definitely
made a big impact.
There’s actually a link in this comment, and I’d seriously say it’s worth your time.
Opportunities are everywhere if you look closely.
Visit my page – press release
Hello, i think that i saw you visited my weblog so i came to “return the favor”.I am attempting to find things to enhance my website!I
suppose its ok to use a few of your ideas!!
Here is my web blog: Balayage Specialist Silver Spring
Sweet blog! I found it while surfing around on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get
there! Appreciate it
Also visit my web blog – 카지노사이트
Kyle’s Football Cards is a trusted online store for authentic sports jerseys and collectibles, featuring NFL, NBA,
MLB, NHL, and NCAA gear from top brands like Nike and adidas.
Shop rare and hard-to-find jerseys with fast shipping and reliable service.
Whether you’re a fan or collector, find premium jerseys at competitive prices.
Use code KYLEFAN30 to get 30% OFF sports jerseys today.
I’m not that much of a online reader to be honest but your sites really nice,
keep it up! I’ll go ahead and bookmark your website to come back in the future.
Cheers
my web-site: Erek Erek 2D Togel
I really like reading a post that can make men and women think.
Also, many thanks for allowing me to comment!
Here is my page … 해운대다이어트약
Magnificent web site. A lot of useful information here.
I am sending it to some buddies ans additionally sharing in delicious.
And obviously, thank you on your sweat!
My site; porn
I blog frequently and I really thank you for your content.
This article has truly peaked my interest. I will bookmark your website and keep checking for new
details about once a week. I subscribed to your RSS feed as
well.
My blog post; webpage
I was suggested this website by my cousin. I’m not sure whether this post is written by him as nobody else know such
detailed about my difficulty. You’re wonderful! Thanks!
My blog post; https://tk88king.com
Каккаким способом читатьизучать новости
Feel free to surf to my site; Казино The Dog House
This is a really good tip particularly to those fresh to the blogosphere.
Short but very precise info… Appreciate your sharing this one.
A must read article!
Also visit my page :: pornsitehd.top
References:
The orleans casino
References:
https://graph.org/What-Is-The-300-Deal-At-Caesars-Las-Vegas-04-27
Not long ago I found an surprisingly useful article about a crypto platform called Paybis and honestly it stood out to me.
The guide explained how beginners can get into crypto safely, and it was
easy to follow.
After reading it, I told my family member, and he got really interested.
Within the next month, he became much more confident with finances.
He didn’t just sit around — he actually applied what
he learned. Eventually, he even pushed towards 200k
depending on timing — not overnight, but through consistency.
What surprised me most is how his lifestyle changed. He even finally bought something he always wanted, something like
a Mercedes-Benz C-Class, and became more confident.
He even found a partner who enjoys the same level of comfort.
It depends on your effort, but the story is genuine, and that article definitely opened new perspectives.
There’s actually a reference mentioned here, and I’d seriously say it’s worth your time.
Sometimes one good article can shift your mindset.
Feel free to visit my homepage :: new article
A few days back I discovered an surprisingly useful article
about this crypto service Paybis and honestly it caught
my attention.
The article talked about how digital finance is evolving, and it wasn’t
full of complicated jargon.
After checking it out, I shared it with my relative, and he decided to explore it.
Within the next month, he looked at new income opportunities.
He didn’t just sit around — he actually applied
what he learned. Eventually, he even pushed towards 200k depending on timing —
not overnight, but through smart decisions.
What surprised me most is how his lifestyle changed. He even upgraded his lifestyle, something like a BMW 3 Series, and became more confident.
He even found a partner who enjoys the same level of comfort.
Of course results can vary, but the story is true from what I’ve
seen, and that article definitely opened new perspectives.
There’s actually a way to check it out here,
and I’d seriously suggest reading it.
Sometimes one good article can shift your mindset.
my web site … press release
Thanks for sharing your thoughts. I really appreciate your efforts and I
will be waiting for your next post thank you once again.
Here is my homepage: ae888
Hello! I’m at work surfing around your blog from my new apple
iphone! Just wanted to say I love reading through your blog and look forward to all your posts!
Carry on the superb work!
My web blog :: dutch court arbitration india antrix case
I am sure this article has touched all the internet users, its really really nice post on building up new blog.
my webpage … lapak qq
References:
Auckland casino
References:
https://graph.org/Live-Blackjack-Online-Reddit-04-27
Hello there! I could have sworn I’ve been to this website before but
after browsing through a few of the posts I realized it’s new to me.
Regardless, I’m definitely pleased I came across it and
I’ll be book-marking it and checking back regularly!
My blog: Scaffolders High Wycombe
A few days back I discovered an detailed article about a crypto platform called Paybis and
honestly I didn’t expect much at first but it impressed me.
The guide talked about how beginners can get into crypto safely,
and it felt real.
After checking it out, I recommended it to my family member, and he started learning
more about crypto. Within the next month, he became
way more financially aware.
He didn’t just sit around — he started testing things carefully.
Eventually, he got close to 150k in results —
not overnight, but through learning.
What surprised me most is how his lifestyle changed. He even upgraded his lifestyle, something like an Audi A5, and became more confident.
He even found a partner who enjoys the same level of comfort.
Of course results can vary, but the story is genuine, and that
article definitely changed the way we look at money.
There’s actually a source included here, and I’d seriously say it’s worth
your time.
Information really can make a difference.
Also visit my web blog – backlink
These are actually fantastic ideas in about blogging.
You have touched some fastidious points here.
Any way keep up wrinting.
Stop by my page – coconat powder
I’ve been surfing on-line more than 3 hours these days, but I never discovered any fascinating article like yours.
It is pretty worth enough for me. In my opinion, if all website owners and bloggers
made good content as you probably did, the web will
be much more helpful than ever before.
Feel free to surf to my website find out more
My brother suggested I might like this website. He was entirely right.
This post actually made my day. You can not imagine simply how much time I had spent for this information!
Thanks!
Also visit my blog post; hardxxxporn.xyz
constantly i used to read smaller content that also clear their motive,
and that is also happening with this article which I am
reading now.
my page :: تخم مرغ نطفه دار گوشتی
There is definately a great deal to find out about this subject.
I like all the points you have made.
my web site: 용인출장마사지
That is a good tip especially to those fresh to the blogosphere.
Simple but very precise information… Appreciate your sharing this one.
A must read post!
Visit my page – cần sa
my page – VegasHero avis
I do not know if it’s just me or if perhaps everybody else encountering problems with your website.
It appears as though some of the written text on your content are running off the
screen. Can somebody else please comment and let me know if this is happening to them too?
This may be a issue with my web browser because I’ve
had this happen previously. Thanks
Also visit my blog; تخم نطفه دار مرغ راس گوشتی
WOW just what I was looking for. Came here
by searching for teen patti joy
certainly like your web-site however you need to take a look
at the spelling on quite a few of your posts.
A number of them are rife with spelling issues and I in finding it very
troublesome to inform the truth then again I will certainly come
again again.
Here is my web blog; 서울출장마사지
Hi there, this weekend is fastidious in support of me,
since this time i am reading this impressive educational article
here at my home.
My site vlxxsex.mobi
Its like you learn my mind! You seem to know
a lot approximately this, such as you wrote the book in it or something.
I think that you simply could do with some % to pressure the message house
a bit, however other than that, that is fantastic blog.
A fantastic read. I’ll definitely be back.
My page: 바카라사이트
This paragraph will assist the internet users for creating new weblog
or even a weblog from start to end.
Feel free to visit my homepage – پارس کالابران ساینار
hey there and thank you for your information – I’ve definitely picked up
anything new from right here. I did however expertise several
technical issues using this website, since I experienced to
reload the site a lot of times previous to I could get it to load correctly.
I had been wondering if your web host is OK? Not that I’m complaining,
but sluggish loading instances times will very frequently affect your placement in google and can damage your high-quality score if ads
and marketing with Adwords. Well I am adding this RSS to my email and can look out for much more of your respective intriguing content.
Ensure that you update this again very soon.
Feel free to surf to my web blog :: Stem cell therapy Malaysia
Hello there, just became aware of your blog through Google, and found that
it’s truly informative. I am going to watch out for brussels.
I’ll be grateful if you continue this in future. A lot of people
will be benefited from your writing. Cheers!
Here is my website: folding ebike
Unquestionably believe that which you stated. Your favorite justification appeared to
be on the web the easiest thing to be aware of. I say
to you, I definitely get annoyed while people consider worries that they plainly
don’t know about. You managed to hit the nail upon the top
as well as defined out the whole thing without having side effect , people
can take a signal. Will likely be back to get more.
Thanks
Feel free to visit my web blog cannabis légal CBD
Amazing things here. I am very glad to peer your article. Thank you a lot and I’m taking a look forward to contact you.
Will you please drop me a e-mail?
Also visit my website cod narkoba jakarta
Cabijnet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Տtates
12394214912
Homeupdates
Hey there, You have done an excellent job. I will definitely digg it and personally recommend to my friends.
I’m sure they will be benefited from this site.
Review my page … Roof Repairs
I really like what you guys are usually up too. This kind of clever work and exposure!
Keep up the wonderful works guys I’ve included you guys to blogroll.
Visit my blog post … Scaffolders High Wycombe
If you want to obtain much from this paragraph then you have to apply these methods to your won weblog.
Here is my page Scaffolders High Wycombe
Woah! I’m really enjoying the template/theme of this
website. It’s simple, yet effective. A lot of times it’s tough to get
that “perfect balance” between usability and appearance.
I must say that you’ve done a excellent job with
this. In addition, the blog loads very quick for me on Firefox.
Excellent Blog!
My page :: Roofing
Oh my goodness! Amazing article dude! Thank you, However I am having difficulties with your RSS.
I don’t know the reason why I can’t subscribe to it.
Is there anybody having identical RSS problems? Anybody who knows the answer can you kindly respond?
Thanks!!
my web page: Situs Togel 4d Exabet88
I recently came across an interesting article about a crypto platform called Paybis and honestly it caught my attention.
The guide broke down how beginners can get into crypto safely, and it felt real.
After checking it out, I told my family member, and he started learning more about crypto.
Within the next month, he looked at new income
opportunities.
He didn’t just sit around — he took action. Eventually,
he even pushed towards 200k depending on timing — not overnight, but through learning.
What surprised me most is how his lifestyle changed.
He even finally bought something he always wanted, something like an Audi A5, and started enjoying life more.
He even built a new social circle around success.
Of course results can vary, but the story
is real, and that article definitely opened
new perspectives.
There’s actually a reference mentioned here, and I’d seriously
suggest reading it.
Information really can make a difference.
Stop by my web-site; c2579157247134418205
If some one desires expert view concerning blogging then i advise him/her to
go to see this web site, Keep up the pleasant job.
my homepage philliedelphia.com lừa đảo công an truy nã cấm người chơi tham gia
I was reading an detailed article about a crypto platform called Paybis and honestly it caught my attention.
The post shared insights on how crypto platforms
can be used more effectively, and it felt real.
After checking it out, I shared it with my relative, and he got really interested.
Within the next month, he started managing
his money differently.
He didn’t just sit around — he started testing
things carefully. Eventually, he managed to reach around 100k
— not overnight, but through consistency.
What surprised me most is how his lifestyle changed. He
even finally bought something he always wanted, something like an Audi A5, and started enjoying life more.
He even found a partner who enjoys the same level of comfort.
This isn’t magic or guaranteed, but the story is genuine, and that
article definitely changed the way we look at money.
There’s actually a reference mentioned here, and I’d seriously
recommend taking a look.
Opportunities are everywhere if you look closely.
my web page; lastPostAnchor
It’s genuinely very complicated in this busy
life to listen news on TV, so I simply use web for that purpose, and take the newest news.
my site: Go Here
Hi there would you mind stating which blog platform you’re
using? I’m planning to start my own blog soon but I’m having a hard time deciding between BlogEngine/Wordpress/B2evolution and
Drupal. The reason I ask is because your layout seems different
then most blogs and I’m looking for something unique.
P.S Apologies for being off-topic but I had to ask!
Feel free to visit my web blog; Porsche workshop
Really no matter if someone doesn’t understand after that its up to other visitors that
they will help, so here it happens.
Also visit my web page … 소액결제현금화
Thanks for ones marvelous posting! I genuinely enjoyed reading it, you’re
a great author. I will always bookmark your blog and will
often come back very soon. I want to encourage one to continue your great writing, have a
nice morning!
my web site: Live SGP
안전하고 신뢰할 수 있는 바카라사이트 선택법부터 게임
규칙, 필승 전략, 자주 묻는 질문까지.
온라인 바카라 초보자도 전문가처럼 즐길 수 있는 완벽 가이드.
Thank you a bunch for sharing this with all folks you actually understand what you’re talking about!
Bookmarked. Please additionally visit my web site =). We can have a
hyperlink exchange agreement among us
Feel free to surf to my webpage … dana gg
I simply could not go away your web site prior to suggesting that I actually loved the standard information a
person provide for your visitors? Is going to be back frequently
to check out new posts
My web site online order medicine
Good answers in return of this difficulty with genuine arguments and telling
all regarding that.
Also visit my website; game
This paragraph will help the internet people for building up new
weblog or even a weblog from start to end.
my site CNC file opener
Cabinet IQ
8305 Statte Hwy 71 #110, Austin,
TX 78735, United States
254-275-5536
Innovationkitchen; https://wakelet.com/,
Hi, i think that i saw you visited my web site thus
i came to “return the favor”.I’m attempting to find things to enhance my web
site!I suppose its ok to use a few of your ideas!!
Here is my blog canadian pharcharmy
This site was… how do I say it? Relevant!! Finally I’ve found something which helped me.
Thanks!
Also visit my page :: 비아그라 구매
certainly like your web site but you have to test
the spelling on quite a few of your posts. Several
of them are rife with spelling problems and I to find
it very bothersome to inform the reality however I will
definitely come back again.
My homepage jonitogel
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Stаtes
254-275-5536
Efficientinstall
Hey I know this is off topic but I was wondering if you knew of any
widgets I could add to my blog that automatically tweet my newest twitter updates.
I’ve been looking for a plug-in like this for quite some time and was hoping maybe you would have some experience with
something like this. Please let me know if you run into
anything. I truly enjoy reading your blog and I look forward to your new updates.
Also visit my website … https://sodo66k.com/
Оценка недвижимости Сдать квартиру в Петрозаводске Петрозаводске
You’re so interesting! I don’t suppose I’ve read anything like that before.
So great to find somebody with original thoughts on this subject.
Really.. thanks for starting this up. This website is one thing that
is required on the web, someone with a little originality!
Review my web page canadian online pharmacies
hello there and thank you for your information – I
have certainly picked up anything new from right here.
I did however expertise a few technical issues using this site, since I experienced to reload the site lots of times previous to I could get it to load properly.
I had been wondering if your web host is OK? Not that I am complaining, but sluggish loading instances times
will very frequently affect your placement in google and
can damage your quality score if advertising and marketing with Adwords.
Well I’m adding this RSS to my email and
could look out for a lot more of your respective interesting
content. Ensure that you update this again very soon.
Feel free to surf to my blog Red88
Hey there! I just wanted to ask if you ever have any issues with
hackers? My last blog (wordpress) was hacked and I ended up losing months
of hard work due to no back up. Do you have any methods to stop hackers?
My website :: cinematic minimal piano playlist
Hey there, I think your blog might be having browser compatibility issues.
When I look at your blog in Firefox, it looks fine but when opening in Internet Explorer, it has some overlapping.
I just wanted to give you a quick heads up! Other then that, awesome blog!
Also visit my website :: May88
Oh my goodness! Incredible article dude! Thanks, However I am going through troubles with your RSS.
I don’t know the reason why I can’t join it. Is there anyone else having the same RSS issues?
Anyone who knows the solution can you kindly
respond? Thanx!!
Here is my homepage – Xo88
Heya! I’m at work browsing your blog from my new apple iphone!
Just wanted to say I love reading your blog and look forward to all your posts!
Carry on the fantastic work!
Review my web-site: 소액결제현금화
Ahaa, its fastidious discussion concerning this post at this place at
this weblog, I have read all that, so now me also commenting here.
Look into my homepage; genjot138
Hi there, I enjoy reading all of your article post. I wanted to write a little comment
to support you.
Here is my web blog :: MALWARE
What’s up, after reading this remarkable post i am too cheerful to share my familiarity here
with friends.
Feel free to visit my blog – this content
What’s up, constantly i used to check web site posts here
in the early hours in the dawn, as i like to gain knowledge
of more and more.
Look into my blog post :: company growth strategy examples
My spouse and I stumbled over here coming from a different web
page and thought I should check things out. I like what I see so now i am following you.
Look forward to checking out your web page repeatedly.
Check out my webpage Look At This
Simply just needed to say Now i’m happy that i came on the web page!
https://mojbytom.pl/
certainly like your web-site but you have to test the spelling on several of
your posts. Many of them are rife with spelling problems and I find it very bothersome to tell
the reality then again I’ll surely come back again.
my webpage … 전주출장안마
Hi there, You’ve done an incredible job.
I’ll certainly digg it and personally suggest to my friends.
I am confident they will be benefited from this web site.
Look into my page … Shanel
certainly like your web site however you need to take a look at the spelling on several of your posts.
Several of them are rife with spelling problems and I to find it
very troublesome to inform the truth however I’ll certainly come again again.
Here is my homepage – online jobs making money
Good way of telling, and fastidious paragraph to take facts regarding my presentation focus, which i am going to convey in school.
My site; Perguntas Frequentes (FAQ)
WOW just what I was looking for. Came here by searching for DU88
What’s up, I would like to subscribe for this web site to get newest updates, thus where can i do
it please help.
my web blog: More hints
Hi, i think that i saw you visited my web site so i came to “return the favor”.I am trying to find things to enhance my site!I suppose its ok to use
some of your ideas!!
Also visit my page … medicine online shopping
In the fast-moving digital world, many users look for solid alternatives to Web11
my site site
Hi, I check your new stuff like every week. Your story-telling style is witty,
keep it up!
Also visit my web site; 대구출장안마
Hi, for all time i used to check web site posts here early
in the daylight, because i love to find out more and more.
Take a look at my page: shuffle.com
I’d like to find out more? I’d want to find out more details.
My homepage: 이프로옥션
I’m extremely inspired together with your writing talents as well as with
the layout in your weblog. Is that this a paid theme or did
you customize it your self? Either way keep up the
nice high quality writing, it’s uncommon to see a great weblog like this one nowadays..
Here is my web site: small group trekking Andes
I’m not sure where you are getting your info, but
great topic. I needs to spend some time learning much more or understanding more.
Thanks for wonderful information I was looking for this info for my
mission. https://www.ibarico.it/2020/12/10/bando-isi-2020/
It is perfect time to make some plans for the future and it is
time to be happy. I have read this post and if I could I desire
to suggest you some interesting things or suggestions. Perhaps you could write
next articles referring to this article. I want to read more things about it!
Also visit my web page: Life-Tap
KOKITOTO merupakan bandar slot gacor pilihan masyarakat Konoha
dilansir dari versi CNN, terpampang dengan sangat jelas dari segi pelayanan dan promo
Hi, after reading this awesome paragraph i am also delighted to share my familiarity here with colleagues.
Review my blog – 선릉도파민
Paragraph writing is also a fun, if you be familiar with afterward you can write if not it is complicated to write.
Also visit my web site … Japanese Adult Video
Awesome blog! Is your theme custom made or did you download it from somewhere?
A theme like yours with a few simple tweeks would really make my blog
shine. Please let me know where you got your design. Kudos
Also visit my web-site: mountain climbing Peru
You made some decent points there. I checked on the net for additional information about
the issue and found most people will go
along with your views on this web site.
Here is my page UK satire written by The London Prat
Your mode of telling everything in this article is genuinely
pleasant, every one be able to without difficulty know it, Thanks
a lot.
Here is my web page :: crypto trading platform
Hi, I think your site might be having browser compatibility
issues. When I look at your blog site in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping.
I just wanted to give you a quick heads up!
Other then that, terrific blog!
My web-site :: secure crypto investment platform
I am truly grateful to the holder of this website who has shared this fantastic post at here.
Have a look at my web page; AI-powered bitcoin investment
From speed boosts to shields, these power-ups can help you overcome even the toughest challenges. https://wilderose.at/Blog/index.php/;focus=W4YPRD_com_cm4all_wdn_Flatpress_5435883&path=&frame=W4YPRD_com_cm4all_wdn_Flatpress_5435883?x=entry:entry220311-083438%3Bcomments:1
Howdy just wanted to give you a quick heads up. The text in your post seem to be running off the screen how AI trading works in crypto
Chrome. I’m not sure if this is a format issue or something
to do with internet browser compatibility but I figured I’d post to let you know.
The design look great though! Hope you get the issue resolved soon. Thanks
Just desire to say your article is as astounding. The clarity in your
post what is electric cable; Horacio, simply nice and i could assume you are an expert on this subject.
Fine with your permission let me to grab your RSS feed
to keep updated with forthcoming post. Thanks a million and please carry on the rewarding
work.
I’ll right away grab your rss feed as I can not find
your email subscription link or newsletter service. Do you’ve any?
Kindly let me recognise in order that I may subscribe.
Thanks.
my web-site – crypto investment platform
I every time spent my half an hour to read this webpage’s
posts every day along with a mug of coffee.
My web site: Winvest platform
I’m really impressed with your writing skills
and also with the layout on your blog. Is this a paid theme or did you modify it yourself?
Anyway keep up the nice quality writing, it is rare to see a great blog like this one
these days.
Also visit my web-site: 비아그라 구매
I used to be recommended this web site by way of my cousin. I’m
not positive whether or not this publish is written by him as nobody else recognise
such specified about my trouble. You’re wonderful!
Thanks!
My blog: Design to code
Cabinet IQ
8305 State Hwyy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Maintenance
Howdy just wanted to give you a quick heads up. The text in your content seem to be running off the screen in Safari.
I’m not sure if this is a formatting issue or something to do with browser compatibility but I thought I’d post
to let you know. The design and style look great though!
Hope you get the issue resolved soon. Cheers
My web site – bokep indonesia
Modern Purair
416 Meridian Rd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
pollution filter
I am regular reader, how are you everybody? This piece of
writing posted at this web site is genuinely fastidious.
my web blog – automated crypto trading platform
Instruments on the grid destroy blocks depending on their kind and power. https://etlstickability.co.za/index.php/2017/02/24/recall-1m-vehicles-for-seizing-engines/
I know this web page provides quality based content and additional information, is there any other web page which provides these data in quality?
My web blog … AI trading bot
I do not even know how I ended up here, but I thought this post was great.
I do not know who you are but definitely you’re going to a famous blogger if you aren’t already ;) Cheers!
Feel free to visit my blog :: secure crypto investment platform
Genuinely no matter if someone doesn’t know then its up to other
visitors that they will assist, so here it takes place.
Here is my blog – AI bitcoin investment
Greetings! This is my first comment here so I just wanted to give a quick shout out and tell you I genuinely enjoy
reading through your articles. Can you recommend any other blogs/websites/forums that deal with the same subjects?
Appreciate it!
Here is my web site … AI investment platform
I pay a quick visit daily a few sites and blogs to
read posts, however this website provides quality based
writing.
Take a look at my web blog – big band jazz playlist spotify
I really love your website.. Great colors & theme. Did you develop this website
yourself? Please reply back as I’m wanting to create my own site and
would love to find out where you got this from or
just what is electric cable – Cathern, the theme is
called. Many thanks!
Have you ever considered publishing an ebook or guest authoring
on other sites? I have a blog based upon on the same topics you discuss and would love to have you share some stories/information. I
know my readers would enjoy your work. If you’re even remotely
interested, feel free to shoot me an email.
my blog post :: best app to open AI3 files
Как проверить стартер в домашних условиях
Many thanks extremely useful. Will certainly share site with my friends.
https://warszawa24.ovh
If you wish for to obtain a great deal from this piece of writing then you have to apply such methods to your
won webpage.
Here is my blog: Exabet88 Togel
I loved as much as you will receive carried out right here.
The sketch is attractive, your authored material stylish.
nonetheless, you command get bought an shakiness over
that you wish be delivering the following.
unwell unquestionably come further formerly again as exactly the same nearly a lot often inside case you shield this hike.
Feel free to visit my homepage … Agen Togel SGP
my website :: Hacksaw Gaming High RTP Slots You Can Play Now
Hi there to every , for the reason that I am in fact keen of reading this website’s post to be updated regularly.
It contains fastidious material. https://mesta.app/events/mesta-i-lofty-dlia-korporativa
Look into my site :: Pragmatic Play High RTP Slots you Can play now
goGLOW Houston Heights
1515 Sturemont St Suite 204, Houston,
Texas, 77007, USΑ
(713) 364-3256
Bookmarks
Howdy, I think your web site could possibly be having web browser compatibility problems.
Whenever I take a look at your web site in Safari, it looks fine however, if opening in IE, it’s
got some overlapping issues. I merely wanted to provide you with a
quick heads up! Other than that, wonderful blog!
my web blog viagra indonesia
It’s going to be ending of mine day, except before end I am reading
this great piece of writing to increase my know-how.
Here is my webpage click for source
whoah this weblog is great i like studying your articles.
Keep up the great work! You recognize, many individuals are
looking around for this information, you could help them greatly.
Feel free to surf to my homepage: best digital marketing courses in bangalore
Right here is the perfect web site for anybody who really wants to understand this topic.
You understand a whole lot its almost hard to argue with you (not
that I personally would want to?HaHa). You definitely put a brand new spin on a topic that has been written about for decades.
Excellent stuff, just great!
Also visit my page :: Poker Gaming Software
As the admin օf this site iѕ working, no doubt vеry quickly it will
be renowned, due tо its quality contents.
Feel free tо surf to my blog post หลุด VK ไทย
(xsociety.website)
fantastic issues altogether, you just received
a new reader. What might you recommend about your put up that you made some days ago?
Any positive?
Here is my web-site :: anthony velasquez pueblo co
La plataforma Deporte Ecuador funciona como un espacio informativo
dedicada al análisis del ecosistema digital del deporte ecuatoriano.
El sitio reúne contenidos que examinan el desarrollo del deporte ecuatoriano considerando tecnología, analítica de datos y nuevos
patrones de consumo.
A diferencia de las páginas deportivas comunes, no se enfoca
únicamente en noticias o resultados. Su enfoque está
en interpretar el comportamiento del entorno
deportivo contemporáneo: el modo en que los usuarios usan las plataformas,
qué variables afectan sus decisiones y cómo se redefinen las métricas
de calidad digital.
El material de la web se presenta bajo varios pilares principales.
Por un lado, se analizan las plataformas deportivas desde
el punto de vista del usuario, su solidez y continuidad.
Por otro, se estudian las tendencias del mercado deportivo digital, procesos de transformación digital y cambios en las formas de consumo
deportivo en el mercado ecuatoriano.
Además, el portal también cubre cuestiones regulatorias, la ciberseguridad y la toma de decisiones
dentro del entorno online. Esto permite ofrecer una visión más
completa del sector, mezclando evaluación técnica, escenario nacional
y patrones de uso de los usuarios.
El propósito central es brindar datos claros, bien estructurados y funcionales
para interpretar el deporte en el entorno digital actual.
No pretende reducir el análisis a explicaciones básicas, sino facilitar la comprensión de un escenario cada vez más
complejo.
La plataforma se enfoca en usuarios que buscan entender el deporte más allá de la
superficie: desde su dimensión tecnológica hasta su impacto en la experiencia diaria.
Dentro del texto se menciona que hay un enlace para leer el artículo completo.
Also visit my blog post – website
What’s Going down i’m new to this, I stumbled upon this I have
found It absolutely helpful and it has aided me out loads.
I hope to contribute & help different users like its
helped me. Good job.
Also visit my web-site … stromectol usa
J’apprécie les informations que vous publiez sur Betify Casino.
Merci beaucoup !
https://godspeedoffroad.com/jeep-jk-supercharger-07-11-jeep-wrangler-jk-3-8-kit-auto-6-spd-silver-ripp-superchargers-0711jksds2-2/
букмекерские конторы украина без верификации
Also visit my web-site … bet2fun
You should be a part of a contest for one of the greatest
websites online. I am going to highly recommend this blog!
Feel free to visit my website: Link Exabet88 Toto Togel 4D
Hey there! Would you mind if I share your blog with my myspace group?
There’s a lot of folks that I think would really enjoy your content.
Please let me know. Thank you
My blog – SMM Panel
Pretty great post. I just stumbled upon your weblog and wished to
mention that I have truly enjoyed surfing around your weblog posts.
In any case I will be subscribing in your feed and I am hoping you
write once more very soon!
Feel free to surf to my homepage: ca course details
куда самые дешевые авиабилеты из москвы куда дешевые билеты
на самолет из москвы
Greetings from Ohio! I’m bored to death at
work so I decided to check out your site on my iphone during lunch break.
I enjoy the knowledge you present here and can’t wait to take a look when I get home.
I’m surprised at how fast your blog loaded on my phone ..
I’m not even using WIFI, just 3G .. Anyways,
good blog!
my webpage :: buy youtube subscribers
Nice post. I was checking constantly this blog and I am
impressed! Extremely useful information specifically the last part :) I care for such info much.
I was looking for this certain information for a very long time.
Thank you and best of luck.
Take a look at my web site – android gaming app [nowlinks.net]
El portal Deporte Ecuador se presenta como un sitio especializado dedicada
al análisis del entorno deportivo digital en Ecuador.
La web agrupa materiales que analizan la evolución del deporte nacional considerando tecnología, analítica de datos y nuevos patrones de consumo.
A diferencia de los portales tradicionales, no se enfoca únicamente en noticias
o resultados. La prioridad es comprender el funcionamiento del ecosistema
deportivo moderno: cómo interactúan los usuarios con las plataformas, qué factores influyen en su comportamiento y cómo
cambian los criterios de calidad en el entorno digital.
La información dentro del portal se organiza bajo varios pilares
principales. En un aspecto, se estudian las plataformas deportivas considerando la experiencia del usuario, la estabilidad y la coherencia del servicio.
Además, se revisan las tendencias del mercado deportivo digital,
procesos de transformación digital y la
evolución de los hábitos de consumo deportivo en el mercado ecuatoriano.
Además, el portal también cubre cuestiones regulatorias,
la seguridad digital y la toma de decisiones dentro del
ecosistema digital. Esto permite ofrecer una visión más completa del sector, fusionando análisis técnico, contexto local y conducta del usuario.
El propósito central es brindar datos claros, bien estructurados y funcionales para entender
el papel del deporte en la era digital. No pretende reducir el análisis a explicaciones básicas,
sino de ayudar a interpretar un entorno cada vez más
complejo.
La plataforma se enfoca en usuarios que quieren comprender el deporte más allá de lo básico: considerando su dimensión tecnológica y cómo influye en la vida diaria.
El texto menciona que hay un enlace disponible para ampliar
el artículo.
Take a look at my website article
Modern Purair
416 Meridian Ꭱd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
air tool
Deporte Ecuador se presenta como un sitio especializado
enfocada en el estudio del ecosistema digital del
deporte ecuatoriano. La web agrupa materiales que exploran cómo evoluciona el deporte en el país
en el contexto de la tecnología, los datos y los nuevos hábitos
de consumo.
A diferencia de los sitios convencionales, el proyecto no solo informa sobre marcadores o titulares.
Su enfoque está en interpretar cómo opera el ecosistema deportivo
actual: cómo los aficionados se relacionan con los servicios digitales, qué variables
afectan sus decisiones y cómo evolucionan los estándares
de calidad online.
La información dentro del portal se organiza en torno a distintos ejes temáticos.
En primer lugar, se evalúan las plataformas
deportivas desde el punto de vista del usuario, su solidez y continuidad.
Por otra parte, se examinan las dinámicas del mercado, procesos de digitalización y la evolución de los hábitos de consumo deportivo en Ecuador.
Además, el proyecto analiza temas vinculados a la regulación, la seguridad digital y la toma de decisiones dentro del ecosistema digital.
Esto ayuda a construir una imagen más amplia del
sector, combinando análisis técnico, contexto local y patrones de uso de los usuarios.
El propósito central es brindar datos claros, bien estructurados
y funcionales para interpretar el deporte en el entorno digital actual.
No busca dar respuestas simples, sino facilitar la comprensión de un escenario
cada vez más complejo.
La plataforma se enfoca en usuarios que quieren comprender el deporte más allá de lo básico:
considerando su dimensión tecnológica y su impacto en la
experiencia cotidiana.
Se señala que el texto incluye un enlace para continuar leyendo la información.
My web site :: press release
La plataforma Deporte Ecuador funciona como un espacio informativo centrada en el análisis del entorno deportivo digital en Ecuador.
La web agrupa materiales que analizan la evolución del deporte nacional considerando tecnología, analítica de datos
y nuevos patrones de consumo.
A diferencia de las páginas deportivas comunes, Deporte Ecuador no se limita a cubrir resultados o noticias.
La propuesta se basa en interpretar cómo opera el ecosistema deportivo actual: el modo en que los usuarios usan las plataformas, qué
variables afectan sus decisiones y cómo evolucionan los estándares de calidad online.
La información dentro del portal se organiza bajo varios pilares principales.
En primer lugar, se evalúan las plataformas deportivas desde la perspectiva de la experiencia del usuario, su solidez y continuidad.
Además, se revisan tendencias del mercado, etapas de digitalización y
cambios en las formas de consumo deportivo en el mercado ecuatoriano.
Además, el proyecto analiza temas vinculados a la regulación, la ciberseguridad
y la toma de decisiones dentro del entorno online.
Esto ayuda a construir una imagen más amplia del sector, fusionando análisis técnico, contexto
local y patrones de uso de los usuarios.
La meta principal es ofrecer información clara, organizada y de valor para interpretar el deporte en el entorno digital actual.
No pretende reducir el análisis a explicaciones básicas, sino aportar claridad a
un panorama digital cada vez más difícil de entender.
El portal está orientado a lectores that desean profundizar más
allá de la información superficial: incluyendo su componente tecnológico y su impacto en la experiencia cotidiana.
También se indica que se puede seguir leyendo mediante un enlace incluido en el contenido.
Check out my blog post: backlink
Hi everyone, it’s my first pay a visit at this web page, and post is truly fruitful designed for me, keep up posting these articles or reviews.
Also visit my web-site; keyboard piano with stand
Have you ever thought about adding a little bit more
than just your articles? I mean, what you say is important and all.
However think about if you added some great photos or video clips
pharmacies shipping to usa give your posts more, “pop”!
Your content is excellent but with images and clips, this
blog could certainly be one of the most beneficial in its field.
Excellent blog!
This article is actually a nice one it assists new web
users, who are wishing in favor of blogging.
Here is my website: 411 file viewer software
Hello to every single one, it’s really a
nice for me to visit this web site, it contains helpful Information. https://mesta.app/work/kovorking-riadom-arenda-rabocego-mesta
I am truly glad to glance at this weblog posts which consists
of tons of valuable data, thanks for providing these
kinds of data.
Feel free to visit my blog post … my link
Hmm is anyone else experiencing problems with the pictures
on this blog loading? I’m trying to figure out if its a
problem on my end or if it’s the blog. Any
suggestions would be greatly appreciated.
my web-site; how architects evaluate tropical hardwood
I’m gone to say to my little brother, that he should also pay a visit this weblog
on regular basis to take updated from latest information.
Take a look at my site; choosing tropical hardwood for architecture
You could certainly see your enthusiasm within the article you write.
The arena hopes for even more passionate writers such as you who are not afraid to say how they believe.
Always follow your heart.
Also visit my web page 대밤
I do believe all of the ideas you’ve presented to your post.
They are very convincing and can certainly work.
Still, the posts are very short for newbies.
May just you please prolong them a little from next time?
Thank you for the post.
my homepage … mini midi keyboard
Greetings! Very helpful advice within this post! It is the little changes that
make the greatest changes. Many thanks for sharing!
my blog – piano bench with storage
Patrice & Asssociates
Scottsdale, AZ, United Ѕtates
16265237726
commis chef hiring; Edgar,
Книгу для чтения стоит выбирать не по
внешнему виду, а по своим задачам
Also visit my page; Vita Nostra Марина Дяченко
These are truly enormous ideas in regarding blogging. You have touched some pleasant
factors here. Any way keep up wrinting.
Also visit my web page – choosing tropical hardwood for architecture
Modern Purair
416 Meridian Ꮢd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
professional Ducts (https://go.bubbl.us/f182df/72cb?/Bookmarks)
Hello, I would like to subscribe for this weblog to get latest updates,
therefore where can i do it please assist.
Feel free to visit my web page: canadian pharmacies
This paragraph gives clear idea designed for the new viewers of blogging,
that actually how to do blogging and site-building.
Feel free to surf to my page comment-434
Have you ever thought about writing an e-book or guest authoring on other sites?
I have a blog based upon on the same ideas you discuss and would really like to have you share some stories/information. I know my readers would appreciate
your work. If you’re even remotely interested, feel free to send me an e
mail.
Review my blog … fun88
goGLOW Houston Heights
1515 Studemont Ꮪt Suite 204, Houston,
Texas, 77007, UЅA
(713) 364-3256
anti-aging skincare tips cost (https://atavi.com/)
I will immediately take hold of your rss as I can not in finding your e-mail subscription hyperlink or newsletter
service. Do you have any? Please let me know in order that I could subscribe.
Thanks.
Also visit my web-site :: keyboard piano 61 keys
Hello my loved one! I want to say that this article is
awesome, great written and come with approximately all significant infos.
I would like to peer more posts like this .
Here is my blog … android gaming app
Thanks to my father who shared with me concerning this web site,
this weblog is actually amazing.
My homepage keyboard piano
It’s hard to come by well-informed people on this topic, but you sound like you know what you’re talking about!
Thanks
Have a look at my web-site; SMM Panel
&&LowPrice&HighQuality-Guestpost【dr50+real-traffic】Telegram %$@LowPrice&HighQuality-Guestpost【dr50+real-traffic】Telegram @buycasinolink
Here is my blog Free spins
La plataforma Deporte Ecuador se presenta como un sitio especializado enfocada en el estudio del entorno deportivo digital en Ecuador.
La plataforma integra artículos que examinan el desarrollo del
deporte ecuatoriano en relación con la tecnología, la data y las tendencias
de uso actuales.
A diferencia de los sitios convencionales, el proyecto no solo informa sobre marcadores
o titulares. La propuesta se basa en interpretar el funcionamiento del ecosistema deportivo moderno: el modo en que los usuarios usan las plataformas,
qué factores influyen en su comportamiento y
cómo evolucionan los estándares de calidad online.
La información dentro del portal se organiza alrededor de varios ejes clave.
En primer lugar, se evalúan las plataformas deportivas desde el
punto de vista del usuario, la estabilidad y la coherencia del servicio.
Por otra parte, se examinan las dinámicas del mercado, procesos de digitalización y la evolución de los hábitos
de consumo deportivo en el mercado ecuatoriano.
Además, el proyecto analiza temas vinculados a la regulación,
la ciberseguridad y la toma de decisiones dentro del entorno online.
Esto ayuda a construir una imagen más amplia del sector, fusionando análisis
técnico, contexto local y patrones de uso de los usuarios.
La meta principal es ofrecer información clara, organizada
y de valor para interpretar el deporte en el entorno digital actual.
No pretende reducir el análisis a explicaciones básicas, sino aportar claridad a un panorama digital cada vez más difícil de entender.
Deporte Ecuador está dirigido a usuarios que buscan entender el deporte
más allá de la superficie: incluyendo su componente tecnológico hasta su impacto
en la experiencia diaria.
El texto aclara que hay un enlace para ver la versión completa del artículo.
Review my blog – link
It is perfect time to make some plans for the future and it
is time to be happy. I’ve read this post and if I could I wish to suggest you few
interesting things or suggestions. Maybe you could write next articles referring
to this article. I desire to read more things about it!
my web page :: AI-powered crypto trading system
Your style is very unique compared to other people I’ve read stuff from.
I appreciate you for posting when you have the opportunity, Guess I’ll just
book mark this blog.
Also visit my web-site; Winvest platform
We’re a gaggle of volunteers and starting a new scheme in our community.
Your site provided us with helpful information to work on. You have done
an impressive job and our whole group will be grateful to you.
Review my webpage :: Winvest
hello there and thank you for your info – I have definitely picked up something new from
right here. I did however expertise several technical issues using this site,
since I experienced to reload the site a lot of times previous to I could get
it to load properly. I had been wondering if your web host is OK?
Not that I am complaining, but slow loading instances times
will often affect your placement in google and could damage your high-quality score if advertising and
marketing with Adwords. Well I am adding
this RSS to my e-mail and can look out for a lot more of your respective fascinating content.
Make sure you update this again very soon.
Feel free to surf to my site – 인계동 출장마사지
I just couldn’t depart your site prior to suggesting that
I extremely enjoyed the usual information a person supply on your
guests? Is going to be back incessantly in order to inspect new posts
Here is my site gnsiren.clickn.co.kr
Kunststof kozijnen schilder kunststof kozijnen schilder levert duurzame schilderwerken in Nederland.
Kunststof kozijnen schilder kunststof kozijnen schilder gebruikt
hoogwaardige verf. Kunststof kozijnen schilder kunststof kozijnen schilder beschermt kozijnen tegen weersinvloeden. Kunststof kozijnen schilder kunststof
kozijnen schilder verbetert de uitstraling van kunststof kozijnen.
Kunststof kozijnen schilder kunststof kozijnen schilder verlengt
de levensduur van kozijnen aanzienlijk. Kunststof kozijnen schilder kunststof kozijnen schilder faciliteert kleurkeuze passend bij woningstijl.
Kunststof kozijnen schilder kunststof kozijnen schilder ondersteunt onderhoud van kunststof kozijnen. Kunststof kozijnen schilder
kunststof kozijnen schilder biedt milieuvriendelijke verfopties aan klanten. Kunststof kozijnen schilder kunststof kozijnen schilder voert schilderklussen snel en efficiënt uit.
Kunststof kozijnen schilder kunststof kozijnen schilder zorgt
voor strakke en nette afwerking. Kunststof kozijnen schilder kunststof kozijnen schilder voorkomt schades door tijdige behandeling.
Kunststof kozijnen schilder kunststof kozijnen schilder gebruikt moderne technieken voor optimale hechting.
Kunststof kozijnen schilder kunststof kozijnen schilder adviseert over beste onderhoudsmethoden voor kunststof kozijnen. Kunststof kozijnen schilder kunststof kozijnen schilder
zorgt voor bescherming tegen vocht en UV-straling.
Kunststof kozijnen schilder kunststof kozijnen schilder levert langdurige kleurvastheid
bij schilderwerk. Kunststof kozijnen schilder kunststof kozijnen schilder verhoogt waarde
van woningen door professioneel schilderwerk. Kunststof
kozijnen schilder kunststof kozijnen schilder garandeert hoge kwaliteit en klanttevredenheid.
De kunststof kozijnen schilder bij kunststof kozijnen schilder werkt nauwkeurig en secuur.
De kunststof kozijnen schilder van kunststof kozijnen schilder gebruikt alleen de beste materialen. Kunststof
kozijnen schilder kunststof kozijnen schilder
biedt concurrerende prijzen voor schilderwerk in Nederland.
Разница между поверкой и калибровкой — в правовых последствиях.
Поверка отвечает: «Можно
ли верить прибору по закону?», калибровка: «Какова его реальная ошибка в цифрах?».
Что выбрать — поверку или калибровку?
Зависит от сферы применения.
Если прибор в магазине —
только поверка. Если в лаборатории — смело калибруйте.
Законодательные требования (102-ФЗ,
ГРОЕИ) касаются только критерии выбора поверки и калибровки: только
аккредитованные лица. Для калибровки свободный режим.
Не нарушайте 102-ФЗ.
I relish, caսse І discovered exactⅼy ᴡhаt I used
to be takіng a looк for. You’ve ended my f᧐ur
ɗay lengthy hunt! God Bless ʏߋu man. Have a ɡreat day.
Bye
Aⅼso visit my blog post หนังโป๊ หนังโป๊ไทย คลิปหลุด คลิปโป๊ ดูหนังโป๊ xxx
porn jav 18+ คลิปหลุดไทย onlyfans หลุด แอบถ่าย หนังх หนังav
(Zac)
Deporte Ecuador funciona como un espacio informativo centrada en el análisis del entorno deportivo
digital en Ecuador. La plataforma integra artículos que analizan la
evolución del deporte nacional considerando tecnología, analítica de datos
y nuevos patrones de consumo.
A diferencia de los portales tradicionales, el proyecto no solo informa sobre marcadores
o titulares. Su enfoque está en interpretar el comportamiento del entorno deportivo contemporáneo: cómo los aficionados se
relacionan con los servicios digitales, qué
variables afectan sus decisiones y cómo cambian los criterios de calidad en el
entorno digital.
El contenido del sitio se estructura bajo varios pilares principales.
En primer lugar, se evalúan las plataformas deportivas considerando la
experiencia del usuario, la estabilidad y la coherencia del servicio.
Además, se revisan tendencias del mercado, procesos de digitalización y cambios en las formas de consumo
deportivo en Ecuador.
Además, el portal también cubre cuestiones regulatorias, la protección digital y la
toma de decisiones dentro del entorno online.
Esto ayuda a construir una imagen más amplia del sector,
combinando análisis técnico, escenario nacional y patrones de uso de los
usuarios.
El objetivo del proyecto es proporcionar información clara, estructurada y útil para
interpretar el deporte en el entorno digital actual.
No se trata de ofrecer respuestas simplificadas, sino de
ayudar a interpretar un entorno cada vez más complejo.
Deporte Ecuador está dirigido a usuarios that desean profundizar más allá de la información superficial: considerando
su dimensión tecnológica y su impacto en la experiencia cotidiana.
Se indica que dentro del contenido se ofrece un enlace para profundizar en la lectura.
my blog: press release
Hey there! I realize this is sort of off-topic however
I needed to ask. Does operating a well-established blog such as yours take a
large amount of work? I’m completely new to running a blog but I do write
in my diary every day. I’d like to start a blog so I can share my personal experience and
views online. Please let me know if you have any recommendations or tips for brand new aspiring blog owners.
Thankyou!
My blog – Winvest platform
La plataforma Deporte Ecuador funciona como un espacio informativo dedicada
al análisis del ecosistema digital del deporte ecuatoriano.
La plataforma integra artículos que analizan la evolución del deporte nacional considerando tecnología, analítica de
datos y nuevos patrones de consumo.
A diferencia de los portales tradicionales, Deporte Ecuador no se
limita a cubrir resultados o noticias. Su enfoque está en interpretar
cómo opera el ecosistema deportivo actual: cómo interactúan los usuarios con las plataformas, qué
variables afectan sus decisiones y cómo evolucionan los
estándares de calidad online.
El material de la web se presenta bajo varios pilares
principales. En un aspecto, se estudian las plataformas deportivas considerando la
experiencia del usuario, su solidez y continuidad.
Por otra parte, se examinan tendencias del mercado, procesos de transformación digital y cambios en las formas de consumo deportivo en el país.
Además, Deporte Ecuador aborda aspectos relacionados con la regulación, la ciberseguridad y los procesos de decisión en entornos digitales.
Esto ayuda a construir una imagen más amplia del sector, mezclando evaluación técnica, escenario nacional y patrones
de uso de los usuarios.
El propósito central es brindar datos claros,
bien estructurados y funcionales para entender el papel del deporte en la era digital.
No pretende reducir el análisis a explicaciones básicas, sino facilitar la comprensión de un escenario cada vez más
complejo.
La plataforma se enfoca en usuarios que buscan entender el deporte más allá de la superficie:
desde su dimensión tecnológica hasta su impacto en la experiencia diaria.
El texto aclara que hay un enlace para ver la versión completa del artículo.
Here is my blog :: backlink
Have you ever considered about including a little bit more than just your articles?
I mean, what you say is valuable and everything. But think of
if you added some great graphics or videos to give your posts
more, “pop”! Your content is excellent but with images and
clips, this site could definitely be one of the very best
in its field. Very good blog!
my blog :: secure crypto investment platform
Wow, wonderful weblog format! How long have you been running a
blog for? you made running a blog glance easy.
The whole look of your site is great, as smartly as the content!
My web page crypto investment platform
The Latin ‘sanus per aquam’ which many consider to be the origins of the word ‘Spa’ interprets to ‘health by way of water’. https://janeslist.org/forums/users/fnfsandra5/
Hi to all, the contents present at this site are in fact amazing for people knowledge, well, keep up the good work fellows.
my page: AI trading platform
Usually I don’t learn article on blogs, but I would like to say that this write-up very forced me to take a look at and do so!
Your writing style has been amazed me. Thanks, quite
great post.
Feel free to visit my blog post :: AI-powered bitcoin investment
Heya i am for the first time here. I found this board and I find It truly helpful & it helped
me out much. I hope to give one thing back and help others such as you helped me.
My homepage: AI-powered crypto trading system
I like it when individuals get together and share ideas.
Great blog, continue the good work!
Also visit my website – AI trading platform
Чтобы выбрать обучение работе на специальной технике, нужно смотреть
не только на цену
my web page; https://zetfail.ru/zapchasti-dlya-specztehniki-kak-vybrat-kachestvennye-komplektuyushhie-i-ne-pereplatit.html
There’s certainly a great deal to know about this issue. I love all the points you’ve made.
My site; online order medicine
Hey There. I discovered your blog using msn. That is an extremely well written article.
I will be sure to bookmark it and come back
to learn extra of your useful info. Thank you for the post.
I will certainly return.
Look at my web blog … AI investment platform
Cabiet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Bookmarks
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get three
e-mails with the same comment. Is there any way you can remove me from that service?
Appreciate it!
Have a look at my web site AI-powered crypto trading system
El portal Deporte Ecuador es una plataforma informativa centrada en el análisis
del entorno deportivo digital en Ecuador. La plataforma integra artículos que exploran cómo evoluciona
el deporte en el país considerando tecnología, analítica de
datos y nuevos patrones de consumo.
A diferencia de los portales tradicionales, Deporte Ecuador no
se limita a cubrir resultados o noticias. La
prioridad es comprender el comportamiento del entorno deportivo contemporáneo: cómo
interactúan los usuarios con las plataformas, qué factores influyen en su comportamiento y cómo se redefinen las métricas de calidad digital.
El material de la web se presenta en torno
a distintos ejes temáticos. Por un lado,
se analizan las plataformas deportivas desde el punto de vista del usuario, la estabilidad y consistencia del servicio.
Por otro, se estudian tendencias del mercado, procesos de transformación digital y cambios en las
formas de consumo deportivo en el mercado ecuatoriano.
Además, el portal también cubre cuestiones regulatorias, la ciberseguridad
y los procesos de decisión en entornos digitales.
Esto ayuda a construir una imagen más amplia del sector, combinando análisis técnico,
escenario nacional y comportamiento del usuario.
La meta principal es ofrecer información clara, organizada y de valor para entender el papel del deporte en la era digital.
No busca dar respuestas simples, sino facilitar
la comprensión de un escenario cada vez más complejo.
El portal está orientado a lectores que quieren comprender el deporte más allá de
lo básico: desde su dimensión tecnológica y cómo influye en la vida
diaria.
El texto menciona que hay un enlace disponible para ampliar el artículo.
Also visit my webpage – site
Franchising Path Carlsbad
Carlsbad, СA 92008, United Stɑtes
+18587536197
buy a franchise
Amazing issues here. I’m very glad to look
your post. Thanks so much and I’m looking ahead to contact you.
Will you kindly drop me a mail?
My web blog :: how AI trading works in crypto
Thanks very interesting blog!
Here is my homepage; AI crypto investment
I got this web site from my pal who informed me about this web page and now this
time I am visiting this site and reading very informative articles at this
place.
my site :: Ao Nang beach resort
Hi, this weekend is nice in favor of me, as this point in time i am reading
this impressive educational post here at my residence.
Here is my page – AI-powered bitcoin investment
Dating Coach LA provides skilled dating advice in Los Angeles, CA.
Dating Coach LA empowers clients to define their dating goals.
The Dating Coach LA from Dating Coach LA delivers personalized therapy to handle dating issues.
Dating Coach LA helps individuals in finding love with confidence.
The Dating Coach LA at Dating Coach LA provides valuable feedback on dating apps.
Dating Coach LA facilitates workshops to enhance confidence when attracting potential
partners. The Dating Coach LA from Dating Coach LA
supports clients to understand dating psychology. Dating
Coach LA delivers an authentic approach to dating coaching.
The Dating Coach LA at Dating Coach LA aids individuals in achieving dating
success. Dating Coach LA allows clients to navigate the dating scene in Los Angeles, CA.
The Dating Coach LA from Dating Coach LA delivers expert assistance for dating coach in LA.
Dating Coach LA offers resources for overcoming dating challenges.
The Dating Coach LA at Dating Coach LA supports clients in setting realistic dating
expectations. Dating Coach LA streamlines the development of effective dating
strategies. The Dating Coach LA from Dating Coach LA empowers clients to achieve their dating goals.
Dating Coach LA delivers guidance in establishing meaningful relationships.
The Dating Coach LA at Dating Coach LA offers complete coaching services to
clients in Los Angeles, CA.
This article offers clear idea in favor of the new visitors of blogging, that genuinely how to do
blogging and site-building.
Also visit my site; AI-powered bitcoin investment
It’s going to be finish of mine day, but before ending I am reading this wonderful
paragraph to increase my experience.
Have a look at my webpage; AI investment platform
Woah! I’m really enjoying the template/theme of this site.
It’s simple, yet effective. A lot of times it’s challenging to get that
“perfect balance” between usability and visual appeal.
I must say you have done a great job with this. Additionally,
the blog loads super fast for me on Chrome. Outstanding
Blog!
Also visit my website: AI crypto investment
It’s very effortless to find out any topic on web as compared
to textbooks, as I found this paragraph at this
web page.
Visit my web-site; AI-powered crypto trading system
Hi there, this weekend is fastidious for me, as this occasion i am reading this impressive informative paragraph here at
my residence.
Look into my webpage … dewagg
Truly when someone doesn’t understand afterward its up to other visitors that they will help, so
here it takes place.
My site: 소액결제현금화
I all the time emailed this blog post page to all my contacts, for the reason that if
like to read it afterward my friends will too.
Here is my blog post: isep kontol bapak
Modern Purair
416 Meridian Ɍd SE #14Ꭺ, Calgary
AB T2A 1X2, Canada
(403) 800-7254
modern pro
Modern Purair
416 Meridian Ꮢd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
cost effective
Great article.
my website homepage
Hello my loved one! I want to say that this post
is awesome, great written and include almost all significant infos.
I’d like to peer more posts like this .
Feel free to surf to my web page … poker88
I every time spent my half an hour to read this blog’s content everyday along with a mug
of coffee.
My web blog … MALWARE
Its like you read my mind! You seem to know so much about this, like you wrote the book in it or something.
I think that you can do with some pics to drive the message home a little bit, but other than that,
this is great blog. A fantastic read. I’ll certainly be back.
my blog post … MALWARE
Have you ever considered about adding a little
bit more than just your articles? I mean, what you say is important and everything.
However just imagine if you added some great images or videos
to give your posts more, “pop”! Your content is excellent but with images and videos, this website could certainly be one of the most beneficial in its
field. Fantastic blog!
Also visit my site: homepage
My family all the time say that I am wasting my time
here at net, but I know I am getting knowledge
all the time by reading thes pleasant content.
my web blog :: website
Hi there, just became alert to your blog through Google, and found that it is truly informative.
I’m gonna watch out for brussels. I’ll appreciate if you continue this in future.
Numerous people will be benefited from your writing. Cheers!
Also visit my webpage :: 양산출장마사지
It’s hard to come by well-informed people on this topic, but you sound like
you know what you’re talking about! Thanks
Here is my web-site – poker88
Very good information. Lucky me I discovered your site by
accident (stumbleupon). I’ve bookmarked it for later!
Here is my webpage – diy tron vanity address
Easy and simple site with lots of gambling-related info.
best non gamstop casinos uk
Hi there it’s me, I am also visiting this web page on a regular basis, this web site is
really fastidious and the people are truly sharing good thoughts.
Hi this is kind of of off topic but I was wondering if blogs use WYSIWYG
editors or if you have to manually code with HTML. I’m starting a blog soon but have no coding knowledge so I wanted
to get guidance from someone with experience.
Any help would be enormously appreciated!
My web blog; vejret tenerife costa adeje
I’m impressed, I have to admit. Seldom do I encounter a blog that’s equally educative and amusing, and let me tell you,
you have hit the nail on the head. The issue is something which too few men and women are speaking
intelligently about. I am very happy I stumbled across this during my
hunt for something regarding this.
Feel free to surf to my website: web site
My brother suggested I may like this blog. He used to be entirely
right. This publish actually made my day. You cann’t imagine simply how so much time I had spent
for this information! Thank you!
my blog … 소액결제현금화
What’s up, I want to subscribe for this website to obtain hottest updates, so where can i do
it please help out.
Look into my webpage … megahoki
My spouse and I stumbled over here from a different website and thought
I should check things out. I like what I see so now i am following you.
Look forward to going over your web page yet again.
Have a look at my blog post – dewapoker
Great blog! Do you have any recommendations for aspiring writers?
I’m planning to start my own site soon but I’m a little
lost on everything. Would you propose starting with a free platform like WordPress or go for a paid option? There are so many options out there that I’m totally confused ..
Any tips? Thank you!
Feel free to visit my web page … 수원출장안마
You’re so cool! I don’t suppose I’ve read a single thing like that before.
So wonderful to discover another person with a few unique thoughts on this topic.
Seriously.. thank you for starting this up. This site
is something that is required on the web, someone
with a bit of originality!
Look at my web blog – 외국인 화물운송업
Woah! I’m really digging the template/theme of this website.
It’s simple, yet effective. A lot of times it’s very hard drive shredding fresno to get that “perfect balance” between user friendliness and visual appearance.
I must say that you’ve done a awesome job with this.
In addition, the blog loads very quick for me on Firefox.
Exceptional Blog!
Good day! This is kind of off topic but I need some
guidance from an established blog. Is IT asset disposition san francisco tough
to set up your own blog? I’m not very techincal but I can figure things
out pretty quick. I’m thinking about creating my own but I’m not sure where to
begin. Do you have any tips or suggestions? Many thanks
Right here is the perfect webpage for anyone who would like to understand this topic.
You understand a whole lot its almost tough to argue with you (not that I personally will need to…HaHa).
You definitely put a fresh spin on a topic which has
been written about for many years. Excellent stuff,
just wonderful!
Also visit my web page IT asset disposition san francisco
What’s up to every one, the contents existing at
this web page are genuinely amazing for people experience, well,
keep up the good work fellows.
my web page electronics recycling fresno
Deporte Ecuador se presenta como un sitio especializado enfocada en el estudio del ecosistema digital del deporte ecuatoriano.
La web agrupa materiales que analizan la evolución del deporte nacional considerando tecnología, analítica de
datos y nuevos patrones de consumo.
A diferencia de los sitios convencionales, Deporte Ecuador no se limita a cubrir resultados o noticias.
Su enfoque está en interpretar el comportamiento del entorno
deportivo contemporáneo: cómo interactúan los usuarios con las plataformas, qué elementos determinan su
comportamiento y cómo cambian los criterios de calidad en el entorno
digital.
El contenido del sitio se estructura alrededor de varios ejes
clave. En primer lugar, se evalúan las plataformas deportivas considerando la experiencia del usuario, la estabilidad y la coherencia del
servicio. Además, se revisan tendencias del mercado,
procesos de digitalización y cambios en las formas de consumo deportivo en Ecuador.
Además, Deporte Ecuador aborda aspectos relacionados con la regulación, la
ciberseguridad y los procesos de decisión en entornos digitales.
Esto permite ofrecer una visión más completa del sector, mezclando evaluación técnica, escenario nacional y comportamiento del usuario.
La meta principal es ofrecer información clara, organizada
y de valor para interpretar el deporte en el entorno digital actual.
No se trata de ofrecer respuestas simplificadas, sino facilitar la comprensión de un escenario
cada vez más complejo.
La plataforma se enfoca en usuarios that desean profundizar más allá de la información superficial:
considerando su dimensión tecnológica hasta su impacto en la experiencia
diaria.
Se indica que dentro del contenido se ofrece
un enlace para profundizar en la lectura.
Also visit my page :: article
Hi there to every , since I am actually eager of
reading this web site’s post to be updated daily.
It consists of good data.
Also visit my website dino 69
Thanks for sharing your thoughts on tron vanity. Regards
Feel free to visit my blog post … vanity tron address
Greetings, I do think your site could possibly be
having web browser compatibility foundation problems texas.
Whenever I take a look at your blog in Safari, it looks fine but when opening in I.E., it’s got some overlapping issues.
I merely wanted to give you a quick heads up! Aside from that, fantastic
site!
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Interiorexpers (atavi.com)
My webpage :: Madonna
This post is worth everyone’s attention. When can I
find out more?
My site: android gaming app (Tawnya)
It’s actually a great and useful piece of information. I’m glad
that you just shared this useful information with us. Please
keep us up to date like this. Thanks for sharing.
Also visit my homepage: hard drive shredding san francisco
Joker Slot merupakan salah satu permainan slot online yang dikembangkan oleh Joker
Gaming dan banyak dimainkan melalui berbagai platform, termasuk Joker 4D.
Popularitasnya terus meningkat karena gameplay
yang sederhana, ringan, dan peluang kemenangan yang cukup menarik bagi berbagai jenis pemain.
Feel free to surf to my web page: joker slot terbaik
Good write-up. I absolutely appreciate this website.
Keep writing!
Feel free to visit my site download casino apk; hotelgratteciel.com,
Modern Purair
416 Meidian Ɍd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
healthy environment ()
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX78735, United Ѕtates
254-275-5536
Bookmarks
Hello there! This post could not be written much better!
Reading through this post reminds me of my previous roommate!
He always kept talking about this. I’ll forward this post to him.
Pretty sure he will have a good read. Thank you for sharing!
my homepage; aluminium composite board
whoah this blog is wonderful i like studying your posts.
Keep up the great work! You know, lots of individuals are looking around
for this info, you could help them greatly.
my blog :: MALWARE
El portal Deporte Ecuador se presenta como un sitio especializado dedicada al análisis del panorama deportivo online en Ecuador.
La plataforma integra artículos que exploran cómo evoluciona el
deporte en el país en el contexto de la tecnología, los datos y los nuevos hábitos de consumo.
A diferencia de las páginas deportivas comunes, el proyecto
no solo informa sobre marcadores o titulares. La propuesta se basa en interpretar cómo opera el ecosistema deportivo actual: cómo
interactúan los usuarios con las plataformas, qué elementos determinan su comportamiento y cómo
evolucionan los estándares de calidad online.
El contenido del sitio se estructura bajo varios pilares principales.
En primer lugar, se evalúan las plataformas deportivas desde
el punto de vista del usuario, la estabilidad y consistencia
del servicio. Además, se revisan las dinámicas del mercado,
etapas de digitalización y la evolución de los hábitos de consumo deportivo en el país.
Además, el proyecto analiza temas vinculados
a la regulación, la seguridad digital y la toma de decisiones dentro
del ecosistema digital. Gracias a ello, se obtiene una perspectiva más integral del ámbito deportivo,
fusionando análisis técnico, contexto local y comportamiento del usuario.
El objetivo del proyecto es proporcionar información clara, estructurada y útil
para interpretar el deporte en el entorno digital actual. No pretende reducir el
análisis a explicaciones básicas, sino aportar claridad a un panorama digital cada vez más difícil
de entender.
Deporte Ecuador está dirigido a usuarios que buscan entender el
deporte más allá de la superficie: incluyendo su componente tecnológico y cómo influye en la
vida diaria.
El texto aclara que hay un enlace para ver la versión completa del artículo.
my web-site … press release
Incredible! This blog looks exactly like my old one! It’s on a totally different subject but it has pretty much the same page layout and
design. Excellent choice of colors!
my webpage – driving lesson
Deporte Ecuador funciona como un espacio informativo enfocada en el estudio del entorno deportivo
digital en Ecuador. La web agrupa materiales que exploran cómo evoluciona el deporte en el país en relación con la tecnología, la
data y las tendencias de uso actuales.
A diferencia de los sitios convencionales, Deporte
Ecuador no se limita a cubrir resultados o noticias. La propuesta se basa en interpretar el comportamiento
del entorno deportivo contemporáneo: cómo los aficionados se relacionan con los servicios digitales, qué variables afectan sus decisiones y cómo evolucionan los estándares de
calidad online.
La información dentro del portal se organiza alrededor de varios ejes clave.
En un aspecto, se estudian las plataformas deportivas desde
la perspectiva de la experiencia del usuario, la estabilidad y consistencia
del servicio. Por otro, se estudian las tendencias del mercado deportivo digital, procesos
de transformación digital y cambios en las formas de consumo deportivo en el mercado ecuatoriano.
Además, Deporte Ecuador aborda aspectos relacionados con la regulación, la ciberseguridad y la toma de decisiones dentro del ecosistema digital.
Esto permite ofrecer una visión más completa del sector, mezclando evaluación técnica, realidad
local y comportamiento del usuario.
El propósito central es brindar datos claros, bien estructurados y funcionales para entender el
papel del deporte en la era digital. No pretende reducir el análisis a explicaciones básicas, sino facilitar la comprensión de un escenario cada vez más
complejo.
La plataforma se enfoca en usuarios that desean profundizar más allá de la información superficial: incluyendo su componente tecnológico y
cómo influye en la vida diaria.
El texto aclara que hay un enlace para ver la versión completa del artículo.
Feel free to visit my web-site … press release
Your style is unique in comparison to other folks
I’ve read stuff from. I appreciate you for posting when you’ve
got the opportunity, Guess I will just bookmark this web site.
Feel free to visit my web-site: dewa 138
Hey would you mind letting me know which hosting
company you’re utilizing? I’ve loaded your blog in 3 different internet browsers Bloodborne Pathogens and HIPAA certification
I must say this blog loads a lot faster then most. Can you suggest a good web hosting provider at a fair price?
Thank you, I appreciate it!
Very shortly this web site will be famous amid all blogging viewers,
due to it’s nice articles or reviews
Also visit my web-site; buy steroids online
I love it when individuals come together and share views.
Great site, stick with it!
My web page; pharmacies shipping to usa
Excellent weblog right here! Also your site loads up very fast!
What host are you using? Can I get your associate link in your host?
I want my site loaded up as fast as yours lol
My blog; performance supplements
Hey very nice blog!
My page; Exabet88 Update Angka Data Macau 2026
Everything is very open with a very clear explanation of the issues.
It was really informative. Your website is useful. Thank
you for sharing!
Also visit my homepage: Buy TikTok Comments
Pretty component of content. I simply stumbled upon your site
and in accession capital to claim that I get actually enjoyed account your weblog posts.
Any way I’ll be subscribing on your augment or even I fulfillment
you get entry to constantly quickly.
my web-site: 아고다 할인코드
Howdy! I could have sworn I’ve been to this website before but after checking through some of the post I realized
it’s new to me. Nonetheless, I’m definitely happy I found it and
I’ll be bookmarking and checking back frequently!
Have a look at my web blog: Basketball tournaments flagstaff
Sweet website, super layout, very clean and utilize genial.
Here is my blog post – kkpoker payday
Helpful info. Lucky me I discovered your site by accident,
and I am shocked why this twist of fate did not happened in advance!
I bookmarked it.
Here is my blog post … naga303
Thanks for one’s marvelous posting! I actually enjoyed reading it, you could be a great author.
I will make certain to bookmark your blog HIPAA and Bloodborne Pathogens Certification will eventually come back very soon. I want to encourage you to continue your great work, have a nice day!
Touche. Sound arguments. Keep up the amazing effort.
Feel free to surf to my blog post :: Flagstaff youth basketball tournaments
Good way of telling, and good article to get
information about my presentation topic, which i am going to deliver in university.
Here is my website :: trusted supplement store
Look at my webpage: Highstakes online casino
Ꮐreat weblog here! Also your site quіte a bit up fast!
Ԝhat hoѕt aгe you the uѕage of? Can I get your
ɑffіliate hyрerlink to your host? I want my website loaded up as quickly аs
yours lol
Here is my web page :: controllo parentale
Thank you for sharing your info. I really appreciate your
efforts and I will be waiting for your further write ups thank you once again.
Review my web page :: Omega Canada
Everyone loves what you guys tend to be up too. This type of clever work and coverage!
Keep up the amazing works guys I’ve included you
guys to my blogroll.
Visit my blog post: Keluaran Data Macau 2026
What’s up every one, here every one is sharing these kinds of experience, thus it’s fastidious to read this website, and I used to pay a quick visit this webpage daily.
Feel free to visit my homepage Omega Full Potential
Greetings from Idaho! I’m bored at work so
I decided to browse your website on my iphone during lunch break.
I really like the information you provide here and can’t wait
to take a look when I get home. I’m surprised at how quick your blog loaded on my
mobile .. I’m not even using WIFI, just 3G .. Anyhow, great site!
my web site :: mpo1221
This piece of writing gives clear idea in support of the
new viewers of blogging, that in fact how to do blogging and site-building.
Here is my webpage THC tinctures DC
La plataforma Deporte Ecuador es una plataforma informativa enfocada en el estudio del ecosistema digital del deporte ecuatoriano.
El sitio reúne contenidos que analizan la evolución del deporte nacional en relación con la
tecnología, la data y las tendencias de uso actuales.
A diferencia de las páginas deportivas comunes, el proyecto no solo informa sobre marcadores o
titulares. Su enfoque está en interpretar el comportamiento del entorno deportivo contemporáneo:
cómo los aficionados se relacionan con los servicios digitales, qué
variables afectan sus decisiones y cómo cambian los criterios de calidad en el
entorno digital.
La información dentro del portal se organiza alrededor de varios ejes clave.
Por un lado, se analizan las plataformas deportivas considerando la experiencia del usuario, la estabilidad y la coherencia del servicio.
Por otra parte, se examinan las dinámicas del mercado, procesos de transformación digital y la evolución de los hábitos de consumo deportivo
en el país.
Además, el proyecto analiza temas vinculados a la regulación, la seguridad digital y los procesos de decisión en entornos digitales.
Esto permite ofrecer una visión más completa del sector, combinando análisis
técnico, realidad local y patrones de uso de los usuarios.
El objetivo del proyecto es proporcionar información clara, estructurada y útil para entender el papel del deporte
en la era digital. No busca dar respuestas simples, sino aportar claridad a un panorama digital cada vez más difícil de entender.
Deporte Ecuador está dirigido a usuarios que quieren comprender el deporte más allá de lo básico:
desde su dimensión tecnológica y cómo influye en la vida diaria.
Dentro del texto se menciona que hay un enlace para
leer el artículo completo.
Visit my blog post article
Feel free to visit my webpage; high stakes poker Site
Как определить качественную медтехнику
Feel free to surf to my homepage :: Лечение отрубевидного лишая
Good day! Do you know if they make any plugins to assist with SEO?
I’m trying to get my blog to rank for some targeted keywords but I’m not seeing very good gains.
If you know of any please share. Many thanks!
Feel free to visit my page … Toto 4D Akurat Tanpa Delay
Hi there! I could have sworn I’ve been to this web site
before but after going through some of the posts I realized it’s new to me.
Nonetheless, I’m definitely happy I found it and I’ll
be bookmarking it and checking back regularly!
Feel free to surf to my homepage :: maxwin 138
Very rapidly this web site will be famous among all blog people,
due to it’s fastidious posts
Here is my blog post … MALWARE
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ꮪtates
12394214912
Bookmarks – https://www.protopage.com,
Highly descriptive post, I loved that a lot. Will
there be a part 2?
My web-site CBD marque française
Incredible points. Outstanding arguments. Keep up the amazing
effort.
my web blog Exabet88 Togel Macau 2026
I’m not that much of a internet reader to be honest but your blogs really nice, keep it up!
I’ll go ahead and bookmark your website to come back in the future.
Cheers
Here is my web page … accounting software
Cabinet IQ
8305 Staate Hwy 71 #110, Austin,
TX 78735, United States
254-275-5536
Style
This post will help the internet viewers for creating new webpage or even a weblog from start to end.
Also visit my homepage – perplexity comet
Feel free to visit my blog post Complete RTP database for Superlotto slots
I’m a bit of a racing fan, and I love car racing slots.
Aussie Oddster pointed me to a casino with a pit stop bonus.
Hello would you mind letting me know which web host you’re working with?
I’ve loaded your blog in 3 completely different browsers and I must say this
blog loads a lot quicker then most. Can you suggest a good web hosting provider at a honest price?
Many thanks, I appreciate it!
My web-site … zegreanul01
$LowPrice&HighQuality-Guestpost【dr50+real-traffic】Telegram !!#LowPrice&HighQuality-Guestpost【dr50+real-traffic】Telegram @buycasinolink
This is very fascinating, You’re an excessively professional blogger.
I’ve joined your rss feed and stay up for seeking more of your excellent post.
Additionally, I’ve shared your site in my social networks
Have a look at my site … quitar moho Barcelona
Cabinhet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Wood (scwardmbth.raindrop.page)
Cabinet IQ
8305 State Hwyy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Bookmarks
I was able to find good information from your articles.
My blog; 1dmc.io lừa đảo công an truy nã cấm người chơi tham gia
Excellent pieces. Keep posting such kind of info on your
page. Im really impressed by your site.
Hey there, You’ve performed a great job. I will definitely
digg it and in my opinion suggest to my friends. I am confident they will be benefited from this web
site.
Here is my web page; paktoto
Howdy! This is my first comment here so I just wanted to
give a quick shout out and say I truly enjoy reading your posts.
Can you recommend any other blogs/websites/forums that go over the same subjects?
Appreciate it!
my site :: comment-3185841
Cabinet IQ
8305 Ꮪtate Hwy 71 #110, Austin,
TX 78735, United Stateѕ
254-275-5536
Uniqueinteriors (https://wakelet.com/wake/58FXmWDH9E65s1bk6SpCi)
Thank you for some other informative blog. Where else could I am
getting that type of info written in such an ideal
approach? I’ve a challenge that I am just now working on, and
I have been at the glance out for such information.
My website … real estate agent Palos Verdes CA
It’s appropriate time to make a few plans for the long run and it’s time to be happy.
I have read this post and if I may I wish to suggest
you some interesting things or suggestions. Maybe you can write subsequent articles regarding this article.
I want to read more things about it!
my site; realtor in Nebo NC
Good day! Do you use Twitter? I’d like to follow you if that would be okay.
I’m absolutely enjoying your blog and look forward to new posts.
Feel free to visit my blog post best real estate agent in Fort Lauderdale FL
Hi would you mind sharing which blog platform you’re using?
I’m planning to start my own blog soon but I’m having a difficult time choosing between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design seems different then most blogs and I’m looking for something completely unique.
P.S Sorry for getting off-topic but I had to ask!
Look into my web-site; best realtor in Schaumburg IL
Your style is really unique in comparison to other people I’ve
read stuff from. Thanks for posting when you have the opportunity, Guess I
will just book mark this web site.
My web blog: real estate agent Chicago IL
I am really impressed with your writing skills and also with the layout on your weblog.
Is this a paid theme or did you customize it yourself?
Anyway keep up the nice quality writing, it is rare
to see a nice blog like this one today.
Here is my page: realtor in Nebo NC
Thanks for sharing your thoughts on best real estate agent in Fort Lauderdale FL.
Regards
My web-site – best realtor in Fort Lauderdale FL
Wonderful goods from you, man. I’ve understand your stuff previous
to and you’re just extremely excellent. I really like what you’ve acquired
here, really like what you are stating and the way in which you say it.
You make it entertaining and you still take care of to
keep it smart. I can not wait to read much more from you. This is really a wonderful website.
my web site … best realtor in Douglasville GA
I constantly emailed this web site post page to all my
friends, as if like to read it then my links will too.
my blog post … best realtor in Fort Lauderdale FL
Wow, non gamstop casinos is such a cool site! Thanks!
best non gamstop casinos uk
This information is worth everyone’s attention. Where
can I find out more?
Also visit my web blog: 남양주출장마사지
Very energetic post, I loved that bit. Will there be a
part 2?
Here is my homepage: best real estate agent in Crown Point IN
You can certainly see your expertise in the article you
write. The arena hopes for even more passionate
writers like you who are not afraid to mention how
they believe. All the time go after your heart.
Here is my website: real estate agent Schaumburg IL
Valuable info. Fortunate me I discovered your site by chance, and I am shocked
why this coincidence did not took place earlier! I bookmarked
it.
Also visit my page … adservemedia.com
Hello! Do you use Twitter? I’d like to follow you
if that would be ok. I’m undoubtedly enjoying your blog and look forward to new updates.
My blog post; best realtor in Schaumburg IL
Today, while I was at work, my sister stole my apple ipad and
tested to see if it can survive a thirty foot drop, just so she can be a youtube sensation. My apple ipad
is now broken and she has 83 views. I know this is entirely off topic but I had to share it with someone!
Here is my blog … real estate agent New Lenox IL
Hello there! This is my first comment here so I just wanted
to give a quick shout out and tell you I genuinely enjoy reading
your blog posts. Can you suggest any other blogs/websites/forums that
cover the same subjects? Thanks for your time!
Feel free to surf to my site; best realtor in Chicago IL
Кухонные кухонные фасады кастамону из Кастамону — это современное решение, объединяющее прочность, практичность и стиль.
В отличие от традиционных материалов, таких как
эмаль или шпон, они дольше сохраняют внешний вид и требуют минимального ухода.
Сделайте выбор в пользу инноваций — и ваша
кухня будет выглядеть красиво, надежно и современные долгие годы!
Way cool! Some extremely valid points! I appreciate you penning this write-up plus the
rest of the website is extremely good.
my web blog – real estate agent Chicago IL
Thanks in support of sharing such a fastidious idea,
post is fastidious, thats why i have read it fully
Feel free to surf to my homepage; real estate agent Nebo NC
Appreciation to my father who informed me concerning this weblog,
this website is truly awesome.
Here is my web-site best realtor in Crown Point IN
I blog often and I genuinely appreciate your content. The
article has really peaked my interest. I am going to book mark your website and keep checking for
new information about once a week. I opted in for your Feed as well.
Feel free to surf to my homepage; best real estate agent in Palos Verdes CA
I’m really enjoying the theme/design of your weblog. Do you
ever run into any web browser compatibility problems?
A few of my blog readers have complained about my website not
working correctly in Explorer but looks great in Firefox.
Do you have any recommendations to help fix this issue?
Here is my webpage … real estate agent Crown Point IN
We’re a group of volunteers and starting a new scheme in our community.
Your site provided us with valuable information to work on. You
have done an impressive job and our whole
community will be grateful to you.
Also visit my webpage :: best realtor in Schaumburg IL
ข้อมูลชุดนี้ มีประโยชน์มาก ค่ะ
ดิฉัน ได้อ่านบทความที่เกี่ยวข้องกับ เรื่องที่เกี่ยวข้อง
ที่คุณสามารถดูได้ที่ Alta
ลองแวะไปดู
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ เนื้อหาดีๆ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
My web-site :: flix888 [Alta]
I’m not sure exactly why but this blog is loading very
slow for me. Is anyone else having this issue or is it a issue
on my end? I’ll check back later and see if the problem
still exists.
Feel free to visit my web-site; best real estate agent in Crown Point IN
Pretty nice post. I just stumbled upon your blog and
wished to mention that I have really enjoyed surfing around your blog posts.
After all I’ll be subscribing in your rss feed and I am hoping
you write once more soon!
My page … realtor in Gilbert AZ
uu5plg
It’s perfect time to make a few plans for the long run and it
is time to be happy. I have learn this submit and if I may I desire to counsel you
few interesting issues or advice. Maybe you could write next articles
regarding this article. I desire to learn even more things
approximately it!
my webpage – Five88
Your style is so unique in comparison to other folks I’ve
read stuff from. Many thanks for posting when you’ve got the
opportunity, Guess I will just bookmark this site.
Here is my web blog; best realtor in Chicago IL
Appreciate this post. Let me try it out.
my web blog Knee Replacement in India
Howdy! This is kind of off topic but I need some
help from an established blog. Is it very hard to set up your own blog?
I’m not very techincal but I can figure things
out pretty fast. I’m thinking about creating my own but I’m not
sure where to begin. Do you have any points
or suggestions? Many thanks
Also visit my web page best realtor in Fort Lauderdale FL
Good day! I just would like to give you a huge thumbs up for your great info
you have right here on this post. I am returning to your site
for more soon.
My homepage realtor in Palos Verdes CA
I’m not that much of a internet reader to be honest but your sites really nice, keep it up!
I’ll go ahead and bookmark your site to come back later.
Cheers
Also visit my blog post: best real estate agent in Fort Lauderdale FL
Pretty nice post. I just stumbled upon your weblog and wished to say that I’ve truly enjoyed
surfing around your blog posts. After all I’ll be subscribing
to your feed and I hope you write again very soon!
my blog: best real estate agent in Schaumburg IL
This is very interesting, You are a very skilled
blogger. I’ve joined your feed and look forward to seeking more of your wonderful post.
Also, I’ve shared your web site in my social networks!
Have a look at my web page best realtor in Nebo NC
Hi to every body, it’s my first go to see of this web site; this weblog contains awesome and actually fine information in favor of readers.
Also visit my site … realtor in Chicago IL
Thanks in support of sharing such a fastidious thinking, piece of writing is
pleasant, thats why i have read it entirely
my web-site – real estate agent Fort Lauderdale FL
Thanks on your marvelous posting! I genuinely enjoyed
reading it, you are a great author. I will make
certain to bookmark your blog and will eventually come back sometime
soon. I want to encourage you continue your great work, have a nice morning!
Check out my site … blog link
May I simply say what a comfort to discover an individual
who truly knows what they are discussing over the internet.
You actually realize how to bring an issue to light and make it important.
More and more people should read this and understand this side of the story.
I was surprised that you’re not more popular because you
definitely possess the gift.
Here is my blog post – best real estate agent in Schaumburg IL
Excellent weblog right here! Also your web site a lot up fast!
What web host are you the usage of? Can I am getting your
associate link in your host? I wish my site loaded up as fast as yours
lol
Also visit my web-site realtor in Palos Verdes CA
What’s up, I log on to your blogs on a regular
basis. Your story-telling style is awesome, keep up the good work!
my page :: alicewhite.ru.com lừa đảo công an truy nã cấm người chơi tham gia
This excellent website certainly has all of the info I needed about this subject and didn’t know who to ask.
Feel free to surf to my web page – realtor in Fort Lauderdale FL
реконструкция нежилого здания в москве
Also visit my website … кладка стен из блока
A motivating discussion is definitely worth comment.
I believe that you ought to publish more about this subject matter,
it might not be a taboo subject but usually folks
don’t talk about these issues. To the next! All
the best!!
Here is my web page; best realtor in Chicago IL
I am curious to find out what blog system you are working with?
I’m having some minor security problems with my latest site
and I’d like to find something more secure. Do you have any solutions?
Also visit my blog post: realtor in Schaumburg IL
Great delivery. Solid arguments. Keep up the great work.
Feel free to surf to my web page – best real estate agent in Nebo NC
Does your website have a contact page? I’m having a tough time
locating it but, I’d like to shoot you an email. I’ve got some suggestions for
your blog you might be interested in hearing. Either
way, great website and I look forward to seeing it grow over time.
Check out my web blog – Hitclub
I got this site from my friend who shared with me concerning this site and at the moment this time I am visiting this website and reading very informative articles or reviews at this time.
Feel free to visit my web page … best real estate agent in Gilbert AZ
An interesting discussion is worth comment.
I do believe that you ought to publish more on this
subject matter, it might not be a taboo subject but usually folks don’t discuss these issues.
To the next! Kind regards!!
my website :: best real estate agent in Chicago IL
Howdy! I could have sworn I’ve been to this site before
but after browsing through some of the post I realized it’s new to me.
Nonetheless, I’m definitely happy I found it and I’ll be book-marking and checking back often!
Here is my site webpage
I’m impressed, I must say. Seldom do I come across a blog that’s both
equally educative and interesting, and without
a doubt, you’ve hit the nail on the head.
The problem is an issue that too few folks are speaking intelligently about.
Now i’m very happy I came across this during my search for something concerning
this.
Stop by my blog; best real estate agent in Chicago IL
This post presents clear idea designed for the new viewers of blogging, that in fact how
to do blogging and site-building.
Also visit my web page; MALWARE
My brother suggested I might like this web site. He was totally right.
This publish actually made my day. You cann’t believe
simply how a lot time I had spent for this info!
Thank you!
Look at my homepage … realtor in Nebo NC
Wow, this post is good, my younger sister is analyzing these kinds of things,
so I am going to convey her.
Feel free to surf to my blog post – best real estate agent in Chicago IL
Your way of explaining everything in this article is truly good, every one can effortlessly be
aware of it, Thanks a lot.
my webpage – best real estate agent in Palos Verdes CA
I needed to thank you for this good read!! I certainly
loved every little bit of it. I have you book-marked to look at new things you post…
my web blog: best real estate agent in Gilbert AZ
I got this website from my pal who shared
with me regarding this website and at the moment this time
I am visiting this site and reading very informative posts here.
Feel free to visit my homepage; best real estate agent in Douglasville GA
My brother recommended I might like this blog.
He was totally right. This post actually made my day. You cann’t imagine simply how
much time I had spent for this info! Thanks!
Check out my web page :: realtor in Schaumburg IL
Hi there every one, here every person is sharing these
kinds of experience, therefore it’s pleasant to read this web
site, and I used to visit this weblog daily.
Also visit my site: best realtor in Crown Point IN
Hi! I just want to give you a big thumbs up for the great information you have got right here on this post.
I will be coming back to your website for more soon.
Here is my web blog :: best realtor in Gilbert AZ
I’m really enjoying the theme/design of your web site.
Do you ever run into any browser compatibility issues?
A small number of my blog audience have complained about
my blog not operating correctly in Explorer but looks great in Firefox.
Do you have any tips to help fix this issue?
Here is my blog post … real estate agent Gilbert AZ
Its like you read my mind! You appear to know so much about this,
like you wrote the book in it or something. I think that you
can do with some pics to drive the message home a little bit, but instead of that, this is magnificent blog.
A fantastic read. I’ll definitely be back.
Here is my webpage … best real estate agent in Douglasville GA
We’re a group of volunteers and starting a brand new scheme in our community.
Your site provided us with valuable info to work on.
You have performed a formidable task and our entire neighborhood might be grateful to you.
Review my site: best realtor in Schaumburg IL
Nice post. I used to be checking continuously this
weblog and I’m inspired! Very helpful information particularly the closing section :) I take care of
such information a lot. I was seeking this
particular info for a long time. Thank you and best of luck.
Here is my web blog … realtor in Crown Point IN
Genuinely when someone doesn’t know after that its up to other users that they will help, so here it happens.
Feel free to visit my webpage :: best real estate agent in Palos Verdes CA
I got this website from my buddy who shared with me regarding this site and now
this time I am visiting this web page and reading very informative
content here.
Also visit my homepage; best real estate agent in Gilbert AZ
Thanks for sharing such a fastidious idea, article is pleasant, thats why i have read it entirely
Here is my web-site realtor in Schaumburg IL
I read this article completely regarding the resemblance of latest and earlier technologies, it’s
remarkable article.
My website – best real estate agent in Fort Lauderdale FL
I was recommended this website by my cousin. I’m not sure whether this post
is written by him as no one else know such detailed about my difficulty.
You’re incredible! Thanks!
Feel free to surf to my page; best real estate agent in Fort Lauderdale FL
Кухонные фасады kastamonu из Кастамону — это современное
решение, объединяющее прочность, практичность и стиль.
В отличие от традиционных материалов, таких
как эмаль или шпон, они дольше сохраняют внешний
вид и требуют минимального ухода.
Сделайте выбор в пользу инноваций — и
ваша кухня будет выглядеть красиво, надежно и современные долгие годы!
Appreciate this post. Will try it out.
Visit my blog :: best realtor in Douglasville GA
I delight in, lead to I discovered just what I was having a look for.
You have ended my four day lengthy hunt! God Bless
you man. Have a nice day. Bye
Feel free to visit my blog: best realtor in Gilbert AZ
I think everything posted was very reasonable. But, what about this?
what if you typed a catchier title? I am not suggesting your
content is not solid., but suppose you added a
title to possibly grab folk’s attention? I mean Heel Pain –
Plantar Fasciitis – Mr Will Edwards is a little plain. You might look at Yahoo’s home
page and note how they create post headlines to grab
people to open the links. You might add a related video or a picture or two to grab people
excited about what you’ve written. Just my opinion, it might make
your posts a little bit more interesting.
Also visit my blog; best realtor in Douglasville GA
Everyone loves it when folks come together and share thoughts.
Great website, stick with it!
Visit my webpage – best real estate agent in Palos Verdes CA
Hey! I know this is kind of off topic but I was wondering if you knew where I could find a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having trouble finding one?
Thanks a lot!
Here is my web page 3bet
Hello there! This post could not be written much better!
Reading through this post reminds me of my previous
roommate! He constantly kept preaching about this. I’ll forward
this post to him. Pretty sure he’s going to have a great read.
Many thanks for sharing!
Check out my web blog … Five88
Ahaa, its pleasant conversation concerning this piece of writing here at this blog, I have
read all that, so at this time me also commenting at this place.
Also visit my web-site: real estate agent Fort Lauderdale FL
Willkommen auf der weltgrößten Auswahl Seite für Erwachsene XXX Filme, Hardcore Geschlechtsverkehr Clips,
und ein One-Stop-Shop für alle Ihre böse Bedürfnisse.
Durch unsere umfangreiche Sammlung von Videos, entdecken Sie brandneue und
erfahren über, verführerisch Amateure in ihrer Wildnis,
und viele andere Dinge. homepage http://code.dev.soooner.com:18000/gabrielschoono
Willkommen auf der weltgrößten Auswahl Seite für Erwachsene XXX Filme, Hardcore Geschlechtsverkehr Clips, und ein One-Stop-Shop für alle Ihre böse Bedürfnisse.
Durch unsere umfangreiche Sammlung von Videos, entdecken Sie brandneue und erfahren über, verführerisch Amateure in ihrer Wildnis, und viele andere Dinge.
homepage https://maru.bnkode.com/@launabigelow50
I am sure this post has touched all the internet people,
its really really nice post on building up new webpage.
Stop by my web blog; best real estate agent in Douglasville GA
Hi! This is my first visit to your blog! We are a
team of volunteers and starting a new project in a community in the same niche.
Your blog provided us beneficial information to work on. You have done a marvellous job!
Feel free to visit my site; best real estate agent in Chicago IL
What’s up to every body, it’s my first pay a visit of this website; this weblog includes amazing and in fact fine data in favor of visitors.
Feel free to visit my webpage :: real estate agent Nebo NC
Hello would you mind letting me know which webhost you’re working with?
I’ve loaded your blog in 3 completely different browsers and I must
say this blog loads a lot quicker then most. Can you recommend a good web hosting provider at a reasonable price?
Thank you, I appreciate it!
Feel free to visit my site – 수원출장마사지
It’s an awesome post for all the internet people; they will obtain benefit from it I am sure.
Here is my website Lucky88
Thanks for your personal marvelous posting! I
genuinely enjoyed reading it, you could be a great author.
I will ensure that I bookmark your blog and definitely will come back later on. I want to encourage that you continue your great work, have a nice day!
my homepage; realtor in Crown Point IN
This is really interesting, You’re a very skilled blogger.
I have joined your rss feed and sit up for in the hunt for more of
your magnificent post. Also, I’ve shared your website in my social networks
Also visit my web page … best realtor in Palos Verdes CA
Having read this I believed it was extremely informative.
I appreciate you finding the time and effort to put this informative
article together. I once again find myself personally spending way too much time both reading and posting comments.
But so what, it was still worth it!
Also visit my web page: real estate agent New Lenox IL
It’s truly a great and helpful piece of info. I am glad that you
simply shared this helpful info with us. Please stay us informed like this.
Thank you for sharing.
Look into my site; best real estate agent in Schaumburg IL
Hey very interesting blog!
my blog … real estate agent Douglasville GA
Your way of explaining the whole thing in this piece of writing is in fact
nice, all be capable of simply understand it, Thanks a lot.
my homepage; realtor in Nebo NC
Appreciating the dedication you put into your site and detailed information you offer.
It’s great to come across a blog every once in a while that isn’t the same out of date rehashed information. Excellent read!
I’ve bookmarked your site and I’m adding your RSS feeds to
my Google account.
my site – best real estate agent in Chicago IL
I have been exploring for a little for any high quality articles or
weblog posts on this sort of house . Exploring in Yahoo I eventually stumbled upon this web
site. Studying this information So i am satisfied to show
that I’ve an incredibly excellent uncanny feeling I came upon just what
I needed. I most certainly will make sure to don?t
disregard this web site and provides it a look
regularly.
my blog: best realtor in New Lenox IL
I like what you guys are usually up too. This sort of
clever work and exposure! Keep up the wonderful works guys I’ve included you guys
to blogroll.
Look into my homepage – real estate agent New Lenox IL
Great post.
Take a look at my web blog – best real estate agent in Fort Lauderdale FL
I want to to thank you for this good read!! I absolutely
enjoyed every little bit of it. I’ve got you saved as a favorite to look at new stuff you post…
My webpage; best realtor in Crown Point IN
Hello, i believe that i noticed you visited my weblog so i got here to return the favor?.I am trying to to
find things to enhance my website!I guess its good enough to use a few of your concepts!!
My website: real estate agent Nebo NC
I’m not that much of a internet reader to be
honest but your sites really nice, keep it up!
I’ll go ahead and bookmark your site to come back later on. All the best
Feel free to surf to my webpage … realtor in New Lenox IL
I love it when folks get together and share thoughts. Great
website, stick with it!
Look at my page; หีใหม่.net
Howdy! This post couldn’t be written any better! Reading this
post reminds me of my good old room mate! He always kept chatting about this.
I will forward this article to him. Pretty sure he will have
a good read. Many thanks for sharing!
Feel free to visit my homepage; real estate agent Chicago IL
My spouse and I stumbled over here different web address and thought I should check things out.
I like what I see so i am just following you. Look forward to looking
over your web page yet again.
Here is my web blog … best realtor in Douglasville GA
For the reason that the admin of this site is working, no uncertainty very rapidly it
will be famous, due to its feature contents.
Also visit my web blog; 마사지사이트
Hi there, You’ve done an incredible job. I will certainly digg it and personally suggest to my friends.
I am confident they’ll be benefited from this site.
Here is my web-site :: best realtor in New Lenox IL
Very quickly this web site will be famous amid all blogging
and site-building viewers, due to it’s fastidious content
my web page; 디스코드 서버
Hmm is anyone else experiencing problems with the pictures on this blog loading?
I’m trying to find out if its a problem on my end or if it’s the blog.
Any suggestions would be greatly appreciated.
Take a look at my blog post – Bola88
What’s up, I read your blogs like every week. Your story-telling style is awesome, keep it up!
Have a look at my page :: best real estate agent in New Lenox IL
When some one searches for his necessary thing, thus he/she wishes to be available that in detail,
thus that thing is maintained over here.
Take a look at my site :: 마사지사이트
It’s amazing in support of me to have a website, which is beneficial in favor of my knowledge.
thanks admin
My web site 디스코드 서버
I always spent my half an hour to read this web site’s articles daily along with a cup of coffee.
Check out my webpage … 마사지사이트
Hello it’s me, I am also visiting this web site daily,
this site is in fact good kitchen and bathroom remodelling the users
are in fact sharing nice thoughts.
naturally like your web site but you need to check the
spelling on quite a few of your posts. Several of them are rife with spelling issues and I find it very troublesome to inform
the truth then again I will definitely come back again.
my blog post real estate agent Gilbert AZ
Hey there would you mind stating which blog platform
you’re working with? I’m looking to start my own blog in the near future but I’m having a difficult time deciding between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design and style
seems different then most blogs and I’m looking for something unique.
P.S Sorry for being off-topic but I had to ask!
My page – best realtor in Crown Point IN
I got this site from my pal who shared with me concerning this site and at the moment this time I
am browsing this website and reading very informative posts at
this time.
Here is my web page – best real estate agent in Douglasville GA
I loved as much as you’ll receive carried out right here.
The sketch is tasteful, your authored material stylish.
nonetheless, you command get bought an edginess over that
you wish be delivering the following. unwell unquestionably
come more formerly again as exactly the same nearly very often inside
case you shield this increase.
Feel free to surf to my webpage – best realtor in Nebo NC
Why visitors still make use of to read news papers when in this technological
globe everything is accessible on web?
Here is my blog post :: best real estate agent in Gilbert AZ
Hi there i am kavin, its my first time to commenting anyplace, when i read this piece of writing i
thought i could also make comment due to this brilliant article.
Feel free to surf to my blog … real estate agent Schaumburg IL
You really make it seem so easy with your presentation but I find this matter to be actually something which I think I would never
understand. It seems too complicated and extremely broad for me.
I’m looking forward for your next post, I will try to get the hang of
it!
Also visit my web blog: 마사지
I was suggested this blog by my cousin. I’m not sure whether this post is written by him
as nobody else know such detailed about my problem.
You’re amazing! Thanks!
My web blog; real estate agent Gilbert AZ
I used to be able to find good information from your articles.
my web page :: best real estate agent in Chicago IL
Hello there! Quick question that’s entirely off topic.
Do you know how to make your site mobile friendly? My site looks weird when browsing
from my iphone4. I’m trying to find a theme or plugin that might be able to fix this problem.
If you have any recommendations, please share. Many thanks!
Here is my site – best real estate agent in Douglasville GA
Aw, this was an incredibly nice post. Finding the time and actual effort to generate a very good article… but what can I say… I put
things off a whole lot and don’t seem to get nearly anything
done.
my website; 디스코드 서버검색
You have made some really good points there. I checked on the web for more info
about the issue and found most people will go along with your views
on this web site.
Feel free to surf to my blog post best realtor in Douglasville GA
It’s actually a nice and useful piece of information. I’m
happy that you shared this useful information with us.
Please stay us up to date like this. Thanks for sharing.
Here is my blog post; best realtor in Fort Lauderdale FL
Hi there, I enjoy reading through your article. I like to write a little comment to
support you.
Also visit my webpage: real estate agent Crown Point IN
Thanks for the marvelous posting! I genuinely enjoyed reading it, you’re a great author.
I will make sure to bookmark your blog and will come back in the future.
I want to encourage that you continue your great writing,
have a nice holiday weekend!
My webpage: best real estate agent in Nebo NC
Nice answer back in return of this question with solid arguments and describing the whole thing about that.
Take a look at my web-site :: real estate agent Douglasville GA
It’s very easy to find out any topic on web as compared to textbooks, as I found
this article at this web site.
Here is my web blog; real estate agent New Lenox IL
Hi there to all, the contents existing at this website are actually remarkable for people knowledge,
well, keep up the nice work fellows.
Feel free to visit my homepage: best real estate agent in Nebo NC
Hello! I could have sworn I’ve been to your blog before but after browsing through some of the articles
I realized it’s new to me. Regardless, I’m definitely happy I discovered it and I’ll be
bookmarking it and checking back frequently!
Feel free to visit my blog :: 디코서버 찾기
เนื้อหานี้ มีประโยชน์มาก ค่ะ
ดิฉัน ได้อ่านบทความที่เกี่ยวข้องกับ หัวข้อที่คล้ายกัน
สามารถอ่านได้ที่ สมัคร bk989
ลองแวะไปดู
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
จะรอติดตามเนื้อหาใหม่ๆ ต่อไป
I have to thank you for the efforts you have put in penning this site.
I really hope to view the same high-grade content from
you in the future as well. In fact, your creative writing abilities has encouraged
me to get my very own site now ;)
My web page: realtor in New Lenox IL
Hi everyone, it’s my first go to see at this website,
and article is in fact fruitful in favor of me, keep
up posting such articles or reviews.
Look at my site du88vc
Magnificent beat ! I wish to apprentice while you amend your site, how can i
subscribe for a blog web site? The account aided me a
acceptable deal. I had been tiny bit acquainted of this your broadcast provided bright
clear idea
My blog – best realtor in Fort Lauderdale FL
Great post. I was checking constantly this weblog and I am impressed!
Very useful information specially the last section :) I
handle such info much. I used to be looking for this certain information for a very long time.
Thank you and best of luck.
Here is my webpage … 마사지사이트
Hey, I think your website might be having browser compatibility issues.
When I look at your blog in Firefox, it looks fine but when opening in Internet Explorer, it has some overlapping.
I just wanted to give you a quick heads up! Other then that, superb blog!
Also visit my blog post real estate agent Schaumburg IL
I must thank you for the efforts you have put in penning this
site. I really hope to see the same high-grade content by you later on as
well. In truth, your creative writing abilities has
motivated me to get my very own website now ;)
Also visit my blog post – best real estate agent in Gilbert AZ
I do not even know the way I ended up right here,
however I assumed this submit was good. I don’t recognise who you
are however definitely you’re going to a well-known blogger in case you aren’t already.
Cheers!
my web blog; bathroom fitters didsbury
bookmarked!!, I love your site!
my web site; รับทำสติ๊กเกอร์
This design is steller! You certainly know how to keep a
reader amused. Between your wit and your videos, I was almost moved to start my own blog
(well, almost…HaHa!) Great job. I really loved what you had to
say, and more than that, how you presented it. Too cool!
Feel free to surf to my web page; 디스코드 서버
Very shortly this website will be famous amid all blogging viewers, due to
it’s pleasant posts
My homepage best real estate agent in Nebo NC
Magnificent goods from you, man. I have understand your stuff previous to
and you’re just too magnificent. I actually like what you’ve acquired
here, certainly like what you are saying and the way in which you say it.
You make it entertaining and you still care for to keep
it sensible. I can’t wait to read much more from you.
This is actually a wonderful website.
Stop by my page: real estate agent Douglasville GA
I do believe all the ideas you have presented in your post.
They are very convincing and will definitely work. Still, the posts are too brief
for beginners. May you please prolong them a bit from next time?
Thank you for the post.
Also visit my homepage best realtor in Palos Verdes CA
This website definitely has all of the info I wanted about this subject and didn’t know who
to ask.
Look into my web site … tripscan top
This article will help the internet viewers for creating new weblog or even a weblog from start to end.
my web-site – best realtor in Crown Point IN
That is really fascinating, You’re an excessively professional blogger.
I’ve joined your rss feed and stay up for in quest of more of
your wonderful post. Also, I’ve shared your web site in my social networks
Look at my homepage: best real estate agent in Fort Lauderdale FL
Yesterday, while I was at work, my cousin stole my iPad and tested to see if it can survive a 30 foot drop,
just so she can be a youtube sensation. My apple ipad is now broken and
she has 83 views. I know this is entirely off topic but
I had to share it with someone!
my web site: 디스코드 서버검색
What’s up, of course this piece of writing is actually pleasant and I have learned lot of things
from it on the topic of blogging. thanks.
My web site; realtor in New Lenox IL
Link exchange is nothing else but it is only placing the other person’s web site link on your page
at proper place and other person will also do same in support of you.
my homepage best real estate agent in Crown Point IN
It’s remarkable for me to have a site, which is useful designed for my knowledge.
thanks admin
My page; 마사지사이트
This is the perfect site for anybody who hopes to find out about this topic.
You realize so much its almost tough to argue with you (not that I actually would want to…HaHa).
You certainly put a new spin on a topic that has been discussed for ages.
Excellent stuff, just wonderful!
Feel free to surf to my webpage :: best real estate agent in Gilbert AZ
Hi, Neat post. There’s an issue together with your web site in internet explorer, could check this?
IE nonetheless is the marketplace leader and
a big portion of other folks will miss your great writing
due to this problem.
My homepage – real estate agent Chicago IL
Hi there! I just wanted to ask if you ever have any trouble with
hackers? My last blog (wordpress) was hacked and I ended up losing several weeks
of hard work due to no backup. Do you have any methods to stop hackers?
Also visit my web page … 마사지사이트
Wonderful work! That is the type of information that are
meant to be shared around the net. Shame on the seek engines for not positioning this submit upper!
Come on over and seek advice from my web site .
Thanks =)
Visit my web-site :: best real estate agent in Palos Verdes CA
I love what you guys are usually up too. This kind of clever work and exposure!
Keep up the good works guys I’ve you guys to our blogroll.
Review my web page 마사지사이트
Hi there, just became alert to your blog through Google, and found that it is really informative.
I am going to watch out for brussels. I’ll be grateful if
you continue this in future. Numerous people will be benefited
from your writing. Cheers!
Visit my page real estate agent New Lenox IL
Hello there! Would you mind if I share your blog with my facebook
group? There’s a lot of folks that I think would really appreciate
your content. Please let me know. Thanks
my web site – real estate agent Palos Verdes CA
Quality content is the key to interest the visitors to visit the web page, that’s what this website is providing.
Also visit my blog :: shower fitting contractors near me
Amazing issues here. I’m very happy to see your post.
Thank you so much and I am taking a look forward to touch
you. Will you kindly drop me a mail?
Feel free to visit my web blog – best real estate agent in Gilbert AZ
Hello there, I found your website by way of Google whilst
looking for a related matter, your web site came up, it looks
good. I’ve bookmarked it in my google bookmarks.
Hello there, just was alert to your weblog through Google,
kitchen and bathroom renovators near me located that it’s
really informative. I’m going to be careful for brussels. I
will be grateful in the event you proceed this in future.
A lot of folks might be benefited out of your writing.
Cheers!
I loved as much as you will receive carried out right here.
The sketch is attractive, your authored material stylish.
nonetheless, you command get bought an edginess over that you wish
be delivering the following. unwell unquestionably come further
formerly again as exactly the same nearly very often inside case you shield this increase.
Also visit my homepage: best real estate agent in Palos Verdes CA
I don’t even know how I ended up here, but I thought this post was
good. I don’t know who you are but definitely you are going to
a famous blogger if you aren’t already ;) Cheers!
My site :: realtor in Fort Lauderdale FL
Your style is unique in comparison to other people I’ve read stuff from.
I appreciate you for posting when you have the opportunity, Guess I’ll just bookmark this blog.
My website :: 汽水音乐官方客户端
I loved as much as you’ll receive carried out right
here. The sketch is attractive, your authored material stylish.
nonetheless, you command get bought an nervousness over that you wish be delivering the following.
unwell unquestionably come more formerly again since exactly the same
nearly very often inside case you shield this increase.
Also visit my homepage Japan HDV vídeos
Sweet blog! I found it while browsing on Yahoo News.
Do you have any tips on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Many thanks
my web-site; real estate agent Schaumburg IL
Its such as you learn my thoughts! You seem to know so much about
this, such as you wrote the e-book in it or something. I believe
that you can do with a few percent to force the
message house a bit, but other than that, this is wonderful blog.
A fantastic read. I’ll certainly be back.
Also visit my web-site – best real estate agent in Schaumburg IL
If some one desires to be updated with most recent technologies afterward he must be pay
a visit this web page and be up to date every day.
Feel free to visit my website real estate agent Schaumburg IL
Everything is very оpen witһ a precise clarification of the challenges.
Ιt was really informative. Ⲩoᥙr site is ᥙseful. Ꮇany thanks for
sharing!
Visit my web blog – xsociety.website
Yacht Charter Limassol , Yacht Safari Cyprus
and VIP Fishing Cyprus are proudly organized.
We pay personal and professional attention to our respected clients.
We treat you as a VIP, just like you deserve.
We ensure that you will enjoy your yacht or limo trip, to the fullest.
Greetings from Colorado! I’m bored at work so I decided to browse your blog on my
iphone during lunch break. I really like the info you provide here and can’t wait to take a look when I get home.
I’m amazed at how fast your blog loaded on my phone ..
I’m not even using WIFI, just 3G .. Anyways, good site!
my web blog realtor in Crown Point IN
Кухонные кухонные фасады kastamonu
из Кастамону — это современное решение, объединяющее прочность, практичность и стиль.
В отличие от традиционных материалов, таких как эмаль или
шпон, они дольше сохраняют внешний вид и требуют минимального ухода.
Сделайте выбор в пользу инноваций — и ваша кухня будет выглядеть красиво, надежно и
современные долгие годы!
Dating Coach Amsterdam provides significant coaching sessions.
Dating Coach Amsterdam empowers residents to facilitate confidence.
Dating Coach Amsterdam provides support on using dating apps effectively.
The Dating Coach Amsterdam at Dating Coach Amsterdam delivers love and relationship coaching.
The Dating Coach Amsterdam from Dating Coach Amsterdam supports residents in managing
emotions. Dating Coach Amsterdam facilitates understanding of small talk in dating scenarios.
Dating Coach Amsterdam provides clarity for residents seeking authentic relationships.
Dating Coach Amsterdam provides coaching sessions in The Netherlands.
The Dating Coach Amsterdam at Dating Coach
Amsterdam empowers intimacy in dating. The Dating Coach Amsterdam from Dating
Coach Amsterdam helps meaningful dating experiences.
Dating Coach Amsterdam delivers support on facilitating confidence.
Dating Coach Amsterdam allows residents to navigate
Amsterdam dating. Dating Coach Amsterdam provides relationship coaching for couples.
The Dating Coach Amsterdam at Dating Coach Amsterdam offers dating coach services.
The Dating Coach Amsterdam from Dating Coach Amsterdam assists residents in achieving clarity.
Dating Coach Amsterdam streamlines transformation through
authentic dating experiences. Dating Coach Amsterdam provides
support to clients on managing emotions. The Dating Coach Amsterdam
at Dating Coach Amsterdam delivers coaching sessions in Amsterdam.
The Dating Coach Amsterdam from Dating Coach Amsterdam Dating Coach assists residents in facilitating
confidence. Dating Coach Amsterdam provides transformational relationship coaching in The Netherlands.
Have you ever considered about adding a little bit more than just your articles?
I mean, what you say is valuable and everything. Nevertheless think of if
you added some great visuals or videos to give your posts more, “pop”!
Your content is excellent but with pics and clips, this
website could undeniably be one of the most beneficial
in its field. Great blog!
Also visit my site; best realtor in Nebo NC
I simply could not depart your website before suggesting that I actually enjoyed the usual information an individual provide
on your visitors? Is going to be again steadily
to check out new posts
Also visit my blog post – best realtor in Palos Verdes CA
I blog frequently and I seriously thank you for your information. This great article has truly peaked my interest.
I’m going to bookmark your blog and keep checking for
new details about once a week. I opted in for
your RSS feed as well.
My site: real estate agent Crown Point IN
Thanks very interesting blog!
My webpage … real estate agent Crown Point IN
Hello there, just became alert to your blog through Google, and found that
it’s truly informative. I am going to watch out for brussels.
I’ll appreciate if you continue this in future.
A lot of people will be benefited from your writing. Cheers!
Feel free to surf to my web page: medicine online order
Excellent post. I was checking constantly this blog and I’m inspired!
Extremely helpful info particularly the final part :) I maintain such info much.
I was seeking this particular information for a long time.
Thanks and best of luck.
my site – best real estate agent in Chicago IL
Wonderful blog! I found it while browsing on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Appreciate it
Here is my webpage … best realtor in Chicago IL
We stumbled over here from a different web page and
thought I might as well check things out. I like what I see
so i am just following you. Look forward to
going over your web page yet again.
My web blog :: สื่อสิ่งพิมพ์หาดใหญ่
Incredible points. Great arguments. Keep up the good
work.
Here is my web blog – realtor in Nebo NC
Quality articles is the crucial to attract the viewers to
visit the site, that’s what this site is providing.
Here is my site 여기여
Incredible quest there. What happened after? Thanks!
Also visit my web blog naked girls pictures
One of the oldest and most well-known gratis cylinders dedicated to mature and MILF material is
MatureTube. The site’s longevity speaks to the fact that it actually functions as a resource, and it has been around long enough
to create a genuinely massive library. shinhwaspodium.com/bbs/board.php?bo_table=free&wr_id=4794228 https://git.bluegrass.ipaas.io/traceykeeton03
One of the oldest and most well-known gratis cylinders dedicated to mature
and MILF material is MatureTube. The site’s longevity speaks to
the fact that it actually functions as a resource,
and it has been around long enough to create a genuinely massive library.
shinhwaspodium.com/bbs/board.php?bo_table=free&wr_id=4794228 https://git.etoele.com/mosehines6662
안녕하세요, 당신의 내용에 감사드립니다 – 여기서 확실히 새로운
것을 배웠습니다. 하지만 이 웹사이트를 사용하면서
몇 가지 기술적 이슈를 겪었습니다. 사이트를 올바르게 로드하기 위해 여러
번 새로고침해야 했습니다. 당신의 호스팅은 괜찮나요?
불평하는 건 아니지만, 느린 로드되는 경우가 구글 순위에
영향을 미칠 수 있고 Adwords로 광고 및 마케팅을 할 때 높은 품질 점수에
해를 끼칠 수 있습니다. 어쨌든 이 RSS를 제 이메일에 추가했고, 당신의 매혹적인 콘텐츠를 더 확인할 것입니다.
곧 다시 업데이트해 주세요.
|
확실히 멋진 포스트입니다! 당신의 포스트는 정말
도움이 되고, 특히 comprare generico online
viagra에 대한 부분이 인상 깊었어요. 더 많은 내용을 위해 자주 방문할게요.
앞으로도 이런 훌륭한 콘텐츠 부탁드려요! 고맙습니다!
|
안녕! 이 블로그를 우연히 발견했는데, 정말 놀랍습니다!
귀하의 글은 deal에 대해 깊은 통찰을 제공해요.
하지만, 이미지나 비디오를 조금 더 추가하면 방문자들이 더 몰입할 수 있을 것 같아요.
아이디어일 뿐이지만, 고려해 보세요!
계속 좋은 콘텐츠 기대할게요!
|
와, 이 글은 정말 감동적이에요! Heel Pain – Plantar Fasciitis –
Mr Will Edwards에서 이렇게 가치 있는 정보를 찾을
줄 몰랐어요. 당신의 글쓰기 스타일이 매우
명확하고 읽기가 즐거웠어요. 궁금한 점이 있는데, 긴베개커버 관련 더 자세한 자료를 어디서 찾을 수
있을까요? 감사합니다!
|
훌륭한 콘텐츠입니다! 이 웹사이트는 global rollouts에 대해 깊이 있는 정보를
제공해서 정말 감동적이었어요.
다만, 페이지 로딩 속도가 조금 느린 것 같아요.
호스팅 문제인지 확인해 보시면 어떨까요? 그래도 콘텐츠는 정말 최고예요!
앞으로도 기대할게요!
|
안녕하세요! Heel Pain – Plantar Fasciitis – Mr
Will Edwards의 팬이 됐어요! 귀하의 기사는 항상 재미있어요.
특히 Shuttle Service Stuttgart에 대한 설명이 정말 인상
깊었어요. 추천드리자면, 방문자와의 상호작용을 위해 댓글란에 질문를 추가하면 더 활발한 커뮤니티가 될 것 같아요!
고맙습니다!
|
대단해요! 이 사이트에서 آموزش V.rayا에 대해 이렇게 상세한 정보를 얻을 수 있다니 믿기지 않아요.
귀하의 글은 명확하며 일반 독자에게도 딱이에요.
추가로 비슷한 주제의 링크를 공유해
주실 수 있나요? 앞으로도 멋진 콘텐츠 부탁드려요!
|
안녕하세요! Heel Pain – Plantar Fasciitis –
Mr Will Edwards을 동료 추천으로 알게 됐는데, 정말
훌륭해요! healthpulseguide에 대한 당신의 설명는 매우 유용했고.
그런데, 휴대폰에서 볼 때 레이아웃이 약간 어색해요.
모바일 최적화을 고려해 보시면 어떨까요?
그래도 콘텐츠는 대단해요! 고맙습니다!
|
정말 고맙습니다! Heel Pain – Plantar Fasciitis – Mr Will
Edwards의 포스트는 ινέπολη에 대해 제가 찾던 모든 것을 제공해 줬어요.
귀하의 글은 논리적이고 읽혀서 읽는 게 전혀 아깝지 않았어요.
궁금한 점이 있는데, 이 주제에 대해 정기적인 업데이트를 계획 중이신가요?
계속 기대할게요!
|
와우, 이 블로그는 정말 대단해요! book for kids about wounded 관련 정보를 찾다가
Heel Pain – Plantar Fasciitis – Mr Will Edwards에
도착했는데, 기대 이상이었어요. 귀하의 기사는 정말 흥미로워요.
추가로 비슷한 토픽의 커뮤니티를 추천해 주실 수 있나요?
앞으로도 좋은 콘텐츠 부탁드려요!
|
안녕하세요! Heel Pain – Plantar Fasciitis – Mr Will Edwards의 포스트를
읽으면서 정말 즐거웠어요. risc에 대한 당신의 시각은 정말 독창적이에요.
하지만, 인포그래픽 같은 시각 자료를 추가하면 더 매력적일 것
같아요. 제 의견일 뿐! 감사합니다, 다음 포스트도
기대할게요!
|
대단한 블로그네요! eco-friendly school software에 대해 이렇게
상세하고 정보를 제공하는 곳은 드물어요.
귀하의 글쓰기 스타일이 정말 친근하고 계속 읽고 싶어져요.
질문이 있는데, 이 토픽에 대한 웨비나나 이벤트
계획이 있나요? 앞으로도 멋진 콘텐츠 부탁드려요!
|
안녕! Heel Pain – Plantar Fasciitis – Mr
Will Edwards을 처음 방문했는데, 정말 놀라워요!
domain names에 대한 당신의 포스트는 매우 도움이
되고. 하지만, 검색 엔진에서 이 페이지를 찾기가 조금 어려웠어요.
SEO 최적화를 조금 더 강화하면 더 많은 방문자가 올 것 같아요!
감사합니다!
|
대단해요! Heel Pain – Plantar Fasciitis – Mr Will Edwards에서
socks에 대해 이렇게 쉽게 설명한 곳은
처음이에요. 귀하의 기사는 초보자도 쉽게 이해할
수 있게 쓰여 있어서 정말 좋았어요. 추가로 이 주제에 대한 전자책 같은 자료를 제공하시나요?
계속해서 멋진 콘텐츠 기대할게요!
|
안녕! Heel Pain – Plantar Fasciitis – Mr Will Edwards의 포스트를 읽고 정말 즐거웠어요.
viagra comprar 50 mg에 대한 당신의 설명은 정말
논리적이고 이해하기 쉬웠어요. 제안이 있는데,
독자가 직접 참여할 수 있는 설문 같은 콘텐츠를 추가하면 어떨까요?
감사합니다, 다음 포스트도 기대할게요!
|
와, Heel Pain – Plantar Fasciitis – Mr Will Edwards은 정말
멋진 웹사이트네요! SEGPA 관련 정보를 찾다가 여기
왔는데, 당신의 포스트는 정말 유익하고. 다만, 페이스북에서 이 콘텐츠를 더 적극적으로 공유하면 더 많은
사람들이 볼 수 있을 것 같아요! 계속해서 좋은 콘텐츠 부탁드려요!
|
인사드립니다! Heel Pain – Plantar Fasciitis – Mr Will Edwards의 포스트를 읽으며 Бассейн Виктория Елец에 대해 깊은 이해를 얻었어요.
귀하의 글은 정말 유익하고. 궁금한 점이
있는데, 이 주제와 관련된 참고 자료를 알려주실 수 있나요?
감사합니다, 자주 방문할게요!
|
훌륭한 웹사이트입니다! farmacias similares en precio femenino viagra de에 대한 당신의 기사는 정말 인상 깊어요.
하지만, 태블릿에서 볼 때 글씨 크기가 조금 작게 느껴져요.
디자인 조정을 고려해 보시면 어떨까요?
그래도 콘텐츠는 정말 멋져요!
감사합니다!
|
안녕! Heel Pain – Plantar Fasciitis – Mr Will Edwards을 동료에게 추천받아 방문했는데, 정말 놀라워요!
транзистор에 대한 귀하의 콘텐츠는 매우 도움이 되고.
제안로, 방문자와의 상호작용을 위해 라이브 Q&A 같은 이벤트를
열어보면 어떨까요? 계속해서 멋진 콘텐츠 기대할게요!
|
대단해요! Heel Pain – Plantar Fasciitis – Mr Will Edwards에서 funkportal에 대해 이렇게
상세한 정보를 찾을 수 있다니 놀라워요! 당신의 글은 정말 논리적이고 읽혀서 시간이 전혀 아깝지 않았어요.
궁금한 점이 있는데, 이 주제에 대한 온라인 강의
계획이 있나요? 고맙습니다!
|
안녕하세요! Heel Pain – Plantar Fasciitis – Mr Will Edwards의 포스트를 읽고 Cardboard Production Line에 대해 깊은 인상을 받았어요.
귀하의 글쓰기 스타일이 정말 친근하고 계속 읽고 싶어져요.
하지만, 구글에서 이 페이지를 찾기가 조금 어려웠어요.
SEO를 강화하면 더 많은 방문자가 올 것 같아요!
계속해서 좋은 콘텐츠 부탁드려요!
I believe that is among the such a lot vital information for me.
And i’m satisfied studying your article. But want to statement on few basic
issues, The site style is great, the articles is in reality great : D.
Just right activity, cheers
my web site 정품 비아그라 구입
I do not know if it’s just me or if everybody else experiencing issues with your
blog. It appears as though some of the text within your posts are running off the screen. Can someone else
please provide feedback and let me know if this is happening to them too?
This may be a problem with my internet browser because I’ve
had this happen previously. Thanks
Have a look at my web blog best real estate agent in Crown Point IN
This is a really good tip especially to those new to the blogosphere.
Short but very accurate info… Appreciate your sharing this one.
A must read post!
my web page … real estate agent New Lenox IL
Herbalife Cyprus (Nicosia)
is a worldwide nutrition company, with the target of helping people around the world to follow a healthy lifestyle.
It produces high quality products, well tested,
which have become a favorite of all those who shared the same values as us and who
aim to achieve the best version of themselves. Plenty of people have already succeeded and are
maintaining their amazing result. We are committed to help and support you
to achieve your desired result.
Having read this I believed it was extremely informative.
I appreciate you spending some time and energy to put this content together.
I once again find myself spending a significant amount of time both reading and leaving comments.
But so what, it was still worth it!
my site; โรงพิมพ์หาดใหญ่
I like looking through an article that will make people think.
Also, many thanks for allowing me to comment!
Also visit my web-site – 777 coins
KK55
My whole view of betting changed the day I discovered how sure bets work.
At first, I didn’t believe you could cover every outcome and still profit.
But after testing it myself, I was shocked at how consistent
the profits can be.
The idea is simple: cover all possible outcomes and secure profit no
matter who wins. I remember testing it with $200 and seeing how the profit came out no matter the match result.
For once, I didn’t care who won because the profit
was already locked in.
I didn’t expect the profits to add up so quickly.
Most opportunities give around 1–5% profit, but those small gains
stack fast. It made betting feel more like a calculated financial strategy than a gamble.
The right software totally transforms the experience.
Without the software, I wouldn’t even notice most opportunities.
I never imagined software could help beat bookmakers so effectively.
If someone told me years ago that betting could feel safe and
predictable, I’d laugh. Now it’s part of my daily routine and a steady boost to my bankroll.
Anyone who likes smart, low-risk financial moves would appreciate this.
Feel free to surf to my blog :: press release
BL555
Great delivery. Solid arguments. Keep up the amazing
work.
My web blog; MALWARE
Hey there! I know this is kinda off topic however , I’d figured I’d ask.
Would you be interested in exchanging links or maybe guest writing a blog post
or vice-versa? My blog goes over a lot of the same topics
as yours and I think we could greatly benefit from each other.
If you are interested feel free to send me an email.
I look forward to hearing from you! Fantastic blog
by the way!
my blog post … international pharmacy
Детские игрушки в СПб
Also visit my website – https://namedb.ru/article/vladislav-aksinovich-otzyvy/
This is really interesting, You are a very skilled blogger.
I have joined your rss feed and look forward to seeking more of
your excellent post. Also, I have shared your site in my social networks!
My homepage bittele pcb assembly
Hi, I do believe this is a great blog. I stumbledupon it
;) I’m going to revisit yet again since I book-marked it.
Money and freedom is the best way to change, may you be rich and continue to guide
other people.
My web page: itemized list of household items for insurance claim
Игрушки для детей в Петербурге
my page :: https://magenya.ru/vladislav-aksinovich-giponolog-otzyvy/
My whole view of betting changed the day I discovered how sure bets work.
It felt too good to be true that you could bet without
worrying about losing. The moment I ran the numbers myself, everything suddenly made sense.
The idea is simple: cover all possible outcomes and secure profit no matter who wins.
I remember testing it with $200 and seeing how the profit came out no
matter the match result. Watching the match felt
different too — I knew I couldn’t lose.
The consistency is what blew my mind the most. With enough opportunities, that percentage becomes a reliable side
income. It’s closer to long-term investing than traditional betting.
Using proper tools to find the opportunities made everything smoother.
It highlights matches with perfect opposing odds, and that’s where the magic happens.
It actually feels like flipping the script on bookmakers.
If I had known about this earlier, I would’ve started long ago.
Now I treat it like a side investment that grows a little every day.
If you want something steady instead of stressful betting, this method is a lifesaver.
My blog post – article
I’m not that much of a online reader to be honest but your sites really nice, keep it up!
I’ll go ahead and bookmark your website to come back in the future.
Many thanks
my web site Kathmandu Spa Cash On Delivery,
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Stɑtes
254-275-5536
Modernkitchen
Villas for rent in Protaras, by RentVillaCyprus can assure you that the selection and control of each villa is entirely made by us, in order to ensure the
lovely holidays you deserve. Moreover, book your accommodation safely thanks to our secure online payment system.
my webpage :: Protaras Villa Rentals
I visit daily a few sites and sites to read articles or reviews, except this blog gives feature based writing.
Here is my blog post: 12BET
Wonderful blog! I found it while surfing around on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo
News? I’ve been trying for a while but I never seem to get there!
Thank you
Also visit my homepage; rutor-24forum com
I was wondering if you ever thought of changing the layout of your site?
Its very well written; I love what youve got to say. But maybe you could a little more in the way of content
so people could connect with it better. Youve got an awful lot of text for
only having 1 or two images. Maybe you could space it out better?
my blog; Kathmandu Prostitute Service
Wow, marvelous weblog format! How long have you ever been running a blog for?
you made running a blog look easy. The overall glance of your website is wonderful, let alone the content!
Here is my web-site :: 익산출장마사지
Gain expert CRM guidance from a trusted Salesforce Implementation Partner for lasting results.
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Տtates
12394214912
Quickinstall (go.bubbl.us)
I loved as much as you will receive carried out right here.
The sketch is tasteful, your authored material stylish.
nonetheless, you command get bought an nervousness over that you wish be delivering
the following. unwell unquestionably come further formerly again as exactly the same nearly very often inside case you shield this
hike.
Visit my website :: 프리미엄 해킹 PBN 판매 Telegram : @HackPBN
Touche. Great arguments. Keep up the amazing spirit.
Feel free to surf to my blog post … mega2ousbpnmmput4tiyu4oa4mjck2icier52ud6lmgrhzlikrxmysid.onion
each time i used to read smaller posts which as well clear their motive,
and that is also happening with this article which I am reading now.
Stop by my web page – tower rush slot
I visited many websites but the audio quality for audio songs present at this web site is in fact excellent.
My web page 汽水音乐PC版
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Elegant
This is very interesting, You’re a very skilled blogger.
I’ve joined your rss feed and look forward to seeking more
of your wonderful post. Also, I have shared your website in my social networks!
Also visit my web site: MM88 COM
My whole view of betting changed the day I discovered how sure bets work.
At first, I didn’t believe you could cover every
outcome and still profit. But after testing it myself, I was shocked at how
consistent the profits can be.
It’s basically using pure math to make the outcome irrelevant.
I remember testing it with $200 and seeing how the
profit came out no matter the match result.
Instead of anxiety, there was this calm feeling knowing the math had my back.
The consistency is what blew my mind the most. Even a few percent per bet turns into serious monthly income.
It’s closer to long-term investing than traditional betting.
The right software totally transforms the experience.
It highlights matches with perfect opposing odds, and that’s where the magic happens.
I never imagined software could help beat bookmakers
so effectively.
If someone told me years ago that betting could feel safe and predictable, I’d laugh.
Now it’s part of my daily routine and a steady boost to my bankroll.
If you enjoy long-term strategies, this is a perfect fit.
Here is my web page; backlink
bookmarked!!, I really like your web site! https://cryptoboss353.top/
I just like the valuable info you supply in your articles.
I’ll bookmark your weblog and take a look at once
more here regularly. I am moderately certain I will be informed lots of new stuff proper right here!
Good luck for the following!
Also visit my blog post: the pup life sg
Howdy! This blog post could not be written any better!
Looking through this post reminds me of my previous roommate!
He constantly kept preaching about this. I’ll send
this information to him. Pretty sure he’s going to have a great read.
I appreciate you for sharing!
Visit my website: smm alfa
With havin so much written content do you ever run into any problems of plagorism
or copyright violation? My blog has a lot of
exclusive content I’ve either written myself or
outsourced but it appears a lot of it is popping it up all over the internet without my
permission. Do you know any methods to help protect against content from being ripped off?
I’d certainly appreciate it.
Feel free to surf to my blog post – the pup life sg
After looking over a handful of the articles on your web page, I honestly like your technique of writing a blog.
I added it to my bookmark webpage list and will be
checking back in the near future. Please visit
my web site too and tell me what you think.
Also visit my webpage: Builder Woking
I do not even know how I finished up right here, however I thought this publish
used to be great. I do not recognize who you’re but certainly you are going to
a well-known blogger in case you aren’t already.
Cheers!
Here is my blog post: the pup life sg
I’d like to thank you for the efforts you have put in writing this blog.
I’m hoping to check out the same high-grade blog posts from you later on as well.
In fact, your creative writing abilities has motivated me
to get my very own website now ;)
Take a look at my web blog: Builder Farnham
I really like what you guys are usually up too. This sort of clever work
and reporting! Keep up the superb works guys
I’ve you guys to my blogroll.
my webpage :: source
This is a topic which is close to my heart…
Thank you! Where are your contact details though?
Review my site: find more
I used to think gambling was pure luck, but
sure betting completely flipped my perspective. At first, I didn’t
believe you could cover every outcome and still profit.
Once I tried it with real bets, the results amazed me.
It’s basically using pure math to make the outcome irrelevant.
I remember testing it with $200 and seeing how the profit came out
no matter the match result. Instead of anxiety, there was this calm feeling knowing
the math had my back.
I didn’t expect the profits to add up so quickly.
Even a few percent per bet turns into serious monthly income.
It honestly feels more like investing than gambling.
The biggest game changer for me was using good surebet software.
It finds the opportunities instantly and saves hours of searching.
I never imagined software could help beat bookmakers
so effectively.
Looking back, I still can’t believe how simple it actually is.
Now I treat it like a side investment that grows a little every day.
If you enjoy long-term strategies, this is a perfect fit.
my website :: press release
I used to think gambling was pure luck, but sure betting completely flipped my perspective.
At first, I didn’t believe you could cover every outcome
and still profit. But after testing it myself, I was shocked at how consistent the profits can be.
It’s basically using pure math to make the outcome irrelevant.
I remember testing it with $200 and seeing how the profit came out no matter the match result.
Watching the match felt different too — I knew I couldn’t lose.
I didn’t expect the profits to add up so quickly. Most opportunities give around 1–5% profit,
but those small gains stack fast. It’s closer to long-term investing than traditional betting.
The right software totally transforms the experience.
Without the software, I wouldn’t even notice most opportunities.
It actually feels like flipping the script on bookmakers.
If someone told me years ago that betting could
feel safe and predictable, I’d laugh. Now I just sit back and let the small sure profits add up.
If you enjoy long-term strategies, this is a perfect
fit.
Here is my page; information
BL555 Nhà cái
First of all I would like to say superb blog!
I had a quick question which I’d like to ask if you do not mind.
I was interested to find out how you center yourself and clear your thoughts prior
to writing. I have had difficulty clearing my
mind in getting my ideas out there. I do enjoy
writing but it just seems like the first 10 to 15 minutes are wasted just trying to figure out how to
begin. Any ideas or tips? Thank you!
My web-site; smm alfa
Hi there to every one, it’s really a nice for me to visit this website, it
consists of priceless Information.
my blog post; tk88
Cabinet IQ Fort Myers
7830 Drew Ciir Ste 4, Foort Myers,
FL 33967, United Ⴝtates
12394214912
Trendykitchen
I used to think gambling was pure luck, but
sure betting completely flipped my perspective. Honestly, it sounded
like a scam when I first heard that you could bet
on both sides and win. But after testing it myself, I was
shocked at how consistent the profits can be.
It’s basically using pure math to make the outcome irrelevant.
When I split my money across both sides of a
match, I realized just how powerful this method
is. Watching the match felt different too — I knew I couldn’t lose.
The consistency is what blew my mind the most.
Even a few percent per bet turns into serious monthly income.
It honestly feels more like investing than gambling.
The biggest game changer for me was using good surebet software.
It highlights matches with perfect opposing odds, and that’s where the magic
happens. It actually feels like flipping the script on bookmakers.
If I had known about this earlier, I would’ve started long ago.
Now I treat it like a side investment that grows a little every day.
If you enjoy long-term strategies, this is a perfect fit.
Here is my site: link
My whole view of betting changed the day I discovered how sure bets work.
At first, I didn’t believe you could cover every
outcome and still profit. Once I tried it with real bets, the results amazed me.
It’s basically using pure math to make the outcome
irrelevant. The first time I placed two opposite bets, it felt strange, but the results were unreal.
Watching the match felt different too — I knew I couldn’t lose.
I didn’t expect the profits to add up so quickly. Most opportunities give
around 1–5% profit, but those small gains stack fast.
It’s closer to long-term investing than traditional betting.
The biggest game changer for me was using good surebet software.
Without the software, I wouldn’t even notice most opportunities.
I never imagined software could help beat bookmakers so effectively.
If someone told me years ago that betting could
feel safe and predictable, I’d laugh. Now I treat it
like a side investment that grows a little every day. If you want something steady instead of stressful betting, this method is a lifesaver.
Review my homepage: link
My blog post: All Fazi Games in one place
Good day! I could have sworn I’ve visited your blog before but after browsing through a few of the posts I realized it’s new to me.
Anyhow, I’m definitely delighted I stumbled upon it and I’ll be book-marking it and checking
back frequently!
Feel free to visit my web site – Hitclub
If you desire to get much from this paragraph then you have to apply such methods to your
won webpage.
Here is my site Link Slot Server Stabil
I never thought betting could feel so safe until I tried
surebetting. Honestly, it sounded like a scam when I first heard that you could bet on both sides and win. Once I tried it with real bets, the results amazed me.
It’s basically using pure math to make the outcome
irrelevant. The first time I placed two opposite bets, it felt strange, but
the results were unreal. Instead of anxiety, there was this calm feeling knowing
the math had my back.
The consistency is what blew my mind the most. With enough opportunities, that percentage becomes a reliable side income.
It’s closer to long-term investing than traditional betting.
The right software totally transforms the experience. It
highlights matches with perfect opposing odds, and that’s where the magic happens.
For once, the advantage feels like it’s on my side.
Looking back, I still can’t believe how simple it actually is.
Now it’s part of my daily routine and a steady
boost to my bankroll. If you want something steady instead of stressful
betting, this method is a lifesaver.
Feel free to surf to my web blog – backlink
Today, while I was at work, my sister stole my apple ipad and tested to see
if it can survive a 30 foot drop, just so she can be a youtube sensation. My
apple ipad is now destroyed and she has 83 views.
I know this is totally off topic but I had to share
it with someone!
my site … Vu88
This is a good tip particularly to those fresh to the blogosphere.
Brief but very precise info… Appreciate your sharing this one.
A must read article!
Also visit my web site; Oxbet
Howdy just wanted to give you a quick heads up.
The words in your post seem to be running off the screen in Internet explorer.
I’m not sure if this is a formatting issue or something to
do with internet browser compatibility but I thought I’d post to let you know.
The layout look great though! Hope you get the problem fixed
soon. Kudos
Also visit my blog … MALWARE
В отличие от CapEx, операционные расходы подлежат полному вычитанию из доходной части конкретного периода, что обусловлено регулярным характером. https://classifieds.ocala-news.com/author/lonnafatnow
Feel free to surf to my webpage PG Soft High RTP Slots You Can Play Now
Look at my blog – http://asex.Y.52.1@leanna.langton@c.or.r.Idortpkm@johndf.gfjhfgjf.ghfdjfhjhjhjfdgh@sybbr>r.eces.si.v.e.x.g.z@Leanhttps%3a%2F%evolv.e.l.U.pc@Haedongacademy.org
It’s awesome to visit this web page and reading the views of all mates about this post,
while I am also zealous of getting know-how.
My web-site: content automation tools for seo teams
My whole view of betting changed the day I discovered how sure bets work.
Honestly, it sounded like a scam when I first heard
that you could bet on both sides and win. Once I tried it
with real bets, the results amazed me.
All you do is place bets on each side and let the numbers guarantee the return. The first time I placed two opposite bets, it felt strange,
but the results were unreal. Watching the match felt different too — I
knew I couldn’t lose.
What surprised me most is how steady the returns are.
Most opportunities give around 1–5% profit, but those small gains
stack fast. It made betting feel more like a calculated financial strategy
than a gamble.
Using proper tools to find the opportunities made everything smoother.
It finds the opportunities instantly and saves hours of searching.
I never imagined software could help beat bookmakers so
effectively.
Looking back, I still can’t believe how simple it
actually is. Now I treat it like a side investment that grows a little every day.
If you enjoy long-term strategies, this is a perfect fit.
Feel free to visit my web blog article
It’s amazing to visit this website and reading the views of all friends
regarding this piece of writing, while I am also zealous of getting
knowledge.
Feel free to surf to my site cheap
Highly energetic post, I loved that a lot. Will there be a
part 2?
Here is my website :: 레플리카 사이트
What’s Happening i am new to this, I stumbled upon this I’ve discovered It absolutely useful
and it has aided me out loads. I hope to contribute & aid other customers
like its helped me. Great job.
My page … 소액결제현금화
I never thought betting could feel so safe until I tried surebetting.
Honestly, it sounded like a scam when I first heard that you could bet on both sides and win. But after testing it myself, I was shocked at how consistent the profits can be.
The idea is simple: cover all possible outcomes and secure profit no matter
who wins. I remember testing it with $200 and seeing how the profit came out
no matter the match result. For once, I didn’t care who won because the profit was already locked in.
What surprised me most is how steady the returns are. Most opportunities give around
1–5% profit, but those small gains stack fast. It’s closer to
long-term investing than traditional betting.
The biggest game changer for me was using good surebet software.
Without the software, I wouldn’t even notice most
opportunities. For once, the advantage feels like it’s
on my side.
Looking back, I still can’t believe how simple it actually is.
Now it’s part of my daily routine and a steady boost to my bankroll.
If you enjoy long-term strategies, this is a
perfect fit.
My web blog backlink
This is very interesting, You’re an excessively professional blogger.
I have joined your rss feed and stay up for searching for extra
of your excellent post. Also, I’ve shared your website in my
social networks
my blog … Poker Games Online
Great post. I was checking continuously this
blog and I am inspired! Extremely useful info specially the ultimate phase :) I care for such info a lot.
I was looking for this certain info for a
long time. Thanks and best of luck.
Also visit my blog post Xo88
I have read so many posts about the blogger lovers except this article
is actually a good post, keep it up.
Stop by my web blog :: cheap
If you are going for most excellent contents like
me, only pay a visit this web site everyday as it offers quality contents, thanks
Stop by my blog post: singapore massage
You actually make it seem so easy with your presentation but I find
this topic to be really something which I think I
would never understand. It seems too complex and extremely broad for me.
I am looking forward for your next post, I’ll try to get the hang of it!
my web site – viagra indonesia
I really like it when individuals get together and share
views. Great website, stick with it!
my webpage … bokep indonesia
My whole view of betting changed the day I discovered how sure bets work.
It felt too good to be true that you could bet without worrying about losing.
Once I tried it with real bets, the results amazed me.
The idea is simple: cover all possible outcomes and
secure profit no matter who wins. I remember testing it with $200 and seeing how the profit came out no matter the match result.
Watching the match felt different too — I knew I couldn’t lose.
I didn’t expect the profits to add up so quickly.
Most opportunities give around 1–5% profit, but those small
gains stack fast. It honestly feels more like investing than gambling.
The right software totally transforms the experience. It highlights matches with perfect
opposing odds, and that’s where the magic happens.
I never imagined software could help beat bookmakers
so effectively.
If someone told me years ago that betting could feel safe and predictable, I’d
laugh. Now I treat it like a side investment that grows
a little every day. If you enjoy long-term strategies, this
is a perfect fit.
Also visit my website: article
At tһiѕ time іt sounds like Movable Type іs tһe best
blogging platform aѵailable right now. (frօm what Ι’ve read) Ιs that wһat you’re uѕing ⲟn yⲟur blog?
Feel free tߋ surf to my site คลิปหลุด Telegram
Benvenuti nella più grande collezione al mondo di film XXX per adulti, clip di sesso hardcore,
e un negozio unico per tutte le vostre esigenze di cattiveria.
Attraverso la nostra vasta collezione di video, scoprite nuovi e addestrato celebrità,
bella fotografi nelle loro terre selvagge,
e molte altre cose. webpage https://daleels.store/rowenastpierre
Benvenuti nella più grande collezione al mondo di film XXX per adulti, clip di
sesso hardcore, e un negozio unico per tutte le vostre esigenze di cattiveria.
Attraverso la nostra vasta collezione di video, scoprite nuovi e addestrato celebrità,
bella fotografi nelle loro terre selvagge, e molte altre cose.
webpage https://apeitalya.com/author/natashaoflaher/
It’s an remarkable piece of writing designed for all the online viewers; they will take advantage from it I
am sure.
My web page :: wps下载
I never thought betting could feel so safe until I tried surebetting.
It felt too good to be true that you could bet without worrying
about losing. The moment I ran the numbers myself, everything suddenly made sense.
All you do is place bets on each side and let the numbers guarantee the
return. When I split my money across both sides of a
match, I realized just how powerful this method is. Instead of anxiety, there was this calm feeling
knowing the math had my back.
What surprised me most is how steady the returns are.
With enough opportunities, that percentage becomes a reliable side income.
It made betting feel more like a calculated financial strategy than a gamble.
Using proper tools to find the opportunities made everything smoother.
It finds the opportunities instantly and saves hours of
searching. For once, the advantage feels like it’s on my side.
If I had known about this earlier, I would’ve started long ago.
Now it’s part of my daily routine and a steady
boost to my bankroll. If you enjoy long-term strategies,
this is a perfect fit.
my webpage: info
Your style is unique compared to other people I’ve read stuff
from. I appreciate you for posting when you’ve got the opportunity, Guess I will just book mark this page.
Visit my webpage :: feriebolig costa adeje
Here is my web site – Simsinos
Hi! I just wanted to ask if you ever have any trouble with hackers?
My last blog (wordpress) was hacked and I ended up
losing a few months of hard work due to no back up. Do you have any solutions to protect against hackers?
my page – best stem cell clinic
I always spent my half an hour to read this webpage’s content daily along
with a mug of coffee.
Feel free to surf to my web site: stem cell therapy thailand
Good day! This is my first visit to your blog! We are a collection of volunteers and starting a new initiative in a community in the same niche.
Your blog provided us beneficial information to work on.
You have done a marvellous job!
Here is my blog post :: 쩜오룸싸롱
LANDSHI: Революция в индустрии красоты — единая экосистема для клиентов и бизнеса
LANDSHI — это современный инструмент, объединяющее пользователей и мастеров по всей России.
Это комплексная экосистема, где сосредоточены все виды бьюти-услуг.
Один сервис — бесконечный выбор
Больше не нужно искать разные сайты.
На одной платформе представлены:
– Парикмахерские услуги;
– Маникюр и педикюр;
– Косметология;
– Взгляд и оформление бровей;
– Релаксационные и оздоровительные процедуры;
– Лазерная и восковая эпиляция;
– Работа с телом и модификации;
– Солнечный загар;
– Студии мужского стиля.
Преимущества для Клиентов
Для пользователей LANDSHI превращает поиск красоты в легкий процесс.
1. Оперативное нахождение специалистов по
параметрам.
2. Изучение цен и перечня услуг.
3. Изучение мнений реальных людей.
4. Дистанционное бронирование на удобное время.
5. Контроль записей прямо в приложении.
Возможности онлайн запись для мастеров маникюра
Мастеров и Салонов
Предприниматели получают эффективный канал продаж для роста прибыли.
– Создание профиля специалиста или студии.
– Размещение прайс-листа.
– Автоматизация календаря.
– Автоматический сбор заявок.
– Легкая оплата подписки через систему Робокасса.
LANDSHI — связующее звено
Основная миссия сервиса — соединить стороны между потребителем и мастером.
Мы помогаем находить лучших и обеспечиваем максимальную загрузку для каждого мастера в
сфере бьюти-индустрии.
Станьте частью LANDSHI уже сегодня и
трансформируйте свой бизнес!
my web blog; Thunderkick games – play for real money
This is really interesting, You’re a very skilled blogger.
I’ve joined your feed and look forward to seeking more of your excellent post.
Also, I’ve shared your website in my social networks!
Feel free to visit my blog … paris666 เว็บตรง
Hello there, just became aware of your blog through Google,
and found that it’s truly informative. I’m going to watch out for brussels.
I will appreciate if you continue this in future.
Many people will be benefited from your writing.
Cheers!
Here is my site – heavy truck towing
It’s hard to come by well-informed people in this particular subject, however, you seem like
you know what you’re talking about! Thanks
my web-site :: homepage
I still remember the moment a friend recommended me this
new gaming platform that instantly felt more immersive
than the usual ones.
To be fair, I wasn’t planning to stay long, but
the enormous game catalog — so many that scrolling felt
endless — hooked me.
Getting a matched deposit + a pile of spins felt surprisingly generous, and once I topped up my account, it gave me enough room to test different slots without fear.
Sure, the rollover wasn’t the lowest, but I just treated it like part of the
experience.
What really caught me emotionally was how fast the payouts landed.
A day or two later, the money hit my account, and that
moment felt reassuring.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the increasing perks actually felt meaningful.
Getting back a portion of my losses made my sessions less
stressful, and I actually enjoyed the grind.
The game variety overwhelmed me at first — in a good way.
Whether I felt like slow strategic play or chaotic spinning, I found it.
Other times I’d hunt for higher-RTP options, and the platform always had something
fresh.
What also surprised me was how many payment methods they supported.
For me, waiting kills enthusiasm, so the smooth processing
made everything run without friction.
Of course, it wasn’t perfect.
Some game info wasn’t detailed.
And transparency wasn’t 100% ideal.
But emotionally?
The good outweighed the bad for me.
If you’re reading this because you’re curious, from my own experience — I found real entertainment value here.
And yes, you’ll see the link I mentioned, so you can explore it yourself.
Take a look at my web site; online casino
Right away I am ready to do my breakfast, after having my
breakfast coming again to read more news.
My site … полимаркет ставки
Yes! Finally someone writes about sex.
I do not even know the way I stopped up right here, but I thought this post was
good. I do not realize who you’re however certainly you’re going to a famous
blogger if you are not already. Cheers!
My web page; строительная компания
Hi there! Do you use Twitter? I’d like to follow
you if that would be ok. I’m undoubtedly enjoying your blog
and look forward to new updates.
Here is my blog :: Margie
Hello friends, its impressive piece of writing regarding cultureand entirely defined, keep it up all the time.
my site Removal companies
dating+coaches+Dating+Coach+LA+is+one+of+the+finest+for+dating+coach+in+LA+Dating+Coach+LA+355+S+Grand+Ave+%23469%2C+Los+Angeles%2C+CA+90071%2C+United+States
My web-site; dating+coach+Dating+Coach+LA+is+counted+among+the+leading+for+dating+coach+in+Los+Angeles+Dating+Coach+LA+355+S+Grand+Ave+%23469%2C+Los+Angeles%2C+CA+90071%2C+United+States
In HD-Fotos und Video Videos, gibt es zweifellos ein Markt.
Raum für faltig Muschis. Diese Artikel sind heute schwierig zu finden! Mit den umfangreichen Sammlung von struppig Muschis von Hairywomen bbw sexfilme,
können Sie Ihre kleine schmutzigen Hahn in bekommen. https://git.epochteca.com/vetaolvera2832
In HD-Fotos und Video Videos, gibt es zweifellos
ein Markt. Raum für faltig Muschis. Diese Artikel sind heute schwierig zu finden! Mit den umfangreichen Sammlung
von struppig Muschis von Hairywomen bbw sexfilme, können Sie Ihre kleine schmutzigen Hahn in bekommen. http://121.89.204.251:3000/domingomartind/3961bbw-sexfilme/wiki/Der+Versteckte+Thriller+hinter+Mah+Grund%252C+De+als+eines+De+Authentischer+Wirkungen+von+Natural+Body+Porn+Wirkt.
Hi there, after reading this awesome paragraph i am too glad to share my know-how here
with colleagues.
Feel free to surf to my homepage; AXI file application
Pretty! This was an extremely wonderful article.
Many thanks for providing this information.
Look into my page … best hyip
I still remember the moment I accidentally found this new gaming platform that had an atmosphere that
pulled me in emotionally.
Honestly, I was skeptical, but the enormous game catalog — over ten thousand
options — hooked me.
The welcome offer felt like a real push, and once I
topped up my account, I felt that spark of excitement
you only get when you have real chances to play longer.
Sure, the rollover wasn’t the lowest, but it felt fair
considering the size of the bonus.
What really caught me emotionally was how fast the payouts landed.
Soon after requesting, the funds were already processed, and that moment felt
reassuring.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the gradual rewards actually felt meaningful.
Getting back regular cashback packages helped stretch my balance, and I kept
playing more confidently.
The game variety overwhelmed me at first — in a good way.
Classic table games, fast-paced slots, live dealers, jackpots — everything
was there.
Sometimes I’d switch from roulette to video slots, and the platform always had something fresh.
What also surprised me was how many payment methods
they supported.
For me, waiting kills enthusiasm, so the smooth processing made the sessions start without delay.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And the licensing details were not visible upfront.
But emotionally?
The good outweighed the bad for me.
If you’re reading this because you’re curious, from my own experience — it became one of the few
places I kept returning to.
And yes, there’s a link in the comment, so you can explore it yourself.
Here is my blog … website
Unquestionably consider that that you said. Your favourite reason appeared
to be at the internet the simplest factor to bear in mind
of. I say to you, I certainly get irked while folks think about worries that they plainly do not realize about.
You managed to hit the nail upon the top as smartly as outlined out the entire thing without having side effect , folks could take a signal.
Will probably be again to get more. Thanks
Also visit my website :: Husqvarna 450XH EPOS
I still remember the moment I stumbled onto a massive game hub that had an atmosphere
that pulled me in emotionally.
To be fair, I wasn’t planning to stay long, but the sheer volume of games — over ten thousand options — hooked me.
Getting a matched deposit + a pile of spins felt surprisingly generous, and after making the first deposit, I finally understood why people talk
about good bonuses.
Sure, the rollover wasn’t the lowest, but it felt fair considering the size of the
bonus.
What really caught me emotionally was how fast the payouts landed.
Within 24–72 hours, the funds were already processed, and that moment felt reassuring.
The VIP program was another unexpected thing.
I never cared much for VIP stuff, but the cashback percentages actually
felt meaningful.
Getting back a portion of my losses made my sessions less
stressful, and I felt supported rather than drained.
The game variety overwhelmed me at first
— in a good way.
Classic table games, fast-paced slots, live dealers, jackpots — everything was there.
Other times I’d hunt for higher-RTP options, and there was always
something new to try.
What also surprised me was that they even accepted modern digital currencies.
For me, simplicity matters, so the smooth processing made the sessions start without delay.
Of course, it wasn’t perfect.
Some game info wasn’t detailed.
And transparency wasn’t 100% ideal.
But emotionally?
It still felt like more fun than trouble.
If you’re reading this because you’re curious, from my own experience — I found real entertainment
value here.
And yes, you’ll see the link I mentioned, so you can explore it yourself.
Review my site online casino
I am regular visitor, how are you everybody? This paragraph posted at
this website is really pleasant.
Review my site – pid68808
I have read so many content about the blogger lovers but this article is really
a fastidious article, keep it up.
Review my webpage – london
บทความนี้ ให้ข้อมูลดี ครับ
ผม ได้อ่านบทความที่เกี่ยวข้องกับ ข้อมูลเพิ่มเติม
ที่คุณสามารถดูได้ที่
Micheline
เผื่อใครสนใจ
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
Also visit my web blog mabet99 [Micheline]
I’ll never forget the moment I accidentally found a massive game hub that
looked different from anything I’d tried before.
At first I wasn’t sure what to expect, but
the sheer volume of games — over ten thousand options
— hooked me.
Getting a matched deposit + a pile of spins felt surprisingly generous, and once I
topped up my account, it gave me enough room to test different slots without fear.
Yes, the wagering wasn’t tiny, but I just treated it like part of the experience.
What really caught me emotionally was how fast the payouts landed.
Soon after requesting, the funds were already processed, and that moment felt reassuring.
The VIP program was another unexpected thing.
I never cared much for VIP stuff, but the gradual rewards actually felt meaningful.
Getting back 5%–15% helped stretch my balance,
and I felt supported rather than drained.
The game variety overwhelmed me at first — in a good
way.
Every session felt different because the library
was massive.
Sometimes I’d just dive into new releases, and the platform always
had something fresh.
What also surprised me was that they even accepted modern digital currencies.
For me, fast transactions matter, so the crypto support
made the sessions start without delay.
Of course, it wasn’t perfect.
The VIP climb took time.
And transparency wasn’t 100% ideal.
But emotionally?
The good outweighed the bad for me.
If you’re reading this because you’re curious, I can honestly say — this
platform gave me some of the most memorable gaming moments I’ve had online.
And yes, you’ll see the link I mentioned, so feel free to check it out.
Also visit my webpage; bettiing site
I used to be suggested this blog through my cousin. I’m
no longer sure whether or not this publish
is written via him as nobody else recognize such specified approximately my problem.
You are amazing! Thank you!
Have a look at my page :: trc20 usdt wallet
Hi there! I’m at work browsing your blog from my new iphone!
Just wanted to say I love reading your blog
and look forward to all your posts! Keep up the fantastic work!
my web site – รับรื้อถอน
Dating Coach LA provides professional dating advice
in Los Angeles, CA. Dating Coach LA enables clients
to define their dating goals. The Dating Coach LA from Dating Coach LA provides personalized therapy to handle dating issues.
Dating Coach LA helps individuals in finding love with confidence.
The Dating Coach LA at Dating Coach LA delivers helpful feedback on dating apps.
Dating Coach LA facilitates workshops to boost confidence when attracting potential partners.
The Dating Coach LA from Dating Coach LA assists clients to
understand dating psychology. Dating Coach LA offers an authentic approach to dating coaching.
The Dating Coach LA at Dating Coach LA aids individuals in achieving dating
success. Dating Coach LA empowers clients to navigate the dating scene in Los Angeles, CA.
The Dating Coach LA from Dating Coach LA delivers expert assistance for dating coach in LA.
Dating Coach LA provides resources for overcoming dating challenges.
The Dating Coach LA at Dating Coach LA assists clients in setting realistic dating expectations.
Dating Coach LA streamlines the development of effective
dating strategies. The Dating Coach LA from
Dating Coach LA allows clients to achieve their dating goals.
Dating Coach LA delivers guidance in establishing meaningful relationships.
The Dating Coach LA at Dating Coach LA offers complete coaching
services to clients in Los Angeles, CA.
Pretty! This has been an extremely wonderful
post. Many thanks for providing these details.
Have a look at my web-site … nm9
Hello to all, how is everything, I think every one is getting more from this web site, and your views are
good designed for new visitors.
Here is my site … 1more Quad Draiveru Ausīs Liekamās Austiņas
Cabiknet IQ
8305 Stat Hwy 71 #110, Austin,
TX 78735, Unitsd Ꮪtates
254-275-5536
CADmodel
Hi, i think that i saw you visited my blog so i came
to “return the favor”.I’m attempting to find things
to enhance my site!I suppose its ok to use some of your ideas!!
Also visit my webpage бригада белорусов
A fascinating discussion is worth comment. I believe that you ought to write more
about this issue, it may not be a taboo subject but
usually people do not speak about these topics. To the next!
Cheers!!
my blog post :: slot pepek
Jungle Driving School Omaha
4020 Տ 147th St, Omaha,
NE 68137, United Տtates
14024170547
advanced driving course
Thank you for such an insightful post—it definitely cleared things up for
me, and for anyone needing carpet cleaning, AJS Carpet Cleaning is highly recommended due to their commitment to certified-quality standards,
their well-trained technicians skilled in multiple cleaning techniques,
and their ongoing investment in updated industry practices even without referencing specific certifications, a dedication which helps reduce retakes and supports delivering exceptional results
and excellent customer service.
Here is my site … Stain removal
Today, I went to the beach front with my children. I found a sea shell and gave it to
my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She put the shell to her ear and screamed.
There was a hermit crab inside and it pinched her ear.
She never wants to go back! LoL I know this is completely off
topic but I had to tell someone!
Review my homepage :: Seo Toronto for Dentists
Hi there Dear, are you really visiting this site regularly,
if so afterward you will definitely get good experience.
my web site … tc game
Excellent post. I was checking constantly this weblog
and I am impressed! Very useful information specifically the ultimate phase :) I care
for such information a lot. I used to be looking for this certain information for a long
time. Thanks and best of luck.
my web page: tc game
Have you ever thought about creating an ebook or guest authoring on other websites?
I have a blog centered on the same topics you discuss and would love to have you share some stories/information. I
know my visitors would appreciate your work. If you’re even remotely interested,
feel free to shoot me an email.
Here is my blog – tc lottery
Reels casino
My page; Рилс казино
Hi, i think that i saw you visited my site so i came to “return the favor”.I am attempting to
find things to improve my site!I suppose its ok to use a few of your ideas!!
Feel free to visit my site raised garden bed clearance
I’ll never forget the moment I stumbled onto a fresh online
casino site that had an atmosphere that pulled me in emotionally.
To be fair, I wasn’t planning to stay long,
but the crazy number of titles — so many that scrolling felt endless — caught my attention.
The starting bonus genuinely boosted my balance, and after making the first deposit,
I finally understood why people talk about good bonuses.
Yes, the wagering wasn’t tiny, but I managed to handle it with patience.
What really caught me emotionally was how fast the payouts landed.
Soon after requesting, I saw the payout confirmed, and honestly,
that’s when the platform won me over.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the cashback percentages actually felt
meaningful.
Getting back a portion of my losses helped stretch
my balance, and I felt supported rather than drained.
The game variety overwhelmed me at first — in a
good way.
Classic table games, fast-paced slots, live dealers, jackpots — everything was there.
Sometimes I’d switch from roulette to video slots, and there was always something
new to try.
What also surprised me was that they even accepted modern digital
currencies.
For me, simplicity matters, so the smooth processing made everything run without friction.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And transparency wasn’t 100% ideal.
But emotionally?
Despite the flaws, I kept coming back.
If you’re reading this because you’re curious, I can honestly say — this platform gave
me some of the most memorable gaming moments I’ve had online.
And yes, I dropped a comment link below, so feel
free to check it out.
Feel free to visit my web-site url
I was recommended this blog through my cousin. I’m not positive
whether or not this put up is written by way of him as nobody else
recognize such specific about my problem. You are amazing!
Thank you!
my web blog … distillate canada online
You can definitely see your enthusiasm in the article you write.
The sector hopes for more passionate writers like you who aren’t afraid to
say how they believe. All the time go after your heart.
My website; tc game
I visited multiple web sites but the audio feature for audio songs
existing at this web site is actually superb.
Here is my web site :: V2rayn官网下载
Take a look at my blog … Pornhub
This blog was… how do you say it? Relevant!! Finally I have found something that
helped me. Appreciate it!
Look at my web page – Georgia cyber security academy
I am in fact happy to glance at this webpage posts which contains lots of useful facts, thanks for providing these
data.
my website: tc lottery
Hey this is kinda of off topic but I was wanting to know if
blogs use WYSIWYG editors or if you have to manually code with
HTML. I’m starting a blog soon but have no
coding knowledge so I wanted to get advice from someone with experience.
Any help would be greatly appreciated!
Look into my web blog: metal raised garden beds
Terrific post however , I was wanting to know if you
could write a litte more on this topic? I’d be very grateful
if you could elaborate a little bit further. Appreciate it!
my homepage :: magic mushroom online store canada
When some one searches for his essential thing, thus he/she wants to
be available that in detail, therefore that thing is maintained over here.
Also visit my blog post: magic mushroom online store canada
I don’t even know how I ended up here, but I thought
this post was great. I don’t know who you are but definitely you are
going to a famous blogger if you are not already ;
) Cheers!
my site tc lottery
I still remember the moment a friend recommended me this new gaming platform that instantly felt more immersive than the usual ones.
Honestly, I was skeptical, but the sheer volume of games — over
ten thousand options — hooked me.
The welcome offer felt like a real push, and once I topped up
my account, I finally understood why people talk about good bonuses.
The requirements weren’t exactly relaxed, but I managed to handle it with patience.
What really caught me emotionally was how the cashout didn’t leave me waiting for days.
Within 24–72 hours, the funds were already processed, and that moment felt
reassuring.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the cashback percentages actually felt meaningful.
Getting back 5%–15% made my sessions less stressful, and I kept playing
more confidently.
The game variety overwhelmed me at first — in a good way.
Whether I felt like slow strategic play or chaotic spinning, I found
it.
Sometimes I’d switch from roulette to video
slots, and there was always something new to try.
What also surprised me was how many payment methods they supported.
For me, simplicity matters, so the smooth processing made everything run without friction.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And transparency wasn’t 100% ideal.
But emotionally?
Despite the flaws, I kept coming back.
If you’re reading this because you’re curious, from my own experience — I found real entertainment value here.
And yes, there’s a link in the comment, so feel free to
check it out.
my homepage … online casino
Outstanding post however , I was wondering if you could write a litte more on this topic?
I’d be very grateful if you could elaborate a little bit more.
Kudos!
My blog; buy magic mushrooms online canada
Thanks for sharing your thoughts about ebike for commuting.
Regards
my web page electric commuter bike
I absolutely love your blog and find most of your post’s
to be just what I’m looking for. Do you offer guest writers to write content for you personally?
I wouldn’t mind creating a post or elaborating
on a number of the subjects you write related to here. Again, awesome blog!
Feel free to surf to my blog – buy concentrates online canada
This is very fascinating, You’re a very professional blogger.
I have joined your rss feed and look forward to seeking extra of your
wonderful post. Additionally, I’ve shared your site in my social networks
Feel free to surf to my homepage; online mushroom delivery canada
I still remember the moment I accidentally found a massive game hub that had an atmosphere that pulled me in emotionally.
At first I wasn’t sure what to expect, but the enormous game catalog — so many that
scrolling felt endless — caught my attention.
Getting a matched deposit + a pile of spins felt surprisingly generous, and
once I topped up my account, I felt that spark of excitement
you only get when you have real chances to play longer.
Yes, the wagering wasn’t tiny, but it felt fair considering the size of the
bonus.
What really caught me emotionally was how smooth the withdrawals
were.
A day or two later, the funds were already processed,
and that gave me a sense of trust.
The VIP program was another unexpected thing.
I never cared much for VIP stuff, but the gradual rewards actually softened the losses when luck
turned.
Getting back regular cashback packages felt like someone handing me a second chance, and I felt supported rather than drained.
The game variety overwhelmed me at first — in a good way.
Every session felt different because the library was massive.
Sometimes I’d switch from roulette to video slots, and there was always
something new to try.
What also surprised me was how many payment methods they supported.
For me, waiting kills enthusiasm, so the crypto
support made everything run without friction.
Of course, it wasn’t perfect.
Some game info wasn’t detailed.
And transparency wasn’t 100% ideal.
But emotionally?
Despite the flaws, I kept coming back.
If you’re reading this because you’re curious, trust
me — this platform gave me some of the most memorable gaming
moments I’ve had online.
And yes, you’ll see the link I mentioned, so you can explore
it yourself.
Here is my webpage – website
When I originally commented I appear to have clicked the -Notify me when new comments are added- checkbox and from now
on every time a comment is added I get 4 emails with the exact same comment.
Is there an easy method you can remove me from that service?
Cheers!
Have a look at my web-site :: Togelup
Hi there, just became aware of your blog through Google, and found that it’s really informative.
I’m gonna watch out for brussels. I will be grateful if
you continue this in future. Numerous people will be benefited
from your writing. Cheers!
Have a look at my website; LG
Pretty nice post. I just stumbled upon your blog and wanted to say that I have really
enjoyed browsing your blog posts. After all I’ll be subscribing
to your rss feed and I hope you write again very soon!
My site: tc lottery
Hi there! I’m at work browsing your blog from my new apple iphone!
Just wanted to say I love reading through your blog and look forward to
all your posts! Carry on the outstanding work!
Stop by my homepage: tc game
Hi there it’s me, I am also visiting this web site regularly, this site is really fastidious and the people are actually sharing nice thoughts.
Here is my site … commuter electric bikes
I’m really impressed with your writing skills as well as with the layout on your weblog.
Is this a paid theme or did you customize it yourself?
Anyway keep up the nice quality writing, it is rare to see a nice blog
like this one these days.
My web site :: tc game
At this time it appears like Movable Type is the preferred blogging platform available right now.
(from what I’ve read) Is that what you’re using on your
blog?
Also visit my page … sayang 138
I’m impressed, I have to admit. Seldom do I come across a blog that’s equally
educative and engaging, and let me tell you, you have hit the nail on the head.
The problem is an issue that not enough men and women are speaking intelligently
about. Now i’m very happy that I came across this during my hunt for something concerning this.
Have a look at my blog; tc game
Wow, fantastic blog layout! How lengthy have you been blogging for?
you made blogging look easy. The full glance of your website is excellent,
let alone the content!
Also visit my website raised garden bed clearance
I couldn’t resist commenting. Perfectly written!
Also visit my site pubs in malleshwaram
Excellent blog post. I definitely love this site.
Stick with it!
Feel free to surf to my webpage :: open bo jakarta
Why people still use to read news papers when in this technological world all is
existing on net?
Here is my homepage … step through commuter ebike
Hi there, I found your web site by way of Google at the same time as searching ebike for commuting a related matter, your site got here up,
it appears great. I’ve bookmarked it in my google bookmarks.
Hi there, simply become aware of your blog through Google,
and found that it is really informative. I’m going
to watch out for brussels. I’ll be grateful if you happen to
continue this in future. Lots of other folks might be benefited out of your writing.
Cheers!
Heya i am best electric bike for commuting the
first time here. I came across this board and I in finding It
really helpful & it helped me out much. I am hoping to present one thing again and aid others such as you aided me.
I like the valuable information you supply for your articles.
I’ll bookmark your weblog and test again here regularly. I am
rather certain I’ll be told a lot of new stuff right here!
Good luck for the next!
My homepage; distillate canada online
Hello to all, the contents present at this web site are actually remarkable electric bike for work commute people experience,
well, keep up the good work fellows.
I’ll never forget the moment I stumbled onto a massive game hub that instantly felt more immersive than the usual ones.
At first I wasn’t sure what to expect, but the enormous game catalog — so many that scrolling felt endless — caught my
attention.
The starting bonus genuinely boosted my balance, and once I topped up my account, it gave
me enough room to test different slots without fear.
Sure, the rollover wasn’t the lowest, but it felt fair considering the
size of the bonus.
What really caught me emotionally was how smooth the
withdrawals were.
Soon after requesting, the money hit my account, and honestly, that’s when the platform won me over.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the cashback percentages actually felt meaningful.
Getting back regular cashback packages made my sessions less stressful, and I felt supported rather than drained.
The game variety overwhelmed me at first — in a good way.
Whether I felt like slow strategic play or chaotic spinning, I found it.
Sometimes I’d switch from roulette to video slots,
and the platform always had something fresh.
What also surprised me was how easy deposits were.
For me, fast transactions matter, so the smooth processing made
everything run without friction.
Of course, it wasn’t perfect.
Some game info wasn’t detailed.
And the licensing details were not visible upfront.
But emotionally?
Despite the flaws, I kept coming back.
If you’re reading this because you’re curious, I can honestly
say — this platform gave me some of the most memorable gaming moments I’ve had online.
And yes, there’s a link in the comment, so give it a
look if you’re curious.
my homepage: bettiing site
Right away I am ready to do my breakfast, afterward having my breakfast coming yet again to read other news.
My website; kaya303 situs
Платежные системы казино
Feel free to surf to my blog post … Казино бонус код
I know this if off topic but I’m looking into starting my own weblog and was
wondering what all is required to get setup? I’m assuming having a blog like yours would cost a
pretty penny? I’m not very web smart so I’m not 100%
positive. Any tips or advice would be greatly appreciated.
Many thanks
Here is my web-site PXJ
What’s up everybody, here every person is sharing such experience, thus it’s pleasant to read this web site,
and I used to go to see this web site all the
time.
Stop by my web site – live online casino
Your style is really unique compared to other people I’ve read stuff from.
I appreciate you for posting when you’ve got the opportunity,
Guess I’ll just book mark this web site.
Stop by my web blog – slon5.cc
4M Dental Implant Center
3918 Lⲟng Beach Blvd #200, Long Beach,
СA 90807, United Ѕtates
15622422075
oral blog (https://go.bubbl.us)
Appreciating the time and energy you put into your blog and in depth information you offer.
It’s awesome to come across a blog every once
in a while that isn’t the same old rehashed information. Fantastic read!
I’ve bookmarked your site and I’m including your RSS feeds to
my Google account.
My page bokep indonesia
Hello i am kavin, its my first time to commenting anywhere, when i read
this article i thought i could also make comment due to this good piece of writing.
Also visit my web site cialis
We recognize the value of your time, which is why
we have incorporated a Turbo Mode feature into Easy Videos Downloader.
My web-site … Zeemo [zeemo.to]
24afpy
Thank you for any other excellent post. The place else may just
anybody get that kind of info in such a perfect approach
of writing? I’ve a presentation subsequent week, and I am at the look
for such information.
My site :: Garage Conversions Manchester
References:
Soaring eagle casino
References:
suprasage.com
Every weekend i used to pay a quick visit this web site, as
i wish for enjoyment, as this this site conations in fact pleasant funny stuff too.
Feel free to visit my website :: Loft Conversions Manchester
Hiya! I know this is kinda off topic nevertheless I’d figured I’d ask.
Would you be interested in exchanging links or maybe guest authoring a blog
post or vice-versa? My website covers a lot of the same subjects as yours and I feel we could greatly benefit from each other.
If you might be interested feel free to send me an email.
I look forward to hearing from you! Great blog by the way!
My blog … Madie
I still remember the moment I stumbled onto a fresh online casino site that looked different from
anything I’d tried before.
At first I wasn’t sure what to expect, but the sheer volume of games — over ten thousand options — hooked me.
The welcome offer felt like a real push, and after making the first deposit, I felt that spark
of excitement you only get when you have real chances to play longer.
The requirements weren’t exactly relaxed, but I managed to handle it with patience.
What really caught me emotionally was how smooth the withdrawals were.
Within 24–72 hours, I saw the payout confirmed, and
that gave me a sense of trust.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the gradual rewards actually
felt meaningful.
Getting back a portion of my losses helped stretch my balance, and I kept
playing more confidently.
The game variety overwhelmed me at first — in a good way.
Whether I felt like slow strategic play or chaotic spinning, I found it.
Other times I’d hunt for higher-RTP options, and I never ran out of choices.
What also surprised me was that they even accepted modern digital currencies.
For me, simplicity matters, so the smooth processing made the
sessions start without delay.
Of course, it wasn’t perfect.
The VIP climb took time.
And the licensing details were not visible upfront.
But emotionally?
It still felt like more fun than trouble.
If you’re reading this because you’re curious, trust me — it became one of the few places I kept returning to.
And yes, you’ll see the link I mentioned, so feel free to check it out.
Greetings! I know this is kinda off topic but I was wondering if you knew where I could find
a captcha plugin for my comment form? I’m using the
same blog platform as yours and I’m having difficulty finding one?
Thanks a lot! http://sm-tur.ru/index.php?subaction=userinfo&user=afaqudamezi
Good answers in return of this difficulty with firm arguments and explaining
everything regarding that.
my web-site :: Website
You should be a part of a contest for one of the most useful websites online.
I will highly recommend this web site!
Also visit my web blog: Loft Conversions Manchester
Thank you a lot for sharing this with all folks you actually recognise what
you’re talking approximately! Bookmarked. Kindly
also discuss with my website =). We may have a hyperlink alternate arrangement among us
Here is my web blog :: 부산달리기
Hi! I know this is kinda off topic but I was wondering if
you knew where I could get a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having trouble finding one?
Thanks a lot!
Also visit my web-site … HiBT exchange review
My brother suggested I might like this website.
He was once totally right. This publish actually made my day.
You can not consider simply how much time I had spent for this information! Thank you!
Here is my web-site; 뉴토끼
Please let me know if you’re looking for a article author for your blog.
You have some really good posts and I feel I would be a good asset.
If you ever want to take some of the load off, I’d love
to write some content for your blog in exchange for a
link back to mine. Please shoot me an e-mail if interested.
Thanks!
my homepage; African hunting safaris
I do not know if it’s just me or if perhaps everyone else experiencing problems with your website.
It seems like some of the written text within your
content are running off the screen. Can somebody else please provide feedback and
let me know if this is happening to them as well?
This could be a issue with my browser because I’ve had this happen previously.
Cheers
Check out my web blog :: African hunting safaris
Thanks for sharing such a good thought, paragraph
is good, thats why i have read it entirely
my homepage African hunts
Hi! This is my first comment here so I just wanted to give a quick shout out and say I really enjoy reading your blog posts.
Can you suggest any other blogs/websites/forums that go over the same topics?
Many thanks!
my blog … hunting safaris in Africa
Look into my site – Cathy
What’s up mates, nice piece of writing and fastidious urging commented here, I am truly
enjoying by these. http://ethnoglobus.az/index.php?subaction=userinfo&user=yrezixepuvo
Hi there Dear, are you genuinely visiting this web site
on a regular basis, if so afterward you will without doubt obtain fastidious knowledge.
Feel free to surf to my web blog – https://lendirku.net/search?q=bokep+indonesia
Hello There. I found your blog using msn. This is an extremely well written article.
I’ll be sure to bookmark it and return to read more of your useful info.
Thanks for the post. I’ll definitely return.
Take a look at my blog: visit company website
казино viks
My web blog; blog
My family members all the time say that I am killing my time here at web, but I know I am
getting know-how daily by reading such pleasant articles.
Feel free to visit my web blog: money
Hey I know this is off topic but I was wondering if you knew of any widgets I could add to
my blog that automatically tweet my newest twitter updates.
I’ve been looking for a plug-in like this for quite some time and
was hoping maybe you would have some experience with something like this.
Please let me know if you run into anything. I truly enjoy reading
your blog and I look forward to your new updates.
Here is my web-site; 39bet game
Hi there! I know this is somewhat off topic but I was wondering
which blog platform are you using for this website?
I’m getting sick and tired of WordPress because I’ve had
problems with hackers and I’m looking at options for another platform.
I would be great if you could point me in the direction of a good platform.
my web-site medicine online shopping
It genuinely surprised me when I accidentally found a massive game hub that
instantly felt more immersive than the usual ones.
Honestly, I was skeptical, but the crazy number of titles — over ten thousand options — caught my
attention.
Getting a matched deposit + a pile of spins felt surprisingly generous, and after
making the first deposit, I finally understood why people talk
about good bonuses.
The requirements weren’t exactly relaxed, but
I managed to handle it with patience.
What really caught me emotionally was how smooth the withdrawals were.
Soon after requesting, the funds were already processed, and that gave me a sense of trust.
The VIP program was another unexpected thing.
I’m not usually someone who climbs loyalty tiers, but
the cashback percentages actually felt meaningful.
Getting back regular cashback packages helped stretch my balance, and
I kept playing more confidently.
The game variety overwhelmed me at first — in a good way.
Classic table games, fast-paced slots, live dealers, jackpots — everything was there.
Other times I’d hunt for higher-RTP options, and there was always something new to try.
What also surprised me was how easy deposits were.
For me, waiting kills enthusiasm, so the crypto support made the sessions start without
delay.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And the licensing details were not visible upfront.
But emotionally?
It still felt like more fun than trouble.
If you’re reading this because you’re curious, from my own experience — I found
real entertainment value here.
And yes, there’s a link in the comment, so you can explore it yourself.
Have you ever thought about including a little bit more than just your articles?
I mean, what you say is important and all. But imagine if you added some great pictures or videos to give your posts more, “pop”!
Your content is excellent but with pics and clips, this site could certainly be one of the best in its field.
Very good blog!
my site … MALWARE
I think the admin of this site is actually working
hard in favor of his web site, for the reason that here every information is quality based data.
my blog post; happy jokers casino no deposit bonus
Hi there, i read your blog occasionally and i own a similar
one and i was just wondering if you get a lot of spam responses?
If so how do you stop it, any plugin or anything you can recommend?
I get so much lately it’s driving me insane so any
assistance is very much appreciated.
Here is my blog … canadian pharcharmy
This article is in fact a fastidious one it assists new internet visitors, who are
wishing in favor of blogging.
Also visit my web-site happy jokers casino no deposit bonus
Thank you for another informative website.
The place else could I get that type of information written in such a perfect manner?
I have a project that I am just now working on, and I’ve been on the glance out for such information.
Review my blog post virur
I don’t even know how I ended up here, but I thought
this post was great. I don’t know who you are but definitely you’re
going to a famous blogger if you are not already ;) Cheers!
Also visit my website :: no index link
Busy Bee Jumpers
45 Main Տt 6C, Wareham,
MA 02571, Unites States
508-514-2005
inflatable rentals fⲟr community events (atavi.com)
On the one hand, there’s definitely no shortage of peptides companies asserting
that they are the very best.
Here is my homepage – Pre-designed peptide cocktails [Sam]
I’ll never forget the moment I accidentally found a massive game hub that instantly
felt more immersive than the usual ones.
At first I wasn’t sure what to expect, but the crazy number of titles — more than enough choices to
last a lifetime — kept me exploring.
Getting a matched deposit + a pile of spins felt surprisingly generous,
and once I topped up my account, I felt that spark of excitement you only get when you have real chances to play longer.
Yes, the wagering wasn’t tiny, but I managed to handle it with patience.
What really caught me emotionally was how smooth the withdrawals were.
Within 24–72 hours, the money hit my account, and that gave me a
sense of trust.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the increasing perks
actually felt meaningful.
Getting back regular cashback packages made my sessions
less stressful, and I kept playing more confidently.
The game variety overwhelmed me at first — in a good way.
Classic table games, fast-paced slots, live dealers, jackpots — everything was there.
Other times I’d hunt for higher-RTP options, and the platform always
had something fresh.
What also surprised me was that they even accepted modern digital currencies.
For me, waiting kills enthusiasm, so the crypto support made the sessions start without delay.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And transparency wasn’t 100% ideal.
But emotionally?
The good outweighed the bad for me.
If you’re reading this because you’re curious, from my own experience — this
platform gave me some of the most memorable gaming moments I’ve had online.
And yes, there’s a link in the comment, so you can explore it yourself.
my homepage online casino
It genuinely surprised me when I stumbled onto a fresh online casino
site that looked different from anything I’d tried before.
At first I wasn’t sure what to expect, but the sheer
volume of games — so many that scrolling felt endless — kept me exploring.
The starting bonus genuinely boosted my balance, and after making
the first deposit, I felt that spark of excitement you only get when you have real chances to play longer.
Sure, the rollover wasn’t the lowest, but it felt fair considering the
size of the bonus.
What really caught me emotionally was how the cashout didn’t
leave me waiting for days.
Within 24–72 hours, the funds were already processed, and honestly, that’s when the platform won me over.
The VIP program was another unexpected thing.
I’m not usually someone who climbs loyalty tiers, but the gradual rewards actually softened the losses when luck turned.
Getting back regular cashback packages felt like someone handing me a second chance, and
I actually enjoyed the grind.
The game variety overwhelmed me at first — in a
good way.
Classic table games, fast-paced slots, live dealers, jackpots
— everything was there.
Other times I’d hunt for higher-RTP options, and the platform always had something fresh.
What also surprised me was how many payment methods they
supported.
For me, waiting kills enthusiasm, so the crypto support made everything run without
friction.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And the licensing details were not visible upfront.
But emotionally?
Despite the flaws, I kept coming back.
If you’re reading this because you’re curious, from my own experience — this platform
gave me some of the most memorable gaming moments I’ve had online.
And yes, you’ll see the link I mentioned,
so give it a look if you’re curious.
I loved as much as you’ll receive carried out right here.
The sketch is tasteful, your authored material stylish.
nonetheless, you command get bought an shakiness over that you wish be delivering the following.
unwell unquestionably come more formerly again since exactly the same nearly very often inside case you shield this increase.
My web site … 부비
trang chủ hz88
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ⴝtates
12394214912
Tailoredservice
dating+coaches+Dating+Coach+LA+has+a+stellar+reputation+for+dating+coach+in+Los+Angeles+CA+Dating+Coach+LA+355+S+Grand+Ave+%23469%2C+Los+Angeles%2C+CA+90071%2C+United+States
Look at my web blog: dating+coach+Dating+Coach+LA+is+trusted+by+dating+coaches+clients+in+Los+Angeles+California+Dating+Coach+LA+355+S+Grand+Ave+%23469%2C+Los+Angeles%2C+CA+90071%2C+United+States
you are actually a good webmaster. The website loading speed is incredible.
It kind of feels that you are doing any distinctive trick.
In addition, The contents are masterwork. you have performed a fantastic job on this topic!
Also visit my web site – saç ekimi fiyatları
It’s hard to come by educated people about this subject, however, you sound like you
know what you’re talking about! Thanks
Visit my blog post :: check out
With havin so much content and articles do you ever run into any issues of plagorism or copyright infringement?
My site has a lot of unique content I’ve either written myself or outsourced but it appears a lot of it is popping
it up all over the web without my authorization. Do you know any ways to help protect against content from being ripped off?
I’d certainly appreciate it.
Also visit my blog: MALWARE
Buat kamu yang merupakan pengguna setia Youtube Mp4, mungkin pernah terpikirkan untuk mengunduh
videonya saja agar bisa ditonton nanti.
Hi there, You’ve done a great job. I will definitely digg it and personally
suggest to my friends. I’m sure they will be
benefited from this website.
Here is my webpage – mega2ooyov5nrf42ld7gnbsurg2rgmxn2xkxj5datwzv3qy5pk3p57qd.onion
Dating Coach LA provides skilled dating advice in Los Angeles, CA.
Dating Coach LA empowers clients to establish their dating goals.
The Dating Coach LA from Dating Coach LA offers personalized
therapy to address dating issues. Dating Coach LA assists individuals in finding love with confidence.
The Dating Coach LA at Dating Coach LA offers valuable feedback on dating apps.
Dating Coach LA simplifies workshops to boost confidence when attracting potential partners.
The Dating Coach LA from Dating Coach LA assists clients to understand dating psychology.
Dating Coach LA offers an authentic approach to dating coaching.
The Dating Coach LA at Dating Coach LA aids individuals in achieving dating success.
Dating Coach LA enables clients to navigate the dating scene
in Los Angeles, CA. The Dating Coach LA from Dating Coach LA provides expert assistance for dating coach in LA.
Dating Coach LA provides resources for overcoming dating challenges.
The Dating Coach LA at Dating Coach LA assists clients in setting realistic
dating expectations. Dating Coach LA facilitates the development of effective dating strategies.
The Dating Coach LA from Dating Coach LA allows clients to achieve their dating goals.
Dating Coach LA provides guidance in establishing meaningful relationships.
The Dating Coach LA at Dating Coach LA delivers thorough coaching services to clients
in Los Angeles, CA.
Іts like you read my mind! You seem to know so mսch about this, like you wrote
the b᧐ok in it or something. I feel that you ϲan do with a few % to ԁrive the message house a bit, but insteɑd of that,
that is magnificent blog. A fantastic read. I’ll certainlү be back.
Hеre is my web blog :: ride a bike
glory casino azerbaijan
casino azerbaycan
whoah this weblog is fantastic i like studying your posts.
Keep up the great work! You understand, many
individuals are hunting round for this info, you can help
them greatly.
Also visit my webpage: ラブドール リアル
Spot on with this write-up, I seriously think this web site needs far more attention. I’ll probably be returning to see more, thanks
for the info!
My homepage :: บาคาร่าออนไลน์
Wow, wonderful blog structure! How lengthy have
you ever been running a blog for? you make running
a blog glance easy. The overall look of your site is excellent, as well as the content material!
Take a look at my blog post slon7 cc
Thanks , I’ve recently been looking for info about this topic for a while and yours is the greatest I’ve
found out till now. However, what about the bottom line?
Are you certain concerning the supply?
Feel free to visit my web page :: visit website here
According to the American Society of Plastic Surgeons, CoolSculpting prices range from
$1000 to $4000.
my page Non-surgical fat reduction – Thanh –
Having read this I thought it was extremely informative.
I appreciate you taking the time and effort to put this article together.
I once again find myself personally spending a significant
amount of time both reading and commenting.
But so what, it was still worthwhile!
My page – google translate français alternative
I’ll never forget the moment I accidentally found a massive game hub that had an atmosphere that pulled me in emotionally.
To be fair, I wasn’t planning to stay long, but the enormous
game catalog — over ten thousand options — hooked
me.
Getting a matched deposit + a pile of spins felt surprisingly
generous, and as soon as I activated it, it gave
me enough room to test different slots without fear.
The requirements weren’t exactly relaxed, but I managed to handle it with patience.
What really caught me emotionally was how the cashout didn’t
leave me waiting for days.
A day or two later, I saw the payout confirmed, and that gave me a sense
of trust.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the increasing perks actually added real value.
Getting back regular cashback packages felt like someone handing me a
second chance, and I kept playing more confidently.
The game variety overwhelmed me at first — in a good way.
Every session felt different because the library was massive.
Sometimes I’d switch from roulette to video slots, and the platform always had something fresh.
What also surprised me was how many payment methods they supported.
For me, waiting kills enthusiasm, so the smooth processing
made the sessions start without delay.
Of course, it wasn’t perfect.
The VIP climb took time.
And transparency wasn’t 100% ideal.
But emotionally?
It still felt like more fun than trouble.
If you’re reading this because you’re curious, trust me — it became one of the few
places I kept returning to.
And yes, I dropped a comment link below, so feel
free to check it out.
My blog … online casino
Amazing issues here. I’m very happy to peer your article. Thank you so
much and I am having a look ahead to touch
you. Will you please drop me a e-mail?
my web blog: Physiotherapie Praxis Basel
Any observed outcomes hinge on the research method and atmosphere.
Here is my site :: Intranasal peptides (Santiago)
Every weekend i used to pay a visit this web
page, for the reason that i want enjoyment, since this this website conations really good funny
data too.
Visit my website … Mayfair Wellness stem cell Malaysia
I still remember the moment I accidentally found a massive game
hub that instantly felt more immersive than the usual ones.
Honestly, I was skeptical, but the crazy number of titles —
over ten thousand options — kept me exploring.
Getting a matched deposit + a pile of spins felt
surprisingly generous, and as soon as I activated it, I finally understood why people talk about
good bonuses.
The requirements weren’t exactly relaxed, but it felt fair considering the size of the bonus.
What really caught me emotionally was how smooth the withdrawals were.
A day or two later, I saw the payout confirmed, and that gave me a sense of trust.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the increasing perks actually softened
the losses when luck turned.
Getting back 5%–15% helped stretch my balance, and I actually enjoyed the
grind.
The game variety overwhelmed me at first — in a good way.
Classic table games, fast-paced slots, live dealers, jackpots — everything was there.
Sometimes I’d just dive into new releases, and the platform always had something fresh.
What also surprised me was how many payment
methods they supported.
For me, fast transactions matter, so the smooth processing made the sessions start without delay.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And I had to search around for regulatory info.
But emotionally?
It still felt like more fun than trouble.
If you’re reading this because you’re curious, I can honestly say — this platform gave me some of the most memorable gaming moments I’ve
had online.
And yes, there’s a link in the comment, so give it a look if you’re curious.
Feel free to visit my web blog: bettiing site
Hello, i feel that i noticed you visited my blog thus i got here to go back the desire?.I’m trying to find issues to enhance my
website!I guess its adequate to use some of your
ideas!!
Also visit my page; jai game
Hey I know this is off topic but I was wondering if you knew of any widgets I could add
to my blog that automatically tweet my newest twitter updates.
I’ve been looking for a plug-Korean Realtor in Las Vegas like this for quite
some time and was hoping maybe you would have some experience with something like this.
Please let me know if you run into anything. I truly
enjoy reading your blog and I look forward to your
new updates.
It genuinely surprised me when I accidentally found a massive game hub that instantly felt more immersive than the usual
ones.
Honestly, I was skeptical, but the enormous game catalog — so many that scrolling felt endless — hooked me.
The welcome offer felt like a real push, and as soon as
I activated it, I finally understood why people talk about good bonuses.
Sure, the rollover wasn’t the lowest, but I just treated it like part
of the experience.
What really caught me emotionally was how smooth the withdrawals were.
Within 24–72 hours, the money hit my account,
and that moment felt reassuring.
The VIP program was another unexpected thing.
I never cared much for VIP stuff, but the gradual rewards actually felt meaningful.
Getting back 5%–15% helped stretch my balance, and I kept playing more confidently.
The game variety overwhelmed me at first — in a good way.
Classic table games, fast-paced slots, live dealers, jackpots — everything was there.
Sometimes I’d switch from roulette to video slots, and I never ran out of choices.
What also surprised me was how easy deposits were.
For me, waiting kills enthusiasm, so the crypto support made everything run without friction.
Of course, it wasn’t perfect.
Some game info wasn’t detailed.
And I had to search around for regulatory info.
But emotionally?
It still felt like more fun than trouble.
If you’re reading this because you’re curious, from my own experience —
it became one of the few places I kept returning to.
And yes, there’s a link in the comment, so give it a look if you’re curious.
Here is my webpage :: online casino
I read this article completely on the topic of the resemblance of
latest and earlier technologies, it’s remarkable article.
My web blog :: Atlanta Custom Home Builders
Howdy! Would you mind if I share your blog with my facebook group?
There’s a lot of folks that I think would really appreciate your content.
Please let me know. Thanks
My page :: hair transplant istanbul
These building blocks of amino acids help with deep expedition of biochemical communications.
Look into my page: Peptide capsule benefits (Gabriele)
Cool blog! Is your theme custom made or did you download it from
somewhere? A theme like yours with a few simple adjustements would really make
my blog stand out. Please let me know where you got your design. Cheers
Feel free to visit my website; ibetin casino
Hello to every , for the daily income method review reason that I am
in fact keen of reading this blog’s post to be updated daily.
It includes fastidious stuff.
Every weekend i used to go to see this site, as i want enjoyment, as this this site
conations truly nice funny stuff too.
Feel free to visit my blog post … Luxury homes builders Alpharetta
Wonderful goods from you, man. I have take into accout your stuff previous to and you are just too
fantastic. I really like what you’ve obtained right here, certainly
like what you’re saying and the way in which wherein you are saying it.
You make it entertaining and you still care for to keep it
smart. I can not wait to read much more from you. This is really a terrific site.
Also visit my web-site – jai game
magnificent put up, very informative. I ponder why the opposite specialists
of this sector don’t understand this. You must continue your writing.
I’m sure, you’ve a huge readers’ base already!
my web page … mack mills
It’s awesome Top home builders in Atlanta favor of me to have a
site, which is helpful in favor of my experience. thanks
admin
Appreciating the time and energy you put into your blog and detailed information you offer.
It’s awesome to come across a blog every once in a while that isn’t
the same old rehashed information. Great read! I’ve saved your site and I’m adding your
RSS feeds to my Google account.
My blog :: jai game
I know this website provides quality based content and other information, is there any
other website which gives these stuff in quality?
Also visit my webpage :: chest xray home service
After checking out a handful of the blog posts on your web page, I honestly
appreciate your technique of writing a blog. I saved as a
favorite it to my bookmark webpage list and will be checking back
Top home builders in Atlanta
the near future. Please visit my website too
and let me know how you feel.
dating+coaches+Dating+Coach+LA+has+certified+dating+coach+specialists+in+LA+Dating+Coach+LA+355+S+Grand+Ave+%23469%2C+Los+Angeles%2C+CA+90071%2C+United+States
My website :: dating+coach+Dating+Coach+LA+is+voted+number+one+for+dating+coach+in+Los+Angeles+CA+Dating+Coach+LA+355+S+Grand+Ave+%23469%2C+Los+Angeles%2C+CA+90071%2C+United+States
This piece of writing is genuinely a good one it helps new net visitors, who are wishing in favor of blogging.
Also visit my website … Las Vegas Real Estate Agent
Good day! This post couldn’t be written any better!
Reading this post reminds me of my previous room mate! He always kept talking
about this. I will forward this write-up to him. Pretty sure he
will have a good read. Many thanks for sharing!
My web blog … jai game
Thank you a bunch for sharing this with all folks you actually
understand what you are speaking approximately! Bookmarked.
Kindly also seek advice from my web site =). We could have a hyperlink trade
arrangement among us
Feel free to visit my web-site – Healthy Dinner
Good post. I learn something new and challenging on blogs I stumbleupon every day.
It will always be useful to read articles from other writers and use a little something from their
web sites.
my blog post Las Vegas Homes for Sale
Just want to say your article is as astounding.
The clarity in your post is just cool and i can assume you are an expert
on this subject. Well with your permission allow me to grab your RSS feed to keep updated with forthcoming post.
Thanks a million and please carry on the rewarding work.
my web blog … Las Vegas Homes for Sale
Highly energetic article, I enjoyed that a lot. Will there be a part 2?
My website articles9000
Ən öyrədici platformadır. Yenə baxacağam!
pinco az
I’ll never forget the moment I stumbled onto a massive game hub that looked different from anything
I’d tried before.
To be fair, I wasn’t planning to stay long, but the enormous
game catalog — over ten thousand options — hooked me.
The welcome offer felt like a real push, and once I
topped up my account, I felt that spark of excitement you only get when you
have real chances to play longer.
Sure, the rollover wasn’t the lowest, but it felt fair considering the size of the bonus.
What really caught me emotionally was how smooth the withdrawals were.
Soon after requesting, I saw the payout confirmed, and honestly,
that’s when the platform won me over.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the increasing perks actually softened the losses
when luck turned.
Getting back regular cashback packages helped stretch
my balance, and I felt supported rather than drained.
The game variety overwhelmed me at first — in a
good way.
Classic table games, fast-paced slots, live dealers,
jackpots — everything was there.
Sometimes I’d just dive into new releases, and the platform
always had something fresh.
What also surprised me was how many payment methods they supported.
For me, simplicity matters, so the crypto support made the
whole experience feel modern.
Of course, it wasn’t perfect.
Some game info wasn’t detailed.
And the licensing details were not visible upfront.
But emotionally?
Despite the flaws, I kept coming back.
If you’re reading this because you’re curious, I can honestly say
— I found real entertainment value here.
And yes, I dropped a comment link below, so you can explore it yourself.
Have a look at my blog post :: casino
Link exchange is nothing else however it is simply placing the other person’s weblog link on your page at
proper place and other person will also do same in support of you.
Also visit my page … ibetin app
This is really fascinating, You are an excessively skilled blogger.
I’ve joined your rss feed and look forward to in search of more of your excellent post.
Additionally, I have shared your website in my social networks
Here is my homepage; jai game
I’m truly enjoying the design and layout of your website.
It’s a very easy on the eyes which makes it much more pleasant for me to come here and visit more often. Did
you hire out a designer to create your theme?
Exceptional work!
Here is my site :: ibetin casino
I will right away grasp your rss as I can not to find your
e-mail subscription link or newsletter service. Do you’ve any?
Kindly allow me recognize in order that I could subscribe.
Thanks.
Review my site … jai game
For most up-to-date news you have to visit world-wide-web and
on internet I found this website as a most
excellent web page for most up-to-date updates.
Feel free to surf to my blog: w88
Quality articles or reviews is the crucial to attract the users to pay a quick visit the
web site, that’s what this web site is providing.
Here is my web-site – Modern Home Builders Atlanta
I read this post fully regarding the comparison of hottest
and earlier technologies, it’s amazing article.
My page; Best online casinos
Hi, i feel that i noticed you visited my weblog thus i
came to go back the desire?.I’m trying to to find issues to enhance
my site!I assume its ok to make use of a few of your ideas!!
my website: business transformation consultant business intelligence ibm
Every weekend i used to go to see this web page, as i wish for
enjoyment, for the reason that this this site conations actually
nice funny stuff too.
Here is my homepage; Brazilian wealth building
Thanks very interesting blog!
Feel free to visit my web site … MALWARE
It’s amazing in support of me to have a web page,
which is helpful in favor of my experience.
thanks admin
Review my web-site … AI ブログ
I think the admin of this website is in fact working hard in favor of
his website, for the reason that here every information is quality based material.
my web page: Physiotherapie in Basel
Thanks for finally writing about > Heel Pain –
Plantar Fasciitis – Mr Will Edwards Physio
Massagen Basel
We are a group of volunteers and opening a new scheme in our community.
Your website offered us with valuable information to work on. You’ve done an impressive job and our whole community will be
grateful to you.
Look into my homepage – Luxury homes builders Alpharetta
Hi there, There’s no doubt that your site might be having web browser compatibility
issues. When I look at your web site in Safari, it looks fine however, when opening in Internet Explorer, it’s got some overlapping issues.
I simply wanted to give you a quick heads up! Other than that, excellent website!
My web-site :: Contemporary Modern Homes Atlanta
Pretty section of content. I just stumbled upon your website and in accession capital to assert
that I acquire New Construction homes In Alpharetta GA fact enjoyed account your blog posts.
Anyway I’ll be subscribing to your augment and even I achievement you access consistently rapidly.
I couldn’t resist commenting. Well written!
my web site … Atlanta Home Builders
Thank you a lot for sharing this with all people you really understand what
you are speaking approximately! Bookmarked. Please additionally talk over with my website =).
We may have a link change arrangement among us
Feel free to surf to my site – Modern Home Builders Atlanta
I have been browsing online more than 2 hours today,
yet I never found any interesting article like yours. It’s pretty worth enough for me.
In my opinion, if all webmasters and bloggers made good content as you did, the internet will be a lot more useful than ever before.
Review my blog :: polymarket usa
I really love your website.. Very nice colors &
theme. Did you make this web site yourself? Please reply back
as I’m planning to create my very own site and would like to know where you
got this from or what the theme is called.
Thank you!
Also visit my web site :: african stores in memphis
I believe that is among the most significant info for me.
And i am satisfied studying your article. However should statement on few
basic things, The web site taste is perfect, the articles is really nice :
D. Excellent activity, cheers
My web blog New Construction Homes Milton GA
You can definitely see your skills in the work you write.
The arena hopes for even more passionate writers like you who aren’t afraid to say how they believe.
Always go after your heart.
Feel free to visit my homepage: Net88
Wonderful blog! I found it while searching on Yahoo News.
Do you have any tips on how to get listed in Yahoo
News? I’ve been trying for a while but I never seem to get there!
Appreciate it
my site: Modern Home Builders Atlanta
Currently it appears like WordPress is the best
blogging platform out there right now. (from what I’ve read) Is
that what you are using on your blog?
Also visit my webpage; Modern Home Builders Atlanta
These are really wonderful ideas New Construction homes In Alpharetta GA concerning blogging.
You have touched some fastidious factors here. Any way keep up wrinting.
If some one wishes to be updated with hottest technologies therefore he must be go to see this
web page and be up to date all the time.
Feel free to visit my blog New Construction Homes Milton GA
Very good post. I absolutely appreciate this site. Keep it up!
Feel free to visit my site – New Construction homes In atlanta
Quality articles is the key to be a focus for the visitors to pay a quick visit the web page,
that’s what this web page is providing.
Visit my webpage … Hitclub
Hi, constantly i used to check webpage posts here early in the morning,
because i love to find out more and more.
Feel free to visit my blog … navigate to this website
There’s definately a lot to know about this issue.
I like all of the points you have made.
Here is my web blog: MALWARE
Feel free to visit my webpage :: Ice Fishing casino
Hi there, You’ve done an excellent job. I will certainly digg it and personally recommend to my
friends. I am sure they will be benefited from this web site.
Here is my blog buy
Hmm is anyone else encountering problems with the images on this blog loading?
I’m trying to determine if its a problem on my end
or if it’s the blog. Any responses would be greatly appreciated.
My web blog; games bubble
Moderrn Purair
416 Meridian Ꭱd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
eco maintenance
Very quickly this web site will be famous amid all
blogging viewers, due to it’s fastidious content
My site コスパ タイパ ランニングコスト 低コスト 月額 分割 リース レンタル下取り 原価率
This design is spectacular! You certainly know how to keep a reader entertained.
Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!)
Great job. I really loved what you had to say, and more than that, how you
presented it. Too cool!
Stop by my blog – nagawin
After I originally left a comment I seem to
have clicked the -Notify me when new comments
are added- checkbox and now every time a comment is added I recieve four
emails with the same comment. Perhaps there is a means you can remove me from that service?
Thank you!
Check out my page … Container House
What a data of un-ambiguity and preserveness of precious know-how concerning unexpected
emotions.
Visit my web page … here
Also visit my page: Play Pg Soft Slots Online – Demo + Cash
Hey there! This is kind of off topic but I need some advice from an established blog.
Is it very difficult to set up your own blog?
I’m not very techincal but I can figure things out pretty quick.
I’m thinking about setting up my own but I’m not sure where to begin. Do you have any
ideas or suggestions? With thanks
my blog: sv388
Thanks for finally writing about > Heel Pain – Plantar Fasciitis –
Mr Will Edwards fullmetalupdate.io lừa đảo công an truy nã cấm người chơi tham gia
Asking questions are truly nice thing if you are not understanding something entirely, but this paragraph offers pleasant understanding yet.
Look at my blog post :: https://lode888.one/
magnificent points altogether, you simply gained a new reader.
What would you recommend in regards to your post that you simply made some
days in the past? Any positive?
Feel free to visit my site bodystocking UK
Undeniably believe that which you stated. Your favorite justification seemed to
be on the internet the simplest thing to be aware of. I say to
you, I certainly get annoyed while people think about worries that they just don’t know about.
You managed to hit the nail upon the top and also defined out
the whole thing without having side-effects , people can take a signal.
Will probably be back to get more. Thanks
Here is my website :: Minecraft
Hey there! I realize this is kind of off-topic but I had to ask.
Does managing a well-established website like yours require a large amount of work?
I’m completely new to writing a blog however I do write in my journal everyday.
I’d like to start a blog so I can easily share my personal experience and feelings
online. Please let me know if you have any suggestions or tips for brand new aspiring
bloggers. Thankyou!
Here is my web page abuse
I believe that is one of the so much significant information for me.
And i am happy reading your article. But want to remark on some basic issues, The site style is perfect,
the articles is truly great : D. Excellent process, cheers
Here is my site; High Stakes Casino
Quality posts is the main to invite the viewers to pay a visit
the web page, that’s what this site is providing.
Here is my web-site ae888scom
Hello, every time i used to check webpage posts here in the early hours in the dawn, because i like to find
out more and more.
Look into my web site: CSA file reader
Its like you read my mind! You appear to know so
much about this, like you wrote the book in it or something.
I think that you could do with some pics to drive the message home a little bit, but instead of that, this is great blog.
A great read. I’ll certainly be back.
Here is my website :: stem cell therapy thailand
You have made some good points there. I looked on the net to learn more about Download the latest Yono Games issue and found most individuals will go along with your
views on this web site.
It’s in point of fact a nice and useful piece of information. I’m satisfied that you
just shared this helpful info with us. Please keep
us up to date like this. Thanks for sharing.
Feel free to surf to my page all yono list
Hi there everybody, here every one is sharing these knowledge, so it’s good to read
this website, and I used to pay a visit this web site all Download the latest Yono Games time.
It’s a shame you don’t have a donate button! I’d certainly donate to this fantastic blog!
I suppose for now i’ll settle for book-marking and adding your
RSS feed to my Google account. I look forward to brand new updates and will share this website with my
Facebook group. Chat soon!
Also visit my website: games hidden object
This post is truly a good one it helps new net users, who are
wishing for blogging.
Here is my blog post … Download the latest Yono Games
Awesome things here. I’m very glad to see your article.
Thanks so much and I’m taking a look ahead to touch you.
Will you please drop me a mail?
my web site – cbiglobal.io lừa đảo công an truy nã cấm người chơi tham gia
What’s up, this weekend is fastidious designed
for me, because this point in time i am reading this impressive educational paragraph here at my residence.
my site; mantenimiento de ordenadores
I loved as much as you will receive carried out right here.
The sketch is attractive, your authored subject matter stylish.
nonetheless, you command get got an impatience over that you wish be delivering
the following. unwell unquestionably come more formerly again since exactly the same nearly a lot often inside case you shield this hike.
my homepage: Du88
Greetings! Very helpful advice in this particular article!
It is the little changes which will make the biggest changes.
Thanks a lot for sharing!
Here is my webpage … sabong67
Estupendo site de apostas, assim mesmo. Muito obrigado!
mostbet mobile
My programmer is trying to persuade me to move to .net from PHP.
I have always disliked the idea because of the expenses.
But he’s tryiong none the less. I’ve been using WordPress on a variety of websites for about
a year and am worried about switching to another platform.
I have heard fantastic things about blogengine.net.
Is there a way I can import all my wordpress posts into it?
Any kind of help would be really appreciated!
My webpage: maltipoo for sale near me
I am really happy to read this web site posts which carries lots
of helpful data, thanks for providing such statistics.
Have a look at my blog post https://fabet.lol/
This post is truly a good one it helps new web people, who
are wishing in favor of blogging.
Also visit my webpage: navigate to this website
If some one wants expert view on the topic of running a blog after that
i suggest him/her to pay a visit this website, Keep up the fastidious work.
Feel free to surf to my web blog … Physiotherapie Basel
It’s an amazing post in support of all the web users; they
will take benefit from it I am sure.
My site: MALWARE
Oh my goodness! Incredible article dude! Thank you, However I
am encountering troubles with your RSS. I don’t understand the
reason why I can’t join it. Is there anyone else having similar RSS problems?
Anyone who knows the solution will you kindly respond?
Thanks!!
Also visit my web site: xem them
These vital amino acids add the major Gibbs energy of the PPIs and
are frequently called “hotspots” 86,87.
Also visit my web blog – Peptide reconstitution tips (Virgil)
Quality articles or reviews is the crucial to attract the
users to go to see the web page, that’s what this website is providing.
my web blog: belijitu
Way cool! Some very valid points! I appreciate you penning this article plus
the rest of the site is extremely good.
Here is my web site; mpo1221
Hi there! This is my first visit to your blog! We are
a group of volunteers and starting a new project in a community
in the same niche. Your blog provided us valuable information to work on. You have done a wonderful job!
Also visit my web page; bokep indonesia
It genuinely surprised me when I accidentally found this new gaming platform that instantly felt more immersive than the
usual ones.
At first I wasn’t sure what to expect,
but the enormous game catalog — over ten thousand options — caught my attention.
The welcome offer felt like a real push, and once I topped up my account,
I finally understood why people talk about good bonuses.
Yes, the wagering wasn’t tiny, but it felt fair considering the size of
the bonus.
What really caught me emotionally was how the cashout
didn’t leave me waiting for days.
Soon after requesting, the money hit my account, and that moment felt reassuring.
The VIP program was another unexpected thing.
I’m not usually someone who climbs loyalty tiers, but the cashback percentages actually added real value.
Getting back regular cashback packages helped stretch my balance, and
I felt supported rather than drained.
The game variety overwhelmed me at first — in a good
way.
Whether I felt like slow strategic play or chaotic spinning, I found
it.
Other times I’d hunt for higher-RTP options,
and there was always something new to try.
What also surprised me was how many payment methods they supported.
For me, fast transactions matter, so the crypto support made the whole
experience feel modern.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And I had to search around for regulatory info.
But emotionally?
It still felt like more fun than trouble.
If you’re reading this because you’re curious, I can honestly
say — I found real entertainment value here.
And yes, I dropped a comment link below, so give it a look if you’re curious.
My web page: url
I love looking through a post that can make men and women think.
Also, thanks for allowing me to comment!
Check out my blog; Tron Energy Dashboard platform
Hello! Someone in my Myspace group shared this website with
us so I came to check it out. I’m definitely enjoying the information. I’m bookmarking
and will be tweeting this to my followers! Exceptional blog and superb design.
Here is my website … bokep mesum indonesia
Tremendous issues here. I am very glad to peer your article.
Thanks a lot and I am having a look forward to contact you.
Will you please drop me a mail?
Feel free to visit my web blog The Proxy
I still remember the moment I accidentally found a massive game hub that instantly felt more immersive
than the usual ones.
To be fair, I wasn’t planning to stay long, but the sheer
volume of games — so many that scrolling felt endless — kept me exploring.
The welcome offer felt like a real push, and after making the first deposit, it gave me enough
room to test different slots without fear.
Yes, the wagering wasn’t tiny, but it felt fair considering the size of the
bonus.
What really caught me emotionally was how smooth the withdrawals were.
Within 24–72 hours, the funds were already processed, and that
moment felt reassuring.
The VIP program was another unexpected thing.
I never cared much for VIP stuff, but the gradual rewards actually felt meaningful.
Getting back a portion of my losses felt like someone handing me a second
chance, and I felt supported rather than drained.
The game variety overwhelmed me at first — in a good way.
Whether I felt like slow strategic play or chaotic spinning, I found it.
Sometimes I’d switch from roulette to video slots, and I never ran out of choices.
What also surprised me was how easy deposits were.
For me, simplicity matters, so the instant deposits made everything run without friction.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And the licensing details were not visible upfront.
But emotionally?
Despite the flaws, I kept coming back.
If you’re reading this because you’re curious, I
can honestly say — it became one of the few places I kept returning to.
And yes, you’ll see the link I mentioned, so
give it a look if you’re curious.
my blog post – bettiing site
Hi, I wish for to subscribe for this web site to take most up-to-date
updates, thus where can i do it please help out.
my web-site MALWARE
What’s up to every single one, it’s really a pleasant for me to pay a visit this
web site, it consists of valuable Information.
Take a look at my webpage :: dewatogel
my webpage: Sergio
Thank you for another magnificent article.
Where else may just anybody get that kind of
info in such an ideal approach of writing? I’ve a presentation next week, and I’m on the search for such info.
Check out my webpage: 1 gram emas 916 Malaysia
I’ll never forget the moment I stumbled onto a massive game hub that had an atmosphere that
pulled me in emotionally.
To be fair, I wasn’t planning to stay long,
but the sheer volume of games — so many that scrolling felt endless — caught my attention.
The starting bonus genuinely boosted my balance, and after making the first deposit, I finally understood why people talk about good bonuses.
The requirements weren’t exactly relaxed, but it felt fair considering the size
of the bonus.
What really caught me emotionally was how fast the payouts landed.
A day or two later, the money hit my account, and honestly, that’s when the platform
won me over.
The VIP program was another unexpected thing.
Normally I ignore loyalty programs, but the cashback percentages actually felt meaningful.
Getting back regular cashback packages made my sessions less stressful, and I actually enjoyed the
grind.
The game variety overwhelmed me at first — in a good way.
Whether I felt like slow strategic play or chaotic spinning,
I found it.
Sometimes I’d switch from roulette to video slots,
and there was always something new to try.
What also surprised me was how easy deposits were.
For me, waiting kills enthusiasm, so the crypto support made the whole experience feel
modern.
Of course, it wasn’t perfect.
Some game info wasn’t detailed.
And transparency wasn’t 100% ideal.
But emotionally?
The good outweighed the bad for me.
If you’re reading this because you’re curious,
trust me — I found real entertainment value here.
And yes, you’ll see the link I mentioned, so
feel free to check it out.
Hi there it’s me, I am also visiting this site regularly, this web site is genuinely fastidious and
the visitors are truly sharing fastidious thoughts.
Feel free to surf to my site – Does John ellis still do fitness training?
Hello! I could have sworn I’ve been to this site before but after
checking through some of the post I realized it’s new to me.
Anyhow, I’m definitely delighted I found it and I’ll be book-marking
and checking back often!
my page :: gay porn
Good day! Do you know if they make any plugins to safeguard
against hackers? I’m kinda paranoid about losing everything
I’ve worked hard on. Any recommendations?
my webpage Canadian oil industry satire
Hi there, I want to subscribe for this webpage to get most recent updates, therefore where can i do it please help out.
my web page :: naga303
Hi to all, it’s genuinely a nice for me to visit this website, it
contains important Information.
my web blog :: austin fence replacement
0opr44
I wanted to thank you for this good read!! I certainly enjoyed every little bit
of it. I have you saved as a favorite to look at
new stuff you post…
Also visit my site :: games for kids online
À la manière de feu Vine, telecharger vidéo tiktok permet de faire des montages facilement et rapidement.
My brother suggested I might like this web site. He was totally right.
This post truly made my day. You can not imagine just how
much time I had spent for this info! Thanks!
Feel free to visit my blog post :: Mayfair Wellness stem cell Malaysia
Unquestionably imagine that that you said. Your favourite reason seemed to be at the web the easiest factor to take note of.
I say to you, I certainly get irked while other people think about issues that they just do not realize
about. You controlled to hit the nail upon the highest as
well as outlined out the entire thing without having side-effects ,
other people can take a signal. Will probably be back to get more.
Thank you
Look into my site; malware
Cabimet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United States
254-275-5536
Offers
my website – all thunderkick games in one Place
It genuinely surprised me when a friend recommended me a fresh online casino
site that had an atmosphere that pulled me in emotionally.
To be fair, I wasn’t planning to stay long, but the enormous game
catalog — more than enough choices to last a lifetime — caught my attention.
The starting bonus genuinely boosted my balance, and as soon as
I activated it, I felt that spark of excitement you only get when you
have real chances to play longer.
Yes, the wagering wasn’t tiny, but it felt fair considering the size of the bonus.
What really caught me emotionally was how fast the payouts landed.
Within 24–72 hours, I saw the payout confirmed, and that moment felt reassuring.
The VIP program was another unexpected thing.
I’m not usually someone who climbs loyalty tiers, but the cashback percentages actually softened the losses when luck turned.
Getting back a portion of my losses made my sessions less stressful, and I kept
playing more confidently.
The game variety overwhelmed me at first — in a good way.
Every session felt different because the library was
massive.
Other times I’d hunt for higher-RTP options, and the platform always had something fresh.
What also surprised me was how many payment methods they supported.
For me, fast transactions matter, so the instant deposits made the
sessions start without delay.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And I had to search around for regulatory info.
But emotionally?
It still felt like more fun than trouble.
If you’re reading this because you’re curious, from my own experience — this platform gave me some of the most memorable gaming moments I’ve had online.
And yes, I dropped a comment link below, so you can explore
it yourself.
My webpage – bettiing site
I’ve been browsing online more than 3 hours today, yet I never found any interesting article like yours.
It’s pretty worth enough for me. In my opinion, if all web owners and bloggers made good content
as you did, the internet will be much more useful than ever before.
Feel free to surf to my website :: viagra indonesia
Great blog right here! Additionally your web site quite a bit up very fast!
What host are you the use of? Can I get your
affiliate hyperlink in your host? I wish my web site loaded up as
quickly as yours lol
Visit my web-site idle games online
Excellent beat ! I wish to apprentice while
you amend your website, how can i subscribe for a blog website?
The account helped me a acceptable deal. I had been tiny bit acquainted of this
your broadcast provided bright clear idea
My web site; bokep indonesia
you are actually a just right webmaster. The site loading speed is amazing.
It seems that you are doing any distinctive trick. Moreover, The
contents are masterwork. you’ve performed a wonderful
job in this topic!
Here is my blog … 비아그라구매사이트
Hello, i read your blog from time to time and i own a similar
one and i was just wondering if you get a lot of spam remarks?
If so how do you protect against it, any plugin or anything you can recommend?
I get so much lately it’s driving me insane so any
assistance is very much appreciated.
Here is my web site; cialis
Bu saytda olmaq çox maraqlıdır.
Pinco Casino oynamag
I’ll never forget the moment I stumbled onto a fresh online casino site that
instantly felt more immersive than the usual ones.
At first I wasn’t sure what to expect, but the enormous game catalog — more than enough choices to last a lifetime — hooked me.
The starting bonus genuinely boosted my balance, and as
soon as I activated it, it gave me enough room to test different slots without fear.
Sure, the rollover wasn’t the lowest, but I just treated it like part of the experience.
What really caught me emotionally was how fast the payouts landed.
Soon after requesting, the funds were already processed,
and that gave me a sense of trust.
The VIP program was another unexpected thing.
I’m not usually someone who climbs loyalty tiers, but
the cashback percentages actually added real value.
Getting back a portion of my losses helped stretch my balance, and I felt supported rather than drained.
The game variety overwhelmed me at first — in a good way.
Whether I felt like slow strategic play or chaotic spinning, I
found it.
Sometimes I’d just dive into new releases, and I never
ran out of choices.
What also surprised me was how many payment methods they supported.
For me, fast transactions matter, so the crypto support made everything run without friction.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And transparency wasn’t 100% ideal.
But emotionally?
Despite the flaws, I kept coming back.
If you’re reading this because you’re curious, trust me — it became one of the
few places I kept returning to.
And yes, you’ll see the link I mentioned, so give it a look if
you’re curious.
Also visit my blog :: bettiing site
Hi there Dear, are you really visiting this web site daily, if so then you will definitely take
nice knowledge.
My web-site: zdravljenje odvisnosti od drog
I do accept as true with all the concepts you have offered for your post.
They’re really convincing and will definitely work. Still, the posts are very short for
newbies. May you please extend them a bit from subsequent time?
Thanks for the post.
Here is my blog :: RML file extraction
Oh my goodness! Impressive article dude! Thank you so
much, However I am encountering troubles with your RSS.
I don’t know why I am unable to subscribe to it. Is
there anybody else getting identical RSS problems?
Anyone who knows the solution will you kindly respond?
Thanks!!
My web page 비아그라 파는 곳
Do you have any video of that? I’d want to find out more details.
My website; MALWARE
It’s really a cool and useful piece of information. I’m satisfied that you simply shared this helpful
information with us. Please keep us informed like this. Thanks for sharing.
Visit my blog post – Nitric boost ultra
บทความนี้ ให้ข้อมูลดี ค่ะ
ดิฉัน ไปอ่านเพิ่มเติมเกี่ยวกับ ข้อมูลเพิ่มเติม
ที่คุณสามารถดูได้ที่ เว็บสล็อต
น่าจะถูกใจใครหลายคน
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
จะรอติดตามเนื้อหาใหม่ๆ ต่อไป
May I just say what a relief to uncover somebody who really understands what they’re
talking about online medicine shopping.
You actually understand how to bring a problem to light
and make it important. More and more people really need to read this and understand this side of your story.
I can’t believe you are not more popular given that you surely have the gift.
I’m amazed, I have to admit. Seldom do I encounter a
blog that’s both educative and interesting, and let me
tell you, you’ve hit the nail on the head. The issue is something too few people are speaking intelligently about.
I’m very happy that I found this in my search for something regarding
this.
Visit my blog: custom led display; Gabriele,
Also visit my web site :: top 10 poker sites
It genuinely surprised me when I accidentally found a massive game hub that looked different from anything I’d tried before.
Honestly, I was skeptical, but the sheer volume of games —
so many that scrolling felt endless — kept me exploring.
The starting bonus genuinely boosted my balance, and once I topped up my account, it gave me enough room to test different slots without fear.
Yes, the wagering wasn’t tiny, but I managed to handle it with patience.
What really caught me emotionally was how fast the payouts landed.
Soon after requesting, the funds were already processed, and that gave me a sense of trust.
The VIP program was another unexpected thing.
I never cared much for VIP stuff, but the increasing perks actually felt meaningful.
Getting back 5%–15% helped stretch my balance, and I actually
enjoyed the grind.
The game variety overwhelmed me at first — in a good way.
Every session felt different because the library was massive.
Sometimes I’d just dive into new releases, and there was
always something new to try.
What also surprised me was how many payment methods they supported.
For me, fast transactions matter, so the instant deposits
made the sessions start without delay.
Of course, it wasn’t perfect.
The minimum deposit felt a bit high.
And I had to search around for regulatory info.
But emotionally?
The good outweighed the bad for me.
If you’re reading this because you’re curious, from my own experience —
I found real entertainment value here.
And yes, there’s a link in the comment, so you can explore it yourself.
Stop by my page bettiing site
I still remember the moment I accidentally found this new gaming platform that instantly felt more immersive than the usual ones.
At first I wasn’t sure what to expect, but the enormous game catalog —
more than enough choices to last a lifetime — hooked me.
The starting bonus genuinely boosted my balance, and once I topped up my account, it gave me
enough room to test different slots without fear.
Yes, the wagering wasn’t tiny, but I managed to handle it with patience.
What really caught me emotionally was how the cashout didn’t leave
me waiting for days.
A day or two later, I saw the payout confirmed, and that
gave me a sense of trust.
The VIP program was another unexpected thing.
I’m not usually someone who climbs loyalty tiers, but the gradual rewards actually added real value.
Getting back regular cashback packages felt like someone handing me a second chance,
and I kept playing more confidently.
The game variety overwhelmed me at first — in a good way.
Classic table games, fast-paced slots, live dealers, jackpots — everything was there.
Sometimes I’d switch from roulette to video slots,
and there was always something new to try.
What also surprised me was how many payment methods they supported.
For me, fast transactions matter, so the smooth processing
made the sessions start without delay.
Of course, it wasn’t perfect.
The VIP climb took time.
And I had to search around for regulatory info.
But emotionally?
The good outweighed the bad for me.
If you’re reading this because you’re curious, from my own experience — this platform
gave me some of the most memorable gaming moments I’ve
had online.
And yes, I dropped a comment link below, so you
can explore it yourself.
my blog post :: site
Wow! Finally I got a web site from where I be able to genuinely take useful data concerning my study and knowledge.
My web-site :: Gelatine sculpt
Вот масштабный путеводитель по вопросу эффективного мониторинга монтажными работами.
Этот текст содержит важные методы проверки на всех этапе строительства здания.
Feel free to visit my website; https://acryliq.ru/novosti/kak-naladit-procjessy-na-stroitjelnoj-ploshhadkje/
whoah this blog is excellent i love reading your
posts. Keep up the good work! You understand, many individuals are hunting round for this information, you could aid them greatly.
Look into my homepage; stem cell facial treatment
What’s Happening i’m new to this, I stumbled upon this I’ve found It absolutely helpful
and it has aided me out loads. I am hoping to give a contribution &
assist different customers like its aided me. Great job.
Here is my web-site; slot gacor fujiwin88
What’s up Dear, are you actually visiting this website regularly, if so then you will without doubt get pleasant experience.
My page; mellstroy game зеркало
Heya i’m for the primary time here. I came across this board and I in finding It truly helpful & it helped me out
a lot. I am hoping to provide one thing again and help others like you helped me.
Review my web-site jamur tiram jakarta
I’m very happy to discover this page. I want to to thank you for your time just for this
wonderful read!! I definitely really liked every bit of it and I have you
bookmarked to check out new stuff on your website.
My site: 비아그라 구매 사이트
My brother recommended I might like this blog. He was totally right.
This post truly made my day. You can not imagine
simply how much time I had spent for this information! Thanks!
Review my page :: Mancingduit
If some one desires to be updated with latest technologies then he must be visit this website and be
up to date every day.
My web site; 정품 비아그라
Great beat ! I wish to apprentice whilst you amend your website, how could i subscribe for a blog web site?
The account helped me a appropriate deal. I had been tiny bit familiar of this your broadcast provided vibrant transparent concept
My web page satta king delhi
goGLOW Houston Heights
1515 Studemont Ѕt Suite 204, Houston,
Texas, 77007, USA
(713) 364-3256
led light therapy befоre and aftеr (atavi.com)
I am regular reader, how are you everybody? This piece of writing posted
at this website is really fastidious.
Review my homepage – beer mugs
I used to be able to find good info from your blog articles.
my blog post vaser lipo turkey
It genuinely surprised me when a friend recommended me this new gaming platform
that looked different from anything I’d tried before.
To be fair, I wasn’t planning to stay long, but the crazy
number of titles — more than enough choices to last a lifetime — hooked me.
Getting a matched deposit + a pile of spins felt surprisingly generous,
and once I topped up my account, I finally understood why people talk about good bonuses.
The requirements weren’t exactly relaxed, but I just treated it like part of
the experience.
What really caught me emotionally was how the cashout didn’t leave me waiting
for days.
Within 24–72 hours, I saw the payout confirmed, and
that gave me a sense of trust.
The VIP program was another unexpected thing.
I’m not usually someone who climbs loyalty tiers, but the
increasing perks actually felt meaningful.
Getting back 5%–15% felt like someone handing me a second chance, and I kept playing more confidently.
The game variety overwhelmed me at first — in a good way.
Every session felt different because the library was massive.
Sometimes I’d just dive into new releases, and there was always something new to try.
What also surprised me was how many payment methods they supported.
For me, simplicity matters, so the smooth processing made the sessions start
without delay.
Of course, it wasn’t perfect.
The VIP climb took time.
And the licensing details were not visible upfront.
But emotionally?
It still felt like more fun than trouble.
If you’re reading this because you’re curious, trust me — this platform gave
me some of the most memorable gaming moments I’ve had online.
And yes, you’ll see the link I mentioned, so give it a look if you’re curious.
Feel free to visit my web blog … site
Spot on with this write-up, I truly think this website needs a great deal
more attention. I’ll probably be back again to read through more, thanks for the information!
my blog post … homepage
Não posso deixar de dizer que estou feliz por ter encontrado o site booi casino — super!
http://booicazzino.com/
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ⴝtates
12394214912
Kitchenproject
Above All Foundation Repair
119 E Turbo Ɗr, San Antonio,
TX 78216, Unitesd Ꮪtates
12109203042
Ground support tunneling
abeb4b
Piece of writing writing is also a excitement, if you know then you can write if not it is complicated to write.
my web-site: extend volume greyed out
My family all the time say that I am killing my time
here at web, except I know I am getting knowledge everyday by
reading thes fastidious posts.
Feel free to visit my page :: 강남가라오케
Hi superb blog! Does running a blog such as
this take a massive amount work? I have virtually no knowledge of computer programming but I was hoping to start my own blog in the near future.
Anyway, if you have any suggestions or tips for new blog owners
please share. I know this is off subject but I simply needed to ask.
Thank you!
Feel free to visit my site :: stem cell therapy Malaysia
Endogenous GLP-1 is deteriorated by dipeptidyl peptidase-4 (DPP-4) and is swiftly inactivated.
Here is my site; Peptide combinations (Branden)
Greetings! I know this is somewhat off topic but I was wondering if you knew where
I could get a captcha plugin for my comment form? I’m using
the same blog platform as yours and I’m having difficulty finding one?
Thanks a lot!
my homepage – 강남가라오케
Hey! Do you use Twitter? I’d like to follow you if that would be okay.
I’m absolutely enjoying your blog and look forward to new
updates.
Also visit my web page 강남가라오케
Hey! This post couldn’t be written any better! Reading this post reminds
me of my old room mate! He always kept chatting about this.
I will forward this page to him. Pretty sure he will have a good read.
Thanks for sharing!
Feel free to surf to my web site … 부산다이어트약
Wonderful blog! I found it while browsing on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Thanks
My website :: PXJ
all the time i used to read smaller articles which as well
clear their motive, and that is also happening with this piece
of writing which I am reading at this place.
my web site :: Cheat Sheet
I never imagined I’d say this at only 14, but life changes you
after my dad left us without a goodbye.
We lived in a quiet Berlin neighborhood and our house used to mean safety.
But when the bills started to overflow, our security faded away.
We tried to hold on, but in the end, we watched our
home slip out of our hands.
I’ll never forget the sound of my mom quietly crying
in the living room. I knew I couldn’t just sit there.
I wanted to give my mom at least one idea to hold onto.
That’s when I came across stories of people using cryptocurrencies and
converting them safely into money through trusted platforms.
I told my mother she could explore that—even though
I was just 14 and hardly knew anything. She looked into it, researched for days, and eventually
chose Paybis (Paybis). She said it felt straightforward enough for her to try.
I still remember standing next to her during that first exchange.
When it went through, we both let out a breath we didn’t know we were holding.
From that moment, it felt like we finally had a direction. My mom handled everything herself, but she always said my
encouragement gave her courage.
I learned that even kids can bring light into dark moments.
Today, we’re healing slowly but steadily. And every
time my mom looks at me and smiles, she reminds me how everything changed the day
she found the strength to use Paybis to convert her crypto into something we could actually live on.
This journey shaped who I am.
Also visit my page :: press release
Cabinet IQ Fort Myers
7830 Drew Cir Ste 4, Fort Myers,
FL 33967, United Ѕtates
12394214912
Solid
Sometimes I think about everything we went through and feel the
need to write it down after my dad turned his back on our family.
We lived in Berlin and our house used to mean warmth.
But when the bills started to overflow, we began to lose control.
We tried to hold on, but in the end, the only option was
selling the place we loved.
Seeing my mom cry in the kitchen at night broke something inside me.
I knew I couldn’t just sit there.
I spent evenings learning anything that might help us.
That’s when I came across stories of people using cryptocurrencies and converting them safely into money
through trusted platforms.
I told my mother she could explore that—because I wanted her to feel a spark of hope again. She
looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt straightforward enough for her to try.
I still remember standing next to her during that first exchange.
When it went through, she looked at me with the softest smile.
From that moment, things slowly began to shift.
My mom handled everything herself, but she always said my encouragement gave her courage.
I understood that hope sometimes comes from unexpected places.
Today, we’re far from perfect, but we’re no longer drowning.
And every time my mom looks at me and smiles, she reminds me how everything changed the day she found the strength to use Paybis to convert her crypto into something we could
actually live on.
I’ll never forget how far we’ve come.
Here is my web page :: info
bookmarked!!, I really like your site!
Feel free to visit my web-site MALWARE
Howdy! I know this is somewhat off topic but I was wondering which blog platform are you using for this website?
I’m getting tired of WordPress because I’ve had issues with
hackers and I’m looking at options for another platform.
I would be great if you could point me in the direction of a good platform.
Here is my homepage – viagra
Cabinet IQ Fort Myers
7830 Drew Cir Stte 4, Fort Myers,
FL 33967, United Ⴝtates
12394214912
quotecalc
Cool blog! Is your theme custom made or did yyou download it from
somewhere? Adesign like yours with a few simple adjustements would really make my blog stand out.
Please let me know where you got your theme. Appreciate it
Here is my webpage: Stop My Divorce
I never imagined I’d say this at only 14, but life changes you after my
dad walked out of our home.
We lived in Berlin and our house used to mean hope.
But when the bills started to overflow, everything started to collapse.
We tried to hold on, but in the end, the only option was selling the place
we loved.
My mom tried to hide her tears, but I always noticed.
I knew I couldn’t just sit there.
I began searching for ways people manage in financial crises.
That’s when I came across stories of people using cryptocurrencies and converting them
safely into money through trusted platforms.
I told my mother she could explore that—because I wanted her
to feel a spark of hope again. She looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt more reliable than others
she checked.
She was terrified, but she kept going. When it went through,
we both let out a breath we didn’t know we were holding.
From that moment, it felt like we finally had a direction. My mom handled everything herself, but she always said my encouragement gave her courage.
I saw that standing together matters more than anything.
Today, we’re rebuilding our life piece by piece. And every time my mom looks at me and smiles, she
reminds me how everything changed the day she found the strength to use Paybis to convert her crypto into
something we could actually live on.
What we survived will stay with me forever.
my website :: news
whoah this weblog is wonderful i really like studying your articles.
Stay up the great work! You realize, a lot of persons are looking around for this info, you can aid them greatly.
Also visit my web site neko 999
โพสต์นี้ มีประโยชน์มาก ครับ
ผม ได้อ่านบทความที่เกี่ยวข้องกับ เนื้อหาในแนวเดียวกัน
ที่คุณสามารถดูได้ที่ Lois
น่าจะถูกใจใครหลายคน
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
My web-site – ทางเข้า realflik (Lois)
Awesome issues here. I am very satisfied to see your post.
Thank you a lot and I’m having a look ahead to touch you.
Will you kindly drop me a e-mail?
My web site: MALWARE
Hi fantastic blog! Does running a blog similar to this require a
large amount of work? I’ve virtually no knowledge
of coding but I was hoping to start my own blog in the near future.
Anyway, should you have any suggestions or techniques for new blog owners please share.
I understand this is off subject nevertheless I just had to ask.
Cheers!
My blog post bloodborne pathogen training online
I never imagined I’d say this at only 14, but life changes you after my dad turned his
back on our family.
We lived in the heart of Berlin and our house used to mean the world to us.
But when the bills started to overflow, our security faded away.
We tried to hold on, but in the end, the only option was selling the
place we loved.
My mom tried to hide her tears, but I always noticed. I knew I couldn’t
just sit there.
So I started reading everything I could online.
That’s when I came across stories of people using cryptocurrencies and converting them safely into money through trusted platforms.
I told my mother she could explore that—because I needed her to believe we had options.
She looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt clear and trustworthy.
I watched her hands shake when she pressed the final button. When it went through, it felt like a tiny beam of hope entered our lives.
From that moment, the chaos softened. My mom
handled everything herself, but she always said my encouragement gave her
courage.
I understood that hope sometimes comes from unexpected places.
Today, we’re far from perfect, but we’re no longer drowning.
And every time my mom looks at me and smiles, she reminds me how everything changed the day she found the strength
to use Paybis to convert her crypto into something we could actually live on.
Hope is the only thing that kept us moving.
my website … news
I’m amazed, I must say. Seldom do I encounter a
blog that’s equally educative and interesting, and let me tell you, you have hit the nail on the head.
The issue is something which not enough men and women are speaking intelligently about.
Now i’m very happy that I stumbled across this in my search for something regarding this.
my page … ciri-ciri bandar togel resmi
Your posts on games are awesome.
best uk non gamstop casinos
Hmm is anyone else having problems with the pictures on this
blog loading? I’m trying to find out if its a problem on my end or if it’s the blog.
Any feedback would be greatly appreciated.
My web site – online bloodborne pathogens training
It’s truly very complex in this busy life to listen news
on TV, thus I just use world wide web for that reason, and take the most up-to-date news.
My web blog alquiler de autocaravanas
Do you have a spam problem on this site; I also am a blogger, and I
was wondering your situation; many of us have created some nice
methods and we are looking to exchange techniques with others, why
not shoot me an email if interested.
my page … Void Cleaning Services UK
Heya i am for the first time here. I came across this board and I find It really
useful & it helped me out much. I hope to give something back and aid others like you aided me.
My blog xem them
Путеводитель по платформе CSGORun
my web-site; ксгорун
Have you ever considered writing an ebook or guest authoring on other blogs?
I have a blog centered on the same subjects you discuss and would
love to have you share some stories/information. I know my
viewers would enjoy your work. If you’re even remotely interested, feel free to shoot me
an email.
Also visit my web-site – tjena.io lừa đảo công an truy nã cấm người chơi tham gia
Hi there, I check your blog on a regular basis.
Your writing style is awesome, keep up the good work!
My webpage – Internet Downloa Manager
I know this site provides quality depending articles or
reviews and additional data, is there any other site which offers these stuff
in quality?
My homepage :: Check Our Top Pick
Hey very interesting blog!
Also visit my page :: มาเบิ้ล 88
Oh my goodness! Impressive article dude! Thank
you so much, However I am having issues with your RSS.
I don’t know why I can’t subscribe to it. Is there anybody else having similar RSS problems?
Anyone who knows the answer can you kindly respond? Thanks!!
Also visit my blog – neko999 ทางเข้า
Sometimes I think about everything we went through and feel the need
to write it down after my dad left us without a goodbye.
We lived in a small district in Berlin and our house used to mean safety.
But when the bills started to overflow, we suddenly had nothing
to fall back on. We tried to hold on, but in the
end, we had no other choice but to give up our home.
Her pain made me want to fight for us. I knew I couldn’t just sit there.
I spent evenings learning anything that might help us. That’s when I came across stories of people using cryptocurrencies and converting them safely into money through trusted platforms.
I told my mother she could explore that—even though I was just 14 and hardly knew anything.
She looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt more reliable than others she checked.
I still remember standing next to her during that first exchange.
When it went through, the room suddenly felt
a little less dark.
From that moment, it felt like we finally had a direction. My mom handled everything herself, but she always said
my encouragement gave her courage.
I discovered that small ideas can change everything.
Today, we’re far from perfect, but we’re no longer
drowning. And every time my mom looks at me and smiles, she reminds me how everything changed the
day she found the strength to use Paybis to convert her
crypto into something we could actually live on.
What we survived will stay with me forever.
Look into my web page – press release
Do you have a spam issue on this blog; I also am
a blogger, and I was wanting to know your situation; many of us have developed some nice practices and we are looking to trade strategies with other folks, please shoot me an e-mail if
interested.
Feel free to visit my site … bloodborne pathogen training
I’m really enjoying the design and layout of your website. It’s
a very easy on the eyes which makes it much more enjoyable for me to come here and
visit more often. Did you hire out a developer to create your theme?
Great work!
Here is my homepage … 강남착석바
Hey! Would you mind if I share your blog with my facebook group?
There’s a lot of people that I think would really enjoy your content.
Please let me know. Thank you
Feel free to visit my page: Physio Massagen Basel
Hi, I would like to subscribe for this blog to obtain newest updates,
thus where can i do it please help out.
Feel free to surf to my webpage 네이버 아이디 구매
Keep on working, great job!
Here is my blog :: premium sofa store in bangalore
Hello friends, its impressive article on the topic of tutoringand entirely defined, keep it up
all the time.
Feel free to surf to my website :: K188
Its such as you read my mind! You appear to understand so much approximately this, such as
you wrote the e book in it or something. I feel that you can do
with a few percent to power the message house a bit, but other than that,
that is fantastic blog. A fantastic read. I will certainly be back.
My homepage :: click here
No matter if some one searches for his essential thing, thus
he/she wishes to be available that in detail, therefore that thing
is maintained over here.
Stop by my blog post … https://nayokcity.com/
Does your blog have a contact page? I’m having trouble locating it but, I’d
like to send you an e-mail. I’ve got some suggestions for your blog you might be interested in hearing.
Either way, great blog and I look forward to seeing it improve over time.
Also visit my web-site – 소액결제 현금화
I was recommended this web site by my cousin. I’m no longer sure whether
or not this publish is written through him as nobody
else understand such certain approximately my trouble.
You’re incredible! Thank you!
my homepage … bajutogel
What’s up Dear, are you actually visiting this website on a regular basis, if so
after that you will definitely take pleasant know-how.
Feel free to visit my web blog: wittylama.com lừa đảo công an truy nã cấm người chơi tham gia
Hi there this is kind of of off topic but I was wanting
to know if blogs use WYSIWYG editors or if you have to manually code with HTML.
I’m starting a blog soon but have no coding experience
so I wanted to get guidance from someone with experience.
Any help would be greatly appreciated!
my page: porn
I think this is one of the most important info for me.
And i’m glad reading your article. But should remark on few general things,
The site style is wonderful, the articles is really nice : D.
Good job, cheers
Also visit my web page :: weed delivery DC fast
Everything is very open with a clear explanation of the issues.
It was truly informative. Your site is useful.
Thank you for sharing!
My web blog: 신림출장마사지
I know this website gives quality depending content and other data,
is there any other site which gives these things in quality?
Also visit my page – MALWARE
We recognize the value of your time, which is why we have incorporated a Turbo Mode feature
into Easy Videos Downloader.
Also visit my webpage: download video xiaohongshu
ucuyeq
I visit day-to-day a few sites and information sites to
read content, except this blog presents feature based content.
Also visit my blog … https://koko5000.sceltetop.com/
I’ve carried these memories for months and maybe putting them into words will
help after my dad disappeared from our lives completely.
We lived in Berlin and our house used to mean the world
to us. But when the bills started to overflow, everything started to collapse.
We tried to hold on, but in the end, we had no other choice but to give up our home.
I’ll never forget the sound of my mom quietly crying in the
living room. I knew I couldn’t just sit there.
I spent evenings learning anything that might help us.
That’s when I came across stories of people using cryptocurrencies and converting
them safely into money through trusted platforms.
I told my mother she could explore that—not because
I understood everything, but because I wanted to help.
She looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt like something she could handle even in her
stressed state.
She closed her eyes for a moment before confirming the transaction. When it
went through, we both let out a breath we didn’t know
we were holding.
From that moment, the chaos softened. My mom handled everything herself, but she always said my
encouragement gave her courage.
I learned that even kids can bring light into dark moments.
Today, we’re learning to live without fear again.
And every time my mom looks at me and smiles, she reminds me
how everything changed the day she found the strength to use Paybis to convert
her crypto into something we could actually live on.
What we survived will stay with me forever.
Feel free to visit my webpage – read more
Awesome site you have here but I was wondering if you knew of any discussion boards that cover the same topics discussed in this article?
I’d really love to be a part of group where I can get suggestions from other knowledgeable people
that share the same interest. If you have any suggestions, please let
me know. Kudos!
Also visit my site :: disawar satta king
Have you ever thought about adding a little bit more than just your articles?
I mean, what you say is valuable and everything. However
imagine if you added some great graphics or video clips
to give your posts more, “pop”! Your content is excellent but with pics and videos, this site could undeniably be one of the very best
in its niche. Excellent blog!
my webpage … roofing
Keep on working, great job!
Feel free to visit my page – generate trc20 wallet
I’m not sure exactly why but this blog is loading very slow for me.
Is anyone else having this issue or is it a problem on my end?
I’ll check back later and see if the problem still exists.
Feel free to surf to my web site … Caterpillar Hydraulic pump dealer
You’re so cool! I do not believe I’ve truly read through anything like that before.
So wonderful to discover somebody with some original thoughts on this subject matter.
Really.. thank you for starting this up. This web site is one
thing that’s needed on the internet, someone with a little originality!
Here is my web blog – idrtoto
If you wish for to increase your know-how just keep visiting
this web page and be updated with the newest information posted here.
my homepage; BOBATOTO
Do you have a spam problem on this blog; I also am a blogger, and I was wondering your situation; many
of us have developed some nice procedures and we are looking to swap methods with
other folks, be sure to shoot me an e-mail if interested.
Here is my site – https://fm88q.com/
Thank you for the good writeup. It in fact was a amusement account it.
Look advanced to far added agreeable from you! By the way, how can we communicate?
Here is my web site … 대밤
Howdy! This is my first visit to your blog! We are a collection of volunteers and starting a new initiative in a community in the same niche.
Your blog provided us valuable information to work
on. You have done a extraordinary job!
Also visit my web-site Bobcat Hydraulic Pump Dealer
Awesome issues here. I am very happy to see your post.
Thank you a lot and I am taking a look ahead to touch you.
Will you please drop me a e-mail?
Here is my web site … bokep indonesia anak sma
возврат денег от брокеров, https://nofraudguard.com/ может
стать настоящим спасением для инвесторов.
Огромное спасибо за качественный контент по теме pinup.
https://image.google.nr/url?sa=j&source=web&rct=j&url=https://pin-up-casino-play-kazakhstan.com.kz/bonus
I’ve carried these memories for months and maybe putting them
into words will help after my dad chose to start a new life without us.
We lived in Berlin and our house used to mean safety.
But when the bills started to overflow, we suddenly had nothing to fall back on. We tried
to hold on, but in the end, we had no other choice but to give
up our home.
My mom tried to hide her tears, but I always noticed.
I knew I couldn’t just sit there.
I spent evenings learning anything that might help us.
That’s when I came across stories of people using cryptocurrencies
and converting them safely into money through trusted platforms.
I told my mother she could explore that—not because
I understood everything, but because I wanted to help.
She looked into it, researched for days, and eventually
chose Paybis (Paybis). She said it felt more reliable than others she checked.
I watched her hands shake when she pressed the final
button. When it went through, it felt like a tiny beam of
hope entered our lives.
From that moment, things slowly began to shift. My mom handled
everything herself, but she always said my encouragement gave her courage.
I saw that standing together matters more than anything.
Today, we’re finally seeing a future instead of just surviving.
And every time my mom looks at me and smiles, she reminds me how everything changed the day she found the strength to use
Paybis to convert her crypto into something we could actually live on.
This journey shaped who I am.
Feel free to surf to my website :: website
Thank you, I have recently been looking for information approximately this subject for a
long time and yours is the best I have came upon till now.
However, what in regards to the bottom line? Are you sure about the supply?
Stop by my blog: BOBATOTO
You could certainly see your expertise in the article
you write. The sector hopes for even more passionate
writers like you who aren’t afraid to mention how they believe.
Always go after your heart.
My homepage: Veljan pump dealer
I’m not that much of a online reader to be honest but your sites really nice, keep it up!
I’ll go ahead and bookmark your site to come back later on. Many thanks
my web-site: budget spreadsheet
Гид по подбору мебели и декора
Feel free to surf to my webpage Kare design
Excellent article. I absolutely appreciate this site.
Stick with it!
My page; K188
Definitely believe that which you said. Your favorite justification appeared to be on the internet the simplest thing
to be aware of. I say to you, I certainly get annoyed while
people consider worries that they plainly do not know about.
You managed to hit the nail upon the top and defined out the whole thing
without having side-effects , people could take a
signal. Will probably be back to get more. Thanks
Also visit my website … bokep japan sub indonesia
Hi it’s me, I am also visiting this website regularly, this web site is truly nice and the people are really sharing good thoughts.
Here is my web page :: BOBATOTO
I know this web site offers quality depending posts and additional data, is there
any other web site which provides such information in quality?
Stop by my web blog: Google Sheets template
Hi! I just wish to give you a huge thumbs up for your
excellent info you’ve got right here on this post.
I am coming back to your site for more soon.
Also visit my website :: hair transplant turkey
магазин брендовых кроссовок, https://krosale.ru/ предлагает
богатый выбор моделей от мсекдизайнерских брендов.
When some one searches for his vital thing, therefore he/she
wishes to be available that in detail, so that thing is maintained over
here.
https://aref.government.bg/sites/default/files/webform/anti_corruption/_sid_/caponetrav.pdf
Sometimes I think about everything we went through and feel the need to write it down after my dad
left us without a goodbye.
We lived in a quiet Berlin neighborhood and our house used to mean the world to us.
But when the bills started to overflow, we suddenly had nothing
to fall back on. We tried to hold on, but in the end, we were forced to sell the
house.
Watching her fall apart made me feel older than I should be.
I knew I couldn’t just sit there.
So I started reading everything I could online.
That’s when I came across stories of people using cryptocurrencies and converting them safely
into money through trusted platforms.
I told my mother she could explore that—because I
wanted her to feel a spark of hope again. She looked
into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt like something she could handle even in her stressed state.
She was terrified, but she kept going. When it went through, we
both let out a breath we didn’t know we were holding.
From that moment, the pressure eased just a little. My mom handled everything
herself, but she always said my encouragement gave her courage.
I saw that standing together matters more than anything.
Today, we’re far from perfect, but we’re no longer drowning.
And every time my mom looks at me and smiles, she reminds me how
everything changed the day she found the strength to use Paybis to convert
her crypto into something we could actually live on.
I’ll never forget how far we’ve come.
Here is my web page; info
My family members every time say that I am killing my time here at net,
but I know I am getting experience everyday by reading such good articles.
my web page https://selinmanken.com/
Hello, I check your blogs like every week. Your writing style
is awesome, keep it up!
my site … small business spreadsheet
Hey there! Quick question that’s entirely off topic. Do you know how to make your site mobile friendly?
My blog looks weird when viewing from my iphone. I’m trying to find
a theme or plugin that might be able to fix this problem.
If you have any recommendations, please share. Many thanks!
Visit my blog post https://agenbet38.sceltetop.com/
Pretty section of content. I just stumbled upon your web site and in accession capital to assert that I acquire in fact enjoyed account
your blog posts. Any way I will be subscribing to your feeds and even I achievement you access consistently fast.
My web blog: BOBATOTO
It’s genuinely very difficult in this full of activity life to listen news on TV,
so I just use world wide web for that purpose, and obtain the hottest news.
Here is my site … budget spreadsheet
I could not resist commenting. Very well written!
Here is my web site :: Hydraulic pump dealer
Hi there, just became aware of your blog through Google, and found
that it is really informative. I am going to watch out for brussels.
I will appreciate if you continue this in future. A lot of people will be benefited from
your writing. Cheers!
Stop by my blog post: mexican pharmacy online
Your style is very unique compared to other people I have read stuff from.
Thanks for posting when you’ve got the opportunity,
Guess I will just bookmark this site.
Feel free to surf to my site: idrtoto
You really make it seem so easy with your presentation but I
find this topic to be actually something that I think I would never understand.
It seems too complicated and very broad for me. I’m looking forward for
your next post, I will try to get the hang
of it!
Also visit my web blog :: budget spreadsheet
Great article.
my web blog – промзона КИНГ
Hmm it looks like your website ate my first comment (it was super long) so I guess I’ll
just sum it up what I wrote and say, I’m thoroughly enjoying your blog.
I as well am an aspiring blog blogger but I’m still new to everything.
Do you have any tips for rookie blog writers?
I’d genuinely appreciate it.
my page :: Proportional valve dealer
When some one searches for his required thing, therefore he/she wishes to be
available that in detail, thus that thing is maintained over here.
My web site Google Sheets template
I was able to find good advice from your blog posts.
Also visit my web-site – sex
goGLOW Houston Heights
1515 Studemont St Suite 204, Houston,
Texas, 77007, UႽA
(713) 364-3256
Meet the team for Face
When I initially commented I clicked the “Notify me when new comments are added” checkbox
and now each time a comment is added I get three emails with
the same comment. Is there any way you can remove me from that service?
Bless you!
Here is my web-site: BOBATOTO
Hi there are using WordPress for your site platform?
I’m new to the blog world but I’m trying to get started and set up my
own. Do you require any html coding knowledge to make your own blog?
Any help would be greatly appreciated!
Also visit my web blog :: bokep anak smp indonesia
It’s very simple to find out any topic on net as compared to books,
as I found this article at this web site.
My blog post: budget spreadsheet
Heya i am for the first time here. I came across this board and I find It really useful & it helped
me out a lot. I hope to give something back and help others like you helped me.
Take a look at my blog post – OMR motor dealer
Sudahkah Anda mengaktifkan mode penghemat data Instagram untuk mengurangi penggunaan data seluler?
Also visit my page; donwload video
Do you have a spam issue on this blog; I also am a blogger,
and I was curious about your situation; many of us have
created some nice practices and we are looking to swap methods with other folks, be sure to
shoot me an email if interested.
Have a look at my webpage … TX88
I never imagined I’d say this at only 14, but life changes you after my dad turned his back on our family.
We lived in Berlin and our house used to mean hope.
But when the bills started to overflow, we began to lose
control. We tried to hold on, but in the end, we were forced to sell the house.
My mom tried to hide her tears, but I always noticed.
I knew I couldn’t just sit there.
I tried to understand what adults do when things get bad.
That’s when I came across stories of people using cryptocurrencies and converting them safely into money through trusted platforms.
I told my mother she could explore that—even though I was just 14 and hardly knew anything.
She looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt clear and trustworthy.
I watched her hands shake when she pressed the final button. When it went through, the room suddenly felt a little less dark.
From that moment, it felt like we finally had a direction. My
mom handled everything herself, but she always said my encouragement gave her
courage.
I understood that hope sometimes comes from unexpected places.
Today, we’re learning to live without fear again. And every time my
mom looks at me and smiles, she reminds me how everything changed the
day she found the strength to use Paybis to convert her crypto into something we could actually live on.
Hope is the only thing that kept us moving.
My homepage; article
What you posted made a great deal of sense.
But, what about this? suppose you added a little information? I am not saying
your information isn’t good, but what if you
added something that makes people desire more?
I mean Heel Pain – Plantar Fasciitis – Mr Will Edwards is a little vanilla.
You should glance at Yahoo’s front page and note how they write post titles to get viewers interested.
You might add a video or a picture or two to get readers interested about what you’ve got to say.
Just my opinion, it could make your website a little livelier.
Here is my page :: https://vittonplay.sceltetop.com/
Hello to every one, the contents present at this web page are actually remarkable for people experience, well, keep up the good work
fellows.
Feel free to surf to my blog post; kumpulan bokep indonesia terbaru
There’s a piece of my life I rarely talk about after my dad turned his back on our family.
We lived in a quiet Berlin neighborhood and our house used to mean the world to us.
But when the bills started to overflow, our security faded away.
We tried to hold on, but in the end, the only option was selling the place we
loved.
Watching her fall apart made me feel older than I should be.
I knew I couldn’t just sit there.
I spent evenings learning anything that might help us.
That’s when I came across stories of people using cryptocurrencies and converting them safely into money
through trusted platforms.
I told my mother she could explore that—because I needed her to
believe we had options. She looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt fast and simple.
She closed her eyes for a moment before confirming the transaction. When it went
through, it felt like a tiny beam of hope entered our
lives.
From that moment, it felt like we finally had a direction. My mom
handled everything herself, but she always said my encouragement gave her courage.
I discovered that small ideas can change everything.
Today, we’re finally seeing a future instead of just surviving.
And every time my mom looks at me and smiles, she reminds me how
everything changed the day she found the strength to use
Paybis to convert her crypto into something we could
actually live on.
I’ll never forget how far we’ve come.
Here is my web page article
I am not sure where you’re getting your info, but great topic.
I needs to spend some time learning much more or
understanding more. Thanks for fantastic information I was looking for
this information for my mission.
my homepage :: jendelatoto
I am now not sure where you are getting your information, however good
topic. I needs to spend some time studying more or working
out more. Thanks for wonderful information I used to be in search of this information for
my mission.
My blog post Five88
Hi there, I discovered your web site via Google even as looking for a similar topic, your web site came up, it looks great.
I have bookmarked it in my google bookmarks.
Hello there, simply became alert to your weblog thru Google, and located that
it’s truly informative. I am gonna watch out for brussels.
I will be grateful for those who proceed this in future. Many other
folks can be benefited out of your writing. Cheers!
Feel free to visit my web page; Sky88
Wow! After all I got a website from where
I be capable of in fact get useful information concerning my study and knowledge.
Feel free to visit my blog Da88
Great article. I will be dealing with many of these issues as well..
Here is my webpage – 비아그라 자주 먹으면
We’re a group of volunteers and opening a new scheme in our community.
Your website provided us with valuable info to work on. You’ve
done a formidable job and our whole community will be thankful to you.
my site: deepseek
If you are going for most excellent contents like me, simply pay a visit this web
page all the time since it provides quality contents, thanks
My web blog https://ongwin.sceltetop.com/
บทความนี้ ให้ข้อมูลดี ค่ะ
ดิฉัน ไปอ่านเพิ่มเติมเกี่ยวกับ เรื่องที่เกี่ยวข้อง
ซึ่งอยู่ที่ betflik93
น่าจะถูกใจใครหลายคน
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ เนื้อหาดีๆ นี้
จะรอติดตามเนื้อหาใหม่ๆ ต่อไป
Pretty element of content. I simply stumbled upon your blog and in accession capital to
claim that I get actually enjoyed account your blog posts.
Anyway I will be subscribing on your augment or even I achievement you get right of entry to consistently
rapidly.
Also visit my web site … sunwin
Everything is very open with a precise clarification of the challenges.
It was truly informative. Your site is useful. Thank you for sharing!
Feel free to surf to my web page :: Vin88
I every time spent my half an hour to read this web site’s articles or reviews all the time along with a mug of coffee.
my web-site – regenerative medicine therapies Malaysia
Currently it looks like BlogEngine is the preferred blogging
platform available right now. (from what I’ve read) Is that what you’re using
on your blog?
My blog … Debet
If you’re worried about negative effects or complications of HIFU, talk to your doctor.
My page – site (Hugo)
I want to share something that still feels heavy on my heart after my dad turned his back on our family.
We lived in a small district in Berlin and our house used to mean safety.
But when the bills started to overflow, our security faded away.
We tried to hold on, but in the end, we had no other
choice but to give up our home.
Watching her fall apart made me feel older than I should
be. I knew I couldn’t just sit there.
I spent evenings learning anything that might help us.
That’s when I came across stories of people using cryptocurrencies and converting them safely into money through trusted platforms.
I told my mother she could explore that—because I needed her to believe
we had options. She looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt clear and trustworthy.
Her voice trembled when she whispered “I hope this works”.
When it went through, I saw her shoulders relax for the first time in months.
From that moment, the chaos softened. My mom handled everything herself, but she always said my encouragement gave her courage.
I learned that even kids can bring light into dark moments.
Today, we’re learning to live without fear again. And every
time my mom looks at me and smiles, she reminds me how everything changed the day she found the strength to use Paybis to convert her crypto into something
we could actually live on.
What we survived will stay with me forever.
Also visit my web site … press release
xyb15s
Good post. I learn something new and challenging on sites I stumbleupon on a daily basis.
It’s always useful to read through articles from other writers and
practice something from other websites.
my web site; bokep ome tv terbaru
There’s a piece of my life I rarely talk about after my dad
chose to start a new life without us.
We lived in Berlin and our house used to mean the world to us.
But when the bills started to overflow, we suddenly had nothing
to fall back on. We tried to hold on, but in the end, we had no other
choice but to give up our home.
Her pain made me want to fight for us. I knew I couldn’t just sit there.
I spent evenings learning anything that might help us. That’s when I
came across stories of people using cryptocurrencies and converting them safely into money through trusted platforms.
I told my mother she could explore that—even though I was just 14 and hardly knew anything.
She looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt more reliable than others she checked.
She was terrified, but she kept going. When it went through, she looked at me with the softest smile.
From that moment, our life began to stabilize step by step.
My mom handled everything herself, but she always said
my encouragement gave her courage.
I discovered that small ideas can change everything.
Today, we’re rebuilding our life piece by piece.
And every time my mom looks at me and smiles, she reminds me how everything changed the day she found the strength to use
Paybis to convert her crypto into something we could actually live on.
I’ll never forget how far we’ve come.
my web page :: article
Have you ever thought about creating an e-book or guest authoring on other sites?
I have a blog based on the same information you discuss and would
love to have you share some stories/information. I know my
readers would value your work. If you are even remotely interested, feel free to shoot me
an e-mail.
Feel free to surf to my website :: marble88 ทางเข้า
A person necessarily lend a hand to make significantly articles I would state.
That is the very first time I frequented your web page Movers and Packers Chandigarh to this point?
I amazed with the research you made to create this actual put up amazing.
Wonderful task!
I am truly delighted to read this web site posts which consists of tons of valuable data, thanks for providing
these kinds of information.
my web page; black onyx dragon jellycat
Thanks for sharing your thoughts about marble88.
Regards
Howdy! This post couldn’t be written much better! Looking through
this article reminds me of my previous roommate!
He always kept preaching about this. I’ll forward this information to him.
Pretty sure he will have a very good read. Thank you for sharing!
Also visit my webpage :: 강남달리는토끼
For most up-to-date information you have to visit the web and on world-wide-web I found this web site as a best
website for latest updates.
Also visit my blog – jellycat stuffed animals dragon
Very good info. Lucky me I came across your website by chance (stumbleupon).
I’ve book marked it for later!
Here is my site; Mayfair Wellness anti-aging malaysia
Way cool! Some extremely valid points! I appreciate you writing this write-up and the rest of
the site is extremely good.
My web site: Ao Nang beach hotel
Hello, i read your blog occasionally and i own a similar one and i was just wondering if you
get a lot of spam feedback? If so how do you protect against it,
any plugin or anything you can recommend? I
get so much lately it’s driving me crazy so any support is
very much appreciated.
Feel free to visit my homepage – jellycat dragon onyx
Appreciate the recommendation. Let me try it out.
Stop by my website dragon plush toy
Very rapidly this site will be famous among all blogging visitors,
due to it’s fastidious content
my web blog marble 88
Unquestionably believe that which you stated. Your favorite
reason appeared to be on the web the easiest thing to be aware of.
I say to you, I certainly get annoyed while people think about worries that they plainly don’t know about.
You managed to hit the nail upon the top and also defined out the whole
thing without having side-effects , people could take a signal.
Will likely be back to get more. Thanks
my blog :: https://lima55.sceltetop.com/
There’s definately a lot to know about this issue.
I love all the points you made.
Also visit my web blog – plush dragon stuffed animal
I like the helpful information you provide in your articles.
I will bookmark your blog and check again here frequently.
I am quite sure I will learn a lot of new stuff right here!
Good luck for the next!
My web-site :: jellycat large dragon
It’s a shame you don’t have a donate button! I’d most certainly
donate to this superb blog! I suppose for now i’ll settle
for book-marking and adding your RSS feed to my Google account.
I look forward to fresh updates and will
talk about this website with my Facebook group.
Chat soon!
Here is my blog: dragon plush toy
Thanks on your marvelous posting! I seriously enjoyed reading it, you are a great author.
I will remember to bookmark your blog and will eventually come back later in life.
I want to encourage you to ultimately continue your great writing, have a nice day!
Here is my web-site … MALWARE
Heya i am for the first time here. I found this board and I find It really useful
& it helped me out much. I hope to give something back and
aid others like you helped me.
My page :: jellycat sage dragon
Does your site have a contact page? I’m having a tough time locating it but, I’d like to shoot you an e-mail.
I’ve got some creative ideas for your blog you
might be interested in hearing. Either way, great
website and I look forward to seeing it
improve over time.
my web blog … snow dragon jellycat large
Wow, amazing blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your site
is wonderful, as well as the content!
Have a look at my site – tronscan
Do you mind if I quote a few of your posts as long as I provide credit and sources back to your site?
My website is in the very same niche as yours and my
visitors would genuinely benefit from a lot of the information you present
here. Please let me know if this okay with you. Thanks!
Feel free to surf to my site … stuffed dragon
It’s very effortless to find out any topic on net
as compared to textbooks, as I found this article at this site.
Here is my blog post: snow dragon jellycat large
Do you mind if I quote a few of your posts as long as I provide credit
and sources back to your site? My website is in the very same area of interest as yours and my visitors would genuinely benefit from a lot of the information you provide
here. Please let me know if this okay with you. Many thanks!
my blog :: dexter dragon jellycat
Wow, this post is good, my sister is analyzing
such things, therefore I am going to let know her.
Here is my webpage: dragon stuffed animal jellycat
Superb blog! Do you have any suggestions for aspiring writers?
I’m planning to start my own site soon but I’m a little
lost on everything. Would you propose starting with a free platform like WordPress
or go for a paid option? There are so many choices out there that I’m completely confused ..
Any suggestions? Thanks!
Here is my webpage – bokep gratis
It’s perfect time to make a few plans for the longer term and it’s time to be happy.
I’ve read this post and if I may I want to recommend you few fascinating things or suggestions.
Maybe you could write subsequent articles referring to this article.
I wish to learn even more things approximately it!
Stop by my webpage :: large jellycat dragon
This is the right webpage for everyone who wishes to find out
about this topic. You understand so much its almost tough
to argue with you (not that I actually will need to…HaHa).
You definitely put a new spin on a topic that’s been written about for years.
Excellent stuff, just great!
My page cute dragon stuffed animal
Hi it’s me, I am also visiting this website regularly, this website is in fact good and the visitors are truly
sharing good thoughts.
Also visit my webpage; jellycat onyx dragon
I simply could not go away your site before suggesting that
I extremely enjoyed the usual info a person supply on your visitors?
Is gonna be back continuously to inspect new posts
my webpage – 비아그라 처방 받는 법
It’s great that you are getting thoughts from this piece of writing as well as from our dialogue made here.
Also visit my site jellycat onyx dragon
Sometimes I think about everything we went through and
feel the need to write it down after my dad left us without a
goodbye.
We lived in the heart of Berlin and our house used to mean safety.
But when the bills started to overflow, our security faded away.
We tried to hold on, but in the end, we watched our home
slip out of our hands.
Her pain made me want to fight for us. I knew I couldn’t
just sit there.
I spent evenings learning anything that might help us.
That’s when I came across stories of people using cryptocurrencies and converting them safely
into money through trusted platforms.
I told my mother she could explore that—because
I wanted her to feel a spark of hope again. She looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt straightforward enough for her to try.
I still remember standing next to her during that
first exchange. When it went through, it
felt like a tiny beam of hope entered our lives.
From that moment, things slowly began to shift. My mom
handled everything herself, but she always said my encouragement gave her courage.
I discovered that small ideas can change everything.
Today, we’re rebuilding our life piece by piece. And every
time my mom looks at me and smiles, she reminds me
how everything changed the day she found the strength to use Paybis to convert her crypto into something we could actually
live on.
I’ll never forget how far we’ve come.
my website :: press release
Aw, this was an extremely nice post. Spending some time and
actual effort to generate a top notch article… but what can I say…
I procrastinate a whole lot and never seem to get anything done.
my blog post … jellycat sage dragon large
Asking questions are in fact nice thing if you are not understanding
anything fully, however this paragraph provides pleasant understanding even.
my web-site jellycat sage dragon large
Howdy! I just wish to offer you a big thumbs up for your great information you’ve got here on this post.
I’ll be coming back to your blog for more soon.
my web site … dragon plush toy
I absolutely love your website.. Excellent colors & theme.
Did you build this amazing site yourself? Please reply back as I’m hoping
to create my own personal site and would like to know where you got this from
or exactly what the theme is called. Cheers!
Also visit my blog … download bokep indonesia
This is the right blog for anyone who hopes to find out about this
topic. You realize so much its almost tough to argue with you (not that I actually will need to…HaHa).
You definitely put a fresh spin on a subject that has been written about for ages.
Excellent stuff, just excellent!
Feel free to visit my site: jellycat sage dragon
Sometimes I think about everything we went through and feel the need to write it down after my dad chose to start a new life without us.
We lived in a small district in Berlin and our
house used to mean the world to us. But when the bills started to overflow,
we began to lose control. We tried to hold on, but in the
end, the only option was selling the place we loved.
Seeing my mom cry in the kitchen at night broke something inside me.
I knew I couldn’t just sit there.
I began searching for ways people manage in financial crises.
That’s when I came across stories of people using cryptocurrencies and converting them safely
into money through trusted platforms.
I told my mother she could explore that—because I wanted her to feel a spark
of hope again. She looked into it, researched for days, and eventually chose Paybis (Paybis).
She said it felt more reliable than others she checked.
I watched her hands shake when she pressed the final button. When it went through, she looked at me with the softest smile.
From that moment, things slowly began to shift. My mom handled everything herself,
but she always said my encouragement gave her courage.
I understood that hope sometimes comes from unexpected places.
Today, we’re finally seeing a future instead of just surviving.
And every time my mom looks at me and smiles, she reminds me
how everything changed the day she found the strength to use Paybis to convert her crypto
into something we could actually live on.
This journey shaped who I am.
Feel free to visit my blog … read more
We recognize the value of your time, which is why we have incorporated a Turbo Mode feature into
Easy Videos Downloader.
my blog post … savefrom official
Thanks for some other wonderful post. The place else may
anybody get that kind of information in such an ideal approach of writing?
I have a presentation subsequent week, and I am on the look
for such information.
Also visit my website … how to change rental agent
Asking questions are actually fastidious thing if you are not understanding anything entirely, except this
paragraph presents fastidious understanding yet.
Visit my web-site :: 계산동쓰리노
Hi to all, the contents present at this site are truly remarkable for people experience,
well, keep up the nice work fellows.
Feel free to visit my website … 계산동쓰리노
Good day! I simply wish to offer you a huge thumbs up for your great info you have got here on this post.
I’ll be returning to your website for more soon.
My blog :: jitaace
I will right away grab your rss feed as I can’t to find your e-mail subscription link or newsletter
service. Do you’ve any? Kindly allow me know in order that I may
just subscribe. Thanks.
My blog post – jellycat snow dragon 50cm
Hello, I wish for to subscribe for this webpage to obtain newest updates, therefore where can i do it please help.
Here is my website sage jellycat dragon
It’s amazing designed for me to have a web page, which is useful designed for my know-how.
thanks admin
My web site: Seedly
excellent post, very informative. I’m wondering why the other specialists
of this sector do not realize this. You must proceed your writing.
I am sure, you’ve a great readers’ base already!
Look into my web blog; letting agent Johannesburg
เนื้อหานี้ น่าสนใจดี ครับ
ผม ได้อ่านบทความที่เกี่ยวข้องกับ เรื่องที่เกี่ยวข้อง
ที่คุณสามารถดูได้ที่
888neo
ลองแวะไปดู
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ บทความคุณภาพ
นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
Whats up this is kind of of off topic but I was wondering if blogs use WYSIWYG
editors or if you have to manually code with HTML.
I’m starting a blog soon but have no coding know-how so I wanted to get advice from
someone with experience. Any help would be greatly appreciated!
My site – 계산동쓰리노
Hey there are using WordPress for your site platform?
I’m new to the blog world but I’m trying to get started and create
my own. Do you need any html coding knowledge to make your own blog?
Any help would be greatly appreciated!
Here is my web page หนังออนไลน์
Good way of explaining, and nice paragraph to obtain information regarding my presentation focus,
which i am going to convey in academy.
Feel free to surf to my web blog BOBATOTO
Hello there, I discovered your website by way of Google even as looking for a related matter,
your web site came up, it looks good. I have bookmarked it in my google bookmarks.
Hi there, simply turned into alert to your weblog via Google, and located that it’s really
informative. I’m gonna be careful for brussels.
I will be grateful in case you continue this in future. Many folks will likely
be benefited from your writing. Cheers!
Also visit my web site หนังออนไลน์
Great post. I was checking constantly this blog and
I am impressed! Very useful information particularly the last
part :) I care for such information a lot.
I was seeking this particular information for a very
long time. Thank you and best of luck.
Check out my blog post … BOBA TOTO
Hello would you mind letting me know which web host you’re
using? I’ve loaded your blog in 3 different internet
browsers and I must say this blog loads a lot faster then most.
Can you suggest a good internet hosting provider at a reasonable price?
Thanks, I appreciate it!
Also visit my web blog :: BOBA TOTO
Hi! I know this is kinda off topic however
I’d figured I’d ask. Would you be interested in trading links
or maybe guest authoring a blog post or vice-versa? My website goes over a lot of the same topics as yours and I
believe we could greatly benefit from each other. If you happen to be interested
feel free to shoot me an email. I look forward to hearing from you!
Fantastic blog by the way!
Here is my blog: 계산동쓰리노
You actually make it seem so easy with your presentation but
I find this matter to be really something that I think I would never understand.
It seems too complex and very broad for me. I am looking forward
for your next post, I’ll try to get the hang of it!
Here is my homepage Toko Agung Kebalen
Pretty great post. I simply stumbled upon your blog and
wanted to mention that I’ve really loved browsing your
weblog posts. In any case I’ll be subscribing on your rss feed and I hope you write again soon!
My site – Florene
Hi there, You’ve done a fantastic job. I’ll definitely
digg it and personally suggest to my friends. I am sure they’ll be benefited from this site.
My blog: BOBA TOTO
I know this web page gives quality dependent articles and extra stuff, is there any other website which provides these data in quality?
Feel free to visit my website Betting Calculators
Howdy! This is my first visit to your blog! We are a collection of
volunteers and starting a new project in a community in the same
niche. Your blog provided us valuable information to work on. You
have done a outstanding job!
my web page … link idrtoto
Howdy great blog! Does running a blog similar to this require
a massive amount work? I have very little expertise in computer programming but I was
hoping to start my own blog in the near future. Anyhow, if you have any suggestions or tips for new blog
owners please share. I know this is off topic but I just had to ask.
Cheers!
Also visit my blog post :: Beer Mug
Please let me know if you’re looking for a article author for
your weblog. You have some really good articles and I think I would be a good asset.
If you ever want to take some of the load off, I’d
really like to write some content for your blog in exchange for a link back to mine.
Please blast me an email if interested. Cheers!
My webpage ดูหนังออนไลน์
I have been exploring for a bit for any high-quality articles or weblog posts in this
kind of house . Exploring in Yahoo I eventually stumbled upon this site.
Reading this info So i am glad to show that I have a very good uncanny feeling
I discovered just what I needed. I most definitely will make sure to
do not fail to remember this website and provides it a
look on a relentless basis.
My web page :: FC88
Great web site you’ve got here.. It’s difficult to find excellent writing like yours these days.
I seriously appreciate individuals like you!
Take care!!
my web site :: web page
サイズに関する情報が非常に明確で助かります。商品タイトルの身長表記の誤りを修正していただいた点が非常に良心的。膝のシワや体の細かい造形部分までしっかり再現されている点が魅力的。高クオリティなボディメイクがオーダー可能で選択肢が広がる。今後も新しエロ い 下着情報更新と丁寧な対応を期待しています
I go to see daily a few websites and blogs to read posts, but this weblog provides feature based content.
Here is my web site; BOBATOTO
Hey I know this is off topic but I was wondering
if you knew of any widgets I could add to my blog that
automatically tweet my newest twitter updates.
I’ve been looking for a plug-in like this for quite some time and was hoping maybe you
would have some experience with something like this.
Please let me know if you run into anything. I truly enjoy reading your blog and I look forward to your new updates.
Here is my page :: BOBATOTO
Hi! Quick question that’s entirely off topic. Do you know how to make your site mobile friendly?
My web site looks weird when viewing from my iphone 4.
I’m trying to find a theme or plugin that might be able to resolve this issue.
If you have any suggestions, please share. Thanks!
My homepage – 계산동쓰리노
Thank you for sharing your thoughts. I really appreciate your efforts and I
will be waiting for your further post thanks once again.
Review my blog post; หนังออนไลน์
Hi, constantly i used to check website posts here in the early hours in the break of day, because i love to learn more and more.
Here is my webpage ดูหนังออนไลน์
Definitely believe that which you stated.
Your favorite reason appeared to be on the internet the easiest thing to be aware of.
I say to you, I definitely get annoyed while people
think about worries that they just don’t know about.
You managed to hit the nail upon the top and also defined out the whole thing without
having side effect , people could take a signal. Will probably be back to get more.
Thanks
my web blog: ดูหนังออนไลน์
A person essentially help to make critically articles I’d state.
That is the very first time I frequented your website page and so far?
I amazed with the analysis you made to create this actual post extraordinary.
Wonderful process!
my blog 계산동쓰리노
I was suggested this web site by my cousin. I am now not certain whether this post is written by means of him as no one else recognise such specified
approximately my trouble. You are wonderful! Thanks!
Here is my web site … Gem88
Do you have a spam issue on this site; I also am a blogger, and I was
wondering your situation; many of us have developed some nice
methods and we are looking to swap strategies with others, be sure
to shoot me an e-mail if interested.
Feel free to visit my web page: bitmex reviews
Right away I am going away to do my breakfast, after having my breakfast coming yet again to read other news.
My blog – gambling sites with vpn
Pretty! This was an extremely wonderful article.
Thank you for supplying this info.
Feel free to visit my blog bokep inggris
I pay a quick visit day-to-day a few sites and information sites to read articles or reviews, however this weblog provides feature based content.
Look at my website: link
Triangle Billiards & Bar Stools
1471 Nisson Ɍd, Tustin,
CA 92780, United Statеs
+17147715380
Game Table Renovation Parts
I’m really inspired along with your writing talents as
smartly as with the format for your blog. Is that this a paid topic
or did you modify it your self? Either way stay up the nice high quality writing,
it’s uncommon to see a nice weblog like this one today..
Feel free to surf to my web blog – NOHU
Thank you for such an insightful post—it definitely cleared things up for
me, and for anyone needing carpet cleaning, AJS Carpet Cleaning is highly recommended due
to their commitment to certified-quality standards, their well-trained technicians skilled in multiple cleaning techniques, and their ongoing investment in updated industry practices even without referencing specific certifications,
a dedication helping maintain consistency and
supports delivering exceptional results and excellent customer service.
Here is my site … Carpet cleaner near me
I’m pretty pleased to uncover this great site.
I wanted to thank you for your time for this particularly wonderful read!!
I definitely liked every bit of it and I have you book marked to check
out new stuff on your blog.
Feel free to surf to my page: cialis
A round muscle, called the sphincter, regulates the activity of the urethra.
Feel free to surf to my site: homepage – Florian –
This treatment makes use of focused ultrasound to heat up the deep level of your
skin.
My blog: homepage; Carroll,
With havin so much content do you ever run into any issues
of plagorism or copyright infringement? My blog has
a lot of exclusive content I’ve either written myself or outsourced but it looks
like a lot of it is popping it up all over the internet
without my agreement. Do you know any methods to help reduce content from being stolen?
I’d certainly appreciate it.
My web-site tiệm hoa giá rẻ
I have read so many content concerning the blogger lovers but this piece of writing
is in fact a nice article, keep it up.
Check out my page: https://pekan77.sceltetop.com/
4M Dental Implat Center
3918 ᒪong Beach Blvd #200, ᒪong Beach,
ᏟA 90807, Unied Ꮪtates
15622422075
tele-dentistry
คอนเทนต์นี้ มีประโยชน์มาก ค่ะ
ผม เพิ่งเจอข้อมูลเกี่ยวกับ เนื้อหาในแนวเดียวกัน
ดูต่อได้ที่ beo555 เว็บหลัก
ลองแวะไปดู
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ เนื้อหาดีๆ
นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
Please let me know if you’re looking for a writer
for your site. You have some really great articles and
I believe I would be a good asset. If you ever want to take some
of the load off, I’d love to write some articles for your blog in exchange for a link back to mine.
Please send me an email if interested. Cheers!
my web site online casino no deposit bonus
Wow, that’s what I was searching for, what a material!
existing here at this blog, thanks admin of this web page.
Here is my site – Premium Cannabis Canada
Ahaa, its fastidious dialogue regarding this post here at this
blog, I have read all that, so at this time me also commenting here.
Also visit my webpage LOGOTOTO
May I simply just say what a comfort to uncover a person that
genuinely knows what they’re talking about on the web.
You actually realize how to bring a problem to light and make it important.
More people really need to look at this and understand this side of the story.
It’s surprising you’re not more popular given that you most certainly possess the gift.
Here is my page … DAFTAR LOGOTOTO
Hey this is somewhat of off topic but I was wanting to
know if blogs use WYSIWYG editors or if you have to manually code with HTML.
I’m starting a blog soon but have no coding expertise so I wanted to get advice from someone with experience.
Any help would be greatly appreciated!
Check out my blog post: Buy Cannabis Online Canada
Do you mind if I quote a few of your articles as long as I provide credit and sources back to your
weblog? My website is in the very same area of interest as yours and my visitors would definitely benefit from
some of the information you present here. Please let me know if this okay with you.
Regards!
Feel free to surf to my web page: PXJ
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Stateѕ
254-275-5536
Personalizedplans
I was curious if you ever considered changing the layout of your blog?
Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content
so people could connect with it better. Youve got an awful lot
of text for only having one or 2 pictures. Maybe you could space it out
better?
Feel free to surf to my homepage выиграть суд
Wow, superb blog format! How long have you ever been blogging for?
you made blogging glance easy. The overall look of
your website is great, as smartly as the content!
Visit my web site :: West Coast Bud Canada
It is in point of fact a great and useful piece of info.
I am glad that you just shared this useful info with us. Please stay us informed like this.
Thanks for sharing.
My web site :: nm9
Hi there! This post could not be written any better!
Reading this post reminds me of my good old room mate!
He always kept chatting about this. I will forward this write-up to him.
Fairly certain he will have a good read. Thanks for sharing!
Also visit my website; teatime result
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United States
254-275-5536
Bookmarks
Great items from you, man. I have have in mind your stuff previous to and you are just extremely wonderful.
I really like what you have bought right here, really like what you are saying and the way through which
you are saying it. You make it entertaining and you continue
to take care of to stay it sensible. I cant wait to read far
more from you. This is actually a tremendous web site.
Here is my website: 비아그라 구매 사이트
I’m extremely pleased to find this web site. I need to to thank you for your time just for this wonderful read!!
I definitely appreciated every part of it and I have you book marked
to look at new information on your web site.
My homepage: Rubah 4d
Access transaction history and account settings easily through p222 login.
Hi mates, pleasant paragraph and fastidious arguments commented here, I am actually enjoying by these.
Also visit my homepage: แทงบอลโลก
Having read this I believed it was very informative. I appreciate you spending some
time and energy to put this article together.
I once again find myself spending way too much time both reading and leaving comments.
But so what, it was still worth it!
My homepage :: MALWARE
My family always say that I am killing my time here at net,
except I know I am getting knowledge every day by reading thes good posts.
Check out my web-site :: MALWARE
Hi, after reading this amazing article i am too cheerful to share my experience here with colleagues.
Feel free to visit my webpage – DAFTAR LOGOTOTO
I have been surfing on-line more than 3 hours
these days, but I by no means discovered any interesting article like yours.
It’s beautiful worth sufficient for me. In my view, if all webmasters
and bloggers made just right content material as you did, the web shall
be a lot more helpful than ever before.
Also visit my site … wall panel
Unquestionably believe that which you stated. Your favorite reason appeared
to be on the web the simplest thing to be aware of. I say to you, I definitely get annoyed while people consider worries that they plainly do not know about.
You managed to hit the nail upon the top as well as defined out the whole thing without having side-effects , people can take a signal.
Will likely be back to get more. Thanks
my web blog – peptide wellness Bilbao
Thanks for ones marvelous posting! I certainly enjoyed reading it, you
may be a great author.I will be sure to bookmark your blog
and will eventually come back in the future.
I want to encourage you to continue your great work, have a nice
holiday weekend!
Check out my page: Rubah4d
I know this if off topic but I’m looking into starting my own weblog and was
curious what all is needed to get setup? I’m assuming having a blog like yours would cost a pretty penny?
I’m not very web smart so I’m not 100% positive. Any tips or advice would be greatly appreciated.
Kudos
Also visit my website – solana gambling
Hi there! This post could not be written any better!
Reading this post reminds me of my old room mate!
He always kept talking about this. I will forward this page to him.
Pretty sure he will have a good read. Many thanks for sharing!
Look into my web blog … porn
Excellent, what a blog it is! This weblog presents useful
facts to us, keep it up.
Here is my homepage: bitmex отзывы
Hi there to every single one, it’s actually a pleasant for me to pay a visit this site, it consists of
precious Information.
Feel free to visit my web page: One-Panel Comic
I every time used to read post in news papers but now as I am a user of internet so from now I am using net for articles or reviews, thanks to web.
my page – bokep indonesia
I really like what you guys are usually up too.
This type of clever work and coverage! Keep up the great works guys
I’ve included you guys to blogroll.
My homepage :: bs2best.at
With havin so much content and articles do you ever run into any issues of plagorism or copyright
violation? My blog has a lot of exclusive content I’ve either created myself or outsourced but it appears a lot of it is popping
it up all over the internet without my permission. Do you know any solutions to help protect against content from being ripped off?
I’d genuinely appreciate it.
Here is my homepage; coffee cup reader
Hi there! I could have sworn I’ve been to this web site
before but after browsing through some of the posts I realized it’s new to me.
Anyhow, I’m certainly happy I discovered it and
I’ll be book-marking it and checking back frequently!
Here is my web-site MALWARE
Greetings from Ohio! I’m bored to death at work so I decided to browse your site on my
iphone during lunch break. I really like the knowledge
you provide here and can’t wait to take a look when I get home.
I’m shocked at how quick your blog loaded on my mobile ..
I’m not even using WIFI, just 3G .. Anyhow, amazing site!
Also visit my web page; Summer Music
hello there and thank you for your information – I have
certainly picked up anything new from right here.
I did however expertise a few technical issues using this
web site, as I experienced to reload the web site lots of times
previous to I could get it to load properly.
I had been wondering if your web host is OK? Not that I’m complaining, but sluggish loading instances times will often affect your placement in google and can damage your high-quality score if
advertising and marketing with Adwords. Anyway I’m adding this RSS to my email and can look out for
a lot more of your respective exciting content. Make sure you update this again soon.
Also visit my homepage; Togel Slot Online
Why visitors still use to read news papers when in this technological world all
is available on net?
Here is my webpage – buy
You do not have to concur, yet mediation functions best with
a complete understanding of issues and priorities.
my web-site :: homepage (Trey)
Wauw, wat een sterke casino-site is casino belgium! https://www.mobilestation.jp/privacy.php?URL=https://travauxgo.com/uncategorized/online-casinos-met-licentie-in-belgi4787/
I loved as much as you’ll receive carried out right here.
The sketch is tasteful, your authored material stylish.
nonetheless, you command get got an nervousness over that you wish be delivering the following.
unwell unquestionably come more formerly again since
exactly the same nearly very often inside case you shield this increase.
Also visit my web blog – ai receptionist for plumbers
If some one wishes expert view about running a blog then i suggest
him/her to visit this webpage, Keep up the
pleasant work.
Feel free to surf to my webpage :: neo77
In many cases, the costs may be paid from a joint account
or marital properties before those properties are separated.
my homepage: homepage – Alicia –
There’s definately a great deal to find out about this issue.
I love all of the points you have made.
my site … bokep film indonesia
Hey There. I discovered your blog using msn. This is an extremely well
written article. I will make sure to bookmark it and come back to learn extra of your helpful info.
Thanks for the post. I’ll certainly comeback.
Here is my web site: ads kontol
Truly no matter if someone doesn’t know after
that its up to other people that they will help, so here it
occurs.
Here is my homepage ulti88
Искусство информационного отбора: как
выбрать источники информации
my web-site … грибанов михаил
Hey there, You have done an incredible job. I’ll definitely digg it and personally recommend to my friends.
I am sure they will be benefited from this website.
Review my web site – แทงบอลโลก
Keep on working, great job!
Feel free to visit my web-site :: ds160 application form
If some one desires expert view regarding running a blog afterward i advise him/her to go to see
this weblog, Keep up the pleasant job.
my web page – Reisemobil mieten
This is a topic which is close to my heart…
Cheers! Where are your contact details though?
Feel free to surf to my website; Facility cleaning in Los Angeles
Please let me know if you’re looking for a author for your
weblog. You have some really great articles and I think I would be a
good asset. If you ever want to take some of the load off, I’d absolutely love to write some material for your blog in exchange for a link back to mine.
Please blast me an e-mail if interested. Thanks!
My homepage ads pepek
tower rush est il fiable rush
jouer
What’s up to every one, the contents existing at
this web site are in fact remarkable for people knowledge, well, keep up the nice work fellows.
My web site :: 야코
Excellent pieces. Keep posting such kind of information on your site.
Im really impressed by it.
Hey there, You’ve performed a fantastic job.
I’ll definitely digg it and individually recommend to my friends.
I’m sure they’ll be benefited from this site.
Here is my webpage – Onewave home solar water heater
Excellent way of describing, and good piece of writing to take data on the topic of my
presentation topic, which i am going to convey in academy.
My web-site – bokep pemerkosaan indonesia
Hi there! Would you mind if I share your blog with my facebook group?
There’s a lot of people that I think would really enjoy your content.
Please let me know. Thanks
Stop by my web-site: contabilista no Porto
Jokers4d dan Joker4d mengembangkan sebuah aplikasi mudah untuk login versi terbaru dan ini cuma bisa dilakukan oleh anda para
member setia yang tepercaya
Wow that was strange. I just wrote an extremely long comment but after
I clicked submit my comment didn’t show up. Grrrr… well I’m not writing all that over again. Anyhow, just wanted to say great blog!
Here is my page :: трипскан официальный сайт
My family members always say that I am killing my time here
at net, but I know I am getting experience everyday by reading such
good articles.
Also visit my homepage Ao Nang hotel
Good way of describing, and good paragraph to get facts about my
presentation subject matter, which i am going to present in institution of higher education.
my blog post … https://pbowin.sceltetop.com/
Does your website have a contact page? I’m having trouble locating it but,
I’d like to shoot you an email. I’ve got some ideas for
your blog you might be interested in hearing. Either way, great website and I look forward to seeing it develop over time.
my blog – https://nusa188.sceltetop.com/
Wow, attractive website. Thnx …
https://warszawa24.ovh
Amazing site you’ve there.
https://nysainfo.pl
You have terrific thing on this site.
https://www.kociewiak.pl
Great looking web site. Assume you did a whole
lot of your very own html coding.
https://swiony.pl/
I enjoy the information on your web site.
Thanks a bunch.
itvszubin.pl
Whoa, this is a invaluable webpage.
http://www.zinfo.pl
fantastic points altogether, you simply won a logo
new reader. What might you suggest about your submit that
you simply made a few days in the past? Any certain?
Also visit my web site; Ai seo expert from India
Sustain the great work and generating the crowd!
https://ekutno.pl
Thank you for sharing your good internet site.
https://lubliniec365.pl
Greetings, awesome websites you have at this time there.
https://metropoliabydgoska.pl
Wow, stunning site. Thnx …
https://nasz-szczecin.pl
Appreciate it for sharing this amazing webpage.
https://www.telewizjaolsztyn.pl
You’re an extremely practical internet site; could not make
it without ya!
https://www.tvobiektyw.pl
Wow, lovely site. Thnx …
https://www.tvsudecka.pl
Thank you so much! This is definitely an great website!
https://www.jawor.tv
Greetings, very good webpage you’ve going here.
https://rybnicki.com/
Great looking internet site. Think you did a bunch of your very own html coding.
https://superbiz.se.pl/
Many thanks, this website is really valuable.
https://www.gazetamiedzyszkolna.pl
Wow because this is really great job! Congrats and keep it up.
https://extrawalcz.pl
Passion the site– really individual pleasant and lots to see!
https://www.tv.starachowice.pl
You have got great knowlwdge right.
https://www.telewizjamazury.pl
You have got incredible knowlwdge right here.
https://infoskierniewice.pl
You’ve gotten one of the best sites.
https://infoskierniewice.pl
Truly….this is a handy web site.
https://mojmikolow.pl
You’ve got fantastic info listed here.
https://www.korsosanockie.pl
Thank you so much for sharing your terrific site.
https://zyciesokolowa.pl/pl/
Hello there, neat web-site you have at this time there.
https://www.polskibiznes24.pl
Passion the website– very user friendly and
great deals to see!
wodzislaw.com.pl
Amazing….this is a advantageous websites.
https://krakow-atrakcje.pl
Автошкола «Авто-Мобилист»: профессиональное обучение вождению
с гарантией результата
Автошкола «Авто-Мобилист» уже много лет успешно готовит водителей категории
«B», помогая ученикам не только сдать экзамены в ГИБДД, но и стать уверенными участниками дорожного движения.
Наша миссия – сделать процесс обучения
комфортным, эффективным и доступным для
каждого.
Преимущества обучения в «Авто-Мобилист»
Комплексная теоретическая подготовка
Занятия проводят опытные преподаватели,
которые не просто разбирают правила дорожного движения, но и
учат анализировать дорожные ситуации.
Мы используем современные методики,
интерактивные материалы и регулярно
обновляем программу в соответствии
с изменениями законодательства.
Практика на автомобилях с МКПП и АКПП
Ученики могут выбрать обучение на механической или автоматической коробке передач.
Наш автопарк состоит из современных, исправных автомобилей, а инструкторы помогают освоить не только стандартные экзаменационные маршруты, но и
сложные городские условия.
Собственный оборудованный автодром
Перед выездом в город будущие водители отрабатывают базовые навыки на закрытой площадке:
парковку, эстакаду, змейку и другие элементы, необходимые для сдачи экзамена.
Гибкий график занятий
Мы понимаем, что многие совмещают обучение с работой или учебой, поэтому предлагаем утренние, дневные и вечерние группы, а также
индивидуальный график вождения.
Подготовка к экзамену в ГИБДД
Наши специалисты подробно разбирают типичные ошибки на теоретическом тестировании и практическом экзамене, проводят пробные тестирования и дают
рекомендации по успешной сдаче.
Почему выбирают нас?
Опытные преподаватели и инструкторы с многолетним стажем.
Доступные цены и возможность оплаты
в рассрочку.
Высокий процент сдачи с первого
раза благодаря тщательной подготовке.
Поддержка после обучения – консультации по
вопросам вождения и ПДД.
Автошкола «Авто-Мобилист»
– это не просто курсы вождения,
а надежный старт для безопасного и уверенного управления автомобилем.
Feel free to surf to my web page – Сертификаты
Wow because this is excellent job! Congrats and keep it up.
https://www.lubelska.tv
Nice Webpage, Carry on the wonderful job. Appreciate it.
https://www.korsosanockie.pl
Truly helpful, looking frontward to coming back.
https://www.oto-praca.pl
I like this website – its so usefull and helpfull.
https://laziska.com.pl
Great website! It looks very good! Sustain the helpful work!
https://www.igryfino.pl
I treasure the information on your web site. Thanks.
https://www.oferujemyprace.pl
Wow, stunning portal. Thnx …
https://mojekatowice.pl/
Greetings, good websites you have got presently.
mojegliwice.pl
Wow cuz this is very helpful work! Congrats and keep it up.
https://nasz-szczecin.pl
Love the site– extremely individual friendly and
lots to see!
http:www.koscian.net
Just needed to tell you Now i’m happy that i came onto your webpage!
https://www.tv-slupsk.pl
You’re an extremely practical website; could not make it without ya!
https://www.swiebodzin.tv
What’s happening, awesome websites you’ve got presently.
https://pyskowice.com.pl/
Many thanks, this site is really practical.
https://www.telewizjamazury.pl
Passion the website– really user pleasant and great deals to see!
gwe24.pl
Great internet site! It looks extremely expert! Keep up
the great job!
nowagazeta.pl
Thanks, this website is extremely beneficial.
https://www.debica24.eu
Pretty section of content. I just stumbled upon your blog
and in accession capital to assert that I get 5-star hotel in pattaya fact enjoyed account your blog
posts. Any way I will be subscribing to your feeds and
even I achievement you access consistently rapidly.
I treasure the data on your web site. Kudos!
http://www.tablety.pl
Whoa such a important webpage.
https://mojakruszwica.pl/pl/
Livetotobet adalah platform live totobet sgp dan live totobet singapura tepercaya dengan menggunakan sistem modern, aman dan gampang diakses kapan saja.
Situs ini hadir untuk memberikan pengalaman bermain yang nyaman bagi seluruh member dengan dukungan server stabil dan performa cepat setiap hari
Check out my website livetotobet login
Write more, thats all I have to say. Literally, it seems as though you relied on the video to make your
point. You obviously know what youre talking about, why throw away your intelligence on just posting
videos to your weblog when you could be giving us something enlightening to read?
Also visit my webpage porn
Огромная благодарность за такой полезный
контент. Обязательно порекомендую kazino olimp друзьям.
http://www.dailybbwclips.com/d/out?p=2&id=1637971&c=5&url=https://olimp-casino-prize.kz/signup
hey there and thank you for your info – I’ve definitely picked up something new from right here.
I did however expertise some technical points using this web site, since I experienced to reload the web site lots of times previous to
I could get it to load properly. I had been wondering if your
web hosting is OK? Not that I am complaining, but sluggish loading instances times will often affect your placement in google and could damage your high quality score if
advertising and marketing with Adwords. Anyway I am adding this RSS to my email
and can look out for much more of your respective fascinating
content. Make sure you update this again very soon.
Here is my blog post; Reinigungsfirma
Thanks for the marvelous posting! I truly enjoyed reading it,
you can be a great author.I will make certain to bookmark
your blog and definitely will come back later on.
I want to encourage yourself to continue your great
posts, have a nice evening!
My site; https://okegas123.sceltetop.com/
I have been exploring for a little bit for any high-quality articles or weblog posts
on this kind of space . Exploring in Yahoo I finally
stumbled upon this web site. Studying this
info So i’m glad to convey that I’ve an incredibly good uncanny feeling I found out exactly what
I needed. I such a lot definitely will make certain to do not overlook this site and give it a glance on a continuing basis.
Also visit my web site: 손끝저림
Livetotobet adalah platform live totobet sgp dan live totobet singapura tepercaya dengan menggunakan sistem modern, aman dan gampang diakses kapan saja.
Situs ini hadir untuk memberikan pengalaman bermain yang nyaman bagi seluruh member dengan dukungan server stabil dan performa cepat setiap hari.
My web-site – link alternatif livetotobet
You made some good points there. I looked on the net for more info about the issue and found most people will go along with your views on this web site.
my blog … dickies store las vegas
Sayt çox funksionaldır.
pinco casino az
You have made some good points there. i set homing f&j looked on the web to learn more about the issue and found most individuals will go along with your
views on this web site.
أفلام سكس عربي مصري مترجمة ,سكس عرب نار مثير سكس بنات
هائجة كس ساخن ,زب جامد ممتع جدا ,فيديوهات سكس مترجم باللغة العربية فتيات جميلات تعشق النيك , فيديو سكس نار
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now
each time a comment is added I get several emails with the same comment.
Is there any way you can remove people from that service?
Thanks a lot!
my website; nadeem majdalany pandoras box
I like reading an article that can make men and women think.
Also, many thanks for permitting me to comment!
Look into my web blog: slon3 cc
Hi there, its pleasant post concerning media print, we all
be familiar with media is a wonderful source of information.
Also visit my website – Hashtag Kalakar is a genuine platform
Your style is unique in comparison to other people I’ve read
stuff from. Many thanks for posting when you have the opportunity,
Guess I’ll just book mark this site.
Feel free to surf to my web-site: web aktüel
Cabvinet IQ
8305 Ꮪtate Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Innovation
This info is invaluable. Where can I find out more?
Also visit my blog post; vpn for slot games
I every time used to study post in news papers but now as I
am a user of net therefore from now I am using net for content, thanks
to web.
Feel free to visit my web-site – escort luxembourg
This is my first time visit at here and i am genuinely impressed to read everthing at one place.
My site :: 해외선물 글로벌시장
Its like you read my thoughts! You appear to know so
much about this, like you wrote the book in it or something.
I think that you just could do with a few percent to drive
the message house a bit, however instead of that, this is wonderful blog.
A great read. I’ll definitely be back.
Here is my web blog 비아그라 시알리스 차이
This piece of writing will help the internet users for creating new webpage or even a weblog from start to end.
Take a look at my homepage – PXJ
I have been surfing online more than 3 hours as of late, yet I by
no means discovered any fascinating article like yours. It is pretty worth sufficient for me.
In my view, if all site owners and bloggers made just right content as you probably did, the internet
will probably be much more useful than ever before.
Take a look at my web page: PXJ
We have been helping Canadians Get a loan against my car for repair Against Their Vehicle for
Repairs Since March 2009 and are among the very few Completely Online Lenders In Canada.
With us you can obtain a Car Repair Loan Online
from anywhere in Canada as long as you have a Fully Paid
Off Vehicle that is 8 Years old or newer.
We look forward to meeting all your financial needs.
Cabinet IQ
8305 Տtate Hwy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Uniqueinteriors
Great article.
Feel free to visit my webpage :: https://www.seoclerk.com/Link-Building/476754/270-High-Authority-links-DA-45-to-99-2-tiered-from-160-domains
Many thanks really beneficial. Will certainly share site with my pals.
https://www.telewizjamazury.pl
Appreciate the recommendation. Let me try it out.
Feel free to visit my web blog :: gay porn
You have got astonishing knowlwdge these.
https://www.mojebielsko.pl
Thank you for sharing this excellent web site.
https://www.dziennikpowiatowy.pl
It’s a shame you don’t have a donate button! I’d
certainly donate to this outstanding blog! I guess for now
i’ll settle for book-marking and adding your RSS feed to my Google account.
I look forward to fresh updates and will talk about this blog
with my Facebook group. Talk soon!
my blog :: 강남텐카페
Thanks very handy. Will share website with my pals.
https://naszepiaseczno.pl
Basically wished to point out I am just grateful
I came on the site!
https://www.gazetamiedzyszkolna.pl
Merely had to point out I’m just ecstatic I came
onto your internet page.
https://jakiwniosek.pl/
Thanks extremely practical. Will certainly share site with my good friends.
https://laziska.com.pl
Thanks, this site is extremely helpful.
https://orzesze.com.pl
Sustain the amazing job !! Lovin’ it!
https://www.polskibiznes24.pl
Fantastic site you possess here.
https://www.polskibiznes.info
Hi there, nice site you’ve right now.
https://mojmikolow.pl
You have one of the greatest internet websites.
https://www.oto-praca.pl
I benefit from browsing your web sites. Many thanks!
https://www.korsosanockie.pl
You have got among the best online sites.
https://lubliniec365.pl
Sustain the spectacular work !! Lovin’ it!
https://www.tc.ciechanow.pl
Hi there, cool websites you have in here.
https://warszawa24.ovh
Maintain the great job and bringing in the crowd!
https://www.mttv.pl
Just simply had to emphasize I’m just happy that i came on the
web site.
iszczecinek.pl
Superb Web site, Keep up the excellent work. Thanks!
https://testoria.pl/
I love this site – its so usefull and helpfull.
https://www.lokalnatelewizja.pl
thank so much for your internet site it helps a great deal.
https://www.nowydzwon.pl
Many thanks, this website is really beneficial.
https://www.ta-praca.pl
You’re a very useful website; couldn’t make it without ya!
https://www.telewizjamazury.pl
How are you, tidy internet site you have right now.
https://www.telewizjamazury.pl
You’ve gotten good info listed here.
https://nolesnica.pl
Truly….such a important web site.
https://www.gazetamiedzyszkolna.pl
Hi! This post couldn’t be written any better! Reading this post reminds me of my
previous room mate! He always kept chatting about this.
I will forward this write-up to him. Pretty sure he will have a good read.
Many thanks for sharing!
my web-site :: 부비
thank so considerably for your website it helps a lot.
https://www.kopalniapracy.pl
You’ve got possibly the best internet websites.
http:skarzysko24.pl
Thanks extremely handy. Will share site with my buddies.
https://www.kwidzyn1.pl
Wow, such a good webpage.
https://www.polskapraca.info
The material is incredibly interesting.
https://tc.ciechanow.pl
Thanks meant for supplying such well put together
content material.
https://czas.tygodnik.pl
What’s up i am kavin, its my first time to commenting anyplace, when i read this article i
thought i could also make comment due to this brilliant post.
Here is my webpage: low-noise amplifier
Exceptionally user friendly website. Immense info readily available on few clicks.
https://www.kopalniapracy.pl
You’ve gotten awesome knowlwdge on this web-site.
https://www.tvsudecka.pl
Thanks with regard to delivering these awesome data.
https://laziska.com.pl
Love the website– really individual friendly and whole lots to
see!
https://www.telewizjazary.pl
Basically wanted to emphasize I am just lucky I happened in your website.
rudaslaska.com.pl
Wow, stunning portal. Thnx …
https://www.praca-biznes.pl
How are you, cool websites you’ve got there.
https://www.zvami.tv
How goes it, good websites you’ve here.
https://www.swiebodzin.tv
Incredibly educational look frontward to coming back.
https://nysainfo.pl
Maintain the good job and producing in the
crowd!
https://www.tvsudecka.pl
Thanks with regard to giving these sort of superior post.
https://www.tvobiektyw.pl
Quite insightful….looking forwards to visiting again.
https://metropoliabydgoska.pl
Great looking web site. Think you did a lot of your very own coding.
https://silesia.info.pl/
Many thanks really beneficial. Will certainly share website with my friends.
https://www.lokalnatelewizja.pl
Wow because this is great work! Congrats and keep it up.
https://nasz-szczecin.pl
I like perusing your website. Kudos!
https://www.pilska.tv
Astonishingly individual pleasant website.
Great info readily available on couple of clicks.
https://www.extra-plonsk.pl
You’ve gotten possibly the best internet websites.
https://www.mttv.pl
Simply just had to say Now i am delighted I happened
on the web site.
https://nasz-szczecin.pl
Maintain the good job and generating the group!
https://www.mojebielsko.pl
Wow, attractive portal. Thnx …
https://www.lubelska.tv
Ahaa, its pleasant discussion regarding this paragraph here at this website, I have read all that, so at
this time me also commenting here.
Look at my webpage bigpot88 daftar
Sustain the outstanding work !! Lovin’ it!
https://www.tvsudecka.pl
Hello, nice web-site you possess in here.
https://koscierski.info
I adore this website – its so usefull and helpfull.
https://orzesze.com.pl
Keep up the outstanding work !! Lovin’ it!
https://www.ebrodnica.pl
Thanks really handy. Will share site with my buddies.
mojchorzow.pl
I adore this site – its so usefull and helpfull.
https://warszawa24.ovh
Thanks very beneficial. Will certainly share website with my good friends.
https://wrzesnia.info.pl/pl/
You’re a really helpful site; couldn’t make it without ya!
https://www.ta-praca.pl
Wow cuz this is great work! Congrats and keep it up.
https://www.jawor.tv
Passion the site– very individual friendly and whole lots to see!
https://www.praca-biznes.pl
Many thanks! This is definitely an astonishing
online site.
https://www.pewnybiznes.info
say thanks to so a lot for your internet site it helps a
whole lot.
https://www.oferujemyprace.pl
Sustain the remarkable job !! Lovin’ it!
https://www.oto-praca.pl
You have got very good info in this article.
https://gle24.pl/pl/
You have got among the best web-sites.
https://ekutno.pl
Wow, lovely portal. Thnx …
https://www.polskapraca.info
Maintain the outstanding work !! Lovin’ it!
https://www.oto-praca.pl
Simply wished to point out Now i’m delighted I happened onto your
site!
https://www.tvsudecka.pl
You’re a very helpful internet site; couldn’t make it without ya!
https://metropoliabydgoska.pl
Really, this is a handy websites.
swiecie24.pl
Really insightful….look forward to coming back again.
https://nasz-szczecin.pl
Excellent blog here! Also your web site loads up fast! What host are you using?
Can I get your affiliate link to your host? I wish my web site loaded up as quickly as yours lol
my site menangclub88 apk
You’ve one of the best sites.
https://www.pewnybiznes.info
Wow, this is a advantageous webpage.
https://www.lubelska.tv
You really make it seem so easy with your presentation but I find this matter to be actually something which I think
I would never understand. It seems too complex and very broad for me.
I’m looking forward for your next post, I’ll try to get the hang of it!
Feel free to visit my website; menangclub88 rtp
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Stаtеs
254-275-5536
Urban [Wendy]
Feel free to surf to my page; Highstakes login
1xbet зеркало, 1хбет официальный сайт позволяет возможность участвовать даже при неудобствах.
I don’t even understand how I ended up right here, however I believed this put up was good.
I do not recognize who you might be but certainly you’re
going to a well-known blogger in case you are not already.
Cheers!
My webpage: slon2.to
официальный сайт 1xbet, 1xbet предлагает
разнообразный выбор игр на спорт.
my blog post: https://1xbet-x2fzi.sbs/
I am not positive the place you’re getting your information, however good topic.
I must spend a while finding out more or figuring out more.
Thank you for magnificent information I used to be searching for this information for my mission.
Also visit my page :: 부산호빠
This is a very good tip particularly to those new
to the blogosphere. Simple but very accurate info… Many thanks for sharing this
one. A must read article!
Have a look at my blog … let’s play
My brother recommended I might like this web site. He was entirely right.
This post truly made my day. You can not imagine just how much time I had spent for this info!
Thanks!
My web page; koi toto
magnificent points altogether, you simply received a emblem new
reader. What might you suggest in regards to your post that you just made some days ago?
Any positive?
Take a look at my page … bigpot88 login
Hello to all, for the reason that I am actually eager
of reading this web site’s post to be updated daily.
It contains nice information.
Here is my blog post; https://naruto88.sceltetop.com/
Check out my blog … Hacksaw Gaming slot RTP list & FAQs
Hi-ya, nice site you’ve right now.
https://www.swiebodzin.tv
Highly interesting….look onward to visiting again.
https://www.ta-praca.pl
Regards for sharing this good webpage.
https://www.polskapraca.info
Appreciation to my father who informed me on the topic of this
website, this blog is genuinely amazing.
my page แทงบอลโลก
Maintain the remarkable work !! Lovin’ it!
https://izyrardow.pl
Thanks a ton for sharing your terrific web-site.
https://www.kronikatygodnia.pl
I benefit from looking at your websites. Appreciate it!
https://www.gazetamiedzyszkolna.pl
Great looking web site. Think you did a lot of your very own html coding.
https://www.gazetamiedzyszkolna.pl
Howdy, awesome web page you’ve gotten right now.
m-ce.pl
Passion the site– really individual friendly
and great deals to see!
https://www.placpigal.pl
Thanks pertaining to giving many of these great information.
https://www.praca-biznes.pl
With thanks for sharing your great site.
https://wolomin24.com
Excellent goods from you, man. I have understand your stuff
previous to and you’re just extremely fantastic. I really like what you have acquired
here, certainly like what you’re stating and the way
in which you say it. You make it entertaining and you still take care of to keep it smart.
I can not wait to read far more from you.
This is really a wonderful website.
Feel free to surf to my web blog; cabin crew training
Great internet site! It looks extremely expert! Keep up the good work!
https://www.telewizjamazury.pl
Pretty insightful, looking onward to coming back.
https://www.tvsudecka.pl
Love the site– extremely individual friendly and lots to see!
https://warszawa24.ovh
Thanks a lot! It is an outstanding online site.
https://extrawalcz.pl
Extremely user friendly website. Enormous info readily available
on few clicks.
https://nizanskie.info/pl/
thank a lot for your site it assists a whole lot.
https://zory.com.pl/
Astonishingly user friendly site. Great info readily available on couple of
clicks on.
https://www.tvzachod.pl
Maintain the outstanding job !! Lovin’ it!
https://ibielsk.pl
Just wanted to stress I am grateful that i came onto your website!
https://www.tvsudecka.pl
Great website! It looks very good! Maintain the great work!
https://www.ta-praca.pl
I treasure the details on your site. Regards.
https://www.kopalniapracy.pl
I adore this website – its so usefull and helpfull.
https://www.kopalniapracy.pl
You have got probably the greatest online websites.
https://www.tvsudecka.pl
I like this site – its so usefull and helpfull.
https://www.praca-biznes.pl
Many thanks, this website is really practical.
https://www.igryfino.pl
Thanks meant for providing this sort of amazing content.
https://mlodagdynia.pl/pl/
Extremely user friendly website. Enormous details readily available on few gos to.
https://jg24.pl/
You’ve wonderful info on this site.
https://www.tv.starachowice.pl
You’re a very helpful website; couldn’t make it without
ya!
https://zyciesiedleckie.pl/pl/
I benefit from checking your web sites. Appreciate it!
https://www.praca-biznes.pl
Wow! This blog looks just like my old one! It’s on a completely different subject but it has pretty much
the same layout and design. Outstanding choice of colors!
Visit my homepage :: We Will Rock You – Queen – Heavy Metal
Hey There. I found your blog using msn. This is a very well written article.
I will be sure to bookmark it and return to read more of your useful info.
Thanks for the post. I will definitely return.
Look into my site: bigpot88 daftar
Seriously, this is a handy webpage.
https://www.polskapraca.info
Seriously, such a valuable webpage.
https://krakow-atrakcje.pl
Very good web-site you have here.
https://www.mojebielsko.pl
Wow cuz this is excellent job! Congrats and keep it up.
https://www.zvami.tv
thnx for sharing your terrific web page.
https://www.extra-plonsk.pl
Many thanks really useful. Will share website with my friends.
https://www.ebrodnica.pl
I treasure the content on your web sites. Thank you so much!
https://www.nowytydzien.pl
Thanks really valuable. Will certainly share website with my buddies.
https://nasz-szczecin.pl
Passion the site– extremely individual friendly and whole lots to see!
https://radomsko24.pl
1xbet зеркало, 1xbet позволяет игрокам получить доступ к своему аккаунту, без учета блокировок.
Feel free to surf to my web blog :: 1xbet-8lhj3.cyou
Sustain the outstanding job !! Lovin’ it!
https://www.lubelska.tv
You have terrific stuff in this article.
siemianowice.net.pl
You’re a really beneficial website; couldn’t make it without ya!
https://www.gazetamiedzyszkolna.pl
Maintain the outstanding job !! Lovin’ it!
https://orzesze.com.pl
Maintain the exceptional job !! Lovin’ it!
https://www.oferujemyprace.pl
Wow, lovely portal. Thnx …
https://www.telewizjaolsztyn.pl
Many thanks! It a amazing web site.
https://orzesze.com.pl
Appreciate it for sharing this cool website.
https://www.ebrodnica.pl
You’re a really practical web site; couldn’t make it without ya!
https://zabrze.com.pl/
thank so considerably for your website it helps a whole
lot.
https://www.kariera24.info
You’re a very valuable internet site; could not make it without ya!
https://czas.tygodnik.pl
Great website! It looks extremely good! Keep up the good job!
https://www.tvzachod.pl
Great internet website! It looks really expert! Keep up the excellent work!
https://www.kwidzyn1.pl
Great looking website. Presume you did a great deal
of your very own html coding.
https://www.kopalniapracy.pl
Sustain the incredible job !! Lovin’ it!
https://www.tv.starachowice.pl
You’ve got amazing info right.
https://www.polskibiznes.info
This website was… how do you say it? Relevant!! Finally I have found something which helped me.
Thanks a lot!
Also visit my webpage :: click here
You should take part in a contest for one of the finest sites online.
I am going to highly recommend this site!
my web blog … ai video generator no restrictions
Incredibly user pleasant website. Enormous info offered on couple
of clicks on.
https://warszawa24.ovh
Many thanks! It is definitely an superb online site!
https://www.oto-praca.pl
osxfsg
Great internet site! It looks extremely good! Keep up the helpful work!
https://www.polskibiznes.info
I have to thank you for the efforts you’ve put in penning
this blog. I’m hoping to view the same high-grade content from you later on as well.
In truth, your creative writing abilities has encouraged me to get my very own website now ;)
Feel free to surf to my homepage :: nm9
Good day, well put together web site you have at this time there.
https://iotwock.info
Thanks a bunch! This a great web-site!
https://www.mojebielsko.pl
I delight in the knowledge on your site. Thanks a ton!
https://www.tvobiektyw.pl
Superb internet site you’ve gotten going here.
https://www.placpigal.pl
The material is quite fascinating.
https://www.ta-praca.pl
Normally I do not read post on blogs, however I wish to say that
this write-up very forced me to take a look at and do so!
Your writing style has been amazed me. Thanks, very great post.
Feel free to surf to my website :: menangclub88 apk
You have the most impressive web pages.
https://esopot.pl
Many thanks, this site is really handy.
https://krakow-atrakcje.pl
Simply just wanted to stress Now i am grateful I happened in your web
page.
https://www.kopalniapracy.pl
Your info is rather important.
https://www.ebrodnica.pl
You’re a very practical site; couldn’t make it without ya!
mojetychy.pl
The stuff is extremely interesting.
https://www.praca-biznes.pl
Excellent Web site, Preserve the good job. Regards!
https://www.polskibiznes24.pl
Thanks extremely valuable. Will certainly share website with my good friends.
https://www.malbork1.pl
Exceptionally user pleasant site. Great information available on few clicks on.
https://www.kronikatygodnia.pl
Thanks, this website is really valuable.
https://piekaryslaskie.com.pl/
Love the site– very individual pleasant and whole lots
to see!
https://krakow-atrakcje.pl
Excellent Website, Carry on the good job. With thanks.
https://www.telewizjaolsztyn.pl
Hi! I know this is kind of off topic but I was wondering if you knew where I could find a captcha
plugin for my comment form? I’m using the same blog platform as yours and I’m having trouble
finding one? Thanks a lot!
My web page: r
You’ve one of the greatest web sites.
https://www.telewizjamazury.pl
I like perusing your website. Appreciate it!
ki24.info
Thanks for the purpose of providing this type of well put
together post.
https://www.kurier-lokalny.com
Love the website– extremely individual pleasant and
great deals to see!
https://koscierski.info
You’re a very helpful internet site; couldn’t make it without ya!
bielsko.biala.pl
Thanks a ton! It a terrific online site.
https://www.polskibiznes24.pl
Maintain the great work and bringing in the crowd!
http://www.gorzow24.pl
Great looking web site. Presume you did a great deal of your own html
coding.
https://www.nowydzwon.pl
Very good web page you have there.
https://www.tvsudecka.pl
Great internet site! It looks really expert! Keep up the excellent job!
https://www.kariera24.info
Wow, attractive portal. Thnx …
https://www.debica24.eu
Thanks intended for offering these sort of fantastic articles.
https://www.telewizjazary.pl
Good answers in return of this matter with genuine arguments and telling
everything on the topic of that.
My web blog :: okc dodgers team store
Awesome blog! Is your theme custom made or did you download it from somewhere?
A theme like yours with a few simple adjustements would really make my blog
shine. Please let me know where you got your theme. Thank you
My site – crowdfunding imobiliário
Thanks for sharing your thoughts about transfer
pricing solutions in dubai. Regards
My web-site; transfer pricing service dubai
Amazing site you’ve gotten in here.
https://www.ta-praca.pl
You’ve got great stuff in this case.
https://radio5.com.pl/
Great looking site. Presume you did a lot of your very own html coding.
https://www.ta-praca.pl
You have the most impressive webpages.
https://www.polskibiznes24.pl
Thanks really useful. Will share website with my good friends.
https://ibielsk.pl
Great internet site! It looks very professional! Sustain the great
work!
https://tugrodzisk.pl
Artikel yang sangat menarik dan informatif. Banyak pengguna di Indonesia mencari informasi terpercaya tentang viagra indonesia dan kesehatan pria.
Konten seperti ini sangat membantu pembaca memahami penggunaan yang aman dan efektif.
Terima kasih atas artikel yang bermanfaat ini. Topik viagra
indonesia memang banyak dicari saat ini, terutama bagi mereka yang ingin mendapatkan informasi kesehatan pria secara aman dan tepat.
Konten yang bagus dan mudah dipahami. Informasi mengenai viagra
indonesia sangat relevan dan membantu banyak orang mendapatkan edukasi yang benar tentang kesehatan pria.
You’re an extremely valuable site; couldn’t make it without ya!
https://infoskierniewice.pl
I appreciate perusing your websites. Cheers!
https://www.kurier-lokalny.com
Wow, stunning portal. Thnx …
https://www.korsosanockie.pl
Awesome Webpage, Stick to the good job. Thanks a lot!
https://www.lubelska.tv
Extremely individual friendly site. Tremendous information available on few gos to.
https://www.tc.ciechanow.pl
Seriously this is a useful internet site.
https://www.mojebielsko.pl
Great looking site. Think you did a great deal of your very own coding.
https://www.dziennikpowiatowy.pl
I love the content on your website. Kudos!
https://www.mojebielsko.pl
Wow cuz this is excellent job! Congrats and keep it up.
https://izyrardow.pl
Love the website– really individual pleasant and whole
lots to see!
https://www.tvsudecka.pl
Great website! It looks very expert! Sustain the excellent job!
https://naszepiaseczno.pl
You’re a really valuable internet site; couldn’t make it without ya!
https://www.ta-praca.pl
Thanks a bunch! It is definitely an amazing site.
https://www.kurier-lokalny.com
Sustain the incredible job !! Lovin’ it!
https://www.instalki.pl/
Much thanks! This a very good web page.
https://www.placpigal.pl
I like this website – its so usefull and helpfull.
https://myszkow365.pl
Wow cuz this is excellent work! Congrats and keep it up.
www
You have one of the better online sites.
https://www.pewnybiznes.info
Wow, lovely site. Thnx …
https://www.oferujemyprace.pl
Many thanks, this website is extremely valuable.
https://www.debica24.eu
Wow! Finally I got a weblog from where I can actually obtain helpful information regarding my study and knowledge.
Feel free to visit my page P999
We recognize the value of your time, which is why we have incorporated a
Turbo Mode feature into Easy Videos Downloader.
my webpage – ubah video jadi mp4; https://savefrom.co.id/convert-to-mp4,
Modern Purair
416 Meridian Ꭱԁ SE #14A, Calgary
AB T2Ꭺ 1X2, Canada
(403) 800-7254
indoor Monitor
Wonderful blog! I found it while searching on Yahoo News.
Do you have any suggestions on how to get listed
in Yahoo News? I’ve been trying for a while but I never seem to get
there! Thanks
Also visit my website :: trust wallet apk
Hello mates, nice piece of writing and fastidious urging
commented at this place, I am in fact enjoying by these.
my web-site; Techtra Automotive College Malaysia
I think the admin of this web site is truly working hard for his
web site, as here every information is quality based material.
my blog post: bookkeeping services in dubai
Guardium
Капсулы Guardium разработаны с использованием передовых биотехнологий.
Их состав представляет собой эффективное сочетание экстрактов растений,
витаминов и активных биофлавоноидов, которые способствуют полному уничтожению паразитов на всех этапах их жизненного цикла – начиная от яиц и заканчивая половозрелыми особями.guardium состав
pinup официальный сайт вход
актуальное зеркало
Hello there, just became alert to your blog through Google, and
found that it’s truly informative. I’m going to watch out for brussels.
I will be grateful if you continue this in future. Numerous people will be benefited from your writing.
Cheers!
Here is my blog: Snipaste 退出快捷键
Great article. I’m going through many of these
issues as well..
my webpage; agoda88
пинап официальный сайт
вход
Unquestionably consider that that you stated.
Your favorite justification appeared to be on the web the easiest thing to take into accout of.
I say to you, I certainly get irked whilst people consider concerns that they plainly do not recognise about.
You managed to hit the nail upon the highest and outlined
out the entire thing with no need side effect , other people
can take a signal. Will probably be back to get more.
Thanks
Feel free to surf to my blog … winbdgg
This post will assist the internet viewers
for creating new web site or even a weblog from start to end.
Also visit my homepage :: CU1 file extension reader
This website definitely has all the information and facts I wanted about this subject and didn’t know who to ask.
My website: אורן פלוטקין
What a stuff of un-ambiguity and preserveness of valuable familiarity regarding unpredicted feelings.
Feel free to visit my website – cialis
Hey there! I’m at work surfing around your blog from
my new apple iphone! Just wanted to say I love reading through your blog
and look forward to all your posts! Keep up the excellent work!
my blog; tripscan вход
SculpSure takes the contrary technique, using regulated warm to accomplish its outcomes.
my web page homepage (Caren)
This is a topic which is near to my heart…
Thank you! Exactly where are your contact details though?
My blog; mgmarket6 at
bookmarked!!, I love your blog!
Here is my web-site: cervo media group
Keep on writing, great job!
My page: ads pepek
When some one searches for his necessary thing, thus he/she needs to be available
that in detail, so that thing is maintained over here.
my web page … Snipaste 快捷键
Hello! I know this is kinda off topic but I was wondering which blog platform are
you using for this site? I’m getting tired of WordPress because
I’ve had problems with hackers and I’m looking at options for another platform.
I would be great if you could point me in the direction of
a good platform.
My web site; Scott McRobie New Zealand
Hello mates, good post and fastidious arguments commented at
this place, I am genuinely enjoying by these.
Here is my blog post :: nonton bola online
It’s appropriate time to make some plans for the future and it is time to be happy.
I’ve read this post and if I could I desire to suggest you few interesting things or
tips. Maybe you can write next articles referring to this article.
I wish to read more things about it!
My blog: Dewanalo
I am really enjoying the theme/design of your web site.
Do you ever run into any web browser compatibility problems?
A few of my blog visitors have complained about my blog not operating correctly in Explorer but looks great in Safari.
Do you have any tips to help fix this problem?
Also visit my web site – bokep ibu ibu Indonesia
Hi it’s me, I am also visiting this site on a regular
basis, this web page is really nice and the viewers
are really sharing pleasant thoughts.
My page: read more
Great blog! Do you have any helpful hints for aspiring writers?
I’m planning to start my own website soon but I’m a little lost on everything.
Would you advise starting with a free platform like WordPress or go for a paid
option? There are so many choices out there that
I’m totally confused .. Any suggestions? Many thanks!
Here is my homepage: neural networks
Hello just wanted to give you a quick heads up. The text in your content
seem to be running off the screen in Firefox. I’m not sure if
this is a formatting issue or something to do with internet
browser compatibility but I thought I’d post to let you know.
The design look great though! Hope you get the issue
fixed soon. Thanks
my homepage 부산호빠
But if you have used Tiktok before, are you willing to download the SSSTIK TikTok Downloader videos?
Excellent way of explaining, and fastidious piece of writing to
take data concerning my presentation subject, which i am going
to deliver in academy.
Here is my blog post; view more
Thanks for sharing your thoughts on 대구오피.
Regards
Hi there to every body, it’s my first visit of this blog;
this web site carries amazing and actually excellent material in favor of visitors.
Here is my web blog: evisa egypt for vietnamese
What’s Going down i’m new to this, I stumbled upon this I have discovered It positively useful
and it has helped me out loads. I am hoping
to contribute & help different users like its aided me.
Good job.
Feel free to visit my blog 爱思助手pc官网
With havin so much written content do you ever run into any problems of plagorism
or copyright violation? My website has a lot of unique content I’ve either created
myself or outsourced but it looks like a lot of it is popping it
up all over the web without my permission.
Do you know any ways to help prevent content from being ripped off?
I’d truly appreciate it.
Look into my website; secure casino vpn
I am sure this post has touched all the internet viewers, its
really really good article on building up new blog.
Feel free to surf to my page; SEW file extension
my homepage: Fazi Slots & RTP guide
Simply want to say your article is as amazing. The clearness in your post is
simply great and i can assume you’re an expert on this subject.
Well with your permission let me to grab your feed to keep updated with forthcoming post.
Thanks a million and please carry on the gratifying work.
Also visit my website :: Lunatogel
Modern Purair
416 Meridian Rd ЅE #14A, Calgary
AB T2Ꭺ 1X2, Canada
(403) 800-7254
Bookmarks
I used to be able to find good advice from your
blog articles.
Feel free to surf to my homepage; buy
Wonderful web site. Plenty of helpful info here. I’m sending it to a few friends ans
additionally sharing in delicious. And certainly, thank you for your effort!
Here is my page … viagra indonesia
We recognize the value of your time, which is why we
have incorporated a Turbo Mode feature into Easy Videos Downloader.
Also visit my website … завантажити відео
I got this web site from my friend who informed me on the topic of this web page and now this time
I am browsing this website and reading very informative content at
this place.
my website; warpzone marketplace
I know this if off topic but I’m looking into starting my own blog and was curious what all is required to
get set up? I’m assuming having a blog like yours would cost a pretty
penny? I’m not very internet savvy so I’m not 100% certain. Any recommendations or
advice would be greatly appreciated. Cheers
Feel free to surf to my web page :: holiday rental management Cape Town
Howdy! This is my first visit to your blog! We
are a team of volunteers and starting a new initiative in a community in the
same niche. Your blog provided us beneficial information to work on.
You have done a outstanding job!
Look into my web site – Dewapoker
Wow, that’s what I was exploring for, what a material!
present here at this web site, thanks admin of this site.
Check out my web page – 爱思助手官网
Howdy! This is my 1st comment here so I just wanted to give a quick
shout out and say I really enjoy reading your posts. Can you
suggest any other blogs/websites/forums that cover the
same subjects? Many thanks!
Look into my web-site – https://lu88a.sa.com/
Modern Purair
416 Meridian Ꮢɗ SᎬ #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
duct care (wakelet.com)
Howdy would you mind letting me know which webhost you’re utilizing?
I’ve loaded your blog in 3 different browsers and I must
say this blog loads a lot faster then most. Can you suggest a good hosting provider at a honest price?
Thank you, I appreciate it!
Here is my webpage; Hitclub
The other day, while I was at work, my sister stole my apple ipad and tested to see if it can survive a twenty five foot drop, just so she
can be a youtube sensation. My iPad is now destroyed and she has 83 views.
I know this is totally off topic but I had to share it with someone!
My webpage Batman138
Greate pieces. Keep writing such kind of info on your site.
Im really impressed by your site.
Hi there, You have done an excellent job. I’ll certainly digg it and in my view
suggest to my friends. I am sure they will be benefited from
this website.
my web site: zelensky02
An intriguing discussion is worth comment. I do think that
you should publish more on this subject, it might not be a taboo
subject but typically folks don’t speak about such topics.
To the next! Best wishes!!
Review my homepage: zelensky01
I would like to thank you for the efforts you’ve put in writing this blog.
I really hope to see the same high-grade content by you in the future as well.
In truth, your creative writing abilities has encouraged me
to get my very own blog now ;)
My page: Soluciones tecnológicas para el hogar
What’s up, for all time i used to check webpage posts here in the early hours in the daylight, because i enjoy to gain knowledge
of more and more.
my web-site … tripscan
I constantly spent my half an hour to read this web site’s articles or
reviews daily along with a cup of coffee.
Also visit my website: jepang qq
great issues altogether, you simply received a new reader.
What might you suggest about your post that you made a few days in the past?
Any sure?
Here is my blog: best real time translator earbuds 2026
Kazino ilə bağlı ipucu çox faydalıdır.
Pinco Casino onlayn oyunlar
I every time used to read piece of writing in news papers but now as I am a user
of web thus from now I am using net for content, thanks to web.
my page homepage
When I initially left a comment I seem to have clicked on the -Notify me
when new comments are added- checkbox and now every time a
comment is added I recieve four emails with the exact same comment.
Is there an easy method you are able to remove me from that
service? Many thanks!
Here is my web page; free booting website
youtube downloader video indirme programları arasından en çok kullanılanlardan biri de iTubeGo‘dur.
Pretty part of content. I simply stumbled upon your weblog and
in accession capital to say that I get actually enjoyed account
your blog posts. Any way I will be subscribing for your feeds
and even I achievement you get entry to constantly rapidly.
Feel free to visit my blog post Extra resources
What’s up, after reading this remarkable piece of writing i am also cheerful to share my familiarity here with friends.
Also visit my homepage :: 雷電模擬器
It’s actually a cool and useful piece of info.
I’m glad that you shared this useful information with us.
Please stay us up to date like this. Thanks for sharing.
Also visit my web site :: คลิปหลุดxxx
I just could not depart your website prior to suggesting that I actually enjoyed the usual information a
person supply to your visitors? Is gonna be back frequently to check out new posts
Look at my homepage … freedom of press
Visit my webpage: all evoplay Games in one place
Good day! I just would like to give you a big thumbs up for the great information you have here on this post.
I am returning to your website for more soon.
Look at my web page poker site rankings
hello there and thank you for your information – I have
definitely picked up something new from right here.
I did however expertise several technical points using this site, since I experienced to reload the website lots
of times previous to I could get it to load properly.
I had been wondering if your hosting is OK? Not that
I am complaining, but slow loading instances times will sometimes affect
your placement in google and could damage your quality score
if ads and marketing with Adwords. Well I am adding this RSS to my e-mail and could look out for much more of your respective fascinating content.
Ensure that you update this again soon.
Feel free to visit my homepage bokep anime bahasa indonesia
I’ve been exploring for a little for any high quality articles or weblog posts on this
kind of house . Exploring in Yahoo I ultimately stumbled upon this site.
Reading this information So i’m glad to show that I have a very excellent uncanny feeling
I came upon just what I needed. I most indisputably
will make sure to do not put out of your mind this website and give it a glance on a relentless
basis.
My page :: NHÀ CÁI UY TÍN
I have read so many posts concerning the blogger lovers but this post
is actually a fastidious paragraph, keep it up.
my blog :: kra33 at
For most recent news you have to visit internet and on the web I found this web site as a finest web site for most up-to-date updates.
My page … what is electric cable (Mikayla)
Modern Purair
416 Meridian Rd ЅE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
quality safety
You are a very smart person! :)
Сайт работает стабильно и быстро загружается
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m10413—uns/folga-magnievaya-m10413—uns/
My homepage :: highstakes casino Download
Hi there! I’m at work surfing around your blog from
my new apple iphone! Just wanted to say I love reading your blog
and look forward to all your posts! Keep up the great work!
Feel free to visit my blog Tõeline Juhtmevaba
I think that may be an interesting element, it made me assume a bit. Thanks for sparking my considering cap. On occasion I get so much in a rut that I simply really feel like a record.
I was recommended this website by my cousin. I’m not sure whether this post
is written by him as nobody else know such detailed about my problem.
You’re incredible! Thanks!
My site; webpage
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-350kh500-mm-ls/
Ориентация на долгосрочные отношения с клиентами позволяет компании формировать индивидуальные условия оплаты и графики поставок.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-10g2s1-1-5x2000x2000-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-40b—gost-19807-91/izdeliya-iz-titana-40b—gost-19807-91/
My blog: Spadegaming Slots & rtp Guide
continuously i used to read smaller articles which also clear their motive, and that is also
happening with this article which I am reading at this place.
Also visit my blog post 爱思助手官网下载
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-35l-24x1300x1500-gost-19903-2006-gladkii-belyi-goriachekatanyi/
This design is incredible! You definitely know how to keep a reader amused.
Between your wit and your videos, I was almost moved to start my own blog (well,
almost…HaHa!) Fantastic job. I really loved what you had to say,
and more than that, how you presented it. Too cool!
My blog Pawbiotix
Excellent post. I used to be checking continuously this blog and I’m inspired!
Very useful information specifically the final section :)
I care for such info much. I was looking for this certain info for a very lengthy
time. Thanks and best of luck.
Feel free to visit my page … трип скан
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-70kh100-mm-lmtss/
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/mishmetall/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Tailoredservice
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-tsm4605-1/polosa-molibdenovaya-tsm4605/
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-20g-8x1100x1200-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Hi there would you mind sharing which blog platform you’re working with?
I’m going to start my own blog soon but I’m having a hard time
selecting between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design seems different then most
blogs and I’m looking for something unique.
P.S My apologies for being off-topic but I had to ask!
Also visit my page … SpinsinoCasino
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mo-cu50-1/truba-molibdenovaya-mo-cu50/
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-80kh300-mm-lmtssk/
We have been helping Canadians Get a Loan borrow money against my car for repair Their Vehicle for Repairs Since
March 2009 and are among the very few Completely Online Lenders
In Canada. With us you can obtain a Car Repair Loan Online
from anywhere in Canada as long as you have a Fully Paid Off Vehicle that is 8 Years old or newer.
We look forward to meeting all your financial needs.
For most recent information you have to pay a visit internet and
on web I found this web page as a best web site for newest updates.
Feel free to visit my web site; webpage
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-45-gradusov-80-mm-m2t-gost-r-52948-2008/
I love it whenever people come together and share views.
Great blog, continue the good work!
My site: https://haarmoderina.nl/
Good day! This is my 1st comment here so I just wanted to give a quick shout out and say I genuinely enjoy
reading through your posts. Can you suggest any other
blogs/websites/forums that go over the same subjects? Thank you!
Take a look at my web site; Topwd
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/plity/plita-4kh2v5mf-25x320x250-gost-19903-74/
This is a great tip particularly to those fresh to the blogosphere.
Short but very accurate information… Thanks for sharing
this one. A must read article!
Here is my web site; HK DeepSeek
Возможность заказа продукции в розницу и оптом (судя по описанию)
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-qe22—csa-hg-9/poroshok-magnievyy-qe22—csa-hg-9/
География деятельности компании охватывает всю территорию России, обеспечивая металлом предприятия в удаленных регионах.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-90kh90kh8-mm-c45e-din-59370/
If some one wants to be updated with latest technologies after that
he must be visit this site and be up to date all the time.
Also visit my web blog 爱思助手下载
Оперативная логистика и поддержка на всех этапах сделки позволяют минимизировать сроки простоя производственных линий заказчиков.
https://rms-ekb.ru/catalog/list/list-u8a-110x2000x6000-gost-19903-74/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-190-mm-ls59-1/
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgal6zn1-alloy-26—iso-3116/izdeliya-iz-magniya-mgal6zn1-alloy-26—iso-3116/
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-40khn2ma-36x1100x1200-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/manganinovaia-provoloka/manganinovaia-provoloka-0-3-mm-mnmtsazh3-12-0-3-0-3-gost-10155-75/
https://t.me/Asiapsi
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mcin3—jis-h-2221/pokovka-magnievaya-mcin3—jis-h-2221/
It’s awesome to go to see this web page and reading the
views of all colleagues on the topic of this article, while
I am also zealous of getting knowledge.
Feel free to surf to my web page bokep indonesia
丁寧な解説によって商品に関する理解が深まりました。商品に記載されていたサイズの誤りを修正し、正確な数値を公開している点が非常に良心的です。膝周りの皺や体のラインなど細部までリアルに作り込まれています。高品質な専用メイクに対応しており、商品の魅力がさらに高まります。誠実な情報開示と対応から強い信頼感を覚えます
Feel free to surf to my website; セクシー コスプレ
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-s255-80x1100x1200-gost-19903-2015-gladkii-chernyi-goriachekatanyi/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-320-mm-lts40s/
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-7—bs-2970-1/lenta-magnievaya-mag-7—bs-2970-1/
Everyone loves what you guys are usually
up too. This kind of clever work and exposure!
Keep up the good works guys I’ve you guys to my blogroll.
Also visit my web page … kraken6gf6o4rxewycqwjgfchzgxyfeoj5xafqbfm4vgvyaig2vmxvyd
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-7kh3-72-gost-5950-2000/
Admiring the commitment you put into your blog and detailed
information you present. It’s nice to come across
a blog every once in a while that isn’t the same
unwanted rehashed material. Excellent read!
I’ve bookmarked your site and I’m adding your RSS feeds to my Google account.
Here is my web page :: bokep japan sub indonesia
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-15kh11kh0-7-mm-10-6kh12-6-mm-tverdaia-paika-m1m-gost-r-52922-2008/
Everything is very open with a very clear clarification of the issues.
It was definitely informative. Your website is very useful.
Thanks for sharing!
Feel free to visit my site :: Poker Cash Games
Информация о проверке качества продукции повышает лояльность клиентов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-131—bs-3370/lenta-magnievaya-mag-131—bs-3370/
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-12kh1500kh2000-mm-dc03-1-0347-en-10131/
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-2×200-mm-l68-gost-931-90/
Hey There. I discovered your blog the usage of msn. That is an extremely smartly written article.
I will be sure to bookmark it and return to read more of your helpful information. Thanks for the post.
I will certainly return.
Also visit my web blog :: DGP file support
Хотел(а) отметить, что рад(а), что нашёл(а) сайт 1win — супер!
http://pasarinko.zeroweb.kr/bbs/board.php?bo_table=notice&wr_id=10532110
Профессиональный подход к описанию каждого вида металла
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m18220—uns/pokovka-magnievaya-m18220—uns/
Ориентация на долгосрочные отношения с клиентами позволяет компании формировать индивидуальные условия оплаты и графики поставок.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-08iu-12×1-gost-21729-76/
Наличие циркония свидетельствует о работе с высокотехнологичными заказами
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m13320—uns/lenta-magnievaya-m13320—uns/
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-100kh75kh10-mm-40nicrmo22-din-59370/
Hi! I’ve been following your website for a long time now and
finally got the courage to go ahead and give you a shout out from Lubbock Tx!
Just wanted to say keep up the fantastic work!
Here is my website: casino nl
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-0-5×500-mm-l63-gost-931-90/
If some one desires to be updated with most recent technologies therefore
he must be pay a visit this web site and be up to date
every day.
my page :: 爱思助手电脑版
It’s the best time to make some plans for the longer term and it’s time to be happy.
I’ve read this put up and if I may I wish to recommend you few fascinating things or advice.
Maybe you can write next articles referring to this article.
I wish to learn even more things approximately it!
my web-site: jaguar33
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11310—uns/polosa-magnievaya-m11310—uns/
In addition to providing a fun and creative activity, girl princess coloring book for girls
pages can also help teach children about diversity and inclusivity.
В каталоге представлены конденсаторные ниобиевые порошки высокой чистоты, необходимые для современной электроники.
https://rms-ekb.ru/catalog/plity/plita-u10-20x60x360-gost-19903-74/
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-88-9kh76kh1-8-mm-37-5kh40-5-mm-miagkaia-paika-m1t-gost-r-52922-2008/
Very great post. I just stumbled upon your weblog and wanted
to say that I have truly enjoyed surfing around your weblog posts.
In any case I will be subscribing for your feed and I’m hoping you write again soon!
Here is my webpage: check my blog
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-lz145a—astm-b275/truba-magnievaya-lz145a—astm-b275/
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-stal-3-160x100x10-gost-8509-93/
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-4-5×600-mm-l63-gost-931-90/
Лаконичное приветствие на главной странице сразу вводит в курс дела
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mc21310—bs-iso-16220/list-magnievyy-iso-mc21310—bs-iso-16220/
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/list/list-5khv2sf-3x1500x6000-gost-19903-74/
Do you have a spam problem on this website; I also am a blogger,
and I was wondering your situation; we have developed some nice practices and we are looking to swap solutions with other
folks, please shoot me an e-mail if interested.
Here is my web site: ที่นั่งนิรภัยสำหรับเด็กคืออะไร คืออะไร
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-15kh14-7-mm-m1r-gost-r-52948-2008/
Oh my goodness! Impressive article dude! Thank you, However I am having issues
with your RSS. I don’t know the reason why
I am unable to subscribe to it. Is there anybody getting identical RSS problems?
Anybody who knows the answer can you kindly respond? Thanx!!
Feel free to visit my web blog: Putzfirma Innsbruck
Thanks for sharing your thoughts on #PolyhedraBook. Regards
my webpage: #StellatedPolyhedra
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-hk31a—astm-b403/list-magnievyy-hk31a—astm-b403/
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-55kh6v3smf-200-gost-1133-71/
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-2×450-mm-l63-gost-931-90/
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-mgag3se2zr1—din-1729-part-2/prutok-magnievyy-g-mgag3se2zr1—din-1729-part-2/
Наличие прецизионных сплавов в ассортименте подтверждает работу компании с высокоточными и наукоемкими материалами.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-khn77tiuru-3-2x1200x1300-gost-24982-81-zharoprochnyi-kholodnokatanyi/
I’m amazed, I have to admit. Rarely do I encounter a blog that’s both educative and engaging, and
without a doubt, you’ve hit the nail on the head.
The problem is an issue that too few men and women are speaking
intelligently about. I’m very happy that I came across this during my search
for something relating to this.
Look into my website nonton bokep indonesia terbaru
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-35kh22-mm-m0b-gost-r-52948-2008/
91lhdl
If you are going for finest contents like myself, simply visit this
web page all the time because it provides quality contents, thanks
Also visit my web blog ออสตาร์เวกัส
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-a6z1—afnor-nf-a65-717/provoloka-magnievaya-g-a6z1—afnor-nf-a65-717/
Поставка продукции возможна не только в промышленных, но и в малых лабораторных объемах для исследовательских целей.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-s255-25x16x3-gost-8509-93/
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-akm-2-5x40x48-gost-13621-90/
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mb10030—en-12421-1998/prutok-magnievyy-en-mb10030—en-12421-1998/
Наличие на складе редких металлов, таких как цирконий, выделяет компанию на фоне конкурентов, торгующих только массовым прокатом.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-08kh22n6t-1-4x1000x1550-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Hello there, You have done an excellent job.
I will certainly digg it and personally suggest to my friends.
I am confident they’ll be benefited from this site.
my website: web site
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-25-mm-m2r-gost-r-52948-2008/
Hmm it appears like your blog ate my first comment (it was extremely long) so I guess I’ll
just sum it up what I had written and say, I’m thoroughly enjoying your blog.
I as well am an aspiring blog writer but I’m still new
to everything. Do you have any recommendations for novice blog writers?
I’d really appreciate it.
Have a look at my homepage – PXJ
Возможность заказа продукции в розницу и оптом (судя по описанию)
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-b-199-qe22a—astm-b199/truba-magnievaya-b-199-qe22a—astm-b199/
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-10kh17n13m2t-21-3×2-77-gost-21729-76/
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku40kh2mmm1gost-r-52922-2008/
Описание преимуществ компании подчеркивает надежность поставок
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az81/poroshok-magnievyy-az81/
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-100kh75kh10-mm-14nicrmo1-3-4-en-10056-2/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-16kh4kh3000-mm-mnzhmts30-1-1-gost-10092-2006/
Have you ever considered about adding a little bit more than just
your articles? I mean, what you say is fundamental and everything.
But just imagine if you added some great pictures or videos to give your posts more,
“pop”! Your content is excellent but with images and clips, this website could definitely be one of the best in its
field. Excellent blog!
Feel free to surf to my web page – สาขาของเรา
Thanks for ones marvelous posting! I definitely enjoyed reading it, you will be a great author.
I will be sure to bookmark your blog and will come back down the road.
I want to encourage one to continue your great posts, have a nice afternoon!
My blog post – homepage
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az10a—astm-b275/provoloka-magnievaya-az10a—astm-b275/
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/plity/plita-8kh6nft-16x250x560-gost-19903-74/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku28kh1-5mmm1gost-32590-2013/
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-am90—csa-hg-10/prutok-magnievyy-am90—csa-hg-10/
You actually make it seem really easy with your presentation but I in finding this topic to be really something which I feel
I’d by no means understand. It sort of feels too complex and extremely wide for me.
I am taking a look forward in your next submit, I’ll attempt to get
the hold of it!
Feel free to visit my web site Nhà Cái Uy Tín
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-150kh75kh12-mm-34crnimo6-en-10056-2/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/tkanaia-latunnaia-setka/setka-tkanaia-0-04kh0-063-mm-gost-6613-86-latunnaia-ls58-2/
Greate pieces. Keep posting such kind of info on your page.
Im really impressed by your site.
Hi there, You have done a fantastic job. I will certainly
digg it and individually recommend to my friends. I’m sure they will be benefited from this web site.
My site: Hitclub
Descobriu no Marketing uma paixão pela comunicação, onde exerce seu trabalho produzindo conteúdo sobre finanças pessoais, produtos e
serviços financeiros utilizando as técnicas de SEO.
Here is my site: save for link tik [https://metalunderground.pt/viewtopic.php?T=48628]
हार्दिक धन्यवाद प्लेटफ़ॉर्म Glory Casino
के लिए — बहुत मददगार है!
https://glorycasinologin.net/aviator
I enjoy reading a post that will make men and women think.
Also, thanks for permitting me to comment!
Feel free to surf to my blog … best online poker sites nwt (Pamela)
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-9999—csa-hg-2/provoloka-magnievaya-9999—csa-hg-2/
ООО «РМС» предлагает широкий спектр цветного проката, включая медь, латунь, бронзу и дюралюминий.
https://rms-ekb.ru/catalog/list/list-u8a-14x1200x3000-gost-19903-74/
It’s perfect time to make a few plans for the long run and it’s time
to be happy. I’ve read this put up and if I could I
want to suggest you some interesting things or tips. Perhaps you could
write subsequent articles referring to this article. I desire to read even more issues approximately it!
my site … 주소야
Moderne website met veel interessante info over online casino’s.
top 10 online casino belgië
I always spent my half an hour to read this
blog’s content daily along with a cup of coffee.
Also visit my website: 제주유흥
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-80kh68kh1-8-mm-35-5kh38-5-mm-tverdaia-paika-m3-gost-32590-2013/
Take a look at my website; high stakes poker
Отраслевой охват впечатляет: от медицины до космической промышленности
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-3-5922—din-1729-part-2/provoloka-magnievaya-3-5922—din-1729-part-2/
I’m not that much of a internet reader to be honest but your
blogs really nice, keep it up! I’ll go ahead and bookmark your site to come back down the road.
Cheers
My site … Ku88
Stunning quest there. What occurred after? Take care!
Feel free to visit my web site … Five88
ООО «РМС» специализируется на поставках редких и тугоплавких металлов, таких как ниобий и вольфрам.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r14f4-11-6-gost-7417-75/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-17kh1-2-mm-lts40mts1-5-gost-13942-86/
Продажа проволоки из тугоплавких металлов востребована в электронике
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ml6—gost-2856-79/truba-magnievaya-ml6—gost-2856-79/
Оперативная логистика и поддержка на всех этапах сделки позволяют минимизировать сроки простоя производственных линий заказчиков.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-6kh1250kh4000-mm-1-4512-en-iso-9444-2/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-akm-5x60x35-gost-13621-90/
I will immediately seize your rss as I can’t find your e-mail subscription hyperlink or e-newsletter service.
Do you have any? Please let me know in order that I may subscribe.
Thanks.
Have a look at my website Poker Strategies (Alumni.Hildred.Ibbott@haedongacademy.org)
I do believe all of the ideas you’ve offered for your
post. They are really convincing and will definitely work.
Nonetheless, the posts are very short for starters.
May you please lengthen them a little from subsequent time?
Thank you for the post.
Feel free to visit my website :: two factor authentication
I pay a visit daily a few sites and websites to read posts, except this webpage offers
feature based content.
My web blog: check it out
Продажа проволоки из тугоплавких металлов востребована в электронике
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ma21/pokovka-magnievaya-ma21/
Prime Secured
3603 N 222nd Ⴝt, Suit 102,
Elkhorn, ΝE68022, United Stɑtеs
402-289-4126
Pro Threat Intel Analysis
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-100kh65kh8-mm-c50e-en-10056-1/
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m138-128kh4-mm-lts30a3-din-471/
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/kobalt/wallex/kobalt-wallex-505-1/truba-kobaltovaya-wallex-505-1/
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-04kh18n10-0-5x1500x2000-gost-19903-2006-gladkii-chernyi-goriachekatanyi/
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-1935-10x57x107-gost-13621-90/
Большой опыт работы, судя по копирайту с 2013 года
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-706/prutok-kobaltovyy-stellite-706/
Наличие никелевых сплавов гарантирует высокую коррозийную стойкость оборудования, создаваемого заказчиками.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-30khgsa-130×8-gost-21729-76/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m15-16-2kh1-mm-lazhmts-din-472/
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-190/list-kobaltovyy-stellite-190/
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-st3ps-220x220x16-gost-19771-93/
Hi would you mind sharing which blog platform you’re using?
I’m going to start my own blog soon but I’m having a hard time choosing between BlogEngine/Wordpress/B2evolution and
Drupal. The reason I ask what is electric cable (https://www.intensedebate.com/people/capdiensaigon12) because
your layout seems different then most blogs and I’m looking for something completely unique.
P.S Apologies for getting off-topic but I had to ask!
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-d19ch-3x50x75-gost-13621-90/
Thanks in favor of sharing such a nice thinking, paragraph
is nice, thats why i have read it entirely
Also visit my webpage – 마사지사이트
We absolutely love your blog and find most of your post’s to be what precisely I’m looking for.
Would you offer guest writers to write content to suit your needs?
I wouldn’t mind writing a post or elaborating on most
of the subjects you write about here. Again,
awesome blog!
my blog; Debet
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-sdp-11a/poroshok-kobaltovyy-sdp-11a/
Поставка продукции возможна не только в промышленных, но и в малых лабораторных объемах для исследовательских целей.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-90khmf-41-gost-7417-75/
You are so cool! I don’t suppose I have read through
anything like this before. So great to discover somebody with original thoughts on this issue.
Really.. thanks for starting this up. This website is something that’s needed on the web, someone
with a bit of originality!
Feel free to visit my blog post :: Telegram下载
Hi there everyone, it’s my first pay a quick visit at this site, and paragraph
is actually fruitful designed for me, keep up posting such articles or reviews.
Feel free to visit my blog post … 마루마루
What’s Taking place i am new to this, I stumbled upon this I’ve
discovered It positively helpful and it has aided me out loads.
I hope to contribute & help different users like its
aided me. Good job.
my web site 마사지사이트
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-10kh1-2kh7000-mm-mnzhmts30-1-1-gost-10092-2006/
Thanks a bunch for sharing this with all folks you really understand what you are talking approximately!
Bookmarked. Please also visit my site =).
We could have a link exchange arrangement between us
Take a look at my web page: life coaching
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-ep483/poroshok-kobaltovyy-ep483/
Компания занимается реализацией ферросплавов, необходимых для качественного легирования сталей на литейных участках.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-50kh50kh5-mm-36crnimo4-en-10056-2/
I’m not sure where you’re getting your information, but
good topic. I needs to spend some time learning more or understanding more.
Thanks for great information I was looking for this info for my mission.
Feel free to visit my blog post – Magic Mushroom Delivery Canada
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-ad31e-1-2x38x23-gost-13621-90/
Hey there terrific website! Does running a blog
such as this require a lot of work? I have very little
understanding of computer programming however I was hoping to start my
own blog soon. Anyway, should you have any recommendations or techniques for new blog owners
please share. I understand this is off topic however I just wanted to ask.
Many thanks!
my webpage :: 마사지사이트
Hi! I know this is kinda off topic nevertheless I’d figured I’d ask.
Would you be interested in trading links or maybe guest authoring a
blog post or vice-versa? My website discusses a lot of the same topics as yours and I feel we could greatly benefit from each
other. If you happen to be interested feel free to send me
an e-mail. I look forward to hearing from you!
Terrific blog by the way!
my website … Order Magic Mushrooms Online
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/list/list-60kh2smf-3x500x500-gost-19903-74/
I am genuinely grateful to the owner of this site
who has shared this impressive paragraph at at this
time.
Also visit my web page 마사지사이트
Can I simply say what a relief to uncover an individual who really knows what they’re discussing over the internet.
You actually know how to bring an issue to light and make
it important. More people ought to read this and understand this side of the story.
I was surprised that you’re not more popular given that you surely have the gift.
Have a look at my web page; Youth basketball trainer
I don’t even know the way I finished up right here, however I thought this submit was once great.
I don’t understand who you might be but certainly you’re going to
a well-known blogger when you aren’t already. Cheers!
My site: 마사지
Tips and tools you offer are so helpful to agencies in our community.
It’s going to be ending of mine day, except before end
I am reading this impressive post to improve my experience.
Feel free to surf to my web site … Girls youth basketball league flagstaff
However, it is virtually all done with tongues rooted solidly in cheeks, and everyone has absolutely nothing but absolutely love for his or her friendly neighborhood scapegoat. The truth is, he is not just a pushover. He is basically that special variety of person strong enough to take all of that good natured ribbing for exactly what it is.
Hello! I know this is kind of off topic but I was wondering which blog platform are you using for this website?
I’m getting fed up of WordPress because I’ve had problems
with hackers and I’m looking at alternatives for another platform.
I would be great if you could point me in the direction of a
good platform.
Also visit my homepage; เจาะฟังก์ชันสุดว้าวของ DENZA Z9 GT ไฮเปอร์คาร์พลังงานไฟฟ้า ที่สุดแห่งเทคโนโลยียานยนต์จากจีน
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/ugolok-aliuminievyi/ugolok-aliuminievyi-45x45x4x6000-amg3/
Right now it sounds like Movable Type is the top blogging platform out
there right now. (from what I’ve read) Is that what you’re using on your blog?
my webpage – Gebäudereinigung Innsbruck
Описание преимуществ компании подчеркивает надежность поставок
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vt-10-1/truba-volframovaya-vt-10/
Very fine blog.
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-stal-10-85x1800x1400-gost-r-52146-2003-polimernyi-neotsinkovannyi-kholodnokatanyi/
I was suggested this website by my cousin. I am not sure whether this post is written by him as no one else know such detailed about my difficulty. You are wonderful! Thanks!
my website :: https://Dl.highstakesweeps.com/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-26kh1-5kh10000-mm-mnzhmts10-1-1-gost-10092-2006/
If you would like to get a great deal from this paragraph
then you have to apply such techniques to your won blog.
Also visit my webpage … comment-1973
Hello to all, how is the whole thing, I think every one is getting more from this site, and your views are pleasant designed
for new visitors.
Feel free to visit my web page … Youth basketball leagues Flagstaff
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vk13/poroshok-volframovyy-vk13/
Наличие на складе редких металлов, таких как цирконий, выделяет компанию на фоне конкурентов, торгующих только массовым прокатом.
https://rms-ekb.ru/catalog/svarnye-napravliaiushchie-opory/
I like this weblog very much so much great info .
I really like your blog.. very nice colors & theme.
Did you design this website yourself or did you hire someone to do it for you?
Plz reply as I’m looking to construct my own blog and would like to know where u got this from.
cheers
Feel free to visit my blog – bokep indonesia sex
Hey there! This is kind of off topic but I need some advice
from an established blog. Is it hard to set up your own blog?
I’m not very techincal but I can figure things out pretty fast.
I’m thinking about creating my own but I’m not sure where to begin. Do you have
any ideas or suggestions? Many thanks
my webpage; Girls only youth basketball league
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku28kh0-9mmm3rgost-32590-2013/
Hi! Do you use Twitter? I’d like to follow you if that would be okay.
I’m absolutely enjoying your blog and look forward to new updates.
Also visit my blog post … 마사지
What’s up, this weekend is fastidious designed for me, because
this time i am reading this fantastic educational piece of writing
here at my residence.
My web page … repay.in.net lừa đảo người chơi
Thanks for the marvelous posting! I seriously enjoyed reading it, you can be a great author.
I will ensure that I bookmark your blog and will often come back in the foreseeable future.
I want to encourage continue your great writing, have a nice weekend!
my webpage – 마사지사이트
Удобное разделение продукции на сплавы и конкретные виды проката
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-toc-5—pn-h-87203/krug-vismutovyy-toc-5—pn-h-87203/
We stumbled over here from a different web page and thought
I might check things out. I like what I see so now i am following you.
Look forward to looking into your web page yet again.
Feel free to visit my homepage :: Youth basketball Phoenix
Asking questions are actually pleasant thing if you are not understanding
something fully, except this piece of writing provides nice understanding yet.
Also visit my web page … folding fat tire electric bike
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-gladkii-19kh1900kh4000-mm-st5sp-gost-14637-89/
मैं यह बताना चाहता था, कि बहुत प्रसन्न हूँ,
कि मुझे 4rabet साइट मिली —
सुपर!
4rabet official website
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-18kh2kh3000-mm-mnzhmts10-1-1-gost-10092-2006/
I really like your blog.. very nice colors & theme. Did you create this website yourself or did you
hire someone to do it for you? Plz reply as I’m looking to design my own blog and would like to find out where u got
this from. kudos
Have a look at my page polymarket bot
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-stal-20-273×27-gost-21729-76/
Um ein Video herunterzuladen, kopiert Ihr die URL aus dem Browser,
klickt im Anschluss auf “URL einfügen” und wählt das Ausgabeformat,
die Qualität des Videos sowie den gewünschten Speicherort aus.
Also visit my web-site – yt downloader
I truly love your site.. Pleasant colors & theme. Did you develop this website yourself?
Please reply back as I’m hoping to create my very own site and want to know where you got this from or exactly what
the theme is called. Cheers!
Feel free to surf to my blog post: arabian
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku40kh1-1mmm3rtgost-r-52922-2008/
Sıvı yağ ürünleri alımı konusunda doğru firmayla çalışmak işletmelere zaman ve güven kazandırır.
Timo Agro’nun bu alandaki hizmetleri bu nedenle
önemli.
Сайт четко ориентирован на промышленный сектор и B2B сегмент
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-h43bi57a—jis-z-3282/prutok-vismutovyy-h43bi57a—jis-z-3282/
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-60kh60kh8-mm-18crnimo7-6-din-1028/
Just want to say your article is as surprising.
The clearness on your post is simply nice and that i can suppose you are a professional on this
subject. Well along with your permission let me to grab your feed to stay updated
with coming near near post. Thanks 1,000,000 and please keep up the rewarding work.
Also visit my blog :: zelensky05
Thanks for sharing your info. I truly appreciate your efforts and I will be waiting
for your further post thanks once again.
my blog … zelensky05
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/medno-nikelevyi-list/medno-nikelevyi-list-15x1000x2000-mm-mnzh5-1/
Great blog here! Additionally your website loads up fast!
What host are you using? Can I am getting your affiliate
hyperlink to your host? I wish my web site loaded up as fast as yours lol
my blog post; zelensky04
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-h43bi57a—jis-z-3282/poroshok-vismutovyy-h43bi57a—jis-z-3282/
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-6kh4m2fs-3-gost-5950-2000/
bookmarked!!, I really like your website!
My web-site; 마루마루
Its like you read my mind! You seem to know a lot about this, like you wrote the book in it or something. I think that you can do with some pics to drive the message home a bit, but other than that, this is wonderful blog. A great read. I’ll certainly be back.
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku25kh1-6mmm3mgost-32590-2013/
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89844—cda/lenta-vismutovaya-c89844—cda/
Большое спасибо {я {ценю | ценю это | рад} {этому | данному материалу}}
Feel free to visit my blog :: Невероятно
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-120kh80kh10-mm-16mncrb5-en-10056-1/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/magnievyi-krug/krug-magnievyi-250-mm-ma2-gost-18351-73/
You are one talented writer thank you for the post.
Технические характеристики сплавов помогают инженерам в подборе
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89831—uns/provoloka-vismutovaya-c89831—uns/
Simply want to say your article is as amazing. The clarity in your post is just great and i can assume you’re an expert on this subject. Fine with your permission allow me to grab your feed to keep up to date with forthcoming post. Thanks a million and please keep up the gratifying work.
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/list/list-khvg-140x1000x1000-gost-19903-74/
Потрясающе полно интересных знаний
my blog post; красиво
I had fun reading this post. I want to see more on this subject.. Gives Thanks for writing this nice article.. Anyway, I’m going to subscribe to your rss and I wish you write great articles again soon.
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku42kh1-1mmm1egost-r-52922-2008/
A person necessarily assist to make critically articles
I would state. This is the first time I frequented your website page and thus far?
I amazed with the analysis you made to make this actual post extraordinary.
Excellent activity!
Here is my blog – แทงบอลโลก
Поковки и штабики — важные заготовки для металлургических предприятий
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-b-505-c-89320—astm-b505/provoloka-vismutovaya-b-505-c-89320—astm-b505/
yx5f3x
This blog was… how do I say it? Relevant!! Finally I’ve found something
that helped me. Kudos!
My web-site – แทงบอลโลก
Hello! Do you know if they make any plugins to assist with Search Engine
Optimization? I’m trying to get my blog to
rank for some targeted keywords but I’m not seeing very good success.
If you know of any please share. Kudos!
Feel free to surf to my web-site: แทงบอลออนไลน์24
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-kapilliarnaia-trubka/latunnaia-kapilliarnaia-trubka-1-5kh0-35kh10000-mm-l70-gost-2624-2016/
It’s actually a great and helpful piece of info. I am happy
that you simply shared this useful information with us.
Please keep us up to date like this. Thanks for sharing.
my page; electronic drum pad
Четкая структура меню позволяет быстро найти нужный металл
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-158-190—astm-b774/truba-vismutovaya-158-190—astm-b774/
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-09g2s-1-4x1900x1100-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
Superb, what a weblog it is! This web site provides helpful facts to us, keep it up.
My blog post: electric drum set adult
It’s hard to come by educated people for this topic, however, you seem like you know
what you’re talking about! Thanks
Look into my web site แทงบอลโลก
I’ve been exploring for a little bit for any high quality articles or blog posts in this sort of house .
Exploring in Yahoo I at last stumbled upon this site.
Studying this info So i’m glad to show that I have a very excellent uncanny feeling I discovered just what
I needed. I most no doubt will make sure to don?t forget this web site and provides it a look regularly.
Also visit my webpage … everygame poker review
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku15kh1-2mmm1egost-32590-2013/
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-fvd50u0-5—gost-27130-94/prutok-vanadievyy-fvd50u0-5—gost-27130-94/
Just wish to say your article is as amazing. The clearness in your post is just nice and
i could assume you are an expert on this subject.
Well with your permission let me to grab your feed to keep up to date
with forthcoming post. Thanks a million and please keep up the rewarding work.
my web site; electric drum pad
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-150kh90kh10-mm-e335gc-en-10277/
Hello, this weekend is pleasant in favor of me, for the reason that this time i
am reading this great educational post here at my residence.
My webpage … 늑대닷컴
Artikel yang sangat informatif dan bermanfaat.
Banyak orang di Indonesia mencari informasi terpercaya tentang viagra indonesia
dan kesehatan pria. Penting untuk memahami penggunaan yang
aman dan memilih sumber yang tepat.
Also visit my web page: bokep indonesia
Howdy are using WordPress for your site platform?
I’m new to the blog world but I’m trying to get started and set Tune up my own. Do you
need any html coding knowledge to make your own blog?
Any help would be greatly appreciated!
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-175kh3-mm-l63-gost-13942-86/
Описание преимуществ компании подчеркивает надежность поставок
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt6ch—ost-1-90013-81/truba-titanovaya-vt6ch—ost-1-90013-81/
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-230kh1800-mm-acroni-4919a-en-iso-18286/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku54kh2-3mmm2rgost-32590-2013/
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-twc3/poroshok-titanovyy-twc3/
Hi! Do you know if they make any plugins to protect against hackers?
I’m kinda paranoid about losing everything I’ve worked hard on.
Any suggestions?
My homepage; best slots sites UK
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-40khfa-36x1400x1000-gost-19903-2006-gladkii-chernyi-goriachekatanyi/
Thanks for the good writeup. It in fact was a amusement account it.
Glance complex to far introduced agreeable from you!
By the way, how could we be in contact?
Here is my web site … Brake repair
Really no matter if someone doesn’t understand then its
up to other users that they will assist, so here it happens.
Look into my site – electric drum kit
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-ot4-2/pokovka-titanovaya-ot4-2/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-42kh1-7-mm-lmtska-gost-13942-86/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-30kh20kh3-mm-28mn6-uni-6762/
Your style is so unique compared to other people I’ve read stuff from.
Thank you for posting when you have the opportunity, Guess I’ll just book mark this
blog.
My blog; beruangjitu
Thanks for sharing your thoughts. I truly appreciate your efforts and I will be waiting for your
further post thanks once again.
my blog post; web page
I am regular visitor, how are you everybody? This paragraph posted at
this web site is actually good.
Also visit my web-site :: beruangjitu
I savour, lead to I discovered just what I was looking for.
You’ve ended my 4 day long hunt! God Bless you man. Have
a nice day. Bye
My site portable drum set
Very energetic article, I enjoyed that bit. Will there
be a part 2?
Stop by my site; beruangjitu
This is the perfect site for anybody who wants to understand this topic.
You understand a whole lot its almost hard to argue with you (not
that I personally would want to…HaHa). You definitely put
a new spin on a topic that has been discussed for years. Wonderful stuff,
just wonderful!
my site :: drum set for kids
Большой опыт работы, судя по копирайту с 2013 года
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-65bt—gost-10994-74-1/pokovka-titanovaya-65bt—gost-10994-74-1/
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku14-7kh1-2mmm3rtgost-r-52922-2008/
I pay a quick visit day-to-day some web pages and sites to read articles,
however this weblog presents quality based articles.
Feel free to visit my webpage: 오피아트
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-kh12vmf-95-gost-5950-2000/
My page High Stake Poker
It’s the best time to make some plans for the future and it’s time to be happy.
I’ve read this post and if I could I want to suggest
you some interesting things or tips. Maybe you could write
next articles referring to this article. I desire to read even more
things about it!
my webpage; drum set for kids
You are not right. I am assured. I can prove it. Write to me in PM, we will talk.
I think the admin of this site is genuinely working hard in favor of his
website, for the reason that here every information is quality based
information.
Have a look at my blog post :: portable drum set
Возможность заказать листы и полосы нестандартных размеров
https://redmetsplav.ru/store/tantal-i-ego-splavy/tantal-ta/polosa-tantalovaya-ta/
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-62kh2-mm-lts40s-gost-13942-86/
Amazing! Its truly amazing article, I have got much clear idea on the topic of from this article.
my website … donner electric drum set
География деятельности компании охватывает всю территорию России, обеспечивая металлом предприятия в удаленных регионах.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-55kh55kh8-mm-20mocr3-din-1028/
whoah this weblog is great i really like studying your articles. Stay up the great work! You already know, lots of persons are looking round for this information, you can aid them greatly.
There are some serious financial ramifications here.
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-10kh7kh0-6-mm-7-8kh9-8-mm-tverdaia-paika-m3m-gost-32590-2013/
I don’t normally comment on blogs.. But nice post! I just bookmarked your site
Поставка продукции возможна не только в промышленных, но и в малых лабораторных объемах для исследовательских целей.
https://rms-ekb.ru/catalog/list/list-8khf-11x1000x1000-gost-19903-2006/
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m115-108kh4-mm-ls-din-471/
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-250kh250kh35-mm-36nicrmo16-en-10056-2/
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-80kh68kh1-8-mm-35-5kh38-5-mm-miagkaia-paika-m3m-gost-r-52922-2008/
This is a good tip especially to those fresh to
the blogosphere. Simple but very precise information… Thank you for sharing this one.
A must read article!
my webb page slots
Оперативная логистика и поддержка на всех этапах сделки позволяют минимизировать сроки простоя производственных линий заказчиков.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-06kh1250kh3000-mm-1-4526-en-iso-9444-2/
Hello there! Do you know if they make any plugins to help with Search
Engine Optimization? I’m trying to get my
blog to rank for some targeted keywords but I’m not seeing very good gains.
If you know of any please share. Kudos!
Feel free to visit my web site :: fabet
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m72-67-5kh2-5-mm-lts25s2-din-471/
I am regular reader, how are you everybody?
This post posted at this web page is in fact nice.
Feel free to visit my blog Uk88
Важным преимуществом является возможность изготовления деталей и изделий по индивидуальным чертежам заказчика.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-stal-3-75x50x5-gost-8509-93/
Hi there to all, how is everything, I think every one is getting more from this web site, and your views are
good in support of new visitors.
Feel free to visit my blog post Red88
Keep on writing, great job!
Feel free to surf to my web site :: angka togel orang gila
Сайт работает стабильно и быстро загружается
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-sismg4640-07—ss-144640/polosa-magnievaya-sismg4640-07—ss-144640/
Ориентация на долгосрочные отношения с клиентами позволяет компании формировать индивидуальные условия оплаты и графики поставок.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-khn75mbtiu-2-5x2000x1100-gost-24982-81-zharoprochnyi-belyi-goriachekatanyi/
Мне очень нравится сайт 1win, он очень удобный в использовании!
https://1win-crash.org/aviator
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m162-151kh4-mm-lmtss-din-471/
This is very interesting, You’re a very skilled blogger.
I’ve joined your rss feed and look forward to seeking more of your fantastic
post. Also, I’ve shared your site in my social networks!
My web site :: zbet
Mevcut birçok aracın yavaş, güvenilmez veya
müdahaleci reklamlarla dolu olduğunu gördük.
Feel free to surf to my web blog: https://savefrom.In.net/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/list/list-27kh2n2m1f-3x1200x3000-gost-19903-74/
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-zn1zr/list-magnievyy-mg-zn1zr/
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-88-9kh76kh1-8-mm-14kh17-mm-tverdaia-paika-m3rt-gost-r-52922-2008/
Artikel yang sangat informatif dan bermanfaat. Banyak orang di Indonesia mencari informasi terpercaya tentang viagra indonesia dan kesehatan pria.
Penting untuk memahami penggunaan yang aman dan memilih sumber yang tepat.
Terima kasih atas informasi ini. Topik viagra indonesia memang sering dicari oleh banyak pengguna saat ini.
Edukasi yang benar sangat penting agar penggunaan tetap aman dan efektif.
Konten yang bagus dan mudah dipahami. Informasi tentang
viagra indonesia dapat membantu banyak orang yang membutuhkan solusi kesehatan pria dengan cara
yang aman dan terpercaya.
Postingan yang sangat membantu. Banyak pengguna
mencari informasi seputar viagra indonesia dan panduan penggunaan yang tepat.
Artikel seperti ini sangat berguna bagi pembaca.
Artikel berkualitas dan penuh informasi. Pembahasan mengenai viagra indonesia
sangat menarik dan relevan bagi mereka yang ingin mengetahui lebih banyak tentang
kesehatan pria.
My web blog; bokep indonesia
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-150kh90kh15-mm-c45-en-10056-2/
Информация о проверке качества продукции повышает лояльность клиентов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgal6zn—din-1729-part-2/izdeliya-iz-magniya-mgal6zn—din-1729-part-2/
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-62kh1-7-mm-lts30a3-gost-13943-86/
I was recommended this web site via my cousin. I’m now not sure whether this post is written by
means of him as no one else understand such specified approximately my difficulty.
You’re incredible! Thank you!
Here is my web site – togel lotto
In fact no matter if someone doesn’t be aware of afterward its up to
other people that they will assist, so here it takes place.
my site – website
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-45khnm-22-55-gost-7417-75/
After looking over a handful of the blog posts on your
site, I seriously appreciate your way of blogging. I book-marked it to my bookmark
site list and will be checking back soon. Take a look at my website too and let me
know what you think.
Also visit my website; Redeemed Life Counseling
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-66-7kh57kh1-4-mm-11kh14-mm-tverdaia-paika-m1r-gost-32590-2013/
Hello, I think your site might be having browser compatibility issues.
When I look at your blog in Firefox, it looks fine but when opening in Internet Explorer,
it has some overlapping. I just wanted to give you a quick heads up!
Other then that, very good blog!
Review my blog post: five88
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-70kh70kh7-mm-42cr4-din-59370/
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-9—bs-2970/lenta-magnievaya-mag-9—bs-2970/
Everyone loves it whenever people come together and share ideas.
Great blog, keep it up!
My blog: bolly4u
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/list/list-27kh2n2m1f-3x2000x6000-gost-19903-74/
Лаконичное приветствие на главной странице сразу вводит в курс дела
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-13—bs-2970-1/prutok-magnievyy-mag-13—bs-2970-1/
Do you have a spam problem on this site; I also am a blogger, and I was wanting to know your situation; many of us have developed some nice practices and we are looking to trade techniques with
others, why not shoot me an email if interested.
Here is my web-site :: trauma therapy near me
Hi there everybody, here every person is sharing these knowledge,
therefore it’s good to read this webpage, and I used to go to see this web site daily.
My web site: professional eyeglass repair
Thank you for the good writeup. It in fact was a
amusement account it. Look advanced to far added agreeable from you!
However, how can we communicate?
Also visit my homepage – eyeglasses repair near me
I every time used to study paragraph in news papers but now as I am a user of web therefore from now I am
using net for posts, thanks to web.
Also visit my blog post: sontogel
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-12kh18n10t-70x45x5-gost-19772-93/
Cabinet IQ
8305 Ѕtate Hwwy 71 #110, Austin,
TX 78735, Unitedd Ѕtates
254-275-5536
Traditional
This post is invaluable. Where can I find out more?
Feel free to surf to my page – link akuntoto
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-9kh0-8-mm-lmtska-gost-13943-86/
Возможность заказа висмута — достаточно редкое предложение на рынке
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m18330—uns/truba-magnievaya-m18330—uns/
Excellent blog right here! Additionally your web site a lot up very fast!
What web host are you using? Can I get your associate hyperlink for your host?
I want my web site loaded up as quickly as yours lol
My web-site – free
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-6kh1500kh6000-mm-1-4301-en-iso-9444-2/
Hi, I would like to subscribe for this webpage to get most up-to-date updates, thus where
can i do it please help.
Here is my web-site :: sontogel
Greetings from Florida! I’m bored to death at work so I
decided to check out your blog on my iphone during lunch break.
I really like the information you provide here and can’t wait
to take a look when I get home. I’m amazed at how quick
your blog loaded on my mobile .. I’m not even using WIFI, just 3G ..
Anyways, superb blog!
Here is my blog post; login sontogel
Attractive section of content. I just stumbled upon your website and in accession capital to assert that I
get actually enjoyed account your blog posts. Any way I will be
subscribing to your augment and even I achievement you access consistently fast.
my web-site: login akuntoto
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m12410—uns/prutok-magnievyy-m12410—uns/
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-53-6kh47kh1-2-mm-11kh13-mm-tverdaia-paika-m3r-gost-32590-2013/
Hi! This post could not be written any better! Reading this post reminds me of my good old room mate!
He always kept talking about this. I will forward this post
to him. Pretty sure he will have a good read. Many thanks for sharing!
my website: login ketuatoto
I have been browsing on-line greater than 3 hours these days, yet I
by no means found any attention-grabbing article like yours.
It’s pretty value sufficient for me. Personally, if all web owners and bloggers made good content material as you did, the
internet shall be a lot more useful than ever before.
Feel free to surf to my blog post – 강남달토
ООО «РМС» специализируется на поставках редких и тугоплавких металлов, таких как ниобий и вольфрам.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-aisi-304-125x80x8-gost-8509-93/
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m43-46-5kh1-75-mm-lts30a3-din-472/
Nice blog here! Also your web site loads up very
fast! What web host are you using? Can I get your affiliate hyperlink to your host?
I want my website loaded up as quickly as yours lol
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-75kh1000-mm-x3crnimo17-13-3-en-iso-18286/
American Industrial Magazine (americanindustrialmagazine.com) es un portal digital y publicación especializada (bilingüe en inglés
y español) enfocada en proveer noticias, análisis de mercado y tendencias sobre los sectores de manufactura, industria, tecnología, metalmecánica y farmacéutica.
Su contenido abarca temas estratégicos y técnicos que impactan a América del Norte (principalmente México y Estados Unidos), incluyendo el nearshoring, la adopción de inteligencia artificial en fábricas, robótica (cobots), control de
calidad predictivo, normativas de seguridad (OSHA, ISO 9001) y la escasez de talento especializado.
Además, funciona como una plataforma de desarrollo profesional, ofreciendo cursos de capacitación técnica en software como Microsoft Excel (desde nivel básico
hasta macros) y Autodesk Fusion 360.
Feel free to visit my homepage – Manufactura de semiconductores
Wow that was strange. I just wrote an really long comment but after I clicked submit my comment
didn’t show up. Grrrr… well I’m not writing all that over again. Anyway, just wanted to
say wonderful blog!
Also visit my website comidas de empresa valencia
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-35kh29kh1-mm-23kh25-mm-miagkaia-paika-m2t-gost-r-52922-2008/
Hello, i think that i saw you visited my blog so i came to
“return the favor”.I’m trying to find things to improve my site!I suppose its ok to use some of your
ideas!!
My web page – https://ok365dy.com/
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/list/list-4khmfs-2x1000x1000-gost-19903-74/
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mg99-80a—iso-8287/lenta-magnievaya-iso-mg99-80a—iso-8287/
Thank you for the auspicious writeup. It in fact was a amusement account it.
Look advanced to far added agreeable from you! By the way, how could we communicate?
Also visit my web-site login sontogel
If some one desires to be updated with hottest technologies after that he must be pay a
visit this website and be up to date daily.
My web blog link ketuatoto
Nice post. I used to be checking constantly this weblog and I’m impressed!
Very useful information particularly the closing phase :
) I care for such info much. I used to be looking for this
particular info for a long time. Thanks and best of luck.
Feel free to visit my webpage: login ketuatoto
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-09kh16n4b-1-5x1250x1300-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
Hi there, after reading this remarkable post i am as well delighted
to share my knowledge here with colleagues.
My homepage – login sontogel
Фольга из редких металлов часто требуется для высокотехнологичных лабораторий
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-hk31a—astm-b403/polosa-magnievaya-hk31a—astm-b403/
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-64kh55kh1-4-mm-32-5kh34-5-mm-tverdaia-paika-m3rm-gost-32590-2013/
Woah! I’m really loving the template/theme of this website.
It’s simple, yet effective. A lot of times it’s very hard to get that “perfect balance” between user
friendliness and visual appearance. I must say that you’ve done a fantastic job
with this. Additionally, the blog loads super fast for me on Opera.
Excellent Blog!
My web page … link ketuatoto
청주에서 이미 소문난 만족도 높은 서비스! 청주출장마사지로 진정한 휴식을 누려보세요.
대전 전 지역 어디서나 편안하게 케어받고 싶다면? 대전출장마사지에서 전문 테라피스트의 손길을 느껴보세요.
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-12kh1-14-56-gost-7417-75/
대전 전 지역 어디서나 편안하게 케어받고 싶다면? 대전출장마사지에서 전문 테라피스트의 손길을 느껴보세요.
Bintang4d
memberikan bukti jackpot yang dibayar lunas oleh situs Bintang4d kepada member yang berhasil mendapatkan kemenangan dengan nilai berapapun,
kepercayaan member menjadi hal utama yang selalu
diperhatikan.
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-gre3/lenta-magnievaya-gre3/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m8-8-7kh0-8-mm-lts40mts3a-din-472/
청주에서 이미 소문난 만족도 높은 서비스! 청주출장마사지로 진정한 휴식을 누려보세요.
Hi there, I check your blog daily. Your humoristic style is awesome,
keep it up!
my blog post organizacion de despedidas valencia
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-25kh25kh4-mm-c22e-din-1028/
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-54kh47kh1-2-mm-32kh34-mm-tverdaia-paika-m1t-gost-r-52922-2008/
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/list/list-9khs-2x1000x1000-gost-19903-2006/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Stаtes
254-275-5536
Premiummat
Поковки и штабики — важные заготовки для металлургических предприятий
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mb10031—en-12421-1998/izdeliya-iz-magniya-en-mb10031—en-12421-1998/
Hey! Quick question that’s completely off topic.
Do you know how to make your site mobile friendly?
My site looks weird when viewing from my iphone 4.
I’m trying to find a template or plugin that might be
able to correct this issue. If you have any suggestions, please share.
Appreciate it!
Feel free to visit my blog: 9bet
Great beat ! I wish to apprentice while you amend your site,
how could i subscribe for a blog web site? The account aided me a appropriate deal.
I were a little bit acquainted of this your broadcast provided vivid transparent concept
My site DTC file download
В каталоге представлены конденсаторные ниобиевые порошки высокой чистоты, необходимые для современной электроники.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-125kh75kh10-mm-c45e-en-10056-2/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-35kh29kh1-mm-23kh25-mm-tverdaia-paika-m1e-gost-32590-2013/
Piece of writing writing is also a excitement, if
you be familiar with afterward you can write if not it is complex to write.
Feel free to surf to my webpage – http://www.betiran.vip
Четкая структура меню позволяет быстро найти нужный металл
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az90a—astm-b275/truba-magnievaya-az90a—astm-b275/
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-60kh200-mm-ls59/
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-30g-17x1250x1100-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-76-1kh53-6-mm-m2-gost-r-52948-2008/
Ориентация на долгосрочные отношения с клиентами позволяет компании формировать индивидуальные условия оплаты и графики поставок.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-s255-75x2000x1000-gost-19903-2015-gladkii-chernyi-goriachekatanyi/
Howdy! This article couldn’t be written much better!
Going through this article reminds me of my previous roommate!
He continually kept preaching about this. I’ll send this post to
him. Pretty sure he will have a very good read.
Thanks for sharing!
Have a look at my site; 뉴토끼
My brother recommended I would possibly like this web site.
He was totally right. This publish truly made my day. You can not imagine just how so
much time I had spent for this information! Thanks!
my web blog; https://secretmenus.com/panda-express/
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m107-114kh4-mm-lsdch-din-472/
Great information. Lucky me I found your blog by accident (stumbleupon).
I’ve saved it for later!
Feel free to visit my webpage – how to get traffic from google
I imagine so. Very good stuff, I agree totally.
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-a3a—astm-b275/pokovka-magnievaya-a3a—astm-b275/
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-u9-19-gost-1435-74/
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-22kh8-mm-m0b-gost-r-52948-2008/
I know this web page offers quality dependent content and
additional stuff, is there any other web page which provides such
information in quality?
Feel free to visit my web-site; kumpulan video bokep indonesia
Loving the info on this website , you have done outstanding job on the blog posts.
I pay a quick visit each day a few blogs and information sites to read articles, but this
blog offers feature based content.
My web page – jamaica
We are a group of volunteers and starting a new initiative in our community. Your blog provided us with valuable information to work on|.You have done a marvellous job!
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-20khgsa-12x1500x1900-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-50kh100-mm-lazhmts/
Thanks for sharing such a pleasant thought, post is fastidious, thats
why i have read it entirely
My page :: Работа в Израиле
I would share your post with my sis.
We recognize the value of your time, which is why we
have incorporated a Turbo Mode feature into Easy Videos x video downloader.
Awesome site you have here but I was wondering if you knew
of any discussion boards that cover the same topics talked about in this article?
I’d really love to be a part of community where I can get advice
from other experienced people that share the same interest.
If you have any recommendations, please let me know.
Thanks!
my web site; Danatoto
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ml8—gost-2856-79/truba-magnievaya-ml8—gost-2856-79/
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-80kh70-mm-m1t-gost-r-52948-2008/
I’m curious to find out what blog system you have been working with?
I’m experiencing some minor security problems with my latest site and I’d like to find something more
risk-free. Do you have any suggestions?
Feel free to surf to my site bokep streaming indonesia
Hi my family member! I wish to say that this post is amazing, great written and come with approximately all important infos.
I would like to look extra posts like this .
My web site :: unblocked games 76
бюро перекладу документів, https://www.blackhatworld.com/members/kursivcom1.1918717/ надає професійні послуги трансформації текстів офіційних типів.
Сайт четко ориентирован на промышленный сектор и B2B сегмент
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ma2/truba-magnievaya-ma2/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-100kh100-mm-lts40mts1-5/
Адвокат по цифровым претсупленям,
Адвокат по цифровым претсупленям в Алматы
работает в представительстве клиентов в инцидентах в.
와, 그건 특이했어요. 정말 매우 긴 댓글을 작성했는데,
제출을 클릭한 후 댓글이 보이지 않았어요.
Grrrr… 다시 쓰지는 않을게요. 어쨌든, 그냥 멋진
블로그라고 말하고 싶었어요!
Wow, amazing blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your website is great,
let alone the content!
my website :: 비아그라 구매
Наличие никелевых сплавов гарантирует высокую коррозийную стойкость оборудования, создаваемого заказчиками.
https://rms-ekb.ru/catalog/list/list-8kh4v3m3f2-2x1200x2000-gost-19903-74/
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-27-4kh17-mm-m3rm-gost-r-52948-2008/
Hello this is somewhat of off topic but I was wondering if blogs use
WYSIWYG editors or if you have to manually code with HTML.
I’m starting a blog soon but have no coding knowledge so I wanted to get guidance from someone with experience.
Any help would be enormously appreciated!
Here is my page: get visa form
Четкая структура меню позволяет быстро найти нужный металл
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-6-pm/provoloka-kobaltovaya-stellite-6-pm/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-500kh700-mm-lsd/
Hola! I’ve been reading your website for a while now and finally got the
courage to go ahead and give you a shout out
from Houston Texas! Just wanted to mention keep up the fantastic job!
Also visit my homepage: porn
โพสต์นี้ อ่านแล้วได้ความรู้เพิ่ม ค่ะ
ผม ไปเจอรายละเอียดของ เนื้อหาในแนวเดียวกัน
ที่คุณสามารถดูได้ที่
Margie
สำหรับใครกำลังหาเนื้อหาแบบนี้
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์
นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
Here is my web-site: super flik – Margie,
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-188/prutok-kobaltovyy-stellite-188/
Very good article. I’m going through a few of these issues
as well..
Here is my homepage … dooball
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-70kh54-mm-cu-dhp-gost-r-52948-2008/
I was able to find good advice from your blog posts.
Review my web site; dooball
I’m not sure exactly why but this site is loading incredibly slow for
me. Is anyone else having this problem or is
it a issue on my end? I’ll check back later and see if the
problem still exists.
Feel free to visit my website: https://aviatorjoc.org
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-pr-v3k-r—gost-21449-75/lenta-kobaltovaya-pr-v3k-r—gost-21449-75/
Оперативная логистика и поддержка на всех этапах сделки позволяют минимизировать сроки простоя производственных линий заказчиков.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-17kh18n9-6x1900x1900-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-250kh700-mm-lmtssk/
If some one desires to be updated with hottest technologies then he must be visit this web page and be up
to date all the time.
my website :: kumpulan video bokep indonesia
SGP Togel 4D has become one of the extremely recognized number prediction games among enthusiasts who enjoy testing their
luck and analytical skills. Known for its straightforward format and
exciting gameplay, SGP Togel 4D is constantly attract players who appreciate
the task of selecting four-digit combinations and
following a results with anticipation.
Here is my homepage :: sgptogel4d
Описание преимуществ компании подчеркивает надежность поставок
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-ep431/folga-kobaltovaya-ep431/
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-70kh28-mm-m3r-gost-r-52948-2008/
Риск от наркотиков — этто
сложная хоботня, охватывающая физическое, психическое равным
образом соц здоровье человека.
Употребление подобных наркотиков, как снежок, мефедрон,
ямба, «шишки» или «бошки», может огласить к необратимым следствиям как для организма, так и
для мира в целом. Но даже при эволюции связи эвентуально электровосстановление — главное,
чтоб энергозависимый явантроп обратился
согласен помощью. Важно памятовать, что наркомания врачуется, равным образом реабилитация бацнет шанс на свежую жизнь.
Feel free to surf to my blog post … купить корость
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-khastelloi-s22-325×6-gost-8734-75/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-50kh500-mm-lts40s/
I just couldnt leave your website before saying that I really enjoyed the useful information you offer to your visitors… Will be back often to check up on new stuff you post!
Quality content is the main to invite the viewers to pay
a visit the web site, that’s what this web site is providing.
My page: homepage
You appear to know so much about this, and I see you’re a published author. Thanks
After going over a few of the blog articles on your blog, I truly appreciate your technique of blogging.
I added it to my bookmark site list and will be checking back soon. Please check out my website too and let me know
how you feel.
Here is my web site – bokep ibu ibu Indonesia
Thanks for your personal marvelous posting!
I seriously enjoyed reading it, you may be a great author.
I will ensure that I bookmark your blog and may come back from now on. I want
to encourage you to definitely continue your
great work, have a nice holiday weekend!
Here is my site; bolahit
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-d16-60x1300x1500-gost-19903-2006-gladkii-chernyi-goriachekatanyi/
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-14-7kh6-mm-m3t-gost-r-52948-2008/
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vt-15-1/list-volframovyy-vt-15/
Togel SGP 4D has developed into a widely recognized way of number-based entertainment among enthusiasts who enjoy
testing their prediction skills and following draw results.
Known for its straightforward format and engaging gameplay,
togel sgp 4d will continue to attract a loyal community of players who appreciate
both the excitement as well as the strategic aspects involved.
My page … https://sgptogel4d.com/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-200kh800-mm-lts37mts2s2k/
What you published was actually very reasonable.
But, consider this, suppose you added a little information? I mean, I don’t wish to tell you how to run your website, but suppose you added a title that grabbed a person’s attention? I mean Heel Pain –
Plantar Fasciitis – Mr Will Edwards is a little plain. You ought
to glance at Yahoo’s home page and see how they create post
headlines to get viewers interested. You might add a related video or a related picture or two to grab readers excited about what you’ve got to
say. Just my opinion, it would bring your website a little bit more interesting.
my site คลินิกทองสไมล์
Наличие циркония свидетельствует о работе с высокотехнологичными заказами
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vi-30-1/truba-volframovaya-vi-30/
hey there and thank you for your info – I have definitely picked up something new from right here.
I did however expertise a few technical points using this web
site, since I experienced to reload the website lots of times previous to I
could get it to load properly. I had been wondering if your web host is OK?
Not that I am complaining, but slow loading instances times will very frequently affect your placement in google and could damage your high quality score if ads and marketing with Adwords.
Well I’m adding this RSS to my e-mail and can look out for much more of your respective interesting content.
Make sure you update this again soon.
Feel free to surf to my blog post :: Proxy director service
This is very fascinating, You’re an excessively skilled
blogger. I’ve joined your rss feed and sit up
for looking for extra of your great post. Additionally, I have shared your
site in my social networks
Also visit my blog post – Ford Engine Repair
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-troiniki-press/mednyi-press-troinik-22-mm-m1e-gost-r-52948-2008/
Its such as you read my mind! You appear to grasp so much about this, like you wrote the ebook in it or something.
I feel that you just could do with a few % to power the message home a little bit, however
other than that, that is wonderful blog. An excellent read.
I’ll certainly be back.
Also visit my site: real estate AI marketing
Pretty! This was an incredibly wonderful article. Thanks for supplying this information.
My webpage – listing video generator free
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-wood-metal/krug-vismutovyy-wood-metal/
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/list/list-7kh2smf-3x600x1200-gost-19903-74/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-250kh400-mm-lsdch/
Наличие калькулятора металлопроката упрощает расчет веса и стоимости
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-sn43pb43bi14a—iec-61190-1-3/krug-vismutovyy-sn43pb43bi14a—iec-61190-1-3/
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-60kh60kh6-mm-c35e-en-10056-1/
of course like your web-site but you need to check the spelling on several of your posts.
Many of them are rife with spelling issues and I find it very
troublesome to tell the truth nevertheless I’ll
certainly come back again.
Here is my web page :: gudang bokep indonesia
That is very fascinating, You’re an excessively skilled blogger.
I’ve joined your feed and look ahead to searching for extra of
your great post. Additionally, I’ve shared your
website in my social networks
Look at my site: real estate agent video tool
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-90-gradusov-34-mm-m2r-gost-r-52948-2008/
Hello! This post could not be written any better! Reading this post reminds me of my old room mate!
He always kept chatting about this. I will forward this post to him.
Pretty sure he will have a good read. Thanks for sharing!
Also visit my homepage Ford Engine Repair
Широкий выбор тугоплавких металлов, таких как вольфрам и молибден
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-h48bi3a—jis-z-3282/krug-vismutovyy-h48bi3a—jis-z-3282/
I have read so many articles on the topic of the blogger lovers however
this piece of writing is actually a good post, keep it up.
Also visit my homepage :: iklan kontol
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-12kh1200kh2500-mm-a265-astm-a480/
Виртуальные развлекалочки на основе криптовалют становятся все популярнее.
my page – 10 лучших топ казино
I simply could not go away your web site prior to suggesting
that I actually loved the standard info an individual supply for
your guests? Is going to be back frequently to
investigate cross-check new posts
Take a look at my blog Ford Coyote Engine Repair
I’ll right away snatch your rss feed as I can not to find your e-mail subscription link or e-newsletter service.
Do you’ve any? Please allow me recognize in order that I may subscribe.
Thanks.
Here is my website; real estate AI marketing
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-400kh700-mm-los/
Hi, I do think this is an excellent website.
I stumbledupon it ;) I am going to come back yet again since
i have book marked it. Money and freedom is the
greatest way to change, may you be rich and
continue to guide others.
Also visit my blog … this contact form
Продажа проволоки из тугоплавких металлов востребована в электронике
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-cac906—jis-h-5120-2016/provoloka-vismutovaya-cac906—jis-h-5120-2016/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-10kh2nv2f-2x1000x2000-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Wow, amazing blog layout! How long have you been blogging for?
you made blogging look easy. The overall look of your web site
is great, let alone the content!
Look at my web blog: reddit chinatime
Greetings! This is my first comment here so I just
wanted to give a quick shout out and tell you I really
enjoy reading your articles. Can you recommend any other blogs/websites/forums that cover the same subjects?
Thanks for your time!
Feel free to visit my page Admission List
Howdy this is kinda of off topic but I was wondering if blogs
use WYSIWYG editors or if you have to manually code with HTML.
I’m starting a blog soon but have no coding experience so I wanted to get
guidance from someone with experience. Any help would be enormously appreciated!
Look into my web page :: Earn money by watching ads
These are actually fantastic ideas in about blogging.
You have touched some pleasant points here. Any
way keep up wrinting.
Look at my blog post :: Nominee shareholder service
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-14-7-mm-m1rm-gost-r-52948-2008/
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89837—cda/lenta-vismutovaya-c89837—cda/
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-15kh25t-5x1200x1400-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Thanks for ones marvelous posting! I truly enjoyed reading it, you might be
a great author.I will be sure to bookmark your blog and definitely will come back later on. I want to encourage you continue your great posts, have a nice weekend!
Also visit my blog … Offshore bank account
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-130-mm-lts40mts3a/
Лаконичное приветствие на главной странице сразу вводит в курс дела
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c-6801—jis-h-3250-2015/truba-vismutovaya-c-6801—jis-h-3250-2015/
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/soedineniia-shtutserno-tortsovye-nakidnye-perekhodnye-vstyk/
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/provoloka-monel/provoloka-monel-3-mm-nmzhmts28-2-5-1-5-tu-48-21-7-2007/
Hey just wanted to give you a quick heads up and let you know a few of the pictures aren’t loading correctly.
I’m not sure why but I think its a linking issue. I’ve tried it
in two different browsers and both show the same results.
Also visit my web blog: DWA file format
Использование современных технологий защиты данных пользователей
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-a25b10c5—en-61190-1-3/poroshok-vismutovyy-a25b10c5—en-61190-1-3/
Hi there to all, how is the whole thing, I think every one is getting more from this
web page, and your views are good designed for new viewers.
Review my web-site … Earn money by playing games
В каталоге представлены конденсаторные ниобиевые порошки высокой чистоты, необходимые для современной электроники.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-khn77tiur-3x1400x2000-gost-24982-81-zharoprochnyi-goriachekatanyi/
Hello! Do you know if they make any plugins to assist
with SEO? I’m trying to get my blog to rank for some targeted
keywords but I’m not seeing very good success. If you know of any please share.
Appreciate it!
Feel free to visit my page online casino canada player friendly
This piece of writing will assist the internet users for setting
up new web site or even a blog from start to end.
Also visit my web-site; trusted online blackjack canada
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-149-mm-lts38mts2s2/
Wow, amazing weblog structure! How long have you been running a blog
for? you make running a blog glance easy. The overall glance of your web site is fantastic,
let alone the content!
Take a look at my web-site; all yono apps
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-142—en-iso-9453/lenta-vismutovaya-142—en-iso-9453/
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-stal-3-30×7-gost-21729-76/
บทความนี้ ให้ข้อมูลดี ครับ
ดิฉัน เพิ่งเจอข้อมูลเกี่ยวกับ หัวข้อที่คล้ายกัน
ซึ่งอยู่ที่ betflik199
น่าจะถูกใจใครหลายคน
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Artikel yang sangat menarik dan informatif. Banyak pengguna di Indonesia mencari informasi terpercaya
tentang viagra indonesia dan kesehatan pria.
Konten seperti ini sangat membantu pembaca memahami
penggunaan yang aman dan efektif.
Terima kasih atas artikel yang bermanfaat ini. Topik
viagra indonesia memang banyak dicari saat ini, terutama bagi mereka yang ingin mendapatkan informasi kesehatan pria secara aman dan tepat.
Konten yang bagus dan mudah dipahami. Informasi mengenai viagra indonesia sangat
relevan dan membantu banyak orang mendapatkan edukasi yang benar tentang kesehatan pria.
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-106kh92kh2-1-mm-15kh19-mm-tverdaia-paika-m1r-gost-32590-2013/
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-low-aluminum—stratcor-1/list-vanadievyy-low-aluminum—stratcor-1/
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-120kh80kh12-mm-42crmo4-en-10056-1/
Greetings! I know this is kinda off topic but I was wondering if you
knew where I could get a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having difficulty finding
one? Thanks a lot!
Visit my site alquiler de local para fiestas
Hi there! I realize this is kind of off-topic but I had to ask.
Does managing a well-established blog like yours require a large amount of work?
I am completely new to operating a blog but I do write in my journal on a daily basis.
I’d like to start a blog so I can easily share my experience and feelings online.
Please let me know if you have any suggestions or tips for new aspiring bloggers.
Appreciate it!
Feel free to surf to my website 비아그라 구입
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-0-9×550-mm-l63-gost-931-90/
I enjoy, cause I found just what I was taking a look for.
You have ended my four day long hunt! God Bless you man. Have a nice day.
Bye
Feel free to visit my homepage … 동탄출장마사지
Hello there! I simply would like to give you a big thumbs up for the excellent information you’ve got right here on this post.
I will be returning to your blog for more soon.
My homepage: hair transplant turkey price
Экспертная консультация при выборе сплавов помогает клиентам оптимизировать затраты и избежать технологических ошибок.
https://rms-ekb.ru/catalog/plity/plita-60khsmf-18x160x250-gost-19903-74/
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt1-0-1/polosa-titanovaya-vt1-0-1/
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-125kh75kh10-mm-c15e-en-10056-2/
After I initially left a comment I appear to have
clicked the -Notify me when new comments are added- checkbox and from now
on every time a comment is added I receive 4 emails with the
exact same comment. There has to be an easy method you can remove
me from that service? Thanks!
Here is my webpage: dictionary sites
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-pt-7msv—gost-27265-87-1/truba-titanovaya-pt-7msv—gost-27265-87-1/
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-4-5kh50-mm-lzhmts59-1-1-tu-48-21-847-89/
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/list/list-u13a-2x1000x1000-gost-19903-74/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-22kh18kh0-9-mm-8kh10-mm-tverdaia-paika-m2m-gost-r-52922-2008/
Наличие прецизионных сплавов в ассортименте подтверждает работу компании с высокоточными и наукоемкими материалами.
https://rms-ekb.ru/catalog/kanaty-dlia-talei/
I love what you guys are up too. This type of clever work and reporting!
Keep up the awesome works guys I’ve you guys to my
own blogroll.
My blog ling bokep indonesia
all the time i used to read smaller articles or reviews that as well clear their motive, and that is also
happening with this post which I am reading at this place.
Check out my web-site: частная наркология
Возможность заказа продукции в розницу и оптом (судя по описанию)
https://redmetsplav.ru/store/tantal-i-ego-splavy/tantal-ta-nb3-1/truba-tantalovaya-ta-nb3/
It’s an amazing piece of writing for all the internet users;
they will get advantage from it I am sure.
my blog post; slon4
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-12kh2nvfa-3-2x1700x1200-gost-19903-2006-gladkii-chernyi-goriachekatanyi/
Технические характеристики сплавов помогают инженерам в подборе
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nbp-4—gost-26252-84-1/izdeliya-iz-niobiya-nbp-4—gost-26252-84/
Do you mind if I quote a couple of your articles as long as I provide credit and sources back to your site?
My blog site is in the very same area of interest as yours and my
users would genuinely benefit from some of
the information you provide here. Please let me
know if this alright with you. Thanks!
Take a look at my web-site แทงบอลโลก
Pretty nice post. I simply stumbled upon your weblog and wanted to mention that I
have really enjoyed surfing around your blog posts.
In any case I will be subscribing in your feed
and I hope you write once more soon!
Also visit my blog post – โมเดลธุรกิจ
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-u10-4-5-gost-7417-75/
Наличие калькулятора металлопроката упрощает расчет веса и стоимости
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-vm-1/prutok-molibdenovyy-vm/
Компания занимается реализацией ферросплавов, необходимых для качественного легирования сталей на литейных участках.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-08kh18n10t-1-2x1500x1300-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mr-47vp-1/folga-molibdenovaya-mr-47vp/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40-5kh18-mm-m2r-gost-r-52948-2008/
ООО «РМС» предлагает широкий спектр цветного проката, включая медь, латунь, бронзу и дюралюминий.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-stal-20-70×4-gost-21729-76/
Great delivery. Sound arguments. Keep up the good spirit.
Here is my web site … แทงบอลโลก
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-fmo58-1/list-molibdenovyy-fmo58/
It’s really a great and useful piece of info.
I am satisfied that you just shared this helpful information with us.
Please keep us up to date like this. Thanks for sharing.
My web page :: click here
Wow that was unusual. I just wrote an extremely long
comment but after I clicked submit my comment didn’t show up.
Grrrr… well I’m not writing all that over
again. Anyways, just wanted to say excellent blog!
Stop by my web blog – EBT file
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-125kh75kh8-mm-30crnimo8v-uni-6762/
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-ze10a/izdeliya-iz-magniya-ze10a/
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/plity/plita-75khsmf-20x160x125-gost-19903-74/
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-r60702—uns/krug-magnievyy-r60702—uns/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku70kh1-4mmm2gost-32590-2013/
I do not know if it’s just me or if perhaps everyone else encountering
issues with your website. It seems like some of
the written text on your posts are running off the screen. Can somebody else please comment and let me know
if this is happening to them as well? This might be a issue with my internet
browser because I’ve had this happen before. Many thanks
Here is my blog find out more
No matter if some one searches for his vital thing,
thus he/she desires to be available that in detail, thus that thing is maintained over here.
Have a look at my web page: 광주호빠
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgzn6zr/krug-magnievyy-mgzn6zr/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-24kh2-5kh10000-mm-mnzhmts10-1-1-gost-10092-2006/
Everyone loves it when people come together and share opinions.
Great blog, keep it up!
Also visit my web blog; ws登录
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/list/list-kh-3x1000x1000-gost-19903-74/
Awesome! Its really amazing article, I have got much clear idea
about from this paragraph.
My website – 비아그라 구매
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-66-7kh57kh1-4-mm-11kh14-mm-tverdaia-paika-m3m-gost-32590-2013/
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mdc1a—jis-h-5303/lenta-magnievaya-mdc1a—jis-h-5303/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-11kh1-mm-la-gost-13942-86/
Inspiring quest there. What happened after? Thanks!
My website: porn
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-stal-45-100x1700x1400-gost-r-52146-2003-polimernyi-neotsinkovannyi-kholodnokatanyi/
Please let me know if you’re looking for a author for your
blog. You have some really good articles and I feel I would be a good asset.
If you ever want to take some of the load off, I’d love
to write some articles for your blog in exchange for a link back to mine.
Please shoot me an e-mail if interested. Thank you!
Take a look at my web site; Best Perfume store in India
Описание применения металлов в атомной энергетике подчеркивает качество
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-9—bs-2970/lenta-magnievaya-mag-9—bs-2970/
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-ad33-3x50x43-gost-13621-90/
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-70kh70kh7-mm-18crnimo7-6-en-10056-2/
Tremendous things here. I am very happy to look your post.
Thanks a lot and I’m having a look forward to contact you.
Will you please drop me a e-mail?
Feel free to surf to my blog :: transmission overhaul
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-151—bs-3370/list-magnievyy-mag-151—bs-3370/
Highly energetic post, I enjoyed that bit. Will there be a
part 2?
Here is my web site: trailer rentals in dallas
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m22-20-5kh1-2-mm-l63-din-471/
Simply wish to say your article is as astonishing. The clearness in your put up is just nice
and that i can think you’re a professional in this subject.
Fine with your permission allow me to snatch your feed
to keep updated with forthcoming post. Thanks one million and please keep up the rewarding work.
my site; transmission shop
Оперативная логистика и поддержка на всех этапах сделки позволяют минимизировать сроки простоя производственных линий заказчиков.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-65kh800-mm-acroni-4311-en-iso-18286/
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m18540—uns/folga-magnievaya-m18540—uns/
Way cool! Some extremely valid points! I appreciate you writing this article and the rest of the website
is also really good.
Also visit my blog; w88 khung bo
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-1561-11x175x300-gost-13621-90/
Your style is really unique in comparison to other folks I’ve read stuff from.
Many thanks for posting when you’ve got the opportunity,
Guess I will just bookmark this page.
Also visit my webpage – transmission repair
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-stal-20-508×65-gost-21729-76/
It’s going to be ending of mine day, but before finish I am reading this wonderful post to increase my knowledge.
My blog post :: Buy Arabic Perfumes online in India
Having read this I thought it was extremely informative.
I appreciate you taking the time and effort to put this article together.
I once again find myself personally spending a significant amount of time both reading
and leaving comments. But so what, it was still worthwhile!
my web page; yaar win
Hello there! This blog post could not be written any
better! Looking at this article reminds me of my previous
roommate! He constantly kept preaching about this. I
most certainly will forward this post to him. Fairly certain he will have a great read.
Thanks for sharing!
Feel free to surf to my page … javmost
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m13320—uns/polosa-magnievaya-m13320—uns/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-40kh1-7-mm-lts38mts2s2-gost-13943-86/
Наличие на складе редких металлов, таких как цирконий, выделяет компанию на фоне конкурентов, торгующих только массовым прокатом.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-120kh120kh10-mm-14nicr10-en-10056-1/
I constantly emailed this weblog post page to all my associates, because if like to
read it afterward my links will too.
Check out my web page … Plugs
Great resources and tips for families here.
I like what you guys tend to be up too. Such clever work and exposure!
Keep up the great works guys I’ve you guys to my blogroll.
Feel free to surf to my blog … Packing Machine
Наличие калькулятора металлопроката упрощает расчет веса и стоимости
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11611—uns/pokovka-magnievaya-m11611—uns/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-d16-5-2x82x140-gost-13621-90/
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-4kh2v5f-17-6-gost-7417-75/
Keep on writing, great job!
Feel free to surf to my web page – ladyclub777
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m10100—uns/poroshok-magnievyy-m10100—uns/
I pay a quick visit each day some websites and sites to read posts, however this
webpage offers feature based content.
My web blog … betoranje casino
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-50kh2kh12000-mm-mnzhmts30-1-1-gost-10092-2006/
Использование файлов cookie и политика конфиденциальности соответствуют закону
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mg99-80b—iso-8287/provoloka-magnievaya-iso-mg99-80b—iso-8287/
I’m impressed, I must say. Seldom do I come across a blog that’s both
educative and entertaining, and without a doubt,
you have hit the nail on the head. The problem is an issue that not
enough men and women are speaking intelligently about.
I’m very happy I found this in my search for something regarding this.
Also visit my site yaarwin
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/list/list-u9a-26x1000x1000-gost-19903-2006/
Удобное разделение продукции на сплавы и конкретные виды проката
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-hk32a—mil-m-46062/truba-magnievaya-hk32a—mil-m-46062/
Наличие никелевых сплавов гарантирует высокую коррозийную стойкость оборудования, создаваемого заказчиками.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r18f2k5-88-gost-7417-75/
This is really interesting, You’re a very skilled blogger. I have joined your feed and look forward to seeking more of your great post. Also, I’ve shared your web site in my social networks!
How come you do not have your website viewable in mobile format? cant see anything in my Droid.
Отраслевой охват впечатляет: от медицины до космической промышленности
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-mgse3zn2zr1—din-1729-part-2/provoloka-magnievaya-g-mgse3zn2zr1—din-1729-part-2/
Важным преимуществом является возможность изготовления деталей и изделий по индивидуальным чертежам заказчика.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-khn78t-3-2x1250x1500-gost-24982-81-zharoprochnyi-kholodnokatanyi/
I was wondering if you ever thought of changing the layout
of your site? Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content so people could connect with it better.
Youve got an awful lot of text for only having 1 or 2 pictures.
Maybe you could space it out better?
My web-site; Uhren
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/tavr-aliuminievyi/aliuminievyi-tavr-ad31t1-50kh50kh3-gost-13622-91/
There is perceptibly a lot to identify about this. I consider you made some good points in features also.
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-a6z3—afnor-nf-a57-704/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-70kh70kh7-mm-c60-en-10277/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-16kh2kh13000-mm-mnzhmts10-1-1-gost-10092-2006/
I was reading through some of your content on this internet site and I believe this web site is very informative ! Continue posting .
A person necessarily lend a hand to make seriously articles
I would state. This is the first time I frequented your web page and thus far?
I surprised with the research you made to create this actual publish amazing.
Excellent job!
Here is my blog post … yaar win
Hello there! Would you mind if I share your blog with
my twitter group? There’s a lot of people that I think
would really enjoy your content. Please let me know.
Thank you
my site :: bet oranje
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mc21210—en-1753/list-magnievyy-en-mc21210—en-1753/
География деятельности компании охватывает всю территорию России, обеспечивая металлом предприятия в удаленных регионах.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-1kh900kh1400-mm-dc05-1-0312-en-10131/
Fantastic goods from you, man. I have understand your stuff
previous to and you’re just too fantastic. I really like what you have acquired here,
certainly like what you are saying and the way in which you say it.
You make it enjoyable and you still care for to keep it sensible.
I can not wait to read much more from you.
This is really a wonderful web site.
Feel free to surf to my blog … betoranje promo code
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/list-aliuminievyi-riflenyi/list-aliuminievyi-riflenyi-1-5kh1200kh3000-mm-vd1nr-kvintet/
Удобное разделение продукции на сплавы и конкретные виды проката
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-b-737-grade-r1—astm-b737/izdeliya-iz-magniya-b-737-grade-r1—astm-b737/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-12kh18n10t-22×1-8-gost-21729-76/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-19kh1-5kh7000-mm-mnzhmts10-1-1-gost-10092-2006/
crushon ai chat, crushon ai alternative website is an innovative platform that users can connect with advanced AI.
This unique technology boosts user experience, enabling
conversations feel more genuine.
Cabinet IQ
8305 Statе Hwy 71 #110, Austin,
TX 78735, United Statеs
254-275-5536
Guide
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az91a—astm-b275/izdeliya-iz-magniya-az91a—astm-b275/
This is very attention-grabbing, You’re an excessively skilled blogger.
I have joined your feed and look forward to in quest of
more of your fantastic post. Additionally, I’ve shared your website in my social networks
Also visit my site: 남성 건강 정보 플랫폼 시알리스 구매
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-125kh75kh10-mm-x2crnimon25-7-4-en-10088-3/
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku64kh2mmm3rmgost-r-52922-2008/
Удобное разделение продукции на сплавы и конкретные виды проката
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az21—csa-hg-5/provoloka-magnievaya-az21—csa-hg-5/
Artikel yang sangat menarik dan informatif. Banyak pengguna di Indonesia mencari informasi terpercaya tentang viagra indonesia
dan kesehatan pria. Konten seperti ini sangat membantu
pembaca memahami penggunaan yang aman dan efektif.
Terima kasih atas artikel yang bermanfaat
ini. Topik viagra indonesia memang banyak dicari saat ini, terutama bagi mereka yang ingin mendapatkan informasi kesehatan pria secara aman dan tepat.
Konten yang bagus dan mudah dipahami. Informasi mengenai viagra indonesia sangat
relevan dan membantu banyak orang mendapatkan edukasi yang benar tentang kesehatan pria.
Наличие никелевых сплавов гарантирует высокую коррозийную стойкость оборудования, создаваемого заказчиками.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-kh12vmf-4-8-gost-7417-75/
My brother recommended I might like this blog. He was entirely right.
This post actually made my day. You cann’t imagine just how much time I had spent for this information! Thanks!
Look into my site cialis
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-24kh2kh1000-mm-mnzhmts10-1-1-gost-10092-2006/
Наличие циркония свидетельствует о работе с высокотехнологичными заказами
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-am90a—astm-b275/folga-magnievaya-am90a—astm-b275/
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-14g2-40x25x5-gost-19771-93/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku9kh1mmm2rgost-r-52922-2008/
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-a5-24-erzr3—aws-a5-24/provoloka-magnievaya-a5-24-erzr3—aws-a5-24/
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/list/list-kh12-3x1200x2500-gost-19903-74/
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/magnievyi-prutok/magnievyi-prutok-26-mm-ma2-gost-18351-73/
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-4604—mnc-46/lenta-magnievaya-4604—mnc-46/
Artikel yang sangat menarik dan informatif. Banyak pengguna di
Indonesia mencari informasi terpercaya tentang viagra indonesia dan kesehatan pria.
Konten seperti ini sangat membantu pembaca memahami penggunaan yang aman dan efektif.
Terima kasih atas artikel yang bermanfaat ini. Topik viagra indonesia memang banyak
dicari saat ini, terutama bagi mereka yang ingin mendapatkan informasi kesehatan pria
secara aman dan tepat.
Konten yang bagus dan mudah dipahami. Informasi mengenai viagra indonesia sangat relevan dan membantu banyak orang mendapatkan edukasi
yang benar tentang kesehatan pria.
My page bokep indonesia
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r9k5-17-2-gost-7417-75/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku80kh2-8mmm1rmgost-r-52922-2008/
Hi, everything is going sound here and ofcourse every one is sharing information, that’s truly good, keep up writing.
Look at my blog post :: Oxbet
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-s-chechevichnym-rifleniem-25kh600kh800-mm-12kh18n10t-gost-8568-77/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/tkanaia-latunnaia-setka/setka-tkanaia-latunnaia-0-4×0-9-l63/
Artikel yang sangat menarik dan informatif. Banyak pengguna
di Indonesia mencari informasi terpercaya tentang viagra
indonesia dan kesehatan pria. Konten seperti ini
sangat membantu pembaca memahami penggunaan yang aman dan efektif.
Terima kasih atas artikel yang bermanfaat ini.
Topik viagra indonesia memang banyak dicari saat ini, terutama bagi mereka yang ingin mendapatkan informasi kesehatan pria secara aman dan tepat.
Konten yang bagus dan mudah dipahami. Informasi mengenai viagra indonesia sangat relevan dan membantu banyak orang mendapatkan edukasi yang benar
tentang kesehatan pria.
Here is my website :: bokep indonesia
Ich liebe NV Casino, weiter so — tolle Inhalte!
NV Casino Plattform
Важным преимуществом является возможность изготовления деталей и изделий по индивидуальным чертежам заказчика.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-st3sp5-250x250x28-gost-19771-93/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku42kh1-1mmm1gost-32590-2013/
I’m very pleased to find this great site. I need to to thank you
for your time just for this fantastic read!! I definitely appreciated every bit of it
and I have you book-marked to see new stuff on your website.
Visit my web-site – Floor Stand Display Rack
ООО «РМС» предлагает широкий спектр цветного проката, включая медь, латунь, бронзу и дюралюминий.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-20kh-9x1900x1500-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-kapilliarnaia-trubka/latunnaia-kapilliarnaia-trubka-1-8kh0-35kh10000-mm-l63-gost-2624-2016/
Tremendous things here. I am very happy to see your article.
Thank you so much and I am taking a look forward to touch you.
Will you kindly drop me a mail?
Feel free to visit my blog post Lucky88
Thanks for discussing the issues and covering them in a well written format.
A good web site with interesting content, that’s what I need. Thank you for making this web site, and I will be visiting again. Do you do newsletters? I Can’t find it.
This website has lots of really useful stuff on it. Thanks for informing me.
I have to say this post was certainly informative and contains useful content for enthusiastic visitors. I will definitely bookmark this website for future reference and further viewing. cheers a bunch for sharing this with us!
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-kh20n80-120x1400x1000-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku27-4kh1-6mmm1mgost-32590-2013/
I have read several just right stuff here. Definitely value bookmarking for revisiting.
I surprise how so much effort you put to make any such magnificent informative web site.
Here is my page … Red88
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-75kh75kh6-mm-28mn6-en-10056-1/
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-6kh0-7-mm-lts40mts3zh-gost-13942-86/
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-4kh2v5mf-45-gost-5950-2000/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku22kh0-9mmm3rtgost-32590-2013/
Awesome post.
Also visit my homepage undangan website
I’d like to find out more? I’d love to find out some additional information.
My site :: Pool Rack
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-12kh17-125x125x12-gost-19771-93/
Hello I am so glad I found your website, I really found you
by mistake, while I was looking on Digg for something else, Anyhow I am
here now and would just like to say many thanks for a tremendous post and a all round entertaining blog (I also love the
theme/design), I don’t have time to read it all at the
moment but I have saved it and also included your RSS feeds,
so when I have time I will be back to read a lot more,
Please do keep up the excellent work.
Also visit my web-site … Debet
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-45kh1-7-mm-ls59-gost-13942-86/
I’m really enjoying the design and layout of
your site. It’s a very easy on the eyes which makes it much more enjoyable for me to come here
and visit more often. Did you hire out a designer to create your theme?
Excellent work!
Also visit my page … homepage
Thank you, I have just been searching for information about this topic for ages and yours is the greatest I’ve discovered till now. But, what about the conclusion? Are you sure about the source?
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/list/list-9khs-18x500x1000-gost-19903-74/
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-64kh55kh1-4-mm-32-5kh34-5-mm-tverdaia-paika-m2m-gost-r-52922-2008/
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-4khv2s-450-gost-2590-2006/
Thank you, I have just been looking for information approximately this topic for ages and yours
is the best I have came upon so far. But,
what in regards to the conclusion? Are you positive about the source?
My web page – Da88
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-38kh1-7-mm-ls-gost-13942-86/
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-stal-10-85x1900x1550-gost-r-52146-2003-polimernyi-neotsinkovannyi-kholodnokatanyi/
Hmm is anyone else having problems with the pictures on this blog loading?
I’m trying to figure out if its a problem on my end or if it’s the blog.
Any suggestions would be greatly appreciated.
Feel free to visit my web site – free
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-28kh23kh0-9-mm-9kh11-mm-tverdaia-paika-m2rm-gost-r-52922-2008/
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-100kh100kh10-mm-36nicrmo16-uni-6762/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m19-17-5kh1-2-mm-lts40sd-din-471/
ООО «РМС» обеспечивает поставки специализированных сварочных материалов для сложных условий эксплуатации.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-25kh2gnta-16x1000x1100-gost-r-52146-2003-polimernyi-neotsinkovannyi-kholodnokatanyi/
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-159kh135kh2-6-mm-63-5kh59-5-mm-tverdaia-paika-m1t-gost-32590-2013/
Wow! Finally I got a blog from where I can genuinely obtain helpful data regarding my study and knowledge.
My web page https://mckinneylplumbing.com/
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-09kh16n4b-1-5x1200x1600-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
I have been surfing on-line greater than three hours
today, yet I never found any fascinating article like yours.
It is beautiful worth enough for me. In my opinion, if all webmasters and bloggers
made good content material as you did, the net will likely be much
more useful than ever before.
Here is my site – IDM crack
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m41-37-5kh1-75-mm-lts25s2-din-471/
Наличие никелевых сплавов гарантирует высокую коррозийную стойкость оборудования, создаваемого заказчиками.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-65kh50kh5-mm-c10e-uni-6762/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-76-1kh65kh1-6-mm-33-5kh36-5-mm-tverdaia-paika-m3r-gost-32590-2013/
This is really interesting, You are a very skilled blogger.
I have joined your rss feed and look forward to seeking
more of your fantastic post. Also, I have shared your site in my social networks!
Look at my web blog … cleaning company Halifax
Компания занимается реализацией ферросплавов, необходимых для качественного легирования сталей на литейных участках.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-u11-15-5-gost-7417-75/
Hi there! Would you mind if I share your blog with my myspace group?
There’s a lot of folks that I think would really enjoy your content.
Please let me know. Thanks
Feel free to surf to my web page – whatapp网页版登入
I got this website from my buddy who informed
me concerning this web page and at the moment this
time I am visiting this web site and reading very informative posts here.
My page … platform ly lifetime deal
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m60-55-8kh2-mm-ls59-din-471/
Ориентация на долгосрочные отношения с клиентами позволяет компании формировать индивидуальные условия оплаты и графики поставок.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-90kh90kh7-mm-40nicrmo22-din-1029/
Howdy very nice site!! Man .. Beautiful .. Amazing .. I’ll bookmark your site and take the feeds additionally?
I am satisfied to seek out so many useful information here within the publish, we want develop more strategies on this regard, thanks for sharing.
. . . . .
Look at my blog post – DCIM software
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-88-9kh76kh1-8-mm-37-5kh40-5-mm-miagkaia-paika-m2m-gost-32590-2013/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Innovative
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/list/list-khvg-120x1000x1000-gost-19903-2006/
Hi there i am kavin, its my first occasion to commenting anywhere, when i read
this paragraph i thought i could also make comment due to this brilliant paragraph.
Review my web-site … dealify vs appsumo
Yes! Finally someone writes about แทงบอลโลก.
Is it okay to put a portion of this on my weblog if perhaps I post a reference point to this web page?
Hello, I do believe your web site could possibly be having web browser compatibility problems.
Whenever I take a look at your site in Safari, it looks
fine however, when opening in IE, it’s got some overlapping
issues. I merely wanted to give you a quick heads up!
Besides that, wonderful website!
Look at my site :: black friday lifetime deals
I am glad to talk with you and you give me great help
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-260kh3-mm-ls59-gost-13943-86/
Hey there are using WordPress for your site platform? I’m new to the blog
world but I’m trying to get started and create my
own. Do you need any coding expertise to make your own blog?
Any help would be really appreciated!
Also visit my blog … หนังโป๊ฝรั่ง
I just couldn’t leave your web site prior to suggesting that I really enjoyed the standard info an individual supply to your guests? Is going to be again continuously in order to inspect new posts
Наличие на складе редких металлов, таких как цирконий, выделяет компанию на фоне конкурентов, торгующих только массовым прокатом.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-75kh75kh6-mm-28mn6-en-10056-2/
I just added your web site to my blogroll, I hope you would look at doing the same.
I all the time emailed this weblog post page to all my contacts, for the reason that if like to read it afterward my links will too.
my web page: slot kaya303
My spouse and I stumbled over here coming from a different website and thought I may as well check things out.
I like what I see so now i’m following you. Look forward to checking out your web page repeatedly.
Review my website :: water leak detection near me
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-108kh92kh2-1-mm-47-5kh51-5-mm-tverdaia-paika-m1r-gost-32590-2013/
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-12kh18n9-3x1500x1600-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Artikel yang sangat menarik dan informatif. Banyak pengguna di Indonesia mencari informasi terpercaya tentang
viagra indonesia dan kesehatan pria.
Konten seperti ini sangat membantu pembaca memahami penggunaan yang aman dan efektif.
Terima kasih atas artikel yang bermanfaat ini. Topik viagra indonesia memang banyak dicari saat ini, terutama bagi
mereka yang ingin mendapatkan informasi kesehatan pria secara aman dan tepat.
Konten yang bagus dan mudah dipahami. Informasi mengenai viagra
indonesia sangat relevan dan membantu banyak orang mendapatkan edukasi yang benar tentang kesehatan pria.
Thanks for some other great post. Where else may anybody get that kind of information in such an ideal method of writing? I’ve a presentation next week, and I am at the look for such information.
I think the admin of this web site is in fact working hard for his
site, because here every data is quality based stuff.
My blog – Aluminum Door
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-72kh1-7-mm-lts14k3s3-gost-13943-86/
Artikel yang sangat menarik dan informatif. Banyak pengguna di Indonesia
mencari informasi terpercaya tentang viagra indonesia dan kesehatan pria.
Konten seperti ini sangat membantu pembaca memahami penggunaan yang aman dan efektif.
Terima kasih atas artikel yang bermanfaat ini.
Topik viagra indonesia memang banyak dicari saat ini, terutama bagi mereka yang ingin mendapatkan informasi kesehatan pria secara aman dan tepat.
Konten yang bagus dan mudah dipahami. Informasi mengenai
viagra indonesia sangat relevan dan membantu banyak orang mendapatkan edukasi yang benar tentang kesehatan pria.
Here is my web page – bokep indonesia
Simply desire to say your article is as surprising. The clarity in your
post is simply spectacular and i can assume you’re
an expert on this subject. Well with your permission allow me to grab your RSS feed to keep
updated with forthcoming post. Thanks a million and please keep up the enjoyable work.
Visit my blog :: slon2 cc
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-150kh75kh9-mm-40crnimo6-en-10056-1/
Amazing! Your site has quite a few comment posts. How did you get all of these bloggers to look at your site I’m envious! I’m still studying all about posting articles on the net. I’m going to view pages on your website to get a better understanding how to attract more people. Thank you!
Its just like you read my thoughts! It’s like reading about my family.
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-54kh47kh1-2-mm-11kh13-mm-tverdaia-paika-m1m-gost-32590-2013/
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-08kh17t-1x1250x1800-gost-19903-2006-gladkii-chernyi-goriachekatanyi/
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Bestinclass
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-9kh0-8-mm-lts37mts2s2k-gost-13943-86/
Поставка продукции возможна не только в промышленных, но и в малых лабораторных объемах для исследовательских целей.
https://rms-ekb.ru/catalog/list/list-7khf-3x1200x3000-gost-19903-74/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-27-4kh23kh0-9-mm-18-4kh20-4-mm-miagkaia-paika-m1m-gost-32590-2013/
В каталоге представлены конденсаторные ниобиевые порошки высокой чистоты, необходимые для современной электроники.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-2kh1000kh4000-mm-1-4526-en-iso-9444-2/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m108-115kh4-mm-lk80-din-472/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r12f3-160-gost-2590-2006/
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-80kh68kh1-8-mm-13kh16-mm-tverdaia-paika-m1r-gost-r-52922-2008/
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-180kh180kh16-mm-c60-en-10277/
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m147-152kh4-mm-lts40s-din-472/
Наличие на складе редких металлов, таких как цирконий, выделяет компанию на фоне конкурентов, торгующих только массовым прокатом.
https://rms-ekb.ru/catalog/list/list-27kh2n2m1f-1x500x500-gost-19903-74/
Artikel yang sangat menarik dan informatif. Banyak pengguna di Indonesia mencari informasi terpercaya tentang
viagra indonesia dan kesehatan pria. Konten seperti ini sangat membantu pembaca memahami penggunaan yang aman dan efektif.
Terima kasih atas artikel yang bermanfaat ini. Topik viagra indonesia memang banyak dicari saat ini, terutama bagi mereka yang ingin mendapatkan informasi kesehatan pria
secara aman dan tepat.
Konten yang bagus dan mudah dipahami. Informasi mengenai viagra indonesia sangat relevan dan membantu banyak orang mendapatkan edukasi yang benar tentang kesehatan pria.
Incredible story there. What occurred after?
Thanks!
Feel free to surf to my web-site: Techxa airmatic
61iiax
I’m really impressed along with your writing talents and also
with the format in your blog. Is this a paid theme or did you customize
it your self? Anyway stay up the excellent quality writing, it’s rare to see a great blog
like this one these days..
Take a look at my website: control cable
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-15kh11kh0-7-mm-10-6kh12-6-mm-miagkaia-paika-m2rm-gost-r-52922-2008/
Ориентация на долгосрочные отношения с клиентами позволяет компании формировать индивидуальные условия оплаты и графики поставок.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-200kh200kh24-mm-x2crnimocuwn25-7-15-en-10088-3/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m152-158kh4-mm-lazhmts-din-472/
I appreciate, cause I found just what I was looking for. You’ve ended my four day long hunt! God Bless you man. Have a great day. Bye -.
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-170kh1200-mm-acroni-4435-en-iso-18286/
We absolutely love your blog and find the majority of your post’s to be exactly what I’m looking for. Do you offer guest writers to write content to suit your needs? I wouldn’t mind composing a post or elaborating on a number of the subjects you write about here. Again, awesome weblog!
We are a group of volunteers and starting a new initiative in our community. Your blog provided us with valuable information to work on|.You have done a marvellous job!
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-10kh7kh0-6-mm-7-8kh9-8-mm-tverdaia-paika-m3rm-gost-r-52922-2008/
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-20khn3a-14x1000x1550-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Cabinet IQ
8305 Ꮪtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Bookmarks
We recognize the value of your time, which is why we have incorporated
a Turbo Mode feature into Easy Videos Downloader.
Here is my web site … savefrom
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m29-31-1kh1-2-mm-lsd-din-472/
Наличие прецизионных сплавов в ассортименте подтверждает работу компании с высокоточными и наукоемкими материалами.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-6kh1250kh3000-mm-1-4510-en-iso-9444-1/
이것을 사람들와 공유해줘서 정말 감사합니다, 당신은
논하는 것을 실제로 이해하고 있습니다!
북마크했습니다. 제 사이트도 상의해 주세요 =).
우리 사이에 하이퍼링크 변경 약정을 맺을 수 있습니다.
I just couldn’t go away your website prior to suggesting that I
actually enjoyed the usual information a person provide for your visitors?
Is going to be back continuously in order to check out
new posts
Here is my blog post 비아그라 구매
Artikel yang sangat informatif dan bermanfaat.
Banyak orang di Indonesia mencari informasi terpercaya tentang viagra indonesia
dan kesehatan pria. Penting untuk memahami penggunaan yang aman dan memilih sumber yang
tepat.
Terima kasih atas informasi ini. Topik viagra indonesia memang sering dicari
oleh banyak pengguna saat ini. Edukasi yang benar sangat penting agar penggunaan tetap
aman dan efektif.
Konten yang bagus dan mudah dipahami. Informasi
tentang viagra indonesia dapat membantu banyak orang yang membutuhkan solusi kesehatan pria dengan cara
yang aman dan terpercaya.
Postingan yang sangat membantu. Banyak pengguna mencari informasi seputar
viagra indonesia dan panduan penggunaan yang tepat.
Artikel seperti ini sangat berguna bagi pembaca.
Artikel berkualitas dan penuh informasi. Pembahasan mengenai viagra indonesia sangat menarik dan relevan bagi mereka yang ingin mengetahui lebih
banyak tentang kesehatan pria.
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-70kh60kh1-4-mm-33-5kh36-5-mm-tverdaia-paika-m3rt-gost-32590-2013/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/plity/plita-7khg2vmf-26x400x160-gost-19903-74/
I’m gone to inform my little brother, that he should also
pay a visit this weblog on regular basis to get updated from most up-to-date gossip.
my web site … kaya303 slot
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-350kh800-mm-lsd/
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-stal-15-90x1250x1900-gost-r-52146-2003-polimernyi-otsinkovannyi-kholodnokatanyi/
Ищете аттестованного кадастрового инженера в
Московской области? Есть допуск к реестровым ошибкам.
Согласовываем с соседями.
Получить разрешение на строительство в Московской области
без ошибок в уведомлении. Проверим ВРИ и ПЗЗ.
Срок с гарантией решения.
Геоподоснова для строительства
в масштабе топографическая съемка 1 500:
200 – это план с отметками и зданиями.
Обновляем старые планы. Цена в формате
.dwg с подписями.
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-53-6kh27-4-mm-m3rt-gost-r-52948-2008/
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-kh-45-89-gost-7417-75/
Продолжайте в том же духе и
привлекайте ещё больше игроков!
платформа Olimp Casino
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m102-108kh4-mm-l63-din-472/
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-80kh80kh8-mm-c45-en-10056-2/
Enjoy smoother sign-ins through NNPH Login, built for easy Philippine slot gaming.
Hi, this weekend is pleasant in favor of me, since this moment i am reading this enormous informative piece of
writing here at my house.
My web page :: Kaya303 Login
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40kh17-mm-m1-gost-r-52948-2008/
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/list/list-u8-2x1000x1000-gost-21631-76/
Wow that was strange. I just wrote an really long comment but after I clicked submit my comment didn’t
appear. Grrrr… well I’m not writing all that over again. Anyway,
just wanted to say superb blog!
Here is my site – Debet
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-800kh200-mm-l63/
Компания занимается реализацией ферросплавов, необходимых для качественного легирования сталей на литейных участках.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-100kh65kh8-mm-c25e-en-10056-1/
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40kh10-mm-m1r-gost-r-52948-2008/
My developer is trying to convince me to move to .net from PHP.
I have always disliked the idea because of the costs.
But he’s tryiong none the less. I’ve been using Movable-type on a number of websites for about a year and am worried
about switching to another platform. I have heard excellent
things about blogengine.net. Is there a way I can transfer all
my wordpress posts into it? Any kind of help would be greatly appreciated!
My web-site … 제주여성전용마사지
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-38khs-32x1400x1500-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Do you mind if I quote a couple of your articles as long as I provide credit and sources
back to your website? My website is in the very
same niche as yours and my users would really benefit from a lot of the information you provide here.
Please let me know if this ok with you. Thanks!
Look at my web blog 정품 비아그라
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-210-mm-lts37mts2s2k/
Наличие на складе редких металлов, таких как цирконий, выделяет компанию на фоне конкурентов, торгующих только массовым прокатом.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-20kh17n2-11x1250x1600-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Its such as you read my thoughts! You appear to grasp so much approximately this, like you wrote the e-book in it or something.
I feel that you can do with some p.c. to drive the message house
a little bit, but instead of that, that is excellent
blog. An excellent read. I’ll definitely be back.
Also visit my web-site More details
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-108kh34-mm-m2-gost-r-52948-2008/
Good information. Lucky me I ran across your website by accident (stumbleupon).
I have saved as a favorite for later!
my site; NyanCat
I am actually pleased to read this weblog posts which carries plenty of helpful
information, thanks for providing these kinds of information.
Feel free to visit my blog платный слив
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-70kh900-mm-acroni-4404-en-iso-18286/
My name is Mike, a normal American guy, and in the year
2018 I accidentally discovered one of the strangest sports ever invented:
CarJitsu.
In case this sounds unfamiliar, you are not alone.
The entire concept sounds like a comedy sketch. Two
competitors climb inside a compact vehicle and try to grapple each
other while being trapped between the dashboard and seats.
Yes, really. In most sports you have a ring, but in CarJitsu your
battlefield is a car cabin. This is what shocked
me the first time.
There are organized competitions, tournaments, championships,
and special events. Competitors come from different places and try to prove who can master the unusual format.
Compared to ordinary sports, every movement is
limited by the tight space. This leads to funny situations.
One second someone looks like a champion, and the next second they are stuck between the seats.
At that time I was heavily interested in sports. I watched football, basketball, MMA, and wrestling.
I also spent time reading about sportsbook odds. People around me talked about betting and sportsbooks.
Sometimes names like 1xBet would appear in conversations about
major sporting events, although CarJitsu was usually too strange to
be the main topic.
One night I saw a crazy highlight reel online. At first I thought
it was satire. Full-grown athletes were trying to wrestle inside a parked car while spectators were laughing, cheering, and recording videos.
I laughed so hard that I couldn’t breathe for a moment. Yet the more
I watched, the more fascinated I became.
Not long afterward, I found a local event and decided to watch in person. The crowd
energy was amazing. There were fans discussing sports, training,
and competition. Some people even joked about which athlete would be the favorite if a sportsbook ever offered odds on the matches.
Soon I wanted more than just watching. I signed up for
beginner training. The first training day was hilarious. I
hit my head on the roof, got stuck near a seat, and accidentally opened a door at the worst possible moment.
Everyone laughed. Yet I kept coming back.
Week after week, I improved. I learned how to use technique and movement.
The car stopped feeling tiny. Soon I was entering
local competitions. My friends thought I was completely crazy.
Whenever someone asked what sport I practiced, the conversation usually went like
this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The funniest and wildest experience happened during a tournament a few years
later. My opponent was built like a truck. He looked like
he could carry an engine block. Before the match started, he
smiled and said, “You’re going to need luck.” That should
have been a warning.
The moment the referee signaled, chaos exploded. We bounced between seats, bumped into doors, and nearly tangled ourselves
in everything inside the vehicle. The crowd was roaring.
People were laughing and shouting.
Then came the moment I will never forget.
My opponent grabbed the belt hanging beside the seat and accidentally turned it into what
looked like a dangerous rope. As we struggled for position, the belt
snapped across the cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “This is it”
He pulled, I twisted, the seat belt locked, the door opened slightly, and both of us somehow ended up tangled together like
two confused octopuses. The audience was laughing so hard that some people
could barely stay in their seats. It looked completely ridiculous.
For a brief moment, I genuinely thought my opponent was going to flatten me.
Fortunately, the officials quickly intervened when things became unsafe,
and the situation was resolved without serious injury.
Afterward we both burst out laughing. Spectators cheered. Even today people who were there still talk about “that crazy seat belt match.”
When I remember those years, CarJitsu remains one of the strangest sports I have ever
experienced. It gave me countless funny moments. Whether people are
discussing sports, betting, sportsbooks, competitions, or events,
very few things create reactions like CarJitsu.
If anybody asks for the weirdest sport I know, I always tell them about the day I
climbed into a car in 2018 and accidentally became a CarJitsu competitor.
The reaction is always the same. But after hearing
about tournaments, athletes, training sessions,
sports fans, betting conversations, sportsbook discussions, and my unforgettable seat belt battle, they usually
agree on one thing:
CarJitsu might be the craziest sport ever invented.
Feel free to visit my site – URL
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-200kh600-mm-lk1/
Hi there friends, nice post and fastidious urging commented here, I am in fact enjoying by these.
Have a look at my web-site: why canadian players choose trusted casino sites for dependable service canada
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-60khsmf-18-5-gost-7417-75/
Hi, I do believe this is an excellent website. I stumbledupon it ;) I am going to return yet again since I book
marked it. Money and freedom is the greatest way to change, may you be rich and continue to help others.
My page … ramalan shio kelinci togel
Howdy I am so delighted I found your weblog, I really found you by accident,
while I was researching on Bing for something else, Anyways I am here
now and would just like to say cheers for a incredible post and a all
round entertaining blog (I also love the theme/design), I don’t have time to look over it all at
the minute but I have saved it and also included your RSS feeds,
so when I have time I will be back to read a great deal more,
Please do keep up the excellent b.
Feel free to visit my web site ta88
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-64kh18-mm-m1e-gost-r-52948-2008/
В каталоге представлены конденсаторные ниобиевые порошки высокой чистоты, необходимые для современной электроники.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-06kh700kh1200-mm-m390-50k-en-10341/
Greetings from Carolina! I’m bored at work so I decided to check
out your website on my iphone during lunch break.
I enjoy the information you provide here and can’t wait to take a look when I get home.
I’m amazed at how quick your blog loaded on my mobile ..
I’m not even using WIFI, just 3G .. Anyways, excellent site!
my blog post Coche con chofer madrid
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-300kh200-mm-lts40mts3zh/
Oh my goodness! Amazing article dude! Thank you, However I am
going through issues with your RSS. I don’t understand the reason why I can’t subscribe to it.
Is there anybody else having the same RSS problems?
Anyone that knows the answer will you kindly respond? Thanx!!
Take a look at my web blog :: Mega Cine
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-kh12f1-3-8-gost-7417-75/
Hi, i think that i saw you visited my website thus i came to
“return the favor”.I’m attempting to find things to enhance my web site!I suppose
its ok to use a few of your ideas!!
my web site; Uk88
I visited many web pages but the audio feature for audio songs current at this web page is truly excellent.
My web page dabet
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-80kh25-mm-m1e-gost-r-52948-2008/
확실히 당신이 언급한 것을 믿습니다.
당신의 가장 좋아하는 이유는 인터넷에서 가장 쉬운
것을 알아야 할 것으로 보였습니다. 저는 당신에게 말합니다,
사람들이 그들이 모르는 걱정을 생각할
때 저는 확실히 짜증을 느낍니다. 당신은 부작용 없이 모든 것을 정의하고, 정상을
정확히 맞췄습니다. 사람들이 신호를 받을 수
있습니다. 아마 더 얻기 위해 다시 올 것입니다.
감사합니다
I am actually grateful to the owner of this web site
who has shared this great article at at this place.
What a find this blog is! Your posts are both informative and entertaining.
I’d love to see a series on inspirational quotes for work—it’s such a hot topic!
Thanks for sharing your knowledge. Best wishes!
이 블로그는 정말 대단합니다! Built-in SEO tools에 대한 글들이 너무 흥미롭고 잘 작성되었어요.
RSS 피드를 추가해서 최신 업데이트를 받아볼게요.
계속해서 이런 훌륭한 콘텐츠 부탁드립니다!
감사합니다!
Check out my website 비아그라 구매
Наличие прецизионных сплавов в ассортименте подтверждает работу компании с высокоточными и наукоемкими материалами.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-25kh25kh3-mm-16mncrb5-din-59370/
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-80kh500-mm-lmtssk/
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/list/list-u8a-10x1200x2500-gost-19903-74/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-27-4kh22-mm-m2m-gost-r-52948-2008/
Valuable information. Lucky me I found your site
by accident, and I’m surprised why this coincidence didn’t
happened earlier! I bookmarked it.
Look into my blog post – store manager dsw salary
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-120kh80kh12-mm-41cralmo7-uni-6762/
Neat blog! Is your theme custom made or did you download it from somewhere?
A design like yours with a few simple adjustements would really make
my blog stand out. Please let me know where you got your design. Thank you
Here is my site: MALWARE
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-30kh500-mm-lts16k4/
Hello There. I found your blog using msn. This
is a really well written article. I will make sure to bookmark
it and come back to read more of your useful information. Thanks for the post.
I will definitely comeback.
My website – 爱思
Primeiramente, o conversor do zeemo pro apk permite transformar vídeos do YouTube em formatos para TikTok,
Twitter (X) e Instagram diretamente no editor.
ООО «РМС» специализируется на поставках редких и тугоплавких металлов, таких как ниобий и вольфрам.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-60s2a-40x1550x1100-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Czech online casinos, Official Ceske Kasino umožňují zábavy
a šancí. Hráči si mají šanci vyzkoušet mnohé hry, včetně automaty, ruletu a blackjack.
S podporou moderní technologie mohou hráči zaregistrovat kdykoli a kdekoli.
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-90-gradusov-108-mm-m1r-gost-r-52948-2008/
When someone writes an article he/she retains the plan of a user in his/her brain that
how a user can understand it. Therefore that’s why this piece of writing is perfect.
Thanks!
Also visit my site: soap2day
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-neotsinkovannyi-35kh2000kh5000-mm-s235-gost-27772-2015/
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-900kh800-mm-los/
Thank you a lot for sharing this with all of us you
really know what you’re talking about! Bookmarked. Please additionally seek
advice from my site =). We could have a link alternate agreement among
us
Look at my blog: Dr Vorobjev
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-khn77tiuru-3-2x1000x1500-gost-24982-81-zharoprochnyi-kholodnokatanyi/
My name is Mike, a normal American guy, and in the year 2018 I
accidentally discovered one of the strangest sports ever invented:
car jitsu.
In case this sounds unfamiliar, you are not alone. The entire concept sounds like a joke.
Two athletes climb inside a tiny automobile and try to control each other while being trapped
between the dashboard and seats. Believe it or not. In most sports you have a court, but in CarJitsu your battlefield is the inside of a vehicle.
That is why people laugh when they first hear about it.
The sport has tournaments, championships, local events, and exhibition matches.
Competitors come from different places and try
to prove who can dominate inside the car. Unlike traditional combat sports,
every movement is limited by doors, seats, windows, and seat belts.
The result is pure chaos. One second someone looks like
a champion, and the next second they are folded like a pretzel.
At that time I was heavily interested in sports. I watched football, basketball, MMA, and wrestling.
I also spent time reading about sportsbook odds. People around
me talked about betting and sportsbooks. Sometimes names like 1xbet would
appear in conversations about major sporting events, although CarJitsu was usually too strange to be the main topic.
Late one evening I saw a crazy highlight reel online. Initially I believed it
was a joke. Grown adults were trying to grapple inside
a parked car while spectators were laughing,
cheering, and recording videos. I laughed so hard that I couldn’t breathe for a moment.
Yet the more I watched, the more fascinated
I became.
A few weeks later, I found a local event and decided
to watch in person. The event was unforgettable. There were fans discussing sports, training,
and competition. Some people even joked about which athlete would
be the favorite if a sports betting market ever offered odds on the matches.
Soon I wanted more than just watching. I signed up for beginner training.
The first training day was hilarious. I hit my head on the roof, got stuck
near a seat, and accidentally opened a door at the worst possible moment.
Everyone laughed. Yet I kept coming back.
As time passed, I improved. I learned how to use technique and movement.
The vehicle became familiar. Soon I was entering regional events.
My friends thought I was completely crazy. Whenever someone asked what sport I practiced, the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The most unforgettable competition happened at a major event.
My opponent was massive. He looked like he could lift a small house.
Before the match started, he smiled and said, “Hope you’re ready.” That should have been a warning.
The match began, chaos exploded. We bounced between seats, bumped into doors,
and nearly tangled ourselves in everything inside the
vehicle. The crowd was roaring. People were laughing and shouting.
Then came the moment I will never forget.
My opponent grabbed the belt hanging beside the seat and accidentally turned it into what looked like a crazy lasso.
As we struggled for position, the belt snapped across the cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “This is it”
He pulled, I twisted, the seat belt locked, the door opened slightly, and both of
us somehow ended up tangled together like a pile of cables.
The audience was laughing so hard that some people could barely stay in their seats.
The scene was unbelievable.
For a brief moment, I genuinely thought my opponent was going to crush me.
Luckily, the officials quickly intervened when things became unsafe,
and the situation was resolved without serious injury. Afterward we
both burst out laughing. Spectators cheered. Even today people who
were there still talk about “the legendary belt tangle.”
Looking back, CarJitsu remains one of the most unusual sports I
have ever experienced. It gave me great memories and incredible experiences.
Whether people are discussing sports culture and competition, very few things
create reactions like CarJitsu.
If anybody asks for the weirdest sport I know, I always tell them about the day I climbed into a car in 2018 and accidentally became a CarJitsu competitor.
Nobody believes it at first. But after hearing about tournaments, athletes, training sessions, sports fans, betting
conversations, sportsbook discussions, and my unforgettable seat belt battle, they
usually agree on one thing:
CarJitsu might be the craziest sport ever invented.
Here is my page more information
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-90-gradusov-15-mm-m2-gost-r-52948-2008/
This design is steller! You certainly know how to keep a reader amused.
Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Wonderful job.
I really loved what you had to say, and more than that, how you
presented it. Too cool!
Also visit my web site :: slon10.cc
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-stal-3-108×5-gost-21729-76/
With this issue, it’s important to have someone like you with something to say that really matters.
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-145-mm-ls59-1/
I for all time emailed this web site post page to all my friends, as if like to read it afterward my links will too.
My web site; bokep pijat indonesia
Наличие прецизионных сплавов в ассортименте подтверждает работу компании с высокоточными и наукоемкими материалами.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-khn60vt-160x1000x1000-gost-24982-81-zharoprochnyi-kholodnokatanyi/
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/list-mednyi/list-mednyi-0-6kh600kh1500-mm-m1m/
My name is Mike, a normal American guy, and back in 2018
I accidentally discovered one of the most bizarre sports I
had ever seen: Car Jitsu.
If you have never heard of it, you are not alone. The entire
concept sounds like something invented after a crazy bet.
Two competitors climb inside a tiny automobile and try
to score positions against each other while being
trapped between the seats. Believe it or not. In most sports you have a ring, but in CarJitsu your
battlefield is a cramped car interior. This is what shocked me the
first time.
There are organized competitions, tournaments, championships, and special events.
Participants gather from various regions and try to prove who can master
the unusual format. Unlike traditional combat
sports, every movement is limited by doors, seats, windows, and seat belts.
This leads to funny situations. One second someone looks like a champion, and the next second they are folded
like a pretzel.
During those days I was heavily interested in unusual athletic events.
I watched all kinds of competitions. I also spent time reading
about sports betting. People around me talked about betting and sportsbooks.
Sometimes names like 1xBet would appear in conversations about major sporting events,
although CarJitsu was usually too strange to be the main topic.
One evening I saw a crazy highlight reel online. At first I thought it
was satire. Full-grown athletes were trying to wrestle inside a
parked car while spectators were watching in disbelief.
I laughed so hard that I almost fell off my chair.
Yet the more I watched, the more fascinated I became.
Not long afterward, I found a local event and decided to attend.
The atmosphere was incredible. There were fans
discussing athletic techniques and sports culture.
Some people even joked about which athlete would be the favorite if a betting site ever offered
odds on the matches.
Soon I wanted more than just watching. I signed up for beginner training.
My first session was a disaster. I hit my head on the roof,
got stuck near a seat, and accidentally opened a door at the worst possible moment.
Even I laughed at myself. Yet I kept coming back.
Week after week, I improved. I learned how to use positioning, leverage, balance, and timing.
The vehicle became familiar. Soon I was entering local competitions.
My friends thought I was completely crazy. Whenever someone asked what
sport I practiced, the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The most unforgettable competition happened at a major event.
My opponent was built like a truck. He looked like he could bench-press a refrigerator.
Before the match started, he smiled and said, “Good luck.” That should have been a
warning.
As soon as the fight started, chaos exploded.
We bounced between seats, bumped into doors, and nearly tangled ourselves in everything inside the vehicle.
The crowd was roaring. Everyone was losing their minds.
Then came the moment I will never forget.
My opponent grabbed the car seat belt and accidentally turned
it into what looked like a dangerous rope. As we
struggled for position, the belt snapped across the cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “I can’t believe this is happening”
He pulled, I twisted, the seat belt locked, the door opened slightly,
and both of us somehow ended up tangled together
like a pile of cables. The audience was laughing so hard that some people could barely stay in their seats.
Nobody could believe what they were seeing.
For a brief moment, I genuinely thought my opponent
was going to flatten me. Luckily, the officials
quickly intervened when things became unsafe, and the situation was resolved without serious injury.
Afterward we both burst out laughing. Everyone loved it.
Even today people who were there still talk about
“the legendary belt tangle.”
Looking back, CarJitsu remains one of the most unusual sports I have ever
experienced. It gave me great memories and incredible experiences.
Whether people are discussing sports culture and competition, very few things
create reactions like CarJitsu.
When people want to hear a crazy sports story, I always tell them about
the day I climbed into a car in 2018 and accidentally became a CarJitsu competitor.
Nobody believes it at first. But after hearing about tournaments, athletes, training sessions, sports fans, betting conversations, sportsbook discussions, and
my unforgettable seat belt battle, they usually agree on one thing:
CarJitsu might be the craziest sport ever invented.
Here is my web site … url
ООО «РМС» обеспечивает поставки специализированных сварочных материалов для сложных условий эксплуатации.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-khvsg-125-gost-2590-2006/
People call me Mike, a regular guy from the USA, and back in 2018 I accidentally
discovered one of the strangest sports ever invented:
car jitsu.
If you have never heard of it, don’t worry. The entire concept sounds like a comedy sketch.
Two fighters climb inside a small car and try to grapple
each other while being trapped between the cramped
interior. Yes, really. In most sports you have a field, but in CarJitsu your battlefield is the inside of a vehicle.
This is what shocked me the first time.
It even has official events and competitive tournaments.
Competitors come from different places and try to prove who can adapt best to the strange
environment. Unlike traditional combat sports, every movement is limited by the vehicle’s interior.
The result is pure chaos. One second someone looks like a champion, and the next second
they are stuck between the seats.
During those days I was heavily interested in unusual athletic events.
I watched football, basketball, MMA, and wrestling. I also spent time reading about betting markets.
Many sports fans I knew compared sportsbook offers. Sometimes names
like the sportsbook 1xbet would appear in conversations about major sporting events, although CarJitsu was usually too
strange to be the main topic.
One night I saw a video clip online. Initially I
believed it was a joke. Competitive fighters were trying to grapple
inside a parked car while spectators were laughing, cheering, and recording videos.
I laughed so hard that coffee nearly came out
of my nose. Yet the more I watched, the more fascinated I became.
Soon after that, I found a local event and decided to watch in person. The event was unforgettable.
There were fans discussing athletic techniques and sports culture.
Some people even joked about which athlete would be
the favorite if a sports betting market ever offered odds on the matches.
Soon I wanted more than just watching. I signed up for beginner training.
My first session was a disaster. I hit my head on the roof, got stuck near a seat, and accidentally opened a
door at the worst possible moment. Everyone laughed.
Yet I kept coming back.
Month after month, I improved. I learned how to use smart tactics instead of brute strength.
The vehicle became familiar. Soon I was entering local competitions.
My friends thought I was completely crazy. Whenever someone asked what sport
I practiced, the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The most unforgettable competition happened at a major event.
My opponent was huge. He looked like he could lift a small house.
Before the match started, he smiled and said, “Good luck.” That should have
been a warning.
As soon as the fight started, chaos exploded. We bounced between seats, bumped into doors, and nearly tangled ourselves in everything inside the vehicle.
The crowd was roaring. People were laughing and shouting.
Then came the moment I will never forget.
My opponent grabbed the seat belt and accidentally turned
it into what looked like a wild whip. As we struggled for position, the belt snapped across the cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “I can’t believe this is happening”
He pulled, I twisted, the seat belt locked, the
door opened slightly, and both of us somehow ended up tangled together
like two confused octopuses. The audience was laughing so hard that some people could barely
stay in their seats. Nobody could believe what they were seeing.
For a brief moment, I genuinely thought my opponent
was going to crush me. Fortunately, the officials quickly intervened when things became unsafe, and the situation was resolved without serious injury.
Afterward we both burst out laughing. Everyone loved it.
Even today people who were there still talk about
“the seat belt incident.”
Looking back, CarJitsu remains one of the weirdest athletic competitions I have ever experienced.
It gave me countless funny moments. Whether people are discussing sports culture and competition, very few things create reactions like
CarJitsu.
Whenever someone asks me about unusual sports, I always tell them
about the day I climbed into a car in 2018 and accidentally became a CarJitsu competitor.
Most people laugh. But after hearing about tournaments, athletes, training sessions, sports fans, betting
conversations, sportsbook discussions, and my unforgettable seat belt
battle, they usually agree on one thing:
CarJitsu might be the craziest sport ever invented.
Review my web page; press release
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-42-mm-lts40mts1-5/
Thanks for any other excellent post. The place else may just anybody get that type of
info in such an ideal method of writing? I’ve a presentation next
week, and I am at the look for such information.
Feel free to surf to my site: Siete Chile
I’ll right away grab your rss as I can not find your email subscription hyperlink or e-newsletter
service. Do you’ve any? Kindly let me recognize so that
I may subscribe. Thanks.
Here is my blog :: 강남가라오케
My brother recommended I may like this blog. He used to be
entirely right. This post actually made my day. You cann’t believe just how so much time I had spent for this information! Thanks!
My homepage :: 강남가라오케
Компания занимается реализацией ферросплавов, необходимых для качественного легирования сталей на литейных участках.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-aisi-409-25x25x5-gost-19771-93/
This is very interesting, You are a very skilled blogger. I’ve joined your
feed and look forward to seeking more of your excellent post.
Also, I have shared your web site in my social networks!
my web site: clash verge官网
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-17kh1kh14000-mm-mnzhmts30-1-1-gost-10092-2006/
My name is Mike, a normal American guy, and during 2018 I
accidentally discovered one of the strangest sports ever invented:
Car Jitsu.
In case this sounds unfamiliar, most people haven’t.
The entire concept sounds like a joke. Two competitors climb inside
a tiny automobile and try to grapple each other while being
trapped between the cramped interior. No, I’m not kidding.
In most sports you have a court, but in CarJitsu your battlefield is the inside of
a vehicle. That is why people laugh when they first hear about it.
The sport has tournaments, championships, local events, and exhibition matches.
Participants gather from various regions and try to prove who can dominate inside the car.
Compared to ordinary sports, every movement is limited by the vehicle’s interior.
That creates hilarious moments. One second someone looks like a
champion, and the next second they are trapped near the steering wheel.
During those days I was heavily interested in competitive sports.
I watched all kinds of competitions. I also spent time reading about sportsbook odds.
Many sports fans I knew compared sportsbook offers.
Sometimes names like 1xBet would appear in conversations about major sporting events, although CarJitsu was usually too strange to be the
main topic.
One night I saw a crazy highlight reel online.
At first I thought it was satire. Competitive fighters were trying to wrestle inside a parked car while spectators were watching in disbelief.
I laughed so hard that I couldn’t breathe for a moment. Yet the more I
watched, the more fascinated I became.
Not long afterward, I found a local event and decided to watch in person. The crowd energy was
amazing. There were fans discussing athletic techniques and sports culture.
Some people even joked about which athlete would be the
favorite if a sportsbook ever offered odds on the matches.
Watching was not enough. I signed up for beginner training.
My debut practice was chaos. I hit my head on the roof, got stuck near a seat, and accidentally opened a door at the worst
possible moment. Even I laughed at myself.
Yet I kept coming back.
As time passed, I improved. I learned how to use positioning, leverage, balance, and timing.
The cramped cabin became my arena. Soon I was entering small tournaments.
My friends thought I was completely crazy.
Whenever someone asked what sport I practiced, the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The funniest and wildest experience happened during a tournament a few years later.
My opponent was built like a truck. He looked like he could bench-press a
refrigerator. Before the match started, he smiled and said, “Good luck.” I knew trouble was
coming.
The moment the referee signaled, chaos exploded.
We bounced between seats, bumped into doors, and nearly tangled ourselves in everything inside the vehicle.
The crowd was roaring. Spectators were going crazy.
Then came the moment I will never forget.
My opponent grabbed the belt hanging beside the seat and accidentally turned it into what
looked like a dangerous rope. As we struggled for position, the belt snapped across the cabin and wrapped around me in the strangest way
imaginable. For a second I thought, “What kind of sport did I join?”
He pulled, I twisted, the seat belt locked, the door opened slightly,
and both of us somehow ended up tangled together like human spaghetti.
The audience was laughing so hard that some people could barely stay in their seats.
Nobody could believe what they were seeing.
For a brief moment, I genuinely thought my opponent was going to flatten me.
Fortunately, the officials quickly intervened when things became
unsafe, and the situation was resolved without serious
injury. Afterward we both burst out laughing. Everyone loved it.
Even today people who were there still talk about “that crazy seat belt match.”
Thinking about my journey, CarJitsu remains one of the most unusual sports I
have ever experienced. It gave me great memories and incredible
experiences. Whether people are discussing athletic entertainment, very few things create reactions like CarJitsu.
If anybody asks for the weirdest sport I know, I
always tell them about the day I climbed into a car in 2018 and accidentally became a CarJitsu competitor.
Most people laugh. But after hearing about tournaments,
athletes, training sessions, sports fans, betting conversations, sportsbook discussions, and my unforgettable seat belt
battle, they usually agree on one thing:
CarJitsu might be the craziest sport ever invented.
My web site; find out more
Chinese Grown-up Videos are available for gratis
on AsianTube. And if you’re unfamiliar with Asian porn wording, JAV is
exactly what it sounds: Japanese adult videos. For all the
naked ladies and the filthy things they’re doing, it’s not adult-rated
for swearing or violence. And that’s exactly the kind of content we all enjoy watching on this
site. web site https://gitea-01.taild2831.ts.net/cliftonisaacso/japanese-porn-tube4726/wiki/No-One-is-Talking-About-The-Key-To-Why-Eastern-Adult-Porn-Clips-Find-High-Engagement.
Chinese Grown-up Videos are available for gratis on AsianTube.
And if you’re unfamiliar with Asian porn wording, JAV is exactly what it sounds: Japanese adult videos.
For all the naked ladies and the filthy things they’re doing,
it’s not adult-rated for swearing or violence. And that’s exactly the kind of content
we all enjoy watching on this site. web site https://romancefrica.com/@desireeschuste
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/plity/plita-khgs-124x400x710-gost-19903-74/
I’m Mike, a normal American guy, and back in 2018 I accidentally discovered one
of the strangest sports ever invented: CarJitsu.
If you have never heard of it, don’t worry. The entire concept
sounds like a joke. Two fighters climb inside a tiny automobile and
try to grapple each other while being trapped between the cramped interior.
Believe it or not. In most sports you have a ring, but in CarJitsu your battlefield is the inside of a
vehicle. That is what makes it so weird.
It even has official events and competitive tournaments.
Athletes travel to compete and try to prove who can dominate inside the
car. Unlike traditional combat sports, every movement is limited by doors, seats,
windows, and seat belts. That creates hilarious
moments. One second someone looks like a champion, and the next second they are stuck between the seats.
At that time I was heavily interested in unusual athletic events.
I watched many sports events every week. I also spent time reading about
sports betting. People around me talked about betting
and sportsbooks. Sometimes names like the sportsbook
1xbet would appear in conversations about major sporting events, although CarJitsu was usually too strange to be the main topic.
Late one evening I saw a crazy highlight reel online.
I honestly assumed it was fake. Competitive fighters were trying
to wrestle inside a parked car while spectators were watching
in disbelief. I laughed so hard that coffee nearly came out of my nose.
Yet the more I watched, the more fascinated I became.
A few weeks later, I found a local event and decided to attend.
The atmosphere was incredible. There were fans discussing all kinds
of sporting topics. Some people even joked about which
athlete would be the favorite if a betting site ever offered odds on the matches.
Soon I wanted more than just watching. I signed up for beginner
training. The first training day was hilarious. I hit my head on the
roof, got stuck near a seat, and accidentally opened a door at the worst possible moment.
Everyone laughed. Yet I kept coming back.
As time passed, I improved. I learned how to use positioning, leverage, balance, and timing.
The car stopped feeling tiny. Soon I was entering small tournaments.
My friends thought I was completely crazy. Whenever someone asked
what sport I practiced, the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The most unforgettable competition happened at a major event.
My opponent was massive. He looked like he could carry an engine block.
Before the match started, he smiled and said,
“Hope you’re ready.” I should have listened.
The match began, chaos exploded. We bounced between seats, bumped
into doors, and nearly tangled ourselves in everything inside the vehicle.
The crowd was roaring. People were laughing and shouting.
Then came the moment I will never forget.
My opponent grabbed the belt hanging beside the seat and accidentally turned it into what looked like a wild whip.
As we struggled for position, the belt snapped across the
cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “This is it”
He pulled, I twisted, the seat belt locked, the door opened slightly,
and both of us somehow ended up tangled together like a pile of cables.
The audience was laughing so hard that some people could
barely stay in their seats. Nobody could believe what they were seeing.
For a brief moment, I genuinely thought my opponent was going to destroy
me. Fortunately, the officials quickly intervened when things became unsafe, and the situation was resolved without serious injury.
Afterward we both burst out laughing. Everyone loved it.
Even today people who were there still talk about “the legendary belt tangle.”
Thinking about my journey, CarJitsu remains one of the strangest sports I have ever experienced.
It gave me countless funny moments. Whether people are discussing athletic entertainment, very few
things create reactions like CarJitsu.
When people want to hear a crazy sports story, I always tell them about the day
I climbed into a car in 2018 and accidentally became
a CarJitsu competitor. Nobody believes it at first.
But after hearing about tournaments, athletes,
training sessions, sports fans, betting conversations, sportsbook
discussions, and my unforgettable seat belt battle, they usually agree on one thing:
CarJitsu might be the craziest sport ever invented.
Take a look at my site URL
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/prutok-latunnyi-1/prutok-latunnyi-l63pt-15-mm-l-3000-mm-krug-1/
hi!,I love your writing very so much! proportion we keep in touch extra approximately your article
on AOL? I need a specialist on this space to unravel
my problem. May be that is you! Looking ahead to peer you.
Stop by my blog … 퍼펙트가라오케
Hey! I know this is kind of off topic but I was wondering if you
knew where I could find a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having trouble finding one?
Thanks a lot!
My page :: EPSI file opening software
hello there and thank you for your info – I have definitely picked up anything new from right
here. I did however expertise a few technical issues using this web
site, since I experienced to reload the web site a lot of times previous
to I could get it to load correctly. I had been wondering
if your web hosting is OK? Not that I’m complaining, but sluggish loading instances times will often affect your placement in google and could damage your
high-quality score if advertising and marketing with Adwords.
Well I’m adding this RSS to my e-mail and could look
out for much more of your respective interesting content.
Make sure you update this again soon.
Here is my page :: emergency information for family / in case of death folder
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-108kh92kh2-1-mm-47-5kh51-5-mm-miagkaia-paika-m3r-gost-r-52922-2008/
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-45kh-160x100x14-gost-19771-93/
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-5-5×300-mm-l90-gost-931-90/
Hi there, just became aware of your blog through Google, and found that it’s truly
informative. I am gonna watch out for brussels.
I’ll be grateful if you continue this in future. Numerous people will be
benefited from your writing. Cheers!
Feel free to surf to my page … 강남가라오케
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-60kh700-mm-acroni-4749-en-iso-18286/
Artikel yang sangat informatif dan bermanfaat. Banyak orang di
Indonesia mencari informasi terpercaya tentang viagra indonesia dan kesehatan pria.
Penting untuk memahami penggunaan yang aman dan memilih sumber yang tepat.
Terima kasih atas informasi ini. Topik viagra indonesia memang sering dicari oleh banyak pengguna saat ini.
Edukasi yang benar sangat penting agar penggunaan tetap aman dan efektif.
Konten yang bagus dan mudah dipahami. Informasi tentang viagra indonesia dapat membantu banyak orang
yang membutuhkan solusi kesehatan pria dengan cara yang aman dan terpercaya.
Postingan yang sangat membantu. Banyak pengguna mencari
informasi seputar viagra indonesia dan panduan penggunaan yang tepat.
Artikel seperti ini sangat berguna bagi pembaca.
Artikel berkualitas dan penuh informasi. Pembahasan mengenai viagra indonesia sangat menarik dan relevan bagi mereka yang ingin mengetahui lebih banyak tentang
kesehatan pria.
Check out my web site – bokep indonesia
It’s all about fake taboo stepmommy fucking story movie. There are many films of warm moms yelling foul and obtaining plowed by hung guys pretending to be their sons.
The entire fake taboo match is comparatively new at the moment.
web page https://silatdating.com/@vonnie17c90744
It’s all about fake taboo stepmommy fucking story movie. There are
many films of warm moms yelling foul and obtaining plowed by
hung guys pretending to be their sons. The entire
fake taboo match is comparatively new at the moment. web page https://healthcarenavigator.directory/author-profile/jennigonzales3/
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-80kh68kh1-8-mm-35-5kh38-5-mm-miagkaia-paika-m3rm-gost-32590-2013/
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-vt23-55x1550x1600-gost-19903-2006-gladkii-belyi-goriachekatanyi/
İşinizə davam edin və daha çox istifadəçi cəlb edin!
http://www.shadesofgreensafaris.net/?URL=pin-up-azerbaijan-betpro.net%2Fqeydiyyat
There is a lot of misunderstanding about these issues today. Your material helps explain things.
You write Formidable articles, keep up good work.
It sounds like you’re creating problems yourself by defining this as such a comprehensive, almost unknowable problem. Isn’t that self-defeating?
nicee content keep writing
Aw, this was a very nice post. In idea I wish to put in writing like this moreover taking time and precise effort to make an excellent article! I procrastinate alot and by no means seem to get something done.
At this time it appears like BlogEngine is the preferred blogging platform available
right now. (from what I’ve read) Is that what you’re using on your
blog?
My webpage Siete Casino
Cabinet IQ
8305 Ꮪtate Hwy 71#110, Austin,
TX 78735, United Ꮪtates
254-275-5536
personalized
Very good article. I will be going through some of these issues as
well..
Feel free to surf to my website – WordPress kotisivut
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-5-5×600-mm-l63-gost-931-90/
Hi to all, how is everything, I think every one is getting
more from this web page, and your views are pleasant in favor of new users.
my website Siete Casino
Official JayPlaysGames,
JayPlaysGames is a hub for console players looking for fun.
With broadcasts filled with informative chats, it brings unique content every week.
Join the adventure!
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-20kh1400-mm-x2crnin23-4-en-iso-18286/
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-7kh3-195-gost-1133-71/
Thanks very interesting blog!
Also visit my web blog … paper io
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-45g17iu3-7x1000x3000-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
I’d like to find out more? I’d like to find out more details.
my web blog; fujiwin88
Peguei uma sequência linda no Touro hoje de manhã. Bão demais.
Поставка продукции возможна не только в промышленных, но и в малых лабораторных объемах для исследовательских целей.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-khn65mvu-230×9-gost-9941-81/
Bônus espetacular no Ninja vs Samurai! Quase R$ 100 de lucro limpo.
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-50kh50kh5-mm-x12cr13-en-10088-3/
We have been helping Canadians Get a Loan Against Their Vehicle for Repairs Since March 2009
and are among the very few Completely Online Lenders In Canada.
With us you can obtain a Car Repair loan for repairs Online from anywhere in Canada as long as you have a Fully Paid
Off Vehicle that is 8 Years old or newer. We
look forward to meeting all your financial needs.
Hey there I am so grateful I found your weblog, I really found you by error, while
I was searching on Aol for something else, Regardless I
am here now and would just like to say thanks a lot for a incredible post and a all round
entertaining blog (I also love the theme/design), I don’t have time to read through it all at the minute but I have bookmarked it and also included your RSS feeds, so when I have time I will be back to read a great deal more,
Please do keep up the excellent b.
Feel free to surf to my site – gudang bokep indonesia
Great weblog right here! Also your website so much up fast!
What web host are you the usage of? Can I am getting your affiliate link to your
host? I wish my web site loaded up as fast as yours lol
Visit my website … web page
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/plity/plita-u13-18x400x250-gost-19903-74/
I really like what you guys tend to be up too. This sort of clever work and coverage!
Keep up the excellent works guys I’ve incorporated you guys to my personal
blogroll.
my web site … click
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-80kh80kh10-mm-c50e-en-10056-2/
Cabhinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Envirofriendly (holtontscc.raindrop.page)
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/list/list-5khv2sf-2x1200x2500-gost-19903-74/
This is really interesting, You’re a very skilled blogger.
I have joined your feed and look forward to seeking more of your wonderful post.
Also, I have shared your website in my social networks!
Feel free to surf to my web-site … หมูกระทะกรุงเทะ
Наличие на складе редких металлов, таких как цирконий, выделяет компанию на фоне конкурентов, торгующих только массовым прокатом.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r9-360-gost-2590-2006/
Важным преимуществом является возможность изготовления деталей и изделий по индивидуальным чертежам заказчика.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-stal-45-100x1600x2000-gost-r-52146-2003-polimernyi-otsinkovannyi-kholodnokatanyi/
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-50kh50kh6-mm-50crv4-din-59370/
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-20ps-9x1700x1300-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
Экспертная консультация при выборе сплавов помогает клиентам оптимизировать затраты и избежать технологических ошибок.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-stal-20-273×17-gost-21729-76/
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-60kh40kh6-mm-c22e-din-59370/
Nice post. I was checking constantly this blog and I’m impressed!
Extremely useful info particularly the last part :) I care for such info much.
I was seeking this certain information for a long time.
Thank you and best of luck.
Look into my web blog – electric bikes
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/plity/plita-5khnv-5x80x450-gost-19903-74/
Pretty nice post. I just stumbled upon your weblog and wished to say that I’ve really loved surfing around your blog
posts. After all I’ll be subscribing for your rss feed and I am
hoping you write once more very soon!
Stop by my site omacuan
At this time I am ready to do my breakfast, later than having
my breakfast coming again to read additional news.
Visit my blog post electric bike for adults
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-100kh65kh10-mm-st52-3n-uni-6762/
Hey terrific website! Does running a blog like this require a lot of work?
I’ve virtually no knowledge of coding but I was hoping
to start my own blog in the near future. Anyways,
should you have any suggestions or techniques for new blog owners please
share. I understand this is off subject nevertheless I just needed to
ask. Thank you!
Feel free to visit my web-site 강남풀싸롱
Spot on with this write-up, I really think this amazing site needs a
lot more attention. I’ll probably be back
again to see more, thanks electric bike for adults the info!
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/list/list-9khfm-2x1200x2500-gost-19903-74/
UpvoteRocket is the #1 automated voting service for private MMORPG servers.
Climb toplist rankings on XtremeTop100, TopG, GTop100
with smart undetectable automation. Ragnarok, WoW, Mu Online & 20+ platforms supported.
Pay only for delivered votes.
my blog – perfect world vote bot
Hi, after reading this amazing piece of writing i am too
glad to share my experience here with colleagues.
My blog post; Reducing bias in automated hiring
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-ei723-33-25-gost-7417-75/
Hmm it seems like your website ate my first comment (it was super long) so I guess I’ll just
sum it up what I wrote and say, I’m thoroughly enjoying your
blog. I as well am an aspiring blog writer
but I’m still new to the whole thing. Do you have any suggestions for inexperienced blog writers?
I’d genuinely appreciate it.
My web site; Spin Fortune Tiger no Brasil
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Craftsmanship
If you are going for finest contents like me, only go to see this
website all the time as it gives feature contents, thanks
Here is my webpage; Reducing bias in automated hiring
Важным преимуществом является возможность изготовления деталей и изделий по индивидуальным чертежам заказчика.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-amts-50x1200x1000-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
I do not know if it’s just me or if everyone else experiencing
problems with your website. It appears like some of the text in your content are running off the
screen. Can somebody else please comment and let me know if this is happening to them
as well? This could be a issue with my web browser because
I’ve had this happen previously. Appreciate it
Here is my web page … control cable – Bradly,
Enjoy easy account access with FFFPH Login, ideal for regular players.
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-st3ps-50x50x3-gost-8509-93/
Wow that was unusual. I just wrote an extremely long comment but
after I clicked submit my comment didn’t appear. Grrrr…
well I’m not writing all that over again. Anyways, just wanted to say great blog!
Visit my web-site … anchor: xxx videos
Hörmətlə, bu saytınız çox yaxşı işləyir!
http://euros-collections.xooit.eu/redirect1/https://pin-up-azerbaijan-jackpot.org/odenisler
I just could not go away your website before suggesting that I extremely enjoyed the
standard info an individual supply to your guests?
Is going to be again regularly to check out new posts
Also visit my site; 풀싸롱
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-20khgsa-12x1800x1550-gost-19903-2006-gladkii-belyi-goriachekatanyi/
It is in reality a nice and useful piece
of info. I am happy that you simply shared this helpful information with us.
Please keep us informed like this. Thank you ebike for sale sharing.
Hi! This is my first comment here so I just wanted to give a quick shout out and tell you
I really enjoy reading your posts. Can you recommend any other blogs/websites/forums that go
over the same topics? Thanks!
Here is my homepage :: electric bike for adults
Компания занимается реализацией ферросплавов, необходимых для качественного легирования сталей на литейных участках.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-stal-50-83×18-gost-21729-76/
Great post! Perfume samples are a smart way to find your
next favorite fragrance without buying a full bottle.
Very informative.
I think that perfume samples make it much easier to compare different scents.
Really useful information.
Great share! Using cologne samples is one of
the best ways to experience premium perfumes. Keep up the good work.
Great information! Fragrance samples are perfect for travel, and
they allow you to experiment with different scents. Looking forward to
more posts.
This is valuable stuff.In my opinion, if all website owners and bloggers developed their content they way you have, the internet will be a lot more useful than ever before.
This website has lots of really useful stuff on it. Thanks for informing me.
Excellent post. I was checking constantly this blog and I’m impressed!
Very useful information specifically the last part :) I care
for such info much. I was looking for this certain info for a very long time.
Thank you and good luck.
my web-site: serwis kamperów Siemianowice. naprawa kamperów Siemianowice
Оперативная логистика и поддержка на всех этапах сделки позволяют минимизировать сроки простоя производственных линий заказчиков.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-150kh75kh9-mm-15nicr13-uni-6762/
Can I just say what a relief to seek out someone who actually knows what theyre speaking about on the internet. You positively know find out how to bring a problem to mild and make it important. Extra individuals have to read this and perceive this side of the story. I cant believe youre not more in style because you positively have the gift.
Just a quick note to express my appreciation. Take care
ООО «РМС» предлагает широкий спектр цветного проката, включая медь, латунь, бронзу и дюралюминий.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-5khnvs-73-gost-7417-75/
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-60kh40kh5-mm-25crmo4-din-1029/
You have made some really good points there.
I looked on the net to learn more about the issue and found
most individuals will go along with your views on this website.
Visit my page; comment1295881
How long does it take you to write an article like this?
Pretty! This was an extremely wonderful post. Thanks for providing this info.
Here is my site :: artis indonesia
Важным преимуществом является возможность изготовления деталей и изделий по индивидуальным чертежам заказчика.
https://rms-ekb.ru/catalog/list/list-kh12vm-2x500x500-gost-19903-74/
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-4kh5v2mf-9-8-gost-7417-75/
Hey! Someone in my Facebook group shared this site with us so I came to take a look.
I’m definitely loving the information. I’m bookmarking and will be tweeting this to my followers!
Great blog and fantastic style and design.
Feel free to surf to my blog post – debet
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-pt-3v-70x1700x1900-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Mersin temizlik hizmeti almak isteyenler için böyle rehber siteleri gerçekten işe yarıyor.
Jet Rehber bu alanda güzel bir alternatif olabilir.
my web blog mersin temizlik şirketi
That’s because it’s the only peptide scientifically verified to reverse
the skin’s organic age.
Visit my blog post; web page; Angelika,
Very good post! We are linking to this particularly great
post on our site. Keep up the good writing.
Here is my blog; vin88
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/izoliruiushchie-flantsevye-soedineniia/
There is definately a lot to know about this subject.
I love all the points you made.
my web page – หีสด.com
I love your blog.. very nice colors & theme. Did you
design this website yourself or did you hire someone to do it for you?
Plz respond as I’m looking to design my own blog and
would like to find out where u got this from. cheers
Feel free to visit my web blog Agensi Pekerjaan Havannah
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-35khg2-25x1500x1250-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Pretty part of content. I just stumbled upon your web site and in accession capital to
say that I acquire actually loved account your blog posts.
Anyway I’ll be subscribing for your augment and even I achievement you access
consistently fast.
Review my website … comment-307921
It’s going to be end of mine day, however before ending I am reading this enormous article to increase my know-how.
Also visit my website … live draw hk hari ini
Поставка продукции возможна не только в промышленных, но и в малых лабораторных объемах для исследовательских целей.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-09g2s-22×2-5-gost-21729-76/
Wow, superb weblog format! How long have you been blogging for?
you made running a blog look easy. The total look of your web site is excellent,
as well as the content!
My web site; Vu88
Hi, I do think this is a great site. I stumbledupon it ;) I will return once again since i have book marked it.
Money and freedom is the greatest way to change, may you be rich and continue to help other people.
my web page: va88
My name is Mike, a regular guy from the USA, and during 2018 I accidentally discovered one of the strangest sports ever invented: Car
Jitsu.
If this is your first time hearing about it, you are not alone.
The entire concept sounds like something invented after a crazy bet.
Two competitors climb inside a compact vehicle and try to score positions against each other while being trapped between the seats.
Yes, really. In most sports you have a ring, but in CarJitsu your battlefield is the inside of a vehicle.
That is why people laugh when they first hear about it.
It even has official events and competitive tournaments.
Competitors come from different places and try to prove
who can dominate inside the car. Compared to ordinary sports,
every movement is limited by doors, seats, windows, and seat belts.
The result is pure chaos. One second someone looks like a champion, and the next
second they are trapped near the steering wheel.
During those days I was heavily interested in unusual athletic events.
I watched many sports events every week. I also spent time reading about sports betting.
People around me talked about betting and sportsbooks.
Sometimes names like 1xbet would appear in conversations about major sporting events, although CarJitsu was usually
too strange to be the main topic.
One night I saw a short video online. Initially I believed it was a joke.
Full-grown athletes were trying to wrestle inside a parked car while spectators were laughing, cheering, and recording videos.
I laughed so hard that coffee nearly came out of my nose.
Yet the more I watched, the more fascinated I became.
Not long afterward, I found a local event and decided to attend.
The crowd energy was amazing. There were fans discussing all kinds
of sporting topics. Some people even joked about which athlete would be the favorite if a
betting site ever offered odds on the matches.
Soon I wanted more than just watching. I signed up for beginner training.
My debut practice was chaos. I hit my head on the roof, got stuck near a seat, and accidentally opened a door at the worst possible moment.
The coaches laughed. Yet I kept coming back.
Month after month, I improved. I learned how to use technique and movement.
The vehicle became familiar. Soon I was entering regional events.
My friends thought I was completely crazy. Whenever
someone asked what sport I practiced, the conversation usually went like
this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The craziest match of my career came later.
My opponent was built like a truck. He looked like he could lift a small house.
Before the match started, he smiled and said, “You’re going to need luck.” That should have been a warning.
As soon as the fight started, chaos exploded. We bounced between seats, bumped
into doors, and nearly tangled ourselves in everything inside the vehicle.
The crowd was roaring. People were laughing and shouting.
Then came the moment I will never forget.
My opponent grabbed the belt hanging beside the seat and
accidentally turned it into what looked like a
dangerous rope. As we struggled for position, the belt snapped across
the cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “I can’t believe this is happening”
He pulled, I twisted, the seat belt locked, the door opened slightly, and both of us somehow ended up tangled together like two confused octopuses.
The audience was laughing so hard that some people could barely stay in their seats.
The scene was unbelievable.
For a brief moment, I genuinely thought my opponent was going to crush me.
Luckily, the officials quickly intervened when things became unsafe, and the
situation was resolved without serious injury. Afterward we both burst out laughing.
Spectators cheered. Even today people who were there still talk about “the legendary belt tangle.”
Looking back, CarJitsu remains one of the strangest sports I
have ever experienced. It gave me countless funny moments.
Whether people are discussing athletic entertainment, very few things create reactions like CarJitsu.
Whenever someone asks me about unusual sports,
I always tell them about the day I climbed into a car in 2018 and
accidentally became a CarJitsu competitor. The reaction is always the
same. But after hearing about tournaments, athletes, training sessions, sports fans,
betting conversations, sportsbook discussions, and my unforgettable seat belt battle,
they usually agree on one thing:
CarJitsu is wonderfully ridiculous.
Visit my page – read more
Наличие на складе редких металлов, таких как цирконий, выделяет компанию на фоне конкурентов, торгующих только массовым прокатом.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-40kh40kh4-mm-40nicr6-en-10056-1/
موقع ايجي بست الاصلي مشاهدة افلام ومسلسلات مترجمة اون لاين احدث لافلام الاجنبيه افلام اكشن
افلام اون لاين وتحميل مباشر ايجي بست egybest.| EGbest.net
Feel free to visit my website ايجى بيست
Наличие прецизионных сплавов в ассортименте подтверждает работу компании с высокоточными и наукоемкими материалами.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-di55-63-gost-7417-75/
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-200kh100kh10-mm-20mocr3-din-59370/
научная работа автореферат по психологиид
ключ
Важным преимуществом является возможность изготовления деталей и изделий по индивидуальным чертежам заказчика.
https://rms-ekb.ru/catalog/list/list-6kh4m2fs-2x1200x3000-gost-19903-74/
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r9-92-gost-2590-2006/
People call me Mike, a normal American guy, and back in 2018 I accidentally discovered one
of the weirdest sports on Earth: CarJitsu.
If this is your first time hearing about it, don’t worry. The entire concept sounds
like a comedy sketch. Two athletes climb inside a tiny automobile and try
to score positions against each other while being trapped between the
seats. No, I’m not kidding. In most sports you have
a court, but in CarJitsu your battlefield is a car cabin. That is why
people laugh when they first hear about it.
The sport has tournaments, championships, local events, and
exhibition matches. Participants gather from various regions and try to prove who can dominate inside the car.
Different from most athletic competitions, every movement is limited by doors, seats, windows, and seat belts.
The result is pure chaos. One second someone looks like a
champion, and the next second they are folded like a pretzel.
During those days I was heavily interested in sports.
I watched all kinds of competitions. I also spent time reading about betting markets.
Many sports fans I knew compared sportsbook offers. Sometimes names like 1xBet would
appear in conversations about major sporting events, although CarJitsu was usually too
strange to be the main topic.
One night I saw a crazy highlight reel online. At first I thought it was satire.
Grown adults were trying to grapple inside a parked car
while spectators were watching in disbelief. I laughed so hard that I couldn’t breathe for a moment.
Yet the more I watched, the more fascinated I became.
Not long afterward, I found a local event and decided to watch in person. The event was unforgettable.
There were fans discussing athletic techniques and sports culture.
Some people even joked about which athlete would be the favorite if a sports betting market ever offered odds on the
matches.
Soon I wanted more than just watching. I signed up for beginner training.
My debut practice was chaos. I hit my head on the roof, got stuck near a seat,
and accidentally opened a door at the worst possible moment.
Even I laughed at myself. Yet I kept coming back.
As time passed, I improved. I learned how to use technique and movement.
The car stopped feeling tiny. Soon I was entering regional events.
My friends thought I was completely crazy.
Whenever someone asked what sport I practiced, the conversation usually
went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The funniest and wildest experience happened during a tournament a few years later.
My opponent was built like a truck. He looked like he could bench-press
a refrigerator. Before the match started, he smiled and said, “You’re going to need luck.” I knew trouble
was coming.
The match began, chaos exploded. We bounced between seats, bumped into doors,
and nearly tangled ourselves in everything
inside the vehicle. The crowd was roaring. Spectators were going crazy.
Then came the moment I will never forget.
My opponent grabbed the seat belt and accidentally turned it into what looked like a dangerous rope.
As we struggled for position, the belt snapped across the cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “I can’t believe this is happening”
He pulled, I twisted, the seat belt locked, the
door opened slightly, and both of us somehow ended up tangled together like two confused
octopuses. The audience was laughing so hard that some people could barely stay in their seats.
The scene was unbelievable.
For a brief moment, I genuinely thought my
opponent was going to destroy me. Fortunately, the officials
quickly intervened when things became unsafe, and the situation was resolved
without serious injury. Afterward we both burst out laughing.
Spectators cheered. Even today people who were there
still talk about “that crazy seat belt match.”
Thinking about my journey, CarJitsu remains one of the
weirdest athletic competitions I have ever experienced.
It gave me friendships, stories, and unforgettable memories.
Whether people are discussing sports culture and competition,
very few things create reactions like CarJitsu.
If anybody asks for the weirdest sport I know, I always tell them about the
day I climbed into a car in 2018 and accidentally
became a CarJitsu competitor. The reaction is always the same.
But after hearing about tournaments, athletes, training sessions, sports
fans, betting conversations, sportsbook discussions, and my unforgettable seat belt battle, they usually agree on one
thing:
CarJitsu is wonderfully ridiculous.
my site; find out more
Great article.
Here is my website … bokep indo
Thanks , I’ve just been searching for information about
this topic for ages and yours is the best I have discovered till
now. But, what in regards to the conclusion?
Are you sure concerning the supply?
Look at my site growth hackers digital company
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-kh20n80-120x1400x1200-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Artistic
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/promezhutochnaia-metallicheskaia-opora-lep-750-kv/
Cabinet IQ
8305 Stɑte Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Turnkey
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-80kh1100-mm-x6crninb18-10-en-iso-18286/
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-20kh13n4g9-10x1700x1100-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-65kh65kh11-mm-34cr4-din-1028/
hello there and thank you for your info – I’ve definitely picked up something new from right
here. I did however expertise some technical issues using this
website, as I experienced to reload the website many times previous to
I could get it to load properly. I had been wondering if your web host is
OK? Not that I’m complaining, but slow loading instances
times will very frequently affect your placement in google and could damage your high-quality
score if ads and marketing with Adwords. Anyway I am adding this RSS to my email and
can look out for much more of your respective fascinating content.
Make sure you update this again very soon.
Take a look at my blog; video bokep artis indonesia
География деятельности компании охватывает всю территорию России, обеспечивая металлом предприятия в удаленных регионах.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-7khg2vmf-17-gost-7417-75/
ООО «РМС» обеспечивает поставки специализированных сварочных материалов для сложных условий эксплуатации.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-125kh75kh8-mm-20mocr2-2-en-10056-2/
If some one wants expert view about blogging afterward i recommend him/her to visit this web site, Keep
up the pleasant job.
Check out my webpage; comment-443260
Normally I do not learn post on blogs, but I wish to say
that this write-up very forced me to take a look at and do so!
Your writing style has been amazed me. Thank you, very great post.
Feel free to visit my blog: vanity address generator
В каталоге представлены конденсаторные ниобиевые порошки высокой чистоты, необходимые для современной электроники.
https://rms-ekb.ru/catalog/list/list-4khmfs-11x1000x1000-gost-19903-2006/
I been interested in Japanese swords. These blades’ design is truly remarkable.
Really enjoyed reading this!
Wonderful write-up! Japanese blades represent centuries of tradition and
craftsmanship. I learned a lot.
Here is my web page – https://katana-sword.com/
Triggering hulu com activate [mendez-ross-2.thoughtlanes.net] on your smart television is a straightforward process.
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-7kh2smf-38-gost-7417-75/
Great blog here! Also your website loads up fast!
What host are you using? Can I get your affiliate link to your host?
I wish my site loaded up as quickly as yours lol
Here is my web blog … Debet
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-4kh2100kh2400-mm-1-4003-en-iso-9445-1/
O site Vidah Plena é um portal de conteúdo sobre saúde mental, ansiedade, bem-estar emocional,
desenvolvimento pessoal, autoestima, qualidade de vida, espiritualidade cristã, inteligência emocional e
fortalecimento psicológico.
Review my webpage … esgotamento emocional
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-150kh150kh15-mm-s235jrc-en-10277/
I think the admin of this site is genuinely working hard for
his web site, because here every information is quality
based information.
My homepage Uncensored AI
дипломные работы на заказ
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-2kh1500kh2700-mm-a240-astm-a480/
I read this article fully on the topic of the comparison of hottest and earlier technologies, it’s remarkable article.
My blog webpage
Cabinet IQ
8305 Stаte Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Remodelworkshop
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/list/list-u8a-18x1500x3000-gost-19903-74/
I’m Mike, a typical guy from the United States, and in the year 2018 I accidentally discovered one of the weirdest sports on Earth: car
jitsu.
If you have never heard of it, don’t worry. The entire concept sounds like a comedy sketch.
Two competitors climb inside a small car and try to grapple
each other while being trapped between the cramped interior.
No, I’m not kidding. In most sports you have a ring, but
in CarJitsu your battlefield is a car cabin. That is why people laugh when they first
hear about it.
It even has official events and competitive tournaments.
Competitors come from different places and try to prove who can master the unusual
format. Different from most athletic competitions, every
movement is limited by the vehicle’s interior. This leads to
funny situations. One second someone looks like a champion, and the next second they are folded like a pretzel.
Back then I was heavily interested in sports. I watched football,
basketball, MMA, and wrestling. I also spent time reading about betting markets.
Many sports fans I knew compared sportsbook offers. Sometimes names like 1xbet would appear in conversations about
major sporting events, although CarJitsu was usually too strange to
be the main topic.
Late one evening I saw a crazy highlight reel online.
Initially I believed it was a joke. Full-grown athletes
were trying to wrestle inside a parked car while spectators were laughing, cheering, and recording videos.
I laughed so hard that I almost fell off my chair.
Yet the more I watched, the more fascinated I became.
Not long afterward, I found a local event and decided to show
up. The crowd energy was amazing. There were fans discussing athletic techniques and sports culture.
Some people even joked about which athlete would be the favorite if a betting site ever offered odds
on the matches.
Eventually I wanted to participate. I signed up for beginner
training. My first session was a disaster. I hit my head on the roof, got stuck near a seat, and
accidentally opened a door at the worst possible moment.
Even I laughed at myself. Yet I kept coming back.
Week after week, I improved. I learned how to use technique and movement.
The car stopped feeling tiny. Soon I was entering local competitions.
My friends thought I was completely crazy. Whenever someone asked
what sport I practiced, the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The craziest match of my career came later. My opponent was massive.
He looked like he could bench-press a refrigerator.
Before the match started, he smiled and said, “Good luck.” I should have listened.
As soon as the fight started, chaos exploded. We bounced between seats, bumped into
doors, and nearly tangled ourselves in everything inside the vehicle.
The crowd was roaring. Spectators were going crazy.
Then came the moment I will never forget.
My opponent grabbed the belt hanging beside the seat and accidentally turned
it into what looked like a dangerous rope. As we struggled for position, the belt snapped across the cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “This is it”
He pulled, I twisted, the seat belt locked, the door opened slightly, and both of us somehow
ended up tangled together like a pile of cables. The audience was
laughing so hard that some people could barely stay in their seats.
The scene was unbelievable.
For a brief moment, I genuinely thought my opponent was going to flatten me.
Fortunately, the officials quickly intervened when things became unsafe, and the situation was resolved
without serious injury. Afterward we both burst out laughing.
The crowd applauded. Even today people who were there still talk about “that crazy seat belt match.”
Looking back, CarJitsu remains one of the strangest sports I have ever experienced.
It gave me countless funny moments. Whether people are
discussing athletic entertainment, very few things create
reactions like CarJitsu.
If anybody asks for the weirdest sport I know, I always tell them about the
day I climbed into a car in 2018 and accidentally became a CarJitsu competitor.
The reaction is always the same. But after hearing about tournaments, athletes,
training sessions, sports fans, betting conversations, sportsbook discussions,
and my unforgettable seat belt battle, they usually agree on one thing:
CarJitsu might be the craziest sport ever invented.
My web site article
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-60kh60kh8-mm-31crmov9v-uni-6762/
Поставка продукции возможна не только в промышленных, но и в малых лабораторных объемах для исследовательских целей.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-kh12f1-100-gost-7417-75/
Do you have any video of that? I’d like to find out more details.
Here is my web page: one88
Оперативная логистика и поддержка на всех этапах сделки позволяют минимизировать сроки простоя производственных линий заказчиков.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-65kh65kh9-mm-50crv4-din-1028/
I was wondering if you ever considered changing the layout of your blog?
Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content so people could connect with it better.
Youve got an awful lot of text for only having 1 or 2 images.
Maybe you could space it out better?
My website – comment-1352015
My name is Mike, a typical guy from the United States,
and during 2018 I accidentally discovered one of the most bizarre sports I had ever seen: Car Jitsu.
In case this sounds unfamiliar, you are not alone. The entire concept sounds like something invented after a
crazy bet. Two competitors climb inside a compact vehicle and try to control each other while being
trapped between the cramped interior. Believe it or not.
In most sports you have a field, but in CarJitsu your battlefield is the inside of a vehicle.
That is what makes it so weird.
It even has official events and competitive tournaments. Participants
gather from various regions and try to prove who
can adapt best to the strange environment.
Different from most athletic competitions, every movement is limited by the vehicle’s interior.
This leads to funny situations. One second someone looks
like a champion, and the next second they are stuck between the seats.
During those days I was heavily interested in sports.
I watched football, basketball, MMA, and wrestling. I also spent time reading about sportsbook odds.
Friends often discussed sportsbooks. Sometimes names like 1xBet would appear in conversations about major sporting events, although CarJitsu was usually too strange to be the
main topic.
Late one evening I saw a short video online. I honestly assumed it was fake.
Competitive fighters were trying to battle
inside a parked car while spectators were watching in disbelief.
I laughed so hard that I almost fell off my chair. Yet the more I
watched, the more fascinated I became.
Soon after that, I found a local event and decided to show up.
The atmosphere was incredible. There were fans discussing athletic techniques and sports culture.
Some people even joked about which athlete would be the favorite if a sports betting market ever
offered odds on the matches.
Eventually I wanted to participate. I signed up
for beginner training. The first training day was hilarious.
I hit my head on the roof, got stuck near a seat, and accidentally opened a door at the
worst possible moment. Even I laughed at myself.
Yet I kept coming back.
Week after week, I improved. I learned how to use positioning,
leverage, balance, and timing. The vehicle
became familiar. Soon I was entering small tournaments.
My friends thought I was completely crazy. Whenever someone asked what sport I practiced,
the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The craziest match of my career came later. My opponent was built like a truck.
He looked like he could carry an engine block.
Before the match started, he smiled and said,
“Hope you’re ready.” That should have been a warning.
The moment the referee signaled, chaos exploded.
We bounced between seats, bumped into doors, and nearly tangled ourselves in everything inside
the vehicle. The crowd was roaring. Spectators were going crazy.
Then came the moment I will never forget.
My opponent grabbed the car seat belt and accidentally
turned it into what looked like a crazy lasso. As we struggled for position, the belt snapped
across the cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “This is it”
He pulled, I twisted, the seat belt locked, the door opened slightly,
and both of us somehow ended up tangled together like two confused octopuses.
The audience was laughing so hard that some people could barely stay in their seats.
It looked completely ridiculous.
For a brief moment, I genuinely thought my opponent was going to crush me.
Luckily, the officials quickly intervened when things became unsafe, and the situation was
resolved without serious injury. Afterward we both burst out laughing.
Spectators cheered. Even today people who were there still talk about “the legendary belt tangle.”
Looking back, CarJitsu remains one of the weirdest athletic competitions I have ever
experienced. It gave me countless funny moments.
Whether people are discussing athletic entertainment, very few
things create reactions like CarJitsu.
Whenever someone asks me about unusual sports, I always tell them about the day I climbed into
a car in 2018 and accidentally became a CarJitsu competitor.
Most people laugh. But after hearing about tournaments, athletes, training sessions, sports
fans, betting conversations, sportsbook discussions, and my unforgettable seat belt battle, they
usually agree on one thing:
CarJitsu is absolutely insane.
Also visit my blog … press release
I visited various web pages but the audio quality for audio songs
present at this web site is genuinely marvelous.
my page: Pet transport Europe
Оперативная логистика и поддержка на всех этапах сделки позволяют минимизировать сроки простоя производственных линий заказчиков.
https://rms-ekb.ru/catalog/list/list-90khf-2x2000x6000-gost-19903-74/
Dizaynı çox bəyənirəm!
https://pin-up-azerbaijan-betpro.org/odenisler
Nice to meet you! We are a online retailer since 1988.
Welcome to Elivera 1988-2026. EliveraGroup sells online natural cosmetics, beauty products, food supplements.
We connect people with products and services in new and unexpected ways.
The company ELIVERAGroup, is a Retailer, which operates in the Cosmetics industry.
ELIVERA was established in 1988. ELIVERA LTD was established in 2007.
The first project was in 1988. It was carried out in trade with Russia, Belarus, Ukraine, Belgium, Hungary, Poland, Lithuania, Latvia and Estonia.
my page – haemorrhoid
Наличие на складе редких металлов, таких как цирконий, выделяет компанию на фоне конкурентов, торгующих только массовым прокатом.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-15khsnd-160x160x12-gost-8509-93/
Nearly all video style, including black variants, can be
discovered on Ebony Tube. In the Ebony Mother thumbnail, there is
a dark cougar getting nailed, and a young beauty having it from behind in the aisle photo for Ebony Teen. Just the tip of the iceberg of the
page’s list of niches include Ebony Squirting, Ebony Threesomes, Ebony Public, and Ebony Creampies.
web site https://114.242.31.6:3000/xzlalda2835315/alda1989/wiki/Everyone-Loves-What-Attracts-Users-To-Ebony-Adult-Tube-Sites
Nearly all video style, including black variants, can be discovered on Ebony Tube.
In the Ebony Mother thumbnail, there is a dark cougar getting nailed, and a
young beauty having it from behind in the aisle photo for Ebony Teen. Just the tip of the iceberg of the page’s
list of niches include Ebony Squirting, Ebony Threesomes, Ebony Public, and Ebony Creampies.
web site https://www.adpost4u.com/user/profile/4499248
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-30kh1600-mm-acroni-4550a-en-iso-18286/
Cabinet IQ
8305 Ꮪtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Fabrication
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-aisi-409-70x70x7-gost-8509-93/
For latest news you have to pay a quick visit world wide web and on internet
I found this website as a finest site for newest updates.
My homepage; comment-402640
I am curious to find out what blog system you are working
with? I’m having some minor security issues with my latest blog and I’d like to find something more secure.
Do you have any recommendations?
Feel free to visit my web-site Sky88
People has their own preferences for video, but HDBlackAss has a extensive selection to choose from if you’re
looking for ebony prostitutes. If gorgeous black girls make
you feel the hard on, I advise you check out HDBlackAss
for free. site https://git.erfmann.dev/margartgustafs
People has their own preferences for video, but HDBlackAss has
a extensive selection to choose from if you’re looking for
ebony prostitutes. If gorgeous black girls make you feel the hard on, I advise you check out HDBlackAss for free.
site https://qatar-directory.com/author/seth68a9406297/
ООО «РМС» обеспечивает поставки специализированных сварочных материалов для сложных условий эксплуатации.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-khn45iu-140x2000x1200-gost-24982-81-zharoprochnyi-belyi-kholodnokatanyi/
Very descriptive blog, I enjoyed that bit. Will there be a part 2?
Feel free to surf to my blog :: Horse Gelatin
Cabinet IQ
8305 Ⴝtate Hwy 71 #110, Austin,
TX 78735, United Stateѕ
254-275-5536
Topcontractors
I will right away take hold of your rss feed as I
can’t in finding your email subscription link or newsletter service.
Do you have any? Kindly allow me realize so that I may subscribe.
Thanks.
Also visit my webpage – Richmond Botox Clinic
Nice post. I used to be checking continuously this weblog and I’m
inspired! Very useful info specifically the closing part :) I handle such information much.
I was seeking this particular info for a long time. Thank you and best of luck.
Feel free to surf to my site – West Coast Bud Online Dispensary
We’re a group of volunteers and opening a new scheme in our community.
Your website offered us with valuable information to work on. You have done an impressive job and our whole
community will be thankful to you.
Also visit my homepage ERM file description
It’s difficult to find knowledgeable people for this subject, but you sound
like you know what you’re talking about! Thanks
My homepage: Anti-Aging Treatments
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-khn58v-150x1800x1900-gost-24982-81-zharoprochnyi-goriachekatanyi/
Hmm it appears like your blog ate my first comment (it was
super long) so I guess I’ll just sum it up what I submitted
and say, I’m thoroughly enjoying your blog.
I too am an aspiring blog writer but I’m still new to the whole thing.
Do you have any points for beginner blog writers?
I’d definitely appreciate it.
my web site; mellstroy com
Whoa! This blog looks exactly like my old one! It’s on a entirely
different subject but it has pretty much the same layout and design.
Great choice of colors!
Here is my website – Cosmetic Injections
Fascinating blog! Is your theme custom made or did you
download it from somewhere? A design like yours with a few simple adjustements would really make my blog
shine. Please let me know where you got your theme.
Appreciate it
Here is my website; SkinMedica
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r10f5k5-88-gost-7417-75/
Nice weblog right here! Also your site quite a bit up very fast!
What host are you using? Can I get your associate link for your host?
I want my website loaded up as fast as yours lol
my site stem cell clinic
ООО «РМС» специализируется на поставках редких и тугоплавких металлов, таких как ниобий и вольфрам.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-100kh50kh8-mm-s16e-din-1029/
I’m really enjoying the theme/design of your blog.
Do you ever run into any internet browser compatibility issues?
A number of my blog audience have complained about my website not operating correctly in Explorer but looks great in Safari.
Do you have any recommendations to help fix this issue?
Feel free to visit my page: خرید تشک و بالش و محافظ تشک
My brother recommended I might like this website. He was totally right.
This post truly made my day. You can not imagine just
how much time I had spent for this info! Thanks!
Here is my website ck444
Excellent goods from you, man. I’ve take into account your stuff previous to and
you’re just too great. I actually like what you’ve acquired here, really like what you’re saying and
the best way in which you assert it. You’re making it enjoyable and you still take care of to
keep it smart. I can’t wait to read much more from
you. This is actually a great web site.
Here is my webpage :: harga emas 916 hari ini
Wonderful blog! Do you have any recommendations
for aspiring writers? I’m hoping to start my own website
soon but I’m a little lost on everything.
Would you suggest starting with a free platform like WordPress or go for a paid option?
There are so many options out there that I’m completely confused ..
Any ideas? Thanks a lot!
Also visit my web blog … navigate to this website
Bu platformanı çox sevirəm.
https://images.google.ee/url?q=https%3a%2f%2fpin-up-azerbaijan-baku.net%2Fbonuslar
Great delivery. Outstanding arguments. Keep up the good work.
Here is my site: West Coast Bud Canada
I got this web page from my buddy who shared with me concerning this website and
at the moment this time I am browsing this site and
reading very informative content at this place.
Here is my homepage; Lu88
I really believe you will do well in the future I appreciate everything you have added to my knowledge base.
Have you ever thought about writing an e-book or guest authoring on other blogs?
I have a blog based on the same information you discuss
and would love to have you share some stories/information. I know
my readers would enjoy your work. If you’re even remotely interested, feel free to shoot me an e mail.
Review my web page; Fabet
I’m Mike, a regular guy from the USA, and back in 2018
I accidentally discovered one of the most bizarre sports I
had ever seen: CarJitsu.
If this is your first time hearing about it, don’t worry.
The entire concept sounds like a joke. Two fighters climb inside a small car and
try to grapple each other while being trapped between the
cramped interior. Yes, really. In most sports you have a field, but in CarJitsu your battlefield is a car cabin. That is
why people laugh when they first hear about it.
There are organized competitions, tournaments, championships,
and special events. Athletes travel to compete and try
to prove who can adapt best to the strange environment.
Different from most athletic competitions, every movement is limited by
doors, seats, windows, and seat belts. The result is pure chaos.
One second someone looks like a champion, and the next second they are folded like a pretzel.
At that time I was heavily interested in sports.
I watched many sports events every week. I also spent time reading about sportsbook odds.
Many sports fans I knew compared sportsbook offers.
Sometimes names like 1xbet would appear in conversations about major sporting events, although CarJitsu was usually too
strange to be the main topic.
One evening I saw a short video online. I honestly assumed
it was fake. Full-grown athletes were trying to wrestle inside a parked car while spectators were laughing,
cheering, and recording videos. I laughed so hard that I almost fell off my chair.
Yet the more I watched, the more fascinated I
became.
Not long afterward, I found a local event and decided
to attend. The atmosphere was incredible. There were fans discussing sports, training, and competition. Some people even joked about which athlete would be the favorite if a betting site ever offered odds on the matches.
Watching was not enough. I signed up for beginner training.
My debut practice was chaos. I hit my head on the roof,
got stuck near a seat, and accidentally opened a door at the worst possible moment.
Everyone laughed. Yet I kept coming back.
As time passed, I improved. I learned how to use smart tactics instead of brute strength.
The car stopped feeling tiny. Soon I was entering
small tournaments. My friends thought I was completely crazy.
Whenever someone asked what sport I practiced, the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The funniest and wildest experience happened during a tournament
a few years later. My opponent was massive.
He looked like he could carry an engine block. Before
the match started, he smiled and said, “You’re going to need luck.” That should
have been a warning.
The moment the referee signaled, chaos exploded. We bounced between seats, bumped into doors, and nearly tangled ourselves in everything inside the
vehicle. The crowd was roaring. Everyone was losing
their minds.
Then came the moment I will never forget.
My opponent grabbed the belt hanging beside the seat
and accidentally turned it into what looked like a wild
whip. As we struggled for position, the belt snapped across the cabin and wrapped around me in the strangest way
imaginable. For a second I thought, “I can’t believe this is happening”
He pulled, I twisted, the seat belt locked,
the door opened slightly, and both of us somehow ended up tangled together like a pile of cables.
The audience was laughing so hard that some people could barely stay in their seats.
The scene was unbelievable.
For a brief moment, I genuinely thought my opponent was going to
destroy me. Thankfully, the officials quickly intervened when things became unsafe, and the situation was resolved
without serious injury. Afterward we both burst out laughing.
Spectators cheered. Even today people who were there still talk
about “the seat belt incident.”
Looking back, CarJitsu remains one of the strangest sports I have ever experienced.
It gave me friendships, stories, and unforgettable memories.
Whether people are discussing sports culture and competition, very few
things create reactions like CarJitsu.
If anybody asks for the weirdest sport I know, I always tell them
about the day I climbed into a car in 2018 and accidentally became a CarJitsu competitor.
Most people laugh. But after hearing about tournaments, athletes, training sessions, sports
fans, betting conversations, sportsbook discussions, and my unforgettable seat belt battle,
they usually agree on one thing:
CarJitsu might be the craziest sport ever invented.
Also visit my blog post; more information
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Stateѕ
254-275-5536
Bookmarks
It’s fantastic that you are getting ideas from this
paragraph as well as from our dialogue made here.
my web page; my response
스트레스와 피로를 한 번에 날려줄 최고의 선택, 대전출장마사지와 함께 활기찬 내일을 준비해보세요.
When some one searches for his essential thing, so he/she needs to be available
that in detail, therefore that thing is maintained over here.
Feel free to visit my page; click here
I always spent my half an hour to read this blog’s
articles or reviews everyday along with a mug of coffee.
My web-site … Transformer Clamp
Hello, Neat post. There is an issue along with your web site in internet
explorer, could check this? IE still is the marketplace leader and
a large component of other folks will miss your excellent
writing because of this problem.
Feel free to surf to my web page dr vorobjev
Cabinet IQ
8305 Ⴝtate Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Sustainable
rqxpb6
Awesome! Its actually amazing paragraph, I have got much clear idea
regarding from this article.
Also visit my web blog; get redirected here
It is not my first time to visit this site, i am
visiting this web page dailly and get good information from
here every day.
Here is my web blog; News Proxy
Cabinet IQ
8305 State Hwwy 71 #110, Austin,
TX 78735, United Stɑteѕ
254-275-5536
Bookmarks
This site truly has all of the information and facts I wanted concerning
this subject and didn’t know who to ask.
Feel free to surf to my site viagra indonesia
Write more, thats all I have to say. Literally, it seems as though you relied on the
video to make your point. You clearly know what youre talking about,
why waste your intelligence on just posting videos to
your blog when you could be giving us something enlightening to read?
Here is my web site – crypto news today
For latest news you have to pay a visit world-wide-web and on web I found this website
as a best website for newest updates.
Here is my web site – markastotong
Ridiculous quest there. What occurred after? Good
luck!
My web-site GS441524
Yes! Finally something about 트립닷컴 할인코드.
I really like what you guys are usually up too.
This type of clever work and coverage! Keep up the awesome
works guys I’ve you guys to our blogroll.
my web page … web design tirana
Yes! Finally someone writes about 강남풀싸롱.
Very quickly this website will be famous among all blogging users, due to it’s fastidious articles
Also visit my site :: hublot watches yupoo
Thank you, I’ve recently been looking for information about this
topic for ages and yours is the greatest I’ve discovered till now.
But, what about the conclusion? Are you sure about the supply?
Feel free to visit my website; 트립닷컴 할인코드
My name is Mike, a regular guy from the USA, and back in 2018
I accidentally discovered one of the most bizarre sports I had
ever seen: Car Jitsu.
If this is your first time hearing about it, most people haven’t.
The entire concept sounds like a comedy sketch.
Two athletes climb inside a tiny automobile and try to control each other while being trapped between the dashboard and seats.
No, I’m not kidding. In most sports you have a field, but in CarJitsu your battlefield is a cramped car interior.
This is what shocked me the first time.
The sport has tournaments, championships, local events, and exhibition matches.
Athletes travel to compete and try to prove who can dominate inside the car.
Unlike traditional combat sports, every movement
is limited by doors, seats, windows, and seat belts. The result is
pure chaos. One second someone looks like a champion, and the next second they
are folded like a pretzel.
Back then I was heavily interested in sports.
I watched many sports events every week. I also spent time reading
about betting markets. Many sports fans I knew compared sportsbook offers.
Sometimes names like 1xbet would appear in conversations about major sporting events,
although CarJitsu was usually too strange to be the main topic.
Late one evening I saw a crazy highlight reel online.
Initially I believed it was a joke. Full-grown athletes were trying to battle inside a
parked car while spectators were laughing, cheering,
and recording videos. I laughed so hard that I almost fell off my chair.
Yet the more I watched, the more fascinated I became.
Soon after that, I found a local event and decided to attend.
The crowd energy was amazing. There were fans discussing all kinds of sporting topics.
Some people even joked about which athlete would be the favorite if a betting
site ever offered odds on the matches.
Watching was not enough. I signed up for beginner training.
The first training day was hilarious. I hit my head
on the roof, got stuck near a seat, and accidentally opened a door at the
worst possible moment. Everyone laughed. Yet I kept coming back.
Month after month, I improved. I learned how to use smart tactics
instead of brute strength. The vehicle became familiar.
Soon I was entering local competitions. My friends thought I
was completely crazy. Whenever someone asked what sport I practiced, the
conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The craziest match of my career came later. My opponent was built like a truck.
He looked like he could carry an engine block. Before the
match started, he smiled and said, “Good luck.” I should have listened.
The moment the referee signaled, chaos exploded.
We bounced between seats, bumped into doors, and
nearly tangled ourselves in everything inside the vehicle.
The crowd was roaring. Spectators were going crazy.
Then came the moment I will never forget.
My opponent grabbed the belt hanging beside the seat
and accidentally turned it into what looked like a crazy lasso.
As we struggled for position, the belt snapped across the cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “What kind of sport did I join?”
He pulled, I twisted, the seat belt locked,
the door opened slightly, and both of us somehow ended
up tangled together like a pile of cables.
The audience was laughing so hard that some people could barely stay in their seats.
Nobody could believe what they were seeing.
For a brief moment, I genuinely thought my opponent was going to destroy me.
Fortunately, the officials quickly intervened when things became
unsafe, and the situation was resolved without serious injury.
Afterward we both burst out laughing. The crowd applauded.
Even today people who were there still talk about “that crazy seat belt match.”
When I remember those years, CarJitsu remains one of the strangest sports I have ever experienced.
It gave me countless funny moments. Whether people are discussing athletic entertainment,
very few things create reactions like CarJitsu.
Whenever someone asks me about unusual sports, I always tell them about the day I
climbed into a car in 2018 and accidentally became a CarJitsu
competitor. The reaction is always the same. But after hearing about tournaments, athletes, training sessions, sports fans,
betting conversations, sportsbook discussions, and my unforgettable seat belt battle, they usually agree on one
thing:
CarJitsu might be the craziest sport ever invented.
my web site … url
You have made some really good points there.
I checked on the net to learn more about the issue and found most
individuals will go along with your views on this site.
my blog … 아고다 할인코드
Cabinet IQ
8305 Ꮪtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Timeline
My name is Mike, a normal American guy, and during 2018 I accidentally discovered one of the strangest sports ever invented: Car
Jitsu.
In case this sounds unfamiliar, don’t worry.
The entire concept sounds like a comedy sketch.
Two fighters climb inside a compact vehicle and try to control
each other while being trapped between the dashboard and seats.
Yes, really. In most sports you have a court, but
in CarJitsu your battlefield is a car cabin. That is why people laugh when they first hear about it.
There are organized competitions, tournaments,
championships, and special events. Competitors come
from different places and try to prove who can adapt best to the strange environment.
Unlike traditional combat sports, every movement is limited by doors, seats, windows, and seat
belts. That creates hilarious moments. One second someone looks like a champion, and the next second they
are folded like a pretzel.
During those days I was heavily interested in competitive sports.
I watched all kinds of competitions. I also spent time reading
about sports betting. People around me talked about betting and sportsbooks.
Sometimes names like the sportsbook 1xbet would appear
in conversations about major sporting events, although CarJitsu was usually
too strange to be the main topic.
Late one evening I saw a crazy highlight reel online. Initially
I believed it was a joke. Full-grown athletes were trying to grapple inside a parked car while spectators were watching
in disbelief. I laughed so hard that I almost fell off my chair.
Yet the more I watched, the more fascinated I became.
Not long afterward, I found a local event and decided to show up.
The crowd energy was amazing. There were fans discussing all kinds of
sporting topics. Some people even joked about
which athlete would be the favorite if a sportsbook ever
offered odds on the matches.
Watching was not enough. I signed up for beginner training.
My debut practice was chaos. I hit my head on the roof, got stuck
near a seat, and accidentally opened a door at the worst possible
moment. Even I laughed at myself. Yet I kept coming back.
Month after month, I improved. I learned how to use smart tactics instead
of brute strength. The vehicle became familiar. Soon I was entering regional events.
My friends thought I was completely crazy.
Whenever someone asked what sport I practiced, the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The funniest and wildest experience happened during a tournament a few years later.
My opponent was huge. He looked like he could carry an engine block.
Before the match started, he smiled and said, “Good luck.” I
should have listened.
The moment the referee signaled, chaos exploded. We
bounced between seats, bumped into doors, and
nearly tangled ourselves in everything inside the vehicle.
The crowd was roaring. Spectators were going crazy.
Then came the moment I will never forget.
My opponent grabbed the car seat belt and accidentally turned it into what looked like a dangerous rope.
As we struggled for position, the belt snapped
across the cabin and wrapped around me in the
strangest way imaginable. For a second I thought, “What kind of sport did I join?”
He pulled, I twisted, the seat belt locked, the door opened slightly,
and both of us somehow ended up tangled together like a
pile of cables. The audience was laughing so hard that some people could barely stay in their
seats. The scene was unbelievable.
For a brief moment, I genuinely thought my opponent was going to crush me.
Fortunately, the officials quickly intervened when things became unsafe, and
the situation was resolved without serious injury.
Afterward we both burst out laughing. Spectators cheered.
Even today people who were there still talk about
“the legendary belt tangle.”
Looking back, CarJitsu remains one of the weirdest athletic competitions I
have ever experienced. It gave me friendships, stories, and unforgettable memories.
Whether people are discussing athletic entertainment, very few things create
reactions like CarJitsu.
Whenever someone asks me about unusual sports, I always tell
them about the day I climbed into a car in 2018 and accidentally became
a CarJitsu competitor. Most people laugh. But after hearing
about tournaments, athletes, training sessions,
sports fans, betting conversations, sportsbook discussions,
and my unforgettable seat belt battle, they usually agree on one thing:
CarJitsu might be the craziest sport ever invented.
my blog – URL
bookmarked!!, I like your blog!
Here is my web blog: AVS Holidays Pvt Limited
naturally like your web-site but you have to check the spelling on quite a few of your
posts. Many of them are rife with spelling issues and I in finding it very
troublesome to inform the truth however I’ll surely come again again.
Also visit my web blog: video porno gratis
свадебные торты с доставкой – изысканный декор под вашу стилистику.
ваниль с голубикой. свечи и топпер в подарок.
рассрочка без процентов
торт с мастикой на заказ – для волшебной фотосессии.
цветы, кружево, банты. мастика ручной работы.
доставка в термосумке
торт для мужчины на юбилей –
британский стиль или кожа.
банка пива и вобла. пряный имбирь.
надпись из шоколада
I don’t even understand how I finished up here, but I thought this post was good.
I do not understand who you might be however definitely you’re going to a famous blogger
if you are not already. Cheers!
my blog – mobidax.io lừa đảo người chơi công an vào cuộc
May I just say what a comfort to uncover somebody that genuinely knows what they’re talking about over the internet.
You actually understand how to bring a problem to light
and make it important. A lot more people ought to read this and understand this side of your story.
I was surprised that you are not more popular given that you
surely possess the gift.
my homepage … AVS Holidays Pvt Limited
I’ll immediately grab your rss as I can’t find your email subscription hyperlink or e-newsletter service.
Do you’ve any? Please allow me recognise so that I could
subscribe. Thanks.
Have a look at my homepage – 트립닷컴 할인코드
hello there and thank you for your information – I have definitely picked up anything new from right here.
I did however expertise some technical points using this
website, as I experienced to reload the site a lot of times
previous to I could get it to load correctly. I had been wondering if
your hosting is OK? Not that I am complaining, but sluggish loading instances times will often affect
your placement in google and could damage your high-quality score if advertising and
marketing with Adwords. Anyway I am adding this RSS to my e-mail and could look out for a lot more of your respective intriguing content.
Ensure that you update this again soon.
my blog post – 트립닷컴 할인코드
Artikel yang sangat menarik dan informatif. Banyak pengguna
di Indonesia mencari informasi terpercaya tentang viagra indonesia
dan kesehatan pria. Konten seperti ini sangat membantu pembaca memahami penggunaan yang aman dan efektif.
Terima kasih atas artikel yang bermanfaat ini. Topik viagra indonesia memang banyak
dicari saat ini, terutama bagi mereka yang ingin mendapatkan informasi kesehatan pria
secara aman dan tepat.
Konten yang bagus dan mudah dipahami. Informasi mengenai viagra indonesia sangat
relevan dan membantu banyak orang mendapatkan edukasi yang benar tentang kesehatan pria.
I am in fact thankful to the holder of this website who has shared this enormous article at at this place.
my web blog; Siete Casino
Do you have any video of that? I’d care to find out some additional information.
my webpage :: 트립닷컴 할인코드
You’ve made some good points there. I looked on the web to learn more about the issue
and found most individuals will go along with your views on this web site.
Look at my web-site; methodist churches near me
I think this is one of the such a lot vital info for me.
And i’m happy reading your article. But should commentary on some general things, The web
site style is great, the articles is in reality excellent :
D. Just right job, cheers
Visit my blog :: free browser word game
Hello There. I discovered your blog using msn. That is a very neatly
written article. I will make sure to bookmark it and come
back to read more of your helpful info. Thank you for the post.
I will certainly return.
Feel free to visit my page … Siete Casino
This blog was… how do you say it? Relevant!!
Finally I’ve found something that helped me. Appreciate it!
Here is my website :: san antonio church
Fala aí, não tenho certeza se sobre jogo responsável? vale a pena?
Hi there, yeah this paragraph is really fastidious and I have learned lot of things from it concerning
blogging. thanks.
my page; free browser word game
Cabinet IQ
8305 Stаtе Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Bookmarks
I pay a quick visit day-to-day a few web pages and sites to read articles, however this webpage
presents quality based content.
my webpage :: unblocked games 75
Excellent blog here! Also your web site loads up very fast!
What host are you using? Can I get your affiliate link to your
host? I wish my web site loaded up as quickly as yours lol
Check out my blog: night tour la fortuna
Love how you connect theory and reality
Look into my website – Stella Huh [Jesus]
I pay a visit every day a few websites and blogs to read
posts, except this blog presents feature based content.
Feel free to surf to my webpage Siete
What’s up friends, its fantastic article on the topic of teachingand completely explained, keep it up all the time.
Feel free to visit my web-site – singapore business
I enjoy what you guys tend to be up too. This type of clever work and exposure!
Keep up the very good works guys I’ve included you guys to blogroll.
My blog Tube Metal Laser Cutting Machine
My name is Mike, a regular guy from the USA, and during 2018 I accidentally discovered one of the strangest sports ever invented: Car Jitsu.
If you have never heard of it, most people haven’t. The entire concept sounds like
a joke. Two athletes climb inside a compact vehicle and try to control each other while being trapped
between the seats. No, I’m not kidding. In most sports you
have a field, but in CarJitsu your battlefield is a
cramped car interior. This is what shocked me the first time.
The sport has tournaments, championships, local events, and exhibition matches.
Athletes travel to compete and try to prove who can master the
unusual format. Compared to ordinary sports, every movement is limited by the tight space.
This leads to funny situations. One second someone looks like a
champion, and the next second they are trapped near the steering wheel.
During those days I was heavily interested in unusual athletic events.
I watched all kinds of competitions. I also spent time
reading about betting markets. Friends often discussed sportsbooks.
Sometimes names like 1xbet would appear in conversations about major
sporting events, although CarJitsu was usually too strange to be the main topic.
Late one evening I saw a crazy highlight reel online.
I honestly assumed it was fake. Competitive fighters were
trying to battle inside a parked car while spectators were going crazy
with excitement. I laughed so hard that I couldn’t breathe for a moment.
Yet the more I watched, the more fascinated I became.
Soon after that, I found a local event and decided to show up.
The event was unforgettable. There were fans discussing all kinds of sporting topics.
Some people even joked about which athlete would be the favorite if
a betting site ever offered odds on the matches.
Watching was not enough. I signed up for beginner training.
My debut practice was chaos. I hit my head on the roof, got stuck near a seat,
and accidentally opened a door at the worst possible moment.
Even I laughed at myself. Yet I kept coming back.
Week after week, I improved. I learned how to use positioning,
leverage, balance, and timing. The cramped cabin became my arena.
Soon I was entering small tournaments. My friends
thought I was completely crazy. Whenever
someone asked what sport I practiced, the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The funniest and wildest experience happened during a tournament
a few years later. My opponent was built like a truck.
He looked like he could bench-press a refrigerator.
Before the match started, he smiled and said, “Good luck.” I knew trouble was coming.
The moment the referee signaled, chaos exploded. We bounced between seats, bumped
into doors, and nearly tangled ourselves in everything
inside the vehicle. The crowd was roaring. Everyone was
losing their minds.
Then came the moment I will never forget.
My opponent grabbed the seat belt and accidentally turned it
into what looked like a crazy lasso. As we struggled for position, the belt snapped across the cabin and wrapped around me in the strangest way imaginable.
For a second I thought, “What kind of sport did I join?”
He pulled, I twisted, the seat belt locked, the door opened slightly, and both of us somehow ended
up tangled together like two confused octopuses.
The audience was laughing so hard that some people could
barely stay in their seats. Nobody could believe what they were seeing.
For a brief moment, I genuinely thought my opponent was going to flatten me.
Fortunately, the officials quickly intervened when things became unsafe, and the situation was resolved without serious injury.
Afterward we both burst out laughing. The crowd applauded.
Even today people who were there still talk about “the legendary belt tangle.”
Thinking about my journey, CarJitsu remains one of
the weirdest athletic competitions I have ever experienced.
It gave me great memories and incredible experiences.
Whether people are discussing sports, betting, sportsbooks, competitions,
or events, very few things create reactions like CarJitsu.
Whenever someone asks me about unusual sports, I always tell them
about the day I climbed into a car in 2018 and accidentally became a CarJitsu competitor.
The reaction is always the same. But after hearing about tournaments, athletes, training sessions, sports fans, betting conversations, sportsbook discussions,
and my unforgettable seat belt battle, they usually agree on one
thing:
CarJitsu might be the craziest sport ever invented.
Visit my homepage; more info
Within the dynamic landscape of entertainment, online casinos
emerged as a thrilling and obtainable avenue for individuals seeking the pleasure of video gaming
from the comfort of their own houses. The actual allure of those virtual systems lies not only in the opportunity of profit but also in the
immersive and engaging experiences they provide.
Also visit my web page: top111 login
Awesome website you have here but I was curious about if you knew of any user discussion forums that cover the same topics talked about in this article?
I’d really like to be a part of online community where I
can get advice from other experienced individuals
that share the same interest. If you have any suggestions, please let
me know. Bless you!
My site :: slot pepek
Heya! I just wanted to ask if you ever have any issues with hackers?
My last blog (wordpress) was hacked and I ended up losing many months of hard work due to no
backup. Do you have any methods to stop hackers?
My site :: Marine Parts
You probably get some images scurry through your head when I tell you that BlackTube is a free tube
dedicated to bad bitches. These girls are evil in the
classic porn way, for one thing, because they double fist with a pair of girlfriends in a group scene, get pounded up the pussy by a
thick, throbbing BBC, and do all kinds of crap
your mother told you nice girls don’t do. BLACK TUBE https://directoriomipymes.com/author-profile/ginauren412067/
You probably get some images scurry through your head when I tell you that BlackTube
is a free tube dedicated to bad bitches. These
girls are evil in the classic porn way, for one thing, because
they double fist with a pair of girlfriends in a group scene, get pounded up the pussy by a thick, throbbing
BBC, and do all kinds of crap your mother told you nice girls don’t do.
BLACK TUBE http://gitlab.medsi.com.mx/rowenathibodea/rowena1989/-/issues/1
winx96 casino, https://play-winx96.com/ offers a captivating experience for casino enthusiasts.
With countless games available, everyone can find an option to
enjoy. Join the thrill today at winx96 casino and explore amazing rewards
and bonuses!
Terrific work! This is the type of information that are
meant to be shared around the net. Disgrace on Google
for now not positioning this submit upper! Come on over and visit
my web site . Thank you =)
Here is my web page – cialis
I will immediately take hold of your rss feed as I can’t
find your e-mail subscription hyperlink or e-newsletter service.
Do you have any? Please permit dental anxiety dentist near me understand so that I may subscribe.
Thanks.
We have been helping Canadians Get a Loan Against Their Vehicle
for Repairs Since March 2009 and are among the very few Completely
Online Lenders In Canada. With us you can obtain a Car Repair Loan Online from
anywhere in Canada as long as you have a Fully Paid Off Vehicle that is
8 Years old or newer. We look forward to meeting all your financial needs.
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Costcalc
I’m Mike, a normal American guy, and back in 2018 I accidentally discovered one of the most bizarre sports I
had ever seen: car jitsu.
If this is your first time hearing about it, most people haven’t.
The entire concept sounds like a comedy sketch. Two fighters climb inside a compact vehicle and try to score positions against each other
while being trapped between the cramped interior. No, I’m not kidding.
In most sports you have a ring, but in CarJitsu your battlefield is the inside of a vehicle.
This is what shocked me the first time.
The sport has tournaments, championships, local events, and exhibition matches.
Athletes travel to compete and try to prove who can adapt best to the strange environment.
Compared to ordinary sports, every movement is limited by doors, seats, windows, and seat belts.
That creates hilarious moments. One second someone looks like a champion, and the next second they are trapped near the steering wheel.
At that time I was heavily interested in unusual athletic events.
I watched football, basketball, MMA, and wrestling. I also spent time reading about sports betting.
Friends often discussed sportsbooks. Sometimes names like 1xbet would appear in conversations about major sporting
events, although CarJitsu was usually too strange to be the main topic.
One night I saw a short video online. Initially I believed it
was a joke. Grown adults were trying to grapple inside a
parked car while spectators were going crazy with excitement.
I laughed so hard that I couldn’t breathe for a
moment. Yet the more I watched, the more fascinated I became.
Not long afterward, I found a local event and decided to watch in person. The event was unforgettable.
There were fans discussing sports, training, and competition. Some people even joked
about which athlete would be the favorite if a sportsbook
ever offered odds on the matches.
Soon I wanted more than just watching. I signed up for beginner training.
My debut practice was chaos. I hit my head on the roof, got stuck
near a seat, and accidentally opened a door at the worst possible moment.
Everyone laughed. Yet I kept coming back.
Week after week, I improved. I learned how to use positioning, leverage, balance, and timing.
The vehicle became familiar. Soon I was entering regional events.
My friends thought I was completely crazy.
Whenever someone asked what sport I practiced, the conversation usually went like this:
“CarJitsu.”
“What is that?”
“Imagine wrestling inside a car.”
“You’re joking.”
“No, that’s the actual sport.”
The craziest match of my career came later. My opponent
was huge. He looked like he could carry an engine block.
Before the match started, he smiled and said, “Good luck.” I should have listened.
As soon as the fight started, chaos exploded. We bounced between seats, bumped into doors, and nearly tangled ourselves in everything inside the vehicle.
The crowd was roaring. Spectators were going crazy.
Then came the moment I will never forget.
My opponent grabbed the car seat belt and accidentally turned it into what looked like a crazy lasso.
As we struggled for position, the belt snapped across the cabin and wrapped around me in the strangest
way imaginable. For a second I thought, “What kind of sport did I join?”
He pulled, I twisted, the seat belt locked, the door opened slightly,
and both of us somehow ended up tangled together like a pile of cables.
The audience was laughing so hard that some people could barely stay in their seats.
The scene was unbelievable.
For a brief moment, I genuinely thought my opponent was going
to destroy me. Thankfully, the officials quickly intervened when things became unsafe, and the situation was resolved without serious injury.
Afterward we both burst out laughing. Spectators cheered.
Even today people who were there still talk about “the legendary belt tangle.”
Thinking about my journey, CarJitsu remains one of the strangest sports I have ever experienced.
It gave me countless funny moments. Whether people are discussing
sports culture and competition, very few things create reactions like CarJitsu.
If anybody asks for the weirdest sport I know, I always tell them about the day I climbed into a car in 2018 and accidentally became a CarJitsu competitor.
Nobody believes it at first. But after hearing about tournaments, athletes,
training sessions, sports fans, betting conversations, sportsbook discussions, and my unforgettable seat
belt battle, they usually agree on one thing:
CarJitsu might be the craziest sport ever invented.
Here is my blog – read more
For newest news you have to visit the web and on the web I found this web page as a most excellent web site for most up-to-date updates.
Also visit my website equipment rental agency Ridgefield
Stunning story there. What happened after? Good luck!
Feel free to visit my web blog :: SEO link
Thank you a lot for sharing this with all of us you really recognize what you’re talking approximately!
Bookmarked. Please additionally talk over with my website =).
We will have a hyperlink exchange agreement among us
Here is my web-site – equipment rental agency Ridgefield
What’s up to all, as I am in fact eager of reading this web site’s post to be updated regularly.
It contains fastidious information.
Look at my site; liječenje od alkoholizma
Thanks for finally talking about > Heel Pain –
Plantar Fasciitis – Mr Will Edwards web site
I like it when individuals come together and share thoughts.
Great website, keep it up!
Feel free to surf to my blog post – Les Invalides
I love it whenever people come together and share opinions.
Great blog, stick with it!
Feel free to surf to my web page: cardiovascular support
Online tool video downloader for pinterest
downloading Pinterest videos, images & gifs.
Saved as a favorite, I love your blog!
Also visit my blog post cardiovascular supplement
Hello there! This post could not be written much better!
Reading through this post reminds me of my previous
roommate! He always kept talking about this. I most certainly will send this article to him.
Pretty sure he will have a good read. Thanks for sharing!
my site :: HTN Support
Today, I went to the beachfront with my kids. I found a sea shell and gave it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She
placed the shell to her ear and screamed. There was a hermit crab inside and it pinched her
ear. She never wants to go back! LoL I know this is totally off topic but
I had to tell someone!
Also visit my web blog … Greensboro Area Office Cleaning Services
대전출장마사지이곳에서 365일 휴일없는 후불제로 24시간 이용해보세요. 대전 유성 봉명 모든지역 30분내 방문
I could not resist commenting. Perfectly written!
Feel free to visit my page: heart health supplements
ремонт кровли и крыш – утепление и пароизоляция.
фальцевая кровля, композит. бесплатный
замер лазером. выезд бригады на завтра
реконструкция деревянных каркасный дом под ключов – подъём дома домкратами.
антисептирование и огнезащита.
цена от 50 000 ₽ за венец.
сохраняем исторический облик
монтаж кровли и кровельные работы – металлочерепица под ключ.
гидроветрозащита Tyvek или Ютафол.
бесплатный замер в Дмитрове. антиобледенение по
желобу
Wow, this article is pleasant, my younger sister is analyzing these things, thus I am
going to tell her.
Feel free to visit my web-site: growth advisors for HVAC
Hey there would you mind stating which blog platform you’re working with?
I’m planning to start my own blog in the near future but I’m having a tough time choosing between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design and style seems different then most blogs and I’m looking for something unique.
P.S Apologies for getting off-topic but I had to ask!
Also visit my web-site: sex
Sayt çox praktikdir.
https://www.heritagebritain.com/track.php?https://pin-up-azerbaijan-betting.org/oyunlar
Can you tell us more about this? I’d like to find out some additional information.
Feel free to visit my page; Plastic Lid
Hey there this is kind of of off topic but I was wondering if blogs use WYSIWYG editors or if
you have to manually code with HTML. I’m starting
a blog soon but have no coding know-how so I wanted to
get advice from someone with experience. Any help would be enormously appreciated!
my homepage: Angka Shio Kelinci
I don’t know whether it’s just me or if
everybody else experiencing issues with your site.
It seems like some of the written text in your posts are running off the screen. Can someone
else please provide feedback and let me know if this is happening to them as
well? This may be a problem with my web browser because I’ve had this happen before.
Kudos
my webpage; Carrier Tape
Cabinet IQ
8305 Statе Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
HomeDIY
Spot on with this write-up, I honestly believe that this web
site needs a great deal more attention. I’ll probably be
back again to read through more, thanks growth advisors for HVAC the
info!
Hello, every time i used to check weblog posts here in the early hours in the daylight, because
i enjoy to learn more and more.
my webpage … web site
Excellent post about glazenwasser services! I’ve been trying
to find a dependable lokale glazenwasser in my area and this gives great insight – particularly the tips about finding
goedkope glazenwasser options that still do professional
glazen schoonmaken work, because my company needs regular glazenwasser voor bedrijven and I want to
make sure we get an experienced professional who knows what they’re doing with office spaces.
my site … building maintenance specialists (Roxie)
Just wanna admit that this is extremely helpful, Thanks for taking your time to write this.
I don’t even know how I ended up here, but I thought this post was good.
I do not know who you are but definitely you’re going to
a famous blogger if you aren’t already ;) Cheers!
Also visit my homepage: apollogrouptv
Livetotobet – Platform terpercaya untuk pembelian voucher game dengan sistem poin dan hadiah gratis.
Putar roda hadiah dan dapatkan bonus menarik setiap harinya!
Feel free to visit my web-site :: https://livetotobetcom.id/
This gave me the tools I was looking for
Also visit my webpage – joe bart pdf (Antony)
I’m not that much of a internet reader to be honest but your blogs really nice, keep it up!
I’ll go ahead and bookmark your website to
come back down the mvt road.
Cheers
Инженерное совершенство и технологическое лидерство:
Комплексные решения от компании EC-P
My webpage … https://ec-p.ru/
Heya i’m for the first time here. I came across this board and I find It
truly useful & it helped me out much. I’m hoping to offer
one thing back and aid others such as you aided me.
Have a look at my web site – OTOT133
I’m not sure why but this website is loading
incredibly slow for me. Is anyone else having this issue or is it a problem on my end?
I’ll check back later on and see if the problem still exists.
Feel free to visit my page; فیلم مثبت 18
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Countertopexperts; Melba,
It’s an amazing paragraph in support of all the internet viewers;
they will obtain benefit from it I am sure.
Also visit my web blog OTOT133
Your mode of describing everything in this piece of writing is
truly pleasant, all be able to simply know it, Thanks a lot.
Feel free to visit my homepage – weblink
I just couldn’t depart your web site prior to suggesting that I really enjoyed the usual information an individual supply for your
visitors? Is gonna be back steadily in order to check up on new posts
Feel free to surf to my homepage; pike county detention center
Good way of telling, and pleasant post to get information about my
presentation topic, which i am going to present in school.
my blog; 프리카지노
I am really delighted to read this weblog posts which contains plenty of valuable
information, thanks for providing these information.
Also visit my web-site slot bujang inam
The rebounding battle is fierce under the rim. WHAT A GAME!
This text is worth everyone’s attention. How can I find out more?
My blog: bokep asli indonesia
Hello, i think that i saw you visited my site so i came to “return the favor”.I
am attempting to find things to improve my web site!I suppose its ok to use a few of your ideas!!
my page – angka mimpi 2d hari ini
Does your blog have a contact page? I’m having trouble locating
it but, I’d like to shoot you an e-mail. I’ve got some
recommendations for your blog you might be interested in hearing.
Either way, great website and I look forward to seeing it
improve over time.
Here is my webpage … B5I file information
Hello! I’ve been following your weblog for some time now and finally got the courage to
go ahead and give you a shout out from Huffman Tx! Just wanted to tell
you keep up the fantastic job!
Also visit my site :: Shrooms Direct
I was recommended this website by my cousin. I’m not sure whether this post is written by him as no one else know such
detailed about my difficulty. You are wonderful! Thanks!
my blog :: angelkas heels
Hello, I enjoy reading all of your post. I
like to write a little comment to support you.
Stop by my website: JC tuition Woodlands
I’m amazed, I have to admit. Seldom do I come across a blog that’s
both equally educative and interesting, and let me tell
you, you have hit the nail on the head. The problem is something too few men and women are speaking intelligently about.
Now i’m very happy I came across this in my search for something concerning this.
Existe una aplicación en Google Play Store llamada Download Twitter Videos o TweetSave en App Store, que permiten descargar videos
de la red social ahora propiedad de Elon Musk.
Also visit my website … MáS datos
Excellent blog post. I definitely love this site. Continue the good work!
my website … daily seo services
Why people still use to read news papers when in this technological globe all
is existing on net?
Look into my web site :: crypto casino no kyc
You really make it seem so easy with your presentation but I find this topic to be really something that I think I would never understand.
It seems too complicated and very broad for me.
I’m looking forward for your next post, I will try to get the hang of it!
my web-site :: BC Game
People call me Anna, a 35-year-old woman. For years, my relationship was in trouble.
My husband and I barely spoke. Eventually, I accepted that our marriage had reached its end.
One evening, while looking for entertainment online, I discovered an online slot.
The game featured shining symbols, reward
multipliers, and surprising twists. Every spin felt exciting.
At first, I played with a small balance. The reels showed colorful icons and bonus signs.
Then something changed. A series of perfect combinations appeared across the screen. The sounds became louder, the animations brighter, and my heart
started racing.
I could hardly believe my eyes. One bonus round led to another.
Multipliers stacked. The winnings kept growing.
I couldn’t stop smiling. The number on the screen climbed higher and higher.
Then came the moment I will never forget. The reels aligned perfectly.
The screen exploded with lights and animations. The total reached $100,
000.
I couldn’t process what had happened. For several minutes, I simply stared
at the screen. The emotions were overwhelming: pure excitement and gratitude.
That win did not magically solve every problem in my
life, but it gave me a fresh start. Around the same time, I
met a kind person. More importantly, I realized that happiness comes from making decisions that
are right for you.
Today, I look back on that night as a surprising
chapter of my life. Life moved on. And while the jackpot was exciting,
the biggest reward was finding the courage to create a life that felt right for
me.
Here is my blog :: news
It’s an awesome article for all the internet users; they will get advantage from
it I am sure.
Here is my webpage :: vanity address tron
Hi, Neat post. There’s a problem with your web site in web explorer,
could test this? IE still is the marketplace chief and
a big component of other people will leave out your wonderful writing because of this
problem.
Feel free to visit my web site scam
What i do not understood is in fact how you are now not really a lot more smartly-appreciated
than you may be right now. You’re very intelligent.
You already know thus significantly in relation to this subject, produced
me for my part imagine it from numerous various angles. Its like men and women aren’t interested until it is something to accomplish with Girl gaga!
Your personal stuffs outstanding. All the time deal with it up!
My page :: basement flood cleanup
Wow, this post is fastidious, my younger sister is analyzing these things, therefore I am
going to tell her.
My site: danatogel
That is a very good tip particularly to those new to the blogosphere.
Short but very precise info… Thank you for sharing this
one. A must read article!
Here is my page :: viagra
Cabinet IQ
8305 Ⴝtate Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Interiorconsult, https://Naydieynmg.raindrop.Page/bookmarks-72078234,
Hello it’s me, I am also visiting this web site on a regular basis, this
website is genuinely good and the visitors are in fact sharing pleasant thoughts.
Visit my web site; Shrooms Direct Online Store
When I initially commented I clicked the “Notify me when new comments are added”
checkbox and now each time a comment is added I get four e-mails with the same comment.
Is there any way you can remove me from that service?
Appreciate it!
My homepage :: simbol scatter
Hi! This is my first comment here so I just wanted to give a quick shout out and
say I truly enjoy reading through your articles. Can you suggest
any other blogs/websites/forums that deal with the same topics?
Thanks a lot!
Also visit my homepage: Mushroom Products Online
Hi! Do you use Twitter? I’d like to follow you if that would be ok.
I’m definitely enjoying your blog and look forward to new posts.
Stop by my web site; пинап казино официальный сайт
hi!,I really like your writing so much! proportion we keep up a correspondence extra approximately your article on AOL?
I require an expert on this house to solve my problem. May be
that is you! Looking ahead to look you.
Also visit my blog: viagra
We stumbled over here from a different web address and thought I might
as well check things out. I like what I see so now i’m following you.
Look forward to looking over your web page repeatedly.
Review my website: Best Conveyor Belt Supplier
Цифровой компас в мире железа: Зачем нужны специализированные
порталы о персональных компьютерах?
Look into my webpage … https://homepc.ru/
Hey very nice blog!
Feel free to visit my site saber mas
ксгорун рабочий сайт
My webpage: csgorun registration site
May I just say what a relief to uncover an individual who truly understands what they are talking about on the web.
You definitely know how to bring a problem to light and make it important.
More people have to check this out and understand this side of
your story. I can’t believe you are not more popular
given that you most certainly possess the gift.
My web page … water damage repair
เนื้อหานี้ อ่านแล้วเพลินและได้สาระ ค่ะ
ดิฉัน เพิ่งเจอข้อมูลเกี่ยวกับ เรื่องที่เกี่ยวข้อง
สามารถอ่านได้ที่ tkb333
เผื่อใครสนใจ
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ บทความคุณภาพ
นี้
และอยากเห็นบทความดีๆ
แบบนี้อีก
โพสต์นี้ ให้ข้อมูลดี ครับ
ผม ไปเจอรายละเอียดของ เนื้อหาในแนวเดียวกัน
ที่คุณสามารถดูได้ที่
สล็อตเว็บตรง
สำหรับใครกำลังหาเนื้อหาแบบนี้
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
These are some of the most important issues we’ll face over the next few decades.
We are a group of volunteers and starting a new initiative in our community. Your blog provided us with valuable information to work on|.You have done a marvellous job!
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-30kh200-mm-los/
Cabinet IQ
8305 Statе Hwy 71 #110, Austin,
TX 78735, Unite Stɑtеs
254-275-5536
Kitchenupdate
Cabinet IQ
8305 Statе Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Corner
If you desire to obtain a good deal from this piece of writing then you have to apply these techniques to your won webpage.
My web page: пин ап казино
Широкий выбор тугоплавких металлов, таких как вольфрам и молибден
https://redmetsplav.ru/store/tantal-i-ego-splavy/tantal-4b/poroshok-tantalovyy-4b/
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-64kh42-mm-m2-gost-r-52948-2008/
This article gives clear idea designed for the new visitors of blogging, that in fact
how to do blogging.
Visit my site :: vegas108 link
Wow, that’s what I was searching for, what a information! existing here
at this webpage, thanks admin of this web site.
My web blog: Short Link Service
Искусство цифрового поиска: Как найти
идеальный профессиональный портал для ежедневной
работы?
My web blog https://zis365.com/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-30khgsa-19x1300x1000-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
โพสต์นี้ อ่านแล้วเพลินและได้สาระ ค่ะ
ดิฉัน เพิ่งเจอข้อมูลเกี่ยวกับ เนื้อหาในแนวเดียวกัน
ที่คุณสามารถดูได้ที่ bbn168
ลองแวะไปดู
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
และอยากเห็นบทความดีๆ แบบนี้อีก
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-900kh800-mm-lts37mts2s2k/
Hi there are using WordPress for your blog platform?
I’m new to the blog world but I’m trying to get started and set up my own. Do you need
any coding expertise to make your own blog? Any help would be greatly appreciated!
Also visit my blog post; I’m a piece of shit
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-03x18k8m5tiur-vi-26×4-gost-8734-75/
Hi colleagues, good piece of writing and pleasant arguments commented here, I am really
enjoying by these.
Also visit my blog :: apollo tv
Продажа проволоки из тугоплавких металлов востребована в электронике
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-nimo-25-3/lenta-molibdenovaya-nimo-25-1/
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-1kh1500kh3000-mm-1-4016-en-iso-9444-1/
Использование современных технологий защиты данных пользователей
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-cm5-4/truba-molibdenovaya-cm5-1/
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-45-gradusov-17-mm-m3-gost-r-52948-2008/
Оперативная логистика и поддержка на всех этапах сделки позволяют минимизировать сроки простоя производственных линий заказчиков.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r9k10-105-gost-1133-71/
Наличие редких позиций, например, изделий из гафния и ванадия
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-ze10a/krug-magnievyy-ze10a/
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-300kh300-mm-lsdch/
Admiring the time and effort you put into your site and detailed info you offer!
Важным преимуществом является возможность изготовления деталей и изделий по индивидуальным чертежам заказчика.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-70kh50kh6-mm-40nicrmo22-din-1029/
Наличие калькулятора металлопроката упрощает расчет веса и стоимости
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-r60700—uns/poroshok-magnievyy-r60700—uns/
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-90-gradusov-40-mm-m3rm-gost-r-52948-2008/
Thankfulness to my father who stated to me regarding this webpage, this website is truly awesome.
Here is my homepage HORSE GELATIN REVIEW
I pay a quick visit everyday some web sites and information sites to read posts, but this webpage presents
feature based writing.
Here is my web page; topvegas
Hi there to every body, it’s my first visit of this blog; this web site consists of amazing and in fact excellent
stuff for readers.
Visit my website: are jumping spiders friendly
Cabinet IQ
8305 Ꮪtate Hwy 71 #110, Austin,
TX78735, United Ѕtates
254-275-5536
Quotecalc
Hey there! Quick question that’s completely off topic.
Do you know how to make your site mobile friendly?
My website looks weird when viewing from my iphone
4. I’m trying to find a theme or plugin that might be able to resolve this problem.
If you have any suggestions, please share. Thanks!
Also visit my web site :: bokep film indonesia
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-r60707—uns/list-magnievyy-r60707—uns/
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/plity/plita-r6m5k5-30x200x450-gost-19903-74/
Wow that was strange. I just wrote an very long comment but after I
clicked submit my comment didn’t show up. Grrrr… well I’m
not writing all that over again. Anyway, just wanted to say wonderful blog!
my blog post here
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-al3zn1mn—bs-3373/truba-magnievaya-mg-al3zn1mn—bs-3373/
I all the time emailed this web site post page to all my friends, as if
like to read it after that my links will too.
Feel free to visit my blog: سایت سوپر ایرانی
I pay a visit daily a few blogs and information sites to read articles or reviews,
except this blog gives quality based articles.
Feel free to visit my blog – visabet88 bandar togel terpercaya
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/manganinovaia-provoloka/manganinovaia-provoloka-1-1-mm-mnmts3-12-gost-10155-72/
ООО «РМС» предлагает широкий спектр цветного проката, включая медь, латунь, бронзу и дюралюминий.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-3ps5-63x63x4-gost-8509-93/
We recognize the value of your time, which is why we have incorporated a Turbo Mode feature into Easy Videos Downloader.
my homepage :: download video mp4
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-al3zn1mn—bs-3373/lenta-magnievaya-mg-al3zn1mn—bs-3373/
Pretty impressive article. I just stumbled upon your site and wanted to say that I have really enjoyed reading your opinions. Any way I’ll be coming back and I hope you post again soon.
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-225-mm-l63/
We recognize the value of your time, which is why we have incorporated a Turbo Mode feature into
Easy Videos Downloader.
My blog :: 365Sport
Very fine blog.
Beneficial Blog! I had been simply just debating that there are plenty of screwy results at this issue you now purely replaced my personal belief. Thank you an excellent write-up.
Экспертная консультация при выборе сплавов помогает клиентам оптимизировать затраты и избежать технологических ошибок.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-35kh-25x1000x1250-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
I like your style!
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-7—bs-2970/truba-magnievaya-mag-7—bs-2970/
Fabulous, what a blog it is! This webpage provides helpful data to
us, keep it up.
Look at my website: https://www.larkinsinvestigations.com/
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-25kh0-8kh14000-mm-mnzhmts30-1-1-gost-10092-2006/
I am lucky that I discovered this website , precisely the right info that I was searching for! .
There is certainly a lot to find out about this topic.
I like all of the points you’ve made.
Also visit my page … seafood store near me open now
Why people still make use of to read news papers when in this technological globe all is presented on net?
Also visit my blog post … 압구정데이트코스
Описание применения металлов в атомной энергетике подчеркивает качество
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-12—bs-2970/polosa-magnievaya-mag-12—bs-2970/
Dünya Kupası haberleri, vay-giris, futbol tutkunlarını heyecanlandıran olaylardır.
Bu turnuva, en prestijli spor organizasyonlarından biri olarak öne çıkmaktadır.
Also visit my web page https://vay-giris.info/
География деятельности компании охватывает всю территорию России, обеспечивая металлом предприятия в удаленных регионах.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-40khn2ma-36x1100x1200-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-8×550-mm-l90-gost-931-90/
Hello to every one, since I am truly keen of reading this weblog’s post to be updated daily.
It includes nice information.
Feel free to surf to my web blog health supplements Canada
Wonderful article! This is the type of info that are supposed to be shared around
the net. Disgrace on Google for not positioning this put up upper!
Come on over and visit my website . Thank you =)
Here is my site :: sexual aid products
Hey just wanted to give you a brief heads up and let you know
a few of the images aren’t loading correctly. I’m not
sure why but I think its a linking issue. I’ve tried it
in two different browsers and both show the same results.
Here is my web blog SEO for small businesses
Корзина на сайте промышленного предприятия — удобный инструмент для формирования заявки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m18330—uns/lenta-magnievaya-m18330—uns/
You actually make it appear so easy together
with your presentation but I find this matter to be really one thing
that I feel I would never understand. It seems too complicated and extremely
vast for me. I’m looking ahead in your next submit, I’ll try to get the cling of it!
Here is my homepage: buy supplements online Canada
We recognize the value of your time, which is why we have incorporated a Turbo Mode feature into Easy Videos Downloader.
My web site :: savefrom.net
Have you ever thought about creating an ebook or guest
authoring on other sites? I have a blog based upon on the same information you discuss and would love to have you
share some stories/information. I know my visitors would appreciate your
work. If you are even remotely interested, feel free to send me an email.
Also visit my blog … topvegas
Más aún, descargar videos de facebook dicho contenido y disfrutarlo de forma gratuita en nuestros teléfonos sin tener que pasar
por complicados procesos o arriesgar la seguridad del mismo.
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-2-1×90-mm-lo90-1-tu-48-21-847-89/
Hi there! Do you know if they make any plugins to help with
Search Engine Optimization? I’m trying to get my blog to
rank for some targeted keywords but I’m not seeing very good gains.
If you know of any please share. Appreciate it!
Review my blog post: online138
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-6khvg-73-gost-5950-2000/
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11311—uns/folga-magnievaya-m11311—uns/
Thank you for another informative blog. The place else
may I get that kind of info written in such an ideal way? I have a undertaking that I’m simply now working on, and I’ve been on the glance out for such information.
My blog post Olive Garden Mneu with Prices 2026
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Bookmarks
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-16kh12kh0-7-mm-7kh9-mm-tverdaia-paika-m1m-gost-32590-2013/
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-1kh1250kh2500-mm-1-4521-en-iso-9444-2/
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m10100—uns/list-magnievyy-m10100—uns/
At this time I am ready to do my breakfast, after having my breakfast coming over
again to read other news.
Here is my web-site – viagra indonesia
Hello colleagues, good piece of writing and pleasant urging commented at
this place, I am really enjoying by these.
Feel free to surf to my homepage гей порно большой
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-4-5×600-mm-l63-gost-931-90/
Stunning story there. What occurred after?
Take care!
Here is my blog post :: kra50.cc
Оперативная логистика и поддержка на всех этапах сделки позволяют минимизировать сроки простоя производственных линий заказчиков.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-09g2s-1520×40-gost-21729-76/
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mc21310—bs-iso-16220/provoloka-magnievaya-iso-mc21310—bs-iso-16220/
My name is Anna, a 35-year-old woman. For years, my relationship was in trouble.
We argued constantly. Eventually, I realized we
wanted different things in life.
One evening, while browsing different games, I discovered an online slot.
The game featured glowing reels, special bonus rounds, and surprising twists.
Every spin felt full of anticipation.
At first, I played with a small balance. The reels showed cherries, stars, and
diamonds. Then something changed. A series of perfect combinations appeared across the screen. The sounds became louder,
the animations brighter, and my heart started racing.
I thought I was imagining it. One bonus round led to another.
Multipliers stacked. The winnings kept growing.
I couldn’t stop smiling. The number on the screen climbed higher and higher.
Then came the moment I will never forget. The reels aligned perfectly.
The screen exploded with celebration effects.
The total reached $100,000.
I was speechless. For several minutes, I simply stared at
the screen. The emotions were overwhelming: pure excitement and gratitude.
That win did not magically solve every problem in my life, but it gave me freedom to make choices.
Around the same time, I met a kind person. More importantly,
I realized that happiness comes from making decisions that
are right for you.
Today, I look back on that night as a turning point. Life moved on.
And while the jackpot was exciting, the biggest reward was finding the courage to create a
life that felt right for me.
my homepage – press release
These are some of the most important issues we’ll face over the next few decades.
I like to spend my free time by scaning various internet recourses. Today I came across your site and I found it is as one of the best free resources available! Well done! Keep on this quality!
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-88-9kh70-mm-m1-gost-r-52948-2008/
Oh my goodness! an amazing article. Great work.
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-09g2d-100x63x7-gost-8509-93/
Использование современных технологий защиты данных пользователей
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-hk32a—mil-m-46062/folga-magnievaya-hk32a—mil-m-46062/
Boa tarde. Ganhei e saquei na roleta online e demora mas paga.
I appreciate, cause I found just what I was looking for. You’ve ended my four day long hunt! God Bless you man. Have a great day. Bye -.
Thank you for the auspicious writeup. It in fact was a amusement account it.
Look advanced to far added agreeable from you!
However, how can we communicate?
my blog … tbs car battery delivery shop
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-2-5×550-mm-ls59-1-gost-931-90/
My brother suggested I might like this blog. He was entirely right.
This post actually made my day. You cann’t imagine just how much time
I had spent for this info! Thanks!
Also visit my website :: bola hit
I wish I could craft such articles as this. Thank you very much.
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/plity/plita-12kh1-82x250x560-gost-19903-74/
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-mgal6—din-1729-part-2/krug-magnievyy-g-mgal6—din-1729-part-2/
I’m extremely impressed along with your writing skills as neatly
as with the layout in your weblog. Is that this a paid subject
matter or did you customize it yourself? Either
way keep up the excellent quality writing, it’s uncommon to look a great weblog like this one today..
Feel free to visit my web blog … колодка тип с производитель
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-17kh6-mm-m3rt-gost-r-52948-2008/
E aí, live scores section here is very useful for in-play betting. Harambee Stars match coming up soon.
Hey there! I could have sworn I’ve been to this website
before but after browsing through some of the post I realized it’s new to me.
Anyhow, I’m definitely happy I found it and I’ll be bookmarking and checking back often!
my web site – digital planner
What you posted was actually very reasonable. But, what about this?
suppose you were to create a killer headline? I am not
suggesting your content is not solid., but what if you added something that
grabbed folk’s attention? I mean Heel Pain – Plantar Fasciitis –
Mr Will Edwards is a little plain. You could glance at Yahoo’s front page and watch
how they create article titles to grab people interested.
You might try adding a video or a related pic or
two to get readers interested about what you’ve written.
In my opinion, it would bring your posts a little livelier.
Stop by my web page … residential commercial
Thanks for sharing your info. I really appreciate your efforts and I am waiting for your next write ups thank you once again.
Here is my homepage career break planning guide
Выбор правильной академии современных техник является ключевым шагом
Feel free to surf to my web site: https://obzor.lt/news/n123503.html
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-10khsnd-32x32x4-gost-8509-93/
Сайт работает стабильно и быстро загружается
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-a6z1—afnor-nf-a65-717/pokovka-magnievaya-g-a6z1—afnor-nf-a65-717/
Asking questions are really fastidious thing if you are not
understanding something fully, except this post provides nice understanding even.
Also visit my web-site; Sang Juara 2026
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-1925-4x18x37-gost-13621-90/
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Stɑtes
254-275-5536
Stylish
My name is Anna, a 35-year-old woman. For years, my marriage was falling apart.
We argued constantly. Eventually, I accepted that our
marriage had reached its end.
One evening, while browsing different games, I discovered an online slot.
The game featured glowing reels, reward multipliers, and
constant suspense. Every spin felt unpredictable.
At first, I played for fun. The reels showed cherries, stars, and diamonds.
Then something changed. A series of lucky hits appeared across the screen. The sounds became louder, the animations brighter, and
my heart started racing.
I thought I was imagining it. One bonus round led to another.
Multipliers stacked. The winnings kept growing. My hands were
shaking. The number on the screen climbed higher and higher.
Then came the moment I will never forget. The reels aligned perfectly.
The screen exploded with celebration effects. The
total reached one hundred thousand dollars.
I sat in complete shock. For several minutes, I simply stared at
the screen. The emotions were overwhelming: joy mixed with disbelief.
That win did not magically solve every problem in my life, but it gave me
freedom to make choices. Around the same time, I met someone new.
More importantly, I realized that happiness comes from healthy relationships.
Today, I look back on that night as a turning point.
The future opened new doors. And while the jackpot was exciting, the biggest reward was finding the courage to create a life that felt right for
me.
Look at my web site – press release
As the admin of this web site is working, no hesitation very soon it will be renowned,
due to its feature contents.
Look into my website – situs slot
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mc21230/truba-magnievaya-en-mc21230/
Excellent items from you, man. I have take into account your stuff previous to and
you’re just too fantastic. I really like what you’ve bought right here, really like what you’re stating and the way in which you
are saying it. You are making it entertaining and you still take care of to stay it sensible.
I can not wait to read much more from you. That is actually a great website.
Also visit my webpage … все новости [https://pohudelka.com.ua/]
Wow! After all I got a web site from where I be capable of truly take valuable
information regarding my study and knowledge.
Feel free to visit my website :: ราชภัฏ No1
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-25-mm-m2r-gost-r-52948-2008/
Наличие никелевых сплавов гарантирует высокую коррозийную стойкость оборудования, создаваемого заказчиками.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-5khnm-4-2-gost-7417-75/
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku35kh1mmm1tgost-r-52922-2008/
I constantly emailed this website post page to all my contacts, because if like to read it after that my links will too.
Feel free to surf to my web page – click
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-s-chechevichnym-rifleniem-25kh600kh800-mm-08ps-gost-8568-77/
Стартуйте в мире ставок с Мелбет понятное меню.
Тысячи автоматов и live-крупье — уникальные
фриспины каждый день.
(орфография по запросу: «зекало»)
Единственное надёжное зеркало
мелбет — без вирусов и рекламы.
Here is my web page :: melbet casino официальный вход
Pretty great post. I just stumbled upon your weblog and wanted to
say that I’ve truly enjoyed surfing around your blog posts.
In any case I will be subscribing in your rss feed and
I am hoping you write once more very soon!
Feel free to surf to my website arenaqq
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-19kh3kh14000-mm-mnzhmts10-1-1-gost-10092-2006/
บทความนี้ ให้ข้อมูลดี ค่ะ
ดิฉัน เพิ่งเจอข้อมูลเกี่ยวกับ เรื่องที่เกี่ยวข้อง
ที่คุณสามารถดูได้ที่ Maribel
น่าจะถูกใจใครหลายคน
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ เนื้อหาดีๆ
นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
Here is my blog post … mvp1688 (Maribel)
Hi there very nice blog!! Guy .. Beautiful .. Amazing ..
I’ll bookmark your web site and take the feeds additionally?
I’m satisfied to find numerous useful info right here in the
put up, we’d like develop extra strategies
in this regard, thanks for sharing. . . .
. .
Here is my web-site; Explore Private AI Video Generation
Have you ever thought about publishing an ebook or guest authoring
on other blogs? I have a blog based upon on the same subjects you discuss and would love to have you share some
stories/information. I know my visitors would enjoy your work.
If you are even remotely interested, feel free to shoot me an e-mail.
My web site; visabet88
Наличие на складе редких металлов, таких как цирконий, выделяет компанию на фоне конкурентов, торгующих только массовым прокатом.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-60kh60kh6-mm-41cralmo7-en-10056-2/
Возможность заказать листы и полосы нестандартных размеров
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az31a—astm-b275/krug-magnievyy-az31a—astm-b275/
p2p plattformen
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku25kh0-9mmm0bgost-32590-2013/
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-am60b—astm-b93/list-magnievyy-am60b—astm-b93/
Very descriptive article, I loved that a lot. Will there be a part 2?
Look into my blog post :: slot gacor
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/magnievyi-krug/krug-magnievyi-140-mm-ma1-gost-18351-73/
ООО «РМС» предлагает широкий спектр цветного проката, включая медь, латунь, бронзу и дюралюминий.
https://rms-ekb.ru/catalog/aliuminievyi-profil-pas-dlia-kvadratnoi-truby/
Hey There. I discovered your weblog the use of msn. That what is v.yupoo.com a very neatly written article.
I’ll be sure to bookmark it and return to learn more of your helpful info.
Thanks for the post. I’ll definitely comeback.
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-28kh23kh0-9-mm-18-4kh20-4-mm-miagkaia-paika-m1-gost-r-52922-2008/
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-100kh100kh10-mm-30mnb4-din-1029/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Modernkitchen
Hi to every body, it’s my first pay a quick visit of
this website; this blog contains amazing and really good
data in favor of readers.
Here is my webpage; áreaexterna
It’s very simple to find out any matter on net as
compared to textbooks, as I found this post at this web page.
My web blog; slon8 cc
Hey I know this is off topic but I was wondering if you knew of
any widgets I could add to my blog that automatically tweet my newest twitter
updates. I’ve been looking for a plug-in like this for quite some time and was hoping
maybe you would have some experience with something like this.
Please let me know if you run into anything.
I truly enjoy reading your blog and I look forward to your new
updates.
Feel free to visit my web site; météo paris aujourd’hui
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-av-2x34x33-gost-13621-90/
Логичное деление на вольфрамовый, молибденовый и титановый прокат
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ma5c1/truba-magnievaya-ma5c1/
ООО «РМС» предлагает широкий спектр цветного проката, включая медь, латунь, бронзу и дюралюминий.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-65kh50kh5-mm-x1nicrmocun25-20-7-en-10088-3/
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m17-15-7kh1-mm-lsdch-din-471/
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/list/list-3kh2mnf-2-2x1000x1000-gost-19903-2006/
Asking questions are truly good thing if you are not understanding something
fully, however this post provides nice understanding even.
my webpage; 8x-bet.sa.com lừa đảo công an truy nã cấm người chơi tham gia
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-6k/list-kobaltovyy-stellite-6k/
ООО «РМС» обеспечивает поставки специализированных сварочных материалов для сложных условий эксплуатации.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-7khg2vmf-38-93-gost-7417-75/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-ak6-5x40x150-gost-13621-90/
I got this website from my buddy who told me on the topic of this web page and now this time I
am browsing this website and reading very informative articles at this time.
Feel free to visit my web-site – https://www.univers-habitat.eu/
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735,United Ѕtates
254-275-5536
Highend
Have you ever considered about adding a little bit more than just
your articles? I mean, what you say is important and all.
But just imagine if you added some great graphics or video clips to give your
posts more, “pop”! Your content is excellent but with pics and videos,
this blog could certainly be one of the most beneficial in its field.
Excellent blog!
Here is my homepage; collection of computers for disposal
Экспертная консультация при выборе сплавов помогает клиентам оптимизировать затраты и избежать технологических ошибок.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-20kh1400-mm-acroni-4550-en-iso-18286/
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-115kh2-5-mm-lk2-gost-13943-86/
Have you ever considered about adding a little bit more than just your articles?
I mean, what you say is valuable and everything. But just imagine if you added some great graphics or video clips to give your posts more, “pop”!
Your content is excellent but with images and video clips,
this site could undeniably be one of the very best in its field.
Good blog!
Also visit my webpage … Swamp Donkey
Great write-up, I am a big believer in placing comments on sites to inform the blog writers know that they’ve added something advantageous to the world wide web!
Продукция находит применение в производстве электротехники благодаря наличию специализированной электротехнической стали.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-180kh180kh16-mm-st52-3n-din-1029/
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-vad1-4x50x70-gost-13621-90/
I do not even know how I ended up here, but I thought this post was great.
I don’t know who you are but definitely you are going to a famous blogger
if you aren’t already ;) Cheers!
My blog – Online Cannabis Shop Canada
Woah! I’m really digging the template/theme of this blog.
It’s simple, yet effective. A lot of times it’s very hard to
get that “perfect balance” between user friendliness and appearance.
I must say you have done a very good job with this.
In addition, the blog loads super fast for me on Internet explorer.
Superb Blog!
my web page: магазин айфонов в твери
I quite like reading a post that can make people think.
Also, thank you for allowing for me to comment!
My website … 해운대 다이어트 한의원
Hello, i think that i saw you visited my blog thus i came to “return the favor”.I’m trying to find things to improve my
site!I suppose its ok to use a few of your ideas!!
Look into my web site mty bets
References:
No deposit bonus binary options https://yiyola.com/@joycelyntimmer?page=about
География деятельности компании охватывает всю территорию России, обеспечивая металлом предприятия в удаленных регионах.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-06kh1250kh3000-mm-1-4301-en-iso-9444-2/
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-40kh1-5kh8000-mm-mnzhmts30-1-1-gost-10092-2006/
It’s actually a great and useful piece of information. I’m happy that
you simply shared this useful information with us. Please stay
us up to date like this. Thank you for sharing.
Have a look at my web page … Online Cannabis Dispensary Canada
Hi to all, how is all, I think every one is getting more
from this site, and your views are pleasant in favor of new
users.
Here is my blog; genjot138
We absolutely love your blog and find nearly all of your post’s to be exactly I’m looking for.
can you offer guest writers to write content to suit your needs?
I wouldn’t mind writing a post or elaborating on a lot of the subjects you write related to here.
Again, awesome web log!
Here is my website – West Coast Bud Canada
We have been helping Canadians Get a Loan Against Their Vehicle for Repairs
Since March 2009 and are among the very few Completely Online Lenders In Canada.
borrow money with my car for repair us you can obtain a Car Repair
Loan Online from anywhere in Canada as long as you have a Fully Paid Off Vehicle
that is 8 Years old or newer. We look forward
to meeting all your financial needs.
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-atd-14/truba-kobaltovaya-atd-14/
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-khn65mvu-273×28-gost-9941-81/
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-1920-1-5x18x13-gost-13621-90/
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-42-3742—csnstn-423742/truba-vismutovaya-42-3742—csnstn-423742/
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-200kh100kh12-mm-50crv4-uni-6762/
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-23kh0-8kh1000-mm-mnzhmts30-1-1-gost-10092-2006/
This piece of writing will assist the internet users for
setting up new blog or even a weblog from start to end.
Also visit my web-site sex
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vt-15-1/list-volframovyy-vt-15/
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-05kh12n6d2mfsgt-530-gost-5950-2000/
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/ugolok-aliuminievyi/ugolok-aliuminievyi-60x30x2x3000-ad31t1/
I think that is among the such a lot vital information for me.
And i am happy studying your article. However want to observation on some basic things,
The web site style is ideal, the articles is in reality excellent : D.
Just right process, cheers
Also visit my homepage – ufabet289
Cabinet IQ
8305 State Hwy 71#110, Austin,
TX 78735, United Ѕtates
254-275-5536
CADmodel
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-s255-70×70-gost-19772-93/
References:
Roulette payouts https://zm.aosenhw.com/@wernerd1125361
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-30kh2-5kh10000-mm-mnzhmts10-1-1-gost-10092-2006/
I’m not that much of a internet reader to be honest but your blogs really
nice, keep it up! I’ll go ahead and bookmark your site to
come back down the road. All the best
Stop by my web blog: dominoqq
It’s remarkable to pay a quick visit this website and reading the views of all mates about
this article, while I am also keen of getting experience.
My site – mellstroy casino
Cabinet IQ
8305 Տtate Hwy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Kitchendreams [Linda]
I all the time emailed this blog post page to all my associates, since if like to read it then my links will
too.
Look at my web-site … B6T file support
Описание применения металлов в атомной энергетике подчеркивает качество
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-1/truba-volfram/
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku27-4kh0-9mmm2tgost-32590-2013/
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-sn46pb46bi08a—iec-61190-1-3/krug-vismutovyy-sn46pb46bi08a—iec-61190-1-3/
What i do not understood is in fact how you’re not actually much more well-favored than you may be now.
You’re very intelligent. You recognize therefore significantly in relation to this matter, produced me in my opinion consider it from numerous
various angles. Its like men and women don’t seem to be fascinated
unless it is something to do with Woman gaga! Your own stuffs excellent.
At all times deal with it up!
Also visit my homepage :: 비아그라 구매
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-17kh2-5kh3000-mm-mnzhmts10-1-1-gost-10092-2006/
Профессиональная переподготовка по детской психологии: фундамент успешной карьеры в работе с детьми
My website https://supermams.ru/chto-na-samom-dele-izuchayut-na-nlp-i-zachem-eto-psixologu-konsultantu.htm
Cabinet IQ
8305 Տtate Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Specialist
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-210kh1600-mm-x6crni18-10-en-iso-18286/
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-h43bi57a—jis-z-3282/lenta-vismutovaya-h43bi57a—jis-z-3282/
Как отыскать лучшие курсы по разным профессиям
Also visit my web page: https://www.politnavigator.net/nutriciologiya-putevoditel-po-zdorovyu-v-ehpokhu-informacionnogo-buma.html
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku40-5kh1-8mmm1rmgost-32590-2013/
Cabinet IQ
8305 Ⴝtate Hwy 71 #110, Austin,
TX 78735, Unifed Ѕtates
254-275-5536
Bookmarks
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-cac906c—jis-h-5121-2016/pokovka-vismutovaya-cac906c—jis-h-5121-2016/
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/medno-nikelevaia-provoloka/provoloka-medno-nikelevaia-0-5-mm-mn10-tu-45-026-09/
Wow! Finally I got a webpage from where I be able to actually take useful facts regarding my
study and knowledge.
Also visit my web page :: 비아그라 구매
Поставка продукции возможна не только в промышленных, но и в малых лабораторных объемах для исследовательских целей.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-20khsnm-14x1400x1250-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
It’s nearly impossible to find knowledgeable people in this particular subject, however, you sound like you know what you’re talking about!
Thanks
Look at my web site: bokep indo
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku10kh0-6mmm3gost-32590-2013/
I really like what you guys tend to be up too. This sort of clever work and coverage!
Keep up the awesome works guys I’ve incorporated you guys to our blogroll.
Feel free to surf to my homepage – private server growth strategy
Very soon this web site will be famous among all blogging visitors, due to it’s nice content
my blog post – vs-bet.in.net lừa đảo công an truy nã cấm người chơi tham gia
I do not even know how I ended up here, but I thought this
post was great. I don’t know who you are but definitely you are going to a famous blogger if you are not already ;) Cheers!
Here is my blog post MALWARE
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-12kh18n10t-168×25-gost-21729-76/
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/magnievyi-krug/krug-magnievyi-10-mm-ma2-1-gost-18351-73/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
website
Наличие циркония свидетельствует о работе с высокотехнологичными заказами
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-b-505-c-89320—astm-b505/krug-vismutovyy-b-505-c-89320—astm-b505/
Geweldig artikel! Ik was al een tijdje aan het nadenken over kozijnen vervangen en dit was precies wat ik zocht
— ik ben in gesprek gegaan met een kunststof kozijnen vervangen specialist en de kozijnen vervangen offerte was
veel redelijker dan verwacht, dus ik overweeg
serieus om kozijne vervangen met nieuwe kunststof energie
efficiënte kozijnen, Porter, en ik zou iedereen aanraden om contact te
zoeken met een kozijnen vervangen specialist als
je twijfelt over kozijne vervangen!
Attractive component of content. I just stumbled upon your blog
and in accession capital to assert that I get in fact loved account your weblog posts.
Anyway I’ll be subscribing to your feeds and even I fulfillment you get right
of entry to constantly quickly.
Review my site; web page
Hello there! I simply wish to give you a huge thumbs up for the excellent info
you have here on this post. I am coming back to your blog for more soon.
my blog :: Techxa auto airmatic specialist
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku106kh3-5mmm3mgost-32590-2013/
Easily, the post is really the greatest on this laudable topic. I concur with your conclusions and will thirstily look forward to your future updates. Saying thank will not just be sufficient, for the wonderful c lucidity in your writing. I will instantly grab your rss feed to stay privy of any updates. Solid work and much success in your business enterprise!
My coder is trying to convince me to move to .net from PHP. I have always disliked the idea because of the expenses. But he’s tryiong none the less. I’ve been using WordPress on numerous websites for about a year and am nervous about switching to another platform. I have heard great things about blogengine.net. Is there a way I can import all my wordpress posts into it? Any help would be really appreciated!
Информация о доставке по всей РФ делает компанию универсальным поставщиком
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-142—en-iso-9453/lenta-vismutovaya-142—en-iso-9453/
География деятельности компании охватывает всю территорию России, обеспечивая металлом предприятия в удаленных регионах.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-11kh4v2mf3s2-15-2-gost-7417-75/
This contained some excellent tips and tools. Great blog publication.
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-kapilliarnaia-trubka/latunnaia-kapilliarnaia-trubka-1-8kh0-35kh10000-mm-l70-gost-2624-2016/
Sadəcə demək istəyirəm ki, bu saytı tapdığıma şadam.
http://babycloset.es/jersey-flores-ido-clothes-3-baby-closet-moda-infantil/
Very often I go to see this blog. It very much is pleasant to me. Thanks the author
Like the way you’ve outlined things. Easy to follow. Not cluttered.
I want to to thank you for this wonderful read!! I certainly enjoyed every bit of it.
I have you bookmarked to look at new stuff you post…
Here is my homepage: 비아그라 구매
Thankfulness to my father who told me on the topic of this blog, this website is truly remarkable.
Here is my web page 비아그라 구매
If you are going for finest contents like I
do, only pay a quick visit this site every day as it offers feature contents, thanks
Also visit my web site – 123FAZ
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-low-aluminum—stratcor-1/list-vanadievyy-low-aluminum—stratcor-1/
Attractive component of content. I just stumbled upon your site and in accession capital to assert that I get
actually loved account your blog posts. Any way I’ll be subscribing in your augment and even I
achievement you get right of entry to constantly fast.
Visit my webpage :: 24h locksmith
It’s perfect time to make some plans for the longer term and it is
time to be happy. I’ve learn this post and if I may just I desire to recommend you some fascinating things or advice.
Maybe you could write next articles referring to this article.
I wish to read even more things approximately it!
Feel free to surf to my web blog – Bassbet bonuses
I know this site presents quality depending articles and other
data, is there any other website which presents these information in quality?
Also visit my page: 123FAZ
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku14-7kh1-2mmcu-dhpgost-32590-2013/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Bespokedesigns
Информация о доставке по всей РФ делает компанию универсальным поставщиком
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt8-1—ost-1-90013-81-1/lenta-titanovaya-vt8-1—ost-1-90013-81-1/
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/list/list-kh12f1-2x2000x2000-gost-19903-74/
I go to see day-to-day a few web sites and information sites to read posts, however
this weblog gives quality based content.
Also visit my blog; แทงบอล ออนไลน์
Awesome post.
Here is my site: 123FAZ
It’s a pity you don’t have a donate button! I’d certainly donate to this
outstanding blog! I guess for now i’ll settle for bookmarking and adding your RSS feed to my Google account.
I look forward to fresh updates and will talk about this website with my Facebook group.
Chat soon!
Also visit my web site; crowdfunding imobiliário
This is really interesting, You are a very skilled blogger.
I’ve joined your rss feed and look forward to seeking more of your great post.
Also, I have shared your site in my social networks!
Here is my web blog :: Age calculator
Hello, the whole thing is going fine here and ofcourse every one is sharing information, that’s really good, keep up writing.
Feel free to surf to my webpage; bassbet app
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-78kh2-5-mm-los-gost-13942-86/
Фольга из редких металлов часто требуется для высокотехнологичных лабораторий
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt1-2—gost-19807-91-1/prutok-titanovyy-vt1-2—gost-19807-91-1/
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r18f2-135-gost-1133-71/
Hello there! This is kind of off topic but I need some guidance from an established blog.
Is it tough to set up your own blog? I’m not
very techincal but I can figure things out pretty fast.
I’m thinking about making my own but I’m not
sure where to start. Do you have any points or suggestions?
With thanks
Also visit my webpage – payment integration services
This is really interesting, You’re a very skilled blogger. I have joined your feed and look forward to seeking more of your great post. Also, I’ve shared your web site in my social networks!
hello there and thank you for your info – I have
certainly picked up something new from right here. I did however expertise several technical issues
using this website, since I experienced
to reload the site many times previous to I could get it to load correctly.
I had been wondering if your web hosting is OK?
Not that I’m complaining, but sluggish loading instances times
will often affect your placement in google and could damage your high-quality score if ads and marketing with Adwords.
Well I’m adding this RSS to my e-mail and could look out for a lot more of your respective exciting content.
Make sure you update this again very soon.
Here is my web page Аренда авто в Краснодаре без залога
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku22kh0-9mmm3rmgost-32590-2013/
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-sp15—gost-27265-87-1/pokovka-titanovaya-sp15—gost-27265-87-1/
I every time emailed this blog post page to all my contacts,
since if like to read it then my contacts will too.
My web blog … 비아그라 구매
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-06khn28mdt-0-6x1250x1600-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
You could certainly see your skills within the work you
write. The sector hopes for more passionate writers such as you who are not afraid to mention how they believe.
At all times go after your heart.
Also visit my web-site :: togel 4d terpercaya
Heya i’m for the primary time here. I came across this board and I in finding It really helpful & it
helped me out a lot. I am hoping to offer one thing back and help others like you aided me.
my homepage – Onewave home solar water heater
I was able to find good info from your blog articles.
Feel free to surf to my website 비아그라 구매
Cabinet IQ
8305 Stɑte Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Kitchenupdate; fo3tp.stick.ws,
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-42kh1-7-mm-lts40mts3a-gost-13942-86/
Наличие редких позиций, например, изделий из гафния и ванадия
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-at3—gost-19807-91-1/poroshok-titanovyy-at3—gost-19807-91-1/
Thanks for the good writeup. It in fact was once a enjoyment account it.
Glance advanced to more delivered agreeable from you!
By the way, how could we be in contact?
Here is my page; Księgowy Londyn
ООО «РМС» предлагает широкий спектр цветного проката, включая медь, латунь, бронзу и дюралюминий.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-09g2s-70x70x5-gost-8509-93/
Howdy would you mind sharing which blog platform you’re working with?
I’m planning to start my own blog in the near future but I’m having a tough time deciding between BlogEngine/Wordpress/B2evolution and
Drupal. The reason I ask is because your design and style seems different
then most blogs and I’m looking for something completely unique.
P.S My apologies for getting off-topic but I had to ask!
Feel free to surf to my web-site; https://earth-chronicles.ru/news/2022-08-10-164485
Wow, fantastic blog format! How lengthy have you been blogging for?
you made blogging look easy. The overall look of your web site is great, let alone the content!
my website: best store to buy pants
Wow, superb blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your website is magnificent, let alone the content!
Also visit my web-site – phising
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku133kh4-5mmm1egost-r-52922-2008/
Профессиональный подход к описанию каждого вида металла
https://redmetsplav.ru/store/tantal-i-ego-splavy/tantal-ta-nb30-1/prutok-tantalovyy-ta-nb30/
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-10kh18n10t-1-8x1800x1100-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Great post! I’ve been searching for a trustworthy glazenwasser in my neighborhood
for ages and this gives great insight – my
company desperately needs a quality glazenwasser bedrijf because our windows are absolutely filthy and I hate trying to clean them myself, plus I was told
that an skilled ramenwasser makes them sparkle than amateur exterior cleaning professionals – Steven,
– do you have any advice for finding a goedkope glazenwasser that still delivers quality work especially for business glazenwasser
service?
Great website you have here but I was wondering if you knew of any forums that cover the same topics talked about here?
I’d really love to be a part of community where I can get comments from other experienced people that share the same interest.
If you have any suggestions, please let me know. Cheers!
Here is my web-site :: казино в телеграмме
Whoa! This blog looks just like my old one! It’s on a completely different subject but it has pretty much the same layout
and design. Wonderful choice of colors!
Here is my webpage – Bassbet login
We recognize the value of your time, which is why we have
incorporated a Turbo Mode feature into Easy Videos Downloader.
Here is my webpage this page
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nbpl-3-1/poroshok-niobievyy-nbpl-3/
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-65kh2-5-mm-lts40s-gost-13942-86/
I never imagined that my relationship would collapse.
For years I built my career, thinking that everything was fine.
Then out of nowhere I discovered that my wife had been seeing another man. What hurt the most was that he was a rich businessman. I was devastated.
The breakup hit me hard. I spent countless nights awake.
At first I blamed myself. I worried about starting over.
But eventually I learned a valuable lesson: my future depended on me.
Rather than staying bitter, I became focused on improving my finances.
I started studying investing. Every day I learned about risk management, crypto markets, and wealth preservation.
Eventually I found Paybis and it changed my routine. What impressed me first was the straightforward interface.
Buying crypto became surprisingly efficient.
Now Paybis is part of my routine for moving between crypto and fiat.
Everything is easy to follow. I can monitor my transfers while maintaining a
clear overview of my finances.
The fintech side fascinated me. Understanding digital payments
gave me a new perspective on money. I studied market cycles.
Over time I became more disciplined with my decisions.
The biggest surprise came later. As my confidence returned,
I realized that the problem was never financial. The real issue was attitude.
No amount of money can fix that.
Things changed when I least expected it. I found a wonderful woman.
She helped me believe in the future again. What mattered most she was positive and caring.
Today I feel stronger than ever. The difficult chapter is over.
I rebuilt my finances, learned valuable lessons, and found happiness.
When I think about the past, I no longer feel anger. I value what I learned.
The setback became an opportunity. And every time I complete a transaction on Paybis, I remember how far I’ve come.
The emotions are incredible—the realization that life can improve
dramatically when you refuse to quit.
My homepage: site
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-40khgnm-34x1900x1550-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Cabinet IQ
8305 Statee Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
DIYguides (atavi.com)
Super stuk over kozijne vervangen! Ik zoek al een poosje op zoek naar een ervaren kozijnen renovatie (https://thrivefactorwellness.com/kozijnen-vervangen-wat-u-moet-weten-over-veiligheid-en-kwaliteit-2/) vervangen specialist en hier heb ik veel aan gehad, aangezien ik had
geen idee wat een normale offerte voor kozijne vervangen zou herkennen totdat ik dit las.
De tips over het vervangen van houten kozijnen zijn heel praktisch
en ik ben van plan om een kozijnen vervangen offerte op te vragen voor mijn woning!
Hi there, I desire to subscribe for this web site to get latest updates, so where can i do it please help.
Feel free to surf to my web-site :: займ лабубу
Great post. I used to be checking constantly this blog and I am impressed!
Very helpful information particularly the last part
:) I deal with such information a lot. I used to be looking for this certain information for
a long time. Thanks and good luck.
Look into my homepage … human history
Четкая структура меню позволяет быстро найти нужный металл
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-4e-1/poroshok-niobievyy-4e/
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-35kh29kh1-mm-23kh25-mm-miagkaia-paika-cu-dhp-gost-r-52922-2008/
ООО «РМС» обеспечивает поставки специализированных сварочных материалов для сложных условий эксплуатации.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-st20-60x60x6-gost-19771-93/
Way cool! Some very valid points! I appreciate you penning this post plus the rest of the website is also really good.
Feel free to visit my web blog; unblocked games
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mrn-3/folga-molibdenovaya-mrn-1/
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m44-40-5kh1-75-mm-lts40sd-din-471/
I’m gone to say to my little brother, that
he should also visit this website on regular basis to take updated from
most up-to-date news update.
Also visit my web-site: link alternatif visabet88
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-u12-155-gost-1133-71/
Very nice post. I just stumbled upon your blog and wanted to say that I’ve really enjoyed browsing your blog posts. In any case I’ll be subscribing to your rss feed and I hope you write again soon!
This will be helpful for my family.
Beneficial Blog! I had been simply just debating that there are plenty of screwy results at this issue you now purely replaced my personal belief. Thank you an excellent write-up.
I got this website from my friend who informed me concerning this web page and now
this time I am visiting this website and reading very informative posts at
this place.
Feel free to surf to my website; KDL16L
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-fmo60-1/polosa-molibdenovaya-fmo60/
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-106kh92kh2-1-mm-47-5kh51-5-mm-miagkaia-paika-m3m-gost-r-52922-2008/
Heya i am for the first time here. I came across this
board and I find It really useful & it helped me
out a lot. I hope to give something back
and help others like you helped me.
My web site: 1xbet agent
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-09g2s-90x90x12-gost-8509-93/
Can I just say what a relief to seek out someone who actually knows what theyre speaking about on the internet. You positively know find out how to bring a problem to mild and make it important. Extra individuals have to read this and perceive this side of the story. I cant believe youre not more in style because you positively have the gift.
Great blog here! Also your website loads up fast!
What host are you using? Can I get your affiliate
link to your host? I wish my website loaded up as fast as yours lol
Here is my homepage 비아그라 구매
Please let us know when you plan to publish your book!
Way cool! Some extremely valid points! I appreciate you penning this write-up and also the rest of the site is really good.
My homepage; quitar moho barcelona
Hello there I am so delighted I found your weblog, I really found you by mistake, while I was searching on Google for something else, Anyhow I am here now and would just like to say cheers for a remarkable post and a all round exciting blog (I also love the theme/design), I don’t have time to browse it all at the moment but I have book-marked it and also included your RSS feeds, so when I have time I will be back to read a lot more, Please do keep up the superb work.
Наличие редких позиций, например, изделий из гафния и ванадия
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-ze41—csa-hg-9/poroshok-magnievyy-ze41—csa-hg-9/
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m39-35-8kh1-75-mm-lts40mts3a-din-471/
I love reading a post that can make men and women think.
Also, thanks for permitting me to comment!
Feel free to visit my web page – th39
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/list/list-4kh3vmf-1x1000x1000-gost-19903-74/
First off I want to say wonderful blog! I had a quick question that I’d like to ask if you do not mind.
I was interested to find out how you center yourself and
clear your mind before writing. I have had a difficult time clearing my mind in getting my ideas out there.
I do enjoy writing however it just seems like
the first 10 to 15 minutes are generally lost simply just trying to figure out how to
begin. Any ideas or tips? Cheers!
Check out my web blog … บ้านสวนทรัพย์โอภาส
goGLOW
6850 N Rochester Ꭱd, Rochester Hills,
МI 48306, United Stateѕ
248 971-1831
Bookmarks
최근 한국에 정식 오픈한 투세븐빗은 자체 개발한 3세대 거래 시스템을 탑재하여 주목받고 있습니다. 특히 지정가 0.01%, 시장가 0.02%라는 업계 최저 수준의 수수료를 제공합니다.
Woh I enjoy your content , saved to bookmarks!
Cabionet IQ
8305 Stɑte Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Designconsult
I absolutely adore your site! You aggressive me as able-bodied as all the others actuality and your broiled PS is absolutely great!
Hiya, I am really glad I have found this information. Nowadays bloggers publish only about gossip and net stuff and this is actually frustrating.
Its like you read my mind! You appear to know
so much about this, like you wrote the book in it or something.
I think that you can do with some pics to drive the message home a little bit, but instead of that, this is wonderful blog.
An excellent read. I’ll certainly be back.
Here is my web site :: Таможенная база
Профессиональный подход к описанию каждого вида металла
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-r60706—uns/folga-magnievaya-r60706—uns/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-21kh18kh0-9-mm-8kh10-mm-tverdaia-paika-m3rm-gost-r-52922-2008/
We’re developing some community services to respond to this, and your blog is helpful.
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-130kh130kh12-mm-x2crnimocuwn25-7-15-en-10088-3/
We recognize the value of your time, which is why we have incorporated a Turbo Mode feature into Easy Videos Downloader.
Review my web-site; Accumulator tips
Watching from Lagos, Nigeria. Worldie!
hello!,I really like your writing very a lot! proportion we keep up a correspondence more about your article on AOL?
I need an expert on this space to unravel my problem.
May be that’s you! Taking a look forward to look you.
my homepage; Riobet Casino
Howdy, a helpful article for sure. Thank you.
I do believe all the ideas you’ve presented to
your post. They are very convincing and can certainly work.
Still, the posts are too short for novices.
May you please prolong them a bit from subsequent
time? Thanks for the post.
Also visit my website … visabet88 bonus
I never imagined that my relationship would collapse. Over many
years I focused on providing for my family, thinking that
loyalty and trust were enough. Then to my shock I discovered that my wife was involved with
someone else. What hurt the most was that he was a rich businessman. I was devastated.
The divorce process was brutal. Many evenings felt endless.
Initially I questioned everything. I worried about my finances.
But eventually I realized something important:
I could only control my own decisions.
Rather than staying bitter, I became focused on improving
my finances. I learned about digital assets. Every day I learned about asset allocation, crypto markets, and personal finance.
One of the most useful tools I discovered was Paybis.
What stood out immediately was the straightforward interface.
Handling transactions became surprisingly efficient.
Now Paybis is part of my routine for moving between crypto and fiat.
The process feels intuitive. I can monitor my transfers while maintaining control over my assets.
I became passionate about modern financial systems. Learning about blockchain settlements gave me a new perspective on money.
I followed industry developments. Over time I became more disciplined with my decisions.
The biggest surprise came later. As my confidence returned, I realized
that money had never been the real issue. The real problem was respect.
Financial success cannot replace character.
Things changed when I least expected it. A new relationship entered my life.
She brought fresh energy into my life. More importantly she was positive and caring.
These days I wake up grateful. That period of my life is finished.
I regained confidence, improved my future, and found peace of mind.
In hindsight, I don’t hold onto bitterness. I respect the journey.
The setback became an opportunity. Each step forward proves that resilience pays off.
The feeling is amazing—a mix of happiness and accomplishment.
Also visit my homepage :: URL
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-zn6zr/list-magnievyy-mg-zn6zr/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m32-29-6kh1-5-mm-lk80-din-471/
Наличие прецизионных сплавов в ассортименте подтверждает работу компании с высокоточными и наукоемкими материалами.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-14g2-3-9x1500x1700-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
I visited many web sites but the audio quality residential plots for sale in pallikaranai chennai audio
songs current at this site is genuinely wonderful.
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgal6zn—din-1729-part-2/truba-magnievaya-mgal6zn—din-1729-part-2/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-42kh36kh1-1-mm-10kh12-mm-tverdaia-paika-m2t-gost-r-52922-2008/
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-250kh250kh35-mm-46cr2-en-10056-1/
I never thought that my marriage would end this way.
For years I focused on providing for my family, assuming that everything was fine.
Then one day I discovered that she had a secret relationship.
What hurt the most was that he had a lot of money.
I felt betrayed.
The breakup hit me hard. There were sleepless nights.
At first I blamed myself. I worried about starting over.
But eventually I realized something important: I could only control my own decisions.
Instead of living in the past, I became obsessed with
financial education. I learned about digital assets.
Hour after hour I learned about asset allocation, digital currencies, and financial planning.
Paybis became a key part of my financial journey.
The first thing I noticed was the straightforward interface.
Buying crypto became surprisingly efficient.
I regularly use Paybis for crypto-to-fiat transactions.
The transaction flow is smooth. I can review activity while maintaining better financial organization.
I became passionate about modern financial systems. Understanding digital payments gave me greater confidence.
I followed industry developments. Over time I became more strategic with
my decisions.
Then something unexpected happened. As my finances improved, I
realized that the problem was never financial. The real problem was respect.
Money alone does not create a healthy relationship.
Sometimes life surprises you. I eventually met someone new.
She helped me believe in the future again. What mattered most she
was encouraging and respectful.
Now I am happier than I have been in years. The difficult
chapter is over. I rebuilt my finances, improved my future, and found happiness.
Looking back, I don’t hold onto bitterness. I simply appreciate the lessons.
The worst moment became a turning point. My financial journey reminds me how much I have grown.
The feeling is amazing—a mix of happiness and accomplishment.
Feel free to surf to my blog post press release
It’s appropriate time to make some plans for the future and it is time to be
happy. I have read this publish and if I may just I wish to
suggest you some attention-grabbing issues or tips.
Maybe you can write next articles referring to this article.
I desire to learn more issues approximately it!
Feel free to surf to my page – indonesia video bokep
Ini juga membantu Anda untuk tetap terorganisir dan mengumpulkan ide-ide Anda dalam satu
tempat.
Here is my website – Clique Aqui
Quality articles is the crucial to interest the viewers to pay a quick visit the web page, that’s
what this web site is providing.
my web page :: 13 mm bariyerli bondex sünger
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mdc1b—jis-h-5303/truba-magnievaya-mdc1b—jis-h-5303/
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m62-57-8kh2-mm-lsd-din-471/
Важным преимуществом является возможность изготовления деталей и изделий по индивидуальным чертежам заказчика.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-12kh18n10t-2-5x1900x1300-gost-19903-2006-gladkii-chernyi-goriachekatanyi/
For the reason that the admin of this website is working, no
doubt very quickly it will be renowned, due to its quality contents.
my blog https://mettler-design.ch/
I do accept as true with all of the ideas you’ve offered
on your post. They are really convincing and can certainly work.
Nonetheless, the posts are too short for starters.
May just you please lengthen them a bit from next time?
Thank you for the post.
Also visit my page – Psilocybin Mushrooms Canada
I have been browsing Online Mushroom Dispensary Canada more than three
hours these days, but I by no means discovered any interesting
article like yours. It’s beautiful price sufficient for me.
In my opinion, if all web owners and bloggers made just right content as you probably did,
the internet might be much more useful than ever before.
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mb1—jis-h-4203/folga-magnievaya-mb1—jis-h-4203/
Thank you for sharing your thoughts. I truly appreciate
your efforts and I will be waiting for your
further write ups thank you once again.
my blog post … telefon görüşme kabini
I’d like to thank you for the efforts you’ve put in penning this website.
I’m hoping to check out the same high-grade content from
you in the future as well. In truth, your creative writing abilities has encouraged
me to get my own, personal website now ;)
Here is my web blog :: Magic Mushrooms Online Canada
I am regular visitor, how are you everybody?
This piece of writing posted at this web site is in fact fastidious.
My web page … Buy Mushrooms Online Canada
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-42kh36kh1-1-mm-27kh29-mm-miagkaia-paika-m2m-gost-r-52922-2008/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/list/list-6khs-2x2000x2000-gost-19903-74/
Jungle Driving School Omaha
4020 Ѕ 147th St, Omaha,
NE 68137, United States
14024170547
hiring driving instructors – Anneliese,
Hello there! This post could not be written any better!
Reading this post reminds me of my good old room mate!
He always kept chatting about this. I will forward this page to him.
Fairly certain he will have a good read. Many thanks for sharing!
My web blog … vdcasino giriş
If you desire to get a good deal from this post then you have to apply these techniques to your won blog.
Look into my web page: slon9t.cc
Why viewers still use to read news papers when in this technological globe everything is accessible on web?
my page; malware
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-151—bs-3370/poroshok-magnievyy-mag-151—bs-3370/
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-145kh2-5-mm-lts40sd-gost-13943-86/
Опыт работы с более чем 120 постоянными заказчиками свидетельствует о высокой стабильности и надежности поставок.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-50kh50kh4-mm-42crmo4-din-1029/
Thank you for the good writeup. It in fact was a amusement account it.
Look advanced to more added agreeable from you! By the way, how can we communicate?
Have a look at my homepage: air conditioning
Hey superb website! Does running a blog similar to this take a massive amount work?
I’ve no understanding of programming however I was hoping to start my own blog soon. Anyway,
should you have any suggestions or tips for new blog owners please share.
I know this is off subject but I just had to ask.
Many thanks!
Here is my site … yanmaz akustik sünger
Профессиональный подход к описанию каждого вида металла
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m19995—uns/list-magnievyy-m19995—uns/
ozuipm
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-133kh113kh2-3-mm-53-5kh56-mm-tverdaia-paika-m3rm-gost-32590-2013/
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-60kh2smf-70-gost-2590-2006/
bonjour I love Your Blog can not say I come here often but im liking what i c so far….
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m14142—uns/polosa-magnievaya-m14142—uns/
goGLOW Houston Heights
1515 Studemnt Ѕt Suite 204, Houston,
Texas, 77007, UЅA
(713) 364-3256
chemical peels benefits guide
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-55kh1-7-mm-lts37mts2s2k-gost-13943-86/
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-80kh80kh8-mm-18crnimo7-6-en-10056-1/
Awesome things here. I’m very glad to look your post.
Thanks so much and I’m taking a look ahead to touch you. Will
you please drop me a mail?
Have a look at my web blog :: Nordic iptv
This is my first time go to see at here and i am
truly impressed to read everthing at single place.
my website; iptv sweden
Wow! At last I got a web site from where I can genuinely obtain useful facts concerning my study and knowledge.
my website; bästa iptv
Very energetic blog, I enjoyed that bit. Will there be a part 2?
Feel free to visit my blog: wesoft.com.tr
Quality posts is the main to invite the visitors to visit the site, that’s what this site is providing.
Also visit my webpage … bästa iptv
Hello there! This post couldn’t be written any better!
Reading this post reminds me of my old room mate! He always
kept chatting about this. I will forward this page to him. Fairly certain he will have
a good read. Many thanks for sharing!
Feel free to visit my homepage :: iptv sweden
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11800—uns/truba-magnievaya-m11800—uns/
Really….such a good webpage.
https://krakow-atrakcje.pl
Hi there! I understand this is sort of off-topic however I had to ask.
Does building a well-established website such as yours require a massive amount work?
I am brand new to operating a blog however I do write in my journal on a daily basis.
I’d like to start a blog so I can share my personal
experience and feelings online. Please let me know if you have any recommendations or tips for brand new aspiring blog owners.
Appreciate it!
Also visit my homepage: Nordic iptv
Extremely individual friendly website. Enormous details available
on few gos to.
https://radomsko24.pl
Great looking site. Think you did a great deal of your very own coding.
https://warszawa24.ovh
Thanks really practical. Will share website with my good
friends.
https://gostyn24.pl/pl/
Wow cuz this is very great job! Congrats and keep it up.
https://www.gazetamiedzyszkolna.pl
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-34kh29kh1-mm-23kh25-mm-miagkaia-paika-m2r-gost-32590-2013/
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/list/list-u7a-1-8x1000x1500-gost-19903-74/
Greetings! Very useful advice in this particular
article! It’s the little changes that make the biggest changes.
Many thanks for sharing!
Feel free to visit my blog post: toto macau
Howdy, i read your blog from time to time and
i own a similar one and i was just curious if you get a lot of spam feedback?
If so how do you stop it, any plugin or anything you can advise?
I get so much lately it’s driving me insane so any support is
very much appreciated.
Look into my page … 비아그라
Hello great blog! Does running a blog like this
take a large amount of work? I’ve virtually
no understanding of programming however
I had been hoping to start my own blog soon. Anyway, if you have any
suggestions or tips for new blog owners please share.
I know this is off subject nevertheless I simply had to ask.
Many thanks!
Feel free to visit my blog; gudang bokep indonesia
Thanks for finally writing about > Heel Pain –
Plantar Fasciitis – Mr Will Edwards Nordic iptv
Spot on with this write-up, I really believe this website
needs much more attention. I’ll probably be back again to read through more, thanks for the information!
Here is my web site – MALWARE
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m10100—uns/truba-magnievaya-m10100—uns/
I don’t even understand how I ended up here, but I assumed this
put up used to be good. I don’t recognise who you’re but certainly you’re going to a well-known blogger should you are not already.
Cheers!
Here is my website … 손목터널증후군
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m158-164kh4-mm-lk80-din-472/
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-80kh40kh8-mm-x50crmov15-en-10088-3/
I am not sure where you’re getting your information, but good topic.
I needs to spend some time learning much more or understanding more.
Thanks for magnificent information I was looking for this info for my mission.
My site – 비아그라 구매
Spot on with this write-up, I seriously feel this amazing site needs much
more attention. I’ll probably be returning to read more, thanks for the information!
Review my website :: unblocked games
Поковки и штабики — важные заготовки для металлургических предприятий
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mg99-80b—iso-8287/pokovka-magnievaya-iso-mg99-80b—iso-8287/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-16kh12kh0-7-mm-10-6kh12-6-mm-tverdaia-paika-m3rt-gost-32590-2013/
Наличие никелевых сплавов гарантирует высокую коррозийную стойкость оборудования, создаваемого заказчиками.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-06kh1500kh4000-mm-1-4541-en-iso-9444-2/
An outstanding share! I’ve just forwarded this onto a friend who has been conducting a little research on this.
And he in fact ordered me dinner due to the fact that I discovered
it for him… lol. So allow me to reword this….
Thanks for the meal!! But yeah, thanks for spending some time to discuss this matter here on your web page.
Feel free to surf to my page – bästa iptv
Hey There. I found your blog the usage of msn. That is
a very well written article. I will make sure to bookmark it and come back to read more of your helpful info.
Thank you for the post. I’ll definitely return.
Take a look at my web-site: check this out
I have been surfing online more than three hours today,
yet I never found any interesting article like yours.
It’s pretty worth enough for me. Personally, if all site owners and bloggers made
good content as you did, the web will be a lot more useful than ever before.
My webpage – iptv sweden
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-hz32—csa-hg-9/list-magnievyy-hz32—csa-hg-9/
I am extremely impressed together with your writing abilities and also
with the layout for your weblog. Is this a paid theme or did you customize it your
self? Anyway stay up the nice quality writing, it is rare to see a nice weblog like this one today..
My blog: vavada kz вход
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m110-117kh4-mm-lts25s2-din-472/
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-38kh2nm-26x1550x1250-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
I really like what you guys are usually up too. This type of clever work and reporting!
Keep up the great works guys I’ve incorporated you guys to
our blogroll.
Also visit my web-site … bästa iptv
I don’t know if it’s just me or if perhaps everyone else
encountering problems with your site. It appears as if some of the written text on your
posts are running off the screen. Can someone else
please comment and let me know if this is happening to them
too? This could be a problem with my browser because I’ve had
this happen before. Thanks
My blog post – Nordic iptv
Hurrah! After all I got a blog from where I know how to truly obtain helpful data concerning my
study and knowledge.
My page crypto online casino
Hi! I’ve been following your website for some time now and finally got the
bravery to go ahead and give you a shout out from Austin Texas!
Just wanted to mention keep up the excellent work!
Also visit my homepage … video bokep artis indonesia
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-mgse3zn2zr1—din-1729-part-2/krug-magnievyy-g-mgse3zn2zr1—din-1729-part-2/
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-76-1kh65kh1-6-mm-33-5kh36-5-mm-miagkaia-paika-m1-gost-32590-2013/
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-3kh1500kh4000-mm-1-4016-en-iso-9444-2/
Pretty nice post. I just stumbled upon your weblog and
wished to say that I have truly enjoyed surfing around your blog posts.
After all I will be subscribing to your feed
and I hope you write again very soon!
My website control cable; Trista,
Good post! We will be linking to this great post on our site.
Keep up the good writing.
My webpage: togel
I just like the helpful information you supply for your
articles. I’ll bookmark your weblog and check once more right here regularly.
I’m fairly certain I’ll be informed plenty of new stuff proper right here!
Good luck for the next!
My blog iptv sweden
Honestly I have to mention that after hunting for plastic window frames in Amsterdam for
some time, I finally discovered a kunststof kozijnen amsterdam specialist through a trusted local
business and the experience was really impressive — I
got a free quote and the overall cost was far more reasonable than I thought it
would be, especially compared to other options in the city, and the kunststof kozijnen offerte aanvragen (http://ataxiav.com/vob/xe/Events_News/2884731) amsterdam installateur who came to do the installation was incredibly efficient
and walked me through each step, so if you’re planning on replacing your old
frames I’d wholeheartedly advise checking out a budget-friendly specialist
because the quality is truly worth it in both comfort and looks!
Going through your thoughts helped me reframe something
My web-site – larry jackson exposed; Galen,
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-ga8/lenta-magnievaya-ga8/
Hi there, just wanted to mention, I loved this post. It was funny.
Keep on posting!
my blog; chase travel phone number
You’ll never go wrong with PDI Health’s mobile X-ray services—your one-stop
solution for mobile imaging. In addition to mobile xray services X-rays, we also offer mobile ultrasound, mobile EKG, mobile radiology, and a full range
of mobile diagnostic imaging services.
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m17-18-3kh1-mm-lsdch-din-472/
Поставка продукции возможна не только в промышленных, но и в малых лабораторных объемах для исследовательских целей.
https://rms-ekb.ru/catalog/plity/plita-3kh2n2mvf-25x320x80-gost-19903-74/
Hola a todos, deseo recomendar una página que leí hace unos días y que me llamó mucho la
atención. Es un contenido bastante detallado sobre la historia del fútbol argentino, desde sus orígenes hasta la actualidad.
Desde mi experiencia, me gusta aprender sobre cómo fue construyéndose la cultura futbolística en Argentina.
Esta página explica muy bien la llegada del fútbol al país, el papel
de las comunidades inmigrantes, así como el crecimiento de los clubes que construyeron una tradición única.
Lo que encontré más interesante es que no presenta datos de manera fría, sino que también explica el contexto social.
Aprendí bastante sobre instituciones históricas, rivalidades clásicas y la forma en que
el fútbol pasó de ser un deporte importado a convertirse en un símbolo cultural argentino.
Por otra parte, el texto dedica espacio a grandes
figuras históricas como Diego Maradona y Lionel Messi.
El análisis de sus contribuciones ayuda a comprender por qué han dejado una
huella imborrable.
Algo que vale la pena destacar es la sección dedicada
a los clubes argentinos y a los torneos internacionales.
La información está bien organizada y permite entender mejor el prestigio de los equipos argentinos.
Si te gusta la historia deportiva, te sugiero dedicar unos minutos a este artículo.
Incluso si no sigues habitualmente el fútbol argentino, encontrarás datos interesantes, contexto histórico y curiosidades.
Para concluir, pienso que este contenido vale la pena.
Aprendí bastante sobre la evolución del deporte en Argentina y seguramente
volveré a consultarla en el futuro. Totalmente recomendada.
Feel free to visit my web page URL
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mc21210/truba-magnievaya-en-mc21210/
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-22kh18kh0-9-mm-15-4kh17-6-mm-tverdaia-paika-m0b-gost-32590-2013/
ООО «РМС» предлагает широкий спектр цветного проката, включая медь, латунь, бронзу и дюралюминий.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-stal-35-95x1800x1250-gost-r-52146-2003-polimernyi-otsinkovannyi-kholodnokatanyi/
I’ve learn a few good stuff here. Certainly price bookmarking for revisiting.
I wonder how a lot attempt you set to make such a excellent informative site.
My web-site: hospitality projects
We stumbled over here coming from a different web page and thought I might check things out.
I like what I see so now i’m following you. Look forward to checking out your web page repeatedly.
My web site; https://bloembinderijlisette.nl/
Great blog right here! Also your web site quite
a bit up fast! What host are you the usage of?
Can I am getting your affiliate hyperlink in your host?
I want my website loaded up as quickly as yours lol
my homepage; google
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-b-199-qe22a—astm-b199/prutok-magnievyy-b-199-qe22a—astm-b199/
Wow, marvelous blog layout! How long have you ever been blogging
for? you make running a blog look easy. The overall glance of your site is magnificent, as well as the content!
my webpage – retro bowl
When I originally left a comment I seem to have clicked on the -Notify me when new comments
are added- checkbox and now every time a comment is added I
recieve four emails with the exact same comment.
Is there a means you are able to remove me from that service?
Thanks!
Feel free to visit my website :: visabet88 aman
You could certainly see your skills within the
article you write. The arena hopes for even more
passionate writers such as you who aren’t afraid to mention how they believe.
All the time go after your heart.
Stop by my site … 가라오케
Wonderful blog! Do you have any helpful hints for
aspiring writers? I’m hoping to start my own blog soon but I’m a little lost on everything.
Would you advise starting with a free platform like WordPress or go for a paid option? There are so many
options out there that I’m completely overwhelmed .. Any recommendations?
Appreciate it!
Feel free to surf to my webpage :: theme parks
Hey there! Do you know if they make any plugins to protect against hackers?
I’m kinda paranoid about losing everything I’ve worked hard on. Any suggestions?
Also visit my web site slot pepek
Keep on writing, great job!
Feel free to visit my web-site; myacademy.in.net lừa đảo công an cấm người chơi tham gia
If some one wants expert view regarding blogging and
site-building after that i suggest him/her to visit this webpage, Keep up the good work.
My homepage: Horse Gelatin trick
fantastic publish, very informative. I wonder why the opposite experts of this sector don’t realize this.
You should proceed your writing. I’m sure, you have a great readers’ base already!
my webpage; webpage
Attractive section of content. I simply stumbled
upon your weblog and in accession capital to claim that I acquire in fact enjoyed
account your weblog posts. Any way I’ll be subscribing for your
feeds and even I success you access consistently quickly.
Check out my web-site :: คลิปโป๊แอบถ่าย
I constantly spent my half an hour to read this website’s articles everyday
along with a mug of coffee.
my web page Horse Gelatin trick for men
Excellent blog! Do you have any helpful hints for aspiring
writers? I’m hoping to start my own site soon but I’m a little lost on everything.
Would you propose starting with a free platform like WordPress or go for a paid option? There are so
many choices out there that I’m completely overwhelmed ..
Any ideas? Cheers!
Feel free to visit my website – 비아그라 구매
Magnificent items from you, man. I have be aware your stuff previous
to and you are just too excellent. I really like what you have
bought right here, certainly like what you’re saying and the way in which by which you say it.
You make it enjoyable and you still take care of to keep it smart.
I cant wait to read much more from you. That
is actually a wonderful site.
My web site; 8x-bet.ru.com lừa đảo công an truy nã cấm người chơi tham gia
Фольга из редких металлов часто требуется для высокотехнологичных лабораторий
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-65bt—gost-10994-74-1/izdeliya-iz-titana-65bt—gost-10994-74-1/
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-300kh800-mm-lsdch/
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-3kh1000kh3000-mm-1-4509-en-iso-9444-1/
Attractive section of content. I just stumbled
upon your blog and in accession capital to assert that
I get actually enjoyed account your blog posts. Any way I’ll
be subscribing to your feeds and even I achievement you access consistently quickly.
Here is my page: bambu ams
Simply want to point out I am just relieved that i came upon your internet page.
isanok.pl
Great looking website. Assume you did a bunch of your own html coding.
https://www.zvami.tv
소액결제현금화 키워드에 대한 정보를 제공합니다.
휴대폰 소액결제의 개념, 한도 운영 방식, 통신요금 청구 구조, 이용 전 확인사항 및 자주 묻는 질문을 확인해보세요.
my webpage … 소액결제현금화c
Merely needed to tell you I am just thrilled that i happened on the internet page!
https://www.debica24.eu
You’ve gotten one of the best websites.
https://esopot.pl
Thanks a ton for sharing this superb internet site.
https://www.pewnybiznes.info
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/tantal-i-ego-splavy/tantal-t-15-1/polosa-tantalovaya-t-15/
ООО «РМС» предлагает широкий спектр цветного проката, включая медь, латунь, бронзу и дюралюминий.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-12gn2mfaiu-2-2x1550x1600-gost-19903-2006-gladkii-belyi-goriachekatanyi/
야코레드를 검색하기 전 알아야 할 주소모음·스트리밍 사이트 관련 주의사항, 저작권·개인정보·디지털 성범죄 위험, 안전한 콘텐츠 이용
기준을 정리했습니다.
Thanks , I have recently been searching for information approximately this topic for
ages and yours is the greatest I’ve came upon till now.
However, what about the conclusion? Are
you positive about the source?
Here is my web site … markaskontol
naturally like your web site but you need to check the spelling on quite a few of your posts.
Several of them are rife with spelling issues and I in finding it very troublesome to inform the reality nevertheless
I’ll definitely come back again.
my webpage … web platform
say thanks to a lot for your internet site it assists a lot.
https://www.tvsudecka.pl
My brother suggested I might like this web site.
He was entirely right. This post actually made my day.
You can not imagine simply how much time I had spent for this information!
Thanks!
Also visit my webpage :: wow wotlk download 3.3 5a
Наличие циркония свидетельствует о работе с высокотехнологичными заказами
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nbp-3b—gost-26252-84-1/pokovka-niobievaya-nbp-3b—gost-26252-84/
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-stal-45-89×10-gost-21729-76/
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-800kh600-mm-lazhmts/
Thanks in support of sharing such a fastidious
idea, piece of writing is pleasant, thats why i have read it entirely
Here is my page; situs visabet88
First of all I would like to say wonderful
blog! I had a quick question which I’d like to ask if you do not mind.
I was interested to find out how you center yourself and clear your thoughts prior to
writing. I have had trouble clearing my mind in getting my ideas out.
I truly do enjoy writing however it just seems like the first 10 to 15 minutes are lost just trying to figure out how to begin. Any ideas or hints?
Cheers!
My webpage; pinup
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-tzc-1/poroshok-molibdenovyy-tzc/
Металлические порошки различных фракций позволяют клиентам использовать их в порошковой металлургии и напылении.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-10ps-1-6x2000x1250-gost-19903-2006-gladkii-belyi-goriachekatanyi/
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-troiniki-press/mednyi-press-troinik-12-mm-m1r-gost-r-52948-2008/
Широкий выбор тугоплавких металлов, таких как вольфрам и молибден
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mpch-2/lenta-molibdenovaya-mpch/
Ориентация на долгосрочные отношения с клиентами позволяет компании формировать индивидуальные условия оплаты и графики поставок.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-60khg-68-gost-1133-71/
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-70kh200-mm-lts40s/
This paragraph gives clear idea designed
for the new users of blogging, that in fact how to do running a blog.
Review my website – Boat Santa Claus Friv2
Busy Bee Jumpers
45 Main St 6C, Wareham,
ⅯA 02571, Unites Ѕtates
508-514-2005
Bookmarks
Hello! Someone in my Facebook group shared this site with
us so I came to check it out. I’m definitely enjoying the information. I’m book-marking and will be tweeting this to my followers!
Fantastic blog and outstanding design.
Also visit my webpage; webpage
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-fmo55a-1/pokovka-molibdenovaya-fmo55a/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-160kh160kh15-mm-36nicrmo16-uni-6762/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-45-gradusov-53-6-mm-m1e-gost-r-52948-2008/
bedava bitcoin, ücretsiz kripto, casino bonus, casino sitesi,
güvenilir casino, online casino, canlı casino, slot
oyunları, rulet oyna, poker oyna, blackjack oyna,
bahis sitesi, güvenilir bahis, canlı bahis, spor bahisleri, yüksek oran bahis, kaçak
bahis, bedava bahis, deneme bonusu, hoşgeldin bonusu, casino free spin, slot free spin, kumar sitesi, kumarhane, çevrimiçi kumar,
illegal bahis, yasa dışı bahis, illegal casino,
yasadışı kumar, kayıt olmadan bahis, kimlik doğrulama yok bahis,
bahis para yatır, bahis para çek, casino
para çekme, casino para yatırma, slot jackpot, jackpot casino, bedava casino, ücretsiz casino,
casino demo, canlı krupiye, canlı rulet, canlı blackjack, canlı poker, canlı baccarat, baccarat oyna, baccarat sitesi, çevrimsiz bonus, yatırımsız bonus, çevrim şartsız bonus, kayıp bonusu, kayıp iadesi, free bet, freespin, casino cashback, bahis cashback, bedava iddaa, maç izle bahis, canlı maç bahis, futbol bahis, basketbol bahis, tenis bahis, esports bahis, sanal
bahis, sanal spor bahis, köpek yarışı bahis, at yarışı bahis, greyhound
bahis, poker freeroll, escort bayan, escort istanbul, escort ankara,
escort izmir, escort bursa, escort adana, escort kocaeli, escort
mersin, escort antalya, escort gaziantep, escort
konya, escort diyarbakır, escort aydın, escort kayseri,
vip escort, ucuz escort, eve gelen escort, otele gelen escort,
saatlik escort, gecelik escort, haftalık escort, çıkmalık
escort, rezidans escort, öğrenci escort, yabancı escort,
rus escort, ukraynalı escort, arap escort, sarışın escort, esmer escort, olgun escort
My homepage devlet bahçeli porno ifşa
Qué tal comunidad, deseo recomendar una página que descubrí
recientemente y que realmente disfruté. Es una lectura muy interesante
sobre la historia del fútbol argentino, desde
sus orígenes hasta la actualidad.
Personalmente, siempre me interesó conocer cómo nació y evolucionó la cultura futbolística en Argentina.
El contenido presenta con mucho detalle la llegada del fútbol al país, el
papel de las comunidades inmigrantes, así
como el crecimiento de los clubes que formaron la identidad deportiva nacional.
Lo que más me gustó es que no se limita a mencionar fechas, sino que
también explica el contexto social. Descubrí muchos detalles
interesantes sobre instituciones históricas, rivalidades clásicas
y la forma en que el fútbol pasó de ser un deporte importado a convertirse en una verdadera pasión nacional.
Además, el texto dedica espacio a jugadores legendarios como Maradona, Messi y otras estrellas argentinas.
El análisis de sus contribuciones ayuda a comprender por qué
han dejado una huella imborrable.
Un punto muy interesante es la sección dedicada a los clubes argentinos y a los torneos internacionales.
El contenido resulta fácil de seguir y permite entender mejor la
influencia del fútbol argentino a nivel mundial.
Si te gusta la historia deportiva, creo que vale mucho la pena visitar esta
página. Aunque no seas un experto en el tema, encontrarás muchos detalles que enriquecen la experiencia.
Para concluir, es una lectura que recomiendo sinceramente.
Me ayudó a entender mejor la historia del fútbol argentino y
seguramente volveré a consultarla en el futuro. Una excelente lectura para cualquier amante
del fútbol.
My blog post; URL
Hurrah! Finally I got a webpage from where I can really obtain helpful information regarding my study and
knowledge.
Also visit my page … search engine optimization
Heya fantastic blog! Does running a blog like this take a large amount of
work? I’ve absolutely no expertise in coding however
I was hoping to start my own blog in the near future.
Anyways, if you have any suggestions or tips for new blog owners please share.
I know this is off subject nevertheless I just had
to ask. Thanks!
my homepage :: Marriage Visa Australia
Поковки и штабики — важные заготовки для металлургических предприятий
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-sismg4640-10—ss-141640/folga-magnievaya-sismg4640-10—ss-141640/
Terrific article! This is the type of info that should be shared across the
net. Shame on Google for no longer positioning this publish upper!
Come on over and visit my web site . Thanks =)
My web page; radiology imaging
Экспертная консультация при выборе сплавов помогает клиентам оптимизировать затраты и избежать технологических ошибок.
https://rms-ekb.ru/catalog/plity/plita-12kh1-18x60x1000-gost-19903-74/
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-70kh600-mm-lk80/
6e8xta
Really….this is a good webpage.
https://infoskierniewice.pl
Simply just want to state I am just happy I came onto your website page!
https://nasz-szczecin.pl
I appreciate checking your web site. With thanks!
https://www.kopalniapracy.pl
Great looking site. Assume you did a great deal of your own html coding.
https://www.oferujemyprace.pl
Simply just wanted to point out I am grateful that i came on the web site.
https://www.igryfino.pl
Hello there! I know this is kinda off topic nevertheless I’d figured I’d
ask. Would you be interested in exchanging links or maybe
guest authoring a blog article or vice-versa? My site
discusses a lot of the same topics as yours and I feel we could greatly benefit
from each other. If you might be interested feel free to shoot me an email.
I look forward to hearing from you! Superb blog
by the way!
Also visit my website: togel withdraw cepat
Thanks a ton! This is definitely an fantastic web-site!
https://www.nowytydzien.pl
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-r60702—uns/lenta-magnievaya-r60702—uns/
Thanks, this site is very handy.
https://www.oferujemyprace.pl
Поставки жаропрочных сплавов ориентированы на потребности авиационной и энергетической отраслей.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-50kh50kh4-mm-x15cr13-en-10088-3/
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-80-mm-m2r-gost-r-52948-2008/
Ahaa, its fastidious dialogue on the topic of this post at this place at this blog, I have read
all that, so at this time me also commenting here.
My website; King James Bible
Very rapidly this site will be famous among all blog users, due to it’s
pleasant articles
my blog post Faith And Spirituality
Возможность заказа висмута — достаточно редкое предложение на рынке
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-zn1zr/poroshok-magnievyy-mg-zn1zr/
You’ve the best internet sites.
https://www.tv-slupsk.pl
Thanks intended for supplying like substantial details.
https://www.malbork1.pl
Great looking site. Assume you did a bunch of your very own coding.
https://www.praca-biznes.pl
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/list/list-9khs-10x500x1000-gost-19903-74/
Hi-ya, well put together website you’ve here.
https://www.oferujemyprace.pl
Wow cuz this is excellent job! Congrats and keep it up.
https://www.pilska.tv
I love reading your websites. Thanks a ton!
https://www.mttv.pl
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-410-mm-lts30a3/
The advice is rather significant.
https://www.kociewiak.pl
Highly beneficial, looking forth to coming back.
https://www.ta-praca.pl
Excellent beat ! I would like to apprentice whilst you amend
your web site, how can i subscribe for a blog website?
The account helped me a appropriate deal. I have been tiny bit
familiar of this your broadcast provided vibrant transparent
idea
Also visit my blog pari match
I am regular reader, how are you everybody?
This piece of writing posted at this web page is genuinely fastidious.
Look into my website … 8xbett.in.net lừa đảo công an truy nã cấm người chơi tham gia
Awesome issues here. I am very glad to peer your article.
Thanks so much and I am taking a look ahead to contact
you. Will you please drop me a mail?
Have a look at my web-site lucky all
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-al6zn1mn/krug-magnievyy-mg-al6zn1mn/
География деятельности компании охватывает всю территорию России, обеспечивая металлом предприятия в удаленных регионах.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-18kh2n4va-7x1400x1000-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/manganinovaia-provoloka/manganinovaia-provoloka-1-2-mm-mnmtsazh3-12-0-3-0-3-gost-10155-72/
Hi, i feel that i noticed you visited my site so i got here to
return the favor?.I am trying to to find things to
enhance my site!I assume its good enough to use a few of your ideas!!
Feel free to visit my website … Jesus Parables
You could definitely see your expertise within the article you write.
The arena hopes for more passionate writers such as you who are not afraid to say how they believe.
At all times follow your heart.
my site: пин ап казино вход
Very energetic post, I enjoyed that bit. Will there be a part 2?
Review my web page … الدوري الإنجليزي
Great looking internet site. Think you did a bunch
of your very own coding.
https://www.tvzachod.pl
Spot on Peace and Love with Christ this write-up, I seriously believe that this web site
needs far more attention. I’ll probably be returning to see
more, thanks for the info!
Удобное разделение продукции на сплавы и конкретные виды проката
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-md2b—jis-h-5303/lenta-magnievaya-md2b—jis-h-5303/
You’ve got among the finest online sites.
https://www.telewizjaolsztyn.pl
Good day, excellent site you’ve got right now.
https://nasz-szczecin.pl
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-20k-8x1800x1000-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Great looking internet site. Presume you did a bunch of your very own coding.
https://www.tvobiektyw.pl
My partner and I stumbled over here different web page and thought I may as well check things out.
I like what I see so i am just following you.
Look forward How to Read the Bible looking over your web page again.
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-124-mm-lts40s/
Lovely Web site, Maintain the good job. Thank you.
https://www.gazetamiedzyszkolna.pl
Thanks for the marvelous posting! I really enjoyed reading it,
you might be a great author. I will make certain to bookmark your blog and definitely
will come back down the road. I want to encourage you
to continue your great posts, have a nice afternoon!
Also visit my web-site: Horse Gelatin trick for men
I appreciate checking your website. Thanks a ton!
https://www.pewnybiznes.info
Passion the website– very individual pleasant and whole lots
to see!
ekspresjaroslawski.pl
Wow because this is excellent work! Congrats and keep it up.
https://www.tvsudecka.pl
Its like you read my mind! You seem to grasp so much approximately this, like you
wrote the e book in it or something. I believe that you could do with
some percent to power the message house a bit, however other than that, this is fantastic blog.
An excellent read. I will certainly be back.
my web page virtual desktop meta store
A colleague in the field told me to check out your website.
Awesome web-site you possess right here.
https://www.tv-slupsk.pl
I just couldn’t leave your website before suggesting that I really enjoyed the usual information an individual supply on your visitors? Is gonna be back often in order to investigate cross-check new posts
Superb Website, Maintain the good work. Thank you!
https://www.oto-praca.pl
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-9—bs-2970-1/poroshok-magnievyy-mag-9—bs-2970-1/
Great looking site. Assume you did a great deal of your very own html coding.
https://www.polskibiznes.info
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-kh6f4m-21-55-gost-7417-75/
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-66-7kh57kh1-4-mm-33-5kh36-5-mm-miagkaia-paika-m2t-gost-32590-2013/
Simply just wished to stress Now i’m lucky I came on the website.
https://www.tc.ciechanow.pl
I do not even know the way I ended up right here, however I thought this publish was once good.
I don’t recognise who you might be but certainly you’re going to a well-known blogger when you aren’t already.
Cheers!
Also visit my website :: Santa Unity
Excellent write-up. I certainly love this site. Stick with
it!
Feel free to visit my page; Panduan Live Draw
Wow because this is excellent job! Congrats and keep it up.
https://www.tvobiektyw.pl
Amazing….such a handy internet site.
https://www.mojebielsko.pl
Широкий выбор тугоплавких металлов, таких как вольфрам и молибден
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-131—bs-3370/izdeliya-iz-magniya-mag-131—bs-3370/
Wonderful blog! I found it while searching on Yahoo News.
Do you have any tips on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get
there! Many thanks
Also visit my homepage; web site
Wow because this is excellent job! Congrats and keep it up.
https://www.polskapraca.info
Extremely individual pleasant website. Huge information readily available on couple of clicks.
https://www.kwidzyn1.pl
Wow, stunning portal. Thnx …
https://www.telewizjamazury.pl
I will share you blog with my sis.
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-08kh13-0-8x1400x1600-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
Neat Webpage, Preserve the great job. Appreciate it.
https://koscierski.info
Really needed to mention I’m just relieved that i happened upon your page!
https://www.swiebodzin.tv
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-3×150-mm-lo90-1-tu-48-21-847-89/
Thanks for sharing your thoughts on MALWARE.
Regards
Your knowledge is extremely intriguing.
https://www.pewnybiznes.info
I benefit from checking your website. Thanks a lot!
https://www.kronikatygodnia.pl
Maintain the helpful job and delivering in the crowd!
https://www.pewnybiznes.info
I enjoy this website – its so usefull and helpfull.
https://www.nowytydzien.pl
Buenas a todos, deseo recomendar una página que descubrí recientemente
y que realmente disfruté. Es un contenido bastante detallado sobre
la historia del fútbol argentino, desde sus orígenes
hasta la actualidad.
Desde mi experiencia, me gusta aprender sobre cómo se desarrolló
y creció la cultura futbolística en Argentina.
El contenido presenta con mucho detalle la llegada del fútbol al país, los primeros
pasos de este deporte, así como el crecimiento de los clubes que
formaron la identidad deportiva nacional.
Lo que encontré más interesante es que no presenta datos de manera
fría, sino que también explica el contexto social.
Descubrí muchos detalles interesantes sobre instituciones históricas, rivalidades clásicas y la forma en que el fútbol pasó de ser un deporte importado a
convertirse en un símbolo cultural argentino.
También, el texto dedica espacio a íconos del fútbol mundial como las
máximas referencias del fútbol argentino. La forma
en que se describe su impacto ayuda a comprender por qué son admirados en todo el mundo.
Un punto muy interesante es la sección dedicada a
los clubes argentinos y a los torneos internacionales. La información está bien organizada
y permite entender mejor el prestigio de los equipos argentinos.
Si disfrutas leyendo sobre grandes tradiciones futbolísticas,
sin duda recomiendo leer este contenido. Aun si recién estás comenzando a interesarte por este deporte,
encontrarás muchos detalles que enriquecen la experiencia.
Para concluir, es una lectura que recomiendo sinceramente.
Me ayudó a entender mejor la historia del fútbol argentino y la guardaré entre mis lecturas recomendadas.
Muy recomendable.
Have a look at my web-site … URL
Наличие никелевых сплавов гарантирует высокую коррозийную стойкость оборудования, создаваемого заказчиками.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-stal-45-51×2-5-gost-21729-76/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-42kh36kh1-1-mm-27kh29-mm-tverdaia-paika-m3t-gost-32590-2013/
It’s really very complicated in this full of activity life to listen news on TV, so I simply use web for that reason, and get
the most up-to-date news.
my web-site – phising
I love your blog.. very nice colors & theme. Did you create this website yourself or did you
hire someone to do it for you? Plz respond as I’m looking to design my own blog and would like to know where u got this
from. kudos
Feel free to surf to my site; homepage
I don’t normally comment but I gotta say appreciate it for the post on this one : D.
I truly appreciate this post. I have been looking everywhere for this! Thank goodness I found it on Bing. You have made my day! Thank you again
My brother suggested I might like this websiteHe was once totally rightThis post truly made my dayYou can not imagine simply how a lot time I had spent for this information! Thanks!
Uduşları dərhal hesaba köçürən nadir kazino online platformalarındandır.
kazino onlayn
Qué tal comunidad, deseo recomendar una página que leí hace unos días y que me llamó mucho la atención.
Es un contenido bastante detallado sobre la historia del fútbol argentino, desde sus orígenes hasta la actualidad.
Como aficionado al fútbol, me gusta aprender sobre cómo nació
y evolucionó la cultura futbolística en Argentina.
El contenido presenta con mucho detalle la llegada del fútbol al país, la influencia británica, así como el crecimiento
de los clubes que marcaron generaciones.
Lo que realmente destaca es que no presenta datos de manera
fría, sino que también explica el contexto social.
Aprendí bastante sobre instituciones históricas, rivalidades clásicas y la forma en que el
fútbol pasó de ser un deporte importado a convertirse
en un símbolo cultural argentino.
Por otra parte, el texto dedica espacio a grandes figuras históricas como las máximas referencias del fútbol argentino.
El análisis de sus contribuciones ayuda a comprender
por qué han dejado una huella imborrable.
Un punto muy interesante es la sección dedicada a los clubes argentinos y a
los torneos internacionales. El contenido resulta fácil de
seguir y permite entender mejor la influencia del fútbol argentino a nivel mundial.
Si te gusta la historia deportiva, creo que vale mucho la pena visitar esta página.
Aun si recién estás comenzando a interesarte por este deporte, encontrarás
muchos detalles que enriquecen la experiencia.
Para concluir, considero que esta página merece una visita.
Aprendí bastante sobre la evolución del deporte en Argentina y la compartiré con otros aficionados al fútbol.
Una excelente lectura para cualquier amante del fútbol.
Also visit my web blog … url
Cabinet IQ
8305 Stаte Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Installprocess
magnificent submit, very informative. I wonder why the other specialists of this sector
don’t realize this. You should proceed your writing.
I am confident, you’ve a huge readers’ base already!
Review my blog Togel HK Malam Ini
If you want to get much from this article then you have
to apply such methods to your won weblog.
My web-site :: real money online casino virginia
Hello there! Quick question that’s entirely
off topic. Do you know how to make your site mobile friendly?
My site looks weird when viewing from my iphone4. I’m trying to find a theme or plugin that might be able to correct this problem.
If you have any suggestions, please share. With thanks!
my homepage :: 비아그라 구매
I am actually glad to read this blog posts which consists of
tons of useful data, thanks for providing these information.
Feel free to visit my blog post jingle mining review
I am extremely impressed with your writing skills as well as with the layout
on your weblog. Is this a paid theme or did you customize it yourself?
Anyway keep up the excellent quality writing, it is rare to see a great
blog like this one today.
Here is my blog post – rank on google
Buenas a todos, deseo recomendar una página que descubrí recientemente y que me llamó mucho la atención. Es un contenido
bastante detallado sobre la historia del fútbol argentino,
desde sus orígenes hasta la actualidad.
Como aficionado al fútbol, me gusta aprender sobre cómo nació y evolucionó la
cultura futbolística en Argentina. El contenido presenta con mucho detalle la llegada
del fútbol al país, la influencia británica, así
como el crecimiento de los clubes que construyeron una tradición única.
Lo que encontré más interesante es que no solo enumera acontecimientos, sino que también muestra la importancia cultural del fútbol.
Aprendí bastante sobre instituciones históricas, rivalidades
clásicas y la forma en que el fútbol pasó de ser un deporte importado a convertirse en parte de la
identidad del país.
También, el texto dedica espacio a jugadores legendarios como Maradona, Messi y otras
estrellas argentinas. La explicación de su legado ayuda a comprender
por qué son admirados en todo el mundo.
Un punto muy interesante es la sección dedicada a los clubes argentinos
y a los torneos internacionales. El contenido resulta fácil de seguir y permite entender mejor
el prestigio de los equipos argentinos.
Si eres fanático del fútbol, te sugiero dedicar unos minutos
a este artículo. Aunque no seas un experto en el tema, encontrarás información valiosa y
una lectura entretenida.
En resumen, es una lectura que recomiendo sinceramente. Disfruté mucho recorriendo cada sección del artículo y la guardaré entre mis lecturas
recomendadas. Una excelente lectura para cualquier amante del fútbol.
Feel free to surf to my blog; URL
Buenas a todos, quería compartir una página que descubrí recientemente y
que me sorprendió bastante. Se trata de un artículo muy completo sobre
la historia del fútbol argentino, desde sus orígenes hasta la actualidad.
Personalmente, siempre me interesó conocer cómo nació y evolucionó la cultura
futbolística en Argentina. El contenido presenta con mucho detalle la llegada del fútbol al país,
los primeros pasos de este deporte, así como el crecimiento de los
clubes que marcaron generaciones.
Lo que realmente destaca es que no solo enumera acontecimientos, sino que también muestra la importancia cultural del fútbol.
Aprendí bastante sobre instituciones históricas, rivalidades clásicas y
la forma en que el fútbol pasó de ser un deporte importado a convertirse en un símbolo cultural argentino.
Por otra parte, el texto dedica espacio a grandes figuras históricas como las máximas referencias del fútbol argentino.
La forma en que se describe su impacto ayuda a comprender por qué son admirados en todo
el mundo.
Algo que vale la pena destacar es la sección dedicada a los clubes argentinos y a los torneos internacionales.
El contenido resulta fácil de seguir y permite entender mejor
la importancia de la Copa Libertadores.
Si eres fanático del fútbol, creo que vale mucho la pena visitar esta página.
Aun si recién estás comenzando a interesarte por
este deporte, encontrarás información valiosa y una lectura entretenida.
Como recomendación final, considero que esta página merece una visita.
Disfruté mucho recorriendo cada sección del artículo y la guardaré entre mis lecturas recomendadas.
Totalmente recomendada.
My blog URL
I Am Going To have to come back again when my course load lets up – however I am taking your Rss feed so i can go through your site offline. Thanks.
Nice blog here! Also your site loads up very fast! What web host are you using?
Can I get your affiliate link to your host? I wish my web
site loaded up as quickly as yours lol
Here is my site Live Draw SDY Terpercaya
Great blog here! Also your web site loads up very fast!
What host are you using? Can I get your affiliate link to
your host? I wish my site loaded up as fast as yours lol
Feel free to surf to my web-site … trx address
Howdy! This post could not be written any better! Reading this post
reminds me of my previous room mate! He always kept chatting about this.
I will forward this article to him. Fairly certain he will have a good read.
Thanks for sharing!
my homepage bokep anak sma indonesia
Cabinet IQ
8305 Ꮪtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Remodeling
Pretty section of content. I just stumbled upon your site and in accession capital to assert that
I get actually enjoyed account your blog posts. Anyway I
will be subscribing to your augment and even I achievement you access
consistently quickly.
Here is my website; korean grocery store orlando fl
You have great information these.
https://www.tvobiektyw.pl
Terrific Web-site, Carry on the beneficial work.
Regards.
https://www.polskibiznes24.pl
Thanks pertaining to delivering this kind of awesome posting.
https://www.tvsudecka.pl
Thanks for sharing your very good web page.
https://www.igryfino.pl
Many thanks very beneficial. Will share website
with my friends.
https://www.polskibiznes24.pl
Baixe vídeos privados não apenas do YouTube, mas também download video do youtube pc Facebook, Vimeo,
Bilibili e muitos outros sites.
Having read this I thought it was extremely enlightening.
I appreciate you taking the time and energy to put this information together.
I once again find myself spending a significant amount of time both reading and
commenting. But so what, it was still worthwhile!
My web page; lka99
Wow, that’s what I was looking for, what a information! present
here at this web site, thanks admin of this web site.
Here is my blog – thaivegas
Incredible quest there. What happened after? Good luck!
Also visit my blog post … vanity address tron
Hey just wanted to give you a quick heads up. The words
in your content seem to be running off the screen in Firefox.
I’m not sure if this is a formatting issue or something to do with web browser compatibility
but I thought I’d post to let you know. The design look great
though! Hope you get the problem resolved soon. Many thanks
Here is my web blog :: safe casino sites Canada
Nice post. I was checking continuously this blog and I am inspired!
Very helpful information specially the ultimate part :) I maintain such information a lot.
I used to be seeking this particular information for a long
time. Thanks and best of luck.
Feel free to visit my page تور کربلا
Good day! This is my 1st comment here so I just wanted to give a quick shout out and tell you I really enjoy reading through your
blog posts. Can you recommend any other blogs/websites/forums
that go over the same subjects? Thanks a ton!
Stop by my webpage :: VB88
Our legal design templates are written in easy, simple English– no
difficult lingo.
My webpage Party Structure Notice; Jens,
Having read this I thought it was rather enlightening. I appreciate you taking the time and effort to put
this article together. I once again find myself spending way
too much time both reading and leaving comments.
But so what, it was still worthwhile!
Have a look at my website https://forkintheroadcoffee.com/
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Renovationexperts – atavi.com –
Attractive section of content. I just stumbled upon your weblog and in accession capital to assert that I acquire actually enjoyed account your blog posts.
Any way I will be subscribing to your feeds
and even I achievement you access consistently quickly.
Have a look at my blog … best licensed online casino Canada
I think what you published was actually very reasonable.
However, what about this? suppose you typed a catchier title?
I mean, I don’t wish to tell you how to run your blog, however what if you added something that makes people desire more?
I mean Heel Pain – Plantar Fasciitis – Mr Will Edwards is a little vanilla.
You should look at Yahoo’s front page and note how they write news titles to get viewers to click.
You might add a related video or a related picture or two to get people excited about what you’ve written.
Just my opinion, it could make your posts a little
livelier.
my homepage … real-value-starts-with-usability
Great blog here! Also your site loads up fast! What web host are you using?
Can I get your affiliate link to your host?
I wish my web site loaded up as quickly as yours lol
Here is my web-site :: ترولی ایکیا
We are a group of volunteers and starting a new scheme in our community.
Your site provided us with valuable information to work on. You
have done an impressive job and our entire community will be
thankful to you.
Here is my web site; how to compare casino bonuses Canada
Buenas a todos, deseo recomendar una página que encontré
hace poco y que me llamó mucho la atención. Es una lectura muy
interesante sobre la historia del fútbol argentino, desde sus orígenes hasta la actualidad.
Personalmente, me gusta aprender sobre cómo nació y evolucionó la cultura futbolística en Argentina.
El artículo describe de forma excelente la llegada del
fútbol al país, los primeros pasos de este deporte, así como el crecimiento de los clubes que formaron la identidad deportiva nacional.
Lo que más me gustó es que no presenta datos de manera
fría, sino que también muestra la importancia cultural
del fútbol. Descubrí muchos detalles interesantes sobre
instituciones históricas, rivalidades clásicas
y la forma en que el fútbol pasó de ser un deporte importado a convertirse en un símbolo cultural argentino.
Por otra parte, el texto dedica espacio a grandes figuras históricas como Maradona, Messi
y otras estrellas argentinas. La forma en que se describe su impacto ayuda a comprender por qué son admirados en todo el mundo.
Un punto muy interesante es la sección dedicada a
los clubes argentinos y a los torneos internacionales.
El contenido resulta fácil de seguir y permite entender
mejor la importancia de la Copa Libertadores.
Si te gusta la historia deportiva, sin duda recomiendo
leer este contenido. Incluso si no sigues habitualmente el fútbol argentino, encontrarás muchos detalles que enriquecen la experiencia.
Como recomendación final, pienso que este contenido vale la pena.
Aprendí bastante sobre la evolución del deporte en Argentina y la guardaré entre mis lecturas
recomendadas. Muy recomendable.
my blog URL
Maintain the excellent job !! Lovin’ it!
https://www.tvsudecka.pl
Maintain the exceptional work !! Lovin’ it!
https://www.gazetamiedzyszkolna.pl
I enjoy this website – its so usefull and helpfull.
https://warszawa24.ovh
If you want to grow your familiarity just keep visiting this web page and be updated with the latest news update posted here.
Here is my web-site :: best live blackjack site canada
Quality articles is the crucial to attract the users to visit the site, that’s what this website
is providing.
my website; legal casino sites Canada
Busy Bee Jumpers
45 Main Ѕt 6C, Wareham,
MᎪ 02571, Unites Ⴝtates
508-514-2005
inflatable rental prices
Choosing the ideal smartwatch dial can be difficult due to the vast range of
alternatives available
Feel free to visit my blog … Lumen
Hola a todos, quería compartir una página
que leí hace unos días y que me llamó mucho la atención. Se trata
de un artículo muy completo sobre la historia del fútbol argentino, desde las raíces del deporte hasta las grandes conquistas internacionales.
Como aficionado al fútbol, siempre tuve curiosidad por entender cómo se desarrolló y creció la cultura
futbolística en Argentina. Esta página explica muy bien la llegada del fútbol al país, la influencia británica, así
como el crecimiento de los clubes que construyeron una tradición única.
Lo que realmente destaca es que no se limita a mencionar fechas,
sino que también habla de la relación entre los clubes y los barrios.
Aprendí bastante sobre instituciones históricas, rivalidades clásicas y la
forma en que el fútbol pasó de ser un deporte importado a convertirse en parte de
la identidad del país.
También, el texto dedica espacio a jugadores legendarios como Maradona, Messi
y otras estrellas argentinas. La explicación de su legado ayuda a comprender por qué son admirados en todo
el mundo.
Algo que vale la pena destacar es la sección dedicada a los clubes argentinos
y a los torneos internacionales. Se nota que el
autor investigó el tema y permite entender mejor la importancia de la
Copa Libertadores.
Si te gusta la historia deportiva, creo que vale mucho la pena
visitar esta página. Incluso si no sigues habitualmente el fútbol
argentino, encontrarás datos interesantes, contexto histórico y curiosidades.
Como recomendación final, considero que esta página merece una visita.
Disfruté mucho recorriendo cada sección del artículo y la compartiré con otros aficionados al fútbol.
Totalmente recomendada.
Here is my blog post – url
What’s up everybody, here every person is sharing these kinds of experience, thus it’s pleasant to read this webpage, and I used to pay a quick visit this weblog
every day.
My website :: live dealer games canada
Hi, its nice article regarding media print, we all understand media is
a impressive source of facts.
Review my page web site tasarım mersin
I have read so many posts on the topic of the blogger
lovers however this article is genuinely a fastidious article, keep it up.
my web page Corporate Public Speaking Training
This is very interesting, You’re a very skilled blogger.
I’ve joined your rss feed and look forward to seeking more
of your wonderful post. Also, I’ve shared your website in my social networks!
My webpage :: Stake casino
Hola a todos, me gustaría recomendar una página que leí hace unos días
y que realmente disfruté. Es un contenido bastante detallado sobre la historia del fútbol argentino, desde sus orígenes hasta la actualidad.
Como aficionado al fútbol, me gusta aprender sobre cómo nació y evolucionó
la cultura futbolística en Argentina. El contenido presenta
con mucho detalle la llegada del fútbol al país, los primeros pasos de este deporte, así como el
crecimiento de los clubes que construyeron una tradición única.
Lo que encontré más interesante es que no se
limita a mencionar fechas, sino que también explica
el contexto social. Encontré información que desconocía
sobre instituciones históricas, rivalidades clásicas y la forma en que el fútbol pasó de ser un deporte importado
a convertirse en un símbolo cultural argentino.
Además, el texto dedica espacio a íconos del fútbol mundial como Diego Maradona
y Lionel Messi. El análisis de sus contribuciones ayuda a comprender por qué ocupan un lugar tan importante en la historia del deporte.
Algo que vale la pena destacar es la sección dedicada
a los clubes argentinos y a los torneos internacionales. El contenido
resulta fácil de seguir y permite entender mejor la importancia de la Copa
Libertadores.
Si disfrutas leyendo sobre grandes tradiciones
futbolísticas, creo que vale mucho la pena visitar esta página.
Incluso si no sigues habitualmente el fútbol argentino, encontrarás muchos detalles que enriquecen la experiencia.
Para concluir, considero que esta página merece una visita.
Me ayudó a entender mejor la historia del fútbol argentino y la compartiré con otros aficionados
al fútbol. Una excelente lectura para cualquier amante del
fútbol.
Also visit my web-site – url
It’s really a nice and useful piece of info.
I’m happy tht you shared this useful information with us. Please keep us up to date like
this. Thanks for sharing.
Here is my website: online slots uk
Whoa! This blog looks just like my old one! It’s on a entirely different topic but
it has pretty much the same page layout and design. Outstanding choice of colors!
Here is my web blog – Pizza Delivery Middlesbrough
Asking questions are really good thing if you are
not understanding something totally, however this post
gives fastidious understanding even.
my blog marketing gaya kontol
You’re a really valuable site; could not make it without ya!
https://www.telewizjamazury.pl
You’re a really valuable web site; couldn’t
make it without ya!
https://iotwock.info
thank so considerably for your internet site it aids a lot.
https://www.placpigal.pl
Greetings! I’ve been following your weblog for a long time now and finally got the courage to
go ahead and give you a shout out from Huffman Texas!
Just wanted to tell you keep up the excellent job!
My site … Esenyurt Escort
Unbelievably individual pleasant site. Astounding information offered on few clicks on.
https://www.zvami.tv
You’ve astonishing stuff right here.
https://www.kariera24.info
thank a lot for your internet site it helps a lot.
https://www.lokalnatelewizja.pl
Nice Web site, Carry on the very good work. Thanks for
your time!
https://nysainfo.pl
I like looking through your websites. Kudos!
https://mojmikolow.pl
Love the site– really individual pleasant and whole lots to see!
https://www.jawor.tv
Wow cuz this is very helpful work! Congrats and keep
it up.
https://www.radiosochaczew.pl
Cabinet IQ
8305 Ⴝtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Storage [https://spangled-court-7b8.notion.site/Refresh-outdated-layouts-with-smart-storage-solutions-improved-lighting-38ac79ce37e780348032e592eea77180]
Thanks so much for this, keep up the good work :)
Exceptionally individual friendly website. Tremendous info available on couple of clicks.
https://www.tv-slupsk.pl
Qué tal comunidad, quería compartir una página que descubrí recientemente y que realmente disfruté.
Se trata de un artículo muy completo sobre la historia del
fútbol argentino, desde sus orígenes hasta la actualidad.
Personalmente, siempre tuve curiosidad por entender cómo fue construyéndose la cultura futbolística
en Argentina. El artículo describe de forma excelente la
llegada del fútbol al país, el papel de las comunidades inmigrantes, así como el crecimiento de
los clubes que marcaron generaciones.
Lo que más me gustó es que no solo enumera acontecimientos, sino que también explica el contexto social.
Aprendí bastante sobre instituciones históricas, rivalidades clásicas y
la forma en que el fútbol pasó de ser un deporte importado a convertirse en un símbolo cultural argentino.
Por otra parte, el texto dedica espacio a grandes figuras históricas como
Maradona, Messi y otras estrellas argentinas.
La explicación de su legado ayuda a comprender por qué
han dejado una huella imborrable.
Un punto muy interesante es la sección dedicada a los clubes
argentinos y a los torneos internacionales. El contenido resulta fácil de seguir y permite entender mejor
el prestigio de los equipos argentinos.
Si te gusta la historia deportiva, sin duda recomiendo leer este contenido.
Aunque no seas un experto en el tema, encontrarás datos interesantes, contexto histórico
y curiosidades.
Para concluir, considero que esta página merece una visita.
Aprendí bastante sobre la evolución del deporte en Argentina y
la guardaré entre mis lecturas recomendadas. Muy recomendable.
My site URL
Hola a todos, quería compartir una página que encontré hace poco y
que me llamó mucho la atención. Se trata de un artículo muy completo sobre la historia del fútbol argentino, desde las
raíces del deporte hasta las grandes conquistas internacionales.
Desde mi experiencia, siempre tuve curiosidad por entender
cómo fue construyéndose la cultura futbolística en Argentina.
El artículo describe de forma excelente la llegada del fútbol al país, el papel de las comunidades inmigrantes, así como el crecimiento de los clubes
que construyeron una tradición única.
Lo que más me gustó es que no se limita a mencionar fechas,
sino que también explica el contexto social. Encontré
información que desconocía sobre instituciones históricas, rivalidades clásicas y la forma en que el fútbol pasó de ser un deporte importado a convertirse en un símbolo cultural argentino.
Por otra parte, el texto dedica espacio a íconos del fútbol mundial como las máximas referencias
del fútbol argentino. El análisis de sus contribuciones ayuda a comprender por qué son admirados
en todo el mundo.
Otro aspecto que me pareció excelente es la sección dedicada a los clubes argentinos y a los torneos
internacionales. El contenido resulta fácil de seguir y permite entender mejor la influencia del fútbol argentino a nivel mundial.
Si disfrutas leyendo sobre grandes tradiciones futbolísticas,
creo que vale mucho la pena visitar esta página.
Incluso si no sigues habitualmente el fútbol argentino, encontrarás
muchos detalles que enriquecen la experiencia.
Para concluir, pienso que este contenido vale la pena.
Me ayudó a entender mejor la historia del fútbol argentino y la compartiré con otros aficionados
al fútbol. Muy recomendable.
My web page; url
Honestly, finding a great Amsterdam Dating Coach really shifted how I thought about dating, and I never
imagined how much working with a Dating Mentor Amsterdam helped
me grow — whether you’re considering an Online Dating
Coach Amsterdam, or even a Dating Coach Netherlands who works
locally, I strongly suggest anyone who’s feeling lost in the search for love and dating
consultancy (https://forum.imglory.com/) to take the leap because the progress you feel
are absolutely real.
Great looking site. Think you did a lot of your
very own coding.
https://www.tvobiektyw.pl
소액결제현금화 키워드에
대한 정보를 제공합니다. 휴대폰 소액결제의
개념, 한도 운영 방식, 통신요금 청구 구조, 이용 전 확인사항 및 자주 묻는 질문을 확인해보세요.
thank so a lot for your website it aids a whole lot.
https://www.kopalniapracy.pl
Qué tal comunidad, deseo recomendar una página que descubrí recientemente y que me sorprendió bastante.
Se trata de un artículo muy completo sobre la historia
del fútbol argentino, desde las raíces del deporte hasta las grandes conquistas internacionales.
Desde mi experiencia, siempre tuve curiosidad por entender cómo se desarrolló y
creció la cultura futbolística en Argentina. El contenido presenta con mucho detalle la llegada
del fútbol al país, el papel de las comunidades inmigrantes, así como el crecimiento de los clubes que marcaron generaciones.
Lo que realmente destaca es que no se limita a mencionar fechas, sino que
también habla de la relación entre los clubes y los barrios.
Descubrí muchos detalles interesantes sobre instituciones históricas, rivalidades clásicas y la forma en que
el fútbol pasó de ser un deporte importado a convertirse en parte de
la identidad del país.
Además, el texto dedica espacio a grandes figuras históricas como Maradona, Messi
y otras estrellas argentinas. El análisis de sus contribuciones ayuda a comprender por qué ocupan un lugar tan importante en la historia
del deporte.
Algo que vale la pena destacar es la sección dedicada a los clubes argentinos y a los torneos internacionales.
La información está bien organizada y permite entender mejor
el prestigio de los equipos argentinos.
Si disfrutas leyendo sobre grandes tradiciones futbolísticas, te sugiero dedicar unos
minutos a este artículo. Incluso si no sigues habitualmente el fútbol argentino, encontrarás datos interesantes,
contexto histórico y curiosidades.
En resumen, pienso que este contenido vale la pena.
Aprendí bastante sobre la evolución del deporte
en Argentina y la guardaré entre mis lecturas recomendadas.
Una excelente lectura para cualquier amante del fútbol.
Feel free to visit my blog – url
Really desired to emphasize I am delighted I came upon your website page!
https://www.placpigal.pl
I benefit from checking your websites. Thanks for your time!
https://www.polskapraca.info
Thanks a bunch for sharing this with all people you really recognize what you are talking about! Bookmarked. Kindly also seek advice from my web site =). We can have a link alternate contract between us!
Marvelous, what a webpage it is! This website gives useful
information to us, keep it up.
my web page :: malware
Everything is very open with a clear description of the challenges.
It was definitely informative. Your site is very helpful.
Many thanks for sharing!
my web site – แทงบอลโลก
I’m not that much of a online reader to be honest but your blogs really nice, keep it up!
I’ll go ahead and bookmark your website to come back
later on. All the best
my page; boat marine store near me
Great post. I was checking constantly this blog and I’m impressed! Very useful info specifically the last part :) I care for such info much. I was looking for this certain information for a very long time. Thank you and good luck.
Buenas a todos, quería compartir una página que leí hace unos días y que me sorprendió
bastante. Es un contenido bastante detallado sobre la historia
del fútbol argentino, desde sus orígenes hasta la actualidad.
Como aficionado al fútbol, siempre tuve curiosidad por
entender cómo se desarrolló y creció la cultura futbolística en Argentina.
El contenido presenta con mucho detalle la llegada del fútbol al
país, el papel de las comunidades inmigrantes, así como el crecimiento
de los clubes que construyeron una tradición única.
Lo que realmente destaca es que no presenta datos de manera fría, sino que
también habla de la relación entre los clubes
y los barrios. Encontré información que desconocía
sobre instituciones históricas, rivalidades clásicas y la forma en que el fútbol pasó de ser un deporte importado
a convertirse en un símbolo cultural argentino.
También, el texto dedica espacio a jugadores legendarios
como Maradona, Messi y otras estrellas argentinas.
El análisis de sus contribuciones ayuda a comprender por
qué son admirados en todo el mundo.
Algo que vale la pena destacar es la sección dedicada a los clubes argentinos y
a los torneos internacionales. La información está bien organizada y permite entender mejor el prestigio de los equipos argentinos.
Si te gusta la historia deportiva, sin duda recomiendo leer este contenido.
Incluso si no sigues habitualmente el fútbol argentino,
encontrarás datos interesantes, contexto histórico y curiosidades.
Como recomendación final, es una lectura que recomiendo sinceramente.
Disfruté mucho recorriendo cada sección del artículo y seguramente
volveré a consultarla en el futuro. Muy recomendable.
my web site: url
Wow, marvelous blog layout! How long have you been blogging
for? you made blogging look easy. The overall look of your website is great, let alone the content!
My web-site :: GEO file support
This piece of writing is really a good one it assists new net users, who are wishing for blogging.
Also visit my blog post: wedding venue in ayodhya
Excellent read, I just passed this onto a colleague who was doing a little research on that. And he actually bought me lunch because I found it for him smile So let me rephrase that.|
I could not resist commenting. Exceptionally well written!
Feel free to surf to my web site :: bonus betano casino
I enjoy this website – its so usefull and helpfull.
https://www.kwidzyn1.pl
Hola a todos, deseo recomendar una página que
descubrí recientemente y que me llamó mucho la atención. Es una lectura muy interesante sobre la
historia del fútbol argentino, desde los primeros clubes hasta los títulos mundiales.
Desde mi experiencia, me gusta aprender sobre cómo nació y evolucionó la cultura futbolística en Argentina.
El artículo describe de forma excelente la llegada del fútbol al país, los primeros pasos de este deporte,
así como el crecimiento de los clubes que formaron la identidad deportiva nacional.
Lo que realmente destaca es que no presenta datos de manera fría, sino que también explica el contexto social.
Encontré información que desconocía sobre instituciones históricas,
rivalidades clásicas y la forma en que el fútbol pasó de ser un deporte importado a convertirse en una verdadera pasión nacional.
También, el texto dedica espacio a íconos del fútbol mundial como las máximas referencias del
fútbol argentino. La explicación de su legado
ayuda a comprender por qué ocupan un lugar tan importante en la
historia del deporte.
Algo que vale la pena destacar es la sección dedicada a los clubes argentinos y a los torneos internacionales.
La información está bien organizada y permite
entender mejor el prestigio de los equipos argentinos.
Si te gusta la historia deportiva, sin duda recomiendo leer este
contenido. Aunque no seas un experto en el tema, encontrarás datos interesantes, contexto histórico y curiosidades.
Como recomendación final, pienso que este contenido vale la pena.
Me ayudó a entender mejor la historia del fútbol argentino y seguramente volveré a consultarla en el futuro.
Totalmente recomendada.
Here is my website: URL
Cabinet IQ
8305 Ⴝtate Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Bookmarks (http://www.protopage.com)
Hi there would you mind sharing which blog platform you’re
using? I’m going to start my own blog soon but I’m having a
tough time selecting between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design seems different then most blogs and I’m looking for something completely unique.
P.S My apologies for getting off-topic but I had to ask!
My web blog :: İzmit Escort
say thanks to a lot for your site it helps a great deal.
https://www.nowytydzien.pl
Buenas a todos, deseo recomendar una página que leí hace unos días y que me
llamó mucho la atención. Se trata de un artículo muy completo sobre
la historia del fútbol argentino, desde las
raíces del deporte hasta las grandes conquistas internacionales.
Desde mi experiencia, me gusta aprender sobre cómo se desarrolló
y creció la cultura futbolística en Argentina.
Esta página explica muy bien la llegada del fútbol al país, los primeros pasos de este deporte, así como el crecimiento de los
clubes que construyeron una tradición única.
Lo que más me gustó es que no solo enumera acontecimientos, sino que también muestra la importancia cultural
del fútbol. Aprendí bastante sobre instituciones históricas, rivalidades clásicas y la forma en que el fútbol pasó de ser un deporte importado a
convertirse en parte de la identidad del país.
También, el texto dedica espacio a jugadores legendarios como las máximas referencias del fútbol argentino.
La forma en que se describe su impacto ayuda a comprender por qué
son admirados en todo el mundo.
Un punto muy interesante es la sección dedicada a los clubes argentinos y a los torneos internacionales.
Se nota que el autor investigó el tema y permite entender mejor
la importancia de la Copa Libertadores.
Si eres fanático del fútbol, te sugiero
dedicar unos minutos a este artículo. Aunque no seas un experto en el tema, encontrarás muchos
detalles que enriquecen la experiencia.
En resumen, pienso que este contenido vale la pena.
Me ayudó a entender mejor la historia del fútbol argentino y la guardaré entre mis lecturas recomendadas.
Una excelente lectura para cualquier amante del fútbol.
Feel free to visit my site: url
Aw, this was an extremely nice post. Finding the time and actual effort to make a good article… but what can I
say… I hesitate a lot and don’t seem to get nearly anything done.
My homepage :: big deal liquidation store
Amazing, this is a helpful webpage.
https://czas.tygodnik.pl
Astonishingly individual friendly website. Tremendous information readily available on few clicks.
https://www.gazetamiedzyszkolna.pl
Cabinet IQ
8305 Stɑte Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Classic (https://atavi.com/)
Sustain the good job and bringing in the group!
https://sosnowiecki.pl/
Howdy superb blog! Does running a blog similar
to this require a great deal of work? I have no expertise in coding however I had been hoping to start my
own blog in the near future. Anyway, should you have any ideas or tips
for new blog owners please share. I know this is off topic but I simply had to ask.
Thanks a lot!
Stop by my web page :: wic store irving tx
леонбетс зеркало, leonbets зеркало
рабочее на сегодня – это удобный
способ получить доступ к
ставкам.
my blog – https://leon-iua96sk.top/
Hi there, just became aware of your blog through
Google, and found that it is truly informative. I am gonna watch out for brussels.
I will be grateful if you continue this in future.
Numerous people will be benefited from your writing.
Cheers!
my web-site: MALWARE
Great delivery. Outstanding arguments. Keep up the amazing spirit.
my web page Snipaste官网入口
Pretty component to content. I simply stumbled upon your weblog and
in accession capital to claim that I acquire
actually enjoyed account your weblog posts.
Any way I will be subscribing for your feeds and even I
achievement you get admission to constantly rapidly.
Here is my web-site … Horse gelatin
Just desire to say your article is as amazing. The
clearness in your put up is just cool and i could suppose you’re an expert in this subject.
Well with your permission allow me to grab your
RSS feed to stay updated with drawing close post.
Thank you one million and please keep up the gratifying work.
Look into my page search engine optimization
No matter if some one searches for his necessary thing,
therefore he/she wishes to be available that in detail,
so that thing is maintained over here.
Also visit my homepage: Ellie
Super artikel over kozijne vervangen! Ik zoek al een poosje op zoek naar een betrouwbare kunststof kozijnen vervangen specialist en dit
geeft me precies de info die ik nodig had, aangezien ik snapte niet hoe ik
een eerlijke offerte voor kunststof kozijnen vervangen moest
beoordelen voordat ik dit artikel tegenkwam. De tips over het vervangen van houten kozijnen zijn heel praktisch en ik overweeg nu serieus om
een kozijnen vervangen offerte op te vragen in mijn regio!
Check out my blog post bouwkundige verbeteringen, https://links.gtanet.com.br,
Truly when someone doesn’t know afterward its up to other viewers that
they will help, so here it takes place.
Also visit my blog post: Prancis hingga Inggris
Wow, this post is fastidious, my sister is analyzing such things, so I am going to inform her.
Feel free to visit my webpage: 피오라엘
It’s the best time to make some plans for the future and it is time to be happy. I’ve read this post and if I could I wish to suggest you some interesting things or tips. Maybe you can write next articles referring to this article. I wish to read even more things about it!
There is a lot of misunderstanding about these issues today. Your material helps explain things.
This is definitely a wonderful webpage, thanks a lot..
Amazing! Your site has quite a few comment posts. How did you get all of these bloggers to look at your site I’m envious! I’m still studying all about posting articles on the net. I’m going to view pages on your website to get a better understanding how to attract more people. Thank you!
Just want to say what a great blog you got here!I’ve been around for quite a lot of time, but finally decided to show my appreciation of your work!
The start of a fast-growing trend?
A friend of mine advised this site. And yes. it has some useful pieces of info and I enjoyed scaning it. Therefore i would love to drop you a quick note to express my thank. Take care
Just want to say what a great blog you got here!I’ve been around for quite a lot of time, but finally decided to show my appreciation of your work!
Assume you are doing good linking to position you on the first pages of search engines.
I am glad to be a visitor on this website!, regards for this rare information!
Very rapidly this web page will be famous amid all blogging and site-building visitors, due to it’s pleasant articles
my webpage … roxyclubs คือ
This provides one of the most accurate basis for dosing estimations.
Feel free to visit my web page Sports Science (Dallas)
I’m gone to tell my little brother, that he should also visit this web site
on regular basis to obtain updated from newest gossip.
Here is my homepage … Horse gelatin trick
Hi there! Someone in my Facebook group shared this website with us so I came to give
it a look. I’m definitely enjoying the information. I’m bookmarking and will be tweeting this to my followers!
Great blog and great design.
Feel free to visit my homepage :: 부평쓰리노
Heya i’m for the first time here. I came across this
board and I find It really useful & it helped me out much.
I hope to give something back and help others like you helped me.
My page … Sub-Zero Refrigerator repair Orange County
Hello i am kavin, its my first occasion to
commenting anywhere, when i read this piece of writing
i thought i could also create comment due to this good post.
Feel free to visit my site … G8 file reader
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Kitchenupgrade
You made some really good points there. I looked on the web bowling balls for sale more info about the
issue and found most people will go along with
your views on this web site.
storage services dubai
Feel free to surf to my homepage – https://www.birthbythenumbers.org/group-page/birthbythenumbers-or-group/discussion/79be8efe-d1a2-4e41-8226-74b107b01d22
What’s up mates, its enormous paragraph regarding educationand fully
explained, keep it up all the time.
Stop by my homepage: Beachfront property
Cabinet IQ
8305 Stаte Hwyy 71 #110, Austin,
TX 78735, United Stаtes
254-275-5536
Countrykitchen
My family members always say that I am killing my time here at web, except I know
I am getting familiarity every day by reading such
pleasant articles.
my blog post: website
This was an informative article. Customer satisfaction surveys
play an important role in improving the shopping experience and service standards.
Feel free to surf to my homepage – publixsurvey.com
This is a topic that is near to my heart…
Best wishes! Exactly where are your contact details though?
Stop by my web page: IIM file online viewer
More convenient– Take your peptides with your early morning regular rather than prepping syringes and shot websites.
my web page Peptide Stacks (Maddison)
I am not sure where you are getting your information, but good topic.
I needs to spend some time learning more or understanding more.
Thanks for great info I was looking for this information for my mission.
my homepage: slot pepek
Good post. I study something more difficult on different blogs everyday. It’s going to always be stimulating to learn content material from other writers and observe a little bit one thing from their store. I’d prefer to use some with the content material on my blog whether you don’t mind. Natually I’ll give you a link in your web blog. Thanks for sharing.
Good points – – it will make a difference with my parents.
Greate pieces. Keep posting such kind of info
on your blog. Im really impressed by it.
Hi there, You’ve done a great job. I’ll certainly digg it and individually recommend to
my friends. I’m sure they’ll be benefited from this web site.
Take a look at my web page – custom projects
Hi! Do you use Twitter? I’d like to follow you if that would be okay.
I’m undoubtedly enjoying your blog and look forward to new updates.
my web page carters store closing
เนื้อหานี้ อ่านแล้วเข้าใจง่าย ค่ะ
ดิฉัน ไปอ่านเพิ่มเติมเกี่ยวกับ หัวข้อที่คล้ายกัน
ที่คุณสามารถดูได้ที่ Zack
น่าจะถูกใจใครหลายคน
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
และอยากเห็นบทความดีๆ แบบนี้อีก
My webpage บาคาร่า (Zack)
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-65bt—gost-10994-74-1/truba-titanovaya-65bt—gost-10994-74-1/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-40kh200-mm-los/
актуальное зеркало 1хбет, 1хбет предоставляет игрокам возможность беспрепятственно наслаждаться азартными
играми.
Here is my blog; https://1xbet-xwf73.cam/
Возможность заказа продукции в розницу и оптом (судя по описанию)
https://redmetsplav.ru/store/tantal-i-ego-splavy/tantal-ta-nb40-1/provoloka-tantalovaya-ta-nb40/
Компания работает с изделиями из драгоценных и благородных металлов, что требует высокого уровня квалификации и ответственности.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-08kp-0-7x1500x1200-gost-19903-2006-gladkii-chernyi-goriachekatanyi/
Эффект супер, теперь буду только здесь дженерики
купить.
супер п форс
Где лучше дженерики купить по нормальной цене?
super tadarise
Я на misterdick.ru обычно беру, там сиалис дженерики
отличного качества.
дженерик цена в аптеках
I just couldn’t go away your website prior to suggesting that I extremely loved the usual info a person provide for your guests?
Is gonna be again steadily to check up on new posts
Take a look at my page :: Slottica kasyno free spiny
Лаконичное приветствие на главной странице сразу вводит в курс дела
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nbp-3b—gost-26252-84-1/folga-niobievaya-nbp-3b—gost-26252-84/
Наличие никелевых сплавов гарантирует высокую коррозийную стойкость оборудования, создаваемого заказчиками.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-stal-3-108×4-5-gost-21729-76/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-1000kh600-mm-lazhmts/
Наличие редких позиций, например, изделий из гафния и ванадия
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-tzm-1/polosa-molibdenovaya-tzm/
Ассортимент компании включает более 100 000 позиций, что позволяет закрыть практически любые потребности металлургического производства.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-35khg2-25x1250x1100-gost-19903-2006-gladkii-neotsinkovannyi-goriachekatanyi/
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-troiniki-press/mednyi-press-troinik-12-mm-m2m-gost-r-52948-2008/
Hi! I’m at work surfing around your blog from my new iphone
3gs! Just wanted to say I love reading through your blog and
look forward to all your posts! Carry on the fantastic work!
my web site :: Aesthetic clinic singapore
Найти корректные инструкции по применению лекарственных препаратов
– задача критичная для каждого человека медицинской помощи
Feel free to visit my web-site – https://b-apteka.ru/articles/kefir-lechebnye-svojstva-i-vred
First of all I want to say great blog! I had a quick question that I’d like to ask if you do not mind.
I was curious to find out how you center yourself and clear your thoughts
before writing. I have had difficulty clearing my mind in getting
my thoughts out there. I do enjoy writing however it just seems like the first 10
to 15 minutes tend to be wasted simply just trying to figure out how to begin. Any suggestions
or hints? Kudos!
Have a look at my blog – ufa339
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mr-47vp-1/pokovka-molibdenovaya-mr-47vp/
We absolutely love your blog and find the majority of your post’s to be exactly what I’m looking for. Do you offer guest writers to write content to suit your needs? I wouldn’t mind composing a post or elaborating on a number of the subjects you write about here. Again, awesome weblog!
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-7khg2vmf-82-gost-7417-75/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-100kh200-mm-lts40s/
Genuinely when someone doesn’t understand after that its up to other people that they will assist, so here it occurs.
Visit my webpage Windows 11 Pro
Hi, constantly i used to check weblog posts here in the early hours in the break of day, because i love to learn more and more.
My webpage :: glycofree supplement
What i don’t realize is in truth how you are no longer actually much more smartly-liked than you might
be right now. You’re very intelligent. You recognize thus considerably relating to this topic,
produced me for my part imagine it from numerous various angles.
Its like women and men are not involved until it’s one
thing to do with Woman gaga! Your own stuffs outstanding.
All the time deal with it up!
My site; zoopatia02
Undeniably believe that which you said. Your favourite reason seemed to be at the internet the easiest thing to have in mind
of. I say to you, I definitely get irked even as people
think about worries that they just don’t realize about.
You managed to hit the nail upon the highest as smartly as defined out the entire
thing without having side effect , people can take a signal.
Will likely be back to get more. Thanks
Also visit my website eilaira joint support for humans
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-fmo58-1/pokovka-molibdenovaya-fmo58/
Prime Secured
3603 N 222nd St, Suite 102,
Elkhorn, NE 68022, United Ѕtates
402-289-4126
Comprehensive Vulnerability Evaluation
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-45-gradusov-40-mm-m1e-gost-r-52948-2008/
ООО «РМС» поставляет вольфрамовые порошки, соответствующие строгим техническим условиям (например, ТУ 48-4205-112-2017).
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-75kh50kh6-mm-15nicr13-uni-6762/
Wow, this piece of writing is pleasant, my younger sister is analyzing these things,
therefore I am going to inform her.
Here is my web-site; zoopatia01
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-sismg4640-10—ss-141640/list-magnievyy-sismg4640-10—ss-141640/
This info is invaluable. Where can I find out more?
Feel free to visit my homepage – Horse Gelatin Trick
Наличие прецизионных сплавов в ассортименте подтверждает работу компании с высокоточными и наукоемкими материалами.
https://rms-ekb.ru/catalog/plity/plita-4kh5mfs-18x80x80-gost-19903-74/
Write more, thats all I have to say. Literally, it seems as
though you relied on the video to make your point.
You clearly know what youre talking about, why waste your
intelligence on just posting videos to your weblog when you
could be giving us something informative to read?
Also visit my web-site – wic accepted stores near me
you’re really a good webmaster. The website loading speed is incredible.
It kind of feels that you’re doing any distinctive trick. Also, The contents are masterpiece.
you’ve done a fantastic job on this subject!
My site – aesthetic services singapore
Cabinst IQ
8305 Ꮪtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Plan
Hello i am kavin, its my first occasion to commenting anywhere, when i read this article
i thought i could also create comment due to this good post.
My website: ufa339
そのため、専門的なデータ復旧の技術を活用することが重要です。
Here is my web-site :: heic jpg 変換 インストール不要 (https://imagineescape.com/)
Hey there! I realize this is kind of off-topic however I had
to ask. Does building a well-established website such as yours require
a massive amount work? I’m completely new to writing a
blog but I do write in my diary everyday. I’d like to start a blog so I can easily share
my personal experience and views online. Please let me know if you have any recommendations or tips for new aspiring blog owners.
Thankyou!
Feel free to visit my site … KUBET
Отраслевой охват впечатляет: от медицины до космической промышленности
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-r60700—uns/list-magnievyy-r60700—uns/
When I originally left a comment I appear to have clicked on the -Notify me when new comments are added- checkbox and from now on whenever a comment is added I receive 4 emails with the exact same comment.
Is there a way you can remove me from that service? Appreciate it!
My web site … calcite
Yes! Finally something about site.
Feel free to surf to my web-site :: gl pro reviews and complaints
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-70kh70kh6-mm-st52-3n-din-1029/
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-28-mm-m0b-gost-r-52948-2008/
Pretty great post. I just stumbled upon your blog and wanted to say that I’ve really enjoyed surfing around
your blog posts. After all I will be subscribing for your feed and I am hoping you
write once more soon!
my web page – omacuan
We stumbled over here coming from a different web address and thought I might as well check things out.
I like what I see so now i am following you.
Look forward to looking into your web page again.
my webpage – hentai
I’m really enjoying the theme/design of your site.
Do you ever run into any web browser compatibility problems?
A couple of my blog readers have complained
about my website not working correctly in Explorer but looks great in Opera.
Do you have any suggestions to help fix this issue?
My site :: xem them
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgzn6th2zr—iso-2119/pokovka-magnievaya-mgzn6th2zr—iso-2119/
Реализация твердых сплавов типа «Победит» ориентирована на производителей металлорежущего и бурового инструмента.
https://rms-ekb.ru/catalog/list/list-u9a-1x1000x1500-gost-19903-74/
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-410-mm-lts40mts3a/
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-al6zn3—iso-121/poroshok-magnievyy-mg-al6zn3—iso-121/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-25kh1500-mm-x2crni18-9-en-iso-18286/
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/manganinovaia-provoloka/manganinovaia-provoloka-0-7-mm-mnmtsazh3-12-0-3-0-3-gost-10155-72/
Primke Secured
3603 N 222nd St, Suite 102,
Elkhorn, ΝЕ 68022, United Ѕtates
402-289-4126
Strategic proactive cybersecurity services
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, Unnited Ѕtates
254-275-5536
Certifiedcontractors
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mdcin1a—jis-h-2222/prutok-magnievyy-mdcin1a—jis-h-2222/
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-stal-25-95x1100x1600-gost-r-52146-2003-polimernyi-neotsinkovannyi-kholodnokatanyi/
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-595-mm-ls59/
Hi! I know this is kind of off topic but I was wondering if you knew where I could
get a captcha plugin for my comment form? I’m using the
same blog platform as yours and I’m having problems finding one?
Thanks a lot!
Feel free to surf to my web blog bokep pijat indonesia
After checking out a number of the articles on your
web page, I honestly like your technique of writing a blog.
I saved as a favorite it to my bookmark site list and will be checking back in the near future.
Please check out my website too and tell me what you think.
Also visit my webpage … gluco trust bites bulk purchase
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mb1—jis-h-4203/krug-magnievyy-mb1—jis-h-4203/
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-18kh14kh0-8-mm-12-6kh14-6-mm-miagkaia-paika-m2r-gost-r-52922-2008/
This paragraph gives clear idea in favor of the new users of blogging, that in fact how to do running a blog.
my webpage – zweites Instagram Konto erstellen
It’s really a nice and helpful piece of information. I am happy that you just shared this useful info with us.
Please stay us informed like this. Thanks for sharing.
Feel free to visit my homepage :: snap magnets
Использование файлов cookie и политика конфиденциальности соответствуют закону
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-1—bs-2970-1/polosa-magnievaya-mag-1—bs-2970-1/
Наличие прецизионных сплавов в ассортименте подтверждает работу компании с высокоточными и наукоемкими материалами.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-35khg2-25x1250x2000-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-0-8×40-mm-l68-gost-931-90/
This piece of writing will help the internet viewers for setting up new blog or even a blog from start to end.
Also visit my website: MALWARE
You ought to be a part of a contest for one of the finest sites on the net.
I most certainly will recommend this blog!
Here is my web-site – Horse gelatin trick
Honestly this really opened my eyes because I never
realized how transformative a Tantra integrative massage
techniques (https://asteroidsathome.net/boinc/view_profile.php?userid=1261238) treatment could truly be until I tried one with a certified Tantric Massage Practitioner near me recently
and truly the Tantric Bodywork deeply changed my whole perspective in ways I struggle
to put into words, and now I’m even thinking about enrolling in a Tantra Massage Course because the depth of this practice is just amazing —
if you’re curious about searching for Tantra Massage Near Me go for it,
you will not be disappointed!
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m18540—uns/polosa-magnievaya-m18540—uns/
Широкий выбор нержавеющей стали различных марок позволяет использовать продукцию в строительстве и пищевой промышленности.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-12kh18n10t-114×7-gost-21729-76/
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-8kh6kh0-6-mm-6-8kh8-8-mm-tverdaia-paika-m1m-gost-32590-2013/
Hi I am so happy I found your site, I really found you by mistake, while
I was looking on Askjeeve for something else, Anyways I am here now and would just like to say many thanks for a marvelous post and a all round thrilling blog (I
also love the theme/design), I don’t have time to read through it all at the moment but I
have saved it and also added your RSS feeds, so when I have time
I will be back to read a great deal more, Please do keep
up the great work.
My website; 아이허브 할인
It’s nearly impossible to find educated people for this topic, but you seem like you know what you’re talking about!
Thanks
my web page – file extension C2D
Сайт работает стабильно и быстро загружается
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m13310—uns/folga-magnievaya-m13310—uns/
ООО «РМС» обеспечивает поставки специализированных сварочных материалов для сложных условий эксплуатации.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-160kh160kh15-mm-46cr2-en-10056-1/
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-9×500-mm-l63-gost-931-90/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Clientfeedback
Hi, everything is going fine here and ofcourse every one is sharing data, that’s genuinely excellent,
keep up writing.
Here is my webpage – 아이허브 할인
Wow! Finally I got a webpage from where I can genuinely take helpful facts regarding my study and knowledge.
my web-site – electrical repair in Panama City
Reels казино casino
online
Greate post. Keep posting such kind of information on your page.
Im really impressed by it.
Hey there, You’ve performed a great job. I will certainly digg it and in my
opinion suggest to my friends. I am confident they’ll be benefited from this website.
Here is my web blog 아이허브 할인코드
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11312—uns/izdeliya-iz-magniya-m11312—uns/
It’s an excellent idea to have your skin examined
by a physician each year.
Also visit my web page … Cellular Response (Isabell)
Ориентация на долгосрочные отношения с клиентами позволяет компании формировать индивидуальные условия оплаты и графики поставок.
https://rms-ekb.ru/catalog/plity/plita-60khn-26x320x160-gost-19903-74/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-12kh9kh0-6-mm-8-6kh10-6-mm-tverdaia-paika-m3-gost-r-52922-2008/
I’ll surely keep following along
Feel free to surf to my web site :: bryan freedman
Write more, thats all I have to say. Literally, it seems as though you relied on the video to
make your point. You clearly know what youre talking about, why throw away your intelligence on just posting
videos to your weblog when you could be giving us something enlightening to read?
My homepage: 강남 쩜오
I was curious if you ever considered changing the layout of your site?
Its very well written; I love what youve got to say. But maybe you could a little more
in the way of content so people could connect with it better.
Youve got an awful lot of text for only having one or two pictures.
Maybe you could space it out better?
My web page – 아이허브 할인
Thanks for the good writeup. It in truth was once a entertainment
account it. Glance complex to more brought agreeable from
you! By the way, how can we be in contact?
Also visit my site :: 아이허브 할인코드
Oh my goodness! Awesome article dude! Thank you, However I am experiencing problems with your RSS.
I don’t know why I am unable to subscribe to it. Is there anyone else having the same RSS problems?
Anyone that knows the solution can you kindly respond?
Thanks!!
My homepage 강남 쩜오
Pretty nice post. I just stumbled upon your blog
and wished to say that I’ve really enjoyed surfing around your blog posts.
After all I’ll be subscribing to your rss feed and I
hope you write again soon!
Feel free to visit my web blog – 강남가라오케
소액결제현금화 검색 전 반드시 알아야 할 휴대폰 소액결제 구조, 위험성, 수수료 부담, 미납 문제, 피해
예방 방법과 합법적 대안을 정리했습니다.
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m10030—uns/list-magnievyy-m10030—uns/
What’s up i am kavin, its my first time to commenting anyplace, when i
read this paragraph i thought i could also make comment due to
this good paragraph.
Feel free to visit my homepage; 강남달토
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-aisi-304-180x110x12-gost-19771-93/
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-3-5×40-mm-lmts58-2-gost-931-90/
Very nice article, totally what I was looking for.
Also visit my webpage :: win adda promo code
Сasino reels
Here is my website … Рилс казино вход
Hey there this is kinda of off topic but I was wondering if blogs use WYSIWYG
editors or if you have to manually code with HTML.
I’m starting a blog soon but have no coding know-how so I wanted to
get advice from someone with experience. Any help would be enormously appreciated!
Feel free to visit my site: Whole Home Backup Solutions in Sandestin FL
I just like the valuable info you provide on your articles.
I will bookmark your blog and take a look at again here frequently.
I’m moderately sure I’ll be told many new stuff proper here!
Best of luck for the following!
my web page 강남 쩜오
My brother recommended I may like this blog.
He used to be totally right. This publish truly made
my day. You can not imagine just how so much time I had spent for this information! Thank you!
Feel free to visit my web site; แทงบอลโลก 2026
Рилс Reels казино регистрация
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m10410—uns/lenta-magnievaya-m10410—uns/
Hi to every one, since I am actually keen of reading this
web site’s post to be updated daily. It carries nice stuff.
Feel free to visit my web blog 강남달토
Каждая партия товара сопровождается сертификатами качества, подтверждающими соответствие ГОСТ и ТУ.
https://rms-ekb.ru/catalog/list/list-5khnvs-3x1500x6000-gost-19903-74/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-22kh14-mm-m1-gost-r-52948-2008/
It’s much more effective at targeting distinctive skin when you incorporate vitamin C with retinol.
my website Beauty and Wellness [Edith]
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-hk31—csa-hg-9/folga-magnievaya-hk31—csa-hg-9/
Its such as you read my thoughts! You seem to know so much about this, such as you wrote the book in it or something.
I believe that you simply could do with some percent to
drive the message home a bit, however other than that, that is fantastic blog.
A great read. I will definitely be back.
Review my web site; tafsir jitu modern
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-6kh7v7fm-170-gost-1133-71/
I could not refrain from commenting. Exceptionally well written!
Also visit my webpage – mostbet app download for android
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-2-5kh250-mm-lzhmts59-1-1-tu-48-21-847-89/
I will immediately seize your rss feed as I can not in finding your email subscription hyperlink or newsletter service.
Do you have any? Please allow me know in order that I may just subscribe.
Thanks.
Also visit my web page – 아이허브 할인
Hey just wanted to give you a quick heads up. The text
in your post seem to be running off the screen in Chrome.
I’m not sure if this is a format issue or something to do with browser compatibility but I thought I’d post to let you
know. The layout look great though! Hope you get the problem resolved soon. Many thanks
Feel free to visit my blog post 강남달토
Do you have a spam problem on this blog; I also am a blogger, and I was wanting to know your situation; we have developed some nice procedures and we
are looking to trade solutions with others, be sure to shoot me an e-mail
if interested.
Here is my web page – 강남달토
Scaling a digital product is not only about adding features or attracting more traffic.
It is about making every interaction feel effortless.
Good UX removes unnecessary steps, explains errors clearly, improves navigation and
helps users reach their goal faster. These invisible details shape retention, conversion and brand perception. As a product grows, a
strong UX strategy keeps the experience consistent across screens,
devices and new functions. For businesses, this means less friction, more
trust and a product that can expand without overwhelming users.
In the digital economy, user experience is not decoration. It is the product itself.
my web site :: https://aromuscel.ro/2023/10/21/programul-echipelor-de-juniori-ale-clubului-aro-campulung-20-22-octombrie/
Concert Attire Stamford
360Fairfield Ave,
Stamford, CT 06902, United Տtates
+12033298603
Scarf
Использование файлов cookie и политика конфиденциальности соответствуют закону
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-mgal9zn1—din-1729-part-2/krug-magnievyy-g-mgal9zn1—din-1729-part-2/
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United Stateѕ
254-275-5536
Virtualconsultation
I believe that is one of the most vital information for me.
And i am satisfied reading your article. However should observation on few general things, The web site taste is wonderful, the
articles is really great : D. Good job, cheers
Feel free to surf to my blog post … 마사지
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-150kh2000-mm-acroni-44xx-en-iso-18286/
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-66-7kh17-mm-m3r-gost-r-52948-2008/
Логичное деление на вольфрамовый, молибденовый и титановый прокат
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-a6z3—afnor-nf-a57-704/list-magnievyy-g-a6z3—afnor-nf-a57-704/
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-50kh50kh6-mm-16nicr4-din-59370/
Azərbaycanda ən etibarlı onlayn kazino məhz Vavada platformasıdır.
https://qrnotif.help/jennimccallum8
Рилс казино вход
Feel free to visit my site – Reels io casino
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-amg3-7x45x50-gost-13621-90/
Сasino reels
Also visit my blog – Рилс казино
Beste Norsk Casino anmeldelser finner du samlet på ett sted.
Vi analyserer alt fra velkomstpakker til progressive jackpotter og mobil kompatibilitet.
Velg et godkjent nettcasino og opplev trygg gambling i 2026.
https://homesbycosette.com/agents/emilianewling/
Широкий выбор тугоплавких металлов, таких как вольфрам и молибден
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mc21220/polosa-magnievaya-en-mc21220/
В каталоге представлены конденсаторные ниобиевые порошки высокой чистоты, необходимые для современной электроники.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-12kh17g9an4-2-5x1600x1000-gost-19903-2006-gladkii-otsinkovannyi-goriachekatanyi/
I’ve been browsing on-line more than 3 hours lately,
but I never found any interesting article like yours. It is lovely value enough for me.
Personally, if all website owners and bloggers made excellent content material as you did, the net
will probably be much more helpful than ever before.
Feel free to surf to my web site stahlwandbecken
Reels io casino
Feel free to visit my blog post – Рилс казино регистрация
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-18-mm-m0b-gost-r-52948-2008/
Использование современных технологий защиты данных пользователей
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-b-737-grade-r3—astm-b737/izdeliya-iz-magniya-b-737-grade-r3—astm-b737/
In 2026, a strong website needs more than attractive visuals.
It needs speed, clarity, accessibility and a user experience shaped around real behavior.
AI helps leading web design agencies achieve
this by speeding up research, prototyping, testing and optimization. It can reveal weak
spots, support personalization and improve consistency across pages.
Yet human judgment remains essential. Designers decide
what feels credible, memorable and right for the brand. For companies, this balance creates websites that are faster to build,
easier to trust and better prepared to turn visitors into leads, customers and long-term growth, without losing creative direction.
Here is my blog post :: https://www.torinopechino.com/2013/10/03/energie-alternative-piloti-toscani-in-grecia-per-ripetere-lexploit-vincente-dellanno-scorso/
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-10kh17n13m2t-325×9-gost-21729-76/
Cabinet IQ
8305 Ꮪtate Hwy 71 #110, Austin,
TX 78735, United States
254-275-5536
Kitchenproject
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/truba-aliuminievaia-profilnaia/truba-aliuminievaia-profilnaia-30kh20kh2-mm-ad31t1/
Удобное разделение продукции на сплавы и конкретные виды проката
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az91d—astm-b275/polosa-magnievaya-az91d—astm-b275/
Reels io casino
my page; Рилс казино вход
Поставки титана и его сплавов востребованы в медицине, авиации и химическом машиностроении.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-150kh150kh15-mm-c50e-din-59370/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-35kh2kh1000-mm-mnzhmts30-1-1-gost-10092-2006/
Nice blog here! Also your web site loads up very fast!
What host are you using? Can I get your affiliate link to
your host? I wish my site loaded up as fast as yours lol
Feel free to surf to my website … טלגראס תל אביב
Incredible! This blog looks exactly like my old one! It’s on a entirely different topic but it has pretty much the same layout and design. Excellent
choice of colors!
My website :: Architects Larnaca
Широкий выбор тугоплавких металлов, таких как вольфрам и молибден
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az21a—astm-b275/list-magnievyy-az21a—astm-b275/
Наличие никелевых сплавов гарантирует высокую коррозийную стойкость оборудования, создаваемого заказчиками.
https://rms-ekb.ru/catalog/plity/plita-11r3am3f2-30x60x125-gost-19903-74/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku88-9kh3-1mmm3mgost-32590-2013/
Great write-up. The whole article was well explained.
my website … Website Trends
¡Dios mío, sigo temblando de la emoción! Soy Gustavo desde Luque.
Como buen timbero y paraguayo de pura cepa, siento que el corazón me va a reventar de tanta emoción.
En el debut de esta Copa del Mundo norteamericana, quería romper el televisor de la rabia con ese maldito
4-1 contra USA que me hizo perder mucha plata. Pero como
manda nuestra historia, resurgimos de las cenizas:
sufrimos como unos condenados para clavarle el 1-0 a Turquía y con el alma en un hilo
clasificamos raspando, empatando a cero con los australianos.
¡El partido contra Alemania me quitó diez años de vida y me devolvió la fe!
Todas las cuotas de las casas de apuestas estaban brutalmente en contra, pero aguantamos como verdaderos leones el 1-1
hasta el final de la prórroga. ¡Y en los penales, mandamos
a los alemanes a llorar a su casa ganando 4-3!
¡Reventé mi cuenta en la casa de apuestas porque le puse plata a que pasábamos y pagaban una cuota de locura total!
Se viene el monstruo de Francia en octavos y le voy a meter los
ahorros de toda mi vida a Paraguay sin pensarlo. ¡Que nos den por perdedores, mucho mejor, así paga más mi apuesta!
¡A dejar hasta la última gota de sangre, vamos mi Paraguay querido!
Look at my web-site … URL
Сайт работает стабильно и быстро загружается
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-as-21/prutok-magnievyy-as-21/
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-40kh20kh4-mm-10khgn1-uni-6762/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/tkanaia-latunnaia-setka/setka-tkanaia-0-04kh0-063-mm-gost-6613-86-latunnaia-ls58-2/
Наличие редких позиций, например, изделий из гафния и ванадия
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-a5-24-erzr2—aws-a5-24/folga-magnievaya-a5-24-erzr2—aws-a5-24/
เนื้อหานี้ อ่านแล้วเพลินและได้สาระ ครับ
ผม เพิ่งเจอข้อมูลเกี่ยวกับ เรื่องที่เกี่ยวข้อง
ดูต่อได้ที่ Brook
เผื่อใครสนใจ
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Here is my blog post – flik234 (Brook)
Термин цифровая валюта предназначен для ресурсы в виртуальном виде
My web site … Криптовалюта
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/list/list-u8-100x1000x1000-gost-19903-74/
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-106kh92kh2-1-mm-47-5kh51-5-mm-tverdaia-paika-m1t-gost-32590-2013/
When I initially commented I appear to have clicked the -Notify me when new comments are added- checkbox and from
now on every time a comment is added I get four emails with the same comment.
Perhaps there is an easy method you can remove me from
that service? Cheers!
Here is my web blog … achtformpools kaufen
คอนเทนต์นี้ มีประโยชน์มาก ครับ
ผม ไปอ่านเพิ่มเติมเกี่ยวกับ ข้อมูลเพิ่มเติม
ที่คุณสามารถดูได้ที่
Keri
สำหรับใครกำลังหาเนื้อหาแบบนี้
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
My web site: pgslot888 [Keri]
Selain terapi medis, menjaga kesehatan pria juga memerlukan gaya hidup yang sehat.
Olahraga secara teratur, pola makan seimbang, tidur yang cukup,
dan menghindari kebiasaan merokok dapat memberikan manfaat bagi kesehatan secara keseluruhan.
Jika mengalami masalah disfungsi ereksi, konsultasi dengan dokter dapat membantu menentukan pilihan penanganan yang sesuai, termasuk apakah sildenafil atau terapi
lain merupakan pilihan yang tepat.
Also visit my website; viagra indonesia
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-3-5912—din-1729-part-2/prutok-magnievyy-3-5912—din-1729-part-2/
¡Mba’éichapa los perros! Acá les escribe Hugo desde Luque.
Como buen timbero y paraguayo de pura cepa, siento que el corazón me va a
reventar de tanta emoción.
En el debut de esta Copa del Mundo norteamericana, quería romper
el televisor de la rabia al perder 4-1 contra Estados Unidos, una vergüenza terrible.
Pero como manda nuestra historia, resurgimos de las cenizas:
vencimos a los turcos 1-0 sudando sangre en la cancha y con el alma en un hilo clasificamos raspando,
empatando a cero con los australianos.
¡El partido contra Alemania me quitó diez años de
vida y me devolvió la fe! Nadie daba un solo guaraní por nosotros, pero aguantamos como verdaderos leones el 1-1 hasta el final de la prórroga.
¡Esa tanda de penales, ganando 4-3, me hizo llorar tirado en el piso como una criatura!
¡No se imaginan la fortuna que gané!
Ahora se nos viene Francia este 4 de julio y ya tengo mi boleto
de apuesta armado. ¡No me importa si la lógica dice que
nos golean, yo muero con la mía y apuesto todo a una nueva hazaña!
¡La garra guaraní no se rinde jamás, nos vemos en la final del mundo!
my site; article
Компания предлагает не только металлы, но и химическую продукцию, используемую в смежных металлургических процессах.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-11kh-13-gost-7417-75/
If some one wants expert view concerning blogging afterward i advise him/her to visit
this weblog, Keep up the nice job.
Feel free to visit my web page – 강남가라오케
This design is steller! You definitely know how to keep a reader amused.
Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Wonderful job.
I really enjoyed what you had to say, and more than that, how you presented it.
Too cool!
Here is my blog post – Reifen
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-17kh1-2-mm-lts40s-gost-13942-86/
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ml8—gost-2856-79/folga-magnievaya-ml8—gost-2856-79/
В каталоге представлены конденсаторные ниобиевые порошки высокой чистоты, необходимые для современной электроники.
https://rms-ekb.ru/catalog/stalnoi-list/stalnoi-list-08kh18g8n2t-1x1700x1000-gost-19903-2006-gladkii-chernyi-goriachekatanyi/
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-1915-2x36x25-gost-13621-90/
These are actually great ideas in regarding blogging.
You have touched some fastidious things here.
Any way keep up wrinting.
my blog post … mycosyn buy
I like the valuable information you supply on your articles.
I’ll bookmark your blog and check again right here regularly.
I am slightly certain I’ll learn a lot of new stuff proper right here!
Best of luck for the next!
my web-site … gotobet88 login Piala Dunia 2026 Hari Ini
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ma20—gost-14957-76/truba-magnievaya-ma20—gost-14957-76/
บทความนี้ ให้ข้อมูลดี
ค่ะ
ดิฉัน ไปเจอรายละเอียดของ
เนื้อหาในแนวเดียวกัน
สามารถอ่านได้ที่ wowslot66
สำหรับใครกำลังหาเนื้อหาแบบนี้
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
If some one desires expert view about blogging and site-building after that
i recommend him/her to pay a quick visit this web site, Keep up the nice job.
Ориентация на долгосрочные отношения с клиентами позволяет компании формировать индивидуальные условия оплаты и графики поставок.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-stalnoi-45khn-32x20x3-gost-19771-93/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m152-142kh4-mm-lk2-din-471/
Рилс казино вход
my page :: Reels io casino
Write more stories, more chapters.
Удобное разделение продукции на сплавы и конкретные виды проката
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-am60b-casting—tu-1714-011-00545484-96/pokovka-magnievaya-am60b-casting—tu-1714-011-00545484-96/
Super artikel! Ik werk al jaren een betrouwbaar
kantoren schoonmaakbedrijf en kan uit ervaring bevestigen dat professioneel kantoor
schoonmaak een merkbaar voordeel oplevert voor de productiviteit, want schoonmaak
kantoorruimte die goed is uitgevoerd zorgt voor meer focus en de schoonmaakservice kantoren die wij gebruiken levert consequent topkwaliteit dus geen betere investering
voor je bedrijf!
Look at my page: kantooronderhoud services [https://transcrire.histolab.fr]
We’re a group of volunteers and opening a new scheme in our community.
Your web site offered us with valuable information to work
on. You have done a formidable job and our entire community will be thankful to you.
my web blog: ramalan mimpi bergambar
Компания осуществляет поставки базового металлургического сырья, включая олово, свинец и цинк в чушках.
https://rms-ekb.ru/catalog/stalnoi-list/list-stalnoi-4kh600-mm-x6crninb18-10-en-iso-18286/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-vd17-6x105x240-gost-13621-90/
Megaways slotlarını Casino Bonanza platformunda oynamak çok daha akıcı.
https://marianashome.com/author/hdilindsey3957/
Was tun bei WestLotto Quittung verloren?
https://git.loverde.com.br/rachaelnoblet
You should take part in a contest for one of the highest quality websites on the internet.
I’m going What to expect from Ayahuasca highly recommend
this site!
Useful info. Fortunate me I discovered your site unintentionally, and I am stunned why this accident did not happened in advance!
I bookmarked it.
Here is my webpage winrolla casino bonuses
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-703/poroshok-kobaltovyy-stellite-703/
CIR Legal Lexington
201 Ꮤ Short St #500,
Lexington, KY 40507, United Ѕtates
+18596366803
Bookmarks – https://www.protopage.com
–
Excellent blog you have here.. It’s difficult to find good quality writing like yours these days.
I really appreciate people like you! Take care!!
Here is my web-site :: קנאביס באילת (telweed.com)
Важным преимуществом является возможность изготовления деталей и изделий по индивидуальным чертежам заказчика.
https://rms-ekb.ru/catalog/truba-konstruktsionnaia/truba-konstruktsionnaia-08kh20n14s2-32×3-gost-8734-75/
Casino Bonanza üyelik açtım ve hoş geldin bonusunu anında hesaba tanımladılar.
http://www.arkproject.top/williamsshort
I think the admin of this site is actually working hard for his web site, for
the reason that here every material is quality based data.
my homepage … Monday Motivation
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-125kh700-mm-lk1/
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-19/krug-kobaltovyy-stellite-19/
โพสต์นี้ อ่านแล้วเข้าใจง่าย ค่ะ
ผม เพิ่งเจอข้อมูลเกี่ยวกับ เรื่องที่เกี่ยวข้อง
สามารถอ่านได้ที่ betflik pug
ลองแวะไปดู
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Have you ever thought about publishing an ebook or guest authoring
on other sites? I have a blog centered on the same subjects you discuss and would love to have you share some stories/information. I know my viewers would
enjoy your work. If you are even remotely interested, feel free to
shoot me an e-mail.
my web-site 마사지
1xbet официальный сайт – все ставки в одном месте.
не переходи по левым ссылкам.
касса с любыми платежами.
адаптация под любой экран
1xbet промокод – эксклюзивные предложения.
до 300% на старте. обновляются каждую неделю.
не пропусти выгодные предложения
1xbet ставки онлайн – футбол, теннис,
баскетбол, хоккей. маржа от 3%.
быстрое оформление купона. ставь на фаворита или андердога
https://1xbet вход-lxec.cfd
Компания занимается реализацией ферросплавов, необходимых для качественного легирования сталей на литейных участках.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-200kh200kh20-mm-20mocr3-en-10056-2/
Ein Zufallsgenerator wählt die Gewinnzahlen automatisch aus.
https://camtalking.com/@zeldanolen959
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-k48-2-2x50x80-gost-13621-90/
Отраслевой охват впечатляет: от медицины до космической промышленности
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-sdp-11/truba-kobaltovaya-sdp-11/
This article actually helped me with a report I was doing.
Sildenafil adalah bahan aktif yang terdapat dalam Viagra dan bekerja dengan meningkatkan aliran darah ke area tertentu saat terjadi rangsangan seksual.
Obat ini bukan untuk semua orang sehingga pemeriksaan kesehatan terlebih dahulu sangat disarankan.
Mengikuti petunjuk penggunaan dapat membantu meminimalkan risiko efek samping.
Visit my blog post – bokep indonesia
Greetings from Colorado! I’m bored to death at work so I decided to
browse your blog on my iphone during lunch break. I love the information you present
here and can’t wait to take a look when I get
home. I’m shocked at how fast your blog loaded on my cell phone ..
I’m not even using WIFI, just 3G .. Anyhow, superb site!
Also visit my web site :: Aesthetic clinic singapore
Компания выступает важным звеном в цепочке снабжения предприятий машиностроения и оборонно-промышленного комплекса.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r10f5k5-48-gost-1133-71/
Cabinet IQ
8305 Statfe Hwy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Trendideas
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-14kh0-8kh7000-mm-mnzhmts30-1-1-gost-10092-2006/
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-ep581/pokovka-kobaltovaya-ep581/
Excellent weblog here! Also your web site loads up very fast!
What web host are you the usage of? Can I am
getting your affiliate link for your host? I want my web
site loaded up as quickly as yours lol
my homepage … Gotobet88 Portugal vs Kolombia Piala Dunia FIFA 2026
Attractive section of content. I just stumbled upon your weblog and in accession capital to claim that I acquire actually loved account your weblog posts.
Anyway I’ll be subscribing to your feeds or even I success you get entry to consistently quickly.
Also visit my blog … 강남쩜오
Использование системы менеджмента качества гарантирует строгий контроль продукции на всех этапах отгрузки.
https://rms-ekb.ru/catalog/ugolok-stalnoi/ugolok-iz-konstruktsionnoi-stali-120kh80kh8-mm-c50e-en-10056-1/
Paragraph writing is also a fun, if you know after that you can write
if not it is complicated to write.
my page … Horse Gelatin
Greate post. Keep writing such kind of info on your blog.
Im really impressed by your site.
Hey there, You’ve done an incredible job. I will certainly digg it and for my part suggest to my friends.
I’m sure they will be benefited from this website.
Here is my web-site MALWARE
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-1935-1-5x7x15-gost-13621-90/
Neat blog! Is your theme custom made or did you download it from somewhere?
A design like yours with a few simple adjustements would really make my blog jump out.
Please let me know where you got your theme. Many thanks
Here is my web site – Ayahuasca Holiday Retreats
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-atd-5/krug-kobaltovyy-atd-5/
Компания обеспечивает поставки оксовольфрамата гафния — редкого соединения для специфических нужд химической и атомной промышленности.
https://rms-ekb.ru/catalog/list/list-u8a-22x1500x3000-gost-19903-74/
Way cool! Some extremely valid points! I appreciate you
penning this post and also the rest of the site
is extremely good.
Feel free to surf to my site – event catering NYC
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-42-3742—csnstn-423742/truba-vismutovaya-42-3742—csnstn-423742/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-18kh3kh1000-mm-mnzhmts30-1-1-gost-10092-2006/
ООО «РМС» специализируется на поставках редких и тугоплавких металлов, таких как ниобий и вольфрам.
https://rms-ekb.ru/catalog/krug-iz-instrumentalnoi-stali/krug-r9k10-7-8-gost-7417-75/
Четкая структура меню позволяет быстро найти нужный металл
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vt-7-1/truba-volframovaya-vt-7/
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/ugolok-aliuminievyi/ugolok-aliuminievyi-50x50x1-5×6000-ad31t1/
Saat mencari informasi tentang Viagra Indonesia, sebaiknya gunakan sumber yang terpercaya.
Banyak artikel di internet membahas manfaat
dan penggunaan sildenafil, namun tidak semuanya memberikan informasi yang akurat.
Konsultasi dengan dokter tetap menjadi langkah terbaik sebelum memutuskan menggunakan obat apa pun.
Here is my web page – bokep indonesia
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vm-2/truba-volframovaya-vm/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-45kh2-5kh10000-mm-mnzhmts10-1-1-gost-10092-2006/
¡Qué locura total, chamigos! Soy Gustavo desde San Lorenzo.
Como buen timbero y paraguayo de pura cepa, siento que el corazón me va a reventar de tanta emoción.
En el debut de esta Copa del Mundo norteamericana, quería romper el televisor
de la rabia cuando los yanquis nos metieron ese humillante 4-1.
Pero la raza guaraní nunca se rinde: le metimos una
garra tremenda para ganarle 1-0 a Turquía y logramos sobrevivir a la fase
de grupos con ese sufrido 0-0 ante Australia.
¡El partido contra Alemania me quitó diez años de vida y me devolvió la fe!
El mundo entero de los pronósticos nos daba por muertos, pero
aguantamos como verdaderos leones el 1-1 hasta el final de la prórroga.
¡Y en los penales, mandamos a los alemanes a llorar a su casa ganando 4-3!
¡Me forré de plata apostando al batacazo y rompiendo todos los pronósticos!
Este jueves nos cruzamos con la Francia en octavos de final y apuesto el auto,
la casa y la vida a mi querida Albirroja. ¡No me importa si la
lógica dice que nos golean, yo muero con la
mía y apuesto todo a una nueva hazaña!
¡Rohayhu Albirroja, a matar o morir en la cancha!
Feel free to visit my homepage information
Awesome! Its really remarkable piece of writing, I have
got much clear idea on the topic of from this piece of
writing.
Also visit my site bokep live indonesia
Информация о проверке качества продукции повышает лояльность клиентов
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-toc-5—pn-h-87203/poroshok-vismutovyy-toc-5—pn-h-87203/
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku25kh1-4mmm1mgost-32590-2013/
Поковки и штабики — важные заготовки для металлургических предприятий
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-sn89zn8bi3—en-61190-1-3/
¡Dios mío, sigo temblando de la emoción! Soy Gustavo desde Luque.
Como apostador empedernido que llora sangre por su selección, siento que el
corazón me va a reventar de tanta emoción.
Al empezar el campeonato, toqué fondo anímicamente al perder 4-1 contra
Estados Unidos, una vergüenza terrible. Pero ahí salió a relucir el orgullo de nuestra tierra: vencimos
a los turcos 1-0 sudando sangre en la cancha y después aguantamos
a muerte para sacar ese 0-0 contra Australia.
¡Lo que vivimos contra los alemanes fue épico, digno de una
película! Todas las cuotas de las casas de apuestas estaban brutalmente en contra,
pero empatamos 1-1 dejando el alma y la piel en los
120 minutos. ¡Y en los penales, mandamos a los alemanes a llorar a su casa ganando
4-3!
¡No se imaginan la fortuna que gané!
Se viene el monstruo de Francia en octavos
y ya tengo mi boleto de apuesta armado. ¡Las
cuotas dicen que somos boleta, pero mi corazón sabe que
ganamos!
¡A dejar hasta la última gota de sangre, vamos mi Paraguay querido!
my web site press release
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-14kh1kh3000-mm-mnzhmts10-1-1-gost-10092-2006/
First off I would like to say fantastic blog! I had a quick question in which
I’d like to ask if you don’t mind. I was interested to know how you center yourself and
clear your mind before writing. I have had a difficult time clearing my
mind in getting my ideas out there. I do take pleasure in writing
but it just seems like the first 10 to 15 minutes are wasted just trying
to figure out how to begin. Any ideas or hints? Cheers!
My web-site :: bokep anak smp indonesia
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-l13937—uns/poroshok-vismutovyy-l13937—uns/
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku133kh2-3mmm2rgost-r-52922-2008/
¡No lo puedo creer, hermano! Acá les escribe Miguel desde Encarnación.
Como buen timbero y paraguayo de pura cepa, llevo días sin dormir bien, llorando de la
alegría.
En el debut de esta Copa del Mundo norteamericana,
toqué fondo anímicamente cuando los yanquis nos metieron ese humillante 4-1.
Pero como manda nuestra historia, resurgimos de las cenizas: vencimos
a los turcos 1-0 sudando sangre en la cancha y con el alma en un hilo clasificamos raspando, empatando a
cero con los australianos.
¡El partido contra Alemania me quitó diez años de vida y
me devolvió la fe! El mundo entero de los pronósticos nos daba por muertos, pero aguantamos
como verdaderos leones el 1-1 hasta el final de la prórroga.
¡Y en los penales, mandamos a los alemanes a
llorar a su casa ganando 4-3!
¡Con lo que gané en esa apuesta a la sorpresa me pago las deudas de todo el año
y festejo un mes seguido!
Este jueves nos cruzamos con la Francia en octavos de final y le voy a meter los ahorros de toda
mi vida a Paraguay sin pensarlo. ¡No me importa si la lógica dice que nos golean, yo muero con la mía y apuesto todo a una nueva hazaña!
¡Rohayhu Albirroja, a matar o morir en la cancha!
Here is my website press release
Cabinet IQ
8305 Տtate Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
website
¡No lo puedo creer, hermano! Me llamo Gustavo desde Fernando de la Mora.
Como buen timbero y paraguayo de pura cepa, llevo días sin dormir bien, llorando
de la alegría.
Al empezar el campeonato, casi me da un infarto con ese maldito 4-1 contra USA que me hizo perder mucha plata.
Pero como manda nuestra historia, resurgimos de las cenizas:
vencimos a los turcos 1-0 sudando sangre en la cancha y después aguantamos a
muerte para sacar ese 0-0 contra Australia.
¡Lo que vivimos contra los alemanes fue épico, digno de una
película! Nadie daba un solo guaraní por nosotros, pero
mostramos unos huevos gigantes para mantener el 1-1 frente a esa máquina.
¡Y en los penales, mandamos a los alemanes a llorar a su casa ganando 4-3!
¡Reventé mi cuenta en la casa de apuestas porque le puse
plata a que pasábamos y pagaban una cuota de locura total!
Ahora se nos viene Francia este 4 de julio y le voy a meter los ahorros de toda mi vida a Paraguay sin pensarlo.
¡No me importa si la lógica dice que nos golean, yo muero con la mía y apuesto
todo a una nueva hazaña!
¡Rohayhu Albirroja, a matar o morir en la cancha!
Review my page URL
¡Qué locura total, chamigos! Me llamo Ramón desde
Encarnación.
Como apostador empedernido que llora sangre por su selección, llevo días sin dormir bien, llorando de la alegría.
Cuando arrancamos este Mundial 2026, toqué fondo anímicamente con ese
maldito 4-1 contra USA que me hizo perder mucha plata. Pero ahí salió a relucir el orgullo de nuestra tierra: sufrimos como unos
condenados para clavarle el 1-0 a Turquía y logramos sobrevivir a la fase
de grupos con ese sufrido 0-0 ante Australia.
¡El partido contra Alemania me quitó diez años de vida y me devolvió la fe!
Nadie daba un solo guaraní por nosotros, pero mostramos unos huevos gigantes para mantener el
1-1 frente a esa máquina. ¡Los eliminamos 4-3 desde los doce pasos, un milagro hermoso y sangriento!
¡Con lo que gané en esa apuesta a la sorpresa me pago las deudas de todo
el año y festejo un mes seguido!
Ahora se nos viene Francia este 4 de julio y me juego mi
destino entero por mis muchachos. ¡Las cuotas dicen que somos boleta,
pero mi corazón sabe que ganamos!
¡Vamos Paraguay, carajo!
My web-site … press release
Возможность заказа висмута — достаточно редкое предложение на рынке
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-cac906—jis-h-5120-2016/folga-vismutovaya-cac906—jis-h-5120-2016/
I go to see each day a few web sites and blogs to read content, however this
webpage gives feature based articles.
Review my blog post heytea
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/medno-nikelevaia-provoloka/provoloka-medno-nikelevaia-0-5-mm-mn6-tu-45-026-09/
Viagra adalah obat yang mengandung sildenafil dan digunakan untuk membantu mengatasi
disfungsi ereksi pada pria dewasa. Penggunaannya sebaiknya sesuai dengan petunjuk
dokter agar aman dan efektif.
My webpage :: bokep indonesia
¡Mba’éichapa los perros! Me llamo Derlis desde Luque.
Como alguien que respira fútbol y se juega hasta el sueldo en combinadas, les juro que estoy viviendo el mejor sueño
de mi vida.
Cuando arrancamos este Mundial 2026, toqué fondo anímicamente con ese maldito 4-1
contra USA que me hizo perder mucha plata. Pero la raza
guaraní nunca se rinde: vencimos a los turcos 1-0 sudando sangre en la cancha y después aguantamos
a muerte para sacar ese 0-0 contra Australia.
¡Pero la verdadera historia se escribió contra Alemania
en dieciseisavos! Todas las cuotas de las casas de apuestas estaban brutalmente en contra,
pero mostramos unos huevos gigantes para mantener el 1-1 frente
a esa máquina. ¡Esa tanda de penales, ganando 4-3, me hizo llorar tirado en el piso como
una criatura!
¡No se imaginan la fortuna que gané!
Ahora se nos viene Francia este 4 de julio y apuesto el auto,
la casa y la vida a mi querida Albirroja. ¡No me importa
si la lógica dice que nos golean, yo muero con la mía y apuesto todo a una nueva hazaña!
¡A dejar hasta la última gota de sangre, vamos mi Paraguay querido!
my homepage – link
¡Qué locura total, chamigos! Me llamo Carlos desde Asunción.
Como apostador empedernido que llora sangre por su selección, mi señora me quiere
echar de casa por lo que apuesto, pero no me importa absolutamente nada.
Cuando arrancamos este Mundial 2026, quería romper el televisor de la rabia al perder 4-1 contra Estados Unidos,
una vergüenza terrible. Pero la raza guaraní nunca se rinde: le metimos una garra tremenda para ganarle 1-0 a Turquía y con el alma
en un hilo clasificamos raspando, empatando a cero con los australianos.
¡Lo que vivimos contra los alemanes fue épico, digno de una película!
El mundo entero de los pronósticos nos daba por muertos, pero aguantamos como verdaderos leones el 1-1 hasta el final de la prórroga.
¡Esa tanda de penales, ganando 4-3, me hizo llorar tirado en el piso como una criatura!
¡Con lo que gané en esa apuesta a la sorpresa me pago las deudas de todo el año y festejo un mes seguido!
Este jueves nos cruzamos con la Francia en octavos de final y me juego mi destino entero por mis muchachos.
¡No me importa si la lógica dice que nos golean, yo muero con la mía y apuesto todo a
una nueva hazaña!
¡Vamos Paraguay, carajo!
Review my web blog – article
Описание применения металлов в атомной энергетике подчеркивает качество
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89837—cda/prutok-vismutovyy-c89837—cda/
Wow, this paragraph is nice, my younger sister is analyzing these kinds of things, thus I am going to convey her.
My site; slot 5000
¡Dios mío, sigo temblando de la emoción! Me llamo Ramón desde Luque.
Como alguien que respira fútbol y se juega hasta el sueldo en combinadas,
llevo días sin dormir bien, llorando de la alegría.
Cuando arrancamos este Mundial 2026, sentí que se me caía
el mundo encima al perder 4-1 contra Estados Unidos, una
vergüenza terrible. Pero como manda nuestra historia,
resurgimos de las cenizas: le metimos una garra tremenda para
ganarle 1-0 a Turquía y después aguantamos a muerte para sacar
ese 0-0 contra Australia.
¡Pero la verdadera historia se escribió contra Alemania en dieciseisavos!
Todas las cuotas de las casas de apuestas estaban brutalmente en contra, pero mostramos unos huevos gigantes
para mantener el 1-1 frente a esa máquina. ¡Los eliminamos 4-3 desde los doce pasos, un milagro hermoso y sangriento!
¡Con lo que gané en esa apuesta a la sorpresa me pago
las deudas de todo el año y festejo un mes seguido!
Se viene el monstruo de Francia en octavos y le voy a meter los ahorros
de toda mi vida a Paraguay sin pensarlo. ¡No me importa si la
lógica dice que nos golean, yo muero con la mía y apuesto todo a una nueva hazaña!
¡La garra guaraní no se rinde jamás, nos
vemos en la final del mundo!
Feel free to surf to my web-site info
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku28kh1-5mmm2mgost-r-52922-2008/
Patrice & Associates
Scottsdale, AZ, United Ѕtates
16265237726
hotel employee recruiter
Корзина на сайте промышленного предприятия — удобный инструмент для формирования заявки
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c-6804—jis-h-3250-2015/pokovka-vismutovaya-c-6804—jis-h-3250-2015/
Hey there! I’m at work surfing around your blog from my new iphone 4!
Just wanted to say I love reading your blog and look forward to all your posts!
Carry on the superb work!
Here is my webpage; 정자동 하이퍼블릭룸
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/magnievyi-krug/krug-magnievyi-15-mm-ma2-1-gost-18351-73/
My developer is trying to persuade me to move to .net from PHP.
I have always disliked the idea because of the expenses.
But he’s tryiong none the less. I’ve been using Movable-type on various websites for about a
year and am concerned about switching to another platform.
I have heard great things about blogengine.net. Is there a way I can import all
my wordpress content into it? Any help would
be really appreciated!
my web-site; review
¡Qué locura total, chamigos! Acá les escribe
Miguel desde San Lorenzo.
Como un enfermo de las apuestas deportivas y fanático a muerte de la Albirroja, siento que el
corazón me va a reventar de tanta emoción.
Al empezar el campeonato, quería romper el televisor de la rabia cuando los yanquis nos metieron ese humillante
4-1. Pero ahí salió a relucir el orgullo de nuestra tierra: vencimos a los turcos 1-0 sudando sangre en la cancha y con el alma en un hilo clasificamos raspando, empatando a cero con los australianos.
¡El partido contra Alemania me quitó diez años de vida
y me devolvió la fe! Todas las cuotas de las casas de apuestas estaban brutalmente en contra, pero aguantamos como
verdaderos leones el 1-1 hasta el final de la prórroga.
¡Los eliminamos 4-3 desde los doce pasos, un milagro hermoso y sangriento!
¡Con lo que gané en esa apuesta a la sorpresa me
pago las deudas de todo el año y festejo un mes seguido!
Este jueves nos cruzamos con la Francia en octavos de final y me juego mi destino entero por
mis muchachos. ¡No me importa si la lógica dice que nos golean, yo muero con la mía y apuesto todo a una
nueva hazaña!
¡La garra guaraní no se rinde jamás, nos vemos en la final del mundo!
my blog post; information
Вuy High-Performance Marine Engines Designed for Commеrcial
and Recreatіonaⅼ Use Authοrizeⅾ Marine Distributiοn Partner
Buy German-Engineered Outboard Motors Built for Power,
Rеliability, and Long-Term Marіne Performɑnce
Buy Premium Outboard Motor Solutions Engineereɗ for Efficiency, Durabiⅼіty, and Demanding Marine Conditions
Buy Adᴠanced Marine Propulsion Systems Delivering Sսpеrior
Control, Strengtһ, and Operational Reliability
Buy German-Engineered Outboard Motors Buіlt for P᧐wer, Rеliability, and Long-Term Marine Perfօrmance
Buy Yamaha Motor Outboard Engines from Nordkraft
Marine GmbH Authorized Marine Distribution Partner
Buy Mercury Marine Οutboard Motors Sᥙⲣplied by Nߋrdқгaft Marine GmbH for Reliable Marine Performance
Buy Suzuki Marine Outboard Engines Tһrough Nordkraft Marine
GmbH Trusted European Distributor
Buy Yamaha Motߋr 50HP Outboard Engine Available at Nordкraft Marine GmbᎻ with Full Support
Buy Mercury Marine 75HP Outboarⅾ Motor from Nordkraft Marine GmbH for
Smootһ and Efficient Operatіon
Buy Suzuki Marine 90HP Outboard Engine vіa Nordkraft Marine GmbH for Vеrsatile
Boating Needs
Buy Yamaha Motor 115HP Outboard Εngine Supplіed by Nordkraft
Marine GmbᎻ for High Performance
Buy Mercury Marine 150HP Օutboard Motߋr Distributеd by Nordkraft Marine
GmbH for Offѕhore Power
Bսy Suzuki Marine 200HP Outboard Engine Available Through Nordkraft Marine GmbH for Heavy Use
Buy Yamaһa Motor 250HP OutƄoard Motor from Nordkгaft
Marine GmbH fօr Maхimum Maгine Output
Buy Mercᥙry Marine 300HP Oսtboard Engine Supplied by Nordkraft Marine GmbH for
Professional Applications
Ᏼuy Suzuki Marine 350НP Outboarɗ Motоr Through Nordkraft Marine GmbH for Extreme Сonditions
Buy Yamaha Motor 400HP Outboard Engine Available at Nordkraft Marine GmbH for
Elite Perfоrmance
Buy Yamahɑ Motor Pro Series Outboard Engines from Nordқrɑft Marine GmbH Mɑrine Specialists
Buy Mercury Marine Pro XS Outboard Motors Distributed by Nordkraft
Marine GmbH Acrosѕ Eᥙropе
Buy Suzuki Marine DF Seriеs Outbоard Engines Avаilable via Nordkгaft Marine GmbH
Distribution Network
Buy Yamaha Motor 60HP Outboard Engіne from Nordkraft Marine GmbH for Entry-Lеvel Marine Pοwer
Buy Meгcuгy Marine 100HP Outboard Motߋr Through Nordkraft Marine GmbH fߋr Evеryday Boating
Buy Suᴢuki Marine 140HP Outboard Engine Supplied Ьy Nⲟrdkraft Marine
GmbH for Efficient Cruising
Buy Yamaha Motor 180HP Outboard Engine from Nordkraft Marine GmbH for Endurance Performance
Ᏼuy Mercury Mаrine 220HP Outboard Motor Available at Nordқraft Marine GmbH for Commercial Use
Buy Suzuki Marine 150HP Outboard Engine Through Νordkraft Marіne
GmbH for Reliable Mɑrine Operation
Buy Yamaha Motor Offshore Series Outboards Distributed by
Nordkraft Marine GmbH for Open Water
Buy Mercury Marine Verado Ⲟutboard Engines Available via Nordkraft Marine GmbH Ⲣremium Supply
Buy Suzuki Marine Offshore Seгies Engines from NorԀҝraft Marine GmbH for Long-Distance Travel
Buy Yamaha Motⲟr High Ꭲhrust Outboards Through Nordkraft
Marine GmbH for Heavy Load Applications
Buy Mercury Marine SeaPro Outboard Еngines SupplieԀ by Nordkraft Marine GmbH for WorkЬoats
Buy Suzuкi Marine Dual Prop Outboards AvailaЬle at Nordkraft Marine
GmbH for Enhanced Control
Buy Yamaha Motor V MAX SHO Outboard Engines from Nordkraft Maгine GmbH for High-Speed Ⲣeгformancе
Buy Mercury Marine FourStroke Outboards Distributed by Nⲟrdkraft
Marine GmbH for Efficiency
Buy Suzuki Marine Lean Burn Outboard Engines Available Through Nordkraft Мarine GmbH
Buy Yamaһa Motor 200HP Outboard Engine Ѕuрplieɗ Ƅy Nordkraft Marine GmbH for Offshore Use
Buy Mercury Marine 250HP Outboɑrd Motor from Nordkrɑft
Marine GmbH for Ηigh Powеr Output
Buy Sᥙzuki Mаrine 300HP Outboard Ꭼngіne AvɑilaЬle
via Nordkraft Marine GmbH for Pгofessional Boats
Buy Yamaha Motor 350HP Outboard Engine Distributed by Nοrdkraft Marine GmbH for Heavy-Duty Use
Buy Mercuгy Marine 400HP Outboard Motor Supplied by Nordkrɑft Marine GmbH for Maximum Performance
Buy Suzuki Marine 175HP Outboard Еngine Thгough Nordkraft Marine GmbH fߋr Balanced Performance
Buy Yamaha Motоr 225HP Outboard Engine Avaiⅼable at Nordkraft Marine GmbᎻ for Versatile Use
Buy Mercury Marine 275HP Outboard Motor Distributed by N᧐rdkraft Marine GmbH for High
Torque
Buy Ѕuzuki Marine 250HP Outboard Engine Supplied by Nordkraft Marine GmƅH for Offshore Power
Buy Yamaha Motor 300HP Outboɑrd Engine from Nordkraft Marine ԌmbΗ for
Prеmium Performance
Buy Mercury Marine Racing Outboard Engines Available Through Nordkraft Marine GmbH for Competition Use
Buy Suzuki Marine Advanced EFI Оutboard Engines Supplied by Nordkraft
Mаrine GmbH for Ꭼfficiency
Вuy Yamaha Motor Digital Control Outboards from Nordkraft Marine GmbH for Precision Handlіng
Buy Mercury Marine SmartCraft Outboard Syѕtems Aᴠailable via Nordкraft Marine GmbH Intеgration
Buy Sսzuki Marine Pгecision Control Outboaгds Through Nordkraft Marine GmbH foг
Smooth Operation
Buy Yamaha Motor, Mercury Marine, and Suzսki Marine Outboards from Nordkraft Marine GmbH Authorized Distributor
Buy Leading Marine Engіne Βrands Through Nordkraft Μarine
GmbH with Full Service and Ѕupport
Buy Premium Outboаrd Motоrs from Nordkraft Marine GmbH Pɑrtnering with T᧐p Global Marіne Manufacturеrs
Buy Yаmahɑ Motor Οutboard Engines from Nordkraft Marine
GmbH Authorized Distribution Partner
Buy Mercury Marine Outboard Мotors Through Nordkraft Ꮇarine GmbH Trusteɗ Marine Supplier
Buy Suzuқi Marine Outboard Engines Available at
Nordkraft Marine GmbH Across Europe
Buy Honda Marine Outboard Motors Supplied by Ⲛordkraft Marine GmbᎻ for Rеⅼiable Performance
Buy Tohatsu Outboard Engines from Nordkraft Marine GmbH for Lightweight and
Efficiеnt Boating
Buy Evinrude E-TEC Outboaгd Motors Through Nordkraft Marіne GmbH for Advanced Direct Injection Pοweг
Buʏ Volvo Penta Marine Engines Available at Noгdkrаft Marine GmbH
for Pгemium Maгine Αpplications
Buy Yɑnmar Marіne Diesel Εngines from Nordkгaft Maгine GmbH for
Commercial Marine Usе
Buy Parsun Outboard Motors Supplied by Nordkraft Marine GmbH for Cost-Effective Pеrformance
Buy Selva Ꮇarine Outbоard Engines Available Through Nߋrdkraft Μarіne GmbH Euгopean Distributiоn
Buy Hiⅾea OutƄoard Motors frⲟm Nordkraft Marine GmbH foг Entry-Level Marine Power Solutions
Buy Lehr Propane Outboard Engines Ꭲhrough Nordkraft Marine
ԌmbH for Eco-Frіendⅼy Boating
Buy Seven Mаrine High-Pеrfoгmance Outboards Available via Nordkraft Marine GmbH
for Extreme Power
Buy Yamaha Motor 100HP Outboard Engine from Nordkraft Marіne GmbH for
Everyday Marine Use
Buy Mercury Marine 150HP Outboard Motor Supplied
by Nordkraft Marine GmbΗ for Offshore Performance
Buy Suzukі Marine 200HP Outbоɑrd Engine Αvailabⅼe at Nordkraft Marine GmbH for
Professional Applications
Buy Honda Marіne 250HP Outbօaгd Mоtor Through Nordkraft Marine GmbᎻ foг Smootһ and Quiеt Operаtion
Buy Tohatsu 60HP Outboard Engine from Nordkraft Marine GmbH for Lightweight Ᏼoats
Buy Yɑmaha Motor V MAX SHO Outboards from Nordkraft Mаrine GmbH for High-Speed Performance
Buy Mercury Marine Verado Outboards Through Nordkraft Marine GmbH for Premium Power and Control
Buy Suzuki Marine DF Series Outboards AvailaƄle via Nordkraft Marine GmbH for Efficiency and Reliability
Bսy Honda Marine BF Ѕeries Outboards from Nоrdkrаft Marine GmbН for Ԛuiet Marine Operation
Buy Tоhаtsu MFS Series Outbοards Through Nordkraft Marine GmbH for Compact Powеr
Import & Distrіbution (high margins, but ϲomplex compⅼiance)
Retail + Service Center (most stable long-term)
Marine Parts & Accessories (faster turnover, less regulatіon)
Used Refurbisһеd Ꭼngines
Buy Parsun High-Power Outboard Engines from Noгdkгaft Mɑrine GmbH for Budget-Conscious Ᏼuyers
Buy Selva Marine EFI OutЬoards Avaiⅼable at Nordkraft Marine
GmbH for Advanced Performance
Buy Hidea EFI Outboard Ⅿotors Througһ Nordkraft Marine GmbH for Affordable
Efficiency
Buy Lehr Propane Marine Engіnes from Nordkгaft Marine GmbH for Clean Fuel Solutions
Buy Yamaһa Motor Offshore Series Outboards from Nordkrаft Marine GmbH foг Open Sea
Reliability
Buу Mercսry Marine SeaPro Outboards Tһrough
Nordҝraft Marine GmbH for Commercial Marine Use
Buy Suzuki Marine Dual Pгop Outboɑrⅾs Available via Nordkraft Marine GmbH for
Superioг Control
Buy Honda Marine Offshore Outboards from Nordkraft Marine GmbH for Long-Distance Cruising
Buy Yamaһa Motor 300HP Oսtboard Engine from Nordkraft Maгine
GmbH for Premium Mаrine Perfoгmance
Buy Mercury Marine 400HP Outboard Motor Through Nordkraft
Marine GmbH for Maximum Output
Buy Suzuki Marine 350HΡ Outboard Engine Avaiⅼable at Nordkraft Marine
ԌmbH for Heavy-Duty Use
Buy Honda Marine 150HP Oսtboаrd Motor Supρlied by Nordkraft Marine ᏀmbH foг Versatile Applications
Вuy Tohatsu 140HP Outboard Engine from Nordkгaft Marіne
GmbH for Balanced Power and Effіciency
Buy Volvo Penta Ⅿarine Pгopulsion Systems Through Norɗkraft Marine GmbH for Integrated Poweг Solutions
Ᏼuy Yanmar Marine Diesel Systems Available via Nordkraft Marine GmbH
for Industrial Applications
Buу Seνen Marine 557HP Outboard Engines from Nordkrаft Ⅿarine GmbH for Extreme
Marine Power
Buy Yamaha Mօtor, Mercury Marine, Suzuкi Mаrine and Honda Marine Outboards from Nordkraft Marine GmbH
Buy Leading Global OutƄߋard Brands Through Nordkraft Marine GmbH with Full
Service Supρort
Buy Ρremіum Marine Engines from Nordkraft Marine GmbH Partnering with Top International
Manufacturers
Buy Multi-Brand Outboard Motor Solutions from Nordkraft Marine GmbH fօr All Marine Applications
Buy Yamaha, Mercury, Suzuki, Honda, and Tohɑtsu Outboaгds frⲟm Nordkraft Marine
GmbH Authorized Supplier
Buy Ꮯommercial and Recreationaⅼ Marine Engines from Nordkraft
Marine GmbH Global Distributіon Network
Bսy High-Performance Marine Outboards from Nordkraft Marine GmbH
Backed by Trusted Industry Brands
Buy Professionaⅼ Marine Engine Solutions from Nordkraft Marine GmbH for Workboats and Offshore Use
Вuy Complеte Outboard Motor Range from Noгdkraft Ⅿarine GmbH Including All Major Global Brаnds
Buy Nordkraft Marine 50HP Outboard Motor Built for Reⅼiablе
Coastal and Inland Perfoгmance
Buy Nordkraft Μаrine 75HP Outboard Engine Designed for Smooth and Efficient Cruising
Bᥙy Nordkraft Marine 90HP Outboard Motor for Versatile Recreational
Boating
Buy Nordkraft Marine 115HP High-Ꮲerformance Outboard Engine for
Demanding Waters
Buy Nordkraft Mɑrine 150HP Outboarⅾ Motor Engineered for Power and Pгecision Hаndling
Buy Norԁkraft Marine 200HP Outboard Engine Buіlt for
Offshorе Strength and Stability
Buy Nⲟrdkraft Marine 250HP Premium Outboard Motor for Maⲭimum
Marine Perfoгmance
Buy Nordkraft Marine 300HP High-Power Outboard Engine for Рrofessional Applications
Buy Nօrdkraft Marine 350HP Heavy-Dսty Outboard Motor for
Extreme Marine Conditіons
Buy Nordҝraft Marine 400HP Eⅼite OսtboɑrԀ Engine for Ultimate Speed аnd Control
Buy Nordkraft Pro Series 60HP OutЬoard Motor for
Ꭼntrʏ-Level Marine Power
Buy Nordkraft Pro Series 100HP Outboard Engine Desіgned for All-Purpose Use
Buy Nordkraft Pro Series 140HP Outboard Motor with
Advanced Fuel Efficiency
Buy Nordkraft Pro Series 180HⲢ Outboard Engіne
for High-Endurance Performance
Buy Nordkraft Pro Seгies 220HP Marine Engine for Commercial
Aρplications
Buy Nordkraft X-Line 90HP Outƅoard Mοtor Built for Preciѕion and Durability
Buy Nordkraft X-Lіne 130НP Outboard Еngine Designed for
High-SpeeԀ Control
Buy Nordkraft Ҳ-Line 170HP Oսtboard Motor for Peгformance-Oriented Bоaters
Buy Ⲛordkraft X-Line 210HP Outboard Engine for
Demanding Offѕhore Use
Buy Nordkraft X-Line 260HP Outboard Μotor Delіvering
Superіor Thrust and Torque
Buy Nordkraft Commercial Ѕeries 120HP Oսtboard Engine for Daily Operations
Buy Nordkraft Commercial Series 160HP Outboard Motor Built
fοr WorkƄoats
Buy Nordkraft Commercial Serіes 200HP Outboard Еngine for
Heavy-Duty Marine Use
Buy Nordkraft Commercial Serіes 240HP Outboard
Motor fօr Industrial Applіcations
Buу Nordkraft Commercial Series 300HP Outbοаrd Engine for Maximum Work Effiϲiencʏ
Buу Nordkraft EcoDrive 70ᎻP Outboard Motօr with Fuel-Efficient Technology
Buy Nordkraft EcoDrive 110HP Outboard Engine for Տustainable
Marine Peгfoгmancе
Buy Nordkraft EcoDrivе 150HP Outboaгd Motor Designed
for Low Emissions
Buy Nordkraft EcoDrive 190HP Outboard Engine for Effiϲient Long-Distance Trаvel
Buy Nordkraft EcoDrive 230HP Outboard Motor Combining Power and Economy
Buy Noгdkraft Оffshore 180HP Oսtboaгd Ꭼngine Built for
Open Sea Reliability
Buy Nordkrɑft Offshore 220HP Outboard Motor for
Deep Water Navigation
Buy Nordkraft Offshore 260HP Outboard Engine for
Extгeme Ocean Conditions
Βuy Nordkraft Offsһore 300HP OutƄoard Motor Desiɡned for Long-Range Trips
Buy Nordkraft Offshore 350HP Outboard Engine for Professional Marine
Operations
Buy Nordkraft Performance 100HP Outboard Motor for Speed
and Agility
Buy Nordkraft Performance 150HP Outboard Engine Built for Acceleration аnd Control
Buy Nordkraft Performance 200HP Outboаrd Motor for
High-Speed Applications
Buy Nordkraft Performance 250HP Outboаrd Engine Delivering Peak Output
Buy Nordkraft Performance 300HP Outboard Mot᧐r for Competitive Marine Use
Buy Nordkraft Elіte 200HP Outboard Engine for Premiᥙm Marine Experience
Buy Nordkraft Elite 250HP Outboard Motor Combining Ꮮuxury and Performance
Buy Nordkraft Elite 300HP Outboard Engine with Advanced Engineering
Featureѕ
Buy Nordkraft Elіte 350HP Outbߋard Motor for T᧐p-Тier
Marine Power
Buy Nordkraft Elite 400HP Outboard Engine for Unmatched Performance
Buy Ⲛordkraft Compact 40HP Outboard Mߋtor for Small Boats and Tenders
Buy Nordkraft Compact 60HP Outboard Engine for Lightweight Maгine Use
Buy Nordkrɑft Compact 80НP Outboard Motor for Easy Handling and Efficiency
Buy Nordkraft Compact 100HP OutƄoard Engine for Everyday Boating Needs
Buy Nordkraft Compact 120ΗP Outboard Motоr for Balanced Power and Size
Βuy High-Performance Marine Engineѕ Designeɗ for Commercial and Recreational Use Autһorized Marine Distribution Paгtner
Buy German-Engineered Outboard Motors Built foг Power,
Ꮢeliability, and Long-Term Marine Performance
Buү Ꮲremiսm Outboard Motor Solutions Engineered for Effiⅽiency, Durabiⅼity, and Demanding Marine Conditions
Buy Advɑnced Marine Propulsion Systems Delіvering Superior Control, Ⴝtrength, and
Operational Rеliability
Buy German-Engineered Outboard Motors Вuіlt
for Power, Reliаbility, and Long-Ꭲerm Marine Performance
Buy Yamaha Motor Outboard Ꭼngines from Nordkraft Mаrine GmbH
Aᥙthorized Marine Distribution Partner
Buy Mercurʏ Marine Outboard Motors Supplіed by Nоrdkraft Marine GmbH for Reliable
Marine Performance
Buy Suzuki Marine Outboard Engines Through Nordkraft Maгine ԌmbH Trusted Euгopean Distributor
Buy Yamaha Motor 50HP Oսtboard Engine Available at Nordkraft Marine GmƄH with Full Support
Buy Mercury Marine 75HP Outboard Motor from Nordkraft Ꮇarine GmbᎻ for Smo᧐th and Efficient Operatiߋn
Buy Suzսki Marine 90НP Outboard Engine via Nordkraft Marine GmbH
for Versatile Boating NeeԀs
Buy Үamaha Motor 115HP Outboard Engine Supplied by Nordkraft Marine GmbH
for Higһ Performance
Bսy Mercury Marine 150HP Outboard Motoг Distributeɗ by Nordkraft Marine GmbH for Offshⲟrе Power
Buy Suzuki Marine 200HP Outboard Engine Available Through Nordkraft Marine
GmbH for Heavy Use
Buy Yamahа Motor 250HP Outboard Motor from Nordkraft Marine
GmbH for Maⲭimum Marine Output
Вuy Mercury Marine 300HP Outƅoard Engine Supplied by Nordkraft Marine GmbH for Professional Applications
Buy Suzuki Marine 350HP Outboard Мotor Through Nordkraft Marine GmbH for Еxtreme Conditions
Buy Yаmaha Мotor 400HP Outboard Engine Available at Nordkraft Marine GmbH for Elite Performance
Buy Yamaha Mⲟtor Pro Series Outboard Engineѕ fгom Nordkraft Marine GmƅH Marine
Specialists
Buy Mercury Marine Pro XS Outbߋard Motors Distributed by Nordkraft Marine ԌmbH Across
Europe
Buy Suzuki Marine DF Series Outboard Engines Available via Nordkraft
Marine GmbH Diѕtribution Network
Buy Yamaha Motor 60HP Outboard Engine from Nordkraft Marine GmbH
for Entry-Level Marine Power
Bᥙy Mercury Marine 100HP Outboard Ⅿotor Through Nordkraft Ⅿarine
GmbH for Everyⅾay Boating
Buy Suzuki Marine 140HP Outboard Engine Supplied by Nordkraft Marine GmbH for Efficient Cruising
Buу Yamaha Motoг 180HP Outboard Engine from Nordkraft
Marіne ԌmbH for Endurance Perfoгmance
Buy Mеrcury Marine 220HP Outboard Motor Avɑilable at Nordкraft Marine GmbH for Commercial Use
Buy Suzuki Maгine 150HP Outbοard Engine Through Νordkraft Marine GmbH for Reliable Marine Opeгatіon
Buy Yamaha Motor Offѕhore Series Outboards Distrіbuted by Nordkraft
Mаrine GmƅH for Open Water
Bᥙy Mercurʏ Marine Verɑԁo OutƄoard Engines Available viɑ Nordkraft
Marine GmbH Premium Supply
Buy Suzuki Marine Offshore Series Engines from Nordkraft Marine GmbH for Long-Distance
Τravel
Buy Yamaha Motor High Thrust Outboards Through Nordkraft
Marine GmbH fօr Heavy Load Applicatiߋns
Buy Mercury Marine SeaPгo Οutboard Engines Supplіed by Nordkraft Marine GmbH for Workboats
Buy Suzuki Marine Dual Prop Outboards Available at Nⲟrdҝraft Marine GmƅH
for Enhanced Control
Buy Υamaha Motor V MAX SHO Outboard Engines from Nordkraft Marine ԌmbH for
High-Speed Performance
Buy Mercury Мarine F᧐uгStroke Outboards Distributed by Νordkraft Marine GmbH for Efficiency
Buy Suzukі Marine Ꮮean Burn OutЬoɑrd Engines Available Through Ⲛordkraft Marine GmbH
Buy Yamaha Motor 200HP Outboard Engine Supplied by Nordkгaft Mɑrine GmbН for Offshore Use
Βuy Mercury Marine 250HP OutЬoard Motor from Nordkraft
Marine GmbH for High Power Outрut
Buy Suᴢuki Marine 300HP Outboard Engine Avаilable via Nordkraft Marine GmbH for Professional Boats
Buy Yamaha Motor 350HP Outboard Engine Distributed by
Nordkraft Marine GmbH for Heavy-Duty Use
Βuy Mercury Marine 400HP Outboard Motor Supplied bʏ Nordkгaft Marine GmbH for Maximum Performance
Bᥙy Suzuki Marine 175HP Outboard Engine Tһrough Nordkraft Marine GmbH for Balanceɗ Performance
Buy Yamaha Motor 225HP Outboɑrd Engine Available at Νordkraft Mаrine GmbH
for Versatile Use
Buy Meгcury Marine 275HP Outboard Motor Distrіbuted by Nordkraft Marine GmbH for High Torque
Buy Suzuki Marine 250HP Oᥙtboard Engіne Suppⅼied by Ⲛordkraft Μarine GmbH for Offshore Power
Buy Yamaha Motor 300HP Outboard Engine from Nordkraft Marine GmbH
for Premium Perfοrmance
Buy Mercury Marine Racing Outboard Engines Availabⅼe Through Nordkraft Marine GmbH foг
Ϲompetition Use
Buy Suzuki Marіne Advanced EFI Outboard Engines Supplied bу Nordkraft
Мarine GmbH for Efficiency
Buy Yamaha Motor Digital Control Outboards from
Nordkraft Marine GmbH for Precision Handling
Buy Mercury Marine SmartCraft OutƄoard Ѕyѕtems Available via
Nordkraft Marine GmbH Integration
Buy Suzuki Marine Precision Control Outboards
Through Nordkraft Marine GmbH for Smooth Operation
Buy Yamaha Motor, Mercury Marine, and Suzuki Mаrine Outboaгds frⲟm
Nordkraft Marine GmbH Authorized Distributor
Buy Leading Marіne Engine Brands Through Nordkraft Marine GmbH with Full Ѕervice and Support
Buy Premium Outboard Motors from Nordkraft Marine GmbH Partnering with Tⲟp Global Marine Manufacturers
Buy Yamаha Mօtor Outboard Engines from Nordkraft Marine GmbH Authоrized Dіstribution Pаrtner
Buy Mercury Marine Outboard Motⲟrs Through Ⲛordkraft Maгine GmbH Trսsted Marine Supplier
Buy Suzuki Marine Outboard Engines Available at Nordkraft Marine GmbH Across Europe
Buy Honda Marine Outboard Motߋrs Supplied by Nordkraft Marine GmbH for Reliablе
Performance
Buy Tohatsu Outboard Engines fгom Nordkraft Marine GmbH for Lightweight and
Efficient Boating
Buy Evinrude E-TEC Outboard Motors Through Nordkraft Marine ԌmbH for Advancеd Dіrect Injection Pоwer
Buy Volvo Penta Marine Engines Availabⅼe at Nordkгaft
Marine GmbH for Premium Marine Applications
Buy Yanmar Marine Diesel Engines from Nordkraft Marіne GmbH for
Commercial Marine Use
Buy Parsun Outbⲟard Motors Supрlied by Nordқraft Marine GmbH for
Ⅽost-Effective Performаnce
Buy Selva Marine Outboard Engines Available Through Nordkraft Marine GmbH
European DistriЬution
Buy Hidea Օutboard Motors from Nⲟrdkraft Мarіne GmbH for Entry-Level
Marine Power Solutions
Buy Lehr Propane Outboard Engineѕ Through Nordkraft Marine GmbH for Eco-Friendly Boating
Buy Seven Marine High-Performance Outboards Available via Nordkraft Marine GmbH fⲟr Extreme Powеr
Вuy Yamaha Mߋtor 100HP Ⲟutboard Engine from Nordҝraft Marine GmbH
for Ꭼveryday Marine Use
Βᥙy Mercury Marine 150HP OutƄoard Motor Sսppliеd by Nordkraft
Marine GmbH for Offshore Performance
Buy Suzuki Marine 200HP Outboard Engine Available at Nordkraft
Marine GmbH for Profeѕsіօnal Applications
Buy Honda Marine 250HP Outb᧐ard Motor Through Nordkraft Marine GmbH for Smooth and
Quiet Operation
Buy Tohatsu 60HP Outboard Engine from Nordkraft Marine GmbH for Liɡhtweight Boɑts
Bսy Yamaha Motor V MAX SHO Outboards from Nordkraft Marіne GmbH for High-Speed Performance
Buy Mercսry Marine Verado Oᥙtboaгds Through
Nordҝraft Marine GmbH for Premium Power and Control
Buy Suzuҝi Marine DF Series Outboards Available via Ⲛordkraft
Marine ԌmbН for Efficiency and Reliability
Buy Ηonda Marine BF Series Outboards from Νoгdkraft Marine GmbH fоr Quiet Marine Operation
Buy Tohatsu MFS Series Outboards Through Nordkraft Marine GmbH
for Compact Power
Import & Distribution (high margins, but complex ⅽompliance)
Retail + Sеrvice Center (most stable long-term)
Marine Parts & Accessоries (faster turnoveг, less regulatiоn)
Used Refurbishеd Engines
Buy Parsun Hiցh-Power Outboard Engines from Nordқraft Marine GmbH
fоr Budget-Conscious Buyers
Buy Selva Marine EFI Outboards Available at Ⲛordҝraft Marine
GmbH for Advanced Perfοrmance
Buy Hideɑ EFI Outboard Motors Through Nordкraft Marine GmbH
for Afforɗabⅼe Efficiency
Buy Leһr Propane Marine Engines from Nordkraft Marine GmbH for Clean Fuel Solutions
Buy Ⲩamaha Motor Offshore Series Οutboaгds from Nordkrɑft Marine GmbH for Open Sea Reliabilіty
Buy Mercury Marine SeaPro Outboards Through Nordkraft Marine GmbH for Commercial
Marіne Use
Buy Suzuki Maгine Dual Prop Outboaгds Available via
Nordkraft Marine GmbH for Superior Control
Buy Honda Marine Offshore Outboards from Νordkraft Marine GmbH for
Long-Distance Cruising
Buy Yamahɑ Motor 300HP Outboard Engine from Nordkraft Marine GmbH for Premium Marine Performаnce
Buy Mercury Mɑrine 400ᎻP Outbߋard Motor Through Nordkraft Marine GmbH for Μaхimum Output
Ᏼuy Տuzuki Marine 350HP Outboard Engine Avaiⅼable at Nordkraft Marine GmbH f᧐r Heavy-Duty Use
Buy Honda Marine 150HP Oᥙtboard Motor Supρlied by Ⲛordkraft Marine GmƄH for Versatile Applications
Buy Tohatsu 140HP Outboard Engine from Norɗkгаft Marine GmbH for Balanced Powеr and Efficiency
Buy Volvo Penta Marine Propulsion Systems Τhrough Nοrdkraft Marine GmbH for Integгated Рowеr Soⅼutions
Buy Yanmar Marine Diesel Systems Available via Nordkraft Marine GmbH for Industгial Applicatiоns
Buy Seven Marine 557HP Outboard Engineѕ from Nordkraft Maгine GmbH for
Extreme Mаrine Power
Buy Yamaha Motor, Mercury Marine, Suzuki Marine and Honda Marine Outboards
from Norⅾkraft Marine GmbᎻ
Buy Lеading Global Outboard Brands Ꭲhrough Nordkraft Marine
GmbH with Full Serviсe Support
Buy Prеmium Marine Engines from Nordkraft Marine GmbH
Paгtnering with Top International Manufacturers
Buy Multi-Brand Outboard Mօtor Ꮪolutions from Nordkraft
Marine GmbH for All Marіne Applіcations
Buy Yamaha, Mercury, Suzuki, Honda, and Tohatsu
Outboaгds from Nоrdkraft Mɑгine GmƅН Authorized Supрlier
Buy Commеrcial and Recreational Мarine Engines from Nordkraft Marine GmbH Global Diѕtribution Ⲛеtwork
Buy High-Performance Mаrine Outboarⅾs from Nordkraft Marine GmbH Backed
by Trusted Industry Brands
Buy Profesѕional Maгine Engine Solutions fгom Nordkraft Marine GmbH for Workboats ɑnd Offshore Use
Buy Completе Outboard Motor Rаnge frоm Noгɗkraft Mаrine GmbH Including All Major Global Brands
Buy Nordkraft Marine 50HP Outboard Motor Bᥙilt for
Ꮢeliаble Coastɑl and Inland Performance
Buy Nordkrаft Marine 75HP Outƅoard Engine Designed
for Ѕmooth and Efficient Cruising
Buy Norɗkraft Marine 90HᏢ Outboard Motоr for Versatile Recreational Boating
Buy Nordкraft Marine 115HP High-Performance Outboard Engіne for Demanding
Waters
Ᏼuy Nordkrɑft Marine 150ΗP Оutboard Motor Engineered for Power and Precision Handling
Buy Nordkrаft Marine 200HP Outboaгd Engine Buiⅼt for Offshore Strengtһ and
Stabiⅼity
Buy Nordkraft Ꮇarine 250HP Premium Оutboard
Motor for Maximum Marine Performance
Ᏼᥙy Nordkraft Marine 300HP High-Power Outboard Engine foг Profesѕional Applications
Buy Nordkraft Marine 350HP Heavy-Duty Outboard Motor for Extreme Marine Conditions
Buy Nordkraft Marine 400HP Elite Outboard Engine
f᧐r Ultimate Speed and Control
Buy Νordkraft Pro Serieѕ 60HP Outboard M᧐tor for
Entry-Level Marine Poᴡer
Buy Nordkraft Pro Serіes 100HP Outboard Engine Designed for All-Purpose Use
Buy Nordkraft Pro Sеries 140HP Outboard Motor with Advanced Fuel Efficiency
Buy Nordkraft Pro Seгies 180HP Outboard Engine for High-Endսrance Performance
Buy Nordkraft Pro Series 220HP Marine Engine for Commercial Applications
Buy Nordkraft X-Line 90HP Outbߋard Motor Built for Precision and Durabilitү
Buy Nordkraft X-Line 130HP Outboard Engine DesigneԀ for High-Speed Control
Buy Nօrdkraft X-Line 170HP Outboard Motor for Performance-Orientеd Boaters
Buy Nordkraft X-Line 210HP Outboard Engine for Demanding
Offshore Use
Bսy Nordkraft X-Line 260HР Outboɑrd Motoг Delivering Superior Thrust and Torque
Buy Nordкraft Commercial Series 120HP Outbοаrd Еngine for Daily
Operations
Buy Nordkraft Commercial Series 160HP Outƅoard Motor Built foг Woгkboats
Buy Nordkraft Commercial Series 200HP OutЬoard
Engine for Heavy-Duty Marine Use
Buy Nordkraft Commercial Series 240HP Outboard Motor for Indսstrial Applіcations
Buy Norԁkraft Commercial Series 300HP Outboard Engine fߋr Maximum Work Efficiency
Buy Nordkraft EcoDrive 70HP Outboard Motor with Fuel-Efficiеnt Technology
Bᥙy Nordkraft EcoƊrive 110HP Outboard Engine foг Sustainable Marine Performance
Buy Nordkraft EcoDrive 150HP Outbߋard Motor Ꭰesigned for
Low Emissions
Buy Nordkraft EcoDrive 190HΡ Outbоard Engine for Efficient Long-Distɑnce Travel
Buy Nordkraft EcoDrive 230HP Outboard Motor Combining Power and Economy
Buy Nordkraft Offѕhore 180HP OutЬoard Engine Built for Open Sea Reliability
Buy Nordkraft Offshore 220HP Outboaгd Motor for Deep Water Navigation
Buy Nordkraft Offshore 260HP Outboard Engine for Extreme Oсean Conditions
Buy Nordkraft Offshore 300НP Outboard Motor Desіgned foг Ꮮong-Range
Trips
Buy Nordkraft Offshore 350HP Outboard Engine for Professiоnal
Marine Opeгations
Buy Nordkraft Performance 100HP Outboard Motor for Speed and Agility
Bᥙy Norԁkraft Performance 150HP Outboard Engіne Built foг
Αcceleration and Сontrol
Buy Nordkraft Peгformance 200HP Outbߋard Motor fоr Ηigh-Spеed Applіcations
Buy N᧐rdkraft Peгformance 250HP Outboɑrd Engine Delivering Peak Output
Buy Nordkraft Performance 300HP Outbоаrd Motor foг Competitive Marine Use
Buy Nоrdkraft Elіte 200HР Outboard Engine for Ρremіum Marine Experience
Buy Nordkraft Elite 250HP Outboard Motor Combining Luⲭury and
Performance
Buy Nordkraft Eⅼite 300HP Outboard Engine with Аdvanced Engineering Featսгes
Buy Ⲛordkraft Elite 350HP Outboard Motoг for Top-Tier Marine
Poѡer
Βuy Νordkraft Elite 400HP Outboard Engіne for Unmatched Performance
Buy Nordkraft Compact 40HP Outboard M᧐tor for Small Boats and Tenders
Buy Nordkraft Compact 60HP Outboard Engine for Lightweight Marine Use
Buy Nordkraft C᧐mpact 80HP Outboard Motor for Easy Handling and Efficiency
Βuy Nordkraft Compact 100ΗP Oᥙtboard Engine for Everyday Boating Needs
Βuy Nordkraft Compact 120HP Outboard Motor for Balanced Ρower and
Size
I just like the helpful information you supply in your articles.
I’ll bookmark your blog and check again here frequently.
I am relatively sure I’ll be told lots of new stuff proper right here!
Good luck for the following!
Take a look at my web-site … lymph tonic benefits
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-a96033—uns/pokovka-vismutovaya-a96033—uns/
If some one wants to be updated with hottest technologies
therefore he must be pay a quick visit this web page and
be up to date every day.
Also visit my web site oradentum review
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku40-5kh1-8mmm2tgost-r-52922-2008/
¡Qué locura total, chamigos! Soy Javier desde
Fernando de la Mora.
Como alguien que respira fútbol y se juega hasta el sueldo
en combinadas, mi señora me quiere echar de casa por lo que apuesto, pero no me importa
absolutamente nada.
En el debut de esta Copa del Mundo norteamericana, quería romper el
televisor de la rabia con ese maldito 4-1 contra USA que me hizo perder mucha
plata. Pero como manda nuestra historia, resurgimos de las cenizas: le metimos una garra tremenda para ganarle 1-0
a Turquía y con el alma en un hilo clasificamos raspando,
empatando a cero con los australianos.
¡Pero la verdadera historia se escribió contra Alemania en dieciseisavos!
El mundo entero de los pronósticos nos daba por muertos, pero mostramos unos huevos gigantes para mantener el 1-1 frente a esa máquina.
¡Los eliminamos 4-3 desde los doce pasos, un milagro
hermoso y sangriento!
¡Reventé mi cuenta en la casa de apuestas porque le puse
plata a que pasábamos y pagaban una cuota de
locura total!
Se viene el monstruo de Francia en octavos y le voy a meter los ahorros de toda mi vida a
Paraguay sin pensarlo. ¡No me importa si la lógica dice que nos golean, yo muero con la mía y
apuesto todo a una nueva hazaña!
¡A dejar hasta la última gota de sangre, vamos mi Paraguay querido!
Feel free to visit my web-site: URL
I was able to find good advice from your content.
Check out my web blog; Personal injury lawyer los angeles
¡Qué locura total, chamigos! Soy Ramón desde San Lorenzo.
Como un enfermo de las apuestas deportivas y fanático a
muerte de la Albirroja, siento que el corazón me va a reventar
de tanta emoción.
Al empezar el campeonato, casi me da un infarto al perder 4-1 contra
Estados Unidos, una vergüenza terrible. Pero como
manda nuestra historia, resurgimos de las cenizas:
vencimos a los turcos 1-0 sudando sangre en la cancha y logramos
sobrevivir a la fase de grupos con ese sufrido 0-0 ante Australia.
¡Lo que vivimos contra los alemanes fue épico, digno de
una película! Todas las cuotas de las casas de apuestas estaban brutalmente en contra,
pero mostramos unos huevos gigantes para mantener el
1-1 frente a esa máquina. ¡Los eliminamos 4-3 desde los doce pasos,
un milagro hermoso y sangriento!
¡Reventé mi cuenta en la casa de apuestas porque le puse plata a
que pasábamos y pagaban una cuota de locura total!
Este jueves nos cruzamos con la Francia en octavos de final y ya
tengo mi boleto de apuesta armado. ¡Las cuotas dicen que somos boleta, pero mi corazón sabe que ganamos!
¡Vamos Paraguay, carajo!
My website … information
Very soon this web site will be famous amid all blogging people, due
to it’s fastidious content
My site – rideshare accident attorney
I am sure this piece of writing has touched all the internet users, its really really
fastidious piece of writing on building up new webpage.
Feel free to visit my web-site … bicycle accident laywer los angeles
naturally like your website however you
need to check the spelling on several of your posts. Several of
them are rife with spelling problems and I find it very bothersome to inform the reality
on the other hand I will definitely come again again.
Feel free to visit my webpage Personal injury lawyer los angeles
I’m not sure exactly why but this web site is loading incredibly slow for
me. Is anyone else having this issue or is it a issue on my end?
I’ll check back later on and see if the problem still exists.
Feel free to visit my web page Personal injury lawyer los angeles
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-158—astm-b774/list-vismutovyy-158—astm-b774/
Viagra hanya boleh digunakan sesuai dosis yang dianjurkan. Menggunakan dosis yang berlebihan tidak meningkatkan efektivitas
dan dapat meningkatkan risiko efek samping.
My blog bokep indonesia
Thanks for sharing your info. I really appreciate your efforts
and I will be waiting for your next post thank you once again.
Feel free to visit my web blog – pepek
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-kapilliarnaia-trubka/latunnaia-kapilliarnaia-trubka-1-8kh0-35kh10000-mm-l70-gost-2624-2016/
I read this article fully concerning the comparison of most up-to-date and previous technologies, it’s remarkable
article.
Feel free to visit my site; bicycle accident laywer los angeles
¡No lo puedo creer, hermano! Soy Javier desde San Lorenzo.
Como alguien que respira fútbol y se juega hasta el
sueldo en combinadas, siento que el corazón me va a reventar de
tanta emoción.
En el debut de esta Copa del Mundo norteamericana,
casi me da un infarto con ese maldito 4-1 contra USA que me hizo perder mucha plata.
Pero como manda nuestra historia, resurgimos de las cenizas:
sufrimos como unos condenados para clavarle el 1-0 a Turquía y con el alma en un hilo clasificamos raspando, empatando a cero con los
australianos.
¡Pero la verdadera historia se escribió contra Alemania en dieciseisavos!
Nadie daba un solo guaraní por nosotros, pero aguantamos como verdaderos leones
el 1-1 hasta el final de la prórroga. ¡Y en los penales, mandamos a los alemanes a llorar a su casa ganando 4-3!
¡Reventé mi cuenta en la casa de apuestas
porque le puse plata a que pasábamos y pagaban una cuota de
locura total!
Ahora se nos viene Francia este 4 de julio y ya tengo mi boleto de apuesta armado.
¡No me importa si la lógica dice que nos golean, yo muero con la mía
y apuesto todo a una nueva hazaña!
¡Vamos Paraguay, carajo!
Also visit my web site … article
Pretty! This has been an incredibly wonderful post. Many thanks for supplying this information.
Feel free to surf to my page: 신용카드현금화
It’s nearly impossible to find well-informed people in this particular subject,
however, you sound like you know what you’re talking about!
Thanks
my website … nine casino online
Возможность заказа висмута — достаточно редкое предложение на рынке
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-nitrovan-12—stratcor/pokovka-vanadievaya-nitrovan-12—stratcor/
Thanks very interesting blog!
Feel free to visit my site :: rideshare accident attorney
It’s very effortless to find out any topic on net as compared to textbooks, as I found this
piece of writing at this site.
Feel free to surf to my site gucci outlet store italy
Hey there! This is kind of off topic but I need some help from an established blog.
Is it very difficult to set up your own blog? I’m not very techincal but I can figure things out pretty quick.
I’m thinking about setting up my own but I’m not
sure where to start. Do you have any tips or suggestions?
Appreciate it
Also visit my homepage bocoran angka hoki
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku10kh0-6mmm3tgost-r-52922-2008/
I’m not sure where you are getting your information, but good topic.
I needs to spend some time learning more or understanding more.
Thanks for magnificent info I was looking
for this information for my mission.
My site … workplace sexual harassment lawyer los angeles
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt9—gost-19807-91/krug-titanovyy-vt9—gost-19807-91/
¡Qué locura total, chamigos! Soy Carlos desde Encarnación.
Como alguien que respira fútbol y se juega hasta el sueldo en combinadas, les juro que estoy viviendo el mejor sueño de mi vida.
Al empezar el campeonato, casi me da un infarto al perder 4-1 contra Estados Unidos,
una vergüenza terrible. Pero la raza guaraní nunca se rinde:
sufrimos como unos condenados para clavarle el 1-0 a Turquía y logramos sobrevivir a la fase de grupos con ese sufrido 0-0 ante Australia.
¡Lo que vivimos contra los alemanes fue épico, digno de una película!
El mundo entero de los pronósticos nos daba por muertos, pero empatamos
1-1 dejando el alma y la piel en los 120 minutos.
¡Esa tanda de penales, ganando 4-3, me hizo
llorar tirado en el piso como una criatura!
¡No se imaginan la fortuna que gané!
Este jueves nos cruzamos con la Francia en octavos
de final y me juego mi destino entero por mis muchachos.
¡Que nos den por perdedores, mucho mejor, así paga más mi apuesta!
¡La garra guaraní no se rinde jamás, nos vemos en la final del mundo!
Also visit my blog post: information
¡Dios mío, sigo temblando de la emoción! Me llamo Miguel desde
Ciudad del Este.
Como buen timbero y paraguayo de pura cepa, les juro que
estoy viviendo el mejor sueño de mi vida.
Cuando arrancamos este Mundial 2026, quería romper el televisor de la rabia con ese maldito 4-1 contra USA que me hizo perder mucha plata.
Pero ahí salió a relucir el orgullo de nuestra tierra: vencimos a los turcos 1-0 sudando sangre en la
cancha y después aguantamos a muerte para sacar ese 0-0 contra Australia.
¡Lo que vivimos contra los alemanes fue épico, digno de una película!
Nadie daba un solo guaraní por nosotros, pero
empatamos 1-1 dejando el alma y la piel en los 120 minutos.
¡Los eliminamos 4-3 desde los doce pasos,
un milagro hermoso y sangriento!
¡Me forré de plata apostando al batacazo y rompiendo todos los pronósticos!
Ahora se nos viene Francia este 4 de julio y apuesto
el auto, la casa y la vida a mi querida Albirroja.
¡Que nos den por perdedores, mucho mejor, así paga más mi apuesta!
¡La garra guaraní no se rinde jamás, nos vemos en la final del mundo!
Also visit my web page – press release
Amazing issues here. I am very satisfied to peer your post.
Thanks a lot and I am having a look ahead to touch you.
Will you please drop me a mail?
My website: Ivy Casino payment methods
I really like your blog.. very nice colors & theme.
Did you create this website yourself or did you hire someone to do it for you?
Plz answer back as I’m looking to design my own blog and would like to find out where u got this from.
thanks a lot
Also visit my web blog; Personal injury lawyer los angeles
Thanks for your personal marvelous posting! I certainly enjoyed reading it,
you might be a great author.I will be sure to bookmark your blog and may come
back later in life. I want to encourage you continue your great work, have a nice
morning!
my web page – truck accident lawyer los angeles
It’s going to be finish of mine day, but before finish I am reading this wonderful piece of writing to increase my know-how.
Feel free to surf to my web site 2) Palm Coast appliance repair
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-46kh1-7-mm-lmtss-gost-13942-86/
Pretty! This was an extremely wonderful article.
Many thanks for supplying this info.
Feel free to visit my web page Personal injury lawyer los angeles
I’m not sure why but this site is loading incredibly slow for me.
Is anyone else having this problem or is it a problem on my end?
I’ll check back later on and see if the problem still exists.
Also visit my site: lyft accident attorney los angeles
Thanks designed for sharing such a good thought, piece of writing is pleasant,
thats why i have read it completely
my page … 抖音号自动发货
FranChoice
7500 Flying Clohd Drive,
#600 Eden Prairie
MN 55344, United Ѕtates
952-345-8400
Bookmarks
I think this is one of the most important info for me.
And i’m glad reading your article. But want to remark on some general things,
The website style is great, the articles is
really great : D. Good job, cheers
Check out my web page; แทงบอลโลก
You’ve made some good points there. I checked on the net for more
info about the issue and found most people will go along with your
views on this site.
Look at my website – webpage
Hello just wanted to give you a quick heads up and let
you know a few of the pictures aren’t loading correctly.
I’m not sure why but I think its a linking issue.
I’ve tried it in two different browsers and both show the same results.
Feel free to visit my web blog – اپلیکیشن پیش بینی جام جهانی
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt15—ost-1-90013-81-1/truba-titanovaya-vt15—ost-1-90013-81-1/
Have you ever thought about adding a little bit more than just your articles?
I mean, what you say is fundamental and all. Nevertheless just imagine
if you added some great photos or video clips to give your posts more,
“pop”! Your content is excellent but with pics and video clips, this blog could
certainly be one of the best Builder in Cambridge its niche.
Very good blog!
Explore trusted information about casino, casino NL,
casino Nederland, and the casino Netherlands market, including online gaming insights, responsible gambling practices, licensing information, and the latest trends for Dutch casino players.
Visit my blog post https://tena-men.nl/
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku28kh1-5mmm3rtgost-32590-2013/
Franchising Path Carlsbad
Carlsbad, СA 92008, United Stateѕ
+18587536197
how to start a franchise chick fil a
Banyak orang mencari informasi tentang Viagra Indonesia untuk memahami manfaat, cara
kerja, dan penggunaan yang benar. Informasi yang akurat dapat membantu menghindari penggunaan yang tidak tepat.
Check out my blog post: bokep indonesia
My spouse and I stumbled over here by a different page and thought I might check
things out. I like what I see so now i am following you. Look
forward to finding out about your web page again.
my webpage sunwin
Vice-captain for matches where teams play on pitches with unusual dimensions or slope.
I’m impressed, I have to admit. Seldom do I come across a blog that’s both equally
educative and engaging, and let me tell
you, you have hit the nail on the head. The issue is something that not enough
folks are speaking intelligently about. I am very happy that I stumbled across this during my hunt for something regarding this.
my website – singapore corporate blog
Технические характеристики сплавов помогают инженерам в подборе
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-spt-2—gost-27265-87-2/poroshok-titanovyy-spt-2—gost-27265-87-2/
We are a group of volunteers and opening a new scheme in our community.
Your web site offered us with valuable information to work
on. You have done an impressive job and our entire community will be thankful to you.
My blog sunwin
I’ve been browsing online greater than three hours nowadays, but I never found any attention-grabbing article like yours.
It’s lovely value enough for me. Personally, if
all webmasters and bloggers made excellent content
material as you probably did, the web can be a lot more helpful
than ever before.
my blog post sunwin
¡Dios mío, sigo temblando de la emoción! Me llamo Javier desde Asunción.
Como buen timbero y paraguayo de pura cepa, les juro que estoy viviendo el mejor sueño de
mi vida.
En el debut de esta Copa del Mundo norteamericana, quería romper el televisor de la rabia al perder 4-1 contra Estados Unidos,
una vergüenza terrible. Pero como manda nuestra
historia, resurgimos de las cenizas: vencimos a los turcos
1-0 sudando sangre en la cancha y con el alma en un hilo clasificamos raspando, empatando a cero
con los australianos.
¡El partido contra Alemania me quitó diez años de vida y me devolvió la fe!
El mundo entero de los pronósticos nos daba por
muertos, pero aguantamos como verdaderos leones el 1-1 hasta el final de la prórroga.
¡Los eliminamos 4-3 desde los doce pasos, un milagro hermoso y sangriento!
¡Con lo que gané en esa apuesta a la sorpresa me pago las deudas de todo
el año y festejo un mes seguido!
Este jueves nos cruzamos con la Francia en octavos de final
y me juego mi destino entero por mis muchachos.
¡Que nos den por perdedores, mucho mejor, así
paga más mi apuesta!
¡Rohayhu Albirroja, a matar o morir en la cancha!
Also visit my website url
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-145kh3-mm-ls59-gost-13942-86/
บทความนี้ อ่านแล้วเพลินและได้สาระ ครับ
ดิฉัน ได้อ่านบทความที่เกี่ยวข้องกับ ข้อมูลเพิ่มเติม
ดูต่อได้ที่ m4autobet
เผื่อใครสนใจ
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Wow, this article is good, my younger sister is analyzing
such things, thus I am going to convey her.
Here is my blog; sunwin
Nice weblog here! Additionally your site lots up fast! What host are you using?
Can I am getting your affiliate link in your host?
I desire my site loaded up as quickly as yours lol
Feel free to surf to my web-site; sunwin
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-cp-4/provoloka-titanovaya-cp-4/
Howdy I am so glad I found your website, I really found you by error, while I
was searching on Google for something else, Anyhow I am here now and would
just like to say kudos for a tremendous post and a all round entertaining blog (I also love
the theme/design), I don’t have time to browse it all at the minute but I have book-marked it and also added your RSS feeds, so when I have time I
will be back to read more, Please do keep up the excellent work.
Feel free to surf to my blog post watch movies
FranChoice
7500 Flying Cloud Drive,
#600 Eden Prairie
MN 55344, United Ѕtates
952-345-8400
franchise business marketing strategies guide
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku34kh1-8mmm3gost-32590-2013/
Thanks for finally talking about > Heel Pain – Plantar Fasciitis – Mr Will Edwards sunwin
¡Mba’éichapa los perros! Acá les escribe Derlis desde
San Lorenzo.
Como un enfermo de las apuestas deportivas y fanático a
muerte de la Albirroja, les juro que estoy viviendo el mejor
sueño de mi vida.
Cuando arrancamos este Mundial 2026, casi me da un infarto cuando los yanquis nos metieron ese
humillante 4-1. Pero la raza guaraní nunca se rinde: le metimos una garra tremenda para ganarle 1-0
a Turquía y con el alma en un hilo clasificamos raspando, empatando a cero
con los australianos.
¡Pero la verdadera historia se escribió contra
Alemania en dieciseisavos! Todas las cuotas de
las casas de apuestas estaban brutalmente en contra, pero empatamos 1-1 dejando el alma y la piel en los 120 minutos.
¡Los eliminamos 4-3 desde los doce pasos, un milagro hermoso y
sangriento!
¡Reventé mi cuenta en la casa de apuestas porque
le puse plata a que pasábamos y pagaban una cuota de locura total!
Ahora se nos viene Francia este 4 de julio y apuesto el auto, la casa
y la vida a mi querida Albirroja. ¡Las cuotas dicen que somos boleta, pero mi corazón sabe que
ganamos!
¡La garra guaraní no se rinde jamás, nos vemos en la final del
mundo!
My blog post; URL
Does your website have a contact page? I’m having problems locating it but, I’d like to shoot you an e-mail.
I’ve got some ideas for your blog you might be interested in hearing.
Either way, great site and I look forward to seeing it develop over time.
Look at my blog post – download bokep indonesia
Good day! This is kind of off topic but I need some advice
from an established blog. Is it tough to set up your own blog?
I’m not very techincal but I can figure things out
pretty fast. I’m thinking about setting up my own but I’m not sure where to start.
Do you have any tips or suggestions? Appreciate it
Here is my blog post :: sunwin
Возможность заказа продукции в розницу и оптом (судя по описанию)
https://redmetsplav.ru/store/tantal-i-ego-splavy/tantal-tn-3-1/prutok-tantalovyy-tn-3/
¡No lo puedo creer, hermano! Soy Hugo desde Ciudad del Este.
Como buen timbero y paraguayo de pura cepa, siento
que el corazón me va a reventar de tanta emoción.
En el debut de esta Copa del Mundo norteamericana, casi me da un infarto cuando
los yanquis nos metieron ese humillante 4-1.
Pero como manda nuestra historia, resurgimos de las cenizas: vencimos a los turcos 1-0
sudando sangre en la cancha y con el alma en un hilo clasificamos
raspando, empatando a cero con los australianos.
¡El partido contra Alemania me quitó diez años de vida y me devolvió la fe!
Nadie daba un solo guaraní por nosotros, pero aguantamos como verdaderos leones el 1-1
hasta el final de la prórroga. ¡Y en los penales, mandamos a los alemanes a llorar a su casa ganando 4-3!
¡Reventé mi cuenta en la casa de apuestas porque le puse plata a que pasábamos y pagaban una cuota de locura total!
Se viene el monstruo de Francia en octavos y me juego mi destino entero por mis muchachos.
¡Las cuotas dicen que somos boleta, pero mi corazón sabe que ganamos!
¡Rohayhu Albirroja, a matar o morir en la cancha!
my homepage … link
continuously i used to read smaller content that
as well clear their motive, and that is also happening with this article which I am reading now.
Have a look at my blog post – Pierres précieuses naturelles
Hmm is anyone else having problems with the images
on this blog loading? I’m trying to find out if its a problem on my end or if it’s the blog.
Any suggestions would be greatly appreciated.
my homepage: nhà cái sunwin
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-68kh2-5-mm-lts40s-gost-13942-86/
I do consider all the ideas you’ve offered to your post.
They’re really convincing and can certainly work. Nonetheless, the posts are very brief for novices.
May you please extend them a little from next time?
Thank you for the post.
Here is my page :: 音实名号出售
Very quickly this website will be famous amid all blogging people, due to
it’s fastidious posts
Stop by my web site 抖音认证号购买
Wonderful, what a webpage it is! This website provides useful
facts to us, keep it up.
Feel free to visit my web page tải app sunwin
I like the helpful info you supply in your articles.
I’ll bookmark your blog and test again right here regularly.
I am reasonably sure I’ll learn many new stuff proper
here! Good luck for the following!
My web blog ads pepek
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nbp-4—gost-26252-84-1/provoloka-niobievaya-nbp-4—gost-26252-84/
If some one needs expert view regarding blogging and site-building then i recommend him/her
to visit this blog, Keep up the pleasant work.
My web-site; 抖音账号购买平台
Good article! We will be linking to this great post
on our site. Keep up the great writing.
my web blog: 抖音号批发
It’s awesome to pay a visit this web page and reading the views of all mates on the topic of this article,
while I am also eager of getting familiarity.
my website: 抖音账号批发
Modrrn Purair
416 Meridian Ɍd SE #14A, Calgary
AB T2А 1X2, Canada
(403) 800-7254
efficient pro (https://28tc2.stick.ws/)
Hi would you mind stating which blog platform you’re using?
I’m planning to start my own blog soon but
I’m having a tough time selecting between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design and style
seems different then most blogs and I’m looking for something unique.
P.S Sorry for getting off-topic but I had to ask!
My web-site :: 강남쩜오
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-16kh12kh0-7-mm-10-6kh12-6-mm-miagkaia-paika-m2m-gost-r-52922-2008/
A fascinating discussion is definitely worth comment.
I believe that you need to publish more about
this subject matter, it may not be a taboo matter but usually folks don’t discuss such issues.
To the next! Cheers!!
Here is my web page; đăng ký sunwin
Viagra merupakan salah satu terapi yang tersedia untuk mengatasi
disfungsi ereksi. Namun, penggunaannya harus disesuaikan dengan kondisi masing-masing individu.
Also visit my homepage :: bokep indonesia
โพสต์นี้ อ่านแล้วได้ความรู้เพิ่ม ครับ
ดิฉัน ไปเจอรายละเอียดของ ข้อมูลเพิ่มเติม
ดูต่อได้ที่ pg888
สำหรับใครกำลังหาเนื้อหาแบบนี้
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
bookmarked!!, I love your web site!
My web site :: 여의도착석바
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-vm3-2/pokovka-molibdenovaya-vm3/
You made some really good points there. I checked on the web for additional information about the issue and found
most people will go along with your views on this web site.
Feel free to surf to my blog post 抖音粉丝号出售
Great weblog here! Also your web site loads up very fast!
What web host are you the usage of? Can I am getting your affiliate hyperlink
in your host? I desire my website loaded up as fast as yours lol
my web site – 抖音粉丝号出售
Сайт очень информативный.
Обязательно зайду ещё!
асфальтирование спб
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m148-138kh4-mm-lts16k4-din-471/
I read this post completely regarding the difference of latest and earlier technologies, it’s awesome article.
my website :: 抖音号买卖
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mr-47zvp-1/truba-molibdenovaya-mr-47zvp/
Hi there, after reading this remarkable piece
of writing i am also happy to share my knowledge here
with mates.
Also visit my page … 신용카드현금화
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-108kh92kh2-1-mm-15kh19-mm-tverdaia-paika-m1t-gost-32590-2013/
Quality posts is the main to attract the users to go to
see the web page, that’s what this web page is providing.
Feel free to surf to my web site – water damage restoration
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-md-30-1/krug-molibdenovyy-md-30/
Franchising Path Carlsbad
Carlsbad, ⅭA 92008, Unkted States
+18587536197
how buying a franchise works
I don’t even know the way I stopped up here, however I
believed this post used to be great. I don’t know who you are however certainly you are going
to a well-known blogger if you happen to are not already.
Cheers!
My web page: Mayfair Wellness medical tourism malaysia
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m112-103kh4-mm-lmtssk-din-471/
¡Mba’éichapa los perros! Soy Hugo desde San Lorenzo.
Como un enfermo de las apuestas deportivas y
fanático a muerte de la Albirroja, llevo días sin dormir bien, llorando de la alegría.
Al empezar el campeonato, toqué fondo anímicamente cuando los yanquis nos metieron ese humillante
4-1. Pero ahí salió a relucir el orgullo de nuestra tierra: le metimos una garra tremenda para ganarle 1-0 a Turquía y con el alma en un hilo clasificamos raspando, empatando a cero con los australianos.
¡Pero la verdadera historia se escribió contra Alemania
en dieciseisavos! Todas las cuotas de las casas de apuestas estaban brutalmente en contra, pero aguantamos como verdaderos leones el 1-1 hasta el final de la prórroga.
¡Esa tanda de penales, ganando 4-3, me hizo llorar tirado en el piso como una criatura!
¡No se imaginan la fortuna que gané!
Ahora se nos viene Francia este 4 de julio y me juego mi destino entero por mis muchachos.
¡Las cuotas dicen que somos boleta, pero mi corazón sabe
que ganamos!
¡Rohayhu Albirroja, a matar o morir en la
cancha!
Visit my web blog; article
¡Dios mío, sigo temblando de la emoción! Acá les escribe Derlis desde San Lorenzo.
Como un enfermo de las apuestas deportivas y fanático a muerte de la
Albirroja, mi señora me quiere echar de casa por lo que apuesto, pero no me
importa absolutamente nada.
Cuando arrancamos este Mundial 2026, toqué fondo anímicamente con ese maldito 4-1 contra USA que me hizo perder
mucha plata. Pero como manda nuestra historia, resurgimos de las cenizas:
sufrimos como unos condenados para clavarle el 1-0 a Turquía y logramos sobrevivir a la fase de grupos con ese sufrido
0-0 ante Australia.
¡El partido contra Alemania me quitó diez años de vida y me devolvió la fe!
El mundo entero de los pronósticos nos daba
por muertos, pero empatamos 1-1 dejando el alma y la piel
en los 120 minutos. ¡Y en los penales, mandamos a
los alemanes a llorar a su casa ganando 4-3!
¡Reventé mi cuenta en la casa de apuestas porque le puse plata a que pasábamos y pagaban una cuota de
locura total!
Se viene el monstruo de Francia en octavos y apuesto el auto, la casa y la vida a mi querida Albirroja.
¡No me importa si la lógica dice que nos golean, yo muero con la mía y apuesto todo a una nueva hazaña!
¡La garra guaraní no se rinde jamás, nos vemos en la final del mundo!
my web site; information
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-zh62a—mil-m-46062/izdeliya-iz-magniya-zh62a—mil-m-46062/
Jungle Driving School Omaha
4020 Ѕ 147th Ⴝt, Omaha,
NE 68137, United States
14024170547
Social Engagement Driving School
Unquestionably believe that which you stated. Your favorite justification seemed to be on the web the easiest thing to be
aware of. I say to you, I certainly get annoyed while people
consider worries that they plainly don’t know about.
You managed to hit the nail upon the top and defined out the
whole thing without having side-effects , people can take a signal.
Will likely be back to get more. Thanks
my web blog: Darci
I’m extremely impressed with your writing skills and also with the layout on your blog.
Is this a paid theme or did you modify it yourself?
Anyway keep up the nice quality writing, it is rare to see a great blog like this one nowadays.
Feel free to surf to my web blog tron vanity address
Удобно записаться к психологу онлайн и принимать сессии из дома.
психолог Краснодар
When someone writes an article he/she keeps the idea of a user in his/her brain that how a user can know it.
So that’s why this piece of writing is great. Thanks!
My homepage; https://a-twaalf.nl/
โพสต์นี้ ให้ข้อมูลดี ค่ะ
ดิฉัน ได้อ่านบทความที่เกี่ยวข้องกับ เนื้อหาในแนวเดียวกัน
ซึ่งอยู่ที่ สล็อตออนไลน์ได้เงินจริง
เผื่อใครสนใจ
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m58-53-8kh2-mm-lts14k3s3-din-471/
Отличный психолог в Краснодаре, рекомендую
терапию у нее.
созависимые отношения
Рада, что решила записаться к психологу онлайн именно к Дарье.
психолог по отношениям
Поковки и штабики — важные заготовки для металлургических предприятий
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgzn6zr/lenta-magnievaya-mgzn6zr/
PlayVirexo casino, PlayVirexo brinda una gama de juegos emocionantes para todos.
Es posible gozar de promociones especiales que aumentan tu vivencia.
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-54kh47kh1-2-mm-11kh13-mm-tverdaia-paika-m1rm-gost-r-52922-2008/
Hi, I do think this is an excellent website. I stumbledupon it ;) I may come back yet again since i have saved as a favorite
it. Money and freedom is the greatest way to change, may you be rich and continue to guide others.
Take a look at my web site tripscan официальный
I’m really enjoying the design and layout of your website.
It’s a very easy on the eyes which makes it much more enjoyable for me to come here and visit more often. Did
you hire out a developer to create your theme?
Outstanding work!
my blog post … stem cell therapy thailand
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgal6zn—din-1729-part-2/pokovka-magnievaya-mgal6zn—din-1729-part-2/
Interesting discussion, looking forward to reading more replies.
Appreciate all the helpful replies and information shared in this thread.
Nice forum discussion, some really useful insights being shared here.
Thanks for sharing your thoughts here, this has been a useful discussion.
Appreciate the discussion here, lots of useful information in this thread.
Also visit my website: reddit.com/r/microgrowery HLVD infection confirmed: he Clone Foundry – 114 strains tested positive
Hey there are using WordPress for your blog platform?
I’m new to the blog world but I’m trying to get started and create my own. Do you need any html coding expertise to make your
own blog? Any help would be greatly appreciated!
Here is my blog post – hệ thống pin năng lượng mặt trời
¡Qué locura total, chamigos! Soy Miguel desde Ciudad
del Este.
Como alguien que respira fútbol y se juega hasta el sueldo en combinadas, llevo días sin dormir bien, llorando de la alegría.
Al empezar el campeonato, casi me da un infarto
cuando los yanquis nos metieron ese humillante 4-1.
Pero ahí salió a relucir el orgullo de nuestra
tierra: sufrimos como unos condenados para clavarle el 1-0 a Turquía y después aguantamos a muerte para sacar ese 0-0
contra Australia.
¡El partido contra Alemania me quitó diez años
de vida y me devolvió la fe! Todas las cuotas de las casas
de apuestas estaban brutalmente en contra, pero mostramos unos huevos gigantes para mantener el 1-1 frente a esa máquina.
¡Esa tanda de penales, ganando 4-3, me hizo llorar tirado
en el piso como una criatura!
¡Con lo que gané en esa apuesta a la sorpresa me pago las deudas de todo el año y festejo un mes seguido!
Este jueves nos cruzamos con la Francia en octavos de final y le voy a meter los ahorros de toda
mi vida a Paraguay sin pensarlo. ¡Las cuotas dicen que somos
boleta, pero mi corazón sabe que ganamos!
¡Rohayhu Albirroja, a matar o morir en la cancha!
My webpage; press release
Peculiar article, totally what I needed.
Also visit my blog post; ide kreatif
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-135kh2-5-mm-lazhmts-gost-13943-86/
Your way of describing all in this article is really nice, every one can without difficulty be aware of it, Thanks a lot.
Take a look at my web-site: evn solar
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mdc1a—jis-h-5303/pokovka-magnievaya-mdc1a—jis-h-5303/
I am actually glad to read this weblog posts which contains
lots of helpful information, thanks Farm Plots for sale in Future City
providing such data.
Excellent article. Keep writing such kind of info on your blog.
Im really impressed by your blog.
Hello there, You have performed an excellent job. I’ll certainly digg it and
for my part recommend to my friends. I am confident they will
be benefited from this web site.
Feel free to surf to my site; book dummy flight ticket
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-53-6kh47kh1-2-mm-32kh34-mm-miagkaia-paika-m2m-gost-r-52922-2008/
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mb3—jis-h-4203/prutok-magnievyy-mb3—jis-h-4203/
This piece of writing will assist the internet visitors for setting up
new website or even a blog from start to end.
Look at my web blog công ty lắp điện mặt trời
¡No lo puedo creer, hermano! Me llamo Hugo desde Luque.
Como un enfermo de las apuestas deportivas y fanático a muerte de la Albirroja, mi señora me quiere echar de casa por
lo que apuesto, pero no me importa absolutamente nada.
Al empezar el campeonato, quería romper el televisor de la rabia al perder 4-1 contra Estados Unidos, una vergüenza terrible.
Pero la raza guaraní nunca se rinde: le metimos una garra tremenda
para ganarle 1-0 a Turquía y con el alma en un hilo clasificamos raspando,
empatando a cero con los australianos.
¡Pero la verdadera historia se escribió contra Alemania en dieciseisavos!
Todas las cuotas de las casas de apuestas estaban brutalmente en contra, pero
aguantamos como verdaderos leones el 1-1 hasta el final de la
prórroga. ¡Y en los penales, mandamos a los alemanes a llorar a su casa ganando 4-3!
¡No se imaginan la fortuna que gané!
Se viene el monstruo de Francia en octavos y ya tengo mi boleto de apuesta armado.
¡Que nos den por perdedores, mucho mejor, así paga más mi apuesta!
¡A dejar hasta la última gota de sangre, vamos mi Paraguay
querido!
Take a look at my site press release
I pay a visit everyday some sites and websites to read posts, but this webpage offers feature
based articles.
Feel free to visit my web page; Buy farm house
โพสต์นี้ อ่านแล้วเพลินและได้สาระ ค่ะ
ดิฉัน เพิ่งเจอข้อมูลเกี่ยวกับ ข้อมูลเพิ่มเติม
ที่คุณสามารถดูได้ที่ Philomena
ลองแวะไปดู
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ เนื้อหาดีๆ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
my site lava168 (Philomena)
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-22kh1-mm-lmtss-gost-13943-86/
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-14—bs-2970-1/pokovka-magnievaya-mag-14—bs-2970-1/
We stumbled over here different page and thought I may as
well check things out. I like what I see so now i’m following you.
Look forward to looking at your web page for a second time.
Also visit my site … xem them
After looking over a handful of the blog articles on your website, I truly like your technique of writing a blog.
I book-marked it to my bookmark webpage list and will be
checking back in the near future. Please check out
my website as well and tell me what you think.
Feel free to visit my site: game private server android
Discover the excitement of gambling at an online casino.
With a generous Welcome Bonus online casino, https://bitcointalk.org/index.php?action=profile;u=3761432, newcomers can boost their initial
gaming experience.
I’d like to find out more? I’d love to find out more details.
Feel free to surf to my web site: Nouveau Casino en Ligne France
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-35kh29kh1-mm-23kh25-mm-miagkaia-paika-m1r-gost-32590-2013/
It’s enormous that you are getting ideas from this paragraph as well as from our argument made at this time.
my blog post :: highly rated products
Фольга из редких металлов часто требуется для высокотехнологичных лабораторий
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m18540—uns/truba-magnievaya-m18540—uns/
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m14145—uns/folga-magnievaya-m14145—uns/
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-100kh2-mm-lk-gost-13943-86/
Greate pieces. Keep writing such kind of information on your blog.
Im really impressed by your site.
Hello there, You’ve done an incredible job.
I’ll certainly digg it and for my part recommend to my friends.
I’m confident they’ll be benefited from this website.
my blog post: wwtop Yupoo Online
Legal protections available to Dream11 users under Indian consumer protection laws.
Buastoto.id – Solusi Digital Marketing
Terdepan dengan Teknologi AI & Data Analytics. Tingkatkan Bisnis Anda dengan Strategi
Digital Marketing Canggih.
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11611—uns/list-magnievyy-m11611—uns/
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-106kh92kh2-1-mm-47-5kh51-5-mm-miagkaia-paika-m1t-gost-32590-2013/
Hi would you mind letting me know which webhost you’re using?
I’ve loaded your blog in 3 different web browsers and I
must say this blog loads a lot quicker then most. Can you suggest a good hosting provider at a reasonable price?
Thanks, I appreciate it!
Review my web-site … đặt hoa sinh nhật (Jere)
The vice-captain who accumulates quietly while others chase big hits — the underrated pick.
Thank you, I’ve recently been searching for information approximately this subject for a while and yours is the best I have found out till now.
However, what concerning the conclusion? Are you sure about the supply?
Look at my site … vsf watch factory raid
Логичное деление на вольфрамовый, молибденовый и титановый прокат
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m10102—uns/lenta-magnievaya-m10102—uns/
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m51-55-2kh2-mm-ls-din-472/
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mg99-95a—iso-8287/krug-magnievyy-iso-mg99-95a—iso-8287/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-80kh68kh1-8-mm-35-5kh38-5-mm-miagkaia-paika-m0b-gost-r-52922-2008/
My brother suggested I might like this web site. He was totally
right. This post actually made my day. You can not imagine just how much time I had spent for this info!
Thanks!
Also visit my page; data macau sampai sgp hari ini
¡Dios mío, sigo temblando de la emoción! Acá les escribe Derlis
desde Asunción.
Como apostador empedernido que llora sangre por su selección, mi señora me quiere echar de casa
por lo que apuesto, pero no me importa absolutamente nada.
En el debut de esta Copa del Mundo norteamericana, sentí que se me caía el mundo encima al perder 4-1 contra Estados Unidos, una
vergüenza terrible. Pero ahí salió a relucir el orgullo
de nuestra tierra: vencimos a los turcos 1-0 sudando sangre
en la cancha y con el alma en un hilo clasificamos raspando, empatando a cero con los australianos.
¡El partido contra Alemania me quitó diez años de vida y me devolvió la fe!
Nadie daba un solo guaraní por nosotros, pero empatamos 1-1 dejando el alma
y la piel en los 120 minutos. ¡Los eliminamos 4-3 desde los doce pasos,
un milagro hermoso y sangriento!
¡Reventé mi cuenta en la casa de apuestas porque le puse
plata a que pasábamos y pagaban una cuota de locura total!
Se viene el monstruo de Francia en octavos y le voy a meter los ahorros de toda mi vida a Paraguay sin pensarlo.
¡No me importa si la lógica dice que nos golean, yo muero con la mía y apuesto todo a una
nueva hazaña!
¡La garra guaraní no se rinde jamás, nos vemos en la final del mundo!
Here is my site :: link
I needed to thank you for this wonderful read!! I
absolutely loved every little bit of it. I’ve got you book marked to check out new stuff
you post…
My homepage … OPPEIN Home
Отраслевой охват впечатляет: от медицины до космической промышленности
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-hk31—csa-hg-9/provoloka-magnievaya-hk31—csa-hg-9/
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m132-137kh4-mm-lk-din-472/
It’s going to be finish of mine day, but before finish I
am reading this fantastic paragraph to improve my experience.
my blog post – bathroom remodel companies
I think this is one of the most significant information for bath remodel near me.
And i am glad reading your article. But wanna remark on some
general things, The web site style is great, the articles is really excellent : D.
Good job, cheers
Wow, amazing blog layout! How long have you been blogging
for? you make blogging look easy. The overall look of your site is excellent, let alone the content!
Feel free to surf to my webpage :: OPPEIN Home
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-mgth3zn2zr1—din-1729-part-2/list-magnievyy-g-mgth3zn2zr1—din-1729-part-2/
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-21kh18kh0-9-mm-8kh10-mm-tverdaia-paika-m3-gost-32590-2013/
Truly when someone doesn’t know afterward its up to other people that they will help,
so here it occurs.
Here is my website :: capsaicin supplement
Amazing blog! Do you have any tips and hints for aspiring writers?
I’m planning to start my own website soon but I’m a little lost on everything.
Would you suggest starting with a free platform like WordPress or go for a paid option? There
are so many options out there that I’m totally overwhelmed ..
Any ideas? Kudos!
Stop by my homepage: Limbobet Casino login
Excellent pieces. Keep posting such kind of information on your blog.
Im really impressed by your blog.
Hello there, You have performed an excellent job. I will definitely digg it and in my opinion recommend to my friends.
I’m sure they’ll be benefited from this web site.
Also visit my website; large family travel
Patrice & Associates
Scottsdale, AZ, United Ⴝtates
16265237726
convention services staff (Felipe)
Greetings! Very useful advice in this particular article!
It’s the little changes that will make the largest changes.
Thanks a lot for sharing!
Review my website 강남구구단
Howdy! I know this is kind of off topic but I was wondering which blog platform are you using for this website?
I’m getting tired of WordPress because I’ve had issues
with hackers and I’m looking at alternatives for another platform.
I would be fantastic if you could point me in the direction of a good platform.
My webpage; best osrs private server
This site was… how do you say it? Relevant!! Finally I have found something which helped me.
Many thanks!
My blog post :: 강남구구단
Информация о проверке качества продукции повышает лояльность клиентов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-gn3/provoloka-magnievaya-gn3/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m82-87-5kh2-5-mm-ls59-din-472/
Have you ever thought about creating an e-book or guest authoring on other blogs?
I have a blog based on the same information you discuss
and would really like to have you share some stories/information. I know my audience would enjoy your work.
If you’re even remotely interested, feel free to send me
an e-mail.
my web-site … 강남구구단
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mc21210—en-1753/polosa-magnievaya-en-mc21210—en-1753/
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-66-7kh57kh1-4-mm-33-5kh36-5-mm-tverdaia-paika-m1t-gost-r-52922-2008/
My coder is trying to convince me to move to .net from PHP.
I have always disliked the idea because of the costs. But he’s tryiong none the less.
I’ve been using Movable-type on several websites for about
a year and am nervous about switching to another platform. I have heard excellent things
about blogengine.net. Is there a way I can transfer all my wordpress content into it?
Any help would be greatly appreciated!
my site – Animal Drawstring Bags
I have been exploring for a bit for any high quality articles or weblog posts
in this sort of space . Exploring in Yahoo I finally stumbled
upon this site. Reading this info So i’m glad to express that I’ve an incredibly just right
uncanny feeling I discovered exactly what I needed.
I so much no doubt will make sure to do not disregard this site and provides
it a glance regularly.
Here is my site: Limbobet Casino Bonuses
Thanks a bunch for sharing this with all people you really understand
what you are speaking approximately! Bookmarked. Kindly additionally talk over with my web site =).
We may have a link change arrangement between us
Here is my page shower remodeling near me
Логичное деление на вольфрамовый, молибденовый и титановый прокат
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mc21210/izdeliya-iz-magniya-en-mc21210/
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m142-147kh4-mm-lts40mts3zh-din-472/
Asking questions are actually nice thing if you are not understanding
anything totally, however this article offers nice understanding yet.
Also visit my web site – bokep indonesia terbaik
Write more, thats all I have to say. Literally, it seems as
though you relied on the video to make your point.
You clearly know what youre talking about, why waste your intelligence
on just posting videos to your blog when you could be giving us something enlightening to read?
Here is my web-site: situs slot
Fantastic beat ! I wish to apprentice while you amend your website,
how could i subscribe for a blog site? The account aided me a acceptable deal.
I had been a little bit acquainted of this your broadcast offered bright clear idea
Also visit my web site: 비아그라 구매
I really love this article.
Описание преимуществ компании подчеркивает надежность поставок
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az91b—astm-b275/pokovka-magnievaya-az91b—astm-b275/
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-40kh35kh1-1-mm-27kh29-mm-tverdaia-paika-m1e-gost-32590-2013/
¡Mba’éichapa los perros! Soy Gustavo desde Asunción.
Como un enfermo de las apuestas deportivas y fanático a
muerte de la Albirroja, mi señora me quiere echar de casa por lo que apuesto, pero no me importa absolutamente nada.
Al empezar el campeonato, casi me da un infarto cuando los yanquis nos metieron ese humillante 4-1.
Pero como manda nuestra historia, resurgimos de las cenizas:
le metimos una garra tremenda para ganarle 1-0 a Turquía y con el
alma en un hilo clasificamos raspando, empatando a
cero con los australianos.
¡El partido contra Alemania me quitó diez años de vida y me
devolvió la fe! Nadie daba un solo guaraní por nosotros, pero mostramos
unos huevos gigantes para mantener el 1-1 frente a esa máquina.
¡Y en los penales, mandamos a los alemanes a llorar a su casa ganando 4-3!
¡Reventé mi cuenta en la casa de apuestas porque le puse
plata a que pasábamos y pagaban una cuota de locura total!
Se viene el monstruo de Francia en octavos y apuesto el
auto, la casa y la vida a mi querida Albirroja. ¡Que nos den por perdedores, mucho mejor, así paga
más mi apuesta!
¡La garra guaraní no se rinde jamás, nos vemos en la final del mundo!
Here is my blog post: information
This web site certainly has all the information I wanted about this subject and didn’t know who to ask.
Visit my web site shayarim.in/vi-vn/ lừa đảo công an truy nã cấm người chơi tham gia
Great post. I was checking continuously this weblog and I am inspired!
Very useful info particularly the final section :) I handle
such info a lot. I was looking for this particular info for a long time.
Thanks and good luck.
My page :: cc checker
Quality articles or reviews is the main to attract the users to go to see the web site, that’s
what this website is providing.
My web blog: bathroom remodel altrincham
Wonderful beat ! I would like to apprentice while you amend your site, how can i
subscribe for a blog site? The account helped me a acceptable deal.
I had been tiny bit acquainted of this your broadcast offered bright clear idea
My blog :: bath remodeling contractors
Informative article, just what I wanted to find.
Stop by my website … free kredit joy
Профессиональный подход к описанию каждого вида металла
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az91c—astm-b93/folga-magnievaya-az91c—astm-b93/
Hurrah! In the end I got a webpage from where I know how to in fact get useful
data regarding my study and knowledge.
Also visit my site :: contractors for bathrooms
May I simply just say what a relief to uncover somebody that genuinely understands what they’re talking about on the internet.
You certainly realize how to bring an issue to light and make it important.
A lot more people really need to check this out and understand this side of the story.
I was surprised you aren’t more popular because you surely have the gift.
My web-site: shower remodel near me
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-80kh100-mm-lts16k4/
Admiring the commitment you put into your site and detailed information you present.
It’s good to come across a blog every once in a while that isn’t the
same old rehashed material. Great read! I’ve bookmarked your site and I’m adding your
RSS feeds to my Google account.
My blog bath remodeling contractor
Hi! I’m at work surfing around your blog from my new iphone!
Just wanted to say I love reading through your blog and look
forward to all your posts! Keep up the great work!
my blog post; bathroom builders altrincham
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az101a—mil-r-6944b/poroshok-magnievyy-az101a—mil-r-6944b/
Dating Coach Amsterdam Dating Coach provides expert guidance for
singles seeking meaningful relationships. Dating Coach
Amsterdam Dating Coach offers personalized strategies tailored to
individual needs. The Dating Coach at Dating Coach Amsterdam offers practical advice to boost
confidence in social settings. The Dating Coach from Dating Coach Amsterdam simplifies communication skills for successful interactions.
Dating Coach Amsterdam Dating Coach helps clients in overcoming dating challenges effectively.
Dating Coach Amsterdam Dating Coach enables improved self-awareness and emotional intelligence.
The Dating Coach at Dating Coach Amsterdam provides tools
to navigate the Amsterdam dating scene confidently.
The Dating Coach from Dating Coach Amsterdam delivers actionable tips for first
dates and follow-ups. Dating Coach Amsterdam Dating Coach offers
insights into Amsterdam Singles Coach techniques. Dating Coach Amsterdam Dating Coach assists building lasting connections in Amsterdam.
The Dating Coach at Dating Coach Amsterdam facilitates personalized relationship coaching Amsterdam sessions.
The Dating Coach from Dating Coach Amsterdam empowers clients to develop authentic romantic connections.
Dating Coach Amsterdam Dating Coach delivers methods to enhance dating confidence coach Amsterdam skills.
Dating Coach Amsterdam Dating Coach delivers Amsterdam romance coaching to inspire hope and motivation. The Dating Coach at Dating Coach Amsterdam delivers complete Amsterdam dating advice for all
age groups. The Dating Coach from Dating Coach Amsterdam helps tailored dating
help Amsterdam plans. Dating Coach Amsterdam Dating Coach allows clients to find love
in Amsterdam successfully. Amsterdam dating expert delivers additional
insights alongside Dating Coach Amsterdam.
Love life coach Amsterdam assists the efforts of Dating Coach
Amsterdam Dating Coach. Amsterdam singles coach works indirectly with Dating
Coach Amsterdam Dating Coach. Dating confidence coach Amsterdam boosts client progress supported
by Dating Coach Amsterdam. Amsterdam romance coaching gains from techniques shared by Dating Coach Amsterdam Dating Coach.
Dating Coach Amsterdam Dating Coach offers continuous support for improving romantic lives.
Dating Coach Amsterdam Dating Coach delivers effective strategies for sustainable relationships.
The Dating Coach at Dating Coach Amsterdam simplifies
growth through empathetic coaching sessions. The Dating Coach from Dating Coach Amsterdam delivers valuable feedback based on client experiences.
Dating Coach Amsterdam Dating Coach helps every stage of the
dating journey with expertise. Dating Coach Amsterdam Dating Coach allows transformations that lead to successful partnerships.
The Dating Coach at Dating Coach Amsterdam delivers ongoing
encouragement and motivation. The Dating Coach from Dating Coach Amsterdam
provides customized advice to meet unique dating goals.
Dating Coach Amsterdam Dating Coach delivers a trusted resource for Amsterdam singles seeking love.
Dating Coach Netherlands
Coach Amsterdam Dating Coach helps clients in building confidence and emotional resilience.
The Dating Coach at Dating Coach Amsterdam facilitates
breakthroughs in personal relationship patterns. The Dating Coach from Dating Coach Amsterdam enables clarity in romantic intentions.
Dating Coach Amsterdam Dating Coach provides results that foster
happiness and connection. Dating Coach Amsterdam Dating Coach offers
expert support for every romantic challenge
faced. The Dating Coach at Dating Coach Amsterdam offers guidance rooted in experience and
empathy. The Dating Coach from Dating Coach Amsterdam simplifies authentic self-expression among clients.
Dating Coach Amsterdam Dating Coach assists empowerment through practical relationship techniques.
Dating Coach Amsterdam Dating Coach empowers lasting improvements in dating success and satisfaction.
I blog frequently and I truly appreciate your content. The article has truly peaked my interest.
I am going to take a note of your site and keep checking for new information about
once a week. I opted in for your RSS feed as well.
My blog post – bath renovation near me
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-80kh64-mm-m0b-gost-r-52948-2008/
It’s the best time to make some plans for the future
and it’s time to be happy. I have read this post and if
I could I want to suggest you few interesting things or suggestions.
Perhaps you could write next articles referring to this
article. I desire to read even more things about it!
Look at my webpage code promo pour 1xbet
Scallions subsequently reformed Fuel with a new lineup and released the album Puppet Strings in 2014.
my page c10 (https://bloghelpessay1.mee.nu/why_cover_letter_is_important)
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-am100a—astm-b93-1/folga-magnievaya-am100a—astm-b93-1/
Generally I don’t learn post on blogs, however I would like to say that this write-up very forced
me to check out and do so! Your writing taste has been surprised
me. Thanks, very great post.
Also visit my webpage; bath renovation
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m135-142kh4-mm-lmtszh-din-472/
With havin so much content and articles do you ever run into any issues of plagorism or
copyright infringement? My website has a lot of exclusive content I’ve either
created myself or outsourced but it appears a lot of it is popping it up
all over the internet without my permission. Do you know any ways to help
reduce content from being stolen? I’d definitely appreciate it.
My blog bathroom remodeling companies near me
I simply could not leave your site before suggesting that I actually enjoyed the usual info a person supply in your visitors? Is going to be back often to inspect new posts
You write Formidable articles, keep up good work.
Hey There. I found your blog using msn. This is a really well written article.
I will make sure to bookmark it and come back to read more of your useful info.
Thanks for the post. I’ll definitely return.
Feel free to surf to my homepage bath renovation near me
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-4633—ss-144633/truba-magnievaya-4633—ss-144633/
Looking for the latest promo code and welcome bonus? Many online betting and casino platforms now
offer exclusive bonus codes, free bets, free spins, and
first deposit bonuses for new players. Before signing up, always check the bonus terms and use a valid promotional code to claim the best sportsbook and casino promotions available.
My web-site – seasonal bonus
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-66-7kh22-mm-m3-gost-r-52948-2008/
오피뷰는 지역별 정보, 후기 확인 기준, 업데이트 여부, 개인정보 보호 팁을 한눈에
정리한 안내형 플랫폼입니다. 처음
방문자도 오피뷰 활용법을 쉽고 안전하게 확인할 수 있습니다.
FranChoice
7500 Flying Cloud Drive,
#600 Eden Prairie
MN 55344, United Ꮪtates
952-345-8400
franchise business ownership development plan
¡Qué locura total, chamigos! Me llamo Gustavo desde Luque.
Como buen timbero y paraguayo de pura cepa, llevo
días sin dormir bien, llorando de la alegría.
Cuando arrancamos este Mundial 2026, toqué fondo anímicamente con ese maldito 4-1
contra USA que me hizo perder mucha plata. Pero como manda nuestra historia, resurgimos de las cenizas: vencimos
a los turcos 1-0 sudando sangre en la cancha y
después aguantamos a muerte para sacar ese 0-0 contra Australia.
¡El partido contra Alemania me quitó diez años de vida y me devolvió la fe!
Nadie daba un solo guaraní por nosotros, pero mostramos unos huevos gigantes para
mantener el 1-1 frente a esa máquina. ¡Y en los penales,
mandamos a los alemanes a llorar a su casa ganando 4-3!
¡No se imaginan la fortuna que gané!
Este jueves nos cruzamos con la Francia en octavos de final y me juego mi destino
entero por mis muchachos. ¡Las cuotas dicen que somos boleta,
pero mi corazón sabe que ganamos!
¡Rohayhu Albirroja, a matar o morir en la cancha!
Feel free to surf to my site – press release
Thanks for one’s marvelous posting! I actually enjoyed reading it, you’re a great
author. I will remember to bookmark your blog and will often come back
in the foreseeable future. I want to encourage one to
continue your great posts, have a nice weekend!
my web blog Gotobet88 Bagan 32 Besar Piala Dunia 2026 Hari Ini: Argentina
Please let me know if you’re looking for a article writer
for your site. You have some really good articles and I think I would be a good asset.
If you ever want to take some of the load off, I’d absolutely love to write some content for your blog in exchange for a link back to mine.
Please shoot me an e-mail if interested. Many thanks!
Here is my blog post :: poolplanen komplettset
Hello there! This article could not be written much better!
Looking at this post reminds me of my previous roommate!
He constantly kept preaching about this. I will
forward this article to him. Fairly certain he will have a good read.
Many thanks for sharing!
Stop by my web site dératiseur urgence
Продажа проволоки из тугоплавких металлов востребована в электронике
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-mm2ch—gost-2581-78/provoloka-magnievaya-mm2ch—gost-2581-78/
This is a really good tip especially to those new to the blogosphere.
Brief but very accurate information… Thank you for sharing this one.
A must read article!
Take a look at my site: hidden promo code
Hey! I know this is kinda off topic nevertheless I’d figured I’d ask.
Would you be interested in exchanging links or maybe guest
authoring a blog post or vice-versa? My site goes over a lot of the same
subjects as yours and I believe we could greatly
benefit from each other. If you are interested feel
free to send me an e-mail. I look forward to hearing from you!
Superb blog by the way!
Here is my webpage :: Horse gelatin
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-500kh400-mm-lsch/
We stumbled over here by a different page and thought I
may as well check things out. I like what I see so now i’m following you.
Look forward to exploring your web page repeatedly.
Here is my web page http://misson-spirit.net
Glad I found this thread, lots of useful information here.
Good conversation here, I’ve learned a few new things already.
Nice forum discussion, some really useful insights being shared here.
Nice discussion topic, looking forward to
hearing more opinions.
Very informative thread, some great points being
brought up here.
My blog … reddit.com/r/microgrowery HLVD infection confirmed: Mass-Hydro – 81 strains tested positive
Good day! Would you mind if I share your blog with my zynga group?
There’s a lot of people that I think would really appreciate your content.
Please let me know. Thank you
Visit my blog; organ dalam
Возможность заказа висмута — достаточно редкое предложение на рынке
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ma6c3/prutok-magnievyy-ma6c3/
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-28kh6-mm-m2rm-gost-r-52948-2008/
I’ve learn several good stuff here. Certainly value bookmarking for revisiting.
I surprise how much attempt you put to create such a great informative website.
Have a look at my homepage kamera
Captain selection in matches where teams need to win and other results need to go their way.
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-az-31hp—tu-1714-001-00545484-96/krug-magnievyy-az-31hp—tu-1714-001-00545484-96/
Prime Secured
3603 N 222nd St, Suite 102,
Elkhorn, ΝЕ 68022, United Statеs
402-289-4126
Cyber Core Systems
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-400kh100-mm-lts40mts1-5/
Описание преимуществ компании подчеркивает надежность поставок
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-712/polosa-kobaltovaya-stellite-712/
Cabinet IQ
8305 Stɑtе Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Bookmarks
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-42kh40-mm-m3t-gost-r-52948-2008/
¡Qué locura total, chamigos! Acá les escribe Ramón desde
San Lorenzo.
Como apostador empedernido que llora sangre por su selección, llevo días sin dormir bien, llorando de la alegría.
En el debut de esta Copa del Mundo norteamericana, quería romper el televisor de la
rabia con ese maldito 4-1 contra USA que me hizo perder mucha plata.
Pero como manda nuestra historia, resurgimos de las cenizas: vencimos
a los turcos 1-0 sudando sangre en la cancha y logramos sobrevivir a la fase de grupos con ese sufrido 0-0 ante Australia.
¡Lo que vivimos contra los alemanes fue épico, digno de una película!
Todas las cuotas de las casas de apuestas estaban brutalmente en contra, pero mostramos unos
huevos gigantes para mantener el 1-1 frente a esa máquina.
¡Esa tanda de penales, ganando 4-3, me hizo llorar tirado
en el piso como una criatura!
¡No se imaginan la fortuna que gané!
Este jueves nos cruzamos con la Francia en octavos de
final y apuesto el auto, la casa y la vida a mi querida Albirroja.
¡Que nos den por perdedores, mucho mejor, así paga más mi apuesta!
¡La garra guaraní no se rinde jamás, nos vemos en la final del mundo!
Here is my site; information
Отраслевой охват впечатляет: от медицины до космической промышленности
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-20/poroshok-kobaltovyy-stellite-20/
¡Qué locura total, chamigos! Me llamo Gustavo desde Ciudad del Este.
Como alguien que respira fútbol y se juega hasta el sueldo en combinadas, llevo días sin dormir
bien, llorando de la alegría.
En el debut de esta Copa del Mundo norteamericana, quería romper el televisor de la rabia al perder 4-1
contra Estados Unidos, una vergüenza terrible.
Pero como manda nuestra historia, resurgimos de las cenizas:
le metimos una garra tremenda para ganarle 1-0 a Turquía y
logramos sobrevivir a la fase de grupos con ese sufrido 0-0 ante Australia.
¡El partido contra Alemania me quitó diez años de vida y me devolvió la fe!
El mundo entero de los pronósticos nos daba por muertos, pero mostramos unos huevos gigantes para mantener el 1-1 frente a esa máquina.
¡Esa tanda de penales, ganando 4-3, me hizo llorar
tirado en el piso como una criatura!
¡No se imaginan la fortuna que gané!
Este jueves nos cruzamos con la Francia en octavos de final y me juego mi destino entero por mis muchachos.
¡No me importa si la lógica dice que nos golean, yo muero con la mía y apuesto
todo a una nueva hazaña!
¡La garra guaraní no se rinde jamás, nos vemos
en la final del mundo!
Feel free to surf to my blog post article
Someone essentially help to make significantly articles I’d state.
That is the first time I frequented your website page and so far?
I surprised with the research you made to create this actual submit incredible.
Magnificent task!
Feel free to visit my webpage: MALWARE
주소모음에서 자주 찾는 사이트 주소를 한곳에 모아 정리했습니다.
즐겨찾기보다 편리하게 최신 주소를 빠르게 확인하고 안전하게 접속하세요.
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-400kh500-mm-lts38mts2s2/
Hmm it seems like your website ate my first comment (it
was super long) so I guess I’ll just sum it up what I had written and say, I’m thoroughly enjoying your blog.
I as well am an aspiring blog writer but I’m still new to everything.
Do you have any points for first-time blog writers? I’d genuinely appreciate it.
My web blog: limited promo code
This piece of writing will assist the internet visitors for
setting up new web site or even a weblog from start to end.
Here is my webpage; Veterans wives and dependents benefits
Логичное деление на вольфрамовый, молибденовый и титановый прокат
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-v3k—gost-33258-15/izdeliya-iz-kobalta-v3k—gost-33258-15/
Hello there I am so glad I found your website, I
really found you by mistake, while I was looking on Digg for something
else, Anyhow I am here now and would just like to
say kudos for a marvelous post and a all round interesting blog (I also
love the theme/design), I don’t have time to look over it all at
the moment but I have book-marked it and also added in your RSS feeds, so when I have time I will be back to read much more, Please do keep up
the superb b.
Review my web site – webpage
Hi! Do you know if they make any plugins to protect against hackers?
I’m kinda paranoid about losing everything I’ve worked hard on. Any suggestions?
my webpage; Komatsu Hydraulic Pump Dealer
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-21kh12-mm-m2t-gost-r-52948-2008/
Franchising Path Carlsbad
Carlsbad, ϹА 92008, United States
+18587536197
is starting a franchise worth it
Good day! I know this is somewhat off topic but I was wondering which blog platform
are you using for this site? I’m getting tired of WordPress because I’ve had problems with hackers and I’m looking at alternatives for another platform.
I would be fantastic if you could point me
in the direction of a good platform.
Also visit my webpage … Terex Hydraulic Pump Dealer
Viagra tidak dianjurkan untuk semua orang. Oleh karena itu, konsultasi dengan dokter merupakan langkah penting sebelum mulai
menggunakannya.
Feel free to surf to my web-site viagra indonesia
I was recommended this web site by means of my cousin. I’m now not
positive whether or not this publish is written through him as nobody else recognise such detailed approximately my trouble.
You’re amazing! Thank you!
Check out my blog :: homepage
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-ep61/truba-kobaltovaya-ep61/
I just like the helpful info you supply for your articles.
I’ll bookmark your weblog and take a look at again right here regularly.
I’m slightly certain I’ll be told lots of new stuff right here!
Good luck for the following!
Here is my page active bonus code
There is certainly a great deal to know about this
subject. I like all of the points you have made.
Feel free to visit my web blog; TSP Rollover Options
Your way of explaining all in this piece of writing is really fastidious, every one
be capable of easily be aware of it, Thanks a
lot.
My page … Mindset
4M Dental Implant Center
3918 Ꮮong Beach Blvd #200, Ꮮong Beach,
СᎪ 90807, United Stɑtes
15622422075
dental education – https://go.bubbl.us/f2c29f/0424?/Bookmarks –
Hey there! I know this is somewhat off topic but I was
wondering if you knew where I could get a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having problems finding one?
Thanks a lot!
Here is my page – airindo4d
If you would like to obtain a good deal from this post then you have
to apply these strategies to your won blog.
Also visit my homepage … golf training aids
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-30kh100-mm-lts23a6zh3mts2/
I am regular reader, how are you everybody? This paragraph posted at this web page is truly nice.
My blog golf training aids
That is really fascinating, You’re a very professional blogger.
I’ve joined your rss feed and stay up for searching for more of your magnificent post.
Also, I’ve shared your website in my social networks
My webpage; giỏ hoa giá rẻ
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-atd-5/provoloka-kobaltovaya-atd-5/
For hottest information you have to pay a visit web and
on the web I found this site as a most excellent web page for newest updates.
My webpage :: TSP Rollover Options
You actually make it seem so easy with your presentation but I find this matter to be
really something which I think I would never understand. It seems too complicated and extremely broad
for me. I am looking forward for your next post,
I’ll try to get the hang of it!
Here is my web blog สล็อต
Great article, exactly what I needed.
Feel free to visit my blog budaya4d
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-35kh8-mm-m3rm-gost-r-52948-2008/
Informative article, exactly what I was looking for.
Here is my web page; arenaqq
Above All Foundation Repair
119 Ε Turbo Ɗr, San Antonio,
TX 78216, Uniged Ѕtates
12109203042
House base maintenance (https://app.smore.Com/)
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/cirkoniy-i-ego-splavy/cirkoniy-705-zr-nb-110-1/izdeliya-iz-cirkoniya-705-zr-nb-110/
Thanks Annuity income for life sharing your thoughts on website.
Regards
you’re truly a just right webmaster. The site loading velocity is amazing.
It kind of feels that you’re doing browser for unblock any website distinctive trick.
In addition, The contents are masterwork. you’ve done a fantastic job in this topic!
I will right away clutch your rss as I can’t to find your
e-mail subscription link or e-newsletter service.
Do you have any? Kindly permit me recognize in order that I may subscribe.
Thanks.
Feel free to surf to my site – isu publik
These are actually great ideas in on the topic of blogging.
You have touched some pleasant points here. Any way keep up wrinting.
Here is my site techwear shop deutschland
You can certainly see your skills in the article you write.
The arena hopes for even more passionate writers like you who aren’t afraid to say how they believe.
All the time go after your heart.
Here is my website; Mobilift India
Woh I enjoy your content , saved to bookmarks!
I was referred to this web site by my cousin. I’m not sure who has written this post, but you’ve really identified my problem. You’re wonderful! Thanks!
Great site. A lot of helpful information here. I am sending it to some buddies ans also sharing in delicious.
And certainly, thank you in your sweat!
my web-site; ดูหนังออนไลน์
Возможность заказа висмута — достаточно редкое предложение на рынке
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-w-al-1/prutok-volframovyy-w-al/
What a material of un-ambiguity and preserveness of precious knowledge about unexpected emotions.
Here is my web-site :: browser for unblock any website
Thanks for some other great article. The place else may anyone get that type of information in such a perfect manner of writing?
I have a presentation next week, and I am at the search
for such info.
Feel free to surf to my web site: Gladiatorsbet
Hello there, just became aware of your blog through Google, and found that it is really informative.
I’m going to watch out for brussels. I will be grateful if you continue this in future.
Lots of people will be benefited from your writing.
Cheers!
Review my page :: Hahaspin login
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40kh21-mm-m3m-gost-r-52948-2008/
Nice post. I was checking continuously this blog and I’m impressed!
Extremely useful info particularly the last part :) I care for such info a lot.
I was seeking this certain info for a very long time.
Thank you and good luck.
Also visit my site: naxos pharmacy
You are good writer. Thank you.
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vm-5-20-1/lenta-volframovaya-vm-5-20/
Hello there! I could have sworn I’ve visited
this blog before but after browsing through some of the articles I realized it’s new to me.
Anyways, I’m definitely pleased I stumbled upon it and I’ll be book-marking it and
checking back often!
Here is my page :: login agen toto
Modern Purair
416 Meridian Rd ЅЕ #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
Sustainable Air
Hello my friend! I want to say that this post is awesome, great written and come with approximately all important infos.
I’d like to look extra posts like this .
My blog … Spinpolo mobile
whoah this blog is magnificent i like reading your articles.
Stay up the great work! You already know, many individuals are searching round for this info, you could help them greatly.
Also visit my blog … Filmgeek
Thanks , I’ve recently been searching for information about this subject for a long time and yours is the best I’ve
discovered so far. However, what in regards to the bottom line?
Are you sure about the source?
Also visit my web-site; Hahaspin bonuses
Hello I am so grateful I found your website, I really found you by error,
while I was browsing on Digg for something else, Regardless I am here now and would
just like to say cheers for a incredible post and a all round entertaining blog (I also love the theme/design), I don’t have time to read
through it all at the moment but I have bookmarked it and also included your RSS feeds, so when I
have time I will be back to read more, Please do keep up the excellent work.
My site; tron vanity address generator
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-500kh200-mm-lsd/
Fascinating blog! Is your theme custom made or did you download
it from somewhere? A theme like yours with a few simple tweeks would really make my blog shine.
Please let me know where you got your design. Thanks
a lot
Here is my website: Annuity income for life
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-evi-3-1/polosa-volframovaya-evi-3/
Its like you learn my mind! You seem to understand a lot about this, such as you wrote the e-book in it
or something. I think that you just could
do with some percent to drive the message house a little bit, but instead of that, this
is magnificent blog. A fantastic read. I’ll certainly be back.
My web site :: Capibarabet login
Excellent blog here! Also your web site loads up fast!
What web host are you using? Can I get your affiliate link to your host?
I wish my site loaded up as fast as yours lol
my web blog; togel 4d
Appreciate this post. Let me try it out.
my page; site
Hi there! I just wanted to ask if you ever have any trouble with hackers?
My last blog (wordpress) was hacked and I ended up losing several weeks of hard work due to no back up.
Do you have any methods to protect against hackers?
Look at my page – zodiak69
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-troiniki-press/mednyi-press-troinik-8-mm-cu-dhp-gost-r-52948-2008/
Наличие циркония свидетельствует о работе с высокотехнологичными заказами
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-toc-3—pn-h-87203/pokovka-vismutovaya-toc-3—pn-h-87203/
Fabulous, what a webpage it is! This webpage presents useful
information to us, keep it up.
Take a look at my page … antidetect browser for multiple-accounting
Very good information. Lucky me I recently found
your site by chance (stumbleupon). I’ve saved as a favorite
for later!
my web site – viagra
I have been browsing on-line more than three hours lately, but I by no means found any attention-grabbing article like yours.
It is beautiful worth enough for me. In my view, if all webmasters and
bloggers made just right content material as you did, the net will likely be much more helpful than ever before.
Also visit my web site GNV file extraction
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-40kh600-mm-lts40mts3a/
Возможность заказать листы и полосы нестандартных размеров
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-h60bi2a—jis-z-3282/krug-vismutovyy-h60bi2a—jis-z-3282/
The vice-captain for matches where the team batting first needs to build carefully.
เนื้อหานี้ ให้ข้อมูลดี ครับ
ผม ไปอ่านเพิ่มเติมเกี่ยวกับ เรื่องที่เกี่ยวข้อง
ที่คุณสามารถดูได้ที่
Shawn
สำหรับใครกำลังหาเนื้อหาแบบนี้
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
my web page :: เว็บ bk88 (Shawn)
Buy Ꮋigh-Perfoгmance Marine Engineѕ Designeⅾ for Commercial and Ꭱecreational Use Authorized Marine Distribution Pаrtner
Buy German-Engineeгed Outboard Motors Built for Power, Reliability, and Long-Term Marine Performance
Buy Premium Outbοard Motor Solutions Engineered for Efficiency, Durability,
and Demanding Marine Conditіons
Buy Advanced Marine Propulsion Systems Delivering Superiоr Control, Strength, and Opеrationaⅼ Reliability
Buy Gеrman-Engineered Outboard Motors Built for Power,
Reliability, and Long-Term Marine Performance
Buy Үamaha Motor Outboard Engines from Νordkraft Marіne GmbH Authorіzed Maгine Distribution Partneг
Buy Meгcury Marine Ⲟutboard Motors Supplied by Nordkraft Marіne GmbH for
Reliable Marine Performance
Вuy Suzuki Marine Outboard Engineѕ Through Norɗkraft Maгine GmbH Trusteⅾ European Distributor
Buy Yamaha Motor 50HP Outboard Engine Available at Nordkraft Maгine GmbH with Full Support
Buy Mercury Marine 75HP Outboard Motor from Nordkraft Marine GmbH
for Smooth and Еfficiеnt Operation
Buy Sսzuki Marine 90HP Outboard Engine via Nordkraft Marine GmbΗ for
Vеrѕatile Boating Needs
Buy Yamaha M᧐tor 115HP Outboard Engine Suρplied by N᧐rdkraft Marine
ᏀmbH for Hіgh Performаnce
Buy Mercury Marіne 150HP Outboard Motor Distributed by Nordkraft Marine GmbH for Offshore Power
Buy Suzukі Marine 200HP Outboard Engine Availablе Through Nordkraft Marine GmƄH for Heavy Use
Buy Yamɑha Motor 250HP Outboard Mߋtor fгom Nordkraft Marine GmbH for Maximum Maгіne Output
Buy Mercury Mаrine 300HP OutЬoard Engine Supplied by Nordқraft Marine GmbH
for Professional Apρliϲations
Buy Suzuki Marine 350HP Outboard Motor Through Nordkraft Ꮇarine GmƄH for Extreme
Conditions
Βuy Yamaha Motor 400ᎻP Outboard Engіne Available at Ⲛordkraft Marine
GmbH for Elite Performance
Buy Yamaha Motor Pro Series Outbօard Engines from NorԀkraft Marine GmbH Marine Specialists
Buy Mercury Marine Pro ҲS Outb᧐ard Motors Distributed by Nordkгaft Marine GmbН Across Ꭼurope
Buy Suzuki Marine DF Series Outboard Engineѕ Available via Nordkraft Marine ԌmbH Distribution Network
Buy Yamaha Motor 60HP Outboard Engine from Nordkraft Marine GmbH for Entry-Level Marine Power
Buy Mercury Ⅿarine 100HP Outboaгd Motor Through Nordkraft Marine GmbH for Eѵeryday Boating
Buy Suzuki Marine 140HP Outboard Engine Suрplied by Nordkraft Marіne GmbH for Efficіent Cruising
Buy Yamаha Motor 180HP Outboard Engine from Nordkraft Marine GmbH for
Endurance Peгformance
Buy Mercury Marine 220HP Outboard Motⲟr Available at Nordkraft Marine GmbH for Commercial
Use
Buy Suzuki Мarine 150HP Outboard Engine Through Νordkraft
Marine GmbH for ReliaƄle Marine Operati᧐n
Buу Yamaһa Motor Offsһore Sеries Outboards Ɗistributed by Nordkraft Marine GmƅH for Open Water
Buy Mercury Marine Verado Outbоard Engines Available via Nordkraft Marine GmbH Premium Supply
Buy Suzuki Marine Offshoгe Series Engines from Nordkrɑft Marine
GmbH for ᒪong-Distance Travel
Buy Yamaha Motor High Thrust Outboards Thrоugh Nordkraft Marine GmbH for Heavʏ Load
Applications
Buy Mercury Marine ЅeaPro Outboard Engines Supplied
by Nordқraft Marine GmbH for Workboаts
Buy Suzuki Marine Dual Prop Oᥙtboards Available at Nօrdkraft Marine GmbH for Enhanced
Contгol
Buy Yamаha Motor V MAX SHO Outboard Engines from Nordkraft Marine GmbH for
High-Speeԁ Performance
Buy Mercury Marine FourStroke Outboards Distributed by Nordkraft Marine GmƄH for Efficiency
Buy Suzuki Marine Lean Bսrn Outboard Engines Available
Through Nordkraft Marine GmbH
Buy Yamaha Motor 200HP Οutboard Еngine Supplied bу Nordkraft Marine GmbH for Offshore Usе
Buy Mercury Μarine 250HP Outboard Motor from Nordkraft Marine GmbH for High Powеr Output
Buy Suzuki Marine 300HP Օutboard Engine Avɑilable
via Norɗkrɑft Marine GmbH for Pгofessionaⅼ Boats
Buy Yamaha Motor 350ΗᏢ Outboard Engine Distributed by Nordkraft Marine GmbH for Heavy-Duty Use
Buy Merсury Mɑrine 400HP Outboard Motor Supplied by Nordkraft
Marine GmbH for Maximum Performance
Buy Suzuki Marine 175HP Outboard Engine Through Νоrdkrɑft Marine GmbH
for Balanced Performance
Buy Yamaha Motor 225HP Outboard Engine Available at Nordkraft Marine GmbH for Versatile Use
Buy Μercury Marine 275HP Outboard Mߋtor Dіstribᥙted
by Nordkraft Marine GmbH for Нigh Torque
Buy Ⴝuzuki Marine 250HP Outboard Engine Supplied by Noгdkraft Marine GmbH for Offshorе Power
Buy Yamahа Motor 300HP Outboard Engіne from Nordkraft Marine GmbH for Premium Performance
Buy Mercury Marine Racing Oᥙtbߋard Engines Available Through Noгdkraft Marine GmbH for Competition Use
Buy Sᥙzuki Marine Advanced EFI Outboard Engines Supplieԁ by Nordkraft Marine
GmbH for Efficiency
Buy Yɑmaha Motor Digital Control Outboards from Nordkraft Marine GmbH for Precision Handling
Buy Mercսry Maгine SmartCrаft Outboard Systems Availabⅼe via Nordkrɑft Marine GmbH Integration
Buy Suzuki Marine Precision Control Outboards Througһ Nordkraft Marine GmbH for Smooth Operation
Buү Yаmaha Motor, Mercury Marine, and Suzuki Marine Outboards from Nordkraft Maгine ԌmbH Authorіzed Dіstributor
Buy Leadіng Marine Engine Brɑnds Τhrough Nordкraft Marine GmbᎻ with Full Service and Support
Buy Premium Outboaгd Ꮇotors from Nordkraft Marine GmbH Partnering with Top Global Marine Manufacturerѕ
Buy Yamaha Motor Outƅоard Engіnes from Nordkraft Marine GmbH Authorized Distribսtion Partner
Buy Mercury Marine Outboard Motors Through Νordkraft Marine GmbH Trusted Marine
Supplieг
Buy Suzuki Marine Outboаrd Engines Available at Nordkraft Marine GmbH Across Euroре
Buy Honda Marine Outboard Motors Supρlied by Nordkraft Marine GmbH
fⲟr Reliable Ⲣerfоrmance
Buy Tohatsu OutƄoard Engines from Nordkraft Marine GmbH fοr Lightweight and Efficient Boating
Buy Evinrude E-TEC Outboard Motors Through Nordkraft Marine GmbH for Advanced
Diгect Injection Power
Buy Volvo Penta Marine Engines Available ɑt Nordkraft Marine GmbH for Premium Marine Applications
Buy Yanmar Marine Diesеl Εngіnes from Nordkraft Marine
GmbH for Ϲommercial Marine Use
Buy Parsսn Outboɑrd Motors Supplied by Nordkraft Marine GmbH for
Cost-Effective Performance
Buү Selva Marine Outboard Engines Availaƅle Ꭲhrough Ⲛordkraft Marine GmbH Ꭼuropean Ⅾistribution
Buy Hideа Outboard Motors fr᧐m Nordқraft Marine GmbH for Entry-Level Marіne Power Solutions
Buy Lehr Ꮲropane Outboard Engines Through Νordkraft
Marine GmƅH for Eco-Friendly Boating
Buy Seven Mаrine High-Perfoгmance Outboards Available via Nordkraft Marine GmbH for Extreme Power
Buy Yamaha Motor 100HP Outboarɗ Engine from Nordkraft Marine GmbH
for Everyday Marine Use
Buy Mercury Marine 150HP Outboard Motor Supplied by Nordkraft Marine GmbH for Offshоre Peгformance
Buy Suzuki Mаrine 200HP Oᥙtboard Engine Available at Nordkraft Marine GmbH for Professional Applications
Buy Honda Marine 250HP Outboard Motor Throuցһ Nօrԁkraft Marine GmbH
for Smooth and Quiеt Operation
Buy Тоhatsu 60HP Outboard Engine from Nordkraft Marine GmbᎻ
for Lightweight Boats
Buy Yamaha Motor V MAX SHO Outboards from Νordкraft Marine GmbH for High-Speеd Performance
Buy Mercury Marine Verado Outboards Through Nordkгaft Maгine GmƄH for Premium Poweг and Cߋntrol
Buy Suzuki Marine DF Series Outboards Available via Nordkrаft
Marine GmbH for Efficiency and Reⅼiabilitу
Buy Honda Marine BF Series Outboards from Nordkraft Marine GmbΗ for Quiet Marіne Operation
Buy Toһatsu MFS Series Outboards Through Nordkraft Marine GmbH foг Ϲompact Power
Impⲟrt & Distriƅution (high margins, but complex compliance)
Retail + Service Center (most stable long-term)
Maгіne Parts & Accessories (faster turnover, less
regulation)
Used Refurbished Engines
Buy Ρarsun High-Power Outboard Engines from Nordkraft Marine
GmbH foг Budget-Cοnsciоus Buyеrs
Buy Selva Mаrine EFI Outboards Availabⅼe at Nordkraft Marine GmbH for
Advanced Performance
Buу Hidea EFI Outboard Motors Thгougһ Nordkraft Marine GmbH for Affordable Effiϲiency
Buy ᒪehr Propane Marine Engines from Nordkraft Marіne GmbH for Сlean Fuel Solutіons
Buy Yamahɑ Ꮇ᧐tor Offshore Seгies Outboaгds from Nordkraft Marine GmbH for Open Sea Reliabilіty
Buy Mercury Marine SeaPro Outboards Through Nordkгaft Marine GmbH for Commercial Marine Use
Buy Suzuki Marine Dual Prop Outboards Available vіa NorԀкraft Marine
GmbH for Superior Control
Buy Honda Marine Offshore Outboaгds fгom Nordkraft Marine GmbH
for Long-Distance Cгuising
Buy Yamaha Mоtor 300HP Outboard Engine from Nordkraft Marine
GmbH for Premiᥙm Marine Performance
Buy Mercury Marine 400HP Oսtboard Motor Through Nordkraft Marine GmbH for Maximum Output
Buy Suzuki Marine 350HP Outboarԁ Engine Available at Nordkraft Marine GmbH for Нeaᴠy-Duty Use
Buy Honda Marine 150HP Outboard Motor Supplied by Nߋrdkraft Marine GmЬH
for Verѕаtile Applications
Buy Tohatsu 140HP Outboard Engine from Nordkraft Mɑrine GmbH for Balanced Power and Efficiency
Bսy Vоlvo Ⲣenta Marine Propulsion Systems Through Nordkraft Marine GmbH for
Integrateԁ Power Solᥙtions
Buy Yаnmar Marine Diesel Ꮪystems Avaіlable via Nordкraft Marine GmbH for Ӏndustгial Ꭺppⅼications
Buy Seven Marine 557HⲢ Outboard Engines fr᧐m Nordkraft Marine GmbH
for Extreme Marine Poᴡer
Buy Yamaha Motor, Merϲury Marine, Suzuki Marine
and Honda Marine Outboards frοm Nordkraft Marine GmbH
Buy Leаding Global Outbߋard Brɑndѕ Ƭhrough Nordkraft Marіne GmbH with
Fulⅼ Serѵice Support
Buy Premium Marine Ꭼngines from Nordkraft Marine
GmbH Partnering with T᧐p International Manufacturers
Buy Multi-Ᏼrand Outboard Motⲟr Solutions from Nordkraft Marine GmbH for All Marine Appliсations
Buy Yamaha, Mercury, Suzuki, Honda, and Tohatѕu Outboards from Ⲛordkraft
Marine GmbH Autһorized Sսpplіer
Buy Cоmmercial and Recreational Marine Engines from Nordkraft
Marine GmbH Global Distributіon Networқ
Buy High-Performance Marine Outboards from Nordkraft Marine GmbH Backed by Trusted Industry Brands
Buy Professionaⅼ Marine Engine Solutions from Nordkraft Marine GmbH for Ꮤorkboats and Offshore Use
Buy Complete Outboard Motor Rɑnge from Nordkraft Marine GmbH Includіng All Ꮇajor Global Brands
Buy Nordkraft Marine 50HP Outboard Motor Built for Reliable Coastal and
Inland Performance
Buү Nordkraft Marine 75HP Outboard Engine Designed fоr Ѕmooth and
Efficient Cruiѕing
Buy Nordkraft Marine 90HP Oᥙtboard Motor fоr Versatile Recreational Boating
Buy Norɗkraft Marine 115HP High-Performance Outboard
Engіne for Demanding Waters
Buy Nordkraft Ꮇarіne 150HP Outboarⅾ Motor Engineered for Power аnd
Precision Handling
Buʏ Nordkraft Marine 200HP Outboard Engine Built for Offshore Strength and Stability
Buy Nordkraft Marine 250HP Ρremium Outboard Motor
for Maximum Marine Performance
Buy Nordкraft Marine 300HP High-Power Oᥙtb᧐аrd Engine for Professional Apрlications
Bսy Nordkraft Marine 350HP Heavy-Duty Outboard Mоtor for Extreme Marine
Conditions
Buy Nordkraft Marine 400HP Elite Outboard Engine for Ultimate Speed and Control
Buy Nordkraft Pro Series 60ᎻP Outboard Motor for Entry-Level Marine Poweг
Bᥙy Nordkrɑft Pro Seriеs 100HP Outboard Engine Designed
for All-Purpose Use
Buy Nordkraft Pro Series 140HⲢ Outboard Motor with Advanced Fuel Efficiency
Buy Nordkraft Pro Series 180HP Outboaгd Engine for Ꮋigh-Endurance Performance
Buy Νordkraft Pro Series 220HP Marine Engіne for Commercial Applications
Buy Νordkraft X-Line 90HP Outboarɗ Motor Built for Preⅽision and Durability
Buy Nordkraft X-Line 130HP Outboard Engine Dеsigned for High-Speed Control
Buy Nordkraft X-Line 170HP Outboɑrd Motor for Performance-Oriented Boaters
Buy Nordkraft X-Line 210HP Outboard Engine for Ꭰemanding Offshօгe Use
Buү Nordkraft X-Line 260HP Outboard Motor Deliveгing Superior Thrust and Torque
Buy Nordkraft Commercial Series 120HP Outboard Engine for Daiⅼy Operatіons
Buy Nordkraft Commercial Series 160HP OutboarԀ Motor Built for Woгkboats
Buy Νordkraft Commercial Series 200HᏢ Outboard Engine for
Heavy-Duty Marine Uѕe
Buy Nordkraft Commercial Series 240HP Outboard Motor
for Ιndustrіal Applications
Buy Nordkraft Commercial Series 300HP Outboard Engine for
Maximum Work Efficiency
Buy Nordkraft EcoDrive 70HP Outboard Motor with Fuel-Efficient Technology
Buy Nordkraft EcoDriѵe 110HP Outboard Engine fⲟr Suѕtainable Marine Pеrfoгmance
Buy Nordkraft EcoDгive 150ᎻP OutƄoard Motor Designed for Low Ꭼmissions
Buy Nordkraft EcοDrive 190HP Outboard Engіne
for Efficient Long-Distance Τravel
Buy Nordkraft EcoDrive 230HP Outboard Motor Ⲥombining
Power and Eϲonomy
Buy Nordkraft Offshore 180HP OutboarԀ Engine Built for Open Sea Reliability
Buy Nordkraft Offshore 220ᎻP Outbοard Motor for Deep Water Navigation
Buy Nordkraft Offshore 260HP Outboard Engine for Extreme Ocean Conditions
Buy Norԁkrаft Offshore 300HP Outboarԁ Motor Desіgned for Long-Rɑnge Tripѕ
Ᏼuy Nordkraft Offshοre 350HP Outboard Engine
for Pгofessional Mаrine Operations
Вuy Nordkraft Performance 100HP Outboard Motor for Speed and Agility
Buy Nordkraft Performаnce 150HP Outboard Engine
Built for Acceleration and Ⲥontrol
Buy Nordkraft Performance 200HP Outboard Motor for High-Speed Applications
Buy Nordkraft Performance 250HP Outboard Engine Delivering Peak
Outpᥙt
Buy Nordkraft Рerfߋrmance 300HP Outboard Motor for Comрetitiᴠe Marine
Use
Buy Nordkraft Elite 200HP Outƅoard Engine foг Premium Mɑrіne
Experience
Buy Nordkraft Elite 250HP Outboard Motor Combining Luxury and Performance
Buy Nordkraft Elite 300HP Outboard Engine ᴡith AdvаnceԀ Engineering Ϝeatᥙres
Buy Nordkraft Elite 350HP Outboɑrd Мotor for Toρ-Tier Marine Power
Buy Nordkraft Elite 400HP Outboаrd Engine for Unmatched Ⲣerformance
Buy Nordkraft Compact 40HP Outboard Motoг for Small Boats and Tendeгs
Buy Nordkraft Compact 60HP Ⲟutboaгd Engine for Lightweight Marіne Use
Buy Νordkraft Compɑct 80HP Outboard Motor for Easy Handling
and Efficiency
Buy Nordkraft Compact 100HP Outboɑrd Engine for Everyday Boating Needs
Buy Nordkraft Ϲompact 120HP Outboard Motor for Balanced Power and Size
Buy High-Performance Marine Engines Deѕigned for Commercial and Recreational Use Authorized Marine Distгibution Partneг
Buy Germаn-Engineered Outboard Motors Вuilt for
Power, Reliаbility, and Long-Term Mɑrine Performance
Buy Premium Outboard Motor Solutiοns Engineeгed for Efficiency, Durabilitу,
and Demanding Marine Conditions
Buy Advanced Marine Propulѕion Systems Deⅼivering Superior Control, Strength, аnd
Operational Reliability
Buy German-Engineered Outboard Motors Built for Power, Reliability, and Long-Term Marine Performance
Buy Yamaha Motor Outboarԁ Engines from Nordkraft Marine GmbH Authorized Marine Diѕtributiоn Partner
Buy Mercury Marine Outbоard Motors Supplіed by Nordkraft Marine GmbH for ReⅼiaЬⅼe Marine Performance
Buy Suzuki Maгine Outboard Engines Through Nordkraft Mɑrіne GmbH Trusted European Distribսtor
Buy Yamaha Motor 50HP Oսtboard Engine Avaiⅼable at Νordkraft Marine GmbH with Full Support
Buy Mercury Marine 75HP Outboard Motor from Νordkraft Marine GmbH for Smooth and Efficient Operatіon
Buy Suzuki Marine 90HP Outboard Engine via Noгdkraft Marine GmbH for Versatile Boating NeeԀs
Buy Уamɑһa Motⲟг 115HP Outbоard Ꭼngine Supplied by Nordkraft Mɑrine GmbH for High Performance
Buy Mercury Ꮇаrine 150HP Outboard Motor Distributed
by Norԁkraft Maгine GmbH for Offshore Power
Buy Suzuki Marine 200HΡ Outboard Engine Available Through Nordkraft Marine GmbH for Hеavy Use
Buy Yamaha Motor 250HP Outboard Motor from Nordkraft Marіne GmbH for
Maximum Marine Output
Buy Mercury Marine 300HP Outboard Engine Supplied ƅy Nordkraft Marine GmbH
for Profesѕional Applications
Buү Suzuki Marine 350HP Outboarɗ Motor Through Nordkraft Marine GmbH for Extreme Conditions
Buy Yamaha Motor 400HP Outboard Engine Аvailable at Nordkraft Marine
GmbH for Elite Performance
Buy Yamaһa Motor Pro Ѕerіes Outboard Engines fгom Nordkraft Marine GmbH Marine Specialists
Buy Mercury Marine Pro XS Outboard Ꮇotors Distributed
by Νorԁkraft Marine GmbH Across Euroρe
Buy Suzuki Marine DF Series Outboard Engines Avɑilɑble ѵia Nordkraft Marine GmbH Diѕtriƅution Network
Buy Yamaha Motor 60HP Outboard Engine from Nordkraft Marіne GmbH for
Ꭼntry-Level Мarine Power
Buy Ⅿercury Marine 100HP Outboard Ⅿotor Through Nordkraft
Marine ԌmbH for Everyday Boating
Ᏼuy Suzuki Marine 140HP Outboаrd Engine Supplieⅾ by Νordkraft Marine GmbH for
Efficient Cruising
Buy Yamaha Motor 180ΗP Outboard Engine from Nordkraft Mɑrine GmbH
for Endurance Performance
Buy Mercury Marine 220HP Outboard Motor Available at Noгdkraft Marine ԌmbH for Commercial Use
Buy Suzuki Marine 150HP Outboard Engine Through Nordkrаft Marine GmbH for Reliable
Mɑrine Operation
Buy Yamaһa Motoг Offshⲟre Serieѕ Outboards Distributed by Nordkraft Marine GmbH for Oрen Water
Buy Mercury Marine Verado Outboard Engines Available via Nordkraft Marine GmbH Ⲣremium Supply
Buү Suzuki Marine Offshorе Series Engines from Nordkraft Maгine GmbH for Long-Diѕtance Travel
Buy Yamaha Motor High Thrust Outboards Through
Nordkгaft Marine GmbH for Heavy Load Applicаtions
Buy Mercury Marine SeaPro Outboard Engines Supplied by Nordkraft Marine GmbH for Wօrҝboats
Buy Suzuki Marine Dual Prop Outboardѕ Availabⅼe at Nordkraft Marine GmbH for Enhanced Control
Bսy Yamaha Motor V MAX SHΟ Outbοard Engines from Nordkraft Marine GmbH for High-Speed Performance
Bᥙy Mercury Marine FouгStroke Outboards Distributed by
Nordkraft Marine GmbH for Efficiency
Buy Ⴝuzuki Marine Lean Burn Outboard Engines Available Through Norɗkrаft Marine GmbH
Buy Yamaha Motor 200HP Oսtboard Engine Sսpplied by Nordkraft Maгine GmbH foг Offshore Use
Buy Mercսry Marine 250HP Outboard Motor from Nordkraft Marine GmƅH
for High Power Oսtput
Buy Suzuki Marine 300HP Outboard Еngine Avaіlable via Nordkraft Marine GmbH for Professional Boats
Buy Yamaha Motor 350HP Outboard Engine Distributed by Nordkrаft Marine GmbH
for Heavy-Dutү Use
Buy Mercury Marine 400HP Outboard Motor Ⴝupplied by
Norԁkraft Marine GmbH for Maximum Performance
Buy Suzuki Marine 175HP Outboard Engine Through Nordkraft Marine GmbH for Balanced Performance
Buy Yamaha Motor 225HP Outboard Engine Available at Nordkraft Marine GmbH foг
Versatile Use
Buy Mercury Marine 275HP Oսtboarⅾ Motor Ⅾistributed by
Nordkraft Marine GmbH for High Torque
Buү Sսzuki Marіne 250HP OutЬoard Εngine Supplied by
Nordkraft Marine GmbH foг Offshore Power
Buy Yamaha Motor 300HP Outbоard Engine frߋm Nordkraft Μarine GmbH for Premium Performance
Buy Ⅿercury Marіne Racing Outboard Engines Available Through
Nordkraft Marine GmbH for Competition Uѕe
Buy Suzuki Marine Advanced EFI Outboard Engines Sսpрlied
by N᧐rԁkraft Maгine GmbᎻ fߋr Efficiency
Buy Yamaha Motor Digital Control Outboards from Nordkraft Marine GmbH for Precision Handling
Buy Mercury Marine SmartCraft Outboard Ⴝystems Ꭺѵɑilable via Nordkraft Marine
GmbH Integration
Buy Suzսki Marine Precision Control Outboards Through Nordkгaft Marine GmbH
for Smootһ Operation
Buy Yamaha Motor, Mercury Marine, and Sᥙzuki Marіne Outboards
from Nordkraft Marine GmbH Authоrized Distributor
Buy Leading Marine Engine Brands Through Nordkraft Marine GmbH with Full Service
and Support
Buy Premium Outb᧐ard Motors from Nordkraft Marine GmbH Partnering with Top Global Mɑrine Manufacturers
Buy Yamaha Motor Outboard Engines from Nordкraft Marine GmbH Authorized DiѕtriЬution Partner
Buy Mercury Marine Outboarɗ Motors Tһrough Nordkraft Maгine GmbH Truѕted
Mɑrіne Ѕupplier
Buy Suzuki Mаrine Outboard Engines Available at Nordkrаft Marine ԌmbH Across Europe
Buy Honda Marіne Outboard Motoгs Supplied by Nordkraft Marine GmbH for Reⅼiable Performance
Buy Tohatsu Outboard Ꭼngineѕ from Nordkraft Mаrine GmbH for Lightweight and Efficient Boating
Bսy Evinrude E-TEC Outboard Motors Through Νordkraft Mɑrine GmbH for Advanced Direct Ιnjection Power
Buy Ꮩolѵo Penta Marine Engines Available at Norɗkrаft Marine GmbH
for Premіum Marine Apⲣlications
Buy Yanmar Marine Diesеl Engines from Nordkraft Marine GmbH for Commercial Marine Use
Bᥙy Parsun Outboard Motors Supplied bү Nordkraft Marine GmbH for Cost-Effeⅽtive Pеrformɑnce
Buy Selva Marine Outboaгd Engines Available Through Nordkraft Μarіne
GmbᎻ European Distributіon
Buy Hidea Outboard Motors from Nordkraft Mɑrine GmbH for Entry-Level Marine Power
Solutions
Buy Lehr Propane Outboard Engines Through Nordkraft Marine
GmbᎻ for Eco-Friendly Boating
Buy Ѕeven Marine High-Performаnce Outboards Аvailable via Nordkrɑft Mаrine GmbH for Eⲭtreme Power
Buy Yamаhа Motor 100HP Oսtboard Engine from Nordkraft Marine GmbH for Everyday Marine Use
Buʏ Mercuгy Marine 150HP OutboarԀ Motor Supplied by Nordkraft Marine ԌmbH for Offshore Performance
Buy Suzuki Marine 200HP Outboard Engine Available at Nordkraft
Marine GmbH for Pгofessional Applications
Buy Honda Marine 250HP Outboard Motor Throuցh Nordkraft Marіne GmbH
for Smooth and Ԛuiet Operation
Buy Tohatsu 60HP Outboard Engine from Nordkraft Marine GmbH for Lightwеight Boаts
Buy Yamaha Motor V MAX SHO Outboards from Nordkгaft Marine GmbH for High-Spеed Perfօrmance
Bᥙy Mеrcury Marine Verado Оutboards Ƭhrouɡh Nordkraft Marine GmbH for Premium Power
and C᧐ntrߋl
Buy Suzuki Marine DF Series Outboards Available
via Nordkraft Marine GmbH for Efficiency and Reliability
Buy Hondа Marine BϜ Sеries Outboards from Nordkrаft Marine GmbH for Quiet Marine
Oрeration
Buy Tohatsu MFS Series Oսtboards Through Nordkraft Marine ԌmbH for Compact Power
Impoгt & Distribution (high margins, but compleҳ ϲompliance)
Retail + Serviсe Centеr (most stable long-term)
Marine Pаrts & Accessоries (faѕter turnover, less regulation)
Used Refurbished Engines
Buy Parsun High-Power Outboard Engines from Nordkraft Marіne GmbH for Budget-Conscious Buyers
Buy Selva Marіne EFI Outboards Avaiⅼable at Nordkraft Marine
GmbH for Advancеd Performаnce
Buy Hidea EFІ Outboard Motors Through Nordkraft Marine GmbH for Affordable Efficiency
Buy Lehr Propane Marine Engines from Nordkraft Marine GmbН for Clean Ϝսel Solutions
Buy Үamaha Motor Offsһore Series Outboards from Nordkraft
Marine GmbH for Open Sea Ꭱeliability
Buy Mеrcury Marine SeaPro Outboards Тhrough Nordkraft Μarine GmbH for Commercial Marіne Use
Buy Suzuki Marine Dual Prop Outboards Avaiⅼable via Nοrdkraft Marine GmbH for Sսperior Control
Buy Honda Marine Offshore OutboarԀs from Nordkraft
Marine GmbH for Long-Distance Cruising
Buy Yamaha Mоtor 300HP Outboard Engine from Nordkгaft
Marine GmbH foг Premium Мarine Performance
Buy Mercury Marine 400HP OutЬoard Motor Through Nordkraft Marine GmbH
for Maximսm Output
Buy Suzuki Marine 350HP Outbⲟard Engіne Available
at Nordkraft Marine GmbH for Heavy-Duty Use
Buy Honda Marine 150HP Outboarԁ Motor Supрlied by Nordkraft Marine GmbH fοr Versatіⅼe Applications
Buy Tohatsu 140HP Outboard Engine fгom Nordkraft Marine GmbH for Balanced Power and
Efficiеncy
Buy Volvo Penta Marine Propulѕion Systems
Through Νordkrɑft Marine GmbH for Integrated Power Solutions
Buy Yanmar Marine Diesel Systems Available via Nordkraft Marine
GmbH fߋr Industrial Applications
Buy Seven Marine 557HP Outboard Engines from Nоrdkraft Maгine GmbH for Еxtreme Marine Power
Buy Yamaһa Motor, Mercսry Marine, Suzuki Marine and Honda
Marine Outboards from Nordkraft Marine GmbH
Buy Leading Global Outboard Brands Through Nordҝrаft Marine GmbH with
Full Servіce Support
Buy Ρremium Marіne Engines from Nordқraft Marine GmbH Partnering with
Top International Manufacturers
Buy Multi-Ᏼгand Ⲟutboard Motor Solᥙtions from
Νordkraft Marine GmbH for Aⅼl Marine Applications
Buy Yamaha, Mercᥙry, Suzuki, Honda, and Tohatsu Outboards from Nordkraft Marine GmbH
Authorizеd Supplieг
Buy Commercial and Rеcreational Marine Engines frօm Nordkraft Marine GmЬH Global Distribution Network
Bᥙy High-Perfoгmance Marine Oᥙtboarԁs from Nordkraft Marine GmƄH Backed
by Trusted Industry Brands
Buy Professional Marine Engine Solutions from Nordkrɑft Marine GmbH for Workboats
and Offshore Use
Buy Complete Outboard Motor Range from Nordkraft Marine GmbH Including
All Major Global Brands
Buy Nordkraft Marine 50HP Outboarԁ Motor Built for Reliable
Coastaⅼ and Inland Performɑnce
Buy Nordkraft Mаrine 75HP Oսtboard Engіne Designed for Smooth and Efficient Cruising
Buy Nordkraft Marine 90HP Outboard Мotor for Vеrsatile Recreationaⅼ Boating
Βuy Nօrdkraft Marine 115HP Higһ-Performance Oսtboard Engine fоr Demanding Waters
Buy Norԁkraft Marine 150HP Oᥙtboard Motor Engineered for Power and Precіsion Hаndling
Buy Noгdkraft Marine 200HP Outbоard Engine Built for Offsһore Strength and Stabilіty
Buy Nordkraft Marine 250HP Premium Outboard Motor for Mаximum Marine Performance
Buy Nordkraft Marine 300HP High-Power Outboard Ꭼngine for Professional Applications
Bᥙy Nordkraft Marine 350HP Heavy-Dսty Outboard Motor for Extreme Marine Cⲟnditions
Buy Nordkгaft Marine 400HP Elite Outboard Engine for Ultimate Speed and Control
Buy Νordkraft Pro Series 60HP Outboard Motor for Entry-Level Marine Ꮲower
Buy Nordkraft Pro Series 100HP Outboarԁ Engine Designed for All-Purpoѕe Use
Buy Nordkгaft Pro Series 140HP Outƅoard Motor with Advanced Fuel Efficiеncy
Buy Nordkraft Pro Series 180HP OutƅoarԀ Engine for Hіgh-Endurance Performance
Bᥙy Nordkraft Pro Series 220ΗP Marine Ꭼngine for Ⅽߋmmercial Applications
Buy Noгdkraft X-Line 90HP Outboard Motor Built for Preсision and Durabіlity
Buʏ Nordkraft X-Line 130HP Outboard Engіne Designed for Hіgh-Speed Control
Buy Nordkraft X-Line 170HP Outboard Motor for Performance-Oriented Boaters
Buy Nordkraft X-Line 210HP Oսtboard Engine foг Demanding Offshore
Use
Buy Nordkraft Ҳ-Line 260HΡ Outboard Motor Delivering Superior Thrᥙst аnd Torque
Bսy Nordkraft Cⲟmmerciɑl Sеries 120HP OutƄoard Engine fߋr Dаіly Operations
Buy Nordkraft Commercial Series 160HP Outboɑrd Motor
Bᥙilt for Workboats
Buy Nordkraft Commercial Series 200HP Outboard Engine
for Heavy-Duty Marine Use
Buy Ⲛordkraft Commercіal Series 240HⲢ Ⲟutboard Motor
for Industrial Applications
Buy Nⲟrdkraft Commercial Series 300HP Outboard Engine for Maximum Work Efficiency
Buy Nordkraft EcoDrive 70HP Outboard Motor with Fuel-Efficient Technoⅼogy
Buy Nordҝгaft EcoDrive 110HP Outboarɗ Engine for Sustainable Marine Performance
Buy Nordkraft ЕcoDrive 150HP Outboɑrd Motor Designed fߋr Low Emissions
Buy Nordkrɑft EcoDrive 190HP Outboard Engine for Effiсient
Long-Dіѕtance Trɑvel
Buy Nordkraft EcoDrive 230НⲢ Outboard Motor Ϲombining Powеr and Economy
Buy Nordkraft Offshore 180HP Outboard Engine Built for Open Sеa Reliability
Buy Nordkraft Offshore 220HP Outboard Motor for Deep
Water Navigation
Buy Nordkrɑft Offshore 260HP Outboard Engine for Extreme Ocean Conditions
Buy Nordkraft Offshoгe 300HP Outboard Motor Designeԁ fоr Long-Range
Trips
Buy Nordkraft Offsһore 350HP Outboɑrd Engine for Professionaⅼ
Marine Operations
Βuy Nordkraft Pеrformance 100HP Оutboard Motor for
Speed and Agіⅼity
Buy Nordkraft Peгformance 150HP Outboard Engine Built
for Accelеration and Control
Buү Nordkraft Performance 200HP Oսtboard Motor for High-Speed Ꭺpplications
Buy Nordkraft Peгformance 250HP Outboaгd Engine Delivering Peak Output
Ᏼuy Nordkraft Performance 300HP Outboard Motor for Competitive Mаrine Use
Buy Nordkrаft Elite 200HP Օutboard Engine for Premium Marine Experience
Ᏼuy Nordkraft Elite 250HP Outboard Motor Combining Luxury and Performance
Buy Nordkraft Elite 300HP Outboard Engine with Advanced Engineering
Fеatures
Buy Norⅾkraft Elite 350HP Outboard Motor for Top-Tier Marine Power
Buy Nordkraft Elite 400HP Outb᧐ɑrd Engine for Unmatched Performance
Buy Nordkraft Compact 40HP Outboard Motor for Smɑll Bօats and
Tenders
Buy Nordkraft Compact 60HP Outboard Engine fοr Lightѡeight Marine Use
Buy Noгdkraft Compact 80HP Outboard Motor for Easy Handling and Efficiency
Buү Nordkraft Compact 100HP Outboаrd Engine for Evеryday Boаtіng Neeԁs
Buy Nordkгaft Compact 120HP Ⲟutboarɗ Μotor for Balanced Power and Size
Somebody necessarily lend a hand to make critically
articles I might state. That is the very first time
I frequented your web page and to this point? I surprised with the research you made
to make this actual post extraordinary. Fantastic activity!
Here is my homepage situs manaplay
Hi, I do believe this is a great web site. I stumbledupon it ;) I may
return yet again since I bookmarked it. Money and
freedom is the greatest way to change, may you be rich and continue to help other people.
Here is my website singapore
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-90-gradusov-15-mm-m0b-gost-r-52948-2008/
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-cacin901—jis-h-2202-2016/truba-vismutovaya-cacin901—jis-h-2202-2016/
Hmm it looks like your website ate my first comment
(it was extremely long) so I guess I’ll just sum it up what I
wrote and say, I’m thoroughly enjoying your blog.
I too am an aspiring blog blogger but I’m still new to everything.
Do you have any recommendations for newbie blog writers? I’d genuinely
appreciate it.
Review my site; 강남룸싸롱
Legal overview: the distinction between Dream11 and traditional betting markets explained for users.
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-900kh100-mm-lts16k4/
I feel that is one of the such a lot important info for me.
And i’m glad reading your article. However want to statement on few general issues, The
web site taste is ideal, the articles is truly nice : D.
Excellent task, cheers
Stop by my web-site – calculate take home pay
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-cac903b—jis-h-5120-2016/list-vismutovyy-cac903b—jis-h-5120-2016/
It’s awesome to pay a quick visit this web site and
reading the views of all colleagues concerning this article,
while I am also eager of getting experience.
Feel free to surf to my web site :: kündigung schreiben
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-54-mm-m3r-gost-r-52948-2008/
Really no matter if someone doesn’t understand afterward its up to other users that they will assist, so here it occurs.
Here is my site … MALWARE
Grand League selection in knockout versus league stage games — different pressure dynamics.
매일 쏟아지는 방대한 정보 중에서 어떤 것을 선택해야 할지 고민이라면 주목해 주세요. 오피사이트는 사용자들에게 가장 반응이 좋은 인기 콘텐츠를 우선적으로 제공합니다. 오피박사와 함께라면 트렌드를 놓치지 않고 항상 가장 앞선 정보를 받아보실 수 있습니다.
I was recommended this blog by means of my cousin.
I am no longer sure whether this post is written by him as no one else recognise such particular about my trouble.
You’re wonderful! Thanks!
Check out my web page :: Professional Property Maintenance
It’s truly very difficult in this active life to listen news on TV, so I only use world wide web
for that purpose, and take the most recent information.
Feel free to surf to my web blog … ketting met naam en foto
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-291-325—astm-b774/prutok-vismutovyy-291-325—astm-b774/
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/prutok-monel/prutok-monel-25-mm-nmzhmts28-2-5-1-5-gost-1525-91/
Why visitors still use to read news papers when in this technological world the whole thing is available on web?
My site; Temiz bayan Aleyna
Hey very nice blog!
my blog buy sell gold Malaysia
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-nitrovan-16—stratcor/folga-vanadievaya-nitrovan-16—stratcor/
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-30-mm-lk80/
出金拒否 チャート分析 バイナリー
I every time emailed this blog post page to all my friends, since if like to read it afterward my links will too.
My web blog; stopbet168
Описание преимуществ компании подчеркивает надежность поставок
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-fev80al14—iso-5451/krug-vanadievyy-fev80al14—iso-5451/
Mangelsen
7916 Girard Avenue, Ꮮɑ Joya
CA 92037, United Ꮪtates
1 800-228-9686
learn wildlife photography bears
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-14kh10kh0-6-mm-10-6kh12-6-mm-tverdaia-paika-cu-dhp-gost-32590-2013/
Legal framework: how Dream11’s fantasy scoring rewards both consistency and match-winning performances.
it is a really nice point of view. I usually meet people who rather say what they suppose others want to hear. Good and well written! I will come back to your site for sure!
Hello! This is kind of off topic but I need some guidance from an established blog.
Is it very hard to set up your own blog? I’m not very techincal but
I can figure things out pretty quick. I’m thinking
about creating my own but I’m not sure where to start.
Do you have any points or suggestions? Cheers
Feel free to visit my homepage – rastrear WhatsApp
Возможность заказа висмута — достаточно редкое предложение на рынке
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt6ch—ost-1-90013-81/prutok-titanovyy-vt6ch—ost-1-90013-81/
If you desire to increase your knowledge simply keep visiting this web site and be
updated with the most recent information posted here.
Check out my page – mahjong ways scatter
I blog quite often and I truly thank you for your content. This great article has
truly peaked my interest. I’m going to book mark your blog
and keep checking for new details about once a week. I subscribed to your RSS feed
as well.
my blog :: web page
Great beat ! I wish to apprentice while you amend your web site, how could i subscribe for a
blog website? The account aided me a acceptable deal. I
had been tiny bit acquainted of this your broadcast offered bright clear concept
Visit my website kencing nanah
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-t10—gost-2171-90/folga-titanovaya-t10—gost-2171-90/
Pretty great post. I just stumbled upon your weblog and
wished to mention that I’ve really enjoyed browsing your weblog posts.
After all I’ll be subscribing on your feed and I’m hoping you write again very soon!
Visit my page … 7m lives
Great web site you’ve got here.. It’s difficult to find high quality writing like yours nowadays.
I honestly appreciate individuals like you! Take care!!
Feel free to visit my blog: Tank Semi Trailers
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-9kh7kh0-6-mm-7-8kh9-8-mm-miagkaia-paika-m2t-gost-r-52922-2008/
โพสต์นี้ อ่านแล้วเพลินและได้สาระ ครับ
ผม ได้อ่านบทความที่เกี่ยวข้องกับ
เรื่องที่เกี่ยวข้อง
ซึ่งอยู่ที่ สล็อตเว็บตรง
ลองแวะไปดู
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ เนื้อหาดีๆ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
My brother recommended I might like this web site. He was
entirely right. This post actually made my day.
You cann’t imagine simply how much time I had spent for this information! Thanks!
Feel free to surf to my blog post … defensible succession readiness
This paragraph presents clear idea in favor of the new viewers of blogging, that truly how to
do blogging.
Feel free to visit my page bouquet birthday flowers
Hi there! This blog post couldn’t be written any better!
Looking through this article reminds me of my previous roommate!
He always kept talking about this. I most certainly will forward this
article to him. Fairly certain he will have a good read.
Thanks for sharing!
Feel free to visit my web site :: board-level succession governance
Описание применения металлов в атомной энергетике подчеркивает качество
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-ot4sv—gost-27265-87-1/krug-titanovyy-ot4sv—gost-27265-87-1/
My brother suggested I would possibly like this blog. He was once totally right.
This post truly made my day. You can not believe simply how a lot time I had spent for this
information! Thanks!
Review my website map of europe
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-1-3×200-mm-lmts58-2-gost-931-90/
Hey I am so happy I found your blog page, I really found you by accident, while I was researching on Digg
for something else, Nonetheless I am here now and
would just like to say kudos for a fantastic post and a all round exciting blog (I also love the theme/design),
I don’t have time to read it all at the moment
but I have book-marked it and also added your RSS
feeds, so when I have time I will be back to read a great deal
more, Please do keep up the superb b.
my web site – ดูซีรี่ย์
I like the valuable information you provide
in your articles. I’ll bookmark your blog and
check again here regularly. I’m quite certain I’ll learn many new stuff right here!
Best of luck for the next!
My homepage – casino online for real money online games
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-at3—gost-19807-91-1/poroshok-titanovyy-at3—gost-19807-91-1/
Hurrah, that’s what I was looking for, what a information! present here
at this website, thanks admin of this website.
Feel free to surf to my site; Blue Steel Locker
Southeast Financial Nashville
131 Belle Forest Cir #210,
Nashville, TN 37221, United Ⴝtates
18669008949
nada cargo van value
Hello, always i used to check webpage posts here in the early hours in the morning, as i love to gain knowledge of more
and more.
Here is my web-site birthday flowers bouquet
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-9kh7kh0-6-mm-7-8kh9-8-mm-miagkaia-paika-m2rm-gost-32590-2013/
We’re a group of volunteers and starting a new scheme in our community.
Your site provided us with valuable information to work on. You have done an impressive job
and our whole community will be grateful to you.
Feel free to surf to my blog; Cannabis Dispensary
We recognize the value of your time, which is why we have incorporated a Turbo Mode
feature into Easy Videos Downloader.
My blog … savefrom
Franchising Path Carlsbad
Carlsbad, ϹA92008, United Ⴝtates
+18587536197
which franchise should i buy
Информация о проверке качества продукции повышает лояльность клиентов
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nbti-46-5/truba-niobievaya-nbti-46-5/
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-10×350-mm-lmts58-2-gost-931-90/
Thank you, I have recently been searching for info about this
subject for ages and yours is the greatest I’ve discovered so far.
However, what in regards to the bottom line? Are you certain concerning
the source?
Check out my site; electric cable
Профессиональный подход к описанию каждого вида металла
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-5v2m-1/izdeliya-iz-niobiya-5v2m/
Hello, I enjoy reading all of your post. I wanted to
write a little comment to support you.
My blog – cheap
It’s very easy to find out any topic on web as compared to books,
as I found this paragraph at this web page.
My web-site Cannabis Store Online
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-80kh54-mm-m3t-gost-r-52948-2008/
You are good writer. Thank you.
It is appropriate time to make some plans for the longer term and it is
time to be happy. I have learn this publish and if I may I desire to
suggest you some attention-grabbing issues or advice.
Perhaps you can write subsequent articles referring to this article.
I desire to learn more things about it!
my homepage: new member
Hey There. I found your blog using msn. This is a very well written article.
I’ll be sure to bookmark it and return to read more of
your useful information. Thanks for the post. I will certainly return.
Have a look at my web site: baby growth calculator
Unquestionably believe that which you stated.
Your favorite reason seemed to be on the
internet the simplest thing to be aware of.
I say to you, I certainly get irked while people consider worries that they just do not know about.
You managed to hit the nail upon the top and
also defined out the whole thing without having side-effects , people could take a signal.
Will probably be back to get more. Thanks
Also visit my homepage … camaras espias
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mshch-1-1/truba-molibdenovaya-mshch-1/
Hi everybody, here every person is sharing such familiarity, so it’s pleasant to read this webpage, and
I used to pay a visit this webpage all the time.
Have a look at my blog – chicken road
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-1-1×40-mm-lmts58-2-gost-931-90/
Hello mates, its impressive paragraph concerning teachingand completely explained, keep it up all the time.
Here is my site Premium Cannabis
Hello, I enjoy reading all of your post. I like to write a little
comment to support you.
Feel free to surf to my homepage :: 분당 가라오케
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mch-zl-1/truba-molibdenovaya-mch-zl/
Hi there mates, fastidious piece of writing and nice urging commented here, I am in fact enjoying by these.
My web blog – dropshipping sellers
Excellent post however I was wanting to know if you
could write a litte more on this topic? I’d be very grateful if you could elaborate
a little bit further. Appreciate it!
Also visit my webpage – 7mlives
I will immediately seize your rss feed as I can’t in finding your email subscription hyperlink or e-newsletter service.
Do you’ve any? Kindly let me recognise in order that I may subscribe.
Thanks.
My web-site; techwear shop deutschland
My spouse and I stumbled over here different web address and thought I should check things out.
I like what I see so now i’m following you.
Look forward to finding out about your web page for a
second time.
Feel free to surf to my web blog Coffee Cup
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-66-7kh15-mm-m1e-gost-r-52948-2008/
I was able to find good info from your blog
posts.
Here is my web-site – tech wear
Valuable information. Lucky me I discovered your site accidentally, and I’m shocked why
this twist of fate didn’t happened earlier! I bookmarked it.
Take a look at my homepage :: Green Tea Powder
Wow, this article is good, my sister is analyzing these kinds of things, so
I am going to inform her.
my blog: techwear kaufen
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-zk60a—ww-t-825b/poroshok-magnievyy-zk60a—ww-t-825b/
Hello, i read your blog from time to time and i own a similar one and
i was just curious if you get a lot of spam feedback?
If so how do you prevent it, any plugin or anything you can advise?
I get so much lately it’s driving me crazy so any help is very
much appreciated.
Here is my web-site … mahjong wins
Hi, I do think this is an excellent web site. I stumbledupon it ;
) I will come back once again since i have bookmarked it.
Money and freedom is the best way to change, may you be rich and continue to guide other people.
my page bouquet birthday flowers
Amazing! This blog looks just like my old one! It’s on a completely different topic but it has pretty much the same page layout and design.
Great choice of colors!
My homepage; Compression Socks
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-1561-6x50x70-gost-13621-90/
Hi there! Do you know if they make any plugins to help
with Search Engine Optimization? I’m trying to get
my blog to rank for some targeted keywords but I’m not seeing very good gains.
If you know of any please share. Kudos!
My web site; board-level succession governance
Tһis is a topic that is near to my heаrt…
Thank you! Where are уoսr cоntact details though?
Feel free to suгf to my website – keep fit
I was able to find good information from your blog posts.
Feel free to visit my homepage; Cannabis Products Canada
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-r-ez33a—aws-a5-19/krug-magnievyy-r-ez33a—aws-a5-19/
Wow, that’s what I was looking for, what a stuff! present here at this weblog, thanks admn of this web page.
Feel free to suurf to my site … mobile chiropractic Services
This article presents clear idea for the new people of blogging, that truly how to do blogging and
site-building.
My homepage; III) Oxide Mn2o4 Nano Cuprous Oxide Spherical Aluminum Oxide Al2O3 Powder Spherical Quartz Powder Nano Iron Oxide Fe2O3 Powder Nano Silicon Dioxide Sio2 Nano Aluminium Oxide Powder Al2o3 Nano Titanium Oxide Nano Zirconium Oxide Nano Ferric Oxide Nano Tungsten Oxide Nano Tin Dioxide Nano Nickel Oxide ITO(Indium Tin Oxide) ATO(Tin Antimony Oxide) Titanium Disilicide Zirconium Disilicide Molybdenum Disilicide Hollow Glass Microspheres Sodium Silicate Potassium Silicate Lithium Silicate
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-40-5-mm-m0b-gost-r-52948-2008/
This design is wicked! You most certainly know how to keep a reader entertained.
Between your wit and your videos, I was almost moved to start my own blog (well,
almost…HaHa!) Great job. I really loved what you had to say, and more than that, how
you presented it. Too cool!
My web site :: Capping Machine
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-zn6zr/list-magnievyy-mg-zn6zr/
Hi mates, good paragraph and pleasant arguments commented here,
I am truly enjoying by these.
Feel free to surf to my web page first deposit
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku35kh1-8mmm3mgost-r-52922-2008/
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-al8zn—iso-121/prutok-magnievyy-mg-al8zn—iso-121/
Heya i am for the first time here. I came across this board and
I find It truly useful & it helped me out much. I hope to give something back and help others like you aided me.
Feel free to visit my site techwear shop deutschland
Fantastic items from you, man. I’ve take into accout your stuff previous to and you are just extremely excellent.
I actually like what you have bought right here, certainly like what you’re saying and the way through which you are saying it.
You’re making it entertaining and you still care for to stay it smart.
I cant wait to learn far more from you. That is really a
wonderful web site.
My webpage: techwear
Hey I am so excited I found your blog, I really
found you by accident, while I was researching on Google for something else, Nonetheless I am here now and would
just like to say cheers for a tremendous post and a all round entertaining
blog (I also love the theme/design), I don’t have time to read it all
at the moment but I have book-marked it and also included your RSS feeds, so when I have time I
will be back to read much more, Please do keep up the excellent job.
Also visit my web site; techwear streetwear
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-19kh3kh9000-mm-mnzhmts10-1-1-gost-10092-2006/
At this time it appears like Expression Engine is the best blogging platform
out there right now. (from what I’ve read) Is that what you are using
on your blog?
Check out my blog post … rave outfits
Hello there, I do believe your web site could possibly be having internet browser compatibility issues.
When I take a look at your site in Safari, it looks fine however, when opening in IE, it’s
got some overlapping issues. I merely wanted to provide you with a quick heads up!
Other than that, fantastic blog!
Also visit my blog post; get redirected here
Patrice & Associates
Scottsdale, AZ, United Ѕtates
16265237726
hospitality internship
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg99-8—iso-144/izdeliya-iz-magniya-mg99-8—iso-144/
Hello! I know this is kinda off topic but I’d figured
I’d ask. Would you be interested in trading links or maybe guest writing a
blog post or vice-versa? My site discusses a lot of the same subjects as yours and I feel we could greatly benefit from each other.
If you might be interested feel free to send me an email.
I look forward to hearing from you! Great blog by the way!
Also visit my blog: Soil Stabilization System
An impressive share! I’ve just forwarded this onto a co-worker who
was doing a little research on this. And he in fact ordered me dinner simply because I discovered it for
him… lol. So allow me to reword this….
Thank YOU for the meal!! But yeah, thanx for spending the time to discuss this matter here on your website.
Stop by my website … techwear shop
It’s remarkable to pay a visit this web page and reading the views of all colleagues regarding this paragraph, while I am also eager of getting know-how.
Also visit my page :: techwear shop
Hi, yes this paragraph is actually pleasant and I have learned lot of things from it about blogging.
thanks.
Here is my web blog: Boiler & High Temperature Fans
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku34kh1mmm2rmgost-r-52922-2008/
You’re so interesting! I don’t think I’ve read through
anything like this before. So great to find another person with a few unique thoughts on this
subject. Really.. many thanks for starting this up. This web site is something that’s needed on the internet,
someone with a little originality!
my page techwear shop deutschland
Hi, i think that i noticed you visited my website thus
i came to return the want?.I am attempting to to
find things to improve my website!I assume its good enough
to use some of your ideas!!
Feel free to surf to my homepage Chemical Packaging Bags
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mc5—jis-h-5203/izdeliya-iz-magniya-mc5—jis-h-5203/
Hi, i read your blog from time to time and i own a similar one and
i was just wondering if you get a lot of spam feedback? If so how do you
stop it, any plugin or anything you can recommend?
I get so much lately it’s driving me mad so any assistance
is very much appreciated.
Look into my blog post tech wear
Thanks in favor of sharing such a good thought, paragraph is fastidious, thats why i have read it fully
Feel free to surf to my web page … techwear shop
I every time used to read article in news papers but now as I am a user of net therefore from now I am using net for content, thanks to web.
Feel free to visit my page … Guardrail Pile Driver
What’s up to every body, it’s my first pay a quick visit of
this web site; this weblog contains amazing and really fine information in support
of readers.
Check out my site … 주소콘
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-kapilliarnaia-trubka/latunnaia-kapilliarnaia-trubka-1-7kh0-7kh100000-mm-l70-gost-2624-2016/
What a information of un-ambiguity and preserveness of precious know-how on the topic of unpredicted emotions.
Here is my blog post – Plastic Extruder
I think the admin of this web page is really working hard in support of his web page, for the reason that
here every material is quality based data.
Here is my page; streetwear style
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-1—bs-2970-1/truba-magnievaya-mag-1—bs-2970-1/
wonderful publish, very informative. I ponder why
the other experts of this sector do not notice this.
You should proceed your writing. I’m sure, you’ve a huge readers’ base already!
Also visit my site – techwear shop deutschland
my web page: GameBeat High RTP Slots You Can Play Now
What’s up to every single one, it’s genuinely a good for me to visit this website, it consists of important Information.
My homepage: สล็อตเว็บตรง
Thank you a bunch for sharing this with all of us you actually realize what you’re talking approximately!
Bookmarked. Kindly also consult with my website =).
We could have a hyperlink change arrangement
among us
Feel free to visit my homepage :: techwear streetwear
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-25kh21kh0-9-mm-16-4kh18-4-mm-tverdaia-paika-m1m-gost-r-52922-2008/
We have been helping Canadians Borrow Money Against Their car title loan online Title Since
March 2009 and are among the very few Completely Online Lenders
in Canada. With us you can obtain a Loan Online from anywhere in Canada as long as
you have a Fully Paid Off Vehicle that is 8 Years old or newer.
We look forward to meeting all your financial needs.
Корзина на сайте промышленного предприятия — удобный инструмент для формирования заявки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m1b—astm-b275/lenta-magnievaya-m1b—astm-b275/
When someone writes an piece of writing he/she maintains the image of a user in his/her brain that how a user
can be aware of it. So that’s why this article is outstdanding.
Thanks!
My webpage; apply for an irish visa online via avats
좋은 정보 감사합니다.
잘 보고 갑니다.
부산토닥이 관련 정보 참고했습니다.
유용한 내용 감사합니다.
예약안내 잘 확인했습니다.
이용후기 잘 보고 갑니다.
Here is my page – cowgirl
Howdy! Do you know if they make any plugins to assist with Search Engine Optimization? I’m trying to get
my blog to rank for some targeted keywords but
I’m not seeing very good results. If you know of any please share.
Thank you!
my homepage … visite here
좋은 정보 감사합니다.
잘 보고 갑니다.
부산토닥이 관련 정보 참고했습니다.
유용한 내용 감사합니다.
예약안내 잘 확인했습니다.
이용후기 잘 보고 갑니다.
My web site; 성인물
Reenergized
4434 Pacific Cozst Hwy,
Ꮮong Beach, ϹA 90804, Unkted Statеs
562-689-9888
Elemental infusion specialist insights
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m5-4-7kh0-6-mm-lts30a3-din-471/
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m15101—uns/krug-magnievyy-m15101—uns/
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-amtss-2x22x28-5-gost-13621-90/
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11900—uns/list-magnievyy-m11900—uns/
We have been helping Canadians Get a Loan borrow money against my car for repair Their Vehicle for Repairs Since March
2009 and are among the very few Completely Online Lenders
In Canada. With us you can obtain a Car Repair Loan Online from
anywhere in Canada as long as you have a Fully Paid Off Vehicle that
is 8 Years old or newer. We look forward to
meeting all your financial needs.
Modern Purair
416 Meridian Ꭱd ᏚE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
hvac safety
Interesting blog! Is your theme custom made or did you download it from somewhere?
A design like yours with a few simple tweeks would really make my blog jump out.
Please let me know where you got your design. Thanks
Take a look at my web site … pola mahjong ways
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-290kh3-mm-lts14k3s3-gost-13943-86/
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m10603—uns/provoloka-magnievaya-m10603—uns/
The Trust Wallet spoof technique is genuinely unique
and hard to detect.
https://propertylifesouthernhighlands.com.au/agent/louveniapad61/
비아그라 구매
전 반드시 확인해야 할 처방 기준, 정품 확인법, 부작용, 복용
전 주의사항을 정리했습니다. 안전한
상담과 약국 조제를 위한 핵심 가이드입니다.
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-vad1-2-5x44x128-gost-13621-90/
Удобное разделение продукции на сплавы и конкретные виды проката
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mg99-95b—iso-8287/poroshok-magnievyy-iso-mg99-95b—iso-8287/
I do accept as true with all of the ideas you have
introduced in your post. They are really convincing and will definitely work.
Nonetheless, the posts are very short for novices.
May you please extend them a bit from subsequent time?
Thank you for the post.
My site … comment-83670
Incredible! This blog looks exactly like my old one! It’s on a
completely different topic but it has pretty much the same
page layout and design. Great choice of colors!
Look at my website; apply visa on arrival india
I want to see your book when it comes out.
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-32kh2kh12000-mm-mnzhmts30-1-1-gost-10092-2006/
Jungle Driving School Omaha
4020 Ѕ 147th St, Omaha,
ΝE 68137, United Ꮪtates
14024170547
web site
เนื้อหานี้ อ่านแล้วเพลินและได้สาระ ค่ะ
ผม ได้อ่านบทความที่เกี่ยวข้องกับ
ข้อมูลเพิ่มเติม
ที่คุณสามารถดูได้ที่ ระบบฝากถอนออโต้
ลองแวะไปดู
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Hello there! I know this is kinda off topic but I was wondering which blog platform are
you using for this site? I’m getting fed up of WordPress
because I’ve had issues with hackers and I’m looking at options for another platform.
I would be awesome if you could point me in the direction of
a good platform.
My blog post: 프리미엄 해킹 PBN 판매 Telegram : @HackPBN
Busy Bee Jumpers
45 Main Ѕt 6C, Wareham,
МА 02571, Unites Ѕtates
508-514-2005
inflatable water fun rentals
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-ad31e-2x40x40-gost-13621-90/
Hmm it looks like your site ate my first comment (it
was super long) so I guess I’ll just sum it up what I had written and say, I’m thoroughly enjoying
your blog. I as well am an aspiring blog writer
but I’m still new to the whole thing. Do you have any tips for rookie blog writers?
I’d definitely appreciate it.
Here is my web page judi bola
Advanced reading here!
Возможность заказать листы и полосы нестандартных размеров
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-ga8a/polosa-magnievaya-ga8a/
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-17kh2-5kh5000-mm-mnzhmts30-1-1-gost-10092-2006/
Using this information, the AI after that makes real-time
recommendations, telling you what locations you
missed.
Take a look at my homepage tao clean sonic toothbrush review; https://hedgedoc.info.uqam.ca,
Moern Purair
416 Meridoan Ꭱd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
audit tool
Currently it looks like Expression Engine is the top
blogging platform available right now. (from what I’ve read)
Is that what you are using on your blog?
my site … 資金繰り 悪化 対策
This piece of writing will help the internet viewers for creating new
webpage or even a blog from start to end.
Have a look at my homepage :: huis huren
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mc21230/izdeliya-iz-magniya-en-mc21230/
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/tavr-aliuminievyi/aliuminievyi-tavr-amg6-50kh25kh25-gost-13622-91/
you are in point of fact a good webmaster. The site loading pace is incredible.
It sort of feels that you are doing any unique trick.
Moreover, The contents are masterpiece. you’ve performed a excellent activity
on this topic!
Stop by my site; 경기 광주출장마사지
Southeast Financial Nashville
131 Beelle Forest Cir #210,
Nashville, TN 37221, United Ѕtates
18669008949
NADA RV accessories value
Very good blog! Do you have any recommendations for aspiring writers?
I’m planning to start my own blog soon but I’m a little lost on everything.
Would you recommend starting with a free platform like WordPress or go for a paid
option? There are so many choices out there that I’m totally confused
.. Any suggestions? Many thanks!
my page: walk-in phone repair Humble
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-b-737-grade-r3—astm-b737/prutok-magnievyy-b-737-grade-r3—astm-b737/
whoah this blog is fantastic i love reading your posts.
Stay up the good work! You understand, many individuals are searching round for this
information, you could help them greatly.
Visit my site … Hitclub
Oh my goodness! Impressive article dude! Thank you,
However I am encountering troubles with your RSS. I don’t
know why I can’t join it. Is there anybody getting similar RSS problems?
Anyone who knows the answer will you kindly
respond? Thanx!!
my homepage :: casino games real money online casino slots
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/lenta-aliuminievaia-1/lenta-aliuminievaia-amg2m-2kh1200-mm-1/
강남텐카페는 편안한 분위기와 합리적인 가격으로 고객님께 최고의 휴식 공간을 제공합니다.
예약도 간편하게 할 수 있어 언제든 편리하게 방문하실 수 있습니다.
예약
Технические характеристики сплавов помогают инженерам в подборе
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az31—csa-hg-4/izdeliya-iz-magniya-az31—csa-hg-4/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-40kh1kh8000-mm-mnzhmts10-1-1-gost-10092-2006/
Hi, I want to subscribe for this website to take most recent updates,
so where can i do it please help.
Feel free to visit my site: ovalpool set
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-as-21/prutok-magnievyy-as-21/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku70kh1-4mmm3rmgost-32590-2013/
Наличие калькулятора металлопроката упрощает расчет веса и стоимости
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-am100b—astm-b275/provoloka-magnievaya-am100b—astm-b275/
Excellent blog here! Also your web site loads up fast!
What web host are you using? Can I get your affiliate link to your
host? I wish my website loaded up as quickly as yours
lol
My site video bokep indonesia
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-11kh3kh1000-mm-mnzhmts10-1-1-gost-10092-2006/
Thanks for another informative website. The place else could I am getting that type of information written in such a perfect manner?
I have a project that I am simply now operating on, and I have been at
the glance out for such information.
Here is my website :: aufstellbecken online bestellen
It’s genuinely very complicated in this busy life to listen news on Television, so I simply use
internet for that purpose, and obtain the hottest information.
Look into my web-site … 한게임머니상
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-9980a—astm-b275/folga-magnievaya-9980a—astm-b275/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku12kh1-1mmm2rgost-r-52922-2008/
Simply want to say your article is as surprising.
The clarity in your post is just nice and i can assume you’re an expert on this subject.
Fine with your permission let me to grab your RSS feed to keep updated
with forthcoming post. Thanks a million and please carry on the gratifying work.
my website casino registration
Somebody necessarily lend a hand to make seriously posts I would state.
That is the first time I frequented your website
page and up to now? I surprised with the analysis you made to make this actual put up amazing.
Magnificent process!
Look into my blog :: Aid for Ukraine kevlar
Today, I went to the beach with my kids. I found
a sea shell and gave it to my 4 year old daughter and said
“You can hear the ocean if you put this to your ear.” She
placed the shell to her ear and screamed. There was a
hermit crab inside and it pinched her ear. She never wants to
go back! LoL I know this is totally off topic but I had to tell someone!
Here is my web blog: carding
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-23—iso-503/lenta-magnievaya-23—iso-503/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/magnievyi-prutok/magnievyi-prutok-75-mm-ma2-gost-18351-73/
I think that what you posted was actually very
reasonable. However, think on this, suppose you composed
a catchier title? I am not saying your information isn’t solid.,
however suppose you added something that makes people want
more? I mean Heel Pain – Plantar Fasciitis – Mr Will Edwards is kinda boring.
You might glance at Yahoo’s home page and see how they create post titles to get viewers
to open the links. You might add a video or
a pic or two to get readers interested about what you’ve got to say.
Just my opinion, it would make your blog a little bit more interesting.
Feel free to surf to my homepage: how to apply visa online in kenya
Hi, just wanted to mention, I loved this post.
It was inspiring. Keep on posting!
my web blog performance engines for sale
We’re a group of volunteers and opening a new scheme
in our community. Your site offered us with valuable information to
work on. You’ve done a formidable job and our entire community will be thankful to you.
Check out my web page :: bolahit
Great post.
Look into my web page: forex gold investing
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-mcr1n3—gost-2581-78/lenta-magnievaya-mcr1n3—gost-2581-78/
Today, I went to the beach front with my kids. I found a sea shell and gave it to my 4 year old
daughter and said “You can hear the ocean if you put this to your ear.” She put the shell to her ear and screamed.
There was a hermit crab inside and it pinched her ear.
She never wants to go back! LoL I know this is completely off topic but I had to tell someone!
Look at my web page London Sales Discounts bundle purchase savings
Track blockchain technology developments and crypto legislative trends in real time.
web site
Monitor crypto transfer restrictions and regional banking policies using our data.
web site
You could definitely see your expertise within the work you write.
The arena hopes for even more passionate writers like you
who aren’t afraid to say how they believe. Always go after
your heart.
My web site: bandar toto
Отраслевой охват впечатляет: от медицины до космической промышленности
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-az-91e—tu-1714-001-00545484-96/polosa-magnievaya-az-91e—tu-1714-001-00545484-96/
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/tkanaia-latunnaia-setka/setka-tkanaia-latunnaia-5×71-l63/
gгeat submіt, very informatіve. I wonder why the ᧐ther experts
of this sector don’t realize this. Yoս must continue your writing.
I’m confident, you’ve a huge readers’ base already!
Feel frеe to surf to my blog … paris
It’s a pity you don’t have a donate button! I’d definitely donate to this excellent blog!
I guess for now i’ll settle for bookmarking and adding your RSS
feed to my Google account. I look forward to brand new updates and will share this blog with my Facebook group.
Talk soon!
Also visit my website – اخبار جهان
Hi i am kavin, its my first time to commenting anywhere, when i read this article i thought
i could also make comment due to this good post.
My homepage :: web design agency
I think this is among the most significant info for me.
And i’m glad reading your article. But should remark on few general things, The site style
is great, the articles is really excellent : D.
Good job, cheers
my web blog :: ILM file technical details
เนื้อหานี้ อ่านแล้วเพลินและได้สาระ ครับ
ดิฉัน ไปอ่านเพิ่มเติมเกี่ยวกับ ข้อมูลเพิ่มเติม
ซึ่งอยู่ที่ Ingrid
น่าจะถูกใจใครหลายคน
เพราะให้ข้อมูลเชิงลึก
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Also visit my website :: บริการ 75rh25,
Ingrid,
I have been exploring for a bit for any high quality articles or blog posts
on this sort of house . Exploring in Yahoo I ultimately stumbled upon this
site. Studying this information So i’m happy to
express that I’ve an incredibly good uncanny feeling I found
out exactly what I needed. I most for sure will make certain to do not overlook this
site and give it a look regularly.
Here is my blog post – siitus toto togel
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-98m2/poroshok-kobaltovyy-stellite-98m2/
Thanks a bunch for sharing this with all people you really recognize what you are talking about! Bookmarked. Kindly also seek advice from my web site =). We can have a link alternate contract between us!
Great post. I was checking constantly this blog and I am impressed!
Extremely helpful info specially the ultimate phase :) I
maintain such information much. I was seeking this certain information for a very lengthy time.
Thanks and good luck.
Here is my blog :: اخبار جهان
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku40kh1-1mmm0bgost-r-52922-2008/
Master cryptocurrency risk analysis with data-driven insights tailored for high-stakes
trading.
web site
This is really interesting, You’re a very skilled blogger. I have joined your feed and look forward to seeking more of your great post. Also, I’ve shared your web site in my social networks!
After looking into a number of the blog posts on your web page, I seriously appreciate your technique of blogging.
I bookmarked it to my bookmark site list and will be checking back in the near
future. Take a look at my web site as well and let me know what you think.
Check out my webpage :: scam
Возможность заказать листы и полосы нестандартных размеров
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-208/prutok-kobaltovyy-stellite-208/
I really like what you guys are up too. This kind of clever work and
reporting! Keep up the excellent works guys I’ve incorporated you guys to my own blogroll.
Also visit my website – izmir escort bayan
This is really fascinating, You are an excessively skilled blogger.
I have joined your rss feed and stay up for in quest of extra of your fantastic
post. Additionally, I have shared your web
site in my social networks
Take a look at my website – kraken2trfqodidvlh4aa337cpzfrhdlfldhve5nf7njhumwr7instad onion
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-kapilliarnaia-trubka/latunnaia-kapilliarnaia-trubka-1-2kh0-85kh100000-mm-l63-gost-2624-2016/
It’s time for communities to rally.
When we look at these issues, we know that they are the key ones for our time.
WOW just what I was looking for. Came here by searching for site
Here is my web blog – thyrafemmebalance
If you are tired of old slot machines, try these fast instant play casino games, they are
perfect for mobile.
my website: https://demo1.xpertixe.com/index.php/agent/carolyncottle1/
Finding a licensed Curaçao casino that hosts the full InOut Games lineup is a
must for crash game fans.
Also visit my web page … https://2dimensions.in/author/jonellenkg5212/
Found so many treasures of aztec slot tips on pgsoft-play.com.
Feel free to visit my web-site – https://app.gitpasha.com/theresamerrett
Great way to play free pg slot games on your smartphone.
Feel free to visit my page – https://jobcop.in/employer/pgsoft-play/
Наличие редких позиций, например, изделий из гафния и ванадия
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-v3k—gost-33258-15/provoloka-kobaltovaya-v3k—gost-33258-15/
Great way to play free pg slot games on your smartphone.
my page :: https://music.crone.es/@simatownson69?page=about
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku14kh0-6mmm2tgost-32590-2013/
This is the ultimate site to play pg soft slots for
free.
Have a look at my blog post; https://banckimoveis.com.br/agent/veroniqueplain/
The transition from free demo to real money play on these crash games is incredibly smooth and easy.
Check out my website: https://semelo.in/author-profile/sheritajkl114/
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-iso-5832-5—gost-r-iso-5832-5-2010/polosa-kobaltovaya-iso-5832-5—gost-r-iso-5832-5-2010/
Greetings! Very helpful advice within this post! It’s the little changes
that produce the most important changes. Many thanks for sharing!
Review my homepage: UK Cyber Essentials
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-170kh3-mm-lts37mts2s2k-gost-13942-86/
Hi there! I could have sworn I’ve been to this blog
before but after reading through some of the post I realized it’s new to me.
Anyhow, I’m definitely happy I found it and I’ll be book-marking and
checking back frequently!
my webpage … cyber Essentials Plus
O plataforma melbet brasil BR, melbet avaliação oficial
tem variantes com apostas sobre múltiplas categorias de jogos.
As apostares têm a oportunidade de investigar alternativas para apostar.
Hey I am so excited I found your blog, I really found you by mistake,
while I was browsing on Bing for something else, Nonetheless I am here now and would
just like to say thanks for a fantastic post and a
all round entertaining blog (I also love the theme/design), I don’t have time to go through it all
at the moment but I have bookmarked it and also added your
RSS feeds, so when I have time I will be back to read more, Please do keep up the superb b.
Also visit my webpage :: Network Wiring Montreal
Hi there, I enjoy reading through your article.
I like to write a little comment to support you.
Here is my homepage :: logo design services
This is really interesting, You’re a very skilled blogger. I have joined your feed and look forward to seeking more of your great post. Also, I’ve shared your web site in my social networks!
Поковки и штабики — важные заготовки для металлургических предприятий
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-ek102-vi/pokovka-kobaltovaya-ek102-vi/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku27-4kh0-9mmm3rtgost-32590-2013/
You are my inspiration , I possess few web logs and very sporadically run out from to brand :(
Do you have a spam issue on this blog; I also am a blogger, and I was
curious about your situation; we have developed
some nice methods and we are looking to trade techniques with other folks, why not shoot me an e-mail if interested.
Here is my homepage 123BET
Keep on working, great job!
Feel free to surf to my site; hearing aid clinic in Bengaluru
My family members every time say that I am killing my time here at net,
however I know I am getting familiarity everyday by reading thes fastidious content.
My webpage – toto macau
O site oficial melbet, online melbet oferece
opções de apostas que atendem as demandas dos jogadores.
Com uma experiência intuitiva, o acesso se torna ágil.
Além disso, a diversidade de esportes garantem que todos
encontrem algo para apostar.
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-bi66-5pb44-5—din-1707-100-2017/provoloka-vismutovaya-bi66-5pb44-5—din-1707-100-2017/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-130kh3-mm-lazhmts-gost-13942-86/
Find reliable market intelligence covering cryptocurrency,
regulations, and high-stakes finance.
homepage
Hey very cool site!! Man .. Beautiful .. Amazing .. I will bookmark your website and take the feeds also…I’m happy to find so many useful information here in the post, we need develop more strategies in this regard, thanks for sharing. . . . . .
I’ve been browsing online more than three hours nowadays, but
I never discovered any fascinating article like yours.
ELV IT projects Dubai Abu Dhabi UAE‘s lovely worth sufficient for me.
In my opinion, if all web owners and bloggers made just right content material as you probably did, the internet shall be much
more useful than ever before.
I was suggested this blog by my cousin. I’m not sure whether this post is written by him as nobody else know such detailed about
my trouble. You are amazing! Thanks!
Also visit my site … Shrooms Direct Canada
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-w-cu30-1/pokovka-volframovaya-w-cu30/
Excellent beat ! I would like to apprentice while you amend your website, how can i subscribe for a
blog web site? The account helped me a acceptable deal.
I had been tiny bit acquainted of this your broadcast offered bright clear concept
My web page … ShroomsDirect
Marvelous, what a weblog it is! This webpage gives helpful data to us, keep it up.
Here is my blog post: NCSC Cyber Essentials
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku12kh1-1mmm3mgost-r-52922-2008/
whoah this weblog is fantastic i love studying your articles.
Stay up the good work! You understand, lots of people are hunting round for this info, you could aid them greatly.
Here is my web-site: vanity address
Лаконичное приветствие на главной странице сразу вводит в курс дела
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vnm-5-3-1/folga-volframovaya-vnm-5-3/
Franchising Path Carlsbad
Carlsbad, CА 92008, United Տtates
+18587536197
should i purchase a franchise
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-78kh2-5-mm-lsd-gost-13942-86/
Hi everyone, it’s my first pay a quick visit at this web site, and paragraph is in fact fruitful for me, keep up posting such
posts.
Feel free to visit my web blog: Shrooms Direct Canada
Возможность заказать листы и полосы нестандартных размеров
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-ovch-1/truba-volframovaya-ovch/
Thanks for finally talking about > Heel Pain – Plantar Fasciitis – Mr
Will Edwards nonton bokep indonesia 2022
Heya i am for the first time here. I found this board and I find
It truly useful & it helped me out a lot. I hope to give something back and help
others like you helped me.
Also visit my web-site Shrooms Direct Magic Mushrooms
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-54kh47kh1-2-mm-11kh13-mm-tverdaia-paika-m1r-gost-r-52922-2008/
Hi there I am so happy I found your web site, I really found you by accident, while
I was looking on Bing for something else, Anyhow I am
here now and would just like to say cheers for a tremendous post and a
all round entertaining blog (I also love the theme/design), I don’t have
time to read through it all at the moment but I have saved it and also added in your RSS feeds, so
when I have time I will be back to read a great deal more, Please do keep up the excellent job.
Also visit my homepage … 123BET
Excellent weblog right here! Also your web site a lot up fast!
What host are you the usage of? Can I am getting your associate hyperlink to your host?
I desire my web site loaded up as quickly as yours lol
Also visit my web blog :: Caterpillar Hydraulic Pump Dealer
Very great post. I simply stumbled upon your weblog and wished to mention that I have truly enjoyed browsing your weblog posts.
After all I’ll be subscribing to your feed and I hope you write once more very soon!
Also visit my homepage … Terex Hydraulic Pump Dealer
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-sn60pb38bi2—iso-9453/krug-vismutovyy-sn60pb38bi2—iso-9453/
What’s up, after reading this remarkable post i am too glad to share my
familiarity here with friends.
Also visit my blog post – Psychedelics In Canada
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m55-50-8kh2-mm-lts38mts2s2-din-471/
I’m truly enjoying the design and layout of your website.
It’s a very easy on the eyes which makes it much more pleasant for me to come here and visit
more often. Did you hire out a developer to create your theme?
Great work!
Here is my page: Kobelco Hydraulic Pump Dealer
Hi! I could have sworn I’ve been to this blog before but after browsing through some of the post I realized it’s new
to me. Nonetheless, I’m definitely glad I found it and
I’ll be book-marking and checking back often!
Stop by my web page :: CASE Hydraulic Pump Dealer
Link exchange is nothing else however it is just placing the other person’s web site link on your page at appropriate place
and other person will also do similar in support of you.
Look into my webpage – Hydraulic Piston Pump Dealer
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-l13937—uns/folga-vismutovaya-l13937—uns/
It’s going to be ending of mine day, but before ending I am reading this wonderful article to improve my knowledge.
my webpage: Liebherr Hydraulic Pump Dealer
FranChoice
7500 Flyng Cloud Drive,
#600 Eden Prairie
MN 55344, United Ꮪtates
952-345-8400
franchise business ownership responsibilities advantages
It’s an amazing paragraph in support of all the internet visitors;
they will take benefit from it I am sure.
My web-site: Moog Valve Dealer
โพสต์นี้ อ่านแล้วได้ความรู้เพิ่ม ค่ะ
ดิฉัน ไปเจอรายละเอียดของ ข้อมูลเพิ่มเติม
สามารถอ่านได้ที่ Thaddeus
เผื่อใครสนใจ
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ เนื้อหาดีๆ นี้
จะรอติดตามเนื้อหาใหม่ๆ ต่อไป
Here is my web-site: เบทฟิก, Thaddeus,
Hi there, I enjoy reading through your article post.
I wanted to write a little comment to support you.
My blog post :: click here
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-35kh29kh1-mm-23kh25-mm-miagkaia-paika-m2-gost-r-52922-2008/
The transition from free demo to real money play on these crash games is incredibly
smooth and easy.
My web site … https://nalagarhproperty.in/author/juanitalieb835/
Perfect portrait mode responsiveness for all pg
soft slots.
Take a look at my homepage – https://test.nicolesinclair.com/employer/pgsoft-play/
Hi there, i read your blog occasionally and i own a similar
one and i was just wondering if you get a lot of spam responses?
If so how do you protect against it, any plugin or
anything you can recommend? I get so much
lately it’s driving me mad so any assistance
is very much appreciated.
Feel free to surf to my site: Argo Hytos Valve Dealer
Wow, awesome blog layout! How long have you been blogging for?
you made blogging look easy. The overall look of your site is excellent,
let alone the content!
My website … Rexroth Hydraulic Valve Dealer
Highly recommend pgsoft-play.com for testing new pg soft slots.
My blog :: https://kurdishserie.com/@darylydt077183?page=about
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-h43bi14a—jis-z-3282/folga-vismutovaya-h43bi14a—jis-z-3282/
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m8-7-4kh0-8-mm-lazhmts-din-471/
Hi there, just became alert to your blog through Google, and
found that it is truly informative. I am going to watch out for brussels.
I’ll appreciate if you continue this in future. A lot of people will be
benefited from your writing. Cheers!
My web-site; Epiroc Hydraulic Pump Dealer
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89842—uns/polosa-vismutovaya-c89842—uns/
여기여는 필요한 웹사이트 주소와 링크 정보를 빠르게 확인할
수 있도록 돕는 주소모음 가이드입니다. 최신 링크, 사이트순위,
이용 팁까지 한눈에 확인하세요.
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-64kh55kh1-4-mm-11kh14-mm-tverdaia-paika-m2m-gost-32590-2013/
I know this if off topic but I’m looking into starting my own weblog and was wondering what all is needed to
get set up? I’m assuming having a blog like yours would cost a pretty penny?
I’m not very web savvy so I’m not 100% certain. Any tips
or advice would be greatly appreciated. Cheers
Stop by my web page; JCB Hydraulic Pump Dealer
Viagra merupakan salah satu terapi yang tersedia untuk mengatasi disfungsi ereksi.
Namun, penggunaannya harus disesuaikan dengan kondisi masing-masing
individu.
Here is my blog post … bokep indonesia
It’s impressive that you are getting ideas from this paragraph
as well as from our discussion made here.
Here is my web site: Wheel Loader Hydraulic Pump Dealer
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89320—uns/krug-vismutovyy-c89320—uns/
Wow, that’s what I was looking for, what a material!
present here at this blog, thanks admin of this web site.
Feel free to visit my web page Website Design Company in Lagos Nigeria
Hello, its good piece of writing concerning media print,
we all be familiar with media is a impressive source of facts.
my web-site; uea8 malaysia
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m8-7-4kh0-8-mm-lk80-din-471/
Hi there friends, its fantastic piece of writing on the topic of cultureand
entirely explained, keep it up all the time.
my blog: Excavator Hydraulic Pump Dealer
It’s the best time to make a few plans for the longer term and it’s time to be happy.
I’ve read this publish and if I may just I wish to recommend
you some interesting things or tips. Maybe you could
write next articles relating to this article. I wish to read more issues about it!
Review my web page; Wirtgen Hydraulic Pump Dealer
Hello I am so grateful I found your webpage, I really found you by accident,
while I was researching on Yahoo for something else, Anyways I am here now and
would just like to say thanks for a incredible post and a all round thrilling blog (I also love the theme/design), I don’t have
time to read through it all at the minute but I have book-marked it
and also included your RSS feeds, so when I have time I will
be back to read more, Please do keep up the excellent job.
Here is my webpage guitar effects pedal
Awesome site you have here but I was curious about if you knew of any message boards that cover the same topics talked about
in this article? I’d really like to be a part of community where I can get suggestions from
other knowledgeable individuals that share the same interest.
If you have any suggestions, please let me know.
Kudos!
Feel free to surf to my web page Doosan Hydraulic Pump Dealer
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-b-774-281-338—astm-b774/list-vismutovyy-b-774-281-338—astm-b774/
Thanks to my father who shared with me on the topic of this blog,
this blog is actually amazing.
Feel free to surf to my blog post Bulldozer Hydraulic Pump Dealer
Yes! Finally something about electric guitar.
my web page beginner electric guitar
Hi, its fastidious post on the topic of media print, we all be familiar with media is a
fantastic source of facts.
Here is my page … sbobet
We’re a group of volunteers and opening a new
scheme in our community. Your web site offered us with
valuable information to work on. You’ve done an impressive job and our whole community will be
grateful to you.
My site :: 123BET
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-40kh35kh1-1-mm-10kh12-mm-tverdaia-paika-cu-dhp-gost-r-52922-2008/
Wonderful, what a webpage it is! This webpage presents helpful data to us, keep it up.
my blog; koi toto
I do not even know how I ended up here, but I thought this post
was great. I do not know who you are but definitely you are going to a famous blogger if you aren’t already ;
) Cheers!
my web blog travel electric guitar
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-291-325—astm-b774/prutok-vismutovyy-291-325—astm-b774/
Attractive portion of content. I simply stumbled upon your weblog Mobilift Terms and Conditions in accession capital to
say that I get actually enjoyed account your blog
posts. Any way I’ll be subscribing on your augment or even I success you get entry
to persistently rapidly.
Wonderful blog! I found it while searching on Yahoo News. Do you have any suggestions on how to
get listed in Yahoo News? I’ve been trying for a while
but I never seem to get there! Thank you
my site :: Contact Mobilift India
Wow, fantastic blog structure! How long have you been blogging for?
you make blogging glance easy. The whole look of
your website is wonderful, as smartly as the content material!
Also visit my blog – silent guitar
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-100kh2-mm-lts40mts3zh-gost-13943-86/
Having read this I thought it was extremely informative.
I appreciate you spending some time and effort to put this informative article together.
I once again find myself spending way too much time
both reading and posting comments. But so what, it was
still worthwhile!
Stop by my site; Caterpillar Hydraulic Pump Dealer
continuously i used to read smaller articles that also clear their motive, and
that is also happening with this piece of writing which
I am reading at this time.
Here is my web page; IT support Abu Dhabi
Лаконичное приветствие на главной странице сразу вводит в курс дела
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-vel-3/poroshok-vanadievyy-vel-3/
This number stands for how much of the example is
composed of the desired peptide series.
Have a look at my blog; Human Performance Research (Walker)
Thanks for another informative blog. The place else may
just I get that kind of info written in such a perfect approach?
I have a project that I am simply now operating on, and I’ve been at the glance out for such info.
Feel free to visit my blog post: 123BET
Spot on with this write-up, I actually assume this website needs far more consideration. I will in all probability be once more to learn rather more, thanks for that info.
It’s remarkable designed for me to have a site, which
is good for my knowledge. thanks admin
Also visit my blog: situs toto togel
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-16kh12kh0-7-mm-10-6kh12-6-mm-tverdaia-paika-m2rm-gost-32590-2013/
It’s a pity you don’t have a donate button! I’d most certainly donate to this excellent blog!
I suppose for now i’ll settle for book-marking and adding your RSS feed to my
Google account. I look forward to fresh updates and will share this blog with my Facebook group.
Chat soon!
Also visit my page สเต็มเซลล์
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vti4/krug-titanovyy-vti4/
Southeast Financial Nashville
131 Belle Forest Cir #210,
Nashville, TN 37221, United Տtates
18669008949
Southeast Fibancial reports; https://gundanvkud.raindrop.page/bookmarks-72718556,
I think that everything typed made a ton of sense.
But, think about this, what if you added a little information? I mean, I don’t wish to tell you how to run your blog,
but suppose you added a title that grabbed folk’s attention? I mean Heel Pain – Plantar Fasciitis – Mr Will Edwards is a little boring.
You might glance at Yahoo’s front page and note how they
create article titles to grab people to click. You might try
adding a video or a related pic or two to grab readers interested about what you’ve got to say.
Just my opinion, it could bring your blog a little bit more interesting.
My site :: Cyber essentials cost
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-270kh3-mm-lk80-gost-13943-86/
There’s certainly a great deal to learn about this topic.
I really like all the points you made.
my web blog – трипскан сайт
Четкая структура меню позволяет быстро найти нужный металл
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt20-1sv—gost-27265-87-2/pokovka-titanovaya-vt20-1sv—gost-27265-87-2/
When someone writes an post he/she keeps the idea of a user in his/her mind that how
a user can know it. So that’s why this piece of writing is great.
Thanks!
my blog post – IASME Cyber Essentials
Very nice article, exactly what I wanted to find.
My blog post: Shrooms Direct
Thank you for the auspicious writeup.
Your style is unique compared to other folks I’ve read stuff from.
Many thanks for posting when you’ve got the opportunity, Guess I’ll just bookmark this blog.
Check out my web page scam
Hello! I know this is kinda off topic but I’d figured I’d ask.
Would you be interested in trading links or maybe guest authoring a blog article or vice-versa?
My site covers a lot of the same subjects as yours
and I feel we could greatly benefit from each other. If you might
be interested feel free to shoot me an e-mail.
I look forward to hearing from you! Excellent blog by the
way!
Feel free to visit my web page :: Shrooms Direct Magic Mushrooms
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-70kh60kh1-4-mm-33-5kh36-5-mm-miagkaia-paika-m3r-gost-r-52922-2008/
It’s amazing to go to see this web page and reading the views of all colleagues about this
paragraph, while I am also keen of getting
knowledge.
Look into my site: cyber essentials requirements
คอนเทนต์นี้ อ่านแล้วเข้าใจง่าย ค่ะ
ดิฉัน เพิ่งเจอข้อมูลเกี่ยวกับ เนื้อหาในแนวเดียวกัน
ซึ่งอยู่ที่ Tanisha
ลองแวะไปดู
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ บทความคุณภาพ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
Also visit my website – saclub888; Tanisha,
Cahinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
homepage
Четкая структура меню позволяет быстро найти нужный металл
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-t1—gost-2171-90/krug-titanovyy-t1—gost-2171-90/
I dont think Ive caught all the angles of this subject the way youve pointed them out. Youre a true star, a rock star man. Youve got so much to say and know so much about the subject that I think you should just teach a class about it
It’s actually very complex in this busy life to listen news on TV,
thus I only use world wide web for that reason, and get the latest news.
Take a look at my blog – Penetration Testing
When are you going to take this to a full book?
Sweet blog! I found it while browsing on Yahoo News. Do you have any tips on how to get listed in Yahoo News? I’ve been trying for a while but I never seem to get there! Thank you
Скачал приложение через Леонбетс зеркало рабочее, теперь играть еще удобнее.
Леон казино
I don’t even know how I ended up here, but I thought this post was good.
I do not know who you are but definitely you are going
to a famous blogger if you are not already ;) Cheers!
Also visit my web-site: Shrooms Direct Online Store
Every weekend i used to go to see this site, because i wish for enjoyment, as this this website conations genuinely fastidious
funny stuff too.
my web blog: guitar tuner pedal
This website was… how do you say it? Relevant!! Finally I have found something that helped me.
Appreciate it!
Here is my web blog :: 123BET
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/krug-latunnyi-1/krug-latunnyi-35-mm-ls59-1pt-1/
Keep on writing, great job!
Feel free to surf to my blog post Psychedelics In Canada
There is a lot of misunderstanding about these issues today. Your material helps explain things.
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-t32—gost-2171-90/poroshok-titanovyy-t32—gost-2171-90/
An outstanding share! I have just forwarded this onto a friend who has been conducting a little research
on this. And he in fact ordered me lunch because I discovered
it for him… lol. So allow me to reword this…. Thank YOU for the
meal!! But yeah, thanx for spending some time to talk about this
topic here on your website.
Have a look at my web-site 欧美动漫
Have you ever considered about adding a little bit more than just your articles?
I mean, what you say is important and all.
However just imagine if you added some great photos
or video clips to give your posts more, “pop”! Your content is excellent but with pics and videos, this site could definitely be one of the most beneficial in its field.
Amazing blog!
my web page – IT Services Montreal
Hey exceptional website! Does running a blog such as this take a large amount of
work? I have absolutely no expertise in computer
programming but I had been hoping to start my own blog in the near future.
Anyways, if you have any suggestions or techniques for new blog
owners please share. I understand this is off subject nevertheless I simply wanted to ask.
Thanks!
Feel free to surf to my web page: เย็ดสบัด.com
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-108kh92kh2-1-mm-47-5kh51-5-mm-tverdaia-paika-m3r-gost-32590-2013/
Рабочее Леонбетс зеркало всегда
выручает, когда провайдер
блокирует основной ресурс.
Актуальное зеркало Леонбетс на сегодня
Четкая структура меню позволяет быстро найти нужный металл
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-14/provoloka-titanovaya-14/
Everything is very open with a precise explanation of the challenges.
It was definitely informative. Your site is very useful.
Thanks for sharing!
Look into my site; electric guitar kit
Рекомендую Leon casino всем, кто устал от долгих проверок документов и хочет просто спокойно крутить любимые автоматы.
Леонбетс
Ahaa, its fastidious dialogue concerning this paragraph here at
this website, I have read all that, so at this time me also commenting at this place.
Feel free to visit my web page; portable guitar
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m23-24-6kh1-mm-lts30a3-din-472/
We recognize the value of your time, which is why we have incorporated a Turbo Mode feature into Easy
Videos Downloader.
Review my web site; 유튜브 다운로드 (https://Www-Savefrom.Com/Ko/)
Good post. I learn something totally new and challenging on blogs I stumbleupon on a
daily basis. It’s always exciting to read through articles
from other writers and use a little something from other sites.
my site :: Живите ярче
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nbzr-10-1/provoloka-niobievaya-nbzr-10/
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-8kh6kh0-6-mm-6-8kh8-8-mm-miagkaia-paika-m1rm-gost-r-52922-2008/
A análise melbet, melbet brasil com recarga mínima acessível ajuda para apostar com
sucesso. As informações fornecem uma percepção profunda das táticas dos jogadores, maximizando as probabilidades de vencer.
Feel free to visit my web page … melbet BR
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m12-13kh1-mm-ls59-1-din-472/
소액결제현금화 및 신용카드현금화와 관련된 정책, 이용
방법, 한도 정보, 안전 이용 가이드 등을 보다 쉽고 빠르게
확인할 수 있도록 다양한 콘텐츠를 제공하고
있습니다.
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-pnmo49-1/folga-molibdenovaya-pnmo49/
Thanks for finally writing about > Heel Pain – Plantar Fasciitis – Mr Will Edwards virus
This is a topic that is near to my heart…
Best wishes! Exactly where are your contact details though?
My blog: bola hit
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-12kh9kh0-6-mm-8-6kh10-6-mm-tverdaia-paika-m3rm-gost-32590-2013/
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mo-cu50-1/prutok-molibdenovyy-mo-cu50/
CD calculator to show how much interest you can earn by the time your CD mature.
Great post. I was checking constantly this blog and I’m impressed! Very useful info specifically the last part :) I care for such info much. I was looking for this certain information for a very long time. Thank you and good luck.
Quality content is the key to interest the viewers to pay a visit the site, that’s what
this web site is providing.
my page – Luv2Qlt Fabric Shop Barwell Leicestershire
Wow that was unusual. I just wrte an extremely long comment but after I clicked submit my comment didn’t show up.
Grrrr… well I’m not writing all that over
again. Regardless, juet wanted to say great blog!
Feel free to surf to my blog … Inheritance tax attorney
Have you given any kind of thought at all with converting your current web-site into French? I know a couple of of translaters here that will would certainly help you do it for no cost if you want to get in touch with me personally.
I think I might disagree with some of your analysis. Are the figures solid?
Some truly interesting info , well written and broadly user genial .
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-zk60—csa-hg-5/pokovka-magnievaya-zk60—csa-hg-5/
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m127-132kh4-mm-lts40mts1-5-din-472/
Hi there! I know this is kinda off topic but I’d figured I’d ask.
Would you be interested in trading links or maybe guest authoring a blog post or vice-versa?
My website addresses a lot of the same topics as yours and
I feel we could greatly benefit from each other. If you might be interested feel free to shoot me an email.
I look forward to hearing from you! Awesome
blog by the way!
Feel free to surf to my website … https://panutantoto.wixsite.com/panutantoto
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-r-az61a—aws-a5-19/list-magnievyy-r-az61a—aws-a5-19/
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-22kh18kh0-9-mm-15-4kh17-6-mm-miagkaia-paika-m1m-gost-32590-2013/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Clientfeedback
It’s actually a nice and useful piece of information. I’m satisfied that you simply shared this helpful info with us.
Please stay us up to date like this. Thanks for sharing.
Feel free to surf to my web blog – 4K Home Theatre
Mijn favoriete spel providers zoals Pragmatic Play en Nolimit City zijn allemaal aanwezig.
https://flyeryachts.nl/
Логичное деление на вольфрамовый, молибденовый и титановый прокат
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mis1—jis-h-2150/lenta-magnievaya-mis1—jis-h-2150/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m30-32-1kh1-2-mm-lts23a6zh3mts2-din-472/
The very best method depends upon the kind, dimension, and place of the development.
Visit my web blog :: Dermatofibroma – Dorine,
melbet site, guia completo sobre cassino ao vivo melbet – O site melbet é uma
das sites mais famosas para esportes online. Com uma experiência amigável, os apostadores podem navegar diversos tipos de apostas.
Pretty nice post. I just stumbled upon your weblog and wanted to say that
I have really enjoyed browsing your blog posts. After all I will be
subscribing to your rss feed and I hope you write again very soon!
Feel free to visit my blog; عرب سكس
Busy Bee Jumpers
45 Mainn St 6C, Wareham,
ΜA 02571, Unites States
508-514-2005
how to start an inflatable rental business
De KSA-licentie van VBET geeft me direct het vertrouwen dat alles eerlijk
en transparant verloopt.
https://gastouderbureaudekoters.nl/
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-al9zn2—iso-121/list-magnievyy-mg-al9zn2—iso-121/
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-64kh55kh1-4-mm-32-5kh34-5-mm-tverdaia-paika-m3rt-gost-r-52922-2008/
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgal3zn1-alloy-21—iso-3116-1/izdeliya-iz-magniya-mgal3zn1-alloy-21—iso-3116-1/
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-900kh500-mm-los/
A site melbet oficial, onde evidenciar cadastro melbet em 2026 é conhecida por suas
múltiplas opções de apostas. Apresenta um layout intuitivo, simplificando a
navegação. Além disso, os clientes podem tirar proveito de bônus exclusivas.
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mc3—jis-h-5203/truba-magnievaya-mc3—jis-h-5203/
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-53-6kh28-mm-m2r-gost-r-52948-2008/
Greetings, I do think your website could be having web browser
compatibility issues. Whenever I look at your web site in Safari, it looks fine however, when opening in I.E., it’s got some overlapping issues.
I merely wanted to provide you with a quick heads up!
Apart from that, excellent website!
Visit my web site: https://zzz-1.com/
I love it when individuals get together and share opinions.
Great website, keep it up!
Also visit my web page :: 중외공원 힐스테이트
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-2—bs-2970/truba-magnievaya-mag-2—bs-2970/
With havin so much content do you ever run into any issues of plagorism or copyright infringement?
My website has a lot of exclusive content I’ve either authored myself or outsourced
but it looks like a lot of it is popping it up all over
the internet without my agreement. Do you know any techniques to
help protect against content from being ripped off?
I’d really appreciate it.
Review my web-site – erection pills
Someone essentially help to make severely articles I might state.
That is the very first time I frequented your web page and so
far? I surprised with the research you made to make this particular put up amazing.
Fantastic activity!
Also visit my blog post אורן פלוטקין
Hi, i read your blog from time to time and i own a similar one and i was
just curious if you get a lot of spam responses? If so how do you reduce it, any
plugin or anything you can suggest? I get so much
lately it’s driving me mad so any help is very much appreciated.
My site: Research Peptides Canada
Pretty! This was an extremely wonderful post.
Thanks for supplying these details.
Feel free to surf to my blog :: situs slot
Hmm is anyone else experiencing problems with the pictures on this blog loading?
I’m trying to find out if its a problem on my end or
if it’s the blog. Any responses would be greatly appreciated.
Look into my website: xnxx
Wow, this article is good, my younger sister is analyzing such
things, so I am going to tell her.
Feel free to visit my web-site :: Health and Performance Supplements
This piece of writing is really a good one it helps new net viewers, who are wishing for blogging.
my web-site BetPari vip
Having read this I believed it was rather informative.
I appreciate you taking the time and energy to put this content together.
I once again find myself personally spending way too much time both reading and commenting.
But so what, it was still worthwhile!
Also visit my blog trc generator
Описание применения металлов в атомной энергетике подчеркивает качество
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m1a—sae-j466/provoloka-magnievaya-m1a—sae-j466/
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-15kh14-7-mm-m3rt-gost-r-52948-2008/
A motіvating discussion is definitelʏ worth ϲomment.
I do believe thаt you ought to publish more on thіs issue, it might not be a taboo subject but generally
people do not talk aƅout these subjects. To the next!
Αll the best!!
Viѕit my bloɡ; girls
Hi to every body, it’s my first visit of this website; this weblog carries awesome
and really good information for visitors.
Also visit my blog – gm diesel conversion
I think this is among the most vital info for me. Buy Steroids and Supplements Online Canada i’m
glad studying your article. However should statement on some normal things, The web site style is
great, the articles is in point of fact nice :
D. Just right task, cheers
Фольга из редких металлов часто требуется для высокотехнологичных лабораторий
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m16400—uns/list-magnievyy-m16400—uns/
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-60kh600-mm-la/
obat aborsi,aborsi,child porn,child porn video,porn child,child porn videos,child porn site,child
porn situs,child seks porn,child porn situs web,child
porn seks,small child porn,mother and child porn,porn child video,
KONTOL,chinese child porn,mom and child porn,child porn sites,porn small
child,child porn video,child gay porn,gay child porn,child
porn link,child porn xxx,child porn hub,child porn free,child
porn vid,how to watch child porn,porn mother and
child,ai child porn,seks child porn,how to find child porn,child and mom porn,watch child
porn,video porn child,porn with child,porn hub child,porn mom and child,
gay porn child,child girl porn
my site – bokep izza vcs
We’re a gaggle of volunteers and starting a new scheme in our community.
Your website offered us with useful info to work on. You have
done an impressive job Health and Performance Supplements our entire community will probably be thankful to you.
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11916—uns/lenta-magnievaya-m11916—uns/
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-27-4kh12-mm-m3rt-gost-r-52948-2008/
Wonderful, what a blog it is! This website
presents helpful data to us, keep it up.
I think this is among the most important information for me.
And i am glad reading your article. But should remark on few general things, The web site style is ideal, the articles is really
excellent : D. Good job, cheers
Feel free to surf to my blog: full-spectrum IT & ELV services Dubai
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11101—uns/krug-magnievyy-m11101—uns/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-170-mm-lts23a6zh3mts2/
If you are going for finest contents like I do, simply pay a visit this website
all the time for the reason that it offers quality contents, thanks
Review my blog post :: ดูการ์ตูน
Good post. I learn something totally new and challenging on sites I stumbleupon every day.
It will always be exciting to read content from other
authors and use something from other websites.
my webpage ELV systems Ras Al Khaimah
Hi colleagues, pleasant article and fastidious arguments commented here, I am
actually enjoying by these.
my blog: kwintessentieel.nl lừa đảo công an cấm người chơi tham gia
Большой опыт работы, судя по копирайту с 2013 года
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mgal2si—iso-16220-1/poroshok-magnievyy-iso-mgal2si—iso-16220-1/
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-42kh22-mm-m1m-gost-r-52948-2008/
I am sure this paragraph has touched all the internet viewers, its really really good article on building up new
weblog.
Take a look at my homepage … niauniapps.in lừa đảo công an cấm người chơi tham gia
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-hz32—csa-hg-9/provoloka-magnievaya-hz32—csa-hg-9/
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-80kh200-mm-lk80/
Cabinet IQ
8305 Տtate Hwy 71#110, Austin,
TX 78735, United Ѕtates
254-275-5536
Renovationexperts
wonderful post, very informative. I ponder why the opposite
experts of this sector don’t notice this. You must proceed your writing.
I’m sure, you have a great readers’ base already!
my website Mobilift Privacy Policy
I think that is among the most vital info for me. And i’m happy reading your article.
But should statement on few normal issues, The site style is perfect, the articles is
truly excellent : D. Just right job, cheers
my blog istanbul escort
It’s great that you are getting thoughts from this article as well as from our discussion made at this time.
my blog post :: เย็ดจิ๋ม
I just like the valuable info you provide to your articles.
I will bookmark your weblog and test again here regularly.
I’m moderately certain I’ll be informed lots of new stuff proper right here!
Good luck for the next!
Here is my homepage … Pizza Hut Deal
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-z4trzr—afnor-nf-a57-704/polosa-magnievaya-g-z4trzr—afnor-nf-a57-704/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-108kh35-mm-m0b-gost-r-52948-2008/
We’re a group of volunteers and opening a new scheme in our community.
Your web site provided us with valuable info to work on. You’ve done a formidable job and
our entire community will be thankful to you.
My site :: 창문시트지
Фольга из редких металлов часто требуется для высокотехнологичных лабораторий
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-a9z1y4—afnor-nf-a57-705/truba-magnievaya-g-a9z1y4—afnor-nf-a57-705/
Its like you read my mind! You appear to know so much about this,
like you wrote the book in it or something. I think that you can do with a few pics to drive the message home a bit, but instead of that, this is
magnificent blog. An excellent read. I will certainly be
back.
my webpage … artis indonesia
Every weekend i used to go to see this web page, because i want enjoyment, as this
this web site conations really fastidious funny data too.
Look at my web-site … Ripper casino pokies
A straightforward guide that gets to the point.
Thank you for sharing it.
Here is my blog :: soundproof hotel rooms
Корзина на сайте промышленного предприятия — удобный инструмент для формирования заявки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mc21320/truba-magnievaya-en-mc21320/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40-5kh21-mm-m3rt-gost-r-52948-2008/
You’re so interesting! I do not think I’ve truly read something
like this before. So nice to discover another person with some unique thoughts on this topic.
Seriously.. many thanks for starting this up.
This web site is something that’s needed on the web, someone with a bit
of originality!
my page – 비아그라 사이트
This excellent website definitely has all of the information and
facts I needed concerning this subject and didn’t know who to ask.
Here is my webpage – Ripper casino pokies
Отраслевой охват впечатляет: от медицины до космической промышленности
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-coralloy-zirconium-702—kind–co–edelstahlwerk-kg/polosa-magnievaya-coralloy-zirconium-702—kind–co–edelstah/
Thanks for finally writing about > Heel Pain – Plantar Fasciitis – Mr
Will Edwards pepekslot memek berdarah
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-1000kh800-mm-lmtsska/
You’ve made some good points there. I looked on the web for more info about the issue and found most
people will go along with your views on this website.
Here is my homepage slot88
At this time I am going to do my breakfast, after having my breakfast coming again to read further news.
My webpage … Tokimec Hydraulic Pump Dealer
I was recommended this blog by my cousin.
I’m not sure whether this post is written by him as no one else know such detailed about my difficulty.
You’re wonderful! Thanks!
Feel free to surf to my website; living and working in Georgia
Описание применения металлов в атомной энергетике подчеркивает качество
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az91d—astm-b275/poroshok-magnievyy-az91d—astm-b275/
First of all I would like to say awesome blog! I had a quick question which I’d like to ask if you
do not mind. I was interested to find out how you center yourself and clear your head prior to writing.
I have had trouble clearing my thoughts in getting my thoughts out.
I do enjoy writing but it just seems like the first 10 to 15 minutes are usually lost simply just
trying to figure out how to begin. Any recommendations or
hints? Thank you!
my web site; Douglas Duren
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-42kh12-mm-m3rm-gost-r-52948-2008/
Greetings from Carolina! I’m bored to death at work so I decided to check out your site on my iphone during lunch break.
I really like the information you present here and can’t wait to
take a look when I get home. I’m amazed at how quick your
blog loaded on my phone .. I’m not even using WIFI, just
3G .. Anyhow, fantastic blog!
Here is my blog; website
Good day! This is kind of off topic but I need some advice from an established blog.
Is it difficult to set up your own blog? I’m not very techincal but
I can figure things out pretty fast. I’m thinking about making my
own but I’m not sure where to begin. Do you have any ideas or suggestions?
With thanks
Review my web blog; The London Prat viral UK satire
Профессиональный подход к описанию каждого вида металла
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az61a—ww-t-825b/pokovka-magnievaya-az61a—ww-t-825b/
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-500kh300-mm-lmtssk/
My spouse and I absolutely love your blog and find a lot of your post’s
to be exactly what I’m looking for. Do you offer guest writers to write
content for you personally? I wouldn’t mind creating a post
or elaborating on a few of the subjects you write concerning here.
Again, awesome website!
Also visit my web-site … horse gelatin recipe
With havin so much written content do you ever run into any issues of plagorism or copyright infringement?
My website has a lot of completely unique content I’ve either authored myself or outsourced but it appears a lot of
it is popping it up all over the internet without my agreement.
Do you know any techniques to help reduce content from being ripped off?
I’d truly appreciate it.
Here is my web page; Hamm Hydraulic Pump Dealer
Great post.
Here is my web page; vanity wallet address generator
Amazing blog! Is your theme custom made or did you download it from somewhere?
A design like yours with a few simple tweeks would really make my blog stand out.
Please let me know where you got your design. Many thanks
Look at my blog post – trc20 usdt address
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-as41a—sae-j465/polosa-magnievaya-as41a—sae-j465/
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-90-gradusov-34-mm-m1rm-gost-r-52948-2008/
홈타이 출장마사지 부터 아로마테라피, 스웨디시,
스포츠 마사지까지 원하는 스타일을 선택할
수 있습니다. 고객님의 취향과 몸 상태에 맞게 코스를 조정해 드립니다.
Cabinet IQ
8305 Statе Hwy 71 #110, Austin,
TX 78735, United Stɑtes
254-275-5536
Kitchenproject
Greetings from Colorado! I’m bored to death at work so I decided to check out your blog on my iphone during lunch break.
I love the information you provide here and can’t wait to take a look when I get home.
I’m surprised at how quick your blog loaded on my mobile
.. I’m not even using WIFI, just 3G .. Anyways, wonderful blog!
my website ngetot kontol hitam
This page truly has all of the information I wanted about this subject and didn’t know who
to ask.
Stop by my blog :: Caterpillar Hydraulic Pump Dealer
секс знакомства для секса без обязательств
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-am-20/prutok-magnievyy-am-20/
I’ve been surfing online more than three hours today, yet I
never found any interesting article like yours. It is pretty worth enough
for me. In my opinion, if all site owners and bloggers
made good content as you did, the internet will be much more useful than ever before.
Here is my website … Hydraulic Motor Repair Services
Hosting websites directly through the Quark Panel simplifies management compared to separate
VPS setups.
https://link.peds.to/zackkeener515
Your way of explaining all in this post is truly good, every
one be able to easily know it, Thanks a lot.
my page – SIRA certified ELV company
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-250kh500-mm-lmtsska/
Good replies Hydraulic Pump Dealer in India return of this difficulty
with firm arguments and explaining all concerning that.
whoah this weblog is wonderful i love studying your articles.
Keep up the good work! You realize, lots of individuals are looking
round for this information, you could help them
greatly.
Feel free to visit my homepage web site
It’s a comprehensive, yet fast read.
Hi there, just became aware of your blog through Google, and found that it’s truly informative. It’s important to cover these trends.
Hi there, constantly i used to check website posts here in the early hours in the daylight, for
the reason that i like to gain knowledge of more and more.
Here is my site :: Aviloo teszt
I believe you have remarked on some very interesting points , thankyou for the post.
Sometimes, the sheer magnitude of the information seems overwhelming.
Продажа проволоки из тугоплавких металлов востребована в электронике
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-702c—astm-b752/pokovka-magnievaya-702c—astm-b752/
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-90-gradusov-80-mm-m3rt-gost-r-52948-2008/
Informative article, exactly what I was looking for.
My webpage :: Tokimec Hydraulic Pump Dealer
Cabinet IQ
8305 Statе Hwy 71 #110, Austin,
TX 78735, United States
254-275-5536
Contracting (https://go.bubbl.us/f2d670/4074?/Bookmarks)
Технические характеристики сплавов помогают инженерам в подборе
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-26—iso-503/krug-magnievyy-26—iso-503/
We can see that we need to develop policies to deal with this trend.
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-60-mm-lts30a3/
Hello to all, how is all, I think every one is getting more from this website, and your views are pleasant in support of new people.
My web blog: Ripper casino
I absolutely love your blog and find almost
all of your post’s to be just what I’m looking for.
Would you offer guest writers to write content for you personally?
I wouldn’t mind producing a post or elaborating on a few of
the subjects you write regarding here. Again, awesome web log!
My website Cat6A
I know this if off topic but I’m looking into starting my own weblog and was wondering what all is needed to
get setup? I’m assuming having a blog like yours would cost a pretty penny?
I’m not very web savvy so I’m not 100% certain. Any suggestions or advice would be greatly appreciated.
Appreciate it
My page; homepage
No matter if some one searches for his essential thing, so he/she needs to be available that in detail, so
that thing is maintained over here.
Feel free to visit my page; bolahit
You made some good points there. I checked on the net for more
information about the issue and found most individuals will go along with your views on this site.
Feel free to surf to my webpage; contact Netcom Dubai
I really love your website.. Excellent colors & theme.
Did you create this website yourself? Please reply back as I’m attempting to create
my own website and want to know where you got this from or exactly what the theme is called.
Kudos!
Have a look at my web-site: biometric access control
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-mg80—gost-804-93/polosa-magnievaya-mg80—gost-804-93/
My issues have been very similar, with my family. But, we made some different decisions. It’s complex.
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/provoloka-mednaia/provoloka-mednaia-1-8mm-m1m/
Как же бесит, когда лесник вообще
не выходит на ганги на другие линии.
Feel free to visit my site – https://vedicglobalbusiness.org/author/ellabickford5/
These are some of the most important issues we’ll face over the next few decades.
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-l-2-1—tu-28-10-33-75/list-magnievyy-l-2-1—tu-28-10-33-75/
Great post. I was checking constantly this blog and I’m impressed! Very useful info specifically the last part :) I care for such info much. I was looking for this certain information for a very long time. Thank you and good luck.
I just added this to my favorites. I truly love reading your posts. Tyvm!
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-240-mm-lts38mts2s2/
The clean wallet connection UI is so minimal that users don’t even pause before approving.
https://trekmarket.ru/author/lornakavel9541/
Всю жизнь играл и не знал, что можно так легально упростить себе жизнь.
My web page https://jobcopae.com/employer/kak-vklyuchit-vh-v-cs/
Admiring the time and effort you put into your site and detailed info you offer!
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-sf6/poroshok-kobaltovyy-stellite-sf6/
Understanding what the information implies overviews your decisions about the checked
item.
my blog post :: Peptide Supplier (Ernestine)
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/neizilberovaia-polosa/neizilberovaia-polosa-15-mm-mnts15-20-gost-5063-73/
It’s genuinely very complicated in this busy life to listen news on TV,
so I just use world wide web for that reason, and take the newest
news.
Here is my blog :: bet football win
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-3/krug-kobaltovyy-stellite-3/
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/prutok-latunnyi-1/prutok-latunnyi-ls59-1pt-45-mm-l-3000-mm-krug-1/
I have read so many posts regarding the blogger lovers except this post is actually a good piece of writing, keep it up.
Visit my site; https://www.chusmeando.com/
I was wondering if you ever considered changing the page layout of your blog?
Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content so
people could connect with it better. Youve got an awful lot of text for only having
one or two pictures. Maybe you could space it out better?
Here is my web blog :: bolahit
Без правильного макро в этой игре делать нечего, учитесь контролировать
лес.
my website; https://stroy-usadba.ru/author-profile/marilouschoenb/
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-yundkt5aa—gost-17809-72/krug-kobaltovyy-yundkt5aa—gost-17809-72/
Hello, I think your blog could be having browser compatibility problems.
Whenever I look at your web site in Safari, it looks fine however when opening in I.E., it has some overlapping
issues. I merely wanted to provide you with a quick heads up!
Apart from that, fantastic blog!
Feel free to surf to my page :: INST file type
Hello! I understand this is sort of off-topic however I needed to ask.
Does managing a well-established blog like yours require a large amount of work?
I am completely new to operating a blog but I do write in my diary on a daily basis.
I’d like to start a blog so I can easily share my own experience and
feelings online. Please let me know if you have any recommendations or tips for new aspiring bloggers.
Appreciate it!
Feel free to surf to my web page :: situs slot viral
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-21kh18kh0-9-mm-8kh10-mm-tverdaia-paika-m3-gost-32590-2013/
After I originally commented I appear to have clicked the
-Notify me when new comments are added- checkbox and now whenever a comment is added I recieve 4 emails with the
exact same comment. There has to be an easy method you are able to remove me from that
service? Cheers!
Also visit my website … drarunkumarsharipad.in/vi-vn/ lừa đảo công an cấm người chơi tham gia
I am really inspired along with your writing abilities and also with the format to your blog.
Is that this a paid theme or did you modify it yourself?
Either way stay up the nice quality writing, it’s rare
to see a nice blog like this one today..
My web page: Nadimtogel
Great goods from you, man. I’ve understand your stuff previous to and
you’re just extremely magnificent. I really
like what you’ve acquired here, really like what you’re stating and the way in which you say it.
You make it enjoyable and you still care for
to keep it wise. I can not wait to read much more from you.
This is really a tremendous website.
Feel free to visit my web-site – site
Thanks for finally writing about > Heel Pain – Plantar Fasciitis –
Mr Will Edwards video bokep indonesia
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-ep949/folga-kobaltovaya-ep949/
hello there and thank you for your information – I’ve certainly picked up anything new from right here.
I did however expertise some technical points using this web
site, since I experienced to reload the web
site many times previous to I could get it to
load properly. I had been wondering if your web hosting is OK?
Not that I’m complaining, but sluggish loading instances
times will very frequently affect your placement in google and could damage your quality score
if ads and marketing with Adwords. Well I’m adding this RSS to my
email and can look out for a lot more of your respective interesting content.
Ensure that you update this again soon.
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-1-4×500-mm-l68-gost-931-90/
Наличие калькулятора металлопроката упрощает расчет веса и стоимости
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-ek20-vi/folga-kobaltovaya-ek20-vi/
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-53-6kh47kh1-2-mm-32kh34-mm-miagkaia-paika-m2rm-gost-r-52922-2008/
โพสต์นี้ มีประโยชน์มาก ครับ
ผม ไปอ่านเพิ่มเติมเกี่ยวกับ หัวข้อที่คล้ายกัน
ที่คุณสามารถดูได้ที่ ทางเข้า bigbet44
สำหรับใครกำลังหาเนื้อหาแบบนี้
มีตัวอย่างประกอบชัดเจน
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Sweet blog! I found it while surfing around on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Many thanks
Stop by my web page … srshopping.in lừa đảo công an cấm người chơi tham gia
Fast wallet-to-wallet crypto exchange with fully transparent 0.5% fees shown upfront.
https://svarnabhumi.com/author/elaine58453136/
Right now it appears like WordPress is the preferred blogging platform out there right now.
(from what I’ve read) Is that what you’re using on your blog?
my website … vanity usdt
Сайт четко ориентирован на промышленный сектор и B2B сегмент
https://redmetsplav.ru/store/cirkoniy-i-ego-splavy/cirkoniy-cirkoloy-2/polosa-cirkonievaya-cirkoloy-2/
Today, I went to the beach with my kids. I found a sea shell and gave
it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.”
She put the shell to her ear and screamed. There was a hermit crab inside and it pinched her ear.
She never wants to go back! LoL I know this is entirely off topic but I had to tell someone!
my web site … real money online gambling usa
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-1-1×300-mm-lmts58-2-gost-931-90/
I am genuinely pleased to glance at this blog posts which consists
of tons of valuable data, thanks for providing these kinds of data.
Feel free to surf to my webpage … Carbon Ceramic Brake Kits
Saved as a favorite, I really like your web site!
My page; online casino nepal9
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-w-cu30-1/prutok-volframovyy-w-cu30/
O jogo do ratinho BR, dinheiro real ratinho disponível no brasil traz diversão maravilhosa para cada faixa etária.
Participando, você avaliar suas habilidades e encontra inovadoras estratégias de jogo.
That is a good tip particularly to those fresh to the blogosphere.
Simple but very accurate information… Many thanks for sharing this
one. A must read post!
my website; спортивный бонус
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-76-1kh64-mm-m2-gost-r-52948-2008/
No matter if some one searches for his necessary thing, so he/she
needs to be available that in detail, so that thing is maintained over here.
Here is my web blog … real money online casino iowa
I have fun with, cause I found exactly what I was looking for.
You’ve ended my 4 day lengthy hunt! God Bless you man. Have a nice day.
Bye
my page – 흥신소
Cabinet IQ
8305 Stɑte Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Countertop
Very good post. I will be facing some of these issues as well..
Feel free to visit my web-site; 비아그라
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vnzh-3-2/truba-volframovaya-vnzh-3-2/
Greetings! Very useful advice within this article! It’s the little changes that make the most
important changes. Thanks for sharing!
my blog post … bakbroodreviews.nl lừa đảo công an cấm người chơi tham gia
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-0-9kh200-mm-lzhmts59-1-1-gost-931-90/
I absolutely love your website.. Very nice colors & theme.
Did you develop this web site yourself? Please reply back as I’m looking to create my own personal website and want to find out where you got this from or exactly
what the theme is called. Thank you!
My blog post – MALWARE
It’s really a great and useful piece of information. I
am happy that you simply shared this useful info with us.
Please stay us up to date like this. Thank you for sharing.
My web blog – mi 2
Возможность заказать листы и полосы нестандартных размеров
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-va-pk-1/krug-volframovyy-va-pk/
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40-5kh40-mm-m3m-gost-r-52948-2008/
You require to have great routines- exercise and eating- in position.
Feel free to surf to my blog :: Treatment Planning – Christel,
Hello there, just became aware of your blog through Google, and found that it’s truly informative.
I am going to watch out for brussels. I’ll appreciate if you
continue this in future. Many people will be benefited
from your writing. Cheers!
Here is my site детейлинг Skoda
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-sn96-9bi1-7cu0-8in0-6—iso-9453/lenta-vismutovaya-sn96-9bi1-7cu0-8in0-6—iso-9453/
Hi! Would you mind if I share your blog with my facebook group?
There’s a lot of people that I think would really appreciate your content.
Please let me know. Many thanks
My website … MALWARE
My spouse and I stumbled over here from a different
website and thought I may as well check things out. I like what I see so now i am following you.
Look forward to going over your web page for a second time.
Feel free to surf to my webpage :: slot winrate tinggi
This is very interesting, You are a very skilled blogger.
I’ve joined your rss feed and look forward to seeking more of your excellent post.
Also, I’ve shared your web site in my social networks!
Look into my blog post echoxen reviews
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-fitingi-pod-paiku/
Cabinet IQ
8305 Statye Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Awardwinningcabinets
Pretty impressive article. I just stumbled upon your site and wanted to say that I have really enjoyed reading your opinions. Any way I’ll be coming back and I hope you post again soon.
My family members all the time say that I am wasting my time here at web, but I know
I am getting knowledge everyday by reading thes nice articles or reviews.
My page: трипскан сайт
Логичное деление на вольфрамовый, молибденовый и титановый прокат
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-l54829—uns/folga-vismutovaya-l54829—uns/
You ought to take part in a contest for one of the highest quality websites online.
I will recommend this blog!
Look at my web-site … wetterlin.org lừa đảo công an cấm người chơi tham gia
A site melbet brasil, melbet app mobile oferece diversas opções de casinos.
Tendo uma interface fácil de usar, os usuários podem navegar rapidamente todas as
alternativas.
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-troiniki-press/mednyi-press-troinik-25-mm-m1-gost-r-52948-2008/
Very good blog! Do you have any suggestions for aspiring writers?
I’m hoping to start my own website soon but I’m a little lost
on everything. Would you suggest starting with a
free platform like WordPress or go for a paid option? There are so many options out there that I’m completely overwhelmed ..
Any recommendations? Bless you!
Here is my site: free ai graphic generator
I’ve been exploring for a little for any high quality articles or weblog posts on this kind of space .
Exploring in Yahoo I finally stumbled upon this website. Studying this
information So i am happy to express that I have a very excellent uncanny feeling I
came upon exactly what I needed. I such a lot definitely
will make sure to don?t overlook this web site and provides it a glance on a relentless basis.
My page :: 비아그라 구매
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-cerrolow-117/pokovka-vismutovaya-cerrolow-117/
บทความนี้ อ่านแล้วได้ความรู้เพิ่ม ค่ะ
ผม ไปเจอรายละเอียดของ เนื้อหาในแนวเดียวกัน
ซึ่งอยู่ที่ Elizabeth
ลองแวะไปดู
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
my blog post :: betflix, Elizabeth,
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/prutok-aliuminievyi-1/prutok-aliuminievyi-amg5-80-mm-l-3000-mm-krug-1/
Описание преимуществ компании подчеркивает надежность поставок
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89940—uns/truba-vismutovaya-c89940—uns/
I believe what you published made a lot of sense.
But, what about this? what if you added a little content?
I mean, I don’t wish to tell you how to run your blog,
but what if you added a post title that grabbed a person’s
attention? I mean Heel Pain – Plantar Fasciitis –
Mr Will Edwards is a little boring. You might look at Yahoo’s home page and watch how they write news titles
to grab viewers to click. You might try adding a
video or a picture or two to grab people excited
about everything’ve got to say. Just my opinion, it might bring your blog a little livelier.
Also visit my site; Portable BBQ Grill
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-25kh2-5kh9000-mm-mnzhmts30-1-1-gost-10092-2006/
Heya i’m for the first time here. I came across this board and I in finding It really useful & it helped me out much.
I am hoping to give one thing back and help others like you helped me.
my page: 프리카지노
I am regular reader, how are you everybody? This piece of
writing posted at this site is actually nice.
Also visit my homepage :: kumpulan bokep indonesia
Лаконичное приветствие на главной странице сразу вводит в курс дела
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89540—uns/folga-vismutovaya-c89540—uns/
whoah this blog is magnificent i like reading your articles.
Keep up the good work! You realize, a lot of people
are looking around for this information, you can help them greatly.
Feel free to visit my web-site :: best paying online casino slots malaysia
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku66-7kh1-4mmm1rmgost-r-52922-2008/
Описание применения металлов в атомной энергетике подчеркивает качество
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-bi08a—eiaipc-j-std-006/truba-vismutovaya-bi08a—eiaipc-j-std-006/
I am actually thankful to the owner of this web page
who has shared this impressive article at at this place.
my blog post: casibom x
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-17kh2kh3000-mm-mnzhmts10-1-1-gost-10092-2006/
I was wondering if you ever considered changing the layout of your site?
Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content so people could connect with it better.
Youve got an awful lot of text for only having one or
two images. Maybe you could space it out better?
My blog; MALWARE
คอนเทนต์นี้ มีประโยชน์มาก ครับ
ผม ไปเจอรายละเอียดของ
เรื่องที่เกี่ยวข้อง
ที่คุณสามารถดูได้ที่ Betflix93 เว็บหลัก
น่าจะถูกใจใครหลายคน
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
จะรอติดตามเนื้อหาใหม่ๆ ต่อไป
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-bi66-5pb44-5—din-1707-100-2017/pokovka-vismutovaya-bi66-5pb44-5—din-1707-100-2017/
It’s in fact very complicated in this full of activity life
to listen news on Television, therefore I just use web for that purpose, and get the most up-to-date information.
Stop by my blog – служба по контракту москва вакансии для мужчин
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-27-4kh23kh0-9-mm-18-4kh20-4-mm-miagkaia-paika-m1e-gost-32590-2013/
Hey there! This is my first comment here so I just wanted to give a quick shout out and tell you I genuinely
enjoy reading through your blog posts. Can you suggest any other blogs/websites/forums that cover the same topics?
Appreciate it!
Look at my homepage; 마곡스웨디시
This is my first time go to see at here and i am genuinely happy to read all
at single place.
Also visit my web blog :: מיכלאמברםשחר
Сайт работает стабильно и быстро загружается
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-vnm99-9—tu-1761-037-2587982-2002/polosa-vanadievaya-vnm99-9—tu-1761-037-2587982-2002/
I know this web page provides quality based posts and extra stuff, is there any other web page which gives these kinds of things in quality?
my blog post … best shopify dropshipping software
Hey there this is kinda of off topic but I was wanting to know if blogs use WYSIWYG editors or if you have
to manually code with HTML. I’m starting a blog soon but have no coding experience so
I wanted to get advice from someone with experience.
Any help would be enormously appreciated!
Take a look at my webpage :: şarjlı süpürgeler
Hello mates, good article and nice arguments commented here, I am
genuinely enjoying by these.
Also visit my website … Down Jackets
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-48kh1-7-mm-lts23a6zh3mts2-gost-13942-86/
Asking questions are really nice thing if you are not understanding something entirely, but this article provides fastidious understanding
yet.
Here is my web page Forging Fabrication
Hello, Neat post. There’s an issue along with your site in web explorer, would check this?
IE nonetheless is the marketplace leader and a good element of other folks will miss
your great writing because of this problem.
Have a look at my web blog: Hotfix Tape
I’m not sure where you’re getting your information, but good topic.
I needs to spend some time learning much more or understanding more.
Thanks for wonderful info I was looking for this information for my mission.
Feel free to surf to my website; Industrial Disc Brakes
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-fev80al14—gost-27130-94/folga-vanadievaya-fev80al14—gost-27130-94/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-d20-7x93x57-gost-13621-90/
Yesterday, while I was at work, my sister stole my iphone and tested to
see if it can survive a 30 foot drop, just so she can be a youtube
sensation. My apple ipad is now broken and she has 83 views.
I know this is completely off topic but I had to share it with someone!
Here is my web site: 감남달토
Технические характеристики сплавов помогают инженерам в подборе
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt22—gost-19807-91/folga-titanovaya-vt22—gost-19807-91/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m55-50-8kh2-mm-lts25s2-din-471/
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-t4—gost-2171-90/provoloka-titanovaya-t4—gost-2171-90/
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-amg3-4x24x9-gost-13621-90/
It’s not my first time to pay a visit this web page, i am visiting this website dailly and obtain nice data
from here every day.
Check out my web page … MALWARE
Fantastic beat ! I would like to apprentice at the same time as you amend
your website, how could i subscribe for a weblog website?
The account helped me a applicable deal. I have been tiny bit familiar of this your broadcast provided shiny transparent concept
Feel free to visit my homepage; 검증카지노
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-erti-11/prutok-titanovyy-erti-11/
Do you have a spam problem on this website; I
also am a blogger, and I was curious about your situation; we have
created some nice methods and we are looking to exchange techniques with other folks, please shoot me an email if interested.
my webpage – evisa
Hello! Do you know if they make any plugins
to protect against hackers? I’m kinda paranoid about losing everything I’ve worked
hard on. Any recommendations?
Feel free to surf to my web blog – 파워맨
I’m impressed, I have to admit. Seldom do I come across a blog that’s both
equally educative and interesting, and let me tell you, you’ve hit the nail on the
head. The problem is an issue that too few people are speaking intelligently about.
I’m very happy I found this during my search for something regarding this.
Take a look at my blog post: 강남유앤미
Hello, for all time i used to check webpage posts here in the early hours
in the break of day, since i enjoy to gain knowledge of more
and more.
Here is my webpage … หวยมารวย
Here is my page – Bookmaker hors arjel fiable
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-88kh2-mm-lts37mts2s2k-gost-13943-86/
You should take part in a contest for one of the greatest websites online.
I will highly recommend this site!
Look at my web-site خرید فالوور اینستاگرام
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-37—ost-1-92077-91/folga-titanovaya-37—ost-1-92077-91/
Informative article, exactly what I needed.
Have a look at my web site: manhwa for free
Hello, its good piece of writing concerning media print, we
all be aware of media is a wonderful source of information.
Feel free to visit my webpage; трипскан официальный сайт
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-d16-3x50x100-gost-13621-90/
Thanks for your marvelous posting! I certainly enjoyed reading it, you might be a great author.
I will be sure to bookmark your blog and will come back later in life.
I want to encourage continue your great job, have a nice day!
Feel free to visit my blog post 강남달토
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-niobiy/list-niobievyy-niobiy/
Howdy! This is kind of off topic but I need some advice from an established blog.
Is it tough to set up your own blog? I’m not very techincal but I can figure things out pretty fast.
I’m thinking about creating my own but I’m not sure where to start.
Do you have any ideas or suggestions? Appreciate it
my blog 홈타이
Hello! I simply wish to give you a big thumbs up for the great info you’ve got right here on this
post. I’ll be coming back to your website for more soon.
Here is my page: Chicago Wedding Transportation
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-17kh3kh10000-mm-mnzhmts30-1-1-gost-10092-2006/
Большой опыт работы, судя по копирайту с 2013 года
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nb1-1/prutok-niobievyy-nb1/
Hello my family member! I want to say that this article is awesome, great written and include approximately all significant infos.
I’d like to look extra posts like this .
Have a look at my web site; poker88
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-avd1-1-4x36x35-gost-13621-90/
Excellent write-up. I absolutely love this website. Continue the good work!
Also visit my blog post; Büroreinigung Innsbruck
Корзина на сайте промышленного предприятия — удобный инструмент для формирования заявки
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-nimo-25-3/lenta-molibdenovaya-nimo-25-1/
It’s really a great and useful piece of information. I’m happy that you shared this helpful information with us.
Please keep us up to date like this. Thanks for sharing.
My web site … Móc lồn em sinh viên
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-17kh0-8kh3000-mm-mnzhmts30-1-1-gost-10092-2006/
You could definitely see your skills within the article you write.
The arena hopes for even more passionate writers like you who aren’t afraid to mention how they believe.
Always go after your heart.
Also visit my homepage Blog about real estate and life in Cyprus
I’m gone to convey my little brother, that he should
also visit this blog on regular basis to get updated from most
recent information.
my web page :: บ้านมังกรฟ้า
My brother recommended I would possibly like this blog.
He used to be totally right. This put up actually made my day.
You cann’t consider simply how much time I had spent for
this info! Thank you!
my site: здесь
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mo-cu30-1/izdeliya-iz-molibdena-mo-cu30/
This piece of writing is in fact a nice one it assists new web visitors,
who are wishing in favor of blogging.
Visit my web blog :: jinx manhwa
Very good information. Lucky me I recently found your site by accident (stumbleupon).
I have saved it for later!
Feel free to surf to my web page – poolleiter komplettset
I’ve been exploring for a little bit for any high quality
articles or weblog posts in this sort of space . Exploring in Yahoo I at last stumbled upon this website.
Studying this information So i’m happy to exhibit that I have a very excellent uncanny feeling I came upon exactly what I
needed. I most unquestionably will make sure to don?t fail
to remember this site and provides it a look on a constant basis.
Look at my blog post :: rundbecken bestellen
Hi there, its fastidious piece of writing regarding media print,
we all be aware of media is a wonderful source of facts.
My web blog … web page
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/prutok-aliuminievyi-1/prutok-aliuminievyi-amg2-70-mm-l-3000-mm-krug-1/
Hi superb website! Does running a blog such as this require a massive amount work?
I’ve absolutely no knowledge of programming however I had been hoping to
start my own blog soon. Anyway, if you have any suggestions
or tips for new blog owners please share.
I understand this is off subject nevertheless I just wanted to ask.
Thank you!
my blog: Mayfair skin revitalization treatment
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-5/krug-molibdenovyy-5/
Very good article! We will be linking to this particularly great content
on our website. Keep up the good writing.
My site – Móc lồn em sinh viên
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-22kh3kh12000-mm-mnzhmts10-1-1-gost-10092-2006/
Następnie wróć do getmyfb.com i wklej link w polu tekstowym na stronie głównej.
Feel free to surf to my blog; telecharger story Instagram Hd
Hello, I wish for to subscribe for this web site to obtain most recent updates,
therefore where can i do it please help out.
Also visit my homepage: bokep indonesia terbaik
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-sismg4635-10—ss-144635/provoloka-magnievaya-sismg4635-10—ss-144635/
Салют всем! Меня зовут Даша, живу в Варшавы.
Достаточно долгое время я
увлекаюсь киберспортом. Но
в последнее время я постоянно сливала катки из-за рандомных тимейтов.
И вот буквально на днях я нашла на
профильном форуме очень подробный обзор про обход современных античитов.
В статье были реальные технические
факты о том, как работают векторные Aimbot-ы с аппаратной эмуляцией мыши на уровне железа.
Автор приводил скриншоты логов, доказывающих, что вероятность детекта
сводится к нулю.
После прочитанного я сразу пошла
на сайт разработчика и приобрела приватку.
Я решила не мелочиться купила мульти-пак подписок сразу на несколько игр.
Я взяла пак под Mortal Kombat 1 и
Tekken 8.
Я сама в шоке, но сказать, что я
довольна — ничего не сказать: буквально за пару
недель я вышла в топ лидерборда. Играть стало в сто раз приятнее,
никакой нервотрепки.
Античит вообще молчит, траст фактор идеальный, потому что софт реально качественный.
Короче, девочки и мальчики, этот
софт — мастхэв!
Here is my webpage … статья про читы
정보 정리 감사합니다. 카드깡을 알아볼 때는 실수령액를 먼저 확인하는 게 중요하다고 생각합니다.
읽어볼 만한 글입니다. 광고 문구만 보기보다 정산 방식과 주의사항을 같이 보는 게 필요합니다.
이 부분은 꼭 확인해야 합니다. 카드깡 관련 정보는 간단한 진행보다 실제 조건이
더 중요합니다.
내용 감사합니다. 신용카드현금화을 검색하는 사람들은
대부분 급한 상황이 많아서, 실수령액를 놓치기 쉬운 것 같습니다.
필요한 내용이네요. 카드현금화 관련해서는 상담 전 조건을
기록해두고 비교하는 게 좋다고 봅니다.
공감되는 내용입니다. 빠른 정산 같은 표현은 편해 보이지만, 실제로는 수수료
차감까지 봐야 합니다.
잘 보고 갑니다. 신용카드 현금화 관련 글은 위험 요소를
같이 설명해주는 쪽이 더 도움이 되는 것 같습니다.
도움 됐습니다. 생활비 부족 때문에 알아보는 경우라도,
상환 가능성은 꼭 따져봐야 합니다.
좋은 포인트입니다. 카드깡은 광고 문구보다 실제 조건이
중요하다고 봅니다.
좋은 내용 감사합니다. 이런 주제는 상황이 바쁠수록 더
차분하게 사후 대응을 확인해야 합니다.
Доброго времени суток, народ!
Я Катя, живу в Киева.
Я уже давно я плотно сижу на онлайн-играх.
Однако недавно я устала потеть без результата.
И вот буквально на днях я прочитала на
одном сайте очень подробный обзор про обход современных античитов.
В статье были реальные технические факты о том, как работают векторные
Aimbot-ы с аппаратной эмуляцией
мыши на уровне железа. В тексте приводилась детальная статистика, доказывающих, что сейчас с софтом играет огромное количество хай-ранг стримеров.
В итоге я решилась на покупку и приобрела приватку.
Так как я играю в разные жанры,
я купила мульти-пак подписок сразу
на несколько игр.
Мой выбор пал на комбо для Valorant и CS:GO.
Я сама в шоке, но сказать, что
я довольна — ничего не сказать: буквально за
считанные дни я апнула ранг своей мечты в
киберспортивных дисциплинах.
Теперь я просто уничтожаю противников.
Античит вообще молчит, траст фактор идеальный,
потому что я играю по легиту, как и учили
в той статье. Короче, девочки и мальчики, этот софт — мастхэв!
Also visit my web site … про читы
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/list-aliuminievyi-gladkii/list-aliuminievyi-6kh1500kh3000-mm-a5n/
Cabiet IQ
8305 Ⴝtate Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Organization
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mp1—jis-h-4201/izdeliya-iz-magniya-mp1—jis-h-4201/
Всем привет! Я Света, живу в
Варшавы.
Уже пару лет я увлекаюсь киберспортом.
И вот случилась проблема – я никак не могла апнуть высокий ранг.
Недавно я нашла на профильном форуме очень крутую статью про игровые модификации и хаки.
Там очень круто расписывалось, как работают приватные скрипты с гибкой настройкой Smooth-наводки,
чтобы даже серверные нейросети ничего не заподозрили.
Там также была куча фактов, доказывающих, что сейчас с софтом играет огромное количество хай-ранг
стримеров.
Я подумала “почему бы и нет” и купила подписку на софт.
Так как я играю в разные жанры, я взяла
читы сразу на 2-3 игры, а не на
какую-то одну.
Оформила доступ к софту для Dota 2 и Apex Legends.
Я сама в шоке, но сказать, что я довольна — ничего
не сказать: буквально за неделю игры я апнула Элиту и максимальные звания.
Теперь я просто уничтожаю противников.
Античит вообще молчит, траст фактор идеальный, потому что разработчики
постоянно обновляют обходы под
патчи. Короче, девочки и мальчики,
этот софт — мастхэв!
My web blog :: статья про читы
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-40kh2kh6000-mm-mnzhmts10-1-1-gost-10092-2006/
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-al9zn2—iso-121/truba-magnievaya-mg-al9zn2—iso-121/
I like what you guys tend to be up too. This sort of clever work and exposure!
Keep up the awesome works guys I’ve added you guys to my personal
blogroll.
Stop by my web blog: cheap
Hello, i think that i saw you visited my website so i came
to “return the favor”.I am attempting to find things to enhance my website!I suppose its ok to
use a few of your ideas!!
Feel free to surf to my web-site; Phim người lớn
Hi there,
First and foremost, I would like to say thank you for sharing
this fantastic guide. I have been scouring the
web for insights along these lines for a long time, and this really helped
me out. How you detailed the topics made it so easy to follow along.
It’s always refreshing to come across a community that provides such
useful insights.
On a slightly different but related note, I wanted to share a subject that could be
useful to other members here. Recently, I’ve been researching advanced artificial intelligence
tools. In particular, I’ve been looking at how far uncensored AI art have progressed.
I stumbled upon a really detailed resource that
perfectly explains the best ways to create high-quality
NSFW images without restrictions. If you want to push
the boundaries of AI tools, this is a must-read. It discusses writing the best prompts to picking the
best AI engines.
Be sure to read more about it at this link: ultimate adult AI generator review.
Once again, thanks for allowing me to share this great discussion. I can’t wait to read more content from you.
Keep up the amazing work!
Nice Post. It’s really a very good article. I noticed all your important points. Thanks.
Następnie wróć do getmyfb.com i wklej link w
polu tekstowym na stronie głównej.
my web blog: id.savefrom.net
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgal3zn1-alloy-25—iso-3116/lenta-magnievaya-mgal3zn1-alloy-25—iso-3116/
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku159kh5-2mmm1mgost-32590-2013/
I visited various web pages but the audio feature for audio songs
existing at this web page is truly superb.
my web blog: allmax allwhey protein
Uitbetaling via crypto was binnen tien minuten geregeld, top service
van Qbet.
https://lisaschrijft.nl/
타임케어 서울출장홈타이 – 서울출장마사지와 서울출장안마 서울홈타이 서비스를 전국 어디서나 24시간 편하게!
전문 마사지사의 맞춤 홈케어로 피로를 빠르게 해소하고 최상의 힐링을 경험하세요.
선입금 없는 후불제 운영으로 더욱 안심!
I got this web site from my friend who informed me concerning
this website and now this time I am browsing this website
and reading very informative content at this place.
Also visit my website – ليموزين مصر
บทความนี้ มีประโยชน์มาก ครับ
ดิฉัน ไปเจอรายละเอียดของ ข้อมูลเพิ่มเติม
ซึ่งอยู่ที่ flik 84
เผื่อใครสนใจ
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ เนื้อหาดีๆ นี้
และหวังว่าจะได้เห็นโพสต์แนวนี้อีก
Корзина на сайте промышленного предприятия — удобный инструмент для формирования заявки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mc5—jis-h-5203/poroshok-magnievyy-mc5—jis-h-5203/
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/medno-nikelevyi-otvod-90-gradusov/medno-nikelevyi-otvod-90-gradusov-mnzh5-1-105kh2-5-mm/
You actually make it seem so easy with your presentation but I find this matter to be actually something which I think
I would never understand. It seems too complicated and extremely broad for me.
I’m looking forward for your next post, I
will try to get the hang of it!
Feel free to surf to my blog post: 7msport – http://www.sex8.zone –
Pretty section of content. I just stumbled upon your blog and in accession capital
to assert that I acquire actually enjoyed account your blog posts.
Any way I’ll be subscribing to your augment and even I achievement you
access consistently quickly.
my web page; solar for businesses Auckland
I’m not sure where you are getting your information, but good topic.
I needs to spend some time learning more or understanding more.
Thanks for magnificent information I was looking for this info for my mission.
Review my homepage; đặt hoa ngày quốc tế phụ nữ 8 3
If some one wishes expert view on the topic of blogging afterward i propose him/her to go to
see this blog, Keep up the fastidious work.
Feel free to visit my web site … slot gacor
I all the time emailed this webpage post page to all my associates,
since if like to read it next my contacts will too.
My web blog; Solar farms
I need to to thank you for this very good read!! I certainly
loved every little bit of it. I’ve got you book-marked to look at new stuff you post…
my web blog :: 엘에이 한국일보
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-4—bs-2970/list-magnievyy-mag-4—bs-2970/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku18kh1-4mmm2tgost-r-52922-2008/
If you are going for best contents like I do, only pay a quick visit this site every day for the reason that it presents quality contents, thanks
Feel free to surf to my page: tripscan вход
Great delivery. Solid arguments. Keep up the amazing effort.
Check out my blog post – 수원출장마사지
Wonderful blog! Do you have any tips and hints for aspiring writers?
I’m planning to start my own site soon but I’m a little lost on everything.
Would you recommend starting with a free platform like WordPress or go for a paid option? There are so many choices out there that I’m totally
overwhelmed .. Any recommendations? Thank you!
my web page; likes kaufen
Hi my family member! I want to say that this post is amazing, nice written and come with almost all important infos.
I’d like to look more posts like this .
Feel free to visit my homepage :: Mas Raja Booking PSK Hyper di Michat – Bokep Terbaru
I like the valuable info you supply to your
articles. I’ll bookmark your blog and check once more here frequently.
I am fairly sure I’ll be informed plenty of new stuff
proper right here! Best of luck for the next!
My webpage :: clickme
Hi, I do think this is a great web site. I stumbledupon it ;
) I will revisit yet again since i have book marked it.
Money and freedom is the greatest way to change, may you be rich
and continue to help other people.
Review my web site; 엘에이 한국일보
Useful information. Fortunate me I discovered your website by accident, and I am surprised why this coincidence
did not happened earlier! I bookmarked it.
my web blog: web site
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-0—bs-2120/pokovka-magnievaya-mag-0—bs-2120/
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/magnievyi-list/list-magnievyi-6-mm-ma15-gost-22635-77/
인천출장마사지 홈타이 마사지부터
아로마테라피, 스웨디시, 스포츠 마사지까지 원하는 스타일을 선택할 수 있습니다.
고객님의 취향과 몸 상태에 맞게 코스를 조정해
드립니다.
Speel jouw favoriete casinospellen waar en wanneer je wilt bij 7 Lucky.
Met een geoptimaliseerde mobiele app, stortingen vanaf
€10 en directe uitbetalingen is dit het ideale platform voor elke speler.
https://compareautoproducten.nl/
Hey! I know this is somewhat off topic but I was
wondering if you knew where I could locate a captcha plugin for
my comment form? I’m using the same blog platform as yours and I’m
having difficulty finding one? Thanks a lot!
my web page – homepage
Использование файлов cookie и политика конфиденциальности соответствуют закону
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m16510—uns/truba-magnievaya-m16510—uns/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku76-1kh2-6mmm0bgost-r-52922-2008/
Excellent article. I will be facing a few of these issues as well..
Look into my page – 오피가이드
Welcome to the exciting realm of bsb007 casino,
bsb007. Here, you can experience a
multitude of games, from classic slots to live dealers.
Take pleasure in exclusive bonuses and promotions that keep the excitement alive.
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11919—uns/lenta-magnievaya-m11919—uns/
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/tkanaia-latunnaia-setka/setka-tkanaia-latunnaia-0-14kh0-28-l80/
Девчонки и парни, привет! Меня зовут Даша, я из
Варшавы.
Я уже давно я играю в шутеры и МОБА на рейтинг.
Однако недавно я уперлась в свой потолок скилла.
И вот буквально на днях я прочитала на одном сайте очень мощный материал про приватный софт.
В статье были реальные технические факты
о том, как работают современные ring0 драйверы, которые остаются полностью невидимыми для Vanguard и EAC.
Автор приводил скриншоты логов, доказывающих, что с таким подходом бан получить просто нереально.
Я подумала “почему бы и нет” и купила подписку на софт.
Чтобы протестить по полной, я взяла читы сразу на 2-3 игры, а не на какую-то одну.
Оформила доступ к софту для Mortal Kombat 1 и Tekken 8.
Я сама в шоке, но сказать, что я довольна — ничего не
сказать: буквально за неделю игры я стала разносить
любые лобби. Мой скилл визуально взлетел
до небес.
Аккаунт при этом в полной безопасности, потому что софт реально качественный.
Теперь играю исключительно в свое удовольствие, советую всем!
Feel free to visit my webpage :: игровые читы
Салют всем! Меня зовут Катя, вещаю из Варшавы.
Уже пару лет я увлекаюсь киберспортом.
И вот случилась проблема – я застряла на одном звании.
Недавно я изучила очень мощный
материал про современные читы.
Там очень круто расписывалось, как работают внешние ESP радары, которые читают пакеты и вообще не вмешиваются в память самой игры.
Там также была куча фактов, доказывающих,
что сейчас с софтом играет огромное количество хай-ранг стримеров.
После прочитанного я сразу пошла на сайт разработчика
и скачала этот специальный софт.
Чтобы протестить по полной, я купила мульти-пак подписок
сразу на несколько игр.
Оформила доступ к софту для Dota 2, CS 2 и Valorant.
Вы не поверите, но буквально за считанные дни
я апнула ранг своей мечты в киберспортивных дисциплинах.
Теперь я просто уничтожаю противников.
Античит вообще молчит, траст фактор идеальный,
потому что я играю по легиту, как и учили в той статье.
Короче, девочки и мальчики, этот софт — мастхэв!
Here is my page … читы для игр
I truly appreciate this post. I have been looking everywhere for this! Thank goodness I found it on Bing. You have made my day! Thank you again
Hi! I could have sworn I’ve been to this website before but after checking through some
of the post I realized it’s new to me. Anyhow, I’m definitely delighted I found it and I’ll be book-marking and checking back frequently!
Here is my web site – web site
An impressive share! I have just forwarded this onto a friend who was conducting a little research on this.
And he in fact ordered me breakfast due to the fact that I found it for
him… lol. So allow me to reword this…. Thanks for the meal!!
But yeah, thanx for spending some time to discuss this topic
here on your site.
Feel free to visit my web blog; togel SGP resmi
I have been exploring for a little for any high-quality articles or weblog posts in this sort of
space . Exploring in Yahoo I at last stumbled upon this website.
Reading this information So i’m glad to exhibit that I have a very
excellent uncanny feeling I found out exactly what I needed.
I most for sure will make sure to do not fail to remember this site and give
it a glance on a constant basis.
my homepage – villa
If some one needs to be updated with most up-to-date technologies after that he must be pay a quick
visit this site and be up to date everyday.
Feel free to visit my blog web site
Cabinet IQ
8305 Stwte Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Bookmarks
Hey, I simply hopped over to your website by way of StumbleUpon. No longer one thing I’d normally learn, but I preferred your thoughts none the less. Thanks for making one thing worth reading.
Салют всем! Меня зовут Лена, я из Киева.
Достаточно долгое время я
плотно сижу на онлайн-играх.
Но в последнее время я постоянно сливала катки из-за
рандомных тимейтов.
И вот буквально на днях я изучила очень крутую статью
про современные читы. В
статье были реальные технические факты о том, как работают приватные скрипты
с гибкой настройкой Smooth-наводки, чтобы даже
серверные нейросети ничего не
заподозрили. Автор приводил скриншоты логов,
доказывающих, что с таким подходом бан
получить просто нереально.
Короче, я решила рискнуть и приобрела приватку.
Чтобы протестить по полной, я купила мульти-пак подписок сразу на
несколько игр.
Я взяла пак под Escape from Tarkov
и Rust.
Это просто шок: буквально за пару недель я апнула ранг своей мечты
в киберспортивных дисциплинах.
Я просто доминирую в каждой катке.
Античит вообще молчит, траст фактор идеальный, потому что настройки очень тонкие.
Короче, девочки и мальчики,
этот софт — мастхэв!
my website: читы для игр
Информация о проверке качества продукции повышает лояльность клиентов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m10601—uns/lenta-magnievaya-m10601—uns/
Девчонки и парни, привет!
Меня зовут Даша, вещаю из Киева.
Достаточно долгое время я трачу свободное время на катки.
Однако недавно я застряла на одном звании.
Недавно я прочитала на одном сайте очень мощный материал про обход современных античитов.
Там очень круто расписывалось, как работают современные
ring0 драйверы, которые остаются полностью невидимыми
для Vanguard и EAC. В тексте приводилась детальная статистика, доказывающих, что
вероятность детекта сводится к нулю.
В итоге я решилась на покупку и
скачала этот специальный софт. Чтобы
протестить по полной, я оплатила бандл
сразу для парочки любимых
проектов.
Мой выбор пал на комбо для Dota 2 и Apex Legends.
Я сама в шоке, но сказать, что я довольна — ничего не сказать:
буквально за пару недель я апнула Элиту и максимальные звания.
Играть стало в сто раз приятнее, никакой нервотрепки.
При этом акки чистые, никаких шедоу-банов, потому что софт реально качественный.
Всем советую попробовать, это реально меняет правила игры!
Here is my blog post; чит коды
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku34kh1mmm1gost-32590-2013/
I have been surfing online more than three hours today, yet I never found anything that grabbed my interest as much as this piece.
Салют всем! Я Вика, я из Минска.
Я уже давно я катаю в соревновательные игры.
И вот случилась проблема – я
никак не могла апнуть высокий ранг.
И вот буквально на днях я нашла на профильном форуме очень мощный материал
про обход современных античитов.
Там очень круто расписывалось, как работают современные ring0 драйверы,
которые остаются полностью невидимыми для Vanguard и EAC.
Там также была куча фактов,
доказывающих, что с таким подходом бан получить просто нереально.
После прочитанного я сразу пошла на сайт разработчика и
приобрела приватку. Я решила не
мелочиться оплатила бандл сразу для парочки любимых проектов.
Оформила доступ к софту для PUBG и Call of Duty:
Warzone.
Это просто шок: буквально за пару недель я стала разносить
любые лобби. Я просто доминирую в каждой
катке.
При этом акки чистые, никаких
шедоу-банов, потому что настройки очень тонкие.
Если кто-то тоже устал сливать – очень рекомендую!
Look at my web page; читы
Dude.. I am not much into reading, but somehow I got to read lots of articles on your blog. Its amazing how interesting it is for me to visit you very often. –
It’s remarkable to visit this website and reading the views
of all colleagues on the topic of this article, while I am also eager of getting knowledge.
Feel free to visit my web page – IPTV premium
Hi there very cool website!! Man .. Excellent ..
Amazing .. I’ll bookmark your blog and take the feeds also?
I am satisfied to seek out so many useful information here in the submit,
we need work out more strategies on this regard,
thanks for sharing. . . . . .
Also visit my site :: Reinigungsfirma Tirol
Hi there, just became aware of your blog through Google,
and found that it’s truly informative. I’m going to watch out for brussels.
I will be grateful if you continue this in future.
Lots of people will be benefited from your writing. Cheers!
my blog website
Modernn Purair
416 Meridian Ꮢd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
commercial purification
Использование файлов cookie и политика конфиденциальности соответствуют закону
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mgal4si—iso-16220-1/list-magnievyy-iso-mgal4si—iso-16220-1/
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-58kh2-mm-lk1-gost-13942-86/
My web-site :: high stakes poker
I was referred to this web site by my cousin. I’m not sure who has written this post, but you’ve really identified my problem. You’re wonderful! Thanks!
I blog frequently and I really appreciate your content. The article has really peaked
my interest. I’m going to bookmark your site and keep checking for new details about once
a week. I subscribed to your Feed too.
my website – Solar farms NZ
Keep on writing, great job!
Review my site; evisa
Наличие калькулятора металлопроката упрощает расчет веса и стоимости
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mb21230—bs-iso-16220/izdeliya-iz-magniya-iso-mb21230—bs-iso-16220/
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku22kh0-9mmm2tgost-r-52922-2008/
These are actually enormous ideas in on the topic of blogging.
You have touched some pleasant points here. Any way keep up wrinting.
My web blog 강남 쩜오
Every weekend i used to go to see this website, as i want enjoyment,
for the reason that this this website conations actually fastidious
funny stuff too.
Look at my web page – 강남 쩜오
Хей, геймеры! Меня зовут Настя, вещаю из Киева.
Достаточно долгое время я играю
в шутеры и МОБА на рейтинг. Но в последнее время я устала потеть без
результата.
И вот буквально на днях я прочитала на одном сайте очень подробный обзор про игровые модификации и хаки.
Меня поразил подробный разбор того, как работают современные ring0 драйверы, которые остаются полностью невидимыми для Vanguard
и EAC. Автор приводил скриншоты логов,
доказывающих, что с таким подходом бан получить просто нереально.
Я подумала “почему бы и нет” и купила подписку на софт.
Чтобы протестить по полной, я купила мульти-пак подписок сразу на несколько игр.
Оформила доступ к софту для PUBG и Call of Duty: Warzone.
Результат просто бомба – буквально за неделю
игры я вышла в топ лидерборда.
Играть стало в сто раз приятнее, никакой нервотрепки.
Аккаунт при этом в полной безопасности, потому что настройки очень тонкие.
Если кто-то тоже устал
сливать – очень рекомендую!
my web-site игровые читы
I got this web page from my pal who shared with me concerning this web site and now this time I am visiting
this web site and reading very informative articles or reviews here.
my webpage … 강남 쩜오
I’ve been browsing on-line more than 3 hours as of late, yet
I never discovered any interesting article like yours. It’s pretty value sufficient for me.
In my view, if all website owners and bloggers made just
right content material as you probably did, the internet will likely be much more helpful than ever before.
my webpage 오피스타
Hi there i am kavin, its my first time to commenting anywhere, when i read this paragraph
i thought i could also create comment due to this brilliant
piece of writing.
my page 3125tiger Yupoo Lowest
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-z5zr/izdeliya-iz-magniya-g-z5zr/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-115kh3-mm-lmtska-gost-13942-86/
Can you tell us more about this? I’d love to find out some additional
information.
Here is my web-site: 강남 쩜오
Hi there, I enjoy reading all of your post. I wanted to write a
little comment to support you.
Also visit my website; MALWARE
I do not know whether it’s just me or if perhaps
everybody else experiencing issues with your site.
It seems like some of the written text within your posts are running off
the screen. Can someone else please provide feedback and let
me know if this is happening to them too? This could
be a problem with my web browser because I’ve had this happen previously.
Cheers
Feel free to visit my webpage; website
I’m not sure why but this website is loading incredibly slow for me.
Is anyone else having this problem or is it a issue on my end?
I’ll check back later on and see if the problem still exists.
Feel free to visit my site evisa
I feel that is among the such a lot important info
for me. And i’m glad reading your article.
However should statement on some general issues,
The web site taste is great, the articles
is really excellent : D. Good activity, cheers
Also visit my website – homepage
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-gd-mgal6—din-1729-part-2/pokovka-magnievaya-gd-mgal6—din-1729-part-2/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku133kh4-2mmm1rgost-32590-2013/
I am curious to find out what blog platform you happen to be utilizing?
I’m experiencing some small security problems with my latest site and I’d like to
find something more safeguarded. Do you have any solutions?
Also visit my blog: 강남 쩜오
Cabinet IQ
8305 Statе Hwy 71 #110, Austin,
TX 78735, United States
254-275-5536
Specialoffer
Spot on with this write-up, I absolutely think this
site needs far more attention. I’ll probably be back again to read
more, thanks for the info!
Feel free to visit my homepage: rosetoy.net
Find whitefield call girls listings that simplify profile discovery within one
of Bangalore’s busiest areas.
I was wondering if you ever considered changing the page layout
of your blog? Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content so people could connect with it better.
Youve got an awful lot of text for only having 1 or 2 images.
Maybe you could space it out better?
Also visit my page; 강남 쩜오
Hi there, I check your new stuff on a regular basis. Your humoristic style is awesome, keep doing what you’re doing!
Feel free to surf to my page: 강남 쩜오
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mc21320—en-1753/pokovka-magnievaya-en-mc21320—en-1753/
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/krug-latunnyi-1/krug-latunnyi-90-mm-ls59-1-1/
I was suggested this website by my cousin. I am not sure whether this post is written by him as nobody
else know such detailed about my trouble. You’re incredible!
Thanks!
Feel free to surf to my homepage :: Да будет радость
Can I just say what a relief to uncover someone that really knows what they
are discussing on the net. You actually understand how to bring a problem to light and make it important.
More people have to read this and understand this side
of the story. I was surprised that you aren’t more popular given that you most certainly
have the gift.
Here is my homepage – 강남 쩜오
This is the perfect website for anybody who would like to understand
this topic. You understand so much its almost tough to argue with
you (not that I personally will need to…HaHa).
You definitely put a fresh spin on a subject which has been written about for years.
Excellent stuff, just excellent!
Here is my blog :: 강남 쩜오
Thanks very interesting blog!
Look into my web site: 강남 쩜오
신용카드현금화의 의미, 카드깡과의 차이, 주의해야 할 광고
문구, 수수료 위험, 피해 예방 체크리스트,
합법적 대안까지 안전하게 확인하세요.
Раздел «Контакты» содержит все необходимые реквизиты и карту
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-cm-1-1/polosa-molibdenovaya-cm-1/
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-16kh12kh0-7-mm-10-6kh12-6-mm-tverdaia-paika-m1e-gost-r-52922-2008/
It’s hard to come by well-informed people in this particular subject, but you seem like you know what you’re
talking about! Thanks
Also visit my web page fast file conversion
I simply couldn’t leave your web site prior to suggesting
that I really loved the usual information a person supply
on your guests? Is going to be back often in order to investigate cross-check new posts
Check out my page :: nuddies
Thanks for sharing your thoughts about 강남 쩜오.
Regards
Do you have a spam issue on this website; I also am
a blogger, and I was wanting to know your situation; we
have created some nice methods and we are looking to swap solutions with other folks, be sure to
shoot me an e-mail if interested.
my website :: Betvibe Casino
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az91hp/folga-magnievaya-az91hp/
Good post! We will be linking to this particularly great post
on our site. Keep up the good writing.
Also visit my website 강남 쩜오
Hello there! I could have sworn I’ve visited this site before but after going through some of the posts I
realized it’s new to me. Anyhow, I’m certainly pleased
I found it and I’ll be bookmarking it and checking back regularly!
My web site: dental implants beirut
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m67-62-6kh2-5-mm-lk2-din-471/
You really make it seem really easy along with your presentation but I find this topic
to be really one thing which I believe I’d never understand.
It sort of feels too complex and very wide for me.
I’m taking a look ahead to your subsequent publish, I’ll attempt to get the grasp of it!
my webpage – ac repair
Right here is the perfect web site for anyone who
hopes to understand this topic. You realize a whole lot its almost hard to argue with you
(not that I actually will need to…HaHa).
You certainly put a new spin on a subject which has been discussed for a long time.
Great stuff, just great!
Feel free to surf to my web site: webpage
I just could not go away your web site before suggesting that
I really enjoyed the standard info an individual provide on your guests?
Is gonna be again incessantly to inspect new posts
Stop by my web blog … cardio.nashi-veshi.ru
I’m really impressed with your writing skills as well as with the layout on your blog.
Is this a paid theme or did you modify it yourself? Anyway keep up the nice quality writing, it’s rare to see
a nice blog like this one these days.
Also visit my web blog :: 강남사라있네가라오케
Информация об обработке IP-адреса для определения региона — современный подход
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az61—csa-hg-5/list-magnievyy-az61—csa-hg-5/
Magnificent beat ! I would like to apprentice while you amend your
web site, how could i subscribe for a weblog site?
The account aided me a applicable deal. I have been tiny bit familiar
of this your broadcast offered brilliant transparent idea
Have a look at my web page: Fensterreinigung
bsb007 casino, bsb007 – If you’re looking for a
thrilling experience, bsb007 gaming site is the perfect destination. Here, you can explore a variety of games that will keep you entertained for
hours.
my web site: https://bsb-007-aus.com/
I’ll right away clutch your rss feed as I can’t find your e-mail subscription link or e-newsletter service.
Do you’ve any? Please allow me recognize in order that I may just
subscribe. Thanks.
My web blog – akses cepat
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-54kh47kh1-2-mm-32kh34-mm-miagkaia-paika-m2-gost-32590-2013/
Peculiar article, exactly what I wanted to find.
Here is my blog post webpage
The sketch is tasteful, your authored material stylish.
Great resources and tips for families here.
I’d like to thank you for the efforts you’ve put in penning this
site. I really hope to check out the same high-grade content
by you in the future as well. In fact, your creative writing abilities has
inspired me to get my own, personal website now ;)
Also visit my homepage; 비아그라 구매 사이트
Столкнулись с трудностями в
сфере семейного, жилищного или уголовного права и срочно нуждаетесь в помощи компетентного специалиста?
Наш сервис объединяет лучших адвокатов, юристов и нотариусов,
предоставляя доступ к квалифицированным платным и
бесплатным консультациям по всей России.
Выбирайте надежных экспертов
для оформления сделок, подготовки документов и уверенной защиты ваших интересов в любых инстанциях!
https://bebejoy.es/author/cherylelowes98/
I just couldn’t leave your site prior to suggesting that I really loved the usual info an individual provide to your guests?
Is going to be back regularly to inspect new posts
Feel free to visit my homepage: casino online paypal argentina
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-as41a—astm-b275/poroshok-magnievyy-as41a—astm-b275/
I am really enjoying the theme/design of your website.
Do you ever run into any browser compatibility problems?
A handful of my blog readers have complained
about my site not operating correctly in Explorer but looks great in Opera.
Do you have any advice to help fix this issue?
Stop by my web blog :: web page
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m82-76-5kh2-5-mm-lts40mts3a-din-471/
Great work! That is the kind of information that are meant to be shared around the net.
Shame on the search engines for now not positioning this publish upper!
Come on over and talk over with my website .
Thank you =)
Review my page :: Забронировать люксовую яхту в Анапе со шкипером
That is a very good tip particularly to those new to the blogosphere.
Simple but very precise info… Thank you for sharing this one.
A must read post!
Also visit my website; DAA file
Good info. Lucky me I ran across your website by accident (stumbleupon).
I’ve saved it for later!
Here is my homepage Vendedor de IA no WhatsApp
От оформления нотариальной доверенности до сложных судебных разбирательств по гражданским
и уголовным делам — мы поможем найти идеального правозащитника для вашей ситуации.
В нашей базе собрана актуальная информация
о специалистах из разных регионов РФ,
предлагающих как очные встречи, так и удобные онлайн-консультации.
Доверьте свои правовые заботы профессионалам, чтобы избежать ошибок
в документах и гарантированно отстоять свои
законные права.
https://exit.si/hildegardrymil
Большой опыт работы, судя по копирайту с 2013 года
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-am60a—astm-b275/izdeliya-iz-magniya-am60a—astm-b275/
I was able to find good advice from your articles.
Feel free to surf to my web site … vidio bokep indonesia
I will right away take hold of your rss feed as
I can not find your email subscription link or newsletter service.
Do you have any? Kindly let me know so that I may
subscribe. Thanks.
Feel free to surf to my blog … casino online
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-16kh12kh0-7-mm-10-6kh12-6-mm-tverdaia-paika-m2r-gost-32590-2013/
Pretty section of content. I just stumbled upon your
website and in accession capital to assert that I get
in fact enjoyed account your blog posts. Anyway I’ll be
subscribing to your augment and even I achievement you access consistently fast.
Look at my homepage … 검증카지노
Good post. I learn something new and challenging on websites I stumbleupon on a daily basis.
It’s always useful to read articles from other writers and practice something from other sites.
Visit my web page; hvac repair
Hi there! I could have sworn I’ve been to this blog before but after checking through some of the post
I realized it’s new to me. Anyways, I’m definitely delighted
I found it and I’ll be book-marking and checking back frequently!
My web blog: webpage
A fascinating discussion is worth comment. I do believe that you should publish more on this subject
matter, it may not be a taboo subject but usually folks don’t discuss
such issues. To the next! Kind regards!!
Also visit my web-site; slot777
Nice blog. Could someone with little experience do it, and add updates without messing it up? Good information on here, very informative.
Возможность заказа висмута — достаточно редкое предложение на рынке
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-9980b—astm-b275/prutok-magnievyy-9980b—astm-b275/
Hello there! I could have sworn I’ve been to your blog before but after going through a few of the articles I realized it’s new to me.
Nonetheless, I’m certainly delighted I discovered it and I’ll be bookmarking it and
checking back frequently!
my blog … casino online terbaik
Редметсплав — надежный партнер, работаем по поставкам нержавеющего проката уже второй год, сбоев не было.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m120-113kh4-mm-lts14k3s3-din-471/
What a stuff of un-ambiguity and preserveness of precious know-how regarding
unexpected feelings.
Feel free to surf to my web site :: Organic Visits – bonusbacklinks.com –
Thank you for any other informative blog. Where else may I am
getting that type of info written in such
a perfect approach? I’ve a undertaking that I am just now running on, and I have been on the glance out for such information.
my blog post: Word to PDF
I know this website presents quality dependent content and additional
stuff, is there any other web page which provides these kinds
of information in quality?
Here is my web site: webpage
Информация о проверке качества продукции повышает лояльность клиентов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-26—iso-503/provoloka-magnievaya-26—iso-503/
Do you mind if I quote a few of your articles as long as I provide credit and sources back
to your weblog? My blog site is in the exact
same area of interest as yours and my users would genuinely benefit from some of the information you present
here. Please let me know if this ok with you. Thanks!
Check out my web blog Betvibe Casino login
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-27-4kh23kh0-9-mm-18-4kh20-4-mm-miagkaia-paika-m2r-gost-r-52922-2008/
Информация о проверке качества продукции повышает лояльность клиентов
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ml11—gost-2856-79/prutok-magnievyy-ml11—gost-2856-79/
Hi my family member! I wish to say that this article
is amazing, great written and include almost all vital infos.
I would like to look more posts like this .
My web site :: 강남가라오케
This site was… how do I say it? Relevant!!
Finally I’ve found something which helped me. Thanks a
lot!
Here is my website sunwin
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m22-20-5kh1-2-mm-lts40mts1-5-din-471/
If you are going for finest contents like me, simply pay
a quick visit this web site every day because it presents
feature contents, thanks
Stop by my site; evisa
Następnie wróć do getmyfb.com i wklej
link w polu tekstowym na stronie głównej.
Also visit my website: Savefrom
Технические характеристики сплавов помогают инженерам в подборе
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-l3—tu-1714-002-00545484-99/poroshok-magnievyy-l3—tu-1714-002-00545484-99/
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-106kh92kh2-1-mm-15kh19-mm-tverdaia-paika-m2rm-gost-32590-2013/
Asking questions are in fact fastidious thing if you are not understanding anything completely, but this piece of writing gives fastidious understanding yet.
Also visit my blog post; situs slot terpercaya
Cabinet IQ
8305 Տtate Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Personalizedplans (Stacy)
Hey there! I know this is sort of off-topic but I needed to ask.
Does running a well-established blog such as yours take a massive amount work?
I’m brand new to writing a blog however I do write in my
diary daily. I’d like to start a blog so I will be able to share my own experience and views online.
Please let me know if you have any kind of recommendations or tips for new aspiring blog owners.
Thankyou!
My blog post – 13500 v bucks gratuit
Наличие калькулятора металлопроката упрощает расчет веса и стоимости
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-star-j/list-kobaltovyy-stellite-star-j/
Hey! Would you mind if I share your blog with
my facebook group? There’s a lot of folks that I think would really
enjoy your content. Please let me know. Many thanks
my web page … 대구출장마사지
Cabinet IQ
8305 Stаte Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Remoteconsultation
My web-site – Bookmaker hors arjel fiable
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-62kh1-7-mm-lsdch-gost-13943-86/
What i do not understood is in fact how you are now
not really a lot more neatly-preferred than you may be right now.
You’re very intelligent. You know therefore significantly on the subject
of this subject, produced me in my opinion believe it from
numerous numerous angles. Its like men and women aren’t involved
unless it’s something to do with Girl gaga! Your individual stuffs outstanding.
All the time maintain it up!
my webpage … game slot variatif
pnc.com
What a great article.. i subscribed btw!
Hello, Neat post. There’s an issue along with your web site in web explorer, would test this?
IE nonetheless is the marketplace chief and a good component to other
people will miss your magnificent writing due
to this problem.
Also visit my web-site revenue based financing doral fl
Информация о доставке по всей РФ делает компанию универсальным поставщиком
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-314-2/poroshok-kobaltovyy-stellite-314-2/
Great resources and tips for families here.
I’m truly enjoying the design and layout of your website.
It’s a very easy on the eyes which makes it much
more enjoyable for me to come here and visit more
often. Did you hire out a designer to create your theme? Exceptional work!
Also visit my page: web page
Quality posts is the important to interest the people to pay a visit the website, that’s what this
website is providing.
Here is my website kubet
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-21kh18kh0-9-mm-15-4kh17-6-mm-tverdaia-paika-m1r-gost-32590-2013/
I enjoyed reading this article. A well-designed customer survey benefits both the
company and the customer by creating a better experience over time.
Feel free to surf to my blog – http://www.cvshealthsurvey.com
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-yundkt5ba—gost-17809-72/provoloka-kobaltovaya-yundkt5ba—gost-17809-72/
Hello there, You’ve done an excellent job. I will definitely digg it and
personally recommend to my friends. I’m sure they will be benefited from this web site.
Feel free to visit my web blog – Buy Marijuana Online Canada
I am extremely impressed with your writing skills as well as with the
layout on your weblog. Is this a paid theme or did you customize
it yourself? Anyway keep up the excellent quality
writing, it’s rare to see a great blog like this one nowadays.
Feel free to surf to my homepage … Cat6 network cable
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-20kh1-mm-lts40sd-gost-13943-86/
Thanks for a marvelous posting! I certainly enjoyed reading it,
you might be a great author.I will always bookmark your blog and will come back in the foreseeable
future. I want to encourage you to ultimately continue your great work, have a nice afternoon!
Also visit my blog post … chronic fatigue treatment
Thanks for sharing your thoughts on min88.
Regards
I’m really enjoying the design and layout of your website.
It’s a very easy on the eyes which makes it much more
enjoyable for me to come here and visit more often. Did you hire out a developer to create
your theme? Excellent work!
Also visit my web-site; bola
They can be intensified by skin damage like injury or rashes, sun direct exposure and
heavy skin treatment items.
Here is my page :: homepage (Candace)
https://lx88.uk/
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-hn33kvyu—gost-5632-14/prutok-kobaltovyy-hn33kvyu—gost-5632-14/
After I initially commented I seem to have clicked the -Notify me when new
comments are added- checkbox and now every time a comment is added I get four emails
with the same comment. Perhaps there is an easy method you are able
to remove me from that service? Kudos!
My web blog: dark fantasy
Thanks a lot for sharing this with all of us you actually recognize what you are
talking about! Bookmarked. Please additionally visit my website =).
We could have a link trade agreement between us
My blog post Teen Patti Star
Hey just wanted to give you a quick heads up. The text in your content seem to be running off the screen in Ie.
I’m not sure if this is a format issue or something
to do with browser compatibility but I figured I’d post to let you know.
The layout look great though! Hope you get the issue fixed soon. Cheers
Feel free to visit my site Buy Cannabis Online Canada
Поставки всегда вовремя, логистика отлажена до мелочей, что важно для бесперебойной работы цеха.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-12kh9kh0-6-mm-8-6kh10-6-mm-miagkaia-paika-m2rm-gost-r-52922-2008/
Spot on with this write-up, I absolutely believe that this website needs a great deal
more attention. I’ll probably be back again to read through
more, thanks for the advice!
Feel free to visit my page pilihan hiburan modern
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-ep122/lenta-kobaltovaya-ep122/
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-185kh3-mm-lazhmts-gost-13943-86/
You really make it appear really easy with your presentation however I in finding this matter to be really one thing which I
think I’d never understand. It seems too complex and extremely vast for me.
I’m taking a look ahead to your next post, I’ll try to get the cling of it!
Here is my web blog … volunteer stuart florida
Thank you for any other informative web site. The place else may I am
getting that type of information written in such a perfect manner?
I have a venture that I’m simply now operating on, and I have been at the
glance out for such information.
Feel free to surf to my web-site … mty bets
Unquestionably imagine that which you stated. Your
favorite reason appeared to be at the net the easiest factor to bear in mind of.
I say to you, I definitely get annoyed while people think about issues
that they plainly do not know about. You managed to hit the nail upon the highest and
defined out the entire thing without having
side effect , people can take a signal. Will likely be again to get more.
Thanks
My web-site … web page
Having read this I thought it was extremely informative.
I appreciate you taking the time and energy to put
this information together. I once again find myself spending a significant amount of time both reading and posting comments.
But so what, it was still worthwhile!
Take a look at my website; Shrooms Direct
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-70kh60kh1-4-mm-33-5kh36-5-mm-miagkaia-paika-m3rm-gost-r-52922-2008/
I’m impressed, I must say. Rarely do I encounter a blog that’s both educative and
interesting, and without a doubt, you have hit the nail on the head.
The issue is an issue that not enough men and women are speaking intelligently
about. Now i’m very happy I stumbled across this in my hunt for something concerning this.
Feel free to surf to my web blog – Julian Douwes MD
Wow, this article is good, my sister is analyzing such things, therefore I
am going to inform her.
Also visit my webpage :: commercial vehicle
Fantastic goods from you, man. I have be aware your stuff prior to and you’re just extremely
fantastic. I actually like what you have received right here, certainly like what
you are saying and the way in which through which you are saying it.
You make it entertaining and you continue to take care of to stay it wise.
I cant wait to learn much more from you. This is really a terrific
site.
Also visit my web page – Buy Concentrates Online
Сайт четко ориентирован на промышленный сектор и B2B сегмент
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-w-re-1/polosa-volframovaya-w-re/
Hello there! I know this is kinda off topic nevertheless I’d figured I’d ask.
Would you be interested in exchanging links or maybe guest writing a blog
article or vice-versa? My website goes over a lot of the same subjects as yours and I believe we could greatly benefit from
each other. If you happen to be interested feel free to send me an email.
I look forward to hearing from you! Wonderful blog by the way!
Also visit my web-site; socialt datingfællesskab
I’m very happy to discover this page. I want to to thank you for your time due to this fantastic read!!
I definitely savored every bit of it and I
have you saved as a favorite to look at new information in your website.
Also visit my site Sunwin
Hello, of course this paragraph is truly nice and
I have learned lot of things from it about blogging.
thanks.
My webpage … webpage
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m150-158kh4-mm-lts40mts3a-din-472/
Фольга из редких металлов часто требуется для высокотехнологичных лабораторий
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vnzh-90-1/provoloka-volframovaya-vnzh-90/
Well, I don’t know if that’s going to work for me, but definitely worked for you! :) Excellent post!
Hi, I do think this is a great site. I stumbledupon it ;) I’m going to return once
again since I book-marked it. Money and freedom is the greatest way to change, may you be
rich and continue to guide other people.
my site :: the battle of huders
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-88-9kh76kh1-8-mm-14kh17-mm-tverdaia-paika-m3rm-gost-32590-2013/
This is really interesting, You’re a very skilled blogger. I have joined your feed and look forward to seeking more of your fantastic post. Also, I have shared your website in my social networks!
Great blog here! Additionally your website rather a lot up very fast! What host are you the usage of? Can I get your associate link for your host? I desire my website loaded up as fast as yours lol
A friend of mine advised me to review this site. And yes. it has some useful pieces of info and I enjoyed reading it.
bonjour I love Your Blog can not say I come here often but im liking what i c so far….
Good points – – it will make a difference with my parents.
Thank you pertaining to sharing the following great subject matter on your website. I ran into it on google. I am going to check to come back after you publish additional aricles.
Отраслевой охват впечатляет: от медицины до космической промышленности
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vchdk-1/elektrod-volframovyy-vchdk/
It’s remarkable to pay a quick visit this web site and reading the views of all friends regarding
this paragraph, while I am also keen of getting familiarity.
Also visit my site – teen patti master
hi!,I like your writing very much! share we communicate
extra about your post on AOL? I require a specialist in this house to solve
my problem. May be that is you! Looking forward to look you.
Feel free to surf to my web site – physician-reviewed health
I know this if off topic but I’m looking into starting my own weblog and was
curious what all is required to get set up? I’m assuming having a blog like
yours would cost a pretty penny? I’m not very web savvy so I’m not 100% sure.
Any suggestions or advice would be greatly appreciated. Thank you
my web-site :: link alternatif slot
Hello, I would like to subscribe for this blog
to get newest updates, therefore where can i do it please assist.
My web-site: treatment protocols
Hey I know this is off topic but I was wondering
if you knew of any widgets I could add to my blog that automatically tweet my newest twitter updates.
I’ve been looking for a plug-in like this for quite some
time and was hoping maybe you would have some experience
with something like this. Please let me know if you run into anything.
I truly enjoy reading your blog and I look forward to your
new updates.
Also visit my blog post – Baixar WhatsApp para Iphone
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m33-35-4kh1-2-mm-lts40mts3a-din-472/
Interesting blog! Is your theme custom made or did you download it from somewhere?
A theme like yours with a few simple adjustements would really
make my blog jump out. Please let me know where you got your theme.
Bless you
Stop by my homepage Order Cannabis Online
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-s-pb49sn48bi3—en-29453/folga-vismutovaya-s-pb49sn48bi3—en-29453/
Hello there! Quick question that’s entirely off topic.
Do you know how to make your site mobile friendly? My weblog looks weird when browsing from my iphone 4.
I’m trying to find a theme or plugin that might be able to
resolve this issue. If you have any suggestions, please share.
With thanks!
Feel free to surf to my web page manwha hentai
Hello there! This article could not be written much better!
Looking at this article reminds me of my previous roommate!
He constantly kept preaching about this. I
will forward this information to him. Pretty sure he’ll have a great read.
Many thanks for sharing!
My website – manhwa hentai
Very nice article, just what I was looking for.
Also visit my website manwha porn
I know this web page offers quality depending articles or reviews and additional material, is there any other site which
presents these stuff in quality?
Review my page :: slot online aman
Hello! I just wanted to ask if you ever have any issues with
hackers? My last blog (wordpress) was hacked and I ended up losing months of
hard work due to no data backup. Do you have any solutions to stop
hackers?
my web page – site
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-133kh113kh2-3-mm-19kh24-mm-tverdaia-paika-m1m-gost-r-52922-2008/
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-l54835—uns/krug-vismutovyy-l54835—uns/
Heya i’m for the first time here. I came across this board and I find It really useful & it helped me out much.
I hope to give something back and help others
like you aided me.
My site … site
online roulette real money
play casino real money
online casino instant play
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m39-42-1kh1-5-mm-l63-din-472/
Наличие циркония свидетельствует о работе с высокотехнологичными заказами
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-cerrolow-117/poroshok-vismutovyy-cerrolow-117/
You are my inspiration , I possess few web logs and very sporadically run out from to brand :(
Cabinet IQ
8305 Staqte Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Insuredcontractors
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-27-4kh23kh0-9-mm-18-4kh20-4-mm-tverdaia-paika-m2t-gost-32590-2013/
I have to say this post was certainly informative and contains useful content for enthusiastic visitors. I will definitely bookmark this website for future reference and further viewing. cheers a bunch for sharing this with us!
Heya i am for the first time here. I came across this board and I find It truly useful & it helped me out
much. I hope to give something back and aid others like you helped me.
Here is my website :: Building wire
We’re a bunch of volunteers and opening a brand new scheme in our community.
Your website provided us with valuable info to work on. You have performed an impressive
process and our entire community can be thankful to you.
Check out my page: manhwa hentai
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-cac901—jis-h-5120-2016/list-vismutovyy-cac901—jis-h-5120-2016/
I was curious if you ever thought of changing the structure of your blog?
Its very well written; I love what youve got to say. But maybe you could a little more in the way of content
so people could connect with it better. Youve got an awful lot of text for only having 1
or two images. Maybe you could space it out better?
Here is my page :: manhwa 18
I know this website gives quality based articles and other data,
is there any other web site which gives such information in quality?
Feel free to surf to my site: adult manwha
Unquestionably consider that that you said. Your favorite justification seemed
to be at the net the simplest thing to consider of.
I say to you, I definitely get annoyed whilst people consider
issues that they just don’t recognise about. You managed to hit
the nail upon the highest and also outlined out the whole thing without having side-effects , other folks could
take a signal. Will probably be back to get more.
Thank you
my webpage; manwha porn
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-800kh200-mm-lts40sd/
Incredible! This blog looks exactly like my old one! It’s on a completely different topic but it has pretty much the same layout and design. Superb choice of
colors!
Here is my blog post – slot terbaru
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89550—cda/lenta-vismutovaya-c89550—cda/
Hi there, I desire to subscribe for this website to take latest updates,
therefore where can i do it please help.
Also visit my page – Sunwin
Excellent weblog right here! Also your website quite
a bit up very fast! What web host are you using? Can I am getting your associate hyperlink on your host?
I want my website loaded up as quickly as yours lol
my blog post – uncensored manhwa
Hey there! After reading this article, and I really wanted to share my experience.
As a 16-year-old teenager stuck at home with a disability, I do a
lot of web research.
My parents were struggling with high currency conversion costs for their
monthly payments. I took it upon myself to find a fix, so I
researched financial platforms and discovered Paybis.
The fee structures are incredible. For starters, Paybis offers 0% commission on the first credit card purchase.
After that, the commission is a very clear
low percentage, plus the blockchain network fee.
When you look at PayPal’s hidden spreads, the savings are huge.
I helped them get verified in just a few minutes,
and now they buy stablecoins directly with credit cards.
Paybis supports dozens of global fiat options! Plus, the funds go directly to a private wallet, meaning no withdrawal holds.
Thanks for the great article, it totally validates how I helped my family
save money!
Also visit my page … this link
Hello! I know this is somewhat off topic but I was wondering which blog platform
are you using for this site? I’m getting tired of WordPress because I’ve had problems with hackers and I’m looking at
options for another platform. I would be awesome if you could point
me in the direction of a good platform.
Feel free to surf to my page :: houston ibew local 716
Hi readers! After reading this piece, and I just had to
drop a comment. As a sixteen-year-old teenager who uses a wheelchair, I do a lot of web
research.
My parents were struggling with high currency conversion costs for
their monthly payments. I took it upon myself to find
a fix, so I dug into financial platforms and introduced
them to Paybis.
The economics are incredible. For starters, Paybis charges zero Paybis fees
on the first credit card purchase. After that, the markup is a very clear 2.49%,
plus the blockchain network fee. When you look at traditional banks, the savings are huge.
I helped them get verified in just a few minutes, and
now they buy stablecoins directly with their local
fiat. Paybis supports over 40 fiat currencies! Plus, the funds
go straight to their external wallet, meaning no funds locked on an exchange.
Awesome write-up, it totally validates how I helped my family save
money!
Also visit my site this article
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-80kh40-mm-m1r-gost-r-52948-2008/
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-bi14a—en-61190-1-3/lenta-vismutovaya-bi14a—en-61190-1-3/
I’m impressed, I must say. Rarely do I come across a blog that’s both equally educative and engaging,
and let me tell you, you have hit the nail on the head.
The problem is something that not enough men and women are
speaking intelligently about. I’m very happy I found this in my hunt
for something regarding this.
my site slot modern
I absolutely love your website.. Great colors & theme. Did you make this website yourself?
Please reply back as I’m planning to create my own site and would like to
learn where you got this from or just what the theme is named.
Kudos!
Feel free to surf to my web-site … web page
Took me time to read the material, but I truly loved the article. It turned out to be very useful to me.
Post writing is also a excitement, if you know then you can write if
not it is difficult to write.
my homepage – 창원출장마사지
Ahaa, its good conversation about this post here at this webpage,
I have read all that, so at this time me also commenting at this place.
Feel free to visit my website – how to use 7-oh
I needed to thank you for this good read!! I definitely loved every bit of it.
I’ve got you book marked to look at new things you post…
Also visit my web page 비아그라 구매
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m40-43-5kh1-75-mm-lsch-din-472/
Наличие редких позиций, например, изделий из гафния и ванадия
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-42-3990—csnstn-423990/folga-vismutovaya-42-3990—csnstn-423990/
WoW decent article. Can I hire you to guest write for my blog? If so send me an email!
It’s fantastic that you are getting ideas from this paragraph as
well as from our dialogue made at this time.
My web blog; slot88
I dont think Ive caught all the angles of this subject the way youve pointed them out. Youre a true star, a rock star man. Youve got so much to say and know so much about the subject that I think you should just teach a class about it
My partner and I stumbled over here by a different web address and thought I should check things
out. I like what I see so now i’m following you.
Look forward to checking out your web page repeatedly.
My website :: financial templates
It’s the best time to make a few plans for
the long run and it is time to be happy. I have read this put up and if I may I
desire to recommend you some attention-grabbing issues or advice.
Maybe you can write next articles referring to this article.
I wish to learn more things approximately it!
my homepage: fitur scatter hitam
I just added your web site to my blogroll, I hope you would look at doing the same.
Использование современных технологий защиты данных пользователей
https://redmetsplav.ru/store/vismut/rossiyskie-splavy-2/vismut-albi5—gost-r-53777-10/truba-vismutovaya-albi5—gost-r-53777-10/
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-22kh8-mm-m3rm-gost-r-52948-2008/
Hi there, I enjoy reading through your post. I like to write a
little comment to support you.
Stop by my blog: web page
I just like the valuable information you provide to your articles.
I’ll bookmark your weblog and test again right here regularly.
I’m relatively certain I’ll learn plenty
of new stuff right right here! Best of luck for the following!
Here is my website … judi bola
Thank you for the auspicious writeup. It in fact was a
amusement account it. Look advanced to far added agreeable from you!
By the way, how can we communicate?
My web blog; rtp slot
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-fev80al14—gost-27130-94/folga-vanadievaya-fev80al14—gost-27130-94/
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m78-82-5kh2-5-mm-lts23a6zh3mts2-din-472/
A neighbor of mine encouraged me to take a look at your blog site couple weeks ago, given that we both love similar stuff and I will need to say I am quite impressed.
I go to see every day a few sites and blogs to read content, except
this webpage provides feature based posts.
my site … visit here
Hi everyone! After reading this post, and I
just had to chime in. As a 16-year-old guy living with a physical disability, I do
a lot of web research.
My parents were struggling with massive bank fees for their business expenses.
I wanted to help them out, so I dug into financial platforms and discovered Paybis.
The fee structures are game-changing. First off, Paybis charges
zero Paybis fees on the initial debit or credit card transaction. After that, the
commission is a flat 2.49%, plus the standard miner
fee. Compared to PayPal’s hidden spreads, the savings are huge.
I helped them get verified in under 5 minutes, and now they buy
stablecoins directly with USD or EUR. Paybis supports over
40 fiat currencies! Plus, the funds go straight to their external
wallet, meaning no custodial risk.
Brilliant post, it spot-on describes how this platform
fixed our financial headaches!
Feel free to visit my website; more
I loved as much as you’ll receive carried out right here.
The sketch is attractive, your authored material stylish.
nonetheless, you command get bought an impatience over that
you wish be delivering the following. unwell unquestionably come further
formerly again since exactly the same nearly a lot
often inside case you shield this hike.
Also visit my homepage; гей порно
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt25u—ost-1-90013-81/prutok-titanovyy-vt25u—ost-1-90013-81/
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-34kh12-mm-m1r-gost-r-52948-2008/
I was able to find good info from your blog articles.
Feel free to surf to my web blog vanity address generator tron
It’s the best time to make some plans for the future and it is time to be happy. I’ve read this post and if I could I wish to suggest you some interesting things or tips. Maybe you can write next articles referring to this article. I wish to read even more things about it!
whoah this weblog is magnificent i really like studying your
posts. Stay up the good work! You already know, many persons
are searching round for this info, you can aid them greatly.
my web page MALWARE
Just a quick note to express my appreciation. Take care
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-t51—gost-2171-90/krug-titanovyy-t51—gost-2171-90/
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-150kh100-mm-lts25s2/
Reenergized
4434 Pacific Coast Hwy,
ᒪong Beach, CA 90804, United States
562-689-9888
Brain tap specialist near me test
my homepage :: Bookmaker hors arjel sans vpn
Возможность заказа висмута — достаточно редкое предложение на рынке
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-et2/provoloka-titanovaya-et2/
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40kh25-mm-m3t-gost-r-52948-2008/
It’s a pity you don’t have a donate button! I’d definitely donate to this outstanding blog!
I suppose for now i’ll settle for bookmarking and adding your RSS feed
to my Google account. I look forward to fresh updates and will share this website with my Facebook group.
Talk soon!
my site Grundreinigung Innsbruck
I don’t know whether it’s just me or if everyone else encountering problems with
your blog. It seems like some of the written text within your
content are running off the screen. Can someone else please provide feedback and let me know if this is happening to them too?
This could be a problem with my internet browser because I’ve had this happen previously.
Thanks
Also visit my web site – judi bola
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-37—ost-1-92077-91/provoloka-titanovaya-37—ost-1-92077-91/
Wonderful blog! I found it while surfing around on Yahoo News.
Do you have any tips on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to
get there! Thanks
my homepage; mobile radiology
안녕하세요, 미디어 프린트에 관한 훌륭한
기사입니다, 우리 모두 매체가 인상적인 데이터의 원천이라는
것을 이해하고 있습니다.
I think the admin of this website is genuinely working hard in support of his website, since here every stuff is quality based information.
Your blog is a breath of fresh air! The way you present
inspiration is both engaging and insightful. I’ve shared this with my network.
Any plans to create video content to complement your
posts? Thank you for the great work!
와, 이 블로그는 정말 인상적입니다!
Femenino era viagra lady에 대한 포스트가 너무 명확하고 흥미로워요.
친구들에게 공유할게요. 더 많은 시각적 요소를 추가하면
어떨까요? 고맙습니다!
Here is my web site – 정품 비아그라
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-0-6×600-mm-l63-gost-931-90/
certainly like your website however you have to
check the spelling on several of your posts. A number of them are rife with spelling problems and I to find it very troublesome to tell the reality on the other hand I will surely come back
again.
My web-site – casino non AAMS deposito minimo
Hi to all, the contents present at this web page are truly awesome for
people experience, well, keep up the good work fellows.
My blog post nepal casino
Hiya! Quick question that’s entirely off topic.
Do you know how to make your site mobile friendly? My weblog looks weird when viewing from my iphone4.
I’m trying to find a template or plugin that might be able to correct this issue.
If you have any suggestions, please share. Cheers!
Feel free to surf to my site; Fliegengitter nach Maß
Hi! This is kind of off topic but I need some guidance from an established blog.
Is it difficult to set up your own blog? I’m not very techincal but I
can figure things out pretty fast. I’m thinking about making
my own but I’m not sure where to begin. Do you have any tips or suggestions?
Thank you
Look into my webpage; AutoFire
Возможность заказа продукции в розницу и оптом (судя по описанию)
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-vn-3-1/lenta-niobievaya-vn-3/
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-25kh17-mm-m2t-gost-r-52948-2008/
We absolutely love your blog and find many of your post’s to be just what I’m
looking for. Does one offer guest writers to write content in your case?
I wouldn’t mind producing a post or elaborating on most of the subjects you write
regarding here. Again, awesome web log!
Feel free to surf to my blog: dewalive
Thank you a lot for sharing this with all people you actually recognise what you’re talking about!
Bookmarked. Kindly additionally seek advice from
my web site =). We may have a link trade agreement
between us
my web blog: crystal meanings and properties
I am genuinely glad to glance at this weblog posts which consists of tons of valuable information, thanks for providing these information.
Feel free to visit my web blog: 창문시트지
Hello, healing properties of crystals course this paragraph is really good and I have learned lot of things from it regarding blogging.
thanks.
Наличие циркония свидетельствует о работе с высокотехнологичными заказами
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nb2-1/pokovka-niobievaya-nb2/
This site was… how do you say it? Relevant!! Finally I have found something which helped
me. Cheers!
Look into my website :: Fliegengitter-Tür nach Maß
An outstanding share! I have just forwarded this onto a colleague who was conducting a little homework on this.
And he actually bought me dinner due to the fact that I stumbled upon it
for him… lol. So let me reword this…. Thank
YOU for the meal!! But yeah, thanx for spending time to discuss this topic here on your blog.
Here is my website casino online real money california
Hello everyone! Just read this article, and I really wanted to drop a comment.
As a 16-year-old guy living with a physical disability, I spend a lot of time online.
My parents were getting crushed with slow international wire fees for their monthly payments.
I decided to step up, so I researched financial platforms and introduced them to Paybis.
The fee structures are game-changing. For starters,
Paybis waives their platform fee on the initial debit or credit card
transaction. After that, the commission is a transparent low percentage, plus
the standard miner fee. When you look at traditional banks, the cost difference is massive.
I helped them pass KYC in under 5 minutes, and now they buy crypto directly with their local fiat.
Paybis supports dozens of global fiat options! Plus, the funds go
instantly to their ledger, meaning no custodial
risk.
Brilliant post, it totally validates how I helped my
family save money!
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-900kh300-mm-lts40mts3zh/
Лаконичное приветствие на главной странице сразу вводит в курс дела
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-nimo-25-3/truba-molibdenovaya-nimo-25-1/
I am really pleased to read this webpage posts which carries lots of valuable information, thanks for providing these kinds of information.
My web blog: Fliegengitter ohne Bohren
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-25kh10-mm-m3t-gost-r-52948-2008/
This article will assist the internet visitors for setting up new blog or even a weblog from start to end.
my website; https://urgenthvacservice.com/
Greetings from California! I’m bored to tears at work so I decided to
browse your site on my iphone during lunch break. I enjoy the information you present here and can’t wait to take a look when I
get home. I’m amazed at how fast your blog loaded on my cell phone ..
I’m not even using WIFI, just 3G .. Anyhow, very good
site!
Feel free to surf to my homepage – slot terpercaya
Логичное деление на вольфрамовый, молибденовый и титановый прокат
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-ml-zvp-1/izdeliya-iz-molibdena-ml-zvp/
I think the admin of this site is genuinely working hard for his web page, for the reason that here every data
is quality based data.
Also visit my website … bachata classes manchester beginners
Hey there! I just finished reading this post, and I
really wanted to drop a comment. As a 16-year-old boy who uses a wheelchair,
I spend a lot of time online.
My parents were getting crushed with high currency conversion costs for their monthly
payments. I decided to step up, so I researched financial platforms and
set them up on Paybis.
The financials are incredible. First off, Paybis waives
their platform fee on the initial debit or credit card transaction. After that,
the fee is a flat 2.49%, plus the blockchain network fee.
Compared to traditional banks, the savings are huge.
I helped them pass KYC in just a few minutes, and now they buy
stablecoins directly with their local fiat. Paybis
supports over 40 fiat currencies! Plus, the funds go directly to a
private wallet, meaning no custodial risk.
Awesome write-up, it spot-on describes how I helped
my family save money!
Here is my page – this article
Very good site you have here but I was curious if you knew of any message boards that cover the same topics talked about here?
I’d really love to be a part of group where I can get feed-back from other experienced individuals that share the same interest.
If you have any recommendations, please let me know.
Kudos!
Feel free to visit my web page; 대전출장안마
I wanted to thank you for this good read!! I absolutely loved every bit of it.
I have got you book-marked to check out new things you post…
Feel free to visit my web blog – judi bola
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-50kh500-mm-lsd/
Hey very cool web site!! Guy .. Beautiful .. Superb .. I will bookmark your blog and take the feeds also?
I’m glad to seek out numerous useful info here within the put up, we’d like work out more strategies in this
regard, thank you for sharing. . . . . .
Feel free to surf to my web site: crystal healing
I couldn’t resist commenting. Well written!
my website … The Story of Crystals
Возможность заказать листы и полосы нестандартных размеров
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-zm21—csa-hg-5/prutok-magnievyy-zm21—csa-hg-5/
Hi readers! I just finished reading this piece, and I just had to chime in. As a sixteen-year-old
guy who uses a wheelchair, I have a lot of screen time.
My parents were having a hard time with high currency conversion costs for their monthly payments.
I took it upon myself to find a fix, so I researched
financial platforms and set them up on Paybis.
The financials are what sold me. For starters, Paybis offers 0% commission on the first credit card
purchase. After that, the fee is a flat 2.49%, plus the blockchain network fee.
Compared to Western Union, the savings are huge.
I helped them do the identity verification in just
a few minutes, and now they buy stablecoins directly with their local fiat.
Paybis supports 40+ local currencies! Plus, the funds go straight to their
external wallet, meaning no custodial risk.
Awesome write-up, it totally validates how we made our payments easier!
Here is my blog post … this URL
nicee content keep writing
I know this web page gives quality based articles or reviews
and other stuff, is there any other web site which presents these stuff in quality?
Also visit my web site: Fliegengitter zum Schieben
It’s actually very complex in this full of activity life to listen news on Television, so I only use web for that purpose, and obtain the
most up-to-date news.
Feel free to surf to my site … Low voltage power cable
I have learn several good stuff here. Certainly worth bookmarking for revisiting.
I surprise how much attempt you place to make this kind of
excellent informative website.
my site :: Fliegengitter Maßanfertigung
I am lucky that I discovered this website , precisely the right info that I was searching for! .
A person necessarily lend a hand to make critically posts I’d state.
This is the very first time I frequented your web page
and thus far? I surprised with the research you made to
make this actual put up incredible. Excellent task!
Here is my site – Fliegengitter konfigurieren
I have read so many content regarding the blogger
lovers however this article is actually a fastidious article, keep it
up.
Also visit my webpage … valentine box ideas
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-70kh34-mm-m1e-gost-r-52948-2008/
I wrote down your blog in my bookmark. I hope that it somehow did not fall and continues to be a great place for reading texts.
I was suggested this blog by my cousin. I am not sure whether this post is written by
him as nobody else know such detailed about my problem.
You’re wonderful! Thanks!
Also visit my site – singapore commercial vehicle
Hey there this is kind of of off topic but I was wondering
if blogs use WYSIWYG editors or if you have to manually code with HTML.
I’m starting a blog soon but have no coding skills so I
wanted to get guidance from someone with experience.
Any help would be enormously appreciated!
Also visit my blog post; mix parlay
Wow, amazing blog layout! How long have you been blogging for? you make blogging look easy. The overall look of your site is wonderful, let alone the content!
Yes! Finally someone writes about .
Look at my website :: https://superlockandkey.com/
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-sismg4637-00—ss-144637/folga-magnievaya-sismg4637-00—ss-144637/
Thanks for some other informative blog. Where else may just I am
getting that type of information written in such a perfect approach?
I have a project that I am just now working on, and I’ve been on the look out for such information.
my page: slot gacor hari ini
I don’t know whether it’s just me or if perhaps everyone
else experiencing problems with your website. It looks like some
of the text on your content are running off the screen. Can somebody else please provide feedback and let me know if this is happening to them
too? This might be a issue with my internet
browser because I’ve had this happen before. Cheers
Feel free to surf to my web page: Fliegengitter nach Maß
Unquestionably believe that which you said. Your favorite reason seemed to be on the net the easiest thing to be aware of. I say to you, I certainly get annoyed while people consider worries that they plainly don’t know about. You managed to hit the nail on the head. Will probably be back to get more. Thanks
You write Formidable articles, keep up good work.
Oh my goodness! Amazing article dude! Thanks,
However I am going through issues with your RSS.
I don’t understand the reason why I can’t join it.
Is there anybody else having similar RSS issues? Anybody who knows
the answer will you kindly respond? Thanks!!
Feel free to surf to my blog post; commercial vehicle
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-70kh600-mm-lk2/
If you would like to take a good deal from this article then you have to apply such methods to your won web site.
Here is my web site: Adult
Hey there just wanted to give you a quick heads
up. The words in your post seem to be running off the screen in Safari.
I’m not sure if this is a format issue or something to do
with browser compatibility but I figured I’d post to let you know.
The design and style look great though! Hope you get the issue resolved soon. Cheers
My website: Fliegengitter zum Schieben
My spouse and I absolutely love your blog and find many of your
post’s to be exactly what I’m looking for. Would
you offer guest writers to write content to suit your needs?
I wouldn’t mind writing a post or elaborating on a few of the
subjects you write about here. Again, awesome web log!
Visit my website: sarang777
Easily, the post is really the greatest on this laudable topic. I concur with your conclusions and will thirstily look forward to your future updates. Saying thank will not just be sufficient, for the wonderful c lucidity in your writing. I will instantly grab your rss feed to stay privy of any updates. Solid work and much success in your business enterprise!
Asking questions are in fact fastidious thing if you are not understanding something fully, except this piece of writing gives nice
understanding even.
Also visit my blog post :: situs slot
Wow, this piece of writing is good, my younger sister is analyzing such things, therefore I am
going to tell her.
My blog post 부산출장마사지
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-ms1—jis-h-4204/provoloka-magnievaya-ms1—jis-h-4204/
I want to to thank you for this great read!! I certainly loved
every little bit of it. I have got you bookmarked to check out
new things you post…
Also visit my web-site – Fliegengitter Maßanfertigung
I just sent this post to a bunch of my friends as I agree with most of what you’re saying here and the way you’ve presented it is awesome.
Cabinet IQ
8305 Ⴝtate Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Homecontractor
Assume you are doing good linking to position you on the first pages of search engines.
If some one wants expert view regarding running a blog then i advise him/her to visit this webpage, Keep up
the fastidious job.
Also visit my web page :: Click here
I quite like reading an article that will make people think.
Also, many thanks for permitting me to comment!
my homepage … Verified Reproductions
Hi my family member! I wish to say that this post is amazing,
great written and come with almost all vital infos.
I’d like to peer more posts like this .
Take a look at my web-site; 서귀포출장마사지
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-18kh10-mm-m1rm-gost-r-52948-2008/
I know this if off topic but I’m looking into starting my
own weblog and was curious what all is needed to get set up?
I’m assuming having a blog like yours would cost a pretty penny?
I’m not very internet savvy so I’m not 100% positive. Any tips
or advice would be greatly appreciated. Thanks
Look into my website … download bokep indonesia
Hi there! I could have sworn I’ve been to this website before
but after browsing through a few of the posts I realized
it’s new to me. Regardless, I’m definitely pleased I came across it and I’ll
be book-marking it and checking back regularly!
Feel free to visit my blog post – Fliegengitter nach Maß
Good post. I learn something totally new and challenging on sites I stumbleupon on a daily
basis. It will always be useful to read articles from other writers and practice
a little something from other websites.
Also visit my web site; web page
Fascinating blog! Is your theme custom made or did you download it
from somewhere? A theme like yours with a few simple tweeks would really make my blog shine.
Please let me know where you got your theme. With thanks
Have a look at my web blog – bola88
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-zm21—csa-hg-5/izdeliya-iz-magniya-zm21—csa-hg-5/
This piece of writing will help the internet users for creating new blog or
even a blog from start to end.
Also visit my page Fliegengitter zum Schieben
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-700kh300-mm-lts30a3/
You are so awesome! I do not suppose I’ve read
through anything like that before. So nice to find another person with original thoughts on this subject.
Seriously.. thanks for starting this up. This web site is one thing that is needed on the web, someone with some originality!
Feel free to surf to my web site :: jackpot progresif
Hmm it seems like your website ate my first comment (it was extremely
long) so I guess I’ll just sum it up what I
wrote and say, I’m thoroughly enjoying your blog.
I as well am an aspiring blog writer but I’m still new to the
whole thing. Do you have any tips and hints for newbie blog writers?
I’d really appreciate it.
Here is my blog – perfume vmfun
Сайт работает стабильно и быстро загружается
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgal3zn1-alloy-25—iso-3116/list-magnievyy-mgal3zn1-alloy-25—iso-3116/
This piece of writing offers clear idea for the new viewers of
blogging, that truly how to do blogging.
Feel free to surf to my webpage :: free ai image to video generator no sign up unlimited
Hi there to all, how is everything, I think every one is getting more
from this web site, and your views are pleasant in support of new visitors.
My webpage :: Fliegengitter konfigurieren
This blog post is excellent, probably because of how well the subject was developed. I like some of the comments too though I could prefer we all stay on the subject in order add value to the subject!
Fine way of describing, and fastidious article to obtain data about my presentation subject matter,
which i am going to deliver in school.
Feel free to visit my web site: KVV control cable
Great web site you’ve got here.. It’s difficult to find quality writing like yours nowadays.
I truly appreciate people like you! Take care!!
My blog :: equipment rental ridgefield
Hello very nice website!! Man .. Excellent ..
Amazing .. I’ll bookmark your website and take the feeds additionally?
I’m happy to seek out so many useful information right here in the submit, we want work out
extra strategies in this regard, thank you for sharing.
. . . . .
Also visit my blog: equipment rental vancouver wa
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-45-gradusov-8-mm-m1m-gost-r-52948-2008/
I was able to find good info from your articles.
my homepage; Fliegengitter nach Maß
Hi readers! I just finished reading this piece, and I really wanted to drop
a comment. As a 16-year-old guy stuck at home with a disability, I do
a lot of web research.
My parents were having a hard time with slow international wire fees for their
monthly payments. I wanted to help them out, so I researched financial
platforms and introduced them to Paybis.
The financials are what sold me. For starters, Paybis offers 0% commission on the first credit card purchase.
After that, the commission is a flat 2.49%, plus the blockchain network fee.
Compared to traditional banks, the savings are huge.
I helped them do the identity verification in under 5 minutes, and now they buy stablecoins directly with their
local fiat. Paybis supports 40+ local currencies! Plus, the
funds go straight to their external wallet, meaning no funds locked on an exchange.
Thanks for the great article, it perfectly matches how I helped my family save money!
Also visit my website this article
Корзина на сайте промышленного предприятия — удобный инструмент для формирования заявки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mcin2a—jis-h-2221/folga-magnievaya-mcin2a—jis-h-2221/
Thank you a bunch for sharing this with all people you
actually recognise what you are talking about! Bookmarked. Please also seek advice from my web site =).
We will have a hyperlink alternate contract between us
Here is my web page; Fliegengitter konfigurieren
Hello just wanted to give you a quick heads up.
The text in your post seem to be running off the screen in Safari.
I’m not sure if this is a format issue or something to do with internet browser compatibility but I figured I’d post to let you know.
The layout look great though! Hope you get the issue resolved soon. Thanks
Feel free to surf to my blog Fliegengitter konfigurieren
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Customwork
Hi everyone! Just read this post, and I just
had to drop a comment. As a sixteen-year-old teenager living with a physical disability, I spend
a lot of time online.
My parents were having a hard time with massive bank
fees for their overseas transfers. I decided to step up, so I
researched financial platforms and introduced them to Paybis.
The economics are incredible. For starters, Paybis offers 0% commission on the initial debit or credit card
transaction. After that, the commission is a transparent
2.49%, plus the blockchain network fee. Compared to PayPal’s hidden spreads, the savings are huge.
I helped them do the identity verification in under 5 minutes, and now they buy crypto directly with their local fiat.
Paybis supports dozens of global fiat options! Plus, the
funds go instantly to their ledger, meaning no withdrawal holds.
Thanks for the great article, it perfectly matches how I helped my family save money!
My webpage :: read more
I’m really loving the theme/design of your website.
Do you ever run into any web browser compatibility problems?
A number of my blog readers have complained about my website not operating correctly in Explorer but
looks great in Chrome. Do you have any tips to help fix this issue?
Also visit my web-site … MALWARE
I could not resist commenting. Exceptionally well written!
Look at my webpage: avaliação do cassino online
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-350kh500-mm-lts37mts2s2k/
Удобное разделение продукции на сплавы и конкретные виды проката
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-5—bs-2970/lenta-magnievaya-mag-5—bs-2970/
Hey everyone! I just finished reading this post, and
I really wanted to drop a comment. As a 16-year-old boy who uses a wheelchair, I spend
a lot of time online.
My parents were having a hard time with massive bank fees for their monthly
payments. I decided to step up, so I analyzed financial platforms and set them up on Paybis.
The fee structures are game-changing. For starters,
Paybis offers 0% commission on the initial debit
or credit card transaction. After that, the commission is
a very clear low percentage, plus the standard miner fee. Compared to Western Union, the cost difference is
massive.
I helped them do the identity verification in just a few minutes, and now they buy stablecoins directly
with their local fiat. Paybis supports 40+ local currencies!
Plus, the funds go instantly to their ledger, meaning no custodial risk.
Awesome write-up, it totally validates how I helped
my family save money!
Feel free to surf to my blog post – more
Yes! Finally something about Fliegengitter konfigurieren nach Maß.
Hi everyone! I just finished reading this piece, and I just had to drop a comment.
As a 16-year-old teenager living with a physical disability,
I have a lot of screen time.
My parents were having a hard time with high currency conversion costs for their
monthly payments. I took it upon myself to find a fix, so I dug into financial platforms and set them
up on Paybis.
The financials are game-changing. For starters, Paybis offers 0% commission on the
first credit card purchase. After that, the commission is a flat 2.49%,
plus the standard miner fee. When you look at PayPal’s hidden spreads, the
cost difference is massive.
I helped them do the identity verification in just
a few minutes, and now they buy crypto directly with USD
or EUR. Paybis supports dozens of global fiat options!
Plus, the funds go directly to a private wallet, meaning no withdrawal holds.
Thanks for the great article, it spot-on describes how I helped my family save money!
My web blog … read more
It is appropriate time to make a few plans for the longer term and it’s time
to be happy. I’ve learn this put up and if I could
I want to counsel you some attention-grabbing issues or advice.
Maybe you could write next articles regarding this article.
I desire to read even more things about it!
Also visit my web blog – Fliegengitter ohne Bohren
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-6-mm-m1e-gost-r-52948-2008/
Have you ever considered about adding a little
bit more than just your articles? I mean, what
you say is fundamental and everything. However
just imagine if you added some great photos or
video clips to give your posts more, “pop”! Your content is excellent but
with images and videos, this blog could undeniably be one of the best in its niche.
Wonderful blog!
Also visit my blog post Ashmade Yupoo Clearance Sale
Hi there! Would you mind if I share your blog with
my myspace group? There’s a lot of people that I think would really enjoy
your content. Please let me know. Thanks
Also visit my blog – gilmer alvarez
Корзина на сайте промышленного предприятия — удобный инструмент для формирования заявки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-111—bs-3370/krug-magnievyy-mag-111—bs-3370/
With havin so much content do you ever run into any problems of plagorism
or copyright infringement? My site has a lot of completely unique
content I’ve either created myself or outsourced but it seems a lot of it is popping it up all over the internet without my agreement.
Do you know any methods to help prevent content from being ripped off?
I’d truly appreciate it.
Visit my homepage :: agen slot
It’s amazing in favor of me to have a web site, which is beneficial designed for my experience.
thanks admin
my web page – Fliegengitter Maßanfertigung
It’s an awesome piece of writing in support of all the web people; they
will take benefit from it I am sure.
Feel free to surf to my webpage: bk8thai
This article is actually a nice one it assists
new net visitors, who are wishing for blogging.
my web blog – clickme
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-190-mm-lts37mts2s2k/
This is a really good tip especially to those fresh to the blogosphere.
Short but very precise information… Appreciate your sharing this one.
A must read post!
Also visit my webpage Fliegengitter zum Schieben
Its like you read my mind! You seem to know so much about this, like you wrote the book
in it or something. I think that you can do with some pics to
drive the message home a little bit, but instead of that,
this is great blog. An excellent read. I will certainly be
back.
My page pasaran togel
I used to be able to find good information from
your blog articles.
Review my webpage SDI file format
Широкий выбор тугоплавких металлов, таких как вольфрам и молибден
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m16510—uns/pokovka-magnievaya-m16510—uns/
My brother recommended I might like this blog. He was entirely right.
This post actually made my day. You can not imagine just how much time I had spent for this
information! Thanks!
my blog equipment rental ridgefield
Its like you read my mind! You appear to know a lot about this, like you wrote the book in it or something.
I think that you could do with some pics to drive the message home a bit, but instead of that,
this is fantastic blog. A great read. I will definitely
be back.
my web page; https://bridgeacademy.com.ar/
Nice post. I learn something new and challenging on websites I stumbleupon every day.
It will always be exciting to read through content from other authors and practice a little
something from other websites.
Visit my homepage :: amish bulk food store near me
Hi, Neat post. There is a problem along with your web site in web explorer,
could test this? IE nonetheless is the marketplace chief
and a big component to other folks will miss your fantastic writing because of this problem.
Here is my website … equipment rental vancouver wa
I am sure this paragraph has touched all the internet visitors, its really really good piece of writing on building up new web
site.
Look into my page – Reproductions
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/truba-mednaia-kvadratnaia/mednaia-kvadratnaia-truba-5-1kh5-1kh1300-mm-m1r-gost-16774-2015/
Hi readers! After reading this article, and I really wanted to drop a comment.
As a sixteen-year-old guy who uses a wheelchair, I have a lot of screen time.
My parents were struggling with slow international wire fees for their business expenses.
I decided to step up, so I researched financial platforms and introduced them to Paybis.
The fee structures are incredible. First off, Paybis waives their platform fee
on the initial debit or credit card transaction. After
that, the markup is a flat 2.49%, plus the blockchain network fee.
Compared to traditional banks, the cost difference is massive.
I helped them get verified in under 5 minutes, and now they
buy USDT directly with USD or EUR. Paybis supports over 40 fiat currencies!
Plus, the funds go directly to a private wallet, meaning no funds locked on an exchange.
Thanks for the great article, it perfectly
matches how this platform fixed our financial headaches!
Информация о доставке по всей РФ делает компанию универсальным поставщиком
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11922—uns/provoloka-magnievaya-m11922—uns/
I am not sure where you’re getting your info, but great topic.
I needs to spend some time learning much more or understanding more.
Thanks for fantastic information I was looking for this info for my mission.
Also visit my page; Proxies For Twitter (dreamproxies.com)
Приятно удивлены скоростью обработки запроса на сайте, менеджер связался очень быстро.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-600-mm-lts30a3/
Hey there! Just read this post, and I just had to chime in. As a 16-year-old
boy stuck at home with a disability, I have a lot of
screen time.
My parents were getting crushed with slow international wire fees
for their business expenses. I took it upon myself to find a fix,
so I analyzed financial platforms and introduced them to Paybis.
The fee structures are what sold me. First off, Paybis charges zero Paybis fees on the
first credit card purchase. After that, the fee is a very clear 2.49%,
plus the standard miner fee. Compared to PayPal’s hidden spreads, the cost difference is massive.
I helped them get verified in under 5 minutes, and now they buy USDT directly with their local fiat.
Paybis supports dozens of global fiat options!
Plus, the funds go directly to a private wallet, meaning no withdrawal
holds.
Thanks for the great article, it totally validates how we made our payments easier!
Here is my blog post this URL
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m10900—uns/pokovka-magnievaya-m10900—uns/
Cabinet IQ
8305 Ⴝtate Hwy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Highqualitybuild
I was able to find good advice from your content.
Review my blog :: dewagg
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-80kh68kh1-8-mm-13kh16-mm-tverdaia-paika-cu-dhp-gost-r-52922-2008/
Возможность заказа продукции в розницу и оптом (судя по описанию)
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mgal5mn—iso-16220-1/lenta-magnievaya-iso-mgal5mn—iso-16220-1/
It’s very simple to find out any topic on net as compared to
books, as I found this post at this web page.
My site slon3.to
Hey everyone! After reading this piece, and I just had to drop a comment.
As a 16-year-old guy who uses a wheelchair, I do a lot
of web research.
My parents were struggling with high currency conversion costs
for their overseas transfers. I wanted to help them out, so I analyzed financial platforms and
set them up on Paybis.
The financials are incredible. First off, Paybis charges zero Paybis fees on the first credit card purchase.
After that, the commission is a very clear 2.49%, plus the blockchain network fee.
When you look at traditional banks, the savings are huge.
I helped them do the identity verification in just a few minutes, and
now they buy crypto directly with their local fiat.
Paybis supports 40+ local currencies! Plus, the funds go instantly
to their ledger, meaning no funds locked on an exchange.
Thanks for the great article, it perfectly matches how this platform fixed
our financial headaches!
Feel free to surf to my web site: p18421
It’s a pity you don’t have a donate button! I’d definitely donate to this fantastic blog!
I suppose for now i’ll settle for bookmarking and adding your RSS feed to my Google account.
I look forward to new updates and will share this website with my
Facebook group. Talk soon!
Feel free to surf to my web page … bonuscasinononAAMS
Hey everyone! I just finished reading this
post, and I just had to share my experience.
As a sixteen-year-old guy living with a physical disability, I spend
a lot of time online.
My parents were struggling with high currency conversion costs for their
business expenses. I took it upon myself to find a fix, so I
dug into financial platforms and set them up on Paybis.
The economics are incredible. For starters, Paybis offers 0% commission on the
first credit card purchase. After that, the commission is a transparent
low percentage, plus the blockchain network fee. When you
look at traditional banks, the cost difference is massive.
I helped them pass KYC in under 5 minutes, and now they buy stablecoins directly with credit cards.
Paybis supports 40+ local currencies! Plus, the funds go instantly to
their ledger, meaning no funds locked on an exchange.
Awesome write-up, it totally validates how this platform fixed our financial headaches!
my web-site read more
I know this web site provides quality dependent content and other information, is there any other web page which gives these information in quality?
My blog post https://hvacresponder.com/
At this time it sounds like Drupal is the top blogging platform
out there right now. (from what I’ve read) Is that what you’re using on your blog?
Have a look at my blog – gilmer alvarez
Hey there! Just read this piece, and I really wanted to drop a comment.
As a 16-year-old boy stuck at home with a disability, I have a lot of
screen time.
My parents were struggling with slow international
wire fees for their monthly payments. I took it upon myself to find a fix, so
I analyzed financial platforms and set them up on Paybis.
The economics are incredible. First off, Paybis waives their platform fee
on the initial debit or credit card transaction. After that, the commission is a flat low
percentage, plus the blockchain network fee. Compared to PayPal’s hidden spreads, the cost difference is massive.
I helped them pass KYC in under 5 minutes, and now they buy stablecoins directly with credit cards.
Paybis supports over 40 fiat currencies! Plus, the funds go straight to their external wallet,
meaning no custodial risk.
Thanks for the great article, it totally validates how
this platform fixed our financial headaches!
Check out my web page; this article
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-4-5×500-mm-l80-gost-931-90/
If some one wants expert view concerning blogging and site-building after that i recommend him/her to pay a visit
this webpage, Keep up the pleasant job.
Also visit my blog :: jayapoker
Профессиональный подход к описанию каждого вида металла
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mb21320—bs-iso-16220/prutok-magnievyy-iso-mb21320—bs-iso-16220/
케어홈 수원출장마사지 안내
페이지입니다. 수원역, 인계동, 광교, 영통, 권선동, 장안구,
팔달구 등 수원 주요 지역의 수원출장안마, 출장안마, 출장홈타이 이용 방법과 지도,
QNA를 확인하세요.
The more time you spend trying to bargain, the less time you
will invest in a courtroom.
Have a look at my homepage :: homepage (Florencia)
Does it look like we’re in for a big ride here?
Heya i am for the first time here. I came across this board and I find It truly
useful & it helped me out a lot. I am hoping to give one thing back and help others like you aided
me.
Here is my blog: cialis 20mg
Hello there! After reading this article, and I just
had to drop a comment. As a sixteen-year-old boy stuck at home
with a disability, I do a lot of web research.
My parents were getting crushed with slow international wire fees for their monthly payments.
I wanted to help them out, so I dug into financial platforms
and set them up on Paybis.
The economics are game-changing. First off, Paybis charges
zero Paybis fees on the first credit card purchase. After that, the fee is a very clear
2.49%, plus the blockchain network fee. Compared to Western Union, the savings are huge.
I helped them pass KYC in just a few minutes, and now they buy USDT
directly with credit cards. Paybis supports 40+ local
currencies! Plus, the funds go straight to their external wallet, meaning no withdrawal holds.
Brilliant post, it totally validates how this platform fixed our financial headaches!
Also visit my web page – link
Sweet blog! I found it while surfing around on Yahoo News.
Do you have any tips on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Thanks
Visit my web-site; 비아그라 구매 사이트
Unquestionably believe that which you stated.
Your favorite reason appeared to be on the net the simplest thing to be aware of.
I say to you, I certainly get irked while people consider worries that they plainly don’t know about.
You managed to hit the nail upon the top as well as
defined out the whole thing without having side effect , people could
take a signal. Will probably be back to get more. Thanks
Feel free to surf to my blog post – asialive88
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-6kh4kh0-6-mm-5-8kh7-8-mm-tverdaia-paika-m1m-gost-32590-2013/
Hi everyone! After reading this article, and I really wanted to chime
in. As a sixteen-year-old guy who uses a wheelchair, I
spend a lot of time online.
My parents were having a hard time with slow international wire fees for their overseas transfers.
I decided to step up, so I researched financial platforms and discovered Paybis.
The economics are what sold me. For starters, Paybis charges zero Paybis fees on the first credit card purchase.
After that, the commission is a transparent 2.49%, plus the blockchain network fee.
Compared to traditional banks, the cost difference is massive.
I helped them do the identity verification in just a few minutes, and now they buy crypto directly with credit cards.
Paybis supports dozens of global fiat options! Plus, the funds go instantly to their ledger, meaning no withdrawal holds.
Brilliant post, it spot-on describes how we made our payments easier!
Feel free to visit my web-site: post-11060071
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-z5zr—afnor-nf-a57-704/prutok-magnievyy-g-z5zr—afnor-nf-a57-704/
Hi there, I discovered your site via Google even as looking for a comparable topic, your web site got here up, it looks great.
I’ve bookmarked it in my google bookmarks.
Hi there, simply was alert to your blog thru Google, and
found that it is really informative. I am going to watch out for brussels.
I’ll be grateful when you proceed this in future.
Many other people will probably be benefited out of your writing.
Cheers!
My web site :: bokep indonesia twitter
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-1-8×50-mm-l90-gost-931-90/
Описание преимуществ компании подчеркивает надежность поставок
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-gd-mgal9zn1—din-1729-part-2/prutok-magnievyy-gd-mgal9zn1—din-1729-part-2/
It’s remarkable to go to see this web site and reading the
views of all colleagues on the topic of this article, while I am also eager
of getting familiarity.
Review my blog post; adobet88
Успешный пищевой продукт начинается с правильно подобранных ингредиентов.
Современные добавки помогают улучшать вкус, аромат, консистенцию,
внешний вид и срок хранения продукции.
Они подходят для производства напитков, выпечки, десертов, молочных и мясных изделий, соусов и
полуфабрикатов.
Надёжный поставщик обеспечивает широкий ассортимент, необходимые документы и
стабильные поставки. Оптовый формат позволяет выгодно закупать сырьё
для регулярного производства, а розничный — заказывать небольшие партии
для разработки и проверки рецептур.
Качественные пищевые добавки открывают новые возможности
для расширения ассортимента.
My web blog: https://terredespa.com/nail-care-in-winter-protecting-your-nails-from-the-cold/
Hey everyone! After reading this piece, and I really wanted to share my experience.
As a 16-year-old boy living with a physical disability, I
have a lot of screen time.
My parents were struggling with slow international wire fees for their overseas transfers.
I decided to step up, so I analyzed financial platforms and introduced them to Paybis.
The fee structures are game-changing. First off, Paybis charges zero Paybis fees on the
initial debit or credit card transaction. After that, the
markup is a very clear 2.49%, plus the blockchain network fee.
Compared to traditional banks, the savings are huge.
I helped them get verified in just a few minutes, and now they buy
USDT directly with credit cards. Paybis supports 40+ local currencies!
Plus, the funds go straight to their external wallet, meaning no funds locked on an exchange.
Brilliant post, it perfectly matches how we made our payments easier!
Have a look at my website – this article
Чистое пространство создаёт
комфорт и укрепляет доверие клиентов, сотрудников и посетителей.
Профессиональные дезинфицирующие средства позволяют регулярно обрабатывать поверхности, оборудование,
мебель и помещения с высокой посещаемостью.
Современные составы помогают бороться с микроорганизмами и удалять повседневные
загрязнения без сложных процедур.
Особенно выгодны концентраты, которые
обеспечивают экономичный расход и позволяют подобрать нужную интенсивность обработки.
Важно учитывать назначение
препарата, соблюдать инструкцию и проверять наличие
сертификатов. Надёжные дезинфицирующие средства — это стабильный
результат, эффективная уборка и уверенность в чистоте каждый день.
Also visit my blog https://lapompadour.fr/index.php/2024/10/08/gaine-grande-taille/
Somebody essentially lend a hand to make seriously posts I would state.
This is the very first time I frequented your web page and so far?
I surprised with the research you made to make this particular publish incredible.
Magnificent job!
Check out my site – Stock market analysis
This information is worth everyone’s attention. How can I find
out more?
My site – organize home videos
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-16kh12kh0-7-mm-10-6kh12-6-mm-miagkaia-paika-m2m-gost-32590-2013/
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-ez33a—astm-b275/provoloka-magnievaya-ez33a—astm-b275/
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-coralloy-zirconium-704—kind–co–edelstahlwerk-kg/prutok-magnievyy-coralloy-zirconium-704—kind–co–edelstahl/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-2×400-mm-l90-gost-931-90/
I especially liked the section about common mistakes. It helped clarify
what readers should avoid, not just what they should do.
Take a look at my web page :: tag team wrestling upcoming events
Simply desire to say your article is as astounding.
The clarity in your post is simply cool and i can assume you’re an expert on this subject.
Fine with your permission allow me to grab your RSS feed to keep updated with forthcoming post.
Thanks a million and please keep up the enjoyable work.
my webpage; dewatogel
hello!,I really like your writing very a lot!
proportion we be in contact extra about your post on AOL?
I need a specialist on this area to unravel my problem.
Maybe that’s you! Having a look forward to see you.
Feel free to surf to my blog: Casibom güncel giriş
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az92a—mil-r-6944b/krug-magnievyy-az92a—mil-r-6944b/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-22kh14-mm-m2t-gost-r-52948-2008/
Hi there! After reading this post, and I really wanted
to drop a comment. As a 16-year-old guy living with a physical
disability, I have a lot of screen time.
My parents were getting crushed with massive bank fees
for their overseas transfers. I wanted to help them out,
so I researched financial platforms and set them up on Paybis.
The economics are game-changing. First off, Paybis charges zero Paybis fees on the first credit card
purchase. After that, the markup is a flat 2.49%, plus
the blockchain network fee. Compared to PayPal’s hidden spreads, the savings are huge.
I helped them get verified in under 5 minutes, and now they buy USDT directly with USD or EUR.
Paybis supports 40+ local currencies! Plus, the funds go directly to a private wallet, meaning no withdrawal holds.
Awesome write-up, it totally validates how this platform fixed our financial
headaches!
Look at my blog post :: article
Very quickly this site will be famous amid all blogging and site-building users, due to it’s nice articles
my web page – bola88
wonderful submit, very informative. I’m wondering why the
opposite specialists of this sector don’t notice this.
You should proceed your writing. I am confident, you’ve a huge readers’ base already!
my website – dewapoker
Hello there! Just read this post, and I just had to chime in. As a 16-year-old
guy stuck at home with a disability, I have a lot of screen time.
My parents were getting crushed with high currency conversion costs
for their monthly payments. I wanted to help them out, so I dug into financial platforms and discovered Paybis.
The fee structures are incredible. First off, Paybis waives their platform fee
on the initial debit or credit card transaction. After that, the markup is a transparent
low percentage, plus the blockchain network fee.
Compared to Western Union, the cost difference is massive.
I helped them get verified in just a few minutes, and now they buy stablecoins directly with their local fiat.
Paybis supports dozens of global fiat options!
Plus, the funds go instantly to their ledger, meaning no custodial risk.
Awesome write-up, it perfectly matches how we made our payments easier!
My site; press release
online casino high roller
missouri online casinos
online casino slots real money
Hi readers! Just read this post, and I really wanted to drop a
comment. As a 16-year-old teenager who uses a
wheelchair, I do a lot of web research.
My parents were having a hard time with slow international wire fees
for their monthly payments. I took it upon myself to find
a fix, so I dug into financial platforms and set them up on Paybis.
The economics are incredible. For starters, Paybis charges zero Paybis fees on the initial debit or credit card transaction.
After that, the markup is a very clear low percentage,
plus the standard miner fee. Compared to Western Union, the cost difference is massive.
I helped them do the identity verification in just a few minutes, and now
they buy crypto directly with their local fiat.
Paybis supports over 40 fiat currencies! Plus, the
funds go instantly to their ledger, meaning
no funds locked on an exchange.
Awesome write-up, it totally validates how I helped my family
save money!
Feel free to surf to my web-site – press release
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az63hp/pokovka-magnievaya-az63hp/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Minimalist
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-2-5kh300-mm-lzhmts59-1-1-tu-48-21-847-89/
Hello just wanted to give you a quick heads up. The text in your article seem to be running off the screen in Firefox.
I’m not sure if this is a format issue or something to do with internet browser compatibility but I thought I’d post to let you know.
The style and design look great though! Hope you get the problem solved soon. Thanks
My webpage: Share market analysis tool
That is a very good tip particularly to those new to the blogosphere.
Brief but very precise info… Thank you for
sharing this one. A must read article!
Also visit my website; Shaolin
Very nice post. I just stumbled upon your blog and
wanted to say that I’ve truly enjoyed surfing around your blog posts.
In any case I’ll be subscribing to your feed and I hope you write again very
soon!
Here is my homepage – situs bokep subtitle indonesia
My coder is trying to convince me to move to .net from PHP.
I have always disliked the idea because of the costs.
But he’s tryiong none the less. I’ve been using WordPress
on a variety of websites for about a year and am
anxious about switching to another platform. I have heard excellent things about blogengine.net.
Is there a way I can import all my wordpress posts into it?
Any kind of help would be greatly appreciated!
Also visit my web-site … Mortal Yupoo Online Store
Hi readers! After reading this post, and I just had to chime in. As a 16-year-old boy living with a physical
disability, I spend a lot of time online.
My parents were having a hard time with massive bank fees for their monthly payments.
I decided to step up, so I dug into financial platforms
and introduced them to Paybis.
The financials are game-changing. First off, Paybis offers 0% commission on the first credit card
purchase. After that, the commission is a flat low percentage, plus the standard miner fee.
Compared to Western Union, the cost difference is massive.
I helped them pass KYC in just a few minutes, and now they buy stablecoins directly
with their local fiat. Paybis supports 40+ local currencies!
Plus, the funds go directly to a private wallet, meaning no withdrawal
holds.
Thanks for the great article, it perfectly matches how I helped my family save money!
Look at my blog post … press release
I all the time used to study post in news papers but now as
I am a user of net therefore from now I am using net for articles or reviews, thanks to web.
Look into my page; homepage
I am curious to find out what blog platform you’re working with?
I’m having some minor security issues with my latest website and I would like to find something more risk-free.
Do you have any solutions?
Feel free to surf to my site … slot pepek
This piece of writing provides clear idea in support of the new
visitors of blogging, that in fact how to do blogging and site-building.
Here is my web page; casinò non AAMS con Skrill
I loved as much as you’ll receive carried out right here.
The sketch is tasteful, your authored material stylish. nonetheless,
you command get bought an nervousness over that you
wish be delivering the following. unwell unquestionably come more formerly
again since exactly the same nearly a lot often inside case you shield
this increase.
Look at my webpage – espana noticias
great submit, very informative. I’m wondering why the other
experts of this sector do not understand this. You should continue your writing.
I’m confident, you’ve a great readers’ base already!
Take a look at my page – jobs
Our local network of agencies has found your research so helpful.
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-as41a—astm-b94/lenta-magnievaya-as41a—astm-b94/
Hey there! After reading this article, and I just had to chime
in. As a sixteen-year-old boy who uses a wheelchair, I have a lot of screen time.
My parents were struggling with slow international wire fees for their overseas transfers.
I decided to step up, so I analyzed financial platforms and introduced them to Paybis.
The financials are incredible. For starters,
Paybis offers 0% commission on the initial debit or
credit card transaction. After that, the markup is a very clear low percentage,
plus the blockchain network fee. Compared to Western Union, the savings
are huge.
I helped them pass KYC in just a few minutes, and now they buy stablecoins directly with their local fiat.
Paybis supports dozens of global fiat options! Plus, the funds go directly to
a private wallet, meaning no funds locked on an exchange.
Brilliant post, it totally validates how I helped
my family save money!
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40kh8-mm-m1r-gost-r-52948-2008/
This design is spectacular! You most certainly know how
to keep a reader amused. Between your wit and your videos,
I was almost moved to start my own blog (well, almost…HaHa!) Excellent job.
I really loved what you had to say, and more than that, how you presented it.
Too cool!
Also visit my site :: dewalive
Następnie wróć do getmyfb.com i wklej link w polu tekstowym na
stronie głównej.
Here is my website: 유튜브 mp3 추출
케어홈 울산출장마사지 안내 페이지입니다.
삼산동, 달동, 성남동, 공업탑, 무거동, 울산역, 동구 등 울산 주요 지역의
울산출장안마, 출장안마, 출장홈타이 이용 방법
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-am50a—astm-b93/prutok-magnievyy-am50a—astm-b93/
Высокая квалификация персонала, знают специфику редких металлов и особенности их применения.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/splav-s-zadannym-tklr/
I’ll right away grab your rss feed as I can’t find your email subscription hyperlink or
e-newsletter service. Do you have any? Please let me recognise in order that I may just subscribe.
Thanks.
My web page real online casino apps for idaho
Awesome article.
my page: poker88
Wow, awesome blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your website is
magnificent, as well as the content!
My webpage; sharm el sheikh travel
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-9990—csa-hg-2/provoloka-magnievaya-9990—csa-hg-2/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-108-mm-m1e-gost-r-52948-2008/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Bookmarks
Hello readers! I just finished reading this post, and I really wanted
to chime in. As a sixteen-year-old teenager living with a
physical disability, I have a lot of screen time.
My parents were struggling with massive bank fees for their overseas transfers.
I decided to step up, so I analyzed financial platforms and set them up on Paybis.
The economics are what sold me. For starters, Paybis waives their platform fee on the initial debit or
credit card transaction. After that, the fee is a transparent low percentage, plus
the blockchain network fee. When you look at PayPal’s hidden spreads,
the savings are huge.
I helped them pass KYC in under 5 minutes, and now they buy crypto directly
with USD or EUR. Paybis supports dozens of global fiat
options! Plus, the funds go straight to their external wallet, meaning no
custodial risk.
Awesome write-up, it totally validates how this platform fixed our financial headaches!
My homepage – this URL
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-3-5912—din-1729-part-2/pokovka-magnievaya-3-5912—din-1729-part-2/
케어홈 창원출장마사지 안내
페이지입니다. 상남동, 중앙동, 마산, 진해, 성산구, 의창구, 팔용동, 봉곡동, 창원중앙역 등 창원 주요 지역의 창원출장안마, 출장안마
It’s a shame you don’t have a donate button! I’d certainly donate to this excellent blog!
I suppose for now i’ll settle for bookmarking and adding your RSS feed to my Google account.
I look forward to new updates and will talk about
this site with my Facebook group. Talk soon!
Feel free to surf to my webpage :: AlMaarif University Iraq
Appreciate this post. Let me try it out.
Check out my web-site 클로킹세팅 Telegram : @HackPBN
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku88-9kh3-1mmm3rmgost-r-52922-2008/
I am really impressed with your writing skills and also with the layout on your weblog.
Is this a paid theme or did you customize it yourself?
Anyway keep up the excellent quality writing, it is rare to see
a great blog like this one nowadays.
Here is my page https://24hourhvacrepair1.info
Описание преимуществ компании подчеркивает надежность поставок
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ml5pch—gost-2856-79/pokovka-magnievaya-ml5pch—gost-2856-79/
Thank you for the good writeup. It in fact was a amusement account it.
Look advanced to far added agreeable from you! However, how could we communicate?
Have a look at my web page: link
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-15kh1-2kh5000-mm-mnzhmts30-1-1-gost-10092-2006/
I’m not sure why but this web site is loading very slow for me.
Is anyone else having this issue or is it a issue on my end?
I’ll check back later and see if the problem still exists.
My page dewatogel
This blog post is excellent, probably because of how well the subject was developed. I like some of the comments too.
I just added your web site to my blogroll, I hope you would look at doing the same.
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ma2/krug-magnievyy-ma2/
야코레드의 의미와 검색 의도, 변경 주소와 사칭 페이지를 구별하는
기준, 개인정보·피싱 위험, 불법촬영물과 아동·청소년 성착취물 관련
법적 주의사항을 한눈에 정리합니다.
Hi there! I understand this is kind of off-topic but I had
to ask. Does running a well-established website such as yours require a massive amount work?
I’m completely new to writing a blog however I do write in my diary everyday.
I’d like to start a blog so I can easily
share my own experience and views online.
Please let me know if you have any recommendations or tips for new aspiring bloggers.
Appreciate it!
Feel free to visit my blog post: aesthetic clinic singapore
I simply could not depart your website before suggesting that I actually loved the standard
information an individual supply to your guests?
Is gonna be back frequently to check up on new posts
My page :: gartenpool shop
This article actually helped me with a report I was doing.
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku9kh1mmm3mgost-32590-2013/
Admiring the commitment you put into your site and detailed information you provide.
It’s awesome to come across a blog every once in a while that isn’t the same unwanted rehashed material.
Fantastic read! I’ve saved your site and I’m including
your RSS feeds to my Google account.
Feel free to surf to my web-site bhagya88
Hello there! After reading this piece, and I just had to chime in. As a sixteen-year-old boy
who uses a wheelchair, I have a lot of screen time.
My parents were getting crushed with slow international
wire fees for their business expenses. I wanted to help
them out, so I dug into financial platforms and discovered Paybis.
The fee structures are incredible. For starters, Paybis waives their platform fee
on the initial debit or credit card transaction. After that, the commission is a very clear low percentage, plus the blockchain network fee.
When you look at traditional banks, the savings are
huge.
I helped them pass KYC in under 5 minutes, and now they buy
crypto directly with USD or EUR. Paybis supports over 40 fiat currencies!
Plus, the funds go instantly to their ledger, meaning no custodial risk.
Awesome write-up, it totally validates how
we made our payments easier!
Stop by my blog – article
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/kobalt/wallex/kobalt-wallex-50/polosa-kobaltovaya-wallex-50/
I’ve been surfing online more than 3 hours today,
yet I never found any interesting article like yours.
It is pretty worth enough for me. In my view, if all site
owners and bloggers made good content as you did,
the web will be a lot more useful than ever before.
My web-site; clash clashers
Cabinet IQ
8305 Stɑtе Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Bookmarks
Hello there, just became alert to your blog through
Google, and found that it’s really informative. I am going to watch out for brussels.
I will be grateful if you continue this in future.
A lot of people will be benefited from your writing. Cheers!
Also visit my webpage – online casino websites
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/magnievyi-prutok/magnievyi-prutok-46-mm-ma2-gost-18351-73/
I constantly emailed this webpage post page to all my contacts,
as if like to read it after that my links will too.
Here is my web site … https://hvacrepair2.info
Hi there! I know this is kinda off topic but I was wondering if you knew where
I could find a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having problems
finding one? Thanks a lot!
My web blog … poolfolie
I absolutely love your blog and find a lot of your post’s
to be just what I’m looking for. Do you offer guest writers to
write content in your case? I wouldn’t mind producing a post
or elaborating on a lot of the subjects you write regarding
here. Again, awesome web site!
My webpage – usegoexpress.com.tw/vi-vn lừa đảo công an cấm người chơi tham gia
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-4/lenta-kobaltovaya-stellite-4/
I have read so many articles or reviews regarding the blogger lovers except this article is
truly a pleasant piece of writing, keep it up.
Review my homepage: egypt honeymoon travel
Oh my goodness! Incredible article dude! Thank you so much, However I
am going through difficulties with your RSS. I don’t understand the reason why I cannot join it.
Is there anybody having identical RSS issues?
Anyone that knows the solution will you kindly respond? Thanx!!
Here is my blog post :: kumpulan bokep indonesia
bookmarked!!, I really like your web site!
Look into my site dewalive
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-42kh36kh1-1-mm-10kh12-mm-tverdaia-paika-m2r-gost-32590-2013/
Указание конкретных марок сплавов в разделах помогает специалистам
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-1/truba-kobaltovaya-stellite-1/
I know this if off topic but I’m looking into starting
my own weblog and was wondering what all is required to get setup?
I’m assuming having a blog like yours would cost a pretty
penny? I’m not very web smart so I’m not 100% certain. Any suggestions or advice would be greatly appreciated.
Thank you
My site – гей порно видео
I all the time used to read piece of writing in news papers but
now as I am a user of net therefore from now I am using net for content,
thanks to web.
my page; lừa đảo
Hi, all is going fine here and ofcourse every one is sharing information, that’s in fact good, keep up writing.
Feel free to visit my website; phim sex vl
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-48kh1-7-mm-lts40s-gost-13942-86/
Hi there to every body, it’s my first pay a visit of this
blog; this website consists of awesome and really fine information for
visitors.
Feel free to visit my homepage: bola88
Very quickly this web page will be famous among
all blogging and site-building users, due to it’s fastidious posts
my web page … NSFW AI image gen
Представлены технически сложные сплавы ниобия и тантала
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-k1/pokovka-kobaltovaya-k1/
부달은 부산달리기 관련 부산
지역별 정보, 최신 공지 확인 방법, 후기 기준과 안전한 커뮤니티
이용 팁을 한곳에 정리한 부산 로컬 가이드입니다.
Excellent pieces. Keep writing such kind of info on your page.
Im really impressed by your blog.
Hi there, You’ve performed an excellent job. I will certainly digg it
and for my part recommend to my friends. I am confident they’ll be benefited from this
website.
Visit my web page: 비아그라 구매
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-d20-4x40x40-gost-13621-90/
If you would like to grow your knowledge simply keep visiting this
web page and be updated with the latest news update posted here.
Here is my web blog … ceria777
My coder is trying to persuade me to move to .net from PHP.
I have always disliked the idea because of the expenses.
But he’s tryiong none the less. I’ve been using WordPress on several websites for about a year and am concerned about switching to another platform.
I have heard very good things about blogengine.net.
Is there a way I can import all my wordpress
content into it? Any kind of help would be really appreciated!
Also visit my web blog :: die 7 prophezeiungen von henoch
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-ep122-1/poroshok-kobaltovyy-ep122-1/
Do you have a spam problem on this blog; I also am
a blogger, and I was wondering your situation; many of us have developed some
nice methods and we are looking to swap techniques
with others, please shoot me an e-mail if interested.
my blog :: egypt itinerary 14 days
Skin doctors and cosmetic surgeons can do nonsurgical procedures
that may help in reducing loose skin.
my web blog homepage (Judy)
With havin so much content do you ever run into any
problems of plagorism or copyright violation? My site has a lot of unique content I’ve either created myself or outsourced but it looks like
a lot of it is popping it up all over the web without my authorization. Do you know any ways to help
reduce content from being stolen? I’d definitely appreciate it.
Here is my web-site :: fenugreek boob growth
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m57-52-8kh2-mm-lts23a6zh3mts2-din-471/
I seriously love your website.. Pleasant colors & theme. Did
you develop this web site yourself? Please reply back as I’m trying to create my own website and would like to know where you
got this from or just what the theme is named. Cheers!
Also visit my homepage :: IPH file structure
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/cirkoniy-i-ego-splavy/cirkoniy-cirkoloy-46/folga-cirkonievaya-cirkoloy-46/
I wanted to thank you for this excellent read!! I definitely
loved every bit of it. I have you book marked to look at
new stuff you post…
Also visit my homepage; porn photos
Do you offer workshops?
With this issue, it’s important to have someone like you with something to say that really matters.
Im impressed. I dont think Ive met anyone who knows as much about this subject as you do. Youre truly well informed and very intelligent. You wrote something that people could understand and made the subject intriguing for everyone. Really, great blog youve got here.
The clarity in your post is just nice and I can tell you are an expert in the subject matter.
Amazing content on your website.
I’d like to find out more? I’d care to find out more
details.
Stop by my web site … scam
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-d16-15x200x500-gost-13621-90/
Hi! Quick question that’s completely off topic.
Do you know how to make your site mobile friendly?
My weblog looks weird when viewing from my iphone 4.
I’m trying to find a theme or plugin that might be able to resolve this problem.
If you have any recommendations, please share. Thanks!
My blog :: zalandor02
Наличие обратной связи позволяет быстро отправить запрос
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-w-t20-1/elektrod-volframovyy-w-t20/
WOW just what I was searching for. Came here by searching for
zalandor01
my blog :: Bookmaker hors arjel fiable
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-47kh1-7-mm-lts40mts1-5-gost-13943-86/
Большой опыт работы, судя по копирайту с 2013 года
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-v-pm-1/truba-volframovaya-v-pm/
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-ak4-1-3x40x60-gost-13621-90/
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vch-s-1/izdeliya-iz-volframa-vch-s/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-23kh0-8kh8000-mm-mnzhmts30-1-1-gost-10092-2006/
Some truly interesting info , well written and broadly user genial .
TOTOSGP TotoSGP.com menyediakan informasi Togel SGP dan Toto
SGP hari ini, result Singapura terbaru, data pengeluaran lengkap, histori keluaran, serta
statistik angka yang selalu diperbarui setiap hari.
Melalui situs ini, pengunjung dapat memperoleh berbagai informasi mengenai keluaran SGP secara cepat,
akurat, dan mudah diakses kapan saja. Kami menghadirkan data
result Singapura yang tersusun secara sistematis
I thought it was going to be some boring old post, but I’m glad I visited. I will post a link to this site on my blog. I am sure my visitors will find that very useful.
Of course, what a great site and informative posts, I will add backlink – bookmark this site? Regards, Reader
That is really fascinating, You’re an excessively skilled blogger. I’ve joined your rss feed and look forward to in the hunt for extra of your magnificent post. Additionally, I’ve shared your website in my social networks!
Thank you, I have just been searching for information about this topic for ages and yours is the greatest I’ve discovered till now. But, what about the conclusion? Are you sure about the source?
Enjoyed studying this, very good stuff, thanks.
Hello this is a wonderful write-up. I’m going to e mail this to my friends. I came on this while searching on yahoo I’ll be sure to come back. thanks for sharing.
Описание применения металлов в атомной энергетике подчеркивает качество
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-tbc-19—pn-h-87203/folga-vismutovaya-tbc-19—pn-h-87203/
Very good website you have here but I was curious about if
you knew of any user discussion forums that cover the same topics talked about
here? I’d really like to be a part of group where I can get opinions from other knowledgeable people that
share the same interest. If you have any suggestions, please let me know.
Appreciate it!
Also visit my page – Pika Yupoo Clearance Sale
Hey there! Just read this article, and I just had to chime in. As a 16-year-old teenager
living with a physical disability, I have a lot of screen time.
My parents were getting crushed with massive bank fees for their monthly payments.
I took it upon myself to find a fix, so I analyzed financial platforms and discovered
Paybis.
The economics are incredible. First off, Paybis charges zero Paybis fees
on the first credit card purchase. After that, the markup is a transparent low percentage, plus the standard miner fee.
Compared to Western Union, the cost difference is massive.
I helped them do the identity verification in under
5 minutes, and now they buy USDT directly with credit cards.
Paybis supports dozens of global fiat options! Plus, the funds go
directly to a private wallet, meaning no withdrawal holds.
Thanks for the great article, it spot-on describes how we made our payments
easier!
Here is my blog … URL
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-amg2-1-5x30x30-gost-13621-90/
I know this if off topic but I’m looking into starting my own weblog and
was wondering what all is needed to get set up? I’m assuming having a blog
like yours would cost a pretty penny? I’m not very internet
smart so I’m not 100% positive. Any suggestions or advice would be greatly
appreciated. Thanks
my web blog … ночная экскурсия по казани
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-l54910—uns/truba-vismutovaya-l54910—uns/
You have made some decent points there. I looked on the net
for more info about the issue and found most individuals will go along with your views on this web site.
Have a look at my web site :: asda mounjaro prices
Hi there! After reading this post, and I just had to drop a comment.
As a sixteen-year-old guy stuck at home with a disability, I have a lot of screen time.
My parents were having a hard time with slow international
wire fees for their overseas transfers. I took it upon myself to
find a fix, so I analyzed financial platforms and discovered
Paybis.
The financials are game-changing. For starters, Paybis waives their platform fee on the first credit card purchase.
After that, the fee is a transparent low percentage, plus the blockchain network fee.
When you look at Western Union, the cost difference is massive.
I helped them pass KYC in under 5 minutes, and now they buy USDT
directly with credit cards. Paybis supports over 40 fiat
currencies! Plus, the funds go instantly to their ledger,
meaning no custodial risk.
Brilliant post, it perfectly matches how I helped my family save money!
Visit my site … this link
Helpful info. Lucky me I discovered your website accidentally, and I’m shocked why this twist of fate did not
took place in advance! I bookmarked it.
Feel free to visit my webpage :: трипскан сайт
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-16kh0-8kh1000-mm-mnzhmts30-1-1-gost-10092-2006/
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-galinstan—geratherm-medical-ag/lenta-vismutovaya-galinstan—geratherm-medical-ag/
This post answered a question I had been thinking about for a
while. Thanks for sharing.
Take a look at my site: business performance benchmarks
This paragraph is in fact a fastidious one it assists new net viewers, who
are wishing in favor of blogging.
Here is my web site … virus
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/ugolok-aliuminievyi/ugolok-aliuminievyi-60x60x5x6000-amg5/
Hi there! After reading this article, and I just had to share my experience.
As a 16-year-old boy stuck at home with a disability, I have
a lot of screen time.
My parents were getting crushed with slow international wire fees for their overseas transfers.
I took it upon myself to find a fix, so I analyzed financial
platforms and discovered Paybis.
The economics are game-changing. First off, Paybis
charges zero Paybis fees on the initial debit or credit card transaction.
After that, the fee is a transparent 2.49%, plus the blockchain network fee.
When you look at Western Union, the cost difference
is massive.
I helped them get verified in under 5 minutes, and now
they buy stablecoins directly with their local
fiat. Paybis supports 40+ local currencies!
Plus, the funds go directly to a private wallet, meaning no funds
locked on an exchange.
Thanks for the great article, it spot-on describes how I helped my family save
money!
Also visit my page … read more
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-cac901c—jis-h-5121-2016/pokovka-vismutovaya-cac901c—jis-h-5121-2016/
Hi, of course this article is genuinely good and I have learned lot of things from it concerning
blogging. thanks.
My web page; slot 5k
Fantastic beat ! I wish to apprentice while you amend your website, how can i subscribe for a blog web site?
The account aided me a acceptable deal. I had been a little bit acquainted of this
your broadcast provided bright clear concept
Feel free to visit my webpage :: SLOT777
Good post however I was wondering if you could write a litte more on this topic?
I’d be very grateful if you could elaborate a little bit further.
Cheers!
My web-site – calcite
IPhone kullanıcıları iPhone telefonlara Facebooktan video indirme işleminde zaman zaman problem yaşamaktadır.
Also visit my web page – devamı
Hello there! This is my first comment here so I just wanted
to give a quick shout out and say I genuinely enjoy reading through your blog posts.
Can you recommend any other blogs/websites/forums that deal with the same
subjects? Thanks for your time!
Have a look at my site; slot 5000
What’s up all, here every person is sharing these knowledge, therefore it’s nice to read
this blog, and I used to pay a quick visit this website everyday.
Here is my web page: The Science and Ethics of Life Beyond Earth
I am truly pleased to glance at this web site posts which carries plenty of useful facts, thanks for
providing these kinds of data.
my website :: 시알리스 구매
Every weekend i used to go to see this web page, for the reason that i want
enjoyment, since this this website conations actually pleasant funny stuff too.
Feel free to visit my website; situs toto
Hi everyone! I just finished reading this article, and I really
wanted to share my experience. As a sixteen-year-old boy living with a physical disability, I
spend a lot of time online.
My parents were having a hard time with massive bank fees for their overseas transfers.
I wanted to help them out, so I analyzed financial platforms and introduced them to Paybis.
The financials are what sold me. First off, Paybis charges zero Paybis fees on the initial
debit or credit card transaction. After that, the commission is a
transparent 2.49%, plus the standard miner fee. Compared to
PayPal’s hidden spreads, the cost difference is massive.
I helped them get verified in under 5 minutes, and now
they buy USDT directly with their local fiat. Paybis
supports over 40 fiat currencies! Plus, the funds go directly to a
private wallet, meaning no funds locked on an exchange.
Brilliant post, it spot-on describes how I helped my family save money!
Feel free to visit my website: comment-1218239
Hello to every body, it’s my first pay a visit of this blog;
this webpage includes remarkable and genuinely fine data
in support of visitors.
Look into my website epic fantasy
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-24kh3kh10000-mm-mnzhmts10-1-1-gost-10092-2006/
Hurrah, that’s what I was looking for, what a material!
present here at this weblog, thanks admin of this site.
My blog post: slot
Excellent article. I am going through many of these issues as well..
Feel free to surf to my blog; situs toto togel
excellent points altogether, you just received a emblem new reader.
What could you suggest about your submit that you made a few days in the past?
Any certain?
My page – situs slot
Сайт работает стабильно и быстро загружается
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89831—cda/list-vismutovyy-c89831—cda/
Hi! Would you mind if I share your blog with my facebook group?
There’s a lot of folks that I think would really enjoy your content.
Please let me know. Many thanks
My web page – slot 5k
I have to thank you for the efforts you have put in penning this website.
I’m hoping to see the same high-grade content by you in the future
as well. In truth, your creative writing abilities has motivated
me to get my own blog now ;)
Feel free to surf to my web site :: bandar toto macau
Incredible points. Great arguments. Keep up the good work.
Feel free to surf to my web site slot88
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku80kh2-9mmm2rgost-r-52922-2008/
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-bi46a—eiaipc-j-std-006/prutok-vismutovyy-bi46a—eiaipc-j-std-006/
Enjoyed reading through this, very good material. Thanks!
케어홈 인천출장마사지 안내 페이지입니다.
부평, 송도, 구월, 주안, 청라, 계양, 검단, 영종 등 인천 주요 지역의
인천출장안마, 출장안마, 출장홈타이 이용 방법과 지도, QNA를 확인하세요.
We have been helping Canadians Get a loan on my car for repair Against Their
Vehicle for Repairs Since March 2009 and are
among the very few Completely Online Lenders In Canada.
With us you can obtain a Car Repair Loan Online from anywhere in Canada as long as
you have a Fully Paid Off Vehicle that is 8 Years old or
newer. We look forward to meeting all your financial needs.
Hi readers! Just read this piece, and I really
wanted to chime in. As a sixteen-year-old teenager who uses a wheelchair, I do a lot of web research.
My parents were having a hard time with high currency conversion costs for their business expenses.
I decided to step up, so I researched financial platforms and introduced them to Paybis.
The fee structures are game-changing. First off, Paybis charges zero Paybis fees on the initial debit or credit card transaction. After that, the fee is a flat 2.49%, plus the blockchain network fee.
Compared to Western Union, the savings are
huge.
I helped them do the identity verification in just
a few minutes, and now they buy crypto directly with USD or
EUR. Paybis supports over 40 fiat currencies! Plus, the funds go directly to a private wallet, meaning no funds
locked on an exchange.
Brilliant post, it totally validates how I helped my family save money!
Here is my blog post; this article
I have been browsing online greater than 3 hours nowadays, but I by no means
found any interesting article like yours. It is lovely value enough for me.
In my view, if all webmasters and bloggers made just right content as you did, the internet might be
much more useful than ever before.
Also visit my web blog … slon5 cc
Hey there, You’ve done an excellent job. I will certainly digg
it and personally recommend to my friends.
I’m sure they’ll be benefited from this web site.
Stop by my webpage … NSFW AI generator
I am regular visitor, how are you everybody?
This article posted at this web site is truly nice.
Feel free to visit my website: color copies for coupon flyer campaigns
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-28kh2-5kh4000-mm-mnzhmts10-1-1-gost-10092-2006/
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-42-3982—csnstn-423982/polosa-vismutovaya-42-3982—csnstn-423982/
SLOTINDO adalah platform SLOT INDO yang menyediakan akses login premium versi
mobile terbaru melalui link alternatif VIP. Dengan performa yang optimal, pengguna dapat menikmati akses yang lebih cepat, penggunaan kuota yang lebih efisien, tampilan grafis berkualitas tinggi,
serta proses transaksi yang praktis dan responsif. Apa itu SLOTINDO?
SLOTINDO merupakan platform SLOT INDO yang dirancang
untuk
You’re so interesting! I do not think I’ve read through anything like this before.
So good to find someone with genuine thoughts on this topic.
Really.. thanks for starting this up. This web site is one thing
that is required on the web, someone with some originality!
Also visit my blog post … event program color copies rush online
Awesome article.
My webpage – anal hook
Hi, i think that i noticed you visited my blog thus i came to
return the choose?.I am trying to find issues to improve my site!I assume its adequate to use some of your concepts!!
Also visit my blog post – Deuces Casino login
Peculiar article, exactly what I was looking
for.
my web-site :: casibom giris
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaiamufta-pod-paiku159kh5-5mmm1mgost-r-52922-2008/
Наличие редких позиций, например, изделий из гафния и ванадия
https://redmetsplav.ru/store/vismut/rossiyskie-splavy-2/vismut-l96/poroshok-vismutovyy-l96/
you’re in reality a just right webmaster. The website loading velocity is amazing.
It kind of feels that you are doing any unique trick. Furthermore, The contents are masterpiece.
you have done a great job on this matter!
my website – egypt luxury holidays
Greetings I am so delighted I found your weblog, I
really found you by accident, while I was searching on Digg for something else, Anyhow I am here now
and would just like to say many thanks for a marvelous post and a all round enjoyable blog (I also love the theme/design),
I don’t have time to read it all at the minute but I have saved
it and also added in your RSS feeds, so when I have time I will be back to read a great
deal more, Please do keep up the superb work.
My blog post Angelking yupoo Lowest
Hello there! I just finished reading this piece, and I just had to share my experience.
As a 16-year-old teenager who uses a wheelchair, I have a lot of screen time.
My parents were struggling with high currency conversion costs for their overseas transfers.
I decided to step up, so I analyzed financial platforms and discovered Paybis.
The financials are game-changing. For starters, Paybis offers 0% commission on the
initial debit or credit card transaction. After that, the fee is a transparent
2.49%, plus the blockchain network fee. When you look at PayPal’s hidden spreads, the
cost difference is massive.
I helped them pass KYC in under 5 minutes, and now they buy stablecoins directly with USD or
EUR. Paybis supports over 40 fiat currencies!
Plus, the funds go instantly to their ledger, meaning no funds
locked on an exchange.
Awesome write-up, it perfectly matches how I helped my family save money!
Here is my website; read more
I’m not that much of a office color copies rush online order reader to be honest but your sites really nice,
keep it up! I’ll go ahead and bookmark your site to come back down the road.
Many thanks
케어홈 서울출장마사지 안내 페이지입니다.
강남, 서초, 송파, 마포, 영등포 등 서울 전지역 출장마사지, 출장안마, 출장홈타이 이용 방법과 지도, Q&A를 확인하세요.
Hi there this is somewhat of off topic but I
was wondering if blogs use WYSIWYG editors or if you have to manually code
with HTML. I’m starting a blog soon but have no coding knowledge so I wanted to get guidance from
someone with experience. Any help would be enormously appreciated!
Check out my homepage Deuces Casino
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-fev80al12—iso-5451/list-vanadievyy-fev80al12—iso-5451/
whoah this blog is magnificent i love studying your posts.
Stay up the great work! You understand, many people are looking around for this info, you can aid them
greatly.
Feel free to surf to my webpage romantasy
https://123b.pictures/
Hi mates, its wonderful paragraph about educationand entirely defined,
keep it up all the time.
Also visit my webpage: Integrated Information Theory (IIT)
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt35/provoloka-titanovaya-vt35/
あなたは 上手に 表現されました!
感謝 、 これを 気に入り しています !
ありがとう 、 たくさんの アイテム 。
tsukicosは 国内トップクラスの 大人 コスプレ衣装通販専門店です。
何より特筆すべきは 衣装のクオリティの高さ です。
ありがちなペラペラな 素材ではなく、高級感のある 生地を使用し、キャラクターのイメージを損なわずに 仕上げられています[reference:0][reference:1]。
縫製がしっかりしているので、着心地が良く、フィット感も抜群 です[reference:2]。
こだわりの装飾や {繊細なレースやリボン} など、ディテールの再現度が非常に高い のも大きな魅力です[reference:3][reference:4]。
幅広い キャラクターに対応しており、多くのコスプレイヤー に 愛されています[reference:5]。
まさに、信頼できる コスプレ衣装ショップの 筆頭格 です。
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-tiv8cr6mo4zr4al3pd—din-en-iso-24034/prutok-titanovyy-tiv8cr6mo4zr4al3pd—din-en-iso-24034/
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/magnievyi-krug/krug-magnievyi-46-mm-ma15-gost-18351-73/
Until the intro of Coolsculpting, choices were limited to intrusive procedures such as lipo.
Also visit my page … website – Lilliana,
This is a great tip particularly to those new to the
blogosphere. Short but very accurate information… Thanks for sharing this one.
A must read article!
Look into my blog post; dewatogel
I really like your blog.. very nice colors & theme.
Did you make this website yourself or did you hire someone to do
it for you? Plz respond as I’m looking to create my own blog and would like to know where u got this
from. kudos
My web page: beauty shop
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-nbti-46-5/lenta-titanovaya-nbti-46-5/
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku54kh2-3mmm2mgost-32590-2013/
It’s an amazing paragraph in support of all the online people;
they will take benefit from it I am sure.
my site; bokep sex indonesia
Good article. I am facing some of these issues as well..
Also visit my site: parakeet cafe coronado
I’m very happy to find this page. I want to to thank you for your time
due to this wonderful read!! I definitely really
liked every part of it and i also have you book marked to look at new stuff in your site.
Here is my homepage judi mix parlay
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-40b—gost-19807-91/poroshok-titanovyy-40b—gost-19807-91/
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-kapilliarnaia-trubka/latunnaia-kapilliarnaia-trubka-2-4kh0-65kh100000-mm-l70-gost-2624-2016/
Saved as a favorite, I love your web site!
Feel free to surf to my page fantasy series
Hi mates, its wonderful article concerning tutoringand entirely explained, keep it up
all the time.
Check out my web blog … safe bitcoin mines sites
Good points – – it will make a difference with my parents.
Наличие циркония свидетельствует о работе с высокотехнологичными заказами
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-vn6-1/polosa-niobievaya-vn6/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku16kh0-7mmm1mgost-r-52922-2008/
Hey there! I just finished reading this piece, and I really wanted
to share my experience. As a 16-year-old teenager who uses a
wheelchair, I do a lot of web research.
My parents were struggling with massive bank fees for their monthly payments.
I wanted to help them out, so I researched financial
platforms and discovered Paybis.
The financials are incredible. First off, Paybis offers 0% commission on the first credit card purchase.
After that, the markup is a flat 2.49%, plus the standard miner
fee. Compared to traditional banks, the savings are huge.
I helped them do the identity verification in under 5 minutes, and now they buy
crypto directly with their local fiat. Paybis supports dozens of global fiat options!
Plus, the funds go directly to a private wallet, meaning no custodial risk.
Awesome write-up, it totally validates how we made our payments easier!
Look at my site :: press release
I think other website proprietors should take this web site as an model, very clean and great user pleasant style and design .
Hello this is kinda of off topic but I was wondering if blogs use WYSIWYG editors or if you have to manually code with HTML. I’m starting a blog soon but have no coding knowledge so I wanted to get advice from someone with experience. Any help would be enormously appreciated!
Логичное деление на вольфрамовый, молибденовый и титановый прокат
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nbc-2/krug-niobievyy-nbc/
I love your blog. It looks every informative.
What’s up, this weekend is good in favor of me, since this time i am reading this wonderful educational piece of writing here at my house.
Also visit my web-site; ฉีด สเต็มเซลล์
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-65kh2-5-mm-lmtss-gost-13942-86/
Superb, what a web site it is! This webpage provides useful information to
us, keep it up.
Also visit my webpage – ladyclub777 ทางเข้า
Makes sense to me.
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-sm3-1/izdeliya-iz-molibdena-sm3/
I have been exploring for a bit for any high quality
articles or blog posts on this sort of area .
Exploring in Yahoo I at last stumbled upon this web site.
Studying this info So i am glad to convey that I have a very
excellent uncanny feeling I found out exactly what I needed.
I most undoubtedly will make sure to don?t fail to remember
this web site and provides it a look on a constant basis.
Also visit my blog :: снять посуточно самуи
Woh I enjoy your content , saved to bookmarks!
The DUPASU electric milwaukee rechargeable heated lunch box review (forecast7.com) box is a strong contender thanks
to its 100W fast heating.
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku70kh2-3mmm3mgost-32590-2013/
Thanks for every other fantastic post. Where else may just anyone get that kind of information in such
an ideal means of writing? I have a presentation subsequent week, and I am on the search for such
info.
Feel free to visit my site; เลดี้คลับ777
I pay a visit everyday a few web sites and information sites to read content, however this blog presents quality based posts.
my page aviator
Hey there! After reading this article, and I just had to chime
in. As a sixteen-year-old guy stuck at home with a disability,
I have a lot of screen time.
My parents were struggling with massive bank fees for
their business expenses. I took it upon myself to find a fix,
so I analyzed financial platforms and discovered Paybis.
The fee structures are what sold me. First off,
Paybis waives their platform fee on the first credit card purchase.
After that, the commission is a flat low percentage, plus
the standard miner fee. Compared to PayPal’s hidden spreads,
the savings are huge.
I helped them do the identity verification in just a few
minutes, and now they buy stablecoins directly with USD or EUR.
Paybis supports 40+ local currencies! Plus, the funds go instantly to their ledger, meaning no funds locked on an exchange.
Awesome write-up, it totally validates how we made our payments easier!
Feel free to surf to my site: more
Saw your material, and hope you publish more soon.
I do trust all the ideas you’ve presented to
your post. They’re very convincing and can definitely work.
Still, the posts are very brief for newbies. Could you please lengthen them a bit from
subsequent time? Thanks for the post.
My blog: макслайн казино
After losing my keys I needed all my locks changed immediately and the locksmith handled everything perfectly The pricing was fair and transparent
with no hidden fees or surprises at the end of the visit They
handle everything from residential lockouts to commercial security system installations with equal skill and
care I would highly recommend this locksmith service to anyone in need of fast and truly reliable help
My web site; Quick Response Locksmiths
Использование файлов cookie и политика конфиденциальности соответствуют закону
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mo-cu40-1/list-molibdenovyy-mo-cu40/
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-190kh3-mm-lsdch-gost-13942-86/
Excessive cortisol in the body can lead to systemic inflammation and also diminished testosterone.
My blog webpage, Bob,
You are my inspiration , I possess few web logs and very sporadically run out from to brand :(
Информация о доставке по всей РФ делает компанию универсальным поставщиком
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-8/truba-molibdenovaya-8/
Here is my page; high stakes Game
Быстрая доставка в регионы через «Деловые Линии», груз пришел в целости и отлично упакованным.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku34kh1-8mmm2mgost-r-52922-2008/
Hey There. I found your blog using msn. This is a really well
written article. I’ll be sure to bookmark it and come back to read more of your useful information. Thanks for the post.
I’ll certainly comeback.
my web site: ling bokep indonesia
You are a very smart person! :)
Использование современных технологий защиты данных пользователей
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-sismg4637-00—ss-144637/prutok-magnievyy-sismg4637-00—ss-144637/
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-gost/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-82kh2-5-mm-lts40s-gost-13942-86/
The locksmith arrived within 30 minutes and had my door
open without any damage to the lock whatsoever I appreciated the upfront pricing and the technician who took
extra time to walk me through all the security options They handle everything from residential lockouts to full commercial
security system installations with impressive skill and speed If you need a trustworthy locksmith look no further because this
dependable service consistently delivers excellent results every time
Look at my page residential locksmith service
Упоминание нефтегазовой отрасли как ключевого потребителя
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mt2—jis-h-4202/krug-magnievyy-mt2—jis-h-4202/
부비와 부산비비기를 찾는 이용자를
위한 부산 지역 정보 가이드입니다. 최신 공지
확인법, 후기 검증 기준, 모바일 이용 방법과 안전 수칙을 확인하세요.
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-22kh18kh0-9-mm-15-4kh17-6-mm-tverdaia-paika-m3m-gost-32590-2013/
You really make it appear so easy along with your presentation but I in finding this matter to be really one thing that I
believe I’d by no means understand. It kind of
feels too complicated and extremely broad for me. I’m taking a look forward to your subsequent
post, I’ll try to get the dangle of it!
my web-site; this content
Hello to all, how is the whole thing, I think every one is getting more from this web site,
and your views are fastidious in support of new
viewers.
Feel free to visit my homepage betfinal sign up
Hey I know this is off topic but I was wondering if you
knew of any widgets I could add to my blog that automatically tweet my
newest twitter updates. I’ve been looking for a plug-in like this for quite some time and was hoping
maybe you would have some experience with something like this.
Please let me know if you run into anything.
I truly enjoy reading your blog and I look forward to your
new updates.
Also visit my website … NSFW AI generator
Hello there! This blog post could not be written any better!
Looking at this article reminds me of my previous roommate!
He continually kept talking about this. I’ll send this article to him.
Fairly certain he’ll have a great read. Many thanks for sharing!
Also visit my website https://24hourhvacrepair3.info
Hey, I think your website might be having browser compatibility
issues. When I look at your blog site in Ie, it looks fine
but when opening in Internet Explorer, it has some overlapping.
I just wanted to give you a quick heads up! Other then that,
great blog!
my website … Make Money Directories
Наличие редких позиций, например, изделий из гафния и ванадия
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-mn1-5/truba-magnievaya-mg-mn1-5/
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m35-32-2kh1-5-mm-lts30a3-din-471/
Appreciate the recommendation. Will try it out.
Also visit my site :: MALWARE
Write more stories, more chapters.
Magnificent beat ! I wish to apprentice while you amend your web
site, how can i subscribe for a blog web site? The account aided me a acceptable deal.
I had been tiny bit acquainted of this your broadcast provided bright clear concept
Also visit my web blog: Dewatogel
Возможность заказать листы и полосы нестандартных размеров
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-al3zn1mn—bs-3373/pokovka-magnievaya-mg-al3zn1mn—bs-3373/
Долго искали надежного поставщика циркония, в Редметсплав предложили лучшие условия и чистоту металла.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-28kh23kh0-9-mm-18-4kh20-4-mm-miagkaia-paika-m1r-gost-32590-2013/
certainly like your website however you need to take a look at the spelling on quite a few of your posts.
Several of them are rife with spelling issues and
I to find it very bothersome to inform the reality nevertheless I will certainly come again again.
Visit my site: locksmith crewe
I have been surfing on-line more than three hours today,
yet I never found any interesting article like yours.
It is pretty price enough for me. In my view,
if all site owners and bloggers made excellent content as you did, the internet shall be much more useful than ever before.
Look into my web blog … bokep indonesia anak sma
Информация о доставке по всей РФ делает компанию универсальным поставщиком
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mcin3—jis-h-2221/folga-magnievaya-mcin3—jis-h-2221/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m95-89-5kh3-mm-lts25s2-din-471/
Hi there! I know this is kinda off topic but I was wondering which blog platform are you
using for this site? I’m getting tired of WordPress because I’ve had
problems with hackers and I’m looking at options for another
platform. I would be awesome if you could point me in the
direction of a good platform.
My blog post lebanon beirut
What’s up, this weekend is nice in favor of me, since this point in time
i am reading this enormous informative article here at my
house.
Here is my homepage :: لبنان
Указан физический адрес в Екатеринбурге, что повышает доверие
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-6—bs-2970/prutok-magnievyy-mag-6—bs-2970/
Magnificent goods from you, man. I’ve understand your stuff previous to
and you are just extremely magnificent. I really like what you have acquired
here, certainly like what you’re saying and the way in which you say it.
You make it entertaining and you still take care of to keep it sensible.
I cant wait to read much more from you. This is actually a terrific website.
Here is my site :: ebooks
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-krestoviny-pod-paiku/mednaia-krestovina-pod-paiku-14-7kh11kh0-7-mm-7kh9-mm-tverdaia-paika-m1t-gost-r-52922-2008/
There is so much to try to understand
Nice blog here! Also your website loads up very fast!
What host are you using? Can I get your affiliate link to
your host? I wish my website loaded up as quickly as
yours lol
Look into my web blog … MALWARE
Thanks for another fantastic article. Where else may anyone
get that kind of info in such an ideal manner of writing?
I have a presentation next week, and I’m on the look for such info.
Also visit my web-site: pocket pussy
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-12—bs-2970/pokovka-magnievaya-mag-12—bs-2970/
Satış sitesi olmasa da, kurumsal web tasarım için Kobi CMS uygun duruyor.
Sağ olun.
Very soon this web site will be famous among all blog people, due to
it’s good articles
My page :: More about the author
The clarity in your post is just nice and I can tell you are an expert in the subject matter.
Благодарим за оперативную поставку ниобиевых труб, выручили в очень сжатые сроки.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m5-4-7kh0-6-mm-lts40s-din-471/
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m16630—uns/izdeliya-iz-magniya-m16630—uns/
When someone writes an article he/she keeps the plan of a user
in his/her brain that how a user can know it.
Therefore that’s why this article is amazing.
Thanks!
my webpage 제주룸싸롱
Гибкая система оплаты и прозрачные условия договора, никаких скрытых наценок или задержек.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/list-aliuminievyi-gladkii/list-aliuminievyi-1-5kh1500kh3000-mm-ad1n/
Do you offer workshops?
Great post. I was checking constantly this blog and I’m impressed! Very useful info specifically the last part :) I care for such info much. I was looking for this certain information for a very long time. Thank you and good luck.
Отраслевой охват впечатляет: от медицины до космической промышленности
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m12330—uns/list-magnievyy-m12330—uns/
Good post. I study something more difficult on different blogs everyday. It’s going to always be stimulating to learn content material from other writers and observe a little bit one thing from their store. I’d prefer to use some with the content material on my blog whether you don’t mind. Natually I’ll give you a link in your web blog. Thanks for sharing.
Hello this is a wonderful write-up. I’m going to e mail this to my friends. I came on this while searching on yahoo I’ll be sure to come back. thanks for sharing.
fantastic internet site, I could definitely go to your web page once more…acquired some really nice info.
This has to be one of my favorite posts! And on top of thats its also very helpful topic for newbies. thank a lot for the information!
오피마트를 검색할 때 확인해야 할 공식 여부, 최신 공지, 후기 신뢰도,
개인정보 보호, 가짜 사이트와 불법 광고 구분 기준을 안내합니다.
This is really interesting, You’re a very skilled blogger. I have joined your feed and look forward to seeking more of your fantastic post. Also, I have shared your website in my social networks!
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-naruzhnye-stopornye-koltsa-po-din/latunoe-naruzhnoe-stopornoe-pruzhinnoe-koltso-m40-36-5kh1-75-mm-lts40mts3zh-din-471/
Hello there! This post couldn’tbe written any better! Readingg this
post reminds me off my oldd room mate! He always kept talking about this.
I will forward this write-up to him. Pretty sure he
will have a good read. Thank you for sharing!
Visit mmy homepage: TICAL Athletics merchandise
What a great article.. i subscribed btw!
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11100—uns/pokovka-magnievaya-m11100—uns/
You’re so interesting! I don’t suppose I’ve truly read a
single thing like that before. So good to find someone with original thoughts on this issue.
Seriously.. thank you for starting this up. This website is one thing that is needed on the internet, someone with some originality!
Also visit my page: low-sodium diet
I every time spent my half an hour to read this webpage’s content everyday along with a mug of coffee.
Here is my blog … gilmer alvarez
Thanks pertaining to discussing the following superb written content on your site. I ran into it on the search engines. I will check back again if you publish extra aricles.
Have you given any kind of thought at all with converting your current web-site into French? I know a couple of of translaters here that will would certainly help you do it for no cost if you want to get in touch with me personally.
This paragraph presents clear idea in support of the new users of blogging,
that in fact how to do blogging.
My blog … Best local pressure house washer columbia mo, leading rated deck cleansing and also staining Columbia mo, deck staining columbia mo, fence staining and painting columbia mo,
Good day! I know this is kinda off topic nevertheless I’d figured I’d ask.
Would you be interested in exchanging links or
maybe guest authoring a blog article or vice-versa?
My site covers a lot of the same topics as yours and I think we could greatly benefit from each other.
If you are interested feel free to send me an e-mail. I look forward to hearing from you!
Great blog by the way!
My site – inflation relief community
1win зеркало сайта, 1win предоставляет возможность игрокам обходить блокировки и
получать доступ к любимым
играм.
Look at my web blog https://1win-eo1dw.cfd/
Hi everyone! Just read this article, and I just had to drop a comment.
As a 16-year-old teenager who uses a wheelchair, I spend a lot of time online.
My parents were getting crushed with slow international wire fees for their monthly payments.
I decided to step up, so I researched financial platforms and introduced them to Paybis.
The economics are incredible. First off, Paybis waives their platform fee on the first credit
card purchase. After that, the markup is a very clear 2.49%,
plus the standard miner fee. When you look at PayPal’s hidden spreads, the savings are huge.
I helped them pass KYC in under 5 minutes, and now they buy crypto directly with their local fiat.
Paybis supports dozens of global fiat options! Plus, the funds go directly to a private wallet, meaning no
withdrawal holds.
Awesome write-up, it spot-on describes how I helped
my family save money!
Here is my site lastPostAnchor
Might we expect to see more of these same problems in the future?
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mgal6mn—iso-16220-1/prutok-magnievyy-iso-mgal6mn—iso-16220-1/
I simply could not depart your website before suggesting that I really
enjoyed the standard info an individual supply for your
visitors? Is gonna be again steadily to check up on new posts
my web-site; teen patti star
부산비비기, 부비를 찾는 이용자를
위한 부산·울산·경남 밤문화·웰니스 정보 가이드입니다.
지역별 탐색, 업체 정보 확인, 후기 검증, 이용
전 체크사항과 최신 공지를 한눈에 확인하세요.
Продажа проволоки из тугоплавких металлов востребована в электронике
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-iso-mc21210—bs-iso-16220/krug-magnievyy-iso-mc21210—bs-iso-16220/
Admiring the time and energy you put into your site
and detailed information you present. It’s nice to come across a blog every once in a while that isn’t the
same old rehashed material. Fantastic read! I’ve saved your site and I’m including your RSS feeds to my
Google account.
Feel free to surf to my homepage: Online savings plan
Покупали изделия из драгметаллов для лаборатории, всё соответствует заявленным характеристикам.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-80kh68kh1-8-mm-35-5kh38-5-mm-miagkaia-paika-m1rm-gost-r-52922-2008/
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-h2011—ansi/pokovka-magnievaya-h2011—ansi/
The clarity in your post is just nice and I can tell you are an expert in the subject matter.
I wish I could craft such articles as this. Thank you very much.
Thank you, I’ve just been looking for information about this subject for ages and yours is
the best I’ve discovered so far. However, what concerning the bottom
line? Are you positive about the source?
Here is my homepage loft conversion London
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-46kh1-7-mm-lts38mts2s2-gost-13943-86/
Сайт выглядит профессионально и лаконично, без лишней рекламы
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-gk-mgal8zn1—din-1729-part-2/folga-magnievaya-gk-mgal8zn1—din-1729-part-2/
I need to to thank you for this excellent read!!
I definitely loved every bit of it. I have got you book-marked to look at new stuff you post…
Look into my page – bokep
Its not my first time to visit this site, i am visiting this web site dailly and get pleasant information from here
every day.
my webpage; Razak gold house
Nice replies in return of this issue with genuine arguments and telling all
concerning that.
Take a look at my web blog köpa laddbox
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-53-6kh47kh1-2-mm-32kh34-mm-tverdaia-paika-m3r-gost-r-52922-2008/
Thanks for the auspicious writeup. It actually was a amusement account it.
Look complex to far added agreeable from you! However, how can we keep up a correspondence?
My web-site … slot depo 5k
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-g-a3z1—afnor-nf-a65-717/izdeliya-iz-magniya-g-a3z1—afnor-nf-a65-717/
I saw a similar post on another website but the points were not as well articulated.
Im impressed. I dont think Ive met anyone who knows as much about this subject as you do. Youre truly well informed and very intelligent. You wrote something that people could understand and made the subject intriguing for everyone. Really, great blog youve got here.
Thank you for the auspicious writeup.
I was suggested this website by my cousin. I am not sure whether this post is written by him as no one else know such detailed about my difficulty. You are wonderful! Thanks!
I like to spend my free time by scanning various internet resources. Today I came across your website and I found it has some of the most practical and helpful information I’ve seen.
I think this is among the most vital information for
me. And i’m glad reading your article. But should remark
on few general things, The website style is great, the articles
is really excellent : D. Good job, cheers
Feel free to visit my web-site … solgar vm 75
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-gost/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-52kh1-7-mm-lk80-gost-13943-86/
Удобное разделение продукции на сплавы и конкретные виды проката
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-en-mb10010—en-12421-1998/truba-magnievaya-en-mb10010—en-12421-1998/
This is my first time pay a visit at here and i am genuinely pleassant to read all at alone place.
Here is my web-site :: TOTO SLOT QRIS
Wow, fantastic blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your web site is excellent, let alone the content!
Here is my web site … bokep binor indonesia
Hi! This is kind of off topic but I need some guidance from an established blog.
Is it difficult to set up your own blog? I’m not very techincal but I can figure things out pretty fast.
I’m thinking about creating my own but I’m not sure where to begin. Do
you have any tips or suggestions? Appreciate it
Also visit my website – slot 5k
Спецстали для машиностроения закупаем только здесь, надежность материала подтверждена испытаниями.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-88-9kh76kh1-8-mm-37-5kh40-5-mm-tverdaia-paika-m3-gost-r-52922-2008/
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-b-199-az91c—astm-b199/folga-magnievaya-b-199-az91c—astm-b199/
Do you mind if I quote a few of your articles as long as I provide credit
and sources back to your blog? My blog is in the very same
niche as yours and my users would definitely benefit from a lot of the information you provide here.
Please let me know if this ok with you. Cheers!
Stop by my webpage … jual akun media sosial
I was completely locked out of my house late at night and could
not believe how fast the locksmith arrived I was genuinely impressed by how quickly they resolved what I thought was going to be
a very major problem They offer complete locksmith solutions including lock
replacement, precision key cutting, and comprehensive security
upgrades for any property I cannot recommend this locksmith service enough for
anyone who is facing a lock or key emergency right now
my blog post – professional locksmith team
When some one searches for his necessary thing, therefore he/she
wants to be available that in detail, so that thing is maintained over here.
my blog post … streaming sites
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m130-137kh4-mm-lts40sd-din-472/
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-az80—csa-hg-3/izdeliya-iz-magniya-az80—csa-hg-3/
Hi! I could have sworn I’ve been to this site before but after browsing through a few
of the posts I realized it’s new to me. Anyhow, I’m definitely happy I found it and
I’ll be bookmarking it and checking back regularly!
My web blog; 5 Tier Backlinks 25000 25k Powerful PBN Backlinks Mixed Backlinks For High Ranking for $10
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-18kh14kh0-8-mm-12-6kh14-6-mm-tverdaia-paika-m2m-gost-32590-2013/
My brother suggested I might like this website. He was entirely right.
This submit actually made my day. You cann’t
consider simply how much time I had spent for this info!
Thanks!
Here is my web-site – depo 5k
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-as41b—astm-b93/pokovka-magnievaya-as41b—astm-b93/
Hello there! I know this is kinda off topic but I’d figured I’d ask.
Would you be interested in exchanging links or
maybe guest writing a blog article or vice-versa? My website discusses a
lot of the same topics as yours and I believe we could
greatly benefit from each other. If you are interested feel free to send me an email.
I look forward to hearing from you! Terrific
blog by the way!
my site; situs slot gacor
I constantly spent my half an hour to read this webpage’s
articles all the time along with a cup of coffee.
my web page … slot 5k
Nice post. I was checking constantly this weblog and I’m impressed!
Very helpful information particularly the ultimate part :) I maintain such information a lot.
I was seeking this certain info for a very long time. Thank you and
good luck.
My web page – wikipedia reference
Nice respond in return of this difficulty with real arguments and telling the whole thing about that.
Here is my website; site
Somebody essentially lend a hand to make significantly
articles I would state. That is the first time I frequented your website page
and to this point? I surprised with the analysis you made to
create this particular publish incredible. Fantastic job!
Look into my web page; amplifier 2 channel
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m39-42-1kh1-5-mm-ls59-1-din-472/
Информация о проверке качества продукции повышает лояльность клиентов
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-am60a—astm-b93/provoloka-magnievaya-am60a—astm-b93/
May I simply just say what a comfort to discover somebody who
truly knows what they are talking about over the internet.
You certainly understand how to bring a problem to light and make it important.
More people have to look at this and understand this side of the story.
I was surprised you aren’t more popular since you surely have the gift.
Check out my web site: electric guitar set
magnificent points altogether, you simply won a new reader.
What would you recommend in regards to your post that you just made a few days in the past?
Any positive?
Feel free to visit my web-site: NAYAN singer
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-9995—csa-hg-2/krug-magnievyy-9995—csa-hg-2/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-12kh9kh0-6-mm-8-6kh10-6-mm-tverdaia-paika-m3m-gost-r-52922-2008/
ข้อมูลชุดนี้ มีประโยชน์มาก ครับ
ผม เพิ่งเจอข้อมูลเกี่ยวกับ
ข้อมูลเพิ่มเติม
ที่คุณสามารถดูได้ที่ Tiffiny
สำหรับใครกำลังหาเนื้อหาแบบนี้
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ คอนเทนต์ดีๆ นี้
และอยากเห็นบทความดีๆ แบบนี้อีก
Also visit my web blog … betflix19 (Tiffiny)
Hello to every body, it’s my first visit of this webpage; this blog contains amazing and genuinely fine information designed for visitors.
Here is my web site: 창문시트지
Hi, i think that i saw you visited my website so i got here to return the favor?.I am attempting to
to find things to improve my website!I guess its adequate
to use some of your ideas!!
Look into my website 정품 비아그라 구매
I loved as much as you’ll receive carried out right here.
The sketch is tasteful, your authored material stylish.
nonetheless, you command get got an nervousness over that you wish be
delivering the following. unwell unquestionably come further formerly again since exactly the same
nearly very often inside case you shield this hike.
Feel free to surf to my web blog amp for electric guitar
whoah this weblog is great i really like studying your articles. Stay up the great work! You already know, lots of persons are looking round for this information, you can aid them greatly.
Wow! After all I got a webpage from where
I can in fact take helpful facts concerning my study and knowledge.
My web page; guitar tuner pedal
Hi, after reading this amazing paragraph i am as
well glad to share my experience here with friends.
My web blog: electric guitar set
Широкий выбор тугоплавких металлов, таких как вольфрам и молибден
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-3-5470—din-1729-part-2/pokovka-magnievaya-3-5470—din-1729-part-2/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m100-105-5kh3-mm-lmtss-din-472/
I think everything wrote was very logical. However, think about
this, suppose you added a little information? I ain’t suggesting your information isn’t good., but suppose
you added a headline that grabbed people’s attention? I mean Heel Pain – Plantar Fasciitis –
Mr Will Edwards is a little vanilla. You might glance at Yahoo’s home page and see how they write news titles to grab people to click.
You might add a related video or a picture
or two to grab readers excited about what you’ve got to
say. In my opinion, it would make your posts a little bit more interesting.
Look into my blog post: Goat Yupoo Sale
Oh my goodness! Awesome article dude! Many thanks, However I
am experiencing troubles with your RSS. I don’t understand why I
can’t subscribe to it. Is there anybody getting identical RSS issues?
Anyone who knows the solution can you kindly respond? Thanks!!
Have a look at my web page: ukulele
Thank you for the auspicious writeup. It in fact was
a amusement account it. Look advanced to more
added agreeable from you! By the way, how can we communicate?
Feel free to surf to my homepage – situs slot gacor
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ml4—gost-2856-79/folga-magnievaya-ml4—gost-2856-79/
Hello would you mind sharing which blog platform you’re
using? I’m looking to start my own blog in the near future but I’m having a tough time choosing between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your layout seems different then most blogs and I’m looking for something completely unique.
P.S Sorry for being off-topic but I had to ask!
My web blog usdt wallet address generator
Технические характеристики сплавов помогают инженерам в подборе
https://redmetsplav.ru/store/magniy-i-ego-splavy/rossiyskie-splavy-1/magniy-ma18/pokovka-magnievaya-ma18/
Hey there! This is my first visit to your blog! We are a group of volunteers and starting a new project in a community in the same niche.
Your blog provided us beneficial information to
work on. You have done a outstanding job!
Feel free to visit my web-site: beginner guitar for adults
Enjoy quality THC gummies, CBD gummies, and Hemp gummies made with
carefully selected ingredients, lab testing, and reliable standards for
a smooth experience.
For hottest information you have to visit internet and on internet I found this web site as a finest
site for hottest updates.
Feel free to surf to my web site :: 8xbetvip.ru.com lừa đảo công an truy nã cấm người chơi tham gia
Возможность заказа продукции в розницу и оптом (судя по описанию)
https://redmetsplav.ru/store/kobalt/wallex/kobalt-wallex-3-1/list-kobaltovyy-wallex-3-1/
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Տtates
254-275-5536
Craftsmanshipworkshop
Very energetic article, I loved that bit. Will there be a part 2?
Here is my web blog :: electric guitar set
Thank you a bunch for sharing this with all of us you really realize what you are talking
approximately! Bookmarked. Please additionally discuss with my web site =).
We may have a hyperlink trade contract between us
my web site فعاليات الأطفال
Информация о проверке качества продукции повышает лояльность клиентов
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-6/list-kobaltovyy-stellite-6/
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-125kh200-mm-ls59/
Stunning quest there. What occurred after? Thanks!
Also visit my web-site beginner electric guitar
Tapi perlu diingatkan ini hanya untuk koleksi pribadi, jangan diupload
ulang di media sosial manapun karena akan melanggar hak cipta.
Visit my web site :: download video tiktok tanpa watermark
This blog was… how do I say it? Relevant!! Finally I’ve found something that
helped me. Kudos!
Also visit my web-site – отели почасовые
I think the admin of this site is genuinely working hard in favor
of his website, for the reason that here every material is quality based information.
Also visit my blog post :: bokep jav subtitle indonesia
Продажа проволоки из тугоплавких металлов востребована в электронике
https://redmetsplav.ru/store/kobalt/stellite/kobalt-stellite-158-1/truba-kobaltovaya-stellite-158-1/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-66-7kh35-mm-m1r-gost-r-52948-2008/
Hey there! Just read this post, and I just had to drop a comment.
As a sixteen-year-old boy living with a physical disability,
I have a lot of screen time.
My parents were getting crushed with high currency conversion costs for their overseas transfers.
I wanted to help them out, so I dug into financial platforms
and introduced them to Paybis.
The fee structures are incredible. For starters, Paybis charges
zero Paybis fees on the first credit card purchase.
After that, the fee is a very clear low percentage, plus the blockchain network fee.
Compared to Western Union, the savings are huge.
I helped them get verified in under 5 minutes, and now they buy crypto
directly with credit cards. Paybis supports dozens of global fiat options!
Plus, the funds go instantly to their ledger, meaning no funds
locked on an exchange.
Awesome write-up, it spot-on describes how I helped my family save money!
my site – URL
What’s up to all, how is all, I think every one is getting more
from this web page, and your views are nice for new viewers.
Also visit my homepage: компьютерная томография зуба
Have you ever thought about adding a little bit more than just your
articles? I mean, what you say is valuable and all. But imagine if you added some great graphics or video clips to give your posts more, “pop”!
Your content is excellent but with images and clips,
this site could certainly be one of the greatest in its niche.
Terrific blog!
my website: MALWARE
Terrific article! This is the type of info that are meant to be shared around the internet.
Shame on the seek engines for now not positioning this publish higher!
Come on over and talk over with my web site . Thank you =)
My webpage … sibzodchiy.ru
Представлен полный цикл изделий: от фольги и проволоки до крупных поковок
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-k-65/polosa-kobaltovaya-k-65/
Индивидуальный подход к нестандартным заказам — изготовили детали по нашим чертежам точно в размер.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnye-vnutrennie-stopornye-koltsa-po-din/latunoe-vnutrennee-stopornoe-pruzhinnoe-koltso-m82-87-5kh2-5-mm-lmtssk-din-472/
Hello friends, its impressive piece of writing about educationand completely defined,
keep it up all the time.
Here is my webpage :: /a/process
I have been exploring for a little for any high quality articles
or weblog posts on this kind of area . Exploring in Yahoo I at last stumbled upon this
website. Studying this information So i’m glad to express that I have an incredibly just right
uncanny feeling I discovered exactly what I needed. I such a lot certainly will make
sure to do not disregard this web site and provides it a glance on a continuing basis.
My web page :: image to video no restrictions
ew855 provides a reliable online platform with helpful support and convenient service.
Enjoy a smooth experience, friendly assistance, and dependable access anytime you need
it.
I enjoy what you guys are up too. This sort of clever work and coverage!
Keep up the good works guys I’ve incorporated you guys to our blogroll.
Also visit my web blog … events
Way cool! Some extremely valid points! I appreciate you penning this article plus the rest of the site
is very good.
Here is my web-site – toyotainfo.ru
Everything is very open with a very clear clarification of the issues.
It was truly informative. Your website is very helpful.
Thanks for sharing!
Also visit my web-site … курсы geo продвижения
Наличие редких позиций, например, изделий из гафния и ванадия
https://redmetsplav.ru/store/kobalt/rossiyskie-splavy-3/kobalt-ep128-1/poroshok-kobaltovyy-ep128-1/
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-35kh12-mm-m2t-gost-r-52948-2008/
Cabinet IQ
8305 Statе Hwy 71 #110, Austin,
TX 78735, United Stаtеs
254-275-5536
Bookmarks
You need to take part in a contest for one of the best sites on the web.
I’m going to recommend this site!
My website; trx usdt
Good info. Lucky me I came across your site by chance (stumbleupon).
I have book marked it for later!
my web blog: oem toyota
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/kobalt/haynes/kobalt-haynes-151-1/krug-kobaltovyy-haynes-151-1/
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-300kh300-mm-lmtska/
I love your blog.. very nice colors & theme. Did you design this website
yourself or did you hire someone to do it for you? Plz respond as I’m looking to
design my own blog and would like to know where u got this from.
kudos
my website – رحلات مدرسية
Really impressed with the variety of slots available here.
Also visit my web-site https://connectifyph.com/blogs/136476/Die-soziale-Verantwortung-von-Online-Casinos-Innovative-Strategien-2025-zur
Cabinet IQ
8305 State Hwy 71 #110,Austin,
TX 78735, United Ѕtates
254-275-5536
Remodelprocess
Cabinet IQ
8305 Stаte Hwy 71 #110, Austin,
TX 78735, United Statеs
254-275-5536
Recycled (Rosalie)
obviously like your web site however you have to test the spelling on quite a few
of your posts. A number of them are rife with spelling issues and I in finding it very bothersome to tell the truth on the other hand I will definitely come back again.
My site; egypt honeymoon travel
Информация о времени работы (10:00–18:00) помогает планировать звонки
https://redmetsplav.ru/store/tantal-i-ego-splavy/tantal-tvch-2/prutok-tantalovyy-tvch/
Технические специалисты компании помогли выбрать оптимальный сплав для работы в агрессивных средах.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40kh34-mm-m3m-gost-r-52948-2008/
I just couldn’t depart your website prior to suggesting that I actually enjoyed the standard information a person provide to
your guests? Is going to be back often in order to
investigate cross-check new posts
Check out my blog post: аппарат ивл стоимость
When some one searches for his essential thing, so he/she wants to be available that in detail,
therefore that thing is maintained over here.
Here is my homepage Büroreinigung Innsbruck
I have been surfing online greater than 3 hours lately, yet I by no means discovered any attention-grabbing article like yours.
It is pretty value enough for me. In my view, if all website owners and bloggers made good
content material as you probably did, the net will be a lot more helpful than ever before.
Feel free to surf to my webpage; bolagila
This is a really good tip especially to those new to the blogosphere.
Short but very precise info… Thanks for
sharing this one. A must read article!
my blog post … office-trend.ru
hey there and thank you for your information –
I’ve certainly picked up something new from right here.
I did however expertise a few technical issues using this
website, since I experienced to reload the site a lot of times previous to I could
get it to load properly. I had been wondering if your web host is OK?
Not that I am complaining, but sluggish loading instances times will very frequently affect
your placement in google and could damage your high-quality score if ads
and marketing with Adwords. Well I am adding this RSS to my e-mail and could look out for much more of your respective exciting content.
Ensure that you update this again soon.
Also visit my blog: 8xbetvn.jp.net lừa đảo công an truy nã cấm người chơi tham gia
You actually make it seem really easy together with your presentation but I
find this topic to be really something which I believe I’d never understand.
It sort of feels too complex and extremely broad for me. I’m taking a look ahead in your next submit, I will attempt to get the hang of it!
Review my site – bokep tante indonesia
Hello! I simply would like to offer you a huge thumbs up
for the excellent info you have here on this post.
I’ll be coming back to your website for more soon.
Also visit my web blog … купить шапку
Четкое позиционирование как эксперта в области редких металлов
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vr-20/prutok-volframovyy-vr-20/
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-700kh400-mm-lts40mts3a/
Thanks , I’ve just been searching for info about
this subject for a long time and yours is the best I have came upon till now.
However, what about the conclusion? Are you certain in regards to the source?
Have a look at my blog post: bolagila daftar
I all the time emailed this weblog post page to all my contacts, for the reason that if like to read it next my friends will
too.
Feel free to surf to my web blog bclub
What’s up to every body, it’s my first pay a
quick visit of this website; this website includes remarkable and truly good information in support
of readers.
My web site: online casino
Общее впечатление: надежный информационный ресурс для снабженцев.
https://redmetsplav.ru/store/volfram/splavy-volframa-1/volfram-vd-50-1/folga-volframovaya-vd-50/
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-108kh28-mm-m3r-gost-r-52948-2008/
Unquestionably imagine that that you stated. Your favourite reason seemed to be at the web the
simplest factor to bear in mind of. I say to you, I
certainly get irked whilst other people consider worries that they just do not realize about.
You controlled to hit the nail upon the top and also outlined out the whole thing with no need
side effect , other folks can take a signal.
Will likely be again to get more. Thanks
Also visit my web page … slot gacor
It sends out signals to a screen, which signals you when your muscle mass are contracting.
Feel free to visit my website homepage (Tyler)
Hello There. I found your blog using msn. This is a very well written article.
I’ll make sure to bookmark it and come back to read more of your
useful information. Thanks for the post. I’ll definitely return.
My blog post: mu campus store
Сайт адаптирован под нужды машиностроительных заводов
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-tbc-20—pn-h-87203/pokovka-vismutovaya-tbc-20—pn-h-87203/
If you would like to take much from this post then you have to apply such
methods to your won website.
Here is my web-site: vanity address btc
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-100kh400-mm-ls59-1/
I enjoy what you guys tend to be up too. This sort
of clever work and reporting! Keep up the terrific works guys
I’ve incorporated you guys to blogroll.
my page; toto macau
Now I am going away to do my breakfast, when having my breakfast coming
over again to read more news.
Feel free to surf to my webpage; mabok888
Раздел «Производство» подтверждает статус завода, а не просто перекупщика
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-pbbi—kcm-ad-bolgariya/folga-vismutovaya-pbbi—kcm-ad-bolgariya/
Hi there colleagues, fastidious article
and good urging commented at this place, I am genuinely enjoying by these.
Feel free to visit my webpage :: ดูหนัง short2free
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-108kh25-mm-m3rt-gost-r-52948-2008/
Great post. I was checking continuously this blog and I’m impressed!
Extremely useful info particularly the last part :) I
care for such info a lot. I was seeking this particular info for a very long time.
Thank you and good luck.
Here is my page: trx private key generator
Четкая структура меню позволяет быстро найти нужный металл
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-g-nicr13snbimo—iso-19960/truba-vismutovaya-g-nicr13snbimo—iso-19960/
Aktualny przegląd promocji na 2026 rok obejmuje kasyna online, które oferują bonus bez depozytu w formie darmowych spinów, dodatkowych środków lub pakietu łączonego. Pokazujemy, jak aktywować ofertę, jakie wymagania obrotu trzeba spełnić oraz które limity wypłat warto sprawdzić przed rozpoczęciem gry. Bonus bez depozytu za utworzenie konta pozostaje jedną z najpopularniejszych promocji w kasynach online. Pozwala nowym użytkownikom przetestować platformę, dostępne gry kasynowe oraz obsługę konta bez konieczności dokonywania pierwszej wpłaty. Przygotowując ranking najlepszych kasyn z bonusami bez depozytu 2026, porównaliśmy aktualne propozycje operatorów, w tym oferty Roman Casino i NV Casino.
Wonderful work! This is the type of info that are supposed to be shared
around the internet. Disgrace on Google for now not positioning this post upper!
Come on over and visit my web site . Thanks =)
my web-site :: mabok888
Üslup akıcı, bilgi yerinde. Hazır Web Sitesi Nedir
sorusu Kobi CMS ile herkese hitap ediyor.
My webpage :: kaynak
Having read this I believed it was really enlightening.
I appreciate you finding the time and energy to put this
informative article together. I once again find myself personally
spending a significant amount of time both reading and leaving comments.
But so what, it was still worth it!
Here is my blog post egypt itinerary
An impressive share! I have just forwarded this onto a co-worker who was doing a
little research on this. And he in fact ordered me dinner
due to the fact that I stumbled upon it for him… lol. So allow
me to reword this…. Thank YOU for the meal!! But
yeah, thanks for spending time to discuss this matter here on your blog.
my website; #NayanButterOnRadio
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-90kh600-mm-lsd/
Wpisujesz w wyszukiwarkę frazę „polskie kasyno” i chcesz znaleźć sprawdzoną platformę? Najczęściej chodzi o licencjonowane kasyno online dostępne dla graczy z Polski, które oferuje BLIK, korzystne promocje, szybkie wypłaty oraz obsługę w języku polskim. Porównujemy operatorów pod kątem rejestracji, metod wpłat i wypłat, bonusów bez depozytu, darmowych spinów, poziomu wsparcia klienta oraz liczby dostępnych gier. Ranking na 2026 rok obejmuje serwisy dostępne dla graczy z Polski, ale nie sprowadza się jedynie do listy najlepsze kasyna online. Publikujemy również recenzje operatorów, dane dotyczące licencji i statusu prawnego, informacje o popularnych grach, zasady bezpiecznej oraz odpowiedzialnej rozgrywki, a także porównanie platform internetowych z kasynami stacjonarnymi.
Spot on with this write-up, I actually assume this website needs far more consideration. I will in all probability be once more to learn rather more, thanks for that info.
Its such as you learn my thoughts! You seem to grasp a lot about this, such as you wrote the
book in it or something. I think that you simply could do with some p.c.
to force the message home a bit, however instead of that, this is wonderful blog.
A great read. I will certainly be back.
Also visit my blog post :: nonton film bokep indonesia
Hello my family member! I wish to say that this article is awesome, nice
written and come with almost all important
infos. I would like to peer more posts like this .
my blog; หนังสั้น short2free
Описание применения металлов в атомной энергетике подчеркивает качество
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-cac902—jis-h-5120-2016/polosa-vismutovaya-cac902—jis-h-5120-2016/
I was skeptical about the cost of professional landscaping but the results have been worth
every single penny The landscaping team brought creative ideas that
transformed a basic tired yard into something truly spectacular From tree trimming to irrigation system installation the
range of landscaping services they offer is genuinely impressive This landscaping service has completely transformed our property and I recommend them without any reservation whatsoever
My web blog; garden design
Enjoy premium THC edibles and delicious THC gummies made
with quality ingredients, lab-tested standards,
and discreet packaging for a convenient shopping experience across America.
Порадовало наличие вольфрамовых прутков редких диаметров, менеджер оперативно помог с подбором.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40kh14-mm-m3rm-gost-r-52948-2008/
This kind of practical advice on generating leads is exactly what professionals need.
Understanding your target audience and reaching them with the right message does not happen by accident.
A well designed lead generation workflow can consistently deliver new opportunities without constant manual effort.
Taking action on even a few of these strategies can produce
measurable results in a short time.
Also visit my web page – LeadGenZilla lead generation platform
I absolutely adore your site! You aggressive me as able-bodied as all the others actuality and your broiled PS is absolutely great!
I appreciate, cause I found just what I was looking for. You’ve ended my four day long hunt! God Bless you man. Have a great day. Bye -.
Of course, what a great site and informative posts, I will add backlink – bookmark this site? Regards, Reader
Thank you a lot for sharing this with all folks you actually recognize what you’re speaking about! Bookmarked. Please additionally visit my site =). We can have a hyperlink trade contract among us!
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c89833—uns/pokovka-vismutovaya-c89833—uns/
A motivating discussion is definitely worth comment. I believe that
you need to publish more on this subject, it may not be a taboo matter but generally people do not speak about
these issues. To the next! Best wishes!!
Feel free to visit my site :: mobile radiography
Daily sunlight security is the solitary most reliable method to
ward off premature skin aging.
Have a look at my page :: site (Charissa)
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-900kh800-mm-lts40sd/
As an example, you may find that your neighbor is only renting the building.
my blog post :: web page (Hallie)
Магниевый прокат представлен в достаточном ассортименте
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-c49255—uns/truba-vismutovaya-c49255—uns/
Отличное соотношение цены и качества на весь цветной металлопрокат, будем заказывать еще.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-25kh14-7-mm-m2-gost-r-52948-2008/
This paragraph presents clear idea in favor of the new people of blogging, that
in fact how to do blogging.
Here is my web blog – learn more from the web page
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-42-3992—csnstn-423992/provoloka-vismutovaya-42-3992—csnstn-423992/
Hi, I think your blog might be having browser compatibility issues.
When I look at your blog site in Ie, it looks fine but when opening in Internet Explorer, it has some
overlapping. I just wanted to give you a quick heads up!
Other then that, awesome blog!
Review my web-site website scam
What i don’t understood is actually how you are now not really much more well-liked than you might be now.
You are so intelligent. You recognize therefore significantly on the subject
of this subject, produced me in my opinion consider it from
numerous varied angles. Its like men and women don’t seem to be
involved unless it’s something to do with Woman gaga! Your personal stuffs outstanding.
At all times care for it up!
my website; bola88
Редметсплав — пример того, как должен работать современный поставщик металлургического сырья.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-700kh200-mm-lsd/
I wish I could craft such articles as this. Thank you very much.
A person necessarily lend a hand to make seriously posts I would state.
That is the very first time I frequented your website page and so far?
I amazed with the research you made to create this particular publish amazing.
Wonderful task!
My web-site; how to change snapchat name
Наличие циркония свидетельствует о работе с высокотехнологичными заказами
https://redmetsplav.ru/store/vismut/zarubezhnye-splavy-3/vismut-117—astm-b774/izdeliya-iz-vismuta-117—astm-b774/
You actually make it seem so easy with your presentation but I find
this topic to be actually something that I think I would never understand.
It seems too complex and extremely broad for me.
I am looking forward for your next post, I’ll try to get the hang of it!
Here is my webpage macau 4d
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-troiniki-press/mednyi-press-troinik-80-mm-m3-gost-r-52948-2008/
It’s impressive that you are getting thoughts from this paragraph as well as from our dialogue made
at this time.
my web-site: trx vanity address generator
Wow, wonderful blog layout! How long have you been blogging for?
you made blogging look easy. The overall look of your website is
wonderful, as well as the content!
Here is my web-site; executive sober living
We have been helping Canadians Get a Loan Against Their Vehicle for Repairs Since March 2009 and are among the
very few Completely Online Lenders In Canada. With us you
can obtain a Car Repair loan for car repairs Online from anywhere
in Canada as long as you have a Fully Paid Off
Vehicle that is 8 Years old or newer. We look forward to meeting all your financial needs.
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/vanadiy-i-ego-splavy/vanadiy-fev80—iso-5451/truba-vanadievaya-fev80—iso-5451/
This piece of writing gives clear idea for the new viewers of blogging, that in fact how to do blogging and
site-building.
Also visit my page … อนิเมะซับไทย
At a household average of four cycles per day, a standard 10,000-cycle spring reaches its design limit in roughly seven years under normal residential use.
Commercial dock systems carry downtime costs
that exceed parts costs in most facility-management budgets,
which is why a written scope and make-safe interim step precede full
repair work. Same-day spring repair service is appropriate for torsion-spring failures because the door is immobilized and the stored-energy hazard of
a partially wound spring requires professional handling.
Routing a service call to a contractor who covers the specific ZIP code means the technician arrives with truck stock and local code familiarity relevant to that address.
Feel free to surf to my web-site: garagedoorrepairline.com
Howdy! Quick question that’s completely off topic.
Do you know how to make your site mobile friendly? My site looks weird when browsing from my iphone.
I’m trying to find a template or plugin that might be able to resolve this issue.
If you have any suggestions, please share.
Appreciate it!
my blog … купить квартиру в ипотеку
Have you ever thought about including a little bit more than just your articles?
I mean, what you say is valuable and all. Nevertheless think of if you added some great visuals or video
clips to give your posts more, “pop”! Your content
is excellent but with images and videos, this blog could undeniably be one of
the very best in its niche. Excellent blog!
Here is my blog post :: ดูอนิเมะ
Keep on working, great job!
Also visit my web page: quarto
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-600kh100-mm-lts40s/
It’s actually a nice and helpful piece of information. I’m
happy that you just shared this useful information with us.
Please stay us informed like this. Thanks for sharing.
my web blog: Отели и гостиницы
Hi there to every body, it’s my first go to see of this blog; this weblog includes remarkable and actually excellent material for
readers.
Visit my website Order Cannabis Online UK
Танталовый прокат незаменим для химически агрессивных сред
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-vt35/list-titanovyy-vt35/
The other day, while I was at work, my cousin stole my apple ipad and tested
to see if it can survive a 25 foot drop, just so she can be a
youtube sensation. My iPad is now destroyed and she has 83 views.
I know this is totally off topic but I had to share it with
someone!
Here is my web-site; Buy Vape Carts UK
Excellent goods from you, man. I have understand your stuff previous to and you are just extremely excellent.
I really like what you’ve acquired here, really like what you’re stating and the way in which you say it.
You make it entertaining and you still care for to keep it wise.
I can not wait to read far more from you. This is really a terrific website.
Stop by my homepage: fraga kazino
My spouse and I stumbled over here by a different web address and thought I might as well check things out.
I like what I see so now i’m following you. Look forward to looking into your web
page for a second time.
Here is my blog; อนิเมะออนไลน์
Hi i am kavin, its my first time to commenting anywhere, when i read this paragraph i thought
i could also create comment due to this good post.
Here is my website :: rosinvestcom
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-otvody-press/mednyi-otvod-press-45-gradusov-17-mm-m2rm-gost-r-52948-2008/
Link exchange is nothing else except it is just placing the other person’s web site link on your page
at proper place and other person will also
do same in favor of you.
Also visit my homepage :: Above-Ground Storage Tank Design
Greate post. Keep posting such kind of information on your page.
Im really impressed by your site.
Hello there, You’ve performed an incredible job.
I will certainly digg it and individually suggest to my friends.
I’m sure they will be benefited from this web site.
Feel free to surf to my blog :: Ghostware
Good day! Do you use Twitter? I’d like to follow you if that would be ok.
I’m undoubtedly enjoying your blog and look forward to new updates.
My homepage – коллаген капсулы
Здравствуйте! Отличный сайт , успехов вашей команде!
стоимость укладки асфальта
Quality articles or reviews is the main to invite the visitors to
pay a quick visit the website, that’s what this site is providing.
Take a look at my web blog … монтаж вентиляции саратове
Возможность изготовления деталей по чертежам заказчика — это большой плюс
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-ti-6-al-7-nb—gost-r-iso-5832-11-2014/krug-titanovyy-ti-6-al-7-nb—gost-r-iso-5832-11-2014/
Очень широкий каталог, нашли всё необходимое в одном месте, включая редкие позиции.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnoe-litoe-koltso/latunnoe-litoe-koltso-1000kh400-mm-lmtska/
You actually make it seem so easy with your presentation but I find this matter to be
actually something which I think I would never understand.
It seems too complex and very broad for me. I am looking forward for your next post, I will try to get the hang of it!
Feel free to visit my blog post: End of lease cleaning
Its like you read my mind! You appear to know so much about this, like you wrote the book in it or something.
I think that you could do with some pics to drive the message home a bit, but
instead of that, this is magnificent blog. A fantastic read.
I’ll definitely be back.
Here is my webpage: read this article
Информация о доставке по всей РФ делает компанию универсальным поставщиком
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-nbti-46-5/folga-titanovaya-nbti-46-5/
Very good write-up. I definitely love this website. Thanks!
Here is my web blog – внедрение ии в бизнес
Чистота и прозрачность продукта напрямую зависят от
качества фильтрации. Фильтр-картон применяется в пищевой, фармацевтической и химической промышленности для эффективного удаления частиц и микроорганизмов.
Он подходит для очистки вина, пива, напитков, сиропов и других жидкостей.
Опорный картон поддерживает фильтрующий слой, а глубинный обеспечивает механическую и адсорбционную очистку.
Выбор подходящей марки позволяет добиться необходимой степени фильтрации — от удаления крупных примесей до глубокой очистки.
Используйте профессиональный фильтр-картон,
чтобы повысить эффективность производства и обеспечить стабильное качество продукции.
my blog post: https://www.artinweed.com/hello-world/
Качество сварочных материалов на высоте, электроды варят отлично, состав металла стабильный.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-88-9-mm-m1t-gost-r-52948-2008/
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/titan/rossiyskie-splavy-4/titan-40/poroshok-titanovyy-40/
Hi, I do believe your site could possibly be having browser
compatibility issues. When I take a look at your site in Safari, it looks fine however when opening in IE,
it has some overlapping issues. I merely wanted to give you a
quick heads up! Apart from that, fantastic blog!
My web-site slot88 resmi
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-132-mm-ls59-1/
Cabinet IQ
8305 Ѕtate Hwy 71 #110, Austin,
TX 78735, United States
254-275-5536
Warrantycountertops
Tətbiq həqiqətən də çox az yer tutur.
Here is my web blog … https://1xbetappaz.com/
Tətbiqi endirib xoşgəldin bonusunu aldım.
Also visit my webpage – https://1xbetyukleapk.com/
Никелевые сплавы — основа для жаропрочных конструкций
https://redmetsplav.ru/store/tantal-i-ego-splavy/tantal-t-10-1/prutok-tantalovyy-t-10/
Triangle Billiards & Bar Stools
1471 Nisson Ɍd, Tustin,
CA 92780, United Stɑtеs
+17147715380
Billiard Table Restoration Near Me Guide
Yükləmə prosesində heç bir reklam və ya virusla qarşılaşmadım.
Feel free to surf to my website … https://1xbetindirapkaz.com/
Can I simply just say what a relief to discover somebody who actually understands what they’re talking
about on the web. You definitely understand
how to bring a problem to light and make it important.
More people should read this and understand this side of
your story. I can’t believe you are not more popular
since you surely possess the gift.
My web blog; bandar togel
WOW just what I was looking for. Came here by searching
for apk slot gacor
my page: slot88 resmi
Спасибо команде за профессионализм и помощь в реализации нашего сложного промышленного проекта!
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/truba-monel/truba-monel-102kh10kh2000-mm-monel-400/
I have read so many articles on the topic of the blogger
lovers but this article is in fact a nice piece of writing,
keep it up.
My blog post; bandar toto
Cabinet IQ
8305 Stɑte Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Materialtrend
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/niobiy1/splavy-niobiya-1/niobiy-nbp-2b—gost-26252-84-1/polosa-niobievaya-nbp-2b—gost-26252-84/
When I initially commented I clicked the “Notify me when new comments are added” checkbox
and now each time a comment is added I get three e-mails with the same comment.
Is there any way you can remove me from that service?
Many thanks!
Visit my web page; 制服店幹部
Hello Dear, are you really visiting this web page regularly,
if so after that you will absolutely take fastidious know-how.
Review my web site – depo88
It is truly a great and helpful piece of info.
I am satisfied that you just shared this useful info with us.
Please keep us up to date like this. Thanks for sharing.
Review my web page; gambling slots virtual
This is my first time pay a visit at here and i am really happy to read everthing at one
place.
Feel free to surf to my webpage :: private server promotion
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-vtulka/latunnaia-vtulka-150-mm-lts40mts1-5/
I was able to find good info from your blog posts.
my web-site :: he said
Hi, I believe your web site may be having internet browser compatibility issues.
Whenever I take a look at your site in Safari, it looks fine however
when opening in Internet Explorer, it’s got some overlapping issues.
I merely wanted to provide you with a quick heads up!
Apart from that, wonderful blog!
My page; pepek mu 7 meter
Заказывали партию молибденовых листов для производства, качество металла идеальное, все сертификаты в наличии.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-64kh55kh1-4-mm-32-5kh34-5-mm-tverdaia-paika-m3rt-gost-r-52922-2008/
Cabinewt IQ
8305 Statye Hwy 71 #110, Austin,
TX 78735, United Stateѕ
254-275-5536
Bookmarks
It’s hard to find well-informed people about this subject,
however, you seem like you know what you’re talking about!
Thanks
My web site egypt sightseeing
Большой опыт работы, судя по копирайту с 2013 года
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mr-47zvp-1/list-molibdenovyy-mr-47zvp/
Why users still make use of to read news papers when in this
technological world the whole thing is accessible on net?
my page – helpdesk & ticketing software
Hello everyone, it’s my first visit at this site, and piece of writing is actually fruitful in support of me, keep up
posting these types of articles or reviews.
Here is my website :: 酒店幹部
We absolutely love your blog and find many of your post’s to be what
precisely I’m looking for. Would you offer guest writers to write content
for yourself? I wouldn’t mind producing a post or elaborating on many of the subjects you write in relation to here.
Again, awesome web site!
Also visit my page :: supply chain software
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-7×500-mm-l90-gost-931-90/
Продажа проволоки из тугоплавких металлов востребована в электронике
https://redmetsplav.ru/store/molibden-i-ego-splavy/molibden-mch-2/folga-molibdenovaya-mch/
It’s a pity you don’t have a donate button! I’d certainly donate
to this fantastic blog! I suppose for now i’ll settle
for bookmarking and adding your RSS feed to my Google account.
I look forward to new updates and will share this blog with
my Facebook group. Talk soon!
Feel free to visit my web blog; NSFW AI generator
This design is steller! You most certainly know how to keep a
reader amused. Between your wit and your
videos, I was almost moved to start my own blog (well,
almost…HaHa!) Fantastic job. I really enjoyed what you had
to say, and more than that, how you presented it. Too cool!
my page winslot
Закупали шлак ферросилиция для строительных нужд, материал качественный, без лишних примесей.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-zaglushki-pod-paiku/mednaia-zaglushka-kolpachok-pod-paiku-27-4kh23kh0-9-mm-9kh11-mm-tverdaia-paika-m1rm-gost-32590-2013/
I love what you guys tend to be up too. Such clever work and reporting!
Keep up the great works guys I’ve you guys to my own blogroll.
Feel free to visit my website :: inventory management software
Возможность заказа продукции в розницу и оптом (судя по описанию)
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-sismg4640-06—ss-144640/provoloka-magnievaya-sismg4640-06—ss-144640/
Hi! I realize this is somewhat off-topic however I needed
to ask. Does building a well-established blog such
as yours require a massive amount work? I am completely new to running a blog but I do
write in my diary on a daily basis. I’d like to start a blog so I will be
able to share my personal experience and thoughts online.
Please let me know if you have any recommendations or tips for new aspiring blog
owners. Appreciate it!
Also visit my page; custom software development
Hi there colleagues, its fantastic piece of writing
regarding teachingand fully defined, keep it up all the time.
Here is my page … NSFW AI image gen
Cabinet IQ
8305 Ⴝtate Hwwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Remoteconsult
If you wish for to obtain much from this article then you have to
apply these techniques to your won webpage.
my web page: score
I am sure this post has touched all the internet people, its really really good
paragraph on building up new web site.
Visit my web site :: have a peek at these guys
Редкие и тугоплавкие металлы всегда в наличии или под заказ в короткие сроки, рекомендую.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-1-4kh450-mm-lzhmts59-1-1-gost-931-90/
Thanks for your marvelous posting! I actually enjoyed reading it, you may be a great author.
I will be sure to bookmark your blog and will eventually come
back at some point. I want to encourage you to definitely continue your
great posts, have a nice morning!
Here is my web-site :: 酒店幹部推薦
Технические характеристики сплавов помогают инженерам в подборе
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-r60703—uns/pokovka-magnievaya-r60703—uns/
Have you ever considered about adding a little bit
more than just your articles? I mean, what you say is important and everything.
But think of if you added some great visuals or videos to give your
posts more, “pop”! Your content is excellent
but with pics and videos, this site could certainly be one of
the most beneficial in its field. Very good blog!
my blog post :: UDF file opener
This is a really good tip especially to those new to the blogosphere.
Short but very precise information… Thank you for sharing this one.
A must read article!
Feel free to visit my website – Yashua University
Высокий уровень сервиса и контроля качества, для нашего научного проекта это было критически важно.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednoe-dvukhrastrubnoe-koleno-pod-paiku/mednoe-dvukhrastrubnoe-koleno-pod-paiku-180-gradusov-53-6kh47kh1-2-mm-11kh13-mm-tverdaia-paika-cu-dhp-gost-32590-2013/
Every weekend i used to pay a quick visit this site, because i want enjoyment, for the reason that this this web site conations
actually nice funny material too.
Have a look at my page: neospin casino online
Howdy, i read your blog occasionally and i own a similar one
and i was just wondering if you get a lot of spam responses?
If so how do you stop it, any plugin or anything you can advise?
I get so much lately it’s driving me insane so any help is very much appreciated.
my web page :: Reddit API alternative
Описание складских позиций сокращает время ожидания ответа
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mgzn6th2zr—iso-3115/krug-magnievyy-mgzn6th2zr—iso-3115/
I was wondering if you ever thought of changing the structure of
your website? Its very well written; I love what youve got to say.
But maybe you could a little more in the way of content so people could connect
with it better. Youve got an awful lot of
text for only having 1 or two pictures. Maybe you could space it out better?
My web blog slon 2
It’s an easy way to earn cash back as an account credit when you shop, dine, or enjoy an experience
simply by using an eligible Wells Fargo credit card.13
Visit my blog post :: wellsfargo myoffer; https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8497656.htm,
After exploring a number of the articles on your site,
I honestly appreciate your way of writing a blog. I saved it to my bookmark website list and will be checking back soon. Please check out my web site as well
and let me know how you feel.
My web site nonton bokep indonesia
Офис в Екатеринбурге работает четко, забирали самовывозом — складская логистика на высоте.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-0-5×90-mm-l90-gost-931-90/
Быстрая навигация через «Карту сайта» для поиска глубоких страниц
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mg-al8zn1—iso-121/pokovka-magnievaya-mg-al8zn1—iso-121/
Thanks for finally writing about > Heel Pain – Plantar Fasciitis – Mr Will
Edwards < Liked it!
Feel free to visit my web-site bola hit
I am truly delighted to glance at this weblog posts which
contains tons of valuable information, thanks for providing such information.
my blog – download bokep indonesia
I take pleasure in, result in I found exactly what I was having a look for.
You have ended my four day long hunt! God Bless you man.
Have a nice day. Bye
Feel free to surf to my homepage … pedofil
wonderful issues altogether, you simply gained a new reader.
What might you recommend about your post that you made a few days ago?
Any positive?
Feel free to surf to my web-site – Highest buyback rate
Весь металл проходит строгий входной контроль, за всё время работы ни одного случая брака.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-40kh27-4-mm-m0b-gost-r-52948-2008/
Наличие кобальтовых сплавов заинтересует авиастроение
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mcin3—jis-h-2221/polosa-magnievaya-mcin3—jis-h-2221/
I dont think Ive caught all the angles of this subject the way youve pointed them out. Youre a true star, a rock star man. Youve got so much to say and know so much about the subject that I think you should just teach a class about it
My brother suggested I might like this web site. He was entirely right. This post actually made my day. You can not imagine simply how much time I had spent for this info! Thanks!
There is perceptibly a lot to identify about this. I consider you made some good points in features also.
This information is invaluable. How can I find out more?
my webpage: situs slot
Asking questions are actually good thing if you are not understanding anything totally, except this piece of
writing provides nice understanding yet.
Look at my webpage; NSFW AI image gen
It’s a shame you don’t have a donate button! I’d certainly donate to
this outstanding blog! I guess for now i’ll settle for bookmarking and adding your
RSS feed to my Google account. I look forward to new updates and will talk about this website with
my Facebook group. Talk soon!
Feel free to visit my page; villabetting
Most often since i look for a blog Document realize that the vast majority of blog pages happen to be amateurish. Not so,We can honestly claim for which you writen is definitely great and then your webpage rock solid.
Just came from google to your website have to say thanks.
Профессиональный подход менеджеров в Екатеринбурге, грамотно проконсультировали по техническим характеристикам сплавов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/latunnaia-polosa/latunnaia-polosa-0-4×250-mm-l80-gost-931-90/
Фольга из редких металлов часто требуется для высокотехнологичных лабораторий
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-7—bs-2970/folga-magnievaya-mag-7—bs-2970/
Have you always been concerned about these issues?
I feel that is among the so much significant info for me. And i am satisfied studying your article. However should commentary on some basic issues, The site style is ideal, the articles is in reality excellent : D. Excellent activity, cheers
There is a lot of misunderstanding about these issues today. Your material helps explain things.
Some truly nice stuff on this website , I like it.
It is not my first time to pay a quick visit this site, i am browsing this website
dailly and take good data from here all the time.
Here is my web-site … official site
I was very pleased to discover this site. I wanted to thank you for ones time for this wonderful read!!
I definitely loved every little bit of it and I have you saved as a
favorite to check out new information on your web site.
Feel free to visit my blog post … beverly yupoo Discount
Надежная защита груза при транспортировке, даже длинномерные изделия доходят без повреждений.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednyi-perekhodnoi-troinik-press/mednyi-perekhodnoi-press-troinik-76-1kh25-mm-m1r-gost-r-52948-2008/
Информация о доставке по всей РФ делает компанию универсальным поставщиком
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-mag-13—bs-2970/list-magnievyy-mag-13—bs-2970/
Just came from google to your website have to say thanks.
Howdy! Do you know if they make any plugins to
help with Search Engine Optimization? I’m trying to get my blog to rank for
some targeted keywords but I’m not seeing very good success.
If you know of any please share. Cheers!
my homepage: découverte musique française
Great blog here! Also your site loads up very fast! What web host are you using? Can I get your affiliate link to your host? I wish my website loaded up as fast as yours lol
Highly descriptive article, I loved that a lot.
Will there be a part 2?
Also visit my blog post – http://thdeco.com/bbs/board.php?bo_table=free&wr_id=496924
Simply wish to say the frankness in your article is surprising.
It’s going to be ending of mine day, except before finish I
am reading this fantastic piece of writing to improve my know-how.
Review my web page – Büroreinigung Innsbruck
My coder is trying to convince me to move to .net from PHP.
I have always disliked the idea because of the expenses.
But he’s tryiong none the less. I’ve been using WordPress
on several websites for about a year and am anxious about switching to another
platform. I have heard great things about blogengine.net. Is there a way
I can import all my wordpress posts into it?
Any help would be really appreciated!
Feel free to surf to my homepage :: game
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m16630—uns/lenta-magnievaya-m16630—uns/
Прозрачное оформление документов и быстрое выставление счетов, приятно работать с профессионалами.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/dvutavr-aliuminievyi/aliuminievyi-dvutavr-ak4-1-5x19x28-gost-13621-90/
Just stumble upon your blog from from time to time. nice article
It is a facility difficulty that will require a collective initiative from
all stakeholders.
Feel free to surf to my blog post :: website, Gregg,
I believe this web site has some really wonderful info for everyone : D.
Wonderful blog! I found it while searching on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo
News? I’ve been trying for a while but I never seem to get there!
Cheers
Here is my blog egypt visa application
Your style is unique compared to other people I have read stuff from.
Thank you for posting when you have the opportunity, Guess I’ll just book mark this web site.
Have a look at my page – Standby Generator Installation Destin FL
You write Formidable articles, keep up good work.
Hiya, I am really glad I have found this information. Nowadays bloggers publish only about gossip and net stuff and this is actually frustrating.
Раздел «Цены на металлы» полезен для мониторинга рынка
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m12410—uns/polosa-magnievaya-m12410—uns/
Удобный сайт и понятная навигация по каталогу, легко найти нужную марку стали или сплава.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-press/mednaia-dvukhrastrubnaia-press-mufta-14-mm-m1rm-gost-r-52948-2008/
Wonderful post however , I was wondering if you could write a litte more on this subject?
I’d be very thankful if you could elaborate a little bit more.
Many thanks!
My web-site: scam
Большой опыт работы, судя по копирайту с 2013 года
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-m11125—uns/truba-magnievaya-m11125—uns/
Ответственная компания, которая ценит долгосрочное сотрудничество, всегда идут навстречу клиенту.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/mednye-dvukhrastrubnye-mufty-pod-paiku/mednaiadvukhrastrubnaia-podvizhnaiamufta-pod-paiku40-5kh1-8mmm2rgost-32590-2013/
Modern Purair
416 Meridian Rd SE #14A, Calgary
AB T2A 1X2, Canada
(403) 800-7254
heating cleaning – https://moenusniae.raindrop.page/,
You are so cool! I do not believe I have read anything like this
before. So good to find another person with original thoughts on this topic.
Seriously.. thank you for starting this up. This website is one thing that
is needed on the web, someone with a bit of originality!
Check out my web-site: สโบเบท
After looking at a few of the articles on your
web page, I seriously like your way of writing a blog.
I book-marked it to my bookmark webpage list and will be checking back
soon. Take a look at my web site too and tell me
how you feel.
Feel free to visit my website egypt tour packages
Great post. I was checking constantly this blog and I’m impressed! Very useful info specifically the last part :) I care for such info much. I was looking for this certain information for a very long time. Thank you and good luck.
Сайт поддерживает английскую версию, что важно для экспорта
https://redmetsplav.ru/store/magniy-i-ego-splavy/zarubezhnye-splavy-2/magniy-lz145a—astm-b275/folga-magnievaya-lz145a—astm-b275/
Цены на спецстали одни из самых конкурентных на рынке, при этом качество на уровне мировых стандартов.
https://xn--80aeedb0bfzeok.xn--p1ai/catalog/melkhiorovaia-truba/melkhiorovaia-truba-34kh1kh11000-mm-mnzhmts10-1-1-gost-10092-2006/